pact 2011 enviromental hazards -...
TRANSCRIPT
PACT moduleEnviromental hazards
Intensive Care Training ProgramRadboud University Medical Centre Nijmegen
Content
• Infections
• Chemical warfare
• Burns
• Blast wounds
Anthrax
• Bacillus anthracis
• Aerobic, gram-positive spore-forming rod
• Found in soil with infection most commonly in herbivore mammals
• Human contact with contaminated animal products
Anthrax
Clinical infection
• Cutaneous (most frequent)
• Gastrointestinal
• Inhalational (pulmonary)
• Injectional (drug use)
Anthrax - pathogenesis
• Presence of a capsule
• Production of 2 exotoxins (lethal factor - inactivates MAPKK & edema factor - increases intracellular cAMP)
• High microbial concentrations in infected hosts
Cutaneous anthrax
• 95% of reported anthrax cases
• Subcutaneous introduction of spores
• Painless pruritic papule 3 - 5 days following infection developing in characteristic black eschar
• With appropriate antibiotics death uncommon
Cutaneous anthrax
Gastro-intestinal anthrax
• Ingestion of poorly cooked meat
• Oral-pharyngeal (oral or esophageal ulcer with lymphadenopathy, edema and sepsis) or lower GI form (nausea, bloody diarrhea, acute abdomen, ascites and sepsis)
• High mortality (may approach 100%)
Gastro-intestinal anthrax
Inhalational anthrax
• Inhalation of small spores < 5 μm
• Two-stage illness (modal incubation time of 10 days) with flu-like symptoms followed by second fulminant stage with high fever, dyspnea, cyanosis, shock and sometimes hemorrhagic meningitis - very high mortality
• Mediastinal adenopathy and hemorrhagic pleural effusions
Inhalational anthrax
Injectional anthrax
• Mostly after subcutaneous heroin injection
• Tissue swelling and soft tissue infection 1 - 10 days after injection - no black eschar
• Surgical debridement and fasciotomy often necessary
• Intermediate mortality
Injectional anthrax
Diagnosis
• Gram stain and culture from blood and different sites
• Real-time PCR
Treatment (CDC)
• Ciprofloxacin (2 dd 400 mg/iv) + Pen G (6 dd 4 × 106 U) + Clindamycin (3 dd 600 mg) for severe disease (60 days)
• Ciprofloxacin alone for cutaneous form
• Anti-toxin therapies still experimental
• Pleural fluid drainage with inhalational form
Hicks CW. Intensive Care Med 2012;38:1092-1104
Brandwonden - EMSB
• Eerste opvang (buiten ziekenhuis)
• Koelen door spoelen (10 min) met lauw stromend water
• Bij chemische brandwonden 45 minuten
• Koelingsdeken voor transport controversieel
• Ainhalatie-BCO/Cyanide-C-D-Ewarme omgeving
• Infuus vanaf 15% (kinderen 10%) TVLO
• 4 ml/kg/%TVLO per 24 uur waarvan de helft in 1ste 8 uur van af moment van verbranding
Wanneer naar brandwonden centrum?• > 10% TVLO (> 5% bij kinderen)
• > 5% 3de graads verbranding
• Bejaarden en kinderen
• In combinatie met ander trauma/inhalatie
• Verbranding functionele gebieden
• Electriciteit en chemische verbranding
Halfzittend
Beoordeling brandwond
• Uitgebreidheid
• Regel van 9 ( bij kinderen relatief groter hoofd)
• Lund en Browder Chart
• Eerste graad telt niet mee
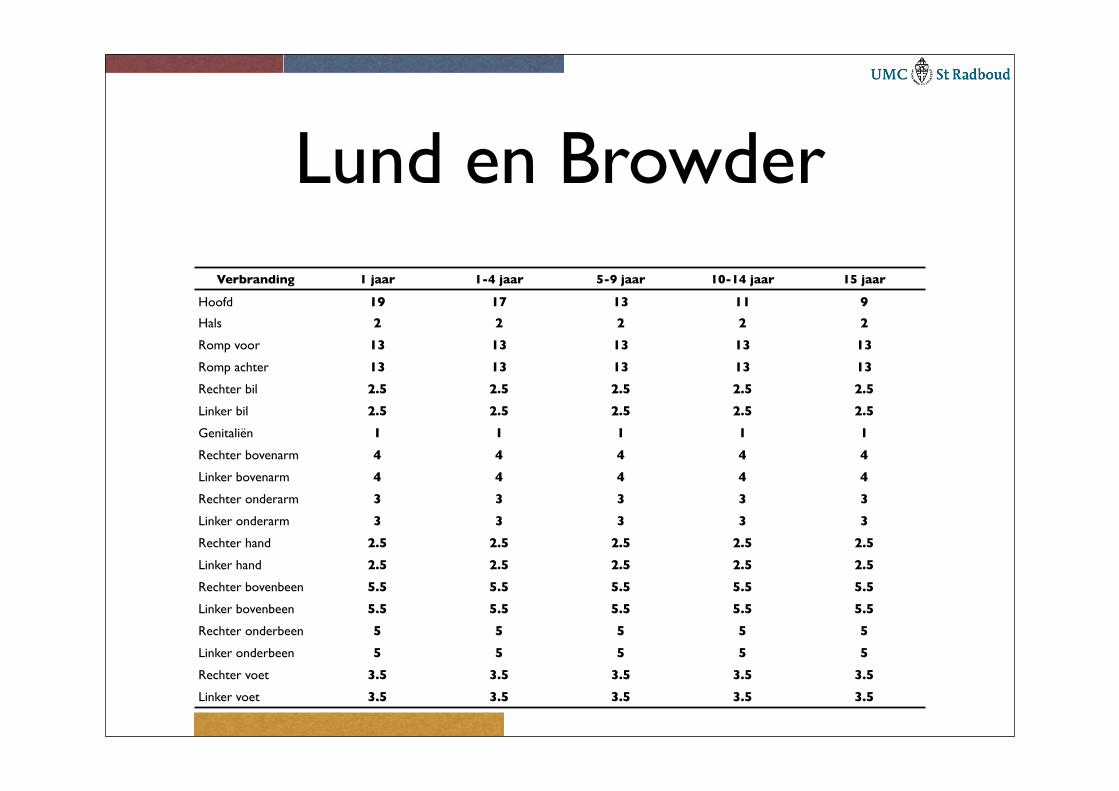
Lund en BrowderVerbranding 1 jaar 1-4 jaar 5-9 jaar 10-14 jaar 15 jaar
Hoofd 19 17 13 11 9
Hals 2 2 2 2 2
Romp voor 13 13 13 13 13
Romp achter 13 13 13 13 13
Rechter bil 2.5 2.5 2.5 2.5 2.5
Linker bil 2.5 2.5 2.5 2.5 2.5
Genitaliën 1 1 1 1 1
Rechter bovenarm 4 4 4 4 4
Linker bovenarm 4 4 4 4 4
Rechter onderarm 3 3 3 3 3
Linker onderarm 3 3 3 3 3
Rechter hand 2.5 2.5 2.5 2.5 2.5
Linker hand 2.5 2.5 2.5 2.5 2.5
Rechter bovenbeen 5.5 5.5 5.5 5.5 5.5
Linker bovenbeen 5.5 5.5 5.5 5.5 5.5
Rechter onderbeen 5 5 5 5 5
Linker onderbeen 5 5 5 5 5
Rechter voet 3.5 3.5 3.5 3.5 3.5
Linker voet 3.5 3.5 3.5 3.5 3.5
Beoordeling brandwond
• Diepte
• Dynamisch proces
• 1ste graad - alleen epidermis (niet meetellen)
• 2de graad - dermis (glanzend, blaren, pijn, CR+)
• 3de graad - subcutis ( blaren kapot, CR-, geen pijn, dof)
• 4de graad - vaak verkoling
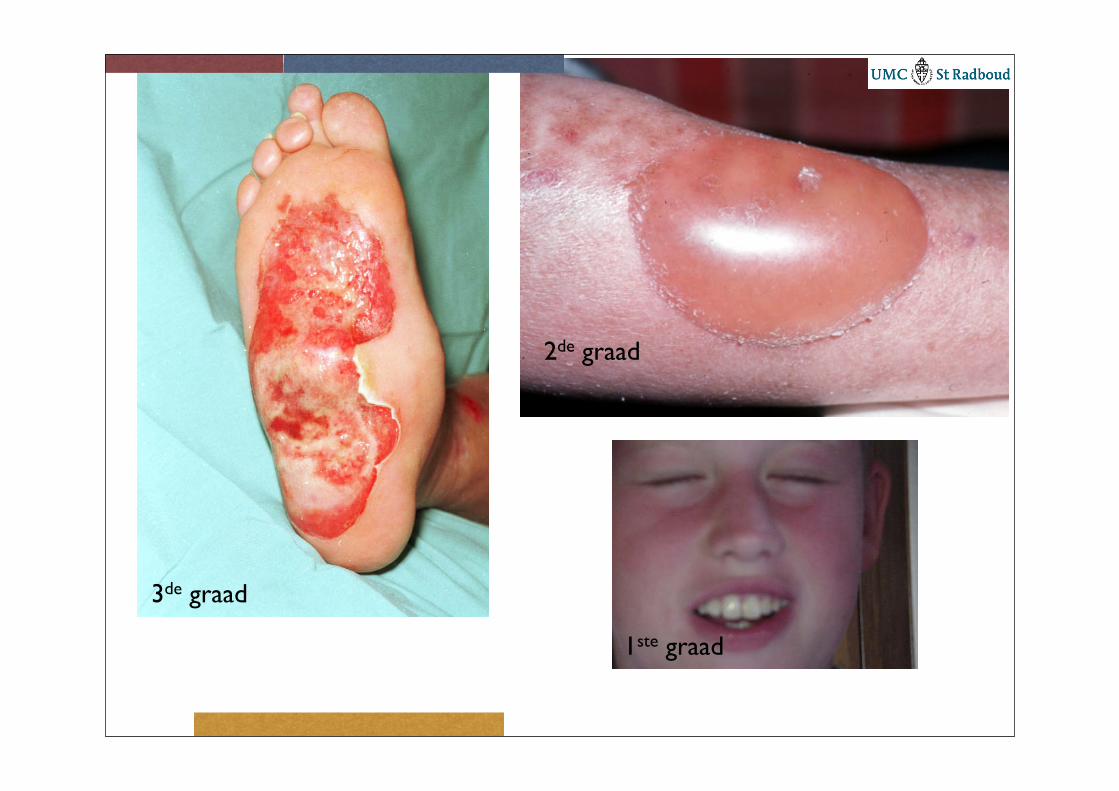
1ste graad
2de graad
3de graad
Inhalatie trauma
• Sterke toename morbiditeit en mortaliteit
• Indicatie overplaatsing centrum
• Bronchoscopie essentieel voor diagnose en vaststellen uitgebreidheid
• Hittetrauma mondkeelholte, chemische tracheobronchitis, CO/cyanide
Therapie
• Vroege intubatie
• Dagelijks bronchoscopie/lavage
Initiële resuscitatie
• Vocht toediening is essentieel maar gebruik geen rigide schema’s
• toename glottis oedeem
• ischemie bij circulaire verbrandingen
• abdominaal compartiment syndroom
• verdiepen van de brandwond
Initiële resuscitatie
• Bij ernstig inhalatietrauma neemt vochtbehoefte met 25% toe
• Vochtbehoefte neemt ook toe bij electriciteitsverbranding
• Oedeemvorming na 24 - 48 uur stop
• Herstel hierna colloïd osmotische druk
• Na 48 uur verdampingsverlies
• (25 + % TVLO) * lichaamsopp (m2) in ml/uur
Experimenteel
• Hoog gedoseerd vitamine C (< 2 uur na verbranding)
• Acetylcysteïne
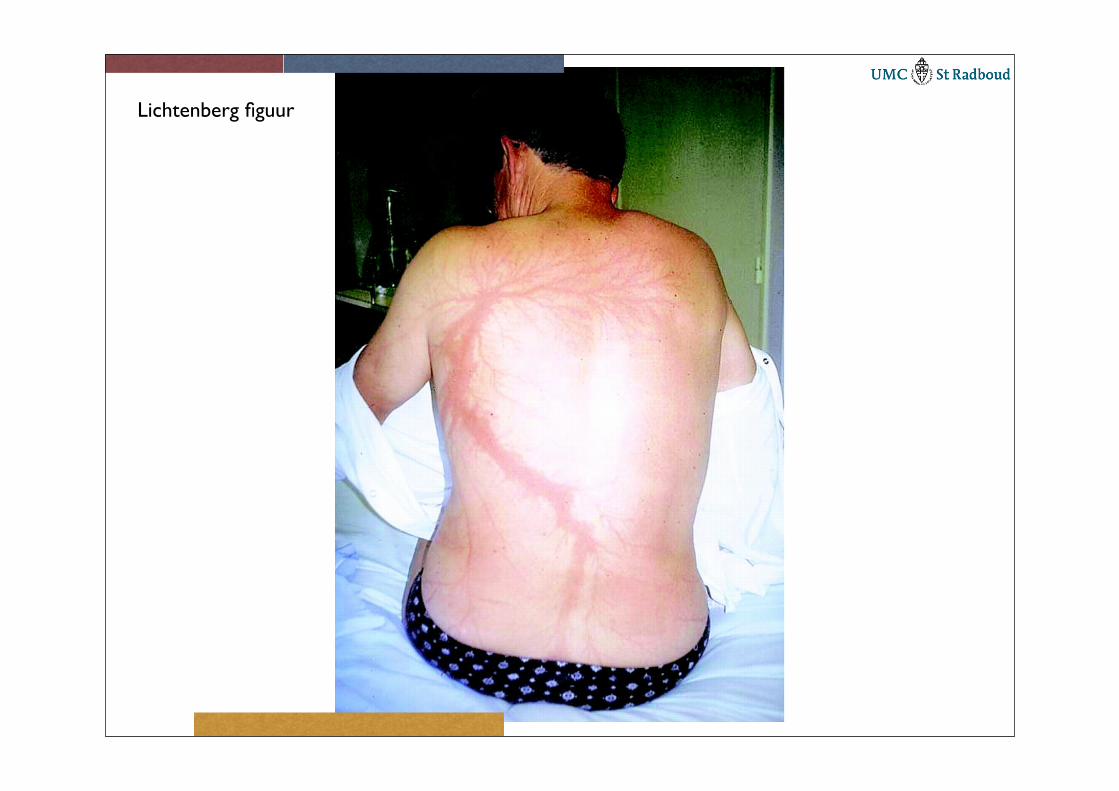
Lichtenberg figuur
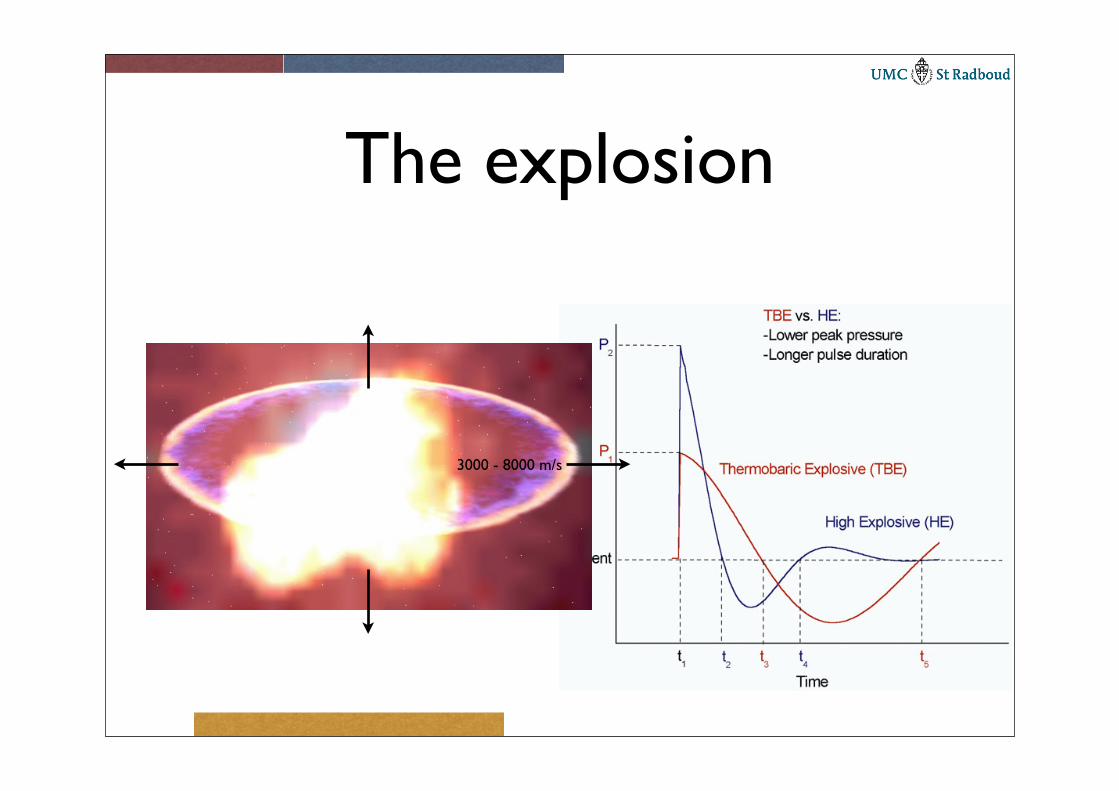
The explosion
3000 - 8000 m/s
Mechanisms
• Detonation resulting in shockwave
• Penetrating injury through bombfragments or material at the site of explosion
• Wind of the explosion - blunt trauma
• Burn wound (flash/clothes), inhalation, asphyxiation
85% of deadly injuries caused by shockwave
Explosion in closed space
• Higher mortality
• Higher ISS
• More damage through detonation
• More burn wounds
Detonation - blast wave
• Ear damage
➡ rupture tympanic membrane, dislocation and bleeding middle ear
• Intestinal damage
➡ contusion, intramural hematoma, perforation 0.1 - 1.2%, often delay between explosion and perforation, especially in colon
Detonation -blast wave
• Lungs
➡ 4.8 - 8.4%
➡ contusion, pneumothorax, lung bleeding, air embolus
➡ bilateral and diffuse with explosion in closed space
• CNS
➡ air embolus, diffuse axonal damage
Detonation - blast wave
• Trias of bradycardia/hypotension/hypoxia
➡ (vagal) pulmonary “defensive” reflex through C fibres in alveolar interstitium activated by acute pulmonary congestion (duration 1 - 2 hours)
Madrid• 243 victims
➡ 99 ruptured tympanic membranes
➡ 97 pulmonary trauma
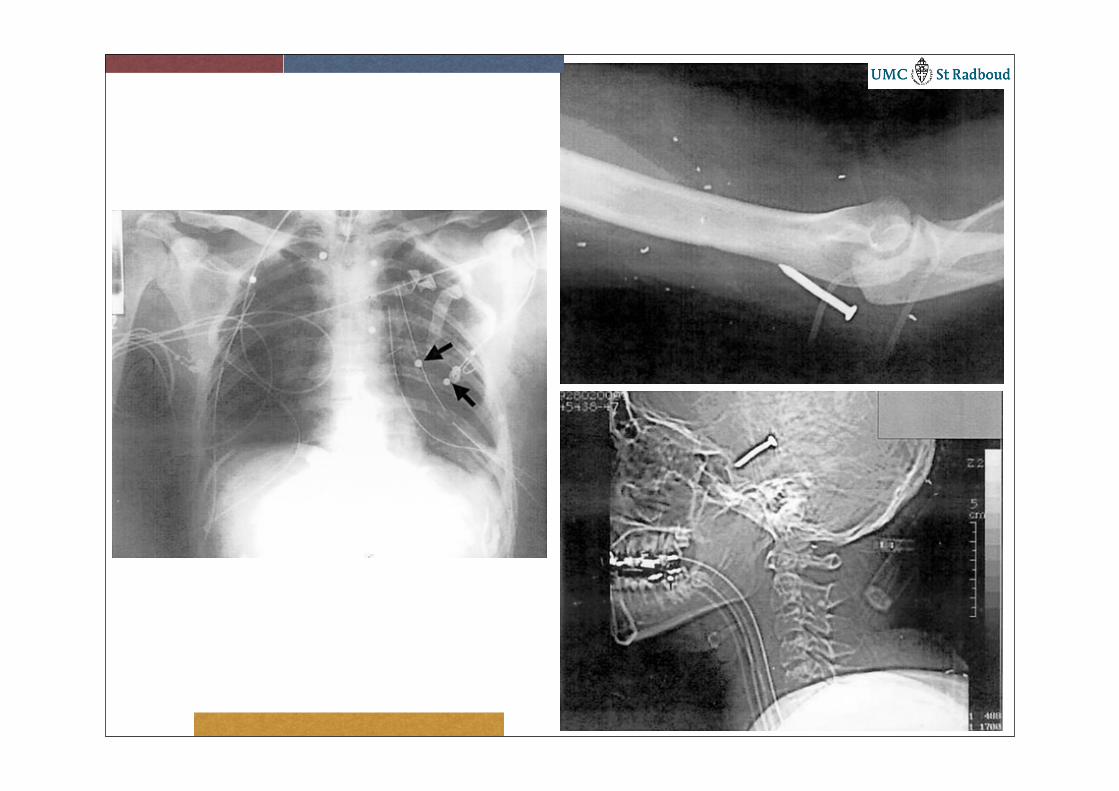
➡ 89 bomb fragments
➡ 44 fractures
➡ 45 burn wounds
➡ 41 eye damage (rupture eye, retinitis)
➡ 12 abdominal damage
➡ 5 traumatic amputations
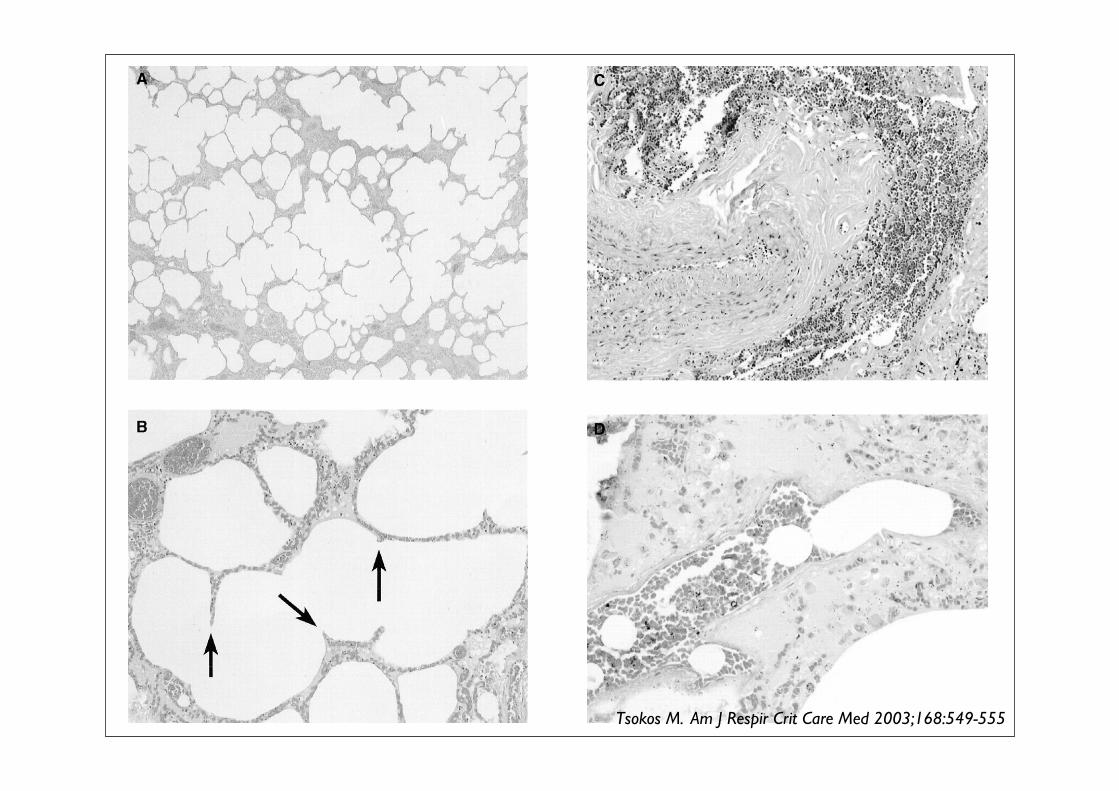
Tsokos M. Am J Respir Crit Care Med 2003;168:549-555
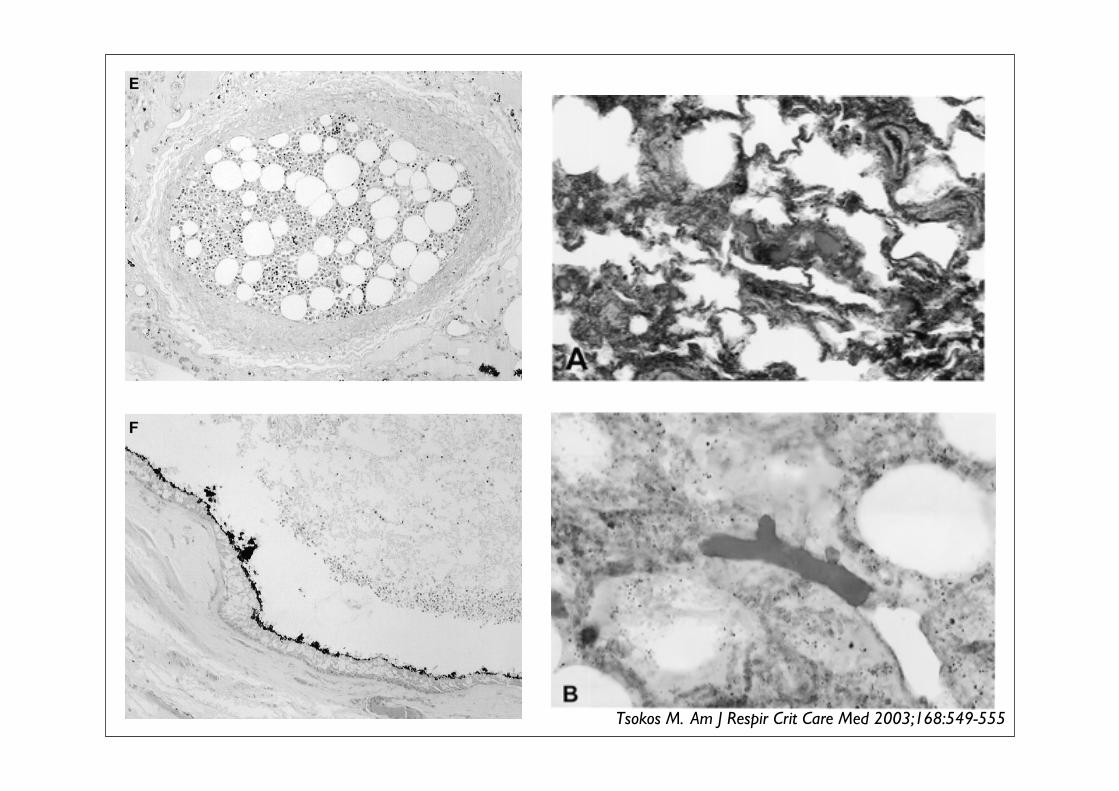
Tsokos M. Am J Respir Crit Care Med 2003;168:549-555
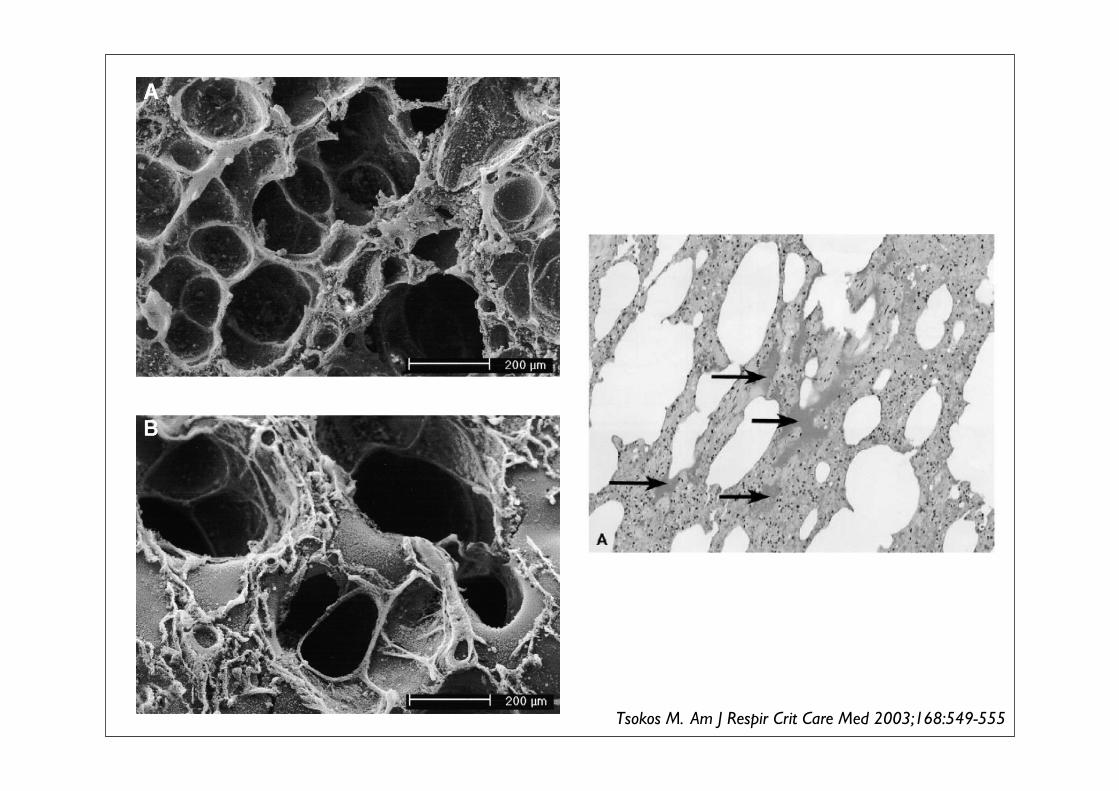
Tsokos M. Am J Respir Crit Care Med 2003;168:549-555
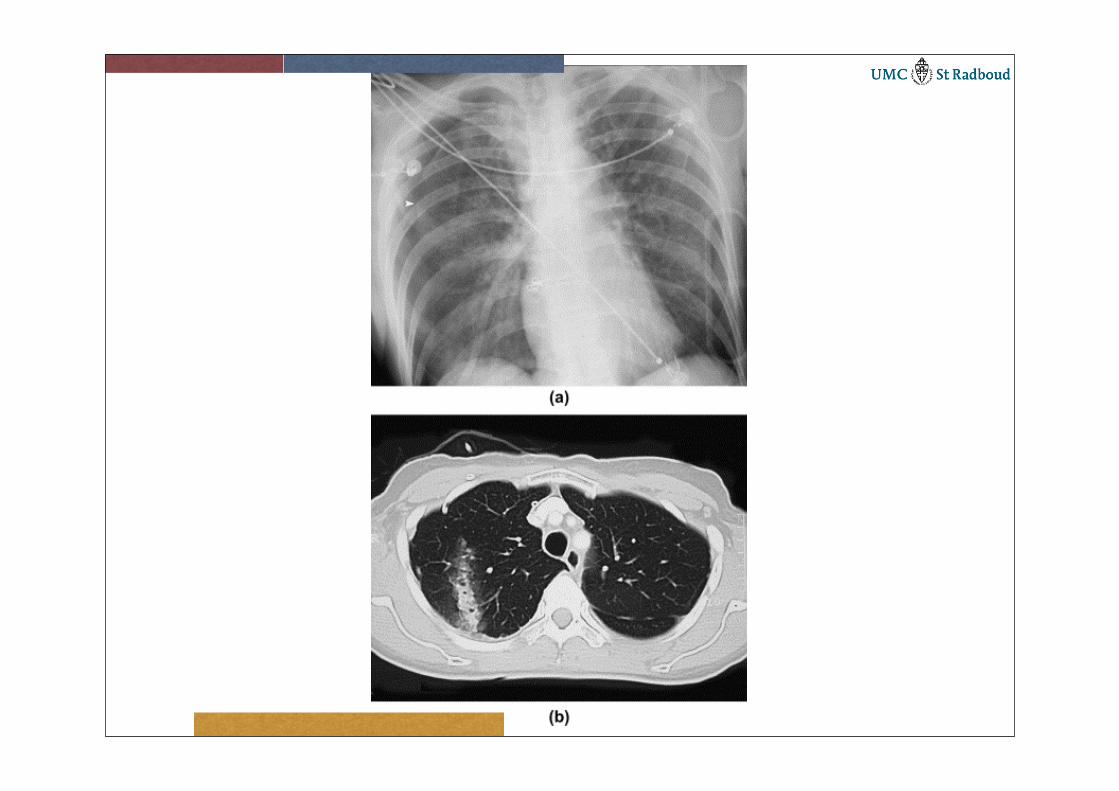
“Blast lung”
• Delay sometimes of 24 - 48 hours
• In closed space always < 6 hours
• Dyspnea, dry cough, hemorrhagic sputum and hemoptoe
• Lung protective ventilation ± preventive chest tube
Intensive Care
• Principes of ATLS + EGDT
• Damage control principles
• Standard intensive care treatment
• Intestinal perforation often after delay
• Unusual infections
➡ Candida, HIV, Hepatitis B
Inhalation trauma
• Especially in closed space
➡ Smoke
➡ Nitric oxides
➡ Phosgene
➡ Carbon monoxide
➡ Cyanide
➡ Heavy metals
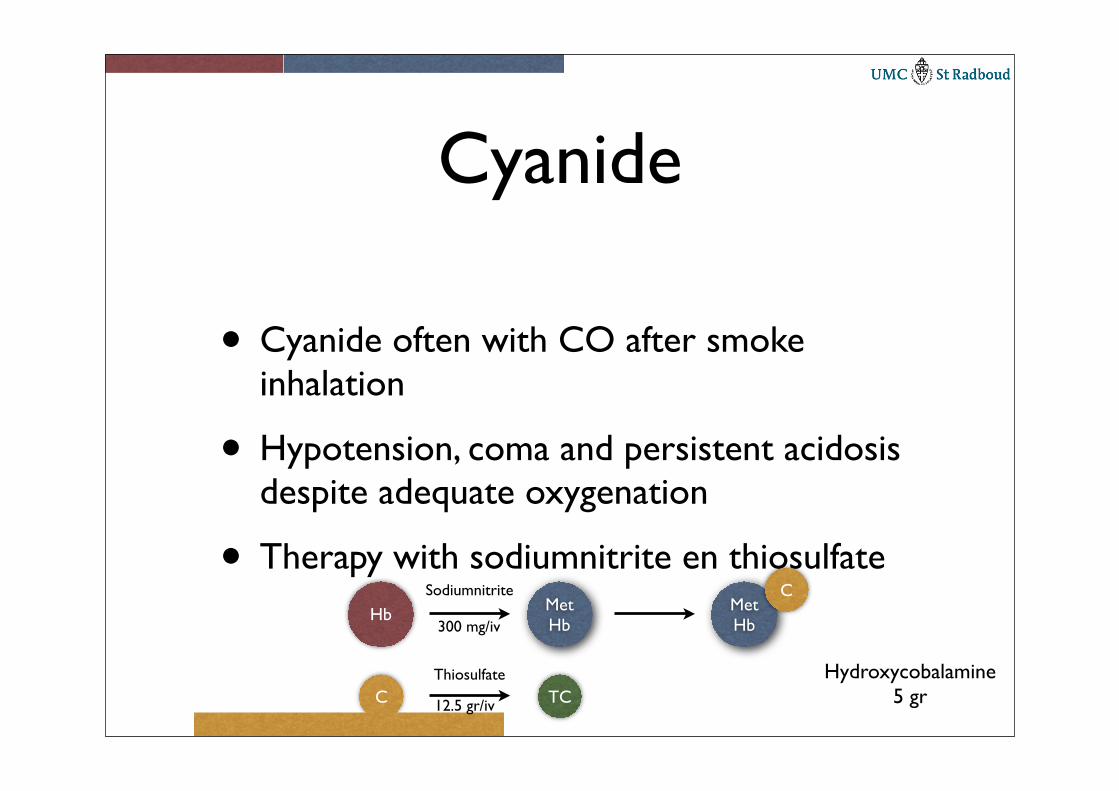
Cyanide
• Cyanide often with CO after smoke inhalation
• Hypotension, coma and persistent acidosis despite adequate oxygenation
• Therapy with sodiumnitrite en thiosulfateHb Met
HbMetHb
CSodiumnitrite
C TCThiosulfate Hydroxycobalamine
5 gr
300 mg/iv
12.5 gr/iv
To remember
• Intestinal damage often after delay
• Lung damage most frequent cause of death in initial survivors
• Air embolus relatively frequent
• Remember toxic gasses
• Wounds often contaminated