p.€¦ · 2.1. definition of environmental sensitivities enwonmental sensitivities is aiso hown in...
TRANSCRIPT

Mount Saint Vincent University
Department of Human Ecology
Environmental Sensitivities: The Dietary fractices
and Beliefs of Women Sufierers.
by
P. Elizabeth Crawley
A Thesis
Submitted in fiilfilment
of the requirements for the degree of
Master of Arts in Human Ecology
May, 1999
Halifax, Nova Scotia

National Library 1+1 of Canada Bibliothèque nationale du Canada
Acquisitions and Acquisitions et Bibliographie Services services bibliographiques
395 Wellington Street 395. rue Wellington OttawaON KlAON4 Ottawa ON KI A ON4 Canada Canada
Your fi& Votre réference
Our fi& Notre rëfdrence
The author has granted a non- exclusive licence allowing the National L i b r q of Canada to reproduce, loan, distribute or sell copies of this thesis in microform, paper or electronic formats.
L'auteur a accordé une licence non exclusive permettant à la Bibliothèque nationale du Canada de reproduire, prêter, distribuer ou vendre des copies de cette thèse sous la forme de microfiche/nim, de reproduction sur papier ou sur format électronique.
The author retains ownership of the L'auteur conserve la propriété du copyright in this thesis. Neither the droit d'auteur qui protège cette thèse. thesis nor substantial extracts f?om it Ni la thèse ni des extraits substantiels may be printed or othehse de celle-ci ne doivent être imprimés reproduced without the author's ou autrement reproduits sans son permission. autorisation.

Environmental Sensitivities:
The Dietary Practices and Beliefs
of Women Sufferers
P. Elizabeth Crawley
May, 1999
COPYRIGHT @ 1999 P. ELiZABmH CRAWLEY

ABSTRACT
Diet therapy is a significant wmponent in the management of environmental
sensitivities (ES), yet there is little research evaluating the efficacy of these therapies.
Rotation and elimination diets supplemented with phamacological doses of vitamin and
minerals are the most common approaches. Those with ES hold strong beliefs about
w b t diet will do for them, but litîle is known about these kliefs and how they affect
eating behaviors. The objectives of this study are to determine if women ES sufferers are
meeting the nutrition recommendations outiined by Health and Welfare Canada (1 WO),
and to assess howledge, attitudes, and beliefs on the cause and treatrnent of ES.
Participants completed a validated, pre-tested 23-item intewiewer adrninistered
questionnaire and a four-day food record. Taped interviews are transcribed verbatim and
codeci; food records are analyzed for nutrient content and food group selection. The
Health Belief and Illness Behavior models predict how a person responds to illness and
provides the iÎamework to describe the lifestyle choices ES sufferers make in an effort to
regain health. Results frorn the 4-day food record indicate that, while the diet is typically
Nova Swtian, it lacks varïety and does not meet the recommended calcium intake.
Avoidance of irritants was the most common treatment moddity. Respondents
demonstrated strong beliefs in ES as a physicai iIlness and only believed îhose who
supported their illness. ES sufEerers reported lack of support by health care professionals
induceci feelings of fiustraîion and abandonment, that resulted in them turning aitexnative
therapists. Health care professionals must accept that ES is real to the sufferer and should
work with them and their alternative pracbtioners to guide them through recovery.
1 would like to take this opportunity to recognize those involved in making this
thesis a reality. First, 1 would like to thank my thesis advisor, Dr. Theresa Glanville, for
her guidance and encouragement throughout the course of this wo* as well as, my
committee members Dr. Janette Taper, Dr- Ilya Blum, and Dr. Anne Crane for their input
and direction provided to me over the last year. 1 would also like to t b d c Dr, Deborah
Nomk for W n g the time to reveal to me some of the mysteries of qualitative research
when 1 embarked upon this joumey.
1 would like to thank the women participants for taking the time out of their Iives
to becorne part of this researcb This truly wuld not have been accomplished without
their words.
1 would aiso Iike to th& my family for their continued encouragement this past
year, whom 1 am sure will be plemed they will no longer have to hear the word "thesis"
again. Last, but certainly not least, 1 want to thank Stephen for giving me his support in
so many ways over the years. You will never h o w what it has meant to me.

Table of Contents
L Introduction 1.1. Statement of Problem 1.2. The Research Questions 1.2.1. Research Objectives 1 The Delimitations 1.4. Signifiaance of the Study
II: Literature Review 2.1. Definition of Environmental Sensitivities 2.2. Etiology of Environmenîal Searitmties 22.1. Thenries for Organic Causes 2.2.2. Thenries for Psychotogical Causes 2.2.3. Theories on IlIness Belief System 22.4. Theory on Stress Manifestation 2.2.5. Theory on Misdiagnosis 2.3. Characteristics of ES Iiidividuals 2.4 Treatments for Environmental Sensitivities 2.4.1. Food Allergies and Hypersensitivities 2.4.1.1. The Principles of Total Load and Masking 2.4.1.2. AIlergy Testing 2.4.2. Diet Therapies 2.4.2.1. The Elimination Diet 2.4.2.2. The Rotation Diet 2.4.2.3. Vitamin and Mineral Supplementation 2-43. Antigen and Enzyme Regima 2.43-1. Antigen Therapy 2.4.3.2. Enzyme Therapy 2.4.4. Alternative therapies
III. Theoretical Framework 3.1. The Eealth Belief Model 3.2. The Illoess Behavior Model
IV. Methodology 39 4.1. Rationale for ushg quantitative and qualitative approaches 39 4.2. Sampling Technique 40 4.2.1. Contact Procedures 40 43. Data Collection Procedures 41 4.3.1. The 4Day Food Record 42 4.3.2. The Questionnaire 42
43.3. The Interview Setting 4.4. Analysis
V. Results of the 4Day Food Record and the Interviewer Administered Questionnaire
5.1. Demogra phie Information 5.2. Four-Day Food Record 5.3- The Ques t io~a i re Results and Discussion 53.1. Food Practices 53-2. Other Practices 53.2.1. Alternative Tbera pies 53.2.2. Nutrition Information 533. Knowledge, Attitudes, and Beliefs About Diet
VL Qualitative Analysis of the Interview Scripts 6.1. Symptoms and Allergies 6.1.1. Appearance of Allergies 6.1.2. Food Induced Reactions 6.1.2.1. Yeast and Sugar 6.12.2. Dairy Products 6.1.23. Processed Foods and Pesticides 6.12.4. Emotional Reactions 6.1.2.5. Other Food Related Symptoms 6.1.3. Chernical Induced Reactions 6.2. Cost 63. Traditional and Alternative Tberapies 63.1. Traditional Medicine 63.1.1. Lack of Support 63.1.2. Combining Traditional and Alternative Practices 63.13. Exprienees with Nutritional Professionals 6.3.2. Alternative Therapies 63.2.1. Participant Definitions of Alternative Therapies 6.3.2.2. Beliefs About the Impact Therapies Have on Health 63.23. Reactïons and Benefits from Alternative Therapies 6.3.2.4. Recommendations from Alternative Physicians 633.5. Coping Strategies 6.4. Avoidance 6.4.1. Food Avoidances 6.4.2. Avoidance of Social and Work Enviroaments 6.43. Avoidance and Fomily Behaviors 6.5. Information Gathering 6.6. Discussion of Illness Bebavior

7.1. Combining Quantitative and Qoaütative Findings 117 7.1.1. Credibility of Respondents 117 7.2. Mode1 of Interaction Between Re~pondents and the Environment 121 7.2.1. Eighüghts and hpücations of Findings 125 7.22. Concluding Remnrks 127
References Appendix A Idormation Sheet Appendîx B Participant Information Sheet Appendix C Informed Consent Appendix D 4Day Food Record Appendïx E Written Instructions Appendïx F Interviewer Administered Questionnaire

List of Tables
Table 1. Table 2. Table 3,
Table 4. Table 5. Table 6,
Table 7, Table 8. Table 9.
Table 10. Table 11 Table 12.
Table 13.
Example of a M a y rotational diet. 24 Example of a M a y rotation of food families. 24 Example of rotation of food families and foods within families. 24 Demographic Information. 47 Macronutn'ent Distribution o f the 4-Day Food Record. 49 The mean nutrient intake of the 44ay food record of rctnal intske and actual intake including supplemeatation. 53 Changes made to diet since diagnosis of ES. 58 Prior allergies of respondents. 60 New food allergies after diagnosis of environmental sensitivities. 60 Foods intentionally avoided by respondents. 61 Foods that have a negritive e f k t on health, 62 Responses to the questions pertaining to dietary kaowledge, attitudes, and beliefs. 64 Excerpts from the intemew scripts comparai witb actual food practices. 118

List of Figures
F r 1 The percentage of recommended daily servings per food groups for each respondent. 50
Figure 2. The % RN1 of selected nutrients calculntetl from the 4-day f d record for actual iatrke and impact of supplementation. 52
Figure 3. The 74 RNI oiseleced nutrients calculated from the M a y food record for actual intake and the impact of supplementation. 54
Figure 4. Distribution of where respondents shop for food. 59 Figure 5. Distribution of where respondenb obtain their nutrition
information. 64 Figure 6. Mode1 of the interaction between respondents and factors
that impact and influence their lifestyles choices. 121
.-- Vlll
CHAPTER 1: Introduction
1.1. Statement of Problem
Environmental semsitivities (ES) is a holistic disease influencing al1 aspects of an
individual's life. While etiology of the disease is controversia!, it is assumed that
exposure to environmental irritants initiates a chronic and reiapshg mdti-system, poly-
symptom disorder in susoeptible uidividuals.
Nunition therapy as a significant component in the management of ES. Clients
are often advised to follow rotation and elimination die& with pharmacologie vitamin
and minera1 supplementation. Although there are little scientific data to support diet
therapy, the underlying assurnption is that ES is exacerbated by nutrient deficiencies and
food-borne antigens that Burden the immune system. Despite the focus on diet therapy in
the treatment of ES, vimially nothing is known about the nutritional status before or
during treatment.
Chronic intake o f restrictive diets to reduce antigen burden and rest enzyme
systems may create secomdary nuirient imbalances. The debilitating nature of ES creates
a sense of desperation and clients may go to extremes to seek help. As a result, they
appear to hold strong beliefs about what diet will do for them, yet very little is h o w n
about what these beliefs are and how they affect eating behavior.

1 The Research Questions
1. Are the diets of women ES sufferers meeting Nutrition Recommendations
outliaed in the Report ofthe Scientific Review Cornmittee (HeaIth and Welfare Canada,
1 WO)?
2. What are the attitudes, knowledge, and beliefs of women ES sufferers on the
cause and treatment of ES?
1,2,1, Research Objectives
There are two research objectives for this study.
1. To obtain descriptive information using food records on the adequacy of diets
wnsumed by women with ES.
2. To assess the knowledge, attitudes, and beliefs about the role diet will play in
the cause and treatment of ES using an interviewer adrninistered questionnaire and
indepth interviews,
13. The Delimitations
This study was limited to women who were patients of the Nova Scotia
Environmental Health Center (NSEHC).
This study was limited to women who lived in central Nova Scotia.
This study was Iimited to women who can read and write English.
1.4. Signüicance of the Study
This study evaluated the dietary beliefs and practices of women ES sufferers to
dermine dietary adequacy and motivations infonning food and lifestyle choices.
Environmental sensitivities has yet to be recognked as a true organic illness, leaving
sufferers feeling fiustrated and abandoned by traditional health care professionals. This
study may help health care professionals understand the particular needs of ES sufferers
while maintahhg trust and contact with them. This research may help nuirition
professionals identi& potential nutritional concems, such as toxicity, deficiency, and
dietary imbalance. This study may also help nutrition professionals counsel ES sufferers
on dietary practices that fit within the Nutrition Recommendations advocated by Health
and Welfare Canada's recommendations and the ES sufferer's needs.

2.1. Definition of Environmental Sensitivities
EnWonmental sensitivities is aiso hown in the literature as multiple chemical
sensitivity (MCS), environmental illness (EI), environmental hypersensitivity, 20%
cenhiry disease, and total allergy syndrome. It is a condition characterized by fatigue,
malaise, dizziness, headache, lack of concentration, memory loss, and CC~paciness"
(Sparks, DanieII, Black, Kipen, Altman, Simon, & Terr, 1994). The most fiequently used
case definition of this disorder was coined by Cullen (1987) and includes four
components: 1) MCS is acquired in relation to some documentable environrnental
exposure that may initially have produced a demonstrable toxic effect; 2) symptoms
involve more than one organ system, and recur and abate in response to some predictable
environrnental stimuli; 3) symptorns are elicited by exposures to chemicals that are
demonstrable but very lovq and 4) the manifestations of MCS are subjective. However,
this definition has been criticized for being too narrow. Environmental sensitivities, as
defined by the Nova Scotia Environmentai Health Centre (NSEHC), is wnsidered to be
more inclusive than described by Cullen (1 987):
"Before the illness, the person was a fully functioning individual, with no
previous history of such syrnptomatology (or at least with no symptomatology of such
intensiîy). Other major iilness and psychiatrie disorder have been ruled out as a major
reason for the symptoms. The person has been exposed to high levels of toxic substances,
5
or chronic low levels of volatile organic compounds, eitheT indoor or outdoor. Exposure
is defined as being near, touching, smelling, breathing in, eating, drinking, swallowing or
injecthg a substance- The delay between exposure and symptoms rnay vary, and
symptoms rnay occur at levels which do not affect most people." (Sawler, 1997).
2.2. Etiology of Environmental Seiisitivities
Although a definition has described ES, the etiology of the condition the remains
the subject of great controversy in the literature. The debate is centered on whether the
cause is organic, psychological, or some combination of both.
2.2.1. Theories for Organic Causes
Disorder in the regulation of neurogenic inflammation, or inflammation of the
nervous system, has been suggested as an organic cause of MCS Weggs, 1993). With
neurogenic inflammation, mediators, including the neuropeptide substance P, are directiy
released fiom semry nerves to produce vasodilatation. edema, and other manifestations
of inflammation. A cell-surface enzyme, neutral endopeptidase (NEP), down-regulates
neurogenic inflammation by degraciahg substance P, however, this enzyme is inhibited
by cigarette smoke, viral infections and toluene diisocynate. Since exposure to certain
t o m depletes NEP, neurogenic inflammation persists, whkh could then heighten
response in subsequent exposures to chernical irritants.
As an alternative explanation, others believe that environmental chemicafs gain
access to the central nervous system (CNS) via the olfactory and limbic pathways
6
because these are not p&tected by a blood-brain barrier (Bell, Miller & Schwarh, 1992).
Repeated expsures to chemicals, such as lipid-soluble pesticides that cross the blood-
brain b&er, produce a kindling effécî. Kindling is the ability of a repeated and
intermittent stimulus that is initially incapable of eliciting a response to eventually
induce a motor seinire fîom later applications of the same stimulus (Bell et d, 1992).
The Iimbic structures, whïch are structures associated with olfaction, autonomie
fîmctions, and certain aspects of emotion and khavior (Dorland's Pocket Medical
Dictionary, 1995), are particularly vulnerable to kindling (Bell et al, 1992). Through
kinding, environmental chemicals trigger andor perpetuate affective and cognitive
disorders, as well as, related somatic dysfûnctions in vulnerable individuals- Some
attentional deficits fomd in MCS patients are consistent with the neuroanatomical links
between the olfactory system and the frontal cortex, suggesting that cognitive deficits
seen in MCS could be derived fiom low level chernical exposure via the olfactory-limbic
pathways.
In support of this, a study examinhg 32 solvent-exposed subjects found evidence
of neuropsychological deficits on measures of leaming and memory, visuo-spatial ability,
psychomotor speed and attention, and mental flexibility in a large number of the subjects
womow, Ryan, Hodgsoq Bi Robin, 1990). However, another study of 41 chemically
sensitive patients showed only slightly poorer performance on immediate verbal recall
than their controls, as well as, indistinguishable resdts on other measures of attention,
visual memory, visuo-motor speed and mental flexibility (Simon, Daniell, Stockbridge,
Clayple, & Rosenstock, 1993). While there is conflicting evidence regarding the

neurologie impact of repeated, low-level chernicd exposues, it appears h t m e r
research in human subjects would be required before the theory of limbic kuldling can be
either accepted or refuted
nie third theory for an organic cause of ES is that it is the result of some
immunologie injury. Several mecIianisms have been postulated. One theory is that
damage to T cells by environmental chemicals results in inversion of normal helper
suppressor T ceils ratios, which affects antibody production by B tells. As a . alternate
explanation, others believe that stimulation of T cells and phenotypic subsets by
environrnental chemicals results in cytokine release that can in tum affect appropriate
target cells in multiple organ systems, resulting in a wîde range of symptoms (h4cGovern7
Lazaroni, Hicks, Adler, & Cleary, 1983). However, there appears to be no firm evidence
that exposure to environrnental chemicals in trace amounts c m selectively damage helper
T cells, suppressor cells, or any other specific cellular component of the immune system
in patients with alleged MCS (Bell et al, 1992; Black, 1993; Fieder, Maccia & Kippen,
1992; Salvaggio, 1996; Sparks et al, 1994; Terr, 1986).
However, Rea and Ross (1989) state that environmentally sensitive patients oîten
present with white blood ceIl counts (WBC) below 4000/mm3 (normal range 4 100-
1 0900hm3) and eosinophil levels below SO/mm3 (nomal range 12-760 b w WC
counts indicate bone marrow depression perhaps due to viral infections or toxic reactions
(Clinicd Laboratory Tests, 1995). Low eosinophil count may exaggerate allergic
reactions (Marieb, 1995). hunosuppression could then lead to increased sensitivity to
environmental allergens.

While immunologie bult has k e n put forth as an organic cause of ES, well
controlled studies to support this theory are cuirently not available. Most recently the
focus of many scientific studies of ES is on the psychologicd profile of the ES patients.
2.2.2. Theories for Psychological Causes
Most reported studies have involved evduation of envûonmentally sensitive
individuals and their state of psychologic health both before and afier the insult. A study
of 26 EI patients found that 65% met the criteria for a mood, anxiety or somatoform
disorder, and that the number of DSM-III lifetime diagnoses in study subjects was
significantly greater among cases than controls @la& Ra* & Goldstein, IWO).
However, in a review of case reports and chart reviews, EI patients appeared to have a
different character structure from sornatization patients (Rosenberg, Freedman,
Schmaling & Rose, 1990). The authors suggest that EI patients appear to be primarily
obsessive / paranoid in character due to their ability to provide detailed, wmprehensive
histories of their illness. Terr's (1986) review of 50 cases of clinical ecology diagnosed
ES found that patients with long histories of multi-symptoms in multi-organs had clinical
features of hypochondriasis, sornatization, conversion hysteria, anxiety, depression, and
obsessive behavior. A study of chemically-induced illness of plastic workers fomd that a
history of psychiatrie morbidity predating the workplace exposure to chernicals was a
much çtronger predictor of the development of ES (Simon, Katon & Sparks, 1990).
However, al1 of these studies have been cnticized because their conclusions were based
exclusively on measmement instruments or strategies that could not distinguish

9
~ i s t i n g psychopathologie traits fiom either unexplained medical sympfoms or distress
caused by the m d c a l symptoms (Davidoff & Fogaw, 1994). While these midies found
tbe incidence ofpsychiatnc morbidity to be greater in ES dere r s , others contend this is
a response to living with a chronic illness. One study found that psychological distress
was higher among MCS patients than their musculoskeletal injury wntrol wunferparts,
but th is difference did not appear to pre-date the onset of chemicai sensitivity (Simon ef
al, 1993). This supports the notion that psychological disturbances are a result of the
chronic illness and are not necessarily the cause. The debate still continues about
whether ES is a psychiatric dishirbance whkh manifests itself as a medical condition, or
if it is a medical condition that has manifested psychiatric disturbances, in respaase to
physical stressors.
Regardless of the origin of the psychological distress, ES sufferers d l 1 need the
support of health professionals to mpe with the illness. Environmentally sensitive
patients do positively respond to psychological counseling that focuses on unconditional
support with a focus on developing healthy coping behaviors (Haller, 1993). This paper
suggests that therapy focus on helping patients lessen the impact the illness has on their
lives and not on avoidance of noxious stimuli. Success of treatment shodd be measured
by the patient's improved understanding of the impact of stress on his/her illness and by
the acquisition of new skills to cope with the illness' impact on his/her life. Thiç paper
also recommends that it does not serve the patients well to focus solely on the etiologic
debate and approaching trament fiom a purely psychological point of view may only
serve to alienate the patients and sabotage improvements. Although patients seem to

=pond best to a senous, non-judgmental approach, their treatment could be
compromised since the medical community has yet to recognize MCS as a syndrome.
In 1992, the Amencan Medical Association put forth a position paper stating
MCS should not be wnsidered a recognized clinical syndrome d l such time that
accurate, reproducible, and well-controlIed studies are available. In Nova Scotia, an
Advisory Committee on Environmental Hypersensitivity was set up in response to the
Camp Hill incident Camp Hill, a hospital in Halifax, had been plagued with poor air
quality and was suggested to be responsible for illness of over 600 employees (Jones,
1992). The Cornmittee agreed that patients were indeed ill; are of the opinion that
environmental hypersensitivity (EH) is a unisystemic condition involving the central
nervous system with symptoms referred to other body systems as secondary phenornena;
and conclude that causation and pathogenesis of patients suffering fiom these symptoms
are unknown, that the extent of involved neuropsychiatrie factors require m e r
quantitation, and as yet there is no effective management beyond general supportive
measures and treatment of concurrent illness (Nova Scotia Department of Health, 1997).
2.23. Theories on IUness Belief System
The active rejection by ES sufferers that their illness is psychologically-based has
ied to the theory that ES is an iiiness belief system. This purports that patients tend to
develop a lifestyle organïzed around their illness and becorne emotionally invested in the
concept of their diagnosis and tend to reject altemate explanations for their symptoms,
particularly psychological ones (Black, 1993). Brodsbq (1983) found that once the

11
intoxication was cited as the cause, patients began to believe that they had been seriously
h m e d and began to experience symptoms expected in toxic exposure or in an allergie
reaction This study also found that many EI sufferers searched for a sympathetic
physician who would give them this physically based explanation for their feelings- By
prolonging the claim and the symptoms, patients fulfill the need to preserve their
psychological integrity and the validity of their convictions (Brodsky, 1983). Finding a
supportive physician will M e r validate the belief that their illness is a r d , organic
condition,
Physician support can play an important role in shaping symptom expression by
patients. Shorter and mlleagues (1992) contend that psychosomatic symptoms becorne
attached to a disease label in phases. Initially, parailels are drawn between common
symptoms and a conventionally accepted disease. Then, sympathetic physicians, patient
support and advocacy groups, and the media publicize the etiologic connection, which
rnay lead to an increase in symptom attribution rather than an achial inerease in the
disease. This wouïd imply that society is seeing an increase on the incidence of
enWonmenta1 illnesses because people want to believe in their illness regardless of
whether it is supported by scientific evidence.
Clinicians have the power to influence the outcome of subjective testing and
potentially foster M e r illness behaviors (Jewett, PM, Fein, & Greenberg, 1990). This
study explored the validity of symptom provocation in a double blind study, and fond
that patient responses to active and placebo injections were indistinguishable. These
were patients who had symptoms consistently provoked during previous unblinded
12
testing with their clinid ecologist, uidicating that the influence of clinician suggestion
could play ai part in patient response. However, this shidy's design did not include
unblindeci testhg as part of its protocol so the innuence of suggestion wuld not be
isolated as an independent variable. The provocation-neutralization testing relies on
subjective reporting of symptoms, thus allowing ES seeters the oppomullty to validate
their illness, particdarly if they sense bias in the clinician.
2.2.4. Tbmry on Stress Manifestation
Inapmropriate symptom reporthg may also be Iinked to stress in patients' lives. A
siudy lookirrg at chronic low back pain and illness behavior found that inappropriate
symptoms were more important to women than men, and appeared to be the result of the
amount of pcsychological distress, the severity and chronicity of the physical problem, and
some social interactions (Waddell, Main, Morris, Paola, & Gray, 1984). Environmentally
sensitive patients present symptoms similar to those inappropriate syrnptoms described,
which were defined as symptoms that are generally vague, ill-localized, and lacking the
normal rela~onship to tirne, physical activity, and anatomy.
In termis of the developrnent of ES, a person experiencing stress rnay exhibit
heightened seositîvity to d o r s or respiratory tract irritants (Sparks et al, 1994). Bell and
colleagues (1 1992) note that novetty, foreignness, and perceived threat are key properties
of stimuli that a n induce tirnedependent sensitization to a wide range of stressors
including psychological and pharmacologïcal factors. Thus the nature of the sensitization
means that a previous acute toxic chernical exposure, or and emotional îraumatic event,

could initiate or increase vulnerability to MCS.
Stress has also been Iinked to the incidence of iIIness in the workplace. Neck and
back pain were shown to increase as perceived psychologid stress in the workplace
increased. m e r studies have linked high psychological demands in combination with
low decision latitude to cardiovascular disease (Am* 1996). These studies support the
notion that stress may be a cause or a risk factor in the development of illness. However,
like the debate with psychological manifestation, it is unclear whether the stress caused
the illness or if the stress response is due to living with the illness.
The Nova Swtia Advisory Cornmittee on Environmental Hypersensitivity (1997)
concluded that stress is an important factor in the disease as a potential initiating event,
or at Ieast a contributor to the negative experiences of sufferers. At thïs point, m e r
investigation is required to determine the role stress has in the development and
persistence of ES.
2.2.5. Theory on Misdiagnosis
Lastly, it has been proposed that chernical exposure is not the cause of ES, but
that it is a misdiagnosis of either a physical or psychological illness that has been
fbrthered by conscious or subconscious attempts by the patient and physician to avoid the
diagnosis of a psychiatrie illness (Black et al, 1990; Brodsky, 1983; Simon et al, 1990;
Sparks et al, 1994; Terr, 1986). Many researchers found higher levels of psychiatrie
symptoms and psychological distress in ES patients (Black et al, 1990; Simon et al, 1990,
and Terr, 1986). In parti*cular, development of ES symptoms was related to a wide variety

of psychiaîric symptoms across diagnostic categones, but showed the strongest
relationship with measures of long-standing distress (Simon et al, 1990). Concem was
raiseci that harm rnay result fkom ~~sdiagnosis and inappropriate trPatments that
subsequently have the potential to cause psychosocial, financial, occupational, and
psychological compiications (Black, 1993). n i e psychosocial implications a.se nom
patient withdrawal fiom society because of a perceived nsk of exposure to environmental
contaminants. There are far reaching h c i a l and occupational implications shce many
cannot work and have the expense of various treatments. Psychological complications
may result since patients are not receiving appropnate diagnosis and treatment of their
illness (Black et al, 1990; Sparks et al, 1992). Misdiagnosis also delays the onset of
proper treatment and prolongs the distress caused by the illness. The possibility that ES is
a misdiagnosed somatization disorder rnay relate to the general characteristics of this
population.
2.3. Characteristics of ES Individuals
Individuals with ES tend to be women (80-85%) between the ages of 30 and 50
years with a . average of 14 years education (Anthony & Maberley, 199 1 ; Black et al,
1990; Davidoff & Keyl, 1996; Fielder et aly 1992; Lax & Henneberger, 1995; Simon er
al, 1993). There have been several theories put forîh to explain the gender difference.
One study suggests the population is primarily women due to the preponderance of
women witb somatization disorder (Rosenberg et aly 1990), which supports the notion
that ES is a misdiagnosis of a psychiatrie illness. Others contend that women have lower

15
olfactory and identification detection thresholds than men, leaving women more
susceptible to chemical insult (Doty, as cited in Bell et al, 1992). Estrogen stimulates
other endocrine factors that also appear to contribute to the gender differences in
olfactory thresholds (Bell et al, 1992). This implies an organic cause since women may
simply be more sensitive to the environment around them-
Interestingly, another shidy that looked at sex differences in response to task
performance and odor suggestion found tbat women generaily performed better under the
suggestion of odor than men indicating that there are sex-based differences in response to
olfactory suggestion (Gilbert, Knasko, & Sabïnï, 1997). This appears to substantiate the
theory of ES as an ilIness Mief system, since the power of suggestion is again
manipulating task performance. These studies do support that gender is integral in the
development of ES, but there are others that argue it is not an issue.
In a sîudy comparing selfireporteci prevalence of dlergy and chemical sensitiviîy
of 1,027 respondents, those reporting chemical sensitivity were in d l age, gender,
income, race, and employment groups (Meggs, D m q Bloch, Goodman, & Davidoff,
1996). While only 3 8.8% of women reporied chemical sensitivity, respondents were
similar to ES sufferers in age and educaîion, i-e. 71% beîween the ages of 18 and 64
years, and 69% with at least 14 years of education.
2.4. Treatments for Environmental Sensitivities
Treatment of ES, like its etiology, is also rife with controversy. Dietary treatments
are based on the notion that ES sufferers have becorne sensitive to many foods, including
16
the additives in and pesticides on fOOdSOOdS The elunuiation diet is the typical treatment
used for food allergies and intolerances, while other less conventional therapies include
the rotational diet and antigen and enzyme regimes. filtemative îherapies, such as muid-
body therapies and homeopathy are also fiequently sought by ES sufferers. Many
treatments used for ES are considered morthodox, unproven, and meet with varyhg
degrees of success.
2.4.1. Food Allergies and Hypersensitivities
A food or gastrointesti-na1 allergy is mediated by an immunologie mecham-sm,
usually manifested by a skin reaction, in which the ingested antigen includes foods and
drugs. Food hypersensitivity is a state of altered reactivity in which the body reacts with
an exaggerated immune response to a foreign agent The terms food allergies and
hypersensitivities are used interchangeably. However, a food intolerance is the inability
to absorb or metaboiize ingested nutrïents (Dorland's Pocket Medical Dictionary, 1995).
There are four types of allergic reaction. Type 1 is an immediate, anaphylactic
type reaction tbat involves a response typically in Iess that 60 minutes. These reactions
may have different degrees of seventy depending on the shock organs affected For
example, d e n the shock organ is the nose, the reaction may be leaky nasal fluid When
the response is systemic (multisrgan), respiratory failure and severe hypotension, or
anaphylactic shock, could result In type II hypersensitivities, IgG or IgM binds to an
antigen on a ce11 membrane and activates compliment, resulting in a toxic eflect on the
ce11 or ce11 lysis. Immune disorden of this îype result in scleroderrna (hardening of the

17
skin) and rend diseases including systemic lupus. In type X I I , antibody-antigen complexes
deposit in tissues and activate wmplement- This is foliowed by release of chernotactic
factors, cell-innltration, and release of tysosomal enzymes, initiating a chronic
idammatory response. Type IV, or delayed, hypersensitivity results from the stimulation
of lymphocytes specificdly sensitized to the antigen Release of lymphokines causes
accumulation and activation of monocytes and macrophages, which M e r incites
cytotoxicity- Symptom severity is usuaily dose-dependent and may occur hours or days
d e r the exposure (Zeman, 199 1). It appears that the allergic responses most cornmonly
fornid in ES patients would be types 1 (non-anaphylactic), III, and IV. Many ES patients
do have family histories of allergies and ofien had allergies before the onset of ES
(AMA, 1992). Common food allergens include eggs, cow's milk, and shellfish, though
the rnajority are plants such as wheat, soya, and corn. Those allergic to plants are
typically allergic to plants within the same botanical family (Zeman, 1991).
2.4.1.1. The Principles of Total Load and Masking
Although allergies have been documented, food and chemical intolerances are the
most cornrnon cornplaints of ES sufferers. This has been explained by the principle of
total body load, a concept that is not well accepted by the medical community. The tobl
body load is the sum total of al1 pollutants taken into the body mess & Rea, 1990). The
ability to cope with the total load is supposedly unique for each person It is compareci to
a rain barrel, where a rain barrel can hold only so much water before it ovedlows, so too
can the body handle only so much pollution before a reaction occurs. However, reactions

18
may be masked simply because our bodies becorne accustomed to the presence of toxïns,
like one getting used to an odor in a room. De-masking involves avoiding exposure to the
sus@ chemical or food allergen for four days' followed by re-exposure. In an
unmasked state, the individual may have a clear and definable reaction to the exposure
making a cause and effect relationship detectable (Ross & Rea, 1990). Once the irritants
have been identified they cm be avoided to decrease the total load on the body- If
identification of these irritants is still unclear, other forms of testing may be used.
2.4.1.2. AIIergy Testing
Typical testing procedures include the RAST (radioallergosorbent test), the
ELISA (enzyme-linked immunosorbent assay), and skïn testing. Skin testing is most
cornmody used since it is less costly than the other in vitro tests. It involves the
application of dilute water-soluble suspensions of food extracts to the skin by a skin
pnck. If the recipient has IgE antibody to the food antigen, Iocd wheal-and-flare
reacîÏons typical of Type 1 hypersensitivity are produced (Metcalfe, 1985). However, this
type of testing commonly produces false positives in Type I hypenensitivities and false-
negatives in Type IV hypersensitivïties (Zeman, 1991)-
.The RAST measures the amount of IgE antibody to a specified antigen.
Measurement of radioactive anti-IgE atiached to the patient's IgE provides a means of
quantitating antigen specific IgE. However, this test strongly correlates with the level of
skin test reacttivïty to that antigen and, Iike the skùi test, tends to be positive for Type 1
sensitivities and negative for Type IV (Zeman, 199 1).

The ELISA also measures antigea-specific IgE and avoids the high costs and
radioactivity &izards associated with the RAST. An enzyme i s attached to the anti-IgE
and the enqmatic activïty is detennined by the wlor produced. The intensiiy of the color
is proportional to the Ievel of antibody which is measured b y a spectrophotometer
(Salvaggio, 1996). The ELISA has the same potential as the RAST in the identification of
food antigen-specific IgE (Metcalfe, 1985).
Given the restrictions associated with these tests, diet challenges are often given
to identi@ problem foods. In this procedure, suspect foods are eliminated fiom the diet
for three to four weeks or until the time that symptoms subside. Once this has occurred, a
large serving of one particular food is reintroduced at each meal for three days. If
symptoms recur, the food is removed fiom the diet. The patient then proceeds to the next
food item, and so on until al1 food allergens are detennined. During this time the patient
will keep a detailed food and symptom diary. Patients are rechecked periodicalIy to
determine any changes in the sensitivity (Zeman, 199 1). This is similar to the de-masking
protocol used with ES patients, though the underlying theory of total load is not
considered here. Based on the results of testing, patients may participate in different
forms of diet therapies.
2.4.2. Diet Therapies
Diet therapies are considered an essential form of treatment for ES sufferers.
Many are diagnosed with numerous food sensitivities and allergies and quite drastically
rnodi@ diet to avoid offending foods. While there are concerm over the adequacy and

20
variety of this diet, M e research ïnto actual food wnsumption by ES sufferers bas been
done. The diet therapies most commonly used are rotation and elimination diets dong
with substantial use of vitamin and mineral supplementaiion The basis of these diet
therapies in the treatment of ES is related to the prevalence of food hypersensitivities and
intolerances that may or may not have been diagnosed by convdonal means.
2.4.2.1. The EIimination Diet
Avoidance of the offending food is a typical practice for those who are deemed to
be allergic to a particular food item (Parker, Sussman, & Krondl, 1988). For ES
individuals, tolerance to a particular food may depend on the total load of the body at
that particular time, with the assumption king that the p a t e r the load, the greater
likelihood of food sensitivity. Avoidance of a particular food may also depend on
pesticides on the food, where the organic counterpart is often tolerated (Rea & Ross,
1989).
In a 1995 follow-up study of patients with MCS, 91% of subjects (n=32) reported
changing their diets (Lax & Henneberger, 1995). This has also been reported in
numerous other studies (Black et al, 1990; BrodsSr, 1983, Dismukes, Wade, Lee,
Dockery, & Hain, 1990; Rea & Ross, 1989; Terr, 1986). This suggests that many ES
sufferers are avoiding foods for fear of reactions, but linle is known about how this is
impacthg their nutritional state.
Avoidance of offending substances has been greatly promoted by physicians
practicing clinical ecology. Clinical ecologists are those physicians who believe
21
exposure to low levels of environmental substances present in the air or uigested fiom
foods and liquids causes, in susceprile ïndividuals, a variety of illdefined symptoms
affiecting nearly every organ system (AM& 1992). While there is a lack of well
controlled studies proving the efficacy of the treatment rnodalities advocated, many ES
sufferers are seeking out and abiding by the advice rendered by clinical ecologists. In a
review of 50 ES cases diagnosed by clinical ecologists, patients were advised to avoid al1
artïficial f d additives, and oflentimes specific foods containing mol& or yeast (Terr,
1986). However follow-up of these patients reveaIed that only two showed any clear
evidence of improvement, 26 were unchangeci and 22 were worse. The failure to produce
remission does not support the use of a v o i h c e as a means of treatment-
An important component of the elimination diet is ihe avoidance of yeast-
containhg and yeast-promoting foods, such as simpIe carbohydrates. The theory behind
yeast avoidance is îhat yeast (Candida albicam), in a weakened imrnunologicd state,
will proliferate uncontrollably in the body and release toxins, which the body can react
to, as well as increase the incidence of yeast infections. It is also believed that this
overgrowth contributes to inflammation of the gut, making it more permeable which, in
tum, allows food particles to pass into the b1oodsîrea.m and cause m e r sensitization to
foods (Lewis, 1995). Controlling the amount of yeast that enters the body through food
will supposedly decrease the total body load of yeast As well, by restricting yeast-
promoting foods, the yeast currenîly residing in the body will supposedly be stanred to
death (Mom-s & Stare, 1993). It is also believed that yeast will create craving in the body
for these sweets as a means to ensure continued growth (Lewis, 1995). However, îhe
22
evidence to support the impact of yeast overgrowîh on the body is purely mecdotal and
has yet to be proven using wefl-controlled studies ( A M . 1992).
Diagnosis of candidiasis is usuaily based on the patient's clinical presentation
and, although allergy testing is o h used for this purpose, laboratory tests are generally
not helpfül (Dismukes et ~2,1990). In a review of therapies, Morris and Stare (1993)
found no evidence that chronic fatigue syndrome (CFS) sufferers benefit fiom yeast
eliminating di& or are more prone to yeast overgrowîh and note a major concen that
these diets are nutritionally unbalanced. Dismukes et al (1990) conducted a 32-week
randomized, double-blind crossover stiidy looking at the efficacy of nystatin therapy for
presumed candidiasis hypersensitivity syndrome. They found no correlation between
positive vaginal and rectal cultures and systemic symptoms, which provideci additional
information that candidiasis hypersensitivity syndrome is not a verifiable syndrome.
Although there are still no clear data on the efficacy of tlie candida diet, many will
incorporate this into their other dietary regimes.
2.4.2.2. The Rotation Diet
Another form of dietary avoidance that is commonly recommended to ES patients
is the rotational diet. The basic premise of this diet, also called the rotary diversified diet,
is avoidance of fiequent ingestion of a food to which the person may be sensitive (Rea &
Ross, 1989). Proponeots of the rotation diet believe pemns rnay react to a food at any
time it is in their system, and that they are most likely eating food they are allergic to on
a daily basis. This does not allow the individual a chance to clear the reactions or identiQ
its source, since they are always reacting to something in the diet. It has been proposed
23
that food reactïons tend to unmask while on a rotation diet since the individual is eating
only one or two foods at each meal (Dallas -Environmental Health Center, n.d$ This
unmasking is based on the same principle used to first identifi fimi allergens describeci
earlier,
Although supporters of this diet regime aclaiowledge that the exact mechanism of
benefit is unknown, they psidate relief may be realized through enhanceci immune
fiuiction and detoxification pathways (Ross, 1992). In this case, poilutant injury may
increase usage of enzyme systems to nd the body of the chernical or antigen (Ross, Rea,
Johnson, Maynard, & Carlisle, 1990). By rotating foods, the toxic load on the body is
minimized and the enzyme systems can rest between exposures. Critics argue that îhere
is no scientific basis that enzyme systems perform better with rest and do not believe this
dietary strategy is sound ( . s & Stare, 1993)-
On a 4-day rotational diet, the same food is not eaten again for four days, and any
closely related foods are avoided for at least two days. The daily diet pattern repeats
itself starting on the fifth day (Rea & Ross, 1989). Four days is considered appropriate
for maximum b e l transit time, ensuring that the food has completely cleared the body
before it is ingested again. However, if the patient has chronic constipation a cycle longer
than four days is recornmended (Lewis, 1995). This relates back to the principle of
mïnimizing the total load on the body at any given time.
Following a rotational diet uui be quite wmplex A *al 4-day rotation diet
taken fiom a commody used popular literature resource is shown in Table 1. Here, foods
are also grouped into botanical food families. Foods within the same family should be
rotated since these foods tend to share comrnon allergens and could cause similar

reactions (Lewis, 1995). Table 2 provides an example of some foods that belong to
various families. Table 3, poitrays how these foods are than rotated every two days in a
44ay rotational diet
Table 1. Example of a 4-day rotational diet.
Table 2. Example of a 4day rotation of food families.
Taken @om Allerav and Candida Cookinn - Rotationai Style by Sondra Lewis, 1990-
D ~ Y I
broccoli
rice
D ~ Y 4
orange
beans
Day 1
broccoli
rice
Day 1 Grass Family
Day 2 Lily Family
rice
1 oat 1 leeks
D ~ Y 2
shrimp
potato
Day 2
garlic
spelt
Taken tiom AlIerav and Candida Cookina - Rotation4
Day 3
carrot
îurkey
s k m p
onion
carrot
cabbage 1 lima beans I Style by Sondra Lewis, 1990.
potato îurkey
broccoli
Table 3. Example of rotation of food families and foods *thin the families.
garbanzo beans
I rice I garlic I oat I Ieeks I I spelt I I =paragus I onion I millet * Taken fiom Aiier~vand Candida Cmkiqg - R o t a i i d Stvle by Sondra Lewis, 1990.
Day 4 Liiy Family
D ~ Y 3 Grass Farnily
Day 1 Grass Family
Day 2 Lily Family

25
Rotating food is supposed to protect the body fiom develophg new sensitivities.
Mer avoiding a food for a p e n d of the, the body may develop tolerance to the foods
which previously provoked reactions. However, this is not hue in d l cases, rneaning the
individuais rnay have to always rotate or completely eliminate a food fiom the diet
(Dallas-Environmentai HeaIth Center, ad). Rotation rnay also decrease the burden on
the detoxification p-thways. Further, oveme of certain enqme pathways may lead to
deficiency in vitamins that are utilized by that pathway (Ross, 1992; Rea, 1982). While
this is still unproven, it has lead to extensive use of vitamin and mineral supplementation
as a form of therapy.
2.4.23. Vitamin and Minera1 Supplernentation
Vitamin and mineral deficiencies rnay result fiom increased vitamin utilization in
enzyme systems, by direct toxic effect of pollutants, by malabsorption due to
gastrointestinal problems, or simply by Iimited intake as a result of food sensitivities
(Ross et al, IWO). Environmentdly sensitive patients rnay undergo weekly injections of
megadoses of vitamin and minerals with the intent to replete deficient nutrients. These
injections rnay co~tinue for years at varying intervals until the patient can retain
suffÏcient nutrients as indicated through blood testhg- In cornparison to traditional blood
nutrient analysis, the ES patient is not deficient (Grant Veldee, & Buchwald 1996; Ross
et al. 1990). However, proponents contend that while levels rnay be considered "normal",
these individuals have a need over and above what is considered sufficient (Ross et al,
1 WO).
Common vitamin and minerals evaluated are magnesiurn, seleniurn, vitamins A,

26
C, E, and the B vitamhs (Ross, 1992). These nutrients are the focus primarily because of
their oxidative properties, their utilization in detoxifjing pathways, and their role in
muscle fiindon and fatigue. Free radicals, generated fiom the accumulation of
peroxides, can interact with DNA and other macromolecules leading to molecular
damage. Vitamin C may act as an antioxïdant by converting oxidipng agents into
substances that may be excreted in urine. It c m also reduce the oxidized form of Vitamin
E thereby r e s t o ~ g antioxidant potenid. Vitamin E, the most important lipid soluble
antioxidant in the body, is considered to be the body's first line of defense against the
formation of peroxide derivatives of lipids. It is abie to prevent the chain reaction that
ensues fkom the attack of ffee radicals on the ce11 membrane, Vitamin E will also work
synergistically with seleniurn by sparing this trace element wïthin the body- SeIeniurn is
an integral part of the enzyme glutathione peroxidase which catalyzes the breakdown of
toxic hydroperoxides. Since there is a hc t ion overlap, the body's need for selenium
declines as the amount of vitamin E in the diet increases (Guthrie & Picciano, 1995).
Incidence of disease appears to be related to low levels of antioxidant nutrients in the
blood and diet While there is evidence that there is an inverse relationship between the
incidence of cardiovascuia. disease and the status of vitamin E and C, recommendations
regarding supplementation are pending results of long term intervention studies (Mahan
& Stump, 1995).
Magnesium deficiency has k e n linked to ES and CFS since they share many
symptoms, such as memory difficulties, depression, myalgias, and fatigue (Grant et al,
1996). A double-blind, randomized, placebo-controlled trial looked at red ce11
magnesium concentrations in CFS patients and how they responded to magnesium

27
therapy and found that, while the treatment group had only slightly lower magnesium
levels than the controls, magnesium treatment seemed to benefit patients' energy and
emotional status (Cox, Campbell k Dawson, 1991), To determine ifmagnesium
deficiency is present, patients are administered a magnesium load test and urine is
monitored for magnesium output, Patients are given doses of magnesium mtil the excess
is excreted, The amount retained is assumed to reflect the amount the individual is
deficient in magnesium. Magnesium retention decreased in patients who received
repeated intravenous infisions of magnesium or oral magnesium supplements as
compared to those given placebos (Gullestad, Dolva, Siriceland, Falch, Fagertun, &
Kjakshus, 1992). This suggests that rnagnesium stores may be norrnalized by intravenous
and oral magnesium supplementation. While this study did not evaluate the clinical
effects of magnesiurn supplementation, some patients did report positive effects and
others reported a dose-dependent lax bowel. To date, the efficacy of magnesium
treatment among ES patients has yet to be detennined despite its Mdespread use.
Supplemental vitamin C, folate and niacin are supposedly required to support
detoxification of pesticides, carbon monoxide, benzene, and other pollutants (Ross et al,
1990). A study on 333 men and women with ES reported that vitamin B, was insufficient
in 57.8%, vitamin C in 27.7%, vitamin A in 5.6%, niacin 2 1 A%, and folate in 32.2% of
the subjects (Ross et al, 1990). However, whiie these prcentages reflect individual
states, the mean levels of these various vitamins were either above or within normal
ranges used in this study. Criteria for deficiency was based on ranges obtained fiom
functional and direct vitamin assays of healthy controls that were taking no supplements.
Subjects were considerd deficient if they fell below these reference ranges. Although

28
statisticai signifrcance was not reported in this study, it does suggest that the deficiencies
reported were most Iikely marginal. As well, this study did not record the amount of oral
vitamin and mineral supplementation of the study group, so the impact this may have on
the results is unknown.
Contraxy to these findings, a study analyzing dietary intake and selected nutrient
concentration in CFS patients did not find consistent patterns of deficien-y or excess
between cases and controls (Grant et al, 1996). It was noted that while CFS subjects
more fiequentiy took vitamin and mineral supplements, dietary intakes and nutrient
concentrations were similar to those of the control group. This study does not support
routine nutrition assessrnents or a major therapeuîic role for vitamin and mineral
supplementation in CFS. Similar work is yet to be done with ES sufferers.
Supporiers of megavitarnin therapy suggest that individuais have a range of
biochemical requirements for specific nutrients, so megadoses of a nutrient may be
merely the minimum daily requirement of his or her particular body chemistry (Pfeiffer,
1975). This concept has been coined biochemical individuality. This theory holds that we
are d l biochemically and genetically unique and show tremendous variation in our
ability to tolerate infections, emotional stress, and chernical exposures (Rea & Ross,
1989). Part of one's ability to tolerate stressors may be dependent on how well one cm
absorb and use vitarnins and minerals in the diet. Those who cannot esectively absorb or
utiiize vitamin and mineds may have a greater requirement for these nutrients.
However, inberent in the RNI is the adjustment of the mean nutrient requirement by two
standard deviations to inçlude individual variability. It has yet to be proven that
megadoses of vitamin and minerals are efficacious.

29
A concern with vitamin and mineral N therapies is the possîbility of nutrient
imbalance in ES patients. Morris and Stare (1993) descrik typical vitamin and mineral
recornmendations for CFS sufferers which are far in excess of the Nutrition
Recornmendations (Health and Welfare Canada, 1990). Recommended daily intake may
be 100,000 IU of vitamin A (RN1 is 800 RE/ 2640 W/ &y), 10,000 mg of vitamin C
(RNT is 30 mg/day), and 800,000 lU of vitamin E (RNI is 6 mg/dl/day or 9 III).
Symptoms of toxicity for vitamin A have been reported between 16,000 RE (53,000 IU)
and 55,000 RE (183,000 IU) (Guthrie & Picciano, 1995). Vitamin C in excess of 1 g/day
can cause abdominal distress and diarrhea in some subjects (Heakh and Welfare Canada,
1990). Vitamin E may cause intestinal disturbances a? intakes greater than 1 g/day (1 500
rU)(Health and Welfare Canada, 1990), although the body adjusts to ùicreased intake by
decreasing absorption. However, vitamin supplementation given intravenously bypasses
the ability of the gut to protect agauist toxicity by decreasing absorption. This has the
potential to exacerbate existing symptoms and place the individuals at risk of toxicity. As
well, it may be considered easier for ES saerers to get their nutrition via injection rather
than through their limited food selection. This type of therapy may not encourage those
practicing avoidance to reintroduce foods into their diet which can further compromise
nutritional balance,
2.43. Antigen and Enzyme Regimes
Antigen and enzyme therapies are intended to desensitize individuals to imtants.
They include desensitization to foods, grasses, weeds, pollen, etc., but do not include
chemical desensitization.
2.4.3.1. Antigen Therapy
Antigen therapy is an alternative therapy used to alleviate allergic reactions- In
this test, symptoms are invoked by giving an intracutaneous injection of a dose of a food
extract. Once injected, patients record symptoms occuming during a ten minute period
immediately following the administration of the dose. TypicaI responses include
headaches, miilaise, dizziness, depression, gas, discodori, memory loss, anger, or
bloating To neutralize these symptoms, the patients are given decreasing doses of the
same food extract, until the symptoms disappear (AM4 1992; Jewett et al, IWO). The
solution that relieves the symptorns is referred to as the neutralizing dose. Patients may
then buy bottles of the antigen neutralizing dose and administer it as sublingual drops to
circurnvent any future reactions to that particular antigen There has been much
controversy in the literature over the efficacy of this technique (AMA, 1992; Jewett et al,
1990; Metcalfe, 1985; Terr, 1986)- One study found subjects were unable to distinguish
between active dergens and placebo when administered in a double blind setîing,
suggesting that symptom reporting can be înfiuenced by the individual administering the
test (Jewett- et al, 1990). Another complaint is that specific sensitivities are diagnosed by
the appearance or disappearance of subjective symptoms and then treatment is based on
these results (Black, 1993)-
2.43.2. Enzyme Therapy
Enzyme potentiated desensitization (EPD) is a therapy currently used at the
NSEHC with varying degrees of success- The therapy involves a standard injection every
two months of small arnounts of antigens for the purpose of strengthening the immune
31
system to cornmon allergens, including foods, mold, grasses, weeds, etc. This is done
periodically to continually boost the immune system. Persons on the EPD regime must
follow a diet including specific supplements prior to the injection, followed by a strict
diet during the week of the injection that typicaily includes foods not as ailergenic, such
as potato, h b and wild game @ d e 7 1994)-
2.4.4. Al ternative thera pies
Vincent and Furnham (1996) found the major reasons why people seek altemative
therapies include lack of effectiveness of orthodox medicines, a belief that
complementary medîcine will be effective, valuing the emphasis on treating the whole
person, and wanting to take an active part in maintaining their health. Similar results
have been found in other s u e s (Furnharn & Bhagrath, 1993; Montbriand, 1995;
Sollner, Zingg-Shir, Rumpold, & Fritsch, 1997).
Since conventional medicine has yet to agree that ES is an illness, many sufferers
turn to alternative methods of support and treatment (AMA, 1992). At the NSEHC, they
currently offer a Freeze-Frame course that involves ways to cope with the stresses of
living with a chronic illness. Therapeutic touch, sunilar to reike, is another therapy
offered that addresses the emotional and spiritual component of healing Cranial sacral
îherapy is a non-invasive technique also used in the treatment of chronic illnesses.
Homeopathy is one of the most widespread and controversial of the alternative therapies
(Linde, Clausius, Ramirez, Melcharî, Eitel, Hedges, & Jones, 1997)
Homeopathy has two main theoretical tenets king the principle of similars and
the use of dilutions called potencies. Thc principle of similars purports that a patient with
32
particular signs and symptoms can be c d if given a dnig that produces the same signs
and symptoms in a healthy individual. The second principle is that remedies retain
biological activity if they are repeatdy diluted and agitateci between dilutions. These
dilutions are said to produce effects even when no original molecules of the starting
substance remain (Hahnemann, 1982)- There is considerable speculation on how a
solution "remernkrs" information fiom the original substance (Linde et al, 1997).
Homeopathy is wmprised of the cIassical and cornplex approaches. Classical
homeopathy matches a toxic symptom of an herb or animal remedy against the patient's
symptoms. The remedy is then given in a very dilute fom. Cornplex homeopathy
involves giving a mixture of various berbal and homeopathic products to treat a patient's
syrnptoms -th & Watkins7 1996). While the clinical benefits of homeopathy are
quite controversial, results fiom a rneta-analysis of placebo-controlled trials did not
support the hypothesis that the clinical effects of homeopathy are completely due to
placebo (Linde et al, 1997). However, there was insufficient evidence to determine if any
one homeopathic treatment is clearly effective in any one clinical condition Regardless
of the lack of scientific validation of these alternative therapies, many studies have found
that health beliefs will inform the therapy sought (Fu- & Bhagrath, 1993; Furnham
& Kirkaldy, 1996; Kelner & Wellman, 1997).

CHAPTER 1II:THEORETICAL FRAMEWORK
The theoretical framework used to interpret the qualitative data involves the
application of the Health Belief Model and the Iilness Belief ModeI. Using both allows
for a more comprehensive explanation of the health behaviors exhiiited by participants
that are airned not ody at promoting heaith, but also coping with illness.
3.1. The Health Belief Model
Further insight into how individuals with ES make behavior choices, such as
alternative therapies, can be gained by applying the six concepts of the Health Belief
Model (HBM). The HBM has been used both to explain change and maintenance of
health behavior and as a guiding fiamework for health behavior interventions (Stretcher
& Rosenstock, 1997).
The first concept, perceived susceptibility, measures an individual's subjective
perception of his or her own risk of contracting a health condition. In the case of a
medically established illness, it includes the individual's acceptance of the diagnosis,
personal estirnates of resusceptibility, and susceptiiîlity to illness in general. One study
looking at student supplement use found that -dents believed extra vitamins were
needed when people felt tired and that vitamin C can prevent col& (Eldridge & ~hee-han,
1994). Environmentally sensitive patients believe they are susceptible to various
environmental exposures and wili take action, like avoidance and home renovations,
based on this belief (Terr, 1986).
34
Perceived sever*, the second concept, addresses the feelings conceming the
senousness of contracthg an illness or leaving it untreated. Tt includes evaluation of
medicai and clinical consequences and social consequences. The combination of
susceptibility and severity is labeled perceived threat. Extensive dietary manipulation has
been demonstratted in pemm d o perceive c e h foods cause adverse reactïons,
regardless of whether the diagnosis has been confirmed (Parker et al, 1993). Those with
ES will often avoid social settings for fear of exposure and subsequent reactions (Fiedler
et al, 1992)-
Many ES sufferers will engage in health behaviors that have perceived benefits,
the third HBM concept The particular course of action to the perceived threat will
depend on beliefs regarding the effectiveness of the available actions to reduce the threat
of disease. Environrnentally sensitive individuals will ofien go to great lengths in the
pursuit of health. Costly treatments, home renovations, and special diets are al1 actions
based on the belief that it will benefit them in some way (AM& 1992; Terr, 1986).
Perceived barriers, the fourth concept, are the potential negative aspects of a
kath action that may impede assuming the recommended health behavior. In a study
exploring the dietary management of ES, cost and time constraints were sighted as major
barriers to meeting food needs, while diet and nutrition were wnsidered essential for
recovery (Kiley-Mullally & Glanville, 1998).
Cues to action, the fïf& concept, suggests that cues can trigger behavior, such as
bodily or environmental events like media and publicity. This would appear to be similar
to the illness belief system theory. Proponents of this theory purport that the media
reinforces beliefs that can result in increased syrnptom association and subsequent

behavior change (Sparks et al, 1992). This concept has yet to be fully iavestigated
because of the difficulty in determinhg the cues that elicits behavior change.
Lastly, ~e~efficacy, is defined as the conviction that one can suecessfully
execute the behavior required to produce the outcornes (Bandura, 1977). The lack of
efficacy is then considered a perceived barrïer to taking the recommended action The
authors note that while selfefficacy was not explicitly incorporated into the original
version of the HBM, the Iiterature supports the importance of self-efficacy in accomting
- for initiation and maintenance of behavioral change. Self-efficacy is a powerful predictor
of health behavior (Abusabha & Achterberg, 1997). It has been linked to choice of
alternative health practices (Furnham & Kirkcaldy, 1996), cancer treatments (Sollner et
al, 1997), and chronic fatigue treatments (Ray, Jeffenes, & Weir, 1997).
The HBM has been used in various studies to demonstrate how beliefs influence
dietary choices. In a study evaluating the diet-cancer beliefs found that respondents
between the ages of 35 to 59 had the strongest belief in the association of diet and cancer
and had the most knowledge about the National Cancer Institute recommendations and
food composition (Pattenon, Kristal, Lynch, & White, 1995). Another study looking at
food safety behavior found that respondenîs who perceived d e food as a personal
threat, who had higher self-efficacy, and were hi& in health motivation were
significantly more likely to engage in food safety behaviors than were respondents who
scored low on these measures (Scbafer, Schafer, Bultena, & Hoiberg, 1993).
Interestingiy, females were more likely to be active in food d e t y behaviors than men.
This study supported the use of the HBM to predict food safety behavior.
The HBM is an appropriate Mework to describe the dietary behaviors of

women with ES. The research previously outlined dernonstrates its usefulness in
descniing how beliefs about health inform both fd-related and lifestyle behavion.
However, hedth beliefs are not the only motivation for the actions and behaviors of ES
sufferers. Behavior is also motivated by the beliefs individuals have abut their illness
and their treatment optiofls-
3.2. The nlness Behavior Model
Illness behavior is an individual reaction to symptoms and illness involving
psychological, environmental, and socio-cultural factors that affect such reactions. It
refers to the way individuals respond to bodily indications, how they monitor intemal
states, define and interpret symptoms, make attn'butions, take remedial actions and
utilize various sources of forma1 and informal Gare- This is important because it shapes
the recognition of the illness, the selection of patients into case, the degree of
compatibility between patients and physician amibutions, patterns of healîh practice and
adherence with medical advice, and the course of illness and the treatment process
(Mechanic, 1995).
Illness is not only a physical state, but may be a means of coping with life's
adversities . Sickness could be used to excuse failure and explain disappointment
(Mechanic, 1995). Employees with psychologically demanding work and those feeling
underutilized in their job are more likely to suffer fiom neck and back pain than those
who do not have this perception of work (Arnetz, 1996). Environrnentally sensitive
suffierers may withdraw from work under the guise the environment is making them ill,

as a means of coping with workplace stressors.
Illness may justi@ release fiom expected social roles and obligations (Mechanic,
1995)- Avoidance is the comerstone in the treabment of ES and patients often withdraw
fiom social settings in fear of exposure to toxic substances (Black, 1993). It is possible
that ES sufferers are obtalning a benefit by king ill.
Sickness could be used to just* sympathy, assistance, and dependence. Chronic
fatigue sufferers have an enormous stake in how its illness and cause are constnicted not
ody to achieve the Iegitirnacy necessary to make various entitlernents accessible, but
alço to elicit sympathy, avoid sti-gma, and protect self-conceptions (Mechanic, 1995). An
evaluation of 70 Worker's Compensation claims of toxic exposure found that some
respondents gained psychological cornfort and connol in their disabled lives (Brodslq,
1983). This sarne study reported respondents wanted vindication and societal
acknowledgment that they were b m e d at work
Interestingly, gender differences in heaith behaviors exist- Women were shown to
have more days of IOW activity due to illness, more bed &YS, discussed their health with
more people, and had greater utilkation of medical seMces than men (Kandrack, Grant,
& Segall, 1991). However, thïs study failed to find gender differences in response to
iliness, preventative health beliefs, and attitudes toward self-reliance and medical
skepticism This suggests k t women tend to engage in more health protective
behaviors, such as reducing activiîy level, staying in bed, and seeking medical attention
when they are sick It is not surprising then that more women are diagnosed with ES than
men, since women are more aggressive in their search for medical treatment.
Understanding illness behavior is essential to adequately explore the motivations
38
that S o m the actions of women ES sufferers. This theoretical h e w o r k will be used
to place the women's words in the context of living and wping with a chronic illness,
while the HBM explains why the women are also engaging in health preventafïve
behaviors for themselves and their families.

CHAPTER IV: METHODOLOGY
4.1. Rationale for using quantitative and qualitative approacbes
This research study was undertaken to descni the dietary practices of women
and to determine what motivates their food selection and eaîing behaviors.
Quantitative measures were used to descni the diets of the women for
macronutrient distniution and vitamin and mineral composition to determine the
adequacy of their diets in meeting the Nutrition Recommendations outlined in the report
of the Scientific Review Cornmittee (Health and Welfare Canada, 1990). This research
will provide dietitians and nutrîtionists with valuable information about whaî ES
sufferers are actually eating and where the potential rkk areas are for these women.
Qualitative measures were used to fiirther explore the knowledge, attitudes and beliefs
that inform their food and lifestyle choices.
Using a combination of quantitative and qualitative research methods is unique
since it not only provides the necessary descriptive component of the data, but also
mainîains the contextual detail of the data. Linking these meth& is a means to
capitalize on the strengths of both approaches in order to gain a broader perspective of a
particular phenornenon (Carey, 1993). Only by knowing the motivation behind dietary
choices can we begin to understand the challenges faced by women with ES and work
with them to ensure nutritional balance.

4.2. Sampling Technique
Convenience sampling was used to acquire 12 subjects for this study. In this
study, subjects were selected to be typical of those suffiering with ES. Subjects were
female, between the ages of 30 and 50 years, with a verified dîagnosis of environmental
illness fiom the Nova Scotia Environmentai Health Centre (NSEHC).
4.2.1. Contact Procedures
Al1 women volunteered to be part of this study. Information was left at the
NSEHC, at a health food store patronized by ES sufferers, and at two doctors' offices
that were known to treat ES sufferen. This provided information about the study and on
how to contact the researcher through phone or e-mail. Patients visiting at the NSEHC
could pick up an information sheet (Appendix A) about the study that contained a contact
phone number or they could fil1 out a Participant Information Sheet (Appendix B) and
leave it at the front desk. The c h i c was periodically contacted to collect names of
volunteers. During the initial contact, al1 women were ùIformed of the intent of the study
and what was expected of them if they were to participate. They were assured complete
confidentiality and tbat theû responses were by no means intended to judge their
behavior. This was an important point since many ES sufEerers have not had their illness
recognized or taken seriously by health Gare professionals.
Al1 potential participants were informed at the initial contact that the interview
was to be taped, although they were not obliged to consent to taping. They were UIformed
that if they chose to be taped, the recorder could be tumed off at their request at any time
41
throughouî the interview and that they would have a chance to revïew the transcribed
typed interview. They were assured that only the researcher wodd have access to the
tapes and know the identity of the participant and that al1 tapes would be erased at the
completion ofthe study. Participants were uiformed that any potentially identifying
information would be changed, i.e. name, occupation. family member names, etc. before
releasing any of the results. Participants were also informed that they codd withdraw
nom the shidy at any time without fear of reprisal.
Al1 participants were informed that this midy received approval f?om the Ethic
Review Committee of Mount Saint Vincent University and was k i n g conducted by a
graduate student as part of the requirements for the Master's of Arts in Human Ecology
degree of the University. Participants were also informeci that this work was supported by
the Canadian Foundation for Dietetic Research, and while this study was not endorsed by
the NSEHC, the c h i c was aware of, and supported, it.
Once the women agreed to participate in the study, arrangements were made for a
pefson-to-person meeting at a place and time that was convenient and cornfortable for
them, The women were assured that the interviewer would be scent-fiee and they were
questioned about any parîi~uiar sensitivities that the intewiewer should be aware of ALI
women signed a written informed consent fom (Appendix C).
4.3. Data Collection Procedures
Food inbke and information on dietary attitudes and beliefs were collected
through the use of 4-day food records and an interviewer administered questionnaire.
42
43.1, The 4-Day Food Record
Food intakes were assessed using 4-day food records. Participants were provided
with a standardized colordeci form (Appendix D) that differentiated each &y with a
different color and participants were prompted to fil1 in the amounts, food items for each
med period including snacks, and the time of &y the meal was consumeh Participants
were provided with verbaI instructions on how to complete a food record and were left
wrïtten instructions (Appendix E) accompanied by the researcher's home phone number
if they had any questions dwing the 4-day period. Participants were asked tu provide
recipes of any combination meals they had and the portion they consurned using common
household measures. Al1 were instnicted not to change their usual eating patterns during
this time. Those following a rotational diet were instructed to begin their food record on
Day 1 of their diet and those not following the rotational diet were instructed to record
three weekdays and one weekend &y.
43.2. The Questionnaire
Background information was gathered on the participant's history of ES through a
personal intem-ew, using a combination of closed and openended questions in an
inte~ewer-administered questionnaire (Appendix F). Al1 i n t e ~ e w s were tape recorded
and responses were also band recorded directly on the questionnaire. The questionnaire
addressed demographic information, i-e. age, education, occupation; information on pre-
existing and current allergies, symptoms associated with exposures and the recurrence
pattern of these symptoms; types of dietary intervention, both formal and informal;
vitamin and supplernent use and perceiveci benefits; traditional and alternative methods
43
of treatment, their experiences and rationaie behind their choices; where they shop for
food and why; and food preparation techniques and perceived benefits. The participant's
bowledge and attitudes on diet and health, source of nutrition information and why, and
perceived impact of diet were also addressed. Changes in family eating patterns and
social activities were assessed, as well as, the burden of cost and energy associated with
this lifestyle.
The questionnaire was reviewed by health professionals (Le. dietitian, the
Research Associate and Director of the NSEHC, and a nurse at the NSEHC) working
with ES patients to establish content validity and revisions were made based on their
input The questionnaire was then pilot tested with ES individuals not part of the study
sampie to ensure that the questions were mutuatly understood by the in te^-ewer and the
respondents; that the questions were not considered offensive by the respondents; to
establish a time line for the questionnaire; that the protocol facilitated dialogue; and that
the questionnaire produced the quantity and quality of information expected and desired
(Shepherd & Achterberg, f 992).
Question 1 established the length of time the respondent was a patient at the
NSEHC. Quesiions 2 to 4 detennined changes to the diet and its preparation. Questions 5
and 6 examined where the subjects purchased their food and its impact on the cost of
their grocery bill- Question 7 addressed the seasonality of their food purchases. Questions
8 and 9 established the history of food allergies both pre- and pst-diagnosis of ES.
Questions 10 and 1 1 expiored respondents' beliefs on how the food they consume affects
their heaIth and any foods that are intentionally avoided. Question 12 addressed
supplement use. Questions 13 and 14 asked about the various therapies respondents

44
engage in and what they believe îhose therapies are doing for them. Question 15
determined the source of nuirition information- Question 16 explored their belief in diet
and health Questions 17 to 20 collected demographic information including age,
education, and ernployrnent history. Question 2 1 explored the association between
partïcuiar food items and its perceived b m f i d effect using questions adapted fiom a 7-
item questionnaire developed to measure the readiness variables that motivate food
safety action (Schafer, Schafer, Bultena, & Hoiberg, 1993). Questions 22 and 23
investigated the knowledge and attitudes of ES sufferers on food and health and were
adapted fiom the Nova Swtia Heart Health Survey (1 995) and based on the previous
work of Kiley-Mullaly and Glanville (1 998) which expiored bamiers faced by women ES
sufferers-
43.3. The Xntewiew Setting
To ensure the interview was conducted in an environmentdly safe and convenient
location, interviews were conducted in the participant's home (n=ll) or at the NSEHC
(n=l). One interview was conducted outside on the participant's deck. For al1 interviews
we were alone and generally undi* In three instances the participants took phone
calls during the interview and the tape recorder was turned off for that time and the
interview was resurned at the sarne point pnor to the d l . During another interview, the
intewiew was intermpted three times with the arriva1 and deparîure of family members.
Again, the i n t e ~ e w was resumed at the point of the disruption On average, interviews
lasted 1.5 hours.
45
4.4. Aiulysis
The analysis of the food records included a complete macro- and micro-mutrient
d y s i s using the QCLNüTS (Quilchena Consulting Ltd., Victoria, B.C.) nuirient
analysis program. The four days were entered individually and the mean intake mf the
four days was detemiined
Results corn the closed-ended portion questionnaire were organized in a n ExcelC
(Mïcrosofi Corporation, 1997) spreadsheet Data were then descnbed using mean and
standard deviation-
Results fiom the open-ended portion of the questionnaire were transcribed
verbatim and coded for emerging themes. Three interviews were transcnï by çomeone
other than the researcher. However, the researcher reviewed these transcripts while
listening to the three tapes'ïhis was not done with the remaining nine transcripts, since
the act of transcribing ailowed the researcher to hear the women's words spoken in
context and with the intended meaning. Al1 transcripts were reviewed individualEy and
notes were hand recorded in the margins to describe the general meanings behind the
participants' comments. B a d on these notes, major categories were constnicted that
linked themes within the transcript of one participant and between participants. A l 1 text
relevant to these categories was then copied to a word processing file under the
appropriate heading- Each file was then m e r reviewed for themes emerging Wnthin the
major categories, and separate files were d e for each of these sub-categories. Analysis
of the sub-categones continued in the same marner until no M e r themes emerged, at
which point, synthesis occurred.
CHAPTER V: Results of the 4Day Food Record and the Interviewer Admiaisterd Questionnaire
5.1. Demographic Information
A target sample of twenty women was arbitrarïly selected with the ùitent of
establishing response categones with a minimum of five participants per groups. Twelve
women completed the intewïew and food records. Al1 respondents are or were patients of
the NSEHC. Participants were similar to the typical ES population for gender, age, and
education (Black, 1990; Lax & Henneberger, 1995; Terr, 1986). Ages of respondents
ranged fiom 37 to 50 years (Table 4). Four respondents (33%) had some community
college education, two others (17%) completed community college programs, four (33%)
completed Bachelor degrees, and two (17%) completed Master's degrees. Eleven
respondents were working pnor to becoming il1 and one was a student Two respondents
are currently employed and either are selfemployed or work with government. Of the 10
respondents not currently employed, four were previously employed in health care, four
in business, and two in the education field.
Demographic characteristics of respondents correspond to the typical person
presenting with ES for age, gender, education level, and employment status. However, a
sample of 12 participants cannot be considered representative of al1 persons with
environmental sensitivities. Women who declined to participate in the study did not want
to cornpiete the food record One woman commenteci that she h e w she did not have a
proper diet and was embarrassed to record her intake. Others wanted to talk of their

47
experiences but did not want the work or responsibility of wmpleting a f d record. This
would bias the sample since this suggests women with particularly poor diets may be less
Table 4. Demographic information of respondents
Total nuncber of respondents
Mean age *SD fyears)
Mean BMI S D (Wm2) Mean Height *SD (cm)
Mean Weight *SD (kg)
Mean # of years as patient of NSEHC *SD
Educational background
Completed community college, etc.
Some university did not complete degree
Completed Bachelor's degrees
Completed Master's degrees
Cunently employed outside of home
Student
Sel f-ernployed
Respondents unemployed pnor to illness
Respondents working pnor to illness
Health care
Business (self & other)
Education
Government
12
43.4 * 4.6
26-8 * 8-1
161.5 * 6-4 7 1 . 2 27.4
3.2 * 2.4
4
2
4
2
2
1
1
1 (student)
11
4
4
2
1
48
5.2. Four-Day Food Record
Al1 respondents completed a 4day food record providing a total of 48 food record
days. Preliminary raiew of food record contents was conductecf at the time of retrieval
and any clarification of the record was sought at that time. When necessary, recipes were
provided for combination-type meals to fhcilitate analysis.
The average cdoric intake was lower than the recommended levels for this age
group with an average BMI higher than the ideal range (Health and Welfare Canada,
1990). Since one respondent had a BMI of 40, calculation of BMI for the remaining 11
participants gave a mean value of 24.8. This is more comparable to the Nova Scotia
Nutrition Survey (NSNS) since 42% of Nova Scotian women in the 35-49 age range had
a BMI between 20 and 25 (Health & Welfare Canada, 1993)- BM17s associated with
increased health risks and low caloric intake imply subjects either under-reported their
intake or that intake is accurate, but activity level is minimal. BMI-dependent under-
reporting of 2O-25% has been observed over a range of BMIs for energy and protein.
Under-reporting of energy intake has been reported for petsons who were oIder,
overweight, and îrying to lose weight (Braarn, Ocke, Bueno-de-Mesquita, & Seidell,
1998; Briefel, Sempos, McDoweIl, Chien, & Aiairno, 2997). Under-repoaing was not
expected with these participants given the emphasis they place on diet. Since several of
the respondents report sufEering fkom overwhelmhg fatigue, it is Iikely inactivity is
affecting intake and BMI. A similar study on 28 CFS patients also used $-&y food
records and found the mean intake to be comparable at 1720 * 575 kcal (Grant et al,
1996).

The maCronutrient distribution (Table 5) is typical of the Nova Scotia diet
described in the NSNS that d e s m i the macronutrient distrr'bution of women the
similar age group to be 47% carbohydrate, 35% fat , and 17% protein (Health & Welfare
Canada, 1993). Respondents were not as concemed with fat intake afkting their health
as they were with carbohydrates. Most respondents felt their sensitivities were
Table 5. Macronutrient distribution of the M a y f d record
Macronutrient
Total Energy (kcal)
Carbohycîrate (g)
Protein (g)
Fat (g)
Polyunsaturated (g)
Monounsaîurated (g)
Saturated (g)
Dietary Fibre (g)
Cholesterol (mg)
% cdories from macronutrient
% Carbohydrate
% Fat
% Protein
# of serving per food group
Grain Products
Vegetables & Fruit
Milk Products
Meat & Alternatives

50
aggravated by carbohydratebaased products, such as sugar, breads with yeast, dairy,
wheat, and gluten. Fat and oils were not reported to cause any symptoms. This may
account for the lower carbohydrate intake (49.3%), and higher average fat intake
(34.4%). Protein was recognized as important for health providing the source was
organic.
Intakes were compared to average number of servings based on Canada's Food
Guide for HeaIthy Eating and are defineci as seven servkgs of grain products, two
servings each of milk products and meat and alternatives, and eight seMngs of
Figurel. The percentage of recommended daily senrings per food group for each respondent
l 1 \ Recommended Servings j
Grain Products Milk Products Meat 8 Aiternatives Vegetables 8 Fruit
Food Groups
vegetables and fruits (Figure 1). Respondents were not meeting the recommended daily
servings of milk products and only 25% (n=3) were meeting the recommended S~M-ngs
for grain products. Less than half are meeting the recommended servings for meat and
51
alternatives (n=7), wfiile five were not meeting the recomrnended servings for vegetables
and nuit Five respondents included organic fhits and vegetables in their food record*
Respondents are not meeting the recomrnendation of va-ety in the diets. Analysis
of food selection revealed that while most respondents under-selected fiom al1 food
groups, milk and milk products and grains were specifically targetd This may result in
over-selection of one food group that is better toIerated while virtually eliminating
another that is poorly tolerated For example, Participant 5 had 280% of recommended
seMngs of grain products and 0% of milk products for the four recorded days.
Vegetables and fruits were better represented in the diet, but variety may still be limited
since respondents prefer organic fniits and vegetables, which are costlier, less available,
and have a shorter shelf life than non-organic produce- Afthough measurements were
taken in spring, the higher cost of produce in winter may affect diet variability for those
months. M a t and alternatives servings, too, may be afk ted by the cost and availability
of organic meats and eggs. Many avoid any canned products which could potentially
Iimit consumption of beans, while others avoid sources such as peanut butter and soya
products because of food sensitivities.
Although variety is limite4 Figures 2 and 3 illustrate the actuaI diet was lacking
ody in calcium (71 -5% RNI) and iodine (80.8% RNl) while satisfjmg the %RNT for iron
(103%), riboflavin (105%), Vitamin D (106%), and zinc (107%). However, when
supplernents were included in the mean daily intake (n=9), intake of al1 nutrients except
iodine (8 1.6%) exceeded the RNI. Iodine should not be an issue for this group given that
salt added to the meal was excluded fiom the calculation. Some supplementation caused
the intake to be fat in excess of the recommendations. Of particular note in Figure 3, the

52
%RN1 ranges k m 757% for Vitamin A to 12,078% for Vitamin B, The actual amounts
for diet alone and diet with supplementation are provided in Table 6. Not al1 participants
(n=3) were taking supplements at the t h e of the study-

Table 6. The mean nutrient intake of the 4-day food rmrd of a h a l intake and
actual intake inchding supplementation.
-
Nutrient Actual Iatake Actual Intake with Supplementatioa
Vit- A (RE)
vhIlh D ( ~ g ) vltmnin E (mg)
VihYnin C (mg)
Niacin (mg)
Thiamin (mg)
Riiflavin (mg)
Vitamin B ,,Or& Folacin (pg)
Calcium (mg)
Phosphorus (mg)
hdine
(mg) Magnesium (mg)
Zinc (mg)
Other nutrients without established RNl['s
Vitamin B, (mg)
Vitamin K (pg)
Pantothenic acid (mg)
Biotin (pg)
!hdi- (mg) Potassium (mg)
COPF
Wganese (w) Fluorine (pg)
(pg)
Selcnium (pg)

Complete avoidance of dairy products bas impIications for bone health and
analysis indicated women were not meeting the recommended calcium intake through
their diet Dietary calcium intake is a deteenant of skeletal health in post-menopausal
women. An evaluation of 13 1 women found that women consuming less than the
population mean for die- calcium had significantly lower bone mineral demity than
those subjects with intakes above the mean (Andon, Smith, Bracker, Sartoris, Saltman, &
Strause, 199 1). Interesîingly, four of the women volunteered they suffered fiom
osteoporosis and while these women were taking calcium supplements, those not

supplementing their diet may be at ïncreased risk for decreased bone density by not
meeting recommended daily calcium intake. Calcium supplementation is indicated for
this group given their poor seleciion of foods fiom the miik and mi& products food
groups. However, even with supplementation respondents are not getting the daily
recommended amount of calcium. DiDietitians should advocate adequate calcium
supplementation for their ES clients based on their dairy intake- If it is detennined the
incidence of osteoporosis is higher in this group, al1 ES women suffierers should be
encouraged to supplement with calcium.
Supplementation was a common practice among respondents particularly of the
antioxidant nutrients- Detoxification increases the need for the antioxidant vitamins C
and E, and trace minera1 selenium (Ross et al, 1990) and they are promoted by the
NSEHC in their treatment protocol- Other supplementation comrnonly inchded
magnesium, calcium, vitamin A and the B vitamins- Chronic fatigue sufferers also have
been reported to supplement with these nutrients (Morris & Stare, 1993). Vitamins E and
C, the B vitamins, and selenium supplementation are not contraindicated based on
respondent reports of their intake. (Miller & Hayes, 1982; Schaumberg, Kaplan,
Windebank, Vick, Rasmus, Pleasure, & Brown, 1983).
Vitamin A supplements should be used cautiously, although Health and Welfare
Canada's Nutrition Recommendation (1990) does not provide a dose not to be exceeded-
Severe hepatoioxicity was reported with a daily ingestion of 25,000 lU of Vitamin A
(Kowalski, Falestiny, Furth, & Malet, 1994)- Hype~taminosis A is characterized by
headaches, drowsiness, nausea, loss of hair, dry skin, diarrhea, rapid resorption of bone,
and menstruation cessation (Hathcock, Hattan, Jenkins, McDonald, Sundaresan, &

56
Wilkening, 1990). Cment vitamin A supplementation should not place respondents at
risk of hypervitaminosis, although prolonged vitamin IV therapy use may place those
users at rïsk
At the NSEHC, blood samples are collected for analysis of vitamin and mineral
deficiencies- Senmi anafysis is a Iess sensitive indicator of vitamin A status since b l d
levels fd1 only when liver stores are depleted after a prolonged W o d of dietary
deprivation Treatment reco~~~xnendaîions based on these tests results could potentially
lead to toxicity. Since symptoms of vitamin A toxicity are similar to ES symptoms, high
intakes may contribute to, or cause some of the physical distress experienced by ES
sufferers.
Magnesium deficiency has been reported to cause CFS-like symptoms such as
fatigue, nausea, and learning disabilities, although the exact cause of low magnesium in
CFS patients is unknown (Cox et al, 1991; Gullestad et al, 199 1). CFS patients have been
reported to have slightly lower magnesium levels than their healthy couterparts and did
seem to benefit fiom magnesium supplementation with improved emotional well being
and energy levels. However, Health and Welfare Canada (1990) does question how
hypomagnesemia could occur with the ingestion of a normal Canadian diet, since the
Iadney will regulate magnesium levels- This reduces the risk of both deficiency and
toxicity of magnesiurn, implying there seems to be no real need for supplementztion
given the efficiency of the magnesium homeostatic mechanism-
53. The Questionnaire Rcsuïts and Discussion
The quantitative component of the questionnaire used in the in-depth intewiew
provides insighî into the food practices of the subjects, challenges they fat+, and beliefs
that motivate food and illness behaviors, It was used to assess cornohration between the
food record and the women's words,
5.3.1, Food Practices
Respondents ummimously stated they changed their diet since k ing diagnosed
with ES. The most cornon changes were the inclusion of organic foods (n=%) and the
practice of rotation diet (n=7), followed by the elimination of foods containing yeast,
sugar, wheat, dairy, additives, preservatives, and food dyes (Table 7). Al1 respondents
prepared their own meals, with one thrd of the meals sometirnes prepared by the spouse
or partner. The spouses / partners usually participated in meal preparation when the
respondents were not feeling well. In one family the teenage daughter occasionally
prepared her own meals. Half of the respondents stated that their meals were different
fiom those of the family. Respondents prepared something different for themselves, or in
one instance, the partner cooked for himself The other half cooked for the family, but
seiected fiom these foods what they would tolerate. Several commented that initiaIly the
meals were cooked separately due to the wst of buying organic food for the whole
family. However, later they absorbed the cost to reduce the time and inconvenience of
preparing two separate meals.
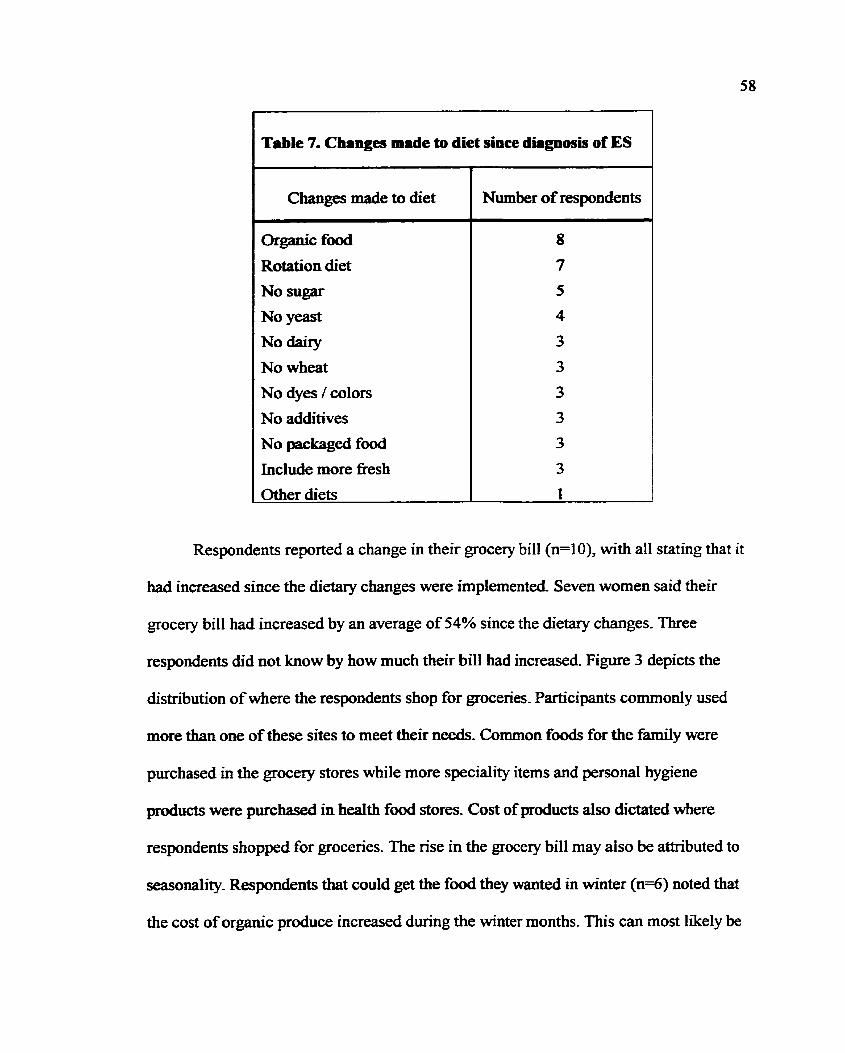
Table 7. Changes made to diet since difgnosis of ES
Changes made to diet
Or&anic food
Rotation diet
No sugar
No yeast
No daixy
No wheat
No dyes / d o r s
No additives
No packaged food
Include more fiesh
Other diets
Number of respondents
Respondents reported a change in their grocery bill (n=10), with al1 stating that it
had increased since the dietary changes were implemented. Seven women said their
grocery bill had increased by an average of 54% since the dietary changes. Three
respondents did not h o w by how much their bill had increased Figure 3 depicts the
distribution of where the respondents shop for goceries. Participants comrnonly used
more than one of these sites to meet their needs. Common foods for the family were
purchased in the grocery stores while more speciality items and personal hygiene
products were purchased in heaIth food stores. Cost of products also dictated where
respondents shopped for grocenes. The nse in the grocery bill may also be attributed to
seasonality- Respondents that could get the food they wanted in winter (n=6) noted that
the cost of organic produce increased during the winter months. This can most likely be
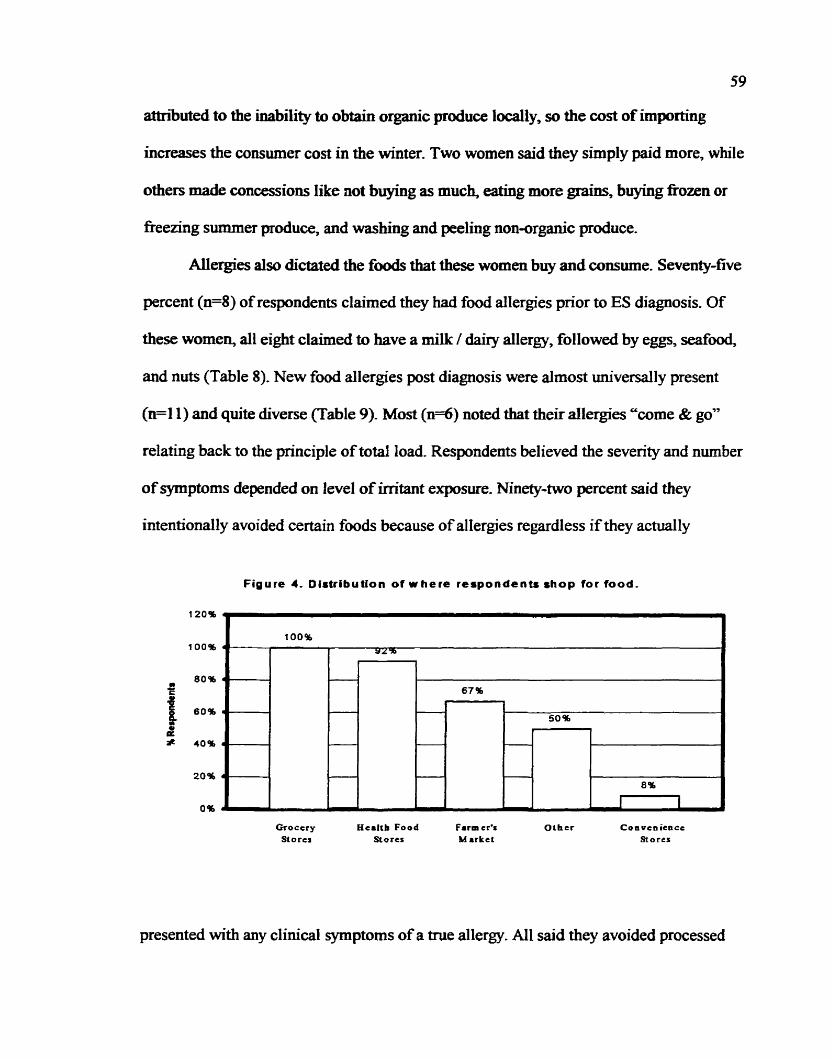
59
attn'buted to the iaability to obtain organic produce locally, so the wst of irnportîng
increases the consumer cost in the winter, Two women said they simply paid more, while
othen made concessions Iike not buyulg as much, eating more grains, buying fiozen or
freezing summer produce, and washing and peeling non-organic produce.
AUergies also dicîated the foods that these women buy and consume. Seventy-fve
percent (n=8) of respondents claimed they had food allergies prior to ES diagnosis. Of
these women, al1 eight claimed to have a miik I dairy allergy, followed by eggs, =food,
and nuts (Table 8). New food allergies pst diagnosis were almost univenally present
@=il) and quite diverse (Table 9). Most ( n 4 ) noted that their allergies "corne & goy'
relating back to the principle of total load. Respondents believed the severity and number
of symptoms dependeci on Ievel of exposure. Ninety-two percent said they
intentionally avoided certain foods because of allergies regardless if they actudly
Figure 4, Oistribution of where respondents shop for food.
Groccry Hci l tb Food f arm cr's Othcr Convcnience S o r c r Stores Market Stores
presented with any clinical symptoms of a true allergy. Al1 said they avoided processed

60
foods, many avoided dahy (n=7) and yeast (n=5). Most of the foods responents avoided
were the same ones they clairned to be allergic to (Table 10).
mew
Milk / Dairy
Esgs seafood Nuts Chernicals / Preservatives Chocolate
orwF Pork Wheaî, Fermenteci foods, Soy, MSG, Tornato, Yeast, Mushroom, Malt, Be& Peas, Bananas
# of Respondents
8
4
3 2
2
2
2 1 each
- - 7
I Table 9. New food allergies after diagnosis of environmental 1
Allergy
Yeast
Dairy
Wheat
Corn
Seafood, potato, tomato, banana, caffeine, fiee range chicken, nuts, s u w
Millet, nce, soy, oranges, dates, chemes, eggs, pas, pork, apples, watermelon, spices, carrots, tumip, broccoli, parsnips
# of Respondents I l
4
3
3
2 each
1 each

61
Not surprisingly, al1 respondents (n=12) felt certain foods had a negative impact
on health. Most of the foods perceived to be bad are the allergic foods listed in Tables 6
and 7. The most wmmon foods were sugar, yeast, mi& and processed foods (TabIe 11).
Four women said '%ad combiningy7 adversely affected their hdth. This occurs when one
consumes two foodç îogether, usually a starch and protein, resulting in gastrointestinal
problems. When these are eaten separately, the foods are tolerated
Parîicipants do consider some foods have a positive impact on their health. These
include vegetables, partïcularly green vegetables tike broccoli, Swiss chard, bok choy
and cabbage and raw, or ccenzymey' foods. Others felt their health was positivety
influenced by eating beef and low fat foods, as well as dnnking clean spring water in
glas bottles.
1 Table 10. Foods iatentionally ivoided by respondeats. I
I
Foods Avoided
Processed foods
Dai ry
Yeast
SLWr, eggs
Fennented foods, seafood, pork, soy
Wheat, coffee, corn, coconut, chicken
I
# of Respondents , i
11 I 1 1
7 1
1
5 t i i
3 each ! i
2 each i ! I i
1 each !

Negative Food
Sugar, yeast, processed foods, bad cornbining
Coffee, miIk
Chocolate, allergic foods, tomatoes,
Egg, corn, soya, strawberries, wheat, moldy foods
Table 11. Foods that have a negative efi'ect on health.
-
# of Respondents
4 each
3 each
2 each
1 each
In summary, 92% of respondents believed that diet contributed to their overall
health, Some women (d) felt that they would simply get sicker if they did not eat righî,
while others felt that their diet promoted hedth and healing by not adding more
chernicals to their body (n=4). Still others believed their diet helped decrease their
allergies, increase their metabolism and affect their imrnunity (n=l). The lone respondent
that did not believe diet contributed to her health felt that the restrictive nature of her diet
was not healthy.
53.2. Other Practices
In addition to modigng food practices, respondents also engaged in other
practices such as alternative therapies and information seeking in an effort to regain their
heal th-
5.3.2.1. Alternative Therapies
MI respondents participated in alternative therapies in an attempt to regain their
health. The most wmmonly used therapies included wunseling (n=8), N vitamin and
mineral supplementation (n=7), massage therapy (&), and enzyme potentiation
63
desemithiion (n=5). Respondents participateci in t h e s therapies with the belief that
they rnight increase their irnmunity (n=6) and energy levels (n=3). Others hoped these
therapies would conîrol yeast growth, break down toxins, allow them to eat more food,
and desensitize them (n=l ).
53.2.2. Nutrition Information
Al1 respondents gathered information fiom more than one source, with books
king their greatest source of nutrition information The sources referred to were pop
literaîure such as Free to Fiy (Rajhathy, 1 W6), The Yeast Connecfion (Crook, 1986),
Prescription for Nuf?ionuZ Healiing palch & Balch, 1997), and a variety of other
cookbooks that helped them cook for their particular sensitivities. Interestingly,
nutritionists / dietitians ranked next to last as a source of ndtion information (Figure 5).
Many (75%) obtaïned nutrition information f?om other health professionals such as
physicians and nurses, not including those seen at the NSEHC. Oddly, although the c h i c
places many of these patients on restricted and rotation diets, only 58% of respondents
said they received any form of nuîritional education fiorn the clinic.
5.33. Knowledge, Attitudes, and Beliefs About Diet
When asked about howledge, attitudes, and beliefs respondents hold about their
diet al1 respondents felt they would very Iikely expenence hannful ef5ects fiom additives
in foods, most also thought this about yeast and artificial sweeteners (n=l 1) (Table 12).
Al1 respondents felt what they ate affected their health and most believed their diet
helped them maintain health (83%). Ail respondents believed that physical activity is a
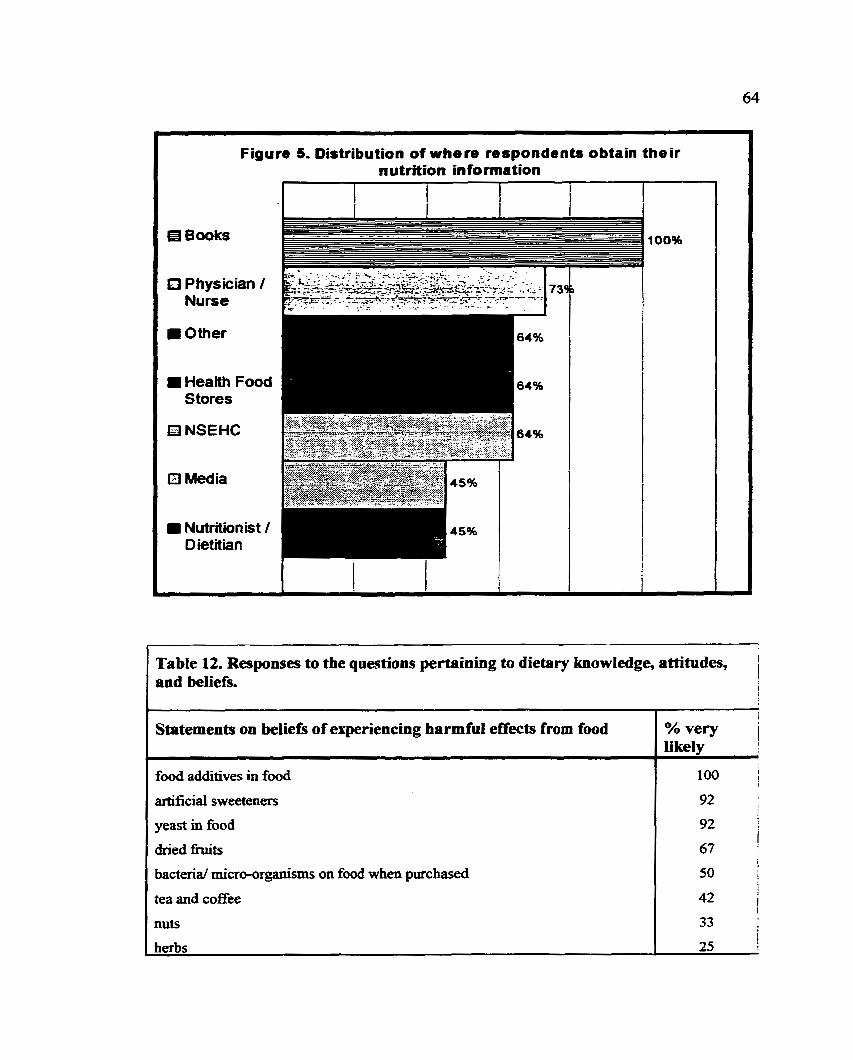
Figure S. Distribution of where respondents obtain their nutrition information
. .-
L e 12. Responses to the questions pertainiag to dietPry knowledge, attitudes, i 1 and beliefs. -
Statements on beliefs of experiencing harmful effects from food
food additives in food
arhficial sweeteners
yeast in food
dried hi&
bacterid micro-organisms on food when purchased
tea and coEee
nuts
1 herbs
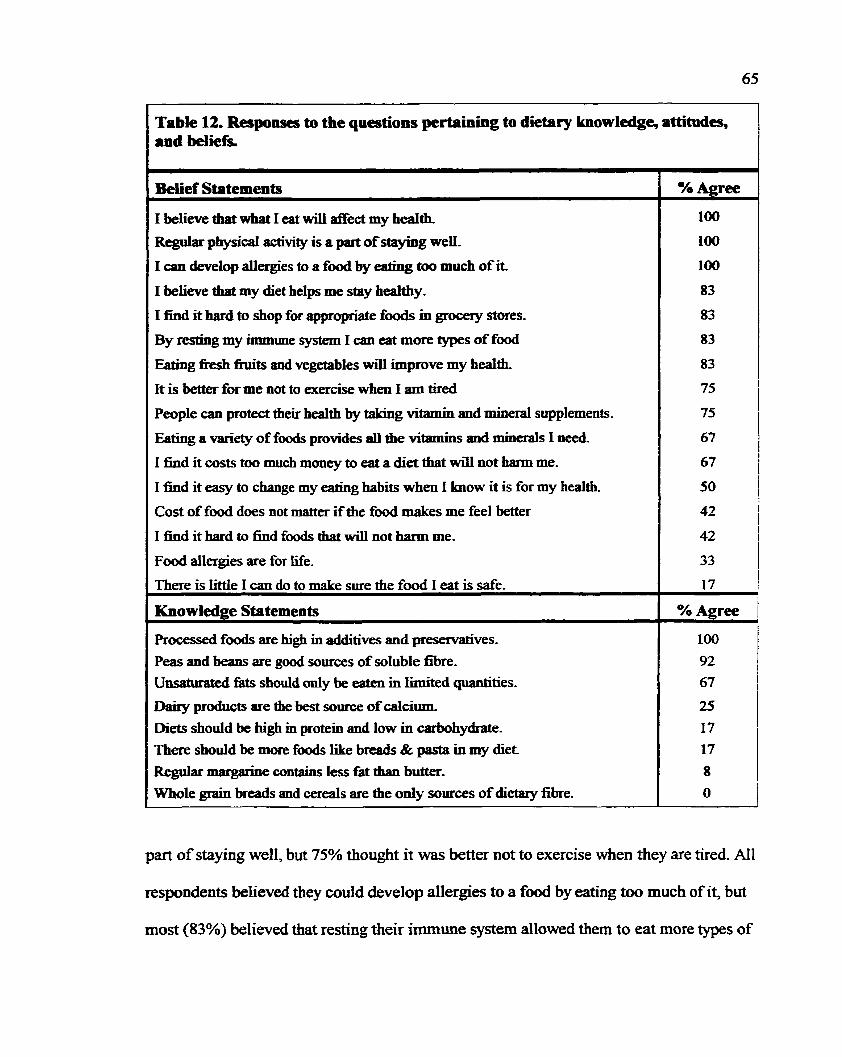
Table 12. Responses to the questions pertaining to dietary knowledge, attitudes, and beliefs
Belief Sîatements
1 believe that what 1 eat will affect my hdth, Regular physical activity is a part of stayhg weK
1 can develop allergies to a f d by enting too much of i t
1 believe that my diet helps me stay healthy-
I find it bard to shop for appropriate foods in grocefy stores-
By resting my mmiune system I can eat more types of food
Eaîing k h bits and vegetables will improve my health
It is better for me not to exercise when 1 am tired
People can protect the5 health by tiih'ng vitamin and mineral supplements-
Eaîïng a Minet . of foods provides all the vitamins and minerals 1 ne&.
1 find it costs too much money to eat a diet thaî will not hann me-
1 fiud it easy to change my eating habits when 1 know it is for my health,
Cost of food does not matter if the food makes me feel better
1 God it hard to h d foods that will not harm me.
Food allergies are for Me,
There is little I can do to make sure the food 1 eat is d e .
Knowledge Statements
Processed foods are hi& in additives and p r d v e s -
Peas and beans are good sources of soluble fibre- Unsatmated fats should only be eaten in Limiteci quantities.
Daby products are the best source of calcium,
Diets should be high in protein and low in carbohydrate. There shodd be more foods like b d & pasta in my diet Regular maqpke contallis less fbî than buûer-
Whole grain breads and cereals are the only sources of dietary fibre.
% Agree
100
100
100
83
83
83
83
75
75
67
67
50
42
42
33
17
% Agree
100
92 67
25
17
17
8
O
part of staying well, but 75% thought it was better not to exercise when they are tired. Al1
respondents believed they could develop allergies to a f d by eating too much of it, but
most (83%) believed that resting their immune system allowed them to eat more types of

66
food Al1 but two, felt they codd control the saféîy of the food they consume- Al1
participants believed processed foods were high in additives and preservatives.
Overali, the nutrition knowiedge was g d with the exception of questions
pertaining to dairy and carbohydrate- Only three individuals thought that dairy products
were the best sources of calcium, and two ïndividuals thought there should be more
breads and pasta in their diet- Interestingly, 75% thought it was possible to protect health
by taking vitamin and minera1 supplements, but 67% thought that eating a variety of
fwds provides al1 the vitamins and minerals needed, This inconsistency suggests that
respondents recognize they are not getting variety in their diet and believe they are
protecting their heaith through supplementation.
These results show both consistencies and discrepancies when compared with the
qualitative data obtained in the second component of the data collection.

CHAPTER VI: Qualitative Analysis of the Interview Scripts
Analysis of the intemiew scripts revealed seven major themes that were M e r
subdivided into categories. The seven major themes include symptorns and allergies,
cost, iraditional and alternative therapies, avoidance behaviors, and information
gathering strategies. These themes are interrelated and inform the respondents' actions
and bebaviors. Illness behavior and health belief models may be used to interpret the
words of the women as they relate to themes derived fkom the in te^-ew scripts.
6.1. Symptoms and Allergies
Much of the behavior and actions of an ES patient is motivated by perceived
symptoms and allergic reactions in response to stresson in the environment. The
presentation of ES is very individual, although there are many foods that appear to be
common ûiggers for these reactions. Symptoms in response to exposure Vary and are
ofien based on the controversial provocation and neutrabation testing. Allergic reactions
described are not considered typical respnses which causes some to question the
credïïility of the illness and patient.
6.1.1. Appearance of Allergies
Respondents commody found that the reaction to a food did not remain static,
meaning that there were times a particular food could be tolerated and other times when
it could not. One woman felt she knew when she could eat a food simply by walking past
P6: 1 know when 1 can tolerate an apple if I can walk past raw apples without feeling very sick to my stomack lfthere is no reaction, 1 know 1 can tolerate apples that day and 1 can have one. But if 1 get that queasy sensation fiom the aroma, 1 know if I were to take that within 20 minutes 1 would be sick to my stomach, You could almost clock it.
This woman believed her response depended on the total load on her body at that time.
Many respondents believed symptorns were the body's way of tellhg them when foods
are tolerable. Other respondents reported when exposed to environmental stressors the
same time as eating, the food may not be tolerated.
Pl: ..-the yeast just makes everything worse.
P9: So when your total load is such that you're now reacting to something, not food, when you eat food that you're not supposeci to have, you react stronger to that,
Interestingly, participant 9's cornments reveaIed participants distinguished
between foods they were "allowed" and "not allowed" to have. Consuming food "not
allowed" may result in feelings of guilt which could establish negative feelings toward
some foods and wntribute to feelings of il1 healtk
Food sensibvities may d i s a p a r over time. Respondents left food out of the diet
for anywhere fiom three months to a year and were able to successfûily reintroduce the
food back into the diet However, this seemed to be dependent on the stage of recovery of
the individual. Those M e r dong in treatment tended to tolerate more types of food
Introduction of problem foods is usuaily gradua1 where the individual is able to tolerate
the food two to three times a week-
1 can now eat ice cream again *ch I couldn't 2 years ago. So as long as 1 don't eat it every &y or every week, I'm fine-
1 had to cut out the millet- Sometimes 1 have to cut out things for a while and then go back to them, so wiîh the millet, I've had to cut it out for a while. I probably won't go back to it for months, now because I had a really bad reaction, so 1 donyt want to really try it again for a while.
Respondents feel that their bodies will tell them when they are ready to reintroduce or
stop a food Close attention to symptoms' the combination of foods, and the current
environment are dl taken into account when deciding if a food is tolerable. One woman
was quite wgnipuit of appearance of syrnptoms while decicihg the fate of a food in her
diet. P4: And then 1-11 wait for a while and go back to them. 1 won? totally
stop hem, because on the other han& sornetimes you stop a food completely and you'll never get it back. If you don? keep it in your diet a little bit, you'll lose it completely. So you just have to kind of feel your way dong and know, well, you can tell by your body. Am 1 gaining with this or am I staying stationary with it, am 1 plateauing out, or am 1 getting worse. And if you're on a plateau, you just keep playing with it until maybe you can h d a time fiame that you can eat that food And if it continues to get worse, you just give up that food for a long üme, then you go back and try it again and if you have a severe reaction the first time around, you've lost that food.
1: Wodd you never go back then and try it again? P: Not for, maybe a year. 1 wouldn't, not for a long time.
6.1.2. Food induced reactions
Many foods were perceived by participants to cause adverse reactions. The most
cornmon offenders were yeast and q a r 7 dairy products, wheat, and corn, as were things
added to foods such as preservatives and pesticides.

6.1.2-1. Yemt and Sugar
One of the more cornmon food reactions involved yeast Ingestion of yeast
containing products, both baker's and brewer's, was reported to aggravate symptoms and
cause a greater occurrence of yeast infections or candidiasis. Linked with this was the
wnsumption of sugar, which was perceived to feed and perpetuate growth of yeast Al1
femiented f d s , such as vinegar and pickles, were also omitied fiom the diet wherever
possible. Much of this behavior was informed by pop literature and was supportai by
alternative health care professionals.
P2: Weil, some.. If1 have been around something else that's sugaryugary.. if I have that that day and figs the next &y7 then my Candida will start up aga in... Too much sugar too close together.
1: Okay. So, how do you know when your Candida's flaring up..how do you feel?
P2: Well, usually 1 just get a yeast discharge, vaginal discharge.
PIO: Because if 1 eat sugars, 1 know what happes. If1 want to be sick, I mean sick in bed, start eating garbage food, junk food, sweets, because I've done it. But since I've been eating healthier, my diet, the allergic reactions that 1 was having is nothing like it was. And overall, 1 feel better, 1 feel more alert. Al1 1 have to do, seriously, if 1 ate a piece of chcicolate right now, 1 wodd guarantee within an hou., you wodd see a difference in me. And so it is definitely food relate& definitely.
Yeast is also associated with some neurologic problems.
1: So how does yeast make you feel? P 1: Oh, g d Depressed, groggy, balance problems, confllsion, you
know, sometimes confusion jusî draggy, it also d e s my allergies worse. I'm now, Iike I'm now got so bad 1 can't even wait for a bus without my mask on because of the cars going by make me sick. 1 wasn't like this a year ago, so the yeast just makes everything worse- And anything that you do have.
P5: ..like tomato stuff, yeasty, like I could really notice. 1 was always, not a manic depressive, but down and depressed and I couldn't really figure out why, what was going on.
Yeast aversion, at some point during the illness, was cornmon to al1 women
Systemic yeast infections are common to individuals that are Mmunosuppressed. While
there is lïttle scientific evidence to warrant yeast elhination as a treatment modality,
many attribute feelings of il1 health to its consumption- ES sufferers were willing to
pursue this therapy since it has been recommended by many who support and accept ES
as a real iilness, SufEerers of ES claim their candidiasis is a direct result of an
overworked immune system that is no longer capable of wmbating the simplest
infections- Respondents eliminating yeast and sugar fiom the diet believe this is a
legitùnate treatment and most report less symptorns when on a yeast-iee, sugar-free diet-
6.1.2.2. Dairy Products
Dairy products were avidly avoided by most participants. Some respondents
reported they fiad milk allergies or sensitivities when they were younger that have carried
into adulthood.
P3: Yes, that's when the food sensitivities were definitely there. Dairy Queen ice cream would nearly kill me if 1 had it.
1: So, you're lactose intolerant? P3: Well, 1 would say that 1 had a true milk allergy, and lactose
intolerance as well. But 1 take the lactose iatolerance pi11 and they work sometimes and sometimes they don't..
Others found reactions to mik and da@ products developed with the onset of the iIlness
P8: If 1 drank rnilk 1 would keel over with temble pains. 1: So do you intentionally leave any foods out of your diet? P: Now? Yes, m i k 1 try not to eat much dairy food at all. 1 know it
does, 1 still react to it because it's still bloat and constipateci, and îhat sort of thing, but nothing compared to what it was. Like 1 still wouldn't even dare &in. half a glass of milk. But I'm fine with

coffee cream, you know, 1: So with srnail amounts more or less- P: Yes, and 1 can now eat ice cream again which 1 couldn't 2 years
ago. So as long as 1 don? eat it every &y or every week, I'm fine.
StiIl oîhers avoid milk because of the processing and treatment of ww's m i k Many feel
that the miik is not d e to consume because of the anb'biotics and hormones injected into
P: 1 believe that milk is the culprit of many forms of disease and 1 think, as a child, a Iot of children can't hande cow's milk, and it depletes the enzymes in your body. .--1 thïnk it's just that no mammal dnnks the milk of another mammai and 1 think that's not natural to our bodies. Up to a point, children up to 2 years old can digest the protein in rnilk because babies have to have rnik right, for that fast growth. But after that, 1 don't think it's needed, at dl. And 1 think if people have it afkr that point, it will harm them. So, our mothers were toid by doctors to pusb milk ... But 1 think milk is the culprit for arthntis, childhood diabetes, al1 these things because it's not natural. But 1 would be called radical for saying that.(P3)
P5: I'd just like to comment that they're injecting hormones in a11 the cows, for the productivity and al1 of thïs. 1 am a strong believer that dairy products are not good for you anymore. 1 don? h o w why, 1 just have this thing even if 1 was healthy. 1 don't know if I'd dnnk milk- But 1 have a problem with that, but 1 think it's because I'm really, really sick. But when 1 see these big cornmercials and poster and ads about milk and stuff, (end of tape). 1 have a probIem with that I really do because 1 read so much on the hormones and the injections and stuff, even with chickens and that's why people get sick
Several women believe that milk is also affecthg their children_
P12: My both children had ear infections, one after the other until 1 took them off milk ... 1 think the hormones and antibiotics in the dairy and in the..you go and buy a box of cereal and you see e v e w n g that's labeled there except the pesticides that have been sprayed on it, but there is no labeling of dairy and there is no Iabeling of mat- You don't know what they put that cow through or that pig through.
P2: And 1 have a real problem because 1 have a daughter who 1 believe
has milk seasitivities and my dmost ex doesn't agree with me. Whenever she eats them, she gets really irritable and impossible to be around
1: Do you think she may be lactose intolerant? Does she have any GI problems?
P: Yes. But 1 don't think she's lactose intolerant- I think she's protein intolerant, which is what 1 am as well. But she can take the goats milk which bas a m i r e n t protein but the same lactase* lactose.
Interestingly, al1 respondents believed that dairy products were contriiuting to
their il1 health partiy because of the presence of hormones and antibiotics added to the
products. By avoiding dairy, participants are engaging in illness behavior for themselves
and health protective behaviors for their families. Respondents perceive that the
additives to milk are contriiuting to their illness, and the behavior is strict avoidance of
dairy- With family, some respondents perceive îhat dajr has already impacted their
health, an opinion that may not be shared by other family members. However, by
restricting access to dairy products, respondents perceive they are protectùig family
members from an illness to which they are susceptible..
6.1.2.3. Processed Foods and f esticides
Many women incorporated organic, pesticide-fiee foods into their diet as a means
of decreasing the totaI load on the body based on the belief that these foods were better
handled by the body.
P3: So like, if 1 have bread, white bread, or even wholewheat, because Iym allergic to wheat, that will keep me up al1 night. So breads without the wheat in it, but then wheat it, it ha . been bioteched, you know. It's been messed with.
P 10: So, I'm thinking if you're spraying your apple trees within 1 00 feet of your cattle, you don't have organic cattle, even if you're feeding

them organic It travels through the air d e n it rains, you h o w the nm off, So them cattle, it's awfiil Iike 1 coddn't believe iî, 1 took 3 bites and my face shot up red and 1 thought I'm going to be really sick and 1 had to take the tri-dts and start tunung myself around- And then I got the shakes and eve-ng that goes dong with it so it was more of a chernicai reaction, because 1 know some foods, it7s not chemïcal, it's just the food itseif, 1 get a flushing, but when it's a chernical 1 get cold and the shakes- 1 got to go and get blankets and 1 need a u and this is what happened to the beef, so I'm assuming that the cattle are absorbing some of the pesticide.
Rocessed f d also provoked reactions because of the preservatives found in them.
P2: Any foods with additives or anything, even if my daughter has some candy, 1.. Or her fnends corne in with gum or something, 1 have to be on the other side of the room or in a different room.
P4: 1 don't eat anything processed. No 1 don't eat anything processed. One of rny big sensitivities is to preservatives in anything. 1 react to parabens, petroleum products, and anything that has a preservative in it 1 have a problem with it. And dyes too, Iike most things îbat are..
1: Like with the yellow dyes, that sort of thing? P4: Oh, yeah, really react severely to yellow dyes.
It is evident from the women's words they believe they are at risk of adverse
reactions fiom processed and pesticide contai-ning foods. Most can predict their reaction
when exposed to these foods and will actively avoid consumuig them. Interestingly, food
records showed that participants consumed processed foods during those four days,
suggesting they may not Mly understand the temi 'procpssed' or may be repeating what
they have k e n told about the potential adverse effects of additives and presematives.
However, given the restricti-ve nature of the diet, and the fatigue associated with the
illness, it is not surprishg respondents would occasionally include processed fmds to
facilitate mealtimes. Regardess, ES sufferers firmly believe their health is affected by
substances added to foods. niey are considered to be another toxin the body has to deal
with, which in turn, limits their ability to regain health,
6.1.2.4. Emotional Reactions
Women reported experiencing emotional reactions, such as crying, depression,
and violence, as a result of exposure to some f d .
P 1 : So, just, it wodd be al1 the things I mentioned before that I'm allergic to and just, just homile mental and physical syrnptoms. And sometimes 1'11 eat something I'm allergic to and 1'11 just start crying, 1711 cry and cry and cry. It's an emotional symptom.
PZ: But one time I had a tuna sandwich, within five minutes I was sitting there in tears. The sound of John and Mary's cutlery on the plate was just too much for me. I had to leave the room and go upstain and lock myself in the bedroom cause I was going to start screaming and crying and then when they were Nushed, I would go and eat-
One theory about emotional reaction to foods suggests that food allergies are
similar to an addiction where one will have a 'high' in response to a food which is then
inevitably followed by a 'low7 withdrawal reaction until the food is eaten again
(Randolph, 1987). However, there are no objective tests to confirm if the emotional
symptoms are psychological or environmental in origin (Miller, 1996). It is possible that
the degree of ernotional symptoms may be linked to the psychologicd morbidity of the
individual or sirnply is a result of the stress encotmtered fiom king il1 but not king
6.1.2.5. Other Food ReIated Symptoms
Women identifid a variety of food related symptom, which tended to be quite
individual, and respondents differed ui syrnptums even to the same food
P9: Corn 1 get coughing My whole face gets bright red, my right ear gets bright red, 1 get disoriented and spacey.
P8: And corn was a r d bad one for me- Back then 1 would eat and immediately it would go right through me.
One woman describes the symptorns she experienced while undergoing the elimination
diet She maintaineci detailed records in an effort to phpoint problem foods.
P: Eggs give me a thick tongue, I can't t& very good and I get very spacey, brain fogged ... Baker's yeast gives me wughng and phlegm producd.. Bananas 1 get very, very hyper and jittery- Brewer's yeast I get strong underarm pin which 1 didn't understand why my underanns would pain al1 the time .... And 1 get a stitch in my side and my legs and ankles tingle. Molds, you wouldn't believe, There's the list of things that happen to me when 1 get molds. Before 1 got back to my seat 1 had total Iaryngitis when I had molds. Cheese, m y eyes are burning and my chest pains are like needles- Sharp needles going through my breasts and my arms, the glands in my armpits swelled up and my arm burned at the sight where they injected it and 1 had a big itchy spot on my m.... Okay, fiom butternut squash, my back broke out in eczema and hives-
1: Do you find that with al1 squash or would it just be..? P9: Just the buttemut squash Okay, some sahon, my upper thighs
were itching very, very bad and my eyes were burning and my upper arms paining. Strawberries gave me extreme sinus pain.
Other women reported more sen-ous, anaphylactic-like symptoms when exposed to
certain foods.
P6: But even with a little bit of mushroom in there, automatically 1 start the itching, swelling tongue and throat, and they say, you carry a kit, and 1 do- And I cany it because I'm sensitive, but 1 don? show np king IgG or IgE on mushrooms.
P 1 : Depending on the reaction. Sometimes it's just I get an upset stomach but sometimes it's like throat choking, you bow, that kind of 1 won't even go near it [millet].
77
Reported d o n s were not typical allergic responses and explains, in part, Wny
traditional medicine has difficulty accepting that ES has an immunologie origin.
Although responses may Vary, Type 1 hypersensitivity responses typically ioclude
urtiwia, eczema, and anaphylaxis. However, anaphylactic-type responses are usually IgE
mediated and are considered tme allergies, not just sensitivities. Respondenîs did report
bloating, cramping, and diarrhea that are consistent with enzyme deficiencies and food
intolerances (Metcalfe, 1985). Sensitivity to vitamin and mineral supplements were also
reported by several women.
1 just had a bad reaction with the one 1 had cornplex supplement]. It had niacin in it and 1 had a niacin flush twice, so 1 stopped taking it, so now the next ones 1 buy will have niacinamide in them.
And 1 think vegetables are very important because you've got to have some form of vitamins and minerais. And 1 can't take them, I'm sensitive to them,
1 rotate my supplernents even Sometimes 1'11 take my B complex that's got everythmg in it and sometirnes 1'11 take the B, seleniurn and the anti-oxidant. It's al1 so I just don? become sensitive to whatever 1 take.
Still others find that the vitamin and mineral supplements, including the IV treatrnents at
the NSEHC have had a positive impact on their physical well-king.
1 fhd that when 1 don? take vitamins, 1 feel terrible. And because of money, I've tried to stop taking them and 1 just felt miserable al1 the time. What do you mean you feel miserable? How do you feel? Tired, more susceptible to haMng bronchitis, asthma, rundown feeling, lethargic, fatigue. 1 don? get headaches, that's not one of my symptoms. Muscle aches. Whole wtiack of So 1 fmd that just vitamins overall improve the way 1 feel.
It helps with the fatigue but it helps a Lot with the fibromyalgia. The rnagnesium does. ... 1 don't feel stiK but 1 also have the energy to
get up out of be-d, and get up and do tbings.... Oh yeah. The difference between night and &y-
Respondents were keenly aware of reactions to various foods and cm rewunt
with great detail experiences with food By takuig such a vested interest in their health,
they feel they are able to pinpoint the source of their ailments and modifL intake
accordirrgly- It is not surpnsing respondents are so committed to uncoverïng irritants
since they feel traditional health care has abandoned their efforts in uncovering the
cause of their distress and has offered no viable treatment aItematives. Respondents
perceived a reduction in symptoms when suspect foods were elirninated fiom the diet.
This is consistent with the reported effects fiom reducing the total I d on the body
(Rea & Ross, 1989)-
Other symptoms reported were often attributed to chernical exposures- These
included ovenvhelming fatigue, violence, mental confusion, and other neurologîc
disturbances. Exposures encountered while out of the home environment can have a
detrimental efFect on the well-king of the person with ES.
P4: They'll light fires in their garda and bum garbage and plastics, and if 1 breathe them in 1 have a lot of problems. They will spray pesticides on their lawns and they cause me a major problem. But they don't are , they don't care.
P6: Yeah, it [malls] smells heavily of formaldehyde and that's because they bnng in al1 the clothes with the formaldehyde on it and do their season's change, and when they do that it gets much worse. That's what 1 have since discovered because there is a smell in there that bothers me, so it's really..so yeah, 1 guess the regime has helped in that respect and ninning into respiratory problems and the

While othen have expenenced problems in their homes, most maintain a very clean,
mold-fiee home using only sent-fiee a d natural cleaning products as a way to
rninimize chernical exposure and alleviate symptoms.
P9: M y brain fog bas been steadily lifting since 1 moved in to the new house, The most signifiant change was moving into the house.
P10: .-..we use the sarne cleaning the cleam-ng soap because there is no way they are going to use scented detergent in my washing machine.-- But I buy Borax in the large because sometimes you'll see a Iittie mold start to grow around the window fiom the dampness. 1 usually try to keep my windows dry. But sometimes it happens, the Borax kills it.
Perfbes and scented products are reporîed to have adverse effects.
Pl 1: 1 used to pass out fiom perftmes, scented products, and 1 had no warning whatsoever. 1 wouldn't even to be able to identify the smell. It would just happen so quickly- A -ter would walk by me and 1 would just fdl right out of the chairy just pass out.
P12: 1 codd s e the fact that when I was exposed to perfume I'd get so tired, And 1 would actuaIIy vomit when 1 was exposed to perfume, and I wouid get weak and get the shakes and not be able to think straight, you know.
For many, chemicals are a source of neurologie disturbances such as confision and can
contribute to "brain fog".
P4: Like for instance, one of my reactions is a chernical, that if its an acid..if 1 get in touch with an acid, or certain chemicals, it gives me what 1 cal1 a racy brain,.. It was like-.I was like a runaway train. It was like a reel, and old-fashioned reel that was out of wntrol and just spiruhg and spinning, that was how my brain was going.
P9: Before 1 couldn't pour tea and carry on a conversation before. I'd spi11 the tea because I'd get distracted, and I'd stutter and stammer
in the conversation. Ifsorneone spoke to me f i l e 1 was doing anything, 1 wodd cut myself-
Chernical exposure also cause or contribute to fatigue experienced by many of the
P12: Well, 1 know 1 remember saying to Dr. Ross at one point the fatigue was so bad that 1 didn't think that 1 could get out of the house if it was on fire.
P3: ,hecause 1 know 1 that I've had chronic fan'gue for a number of years and it just tumed into environmental illness.
Chernical exposure is considered the underlying cause of a11 syrnptoms and
problems currently king enwuntered by ES sufferers. Al1 can recount when and where
the exposure occurred and take many precautionary measures to avoid, or at least limit,
reexposure. Chernicals are everywhere in our society today, so it is challenging to Iive
chernical-fiee. Respondents reported avoiding the public for fear of exposure and toxic
overload Public experiences of ES sufferers indicate that society has yet to accept and
support ES sufferers. This is not surprising since we are al1 exposed to the same
environmental to;icins, yet the majority of people do not experience such discornfort
However, this fom of reasoning invalidates the experiences of woman ES sufferers and
shouid not influence health professionals' decision on a r e for the ES sufferer. Scent-free
policies are difficult to enforce in public places, wbich would make it difficult for a
pemn with chemicai sensiîivities to endure pubiiç environments. Masking outside the
home is an option, although some expressed they rather not mask because of the
unwanted attention they get fiom others. Dramatic changes in food and product
81
co~lsumption are intended to alleviate the symptoms of ES. However, many note that the
cost of these products are a barrier to wmpletely regauiing their health.
6.2. Cost
Cost is Mplicated in almost every aspect of living and coping &th ES. Iilness has
forced most parti-cipants to discontinue w o h g , wkle having to endure the increased
costs of treating ES. Organic produce and meat prices are much higher than their non-
organk comterparts.
1 spend as much on the few things 1 do as 1 would on just being able to go a nomal grocery store and buy, and that's whatever because organic foods are ço expensive. And everything 1 eat is organic food, right..and YI1 tell you it's really expensive. 1 buy the organïc steak Not a lot of steak because it is very expensive.
Are you still eating organic? I really never ate organic.. ..The miff s expensive. Now I just eat ~~ything-
Some women felt that the cost of their grocery bill had not dramatically changed
since the organic foods replaced much of the processed foods.
P12: 1 don? buy a lot of processed foods for the children either, and 1 find them very expensive. People tend to thuik that the organics are that rnuch more expensive, but if your not buying al1 the junk and al1 the p r d food, then the money that you would normally spend on that you spead on the organic stuE
Some women agreed that while the cost was higher, they would continue to buy
food they felt positively aEected their health.
1: The cost of food does not matter if it makes me feel better- PS: Well, yeah. If that was the case, it wouldn't matter. If it made me

feel good, I wodd pay for i t
Winter costs also infiuence ES sufferers ability to buy the f d they feel they need.
P4: In the summer time its not bad, but in the winter, I get it locally, but in the wintter time 1 have paid as high as $8 for a litîle antaloupe.
P6: There are some things, weil 1 guess 1'11 have to say no in a way. There are some things that you can't get in the wintertime without paying exorbitant prices, and because of that we don't, or else we just buy a tiny amount of i t
Increased costs are associated with treatments at the NSEHC, alternative therapies and
vitamin & mineral supplement.
1: 1s that very costly, the antigens? P2: Yeah, 1 spend about six thousand a year, on those.
P5: Oh, it's so expensive. It's very, very expensive- Like in between my treatment 1 have to take medication before and afterwards, and just my injection, 1 have no money. And 1 don't even buy organic fhits or vegetables, and 1 still don't have money.
Cleaning supplies, personal hygiene products, major house renovations, and relocations
can substantially add ro the cost of living with the illness.
P10: Cleaning products alone, like my soap detergent, you can go out and buy it dish detergents for $1-69,I can't use that for washing, and 1 pay $3.89 for a bottle of the Nature Cl- So al1 of your products are much more expensive. Toothpaste is $7 a tube. You go in and 1 buy the aystal rock, well it's quite large, and 1 pay $12 for that. The shampoos, well they're not too bad, but it's still hi& $6.98 1 think it was for mine. And then when you get into your cleaners, it's just up and up and up, $15.99 for a 4L container of wash detergent.
Although al1 women identified how their cost of living has increased, many women have
developed strategies to reduce costs wherever possible.
P2: ... a group of us order together and then they send it up in a few

boxes and that reduces our shipping costs.
P7: I go to CA. It just depends on what's going on 1 go to Pete's Frootique. Or wherever there' s sales.
Many respondents believe that cost diciaies the extent that they can control thnr heaith.
Since wst is such an issue, it implies respondents are expenencing some form of
deprivation This may be deprivation of products and seMces needed to achieve health,
or of other aspects of living in an effort to afford treatment, or a combination of both.
Regardess, financial stress would most Iikeiy negatively impact the physical and
emotional well being of ES sserers. Most respondents do take the initiative io find
innovative ways to reduce costs. It is interesting that while respondents believe that
certain fwds positiveiy affect health, cost will dictate if the food item is shared with
other fmily members and fiïends. Usudly it is a matter of convenience for al1 family
members to eat the same thing, but this depends on the financial situation of the family.
It appears that when resources are Iimited, respondents will try to first address their own
health issues, since they are the ones most afZected by the food choices.
In spite of reduced incornes, respondents will make considerable changes to their
homes, diets, and lifestyles that result in tremendous cost. Respondents do this with the
belief that the curent situation is çontnbuting to their illness and that these changes are
necessary if they are to be restored to good health. This gives them power and reinforces
the belief that they are in control of their iIlness and health, WhiIe traditional health care
professionals may not agree that change to this degree is warrante4 it is recommended
by many alternative health practitioners. Since alternative therapists are sympathetic to
ES sufferers needs, it is not surprising that many do follow their suggestions to the best

of îheir financiai ability.
6.3. Traditional and Alternative Therapies
The use of aiternative therapies o h sîemmed fiom fiustrating experiences with
traditional practitioners. Lack of support, inability to identiQ problems, and offer
possible treatments has Ied ES sufEerers to virtually abandon traditional medicine and
seek relief in alternative therapies.
63.1. Traditional Medicine
Women often expressed that their health concerns were not talcen seriously by
health professionals and were very frustrated and ernbitiered by their experiences. They
commented that health professionals failed to link problems, tended to compartmentalize
symptoms and not look at the individual as a whole. However, respondents had used
traditional rnedicine over the years as a rneans of dealing with the illness.
63.1.1. Lack of Support
Lack of support and belief in ES as a real physicai ailment by health professionals
has significantly impacted the respondents' perceptions of traditional medicine.
Pl : 1 was in the emergency room, when was it, in December cause 1 was you know, blacking out and she.. The doctor said at l e s t you don't have cancer. 1 thought, you bitch. You know, 1 thought well th& you for your support, but you know' it was like what I'rn going through is nothing because I don't have cancer, you how, like it's really insensitive. Cause they couldn't find out what was wrong so it must be me, right? They couldn't find out fiom the tests what was wrong so obviously I'm a wing nut. That khd of

They just say, you how. .. they almost tell you you're fine, I guess. Nothing shows up on the tests and patronin'ng men. Male doctors have been very patronizing and they try to psychologize things and say it's stress. You know when you are under stress and when you're not under stress. And you try to tell hem that, that it's not stress. I've k e n labeled type A pefsonality, aggressive because of my beliefs that I've discussed with doctors. Like my personal ferninist beliefs and been labeled aggressive because of it. In letiers! I've got the letters that the specialist has sent back to the GP. 1 always get a copy of the letters to see what they say about me. And 1 just couldn't believe this one letter fiom this tbroat specialist, unbelievable.
... my doctor just didn7t7 you know, believe what was going on. They would just basically say, well Mary do you think maybe you're sleeping too much and that was the last straw. 1 went out of that office and 1 never went back,,.. That's interesting. 1 wondered how much in the health profession, if people are s tarhg to accept it. Some are, some aren't. You still corne across a lot of doctors that just think your nuts and that's ail there is to it. They don't want anythmg to do with it if you have environmental sensitivities, basically they'll just look at you and tell you it's al1 in your head. And they won't do anything about it. That's got to be really fktrating. It's very hstrating. Even now there are still some people that go to the regular doctors who don't believe in it. So how can you work with somebody who, a doctor that's treating yoy that doesn't believe that environmental sensitivities exist? 1 mean, if it was me, 1 would find another doctor that did believe in it, because al1 it's doing is really holding that person back.
Many respondents had gone through a battery of tests and specialists in an effort to
identie their physical problems. Most found traditional medicine did not treat the
individual as a whole and did not connect symptoms to chernical exposures as they
wanted them to do.
Well, she (the doctor) sent me to every specialist you can think of for every different part, you know how they compartmentaiize, western medicine does, so you know, oh you have diarrhea, let's send you to a GI person, oh, you've pot, you're starting to pass out, oh let's send you to a neurologist, and you know. And, of course, they don? find anything cause it's ail a new system allergy environmental relatai and that doesn't show up on tests.
The allergy specialist, he was quite smart. I've been to a lot of doctor's, and he's about the only one who said stop al1 milk products. He's the only one- I went to GP after GP tqing to find out what was wrong with me, and 1 always said that 1 couidn't digest the food- They never believed me. They never ever connected anything. -.Those doctors. 1 had upper GI, 1 had lower GI, I had x- ray &er x-ray and it al1 related to food allergy--..And the chemicals, and they never comected anything.
Pl 1 : i t was my third GP- No, it was my second GP- The fïrst one really didn't understand what was happening to me. He was very kind, but he wasn't putting it al1 together- He'd just corne back and say, something's wrong with your thyroid and your anemic and you're deficient in this, and your deficient in that. But he wasn't putting it together.
Since ES sufferers present with vague, nonspecific symptoms, traditional doctors are
usually unable to give a diagnosis that is organi-c in origin. Conflict anses when ES
sufferers expected to be offered treatment and were unwilling to accept any other
diagnosis. Respondents felt their experiences were devalued, which undermined their
trust and confidence in traditional healthcare. The only doctors considered crediile were
those that contirni their illness and offered some treatment option. Environmentally il1
patients were much more Likely to accept treatment fiom health care professionals that
they felt treated the individual as a whole person. It is not surprising that respondents
tumed to alternative therapists that focused on treating the mind, body, and spirit.
63.13. Combining Traditional and Alternative Practices
Respondents, although fiustrated with the medical community, had sought
physicians that were sympathetic to their illness. These physicians typically endorsed
alternative therapies such as IV therapies, enzyme piIls, and sauna therapy.
PS: Weli, 1 follow Dr. Goldsmith's.~she's just an MD but she's very aware of this environmental dlness and she's open to help you So she sort of guided me .,... Dr. Goldsmith told me I had mudida, because with al1 those antibiotics, 1 had a yeast overgrowth in my intestinal tract and that's why 1 was reacting to al1 those foods. So she had me 1 Diflucan, acidophïlus, and 1 took Nizerol and different yeast medications to clear up.
P8: Dr. Bruce Elliott He was my god way back when I was first sick. If it hadn't k e n for him, 1 don? know where I'd be.--..I mean Dr- Elliott wiil bring you to the point of getting ready for the clinic, and al1 the clinic has to do is basically start your testing, because Dr. Elliott has brought them that far dong with the IV therapy, with the supplementation, with the sauna, with the change of diet, w i i the different bIood tests that have to be done-
Respondents ~ i l l engage in more traditional therapies that are considered useful for
relief of environmental symptoms or for complications arising from EI. This is consistent
with the findings of other sîudies evaluating the use of iraditional and alternative
therapies (Vincent & Furnham, 1996).
Pd: Dr. Whiteharn, my family doctor suggested I take B6 because of that PMS stuffso 1 don 't take that separate, it's in the muitivitarnin.
P8: I go to physiotherapy now. 1 went today, this morning because 1 sprained my back. 1 have sprained many parts of my body since I've been sick, because I'm just not physically active enough to keep those muscle up. It doesn't take hardly anything and I've done something really bad. Like putting on my socks.
PI 1 : So my doctor told me to take a month off work and 1 just couldn't go back after that. But, you how, I had been just denying the illness up until then Wiîh the first go round, no, they diagnoseci me with chronic fatigue, but they really didn't know anything about it.

6.3.13. Experiences with Nutritional Profmionals
Lack of support and understanding from the nuûition community conîributed to
the feelings of abandonment and finistration Most found tbat the tmlitionai teachings of
n~t~tionistsl dietitians were not applicable to their set of circumstances. Only dietitians
that subscnM to lesser accepteci altemative metfiods were considered credible.
1: Have you ever gone to see a nutritionist or a dietitian? PI : Well, most of them are like you know green Jell-O with red? Do
you know what 1 mean?-..-1 feel like 1 know more tban them about my situation- I mean, 1 know they lcnow about nuirition in general. I've been to them years ago, but 1 wouldn't, no..
P2: What it, what it does for me is it [CFGHE] makes me feel really inadequate.
1: How so? P2: Cause.. I'm just going to get the food guide and look at it ... Because
really, it has nothing to do my iife.
1: Have you ever met with a nutritionist or a dietitian? P9: No ... they are really not equipped to handle this.
Again, the pattern of selecting health professionals sympathetic to their condition was
evident in their selection of n ~ t i o m f advice.
Pl : Yeah, it takes tirne to leam al1 that stuf f [nutrition]. Yeah, 1 find the people I've encountered don? know. But I know there are people out there, iike Mt Rahjathy, she knows, she had environmental illness so she leamed
P2: I've heard there's, there's a couple of nuhitionists around that deal with people with environmental sensitivities and one, Anna Protheroe is supposed to be quite good. nie other one has no concept of wbat a rotation diet involves or what food combining involves. [and it is very difficult you know].
It appears that fnistration is felt by both patients and health care professionals.
89
Physicians have failed to find any physical evidence ofillness after a battery of tests,
suggesting that the patient's illness is more psychosomatic in origin. ES suf5erers were
lefi m t e d and resented this diagnosis, and for this reason, many tumed to altemative
practitionea because they were sympathetic and offered some mode of treatment
Aithough much of the therapy is based on diet manipulation, it was surprising to
find that respondents obtained Little satisfaction form mainStream dietitians, since
dietitians are considerd the most reputable source of nutrition information. Respondents
only heeded advice fkom îhose they felt understood and believed in their illness,
regardless if it was supported by the professional community. Respondents, with the
exception of pain management therapies, essentially rejected al1 foms of traditional
health care and turned to alternative practices.
63.2, Alternative Therapies
Respondents parîicipated in a variety of altemative therapies in an attempt to
regain health. They have expectations of what a îherapy wilI provide. Therapeutic
benefits were very individual and ranged fiom positive, to negative, to unnoticeable.
Alternative therapies include jujitsy horneopathy, omega testing cranial sacral therapy,
therapeutic touch, enzyme and antigen therapy-
6.3.2.1. Participant Definitions of Alternative Therapies
Participants engaged in alternative practices with the hope that they would
alleviate fatigue, combat infêctions, and restore immun@ They ofEered definitions of
how a therapy would benefit their health.

It's called intradermai testhg and what they do is they put the.. They get a dilution and then they put it just under your skin and if it wheais, then you7re reacting, right so then they go to the next weaker dose and you get them till you get a dose that doesn't wheal. And then that's your neutrdizïng dose. And then you get a, 1 always say ten fwds in it, that then you inject yourself with every four &YS.
And what is the purpose of that? To neutralize your symptoms and to neutralize your reactivity.
What does a magnesim loading do? Well, basically what they do, they.. You collect your urine for the 24 hours before and the 24 hours afkr and they see how much magnesium - you collect your urine and you measure what magnesium and other things, calcium 1 think, are in it and you get an N with just rnagnesium and then you collect your urine for the next 24 hours and they measure what's in tbat and if there is.,. if you retain a certain amount of magnesium, it shows that your body needs it. If you excrete it all, then they Say that you don't need it.
Sauna is very wmmon in the detoxification program because it actually pulls the toxins i t J t gets it out of the organs and gets it mobile into the blood Stream, and then the last of it is through the tissue. It's almost like a microwave it starts imer and brings it out.
With EPD what they're trying to do, they are trying to get your immune systern to build a family of suppressor Tcells, and these suppressor T-cells then have a memory and they then go around the body switching off reactions. So you're not actually developing a toierance, but you're actually stopping the process before it starts. So you don? have al1 these symptoms, you don? sneeze, you don't have itchy, watery eyes, you don't have the intestinal gas, or even diarrhea Al1 the types of syrnptoms that you might have had when you are exposed to something and causes a reaction, and then this is the symptom caused by that reaction, so what the EPD is trying to do is to stop the reaction process before it starts.
Understanding the women's interpretation of the therapy provides insight into how
they perceive their illness and what these treatments are doing to restore health.
Respondents engaged in both mind-body therapies and physical treatments with the
belief that these therapies will alleviate symptoms.

633.2. Beliefs About the Impact Therapies Have on Health
Respondents ttm to alternative therapies with the hope of gaining relief. Most
hope that the therapies will work to strengthen their immune system.
Well, I'm hoping to strengthen my immune system so that I won't be allergic to everythng on the fuckuig planet. So I can have a life. Yeah, it's al1 about strengthening your immune system so that like if you do have any retro vinises or Candida, whatever, it can fight it off and you're not ovewhelmed and sick Cause that's what it's about, your immune system ...-j ust making that part stronger so that anything that cornes dong you can handle.
1 have no idea if the B's and the anti-oxidants are doing anything. 1 have no idea--Tm hoping tbat they are trjing to work at strengthening my immune system.
The EPD I think, will hopefully get the immune systern back on track. So that it can take care of itself So the enzyme desensitization, just to the allergy shots are just ûying to desensitize you What the EPD is trying to do is get your immune system to be able to fùnction normally and handle things the way it should be handling things.
Othen hope the îherapy will act to reduce stress on the body.
There's magnesium chloride, vitamin C, the B's, reduced glutathione. What does îhat one do? It detoxifies your body.
And now a lot of the times what I do since I got the Kiva light, 1'11 put rny foods under the Kiva light, What does that do? That neutralizes the pesticides if îhere is any in i t
Others engage in therapies with the hope of increasing energy levels. Most respondents
spoke of the overwhelming fatigue and discodort they experienced as a result of ES.

1: The [V and minera1 therapy, what do you think tbat's doing for you?
P7: I fhd it gives me energy. It gets me out of bed It helps with the fatigue but it helps a lot wïth the fibromyalgia The magnesium does. ... 1 don't feel stiff, but 1 also have the energy to get up out of bed, and get up and do things.....The difference between night and &Y-
PlO: I found my energy starting to go d o m again and as soon as I had the a steak or something, it went back up. And I've read, I'm group O positive, my blood, and it's one of the first men on earth that's the group they were in, group O positive. And they were meat eaters, so my blood type actually needs animal protein, not vegetable protein, in order to survive. 1 was studying different blood types, AB can do either or.
There were a varïety of therapies respondents prticipated in with the hope of
regaining health. Many of these therapies are unproven and not accepted in the
traditional health care sector. However, respondents were willing to 6ry any therapy that
offered some hope of symptom alleviation. Respondents were taki-ng control of their
illness by uudergoing a plethora of alternative treatments. ES sufferers ofien perceiveci
conventional medicine had nothing to offer and felt that they had no other options open
to them. Actively seeking therapy asserts that the respondents' goal is to be healthy, and
that they were not willingly withdrawing fiom life. Regardless of the motivation to seek
therapies, many have experienced both positive and negative outcomes fiom alternative
therapies.
6.3.23. Reaetions and Benefits from Alternative Therapies
Participants describecl a variety of responses to the alternative therapies they
engaged in. Some experienced serious negative reactions fiom a therapy.

Pl: Ifyou've got a lot of Candida, supposedly rve got this systemic Candida, it's al1 through me and what happens is the yeast cells get Wed off when you take the garlic, it kilis the yeast cells and you have this, you know, total overload of dead yeast cells in your body, you know, k i n g eliminated and you start to feel a lot sicker for a while than you normdly would so, it's cdied die off and that could last for a &y or sometimes a few weeks and it's cmmmy- I've did ginseng jujutsu 1 ended up in the hospital fiom that, it can dso make you very sick cause you're shifting things around in there
P4: Sauna, they put you in as long as you can tolerate. Now the first t h e 1 stayed in for 10 minutes and d e n 1 came out 1 had tem%le heart pain and chest pain--l still have cbest pains because of i t Probably because of toxins around the heart, it feels like heart pain. And it creates gases in the chest wall as well-
Interestingly, it was not suggested that chest pains couid be caused by something other
than the release of toxins. Again, this M e r substantiates the daim that the etiology of
ES is a chernicd overload in the body- However, oîhers reported positive results fiom the
treatment.
P4:
1: P6:
P8:
Therapeutic touch .... That's at the clinic. And that helps.. I can't take anything for pain control and that helps tremendously.
Do you have problems if you don't take the enzymes? You know it's h y Y 1 originally thought they didn't do anything. Then 1 stopped for a couple of weeks on the advice of a specialist in Toronto and at the end of 2 weeks 1 realized that it was actually doing something.
Oh yes, it was great. 1 was on IV for 2 years- That's what started bringing me up- When 1 first got sick 1 was on the wuch, and once I started the W s 1 noticed 1 would have more energy each week And if I went a week without N3 boy 1 knew i t J t made a difference
Some participants noticed no change fiom the therapies, but this usually did not
discourage respondents fiom trying other therapies .
1 îrïed acupuncture, last year. Mostly because of my foot and for my energy, but 1 didn't see that much of a difference really.
But 1 was doing that but 1 wasn't feeling ariy better, and I still don3 notice any big difference to be perfectly honest, on the P D diet, or the regime 1 should Say.
But some of the foods 1 didn't realize 1 was reacting to, iike chicken 1 was fine when 1 ate chicken, but accordhg to the tests, chicken was a problem- 1 couldn't have it Did you notice a difference when you stopped having it? No, So 1 don? know if the test was inaccurate or what was going on. But 1 was fine with chicken when 1 ate it so I thought.
Most participants believe that treatment response is very individual, so what may work
for some, wilI not for others or may not work for the sarne person at a different time.
Pl: 1: Pl:
P12:
I've done homeopathy. How did you find that? Well, 1 ended up in the VG this summer fiom that It made me so il1 A t was t w strong of a dosage and it just made me very i11. My sodium level dropped so low, 1 was taken in an ambulance to the VG, I'd lost awareness of where 1 was and that was, 1 think it was fiom the homeopathyY It's weird It also can be really.. Like I've taken it before and it's helped so it depends.
It7s like any therapy, you know. Shiatsu works for some people, some people love tai chi sorne people like homeopathyy some people like naturopathyy some people Eind acupuncture the best So I think what you have to do because everybody is uniquely different, our bodies are different, our reactions are different, our state of h d t h and our genetics, and the whole total picture is different I thbk what you have to do is search and fina you have to search the thïngs out that work for you 1 mean some people are able to handie pain through meditation and some people you're going to have to give them a shot of demerol. So everybody7 s so diffeïent.
Respondents were willing to try any of the therapies if the opportunity or financial
circurnstances allowed i t This perpetuates the hope that some treatment exists that will
relieve symptoms and preserves their belief in the organic nature if the illness. However,
95
this also indicates there is au underlying despration the women feel that is motivating
their actions. Certainly, desperation mixed with refiisd for treatment could place them
under great stress that muid M e r compromise their health By seeking therapies
outside of the NSEHC, were taking control over their illness. This can be
quite empowering since respondents cannot be denied therapy if they are willing to pay
for it,
P2: Yeah, I'm thinking of moving to that.. A fiend of mine she was on antigens and then she started homeopathy about two years ago and she's off ail her antigens nowWW,.so I'm thinking that that may be an, you know, an altemate route for me to go if 1 can't get my antigens teste4 you know, there7s going to be a point where they7re no good to me so what am 1 going to have then? So, I'm going to start looking at that.
Did you ever do any type of massage or acupuncture, any.. No7 but when 1 can afford it I'm goïng to. This is something 1 really want to do and homeopathy.
The sauna therapy, have you ever tried that? No. And I'rn just about to try to get the c h i c to allow me to try that.
Respondents aiso seemed annoyed when they were not considered candidates for
treatrnents offered at the NSEHC. It appeared this denial was taken as a rejection of the
severity of their illness. Most respondents were desperate to ûy anything that was heard
to help other sufferers, so it is not surprising they were antagonized at king denied
access. This represents a loss of power for these women since the decision to get
treatrnent is not theirs, but that of their doctor,
P2: I'm going to try and talk to Dr. Fox into giving me another magnesium test.
P3: 1 just tried a Mg load test at the clinic and 1 apparently, 1 never got a d l back, so they say I'm okay with that. But I've been told kat

that test is inaccufateufate That's about it though.
1: So have you ever done the EPD? P: I'rn not a candidate for that 1: Oh How do they determine if you're a candidate? P: G d questioa Go ask Dr. Fox Ask him. HeW tell you that people
who are really chemically sensitive are not candidates because it doesn't desemitize you to chemicals. So 1 don't redly understaud why I'rn not a candidate seeing as how I'm extremely allergic to rnolds and pollen and foods- And it seems to me that if I were takîng the EPD, it might lessen the load so 1 might not be so reactive ta the chemicals, But no.
Participants Mewed inability to obtain treatments as a bamier to obtaining health
regardless of whether tests did not warrant therapy. Respondents appeared desperate to
try anything and experienced hstration when they were denied potential relief
Respondents believed tests and the health care they were obtaining were failing them
again by preventting access to treatment. Alternative treatments were often rewmmended
by alternative physicians and participants relied on their support during their illness.
6.3.2.4. Recommendations from Alternative Physicians
Recommendations fkom physicians sympathetic to ES tended to be welI followed,
though the efficacy of these treatments is still questionable. Belief in ES as a legitimate
illness establishes trust between patient and physician and promotes patient cornpliance.
P4: Dr. Fox says don't eat potatoes with beef because the sâarch and the beef is too difficult, and that's typical, meat and potatoes, right. So 1 stopped doing that. ... Dr. Fox 1 trust.- He sees how sensitive we are, but even, we're more sensitive than a lot of people at the c h i c even, and to start with somebdy else right now, no, 1 wouldn't even dream of that. 1 m e - if Dr. Fox recommended, 1 mi& but no-

97
P12: 1 went to see DE Baker Lavalle in Chester and one of the things they took me off was al1 yeast produ& and al1 wheat products and al1 sugar products-
Some of these rewmxnendations requïred major life changes that wuld resdt in
increased financial burden These changes include dief household renovations, and
treatment protocols.
He making his own Iittie protocol for me because I'm still on IV's and you're not supposed to be on N's and doing saunas.
Dr, Elliot said to me, well, 1 said the only way 1 can buy a house, Dr. Elliot is that I cash in some of my pension- We have a cottage and we had some savings, and we just spent $1 0,000 right, because the money was sitting and we said lets renovate our camp and put electric heat in, and make the bedrooms bigger, put in closets, al1 that stuffbecause you're out there pretty much 2 months straight and so we did that And then he tells me 1 got to move. So where are you going to corne up with the cash for the d o m payrnent. That's a big request. And also al1 the renovations right. So he said well, okay, so cash in some of your pension What makes you think you'll be amund long enough to enjoy it? The doctor said that to you? Yes he did, 1 said, okay, 1 got that figured out. That's different when you put it in that context. He said look how sick you are.
Alîhough medial care in Canada is universally wvered, patients must pay for
alternative therapies fiom their own resources. While this has limited the use of
alternative therapies, many already under financial constraints will seek these therapies
with no guarantee of results. Kelner and Wellman (1997) found that individuals sought
alternative therapies for pragmatic reasons, such as "nothing else worked". This is a
similar cornplaint voiced by the respondents that traditional physicians offered them no
real solution b their iIls. Alternative therapies provide ES sufFerers with the means of
taking control of their illness. It estabiishes that they are active participants in their
98
health and that they want to be healthy- Current research into the behaviors motivating
the selection of alternative therapy over traditional medicine show that those visiting a
homeopathist felt they had more control of their health than those visiting a GP (Fumham
Br Beard, 1995). Another study examining the motivations of patients who seek
alternative fierapies reported that those using alternatives felt they were taking a
proactive role in maintaïning heaith and preventing illness (Kelner & Wellmm 1997).
These activities included monitoring their diet, exercising more, and taking Mtamins
more reguiarly than those seeing physicians. Patients of alternative therapies placed
emphasis on taking responsibility for their own health, and made it clear they knew their
body best and tnisted their own judgernent most. This is consistent wïth the reasons
respondents provide for seeking alternative therapies.
Cancer patients interested in alternative approaches believed they received less
support fiom their physicians and significantly more wanted to receive emotional support
from their dermatologist and psychotherapist (Sollner, Zingg-Schir, Rumpold, & Fritsch,
1997)- Interest in alternative therapies often seems to represent an intention to actively
influence one's fate and the course of illness and to strengthen hop.
Homeopathic patients strongly believe that treatxnent should fwus on the whole
penon rather than on symptoms (Vincent & Furnharn, 1996), so it is not surprising
respondents acknowledge the need for wunseling Respondents partkipated in a wide
variety of coping strategies including psychotherapy and other types of stress
management tools
99
633.5. Caping Strategiea
Most respondents recognize the need for, and engaged in, some form of stress
management. This included psychotherapy and relaxation techniques, such as Freeze
Frame, Tai Chi, and meditation Some pariicipate in therapy to leam to cope with living
wlth illness.
Pl:
P3:
P 1 O:
I'm dso doing rnedïtation aIso, you know, going to a therapist, - those are two things that help- Yeah, those two things are important- Just l e m how to live with the illness, type of thing.
And other things, coping skills and tbat. Hopefully that will help dealing with people who don't beiieve that you are sick
There are other ones too, off the wall things, iike Jin Shin and some things that Dr. Fox has done at the c h i c with stress management-. . . So I've tried yoga and different, meditation, counseling. I'm always hoping that something will be the magic pill, It's not,
Some recognize that there are other issues in their lives that should be addressed and
prefer not to burden family members.
1 also go to a psychiatrist who I've been going to for quite a Iong time and 1 went to her before 1 was sick so she's really .. my GP died so my psychiatrist is really the only one who knows who 1 am, or who I was and 1 did go to her for quite a long time.
Yes, I'm mean I'rn involved at the clinic with Lauren who's the psychologist. I'd rather whine to her than whine to everybody that's around me. She gets paid to Iisten when others just want to tell me go away. So, 1 think it gives me the opportunity to get rid of a lot of hearîaches, and headaches, and losses that I've had wiîhouî making everybody else get involved.
1 like to go for counseling too because I'm in a new relationship and I have a lot of bullshit to deal with, you know, just psychological issues that I have to.. Because I've only had one relatiomhip and it was bad

P10: 1 went to counseling, right now with Susan. 1 h d that very helpfid, like 1 have a lot of issues, m y Mom bad passed away in '93 and 1 haven't been able to deal with i t Things 1 haven't been able to ta& about and now 1 am able to talk about And talk to my husband, and 1 can't believe that i'm actually tallang to him about it because 1 talked to Susan first and it was easier to talk to her about it, and now l can look at it in a whole different light, and she gave me =me, just a few things that just opened a new dwr for me. And I thought, hmm, she's right.
Homeopathk patients have been shown to b v e a higher psychological rnorbidity and
attach importance to the emotional aspects of their problems and to the counseling
aspects of treatment (Furnham & Bhagrath, 1993; Vincent & Furnham, 1996). Most
respondents felt there is a mind-body comection that should not be ignored and that one
is more likely to achieve wehess by addressing both aspects.
6.4. Avoidance
Avoidance is the comerstone of treatment of ES, including avoidance of many
foods, household products, social and work settings and physical surromdings.
Avoidance is based on the principle of total body load, in that decreasing exposure to
toxias d l decrease the toxic load on the body and so one c m regah heaith (Rea & Ross,
1989). However critics argue that avoidance does not allow ES sufferers to deal with
their illness and patients often becorne socially constri-cted or redusive (Black, 1993).
Most participants in t h i s study did engage in avoidance behaviors, but to varying degrees.
6.4.1. Food Avoidances
Sensitivities to particular food items îypically informed food avoidances. As

previously outiined, the most cornmoniy perceived food sensitiviîies were to daixy, yeast
and sugar, processed foods and those containhg pesticides and presemtives. However,
occasionally rrespondents avoided f& based on physician recommendations or on
allergy testiag results regardless of whether any adverse effects were experienced fiom
the food, This dernonstratecl a willhgness to change behavior to improve health
P2: 1 have no idea what my reaction is except 1 corne out a four here which is not good.
P8: But some of the foods 1 didn't realize 1 was reacting to, like chicken. 1 was fine when I ate chicken, but acçording to the tests, chicken was a problem. 1 couldn't have it.
Pl 1: Well, dl the things that are 1's and î's, if 1 eat them at al1 1 rotate them every four days and 1 don't limit myself with portion size. But then there are things that 1 completely cut out like eggs.. the things that gave me the worst symptoms, pork, garbanzo beans 1 cut out for a while..they say at the clinic, if you're a 1 or a 2 you can rotate, if your a 3 or a 4, you have to cut the food out of your diet for a Ye-c
Many of these avoidances are physician imposed, while many others are self-imposed.
P5: I'm too chicken to try. 1 think it would make me really sick
P7: 1 didn't react to wheat, but 1 don't eat wheat.
There appears to be an underlying belief that avoidance is directly related to
degree of illness, in that the more foods you are sensitive to, the sicker you must be. One
woman staîed that once, for a period of 10 days, she suMved only on water while her
body was recovering fiom an overload. Respondents relayed many stories which imply
they were the sickest seen by their various health consultants.
P2: She tested me for the food cornbining and she said she'd never seen

anybody so sensitive to the combining of foods.
P4: He (Dr. Fox) sees how sensitive we are, but even, we're more sensitive than a lot of people at the chic.
P 1 1: So the next year when 1 finally got into the chic 1 was seen, 1 they think as a favor and b u s e 1 was çonsidered-1 don't want to say criticai, that's not the right wordd was 5 fmt 6 and 102 Ibs, and I was just withering away. So they got me in there really fast. 1 wasn't on the waiting list.
Many looked to theû employers, family, and niends for this support but were often
disappointed by the outcome.
6.43. Avoidance of Social and Work Environments
Avoidance behavior was alw seen in social and work settings. Ofientimes the
work environment was considered the cause of the ailmenî, and most felt they codd no
longer fùnction in a work environment because of incapacitating brain fog and fatigue.
P6: It's so far removed in rny mind now about going back to work now because 1 can't consider that when 1 stniggle to get through the day. 1 would be really nice, it wodd be beyond nice- At first it was al1 I could think about was getting back to work and getting up to that level, but when you're so far down on another level, 1 think finaIly for me came the adjustment.
P 1 1: When 1 absolutely could not work anymore. 1 weighed 102 Ibs, and 1 was eating Iike a pig ..... 1 was anemic. 1 was just totaIly rnalabsorbing f a anything- And 1 was in chronic pain, chronic fatiguey and 1 just couldn't go anymore. 1 just ran out. So my doctor told me to take a month off work and 1 just couldn't go back &er that.
One woman felt that other factors such as discrimination and lack of employer supprt
hindered her ability to work.
P3: 1 can't do what most people do. 1 mean, 1 want to go back to work
if1 could £ind a hedthy work environment But no one will hire me. Discrimination 1 tell them I'm lookng for a healthy work environment
Some women experienced a real sense of loss when they stopped workhg.
P6: It wodd be really nice, it wodd be beyond nice At fïxst it was al1 1 wuld think a b u t was getting back to work and getting up to that level, but when you're so far dom on another level, 1 think finally for me came the adjustment.
P9: 1 worked for 19 years in a banlg ... but I worked ever since, full time, ever since 1 finished school,
1: It m u t have been a big change for you. P9: Yeah, and 1 worked every weekend and sumrners since 1 was 16. It
was a devasfation,
Withdrawal h m work was usually accornpanied by withdrawal fiorn social
fhctions and public places. Most reported that in social events, or going to
public places, exposed them to a lot of environmental contaminants, such as exhaust,
perfumes, cigarette smoke, dust, and pollen, that impacted their heaIth and their abiliîy to
tolerate foods.
P5: Now your getting in a part- and everywhere you go there's smoke. People smoke. You can't avoid it- So that's why we agreed we'd stay only 2 hours, because i f s just going to make me so sick.
P 10: Sobey's, 1 don? go in îhere too often because the fumes bother me. So my husband does the main one in there and 1 have an air machine that 1 Wear. 1 find that good. I don't go down the soap aisles and 1 try to avoid the fish market because of the strong smell of fish. 1 try to avoid people in general. 1 hold my breath a lot and run through Ifs too much and 1 just said to my husband, I have to go sit in the car. He completes it, he's realIy good about it.
However, respondents will occasionally tolerate the reactions fiom socializing and are
not as stringent about their diet when eating out. Respondents recognized that many in
their social circles did not understand their illness and treatment protocols. Rather than
draw more attention to themselves and their illness when socializing, they often tolerated
more exposure than nomal- Conceivably, this could cause M e r stress on the ES
sUnerer, since by not accommodaîing their illness, friends are rejecting its legitimacy.
This may unde~rmine the tmst ES sufferers had in those individuals prior to illness and
add to feelings of isolation,
P2: 1 usually only eat nce when I go out to a pot luck or something.
P3: 1 don't bave any sugar in the diet now, or very little- I shouldn't say any, if 1 go to a piuty 1 eat wbat7s there.
P12: 1 do not eat cheese, If1 was out somewhere and someMy served something, I would have it, but not as a regular.. As a regular diet, 1 am carefid about what 1 eat at home, so then when 1 go out, 1 cm tolerate a few more-
These avoidances are also felt at the family level and are accepted to some degree
by family members,
6.4.3. Avoidance and Family Behaviors
Respondents are keenly aware of how their avoidance behaviors affect those
around them. Sorne respondents express that family members are quite supportive,
although most did not elaborate how their m e r s were supportive. Others stated that
some family members completely fail to understand and accept the illness.
P2: There was quite a long transition getting that acceptance because there was a lot of denial about the illness anyway.
PS: Dad keeps telling me that if 1 start eating like a normal human being, I'd have more energy and Sd feel better. But 1 know darnn well that 1 wouldn't I mean 1 can't take what I have, like just fiesh, fiesh stufK Can you imagine? ... A d , of course, 1 have an aunt who just looks at me, you know, it's al1 in your head. What's a bite of brownie square? One bite. So then when 1 start going on and on
about my supplements and my enzymes. Well, what the hell is an enzyme- Well then you start cluing in_ You know what 1 mean?
There are many family concessions made, particularly around food and meal
preparation OAentimes meals were more work given the Merences in diet tolerances
between the respondent and other family members.
Pd: I'd say okay Sarah let's heat up some soup, let's heat some beans up and Sarah knows those sort of tkngs, and she'll say, if you7re that tüed Momrny can we go d o m to Robin's donuts, they have cream of potato soup today, which she adores. And 1'11 say, yes that's a good one Jillian, we'll just do the fasaest easiest route through this, or I'11 say, it's too hard, you can sit beside me and we'll read or watch TV together, or something, Iike how about you color and 1'11 just Iay here-
P9: 04 there's lots of times that I'Il cook somethîng that I don't eat. I'11 take extra squash or something, like 1'11 cook potatoes, they'll eat it and 1 won't But they eat the organïc foods with me and they eat the organic meats.
P12: My son, one day wanted to transfer to a family who ate meat. So 1 went into the fieezer and pulled out a couple of pork chops. He was so excited So I do that. They occasionally have bacon and occasionally have steak, and it's a treat for them. They at least feel part of the human race.
The cost of buying for the entire family was an issue for some since organic products are
more expensive, however, most found that separating organic foods fiom non-organic
foods w d d be problematic.
PZ: I'd lx having carrots and they would be having some other vegetable, I said this is ridiculous, you know, why don't we al1 have organic carrots together? It's not going to kill them to eat organic mots, nw?
P 10: But I eat everything organic, vegetables, my family eats organic because therey no way I'm going out and buying organic carrots and reguiar canots. They can get mixed up and you don? know what you're eatïng It's too hard for one person to eat it a whole bag
without them going bad.
One woman felt that the changes made in her diet were healthy and are not as expensive
as others may thinEL
P12: Just to give you an example, if you were to buy Piaa Pops for your children, well 1 can go out and buy organic vegetables and 1 can buy my own ingredients to make my own things. So, no 1 wouldn't say..people tend to think that the organics are that much more expensive, but if your not buyuig al1 the junk and al1 the processed food, then the money that you would normally spend on that you spend on the organic stuff.
Interestingly, respondents atiributed their child's health problems to their milk
consumption and imposed some of the same restrictions on the children's diets.
And 1 have a real problem because 1 have a daughter who 1 believe has milk sensitivities and my almost ex doesn't agree with me. Whenever she eats them, she gets really imtable and impossible to be around-
She's got some allergies and she refûses to go to the clinic, so I've had to find other ways. She has asthma, so that tells me that she's allergic. And it tums out that milk is the big culprit for her and she's been reacting to that since she was eight. This nutritionkt was helpful in giving us both..I think thïs was even before 1 got into the chic, she gave us chdenge die6 and taking things out of the diet and bringing them back in And with me it was much harder to see because I had so many things that 1 was allergic to. My daughter was really apparent. Like when she ate milk, her feet stank. Just incredible and she'd have this homile dry cough. As soon as she stopped drinking m a her feet stopped smelling. It was bizane. It was just bizarre.
My both children had ear infections, one after the other until 1 took them off milk.
Most attribute their iII feelings to exposures to food they have cunsumed and feel
107
they are îakhg control of their heaitti by avoiding foods and environrnents believed to
make them ill. Respondents appear to be quite seIf-efficacious given the amount of
change they impose on their Iives with the hope of getting and staying well. SeIf-efficacy
has ken shown to be a powemil predictor of health behavior. It reflects a person's belief
in his or her ability to overwme the difficulties inherent in perfionning a specific task in
a mcular situation. It affects the amount of effort people will expend while adopting a
new behavior and their persisîence in the face of obstacles (AbuSabha & Achterberg,
1997).
Self-efficacy can be confùsed with locus of control, where the former is task
specific and the latter is dornain specific (AbuSabha & Achterkrg, 1997)- An internal
locus of control reflects the patient's belief that an outcome relies entirely on his or her
abilities, a l e an external locus of control reflects the belief an outcorne is controIled by
forces outside their control. Those with an internal locus of control are shown to take
responsibility for their actions and more readily engage in health promoting behaviors.
Respondents demonstrate an internal locus of control by making pervasive, expensive,
and quite restrictive changes in their lifestyle that are believed to promote health. While
this is meant to reflect a high degree of motivation for getting well, it also reflects their
strong belief that the illness is organically derived and that these changes are necessary to
get well. Avoidance is undertaken with the belief that the outcome will result in
improved feelings of heaIth and well-being.
Outcome expectations, or the benefits that result fiom adopting a behavior, have
also been show to be important deteminants in nutrition and health related behavior
(Hofaetter, Sallis, & Hovell, as cited in AbuSabha & Achterberg, 1997). Respondents

108
are willing to adopt a wide variety of behaviors with the outcorne e-tion k ing
improved health, as seen through their use of unproven altemative therapies and dramatic
Iifestyle and dietary changes.
Although avoidance is the comerstone of ES treatment, it may not be conducive to
recovery or to the patient's feeling of control @y, Jefferies, & Weir, 1997). A one year
follow-up study, exarnining 137 CFS sufferers, was conducted to determine factors
rdating to outcornes such as coping skills, locus of control beliefs, and emotional
adjustment. Illness accommodation, or organiring one's life to avoid overexertion and
wntrol stress, predicted change in functional impairment of the CFS sufferers- It
appeared that with increasing illness duration, the more an individual attempts to lirnit
activity and stress, the less that person feels able to do. This was also linked with low
perceived controllability. If the effects of illness accommodation on CFS are conditional
upon perceived wntrol, perhaps interventions aimed at discouraging avoidance
behaviors, rather than encouraging them, rnay help the recovery process and the feelings
of controliability of the illness-
While respondents show an intemal locus of wntrol over the treatment of their
illness, they displayed an external locus of control with regards to tbe omet of their
iIlness. Most agree that their ilhess \vas caused by some insult they had no control over.
P3: 1 guess the VG is when I started g e h g mold sensitivities working there. And then the IWK, that's when 1 developed the worst t h g . 1 got asthma and bronchitis fiom k i n g put in a construction zone, so now I have reactive airways.
P9: 1 don't know what'll happen afterward but 1 do not feel responsible for my health, but I do try to get better. 1 eat, it's on my mind al1 the
time what I'm eating- So you mean when you say that you doda feel responsible for your healîb, that you don? feel responsïble for-.? Getting si&
There was some assault on it [immune system] and it's not functioning properly. Do you know d e n the assault happened? 1 think there was a combination ofthings- The biggest one 1 was working in an 8 by 10 rnoldy oflice. Mold growing like vines.
In my particular case 1 had been poisoned by the autobody shop that was in our school.
The concepts of selfefficacy, locus of control, outcorne expectaîions, and action
proneness al1 appear to be interrelated in the ES sufferer. These actions express that the
ES sufferer desperately wants to regain health. Common to al1 respondents was the active
seeking of information to inform and support their behavior choices.
6.5 Information Gothering
The final theme common to al1 respondents was the need to find out more
information about theu illness, what may affect it, and treatment options. Since much of
what is written about ES is unscientific and unsupported by traditional health care,
respondents relied heavily on pop literature for information Books recommended by
alternative practitioners or other ES patients were the most common sources.
P2: 1 did some reading. 1 went to the rotational Bon Appitite, 1 got the Fit for Life set, I've boughten a couple of cookbooks on various things, right? You know, A Diet for a Small Planet and al1 that kind of books.
P9: I have lots of cookbooks, nutrition cookbooks. 1 don't know what you'd cal1 them, but like the Yeast Connection, the Guide to
Nutrition and Better Healtb, the Heritage &kbook *ch is al1 naturai stuffmostlyy The Candida cookbook, ?he wheat and gluten fiee cookbook So where did you get these, at a regular bookstore? Some of these, tnends of mine have lent thern, most of them I bought at the health fwd store, or wherever 1 could get them. Who killed candida, MaCro.., macrobiotic cooking, secrets to fat fiee bakuig, the allergy cookbook This is what 1 rely on, is cookbooks and self education.
Not sirrpnsingly, the literature read was usually written by people ihat either have
ES or are alternative doctors treating ES. Judit Rajhathy, a self-proclaimed .nutnutntionist,
wrote the popular book Free To Fl'1996) that relates her personal experience with ES.
Upon reading the book, 1 found a lot of similarities between the respondent's words and
the words in this book It appeared many respondents use such books as a guide and took
comfort in their words since it oflen provided corroboration of their own stories.
Respondents also obtained information fiom the community of ES sufferers.
Patients shared expenences and information about their illness and their treatments. This
was typically enjoyed by al1 respondents since it gave them the sense that they are not
alone and that others are experiencing the same problems.
P12: Other tban sharing with one another, sharing with other patients, but that's just on a persona1 basis. It's nice actually because you've made fiends out at the c h i c and we share information and we share this, that, and the other h g . If I'm going to town, 1 might cal1 a couple of them and say, T'm going to get veggies, do you want any, and they might do the same thing.
The NSEHC does foster communication between clients, but there was rnixed
reaction to the information provided by the cIinic- Most respondents did agree that the
c h i c was a source of nutritional infornation, but not a great source. This was somewhat
surprising given the emphasis placed on diet in the treatment of ES. Perhaps,

respondents are not getting the nutntional iaformation they want since most of the
personnel are tradïtionally trained and may not know about or support altemative
remedies. 1: How about at the Health Centre, did they give you any type of
nutrition information? P 1 : A little bit. It was more about just how to rotate your diet, not
about nuirition Like how to.. Yeah, they did that
1: And at the chic, have they given you nutritional advice? P11: No, notreally.
Health food stores were also a common source of information. Participants fiequently
purchased readùig matends fiom there, spoke to the staff, and r a d the information
pamphlets provided.
PI : I've got a lot of knowledge now about just different vitamh and supplements and foods and, just from, yeah and just fiom talking to people in the health food store and things.
P2: -..llnformatioN fiom books and the health food store. 1: 1s it the books that are at the health food store or like the staffthat
work at the health food store. P2: The staff.
These stores do fil1 the need of providing environmentaI1y fiendly products and
organic foods, but the quality of educational training for the staff in naturopathie and
nutritional issues is questionable. Since businesses are profit driven and ES patients are a
captive audience, it raises the possibility that the best interests of the clients rnay not be
s e r v d Environmenîally ill patients are despemfe to find some relief fiom their
symptoms and may be vulnerable to a sales pitch for a particular rernedy.
The greatest concem regarding respondent information sources is their credibility.
These sources are sought because they are sympathetic to the plight of the ES sufFerer.
112
The danger lies in that these sources may not provide an objective, or even accurate,
analysis of the topic king addressed Motivations, such as book sales or profit margins
may affect the integrity of the information, as well as, the lack of weil-informed
individuals who dispense this information Nonetheless, ES sufferers preferentially seek
out these sources rather than information fiom traditional heaith care professionals. This
lends m e r credence to the frustration and wmplete distnist ES sufferers have in
orthodox medicine and the people who praçtice i t
6.6. Discussion of lllness Behavior
The controverq surrounding the etiology of the ES has led to much investigation
into the illness behaviors exhibited by ES sufferers. This discussion is not intended to
judge respondents, but is meant to offer possible motivations and explanations for their
actions as interpreted through the illness behavior model.
Illness behavior refers to the way Uldividuals respond to bodily indications and
how they monitor intemal states ( M e ~ h ~ c , 1995). Physical manifestation is essential to
the individual's perception of illness and the detail with which respondents remunt
symptoms suggests that coping with illness is central to their life. could indicate
theu need to prove the illnws is real. It seemed that respondents believed attention to
detail provides some sort of documentable evidence to non-believers, since feeling this
il1 after consurning a paIticular food cannot be considered normal and healthy. Also, a
necessary part of being sick is actively seeking treatment to get well. This evidence is
presented to health care professionals in an effort to obtain support, treatrnent, and
113
symptom relief However, these ilness behaviors are o h not consistent with the typical
piesentation physicians encounter. Symptoms are finther dismissed as organic in origin
since they do not confonn to medkaI expectations and there is no proporîïonality of
cause and effect However, respondents claim some of their health probIems c m be
attn'buted to immunosuppression, although these women did not ïndicate a greater
incidence of colds, flues, or delayed wound healing, that might be expected with
immunosuppression. has the potential of making the illness less believable to
conventional health care,
Conventional medicine usually considers atypical responses as some form of
somatoform disorder. While this assumption invalidates the respondents' contention that
they lmow their body best, research has shown there is a psychological component in
atypical responses. Evaluation of the psychological factors associated with ES found an
extremeiy strong relationship between the reported number of prior medically
unexplaineci symptoms as rneasured by the National Wtute of Mental Heaith
Diagnostic Interview ScheduIe and the development of ES (p=û.0002) (Simon et al,
1990). Subjects with ES typically d e s c n i d e t y and symptom of autonomie arousal
in response to odours of plastics and petroleum products. The authors suggest that
conditioning and phobic avoidance probably contri'bute to the chronicity of symptoms,
which may be m e r enhanced by a pnor tendency toward symptom amplification.
Development of symptoms was most strongly related with long-standing distress
suggesting that this could contribute to the development and reporting of physical
symptorns,
It is possible that ES women could avoid the stresses of their daily lives by

114
confinhg themselves to their homes. It is difficult to evaluate if the isolation these
women experience is self-imposed as a coping mechanism for daily stressors or for
health related problems. Since sensitivity to some foods can Vary fiom month to month,
respondents could perpetuate the illness and avoid complete recovery until the individual
is psychologically able to wpe with life's demands- It is dso difficult to ascertain
whether the outcome is strictly a placebo-effect or whether dietary and lifestyle changes
are having a positive impact on their health.
The lack of perceived support has contributed to respondent participation in
alternative therapies with reported benefits. However, it is possible that wornen will
daim to notice a difference upon treatment because it is expected they should see a
dinerence, or because it lends more credibility to the organic cause of their illness. By
making what most would consider extraordinary changes to one's diet suggests that the
illness itself is extraordinary in nature, and unlike any other illness seen up to this point
This legitimizes actions taken and detracts from the psychological implications of their
behavior.
By expressing an extemal locus of control over the etiology of their illness,
respondents are also negating the contention that the illness is psychologically bas&
CFS sufferers also separate the body fiom the realm of personal responsibility as a means
of denying a psychological connection In a study that comparai the premorbid &action-
proneness" of 30 CFS patients to 34 patients diagnosed with a chronic organic condition
and to 34 patients suffering fiom neurotic disturbances without somatic complaints, CFS
patients tended to descnbe themselves as significantly more action-prone than neurotic
or chronic organic patients (Van Houdenhove, Onghena, Neerïnckx, & Hellin, 1995).
115
Action-proneness was defined as the extent to which one is oriented toward direct action
and achievement, such as taking on many responsibilities at once. This suggests a link
between action-proneness and somatic illness behavior, in that those wnsidered more
active prior to illness may be using the illness as a means to become inactive in their
current roles- These behaviors are still active in that they actively pursue an illness
identity and accommodate treatments. The secondary gain fiom an 'invalid' role allows
the CFS patient to reverse their relentless activity to a chronic passive-regressive illness
behavior. The authon suggest that physical cornplaints may be viewed as a self-
bandicapping strategy whereby the body is seen as outside the system of personal
responsibility. This could explain the tenacity with which most CFS patients claim viral
or immunological explaoations for their illness and refuse psychological ones.
It appean that action-proneness rnay be iaken a step firther into illness behavior.
Ail energy is now focused on oneself and the illness rather than on extemal matfers such
as work and social obligations that were dominant pnor to illness. One possible
sewndary gain realized is that the illness gives the respondent time to devote care and
attention to one's own needs. The pre-illness lifestyle may not have accommodated or
accepteci any behavior wnsidered self-indulgent nlness provides the justification to step
back fiom work, family, and social obligations that may be physically or psychologically
stressfil. However, these actions also demonstrate withdrawal fiom many activities once
considered integral to their lifestyle, suggesting an inability to cope or, perhaps, a desire
to escape fkom certain aspects of that lifestyle.
Finding behavior-related changes in other family members that cm be contributed
to a specific food supports the contention tbat the illness cannot be psychological if their

116
children are experiencing similar symptorns. However, it is possible that these
individuals may be projecting these symptoms onto their cmdren to fiiaher substantiate
their own iilness claims
Respondents avidly sought more information about their illness fiom alternative
and pop literature sources that supported the legitbacy of the illness- Although these
books may no? be scientifically accurate in content, they fit within the illness belief
system of the respondents and provide 'evidence' that what they are experiencing is
legitimate. This fits within their health behavior pattern of being very active in the
treatment of, and recovery fiom, their illness. Information found could füel the illness
process and inform how the participant should act. Since many of the respondents read
the same books, it was evident that many were repeating what was perceived to be the
'right answer' according to what they had read and what they know about the illness.
However, the spoken word was not always realized in practice, for instance "processed
foods" were said to be avidly avoided yet many of the respondents consunied processed
foods over the four recorded days. Perhaps respondents may be sabotaging their own
health for sorne secondaxy gain, or that food sensitivity is not a true component of the
illness. Altematively, respondents may not have Mly understood the content of what
they read, or simply know how they should eat buî not always wmply. This is not
surprising since diet adherence is difficult at bat, and made even more so by the
restrictive nature of the typical ES diet. WhiIe it is not possible to state unequivocally
that any of these illness behaviors are at work in any of the respondents, this discussion
may provide insight into the fûture management of ES.

CHAPTER VII= CONCLUSION
7.1. Combining Quantitative and Qualitative Findings
The quantitative component of this research provides insight into the actuaI food
comumption of ES suiTerem From this it was detennined that while most are meeting
the RNI's for nutrient intake, respondents were not getting the recommended variety in
their diet, particularly fiom the milk and milk products food group. This was based on
physician tecoumendations and self-imposed restrictions on food intake.
The qualitative component explores why women chose to live and eat in this
manner. The illness behavior mode1 explaineci how individuals may respond and cope
with ES. It provides insight into the factors that may motivate behavior, such as disease
recognition, financial compensation, and sympathy- Health behaviors also contibute to
their lifestyle choices. Respondents engaged in a varïety of behavion, such as home
renovations, diet manipulations, and public withdrawaI as a means to foster health and
recovery.
7.1.1. Credibility of Respondents
Interestingly, words and actions of respondents conflicted in some ways. Review
of food records and claims of avoidance demonstrated some women said one thing but
actually did another. Table 13 provides some examples of discrepancy between the
words and practices of the respondents. 1 do not suspect that respondents intentiomlly
planned to misrepresent their food habits during the interview since they could have
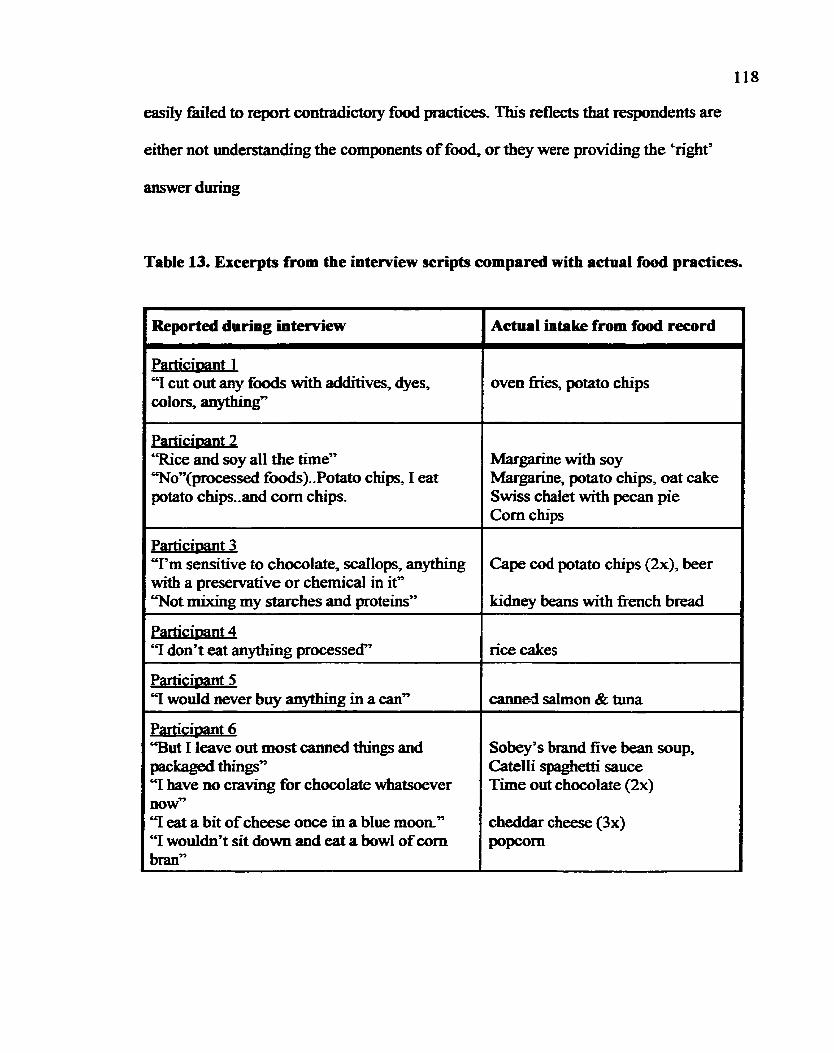
118
easiiy failed to report contradictory food practïces- This reflects that respondents are
either not understanding the components of food, or they were providing the 'rïght'
answer during
Table 13. Excerpts from tbe interview scripts compared with actual food practices.
Particimant 2 '=ce and soy al1 the h e " Ton(processed foods)..Potato chips, 1 eat potato chips..and corn chips.
ParticiDant 3 T m sensitive to chocolate, scdlops, anything with a presewative or chernical in it" T o t mixing my starches and proteins"
Margarine with soy Margarine, potato chips, oat cake Swiss chalet with pecan pie Corn chips
Cape cod potato chips (Sx), beer
k
kidney beans with fiench bread
Reported during interview
Particinant 4 '? don? eat anything processed"
Actual intake from food record
Y would never buy anything in a can"
ParticiDant 6 "But 1 leave out most canned things and packaged things" "I have no craving for chocolate whatsoever now" '7 eat a bit of cheese once in a blue moon" "I woddn't sit down and eat a bowl of wm bran"
L
rice cakes
Particimt 1 "1 cut out any fixxis with additives, dyes,
Sobey's brand five bean soup, Catelli spaghetti sauce T h e out chocolate (2x)
oven fies, potato chips
cheddar cheese (3x) P O P ~
-
-
-
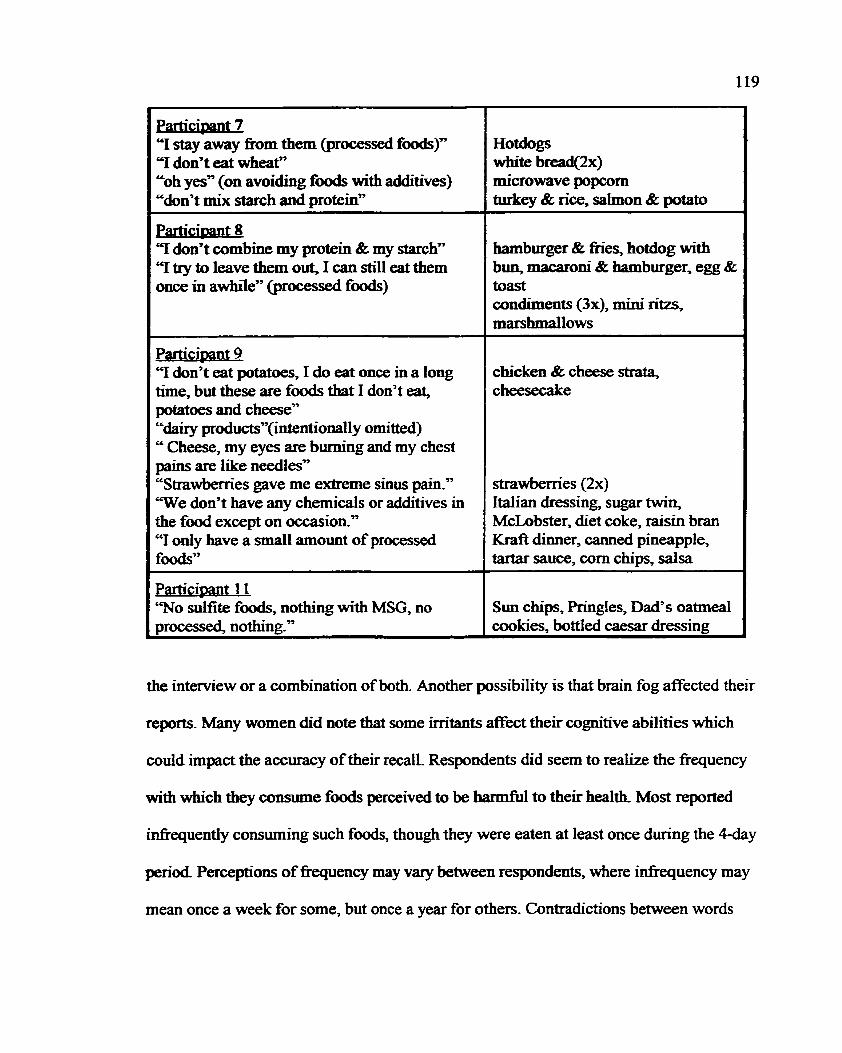
"1 stay away fiom them (processed foods)" "1 don't eat wheatn "oh yes" (on avoiding foods with additives) "don't mix starch and protein"
"I don't combine m y protein & my starch" Y try to leave them out, 1 can still eat them once in awhile" (processed f d )
Participant 9 Y don? eat potatoes, I do eat once in a long time, but these are foods that 1 don't eat, potatoes and cheese" "dairy products"(intentional1y omitted) " Cheese, my eyes are burning and my chest pains are like needIesy' "Strawbemes gave me extreme sinus pain." T e don't have any chernicals or additives in the food except on occasion." "1 only have a small amount of processed f d 7
- . articioant 1 1
'Wo sulfite foods, nothing with MSG, no processed, nothing."
Hotdogs white bread(2x) microwave popcorn aitkey & rice, saimon & potato
hamburger & fies, hotdog with bun, macaroni & hamburger, egg & toast condiments (3x1, mini ritzs, marshmallows
chicken & cheese strata, cheesecake
strawberries (2x) ltalian dressing, sugar twin, McLobster, diet coke, raisin bran Kraft dinner, canned pineapple, tariar sauce, corn chips, salsa
Sun chips, Pringles, Dad's oatmeaI coolcies, bottled caesar dressing
the interview or a combination of both. Another possibility is that brain fog affected their
reports. Many women did note that some irritants afféct their cognitive abilities which
could impact the accuracy of their recall. Respondents did seem to realize the fiequency
with which they consume foods perceiveci to be harmful to theïr health Most reported
infrequently consurning such f d s , though they were eaten at least once during the 4-day
p e n d Perceptions of fiequency may vary between respondents, where infiequency may
mean once a week for some, but once a year for others, Contradictions between words
120
and actions also demonstrates the diaculty individuals have with adhering to restrictive
diets, particularly in North Amencan culture. Such conflict codd lead to feelings of guilt
since they feel they know better, but induige and s&er the consequemes of their actions.
Ifthese foods are contributhg to il1 health, ES sufFerers should be educated by dietitians
to ensure accuracy of uiformation and to provide guidance on healthy eating-
Another statement that questioned the credibility of respondent cIaims was when
parîicipant four commented that she and her good tnend "lost [îheir] foods at the very
same tirne". Given the diversity of respondent reactions to food, it is d ikely that the
same symptoms would occur simultaneously in two different ES sufferers, implying there
is a psychological component to syrnptom provocation. This is supported by one study
that suggested the discrepancy in ES reactions between blinded and unblinded allergen
testing was due to the administering ptiysician7s influence (Jewett, et atJ990). Symptom
provocation by suggestion implies there is a strong psychological component to this
illness.
It is not surpnsing traditional health care questions the ES suf5erers credibility
given the diversity of symptorns and reactions described durhg the interviews. Many
respondents descnid reactions that seemed wmpletely disproportionate to the
provocation However, respondents daim that ES is like nothing the medicai comminiity
has seen before, so they cannot be expected to conform to the current standards and
practices,

TRADITIONAL SYMPTOMS 1 NSEHC MEDICINE
y
l I !
/ ALTERNATIVE THERAPIES 1 !
7.2. Model of Interaction Between Respondents and the Environment.
There is a definite intemon between a11 themes that emerged and the dietary and
lifestyle practices of the respondents. Many facets of the environment have an impact on
the ES patient which, in nirn, infonns their actions and behaviors. This not ody affects
the ES sufferer, but also affects family and fnends. Figure 6 outlines these interactions-
122
The solid lines show how some face& impact on the respondents, while the dashed lines
indicate active interaction.
Traditional medicine, cost, symptoms and allergies al1 impact on the EI patient to
inform theû actions and behaviors. Symptoms motivate respondeats to seek out medical
attention for a diagnosis and symptom relief. Since traditional medicine has yet to find a
cause for the distress, it is Unplied the symptoms are psychosornatic leaving respondents
feeling fhstrated and abandoned. Lack of belief in the reality of their illness has resulted
in rejeztïon of orthodox medicine and its professionals in search of more sympathetic
ones.
Acceptance by alternative therapists is essential to legitirnize ES as a m e , organic
illness and to receive treatments that are hoped to alleviate symptoms. Since respondents
vehemently deny any psychological cause, they reporîed feeling greatly relieved when
they fomd others that supporteci them and their illness. With this support respondents are
willing to follow many of the recommendations made by the NSEHC and other
alternative therapists. However, cost of these therapies may be a barrïer since most
respondents were unemployed and these therapies are not covered by the majority of
heaith care plans. The higher cost of organic and dl-aahiral foods, as well as specidity
items such as yeast-, wheat-, and dairy-fiee ffods were reported to increase the financial
burden ES sufferen endure. Intensive vitamin and mineral supplementation also
contributes to the costs faced by most ES sufferers.
The NSEHC has recommended wstiy home renovations, specid diets and
supplementation for the treatment of ES- However, cost determines the extent to which
respondents can access these various treatment modalities. ES suEerers themselves ofien
123
seek other treatments such as psychotherapy, antigen and physid îherapies which are
not wvered by health insurance.
Once respondents have been accepted at the NSEHC, they are tested for
sensitivities and give rotation die& to follow. S e m testing detemines the respondent's
eligibility for other treatment modalities such as ïV, magnesium, and sauna therapies.
Respondents interact with the staff to obtain information and engage in other treatments
offered at the clinic- Patients form their own support network that serves to validate their
illness by shared experiences. Respondents also share information about various products
and treatments options they have leamed through their own research
Information cm have a significant impact on ES sufferers. Many feel desperate
and actively seek out any information that offers some insight into the cause and
potential alleviation of their symptoms. UnfortunateIy, ES sufferers may be more
vulnerable to creative marketing and claims made by less credible information sources,
such as pop literature and those endorsing unproven treatment regimes. Regardless, it is
those information sources that support ES as an organically based illness that the
sufferers believe and act upon.
Cunrently the most widely recommended treatment of ES is avoidance of
questionable fwd allergens, social and work settings, and products and environments
that are considered toxic. This causes the ES d e r e r to becorne very reclusive, which
can have a great impact on their f d l y and social lives. Respondents withdraw from
work and most social settings for fear of toxic exposure, though it has been argued that
withdrawal is a form of coping with the stresses in their Iives. Although most
respondents daim their work environment caused their illness, they are unable to receive
124
compensation since ES is yet to be recognized as a true illness. This rnay place a great
financial burden on families by reducing household income while treatment and food
expenditures are hcreasing.
Food also plays a major role in the management of the illness. Respondents
engage in radical dietaxy changes that includes omïtting dairy and most grain products
fiom the diet Respondents claim to eat only natural and non-processed foods, and prefer
to buy organïc if possible. While they contend that the mainstream food supply is
deleterious to their health, cost and family preference wiI1 detennine if their food is
shared with other family members. For mosf vitamin and mineral supplementaîion is
intensive since they feel that, although they are eating a healthier diet, their bodies have
p a t e r requirements due to malabsorption and detoxification, Nutrition professionals
should be concerned that ES sufferers are not geîting the recommended variety in their
diet and may not be meeting the RNI for calcium. Intensive supplementation may also be
causing imbalances, though the nsk of toxicity is unlikely.
Much of respondents' time and activity is directeci toward regaining health The
change and work involved in maintaining their illness lifestyle appears to be a statement
on the magnitude and gravi@ of their ilhess. Legitimacy of the ilhess is an essential part
of protecting their own self-conceptions and altering the perceptions of others about the
illness. Respondents take wntrol of their health by actively seeking treatment fiom
sympathetic therapists, and in doing so, feel they are affirming they do not choose or
want to be sick
7.2.1. Highüghts and hpi ia t ions of Findings
1. ES sufierers are not meeting Nutrition Recommendations (Health and
Welfare Canada, 1990) of eating a vaned diet.
Avoidance of problem f& is the central focus in the treatment for ES and has
resulted in the elimrnation of suspected irritants. Foods commonly avoided include
wheat, dairy, yeast, sugar, processed foods, and those containing pesticides. Dairy is
perceived to cause many of the sensitivities in the ES sufferer and has k e n implicated in
their children's health,
The implication of such extensive avoidance is the lack of variety in their food
choices. Perceived food sensitivities, cost, and availability of specialty products has
greatly reduced the food choices of ES sufferers. Dairy is virtually eliminated from the
ES diet, such that sufferers are currentiy not meeting the calcium requirement outlined in
Nutrition Recommendations (Health and Welfare Canada, 1990). Insufficient calcium
intake may place ES sufferers at greater risk for decreased bone density, suggesting
calcium supplementation may be indicated for those avoiding milk products. Dietitians
should work with those ES sufferers sensitive to supplements to identie suitable non-
dairy calcium sources. Dietitians should encourage more variety in the diet while still
respecthg the ES sufferers needs.
2. Respondents have a strong belief ES is a physicat illness.
Respondents deny ES is a somatic disorder and is express4 by the drarnatic
changes they make to diet and lifestyle. These changes appear to be a testament to the

126
sever@ and uniqueness of their illness-
The implication of this belief is that it precludes psychological counseling as a
Iegitimate treatment for ES. While respondents do engage in counseling, it is not because
they believe the root of their problem is psyctiologicai, but is used more as a coping
strate=- Since the debate over ES etiology continues, it cannot be unequivdly stated
that al1 ES sirfferers would experïence syrnptom relief through counseling. However,
some research has shown ES sufferers have a higher incidence of psychiatrie morbidity,
suggesting that some sufferers who daim to have ES may experience reaI benefits fiom
psychological counseling.
3. Lack of support by traditional health care professionals bas resulted in ES
sufferers turning fo alternative practitioners for treatment and care
Respondents relayed feelings of abandonment and fnistration with the medical
community. Most expressed that traditional doctors compartmentaIized their illness and
failed to see that their illness encompassed the total body. Respondents feIt
disexnpowered by îradïtiod health care professionals, since they believed their illness
was not taken serïously. However, respondents assume control over their health by
choosing alternative pfacbces and by taking an active part in îheir wellness.
The implications of the perceived treatment by traditional health care is the
complete rejecîion and mistrust of its @ces by ES Merers Iftraditional medicine
hopes to gain back ES sufferers' confidence, they must first align themselves with
alternative practitioners to obtain a bette, more open-minded, understanding of their
practices. Traditional professionais must recognize the importance ES sufferers place on
127
whole body treatment and work with them to met their needs. Although the medical
community may not consider avoidance the prefened treatment for ES, it is unlikely ES
suBereps wiil change curent behavion unies rhey feel their iIlwss is supporied
Respondents were quite efficacious at making drarnatic changes in lifestyle when they
felt validated and accepted
7.2.2. Concluding Remarks
In conclusion, regardless of the cause of ES, respandents made drarnatic lifestyle
changes that may be rnotivated by the need to legitirnize the illness. ALI aspects of an ES
sufferers lîfe, and ofientimes their families, are impacted by the illness and its
treatmenb. Currently, the medical commufllUfllîy is not meeting the needs of ES sufEerers
compelling them to seek out more sympathetic care givers. Health professionals need to
reesîablish the trust and confidence of ES sufferers if we are to help them live with and
overcome ES,

Abusabha, R & Achterberg, C. (1997). Review of selfefficacy and locus of
1 of the Amencan Dktetic contro1 for nutrition- and health-related behaviour, Jouma 1
Association, - -
97,1122-1 132.
Amen'can Medical Association. (1992). Clinical ecology Council on scientific
I of the Arne ical Assoc - -
affairs. Journa ncan Med iation 268,3465-3467.
Andon, M. B., Smith, K. T., Bracker, M., Sartoris, D., Saltman, P-, & Strause, L-
(1991). Spinal bone density and calcium intake in healthy postmenopausal women
Amencan Jqurnal of Clinical Nutrition, 54,927-929.
Anthony, H. M, & Maberly, D. 1. (199 1). Weight changes in chronically il1
patients with evidence of multiple intolemces to foods, chernicals and inhalants. Journa!
of Nutritional Medicine, 2,13 1-14 1.
Ametz, B. B. (1996). Causes of change in the health of populations: A
biopsychosocial viewpoid Socioloey. Science & Medicine. 43.605608.
Balch, J. F. & Balch, P. A. (1997). Prescnotion For Nutritional H e a l i n ~ 2" ED.
Garden City Park, NY: Avery Publishg Group.
Bandura, A. (1977). Self-efficacy: toward a unifjing theory of behavior change.
& ~ b o f ~ p Review- 84-19 1-2 15.
Bell, 1. R., Miller, C. S., & Schwartz, G. E. (1992). An olfactory-limbic mode1 of
multiple chernical sensitivity syndrome: Possible relationships to kindling and affective
spectm disorders. Biolo~ical Psvchiam. 32.2 1 8-242.
BIack, D. W. (1993). Environmental illness and misdiagnosis - a growing
problem m t a t o r v To~cology and Phitrmpcolw. 18.23-3 1.
Black, D. W., Rathe, A., & Goldstein, R B. (1990). Environmental illness: A
00ntroIled study of 26 subjects with '206 centiiry disease'. Journal of the American . .
cal Associatton- 3.64.3 166-3 170-
Braam, L- A, Ocke, M Ca, Bueno-de-Mesquita, H B-, & Seidell, J. C. (1998).
Determinants of obesity-related underreporthg of energy intake- Amencan Journal of
JZpidemioloev, 147,108 1-1086.
Bnefel, R R, Sempos, C. T., McDowell, M. A., Chien, S., & Alairno, K (1997).
Die- methods in the third National Health and Nutrition Examination Survey:
Underreporting of energy intake. Amencan Journal of Clinical Nutrition. 65.1203s-
1209s-
Brodsky, C. M. (1983). Psychological factors contributing to somatofom diseases
aîtributed to the workplace- The case of intoxication Journal of Oççupational Medicine,
Carey, J- W. (1993). The ethnographie context of illness among single-women-
headed households in rural P ~ N Health Care Women International. 14-26 1-270.
Tests: Values and h ~ l i c a t * . Cl inical Laboratory ions (2" ed.). (1995). Spnnghouse,
PA: Springhouse Corporation
Cox, 1. M., Campbell, M. J., & Dowson, D. (1991). Red blood ce11 magnesium and
chronic fatigue syndrome. The Lancet. 337.757-760.
Crook, W. G. (1 986). The Yeast Comection: A Medical Breakthrou* Jackson,
TN: Professional Publications Inc-
Cullen, M. R (1987). The worker with multiple chexnical sensitivities: an
ovem-ew. In: M R Cullen @), Occ-l M e a e State of the Art Reviews. - .
Philadelphia: Hanley and Belfus Inc. @p. 655661).
Davidoe A L., & Fogarty, L. (1994). Psychogenic ongins of multiple chernical
sensitivities syndrome: A critical review of research literaîure- Archives of
Environmental Health, 49,3 16-325-
Davidoff, A. L., & Keyl, P. M. (1996). Symptoms and health status in individuals
with multiple chem-cal sensitivities syndrome fiom four reported sensitinng exposures
and a general population comparison group- Archives of Environmental Health. 51.20 1-
213,
Dismukes, W. E., Wade, S., Lee, J. Y., Dockery, B. Ky & Hain, J. D. (1990). A
randornid, double-blind hial on nystatin therapy for the candidiasis hypersensitivity
syndrome. The New Enpland Journal of Medicine. 323,171 7-1 723.
Wrland's mcket medical dictionary (25" ed). (1995). Philadelphia: W. B.
Saunders Company.
Dumke, N, M. (1994). The EPD Patient's Cookine and Life-le Guide.
Louisville, CO: Allergy Adapt hc-
Eldridge, A L., & Sheehan, E. T. (1994). Food supplement use and related beliefs:
Survey of communiw college students- Journal of Nutn-tion Education 26,259-265.
Environmental Health Center. Rotational Bon Apxtit! . Unpublished cookbook.
Fieder, N., Maccia, C., & Kipen, K (1 992). Evaluaîion of chemically sensitive
patients. Journal of Occmonal Medicine. 34 529-538.
Fumham, A & Beard, R (1 995). Health, just world beliefs and coping style
preferences in patients of complernenîary and orthodox medicine. Sociology. Science. & . *
Medicine. 40,1425-1432.
Furnharn, A, & Bhagrath, R (1993). A cornparison of health beliefs and - -
behaviours of clients of ortfrodox and complementary medicine. British Ioumal of
Clinical Psvcholo~v- 32,237-246.
Funiham, A & Kirkcaidy, B. (1996). The health beliefs and behaviours of
orthodox and complimentary medicine clients. British Journal of Clinical PsychoIo%
35,49-6 1,
Gilbert, A. N., & Knasko, S. C- (1997). Sex differences in task performance
associated with attention to ambient dora Archives of Environmenial Health, 52,195-
199.
Grant, J, E. Veldee, M S-, & Buchwald, D. (1996). Analysis of the dietary intake
and selected nutrient concentrations in patients with chronic fatigue syndrome. Journal of
She Amencan Dietetic Association- 96,383-386.
Gullestad, L., Doha, L. O., Birkeland, Ky Falch, D., Fagerîun, K, & Kjekshus, J.
(199 1). Oral versus intravenous magnesium supplementation in patients with magnesiwn
deficiency Magnesium & Trace Elements. 92,11-16.
Guthrie, H. A. & Picciano, M. F. (1995). Human Nutrition. St. Louis, MO: Mosby
- Year Book Inc,
Hahnemann, S. (1982). Qpa . . non of Medmne. Los Angeles, CA: J. P. Tarcher.
Haller, E. (1993). Successful management of patients with "multiple chernical
sensitivities" on an inpatient psychiatrie unit Journal of Clinical Psvchim. 54,196-199.
Hathcock, J. N., Hattan, D- G., Jenkins, M. Y., McDonald, J. T., Sundaresan, P.
R, & Wiikening, V. L. (1990). Evduation of vitamin A toxiciîy. American Journal of
C h i c d Nhtion. 52.1 83-202.
Heaith and Welfare Canada (1990). rJutnt10 * -
n Recommen ons: The remrt of . - ~ h e scientific review cornmittee. Ottawa, ON: Canadian Govemment Publishing Centre.
Health and Welfare Canach (1993). Nova Swtia Heart Health Prorrram: Rewrt of
the Nova Scotia Nutrition Swev- Halifax, NS: NSHHP.
Jeweit, D. L., Phil, D., Fein, G., & Greenberg, M H (1990). A double-bhd study
of symptom provocation to detemine food sensitivity. The New Endand Joumal of
Medicine. 323,429433.
Jones, D. (1992). Nova Scotia ody province to provide clinic for
"environmentally sensitive7' patients. Canadian Medical Association Journal. 1 47,93 1 - 933.
Kandrack, M., Grant, K. R., & Segall, A- (1991). Gender differences in hedth
related behaviour. Sorne unanswered questions. Sociolow. Science. & Medicine. 32,
579-590.
Kelner, M. & Wellman, B. (1997). Health care and consumer choice: Medical and
altemative therapies. Sociolo w- Science. & Medicine. 45,203-2 12.
Kiley-Mullaly, S. C. & Glanville, N. T. (1998). Diet and environmental illness:
barriers encountered by womea sufferers. Canadian Joumal of Dietetic Practice and
Research. 59.12 1-124.
Kowalski, T. E., Falestiny, M., Furth, E., & Malet, P. F. (1994). Vitamin A
Ith Per~pectives. 1 chernicals Environmental Hea 01,234238,
Meggs, W. J., DUM, K. A, Bloch, R U, Goodman, P. E., & Davidoff, A. L.
(1996). Prevalence and nature of allergy and chernical sensitivity in a general population
MetMe, D. D.(1985). Diagnosis and matment of food hypersensitivity. In A. P.
Kaplan (Ed), (pp. 579497). New York NY: Churchill Livingstone.
Miller, D. R & Hayes, K C. (1982). Vitamin excess and toxicity. In J. N.
Hathcock, ml, Mltrmona * -
1 Toxicolo~ @p. 8 1- 133). Orlando, FL: Academic Press.
Miller, M. (1996). Diet and psychological healtk Alternative ï'hera~ies in Health
md Medicine, 2,4048.
Montbriand, M J. (1995). Alternative therapies as control behaviours used by
cancer patients. Journal of Advanced Nusinp 22,646-654.
Monis, D. H., & Stare, F. J. (1 993). Unproven diet therapies in the treatrnent of
the chronic fàtigue syndrome. Archives of Familv Medicine. 2,18 1 -1 86.
Morrow, L. A., Ryan, C. M., Hodgson, M, J., & Robin, N. (1990). Alterations in
cognitive and psychologicai fMcîioning after organic solvent exposure. Journal of
Occu~ational Medicine, 32,444450.
Nova Scotia Deparûnent of Health (1997). Report of the Advisorv Committee on
Environmental H m . . . rsensibwtv.
Parker, S. L., Krondl, M, & Coleman, P. (1993). Foods perceived by aduits as
1 of the American D causing adverse reactions. Journa ietetic Association, 93,4044.

hepatotoxicity: A cautionary not regarding 25,000 IU supplements. Amencan Journal of - - Wrcme- 97,523-528,
M. B., & Henneberger, P. K. (1995). Patients with multiple chemical
sensitivities in an occupatiod health clhic: Presentaîion and follow-up. Archives of
Environmental H d h , 50.42543 1-
Lewis, S K (1995). Nlergy & Candida Cookinp- Rotational S a - Ames, IA:
Heuss Printing Inc.
Lewith, G. T., & Watkins, A. D. (1996). Unconventional therapies in asthma: An
o v e ~ e w . Nlerszv- 5 1.76 1-769-
Linde, K., Clausius, N., Ramirez, G., Melchart, D, Eitel, F., Hedges, L. V., &
Jonas, W, B. (1 997). Are the clinical eEects of homwpathy placebo effects? A meta-
analysis of placebo-controlled trials. The Lancet, 350,834-843.
Mahan, L_ K. & Escott-Stump, S- (1996). Krause's F& Nutrition & Diet
Theravv ( 9 ~ ed.). Philadelphia: W.B. Saunders Company.
Marieb, E. N. (1995). Human Anatomv and Phvsidogy (3" ed). Redwood City,
CA: The Benjarnid Cummings Publishing Company.
McGovern, J- 1, rivaroni, J- A, Hicks, MF-, Adler, J. C., & CIeary, P. (1983).
Food and chemical sensitivity. Clinical and immunologie correIates. Archives of
Otolanmg9logv. 109,292-297.
Mechanic, D- (1995). Sociological dimensions of illness behavior. Sociolopu,
Science & Medicine. 4 1,1207- 12 1 6.
Meggs, W. J. (1 993). Neurogenic inflammation and sensitivity to environmental
Parker, S. L., Sussman, G. L., & Krondl, M (1988). Dietary aspects of adverse
reactions to foods in adults. Canadian Medical Association Journal. 1 39,7 1 1-7 17-
Patîenon, R E., Kristal, A. R, Lynch, J. C., & White, E. (1 995). Diet-cancer
related beliefs, knowledge, nom, and tbeir relationship to heaIthfbl diets. Journal of
Nutition Fducation- 27,86-92.
PfeBer, C. C. (1975). Mental and Elemental Nutnents: A Phvsician's Guide to
Nutrition and Health Care. New Canaan: Keats Publisbïng.
Rajhathy, J. (1996). Free to Fly A Joumev Toward Wellness, Halifm NS: New
Worid Publishing.
Randolph, T. G. (1987). F.nvironmenta1 Medicine: Be@mines and Bibliwa~hies
ofCliniçal EEOloglY Fort Collins, CO: Clinical Ecology PubIications.
Ray, C., Jefferies, S., & Weir, W. R C. (1997). Coping and other predictors of
outcome in chronic fatigue syndrome: A 1-year follow-up. Journal of Psvchosomatic
Research, 43,405-4 15.
Rea, W. J. (1982,October).Allery - A disease of the twentieth century. Paper
preseated at the meeting of the AFC public meeting.
Rea, W. J., & Ross, G. H. (1989). Food and chemicals as environmental incitants.
Nurse Pracbbone -
r, 14,17-40.
Rosenberg, S. J., Freedman, M- R., Schmaling, K. B., & Rose, C. (1990).
Pemnality styles of patients asserting environmental ihess. Joumal of Occupational
Medicine, 32,678-68 1,
Ross, G. H. (1992). Hisory and clinical presentation of the chemically sensitive

patient. Toxicolow and Industrial Health & 2 1-28.
Ross, G- H (1992). Treatment options in multiple chemical sensitivity.
Toxicology and Industrial Health. 8.87-94.
Ross, G. H, Rea, W. J., Johnson, k R, Maynard, B. J., & Carlisle, L. (1990).
Evidence for vitamin deficiencies in environmentally-sensitive patients- Cl inical
~ l o w . 6.60-66.
Salvaggio, J. E. (1996). Understanding clinical immunological testing in aIIeged
chemically induced environmental illnesses. w l a t o e Toxicolow and P h m a c o l o ~
Sawler, k (1 997). Environmental sensitivities in children. Unpublished master's
thesis, Mount Saint Vincent University, Halifax, Nova Scotia, Canada-
Schafer, R. B., Schafer, E, Bultena, G. L., & Hoiberg, E. 0. (1993). Food safety:
An application of the HeaIth Belief Model. Jounial of Nhtion Education. 25,17-24.
Schaurnberg, H., Kaplan, J., Windebank, A., Vick, N., Rasmus, S., Pleasure, D., &
Brown, M .Te (1983). Sensoq neuropathy fiom pyridoxine abuse: a new megaviîamin
syndrome. New England of Medicine- 25,445-448.
Shepherd, S. K & Achterberg, C. L. (1 992)- Qualitative research methodology:
data collection, analysis, interpretation, and verification. In E. R. Monsen (Ed.),
Research: Succ~ssful Awroaches @p. 82-99). Chicago, IL: The Amencan Dietetic
Association.
Shorter, E., Abbey, S. E., Gillies, L. A., Singh, M., & Lipowski, 2. J. (1992).
Inpatient treatment of persistent somatization. Psychosomatics- 33,295-30 1.
Simon, G. E., Daniell, W., Stockbridge, H_, Claypoole, K, & Rosenstock, L.
(1993). hunologic , psychological, and neuropsychological factors in multiple
chemical sensitivity. A controlled study. Annals of Intemal Medicine. 19% 97-1 03-
Simon, G- E-, Katon, W- J., & Sparks, P- J- (1990)- Allergic to life: Psychological
factors in enWonmenta1 illness. American Journal of Psychiam 147.90 1-906.
Sollner, W., Zingg-Sc& M., Rumpold, G-, & Fritsch, P. (1997)- Aüïtude toward
alternative therapy, cornpliance, with standard treatment, and a need for emotional
support in patients with melanoma. Archives of Dennatoloey. 133.3 16-32 1.
Sparks, P, J., Daniell, W., Black, D. W., Kipen, H. M., Altman, L, C., Simon, G.
E., & Terr, k 1. (1994). Multiple chexnical sensitivity syndrome: a clinical perspective. 1.
Case definition, theories of pathogenesis, and research needs. American Colle~e of
upational and Environmental Medicine- 36,718-730.
Sparks, P. J., DanielI, W., Black, D. W., Kipen, H- M., Altman, L. C., Simon, G.
E., & Ter, A. 1. (1994). Multiple chemical sensitivity syndrome: a clinical perspective.
II. Evaluation, diagnostic testing, treatment, and social considerations. Amencan College
of Occupational and Environmental Medicine. 36,73 1-737.
Stretcher, V. J., & Rosenstock, 1- M. (1997). The health belief model- In Glanz, IC,
Lewis, F. M, & Rimer, B. K (Eds.), Health Behavior and Heath Educah'on (pp. 41-59).
San Francisco, CA: Jossey-Bass Publishers.
Terr, A 1. (1986). Environmental illness: A clinical review of 50 cases. Archives
pf Interna1 Medicine. 146,145-149.
Van Houdenhove, B., Onghena, P., Neerinckx, E, & Hellin, J. (1995). Does high
'action-proneness' make people more vulnerable to chronic fatigue syndrome? A

controlled psychometric study. Journal of Psychometric Research. 39,633440-
Vincent, C., & Furnbam, A (1996). Why do patients tum to complernentary - - medicine? An empirical study. British Journal of Clinical Psycholopv. 35.37-48.
Waddell G., Main, C. J., Morris, E- W., Di PaoIa, M, & Gray7 L C. M. (1984).
Chronic low-back pain, psychologic distress, and illness behavior. Svine. 9,209-2 13.
Zeman, F- 1. (1991). Çlinical Nutrition and Dietetics (2" ed). New York
Macmillan Publishing Company.

APPENDIX A
Information Sbeet
Hello,
My name is Eluabeth Crawley and I am a graduate student at Mount S t Vincent
University. 1 am currently conducting a shidy on food and wornen with environmental
semitivities. 1 appreciate that you are talong the tïme to read this letter descn'bing my study and
hope that you will consider participatingg
-
About the study.-.
The purpose of this study is to look at what people with environmental semïtivities eat If you
agree to do this, 1 will meet with you for a one-hour session at a time and place that is convenient
for you. As a participant, you will be asked to complete a four-day food record I will provide you
*th wriüen and v d verbalctions on how to do this. A food record means that you will be asked
to write d o m everything you eat for 4 consecutive days on sheeis that will be provided to you. 1 will
pick up the completed record and go over it to make sure everything is cl- During the first
session, 1 will ask you questions about the foods you eat, about any beliefs you may have about the
food you eat, and how the food you eat affects your health and well king This session will be taped
with your permission and the tape recorder may be tumed off at any time on your request. Once the
taped session has k e n transcriied to paper, I will go over it with you again to make sure that it
accurately reflects what you said and believe to be true. During this first session, 1 will also measure
your height and weight for the purposes of sssessing your heaIth. Once this data has been analyzed,
you may be asked to participate in a one hou., more indepth session where you have the nght to
r e f k parbcipation Again these sessions will be taped with your permission and the tape recorder
will be tumed off at your request. The transcn'bed conversation will be reviewed with you to ensure
accuracy. Please be ensured that 1 will respect your sensitivities and will follow the AEHA
recomrnendations. As well, our sessions will be confidential. If 1 am to refer to your comments, a
pseudooym wiil be used to ensure you canmt be identined in any way. During the study, only 1 will
have access to the taped recordings. At the end of the study, al1 taped recordings of the sessions will
be erasecL Please remernber that participation in this study is voluntary and you may withdraw fiom
the study at any tirne without any fom of penalty.
THANK YOU FOR YOUR TIME.
APPENDIX B Participant Information Sheet
ION S-T
How long have you been a patient at the Nova Scotia
Environmental Health Center? years months,
Are you between the ages of 30 and 50 years? - YES - NO
What is vour name?
Your phone number?
Or contact the researcher to leave your information:
Elizabeth Crawley
Graduate Student, Mount St. Vincent University
Phone: 477-7962
E-mail: [email protected]

APPENDIX C
Informed Consent

Letter of Consent
This is to certifjr that ï, agree to participate as a volunteer in a scientific investigation as part of the nutrition research program of Mount Saint Vincent University under the supervision of Dr- N- Theresa Glanville.
The investigation and my part in the investigation have been defined and fully explained to me by Elizabeth Crawley and I understand her explanation.
1 have been given an opportunity to ask whatever questions 1 have had, and al1 such questions have been answered satisfactody.
1 understand that 1 am fkee to deny any specific items or questions in interviews or questionnaires.
1 understand that any data or amavers to questions will remain confidential wîîh regard to my identity-
I have been informed that there is no nsk to my health for participating in this study.
I M e r understand that 1 am fiee to withdraw my consent and terminate my participation at any time.
This project has received approval fkom the Ethics Review Cornmittee of Mount Saint Vincent University. If you have any questions regarding this, please contact Dr. Sheva Medjuck, Director of Research, at 457-6296,
Date
Date
Subject's name
Investigator's signature
Date hvestigator's signature
Witness

APPENDIX D
CDay Food Record
(reduced to fit letter paper)

DATE: NAME:
FOOD INTAKE RECORD - DAY 1

APPENDIX E
Written Instructions
Instructions on completing your food record
Record everything you eat and dnnk (except water) dunng the four day period. Record each day on a separate sheet The food record should be done for 4
consecutive days, with one day a weekend day. If you are on a rotational diet, record Day 1 to Day 4 of your diet.
Include: - amount of food eaten using mmmon household measures ( teaspoon, tablespoon, cup, ounce). - food preparation method (boiled, fned, broiled, steamed. etc.) - time of day the meal was eaten - food description (raw, canned, frozen, wholewheat, skim, Ight, etc.)
For combination items, list each item separately, e.g. a ham sandwich would be
recorded as bread, butter, mayonnaise, ham, etc. For items prepared from a recipe, record the estimated intake of each ingredient for the portion you ate. It is
asked that you provide me a copy of these recipes.
lnclude items added to or eaten with other foods such as butter or margarine on
vegetables, milk and sugar in t e d coffee, salad dressings, pickles, gravy, etc.
fnciude candy or other snack items, soft drinks, coffee, tea, alcoholic beverages.
Record any vitamin andlor mineral supplements by brand name, content, and
dose for each day it was taken .
Please rernember our intent is not to judge you. We ask that you try to
make every effort not to change your usual food habits over the coume of these A
four days. It is important that the food records reflect what you typically eat.

APPENDLX F
Interviewer Admiaistered Questionnaire

INTERVIEWER- ADMINISTERED QUESTIONNAIRE
1. How long have you been a patient of the NSEHC?
2. Have you changed your diet since king diagnosed with ES? YES No -
Ifyes, how is it different?
If applicable: 3. Who prepares the h i l y me&?
3a. Has this changed since becoming ill? YES NO-
If applicable: 4. Are the family meds any different from what you eat? YES NO -
If yes, in what way?
5. Where do you shop for food?
Grocery store Fanner's market Health Food Stores Convenience Store m e r
6. Do you find thaî changes in your diet has changed the cost of your grocery bill?
If yes, how? Increased , by how much? Decreased , by how much?
7. Can you get the food you like in the winter?
If no, what foods?
How do you change your diet because of this?
8. Did you have any food allergies pnor to king diagnosed with ES?
I f yes, which ones?
9. Hiive you developed any aew food allergies suice diagwsis? YES No-
If yes, which ones?
10. Do you intentionally leave any foods out of your diet? YES No-
If yes, which ones?
11. Do you believe that some foods wili affect your health:
In a positive way?
If yes, what foods and in what way?
In a negative way? E S - NO -
Ifyes, what foods and in what way?
12. Are you curreniy taking any vitamin or mineral supplements? YES -
13. Do you parîï~ipate in therapies to help regain your health? YES N o - Ifyes, pIease which ones & how often massage
acupuncture mineral and vitamin therapy homeopathy other counselling other therapies
14. What do you believe these therapies wilI do for you?
15. Where do you obtain your nuîrïtion information?
Nutritionist, Dietitian Physiciad Nurse NSEHC Health food stores Media (TV, newspapers) Books Oîher
16- Do you believe that your diet contributes to your overall health?
ES- NO-
If yes, in what way?
17. Whaî is your age?
28. What is the highest Ievel of schooling you have completed?
No formal schooling Some prirnary Elementary / some high school Compieted high schooi Some communïty college, technical college, etc. Completed community college, technical wllege, etc. Some university did not wmplete degree Completed university degree
Bachelor Master PhD or MD.
19. Do you work outside the home? YES No-
If yes, what do you do?
20. Were you working prior to developing environmental sensitivities (ES)?
=s- NO -
If yes, where?
21. What do you thuik is the likelihood of experiencing harmful effects fiom each of the
following 1 = not very likely 2 = somewtiat likely 3 = very likely
bacterial micro-organisms on food when purchased 1 2
yeast in food 1 2
food additives in food 1 2
artificial sweeteners 1 2
tea and coffee 1 2
dned fruits 1 2
herbs 1 2
nuts 1 2
22. Please respond to the followîng statements with:
D = respondent disagrees with the statement
U = respondent is undecided, neither agrees nor disagees
A = respondent agrees wïth the statement
1 find it costs too much money to eat a diet that will not h m me. D
I believe that my diet helps me stay healthy. D
1 believe that what 1 eat will affect my health. D
1 find it hard to shop for appropnate foods in grocery stores. D
Cost of food does not matter if the food rnakes me feel better. D
1 f5nd it easy to change my eating habits when I know it is D
for my health.
1 find it bard to find foods that will not harm me. D
There is little 1 can do to make sure the food 1 eat is safe D
1 can develop allergies to a food by eating too much of i t D
By resting my immune system, 1 can eat more types of food. D
Food allergies are for life. D
Regular physical activity is a part of staying well. D

23. Please respond to the following statements with:
F = respondent thinks statement is fdse
DK = respondent does not know
T = respondent thinks statement is tme
Unsaturated fats should only be eaten in lirnited quantities.
M o l e grain breads and cereals are the only sources of dietary
fibre.
Dairy products made fkm milk are the best source of calcium-
People can protect their health by talang vitamin and mineral
supplements.
Regular margarine contains less fat than butter.
Processe. foods are high in additives and preservatives.
Diets should be hEgh in protein and low in carbohydrate-
Peas and beans are good sources of soluble fibre.
Eating a variety o f foods provides al1 the vitamins and minerais
1 need.
There should be more foods like breads & pasta in my diet.
Eating fiesh fruits & vegetables wilI improve my health.