pain as a long term condition dr cathy price. long term conditions; matching care to needs kaiser...
Post on 22-Dec-2015
213 views
TRANSCRIPT

Pain as a long term condition
Dr Cathy Price


Long term conditions; matching care to needs
Kaiser Permanente NW Pain care model 2000
Von Korff- Stepped care BMJ 2002
DH LTC 2003
Intensive
or Case Management
Assisted Care or Care Management
Usual Care with Support
Level 170-80% of a CCM pop
Level 2High risk members
Level 3Highly complex members
Intensive
or Case Management
Assisted Care or Care Management
Usual Care with Support
Level 170-80% of a CCM pop
Level 2High risk members
Level 3Highly complex members
Increasing complexity of biopsychosocial factors

Organisation of long term care
Care planning
Care planning
Unscheduled care visits
Unscheduled care visits

What do patients want?
THE KINGS FUND Collective Report from major patient organisations October 2010

6
HCC National Patient Survey
Lack of Patient Involvement and
Empowerment in Health Care - diabetes
Steve Laitner DH 2010

Pain…there’s a lot of it about….Moore, McQuay Bandolier
Grampians:Grampians:• average annual incidence 8.3% average annual incidence 8.3% • average annual recovery rate 5.4%average annual recovery rate 5.4%
• Incidence pain with high level of need: 6.3Incidence pain with high level of need: 6.3% % Elliott: Pain. 2002 Sep;99(1-2):299-307
1:5 Australians have chronic pain1:5 Australians have chronic pain80% are missing out on help they could have $10, 847 per 80% are missing out on help they could have $10, 847 per
person …Australian Pain Strategy person …Australian Pain Strategy

Self management support
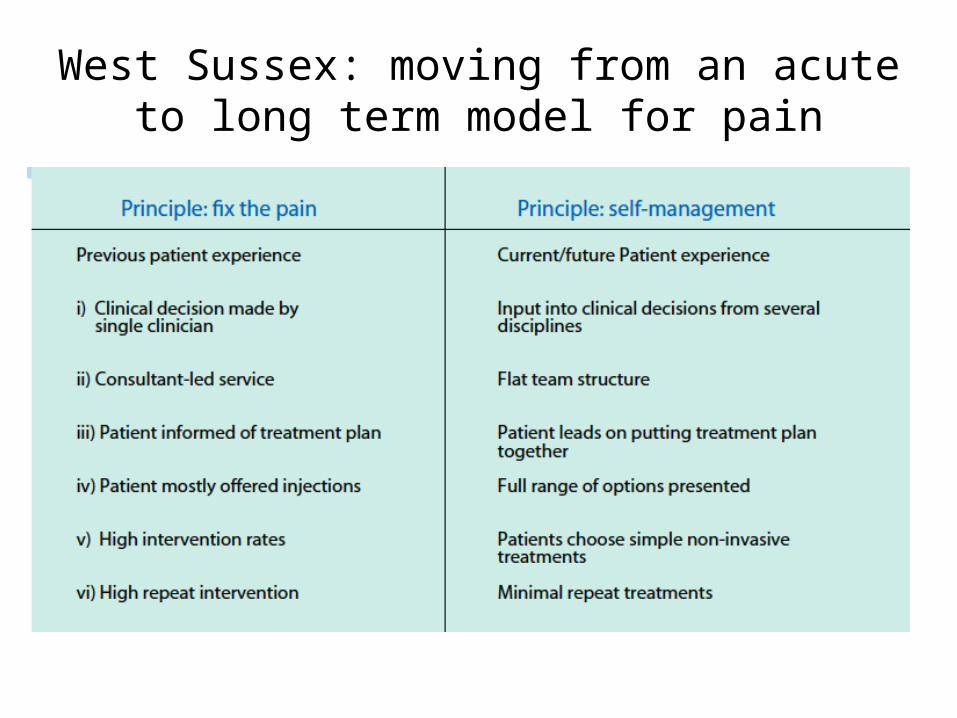
West Sussex: moving from an acute to long term model for pain

Commentary
“We still see the same number of patients but the service now has one procedure session per month instead of 5 sessions per week…patients frequently choose a less interventional option which seems to suffice…with low waiting times and high patient satisfaction”
Simon Dolin: Pain Physician West Sussex Pain Team

Activity 2002-6 Secondary care
0200400600800
100012001400
2002-3
2003-4
2004-5
2005-6
Decreased medical follow-ups Increased emphasis on
coping and self management skills
Decreased short term solutions
Waiting times:steady at 6 weeks
8% do not opt in from assessment
Budget decreased
Southampton

Cole and Hill 2010 Moore 2009

Commentary“Our self management programme is delivered by health trainers. We have found that GP visits are reduced by 50% and 90% said they were
better equipped to manage their pain.”
“Excellent tools to assist in controlling pain and can be referred to at any time”
• Frances Cole GPwSI Pain Management Bradford• Pete Moore Patient Self management Trainer author Pain Toolkit,
Essex

System Design – Southampton Model

Primary Care???
• 4.6 m appointments a year - £69m• 67 m analgesic prescriptions - £584m

GP Survey SW Hampshire 2010 (150/302 GP’s replied) would like education on:
Patient education Prescribing 55% - updated prescribing
guidelines would be useful. Psychological Aspects
46% would like more information on the evidence base.
Use of injections 59% would like more
information on the evidence base.
Complementary Therapies 73% recommend them. 58% wanted information on the
evidence base.
Do you find it easy to educate patients about persistent pain?
no, 26.8%
sometimes, 48.37%
mostly, 22.22%
yes , 2.61%
“How can I know that which I am ignorant of ??”

Primary Care support
•Educational programme for GP’s- pain, aetiology, psychosocial risk factors•GP trainees training session•Pain week for medical students Y2•Prescribing guidelines- support of DPC – pharmacy driven•Pharmacy teaching of community pharmacists•Clear pathways of care
Intensive
or Case Management
Assisted Care or Care
Management
Usual Care with Support
Level 170-80% of a CCM
pop
Level 2High risk members
Level 3Highly complex members
Intensive
or Case Management
Assisted Care or Care
Management
Usual Care with Support
Level 170-80% of a CCM
pop
Level 2High risk members
Level 3Highly complex members

Views…education programme• “I think people have been very positive about this and
they want more information and more involvement”. .. GP focus group member
• “Learning to make a conscious effort to think about how to behave when talking to patients whose injury isn’t visible”.. 2nd year med student
• “I Find access to pain clinic very supportive and helpful in offering a more holistic and multidisciplinary approach”. GP survey respondent

Pain Management – community interventions
Complex individual case management-
Self management programmes-
varying levels of intensity
Usual Care with Support- primary care doctor medicines, explanations of pain within a
biopsychosocial framework, musculoskeletal practitioners, community pharmacists
Level 170-80% of a CCM pop
Level 2High risk members
Level 3Highly complex members
Short secondary prevention groups, physiotherapy lead
Some brief individual care
Operational policy for the community screening teams
Vocational Rehabilitation workers
Interdisciplinary CBT-based pain management Programmes
Council run leisure centre schemes
Patient support groups

Impact of multidisciplinary pain management in Southampton
“Those who attended the group CBT programme found a 64% reduction in physiotherapy visits, 32% reduction in GP visits, 10% reduction in medication use”
Eleanor Hulse 4th year medical student project on 22 1 yr post CBT programme graduates 2006

After multidisciplinary care: 70% have accepted pain 30% are “resigned to it”
“You turn chaos into Order”
injections tended to confuse and lead to further help seeking
Jo Toward, Southampton Physiotherapist’s masters research 2009

Taking it further
• VA USA: 5 primary care clinics 402 patients– Assessment by pain team in surgery– Education and activation through 4 session intervention in specialist unit– Recommended personalised care plan– Clinician training
• Average case load = 180 patients• Moderate improvement in pain/disability/depression
Collaborative Care for Chronic Pain in Primary Care: a cluster randomised trial Dobscha 2009

Where can we do better?
• Prevention, diagnosis and early intervention – better risk profiling (can anyone help?)
• Reducing Emergency visits through more proactive care planning, better identification of those at risk
• Working together with social care , 3rd sector

Common Barriers• Professional:
– Lack of knowledge of systems approach– Lack of knowledge of persistent pain
• System:– Lack of primary care incentives– Financial - money does not flow according to patient
need• Information:
– Lack of knowledge of health care resource use and factors governing this
– Lack of use of common Public Health measures

System barriers to adopting LTC model –care pathways

Overcoming barriers
• Finances– Money doesn’t follow patients– Year of care: diabetes
• Patients choose what care they wish• Greater engagement in treatment• Greater self care
www.diabetes.org.uk/professionals/service -improvement/Year-of-Care

Information Barriers - solutions
• Health Survey for England 2011 – 2012– Euroqol– Specific pain questions on health resource use
• Develop WHO tools– DALY’s– Global estimates of risk
• Benchmark– National Pain Audit Dr Foster/BPS– Essence of Care
Conclusions
Long term conditions management principles applied to pain results in low waiting times, improved patients satisfaction and lower interventional rates for patients.
Good news for patients!!!

