pad launch day - yoanna skrobik
TRANSCRIPT

The ICU challenge – translating the
evidence into everyday practice:
managing Pain, Agitation and
Delirium
Yoanna Skrobik MD FRCP(c) MSc.

Conflicts of interest
Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Vice-chair, SCCM Pain, Agitation, Delirium, Early Mobility
and Sleep guidelines
Member, SCCM family-centered care guideline writing committee
Investigator initiated research funding, Hospira
Academic chair, Université de Montréal

Academic chair
Astellas
Merck
Pfizer
Baxter
Hospira
Otsuka
Novartis
Lilly

Why would you evaluate pain,
agitation, delirium?
Painlessness
Reassurance
– Feeling safe Journal of Nursing Scholarship. 32(4):361-7, 2000
– Information, orientation, cognitive abnormalities American
Journal of Critical Care. 9(3):192-8, 2000 May

plan
Pain assessment and management
Sedation and level of consciousness alterations in the ICU
Delirium
Adding mobility and sleep
Why assessing pain, sedation and delirium matters
Why are we not all doing it

pain
pain
– Incidence of pain:
Adult M&S ICU patients consistently experience pain, at rest
and with routine ICU care (mobilization, suctioning).
Pain in adult cardiac surgery patients, especially women, (i.e.,
incisional pain due to coughing, respiratory care procedures,
and mobilization) remains prevalent and poorly treated .
Procedural pain is common in adult ICU patients .
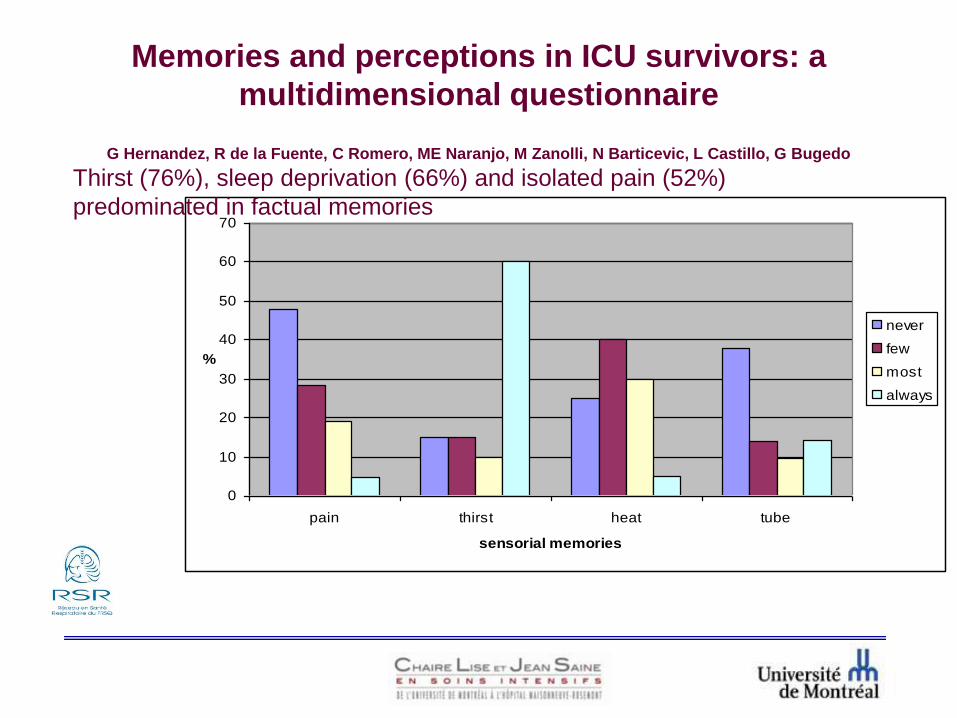
Memories and perceptions in ICU survivors: a
multidimensional questionnaire
G Hernandez, R de la Fuente, C Romero, ME Naranjo, M Zanolli, N Barticevic, L Castillo, G Bugedo
0
10
20
30
40
50
60
70
pain thirst heat tube
sensorial memories
%
never
few
most
always
Thirst (76%), sleep deprivation (66%) and isolated pain (52%)
predominated in factual memories

Pain assessment
Should be routine, right?

Evaluation of pain in my ICU
Even though assessment was done 90% of the time No severity scale used in 17% of patients
Evaluations were not done according to the pain reported by the patient when scales were used 20% of the time
Correlation between “gold standard” adjudicators and nurses was excellent
R= 1,000 (0,88 when using all evaluations)
Obstacles to the use of the NRS: Assumption that the patient has no pain
Nurses relying on their own evaluation of the patient’s pain

pain
Routine pain assessments in adult ICU patients are
associated with improved clinical outcomes.

Assessing Pain Improves
Outcomes
Payen JF, et al. Anesthesiology. 2009;111:1308-1316.
Outcome
Day 2 Pain
Assessment? Unadj. OR P-valueAdjusted
ORP-value
No Yes
ICU Mortality 22% 19% 0.91 0.69 1.06 0.71
ICU LOS 18 d 13 d 1.70 < 0.01 1.43 0.04
MV duration 11 d 8 d 1.87 < 0.01 1.40 0.05
Vent-acquired
pneumonia 24% 16% 0.61 < 0.01 0.75 0.21
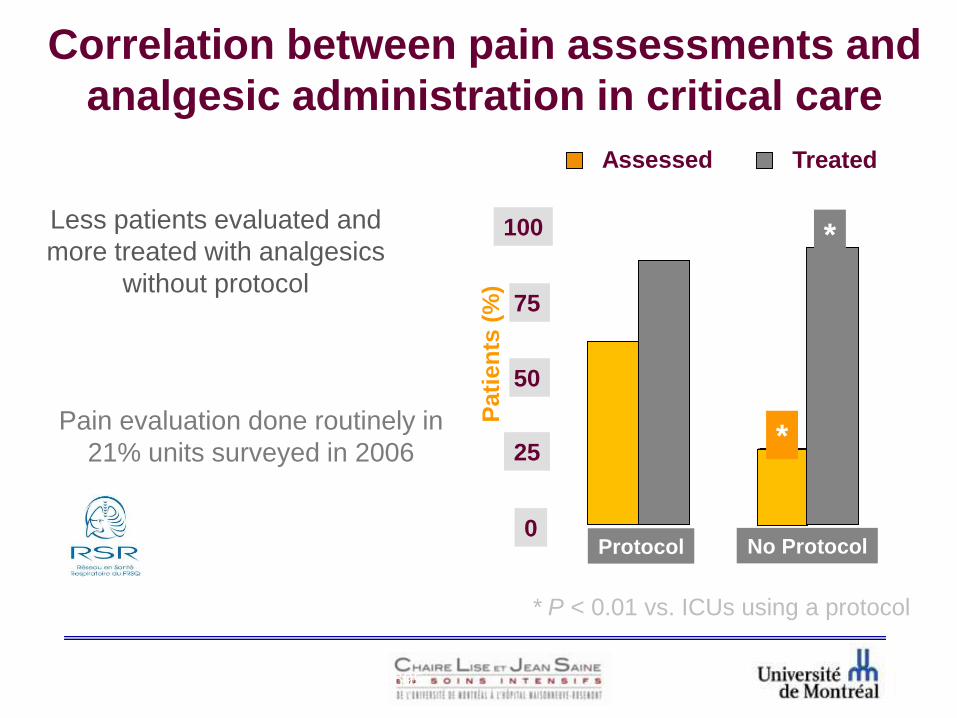
Correlation between pain assessments and
analgesic administration in critical care
Less patients evaluated and
more treated with analgesics
without protocol
Pain evaluation done routinely in
21% units surveyed in 2006
0
25
50
100
75
Pati
en
ts (
%)
Protocol No Protocol
*
*
Assessed Treated
1. Payen JF, et al. Anesthesiol. 2007;106:687-695.
2. Martin J, et al. Crit Care. 2007;11:R124.
* P < 0.01 vs. ICUs using a protocol
Measuring pain
Self-reporting of pain remains the gold standard

Patient-directed
pain control.

Patient assessment

And this is what it looks like
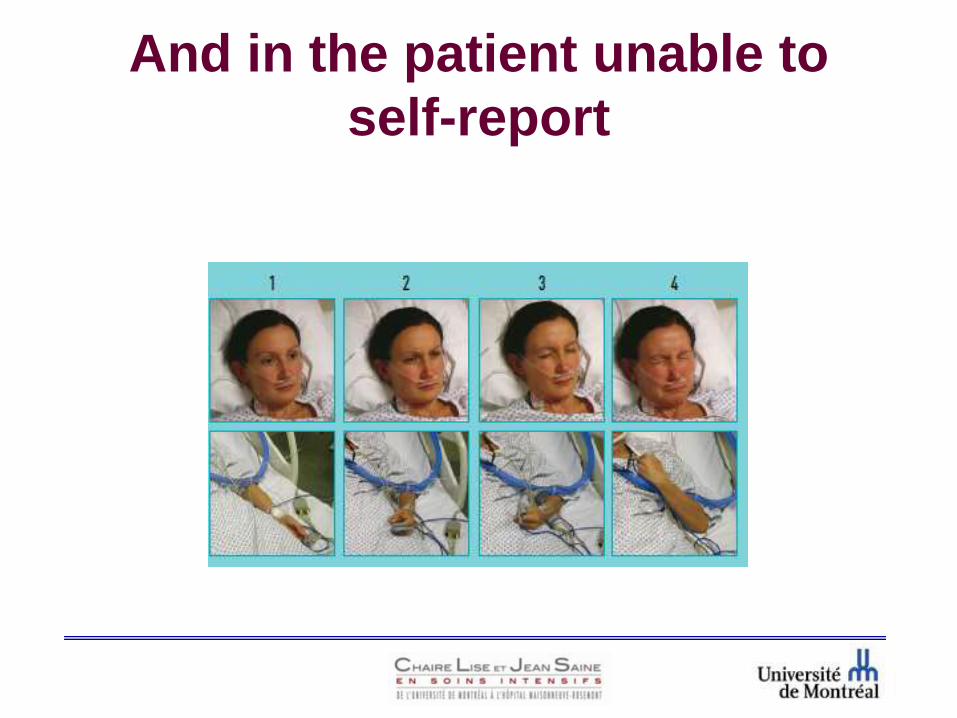
And in the patient unable to
self-report

Keep in mind
Routine pain assessments in adult ICU patients are
associated with improved clinical outcomes.
Self-reporting of pain remains the gold standard.
For medical, postoperative or trauma adult ICU patients
unable to self-report, the BPS and CCPOT (French/ English)
pain scales are considered to be the most valid and reliable.
vital signs (or observational pain scales that include vital
signs) are unreliable in pain assessment in adult ICU patients.

Pain assessment value
Compliance and documentation of pain assessments
Impact of pain assessment on analgesic and other medications
Impact of pain assessment on level of pain
Impact of pain assessment on duration of mechanical ventilation
Impact of pain assessment on occurrence of adverse events
and complications
Impact of pain assessment on patient satisfaction
Impact of pain assessment on ICU length of stay (LOS)
Impact of pain assessment on mortality

sedation
sedation
No text
Monitoring sedation
The RASS and SAS scales are valid and reliable for
measuring quality and depth of sedation in adult ICU patients .

Sedation-Agitation Scale (SAS)
Riker RR, et al. Crit Care Med.1999;27:1325-1329.
Brandl K, et al. Pharmacotherapy.2001;21:431-436.
Score State Behaviors
7Dangerous
Agitation
Pulling at ET tube, climbing over bedrail, striking at staff,
thrashing side-to-side
6 Very AgitatedDoes not calm despite frequent verbal reminding,
requires physical restraints
5 AgitatedAnxious or mildly agitated, attempting to sit up, calms
down to verbal instructions
4Calm and
CooperativeCalm, awakens easily, follows commands
3 SedatedDifficult to arouse, awakens to verbal stimuli or gentle
shaking but drifts off
2 Very SedatedArouses to physical stimuli but does not communicate or
follow commands
1 UnarousableMinimal or no response to noxious stimuli, does not
communicate or follow commands

Richmond Agitation
Sedation Scale (RASS)Score State
+ 4 Combative
+ 3 Very agitated
+ 2 Agitated
+ 1 Restless
0 Alert and calm
-1 Drowsy eye contact > 10 sec
-2 Light sedation eye contact < 10 sec
-3 Moderate sedation no eye contact
-4 Deep sedation physical stimulation
-5 Unarousable no response even with physical
Verbal Stimulus
Physical Stimulus

sedation
– Depth of sedation vs. clinical outcomes:
Maintaining lighter levels of sedation in adult ICU patients is
associated improved clinical outcomes ( duration of
mechanical ventilation and length of stay).
Maintaining lighter sedation levels increases physiologic
stress response, but not incidence of myocardial ischemia .
The relationship between depth of sedation and psychological
stress in these patients is unclear .
sedative medications titrated to maintain light (vs. deep) levels
of sedation in adult ICU patients are associated with better
outcomes .

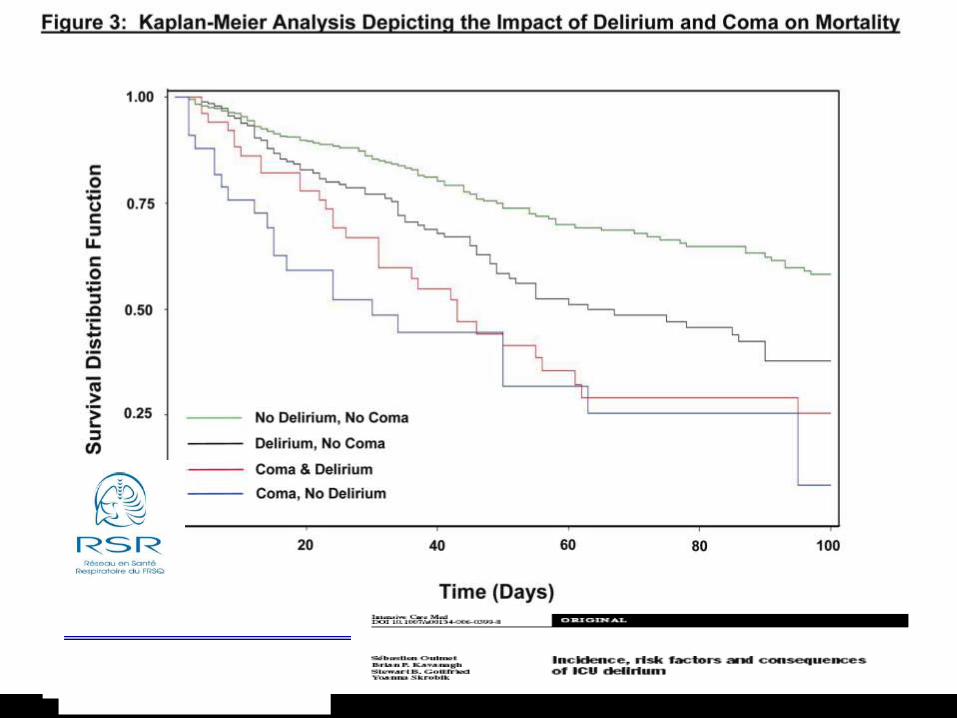
consciousness
Alteration of consciousness and
outcome
Coma is bad for you


In my ICU the baseline RASS is -0.4
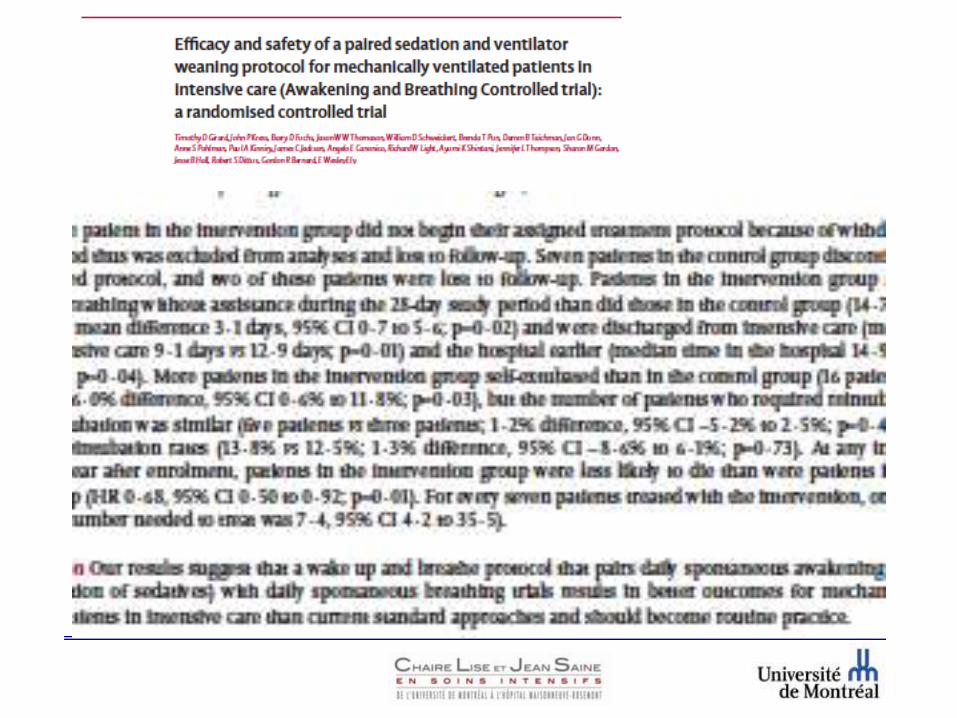
‘wake up and breathe’
‘Why is it that when an ICU
caregiver digs himself into a
hole he talks about the light
at the end of the tunnel?’

Who benefits the most?
adjustment vs. interruption

Outcomes related to sedation
sedation strategies using non-benzodiazepine sedatives have
better outcomes than benzodiazepine infusions in
mechanically ventilated adult ICU patients.
analgesia should be evaluated prior to sedation in adult ICU
patients who are mechanically ventilated .

delirium
Van der Mast. PhD Thesis, Delirium After Cardiac Surgery, Erasmus University, Rotterdam,
1994
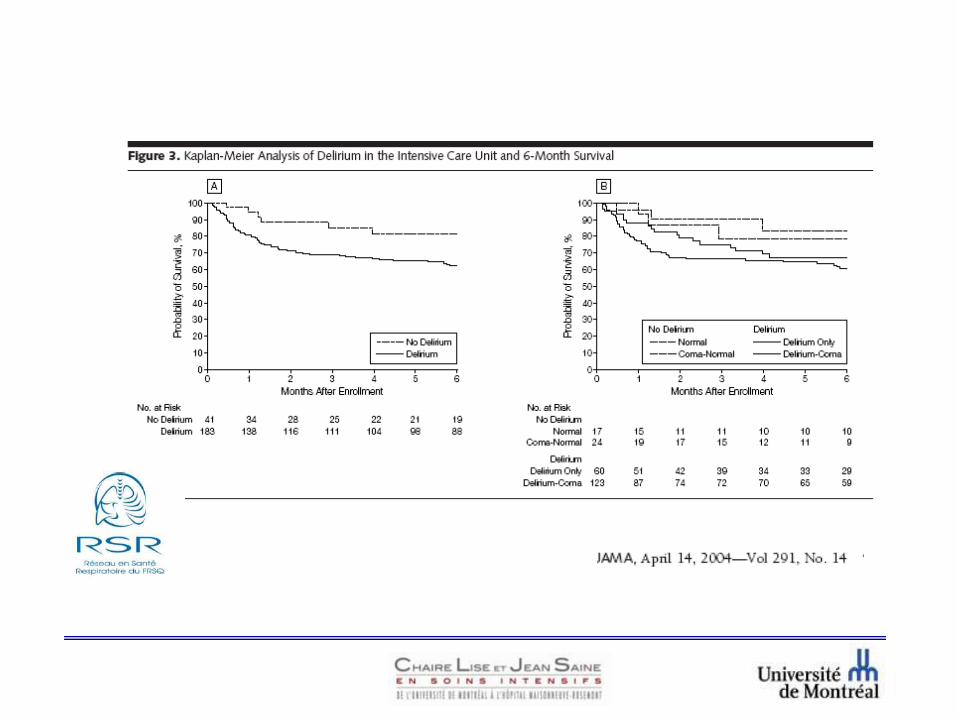
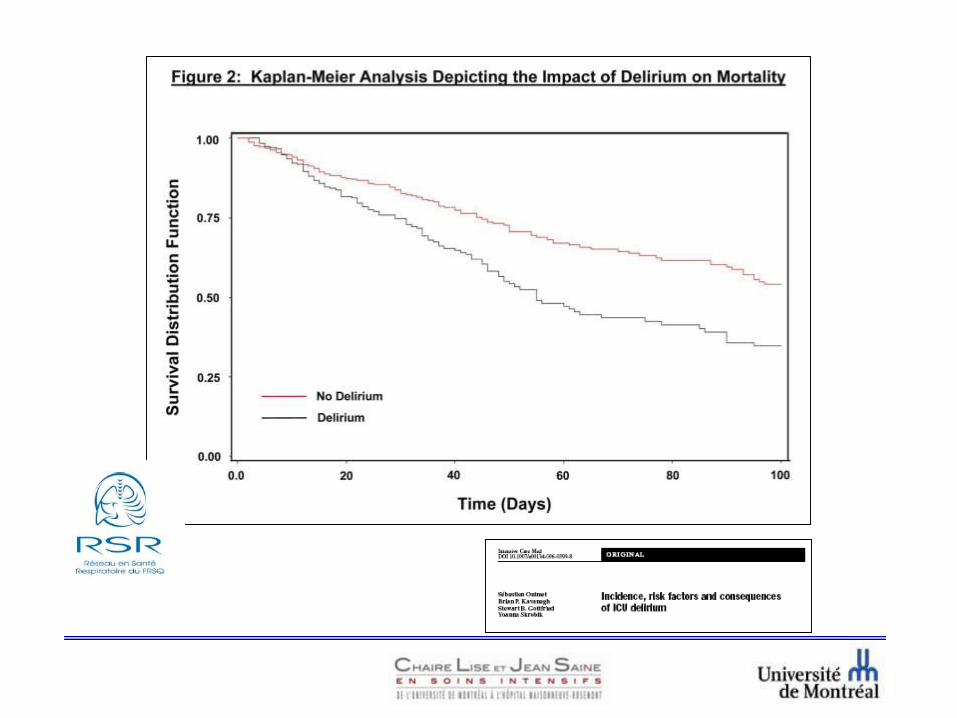
Delirium and outcomes
Delirium is strongly associated with increased mortality and
LOS in adult ICU patients.

delirium and distress
Breitbart W et al. Psychosomatics 2002;43:183
CAM-ICU
(Confusion Assessment Method-ICU)
Delirium scales
ICDSC
(Intensive Care Delirium Screening
Checklist)
http://www.icudelirium.co.uk/ www.icudelirium.org

Delirium nomenclature
Delirium and its consequences

Delirium prevention
early mobilization of adult ICU patients reduces the incidence
and duration of delirium.
Protocol to address patient views
on what is important in the ICU
Painlessness
Reassurance
– Feeling safe Journal of Nursing Scholarship. 32(4):361-7, 2000
– Information, orientation, cognitive abnormalities American
Journal of Critical Care. 9(3):192-8, 2000 May
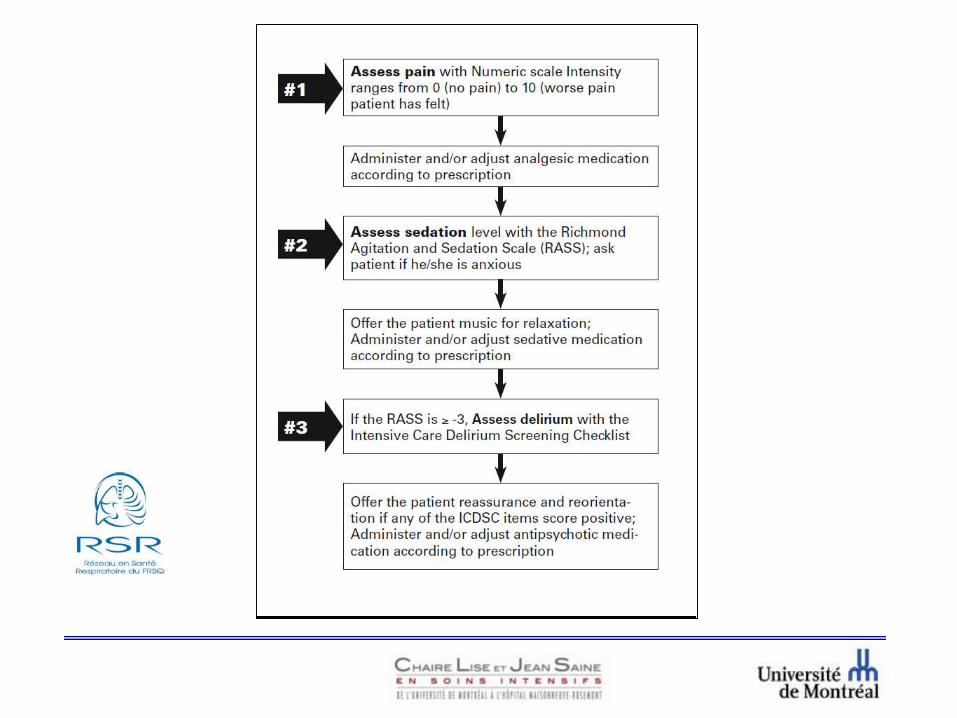

Analgesia Sedation Delirium Protocol
ANALGESIA•Subjective Pain Scale
•Short acting narcotics
SEDATION•Subjective Sedation Scale (ex RASS)
•Avoidance of oversedation and caution with benzodiazepines
DELIRUM•Subjective Delirium Scale (ICDSC or CAM-ICU)
“Agitation”


Before After
Going home 45.2% 52.2% P=0.024
…Patient-driven analgesia, sedation and
delirium management in 1200 patients
Delirium symptoms
Specifically, level of consciousness
wakefulness
Does it influence delirium assessment?

CAM-ICU
(Confusion Assessment Method-ICU)
Delirium scales
ICDSC
(Intensive Care Delirium Screening
Checklist)
http://www.icudelirium.co.uk/ www.icudelirium.org

Assessment of Delirium Relative to Daily
Sedative Interruption
JT Poston MD, MW Sjoding MD, AS Pohlman RN MSN, BK Gehlbach MD, JB Hall MD, JP
Kress MD
Assessment of Delirium Relative to Daily
Sedative Interruption
JT Poston MD, MW Sjoding MD, AS Pohlman RN MSN, BK Gehlbach MD, JB Hall MD, JP
Kress MD
48%higher delirium identification during sedation administration
when compared to assessments made in the same patients
after sedation was lightened to the point of wakefulness.
This difference persisted for analysis of MV days, ICU days, and
total hospital days
wakefulness
Delirium assessment is sensitive to the timing of evaluation
relative to sedative/analgesic infusion and interruption
This robust effect can significantly impact assessed days of
delirium well beyond the administration of sedatives/analgesics
Implications
A standardized assessment accounting for sedatives/analgesics
and daily interruption should be part of future investigations
Delirium due solely to sedative/analgesic infusion may portend a
different prognosis than delirium that persists in its absence

Awake patients mean
Pain can be assessed
Sedation is adjusted
Delirium is minimized
Mobility can be implemented
Sleep can be optimized

How can optimal patient care be
provided?
a multidisciplinary ICU team approach, that includes
provider education, preprinted and/or computerized
sedation protocols and order forms, and a quality rounds
checklist, can be used to facilitate analgesia, sedation and
delirium management in adult ICUs...
But we all know…
…. it takes an average of 17 years for new knowledge to
have an impact on bedside standards of practice
change

Canadian collaborative


Measuring and implemening
change
Champions
Realistic plan and follow through
Objective measures
alternatives
Web-based teaching
Web-based benchmark comparisons
Engaging staff
Engaging patients and families

Engaging staff

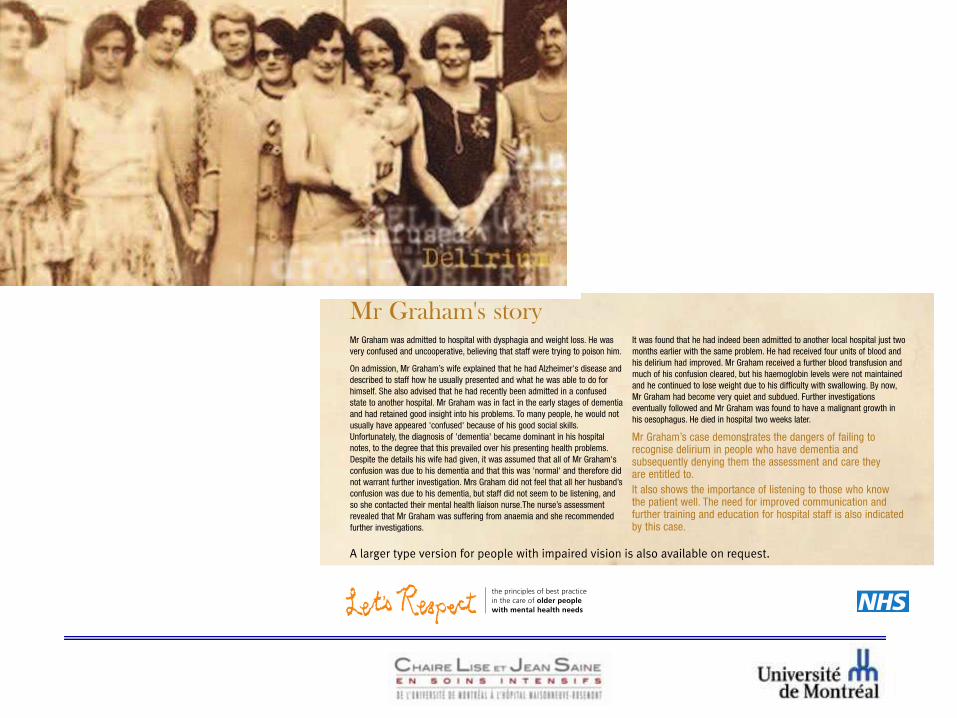
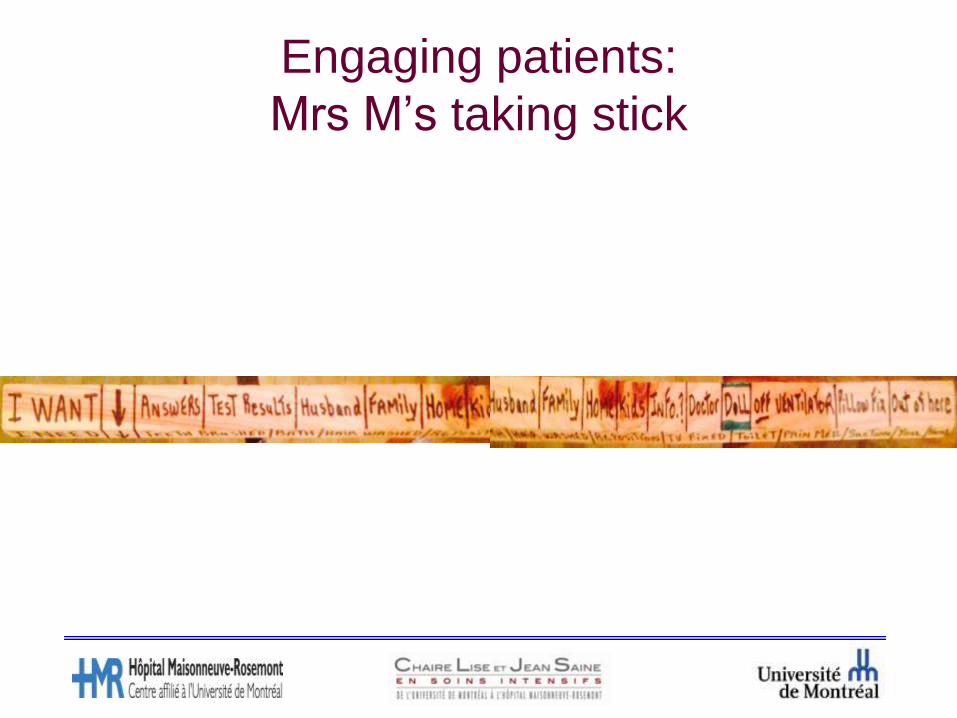
Engaging patients:
Mrs M’s taking stick
recap
Pain assessment and management
Sedation and level of consciousness alterations in the ICU
Delirium
Adding mobility and sleep
Why combining pain, sedation and delirium matters
Why are we not all doing it

Making patient care better
Thank you