pain management for women in labour: an overview of
TRANSCRIPT

Pain management for women in labour: an overview of
systematic reviews (Review)
Jones L, Othman M, Dowswell T, Alfirevic Z, Gates S, Newburn M, Jordan S, Lavender T,
Neilson JP
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2012, Issue 3
http://www.thecochranelibrary.com
Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
27DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
33AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
33ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
34REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
41ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
158APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
160WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
160CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
160DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
160SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
160NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
161INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iPain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Overview of Reviews]
Pain management for women in labour: an overview ofsystematic reviews
Leanne Jones1, Mohammad Othman1, Therese Dowswell1, Zarko Alfirevic2, Simon Gates3, Mary Newburn4, Susan Jordan5, Tina
Lavender6, James P Neilson2
1Cochrane Pregnancy and Childbirth Group, Department of Women’s and Children’s Health, The University of Liverpool, Liverpool,
UK. 2Department of Women’s and Children’s Health, The University of Liverpool, Liverpool, UK. 3Warwick Clinical Trials Unit,
Division of Health Sciences, Warwick Medical School, The University of Warwick, Coventry, UK. 4National Childbirth Trust, Acton,
London, UK. 5Department of Nursing, Swansea University, Swansea, UK. 6School of Nursing, Midwifery and Social Work, The
University of Manchester, Manchester, UK
Contact address: James P Neilson, Department of Women’s and Children’s Health, The University of Liverpool, First Floor, Liverpool
Women’s NHS Foundation Trust, Crown Street, Liverpool, L8 7SS, UK. [email protected].
Editorial group: Cochrane Pregnancy and Childbirth Group.
Publication status and date: Edited (no change to conclusions), published in Issue 6, 2013.
Review content assessed as up-to-date: 31 October 2011.
Citation: Jones L, Othman M, Dowswell T, Alfirevic Z, Gates S, Newburn M, Jordan S, Lavender T, Neilson JP. Pain management
for women in labour: an overview of systematic reviews. Cochrane Database of Systematic Reviews 2012, Issue 3. Art. No.: CD009234.
DOI: 10.1002/14651858.CD009234.pub2.
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
The pain that women experience during labour is affected by multiple physiological and psychosocial factors and its intensity can vary
greatly. Most women in labour require pain relief. Pain management strategies include non-pharmacological interventions (that aim
to help women cope with pain in labour) and pharmacological interventions (that aim to relieve the pain of labour).
Objectives
To summarise the evidence from Cochrane systematic reviews on the efficacy and safety of non-pharmacological and pharmacological
interventions to manage pain in labour. We considered findings from non-Cochrane systematic reviews if there was no relevant Cochrane
review.
Methods
We searched the Cochrane Database of Systematic Reviews (The Cochrane Library 2011, Issue 5), The Cochrane Database of Abstracts
of Reviews of Effects (The Cochrane Library 2011, Issue 2 of 4), MEDLINE (1966 to 31 May 2011) and EMBASE (1974 to 31 May
2011) to identify all relevant systematic reviews of randomised controlled trials of pain management in labour. Each of the contributing
Cochrane reviews (six new, nine updated) followed a generic protocol with 13 common primary efficacy and safety outcomes. Each
Cochrane review included comparisons with placebo, standard care or with a different intervention according to a predefined hierarchy
of interventions. Two review authors extracted data and assessed methodological quality, and data were checked by a third author. This
overview is a narrative summary of the results obtained from individual reviews.
Main results
We identified 15 Cochrane reviews (255 included trials) and three non-Cochrane reviews (55 included trials) for inclusion within
this overview. For all interventions, with available data, results are presented as comparisons of: 1. Intervention versus placebo or
1Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

standard care; 2. Different forms of the same intervention (e.g. one opioid versus another opioid); 3. One type of intervention
versus a different type of intervention (e.g. TENS versus opioid). Not all reviews included results for all comparisons. Most reviews
compared the intervention with placebo or standard care, but with the exception of opioids and epidural analgesia, there were few direct
comparisons between different forms of the same intervention, and even fewer comparisons between different interventions. Based on
these three comparisons, we have categorised interventions into: “ What works” ,“What may work”, and “Insufficient evidence to make
a judgement”.
WHAT WORKS
Evidence suggests that epidural, combined spinal epidural (CSE) and inhaled analgesia effectively manage pain in labour, but may
give rise to adverse effects. Epidural, and inhaled analgesia effectively relieve pain when compared with placebo or a different type of
intervention (epidural versus opioids). Combined-spinal epidurals relieve pain more quickly than traditional or low dose epidurals.
Women receiving inhaled analgesia were more likely to experience vomiting, nausea and dizziness.
When compared with placebo or opioids, women receiving epidural analgesia had more instrumental vaginal births and caesarean
sections for fetal distress, although there was no difference in the rates of caesarean section overall. Women receiving epidural analgesia
were more likely to experience hypotension, motor blockade, fever or urinary retention. Less urinary retention was observed in women
receiving CSE than in women receiving traditional epidurals. More women receiving CSE than low-dose epidural experienced pruritus.
WHAT MAY WORK
There is some evidence to suggest that immersion in water, relaxation, acupuncture, massage and local anaesthetic nerve blocks or
non-opioid drugs may improve management of labour pain, with few adverse effects. Evidence was mainly limited to single trials.
These interventions relieved pain and improved satisfaction with pain relief (immersion, relaxation, acupuncture, local anaesthetic
nerve blocks, non-opioids) and childbirth experience (immersion, relaxation, non-opioids) when compared with placebo or standard
care. Relaxation was associated with fewer assisted vaginal births and acupuncture was associated with fewer assisted vaginal births and
caesarean sections.
INSUFFICIENT EVIDENCE
There is insufficient evidence to make judgements on whether or not hypnosis, biofeedback, sterile water injection, aromatherapy,
TENS, or parenteral opioids are more effective than placebo or other interventions for pain management in labour. In comparison
with other opioids more women receiving pethidine experienced adverse effects including drowsiness and nausea.
Authors’ conclusions
Most methods of non-pharmacological pain management are non-invasive and appear to be safe for mother and baby, however, their
efficacy is unclear, due to limited high quality evidence. In many reviews, only one or two trials provided outcome data for analysis and
the overall methodological quality of the trials was low. High quality trials are needed.
There is more evidence to support the efficacy of pharmacological methods, but these have more adverse effects. Thus, epidural analgesia
provides effective pain relief but at the cost of increased instrumental vaginal birth.
It remains important to tailor methods used to each woman’s wishes, needs and circumstances, such as anticipated duration of labour,
the infant’s condition, and any augmentation or induction of labour.
A major challenge in compiling this overview, and the individual systematic reviews on which it is based, has been the variation in use
of different process and outcome measures in different trials, particularly assessment of pain and its relief, and effects on the neonate
after birth. This made it difficult to pool results from otherwise similar studies, and to derive conclusions from the totality of evidence.
Other important outcomes have simply not been assessed in trials; thus, despite concerns for 30 years or more about the effects of
maternal opioid administration during labour on subsequent neonatal behaviour and its influence on breastfeeding, only two out of 57
trials of opioids reported breastfeeding as an outcome. We therefore strongly recommend that the outcome measures, agreed through
wide consultation for this project, are used in all future trials of methods of pain management.
P L A I N L A N G U A G E S U M M A R Y
Pain management for women in labour - an overview
2Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Women’s experience of pain during labour varies greatly. Some women feel little pain whilst others find the pain extremely distressing.
A woman’s position in labour, mobility, and fear and anxiety or, conversely, confidence may influence her experience of pain. Several
drug and non-drug interventions are available, and in this overview we have assessed 18 systematic reviews of different interventions
used to reduce pain in labour, 15 of these being Cochrane reviews.
Most of the evidence on non-drug interventions was based on just one or two studies and so the findings are not definitive. However,
we found that immersion in water, relaxation, acupuncture and massage all gave pain relief and better satisfaction with pain relief.
Immersion and relaxation also gave better satisfaction with childbirth. Both relaxation and acupuncture decreased the use of forceps
and ventouse, with acupuncture also decreasing the number of caesarean sections. There was insufficient evidence to make a judgement
on whether or not hypnosis, biofeedback, sterile water injection, aromatherapy, and TENS are effective for pain relief in labour.
Overall, there were more studies of drug interventions. Inhaled nitrous oxide and oxygen (Entonox®) relieved pain, but some women
felt drowsy, nauseous or were sick. Non-opioid drugs (e.g. sedatives) relieved pain and some gave greater satisfaction with pain relief
than placebo or no treatment, but satisfaction with pain relief was less than with opioids. Epidurals relieved pain, but increased the
numbers of births needing forceps or ventouse, and the risk of low blood pressure, motor blocks (hindering leg movement), fever and
urine retention. Combined spinal-epidurals gave faster pain relief but more women had itching than with epidurals alone, although
urinary retention was less likely to be a problem. Local anaesthetic nerve blocks gave satisfaction but caused side effects of giddiness,
sweating, tingling, and more babies had low heart rates. Parenteral opioids (injections of pethidine and related drugs) are less effective
than epidural but there was insufficient evidence to make a judgement on whether or not they are more effective than other interventions
for pain relief in labour.
Overall, women should feel free to choose whatever pain management they feel would help them most during labour. Women who
choose non-drug pain management should feel free, if needed, to move onto a drug intervention. During pregnancy, women should be
told about the benefits and potential adverse effects on themselves and their babies of the different methods of pain control. Individual
studies showed considerable variation in how outcomes such as pain intensity were measured and some important outcomes were rarely
or never included (for example, sense of control in labour, breastfeeding, mother and baby interaction, costs and infant outcomes).
Further research is needed on the non-drug interventions for pain management in labour.
B A C K G R O U N D
History
In 2007, 78% of the members of the Cochrane Pregnancy and
Childbirth Group (PCG) consumers’ group identified pain relief
in labour as the topic of most importance to them. In view of the
range of different interventions and the importance of the topic,
the Cochrane PCG recognised that an overview of this topic was
needed. In 2010 we obtained funding as part of the National In-
stitute for Health Research (NIHR) Cochrane-NHS Engagement
Scheme to produce a generic protocol for reviews examining dif-
ferent interventions to manage pain in labour and to produce an
overview summarising the evidence from the individual reviews
in a single publication. At the time of writing, 15 Cochrane re-
views focus on methods to manage pain in labour. It is envisaged
that the overview will provide a coherent and accessible summary
of the totality of evidence about the topic, reducing or obviating
the need for readers to access each individual systematic review.
The generic protocol for the individual reviews has been published
within The Cochrane Library.The development of the overview protocol involved active consul-
tation with members of the Cochrane PCG, authors of individual
reviews and consumers. The methods were derived from Chapter
22 of the Cochrane Handbook of Systematic Reviews of Interventions(Higgins 2011). The list of core outcomes was developed in collab-
oration with members of the PCG consumers’ group; 14 respon-
dents prioritised outcomes from an extended list and added any
further outcomes that were of importance to them. This revised
set of outcomes was then discussed at a meeting on 4 October
2010 of stakeholders representing The Cochrane Collaboration,
the Cochrane PCG, an NCT (formerly National Childbirth Trust)
representative and researchers experienced in systematic reviews.
A list of core outcomes was agreed. After the stakeholders’ meet-
ing, this list of core outcomes was emailed for further considera-
tion by stakeholders and authors of individual reviews. Individual
evaluations were examined and we compiled the final list of core
outcomes.
3Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Description of the condition
The pain experienced in labour is affected by the processing of mul-
tiple physiological and psychosocial factors (Lowe 2002; Simkin
2004). Perceptions of labour pain intensity vary. Very occasionally
women feel no pain in labour and give birth unexpectedly (Gaskin
2003). At the other extreme labour pain has been reported to be
the most severe pain that a woman experiences in her lifetime
(Melzack 1984).
Pain originates from different sites during labour and birth. In
the first stage of labour (defined as the period from the onset of
labour to the complete dilatation of the cervix) (NLM 1991a),
pain occurs during contractions, is visceral or cramp-like in nature,
originates in the uterus and cervix, and is produced by distension
of uterine tissues and dilation of the cervix. In the first stage,
pain is transmitted via spinal nerves T10-L1. Labour pain can be
referred to the abdominal wall, lumbosacral region, iliac crests,
gluteal areas, and thighs. The transition phase of labour refers to
the shift from the late first stage (7 cm to 10 cm cervical dilation)
to the second stage of labour (full dilation). In the second stage
of labour (defined as from full cervical dilation to the delivery of
the baby) (Black 2009), pain occurs from distension of the vagina,
perineum, and pelvic floor. In the second stage, pain is transmitted
via the pudendal nerves, entering the spinal cord via nerve roots S2-
S4. Stretching of the pelvic ligaments is the hallmark of the second
stage of labour. Second stage pain is characterised by a combination
of visceral pain from uterine contractions and cervical stretching
and somatic pain from distension of vaginal and perineal tissues.
In addition, the woman experiences rectal pressure and an urge to
’push’ and gives birth to her baby as the presenting part descends
into the pelvic outlet.
Many factors influence the physiological and psychological pro-
cesses of birth and the extent to which women experience pain,
including parity and the way labour is managed. The pattern of
pain, for instance, appears to be different in nulliparous as com-
pared with multiparous women. Typically, nulliparous women ex-
perience greater sensory pain than multiparous women during
early labour (before 5 cm dilatation) (Lowe 2002). The positions
adopted by women and the extent of their mobility during labour
may also significantly affect the perception of pain (Kibuka 2009;
Lawrence 2009). A Cochrane systematic review (Gupta 2006)
found a reduction in the reporting of severe pain during the second
stage of labour for women using any upright or lateral position as
compared with women lying on their back during labour. Women
may also experience induced labour as being more painful than
spontaneous labour (NICE 2008).
Numerous psychosocial factors also exert an influence on women’s
experience of labour pain. Prior experience of labour and child-
birth, culture and ethnicity, educational attainment and a woman’s
ability to cope are often suggested as significant mediating variables
on the experience of labour pain (Lowe 2002). In the last century,
several philosophies of pain control evolved, using strategies to
break what has been described as the fear-tension-pain cycle (Dick
Read 1954; Dick Read 2004). Grantly Dick-Read, the famous
advocate of ’natural childbirth’, suggested that fear and anxiety
can produce muscle tension, resulting in an increased perception
of pain. Strategies to break the cycle of fear-tension-pain include
being prepared through education and purposeful activity such
as relaxation and focused breathing to relieve tension (Mozingo
1978). A wide range of ’mind-body’ interventions are currently
being used during pregnancy for preventing or treating women’s
anxiety, including autogenic training, auto-suggestion, biofeed-
back, hypnosis, imagery, meditation, prayer, relaxation therapy,
tai chi and yoga (Marc 2011).
The physical and cultural birth environment and the degree of
emotional support provided by clinical carers and the woman’s
birth companions also affect perceptions of pain (Foureur 2008a;
Foureur 2008b). In their work with pregnant woman and expec-
tant fathers, childbirth educators, midwives and doulas (a woman
who assists women during labour and childbirth) adopt a range
of different approaches to the preparation for labour and birth
and ways of planning and managing labour. Leap and Anderson
introduced ’the pain relief paradigm’ and the ’working with pain
paradigm’ to theorise these different approaches (Leap 2008). The
pain relief paradigm is based on a set of beliefs including the con-
viction that labour pain is unnecessary and barbaric in the modern
world, that the benefits of analgesia outweigh the risks and women
should not be made to feel guilty if they choose pain relief (Leap
2004). The working with pain paradigm is based on the view that
pain is an important part of the physiology of normal labour and
that, given optimal support, a woman can cope with levels of pain
in normal labour using her own natural endorphins. Endorphins
are opioids produced by the body in response to pain and other
stressors. A key role for the midwife is to reduce stimulation to the
woman’s senses so as to facilitate endorphin release (Leap 2004).
Various multi-dimensional interventions have been shown to have
an impact on the perception of pain during childbirth such as
continuous support, environment and midwife-led care (Begley
2009; Hatem 2008; Hodnett 2007; Skibsted 1992). A Cochrane
review of continuous support for women during childbirth found
that women who had continuous intrapartum support were likely
to have a slightly shorter labour, were more likely to have a sponta-
neous vaginal birth and less likely to have intrapartum analgesia or
to report dissatisfaction with their childbirth experiences (Hodnett
2007). Another Cochrane systematic review found that women
who receive midwife-led continuity of care from a small number
of midwives are less likely to use pharmacological pain relief in
labour, more likely to have an intervention-free labour and birth,
and report an increased sense of control (Hatem 2008). Drawing
together published sources of evidence, a non-Cochrane overview
suggests that a trusting relationship with caregivers, continuous
support, midwife-led care, preparation for labour, a home or birth
centre setting and use of a birth pool are factors which make it
more realistic to adopt a working with pain approach (Leap 2010).
Within the scope of the Cochrane systematic overview, we are not
4Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

able to focus in detail on the many possible interactions that medi-
ate the pain experience (spontaneous labour versus induced, prim-
iparous versus multiparous, term versus preterm birth, continuous
support versus no continuous support). Instead, we will consider
these in subgroup analyses and evaluate their impact within the
discussion and conclusions of the overview. The interventions that
we will consider for the systematic overview have a primary focus
on helping women to cope with pain in labour and in relieving
pain (NICE 2007).
Description of the interventions
A wide range of pain management methods are used by women
during childbirth (Caton 2002). Commonly, these include non-
pharmacological interventions (hypnosis, biofeedback, intracu-
taneous or subcutaneous sterile water injection, immersion in
water, aromatherapy, relaxation techniques (yoga, music, audio),
acupuncture or acupressure, manual methods (massage, reflex-
ology), transcutaneous electrical nerve stimulation (TENS)) and
pharmacological interventions (inhaled analgesia, opioids, non-
opioid drugs, local anaesthetic nerve blocks, epidural and intrathe-
cal injections of local anaesthetics or opioids, or both). Broadly
speaking, the non-pharmacological interventions primarily aim to
help women cope with pain in labour, whereas the pharmacologi-
cal interventions primarily aim to relieve the pain of labour (NICE
2007). However, we acknowledge that pain in labour is multi-
faceted and that there is obviously some overlap. Also, some in-
terventions are taught in antenatal classes and administered prior
to the onset of labour (hypnosis, biofeedback, aromatherapy, re-
laxation techniques (yoga, music, audio), acupuncture or acupres-
sure, manual methods (massage, reflexology), TENS), whilst oth-
ers are administered only during labour (intracutaneous or subcu-
taneous sterile water injection, immersion in water, inhaled anal-
gesia, opioids, non-opioid drugs, local anaesthetic nerve blocks,
epidural and intrathecal injections of local anaesthetics or opioids,
or both). This issue will be explored within our discussion.
The following section outlines the range of non-pharmacological
and pharmacological interventions in current use for the manage-
ment of pain during childbirth.
Non-pharmacological interventions
1. Hypnosis
Hypnosis has been described as a state of narrow focused attention,
reduced awareness of external stimuli, and an increased response
to suggestions (Gamsa 2003). Suggestions are verbal or non-verbal
communications that result in apparent spontaneous changes in
perception, mood or behaviour. These therapeutic communica-
tions are directed to the person’s subconscious and the responses
are independent of any conscious effort or reasoning. Women can
learn self-hypnosis which can be used in labour to reduce pain
from contractions. Recent advances in neuro-imaging have led to
increased understanding of the neuro-physiological changes oc-
curring during hypnosis induced analgesia (Maquet 1999). The
anterior cingulate gyrus of the limbic system has been demon-
strated, by positron emission tomography, to be one of the sites in
the brain affected by hypnotic modulation of pain (Faymonville
2000). The suppression of neural activity, between the sensory cor-
tex and the amygdala-limbic system, appears to inhibit the emo-
tional interpretation of sensations being experienced as pain.
Hypnosis for childbirth is self-hypnosis, where a practitioner
teaches the mother how to induce a ’state of consciousness similar
to meditation which results in failure of normally perceived expe-
riences reaching conscious awareness’ (Cyna 2004). It uses focused
attention and relaxation, to develop increased receptivity to verbal
and non-verbal communications which are commonly referred to
as ’suggestions’ (August 1961; Cyna 2004; Leap 2010; Werner
1982). These are positive statements used in order to achieve spe-
cific therapeutic goals. In labour and childbirth the goal is to alle-
viate or reduce fear, tension, and pain (Eng 2006; Landolt 2011)
so that the physiological act of birth can progress in a way that
is comfortable for the mother. There is a common misconcep-
tion that when in a hypnotic state the individual loses control of
her thoughts and actions, which would jeopardise their personal
autonomy. Women using self-hypnosis for labour and birth are
fully in control and aware of what is happening to them and those
around them (August 1961).
2. Biofeedback
Biofeedback (or biological feedback) encompasses a therapeutic
technique by which individuals receive training to improve their
health and well-being through signals coming from their own
bodies (including temperature, heart rate, muscular tension). The
underlying principle is that changes in thoughts and emotions
may result in changes in body functioning. Biofeedback aims to
gain control over physiological responses with the aid of electronic
instruments, under the supervision of experts. Instruments in-
clude: electromyographs measuring muscle tension; skin temper-
ature gauges showing changes in heat emission by the skin, reflect-
ing change in blood flow; galvanic skin response sensors, which
assess the volume of sweat produced under stress by measuring
skin conductivity; electroencephalographs which measure brain-
wave activity; electrocardiographs which monitor heart rate and
rhythm and may be useful in detecting and relieving tachycardia
(an overly rapid heartbeat) and, in turn, controlling high blood
pressure. Respiration feedback devices concentrate on the rate,
rhythm, and type of breathing to help lessen symptoms of asthma,
anxiety, and hyperventilation, and also promote relaxation (AMA
1993; Rosenfeld 1996).
5Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

3. Intracutaneous or subcutaneous sterile water injection
Intracutaneous or intradermal injections of sterile water in the
skin over the sacrum have been shown to relieve the pain of labour
(Ader 1990; Trolle 1991; Wiruchpongsanon 2006). This tech-
nique could be of particular use to those practising in hospitals
that do not have access to epidural analgesia. It could also be
helpful for women who want to avoid medication during labour
and birth. The technique is thought to work through the release
of endogenous opioids (the endorphins and encephalins) and is
based on gate control pain theories (Lytzen 1989; Trolle 1991;
Wiruchpongsanon 2006).
4. Immersion in water
Warm water immersion during labour, including birth, used for
relaxation and pain relief, has a long history in lay and clinical care
(Garland 2000). It refers to the immersion in water by a pregnant
woman during any stage of labour (first, second, third), and where
the woman’s abdomen is completely submerged. The immersion
takes place in a receptacle that may be a pool, tub or bath, and
which is larger than a normal domestic bath. Immersion may be
for one or more stages of labour, and for any duration. The buoy-
ancy of water enables a woman to move more easily than on land
(Edlich 1987). This can facilitate the neuro-hormonal interactions
of labour, alleviating pain, and potentially optimising the progress
of labour (Ginesi 1998a; Ginesi 1998b). Water immersion may be
associated with improved uterine perfusion, less painful contrac-
tions, and a shorter labour with fewer interventions (Aird 1997;
Garland 2000; Geissbuehler 2000; Moneta 2001; Otigbah 2000;
Schorn 1993). Also, shoulder-deep warm water immersion reduces
blood pressure due to vasodilatation of the peripheral vessels and
redistribution of blood flow. It is suggested that water immersion
during labour increases maternal satisfaction and sense of control
(Hall 1998; Richmond 2003). It is also suggested that the fetus
benefits from a relaxed mother, as this optimises placental perfu-
sion, and release of ’nature’s opiates’, the endogenous opioids (en-
dorphins and encephalins). Accordingly, when the mother is not
fearful, oxytocin release is optimised, stimulating effective con-
tractions. In addition, the ease of mobility that water immersion
offers may optimise fetal position by encouraging flexion (Ohlsson
2001).
5. Aromatherapy
Aromatherapy is the use of essential oils, drawing on the healing
powers of plants. The mechanism of action for aromatherapy is
unclear. Studies investigating psychological and physiological ef-
fects of essential oils showed no change on physiological parame-
ters such as blood pressure or heart rate but did indicate psycho-
logical improvement in mood and anxiety (Stevensen 1995). Es-
sential oils are thought to increase the secretion of the body’s own
sedative, stimulant and relaxing neurotransmitters (paracrine and
endocrine). The oils may be massaged into the skin, or inhaled by
using a steam infusion or burner. Aromatherapy is increasing in
popularity among midwives and nurses (Allaire 2000).
6. Relaxation techniques (yoga, music, audio)
Relaxation techniques are mind-body interventions which are
based on developing conscious awareness of muscular tension, the
practice of releasing tension and maintaining relaxation often car-
ried out in conjunction with focused breathing, meditation and
visualisation. These kinds of approaches are commonly used for
labour. Unanswered questions include: which approaches are most
effective, the most appropriate timing for preparatory interven-
tions during pregnancy, the extent to which practice makes a dif-
ference and which techniques women find acceptable and useful.
Yoga, meditation, music and hypnosis techniques may all have a
calming effect and provide a distraction from pain and tension
(Vickers 1999). In future updates, this review will be split into
separate reviews on yoga, music and audio.
7. Acupuncture or acupressure
Acupuncture involves the insertion of fine needles into different,
specific parts of the body. Other acupuncture-related techniques
include laser acupuncture and acupressure (applying pressure on
the acupuncture point). These techniques all aim to treat illnesses
and soothe pain by stimulating acupuncture points. Acupuncture
points used to reduce labour pain are located on the hands, feet
and ears. Several theories have been presented as to exactly how
acupuncture works. One theory proposes that stimulation of touch
fibres blocks pain impulses at the ‘pain gates’ in the spinal cord.
The impulses in the pain fibres are thus less likely to reach the
brain stem, thalamus and cerebral cortex (Wall 1967). Since most
acupuncture points are either connected to, or located near, neural
structures, this suggests that acupuncture stimulates the nervous
system. Another theory suggests that acupuncture stimulates the
body to release endorphins (endogenous opioids), which reduce
pain (Pomeranz 1989).
8. Massage, reflexology and other manual methods
Manual healing methods include massage and reflexology. Massage
involves manipulation of the body’s soft tissues. It is commonly
used to help relax tense muscles and to soothe and calm the indi-
vidual. A woman who is experiencing backache during labour may
find massage over the lumbosacral area soothing. Some women
find light abdominal massage, known as ’effleurage’, comforting.
Different massage techniques may suit different women. Massage
may help to relieve pain by assisting with relaxation, inhibiting
sensory transmission in the pain pathways or by improving blood
flow and oxygenation of tissues (Vickers 1999). Reflexologists pro-
pose that there are reflex points on the feet corresponding to or-
gans and structures of the body and that pain may be reduced by
6Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

gentle manipulation or pressing certain parts of the foot. Pressure
applied to the feet has been shown to result in an anaesthetising
effect on other parts of the body (Ernst 1997). In future updates,
this review will be split into separate reviews on massage and re-
flexology.
9. TENS
Transcutaneous electrical nerve stimulation (TENS) uses a de-
vice which emits low voltage electrical impulses which vary in fre-
quency and intensity. In labour, the electrodes from the TENS ma-
chine are usually attached to the lower back and women themselves
control the electrical currents using a hand-held device. TENS can
also be applied to acupuncture points or directly to the head by
trained staff. The way that TENS acts to relieve pain is not well
understood. The electrical pulses are thought to stimulate nerve
pathways in the spinal cord which block the transmission of pain.
A number of theories have been proposed. According to the gate
control theory (Melzack 1965), the transmission of pain is inhib-
ited by the stimulation of large, afferent or sensory touch nerve
fibres which carry impulses towards the central nervous system. It
is also suggested that painful stimuli result in release of endorphins
and encephalins, which mediate the experience of pain (Lechner
1991). It is further thought that by reducing anxiety, increasing
a sense of control, and by providing distraction, TENS increases
a woman’s sense of well-being and thereby reduces pain in labour
(Brucker 1984; Findley 1999; Gentz 2001; Simkin 2004). Lastly,
TENS may reduce the length of labour by suppressing the release
of catecholamines, which can inhibit the contraction of the uterus
and thereby, delay progress (Lowe 2002).
Pharmacological interventions
1. Inhaled analgesia
Inhaled analgesia during labour involves the inhalation of sub-
anaesthetic concentrations of anaesthetic agents while the mother
remains awake and her protective laryngeal reflexes remain in-
tact. Possibilities for inhaled analgesia for pain relief in labour in-
clude isoflurane, sevoflurane, trichloroethylene in air, methoxyflu-
rane, cyclopropane, nitrogen protoxide, nitralgin, anesoxyn and
eutonal. Subanaesthetic concentrations of nitrous oxide, enflu-
rane, isoflurane and methoxyflurane do not significantly decrease
uterine contractions and are preferred for this reason. However,
only nitrous oxide (in 50% oxygen) is widely used for analgesia
in modern obstetric practice. This is attributed to: ease of admin-
istration, relative lack of flammability, absence of pungent odour,
absence of effect on uterine contractions, lack of reports of ma-
lignant hyperthermia, minimal toxicity and minimal depression
of the cardio-vascular system; a favourable partition coefficient
leading to rapid onset and elimination from woman, fetus and
neonate (KNOV 2009; Rosen 2002). The evidence on the use
of nitrous oxide for relief of labour pain has been summarised in
a systematic review (Rosen 2002). The woman can self-admin-
ister under supervision, after initial instruction (Clyburn 1993).
Inhaled analgesia is administered either intermittently, with dis-
continuation of use as the contraction pain eases or disappears
(recommended), or continuously, by inhaling both during and be-
tween contractions. However, there is concern, centring on staff
rather than patients, regarding the effect of prolonged exposure,
because of reported possible associations with loss of fertility, mis-
carriage, preterm birth and lowered concentrations of vitamin B12
(Ahlborg 1996; Axelsson 1996; BOC 2010; Bodin 1999; Boivin
1997; Zielhuis 1999). Accordingly, nitrous oxide concentrations
should be regularly measured, according to manufacturers’ guide-
lines (BOC 2010). Other possible adverse effects are maternal
drowsiness, hallucinations, vomiting, hyperventilation and tetany,
and maternal or fetal hypoxia usually encountered when nitrous
oxide use is excessively prolonged or extensive, especially if the rule
of self-administration is violated.
The precise mechanism of action of inhaled analgesia remains un-
certain, but anaesthetic actions are related to suppression of activ-
ity of the reticuloendothelial network in the brainstem. Maze and
Fuginaga hypothesised that nitrous oxide induces the release of
endogenous opioids in the peri-aqueductual grey area of the mid-
brain (Maze 2000), which could modulate pain stimuli through
the descending spinal cord nerve pathways.
2. Opioids
Most obstetric units in developed countries offer intramuscular
opioids, along with facilities for epidural analgesia. Opioids are
relatively inexpensive drugs, and the use of pethidine, meptazinol
or diamorphine during labour is common midwifery and obstet-
ric practice in some countries. In other parts of the world, par-
enteral (intravenous or intramuscular) opioids commonly used in
labour include morphine, nalbuphine, fentanyl and more recently
remifentanil (Evron 2007). The extent of usage of parenteral opi-
oids during labour worldwide is unclear. Worldwide, pethidine is
the most commonly used opioid (Bricker 2002). There are con-
cerns about maternal effects which include an impaired capacity
to engage in decision making about care, sedation, hypoventila-
tion, hypotension, prolonged labour, urine retention, nausea and/
or vomiting, and the slowing of gastric emptying, which increases
the risk of inhalation of gastric contents should a general anaes-
thetic be required in an emergency. If a woman feels drowsy or
sedated, she is less likely to mobilise and adopt an upright position
and, as a result, this may lengthen her labour and make it more
painful (Lawrence 2009). Opioids readily cross the placenta by
passive diffusion, and some are trapped by ionisation. Neonatal
respiratory depression and hypothermia remain major concerns.
It is estimated that it can take a newborn three to six days to elim-
inate pethidine, and its metabolite, norpethidine, from its system
(Hogg 1977). Pethidine has been shown to significantly affect fe-
7Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

tal heart rate variability, accelerations and decelerations, during
labour (Sekhavat 2009; Solt 2002). Changes in normal fetal heart
indices have consequences for the woman. She will be required
to have electronic fetal heart rate monitoring if she is in hospital,
and transfer to hospital if she is in the community. Results from
observational studies have reported effects of opioids on the new-
born that include inhibited suckling at the breast and decreased
alertness, resulting in delayed effective breastfeeding (Nissen 1995;
Ransjo-Arvidson 2001; Righard 1990) and earlier cessation (Rajan
1994).
3. Non-opioid drugs
Non-opioid medications are drugs that have principally analgesic,
antipyretic, sedative and anti-inflammatory actions. They are not
technically part of the analgesic family, but are nonetheless consid-
ered analgesics in practice. These include acetaminophen (parac-
etamol), the non-steroidal anti-inflammatory drugs (NSAIDs),
such as aspirin, and antispasmodic drugs such as hyoscine
(Bayarski 2006; Hebbes 2000).
Acetaminophen and NSAIDs can effectively relieve mild to mod-
erate pain, and for moderate to severe pain, they can be used in
combination with other drugs to enhance pain relief.
Non-opioids affect some of the chemical changes that normally
take place wherever body tissues are injured or damaged. These
chemical changes at the site of the injury typically result in inflam-
mation and increased pain sensitivity. However, there are limits to
the pain afforded by non-opioids; this is referred to as a ’ceiling
effect’. Once that upper limit or ceiling is reached, taking more
of the non-opioid will not provide any further pain relief. Most
non-opioids are quite safe when used for temporary acute pain;
problems may arise when people take them over a long period of
time (for chronic pain), then they could damage the lining of the
gastro-intestinal tract or the kidneys, or, more rarely, other organs
(Bayarski 2006; Dewhurst 2007; Hebbes 2000).
4. Local anaesthetic nerve blocks
Pudendal and paracervical block (PCB) are the most commonly
performed local anaesthetic nerve blocks which have been used
for decades.
A pudendal block is performed by injection of local anaesthetic
around the trunk of the pudendal nerve. Pudendal block is used
in the second stage of labour, predominantly when instrumental
delivery is performed (Pace 2004). During descent of the present-
ing part of the fetus in the second stage, the primary focus of pain
is in the lower vagina, perineum and vulva, which are innervated
from sacral nerve roots 2, 3 and 4 via the pudendal nerve. Infiltra-
tion of local anaesthetic around the trunk of the pudendal nerve
at the level of ischial spines leads to analgesia of these areas. Prior
to the widespread use of epidural analgesia in obstetrics, pudendal
blocks were the preferred analgesic technique for delivery. Puden-
dal blocks are also used to supplement epidural labour analgesia,
which occasionally may have some ’sacral sparing.’
A paracervical block is performed by infiltration of local anaes-
thetic in the cervix. It is injected into between two to six sites at a
depth of 3 mm to 7 mm alongside the vaginal portion of the cervix
in the vaginal fornices (Mankowski 2009). Paracervical infiltration
interrupts the visceral sensory fibres of the lower uterus, cervix,
and upper vagina (T10-L1) as they pass through the uterovaginal
plexus (Frankenhauser’s plexus) on each side of the cervix.
5. Epidural (including combined spinal epidural)
Epidural analgesia is a central nerve blockade technique, which
involves the injection of a local anaesthetic, with or without an
opioid into the lower region of the spine close to the nerves that
transmit painful stimuli from the contracting uterus and birth
canal. The most commonly prescribed local anaesthetic in the
UK is bupivacaine; levobupivacaine, ropivacaine, and lidocaine/
lignocaine are also used in epidural or intrathecal injections. Local
anaesthetics inhibit nerve conduction by blocking sodium chan-
nels in nerve cell membranes, thereby preventing the propagation
of nerve impulses along these fibres. Blocking impulses from the
sensory nerves as they cross the epidural space results in analge-
sia, which should be apparent within 10 to 20 minutes of ad-
ministration. The anaesthetic placed in the epidural space exerts
a concentration specific effect, affecting all the modalities of sen-
sation of the blocked nerves to varying degrees, such that admin-
istration of a lower-dose anaesthetic (e.g. 0.125% bupivacaine)
partially selectively blocks painful stimuli while preserving motor
function, whereas higher doses of anaesthetic cause complete sen-
sory and motor blockade, limiting mobility in labour. The sec-
ond stage of labour may be prolonged and instrumental delivery is
more likely (Anim-Somuah 2005). Blocking of sympathetic nerves
occurs at varying concentrations and manifests as vasodilatation
and hypotension (Anim-Somuah 2005). Other reported problems
include: urine retention, shivering, fever, tinnitus, tremor, respi-
ratory and cardiovascular depression. Epidural solutions are ad-
ministered either by bolus, continuous infusion or patient-con-
trolled pump. An intermittent technique involves injections of lo-
cal anaesthetic through a catheter positioned in the epidural space.
Boluses of higher concentrations, as used in the earlier years, have
been associated with a dense motor block resulting in reduced mo-
bility, decreased pelvic tone and impairment of the bearing down
effort in the second stage of labour (Thornton 2001). More re-
cently, there has been a trend to use a lower concentration of local
anaesthetic in combination with a variety of opiates; these com-
binations provide analgesic effect while allowing the woman to
maintain some motor function, such as the ability to move during
her labour and retain her ability to bear down (COMET 2001;
Russell 2000). Combined spinal-epidural (CSE) involves a single
injection of local anaesthetic or opiate, or both, into the cerebral
spinal fluid as well as insertion of the epidural catheter. CSE com-
8Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

bines the advantages of spinal analgesia (faster onset of pain relief,
more reliable analgesia) with the advantages of epidural analgesia
such as continuing pain relief, potentially maintained throughout
the entire duration of labour (Hughes 2003). However, some of
the disadvantages of opioid administration remain, including itch-
ing, respiratory depression and, in observational studies, reduced
breastfeeding rates (Jordan 2005; Torvaldsen 2006), but evidence
is uncertain (Reynolds 2011). In addition, the rare but serious
adverse effects of neuraxial administration should be considered,
including introduction of infection, nerve root damage and even
inadvertent intravenous injection (Jordan 2010).
Why it is important to do this overview
The totality of evidence from randomised controlled trials of in-
terventions for pain management in labour has never been assem-
bled before in a systematic and comprehensive way. An ’overview
of reviews’ will provide a clinically meaningful summary of one
of the most important topics in pregnancy and childbirth. The
overview provides a coherent summary of the totality of evidence
without the need to access many individual systematic reviews.
This may help busy clinicians, policy makers, childbirth educators
and consumers.
O B J E C T I V E S
The objectives of this overview are to summarise the evidence
from Cochrane systematic reviews regarding the effects and sa-
fety of non-pharmacological and pharmacological interventions
to manage pain in labour. We also considered findings from
non-Cochrane systematic reviews in the absence of an available
Cochrane review.
M E T H O D S
Criteria for considering reviews for inclusion
In this overview we have included any published Cochrane system-
atic review of randomised controlled trials focusing on the man-
agement of pain in labour. We have only included non-Cochrane
systematic reviews in the absence of an available Cochrane review
in an area listed below. To be considered, the non-Cochrane sys-
tematic review must have used a systematic approach, only in-
cluded randomised controlled trials and have assessed the method-
ological quality of the included clinical trials.
The participants in reviews are women in labour. This includes
women in high-risk groups, e.g. preterm labour or following in-
duction of labour.
We have included the following non-pharmacological (hypno-
sis, biofeedback, intracutaneous or subcutaneous sterile water in-
jection, immersion in water, aromatherapy, relaxation techniques
(yoga, music, audio), acupuncture or acupressure, manual meth-
ods (massage, reflexology), transcutaneous electrical nerve stimu-
lation (TENS)) and pharmacological interventions (inhaled anal-
gesia, opioids, non-opioid drugs, local anaesthetic nerve blocks,
epidural and intrathecal injections of local anaesthetics or opioids,
or both).
We have compared interventions with placebo/no treatment or
with a different intervention.
Each of the contributing Cochrane reviews followed a generic pro-
tocol (Jones 2011). To avoid duplication, each Cochrane review
included comparisons only with the interventions listed above it in
the following list of potential interventions. Thus, the aromather-
apy review (6), from the available evidence, only included com-
parisons with immersion in water (5), sterile water injection (4),
biofeedback (3), hypnosis (2) and placebo/no treatment (1). This
strategy aimed to avoid the same comparisons being included in
more than one of the original Cochrane reviews. Methods of pain
management identified in the future will be added to the end of
the list. The current list is as follows.
1. Placebo/no treatment.
2. Hypnosis (Madden 2012)
3. Biofeedback (Barragán 2011).
4. Intracutaneous or subcutaneous sterile water injection
(Derry 2012).
5. Immersion in water (Cluett 2009).
6. Aromatherapy (Smith 2011c).
7. Relaxation techniques (yoga, music, audio)* (Smith 2011b).
8. Acupuncture or acupressure (Smith 2011a).
9. Massage, reflexology and other manual methods* (Smith
2012).
10. TENS (Dowswell 2009).
11. Inhaled analgesia (Klomp 2012).
12. Opioids (Ullman 2010).
13. Non-opioid drugs (Othman 2012).
14. Local anaesthetic nerve blocks (Novikova 2012).
15. Epidural (including combined spinal epidural)
(Anim-Somuah 2011; Simmons 2012).
* In future updates these individual reviews will be split into sep-
arate reviews on yoga, music, audio and massage and reflexology,
respectively.
Outcomes
Types of outcome measure
The following list of core outcomes was developed in collaboration
with members of the Pregnancy and Childbirth Group (PCG)
consumers’ group - see ’History’ described in Background.
9Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Primary outcomes
Effects of interventions
Pain intensity (as defined by trialists)
Satisfaction with pain relief (as defined by trialists)
Sense of control in labour (as defined by trialists)
Satisfaction with childbirth experience (as defined by trialists)
Safety of interventions
Effect (negative) on mother/baby interaction
Breastfeeding (at specified time points)
Assisted vaginal birth
Caesarean section
Adverse effects (for women and infants; review specific)
Admission to special care baby unit/neonatal intensive care unit
(as defined by trialists)
Apgar score less than seven at five minutes
Poor infant outcomes at long-term follow-up (as defined by trial-
ists)
Other outcomes
Cost (as defined by trialists)
Measuring any subjective outcome is a major challenge. Pain is a
highly subjective phenomenon, with a complex physiological and
psychological basis (Kane 2002). It has been defined as “a complex
constellation of unpleasant sensory, perceptual and emotional ex-
periences and certain associated autonomic, psychological, emo-
tional and behavioural responses” (Bonica 1990). Due to this com-
plexity, there has been little research focused on developing psy-
chometrically sound measures of pain, especially in labour and
childbirth (Lowe 2002). Consequently there is considerable varia-
tion in the way that pain is measured across individual studies con-
tained within individual reviews (Bricker 2002; Dowswell 2009).
It is for these reasons that we have used the trialists’ definitions of
outcome measures from the individual reviews. Similarly, breast-
feeding as an outcome measure is not straightforward in terms of
timing of recording and reporting. The infant feeding literature
offers little consistency regarding the timing of data collection.
Consequently, it is difficult to compare data sets (Britton 2007).
In addition, definitions of exclusive, full and partial breastfeeding
will need to be considered. Where information on pain and infant
feeding has been collected, we have detailed any definitions used
in the results by individual review tables, in Additional tables.
Search methods for identification of reviews
We contacted the Trials Search Co-ordinator of the Cochrane
Pregnancy and Childbirth Group in order to identify all relevant
systematic reviews of pain management in labour. In the absence
of an available Cochrane systematic review in one of the follow-
ing areas (hypnosis, biofeedback, intracutaneous or subcutaneous
sterile water injection, immersion in water, aromatherapy, relax-
ation techniques (yoga, music, audio), acupuncture or acupres-
sure, manual methods (massage, reflexology), TENS, inhaled anal-
gesia, opioids, non-opioids, local anaesthetic nerve blocks, epidu-
ral), we searched the Database of Abstracts of Reviews of Effects
(The Cochrane Library 2011, Issue 2 of 4), MEDLINE (1966 to
31 May 2011) and EMBASE (1980 to 31 May 2011) using the
search strategies detailed in Appendix 1.
Data collection and analysis
The methodology for data collection and analysis is based on
Chapter 22 of the Cochrane Handbook of Systematic Reviews of In-terventions (Higgins 2011).
Selection of reviews
Two review authors independently assessed for inclusion all the
potential systematic reviews we identified as a result of the search
strategy. We resolved any disagreement through discussion or, if
required, we consulted a third person.
Data extraction and management
Two review authors independently extracted data from the reviews
using a predefined data extraction form. We resolved discrepancies
through discussion or, if required, we consulted a third person.
We entered data into Review Manager software (RevMan 2011)
and checked for accuracy. If any information from the reviews
was unclear or missing, we accessed the published reports of the
individual trials. If the information could not be obtained from
the published reports, then we contacted the review authors or
authors of the original reports to provide clarification and further
details.
Assessment of methodological quality of included
reviews
We have addressed two different quality assessments in this
overview: the quality of evidence in the included reviews and the
methodological quality of the systematic reviews. Two review au-
thors assessed methodological quality independently. We resolved
discrepancies through discussion or, if required, we consulted a
third person.
Quality of evidence in included reviews
Two review authors independently assessed the overall quality of
the evidence presented in the included reviews by examining the
methods used for assessing risk of bias of the individual included
10Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

studies. We assessed whether the Cochrane reviews used the do-
main-based evaluation for assessment of risk of bias as outlined in
Chapter 8 of the Cochrane Handbook for Systematic Reviews of In-terventions (Higgins 2011). For non-Cochrane systematic reviews,
we have summarised the methods used to assess methodological
quality, including details regarding the tools used and the dimen-
sions assessed e.g. sequence generation; allocation sequence con-
cealment; blinding; incomplete outcome data.
Quality of included reviews
Two review authors independently assessed the methodological
quality of the included reviews using the ’assessment of multiple
systematic reviews’ (AMSTAR) measurement tool (Shea 2007).
The AMSTAR tool assesses the following criteria.
1. Was an ’a priori’ design provided?
2. Was there duplicate study selection and data extraction?
3. Was a comprehensive literature search performed?
4. Was the status of publication (i.e. grey literature) used as an
inclusion criterion?
5. Was a list of studies (included and excluded) provided?
6. Were the characteristics of the included studies provided?
7. Was the scientific quality of the included studies assessed
and documented?
8. Was the scientific quality of the included studies used
appropriately in formulating conclusions?
9. Were the methods used to combine the findings of studies
appropriate?
10. Was the likelihood of publication bias assessed?
11. Was the conflict of interest stated?
Data synthesis
We have provided a narrative summary of the results for the in-
dividual reviews for each of the primary outcomes and present
these using tables and figures (e.g. characteristics of included re-
views, summary of quality of evidence within individual system-
atic reviews, AMSTAR ratings for each systematic review, results
by individual review tables). It was not anticipated that we would
be able to perform any quantitative data analyses. However, for
future updates of this overview, if the data allow, we may perform
some indirect comparisons of interventions across reviews for the
primary outcomes. We had planned, if possible, to present data
from the following subgroups (if these data were available within
the included systematic reviews).
1. Spontaneous labour versus induced labour.
2. Primiparous versus multiparous.
3. Term versus preterm birth.
4. Continuous support in labour versus no continuous
support.
R E S U L T S
Cochrane systematic reviews
A total of 15 Cochrane systematic reviews were identified by
the Trials Search Co-ordinator of the Cochrane Pregnancy and
Childbirth Group, all of which met the inclusion criteria for this
overview. A priori, the research question and inclusion criteria were
provided in a published generic protocol (Jones 2011). All but
one of the 15 Cochrane systematic reviews (protocols and updates
of reviews), followed this generic protocol. The Cochrane review
on combined spinal-epidural versus epidural analgesia in labour
(Simmons 2012) did not adhere to the generic protocol because
it did not fit in with the hierarchy of interventions.
Non-Cochrane systematic reviews
In order to identify any gaps not already covered by the Cochrane
systematic reviews, we searched The Database of Abstracts of Re-
views of Effects (The Cochrane Library 2011, Issue 2 of 4), MED-
LINE (1966 to 31 May 2011) and EMBASE (1980 to 31 May
2011) using the search strategies detailed in Appendix 1. A total
of 65 potentially eligible reviews were identified from this search.
Three of these filled a gap not already covered by the Cochrane
reviews (Halpern 2003a; Hutton 2009; Mardirosoff 2002). The
remaining 62 were excluded because they were not a systematic
review (N = 26), they were out of date and focused on an area al-
ready covered by one of the included Cochrane or non-Cochrane
systematic reviews (N = 32), or they did not fit the inclusion cri-
teria for this overview (N = 4). A description of the characteristics
of these excluded reviews, and the reasons for exclusion are set out
in an additional table (Table 1).
Figure 1 gives a flow diagram outlining the selection process and
review numbers at each stage.
11Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 1. Study flow diagram.
12Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Description of included reviews
We have included 15 Cochrane reviews: nine non-pharmaco-
logical reviews (hypnosis (Madden 2012), biofeedback (Barragán
2011), intracutaneous or subcutaneous sterile water injection
(Derry 2012), immersion in water (Cluett 2009), aromatherapy
(Smith 2011c), relaxation techniques [yoga, music, audio] (Smith
2011b), acupuncture or acupressure (Smith 2011a), manual meth-
ods (massage, reflexology) (Smith 2012), transcutaneous electri-
cal nerve stimulation (TENS) (Dowswell 2009)) and six exam-
ining pharmacological interventions (inhaled analgesia (Klomp
2012), opioids (Ullman 2010), non-opioid drugs (Othman 2012),
local anaesthetic nerve blocks (Novikova 2012), epidural and
intrathecal injections of local anaesthetics or opioids, or both
(Anim-Somuah 2011; Simmons 2012)). All of these reviews have
recently been updated and the search dates are in 2011. Eleven of
the reviews had already been published or were in-press at the time
this overview was prepared. However, while four of the remaining
reviews had been submitted for publication at this time, they had
not been revised after peer review, or approved for publication.
Therefore, the findings we have reported in this overview for these
reviews (examining hypnosis (Madden 2012), inhaled analgesia
(Klomp 2012), non-opioid drugs (Othman 2012) and combined
spinal epidural (Simmons 2012)) are based on the draft reviews
submitted by the authors for editorial consideration. We are aware
that including data from these non-completed reviews potentially
introduces bias into the overview process. If there are changes in
results in of any of these reviews, new findings will be incorporated
into the first update of this overview.
The titles of the 15 Cochrane reviews are listed below:
1. Hypnosis for pain management during labour and childbirth
(Madden 2012).
2. Biofeedback for pain management during labour (Barragán
2011).
3. Intracutaneous or subcutaneous sterile water injection for pain
management in labour (Derry 2012).
4. Immersion in water in labour and birth Cluett 2009).
5, Aromatherapy for pain management in labour (Smith 2011c).
6. Relaxation techniques for pain management in labour (Smith
2011b).
7. Acupuncture or acupressure for pain management in labour
(Smith 2011a).
8. Massage, reflexology and other manual methods for pain man-
agement in labour (Smith 2012).
9. Transcutaneous electrical nerve stimulation (TENS) for pain
management in labour (Dowswell 2009).
10. Inhaled analgesia for pain management in labour (Klomp
2012).
11. Parenteral opioids for maternal pain management in labour
(Ullman 2010).
12. Non-opioid drugs for pain management in labour (Othman
2012).
13. Local anaesthetic nerve block for pain management in labour
(Novikova 2012).
14. Epidural versus non-epidural or no analgesia in labour (Anim-
Somuah 2011).
15. Combined spinal-epidural versus epidural analgesia in labour
(Simmons 2012).
In addition we have included three non-Cochrane reviews that
focused on methods of pain relief or comparisons not covered by
the Cochrane reviews (Halpern 2003a; Hutton 2009; Mardirosoff
2002) and the dates of publication indicate that these reviews are
less up to date. These reviews examined sterile water injections
(Hutton 2009); intrathecal opioids (Mardirosoff 2002) and epidu-
ral ropivacaine versus bupivacaine (Halpern 2003a), as listed:
1. Sterile water injection for labour pain: a systematic review and
meta-analysis of randomised controlled trials (Hutton 2009).
2. Fetal bradycardia due to intrathecal opioids for labour analgesia:
a systematic review (Mardirosoff 2002).
3. Epidural ropivacaine versus bupivacaine for labor: a meta-anal-
ysis (Halpern 2003a).
The specific inclusion and exclusion criteria in the contributing
reviews varied: all focused on pain in labour and all included ran-
domised trials; however, authors of each review had particular cri-
teria for participants and interventions. For example, in the hyp-
nosis review women may have been recruited and the interven-
tion may have occurred during pregnancy (for example in ante-
natal classes), whereas, for pharmacological interventions women
were predominantly recruited when they were admitted to hospi-
tal during labour. While all but one (combined spinal epidural)
of the Cochrane reviews were based on a generic protocol and
collected outcome data on a prespecified list of primary and sec-
ondary outcomes, individual review authors may also have col-
lected data on other outcomes which we have not reported in this
overview. Outcomes relating to adverse effects are mainly review
(i.e. intervention) specific. For non-Cochrane reviews outcomes
were determined by the individual review authors and may not
have included most of our prespecified outcomes; for this reason
we have reported only limited data from these non-Cochrane re-
views.
The number of trials and participants included in the various
contributing reviews varied considerably from two studies and
535 women in the aromatherapy review, and four studies and 201
women in the biofeedback review, through to 57 included studies
and more than 7000 participants in the parenteral opioids review.
The trials in each of the contributing reviews were carried out in
a variety of settings and over varying periods of time; for example,
epidural has been used widely since the 1980s whereas studies
included in the parenteral opioids review date back as far as the
13Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

1930s.
We have set out the characteristics of the contributing reviews in
four additional tables and it is important that the findings of the
overview are interpreted in the light of information in the tables.
Characteristics of included Cochrane systematic reviews - non-
pharmacological interventions - see Table 2
Characteristics of included Cochrane systematic reviews - phar-
macological interventions - see Table 3
Characteristics of included Non-Cochrane systematic reviews -
non-pharmacological interventions - see Table 4
Characteristics of included Non-Cochrane systematic reviews -
pharmacological interventions - see Table 5
Quality of evidence in included reviews
The quality of the evidence (i.e. the methodological quality of in-
dividual trials) in each of the contributing reviews was assessed us-
ing the Cochrane risk of bias tool set out in the Handbook (Higgins
2011). Just as the number of trials contributing data to each re-
view varied, so too did the overall methodological quality of those
trials. Again, the evidence in each section of the results should be
interpreted in the light of the strengths and weaknesses of indi-
vidual trials. In the Cochrane reviews focusing on non-pharmaco-
logical interventions, for example, blinding staff and participants
in trials was either not attempted, or it was not clear that alterna-
tives (such as sham TENS devices) achieved successful blinding.
In the Cochrane review focusing on sterile water injection trials
were only included if they were double-blind, but this criterion
was not used in all reviews. Many trials included in reviews used
methods to generate the randomisation sequence, and to allocate
participants to groups, with high risk of bias. For example, in the
TENS review, most of the included studies used methods of allo-
cating participants that did not conceal allocations and therefore
were at high risk of bias. Many trials involving pharmacological
methods could achieve blinding through use of placebo, but these
trials often encountered other methodological problems (for ex-
ample high levels of sample attrition or protocol deviations) leav-
ing results at high risk of bias. The quality of the evidence from
Cochrane reviews has been summarised in two additional tables:
Quality of evidence in included Cochrane systematic reviews -
non-pharmacological interventions - see Table 6
Quality of evidence in included Cochrane systematic reviews -
pharmacological interventions - see Table 7
The same issues regarding the strengths and weaknesses of the
evidence in non-Cochrane reviews apply. However, as these reviews
did not use the Cochrane domain based risk of bias tool we were
unable to assess the overall quality of contributing studies. The
quality of evidence in the three non-Cochrane review are set out
in additional tables:
Quality of evidence in included Non-Cochrane systematic reviews
- non-pharmacological interventions - see Table 8.
Quality of evidence in included Non-Cochrane systematic reviews
- pharmacological interventions - see Table 9
Methodological quality of included reviews
The methods used in Cochrane reviews were assessed using the
AMSTAR rating scale described above. As all Cochrane reviews
followed a generic protocol specifying methods, scores were high
for all reviews. The Cochrane Handbook for Systematic Reviews ofInterventions specifies that the search should be comprehensive;
data extraction should be carried out independently by two peo-
ple; methods for data synthesis should be specified; reasons for
excluding studies and characteristics of those included should be
described; the quality of included studies should be assessed; and
data should be analysed and findings reported appropriately. These
are all factors which were adhered to in all contributing Cochrane
reviews and which contribute to achieving positive AMSTAR rat-
ings. In addition, all review protocols go through a peer review pro-
cess before publication when methodological quality is assessed.
So, it was not surprising that all these reviews received high-quality
ratings. For the non-Cochrane reviews scores were less high; this
was generally because some aspects of the review process may not
have been explicit in the published reviews. Findings regarding
the quality of contributing reviews are set out in three additional
tables.
AMSTAR ratings for each Cochrane systematic review - non-phar-
macological interventions - see Table 10
AMSTAR ratings for each Cochrane systematic review - pharma-
cological interventions - see Table 11
AMSTAR ratings for each Non-Cochrane systematic review - see
Table 12
Effect of interventions
For all interventions, where separate data were available, we have
set out the results under three major comparison groups:
1. Intervention versus placebo or standard care;
2. different forms of the same intervention (e.g. one opioid
versus another opioid); and,
3. one type of intervention versus a different type of
intervention (e.g. TENS versus opioid), see Figure 2.
14Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
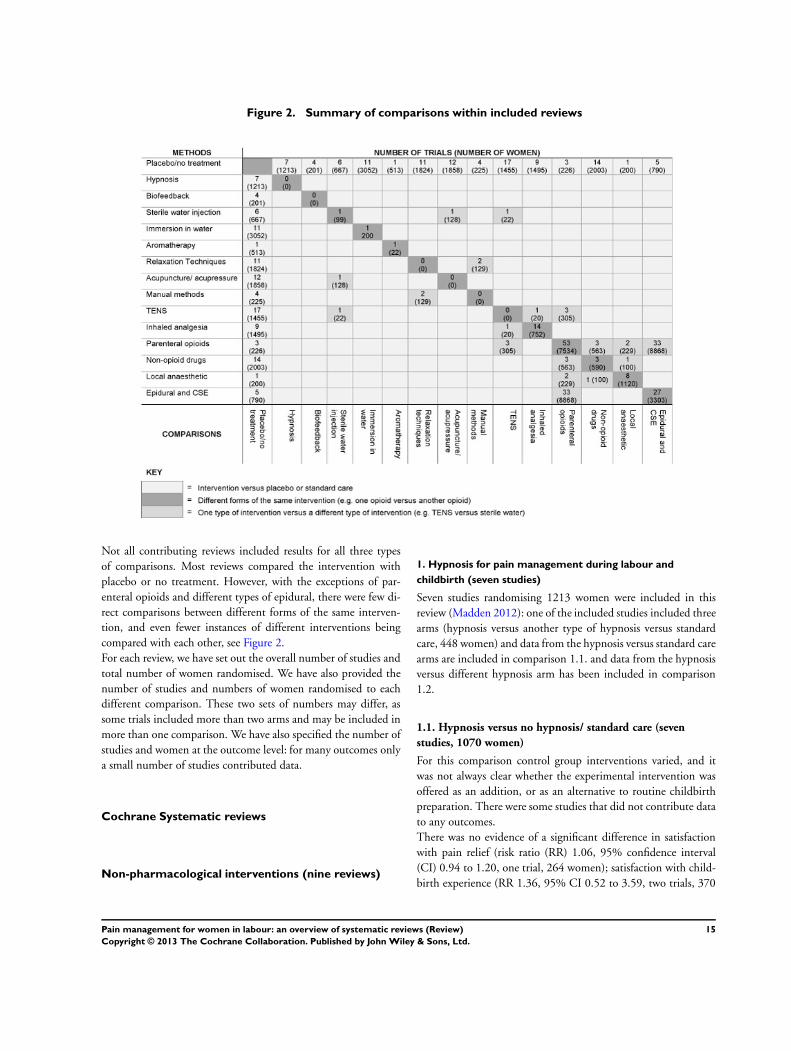
Figure 2. Summary of comparisons within included reviews
Not all contributing reviews included results for all three types
of comparisons. Most reviews compared the intervention with
placebo or no treatment. However, with the exceptions of par-
enteral opioids and different types of epidural, there were few di-
rect comparisons between different forms of the same interven-
tion, and even fewer instances of different interventions being
compared with each other, see Figure 2.
For each review, we have set out the overall number of studies and
total number of women randomised. We have also provided the
number of studies and numbers of women randomised to each
different comparison. These two sets of numbers may differ, as
some trials included more than two arms and may be included in
more than one comparison. We have also specified the number of
studies and women at the outcome level: for many outcomes only
a small number of studies contributed data.
Cochrane Systematic reviews
Non-pharmacological interventions (nine reviews)
1. Hypnosis for pain management during labour and
childbirth (seven studies)
Seven studies randomising 1213 women were included in this
review (Madden 2012): one of the included studies included three
arms (hypnosis versus another type of hypnosis versus standard
care, 448 women) and data from the hypnosis versus standard care
arms are included in comparison 1.1. and data from the hypnosis
versus different hypnosis arm has been included in comparison
1.2.
1.1. Hypnosis versus no hypnosis/ standard care (seven
studies, 1070 women)
For this comparison control group interventions varied, and it
was not always clear whether the experimental intervention was
offered as an addition, or as an alternative to routine childbirth
preparation. There were some studies that did not contribute data
to any outcomes.
There was no evidence of a significant difference in satisfaction
with pain relief (risk ratio (RR) 1.06, 95% confidence interval
(CI) 0.94 to 1.20, one trial, 264 women); satisfaction with child-
birth experience (RR 1.36, 95% CI 0.52 to 3.59, two trials, 370
15Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

women); assisted vaginal birth (RR 0.73, 95% CI 0.36 to 1.50,
three trials, 414 women); caesarean section (RR 0.54, 95% CI
0.18 to 1.62, three trials, 867 women) or admission to neonatal
intensive care unit (RR 0.58, 95% CI 0.12 to 2.83, two trials, 345
women). There was no evidence of a significant difference for any
of the other outcomes analysed (breastfeeding; adverse effects for
women or infants; Apgar score less than seven at five minutes).
None of the following outcomes were analysed within the review:
sense of control in labour; effect on mother/baby interaction; poor
infant outcomes at long-term follow-up; or cost.
1.2. One type of hypnosis versus another type of hypnosis
(one study, 297 women)
When hypnosis administered by a hypnotherapist was compared
with hypnosis on an audio CD administered by a nurse without
training in hypnotherapy, there were no significant differences for
any of the outcomes analysed (satisfaction with pain relief; satis-
faction with childbirth experience; breastfeeding; assisted vaginal
birth; caesarean section; adverse effects for women and infants;
admission to neonatal intensive care unit; Apgar score less than
seven at five minutes).
None of the following outcomes were analysed within the review:
sense of control in labour; effect on mother/baby interaction; poor
infant outcomes at long-term follow-up; or cost.
1.3. Hypnosis versus a different intervention
No studies are included in this comparison.
See Table 13 for all results relating to hypnosis.
2. Biofeedback for pain management during labour (four
studies)
2.1. Biofeedback versus no biofeedback/ standard care (four
studies, 201 women)
Four studies randomising 201 women were included in this re-
view (Barragán 2011): the type of biofeedback and the childbirth
preparation received by women in control arms varied in these
studies . The data relating to pain intensity, satisfaction with pain
relief, sense of control in labour or Apgar score were not reported
in a format that could be included in any analysis.
There was no significant difference between groups comparing
biofeedback with control for assisted vaginal birth (average RR
0.75, 95% CI 0.18 to 3.10, two trials, 103 women (random effects;
heterogeneity: I2 = 80%, Tau2 = 0.86, Chi2 test for heterogeneity
P = 0.02) or caesarean section (RR 0.41, 95% CI 0.14 to 1.15,
two trials, 103 women).
None of the following outcomes were analysed within the review:
satisfaction with childbirth experience; effect on mother/baby in-
teraction; breastfeeding; adverse effects for women and infants;
admission to special care baby unit/neonatal intensive care unit;
poor infant outcomes at long-term follow-up; or cost.
2.2. One type of biofeedback versus a different type of
biofeedback
No studies examined this comparison.
2.1. Biofeedback versus a different intervention
No studies examined this comparison.
See Table 14 for all results on biofeedback.
3. Intracutaneous or subcutaneous sterile water injection for
pain management in labour (seven studies)
Seven studies randomising 766 women were included in this re-
view (Derry 2012): four studies compared intracutaneous sterile
water injections versus placebo (saline injections) (467 women);
two studies compared subcutaneous sterile water injection ver-
sus placebo (saline injection) (200 women); and one study com-
pared intracutaneous or subcutaneous sterile water injection ver-
sus placebo (saline injection) (99 women).
3.1. Intracutaneous or subcutaneous sterile water injection
versus placebo (blinded controls) for pain management in
labour (six studies, 667 women)
Pain intensity: Although pain intensity was reported in several of
the studies contributing data to this review, the review authors did
not consider that data were presented in a way that was suitable
for inclusion in meta-analysis, or that was clinically meaningful.
Therefore, in this overview we have not set out results for this out-
come. Pain intensity data were, however, reported in an included
non-Cochrane review focusing on sterile water injection described
below.
There was no evidence of a significant difference in assisted vaginal
births (RR 1.31, 95% CI 0.79 to 2.18, six trials, 666 women) or
caesarean section (RR 0.58, 95% CI 0.33 to 1.02, seven trials, 766
women) between the sterile water and placebo groups.
None of the following outcomes were analysed within the review:
satisfaction with pain relief; sense of control in labour; satisfac-
tion with childbirth experience; effect on mother/baby interac-
tion; breastfeeding; adverse effects for women or infants; admis-
sion to neonatal intensive care unit; Apgar score less than seven
at five minutes; poor infant outcomes at long-term follow-up; or
cost.
3.2. Intracutaneous versus subcutaneous sterile water
injection (one study, 99 women)
Pain intensity: Although pain intensity was reported in the single
study examining this comparison, review authors considered that
16Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

data were either unsuitable for inclusion in meta-analysis, or were
not clinically meaningful. Therefore, in this overview we have not
set out results for this outcome.
3.3. Intracutaneous water versus a different intervention
One study compared TENS with sterile water injection and
one examined sterile water versus acupuncture (Dowswell 2009).
These studies have been discussed in the relevant sections below.
See Table 15 for all results relating to sterile water injections.
4. Immersion in water in labour and birth (12 studies)
Twelve studies randomising 3252 women were included in this
review (Cluett 2009). Altogether 11 studies compared immersion
versus no immersion (3052 women); eight compared immersion
versus no immersion in the first stage of labour (2766 women);
one study compared immersion versus no immersion in the sec-
ond stage of labour (120 women) and two studies compared im-
mersion versus no immersion in both the first and second stages
of labour (166 women). One study compared early (< 5 cm di-
lation) versus late (>= 5 cm dilation) immersion during the first
stage of labour (200 women). We have presented results separately
for those studies comparing immersion (early or late) versus no
immersion as opposed to the single study comparing immersion
at different stages during labour.
4.1 Immersion in water during the first or second stage of
labour versus no immersion in water/ standard care (11
studies, 3052 women)
Overall, there was little difference between groups for most of the
comparisons including: breastfeeding, assisted vaginal birth, cae-
sarean section, adverse effects for infants, admission to special care
baby unit and Apgar score less than seven at five minutes. The
only differences observed between groups were for pain intensity,
adverse effects for mothers, and satisfaction with childbirth expe-
rience. For all of these outcomes evidence was derived from single
studies.
Pain intensity: In a single trial (120 women) comparing immer-
sion versus no immersion in the first stage of labour significantly
fewer women in the immersion group reported their pain inten-
sity as being moderate to severe at 30 minutes after randomisation
on three different instruments measuring pain intensity (RR 0.75,
95% CI 0.62 to 0.91; RR 0.72, 95% CI 0.58 to 0.90; RR 0.67,
95% CI 0.51 to 0.90). At one hour and two hours after randomi-
sation fewer women in the immersion group reported moderate or
severe pain for two out of the three ordinal scales (one hour - RR
0.76, 95% CI 0.63 to 0.91; RR 0.68, 95% CI 0.53 to 0.86) (two
hours - RR 0.76, 95% CI 0.59 to 0.98; RR 0.72, 95% CI 0.52
to 0.98). There were no significant differences between groups at
three hours after randomisation on any of the three ordinal scales.
Adverse effects for women: In one trial that compared immersion
versus no immersion in the first stage of labour mean systolic,
diastolic and arterial blood pressures were significantly lower in
women in the immersion group, (mean difference (MD) -7.20,
95% CI -13.12 to -1.28; MD -10.20, 95% CI -13.70 to -6.70;
MD -10.50, 95% CI -14.68 to -6.32, 120 women).
Satisfaction with childbirth experience: Of the three trials that
compared water immersion during the second stage with no im-
mersion, one trial (117) showed that significantly fewer women
in the immersion group reported low satisfaction (reported as did
not cope with pushing efforts) with the childbirth experience (RR
0.24, 95% CI 0.07 to 0.80).
None of the following outcomes were analysed in the review: sat-
isfaction with pain relief; sense of control in labour; effect on
mother/baby interaction; poor infant outcomes at long-term fol-
low-up; or cost.
4.2. Immersion in water during early compared with later in
labour (one study 200 women)
Results were reported for two outcomes: adverse effects in infants
and Apgar scores at one minute; there was no significant difference
between groups for either of these outcomes. Results for other
outcomes were not reported.
4.3. Immersion in water versus a different intervention
No studies examined this comparison.
See Table 16 for all results relating to immersion in water.
5. Aromatherapy for pain management in labour (two
studies)
Two studies randomising 535 women were included in this review
(Smith 2011c): one study compared aromatherapy versus standard
care (513 women); and one study compared aromatherapy using
ginger versus aromatherapy using lemon grass (22 women). None
of the data relating to pain assessment were reported in a way that
allowed the review authors to include them in the analysis. In one
study, data were reported for only one arm of the trial and in the
other median values were presented.
5.1. Aromatherapy versus standard care (one study, 513
women)
There was no evidence of a significant difference between groups
comparing aromatherapy with standard care for assisted vaginal
birth or caesarean section (RR 1.04, 95% CI 0.48 to 2.28, and RR
0.98, 95% CI 0.49 to 1.94 respectively; one trial, 513 women).
There was also no evidence of a significant difference between
groups for admission to neonatal intensive care unit (NICU) (RR
0.08, 95% CI 0.00 to 1.42, one trial, 513 women).
17Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

5.2. Aromatherapy (ginger) versus aromatherapy (lemon
grass) (one study, 22 women)
There was no evidence of a significant difference between groups
comparing different types of aromatherapy for assisted vaginal
birth or caesarean section (RR 0.83, 95% CI 0.06 to 11.70, and
RR 2.54, 95% CI 0.11 to 56.25 respectively, one trial, 22 women).
No women in either group had a postpartum haemorrhage and
no babies were admitted to NICU (one trial, 22 women).
None of the following outcomes were analysed within the review:
satisfaction with pain relief; sense of control in labour; satisfac-
tion with childbirth experience; effect on mother/baby interac-
tion; breastfeeding; adverse effects for infants; Apgar score less than
seven at five minutes; poor infant outcomes at long-term follow-
up; or cost.
5.3. Aromatherapy versus a different intervention
No studies examined this comparison
See Table 17 for all results on aromatherapy.
6. Relaxation techniques for pain management in labour (11
studies)
6.1. Relaxation techniques versus standard care (11 studies)
Eleven studies involving 1574 women were included in this re-
view (Smith 2011b): six studies compared relaxation in the form
of progressive muscle relaxation, breathing or psycho-prophylaxis
versus standard care (1147 women); two studies compared yoga
versus standard care (270 women); two studies compared music
versus standard care (133 women); and one study compared au-
dio-analgesia versus standard care (24 women). There was consid-
erable variation in these studies in the way pain, pain relief and
satisfaction with the childbirth experience were measured.
Pain intensity: Five of the 11 included trials reported data on
pain intensity as continuous data. A significant difference was
observed between groups in studies comparing relaxation with
standard care in both the latent and active phases of labour (MD
-1.25, 95% CI -1.97 to -0.53, one trial, 40 women; MD -2.48,
95% CI -3.13 to -1.83, two trials, 74 women) and in one study
comparing yoga versus standard care in the latent phase of labour
(MD -6.12, 95% CI -11.77 to -0.47, one trial, 66 women), with a
reduction in pain intensity for the relaxation and yoga groups. No
evidence of a significant difference between groups was observed
for any of the other comparisons (music versus standard care;
audio-analgesia versus standard care). There was no evidence of
significant difference in memory of pain at three-month follow-
up for the one study examining this outcome (relaxation versus
standard care, one trial, 904 women).
Satisfaction with pain relief: Three of the 11 included trials re-
ported data on satisfaction with pain relief. Two trials reported this
as dichotomous data and one trial as continuous data. A signifi-
cant difference was observed between groups comparing relaxation
with standard care (RR 8.00, 95% CI 1.10 to 58.19, one trial, 40
women) and between groups comparing yoga with standard care
(MD 7.88, 95% CI 1.51 to 14.25, one trial, 66 women), with
significantly greater satisfaction reported for women in the relax-
ation and yoga groups. No significant difference was observed for
the other comparison (audio-analgesia versus standard care, one
trial, 24 women).
Satisfaction with childbirth experience: Two of the 11 included tri-
als reported data on satisfaction with childbirth experience. A sig-
nificant difference was observed between groups comparing yoga
with standard care (MD 6.34, 95% CI 0.26 to 12.42, one trial,
66 women), with greater satisfaction reported for women in the
yoga group. No evidence of a significant difference was observed
for the other comparison (relaxation versus standard care).
Assisted vaginal birth: Three out of the 11 included trials reported
data on assisted vaginal birth. A significant difference was observed
between groups comparing relaxation with standard care (RR 0.07,
95% CI 0.01 to 0.50, two trials, 86 women), with fewer women in
the relaxation group having assisted vaginal births. No evidence of
a significant difference was observed for a cluster trial comparing
relaxation with standard care (one trial, 904 women).
Caesarean section: Four out of the 11 included trials reported data
on caesarean section. The data could not be combined in a meta-
analysis for one of the comparisons because of significant hetero-
geneity (relaxation versus standard care, three trials [one cluster,
two parallel], 990 women). There was no evidence of a significant
difference for the other comparison (music versus standard care,
one trial, 60 women).
Apgar score less than seven at five minutes: Two out of the 11 in-
cluded trials reported on Apgar scores. There was no evidence of a
significant difference between relaxation versus standard care (one
trial, 34 women). In the yoga versus standard care comparison, no
babies in either group had an Apgar score less than seven at five
minutes.
None of the following outcomes were analysed within the review:
sense of control; effect on mother/baby interaction; breastfeeding;
adverse effects for women and infants; admission to special care
baby unit/neonatal intensive care unit; poor infant outcomes at
long-term follow-up; or cost.
6.2. Comparisons of different types of relaxation techniques
No studies compared different types of relaxation for pain man-
agement in labour.
6.3. Relaxation versus different interventions
No studies compared relaxation techniques with other types of
interventions to relieve pain in labour.
See Table 18 for all results on relaxation techniques.
18Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7. Acupuncture or acupressure for pain management in
labour (13 studies)
Thirteen studies with data on 1986 women were included in this
review (2391 women in total randomised) (Smith 2011a): eight
studies examined acupuncture and four acupressure; the control
conditions varied, with women in some studies receiving placebo
interventions and in others no intervention. Results for acupunc-
ture and acupressure and for different control conditions were set
out separately in the review. One study compared acupuncture ver-
sus sterile water injection (128 women) (results for this last study
comparing different types of interventions are set out in section
7.3 below).
7.1. Acupuncture or acupressure versus placebo treatments or
standard care (12 studies, 1858 women)
Pain intensity: The tools used to assess pain were not reported in
the review. Seven of the 12 included trials reported data on pain
intensity as continuous data. A significant difference was observed
between groups in a study comparing acupuncture with no treat-
ment (standardised mean difference (SMD) -1.00, 95% CI -1.33
to -0.67, one trial, 163 women) and in studies comparing acu-
pressure with placebo (SMD -0.55, 95% CI -0.92 to -0.19, one
trial, 120 women) and with a combined control (SMD -0.42, 95%
CI -0.65 to -0.18, two trials, 322 women). Women reported less
intense pain in both the acupuncture and acupressure groups for
these comparisons. However, this evidence was generally limited
to single studies. No evidence of a significant difference between
groups was observed for any of the other comparisons (acupunc-
ture versus placebo; acupuncture versus standard care).
Satisfaction with pain relief: The tools used to assess satisfaction
with pain relief were not reported in the review. Two of the 12
included trials reported data on satisfaction with pain relief. A sig-
nificant difference was observed between groups in the study com-
paring acupuncture with placebo; more women were satisfied with
pain relief in the acupuncture group when compared with placebo
(RR 2.38, 95% CI 1.78 to 3.19, one trial, 150 women). No evi-
dence of a significant difference was observed for the acupuncture
versus standard care comparison.
Assisted vaginal birth: Five of the 12 trials reported data on assisted
vaginal birth. A significant difference was observed between groups
in the studies comparing acupuncture with standard care (RR 0.67,
95% CI 0.46 to 0.98, three trials, 704 women), with significantly
fewer women in the acupuncture group having assisted vaginal
births. No evidence of a significant difference between groups was
observed for any of the other comparisons.
Caesarean section: Eight of the 12 trials reported data on caesarean
section. A significant difference was observed between groups in
the study comparing acupressure with placebo (RR 0.24, 95%
CI 0.11 to 0.54, one trial, 120 women), with significantly fewer
women in the acupressure group having caesarean section. There
was no evidence of a significant difference between groups for any
of the other comparisons.
Apgar score less than seven at five minutes: Five of the 12 trials
reported data on Apgar score less than seven at five minutes. There
was no evidence of a significant difference between groups in any
of the trials.
7.2. Comparisons of different types of acupuncture
No studies compared different types of acupuncture.
7.3. Acupuncture versus sterile water injection (one study,
128 women)
A significant difference in satisfaction with pain relief was observed
between groups in a trial comparing acupuncture with sterile water
injections with increased satisfaction reported in the sterile water
group (MD 18.60, 95% CI 11.54 to 25.66, one trial, 128 women).
There was no evidence of significant differences between groups
for assisted vaginal or caesarean birth. Other outcomes were not
reported.
None of the following outcomes were analysed within the review:
sense of control in labour; satisfaction with childbirth experience;
effect on mother/baby interaction; breastfeeding; adverse effects
for women and infants; admission to special care baby unit/NICU;
poor infant outcomes at long-term follow-up; and cost.
See Table 19 for all results on acupuncture or acupressure
8. Massage, reflexology and other manual methods for pain
management in labour (six studies)
Six trials were included in this review, with data reporting on five
trials and 326 women in the meta-analysis (401 women in total
randomised) (Smith 2012). Only studies examining massage were
identified. Control conditions varied. Four studies examined mas-
sage compared with usual care (225 women). One study exam-
ined massage compared with breathing exercises (28 women) and
one examined massage compared with music. These are reported
separately (101 women).
Overall, there was little difference between groups for most of the
comparisons examining satisfaction with pain relief, sense of con-
trol in labour, assisted vaginal birth, caesarean section or admission
to special care baby unit. The only difference observed between
groups was for pain intensity.
8.1. Massage versus standard care (four studies, 225 women)
In four trials comparing massage with usual care pain intensity
during the first stage of labour was reduced in the massage group
(SMD -0.82, 95% CI -1.17 to -0.47, 225 women). No evidence
of a significant difference between groups for pain intensity was
observed during the second or third stages of labour.
19Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

8.2. Comparisons of different manual methods
No studies compared different types of manual methods for pain
management in labour.
8.3. Massage versus a different intervention (relaxation/
music) (two studies 129 women)
In one trial comparing massage with music therapy the number of
women reporting severe pain was significantly lower in the massage
group (RR 0.40, 95% CI 0.18 to 0.89, 101 women). Data were
not in a suitable format for analysis in one trial comparing massage
with relaxation (28 women).
None of the following outcomes were analysed within the review:
satisfaction with childbirth experience; effect on mother/baby in-
teraction; breastfeeding; adverse effects for women and infants;
Apgar score less than seven at five minutes; poor infant outcomes
at long-term follow-up; or cost.
See Table 20 for all results relating to massage.
9. Transcutaneous electrical nerve stimulation (TENS) for
pain management in labour (17 studies)
Seventeen studies involving 1466 women were included in this
review (Dowswell 2009): thirteen studies examined TENS ap-
plied to the back; two to acupuncture points; and two to the cra-
nium. Fourteen studies compared TENS with placebo or usual
care (1256 women); three studies compared TENS as an adjunct
to epidural analgesia to epidural alone (200 women); and one
study compared TENS versus sterile water injection (23 women).
This study included three arms: TENS, usual care, sterile water.
Results for the TENS versus sterile water comparison are set out
separately.
Overall, there was little difference between groups for most of
the comparisons examining pain intensity, satisfaction with pain
relief or assisted vaginal birth. Any differences observed in these
outcomes were limited to one or two studies, as outlined below.
9.1. TENS (to back, cranium or acupuncture points) versus
placebo / standard care (17 studies, 1455 women)
Pain intensity: In two trials (290 women) comparing TENS to
acupuncture points versus placebo significantly fewer women in
the TENS group reported severe pain during labour compared
with controls (RR 0.41, 95% CI 0.31 to 0.54).
Satisfaction with pain relief: In one trial (90 women) comparing
TENS to acupuncture points versus control (no pain relief ), sig-
nificantly more women in the TENS group were satisfied with
pain relief (RR 4.10, 95% CI 1.81 to 9.29).
Assisted vaginal birth: In one trial (100 women) comparing TENS
to acupuncture points versus placebo, significantly more women
in the TENS group had assisted vaginal births (RR 4.50, 95% CI
1.02 to 19.79).
Other outcomes: There was no evidence of a significant difference
between groups for any of the outcomes relating to caesarean sec-
tion or adverse effects for the infant (fetal distress).
Data were not available in a suitable format for analysis for sense of
control in labour, satisfaction with childbirth experience or Apgar
score (for the last, all data were provided as means).
9.2. Different types of TENS
No studies compared different types of TENS (e.g. TENS to dif-
ferent parts of the body or different intensities).
9.3. TENS versus sterile water injections (one study, 22
women)
Results from a single study comparing TENS with sterile water
injections reported on mean pain scores but results were difficult to
interpret. For other outcomes reported, there were no significant
differences between groups.
None of the following outcomes were analysed within the review:
effect on mother/baby interaction; breastfeeding; adverse effects
for women; admission to NICU or special care baby unit (SCBU);
poor infant outcomes at long-term follow-up; or cost.
See Table 21 for all results on TENS.
Pharmacological interventions (six reviews)
1. Inhaled analgesia for pain management in labour (26
studies)
Twenty-six studies randomising 2967 women were included in
this review (Klomp 2012). The review presented data for five dif-
ferent comparisons; here we have summarised results under three
headings: inhaled analgesia versus placebo/no treatment; versus
another (different) inhaled analgesia and versus different methods
of pain relief.
1.1. Inhaled analgesia versus placebo (oxygen or compressed
air or no treatment) (nine studies, 1495 women)
In the studies comparing inhaled analgesia with placebo or no
treatment, nitrous oxide was found to offer better pain relief (aver-
age RR 0.06, 95% CI 0.01 to 0.34. two studies, 310 women; MD
-3.50, 95% CI -3.75 to -3.25, one study, 509 women). However,
nitrous oxide was associated with more adverse effects for women
such as nausea, vomiting, dizziness and drowsiness (RR 9.05, 95%
CI 1.18 to 69.32, two studies, 619 women; RR 43.10, 95% CI
2.63 to 706.74, one study, 509 women; RR 113.98, 95% CI 7.09
to 1833.69, one study, 509 women; RR 77.59, 95% CI 4.80 to
1254.96, one study, 509 women) when compared with placebo
or no treatment.
20Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

1.2. Inhaled analgesia versus different inhaled analgesia
(different drugs, strength or delivery system)
1.2.1. Inhaled analgesia versus a different type of inhaled
analgesia (nitrous oxide versus flurane derivatives, 14 studies,
752 women)
In the studies comparing different types of inhaled analgesia, mean
pain scores were lower with flurane derivatives and women receiv-
ing flurane derivatives were more likely to have improved pain
relief scores compared with nitrous oxide (average pain score MD
13.87, 95% CI 4.02 to 23.72, three studies, 123 women; pain
relief score MD -16.92, 95% CI -27.64 to -6.20, two studies, 140
women). Substantial heterogeneity was found in the analyses of
pain intensity.
Compared with nitrous oxide, flurane derivatives were associated
with less maternal nausea and vomiting (RR 3.30, 95% CI 1.64 to
6.63, six studies, 378 women; RR 2.66, 95% CI 1.06 to 6.70, four
studies, 261 women), but more drowsiness (MD -12.97, 95% CI
-22.33 to -3.62, two studies, 57 women).
1.2.2 Inhaled analgesia of one strength versus a different
strength (50% nitrous oxide versus 70% nitrous oxide, two
studies, 625 women)
There were no significant differences found for any of the out-
comes in the studies comparing one strength versus a different
strength of inhaled analgesia.
1.2.3. Inhaled analgesia using one type of delivery system
versus a different system (nitrous oxide with or without nasal
supplement, methoxyflurane using Penthrane® analgizer
versus Cyprane® inhaler, two studies, 75 women)
There were no significant differences found for any of the out-
comes in the studies comparing different delivery systems.
1.3. Inhaled analgesia versus different method of pain relief
1.3.1 Inhaled analgesia (nitrous oxide) versus TENS (one
study, 20 women)
There were no significant differences found for any of the out-
comes in the study comparing inhaled analgesia with TENS.
None of the following outcomes were analysed within the review:
sense of control; satisfaction with childbirth experience; effect on
mother/baby interaction; breastfeeding; admission to special care
baby unit; poor infant outcomes at long-term follow-up; or cost.
See Table 22 for all results relating to inhaled analgesia.
2. Parenteral opioids for maternal pain management in
labour (57 studies)
Fifty-seven studies involving over 7000 women were included in
this large review (Ullman 2010). We have presented results for
three main comparisons: first parenteral opioids versus placebo or
no treatment; second, comparisons between different opioids; and
third, comparisons between parenteral opioids and other meth-
ods of pain management in labour. In view of the complexity of
this review, within each main comparison we have included sub-
sections, and results for intramuscular (IM) and intravenous (IV)
drug administration are set out separately.
Pain intensity was reported in a variety of ways and at different
time points across trials. Twenty-eight of the 57 included trials
reported data on pain intensity. A total of twenty-three compar-
isons included data on pain intensity and significant findings were
observed in five comparisons.
Satisfaction with pain relief was reported in a variety of ways and
at different time points across trials. Only 12 of the 57 included
trials reported data on satisfaction with pain relief. A total of nine
comparisons included data on satisfaction with pain relief and
significant findings were observed in two comparisons.
Satisfaction with childbirth experience was reported in only one
of the 57 included trials.
Breastfeeding was reported in only two of the 57 included trials.
Definitions of breastfeeding were not provided.
2.1. Parenteral opioids versus placebo or no treatment (three
studies, 226 women)
2.1.1. IM opioids versus placebo or not treatment (three
studies, 226 women)
Only two studies comparing an IM opioid (pethidine) with
placebo were included in the review (166 women). In a single study
(50 women) more women in the IM pethidine group had a reduc-
tion in pain score (defined as a reduction in visual analogue scale
score of at least 40 mm) compared with the placebo group (RR
25.00, 95% CI 1.56 to 400.54, one study, 50 women). For other
outcomes (maternal satisfaction with pain relief, assisted vaginal
birth, caesarean section, nausea and vomiting, adverse effects on
the baby, and admission to NICU) there was no clear evidence of
differences between groups. A single study (116 women) reported
that women receiving pethidine were more likely to report sleepi-
ness compared with controls (RR 4.67, 95% CI 2.43 to 8.95).
Other outcomes were not reported in either of these two studies
(satisfaction with childbirth experience, breastfeeding, Apgar score
less than seven at five minutes, sense of control in labour, effect
21Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

on mother/baby interaction, poor long-term outcomes in babies
and cost).
One study (60 women) compared IM tramadol versus no treat-
ment. This study reported on only one of the overview’s outcomes:
adverse effects in women (blood loss at delivery). There was no
significant evidence of any difference between groups.
2.1.2. IV opioids versus placebo (no studies)
None of the studies examining IV opioids (including opioids ad-
ministered through PCA systems) were compared with placebo or
no treatment.
2.2. Comparisons of different opioids
2.2.1. IM opioids versus different IM opioids (15 different
comparisons, 36 studies)
A broad range of comparisons was examined, with many com-
parisons confined to evidence from single studies. Studies were
carried out over several decades and in several different countries
and comparisons included IM pethidine versus meptazinol, di-
amorphine, tramadol, dihydrocodeine, pentazocine, nalbuphine
or morphine.
Pain intensity: This outcome was reported for 13 comparisons ex-
amining one type of IM opioid versus another: for 12 comparisons
(predominantly measured in single studies comparing pethidine
with another opioid) there was no significant evidence of differ-
ences between groups. Only one comparison (IM tramadol versus
IM pethidine) examined in four studies (243 women) reported a
statistically significant difference between groups. More women
reported “poor pain relief ” in the IM tramadol group compared
with the IM pethidine groups (RR 1.56, 95% CI 1.10 to 2.21).
See Table 23 for all results relating to pain intensity.
Satisfaction with pain relief: This outcome was reported for three
comparisons.Pooled results for three studies (365 women) exam-
ining IM pentazocine versus IM pethidine found no significant
difference between groups. A single study (10 women) comparing
PCA (IM) meptazinol and PCA (IM) pethidine also reported no
significant difference between groups. In one study fewer women
receiving IM nalbuphine group were dissatisfied with pain relief
compared with those receiving IM pethidine (RR 0.73, 95% CI
0.55 to 0.96, one study, 72 women).
See Table 23 for all results relating to satisfaction with pain relief.
Satisfaction with the childbirth experience: this outcome was not
reported in any of the studies included in this comparison. (Table
23)
Breastfeeding: This outcome was reported for only one study:
there was no evidence of a significant difference between groups
receiving IM meptazinol versus IM pethidine (RR 0.76, 95% CI
0.17 to 3.30, one study, 197 women).
See Table 23 for results relating to breastfeeding.
Assisted vaginal delivery: This outcome was reported for six differ-
ent comparisons (11 studies); there were no significant differences
between groups for any of the comparisons (Table 23).
Caesarean section (CS): The number of women undergoing CS
was reported for five different comparisons (9 studies); there were
no significant differences for any of the comparisons. (Table 23).
Adverse effects: a range of adverse effects was reported, including
nausea, vomiting and sleepiness. Measurement of these outcomes
varied between studies (some studies reported nausea and vomiting
as separate outcomes and some as a combined outcome). The time
at which they were measured also varied considerably, which makes
results difficult to summarise and interpret. Overall, in many of
these trials, women receiving pethidine were more likely to report
adverse effects (including nausea and drowsiness) compared with
women receiving other opioids.
Maternal drowsiness or sleepiness was reported for nine different
comparisons and for eight of these comparisons there were no sig-
nificant differences between women receiving different opioids.
In studies comparing IM tramadol versus pethidine (five studies,
409 women) fewer women in the tramadol group reported sleepi-
ness (RR 0.57, 95% CI 0.33 to 0.97), but there was variation
between the individual studies and substantial heterogeneity was
evident (I2=72%). Results for nausea were reported for six com-
parisons and there were significant differences between groups for
two comparisons: in three studies (391 women) comparing IM
pentazocine with IM pethidine, more women in the pethidine
group reported nausea (RR 0.46, 95% CI 0.24 to 0.90), and in
a single study (301 women) comparing nalbuphine with pethi-
dine, again pethidine was associated with increased rates of nau-
sea (RR 0.62, 95% CI 0.42 to 0.91). Vomiting was recorded for
seven comparisons and for four of these there were differences be-
tween groups; overall women were less likely to experience vom-
iting if they received meptazinol (three studies 1589 women), di-
amorphine (one study, 133 women), nalbuphine (one study, 301
women) and phenazocine (one study 212 women) compared to
groups receiving IM pethidine. In three comparisons, nausea and
vomiting were reported as a single effect: for two comparisons
there was no evidence of significant differences between groups; in
a single study (72 women) comparing nalbuphine and pethidine,
women receiving pethidine were more likely to report nausea and
vomiting. (Table 23)
Adverse effects in infants: a range of adverse effects was reported
including neonatal resuscitation, administration of naloxone, res-
piratory distress and neuro behavioural outcomes. Overall, these
outcomes were reported in single studies and results were mainly
non-significant. Naloxone administration was reported for five dif-
ferent comparisons and there was no significant evidence of dif-
ferences between groups receiving pethidine compared with other
opioids. Numbers requiring neonatal resuscitation were reported
for three comparisons: there was no evidence that infants whose
mothers received pethidine, rather than other opioids, were more
22Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

or less likely to need resuscitation. A single study reported mean
scores on a neurological scale at two to four hours post birth (72
babies) and reported lower mean score for babies whose mothers
had received nalbuphine. (Table 23). The number of babies ad-
mitted to special care was reported for four comparisons (mep-
tazinol, tramadol, diamorphine, nalbuphine, four single studies);
in all four cases the control arm received pethidine. There was no
evidence of any significant differences for any of the comparisons.
(Table 23) Similarly, in four comparisons where Apgar scores at
five minutes were examined there was no clear evidence of dif-
ferences between experimental and control groups (all of which
received pethidine). (Table 23)
Sense of control in labour, mother/baby interaction, poor infant
outcomes at long-term follow-up and cost were not reported for
any comparisons. (Table 23)
2.2.2. IV opioids versus different IV opioids (12
comparisons, 17 studies)
Intravenous opioids were compared with other IV opioids in 17
studies although many outcomes were either not reported at all or
were reported in single studies. The types of opioids compared in
studies included: IV pethidine versus IV fentanyl, butorphanol,
pentazocine, remifentanil or nalbuphine, and in some trials opi-
oids other than pethidine were compared with each other: e.g. fen-
tanyl versus alfentanil. In 10 of the studies (seven different com-
parisons) IVs were administered by staff; in
seven studies (five comparisons) IV drugs were administered
through patient-controlled (PCA) systems. In these comparisons,
the regimens (lockout times, size of bolus, rate of background in-
fusion) as well as drugs varied between trials. While we have com-
bined methods of IV administration in our summary (e.g. staff
or patient-controlled), where results suggest differences between
groups we have specified the mode of administration.
Pain intensity: Pain intensity was examined for seven compar-
isons (eight studies). In five comparisons examining different types
of opioid via PCA there was no evidence of differences between
groups. In a single study looking at staff-administered IV opioids,
the mean pain score in the IV fentanyl group was significantly
lower than in the IV pethidine group (MD -0.20, 95% CI -0.34
to -0.06, one study, 105 women). The mean pain relief score (high
score = better pain relief ) was significantly higher in the IV butor-
phanol group compared with the IV pethidine (MD 0.67, 95%
CI 0.25 to 1.09, one study, 80 women) and this finding was sup-
ported by data for mean pain scores one hour after drug admin-
istration which were significantly lower for women in the butor-
phanol group (MD -0.60, 95% CI -1.02 to -0.18, one study, 80
women).
See Table 24 for all results relating to pain intensity.
Satisfaction with pain relief: This outcome was poorly reported;
only four studies, each describing a different IV comparison pro-
vided data on women’s views of their pain relief. Three of the four
studies reported no significant differences between groups; in a
single study, fewer women in the morphine group were satisfied
with their pain relief compared with an IV pethidine group (RR
0.87, 95% CI 0.78 to 0.98, one study, 141 women, staff-admin-
istered).
See Table 24 for all results relating to satisfaction with pain relief.
Satisfaction with childbirth experience was reported in only one
of the 57 included trials. This study found no significant differ-
ence in satisfaction with childbirth experience between the PCA
remifentanil and PCA pethidine groups (RR 1.10, 95% CI 0.40
to 1.74, one study, 68 women). (Table 24)
Breastfeeding: Results for breastfeeding at hospital discharge were
reported in only one study. There was no evidence of a signifi-
cant difference between groups for PCA pentazocine versus PCA
pethidine (RR 1.00, 95% CI 0.85 to 1.17, one study, 23 women).
(Table 24)
Assisted vaginal birth: this outcome was reported for three differ-
ent comparisons. In all three, pethidine was compared with other
opioids, there was no evidence of differences between groups for
any of the comparisons. (Table 24)
Caesarean section: the number of women having CS was reported
in nine studies (eight comparisons, four with staff-administered
IV drug and four PCA). There was no significant evidence of
differences between groups for any of the comparisons. (Table 24)
Adverse effects for women including nausea and vomiting (re-
ported either separately or together) and sleepiness were recorded
for several comparisons: for most of these there were no clear dif-
ferences between women receiving different types of IV opioids.
Sleepiness was reported for three comparisons; there a difference
between groups for only one comparison. In one study with 105
participants, women receiving IV fentanyl were reported to be less
sedated than those receiving IV pethidine (RR 0.05, 95% CI 0.00
to 0.82). Nausea and vomiting were reported for five comparisons
and again most (4/5) did not find significant differences between
groups; in a single study (200 women) fewer women in the IV bu-
torphanol group experienced nausea and/or vomiting compared
with those in pethidine group (RR 0.04. 95% CI 0.00 to 0.67).
(Table 24)
Adverse effects for infants: The number of babies requiring nalox-
one or resuscitation was reported for four and two comparisons re-
spectively, and neuro-behavioural scores (at different time points)
were reported for four comparisons. None of these comparisons
showed significant differences between groups. (Table 24)
The number of babies admitted to special care was only reported
in one study (17 women) and there was no evidence of differences
between groups. While babies with Apgar scores less than seven at
five minutes was reported for five comparisons (six studies) again,
none showed statistically significant differences for babies whose
mothers had received different opioids.
None of the studies examining IV comparisons reported results
for mothers’ sense of control in labour, effect on mother-baby
interaction, poor infant outcomes at long-term follow-up or cost.
23Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2.3. Parenteral opioids versus different interventions
2.3.1. Parenteral opioids versus a different method of pain
management (TENS) (three comparisons, three studies, 305
women)
Three studies compared parenteral opioids with TENS; each ex-
amined a different comparison (IV pethidine, IM pethidine and
IM tramadol). For most outcomes there was very little evidence
available (data from none or only one of the studies) and there
were few statistically significant differences between trial arms.
Pain intensity was reported for two studies (290 women); there
was no clear evidence of any difference between groups receiving
TENS compared with opioids. Two studies (104 women) reported
satisfaction with pain relief and again there was no significant
difference between women in the TENS and opioid groups. There
was no evidence of differences between groups for assisted vaginal
birth or caesarean section (one study, 200 women).
Adverse effects were reported for two studies (290 women); women
in the opioid groups were more likely to report drowsiness or
nausea and vomiting compared with those in the TENS group,
although the 95% CIs were very broad for both outcomes (RR
8.96, 95% CI 1.13 to 71.07; RR 14.06, 95% CI 1.96 to 100.61
respectively). Fetal distress was reported in one study (200 women)
and there was no evidence of differences between groups. (Table
24)
Satisfaction with the childbirth experience, breastfeeding, admis-
sion to special care, Apgar score less than seven, sense of control
in labour, mother-baby interaction, poor infant outcomes at long-
term follow-up and cost were not reported in any of the three
studies.
2.3.2. Parenteral opioids versus a different method of pain
management (epidural)
Thirty-three studies compared epidural analgesia with IM or IV
opioids; findings from these comparisons are discussed below in the
section on epidural versus non-epidural or no analgesia in labour.
3. Non-opioid drugs for pain management in labour (18
studies)
Eighteen studies randomising 2733 women were included in this
review (Othman 2012). The non-opioid drugs included paraceta-
mol, the non-steroidal anti-inflammatory drugs (NSAIDs) (e.g. as-
pirin, ibuprofen), sedatives (e.g. barbiturates, phenothiazine, and
benzodiazepines), anti-spasmodics (e.g. hyoscine), and anti-his-
tamines (e.g. promethazine, hydroxyzine). There were three main
comparison groups: 14 studies compared non-opioid drugs with
placebo or no treatment (2003 women); three studies compared
one type of non-opioid drug with a different non-opioid drug or
different doses of the same drug (590 women); and three studies
compared non-opioid drugs with opioids (563 women). Three
studies had more than two study arms and so data from different
arms have been included in more than one comparison group.
Most outcomes were not reported for most of the comparisons.
Where outcomes were reported, there was little evidence of any
difference for most comparisons. Any differences observed were
mainly limited to one or two studies, as outlined below.
3.1. Non-opioid drugs versus placebo (14 studies, 2003
women)
Sedatives were found to offer better pain relief (MD -22.00, 95%
CI -35.86 to -8.14, one trial, 50 women), better satisfaction with
pain relief (RR 1.59, 95% CI 1.15 to 2.21, two trials, 204 women)
and better satisfaction with childbirth experience (RR 2.16, 95%
CI 1.34 to 3.47, one trial, 40 women) when compared with
placebo or no treatment. Anti-histamines were also found to offer
better satisfaction with pain relief (RR 1.80, 95% CI 1.16 to 2.79,
1 trial 223 women) when compared with placebo or no treatment.
There was no evidence of a significant difference for any of the
other comparisons.
3.2. Non-opioid drug versus a different type or dose of a non-
opioid drug (three studies 590 women)
Women receiving the anti-histamine hydroxyzine were more likely
to express satisfaction with pain relief than those receiving the anti-
histamine promethazine (RR 1.21, 95% CI 1.02 to 1.43, one trial,
289 women).There was no evidence of a significant difference for
any of the other comparisons reported.
3.3. Non-opioid drug versus a different type of intervention
(opioid) (three studies, 563 women)
Women receiving non-opioid drugs (NSAIDs or anti-histamines)
were less likely to be satisfied with pain relief when compared to
women having opioids (RR 0.50, 95% CI 0.27 to 0.94, one trial,
76 women; RR 0.73, 95% CI 0.54 to 0.98, one trial, 223 women).
None of the following outcomes were analysed within the review:
sense of control in labour; effect on mother/baby interaction; ad-
mission to special care baby unit/neonatal intensive care unit; poor
infant outcomes at long-term follow-up; or cost.
See Table 25 for all results relating to non-opioid drugs.
4. Local anaesthetic nerve block for pain management in
labour (12 studies)
Twelve studies randomising 1549 women were included in this
review (Novikova 2012). The review presented data for the fol-
lowing comparisons: local anaesthetic nerve block versus placebo
(one study, 200 women); local anaesthetic nerve block versus a dif-
ferent local anaesthetic agent for nerve block (eight studies, 1120
women); local anaesthetic nerve block versus a different interven-
tion (local anaesthetic nerve block versus opioids (two studies,
129 women); and local anaesthetic nerve block versus non-opioids
(one study, 100 women)).
For all comparisons results were either not reported or there were
24Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

no significant differences between groups except for the following
results derived from single studies:
4.1. Local anaesthetic nerve block versus placebo (one study,
200 women)
Women who received local anaesthetic nerve block were more
likely to be satisfied with pain relief compared with women who re-
ceived placebo (RR 32.31, 95% CI 10.60 to 98.54, one study, 198
women). However, mothers and infants of mothers who received
local anaesthetic nerve block were more likely to experience ad-
verse effects (mother - giddiness, sweating, tingling of lower limbs;
infant - bradycardia) compared with women who received placebo
(RR 29.00, 95% CI 1.75 to 479.61, one study, 200 women).
4.2. Local anaesthetic nerve block versus a different type of
local anaesthetic nerve block (eight studies, 1120 women)
In studies comparing one type of local anaesthetic nerve block
with a different type of local anaesthetic nerve block, there was
no evidence of a significant difference between groups for any
outcomes analysed (satisfaction with pain relief; assisted vaginal
birth; caesarean section; adverse effects for mother; Apgar score
less than seven at five minutes).
4.3. Local anaesthetic nerve block versus a different interven-
tion (opoid or non-opioid drugs) (three studies, 229 women)
Women who received local anaesthetic nerve block were more
likely to be satisfied with pain relief compared with women who
received intramuscular pethidine (RR 2.52, 95% CI 1.65 to 3.83,
one study, 109 women). There were no significant differences be-
tween local anaesthetic nerve blocks and opioids for assisted vagi-
nal birth or caesarean section (two studies, 129 women) or be-
tween local anaesthetic nerve blocks and non-opioids for satisfac-
tion with pain relief or caesarean section (one study, 100 women).
None of the following outcomes were analysed within the review:
pain intensity; sense of control; satisfaction with childbirth expe-
rience; effect on mother/baby interaction; breastfeeding; admis-
sion to special care baby unit; poor infant outcomes at long-term
follow-up; or cost.
See Table 26 for all results relating to local anaesthetic nerve block.
5. Epidural versus non-epidural or no analgesia in labour (38
studies)
Thirty-eight studies randomising 9658 women were included in
this review (Anim-Somuah 2011). The majority of studies, (33
studies), compared epidural analgesia with IM or IV opioids. In
five of the included studies epidural was compared to no analgesia
during labour.
In this section of the overview we were not able to present separate
results for epidural versus no intervention/placebo and epidural
versus an alternative method of pain management. This is because,
in the original review there was no separate analysis for these dif-
ferent comparisons. Similarly, while most of the women in control
groups received IM or IV opioid drugs, there was considerable
variation in the agents, doses and modes of administration. How-
ever, in the original review results for these different comparisons
were analysed together, therefore we have not specified control
conditions in the results described below.
Results relating to comparisons between different types of epidu-
ral (combined spinal-epidural versus epidural analgesia) were the
subject of a different review, and are described in a separate section
below.
5.1. Epidural versus non-epidural or no analgesia in labour
(38 studies)
Epidural was found to offer better pain relief (MD -3.36, 95%
CI -5.41 to -1.31, three trials, 1166 women), a reduced risk of
acidosis in the newborn (RR 0.80, 95% CI 0.68 to 0.94, seven tri-
als, 3643 women) and a reduced risk of naloxone administration
in the newborn (RR 0.15, 95% CI 0.10 to 0.23, 10 trials, 2645
women) compared with controls. However, epidural analgesia was
associated with an increased risk of assisted vaginal birth (RR 1.42,
95% CI 1.28 to 1.57, 23 trials, 7935 women), maternal hypoten-
sion (RR 18.23, 95% CI 5.09 to 65.35, eight trials, 2789 women),
motor-blockade (RR 31.67, 95% CI 4.33 to 231.51, three trials,
322 women), maternal fever (RR 3.34, 95% CI 2.63 to 4.23, six
trials, 2741 women), urinary retention (RR 17.05, 95% CI 4.82
to 60.39, three trials, 283 women). There was an increased risk of
caesarean section for fetal distress (RR 1.43, 95% CI 1.03 to 1.97,
11 trials, 4816 women). There was no evidence of a significant
difference in the risk of caesarean section overall (RR 1.10, 95%
CI 0.97 to 1.25, 27 trials, 8417 women), long-term back ache
(RR 0.96, 95% CI 0.86 to 1.07, three trials, 1806 women), Apgar
score less than seven at five minutes (RR 0.80, 95% CI 0.54 to
1.20, 18 trials, 6898 women) and maternal satisfaction with pain
relief (RR 1.31, 95% CI 0.84 to 2.05, seven trials, 2929 women).
Substantial heterogeneity was found in the analyses of pain in-
tensity and maternal satisfaction. This could not be explained by
subgroup or sensitivity analyses.
None of the following outcomes were analysed within the review:
effect on mother/baby interaction; breastfeeding; poor infant out-
comes at long-term follow-up; or cost.
See Table 27 for all results on epidural.
6. Combined spinal-epidural versus epidural analgesia in
labour (27 studies)
Twenty-seven studies involving 3303 women were included in this
review (Simmons 2012). There was considerable heterogeneity be-
tween trials with respect to the drug combinations administered,
both intrathecally and epidurally, the timing of subsequent dosing
after initial analgesia and the method of epidural drug delivery. In
the context of categorising the epidural drug dose/concentration
used, the term traditional was used for trials where the epidural
local anaesthetic (LA) concentration was the equivalent of bupiva-
caine 0.25% or more; lower concentrations were defined as low-
25Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

dose. In the CSE groups, there were three types of interventions;
LA plus opioid, opioid alone, or null CSE where there was a dural
puncture with no intrathecal injection of drugs. Using these defi-
nitions the comparisons fell into six categories as detailed below:
1. LA plus opioid CSE versus traditional epidural;
2. LA plus opioid CSE versus low-dose epidural;
3. opioid only CSE versus traditional epidural;
4. opioid only CSE versus low-dose epidural;
5. opioid only CSE versus test LA/opioid epidural;
6. null CSE versus traditional epidural.
Analyses were performed on two separate sets of comparisons.
The first set involved all combined spinal-epidural (CSE) variants
versus traditional epidurals and the second set was all CSE forms
versus low-dose epidurals and variants.
In comparison with traditional epidurals, the mean time of on-
set of effective analgesia was slightly shorter for CSE by approx-
imately three minutes (MD -2.87, 95% CI -5.07 to -0.67, two
studies, 129 women) and there were fewer assisted vaginal births
(RR 0.80, 95% CI 0.67 to 0.97, six studies, 1015 women) and
less urinary retention (RR 0.86, 95% CI 0.79 to 0.95, one study,
704 women) in women in the CSE group. In comparison with
low-dose epidural, again the mean time of onset of effective anal-
gesia was shorter for the CSE group by approximately five min-
utes (average MD -5.42, 95% CI -7.26 to -3.59, five studies, 461
women) and more women in the CSE group reported effective
pain relief at 10 minutes after the first injection (RR 1.94, 95%
CI 1.49 to 2.54, one study, 101 women). However, more women
in the CSE group reported pruritus compared with the low-dose
epidural group (average RR 1.80, 95% CI 1.22 to 2.65, 11 stud-
ies, 959 women). Time to onset of effective analgesia and pruri-
tus showed substantial heterogeneity. There was no evidence of a
significant difference between comparison groups for any of the
other outcomes analysed.
None of the following outcomes were analysed within the review:
satisfaction with pain relief; sense of control in labour; satisfac-
tion with childbirth experience; effect on mother/baby interac-
tion; breastfeeding; poor infant outcomes at long-term follow-up;
or cost.
See Table 28 for all results relating to combined spinal-epidural.
Non-Cochrane Systematic reviews
Non-pharmacological interventions (one review)
Sterile water injection, (eight studies)
Eight studies randomising 783 women were included in this re-
view (Hutton 2009). The review included randomised controlled
trials comparing intracutaneous or subcutaneous injections of ster-
ile water with a placebo (saline water) or with other non-pharma-
cological methods of pain relief such as TENS or acupuncture.
Five studies used intracutaneous sterile water injections and three
used subcutaneous sterile water injections. The control groups
consisted of: acupuncture (one study); TENS and usual care (one
study); and isotonic saline injections (six studies). There was over-
lap in terms of the studies included in this review and the Cochrane
reviews on intracutaneous sterile water injection, acupuncture and
TENS. However, this non-Cochrane review included additional
data on pain intensity and caesarean section, not analysed in the
sterile water Cochrane review, and has been included for this rea-
son.
In comparison with placebo or other intervention groups, there
was a significant reduction in VAS pain score in the sterile water
group at three different time-points: 10 to 30 minutes following
administration of the intervention (WMD -26.04 mm, 95% CI
-34.14 to -17.94, four studies, 289 women); at 45 to 60 minutes
(WMD -36.27 mm, 95% CI -50.80 to -21.74, five studies, 542
women); and at 90 to 120 minutes following administration of
the intervention (WMD -27.74 mm, 95% CI -39.03 to -16.45,
five studies, 488 women). However, substantial heterogeneity was
evident within each of these analyses of pain scores. All analyses of
pain score used random-effects. A significant reduction was also
observed in caesarean sections in a meta-analysis of all eight studies
comparing any sterile water injection with placebo (normal saline
injection) or with other non-pharmacological interventions such
as TENS or acupuncture (RR 0.51, 95% CI 0.30 to 0.87, I2=
0%).
None of the following outcomes were analysed within the review:
satisfaction with pain relief; sense of control in labour; satisfac-
tion with childbirth experience; effect on mother/baby interaction;
breastfeeding; assisted vaginal birth; adverse effects for mother and
baby; admission to special care baby unit; Apgar score less than
seven at five minutes; poor infant outcomes at long-term follow-
up; and cost.
See Table 29 for all results relating to sterile water injection.
Pharmacological interventions (two reviews)
Epidural ropivacaine versus bupivacaine, (23 studies)
Seven studies randomising 2074 women were included in this
review (Halpern 2003a). The review included randomised con-
trolled trials comparing epidural ropivacaine with epidural bupi-
vacaine. There was no evidence of any statistically significant dif-
ference between drugs in the incidence of any obstetric or neona-
tal outcomes assessed (pain intensity; satisfaction with pain relief;
assisted vaginal birth; caesarean section; hypotension; nausea or
vomiting; Apgar score less than seven at five minutes).
None of the following outcomes were reported within the review:
sense of control in labour; satisfaction with childbirth experience;
effect on mother/baby interaction; breastfeeding; admission to
special care baby unit; poor infant outcomes at long-term follow-
up; and cost.
See Table 30 for all results relating to ropivacaine versus bupiva-
caine.
26Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Intrathecal opioids, (24 studies)
Twenty-four studies randomising 3513 women were included in
this review (Mardirosoff 2002). The review included randomised
controlled trials comparing any analgesia using intrathecal opi-
oid with any non-intrathecal regimen. Three intrathecal opioids
were included (sufentanil, fentanyl, morphine), with or without
various doses of intrathecal or epidural bupivacaine. The controls
consisted of different doses of epidural or intrathecal bupivacaine,
epidural lidocaine, combinations of epidural bupivacaine and dif-
ferent doses of epidural sufentanil or fentanyl and intravenous
sufentanil.
A significant increase in the risk of fetal bradycardia was observed
for women in the intrathecal opioid group compared to the con-
trol group (RR 29.6, 95% 13.6 to 64.6, 11 studies, 855 women)
and for maternal pruritus in the intrathecal groups compared with
controls who had not received opioids (RR 29.6, 95% CI 13.6 to
64.6, 11 studies, 855 women). There was no evidence of a sig-
nificant difference for maternal pruritus when intrathecal opioids
were compared with IV or IM opioid controls (average RR 1.71,
95% CI 0.97 to 3.02). There was no evidence of any significant
differences between groups for any other outcomes examined (as-
sisted vaginal birth; caesarean section; fetal heart rate abnormali-
ties; Apgar score less than seven at five minutes).
None of the following outcomes were analysed within the review:
pain intensity; satisfaction with pain relief; sense of control in
labour; satisfaction with childbirth experience; effect on mother/
baby interaction; breastfeeding; poor infant outcomes at long-term
follow-up; and cost.
See Table 31 for all results relating to intrathecal opioids.
D I S C U S S I O N
Summary of main results
The 15 Cochrane systematic reviews included a total of 257 trials.
The non-Cochrane systematic reviews included a total of 55 tri-
als. Most of the comparisons within each individual review were
within treatment comparisons e.g. one type of inhaled analgesia
compared to a different type of inhaled analgesia. There was a
paucity of placebo controlled trials with less than half, 41% (105),
of all included studies comparing the intervention with placebo
or no treatment. Similarly, only 18% (47) of all included studies
compared an intervention with a different type of intervention
according to the hierarchy of interventions. Most of these studies
comparing one form of intervention with another were confined
to one review and examined epidural versus parenteral opioids. In
other reviews, head-to-head comparisons between different types
of interventions were rare, and results were largely derived from
a small number of studies (e.g. TENS versus sterile water, one
study; inhaled analgesia versus TENS, one study; opioids versus
TENS, three studies; non-opioids versus opioids, three studies; lo-
cal anaesthetic nerve blocks versus opioids, two studies; and local
anaesthetic nerve blocks versus non-opioids, one study) (Figure
2).
Based on the following comparisons:
1. intervention versus placebo or standard care;
2. different forms of the same intervention (e.g. one opioid
versus another opioid);
3. one type of intervention versus a different type of
intervention (e.g. TENS versus opioid).
We have categorised interventions into “ What works,” “What
may work”, and “Insufficient evidence to make a judgement”, as
outlined.
WHAT WORKS
There is considerable evidence to suggest that epidurals (including
combined spinal epidurals (CSE)), and more limited evidence to
suggest that inhaled analgesia are effective for managing pain in
labour, but these interventions are not without adverse effects.
Epidural
There was a reduction in mean pain scores for women in the epidu-
ral group when measured during the whole of labour (three studies,
1166 women) and during the first (four trials, 589 women) and
second stages of labour (three trials, 559 women) in comparison
with non-epidural (parenteral opioids) or no analgesia. However,
considerable heterogeneity was observed for these analyses. There
was no significant difference observed for any of the other effec-
tiveness outcomes examined (patient satisfaction with pain relief;
sense of control in labour; satisfaction with childbirth experience).
More women in the epidural group had assisted vaginal births (23
trials, 7935 women) and experienced adverse effects such as hy-
potension (eight trials, 2789 women), motor blockade (three tri-
als, 322 women), fever (six trials, 2741 women) or urinary reten-
tion (three trials, 283 women) in comparison with non-epidural
(parenteral opioids) or no analgesia. More women in the epidu-
ral group had caesarean sections for fetal distress (11 trials, 4816
women) in comparison with non-epidural (parenteral opioids) or
no analgesia, although there was no evidence of a significant dif-
ference between groups in the overall caesarean section rate (seven
trials, 8417 women). The risk of acidosis and the requirement for
naloxone was lower in infants in the epidural group compared
with the non-epidural group (seven trials, 3643 women; one trial,
2645 women). There was no evidence of a significant difference
between groups in admissions to special care baby unit (seven tri-
als, 3125 women) or Apgar scores (18 trials, 6898 women).
Combined spinal epidural (CSE)
In comparison to traditional epidural, the mean time of onset of
effective analgesia was slightly shorter for CSE by approximately
three minutes (two trials,129 women). In comparison to low-dose
epidural, again the mean time of onset of effective analgesia was
shorter for the CSE group by approximately five minutes (five
trials, 461 women). However, considerable heterogeneity was ob-
served for the CSE versus low dose comparison. More women in
27Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

the CSE group reported effective pain relief at 10 minutes after the
first injection in comparison with the low dose epidural (one trial,
101 women), but there was no significant difference observed be-
tween CSE and low dose epidural for satisfaction with pain relief
(seven trials, 520 women). Other effectiveness outcomes (sense of
control; satisfaction with childbirth experience) were not reported.
CSE was associated with fewer assisted vaginal births in compari-
son to traditional epidural (six trials, 1015 women), but there was
no evidence of a significant difference in assisted vaginal birth be-
tween CSE and low dose epidural (11 trials, 1612 women). There
was no evidence of a significant difference in Caesarean section
for any of the comparisons: CSE versus traditional epidural (six
trials, 1015 women); or CSE versus low dose epidural (15 tri-
als, 1960 women). No differences in adverse effects for women
were observed for the following comparisons: post dural puncture;
known dural tap; blood patch; nausea and vomiting; hypoten-
sion; headache; and sedation. In contrast, fewer women in the
CSE group experienced urinary retention compared with tradi-
tional epidural (one trial, 704 women), but more women in the
CSE group experienced pruritus in comparison with the low dose
epidural group (11 trials, 959 women). There was no evidence of
a significant difference in admissions to special care baby unit or
Apgar scores for any of the comparisons: CSE versus traditional
epidural; CSE versus low dose epidural .
Inhaled analgesia
In comparison with placebo, fewer women in the inhaled analgesia
group experienced severe or extreme pain during the first stage of
labour (two trials, 310 women) and the mean pain score in one
large study (one trial, 509 women) was lower. There was insuffi-
cient evidence on efficacy in the comparison of inhaled analgesia
with TENS, with non-significant findings for pain intensity (one
trial, 19 women). More women experienced vomiting (two stud-
ies, 619 women), nausea (one study, 509 women), dizziness (one
study, 509 women) and drowsiness (one study, 509 women) with
inhaled analgesia when compared to placebo. There were no data
on safety outcomes for the comparison of inhaled analgesia with
TENS.
WHAT MAY WORK
There is some evidence to suggest that immersion in water, relax-
ation, acupuncture, massage, local anaesthetic nerve blocks and
non-opioid drugs may assist in managing pain in labour. Few ad-
verse effects are reported. Evidence was mainly limited to individ-
ual trials.
Immersion
Individual trials comparing immersion in water during the first
stage of labour with no immersion or standard care suggested
a reduction in pain (one trial, 120 women) and an increase in
satisfaction with childbirth experience for those in the immersion
group during the second stage of labour (one trial, 117 women).
However, in other studies using different pain intensity measures
or measurement at different time-points, there was no evidence
of a significant difference between groups for pain intensity (one
trials, 141 women) and satisfaction with the childbirth experience
(one trial, 60 women). Mean blood pressure was lower during the
first stage of labour in women in the immersion group in one trial
(120 women), but there was no evidence of a significant difference
between groups for any other of the safety outcomes.
Relaxation
A reduction in pain (two trials, 74 women; one trial 66 women),
greater satisfaction with pain relief (one trial, 40 women; one trial
66 women) and childbirth (one trial, 66 women) were observed in
individual trials of relaxation methods (breathing, yoga) in com-
parison with standard care. However, for other comparisons of re-
laxation methods (music; audio-analgesia), there was no evidence
of a significant difference for these same outcomes. Fewer assisted
vaginal births were observed in two trials comparing relaxation
with standard care (two trials, 86 women), but no evidence of a
significant difference was observed in one cluster trial of the same
comparison (one trial, 904 women).
Acupuncture
A reduction in pain (one trial, 120 women) and greater satisfaction
with pain relief (one trial, 150 women) was observed in individual
trials of acupuncture or acupressure in comparison with no treat-
ment or placebo. In one trial comparing acupuncture with sterile
water injection, more women in the sterile water group were satis-
fied with their pain relief (one trial, 128 women). There was no ev-
idence of a significant difference for pain and satisfaction with pain
relief for other comparisons of acupuncture with placebo or stan-
dard care. Fewer assisted vaginal births (three trials, 704 women)
and caesarean sections (one trial, 120 women) were observed in
comparisons of acupuncture and acupressure with standard care
or placebo. In other comparisons of acupuncture or acupressure,
there was no evidence of a significant difference in assisted vaginal
births (one trial, 208 women; one trial 163 women; one trial, 222
women) or caesarean sections (three trials, 448 women; two trials,
506 women).
Massage
In four trials comparing massage with standard care, pain inten-
sity during the first stage of labour was reduced in the massage
group during the first stage of labour (four trials, 225 women).
No evidence of a significant difference between groups for pain
intensity was observed during the second (two trials, 124 women)
or third stages of labour (two trials, 122 women). In one trial
comparing massage with music therapy, the number of women
reporting severe pain was lower in the massage group (one trial,
101 women). There was no evidence of a significant difference in
assisted vaginal births (two trials, 105 women), caesarean sections
(two trials, 105 women) or admission to special care baby unit
(one trial, 44 women) in trials comparing massage with standard
care. There were no data on safety outcomes in trials comparing
massage with relaxation or music therapy.
Local anaesthetic nerve blocks
More women in the local anaesthetic nerve block group (PCB
1% lidocaine) were satisfied with pain relief (degree of pain relief
28Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

rated as excellent/complete) compared with the placebo group,
(one trial, 198 women). There were no data on pain intensity,
sense of control and satisfaction with the childbirth experience
for this comparison. Women who received local anaesthetic nerve
blocks were more likely to be satisfied with pain relief compared
with women who received intramuscular pethidine (one trial, 109
women), but there was no evidence of a significant difference be-
tween local anaesthetic nerve blocks and (IM promethazine) for
satisfaction with pain relief (one trial, 20 women). Local anaes-
thetic nerve blocks (using lidocaine) were associated with more
adverse effects for women and infants (women - sweating, giddi-
ness, tingling of lower limbs; infants - bradycardia; one trial, 200
women) in comparison with placebo. There was no evidence of
a significant difference in assisted vaginal births (two trials, 129
women) or caesarean sections (two trials, 129 women) between
local anaesthetic nerve blocks and opioids (IM pethidine or PCA
fentanyl).
Non-opioid drugs
There was insufficient evidence on the effectiveness and safety of
most non-opioid drugs. However, evidence from single trials sug-
gests that some drugs may work. Non-opioid drugs (sedatives)
were found to offer better pain relief (one trial, 50 women), better
satisfaction with pain relief (sedatives and anti-histamines: two tri-
als, 204 women; one trial, 223 women) and better satisfaction with
the childbirth experience (one trial, 40 women) when compared
with placebo. There was no evidence of a significant difference
for any of the other comparisons of non-opioids (anti-histamines)
for pain intensity and satisfaction with pain relief. Women having
non-opioid drugs (NSAIDs or anti-histamines) were less likely to
be satisfied with pain relief when compared with women having
opioids (one trial, 76 women).There was little data and no evi-
dence of a significant difference for any of the comparisons of non-
opioids for safety outcomes.
INSUFFICIENT EVIDENCE TO MAKE A JUDGEMENT
There is insufficient evidence to make a judgement on whether or
not hypnosis, biofeedback, sterile water injection, aromatherapy,
TENS, and parenteral opioids, are more effective than placebo or
other interventions for pain management in labour.
Hypnosis
There was no evidence of a significant difference between hypnosis
and either no hypnosis/standard care or a different type of hypnosis
for all effectiveness outcomes analysed (satisfaction with pain relief;
satisfaction with childbirth experience). There was no evidence of
a significant difference in: breastfeeding (one trial, 266 women);
assisted vaginal births (three trials, 414 women); caesarean sections
(three trials, 867 women); adverse effects for women and infants
(one trial, 305 women); admissions to the neonatal intensive care
unit (two trials, 345 women); or Apgar score less than seven at five
minutes (one trial, 305 women).
Biofeedback
There was no evidence of a significant difference between biofeed-
back and standard care for assisted vaginal birth (two trials, 103
women) or caesarean section (two trials, 103 women). No other
data on effectiveness or safety outcomes were reported.
Sterile water injection
In the sterile water versus placebo comparison, data were either
not in a suitable format for analysis (pain intensity) or were not
reported (satisfaction with pain relief; sense of control in labour;
satisfaction with childbirth experience). In the non-Cochrane re-
view, in comparison with placebo or other intervention groups,
there was a significant reduction in VAS pain score in the sterile
water group at three different time-points. However, substantial
heterogeneity was evident within each of these analyses of pain
score.
There was no evidence of a significant difference in assisted vaginal
births (six trials, 666 women) or caesarean section (seven trials,
766 women) between the sterile water and placebo groups. In
the non-Cochrane review, a significant reduction was observed in
Caesarean sections in the sterile water group. However, this review
included sterile water injection versus any comparison (placebo,
TENS, acupuncture) (eight trials, 828 women).
Aromatherapy
There were no data on any effectiveness outcomes. There was no
evidence of a significant difference between groups (aromatherapy
versus standard care) in assisted vaginal births, caesarean sections
or admission to special care baby unit (one trial, 513 women).
TENS
In two trials comparing TENS to acupuncture points with
placebo, fewer women in the TENS group reported severe pain
during labour (two trials, 290 women). No significant differences
were observed for pain in two other trials comparing TENS to the
back with placebo or usual care (two trials, 299 women). In one
trial comparing TENS to acupuncture points with standard care,
more women in the TENS group were satisfied with their pain
relief (one trial, 90 women) but in five trials comparing TENS to
the back with placebo or standard care, there was no difference
between groups for satisfaction with pain relief (five trials, 452
women). There were no significant differences observed between
groups for assisted vaginal births, caesarean sections or adverse ef-
fects for infants.
Parenteral opioids
More women in the IM pethidine group had a reduction in pain
score compared with the placebo group (one trial, 50 women).
In studies comparing parenteral opioids with a different inter-
vention, TENS, pain intensity was reported for two studies (290
women); there was no clear evidence of any difference between
groups receiving TENS compared with opioids. Two studies (104
women) reported satisfaction with pain relief, and again there was
no significant difference between women in the TENS and opioid
groups.
There was no clear evidence of differences between groups (par-
enteral opioids versus placebo) for other outcomes (assisted vaginal
birth, caesarean section, nausea and vomiting, adverse effects on
the baby, and admission to NICU). A single study (116 women)
29Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

reported that women receiving pethidine were more likely to re-
port sleepiness compared with controls. Other safety outcomes
were not reported.
In studies comparing parenteral opioids with TENS, there was no
evidence of differences between groups for assisted vaginal birth
or caesarean section (one trial, 200 women). Adverse effects were
reported for two studies (290 women); women in the opioid group
were more likely to report drowsiness or nausea and vomiting com-
pared with those in the TENS group although 95% CIs were very
broad for both outcomes. Fetal distress was reported in one study
(200 women) and there was no evidence of differences between
groups. Other safety outcomes were not reported.
Overall completeness and applicability ofevidence
The overview has included 18 reviews focusing on 15 different
methods of pain relief in labour and most reviews considered sev-
eral different comparisons. The overview has focused on methods
of pain management that are explicitly intended to relieve pain
and has not included more broadly based interventions.
There remain gaps in the research evidence and some of the evi-
dence presented in this overview has serious limitations. Most out-
come data included in meta-analyses is drawn from only one or
two trials within each of the reviews. There are exceptions to this,
for example in the epidural and combined spinal epidural reviews
a larger number of trials contribute data, but even within these
reviews the variability in the results in individual trials (and the
high heterogeneity) means that results may still be difficult to in-
terpret. Therefore, it may be difficult, under these circumstances,
to generalise findings to other settings.
Most reviews included comparisons with placebo or between dif-
ferent types of the same intervention. However, at the outset we
had hoped that we would be able to compare directly different
methods of pain relief in terms of efficacy and safety; this proved
problematic. Very few of the reviews included any direct compar-
isons with other interventions (Figure 2). Where different meth-
ods were compared (e.g. inhaled analgesia versus TENS), results
for particular outcomes were mainly confined to evidence from
single studies. Thus, with the exception of the comparisons be-
tween epidural versus parenteral opioids, we were not able to draw
any conclusions from direct comparisons regarding the relative ef-
fectiveness and drawbacks of different ways of managing pain in
labour.
We considered making indirect comparisons in order to address
questions concerning the relative performance of different meth-
ods of pain relief. This would have involved using statistical meth-
ods to examine different interventions, each compared with the
same comparator (e.g. placebo), but which had not been directly
compared with each other. However, such methods can only be
used meaningfully if the populations recruited to the trials, and
the way outcomes are measured, are broadly similar. Therefore, we
decided that indirect comparisons would not be appropriate, due
to differences between reviews in terms of contextual and other
factors. For example, women in trials of IM opiates were recruited
over a long period (some trials dating back to the 1930s) while
other methods of pain management have only been introduced
into obstetric and midwifery practice (and been studied in trials)
in the last twenty years. Improved hospital facilities, changes in
custom and practice (for example where women give birth and
whether or not they have support from partners or family) and
the options for pain relief available to women are likely to have
changed women’s expectations about pain relief and their expe-
rience of childbirth. The way pain has been measured has also
altered considerably. Few early trials used VASs or validated pain
scales, and in some older studies, women were not asked to rate
their pain at all. Comparing like with like in terms of populations
and outcomes did not seem possible. This meant that we were
not able to provide a simple answer to the question about which
methods are most effective, safe and acceptable to women.
Many of our prespecified outcomes were not reported in the con-
tributing studies/review. In Table 32 and Table 33 we have pro-
vided a summary of outcomes reported within each of the re-
views. Sense of control in labour and breastfeeding were very rarely
reported within included trials in individual reviews. Effect on
mother/baby interaction, poor infant outcomes at long-term fol-
low-up and cost were never reported. As these are all important
outcomes to women or to providers of healthcare services, it is
surprising that they do not receive more research attention.
The very many ways outcomes were defined and measured in trials
led to problems in interpreting findings. It was not always clear
which tool was used to measure pain or which component of the
McGill pain questionnaire (three components - visual analogue
scale, verbal response scale, present pain intensity scale). Some
trials just reported “pain scores” and presented data as mean scores.
The majority of studies used visual analogue scales, but it was
not always clear how the extremes of the scales were marked and
whether the line was subdivided in any way. Many trials only
presented results graphically or presented median and interquartile
range. Some studies measured pain and pain relief as dichotomous
outcomes; but again there was no consistency in the meaning of
the outcome: a score could mean no pain (or complete relief )
or manageable pain (some relief ). There was similar variation for
satisfaction with pain relief. Many trials also reported mean or
median values for Apgar score. Accordingly, a lot of data could not
be analysed according to our criteria.
It was sometimes difficult to interpret the outcome data within
reviews, as some reviews used different terminology to that spec-
ified within the generic protocol. This was probably due to the
variation of reporting of outcomes in the individual trials. For ex-
ample, in some trials, pain was reported as “memory of pain” ,
“degree of pain relief ”, “perception of pain relief ” and experience
of childbirth as “difficulty of labour.” This made it difficult to map
outcome data to outcomes from the core list.
30Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Interpreting findings from individual reviews and summarising
findings within this overview were complicated by the variation in
both the experimental and control conditions examined within re-
views. In this overview, interventions in individual studies have not
been described in detail; settings, exact content and the intensity
or dose of interventions may have varied; some interventions may
have required specialised staff (e.g. acupuncture) and the training
and skills of operators are likely to have varied over time and loca-
tions. Control conditions are frequently not described at all in tri-
als; understanding what the terms “routine care”, “standard care”
or “no intervention” mean in studies carried out over a period of
more than fifty years in countries across the globe is particularly
difficult. Within this overview we have not been able to provide
details of participants, interventions (and control conditions) in
individual trials and we have given only limited information about
the way outcomes were measured in studies and reviews; we would
therefore encourage readers to consult the individual reviews to
obtain more information on these important factors.
A further difficulty in interpreting evidence and applying findings
from the overview to clinical situations relates to gaps in the evi-
dence concerning co-interventions and to the general lack of con-
sistency and clear information about when in labour interventions
were implemented and outcomes measured. In practice, women
in labour may opt for more than one method of pain relief and
may use different interventions simultaneously (e.g. inhaled anal-
gesia and parenteral opioids) or consecutively (e.g. TENS and then
epidural). Single interventions may be only partially effective and
methods that may provide adequate relief during the early stages
of labour may not do so as labour progresses. Without evidence
about pain relief at different stages in labour it remains difficult to
make recommendations to women when pain intensity is likely to
vary considerably as labour progresses.
No subgroup analyses were conducted on the pre-specified sub-
groups (spontaneous labour versus induced labour; primiparous
versus multiparous; term versus preterm birth; continuous sup-
port in labour versus no continuous support). This was due to the
low number of studies contributing data within the meta-analyses
and also due to a lack of clear subgroup data provided within the
reviews e.g. no data on continuous support in labour was reported
upon within the reviews.
Quality of the evidence
All fifteen of the Cochrane systematic reviews used the domain-
based evaluation for assessments of risk of bias as outlined in Chap-
ter 8 of the Cochrane Handbook for Systematic Reviews of Inter-ventions (Higgins 2011). None of the included systematic reviews
used the GRADE approach to assess the quality of evidence across
studies for each important outcome. We have therefore based our
assessments of the quality on the assessments reported in the ’Risk
of bias’ tables in the included systematic reviews. The risk of bias
of included trials within the Cochrane reviews was variable, but
generally considered to be high.
The proportion of studies assessed as being at low risk of bias in
the non-pharmacological and pharmacological reviews are sum-
marised in Table 6, Table 7. A higher proportion of studies in the
non-pharmacological reviews were considered to be at low risk of
bias for the domains of sequence generation (54% versus 31%)
and allocation concealment (40% versus 27%). A higher propor-
tion of studies in the pharmacological reviews were considered to
be at low risk of bias for blinding of participants, personnel and
outcome assessors (38%, 38%, 25% versus 20%, 18%, 31%). As-
sessment of blinding was not always conducted for all three groups
e.g. some reviews just assessed blinding as a single entity e.g. aro-
matherapy review, combined spinal epidural review. A higher pro-
portion of studies in the pharmacological reviews were considered
to be at low risk of bias for selective outcome reporting and other
potential threats to validity (49%, 41% versus 26%, 39%). An
equivalent number of studies were assessed as low risk of bias for
the domain of incomplete outcome assessment.
All three non-Cochrane systematic reviews used the Jadad scale
(Jadad 1996) or a modified version to assess the methodological
quality of included studies. The Cochrane Collaboration advises
against the use of such scales: these are thought to be a poor way
of assessing risk of bias, as they omit important considerations
and are largely concerned with reporting rather than conduct. The
Jadad scale is based on assessment of three items: method of ran-
domisation; blinding; and withdrawals and dropouts. This scale
has a maximum of five points, with a score of five indicating the
best possible score. In the epidural ropivacaine versus bupivacaine
review (Halpern 2003a), 17 out of 23 studies (74%) were assessed
as being high quality (with a score of three or more). In the in-
trathecal opioids review (Mardirosoff 2002), the median quality
score of the 24 included studies was reported to be 3.5 (range 1 to
5). The sterile water injection review used an initial version of the
Jadad scale (Jadad 1996), which was based on eleven items. The
maximum possible score for this initial instrument is 13 points.
In the sterile water injection review (Hutton 2009), seven out of
eight studies (88%) were assessed as being high quality (with a
score of 10 or more).
The methods used in Cochrane reviews were assessed using the
AMSTAR rating scale described above. As all Cochrane reviews
followed a generic protocol specifying methods, scores were high
for all reviews. For the non-Cochrane reviews scores were less high;
this was generally because some aspects of the review process may
not have been explicit in the published reviews. Findings regarding
the quality of contributing reviews are set out in Table 10, Table
11, Table 12.
Potential biases in the overview process
We are aware that there was a risk of introducing bias at all stages
in the overview process. We took a number of steps to try to re-
31Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

duce this. For non-Cochrane reviews, evidence of using systematic
methods was part of our criteria for selecting reviews for inclu-
sion. For Cochrane reviews, all reviews used a protocol that aimed
to minimise bias. For the overview, two review authors indepen-
dently assessed eligibility for inclusion of reviews, and carried out
data extraction. Data checks were carried out by a third author.
One potential source of bias relates to us, being the authors of some
of the included Cochrane reviews. One advantage of this is that
we are well informed of the weaknesses and strengths on which
these reviews build. No ’Summary findings’ tables were produced
within individual reviews, which limits our ability to assess overall
quality of the evidence against each of our core outcomes.
There is also a risk of bias arising from the fact that not all of the
contributing reviews had been completed at the time of prepar-
ing the overview. Four of the 15 included Cochrane reviews were
in draft form; while all had been submitted for publication in
The Cochrane Library, they had not been revised after peer review,
or approved for publication. Therefore, the findings we have re-
ported in this overview for these four reviews (examining hypno-
sis (Madden 2012), inhaled analgesia (Klomp 2012), non-opioid
drugs (Othman 2012) and combined spinal epidural (Simmons
2012)) are based on the draft reviews submitted by the authors for
editorial consideration. We plan to check all results and make any
necessary corrections in the first update of the overview.
However, it is not possible to eliminate all risk of bias; evidence
synthesis is not an exact science and involves judgement. We would
encourage readers to consider all of the additional tables to assist
them in interpreting results.
Agreements and disagreements with otherstudies or reviews
Many of the non-Cochrane reviews that we excluded from this
overview focused on the same methods of pain management as
the included Cochrane reviews. For the reviews that included ran-
domised controlled trials, there was considerable overlap in the
studies contributing evidence, despite some differences in search
strategies and selection criteria. In view of this overlap, for our
primary outcomes, it is therefore not surprising that the overall
findings of included and excluded reviews were generally in agree-
ment.
Findings for hypnosis from the Cochrane review were inconclu-
sive. This is in line with an earlier review of non-pharmacolog-
ical interventions for pain relief in labour, Simkin 2004a, that
concluded, at that time, there was insufficient evidence to draw
conclusions about the effectiveness of hypnosis and findings. The
included Cochrane review focusing on sterile water injection sug-
gested that there was some limited evidence that this method of-
fers some relief from pain. A review by Fogarty 2008 concluded
that sterile water injection had a beneficial effect on pain and the
included non-Cochrane review Hutton 2009 concurs with this.
Immersion in water was the subject of several excluded reviews
(Benfield 2002; Huntley 2004; Simkin 2002; Simkin 2004a).
While Simkin 2002 suggests that immersion in water reduces
labour pain, the evidence was drawn from non-randomised stud-
ies. The overall conclusion of this and the other reviews was
that there were few differences between intervention and control
groups for most outcomes and for many outcomes there was in-
sufficient evidence from trials to draw any firm conclusions.
For relaxation techniques, massage and reflexology, again other
reviews agree that more evidence is needed (Huntley 2004; Simkin
2002; Simkin 2004a).
The value of acupuncture for pain relief in labour was examined
by Cho 2010, Lee 2004 and Smith 2009. The results of these
reviews are consistent with the findings in the included Cochrane
review; while evidence from single studies suggests that acupunc-
ture reduces pain scores and results in increased satisfaction with
pain relief compared with controls, overall the evidence is mixed,
and for many outcomes there is insufficient evidence to draw firm
conclusions. Cho 2010 also points to the mixed methodological
quality of trials examining this intervention and concludes that the
current evidence from trials does not support the use of acupunc-
ture in labour.
An early review carried out by Carroll 1997 concluded that the
evidence on TENS was weak. While the amount of evidence on
TENS has increased, the evidence remains inconclusive. Although
many women seem to like TENS, it is not clear whether it is an
effective means of relieving pain in labour.
The conclusion of the included Cochrane review on inhaled anal-
gesia is reflected in the findings of another review. Rosen 2002a
suggests that inhaled analgesia offers safe, reasonably effective pain
relief for many women. The review by Klomp 2012, included in
this overview, however, highlights some of the adverse effects (such
as nausea and drowsiness) associated with some types of inhaled
analgesia.
Drawing conclusions regarding the effectiveness and safety of par-
enteral opioids has been hampered by the large number of studies
examining different types, doses and methods of administration
of opioids. Despite the large number of studies focusing on this
widely used form of pain relief, very few studies compare the effects
and adverse effects of different drugs. A decade ago Bricker 2002
indicated the paucity of evidence regarding the relative effects and
the adverse effects of different opioids and called for more research
directly comparing the most frequently used drugs. Many of the
questions raised by that review remain unanswered.
A relatively large number of excluded reviews focused on the use
of epidurals. Again findings are broadly similar to those in this
overview. In earlier studies there was some concern that epidurals
increased the risk of interventions in labour; in particular there was
a suggestion that rates of CS were higher in women who received
epidurals. However, in some reviews at least part of the evidence on
labour interventions was drawn from observational studies rather
than trials (Lieberman 2002; Morton 1994; Thorp 1996; Zhang
1999). In the current overview, while there was no strong evidence
32Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

that, compared with controls, women receiving epidural analgesia
were at increased risk of CS overall, the rate of CS for fetal distress
was greater, as was assisted vaginal birth. While there is now good
evidence that epidural offers good pain relief, there is also evidence
that some women experience adverse effects, in addition to any
risks associated with instrumental birth. Other non-Cochrane re-
views shed more evidence on different types of epidural and dif-
ferent drug regimens (including PCEA) (e.g. Halpern 2009).
An outcome which was considered in very few trials or in included
reviews, was the cost of interventions to healthcare providers, in-
cluding both the direct costs of interventions and the costs of
treating adverse effects and complications in women associated
with different types of labour analgesia. Huang 2002 examined
the costs associated with epidural analgesia; overall however, we
found little evidence on this important process outcome.
A gap in the evidence in this overview relates to broader interven-
tions that may increase women’s comfort and sense of control in
labour, which in turn may increase women’s sense of well being,
their ability to maintain control, and which may mitigate the ex-
perience of pain. Hodnett 2002, in a review of factors which affect
women’s experience of giving birth and their satisfaction with their
labour and birth, pointed to several factors which are important to
women. These include the amount of support from caregivers, the
quality of women’s relationships with caregivers and their sense of
involvement in decision-making. Designing interventions which
operationalise these factors in clinical trials is challenging, but evi-
dence from surveys and qualitative research has demonstrated their
importance to women, and underlines the need for high qual-
ity obstetric and midwifery care, where women are consulted and
their views are respected.
Within the scope of this overview, we have been unable to eval-
uate the impact on pain in labour of broadly based interventions
such as continuity of caregiver, the value of childbirth prepara-
tion classes, mobility in labour and the impact of different types
of physical environment for the birth (including home birth) on
pain in labour. Other Cochrane reviews focus on these important
topics, (Hatem 2008; Hodnett 2007).
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Most methods of non-pharmacological pain management are non-
invasive and appear to be safe for the mother and baby, however
their effectiveness is unclear due to limited high quality evidence.
There is more evidence to support the efficacy of pharmacological
methods but these also have more known adverse effects. Thus,
epidural analgesia provides effective pain relief but at the cost of
increased medical intervention including increased incidence of
instrumental vaginal birth.
It remains important to tailor methods used to an individual
woman’s wishes, needs and individual circumstances (this may in-
clude judgements about anticipated duration of labour, condition
of the infant, or whether the labour is augmented).
Implications for research
A major challenge in compiling this overview, and the individual
systematic reviews on which it is based, has been the variation in
use of different outcome measures in different trials, particularly in
assessment of pain and in its relief. This has made it difficult to pool
results from otherwise similar studies, and to derive conclusions
from the totality of evidence.
Other important outcomes have simply not been assessed in tri-
als; thus, despite concerns for 30 years or more about the effects
of maternal opiate administration during labour on subsequent
neonatal behaviour and its influence on breastfeeding, only two
out of 57 trials of opiates reported breastfeeding as an outcome.
We therefore strongly recommend that the outcome measures,
agreed through wide consultation for this project, are used in future
trials of methods of pain management. Future trialists may, of
course, wish to supplement these core outcome measures with
additional topic-specific or trial-specific outcomes.
Further trials are needed particularly for non-pharmacological
methods of pain management. There were very few data for hyp-
nosis, biofeedback, sterile water injection, aromatherapy and mas-
sage with much < 1000 women recruited in total to all trials of
each method. For TENS, there were more trials and more women
recruited, but also uncertainty about its value. In the UK at least,
TENS is popular with women, very widely recommended by
midwives, but unsupported by the national guideline developer,
NICE. This discordance between the views of women, clinicians
and guidelines reflects the poor evidence base and the uncertainty
should be resolved by a definitive trial.
Pain management in labour is a very high priority for consumer
groups. Health funding agencies need to consider if their priorities
match with those of consumer groups.
A C K N O W L E D G E M E N T S
David Tovey for his contributions to the development of the
overview.
We thank the Editorial Staff of the Cochrane Pregnancy and Child-
birth group for their help in preparing the overview.
We thank Gill Gyte, PCG Consumer Group Co-ordinator, for her
help in writing the plain language summary for the overview.
NISCHR Cymru Children and Young People’s Research Network
supported Sue Jordan’s travel to attend a meeting of the authors
33Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
and members of the Cochrane Pregnancy and Childbirth Group
in Liverpool in 2010.
As part of the pre-publication editorial process, this overview has
been commented on by five peers (an editor and four referees who
are external to the editorial team), five members of the Pregnancy
and Childbirth Group’s international panel of consumers and a
statistical adviser.
The National Institute for Health Research (NIHR) is the largest
single funder of the Cochrane Pregnancy and Childbirth Group.
The views and opinions expressed therein are those of the authors
and do not necessarily reflect those of the NIHR, NHS or the
Department of Health.
R E F E R E N C E S
References to included reviews
Anim-Somuah M, Smyth RMD, Jones L. Epidural versus
non-epidural or no analgesia in labour. Cochrane Database
of Systematic Reviews 2011, Issue 12. [DOI: 10.1002/
14651858.CD000331.pub3]
Barragán Loayza IM, Solà I, Juandó Prats C. Biofeedback
for pain management during labour. Cochrane Database
of Systematic Reviews 2011, Issue 6. [DOI: 10.1002/
14651858.CD006168.pub2]
Cluett ER, Burns E. Immersion in water in labour and
birth. Cochrane Database of Systematic Reviews 2009, Issue
2. [DOI: 10.1002/14651858.CD000111.pub3]
Derry S, Straube S, Moore RA, Hancock H, Collins SL.
Intracutaneous or subcutaneous sterile water injection
compared with blinded controls for pain management in
labour. Cochrane Database of Systematic Reviews 2012, Issue
1. [DOI: 10.1002/14651858.CD009107.pub2]
Dowswell T, Bedwell C, Lavender T, Neilson JP.
Transcutaneous electrical nerve stimulation (TENS)
for pain relief in labour. Cochrane Database ofSystematic Reviews 2009, Issue 2. [DOI: 10.1002/
14651858.CD007214.pub2]
Halpern SH, Walsh V. Epidural ropivacaine versus
bupivacaine for labor: a meta-analysis. Anesthesia andAnalgesia 2003;96(5):1473.
Hutton EK, Kasperink M, Rutten M, Reitsma A, Wainman
B. Sterile water injection for labour pain: a systematic
review and meta-analysis of randomised controlled trials.
BJOG: an international journal of obstetrics and gynaecology
2009;116(9):1158–66.
Klomp T, van Poppel M, Lazet J, Di Nisio M. Inhaled
analgesia for pain management in labour. Cochrane
Database of Systematic Reviews in press.
Madden K, Middleton P, Cyna AM, Matthewson M.
Hypnosis for pain management during labour and
childbirth. Cochrane Database of Systematic Reviews in
press.
Mardirosoff C, Dumont L, Boulvain M, Tramer MR. Fetal
bradycardia due to intrathecal opioids for labour analgesia:
a systematic review. BJOG: an international journal ofobstetrics and gynaecology 2002;109(3):274–81.
Novikova N, Cluver C. Local anaesthetic nerve block
for pain management in labour. Cochrane Database of
Systematic Reviews in press.
Othman M, Jones L, Neilson JP. Non-opioid drugs for pain
management in labour. Cochrane Database of Systematic
Reviews in press.
Simmons SW, Cyna AM, Dennis AT, Hughes D. Combined
spinal-epidural versus epidural analgesia in labour.
Cochrane Database of Systematic Reviews in press.
Smith CA, Collins CT, Crowther CA, Levett KM.
Acupuncture or acupressure for pain management in labour.
Cochrane Database of Systematic Reviews 2011, Issue 7.
[DOI: 10.1002/14651858.CD009232]
Smith CA, Levett KM, Collins CT, Crowther CA.
Relaxation techniques for pain management in labour.
Cochrane Database of Systematic Reviews 2011, Issue 12.
[DOI: 10.1002/14651858.CD009514]
Smith CA, Collins CT, Crowther CA. Aromatherapy
for pain management in labour. Cochrane Databaseof Systematic Reviews 2011, Issue 7. [DOI: 10.1002/
14651858.CD009215]
Smith CA, Levett KM, Collins CT, Jones L. Massage,
reflexology and other manual methods for pain management
in labour. Cochrane Database of Systematic Reviews 2012,
Issue 2. [DOI: 10.1002/14651858.CD009290]
Ullman R, Smith LA, Burns E, Mori R, Dowswell T.
Parenteral opioids for maternal pain management in labour.
Cochrane Database of Systematic Reviews 2010, Issue 9.
[DOI: 10.1002/14651858.CD007396.pub2]
References to excluded reviews
Arnal D, Serrano ML, Corral EM, Garcia del Valle S.
Intravenous remifentanyl for labor analgesia [Remifentanilo
intravenoso para analgesia del trabajo del parto.]. Revista
Espanola de Anestesiologia y Reanimacion 2009;56(4):
34Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

222–31.
Aveline C, Bonnet F. The effects of peridural anesthesia
on duration of labor and mode of delivery [Influence de
l’anesthesie peridurale sur la duree et les modalites de
l’accouchement.]. Annales Francaises d’Anesthesie et de
Reanimation 2001;20(5):471–84.
Benfield RD. Hydrotherapy in labor. Journal of Nursing
Scholarship 2002;34(4):347–52.
Bricker L, Lavender T. Parenteral opioids for labor pain
relief: a systematic review. American Journal of Obstetricsand Gynecology 2002;186(5 Suppl Nature):S94–109.
Bucklin BA, Chestnut DH, Hawkins JL. Intrathecal opioids
versus epidural local anesthetics for labor analgesia: a meta-
analysis. Regional Anesthesia and Pain Medicine 2002;27(1):
23–30.
Capogna G, Camorcia M. Epidural analgesia for childbirth:
effects of newer techniques on neonatal outcome. Paediatric
Drugs 2004;6(6):375–86.
Carroll D, Moore RA, Tramer MR, McQuay HJ.
Transcutaneous electrical nerve stimulation does not relieve
labor pain: updated systematic review. Contemporary
Reviews in Obstetrics and Gynaecology 1997;9(3):195–205.
Carroll D, Tramer M, McQuay H, Nye B, Moore A.
Transcutaneous electrical nerve stimulation in labour
pain: a systematic review. British Journal of Obstetrics and
Gynaecology 1997;104(2):169–75.
Cho S-H, Lee H, Ernst E. Acupuncture for pain relief in
labour: a systematic review and meta-analysis. BJOG: aninternational journal of obstetrics and gynaecology 2010;117
(8):907–20.
Choi PT, Galinski SE, Takeuchi L, Lucas S, Tamayo C,
Jadad AR. PDPH is a common complication of neuraxial
blockade in parturients: a meta-analysis of obstetrical
studies. Canadian Journal of Anaesthesia 2003;50(5):460–9.
Cyna AM, McAuliffe GL, Andrew MI. Hypnosis for pain
relief in labour and childbirth: a systematic review. BritishJournal of Anaesthesia 2004;93(4):505–11.
Fogarty V. Intradermal sterile water injections for the relief
of low back pain in labour. A systematic review of the
literature. Women and Birth 2008;21(4):157–63.
Habib AS, Gan TJ. Use of neostigmine in the management
of acute postoperative pain and labour pain: a review. CNSDrugs 2006;20(10):821–39.
Hager A, Newton W. Comparing epidural and parenteral
opioid analgesia during labor. Journal of Family Practice
1999;48(3):174–5.
Halpern SH, Leighton BL, Ohlsson A, Barrett JFR, Rice
A. Effect of epidural vs parenteral opioid analgesia on the
progress of labor. A meta-analysis. JAMA 1998;280(24):
2105–10.
Halpern SH, Leighton BL. Misconceptions about neuraxial
analgesia. Anesthesiology Clinics of North America 2003;21
(1):59–70.
Halpern S. Low concentration epidural infusion increases
the risk of instrumental vaginal delivery, but not cesarean
delivery - meta-analysis. Evidence-Based Obstetrics and
Gynecology 2005;7(2):66–7.
Halpern S. Recent advances in patient-controlled epidural
analgesia for labour. Current Opinion in Anaesthesiology
2005;18(3):247–51.
Halpern SH, Carvalho B. Patient-controlled epidural
analgesia for labor. Anesthesia and Analgesia 2009;108(3):
921–8.
Hodnett ED. Pain and women’s satisfaction with the
experience of childbirth: a systematic review. American
Journal of Obstetrics and Gynecology 2002;186(5 Suppl
Nature):S160–72.
Huang C, Macario A. Economic considerations related
to providing adequate pain relief for women in labour:
comparison of epidural and intravenous analgesia.
PharmacoEconomics 2002;20(5):305–18.
Huntley AL, Coon JT, Ernst E. Complementary and
alternative medicine for labor pain: a systematic review.
American Journal of Obstetrics and Gynecology 2004;191(1):
36–44.
Koehn ML. Childbirth education outcomes: an integrative
review of the literature. Journal of Perinatal Education 2002;
11(3):10–9.
Kotaska AJ, Klein MC, Liston RM. Epidural analgesia
associated with low-dose oxytocin augmentation increases
cesarean births: a critical look at the external validity
of randomized trials. American Journal of Obstetrics andGynecology 2006;194(3):809–14.
Kuczkowski KM. Neurologic complication of labor
analgesia: facts and fiction. Obstetrical & Gynecological
Survey 2004;59(1):47–51.
Lally JE, Murtagh MJ, Macphail S, Thomson R. More in
hope than expectation: a systematic review of women’s
expectations and experience of pain relief in labour. BMC
Medicine 2008;6:7.
Larkin P, Begley CM, Devane D. Women’s experiences
of labour and birth: an evolutionary concept analysis.
Midwifery 2009;25(2):e49–e59.
Lee H, Ernst E. Acupuncture for labor pain management:
a systematic review. American Journal of Obstetrics and
Gynecology 2004;191(5):1573–9.
Lee H, Cho S-H, Ernst E. ’Meta-analysis of randomised
controlled trials (RCTs) involving acupuncture for
labour pain shows acupuncture to be more effective than
comparison treatments in analgesic consumption’ but
the overall evidence is still limited, calling for further
investigations: Authors’ reply. BJOG: an internationaljournal of obstetrics and gynaecology 2011;118(1):101–2.
Leeman L, Fontaine P, King V, Klein MC, Ratcliffe
S. The nature and management of labor pain: Part I.
Nonpharmacologic pain relief. American Family Physician2003;68(6):1109–12.
Leeman L, Fontaine P, King V, Klein MC, Ratcliffe S.
The nature and management of labor pain: Part II.
Pharmacologic pain relief. American Family Physician 2003;
68(6):1115–22.
Leighton BL, Halpern SH. The effects of epidural analgesia
on labor, maternal, and neonatal outcomes: a systematic
35Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

review. American Journal of Obstetrics and Gynecology 2002;
186(5 Suppl Nature):S69–77.
Leighton BL. The impact of neuraxial analgesia on the
progress and outcome of labor. Techniques in RegionalAnesthesia and Pain Management 2003;7(4):197–203.
Lieberman E, O’Donoghue C. Unintended effects of
epidural analgesia during labor: a systematic review.
American Journal of Obstetrics and Gynecology 2002;186(5
Suppl Nature):S31–S68.
Littleford J. Effects on the fetus and newborn of maternal
analgesia and anesthesia: a review. Canadian Journal of
Anaesthesia 2004;51(6):586–609.
Liu EHC, Sia ATH. Rates of caesarean section and
instrumental vaginal delivery in nulliparous women after
low concentration epidural infusions or opioid analgesia:
systematic review. BMJ 2004;328(7453):1410–2.
Lopard E. Patient-controlled epidural analgesia for labour:
in practice [L’analgesie peridurale obstetricale controlee par
la patiente: en pratique]. Annales Francaises d’Anesthesie et
de Reanimation 2006;25(6):593–8.
Marucci M, Cinnella G, Perchiazzi G, Brienza N, Fiore
T. Patient-requested neuraxial analgesia for labor: impact
on rates of cesarean and instrumental vaginal delivery.
Anesthesiology 2007;106(5):1035–45.
Mayberry LJ, Clemmens D, De A. Epidural analgesia
adverse effects, co-interventions, and care of women
during childbirth: a systematic review. American Journal
of Obstetrics and Gynecology 2002;186(5 Suppl Nature):
S81–S93.
Minty RG, Kelly L, Minty A, Hammett DC. Single-
dose intrathecal analgesia to control labour pain: is it a
useful alternative to epidural analgesia?. Canadian FamilyPhysician 2007;53(3):437–42.
Morton SC, Williams MS, Keeler EB, Gambone JC, Kahn
KL. Effect of epidural analgesia for labor on the cesarean
delivery rate. Obstetrics & Gynecology 1994;83(6):1045–52.
Nystedt A, Edvardsson D, Willman A. Epidural analgesia
for pain relief in labour and childbirth - a review with a
systematic approach. Journal of Clinical Nursing 2004;13
(4):455–66.
Reynolds F, Sharma SK, Seed PT. Analgesia in labour and
fetal acid-base balance: a meta-analysis comparing epidural
with systemic opioid analgesia. BJOG: an international
journal of obstetrics and gynaecology 2002;109(12):1344–53.
Reynolds F. The effects of maternal labour analgesia on
the fetus. Best Practice & Research. Clinical Obstetrics &Gynaecology 2010;24(3):289–302.
Rosen Mark A. Nitrous oxide for relief of labor pain:
a systematic review. American Journal of Obstetrics and
Gynecology 2002;186(5 Suppl Nature):S110–S126.
Rosen MA. Paracervical block for labor analgesia: a
brief historic review. American Journal of Obstetrics andGynecology 2002;186(5 Suppl Nature):S127–S130.
Sharma SK, Leveno KJ. Regional analgesia and progress
of labor. Clinical Obstetrics and Gynecology 2003;46(3):
633–45.
Sharma SK, McIntire DD, Wiley J, Leveno KJ. Labor
analgesia and cesarean delivery: an individual patient meta-
analysis of nulliparous women. Anesthesiology 2004;100(1):
142–8.
Shiflett SC, Schwartz GE. Meta-analysis of randomised
controlled trials (RCTs) involving acupuncture for
labour pain shows acupuncture to be more effective than
comparison treatments in several significant circumstances.
BJOG: an international journal of obstetrics and gynaecology2011;118(1):100–1.
Simkin PP, O’Hara MA. Nonpharmacologic relief of pain
during labor: systematic reviews of five methods. American
Journal of Obstetrics and Gynecology 2002;186(5 Suppl
Nature):S131–S159.
Simkin P, Bolding A. Update on nonpharmacologic
approaches to relieve labor pain and prevent suffering.
Journal of Midwifery & Women’s Health 2004;49(6):
489–504.
Sleth J-C. Paracervical block in obstetrics [Bloc paracervical
en obstetrique]. Annales Francaises d’Anesthesie et de
Reanimation 2006;25(11-12):1119–26.
Smith CA, Cochrane S. Does acupuncture have a place
as an adjunct treatment during pregnancy? A review of
randomized controlled trials and systematic reviews. Birth
2009;36(3):246–53.
Thavaneswaran P, Maddern G, Cooter R, Moyes D,
Rudkin G. Paravertebral blocks for anaesthesia and
analgesia: a systematic review. ASERNIP-S Report No.
47. Adelaide, South Australia: ASERNIP-S, January 2006.
Royal Australasian College of Surgeons, Australian Safety
and Efficacy Register of New Interventional Procedures
(ASERNIP) - Surgical (http://www.surgeons.org/media/
13814/Paravertebral˙Block˙Review˙March2006˙web.pdf)
(accessed 3 February 2011) 2006:263.
Thorp JA, Breedlove G. Epidural analgesia in labor: an
evaluation of risks and benefits. Birth 1996;23(2):63–83.
Van De Velde M. Neuraxial analgesia and fetal bradycardia.
Current Opinion in Anaesthesiology 2005;18(3):253–6.
Van de Velde M. Modern neuraxial labor analgesia: options
for initiation, maintenance and drug selection. Revista
Espanola de Anestesiologia y Reanimacion 2009;56(9):
546–61.
Van der Vyver M, Halpern S, Joseph G. Patient-controlled
epidural analgesia versus continuous infusion for labour
analgesia: a meta-analysis. British Journal of Anaesthesia2002;89(3):459–65.
Writer WDR, Stienstra R, Eddleston JM, Gatt SP, Griffin R,
Gutsche BB, et al.Neonatal outcome and mode of delivery
after epidural analgesia for labour with ropivacaine and
bupivacaine: A prospective meta-analysis. British Journal of
Anaesthesia 1998;81(5):713–7.
Wunsch MJ, Stanard V, Schnoll SH. Treatment of pain in
pregnancy. Clinical Journal of Pain 2003;19(3):148–55.
Zhang J, Klebanoff M A, DerSimonian R. Epidural
analgesia in association with duration of labor and mode
of delivery: a quantitative review. American Journal of
Obstetrics and Gynecology 1999;180(4):970–7.
Zhou J, Lin X-M, Luo L-L, Ma Y-S. Local versus systemic
36Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

application of opioids for labor analgesia: a systematic
review. Chinese Journal of Evidence-Based Medicine 2008;8
(8):652–61.
Additional references
Ader 1990
Ader L, Hansson B, Wallin G. Parturition pain treated by
intracutaneous injections of sterile water. Pain 1990;41:
133–8.
Ahlborg 1996
Ahlborg G Jr, Axelsson G, Bodin L. Shift work, nitrous
oxide exposure and subfertility among Swedish midwives.
International Journal of Epidemiology 1996;25(4):783–90.
Aird 1997
Aird IA, Luckas MJM, Buckett WM, Bousfield P. Effects
intrapartum hydrotherapy on labour parameters. Australianand New Zealand Journal of Obstetrics and Gynaecology
1997;37(2):137–42.
Allaire 2000
Allaire AD, Moos M, Wells SR. Complementary and
alternative medicine in pregnancy: a survey of North
Carolina nurse-midwives. Obstetrics & Gynecology 2000;95
(1):19–23.
AMA 1993
American Medical Association. Reader’s Guide to Alternative
Health Methods. Milwaukee, WI: American Medical
Association, 1993.
Anim-Somuah 2005
Anim-Somuah M, Smyth R, Howell C. Epidural versus
non-epidural or no analgesia in labour. Cochrane Databaseof Systematic Reviews 2005, Issue 4. [DOI: 10.1002/
14651858.CD000331.pub2]
August 1961
August RV. Hypnosis in Obstetrics. New York: McGraw-
Hill, 1961.
Axelsson 1996
Axelsson G, Ahlborg G Jr, Bodin L. Shift work, nitrous
oxide exposure, and spontaneous abortion among Swedish
midwives. Occupational and Environmental Medicine 1996;
53(6):374–8.
Bayarski 2006
Bayarski Y. Differences between opioid and non-opioid
analgesics. Ezine Articles (http://ezinearticles.com/
?Differences-Between-Opioid-and-Non-Opioid-
Anaglesics&id=266768) (accessed November 2010) 2006.
Begley 2009
Begley C, Devane D, Clarke M. An evaluation of midwifery-led care in the Health Service Executive North Eastern Area.
The report of the MidU study. Dublin: Trinity College,
University of Dublin, 2009.
Black 2009
Marcovitch H (editor). Black’s Medical Dictionary 42nd
edition. http://www.library.nhs.uk/default.aspx (accessed
21st April 2011).
BOC 2010
BOC Healthcare. BOC Medical Gas Data Sheet (MGDS)
entonox 50% nitrous oxide, 50% oxygen medicinal gas
mixture SPC. MGDS (www.bocsds.com/uk/sds/medical/
entonox.pdf) (accessed 30 January 2011) 2010.
Bodin 1999
Bodin L, Axelsson G, Ahlborg G Jr. The association of
shift work and nitrous oxide exposure in pregnancy with
birth weight and gestational age. Epidemiology 1999;10(4):
429–36.
Boivin 1997
Boivin JF. Risk of spontaneous abortion in women
occupationally exposed to anaesthetic gases: a meta-analysis.
Occupational and Environmental Medicine 1997;54(8):
541–8.
Bonica 1990
Bonica JJ. Definitions and taxonomy of pain. In: Bonica
JJ editor(s). The Management of Pain. 2nd Edition.
Philadelphia: Lea & Febiger, 1990.
Britton 2007
Britton C, McCormick FM, Renfrew MJ, Wade A, King
SE. Support for breastfeeding mothers. Cochrane Database
of Systematic Reviews 2007, Issue 1. [DOI: 10.1002/
14651858.CD001141.pub3]
Brucker 1984
Brucker MC. Nonpharmaceutical methods for relieving
pain and discomfort during pregnancy. MCN, AmericanJournal of Maternal Child Nursing 1984;9(6):390–4.
Caton 2002
Caton D, Corry MP, Frigoletto FD, Hopkins DP, Lieberman
E, Mayberry L, et al.The nature and management of labor
pain. American Journal of Obstetrics and Gynecology 2002;
186(5 Suppl Nature):S1–S15.
Clyburn 1993
Clyburn P, Rosen M. The effect of opioid and inhalational
analgesia on the newborn. In: Reynolds F editor(s). Effectson the Baby of Maternal Analgesia and Anaesthesia. London:
Saunders, 1993:169–90.
COMET 2001
Comparative Obstetric Mobile Epidural Trial (COMET)
Study Group UK. Effect of low dose mobile versus
traditional epidural techniques on mode of delivery: a
randomised control trial. Lancet 2001;358(9275):19–23.
Cyna 2004
Cyna AM, McAuliffe GL, Andrew MI. Hypnosis for pain
relief in labour and childbirth: a systematic review. BritishJournal of Anaesthesia 2004;93(4):505–11. [PUBMED:
15277295]
Dewhurst 2007
Edmonds DK, Dewhurst J. Chapter 9: Analgesia
and anaesthesia. Dewhurst’s Textbook of Obstetrics andGynaecology. 7th Edition. London: Wiley-Blackwell, 2007:
63–8.
37Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Dick Read 1954
Dick Read G. Childbirth Without Fear: The Principlesand Practice of Natural Childbirth. 3rd Edition. London:
William Heinemann, 1954.
Dick Read 2004
Dick Read G. Childbirth Without Fear: The Principles andPractice of Natural Childbirth. London: Pinter & Martin,
2004.
Edlich 1987
Edlich RF, Towler MA, Goitz RJ, Wilder RP, Buschbacher
LP, Morgan RF, et al.Bioengineering principles of
hydrotherapy. Journal of Burn Care and Rehabilitation 1987;
8:580–4.
Eng 2006
Eng YH, Cyna AM. A comparison of midwives’ knowledge
of and attitudes to hypnosis in hospitals with and without
a hypnotherapy service. Australian Journal of ClinicalHypnotherapy and Hypnosis 2006;34(1):17–26.
Ernst 1997
Ernst E, Koeder K. An overview of reflexology. European
Journal of General Practice 1997;3:52–7.
Evron 2007
Evron S, Ezri T. Options for systemic labor analgesia.
Current Opinion in Anaesthesiology 2007;20:181–5.
Faymonville 2000
Faymonville ME, Laureys S, Degueldre C, DelFiore
G, Luxen A, Franck G, et al.Neural mechanisms of
antinociceptive effects of hypnosis. Anesthesiology 2000;92
(5):1257–67.
Findley 1999
Findley I, Chamberlain G. ABC of labour care: relief of
pain. BMJ 1999;318:927–30.
Foureur 2008a
Foureur M. Theorising birth territory. In: Fahy K, Foureur
M, Hastie C editor(s). Birth Territory and MidwiferyGuardianship: Theory for Practice, Education and Research.
Edinburgh: Books for Midwives, 2008.
Foureur 2008b
Foureur M. Creating birth space to enable undisturbed
birth. In: Fahy K, Foureur M, Hastie C editor(s). Birth
Territory and Midwifery Guardianship: Theory for Practice,Education and Research. Edinburgh: Books for Midwives,
2008.
Gamsa 2003
Gamsa A. Hypnotic analgesia. In: Melzack R, Wall PD
editor(s). Handbook of Pain Management: A ClinicalCompanion to Wall and Melzack’s Textbook of Pain. Sydney:
Churchill Livingstone, 2003:521–31.
Garland 2000
Garland D, Jones. Waterbirths: supporting practice with
clinical audit. MIDIRS Midwifery Digest 2000;10(3):
333–6.
Gaskin 2003
Gaskin IM. The pain/pleasure riddle. Ina May’s Guide to
Childbirth. New York: Bantam Dell, 2003:150–66.
Geissbuehler 2000
Geissbuehler V, Eberhard J. Waterbirths a comparative
study. A prospective study on more than 2,000 waterbirths.
Fetal Diagnosis and Therapy 2000;15(5):291–300.
Gentz 2001
Gentz BA. Alternative therapies for the management of pain
in labor and delivery. Clinical Obstetrics & Gynecology 2001;
44(4):704–32.
Ginesi 1998a
Ginesi L, Niescierowicz R. Neuroendocrinology and birth
1: stress. British Journal of Midwifery 1998;6(10):659–63.
Ginesi 1998b
Ginesi L, Niescierowicz R. Neuroendocrinology and birth
2: The role of oxytocin. British Journal of Midwifery 1998;6
(12):791–6.
Gupta 2006
Gupta JK, Hofmeyr GJ, Smyth RMD. Position in the
second stage of labour for women without epidural
anaesthesia. Cochrane Database of Systematic Reviews 2004,
Issue 1. [DOI: 10.1002/14651858.CD002006.pub2]
Hall 1998
Hall SM, Holloway IM. Staying in control: women’s
experiences of labour in water. Midwifery 1998;14(1):30–6.
Hatem 2008
Hatem M, Sandall J, Devane D, Soltani H, Gates S.
Midwife-led versus other models of care for childbearing
women. Cochrane Database of Systematic Reviews 2008,
Issue 4. [DOI: 10.1002/14651858.CD004667.pub2]
Hebbes 2000
Hebbes C, Lambert D. Non-opioid analgesic drugs.
Anaesthesia & Intensive Care 200;9(2):79–83.
Higgins 2011
Higgins JPT, Green S, editors. Cochrane Handbook for
Systematic Reviews of Interventions Version 5.1.0 [updated
March 2011]. The Cochrane Collaboration, 2011.
Available from www.cochrane-handbook.org.
Hodnett 2007
Hodnett ED, Gates S, Hofmeyr GJ, Sakala C. Continuous
support for women during childbirth. Cochrane Databaseof Systematic Reviews 2007, Issue 3. [DOI: 10.1002/
14651858.CD003766.pub2]
Hogg 1977
Hogg MI, Wiener PC, Rosen M, Mapleson WW. Urinary
excretion and metabolism of pethidine and norpethidine in
the newborn. British Journal of Anaesthesia 1977;49(9):
891–9.
Hughes 2003
Hughes D, Simmons SW, Brown J, Cyna AM. Combined
spinal-epidural versus epidural analgesia in labour. Cochrane
Database of Systematic Reviews 2003, Issue 4. [DOI:
10.1002/14651858.CD003401.pub2]
Jadad 1996
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds
DJ, Gavaghan DJ, et al.Assessing the quality of reports of
38Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

randomized clinical trials: is blinding necessary?. Controlled
clinical trials 1996;17(1):1–12. [PUBMED: 8721797]
Jones 2011
Jones L, Dou L, Dowswell T, Alfirevic Z, Neilson James P.
Pain management for women in labour: generic protocol.
Cochrane Database of Systematic Reviews 2011, Issue 6.
[DOI: 10.1002/14651858.CD009167]
Jordan 2005
Jordan S, Emery S, Bradshaw C, Watkins A, Friswell W.
The impact of intrapartum analgesia on infant feeding.
BJOG: an international journal of obstetrics and gynaecology2005;112:927–34.
Jordan 2010
Jordan S. Pharmacology for Midwives: The Evidence Basefor Safe Practice. 2nd Edition. Basingstoke: Palgrave/
Macmillan, 2010.
Kane 2002
Kane RL, Bershadsky B, Lin WC, Rockwood T, Wood
K. Efforts to standardize the reporting of pain. Journal ofClinical Epidemiology 2002;55:105–10.
Kibuka 2009
Kibuka M, Thornton JG, Kingswood CJ. Position in the
second stage of labour for women with epidural anaesthesia.
Cochrane Database of Systematic Reviews 2009, Issue 4.
[DOI: 10.1002/14651858.CD008070]
KNOV 2009
KNOV werkgroep Entonox. The use of Relivopan in
primary care obstetrics [Adviesrapport: Het gebruik van
Relivopan in de eerstelijns verloskunde]. Adviesrapport
2009; Vol. 3.
Landolt 2011
Landolt AS, Milling LS. The efficacy of hypnosis as an
intervention for labor and delivery pain: a comprehensive
methodological review. Clinical psychology review 2011;31
(6):1022–31. [PUBMED: 21762655]
Lawrence 2009
Lawrence A, Lewis L, Hofmeyr GJ, Dowswell T, Styles C.
Maternal positions and mobility during first stage labour.
Cochrane Database of Systematic Reviews 2009, Issue 2.
[DOI: 10.1002/14651858.CD003934.pub2]
Leap 2004
Leap N, Anderson T. The role of pain in normal birth
and the empowerment of women. In: Downe S editor
(s). Normal Childbirth: Evidence and Debate. Edinburgh:
Churchill Livingstone, 2004:25–39.
Leap 2008
Leap N, Anderson P. The role of pain in normal birth
and the empowerment of women. In: Downe S editor(s).
Normal childbirth: evidence and debate. second edition.
London: Churchill Livingstone, 2008.
Leap 2010
Leap N, Dodwell M, Newburn M. Working with pain in
labour: an overview of evidence. New Digest 2010;49:22–6.
Lechner 1991
Lechner W, Jarosch E, Solder E, Waitz-Penz A,
Mitterschiffthaler G. Beta-endorphins during childbirth
under transcutaneous electric nerve stimulation [Verhalten
von Beta–Endorphin wahrend der Geburt unter
transkutaner elektrischer Nervenstimulation]. Zentralblattfur Gynakologie 1991;113(8):439–42.
Lowe 2002
Lowe NK. The nature of labor pain. American Journal ofObstetrics and Gynecology 2002;186:S16–S24.
Lytzen 1989
Lytzen T, Cederberg L, Moller-Nielsen J. Relief of low back
pain in labor by using intracutaneous nerve stimulation
(INS) with sterile water papules. Acta Obstetricia etGynecologica Scandinavica 1989;68:341–3.
Mankowski 2009
Mankowski J, Kingston J, Moran T, Nager C, Lukacz
E. Paracervical compared with intracervical lidocaine for
suction curettage: a randomized controlled trial. Obstetrics& Gynecology 2009;113(5):1052–7.
Maquet 1999
Maquet P, Faymonville ME, Degueldre C, Delfiore G,
Luxen A, Franck G, et al.Functional neuroanatomy of
hypnotic state. Biological Psychiatry 1999;45(3):327–33.
Marc 2011
Marc I, Toureche N, Ernst E, Hodnett ED, Blanchet C,
Dodin S, et al.Mind-body interventions during pregnancy
for preventing or treating women’s anxiety. Cochrane
Database of Systematic Reviews 2011, Issue 7. [DOI:
10.1002/14651858.CD007559.pub2]
Maze 2000
Maze M, Fujinaga M. Recent advances in understanding
the actions and toxicity of nitrous oxide. Anaesthesia 2000;
Vol. 55, issue 4:311–4.
Melzack 1965
Melzack R, Wall PD. Pain mechanisms: a new theory.
Science 1965;150(3699):971–9.
Melzack 1984
Melzack R. The myth of painless childbirth. Pain 1984;19
(4):321–337.
Moneta 2001
Moneta J, Okninska A, Wielgos M, Przybos A, Szymusik I,
Marianowski L. Patient’s preferences concerning the course
of labor. Ginekologia Polska 2001;72(12):1010–8.
Mozingo 1978
Mozingo JN. Pain in labor: a conceptual model for
intervention. Journal of Obstetric, Gynecologic, and Neonatal
Nursing 1978;7(4):47–9.
NICE 2007
National Institute for Health and Clinical Excellence.
Intrapartum care: care of healthy women and their babies
during childbirth. Clinical Guideline 55. London: NICE,
2007.
39Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
NICE 2008
National Collaborating Centre for Women’s and Children’s
Health. Induction of labour. Clinical Guideline 70. London:
NICE, 2008.
Nissen 1995
Nissen E, Lilja G, Matthiesen AS, Ransjo-Arvidsson AB,
Uvnas-Moberg K, Widstrom AM. Effects of maternal
pethidine on infants’ developing breast feeding behaviour.
Acta Paediatrica 1995;84(2):140–5.
NLM 1991a
National Library of Medicine. Labour stage, first.
National Library of Medicine MeSH Browser (http://
www.ncbi.nlm.nih.gov/mesh/68007747) (accessed 24
January 2011) 1991.
Ohlsson 2001
Ohlsson G, Buchhave P, Leandersson U, Nordstrom
L, Rydhstrom H, Sjolin I. Warm tub bathing during
labor: maternal and neonatal effects. Acta Obstetricia etGynecologica Scandinavica 2001;80:311–4.
Otigbah 2000
Otigbah CM, Dhanjal MK, Harmsworth G. A retrospective
comparison of water births and conventional vaginal
deliveries. European Journal of Obstetrics & Gynecology and
Reproductive Biology 2000;91(1):15–20.
Pace 2004
Pace MC, Aurilio C, Bulletti C, Iannotti M, Passavanti MB,
Palagiano A. Subarachnoid analgesia in advanced labor: a
comparison of subarachnoid analgesia and pudendal block
in advanced labor: analgesic quality and obstetric outcome.
Annals of the New York Academy of Sciences 2004;1034:
356–63.
Pomeranz 1989
Pomeranz B, Stux G. Scientific Bases of Acupuncture. Berlin:
Springer-Verlag, 1989.
Rajan 1994
Rajan L. The impact of obstetric procedures and analgesia/
anaesthesia during labour and delivery on breast feeding.
Midwifery 1994;10:87–103.
Ransjo-Arvidson 2001
Ransjo-Arvidson AB, Matthiesen AS, Lilja G, Nissen E,
Widstrom AM, Uvnas-Moberg K. Maternal analgesia
during labor disturbs newborn behavior: effects on
breastfeeding, temperature, and crying. Birth 2001;28(1):
5–12.
RevMan 2011
The Nordic Cochrane Centre, The Cochrane Collaboration.
Review Manager (RevMan). 5.1. Copenhagen: The Nordic
Cochrane Centre, The Cochrane Collaboration, 2011.
Reynolds 2011
Reynolds F. Labour analgesia and the baby: good news is no
news. International Journal of Obstetric Anesthesia 2011;20
(1):38–50.
Richmond 2003
Richmond H. Women’s experiences of waterbirth. PractisingMidwife 2003;6(3):26–31.
Righard 1990
Righard L, Alade MO. Effect of delivery room routines on
success of first breast-feed. Lancet 1990;336:1105–7.
Rosen 2002
Rosen MA. Nitrous oxide for relief of labor pain: a
systematic review. American Journal of Obstetrics andGynecology 2002;186(5 Suppl Nature):S110–S126.
[PUBMED: 12011877]
Rosenfeld 1996
Rosenfeld I. Dr. Rosenfeld’s Guide to Alternative Medicine.New York: Random House, 1996.
Russell 2000
Russell R. The effects of regional analgesia on the progress
of labour and delivery. British Journal of Anaesthesia 2000;
84(6):799–12.
Schorn 1993
Schorn MN, McAllister JL, Blanco JD. Water immersion
and the effect on labor. Journal of Nurse-Midwifery 1993;38
(6):336–42.
Sekhavat 2009
Sekhavat L, Behdad S. The effects of meperidine analgesia
during labor on fetal heart rate. International Journal of
Biomedical Science 2009;5(1):59–62.
Shea 2007
Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N,
Hamel C, et al.Development of AMSTAR: a measurement
tool to assess the methodological quality of systematic
reviews. BMC Medical Research Methodology 2007;7:10.
[PUBMED: 17302989]
Simkin 2004
Simkin P, Bolding A. Update on nonpharmacologic
approaches to relieve labor pain and prevent suffering.
Journal of Midwifery & Women’s Health 2004;49(6):
489–504.
Skibsted 1992
Skibsted L, Lange AP. The need for pain relief in
uncomplicated deliveries in an alternative birth center
compared to an obstetric delivery ward. Pain 1992;48:
183–6.
Solt 2002
Solt I, Ganadry S, Weiner Z. The effect of meperidine and
promethazine on fetal heart rate indices during the active
phase of labor. Israel Medical Association Journal 2002;4(3):
178–80.
Stevensen 1995
Stevensen CJ. The psychophysiological effects of
aromatherapy massage following cardiac surgery.
Complementary Therapies in Medicine 1995;2:27–35.
Thornton 2001
Thornton JG. Reducing likelihood of instrumental delivery
with epidural anaesthesia. Lancet 2001;358(9275):2.
Torvaldsen 2006
Torvaldsen S, Roberts CL, Simpson JM, Thompson
JF, Ellwood DA. Intrapartum epidural analgesia and
40Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

breastfeeding: a prospective cohort study. International
Breastfeeding Journal 2006;1:24.
Trolle 1991
Trolle B, Moller M, Kronborg H, Thomsen S. The effect
of sterile water blocks on low back labor pain. American
Journal of Obstetrics and Gynecology 1991;164:1277–81.
Vickers 1999
Vickers A, Zollman C. ABC of complementary therapies:
massage therapies. BMJ 1999;319:1254–7.
Wall 1967
Wall PD, Sweet W. Temporary abolition of pain in man.
Science 1967;155:108–9.
Werner 1982
Werner WE, Schauble PG, Knudson MS. An argument
for the revival of hypnosis in obstetrics. American Journal
of Clinical Hypnosis 1982;24(3):149–71. [PUBMED:
7137062]
Wiruchpongsanon 2006
Wiruchpongsanon P. Relief of low back labor pain by using
intracutaneous injections of sterile water: a randomized
clinical trial. Journal of the Medical Association of Thailand2006;89:571–6.
Zielhuis 1999
Zielhuis G, Peelen SJ, Florack EI, Roeleveld N. Hospital
work and fecundability. Scandinavian Journal of Work,
Environment & Health 1999;25 Suppl 1:47–8. [PUBMED:
10235410]∗ Indicates the major publication for the study
A D D I T I O N A L T A B L E S
Table 1. Non-Cochrane reviews: characteristics of excluded reviews
Name of Review Description of review Reason for exclusion
Arnal 2009 This paper examined IV remifentanil for
pain relief in labour. (The paper is in Span-
ish and eligibility assessment was carried
out using the abstract only)
This review examines IV remifentanil and
this topic is covered in a recently updated
Cochrane review
Aveline 2001 This review examined epidural and com-
bined spinal epidural. The main focus of
the review is on the duration of labour and
the mode of delivery. It appeared that only
five studies were included, although others
were discussed in the text. There did not
appear to have been any systematic assess-
ment of bias. (This paper was published in
French, so this assessment mainly relied on
details in the abstract)
The topic of this review is covered in a re-
cently updated Cochrane review
Benfield 2002 This review focused on hydrotherapy for
pain relief in labour.There was no descrip-
tion of the methods used to carry out
this review. There was no systematic search
strategy or method of data extraction, no
clear inclusion and exclusion criteria. There
was no systematic assessment of risk of bias.
All types of studies were included. There
was no meta analysis, rather a narrative de-
scription of findings
This was not a systematic review.
Bricker 2002 This systematic review examined parenteral
opioids. Cochrane methods were used and
This systematic review of parenteral opi-
oids, has been superseded by a recently up-
41Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
analysis was carried out using Review Man-
ager software
dated Cochrane systematic review
Bucklin 2002 The review appeared to have been carried
out in a systematic manner. The search cri-
teria, comparisons, inclusion and exclusion
criteria were stated along with outcomes.
It was not clear that there was a system-
atic quality assessment of studies. One mea-
sure of quality was stated to be publica-
tion in a peer reviewed journal. There was
no mention of domain based quality assess-
ment but in the tables in the review there
were notes re study design that included
risk of bias e.g.. It was stated if the study was
blinded and whether staff collecting out-
come data were blinded
The topic of this review is covered in an
included systematic review
Capogna 2004 This review was a mainly narrative sum-
mary of findings from RCTs and other re-
views (with meta-analysis) focusing on var-
ious types of epidural and CSE. It examined
different doses and types of drugs and com-
parisons. The main focus was on neonatal
outcome. The methods of the review were
not described. There was no search strat-
egy specified, no clear inclusion and exclu-
sion criteria, and no systematic assessment
of quality
Not a systematic review.
Carroll 1997 This review examines TENS in labour. The
review methods were described. The search
strategy and inclusion and exclusion crite-
ria were specified. Outcomes included anal-
gesic effect and adverse effects. There was
systematic assessment of study quality in-
cluding blinding and attrition. The review
included 8 RCTs. The review was carried
published in 1997 and the more recent
Cochrane TENS review examined all of the
eight included trials along with other more
recent RCTs
A more recent Cochrane review examines
TENS for pain relief in labour
Carroll 1997a This is an update of Carroll 1997 and in-
cludes 10 RCTs.
A more recent Cochrane review examines
TENS for pain relief in labour
Cho 2010 This review focusing on acupuncture for
pain relief in labour uses Cochrane meth-
ods and Review Manager software was used
This review covers the same topic as a
Cochrane review.
42Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
to carry out meta-analysis
Choi 2003 This review was not examining pain man-
agement in labour, rather it focused on the
incidence of headache following epidural
The topic of this review is covered in a re-
cently updated Cochrane review
Cyna 2004a There has been a more recent Cochrane re-
view on the same subject by the same au-
thor
The topic of this review is covered in a re-
cently updated Cochrane review
Fogarty 2008 This review on intradermal sterile water
injections for the relief of low back pain
in labour provides a narrative summary of
findings from reviews. There is no meta-
analysis and there has been a more recent
Cochrane review on the same topic
The topic of this review is covered in a re-
cently updated Cochrane review
Habib 2006 This review mainly focused on patients un-
dergoing surgery rather than women in
labour
The primary focus of this review was not
on women in labour.
Hager 1999 This is a critique of an earlier review. This is not a systematic review.
Halpern 1998 This is a systematic review of the effects
of epidural versus parenteral opioid anal-
gesia on the progress of labour. There has
been a more recent Cochrane review on the
same subject, epidural versus non-epidural,
which includes opioids as the non-epidural
arm
The topic of this review is covered in a re-
cently updated Cochrane review
Halpern 2005a This is a well conducted review which up-
dates earlier publications by same author
The topic of this review is covered in a re-
cently updated Cochrane review
Halpern 2003b This is not a systematic review. This is not a systematic review.
Halpern 2005b This is a narrative review considering find-
ings from other systematic reviews and in-
dividual RCTS. It was not clear that there
was a systematic search or assessment of in-
dividual study quality. The review focuses
on PCEA vs a continuous infusion. The
review also discusses studies where PCEA
plus a continuous background infusion are
compared with PCEA alone; and examines
different types of PCEA drugs
This is not a systematic review.
43Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
Halpern 2009 This review used systematic methods to as-
sess different types of patient controlled
epidural analgesia. The search methods
were described (search 1998 to 2008). The
review examined a range of different com-
parisons:
1. PCEA with background infusion vs no
background infusion
2. PCEA ropivacaine vs PCEA bupivacaine
3. High vs low PCEA background doses/
lockout times and bolus doses, and differ-
ent methods of administering drugs
There was no meta- analysis. Main findings
for each study are set out in tables and sum-
marised in the text
No data available from meta-analyses.
Hodnett 2002 This review focuses on all of the primary
outcomes of the overview but examines
broader questions and draws on descriptive
studies. It provides a very useful summary
of literature on satisfaction with pain relief
Not a systematic review including only
RCTs.
Huang 2002 This review examines economic issues re-
lating to pain relief in labour a topic which
is rarely addressed in trials
This is not an effectiveness review.
Huntley 2004 This is a review focusing on a range of com-
plementary and alternative techniques for
pain relief in labour (acupuncture, hypno-
sis, biofeedback, sterile water injection and
massage along with “respiratory autogenic
training”)
The review included clear inclusion, exclu-
sion criteria, a search strategy and inde-
pendent data extraction. There was an as-
sessment of methodological quality (Jadad
score). The review included RCTs and
quasi RCTs. There was no meta-analysis
due to “statistical heterogeneity amongst
the included studies. Results are set out in
tabular and narrative form
This review covers areas already covered in
included Cochrane reviews
Koehn 2002 This is a review looking at studies ex-
amining childbirth education/ antenatal
classes. The reviewer used a systematic
search mechanism although it was not clear
how studies were selected for inclusion.
The review included both qualitative and
quantitative studies but 11/12 studies were
This is not a systematic effectiveness re-
view. Narrative summary of findings from
mainly descriptive studies
44Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
descriptive and there was one before and
after study. No RCTs were included. There
was no systematic evaluation of risk of bias.
Some of the included studies included out-
comes relating to pain perception and satis-
faction with the childbirth experience, but
this was not the main focus of the review.
There was no meta analysis or quantitative
summary of findings. Results were reported
in narrative form and in descriptive tables
Kotaska 2006 This review examines epidural versus par-
enteral opiates. The review included a
search of MEDLINE and the The CochraneLibrary. There was no systematic assess-
ment of risk of bias. Results were reported
in tables and in the text. A recently updated
Cochrane review covers the same topic
A recently updated Cochrane review covers
the same topic.
Kuczkowski 2004 This is not a systematic review, it is a gen-
eral summary of the literature on regional
analgesia
This is not a systematic review.
Lally 2008 This review used systematic methods but it
is not an effectiveness review and included
both qualitative and quantitative studies
describing women’s perceptions of pain re-
lief during childbirth. Results were sum-
marised in tables and the text
This review included non-randomised
studies.
Larkin 2009 This is not a systematic review but a quali-
tative analysis of papers reporting women’s
experiences of childbirth
This is not a systematic review.
Lee 2004 Systematic review examining acupuncture
for pain relief in labour. There was a com-
prehensive search of 7 databases; assessed
methodological quality. All included stud-
ies are in more recent Cochrane systematic
review
A recently updated Cochrane review covers
the same topic.
Lee 2011 This is not a systematic review but a letter
relating to Cho 2010.
This is not a systematic review.
Leeman 2003a This paper focused on non-pharmacologi-
cal methods; It was not clear that this was
a systematic review, there was no descrip-
tion of review methods. It was not clear
This is not a systematic review, rather a nar-
rative summary of findings from reviews
and trials
45Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
if there was a search strategy. There was
some description of the quality of the in-
cluded studies but this was not systematic.
There was no meta-analysis. Findings were
set out in tables and text. The review in-
cluded Cochrane and other systematic re-
views along with other RCTs. It focused on
support in labour, sterile water injection,
massage, baths and warm water. This re-
view has been superceded by more recent
Cochrane reviews
Leeman 2003b This is a broad overview of reviews and
RCT evidence.
This is not a systematic review.
Leighton 2002 This is an update of a well-conducted sys-
tematic review (Halpern 1998) . The re-
view focuses on epidural vs parenteral opi-
oids in labour in relation to progress in
labour and rate of caesarean section. A sys-
tematic search was carried out (1980-2001)
and details of the search strategy and results
of the search are provided. There was in-
dependent data extraction by two review-
ers and a systematic assessment of quality
(Jadad score). The review includes meta-
analysis. This review is now out of date
and has been superseded by a more recent
Cochrane review
Superseded by more recent Cochrane re-
view.
Leighton 2003 This is not a report of a systematic review.
This paper discussed a range of study de-
signs and considered the evidence relating
to labour outcomes
Not a systematic review but draws on find-
ings of earlier systematic review by same
author
Lieberman 2002 This review included a search strategy and
systematic methods for extracting data.
There was no systematic assessment of
study quality using a domain-based risk of
bias assessment tool, rather the strengths
and weaknesses of study designs and anal-
yses were considered. The review looked at
both RCTs and observational studies com-
paring epidural vs opioids and epidural vs
no epidural. Outcomes included rates of
CS, assisted delivery, duration of labour
and adverse neonatal outcomes. More re-
cent Cochrane reviews have examined these
More recent Cochrane reviews examine the
same comparisons in RCTs
46Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
comparisons
Littleford 2004 This is a thorough review of a range of
methods for pain relief in labour. The main
focus of the review is on adverse effects of
analgesia on the fetus and newborn. Al-
though there was a systematic literature
search there was no systematic assessment
of risk of bias. The review cited other
reviews and included discussion of both
randomised and non-randomised studies.
There was no meta-analysis and results are
presented in narrative form
Not a systematic review.
Liu 2004 This systematic review examined low-dose
epidural compared with opioids in nulli-
parous women. Outcomes included rates
of CS, assisted delivery, duration of labour.
Systematic methods; search strategy de-
scribed, included RCTs only, systematic as-
sessment of study quality using Scottish
intercollegiate guideline network checklist
(which includes the same broad areas of risk
of bias as the Cochrane risk of bias tool);
systematic methods for data extraction and
meta-analysis. The focus is on nulliparous
women only and the comparison has been
examined in a more recent Cochrane re-
view
More recent Cochrane review available.
Lopard 2006 This is not a systematic review. It was not
clear that there was a systematic search
strategy or clear inclusion and exclusion cri-
teria. There was no systematic assessment
of risk of bias. The results are reported as a
narrative summary
This is not a systematic review.
Marucci 2007 This review looks at epidural and combined
spinal epidural in nulliparous women. The
main outcomes are CS, assisted delivery
and neonatal and newborn outcomes. In-
cluded both RCTs and cohort studies.
The review used systematic methods; the
search strategy was described (1990-2006)
. The studies were assessed for quality us-
ing standard measures (Jahad score for tri-
als). There were standard methods used for
data collection and meta-analysis was per-
formed
Recently up-dated Cochrane reviews covers
the same area.
47Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
Mayberry 2002 This review looks at adverse effects of
epidural. Included RCTs. The review used
systematic methods; the search strategy
was described (1990-2000). The studies
were assessed for quality. Standard meth-
ods were used for data collection. Meta-
analysis was not performed rather the re-
sults are described narratively. Recently up-
dated Cochrane reviews cover the same area
Topic covered in recently updated
Cochrane reviews.
Minty 2007 This review focuses on intrathecal analge-
sia as an alternative to epidural. There was
a systematic search and the strategy is de-
scribed. The review includes all study types
(reviews, RCTs and observational stud-
ies) and there was no clear systematic as-
sessment of the quality of the evidence.
The review covers a topic not covered by
Cochrane reviews but without a clear as-
sessment of risk of bias results are difficult
to interpret
The review includes a range of study de-
signs.
Morton 1994 This review looks at epidural in nulliparous
women. The main outcomes are CS, as-
sisted delivery and neonatal and newborn
outcomes. Included both RCTs and other
types of studies. The review used some sys-
tematic methods; the search strategy was
described There were standard methods
used for data collection and meta-analysis
was performed. There was no systematic as-
sessment of study quality and risk of bias.
Recently up-dated Cochrane reviews cover
the same area
Review includes non-randomised studies,
no systematic assessment of study quality.
Topic covered in more up to date Cochrane
reviews
Nystedt 2004 This review looks at the use of epidural.
. Included both RCTs and other types of
studies. The review used some systematic
methods; the search strategy was described.
The studies were assessed for quality based
on study design (high, moderate or low
scientific quality) but there was no system-
atic assessment of risk of bias. Recently up-
dated Cochrane reviews cover the same area
Recently up-dated Cochrane reviews cover
the same area.
Reynolds 2002 This review examines epidural vs par-
enteral opioids; the primary focus is on
studies reporting fetal acid-base as an
The topic of this review is covered in a re-
cently updated Cochrane review
48Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
outcome. The review includes both ran-
domised trials and non-randomised stud-
ies. A search strategy is described but there
did not appear to be any systematic as-
sessment of study quality. The topic of
this review is covered in a recently updated
Cochrane review
Reynolds 2010 This is not a systematic review but is a gen-
eral narrative summary of methods of pain
relief in labour and their effects on the baby
This is not a systematic review.
Rosen 2002a This review looks at paracervical block. A
search strategy was described but the au-
thor describes the review as non-exhaus-
tive. The search included MEDLINE and
the Cochrane library. The studies included
RCTs to examine the effects of analgesia
on fetal bradycardia but other studies were
included to describe adverse effects. There
was no systematic assessment of study qual-
ity. The topic of this review has been cov-
ered in a recently updated Cochrane review
The topic of this review has been covered
in a recently updated Cochrane review
Rosen 2002b This review looks inhaled analgesia. A
search strategy was described. The search
included MEDLINE and The Cochrane Li-brary. The studies included RCTs but other
studies were included to describe adverse
effects. It was not clear that there was a
systematic assessment of study quality but
included studies were described as “low to
moderate risk of bias”. The topic of this re-
view has been covered in a recently updated
Cochrane review
The topic of this review has been covered
in a recently updated Cochrane review
Sharma 2003 This review examines epidural analgesia
drawing on evidence from randomised tri-
als and non-randomised studies. It is not a
systematic review and it was not clear that
there was a search strategy or a systematic
assessment of study quality
This not a systematic review. Regional
analgesia is covered in recently updated
Cochrane Reviews
Sharma 2004 This is not a systematic review. This paper
reports findings of a retrospective analysis
of individual patient data collected in a se-
ries of trials over a 7 year period in the same
hospital; a subset of nulliparous women are
included in the sample in this meta-analy-
This is not a systematic review.
49Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
sis. There was no search and no systematic
assessment of risk of bias
Shiflett 2011 This is not a review. It is a letter comment-
ing on the findings of another review. Cho
- acupuncture review
This is not a review.
Simkin 2002 This review focuses on five methods to re-
lieve pain in labour including broad based
interventions such as continuous support
in labour, warm baths, maternal positions
and mobility in labour and massage and
intradermal water. It included RCTs and
non-randomised studies including before
and after studies. There was a search strat-
egy but there was no clear assessment of risk
of bias. There was no meta-analysis. Re-
sults were presented in narrative form and
in tables. The review includes broad base
interventions which we have not included
as methods of pain relief in labour; massage
and water injections are covered in recently
updated Cochrane reviews
Includes non randomised studies and fo-
cuses on broad based interventions
Simkin 2004a This overview focuses on 13 non-pharma-
cological methods to relieve pain in labour
including broad based interventions such
as continuous support in labour, warm
baths, maternal positions and mobility in
labour and massage and intradermal water.
It draws on findings from a series of system-
atic reviews (including Cochrane reviews)
. There was a search strategy but there was
no clear assessment of risk of bias in the re-
views included. There was no meta-analy-
sis. Results were presented in narrative form
and in tables. The review includes broad
base interventions which we have not in-
cluded as methods of pain relief in labour;
massage and water injections and relaxation
methods are covered in recently updated
Cochrane reviews
This is not a systematic review. It is a nar-
rative review.
Sleth 2006 This is not a systematic review. There was
a search strategy but the more recent data
was selected to underpin this discussion of
paracervical block. The topic is covered in a
recently updated Cochrane review. (Assess-
ment from English abstract; original full ar-
Not a systematic review. Cochrane review
covers the same topic
50Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Table 1. Non-Cochrane reviews: characteristics of excluded reviews (Continued)
ticle published in French)
Smith 2009 This review looks at acupuncture during
pregnancy and childbirth. It was carried
out by the author of a recently updated
Cochrane review on acupuncture in labour
included in this overview
Topic covered in recently updated
Cochrane review.
Thavaneswaran 2006 This systematic review looks at the safety
and efficacy of thoracic and lumbar par-
avertebral block in surgical patients. The
review does not examine pain relief during
labour
This review examines pain relief for surgery
(not during childbirth)
Thorp 1996 This review included evidence from both
RCTs and non-randomised studies. There
was a search strategy but no systematic as-
sessment of risk of bias or study quality. The
review focuses on epidural analgesia which
is covered in recently updated Cochrane re-
views
The review focuses on epidural analge-
sia which is covered in recently updated
Cochrane reviews
Van De Velde 2005 This is not a systematic review. It is a nar-
rative review of various types of neuraxial
analgesia and focuses specifically on brady-
cardia
This is not a systematic review.
Van de Velde 2009 This is not a systematic review but a gen-
eral narrative summary and discussion of
methods of neuraxial analgesia in labour
This is not a systematic review.
Van der Vyver 2002 This is a systematic review of RCTs com-
paring PCEA versus Continuous Infusion
for labour.
This topic is covered by more recent reviews
on epidural.
Writer 1998 This is not a systematic review - a report
of 6 RCTs which were conducted and then
the results pooled in a meta-analysis.
This is not a systematic review.
Wunsch 2003 This literature review includes animal and
medical studies, case reports, not RCTs.
Review of pain in pregnancy, not labour
and addiction medicine
This is not a systematic review.
Zhang 1999 This review included both RCTs and ob-
servational studies. Search date up to 1997.
This topic is covered by more recent
Cochrane reviews on epidural
Zhou 2008 This review includes RCTs comparing local
versus systemic application of opioids for
labour analgesia.
This topic is covered by a more recent
Cochrane review.
51Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

CS: Caeserean section; PCEA: Patient Controlled Epidural Analgesia; RCT: randomised controlled trial
Table 2. Characteristics of included Cochrane systematic reviews - non-pharmacological interventions
Review title Date of search No. Studies in-
cluded
(No. Patients in
included stud-
ies)
Inclusion crite-
ria for “Types of
participants”
Comparison in-
terventions (no.
studies)
Outcomes for
which data were
reported
that could be
included in an
analysis
Summary
of quality of evi-
dence in reviews
(risk of bias)
Hypno-
sis for pain man-
agement during
labour and child-
birth (Madden
2012)
7 September
2011
7 studies in 3
countries (Aus-
tralia, USA, UK)
between 1986
and 2010
(1213 women)
Pregnant women
including
women in high
risk groups e.g.
preterm
labour or follow-
ing induction of
labour
Self-hypno-
sis or hypnother-
apy versus con-
trol (standard
childbirth prepa-
ra-
tion; a relaxation
tape; supportive
counselling; psy-
chotherapy)
(7 studies, 1070
women)
Hypnosis & au-
dio
CD versus audio
CD of hypno-
sis (1 study, 297
women)
N.B. one study,
n
= 448, included
three arms and so
data for the dif-
ferent arms are
included in the
separate compar-
isons
• Pain
intensity
• Satisfaction
with pain relief
• Satisfaction
with childbirth
experience
• Breastfeeding
• Assisted
vaginal birth
• Caesarean
section
• Admission
to special care
baby unit/
neonatal
intensive care
• Apgar score
less than seven
at five minutes
• Adverse
effects for
women and
infants
(postnatal
depression,
newborn
resuscitation)
Se-
quence genera-
tion: 2 studies
low risk; 5 stud-
ies unclear risk
Allocation con-
cealment: 1
study low risk; 2
studies high risk;
4 studies unclear
risk
Blinding
(participants &
clinical staff ): 3
studies low risk;
4 studies unclear
risk
Blinding (out-
come assessors)
: 3 studies low
risk; 4 studies
unclear risk
Incomplete
outcome re-
porting: 3 stud-
ies low risk; 2
studies high risk;
2 studies unclear
risk
Selec-
tive outcome re-
porting: 3 stud-
ies low risk; 2
studies high risk;
52Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Characteristics of included Cochrane systematic reviews - non-pharmacological interventions (Continued)
2 studies unclear
risk
Other potential
threats to va-
lidity: 3 studies
low risk; 4 stud-
ies unclear risk
Biofeedback
for pain during
labour (Barragán
2011)
20 March 2011 4 stud-
ies in 3 coun-
tries (UK, USA
and Italy) be-
tween 1978 and
2000
(201 women
ran-
domised, 2 stud-
ies (103 women)
contributed data
to meta-analysis)
Women with low
risk pregnan-
cies e.g. healthy
pregnant women
likely to have a
normal birth
Biofeedback ver-
sus no biofeed-
back/stan-
dard care (2 stud-
ies, 103 women)
• Assisted
vaginal birth
• Caesarean
section
Sequence gen-
eration: 1 study
low risk; 3 stud-
ies unclear risk
Allocation con-
cealment:
4 studies unclear
risk
Blinding:
4 studies unclear
risk
Incomplete
outcome re-
porting: 2 stud-
ies low risk; 2
studies high risk
Selec-
tive outcome re-
porting: 1 study
low risk; 3 stud-
ies high risk
Other potential
threats to valid-
ity: 4 studies low
risk
Intracutaneous
or subcutaneous
sterile water in-
jection for pain
management in
labour (Derry
2012)
30 May 2011 7 studies in 5
countries
(Sweden,
Denmark, Iran,
Thailand, India)
between 1990
and 2009
(766 women)
Women in active
labour who re-
quested analge-
sia for pain of
moderate to se-
vere
intensity. There
were no restric-
tions relating to
place of birth
or to maternal
parity, risk sta-
tus, age, weight,
length of gesta-
tion, or stage of
Intracuta-
neous sterile wa-
ter injection ver-
sus normal saline
injection (4 stud-
ies, 467 women)
Subcuta-
neous sterile wa-
ter injection ver-
sus normal saline
injection (2 stud-
ies, 200 women)
Intracu-
taneous & sub-
cutaneous ster-
• Assisted
vaginal birth
• Caesarean
section
Se-
quence genera-
tion: 4 studies
low risk; 3 stud-
ies unclear risk
Allocation con-
cealment: 4
studies low risk;
4 studies unclear
risk
Blinding
(participants &
clinical staff ): 5
studies low risk;
53Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Table 2. Characteristics of included Cochrane systematic reviews - non-pharmacological interventions (Continued)
labour ile water injec-
tion versus nor-
mal saline injec-
tion (1 study, 99
women)
1 study high risk;
1 study unclear
risk
Blinding (out-
come assessors):
7 studies low risk
Incomplete
outcome re-
porting: 2 stud-
ies low risk; 1
study high risk;
4 studies unclear
risk
Selective out-
come reporting:
4 studies
low risk; 3 stud-
ies unclear risk
Other potential
threats to va-
lidity: 3 studies
high risk; 4 stud-
ies unclear risk
Immer-
sion in water in
labour and birth
(Cluett 2009)
30 June 2011 12 studies in 11
countries (USA,
Canada, UK,
Sweden,
Finland,
Belguim, Iran,
South Africa,
Brazil, Australia)
between 1993
and 2009
(3252 women)
Nul-
liparous or mul-
tiparous women
in labour with
a singleton preg-
nancy, irrespec-
tive of gestation
or labour charac-
teristics
Immersion ver-
sus no immer-
sion in the first
stage of labour
(8 studies, 2826
women)
Immersion ver-
sus
no immersion in
the second stage
of labour (3 stud-
ies, 286 women)
Early versus late
immersion dur-
ing the first stage
of
labour (1 study,
200 women)
N.B. one study,
n = 60, included
data for both first
and second
stages of labour
and so is in-
• Pain
intensity
• Satisfaction
with childbirth
experience
• Breastfeeding
• Assisted
vaginal birth
• Caesarean
section
• Adverse
effects for
women
• Adverse
effects for
infants
• Admission
to special care
baby unit/
neonatal
intensive care
unit
• Apgar score
Sequence gen-
eration: 6 stud-
ies low risk; 2
studies high risk;
4 studies unclear
risk
Allocation con-
cealment: 8
studies low risk;
3 studies high
risk; 1 study un-
clear risk
Blinding (par-
ticipants/clini-
cal staff/out-
come assessor):
12 studies high
risk
Incomplete
out-
come reporting:
11 studies low
risk; 1 study un-
54Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Characteristics of included Cochrane systematic reviews - non-pharmacological interventions (Continued)
cluded in num-
bers for both
comparisons
less than seven
at five minutes
clear risk
Selective out-
come reporting:
10 studies low
risk; 1 study high
risk; 1 study un-
clear risk
Other potential
threats to valid-
ity: 1 study low
risk; 11 studies
unclear risk
Aromatherapy
for pain manage-
ment in labour (
Smith 2011c)
31 October
2010
2 stud-
ies in 2 coun-
tries (Italy, New
Zealand) be-
tween 2000 and
2007
(535 women)
Women in
labour, in-
cluding high risk
groups e.g.
preterm
labour or follow-
ing induction
Aromatherapy
versus standard
care (1 study,
513 women)
One type of aro-
matherapy (gin-
ger) versus a dif-
ferent type
of aromatherapy
(lemon grass) (1
study, 22
women)
• Assisted
vaginal birth
• Caesarean
section
• Adverse
effects for
women
(postpartum
haemorrhage)
• Admission
to special care
baby unit
• Apgar score
less than seven
at five minutes
Sequence gen-
eration: 2 stud-
ies low risk
Allocation con-
cealment: 2
studies low risk
Blinding: 1
study low risk; 1
study high risk
Incomplete
out-
come reporting:
2 studies low risk
Selective out-
come reporting:
2 studies unclear
risk
Other potential
threats to valid-
ity: 1 study low
risk; 1 study high
risk
Relaxation tech-
niques for pain
management in
labour (Smith
2011b)
30 November
2010
11 stud-
ies in 9 countries
(USA, UK, Swe-
den, Italy,
Turkey, Thai-
land, Iran, Tai-
wan, Brazil) be-
tween 1965 and
2010
(1574 women)
Women in
labour, in-
cluding high risk
groups e.g.
preterm
labour or follow-
ing induction
Relaxation (pro-
gres-
sive muscle re-
laxation; breath-
ing; psychopro-
phylaxis) versus
standard care (6
studies,1147
women)
Yoga versus stan-
dard care (2 stud-
ies, 270 women)
Music ver-
• Pain
intensity
• Satisfaction
with pain relief
• Satisfaction
with childbirth
experience
• Assisted
vaginal delivery
• Caesarean
section
• Apgar score
less than seven
Se-
quence genera-
tion: 6 studies
low risk; 5 stud-
ies unclear risk
Allocation con-
cealment: 3
studies low risk;
8 studies unclear
risk
Blinding: 8
studies high risk;
3 studies unclear
55Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Characteristics of included Cochrane systematic reviews - non-pharmacological interventions (Continued)
sus standard care
(2 studies, 133
women)
Audio-analgesia
versus standard
care (1 study, 24
women)
at five minutes risk
Incomplete
outcome re-
porting: 5 stud-
ies low risk; 2
studies high risk;
4 studies unclear
risk
Selec-
tive outcome re-
porting: 1 study
low risk; 10 stud-
ies unclear risk
Other potential
threats to va-
lidity: 5 studies
low risk; 6 stud-
ies unclear risk
Acupuncture or
acupressure
for pain manage-
ment in labour (
Smith 2011a)
31 October
2010
13 studies in 8
countries (Nor-
way, Sweden,
Denmark, India,
Korea, Taiwan,
China, Iran) be-
tween 2002 and
2010
(1986 women)
Women in
labour, in-
cluding high risk
groups e.g.
preterm
labour or follow-
ing induction
Acupuncture or
acupressure ver-
sus placebo/stan-
dard care/
no treatment (12
studies, 1858
women)
Acupunc-
ture versus ster-
ile water injec-
tion (1 study,
128 women)
• Pain
Intensity
• Satisfaction
with pain relief
• Satisfaction
with childbirth
experience
• Assisted
vaginal birth
• Caesarean
section
• Apgar score
less than seven
at five minutes
Se-
quence genera-
tion: 12 studies
low risk; 1 study
unclear risk
Allocation con-
cealment: 9
studies low risk;
4 studies unclear
risk
Blinding: 3
studies low risk;
5 studies high
risk; 5 studies
unclear risk
Incomplete
outcome re-
porting: 9 stud-
ies low risk; 1
study high risk;
3 studies unclear
risk
Selective out-
come reporting:
13 studies un-
clear risk
Other potential
threats to valid-
56Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Characteristics of included Cochrane systematic reviews - non-pharmacological interventions (Continued)
ity: 8 studies low
risk; 3 studies
high risk; 2 stud-
ies unclear risk
Massage, reflex-
ology and other
manual methods
for pain manage-
ment in labour (
Smith 2012)
30 June 2011 6 stud-
ies in 4 countries
(USA, UK, Iran,
Taiwan) between
1997 and 2010
(401 women
ran-
domised, 5 stud-
ies (326 women)
contributed data
to meta-analysis)
Women in
labour, in-
cluding high risk
groups e.g.
preterm
labour or follow-
ing induction
Massage
versus usual care
(4 studies, 225)
Massage ver-
sus breathing ex-
ercises (1 study,
28 women)
Mas-
sage versus mu-
sic (1 study, 101
women)
• Pain
intensity
• Satisfaction
with pain relief
• Sense of
control in labour
• Assisted
vaginal birth
• Caesarean
section
• Admission
to neonatal
intensive care
unit
Sequence gen-
eration: 4 stud-
ies low risk; 1
study high risk;
1 study unclear
risk
Allocation con-
cealment:
1 study low risk;
5 studies unclear
risk
Blinding
(participants &
clinical staff ): 5
studies high risk;
1 study unclear
risk
Blinding (out-
come assessor)
: 4 studies low
risk; 1 study high
risk; 1 study un-
clear risk
Incom-
plete outcome
reporting: 5
studies low risk;
1 study unclear
risk
Selective out-
come reporting:
1 study low risk;
5 studies unclear
risk
Other potential
threats to va-
lidity: 3 studies
low risk; 3 stud-
ies unclear risk
Tran-
scutaneous elec-
trical nerve stim-
ulation (TENS)
for pain manage-
30 April 2011 17 studies in 15
countries (USA,
Canada, UK,
Ireland, France,
Swe-
Women in
labour (risk not
stated)
TENS versus
placebo or usual
care (17 studies,
1455 women)
• Pain
intensity
• Satisfaction
with pain relief
Sequence gen-
eration: 3 stud-
ies low risk; 1
study high risk;
57Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 2. Characteristics of included Cochrane systematic reviews - non-pharmacological interventions (Continued)
ment in labour (
Dowswell 2009)
den, Denmark,
Germany, Nor-
way, the Nether-
lands, India, Tai-
wan, China,
Brazil, Australia)
between 1978
and 2010
(1466 women)
TENS versus
sterile water in-
jection (1 study,
22 women)
• Assisted
vaginal birth
• Caesarean
section
• Side effects
for baby
14 studies un-
clear risk
Allocation con-
cealment: 3
studies low risk;
1 study high risk;
14 studies un-
clear risk
Blinding
(participants): 8
studies high risk;
10 studies un-
clear risk
Blinding (clini-
cal staff )
: 8 studies high
risk; 10 studies
unclear risk
Blinding (out-
come assessor)
: 7 studies high
risk; 11 studies
unclear risk
Incomplete
out-
come reporting:
10 studies low
risk; 2 studies
high risk; 6 stud-
ies unclear risk
Other potential
threats to valid-
ity: 18 studies
unclear risk
N.B. 17 studies
contributed data
to the review, but
18 studies were
included and as-
sessed for risk of
bias
58Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 3. Characteristics of included Cochrane systematic reviews - pharmacological interventions
Review title Date of search No. Studies in-
cluded
(No. Patients in
included stud-
ies)
Inclusion crite-
ria for “Types of
participants”
Comparison in-
terventions (no.
studies)
Outcomes for
which data were
reported
that could be
included in an
analysis
Summary
of quality of evi-
dence in reviews
(risk of bias)
Inhaled analgesia
for pain manage-
ment in labour (
Klomp 2012)
7 September
2011
26 studies in 8
countries (USA,
Canada, UK,
Sweden, Nor-
way, China, Sin-
gapore, Iran) be-
tween 1969 and
2009
(2967 women)
Women in
labour, in-
cluding high risk
groups e.g.
preterm
labour or follow-
ing induction
Inhaled analgesia
versus placebo
control/no treat-
ment (9 studies,
1495 women)
Inhaled analge-
sia versus a dif-
ferent type of
inhaled analgesia
(14 studies, 752
women)
Inhaled analgesia
of one strength
versus a different
strength (2 stud-
ies, 625 women)
Inhaled analgesia
using one type of
delivery system
versus a different
system (2 stud-
ies, 75 women)
Inhaled analgesia
versus TENS (1
study, 20
women)
• Pain
Intensity
• Satisfaction
with pain relief
• Assisted
vaginal birth
• Caesarean
section
• Adverse
effects for
women (nausea;
vomiting;
drowsiness;
dizziness; blood
loss; pre-
eclampsia)
• Adverse
effects for
infants
(hypoxaemia;
neuro-
behavioural
score; neonatal
asphyxia)
• Admission
to special care
baby unit
• Apgar score
less than seven
at five minutes
Se-
quence genera-
tion: 7 studies
low risk; 19 stud-
ies unclear risk
Allocation con-
ceal-
ment: 3 studies
low risk; 23 stud-
ies unclear risk
Blinding
(participants &
clinical staff ): 3
studies low risk;
4 studies high
risk; 19 studies
unclear risk
Blinding (out-
come as-
sessor): 3 stud-
ies low risk; 4
studies high risk;
19 studies un-
clear risk
Incomplete
out-
come reporting:
13 studies low
risk; 4 studies
high risk; 9 stud-
ies unclear risk
Selective out-
come reporting:
16 studies low
risk; 5 studies
high risk; 5 stud-
ies unclear risk
Other potential
59Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
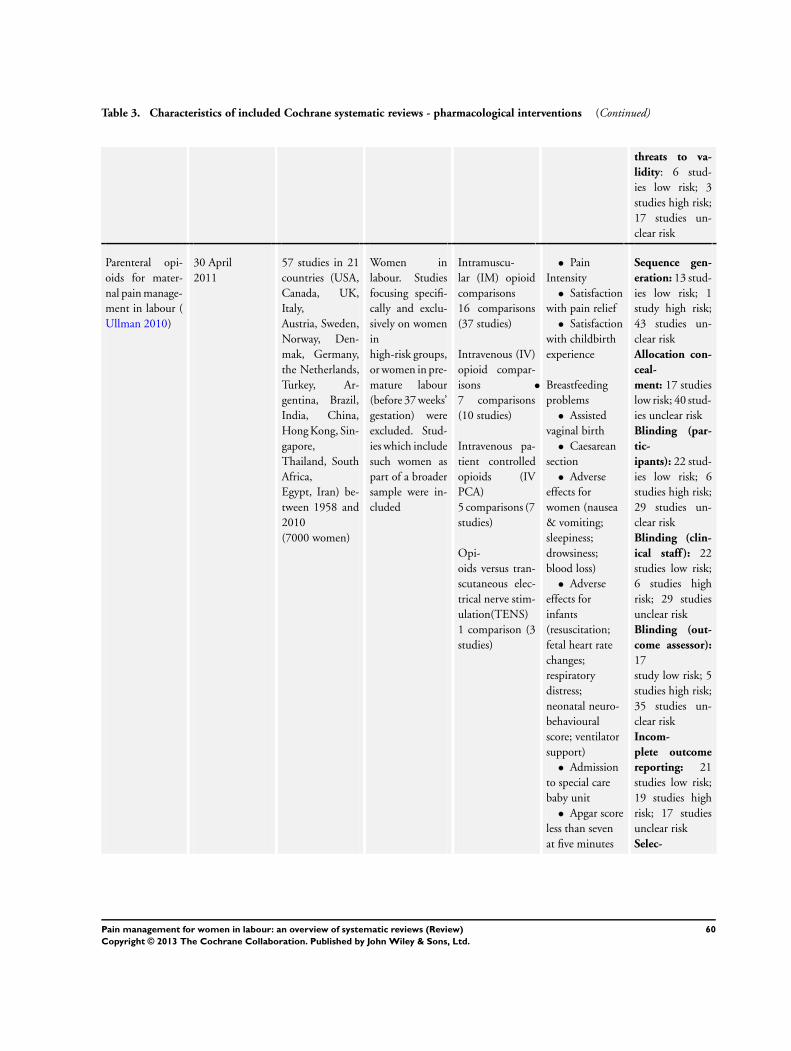
Table 3. Characteristics of included Cochrane systematic reviews - pharmacological interventions (Continued)
threats to va-
lidity: 6 stud-
ies low risk; 3
studies high risk;
17 studies un-
clear risk
Parenteral opi-
oids for mater-
nal pain manage-
ment in labour (
Ullman 2010)
30 April
2011
57 studies in 21
countries (USA,
Canada, UK,
Italy,
Austria, Sweden,
Norway, Den-
mak, Germany,
the Netherlands,
Turkey, Ar-
gentina, Brazil,
India, China,
Hong Kong, Sin-
gapore,
Thailand, South
Africa,
Egypt, Iran) be-
tween 1958 and
2010
(7000 women)
Women in
labour. Studies
focusing specifi-
cally and exclu-
sively on women
in
high-risk groups,
or women in pre-
mature labour
(before 37 weeks’
gestation) were
excluded. Stud-
ies which include
such women as
part of a broader
sample were in-
cluded
Intramuscu-
lar (IM) opioid
comparisons
16 comparisons
(37 studies)
Intravenous (IV)
opioid compar-
isons
7 comparisons
(10 studies)
Intravenous pa-
tient controlled
opioids (IV
PCA)
5 comparisons (7
studies)
Opi-
oids versus tran-
scutaneous elec-
trical nerve stim-
ulation(TENS)
1 comparison (3
studies)
• Pain
Intensity
• Satisfaction
with pain relief
• Satisfaction
with childbirth
experience
• Breastfeeding
problems
• Assisted
vaginal birth
• Caesarean
section
• Adverse
effects for
women (nausea
& vomiting;
sleepiness;
drowsiness;
blood loss)
• Adverse
effects for
infants
(resuscitation;
fetal heart rate
changes;
respiratory
distress;
neonatal neuro-
behavioural
score; ventilator
support)
• Admission
to special care
baby unit
• Apgar score
less than seven
at five minutes
Sequence gen-
eration: 13 stud-
ies low risk; 1
study high risk;
43 studies un-
clear risk
Allocation con-
ceal-
ment: 17 studies
low risk; 40 stud-
ies unclear risk
Blinding (par-
tic-
ipants): 22 stud-
ies low risk; 6
studies high risk;
29 studies un-
clear risk
Blinding (clin-
ical staff ): 22
studies low risk;
6 studies high
risk; 29 studies
unclear risk
Blinding (out-
come assessor):
17
study low risk; 5
studies high risk;
35 studies un-
clear risk
Incom-
plete outcome
reporting: 21
studies low risk;
19 studies high
risk; 17 studies
unclear risk
Selec-
60Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 3. Characteristics of included Cochrane systematic reviews - pharmacological interventions (Continued)
tive outcome re-
porting: 1 stud-
ies low risk; 3
studies high risk;
53 studies un-
clear risk
Other potential
threats to va-
lidity: 11 stud-
ies low risk; 2
studies high risk;
44 studies un-
clear risk
Non-opioid
drugs for pain
management in
labour (Othman
2012)
19 May 2011 18 studies in 7
countries (USA,
Canada,
UK, Sweden, Ar-
gentina, In-
dia, China) be-
tween 1963 and
2004
(2733 women)
Women in
labour, in-
cluding high risk
groups e.g.
preterm
labour or follow-
ing induction
Non-
opioid drug ver-
sus placebo or no
treatment
(14 studies, 2003
women)
Non-opioid
drug versus any
other pain man-
agement
intervention e.g.
opioids (3 stud-
ies, 563 women)
Non-opioid
drug versus dif-
ferent non-opi-
oid drug (2 stud-
ies, 562 women)
Non-
opioid drug ver-
sus same non-
opioid different
dose (1 study, 28
women)
(3 studies have
more than two
arms and are in-
cluded in more
than one com-
parison group)
• Pain
intensity
• Satisfaction
with pain relief
• Satisfaction
with childbirth
experience
• Breastfeeding
• Assisted
vaginal birth
• Caesarean
section
• Adverse
effects for
women
• Adverse
effects for
infants
• Apgar score
less than seven
at five minutes
Se-
quence genera-
tion: 6 studies
low risk; 12 stud-
ies unclear risk
Allocation con-
ceal-
ment: 5 studies
low risk; 13 stud-
ies unclear risk
Blinding (par-
ticipants/clin-
ical staff ): 14
studies low risk;
4 studies unclear
risk
Blinding (out-
come assessor)
: 3 studies low
risk; 15 studies
unclear risk
Incomplete
out-
come reporting:
16 studies low
risk; 2 studies
high risk
Selective out-
come reporting:
12 studies low
risk; 5 studies
high risk; 1 study
61Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 3. Characteristics of included Cochrane systematic reviews - pharmacological interventions (Continued)
unclear risk
Other potential
threats to valid-
ity: 13 studies
low risk; 1 study
high risk; 4 stud-
ies unclear risk
Local anaesthetic
nerve block
for pain manage-
ment in labour (
Novikova 2012)
6 June 2011 12 studies (coun-
tries not stated in
review) between
1969 and 2009
(1549 women)
Women in
labour, in-
cluding high risk
groups e.g.
preterm
labour or follow-
ing induction
Local anaesthetic
nerve block ver-
sus differ-
ent dose/agent or
timing of anaes-
thetic nerve
block (8 studies,
1120 women)
Local anaesthetic
nerve block ver-
sus
placebo (1 study,
200 women)
Local anaesthetic
nerve block ver-
sus
opioid (2 studies,
129 women)
Local anaesthetic
nerve block ver-
sus non-opi-
oid (1 study, 100
women)
• Satisfaction
with pain relief
• Assisted
vaginal birth
• Caesarean
section
• Adverse
effects for
women
• Apgar score
less than seven
at five minutes
Sequence gen-
eration: 2 stud-
ies low risk; 2
studies high risk;
8 studies unclear
risk
Allocation con-
cealment:
1 study high risk;
11 studies un-
clear risk
Blinding (par-
ticipants/
clinical staff ): 4
studies low risk;
4 studies high
risk; 4 studies
unclear risk
Blinding (out-
come assessor)
: 4 studies low
risk; 5 studies
high risk; 3 stud-
ies unclear risk
Incomplete
outcome re-
porting: 6 stud-
ies low risk; 4
studies high risk;
2 studies unclear
risk
Selec-
tive outcome re-
porting: 5 stud-
ies low risk; 7
studies high risk
Other potential
threats to va-
lidity: 9 studies
low risk; 3 stud-
ies high risk
62Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 3. Characteristics of included Cochrane systematic reviews - pharmacological interventions (Continued)
Epidural ver-
sus non-epidural
or no analgesia
in labour (Anim-
Somuah 2011)
31 March 2011 38 studies in 18
countries (USA,
Canada, UK,
France, Sweden,
Fin-
land, Denmark,
Mexico, Russia,
Saudi Ara-
bia, Egypt, Is-
rael, Iran, India,
Taiwan, Thai-
land, China,
Australia) be-
tween 1974 and
2010
(9658 women)
Pregnant women
in
labour request-
ing pain relief,
regardless of par-
ity and whether
labour was spon-
taneous or in-
duced
Epidu-
ral versus opioids
(33 studies, 8868
women)
Epidural
versus no anal-
gesia (5 studies,
790 women)
• Pain
intensity
• Satisfaction
with pain relief
• Sense of
control in labour
• Satisfaction
with childbirth
experience
• Assisted
vaginal birth
• Caesarean
section
• Adverse
effects for
women (long-
term backache;
maternal
hypotension;
postnatal
depression;
motor blockade;
headache;
nausea and
vomiting;
itching; fever;
shivering;
drowsiness;
urinary
retention;
malposition;
surgical
amniotomy)
• Adverse
effects for
infants (acidosis;
naloxone
administration;
meconium
staining of
liquor)
• Admission
to special care
baby unit
• Apgar score
Sequence gen-
eration: 18 stud-
ies low risk; 1
study high risk;
19 studies un-
clear risk
Allocation con-
ceal-
ment: 16 studies
low risk; 22 stud-
ies unclear risk
Blinding
(participants): 4
studies low risk;
6 studies high
risk; 28 studies
unclear risk
Blinding (clini-
cal staff ): 4
studies low risk;
3 studies high
risk; 31 studies
unclear risk
Blinding (out-
come assessor):
1 study low risk;
1 study high risk;
36 studies un-
clear risk
Incom-
plete outcome
reporting: 12
studies low risk;
7 studies high
risk; 19 studies
unclear risk
Selective out-
come reporting:
14 study low
risk; 15 studies
high risk; 9 stud-
ies unclear risk
Other potential
threats to va-
63Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
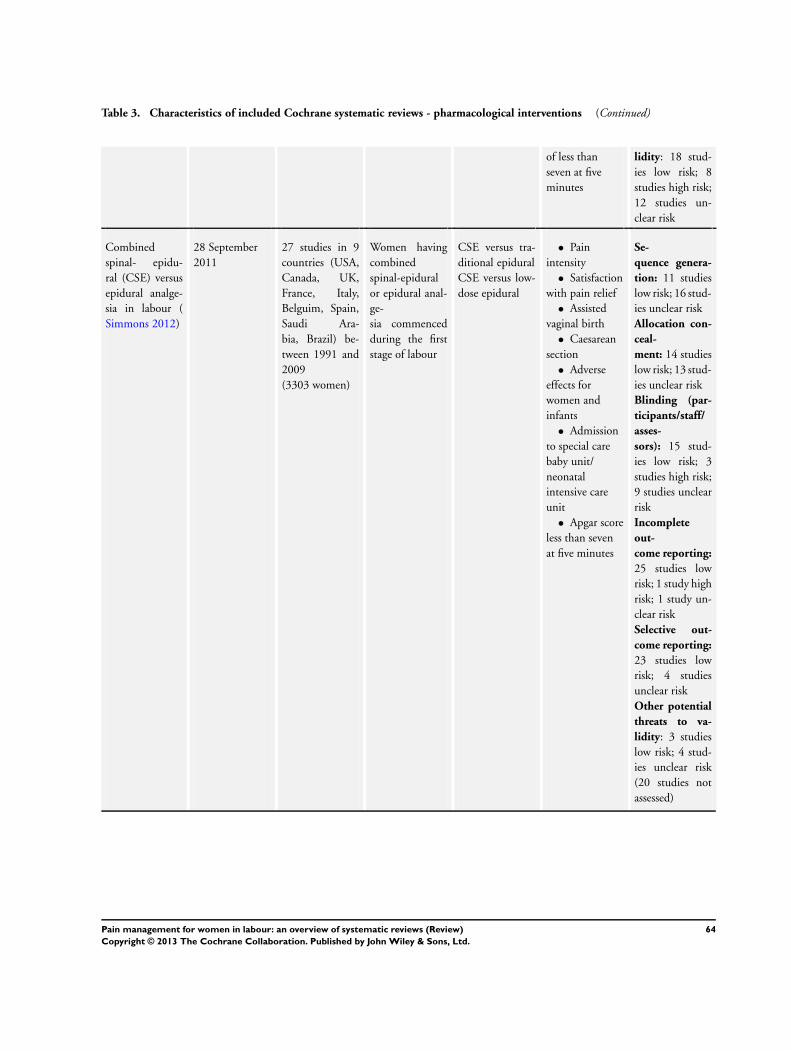
Table 3. Characteristics of included Cochrane systematic reviews - pharmacological interventions (Continued)
of less than
seven at five
minutes
lidity: 18 stud-
ies low risk; 8
studies high risk;
12 studies un-
clear risk
Combined
spinal- epidu-
ral (CSE) versus
epidural analge-
sia in labour (
Simmons 2012)
28 September
2011
27 studies in 9
countries (USA,
Canada, UK,
France, Italy,
Belguim, Spain,
Saudi Ara-
bia, Brazil) be-
tween 1991 and
2009
(3303 women)
Women having
combined
spinal-epidural
or epidural anal-
ge-
sia commenced
during the first
stage of labour
CSE versus tra-
ditional epidural
CSE versus low-
dose epidural
• Pain
intensity
• Satisfaction
with pain relief
• Assisted
vaginal birth
• Caesarean
section
• Adverse
effects for
women and
infants
• Admission
to special care
baby unit/
neonatal
intensive care
unit
• Apgar score
less than seven
at five minutes
Se-
quence genera-
tion: 11 studies
low risk; 16 stud-
ies unclear risk
Allocation con-
ceal-
ment: 14 studies
low risk; 13 stud-
ies unclear risk
Blinding (par-
ticipants/staff/
asses-
sors): 15 stud-
ies low risk; 3
studies high risk;
9 studies unclear
risk
Incomplete
out-
come reporting:
25 studies low
risk; 1 study high
risk; 1 study un-
clear risk
Selective out-
come reporting:
23 studies low
risk; 4 studies
unclear risk
Other potential
threats to va-
lidity: 3 studies
low risk; 4 stud-
ies unclear risk
(20 studies not
assessed)
64Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 4. Characteristics of included non-Cochrane systematic reviews - non-pharmacological
Review title Date of search No. studies in-
cluded
Inclusion crite-
ria for “Types of
participants”
Comparison in-
terventions (no.
studies)
Outcomes for
which data were
reported
that could be
included in an
analysis
Summary
of quality of evi-
dence in reviews
(risk of bias)
Sterile water in-
jec-
tion for labour
pain: a system-
atic review and
meta-analysis of
randomised con-
trolled trials
(Hutton 2009)
Up to 2009 8 (783 women) Pregnant women
who had lower
back pain during
the active stage
of labour and re-
quested pain
medication
Intra-
cutaneous sterile
or subcutaneous
sterile water in-
jection versus
placebo control
(saline) or an-
other non-phar-
ma-
cological modal-
ity (acupuncture;
TENs) (8 stud-
ies, 783 women)
• Pain
intensity
• Caesarean
section
Methodological
quality assessed
using the modi-
fied Jadad scale
Score of 10 or
more = consid-
ered high quality
score 8: 1 study
score 10: 4 stud-
ies
score 12: 2 stud-
ies
score 13: 1 study
Table 5. Characteristics of included non-Cochrane systematic reviews - pharmacological
Review title Date of search No. studies in-
cluded
Inclusion crite-
ria for “Types of
participants”
Comparison in-
terventions (no.
studies)
Outcomes for
which data were
reported
that could be
included in an
analysis
Summary
of quality of evi-
dence in reviews
(risk of bias)
Epidural ropiva-
caine ver-
sus bupivacaine
for labor: a meta-
analysis
(Halpern 2003a)
15 March 2002 23 studies
(2074 women)
Labouring
women
Ropivacaine ver-
sus bupivacaine
(23 studies, 2074
women)
• Pain
intensity (time
to onset of
analgesia)
• Satisfaction
with pain relief
(numbers with
“excellent
analgesia”)
• Assisted
vaginal birth
• Caesarean
section
• Side effects
for mother
As-
sessed the quality
of studies using
the Jadad quality
index score. This
scale has a maxi-
mum of 5 points.
Studie are con-
sid-
ered high quality
if the score is 3 or
more
Score of 5: 4
studies
65Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 5. Characteristics of included non-Cochrane systematic reviews - pharmacological (Continued)
(hypotension;
nausea or
vomiting)
• Apgar score
less than seven
at five minutes
Score of 4: 8
studies
Score of 3: 5
studies
Score of 2: 1
study
NA (not applica-
ble): 4 studies
1 study unpub-
lished data and
so not assessed
Fetal bradycardia
due to intrathe-
cal opioids for
labour analgesia:
a systematic re-
view
(Mardirosoff
2002)
25 January 2001 24 studies (3513
women)
Labouring
women
Any in-
trathecal opioid
with or without
local anaesthetic
versus any anal-
gesic regimen
that excluded in-
trathecal opioids
(24 studies, 3513
women)
• Assisted
vaginal birth
• Casaerean
section
• Side effects
for mother
(pruritus)
• Side effects
for baby (fetal
heart rate
abnormalities;
fetal
bradycardia)
• Apgar score
less than seven
at five minutes
Assessed
adequacy of ran-
domi-
sation; blinding;
and description
of withdrawals,
according to a
5-point Oxford
scale
Median
quality score was
3.5 (range 1 to 5)
Table 6. Quality of evidence in included Cochrane systematic reviews - non-pharmacological interventions
Review Title Sequence gen-
eration assessed
(% studies low
risk)
Allocation
concealment as-
sessed
(% studies low
risk)
Blinding of par-
ticipants, per-
sonnel and out-
come assessors
assessed
(% studies low
risk)
Incom-
plete outcome
data assessed
(% studies low
risk)
Selec-
tive outcome re-
porting assessed
(% studies low
risk)
Other potential
threats to valid-
ity assessed
(% studies low
risk)
Hyp-
nosis (7 studies)
(Madden 2012)
2 studies (28%) 1 study (14%) Participants
& Personnel - 3
studies (43%)
Outcome asses-
sors - 3 studies
(43%)
3 studies (43%) 3 studies (43%) 3 studies (43%)
Biofeed-
back (4 studies)
(Barragán 2011)
1 study (25%) 0 studies (0%) 0 studies (0%) 2 studies (50%) 1 study (25%) 4 studies (100%)
66Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 6. Quality of evidence in included Cochrane systematic reviews - non-pharmacological interventions (Continued)
Intracutaneous/
subcuta-
neous sterile wa-
ter injection (7
studies) (Derry
2012)
4 studies (57%) 4 studies (57%) Participants
& Personnel - 5
studies (71%)
Outcome asses-
sors - 7 studies
(100%)
2 studies (29%) 4 studies (57%) 0 studies (0%)
Immer-
sion in water (12
studies) (Cluett
2009)
6 studies (50%) 8 studies (67%) 0 studies (0%) 11 studies (92%) 10 studies (83%) 1 study (8%)
Aromather-
apy (2 studies) (
Smith 2011c)
2 studies (100%) 2 studies (100%) 1 study (50%) 2 studies (100%) 0 studies (0%) 1 study (50%)
Relaxation tech-
niques (11 stud-
ies) (Smith
2011b)
6 studies (54%) 3 studies (27%) 0 studies (0%) 5 studies (45%) 1 study (9%) 5 studies (45%)
Acupuncture (13
studies) (Smith
2011a)
12 studies (92%) 9 studies (69%) 3 studies (23%) 9 studies (69%) 0 studies (0%) 8 studies (62%)
Mas-
sage, reflexology
and other man-
ual methods (6
studies) (Smith
2012)
4 studies (67%) 1 study (17%) Participants
& Personnel - 0
studies (0%)
Outcome asses-
sors - 4 studies
(67%)
5 studies (83%) 1 study (17%) 3 studies (50%)
TENS (18 stud-
ies) (Dowswell
2009)
3 studies (17%) 3 studies (17%) 0 studies (0%) 10 studies (56%) No - NOT AS-
SESSED
0 studies (0%)
Table 7. Quality of evidence in included Cochrane systematic reviews - pharmacological interventions
Review Title Sequence gen-
eration assessed
(% studies low
risk)
Allocation
concealment as-
sessed
(% studies low
risk)
Blinding of par-
ticipants, per-
sonnel and out-
come assessors
assessed
(% studies low
risk)
Incom-
plete outcome
data assessed
(% studies low
risk)
Selec-
tive outcome re-
porting assessed
(% studies low
risk)
Other potential
threats to valid-
ity assessed
(% studies low
risk)
67Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 7. Quality of evidence in included Cochrane systematic reviews - pharmacological interventions (Continued)
Inhaled analge-
sia (26 studies) (
Klomp 2012)
7 studies (27%) 3 studies (12%) Participants/Per-
sonnel - 3 studies
(12%)
Outcome asses-
sors - 3 studies
(12%)
13 studies (50%) 16 studies (62%) 6 studies (23%)
Parenteral opi-
oids for mater-
nal pain manage-
ment in labour
(57 studies)
(Ullman 2010)
13 studies (23%) 17 studies (30%) Participants - 22
studies (39%)
Personnel - 22
studies (39%)
Outcome asses-
sors - 17 studies
(30%)
21 studies (37%) 1 study (2%) 11 studies (19%)
Non-opioid
drugs (18 stud-
ies) (Othman
2012)
6 studies (33%) 5 studies (28%) Participants/Per-
sonnel - 14 stud-
ies (78%)
Outcome asses-
sors - 3 studies
(17%)
16 studies (89%) 12 studies (67%) 13 studies (72%)
Local anaesthetic
nerve blocks (12
studies)
(Novikova 2012)
2 studies (17%) 0 studies (0%) Participants/Per-
sonnel - 4 studies
(34%)
Outcome asses-
sors - 4 studies
(34%)
6 studies (50%) 5 studies (42%) 9 studies (75%)
Epidu-
ral (38 studies)
(Anim-Somuah
2011)
18 studies (47%) 16 studies (42%) Participants - 4
studies (11%)
Personnel - 4
studies (11%)
Outcome asses-
sors - 1 study
(3%)
19 studies (50%) 14 studies (37%) 18 studies (47%)
Combined
spinal epidu-
ral (27 studies) (
Simmons 2012)
11 studies (41%) 14 studies (52%) 15 studies (56%) 25 studies (93%) 23 studies (85%) 3 studies (11%)
N.B. 20 stud-
ies not assessed
(74%)
68Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
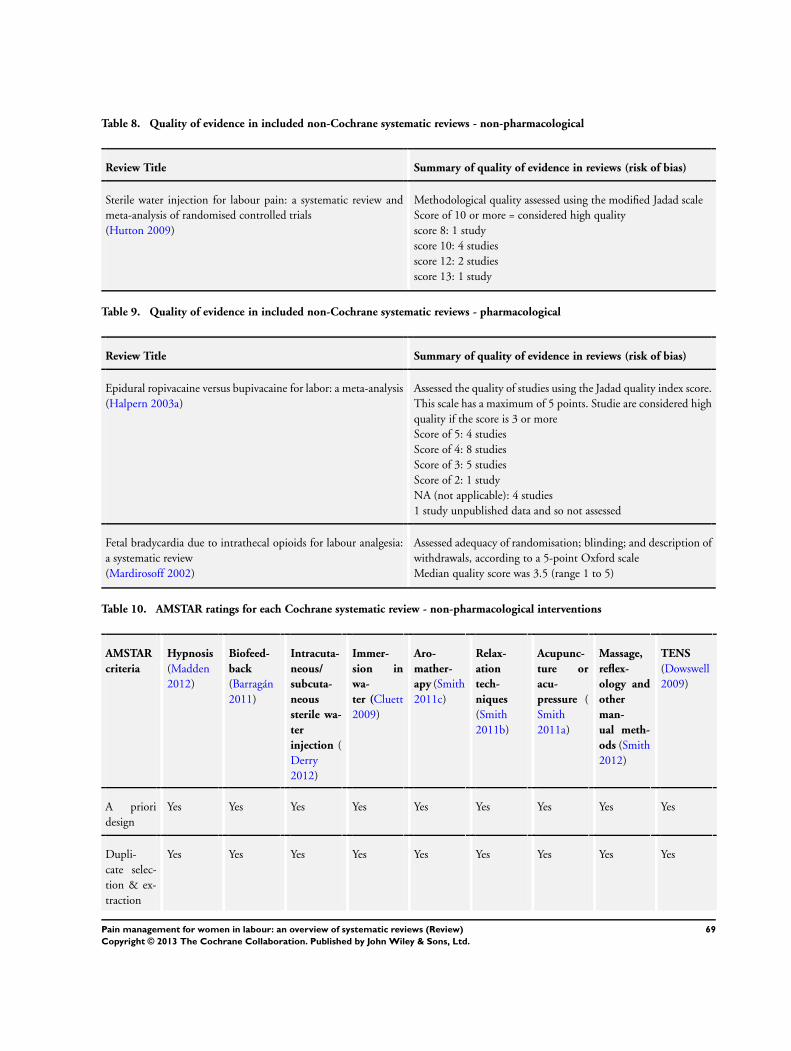
Table 8. Quality of evidence in included non-Cochrane systematic reviews - non-pharmacological
Review Title Summary of quality of evidence in reviews (risk of bias)
Sterile water injection for labour pain: a systematic review and
meta-analysis of randomised controlled trials
(Hutton 2009)
Methodological quality assessed using the modified Jadad scale
Score of 10 or more = considered high quality
score 8: 1 study
score 10: 4 studies
score 12: 2 studies
score 13: 1 study
Table 9. Quality of evidence in included non-Cochrane systematic reviews - pharmacological
Review Title Summary of quality of evidence in reviews (risk of bias)
Epidural ropivacaine versus bupivacaine for labor: a meta-analysis
(Halpern 2003a)
Assessed the quality of studies using the Jadad quality index score.
This scale has a maximum of 5 points. Studie are considered high
quality if the score is 3 or more
Score of 5: 4 studies
Score of 4: 8 studies
Score of 3: 5 studies
Score of 2: 1 study
NA (not applicable): 4 studies
1 study unpublished data and so not assessed
Fetal bradycardia due to intrathecal opioids for labour analgesia:
a systematic review
(Mardirosoff 2002)
Assessed adequacy of randomisation; blinding; and description of
withdrawals, according to a 5-point Oxford scale
Median quality score was 3.5 (range 1 to 5)
Table 10. AMSTAR ratings for each Cochrane systematic review - non-pharmacological interventions
AMSTAR
criteria
Hypnosis
(Madden
2012)
Biofeed-
back
(Barragán
2011)
Intracuta-
neous/
subcuta-
neous
sterile wa-
ter
injection (
Derry
2012)
Immer-
sion in
wa-
ter (Cluett
2009)
Aro-
mather-
apy (Smith
2011c)
Relax-
ation
tech-
niques
(Smith
2011b)
Acupunc-
ture or
acu-
pressure (
Smith
2011a)
Massage,
reflex-
ology and
other
man-
ual meth-
ods (Smith
2012)
TENS
(Dowswell
2009)
A priori
design
Yes Yes Yes Yes Yes Yes Yes Yes Yes
Dupli-
cate selec-
tion & ex-
traction
Yes Yes Yes Yes Yes Yes Yes Yes Yes
69Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 10. AMSTAR ratings for each Cochrane systematic review - non-pharmacological interventions (Continued)
Compre-
hensive lit-
erature
search
Yes Yes Yes Yes Yes Yes Yes Yes Yes
Searched
for reports
regardless
of publica-
tion
type or lan-
guage
Yes Yes Yes Yes Yes Yes Yes Yes Yes
Excluded/
In-
cluded list
provided
Yes Yes Yes Yes Yes Yes Yes Yes Yes
Character-
istics of in-
cluded
studies
provided
Yes Yes Yes Yes Yes Yes Yes Yes Yes
Quality as-
sess-
ment of in-
cluded
studies
assessed &
presented
Yes Yes Yes Yes Yes Yes Yes Yes Yes
Qual-
ity used ap-
propriately
in formu-
lating con-
clusions
Yes Yes Yes Yes Yes Yes Yes Yes Yes
Meth-
ods used to
combine
studies ap-
propriate
Yes Yes Yes Yes Not appli-
cable
Yes Yes Yes Yes
Publi-
cation bias
assessed
Not appli-
cable
Not appli-
cable
Not appli-
cable
Not appli-
cable
Not appli-
cable
Not appli-
cable
Not appli-
cable
Not appli-
cable
Not appli-
cable
70Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 10. AMSTAR ratings for each Cochrane systematic review - non-pharmacological interventions (Continued)
Conflict of
interest
stated
Yes Yes Yes Yes Yes Yes Yes Yes Yes
Total
score (out
of a maxi-
mum of
11)
10 10 10 10 9 10 10 10 10
Table 11. AMSTAR ratings for each Cochrane systematic review - pharmacological interventions
AMSTAR crite-
ria
Inhaled analge-
sia (Klomp
2012)
Opioids
(Ullman 2010)
Non-opioid
drugs (Othman
2012)
Lo-
cal anaesthetic
nerve blocks (
Novikova 2012)
Epidural
(Anim-Somuah
2011)
Combined
spinal epidural
(Simmons 2012)
A priori design Yes Yes Yes Yes Yes Yes
Duplicate selec-
tion & extrac-
tion
Yes Yes Yes Yes Yes Yes
Comprehensive
literature search
Yes Yes Yes Yes Yes Yes
Searched for re-
ports re-
gardless of pub-
lication type or
language
Yes Yes Yes Yes Yes Yes
Excluded/
Included list pro-
vided
Yes Yes Yes Yes Yes Yes
Character-
istics of included
studies provided
Yes Yes Yes Yes Yes Yes
Qual-
ity assessment of
included studies
assessed & pre-
sented
Yes Yes Yes Yes Yes Yes
71Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 11. AMSTAR ratings for each Cochrane systematic review - pharmacological interventions (Continued)
Quality used ap-
propriately in
formulating con-
clusions
Yes Yes Yes Yes Yes Yes
Methods used to
combine studies
appropriate
Yes Yes Yes Yes Yes Yes
Publication bias
assessed
Not applicable
(too few studies
for each outcome
within different
comparisons)
Not applicable
(too few studies
for each outcome
within different
comparisons)
Not applicable
(too few studies
for each outcome
within different
comparisons)
Not applicable
(too few studies
for each outcome
within different
comparisons)
No No
Conflict of inter-
est stated
Yes Yes Yes Yes Yes Yes
Total score (out
of a maximum
of 11)
10 10 10 10 10 10
Table 12. AMSTAR ratings for each non-Cochrane systematic review
AMSTAR cri-
teria
Epidural ropi-
vacaine versus
bupi-
vacaine for la-
bor: a meta-
analysis
(Halpern
2003a)
Fetal brady-
cardia due to
intrathe-
cal opioids for
labour analge-
sia: a system-
atic review
(Mardirosoff
2002)
Ster-
ile water injec-
tion for labour
pain: a system-
atic review and
meta-analysis
of randomised
controlled tri-
als
(Hutton
2009)
A priori design Cannot tell Cannot tell Cannot tell
Duplicate se-
lection & ex-
traction
Yes Yes Yes
Com-
prehensive lit-
erature search
Yes Yes Yes
72Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 12. AMSTAR ratings for each non-Cochrane systematic review (Continued)
Searched for
reports regard-
less of publi-
cation type or
language
No (limited to
English
language pub-
lications)
Yes Yes
Excluded/
Included list
provided
No
(only included
studies)
Yes Yes
Charac-
teristics of in-
cluded studies
provided
Yes Yes Yes
Quality assess-
ment of
included stud-
ies assessed &
presented
Yes Yes Yes
Quality
used appropri-
ately in for-
mulating con-
clusions
No Cannot tell Cannot tell
Methods used
to combine
studies appro-
priate
Yes Yes Yes
Publication
bias assessed
No No No
Conflict of in-
terest stated
No No Yes
Total score
(out of a max-
imum of 11)
4 7 8
73Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
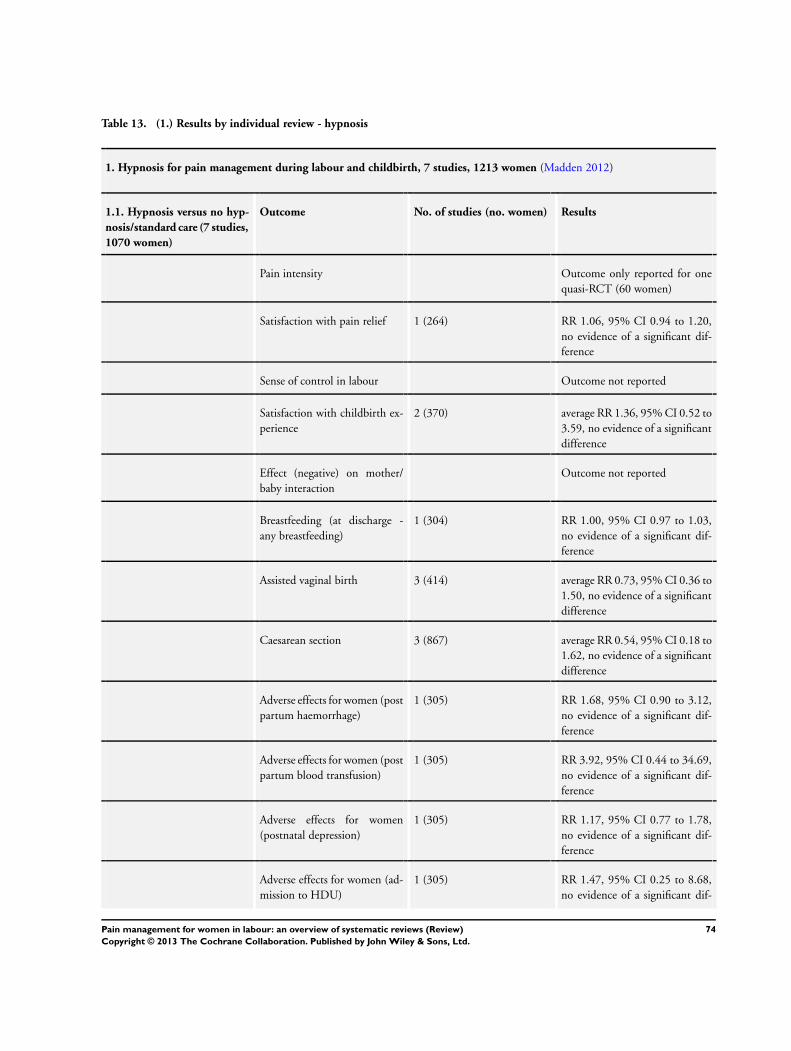
Table 13. (1.) Results by individual review - hypnosis
1. Hypnosis for pain management during labour and childbirth, 7 studies, 1213 women (Madden 2012)
1.1. Hypnosis versus no hyp-
nosis/standard care (7 studies,
1070 women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome only reported for one
quasi-RCT (60 women)
Satisfaction with pain relief 1 (264) RR 1.06, 95% CI 0.94 to 1.20,
no evidence of a significant dif-
ference
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
2 (370) average RR 1.36, 95% CI 0.52 to
3.59, no evidence of a significant
difference
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding (at discharge -
any breastfeeding)
1 (304) RR 1.00, 95% CI 0.97 to 1.03,
no evidence of a significant dif-
ference
Assisted vaginal birth 3 (414) average RR 0.73, 95% CI 0.36 to
1.50, no evidence of a significant
difference
Caesarean section 3 (867) average RR 0.54, 95% CI 0.18 to
1.62, no evidence of a significant
difference
Adverse effects for women (post
partum haemorrhage)
1 (305) RR 1.68, 95% CI 0.90 to 3.12,
no evidence of a significant dif-
ference
Adverse effects for women (post
partum blood transfusion)
1 (305) RR 3.92, 95% CI 0.44 to 34.69,
no evidence of a significant dif-
ference
Adverse effects for women
(postnatal depression)
1 (305) RR 1.17, 95% CI 0.77 to 1.78,
no evidence of a significant dif-
ference
Adverse effects for women (ad-
mission to HDU)
1 (305) RR 1.47, 95% CI 0.25 to 8.68,
no evidence of a significant dif-
74Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 13. (1.) Results by individual review - hypnosis (Continued)
ference
Adverse effects for women
(readmission to hospital)
1 (267) RR 1.56, 95% CI 0.62 to 3.90,
no evidence of a significant dif-
ference
Adverse effects for infants (new-
born resuscitation)
1 (520) RR 0.67, 95% CI 0.11 to 3.96,
no evidence of a significant dif-
ference
Adverse effects for infants (read-
mission to hospital)
1 (267) RR 1.39, 95% CI 0.64 to 3.02,
no evidence of a significant dif-
ference
Admission to special care baby
unit/neonatal intensive care
unit
2 (345) average RR 0.58, 95% CI 0.12 to
2.83, no evidence of a significant
difference
Apgar score less than seven at
five minutes
1 (305) RR 0.49, 95% CI 0.04 to 5.35,
no evidence of a significant dif-
ference
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
1.2. One type of hypnosis ver-
sus another type of hypnosis
(1 study, 297 women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Satisfaction with pain relief 1 (267) RR 1.17, 95% CI 1.02 to 1.34,
no evidence of a significant dif-
ference
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
1 (297) RR 0.96, 95% CI 0.83 to 1.10,
no evidence of a significant dif-
ference
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding (at discharge -
any breastfeeding)
1 (296) RR 0.99, 95% CI 0.97 to 1.02,
no evidence of a significant dif-
ference
75Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
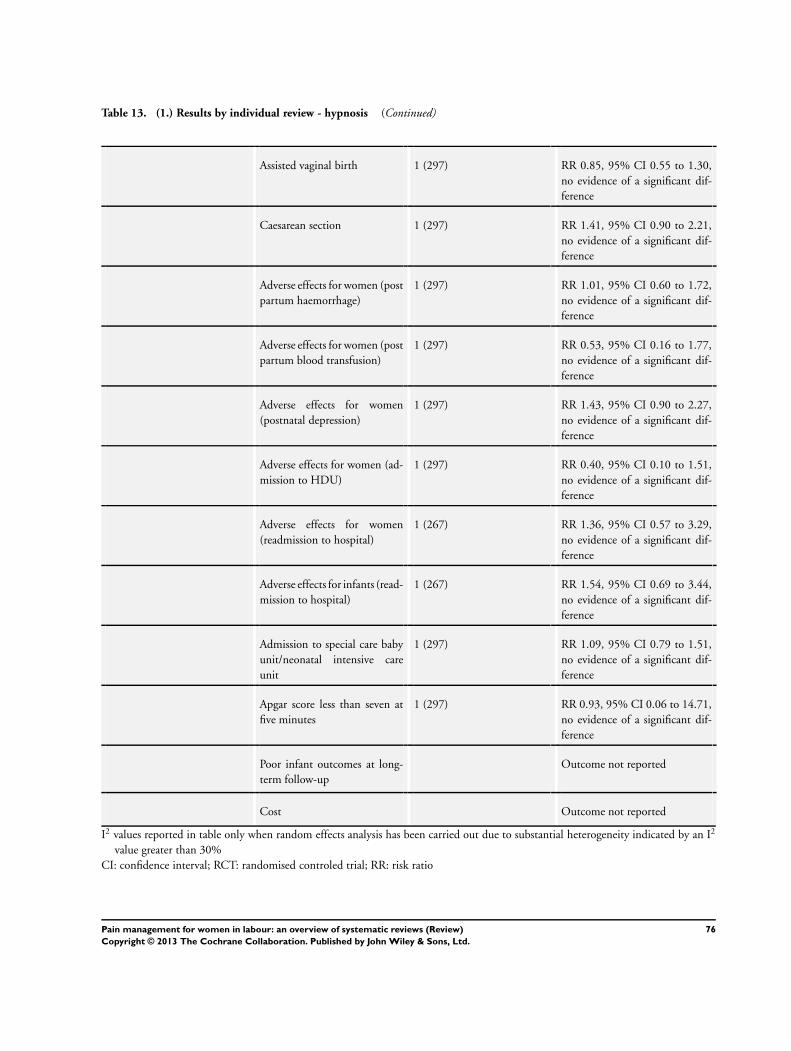
Table 13. (1.) Results by individual review - hypnosis (Continued)
Assisted vaginal birth 1 (297) RR 0.85, 95% CI 0.55 to 1.30,
no evidence of a significant dif-
ference
Caesarean section 1 (297) RR 1.41, 95% CI 0.90 to 2.21,
no evidence of a significant dif-
ference
Adverse effects for women (post
partum haemorrhage)
1 (297) RR 1.01, 95% CI 0.60 to 1.72,
no evidence of a significant dif-
ference
Adverse effects for women (post
partum blood transfusion)
1 (297) RR 0.53, 95% CI 0.16 to 1.77,
no evidence of a significant dif-
ference
Adverse effects for women
(postnatal depression)
1 (297) RR 1.43, 95% CI 0.90 to 2.27,
no evidence of a significant dif-
ference
Adverse effects for women (ad-
mission to HDU)
1 (297) RR 0.40, 95% CI 0.10 to 1.51,
no evidence of a significant dif-
ference
Adverse effects for women
(readmission to hospital)
1 (267) RR 1.36, 95% CI 0.57 to 3.29,
no evidence of a significant dif-
ference
Adverse effects for infants (read-
mission to hospital)
1 (267) RR 1.54, 95% CI 0.69 to 3.44,
no evidence of a significant dif-
ference
Admission to special care baby
unit/neonatal intensive care
unit
1 (297) RR 1.09, 95% CI 0.79 to 1.51,
no evidence of a significant dif-
ference
Apgar score less than seven at
five minutes
1 (297) RR 0.93, 95% CI 0.06 to 14.71,
no evidence of a significant dif-
ference
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; RCT: randomised controled trial; RR: risk ratio
76Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 14. (2.) Results by individual review - biofeedback
2. Biofeedback for pain management during labour, 4 studies, 201 women (Barragán 2011)
2.1. Biofeedback versus no
biofeedback/standard care
Outcome No. of studies (no. women) Results
Pain intensity 3 (193) Data could not be included in
analysis: no data provided for the
control group in one study; data
reported only in a figure in one
study; no numerical data pro-
vided in one study, described nar-
ratively
Satisfaction with pain relief 1 (55) No data provided for the control
group, so data could not be anal-
ysed
Sense of control in labour 1 (55) No data provided for the control
group, so data could not be anal-
ysed
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 2 (103) Average RR 0.75, 95% CI 0.18
to 3.10 (random effects; hetero-
geneity: I2 = 80%, Tau2 = 0.86,
Chi2 test for heterogeneity P = 0.
02), no evidence of a significant
difference
Caesarean section 2 (103) RR 0.41, 95% CI 0.14 to 1.15,
no evidence of a significant dif-
ference
Adverse effects Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
2 (103) Mean values reported without
standard deviations.
77Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 14. (2.) Results by individual review - biofeedback (Continued)
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; RR: risk ratio
Table 15. (3.) Results by individual review - sterile water
3. Intracutaneous or subcutaneous sterile water injection compared with blinded controls for pain management in labour, 7
studies, 766 women (Derry 2012)
3.1.Sterile water injection ver-
sus placebo
Outcome No. of studies (no. women) Results
Intracutaneous sterile water in-
jection versus placebo
Pain intensity Outcome not reported in a suit-
able format
Subcutaneous sterile water in-
jection versus placebo
Pain intensity Outcome not reported in a suit-
able format
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 6 (666) RR 1.31, 95% CI 0.79 to 2.18,
no significant difference between
groups
Caesarean section 7 (766) RR 0.58, 95% CI 0.33 to 1.02,
no significant difference between
groups
Intracutaneous sterile water in-
jection versus placebo
Adverse effects for women -
pain at injection site
1 (62) Outcome data not analysed
78Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 15. (3.) Results by individual review - sterile water (Continued)
Subcutaneous sterile water in-
jection versus placebo
Adverse effects for women -
pain at injection site
1 (62) Outcome data not analysed
Adverse effects for infant Outcome not reported
Admission to neonatal intensive
care unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported in this for-
mat
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; RR: risk ratio
Table 16. (4.) Results by individual review - immersion in water
4. Immersion in water in labour and birth, 12 studies, 3252 women (Cluett 2009)
4.1. Immersion versus no im-
mersion in the first stage
of labour (10 studies, 2932
women)
Outcome No. of studies (no. women) Results
Pain intensity - mean visual ana-
logue pain scores (VAS) at the
start of assessment period
2 (141) MD -0.01, 95% CI -0.54 to 0.
52, no difference between groups
in pain intensity
Pain intensity - mean visual ana-
logue pain scores (VAS) up to
one hour after the start of as-
sessment
2 (141) MD -0.81, 95% CI -1.34 to -0.
28, no difference between groups
in pain intensity
Pain intensity - Ordinal descrip-
tion as moderate to severe, 30
mins after randomisation
1 (120) RR 0.75, 95% CI 0.62 to 0.
91, significantly fewer women
in the immersion group experi-
enced moderate to severe pain
Pain intensity - VAS scale 8 to
10, 30 mins after randomisa-
tion
1 (120) RR 0.72, 95% CI 0.58 to 0.90,
significantly fewer women in the
immersion group had VAS score
79Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 16. (4.) Results by individual review - immersion in water (Continued)
of 8 to 10
Pain intensity - Ordinal scale
pain faces 4 to 5, 30 mins after
randomisation
1 (120) RR 0.67, 95% CI 0.51 to 0.90,
significantly fewer women in the
immersion group had pain faces
4 to 5 on pain scale
Pain intensity - Ordinal descrip-
tion as moderate to severe, 1 hr
after randomisation
1 (117) RR 0.76, 95% CI 0.63 to 0.
91, significantly fewer women
in the immersion group experi-
enced moderate to severe pain
Pain intensity - VAS scale 8 to
10, 1 hr after randomisation
1 (117) RR 1.21, 95% CI 0.69 to 2.11,
no evidence of a significant dif-
ference between groups
Pain intensity - Ordinal scale
pain faces 4 to 5, 1 hr after ran-
domisation
1 (117) RR 0.68, 95% CI 0.53 to 0.86,
significantly fewer women in the
immersion group had pain faces
4 to 5 on pain scale
Pain intensity - Ordinal descrip-
tion as moderate to severe, 2 hrs
after randomisation
1 (57) 0.76, 95% CI 0.59 to 0.98, sig-
nificantly fewer women in the
immersion group experienced
moderate to severe pain
Pain intensity - VAS scale 8 to
10, 2 hrs after randomisation
1 (57) RR 0.83, 95% CI 0.66 to 1.05,
no evidence of a significant dif-
ference between groups
Pain intensity -Ordinal scale
pain faces 4 to 5, 2 hrs after ran-
domisation
1 (57) RR 0.72, 95% CI 0.52 to 0.98,
significantly fewer women in im-
mersion group had pain faces 4
to 5 on pain scale
Pain intensity - Ordinal descrip-
tion as moderate to severe, 3 hrs
after randomisation
1 (32) RR 0.52, 95% CI 0.23 to 1.16,
no evidence of a significant dif-
ference between groups
Pain intensity - VAS scale 8 to
10, 3 hrs after randomisation
1 (32) RR 0.69, 95% CI 0.39 to 1.23,
no evidence of a significant dif-
ference between groups
80Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 16. (4.) Results by individual review - immersion in water (Continued)
Pain intensity - Ordinal scale
pain faces 4 to 5, 3 hrs after ran-
domisation
1 (32) RR 0.57, 95% CI 0.25 to 1.27,
no evidence of a significant dif-
ference between groups
Pain intensity - Ordinal descrip-
tion as moderate to severe, 24
hrs after randomisation
1 (119) RR 0.64, 95% CI 0.50 to 0.
82, significantly fewer women
in the immersion group experi-
enced moderate to severe pain
Pain intensity - VAS scale 8 to
10, 24 hrs after randomisation
1 (119) RR 0.62, 95% CI 0.49 to 0.80,
significantly fewer women in the
immersion group had VAS score
of 8 to 10
Pain intensity - Ordinal scale
pain faces 4 to 5, 24 hrs after
randomisation
1 (119) RR 0.69, 95% CI 0.54 to 0.87,
significantly fewer women in the
immersion group had pain faces
4 to 5 on pain scale
‘ Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding (not breastfeed-
ing after six weeks post delivery)
2 (363) RR 1.17, 95% CI 0.64 to 2.15,
no evidence of a significant dif-
ference between groups
Assisted vaginal birth 7 (2628) RR 0.86, 95% CI 0.71 to 1.05,
no evidence of a significant dif-
ference between groups
Caesarean section 8 (2712) RR 1.21, 95% CI 0.87 to 1.68,
no evidence of a significant dif-
ference between groups
Adverse effects for women
(postpartum haemorrhage)
1 (274) RR 1.58, 95% CI 0.80 to 3.13,
no evidence of a significant dif-
ference between groups
Adverse effects for women
(blood loss - mean blood loss
ml)
2 (153) MD -14.33. 95% CI -63.03 to
34.37, no evidence of a signifi-
cant difference between groups
81Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 16. (4.) Results by individual review - immersion in water (Continued)
Adverse effects for women (per-
ineal trauma - episiotomy)
5 (1272) RR 0.93, 95% CI 0.80 to 1.08,
no evidence of a significant dif-
ference between groups
Adverse effects for women (per-
ineal trauma - second-degree
tear)
5 (1286) RR 0.94, 95% CI 0.74 to 1.20,
no evidence of a significant dif-
ference between groups
Adverse effects for women (per-
ineal trauma - third or fourth
degree tear)
5 (2401) RR 1.37, 95% CI 0.86 to 2.17,
no evidence of a significant dif-
ference between groups
Adverse effects for women (sys-
tolic blood pressure)
1 (120) MD -7.20, 95% CI -13.12 to -1.
28, mean systolic blood pressure
significantly lower in the immer-
sion group
Adverse effects for women (di-
astolic blood pressure)
1 (120) MD -10.20, 95% CI -13.70 to -
6.70, mean diastolic blood pres-
sure significantly lower in the im-
mersion group
Adverse effects for women (ar-
terial blood pressure)
1 (120) MD -10.50, 95% CI -14.68 to
-6.32, mean arterial blood pres-
sure significantly lower in the im-
mersion group
Adverse effects for women (ma-
ternal infection - perineal, sys-
temic, uterine or increase in
temperature)
5 (1295) RR 0.99, 95% CI 0.50 to 1.96,
no significant difference between
groups
Adverse effects for women
(postpartum depression - score
of more than 11 on the Ed-
inburgh Postnatal Depression
Scale EPDS)
2 (370) RR 1.38, 95% CI 0.85 to 2.24,
no significant difference between
groups in the incidence of post-
partum depression
Adverse effects for infants (pres-
ence of meconium stained
liquor)
5 (1260) RR 0.95, 95% CI 0.76 to 1.19,
no evidence of a significant dif-
ference between groups for meco-
nium staining
Adverse effects for infants (ab-
normal fetal heart rate patterns)
3 (487) RR 0.75, 95% CI 0.34 to 1.67,
(random effects; heterogeneity: I2 = 57%, Tau2 = 0.22, Chi2 test
for heterogeneity P = 0.13), no
evidence of a significant differ-
82Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 16. (4.) Results by individual review - immersion in water (Continued)
ence
Adverse effects for infants (um-
bilical artery pH less than 7.20)
1 (110) RR 5.18, 95% CI 0.25 to 105.
51, no evidence of a significant
difference between groups
Adverse effects for infants (tem-
perature greater than 37.8 de-
grees C as an indicator for in-
fection)
1 (274) RR 1.00, 95% CI 0.06 to 15.83,
no evidence of a significant dif-
ference between groups
Adverse effects for infants
(neonatal infection)
5 (1295) RR 2.00, 95% CI 0.50 to 7.94,
no evidence of a significant dif-
ference between groups
Admission to neonatal intensive
care unit
3 (1571) RR 1.06, 95% CI 0.71 to 1.57,
no evidence of a significant dif-
ference between groups
Apgar score less than seven at
five minutes
5 (1834) RR 1.58, 95% CI 0.63 to 3.93,
no evidence of a significant dif-
ference between groups
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
4.1. Immersion versus no im-
mersion in the second stage
of labour (3 studies, 286
women)
Outcome No. of studies (no. women) Results
Pain intensity - number of
women reporting moderate to
severe pain on an ordinal scale
1 (117) RR 1.06, 95% CI 0.73 to 1.53,
no significant difference between
groups in women experiencing
moderate to severe pain
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience (reported that they did
not cope satisfactorily with their
pushing efforts)
1 (117) RR 0.24, 95% CI 0.07 to 0.80,
significantly fewer women in the
immersion group reported low
satisfaction
83Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 16. (4.) Results by individual review - immersion in water (Continued)
Satisfaction with childbirth ex-
perience (satisfaction with
labour and birth on scale of 0-6
where 0 is not at all satisfied)
1 (60) MD 0.03, 95% CI -0.64 to 0.70,
no significant difference between
mean satisfaction scores
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding 1 (60) RR 0.86, 95% CI 0.69 to 1.08,
no evidence of a significant dif-
ference between groups
Assisted vaginal birth 2 (180) RR 0.73, 95% CI 0.21 to 2.54,
no evidence of a significant dif-
ference between groups
Caesarean section 2 (180) RR 0.33, 95% CI 0.07 to 1.52,
no evidence of a significant dif-
ference between groups
Adverse effects for women (per-
ineal trauma - episiotomy)
2 (179) RR 0.75, 95% CI 0.35 to 1.60,
no evidence of a significant dif-
ference between groups
Adverse effects for women (per-
ineal trauma - second-degree
tear)
2 (179) RR 1.21, 95% CI 0.65 to 2.24,
no evidence of a significant dif-
ference between groups
Adverse effects for women (per-
ineal trauma - third or fourth
degree tear)
1 (60) RR 1.54, 95% CI 0.07 to 36.11,
no evidence of a significant dif-
ference between groups
Adverse effects
for women (postpartum haem-
orrhage more than 500 ml)
1 (120) RR 0.14, 95% CI 0.01 to 2.71,
no evidence of a significant dif-
ference between groups
Adverse effects for women (ma-
ternal temperature)
1 (60) MD 0.20, 95% CI -0.18 to 0.58,
no evidence of a significant dif-
ference in mean temperature be-
tween groups
Adverse effects for infants (pres-
ence of meconium stained
liquor)
2 (180) RR 1.32, 95% CI 0.63 to 2.80,
no evidence of a significant dif-
ference between groups
Adverse effects for infants (um-
bilical artery pH less than 7.20)
1 (116) RR 0.89, 95% CI 0.45 to 1.75,
no evidence of a significant dif-
ference between groups
84Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 16. (4.) Results by individual review - immersion in water (Continued)
Adverse effects for infants (an-
tibiotics given to neonate)
1 (60) RR 1.50, 95% CI 0.17 to 13.52,
no evidence of a significant dif-
ference between groups
Adverse effects for infants (posi-
tive neonatal swab of ear, mouth
or umbilicus)
1 (154) RR 1.89, 95% CI 0.90 to 3.96,
no evidence of a significant dif-
ference between groups
Admission to special care baby
unit/neonatal intensive care
unit
2 (180) RR 0.79, 95% CI 0.25 to 2.49,
no evidence of a significant dif-
ference between groups
Apgar score less than seven at
five minutes
1 (119) RR 4.92, 95% CI 0.24 to 100.
31, no evidence of a significant
difference between groups
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
4.2. Early versus late immer-
sion during the first stage of
labour (1 study, 200 women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
Caesarean section Outcome not reported
Adverse effects for women Outcome not reported
85Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
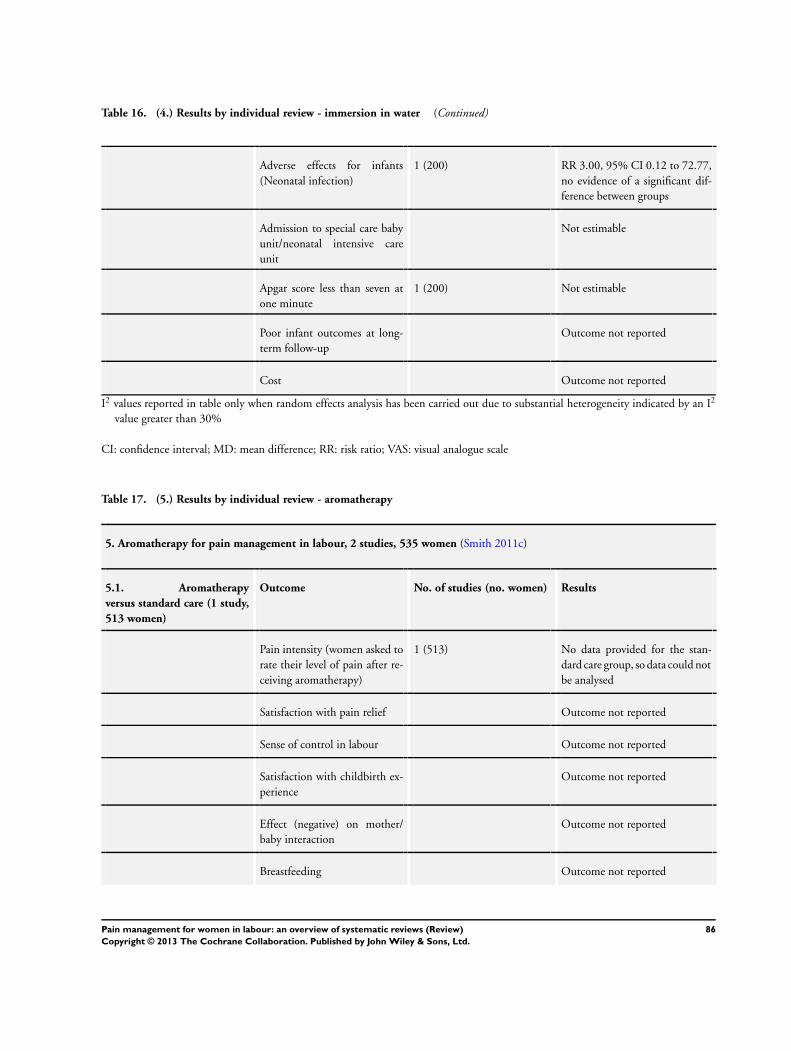
Table 16. (4.) Results by individual review - immersion in water (Continued)
Adverse effects for infants
(Neonatal infection)
1 (200) RR 3.00, 95% CI 0.12 to 72.77,
no evidence of a significant dif-
ference between groups
Admission to special care baby
unit/neonatal intensive care
unit
Not estimable
Apgar score less than seven at
one minute
1 (200) Not estimable
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; MD: mean difference; RR: risk ratio; VAS: visual analogue scale
Table 17. (5.) Results by individual review - aromatherapy
5. Aromatherapy for pain management in labour, 2 studies, 535 women (Smith 2011c)
5.1. Aromatherapy
versus standard care (1 study,
513 women)
Outcome No. of studies (no. women) Results
Pain intensity (women asked to
rate their level of pain after re-
ceiving aromatherapy)
1 (513) No data provided for the stan-
dard care group, so data could not
be analysed
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
86Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 17. (5.) Results by individual review - aromatherapy (Continued)
Assisted vaginal birth 1 (513) RR 1.04, 95% CI 0.48 to 2.28,
no evidence of a significant dif-
ference
Caesarean section 1 (513) RR 0.98, 95% CI 0.49 to 1.94,
no evidence of a significant dif-
ference
Adverse effects Not reported in any trial
Admission to special care baby
unit/neonatal intensive care
unit
1 (513) RR 0.08, 95% CI 0.00 to 1.42,
no evidence of a significant dif-
ference
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
5.2. Aromatherapy (ginger)
versus aromatherapy (lemon
grass) (1 study, 22 women)
Outcome No. of studies (no. women) Results
Pain intensity (assessed on a
visual analogue scale before,
during or after the bath and
24 hours post-partum (McGill
Pain Questionnaire)
1 (22) Median values reported and so
data could not be analysed.
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 1 (22) RR 0.83, 95% CI 0.06 to 11.70,
no evidence of a significant dif-
ference
87Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 17. (5.) Results by individual review - aromatherapy (Continued)
Caesarean section 1 (22) RR 2.54, 95% CI 0.11 to 56.25,
no evidence of a significant dif-
ference
Adverse effects for women
(postpartum haemorrhage)
1 (22) No women in either group had a
postpartum haemorrhage
Admission to special care baby
unit/neonatal intensive care
unit
1 (22) No babies in either group were
admitted to NICU
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; RR: risk ratio
Table 18. (6.) Results by individual review - relaxation techniques
6. Relaxation techniques for pain management in labour, 11 studies, 1574 women (Smith 2011b)
6.1. Relaxation (yoga, mu-
sic or audio-analgesia) ver-
sus standard care (11 studies,
1574 women)
Outcome No. of studies (no. women) Results
Relaxation versus standard care Pain intensity (Latent phase)
(method of pain assessment not
reported)
1 (40 women) MD -1.25, 95% CI -1.97 to -0.
53, a significant reduction in pain
intensity for women receiving in-
struction on relaxation
Pain intensity (Active phase)
(method of pain assessment not
reported)
2 (74 women) MD -2.48, 95% CI -3.13 to -1.
83, a significant reduction in pain
intensity for women receiving in-
struction on relaxation
Pain intensity (memory of pain
at 3 months follow-up assessed
using a Lickert scale from 1 to
7, where 7 is “worst imaginable
pain”)
1 (904) MD 0.00, 95% CI -0.22 to 0.
22, no evidence of a significant
difference
88Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 18. (6.) Results by individual review - relaxation techniques (Continued)
Relaxation versus standard care Satisfaction with pain relief
(postnatal interview 2 hours af-
ter delivery)
1 (40 women) RR 8.00, 95% CI 1.10 to 58.19,
a significant increase in satisfac-
tion for women receiving relax-
ation
Relaxation versus standard care Sense of control in labour Outcome not reported
Relaxation versus standard care Satisfaction with childbirth ex-
perience (Wijma
Delivery Experience Question-
naire 3 months postnatal)
1 (904) MD -0.40, 95% CI -3.47 to 2.
67, no evidence of a significant
difference (analysis adjusted for
clustering)
Relaxation versus standard care Effect on mother/baby interac-
tion
Outcome not reported
Relaxation versus standard care Breastfeeding Outcome not reported
Relaxation versus standard care Assisted vaginal birth 2 (86 women) RR 0.07, 95% CI 0.01 to 0.50,
significantly fewer women had
assisted vaginal birth in the relax-
ation group
Assisted vaginal birth 1 (904 women) cluster trial RR 1.15, 95% CI 0.82 to 1.61,
no evidence of a significant dif-
ference
Relaxation versus standard care Caesarean section 3 (990 women) Data from trials not combined in
a meta-analysis (2 parallel trials
and 1 cluster trial) due to consid-
erable heterogeneity
Relaxation versus standard care Averse effects (for women and
infants)
Outcome not reported
Relaxation versus standard care Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Relaxation versus standard care Apgar score less than seven at
five minutes
1 (34 women) RR 0.47, 95% CI 0.02 to 10.69,
no evidence of a significant dif-
ference
Relaxation versus standard care Poor infant outcomes at long-
term follow-up
Outcome not reported
Relaxation versus standard care Cost Outcome not reported
89Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
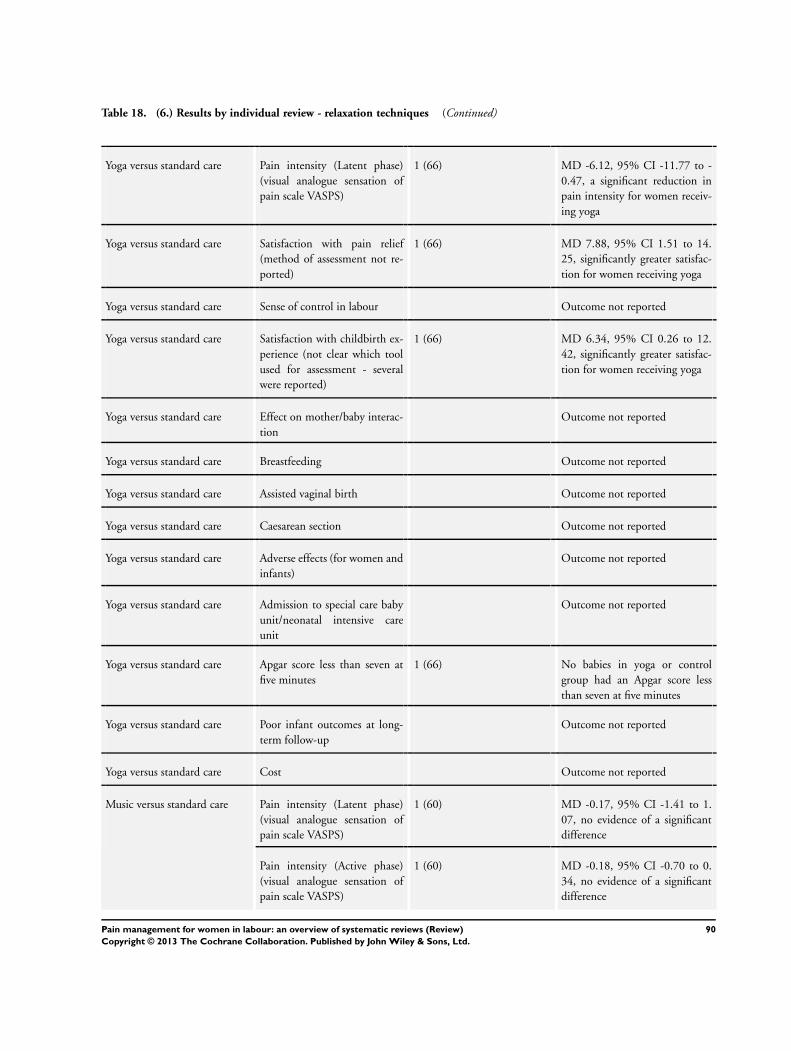
Table 18. (6.) Results by individual review - relaxation techniques (Continued)
Yoga versus standard care Pain intensity (Latent phase)
(visual analogue sensation of
pain scale VASPS)
1 (66) MD -6.12, 95% CI -11.77 to -
0.47, a significant reduction in
pain intensity for women receiv-
ing yoga
Yoga versus standard care Satisfaction with pain relief
(method of assessment not re-
ported)
1 (66) MD 7.88, 95% CI 1.51 to 14.
25, significantly greater satisfac-
tion for women receiving yoga
Yoga versus standard care Sense of control in labour Outcome not reported
Yoga versus standard care Satisfaction with childbirth ex-
perience (not clear which tool
used for assessment - several
were reported)
1 (66) MD 6.34, 95% CI 0.26 to 12.
42, significantly greater satisfac-
tion for women receiving yoga
Yoga versus standard care Effect on mother/baby interac-
tion
Outcome not reported
Yoga versus standard care Breastfeeding Outcome not reported
Yoga versus standard care Assisted vaginal birth Outcome not reported
Yoga versus standard care Caesarean section Outcome not reported
Yoga versus standard care Adverse effects (for women and
infants)
Outcome not reported
Yoga versus standard care Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Yoga versus standard care Apgar score less than seven at
five minutes
1 (66) No babies in yoga or control
group had an Apgar score less
than seven at five minutes
Yoga versus standard care Poor infant outcomes at long-
term follow-up
Outcome not reported
Yoga versus standard care Cost Outcome not reported
Music versus standard care Pain intensity (Latent phase)
(visual analogue sensation of
pain scale VASPS)
1 (60) MD -0.17, 95% CI -1.41 to 1.
07, no evidence of a significant
difference
Pain intensity (Active phase)
(visual analogue sensation of
pain scale VASPS)
1 (60) MD -0.18, 95% CI -0.70 to 0.
34, no evidence of a significant
difference
90Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 18. (6.) Results by individual review - relaxation techniques (Continued)
Music versus standard care Satisfaction with pain relief Outcome not reported
Music versus standard care Sense of control in labour Outcome not reported
Music versus standard care Satisfaction with childbirth ex-
perience
Outcome not reported
Music versus standard care Effect on mother/baby interac-
tion
Outcome not reported
Music versus standard care Breastfeeding Outcome not reported
Music versus standard care Assisted vaginal birth Outcome not reported
Music versus standard care Caesarean section 1 (60 women) RR 1.25, 95% CI 0.37 to 4.21,
no evidence of a significant dif-
ference
Music versus standard care Adverse effects (for women and
infants)
Outcome not reported
Music versus standard care Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Music versus standard care Apgar score less than seven at
five minutes
Outcome not reported
Music versus standard care Poor infant outcomes at long-
term follow-up
Outcome not reported
Music versus standard care Cost Outcome not reported
Audio-analgesia versus standard
care
Pain intensity Outcome not reported
Audio-analgesia versus standard
care
Satisfaction with pain relief
(women’s satisfaction with sea
noise)
1 (24) RR 2.00, 95% CI 0.82 to 4.89,
no evidence of a significant dif-
ference
Audio-analgesia versus standard
care
Sense of control in labour Outcome not reported
Audio-analgesia versus standard
care
Satisfaction with childbirth ex-
perience
Outcome not reported
Audio-analgesia versus standard
care
Effect on mother/baby interac-
tion
Outcome not reported
91Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
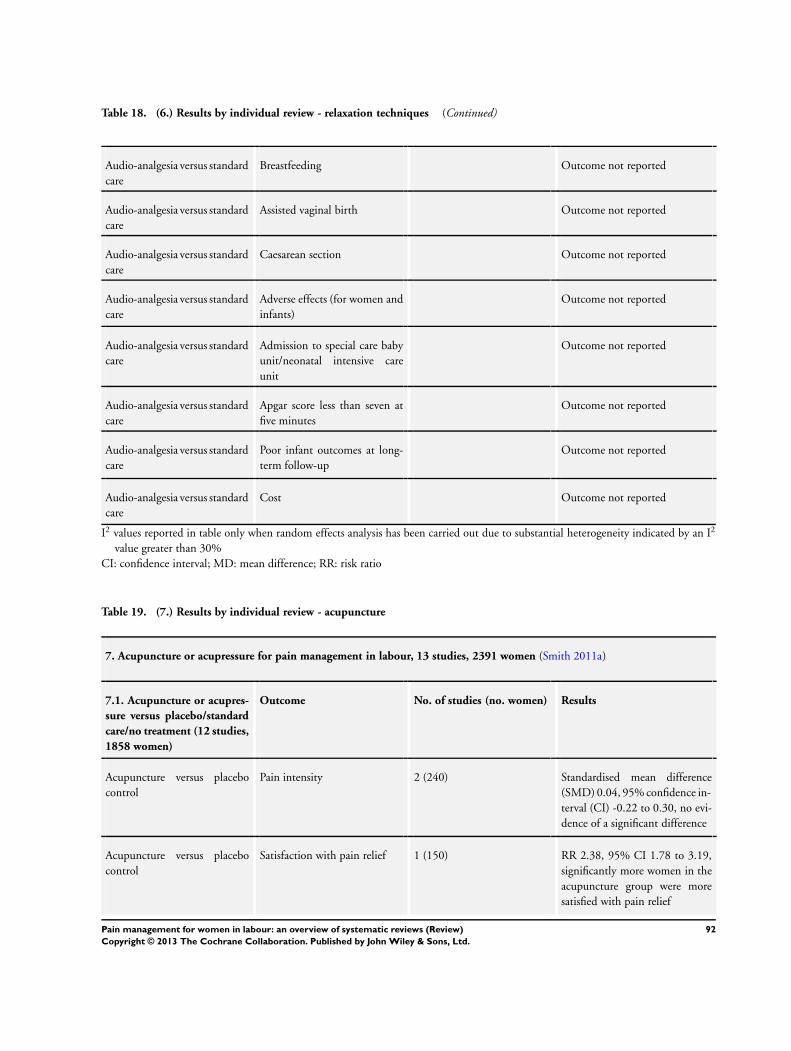
Table 18. (6.) Results by individual review - relaxation techniques (Continued)
Audio-analgesia versus standard
care
Breastfeeding Outcome not reported
Audio-analgesia versus standard
care
Assisted vaginal birth Outcome not reported
Audio-analgesia versus standard
care
Caesarean section Outcome not reported
Audio-analgesia versus standard
care
Adverse effects (for women and
infants)
Outcome not reported
Audio-analgesia versus standard
care
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Audio-analgesia versus standard
care
Apgar score less than seven at
five minutes
Outcome not reported
Audio-analgesia versus standard
care
Poor infant outcomes at long-
term follow-up
Outcome not reported
Audio-analgesia versus standard
care
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; MD: mean difference; RR: risk ratio
Table 19. (7.) Results by individual review - acupuncture
7. Acupuncture or acupressure for pain management in labour, 13 studies, 2391 women (Smith 2011a)
7.1. Acupuncture or acupres-
sure versus placebo/standard
care/no treatment (12 studies,
1858 women)
Outcome No. of studies (no. women) Results
Acupuncture versus placebo
control
Pain intensity 2 (240) Standardised mean difference
(SMD) 0.04, 95% confidence in-
terval (CI) -0.22 to 0.30, no evi-
dence of a significant difference
Acupuncture versus placebo
control
Satisfaction with pain relief 1 (150) RR 2.38, 95% CI 1.78 to 3.19,
significantly more women in the
acupuncture group were more
satisfied with pain relief
92Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 19. (7.) Results by individual review - acupuncture (Continued)
Acupuncture versus placebo
control
Sense of control in labour Outcome not reported
Acupuncture versus placebo
control
Satisfaction with childbirth ex-
perience
Outcome not reported
Acupuncture versus placebo
control
Effect (negative) on mother/
baby interaction
Outcome not reported
Acupuncture versus placebo
control
Breastfeeding Outcome not reported
Acupuncture versus placebo
control
Assisted vaginal birth 1 (208) RR 0.64, 95% CI 0.27 to 1.50,
no evidence of a significant dif-
ference
Acupuncture versus placebo
control
Caesarean section 3 (448) RR 1.39, 95% CI 0.62 to 3.10,
no evidence of a significant dif-
ference
Acupuncture versus placebo
control
Adverse effects Outcome not reported
Acupuncture versus placebo
control
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Acupuncture versus placebo
control
Apgar score less than seven at
five minutes
1 (208) RR 0.32, 95% CI 0.01 to 7.79,
no evidence of a significant dif-
ference
Acupuncture versus placebo
control
Poor infant outcomes at long-
term follow-up
Outcome not reported
Acupuncture versus placebo
control
Cost Outcome not reported
Acupuncture versus standard
care
Pain intensity 1 (90) SMD -0.14, 95% CI -0.55 to 0.
28, no evidence of a significant
difference
Acupuncture versus standard
care
Satisfaction with pain relief 1 (90) RR 1.08, 95% CI 0.95 to 1.22,
no evidence of a significant dif-
ference
Acupuncture versus standard
care
Sense of control in labour Outcome not reported
93Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 19. (7.) Results by individual review - acupuncture (Continued)
Acupuncture versus standard
care
Satisfaction with childbirth ex-
perience
Outcome not reported
Acupuncture versus standard
care
Effect (negative) on mother/
baby interaction
Outcome not reported
Acupuncture versus standard
care
Breastfeeding Outcome not reported
Acupuncture versus standard
care
Assisted vaginal birth 3 (704) RR 0.67, 95% CI 0.46 to 0.98,
significantly fewer women in the
acupuncture group had assisted
vaginal birth
Acupuncture versus standard
care
Caesarean section 2 (506) RR 0.86, 95% CI 0.47 to 1.60,
no evidence of a significant dif-
ference
Acupuncture versus standard
care
Adverse effects Outcome not reported
Acupuncture versus standard
care
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Acupuncture versus standard
care
Apgar score less than seven at
five minutes
3 (706) RR 0.60, 95% CI 0.12 to 2.99,
no evidence of a significant dif-
ference
Acupuncture versus standard
care
Poor infant outcomes at long-
term follow-up
Outcome not reported
Acupuncture versus standard
care
Cost Outcome not reported
Acupuncture versus no treat-
ment
Pain intensity 1 (163) SMD -1.00, 95% CI -1.33 to -0.
67, significantly more women in
the acupuncture group reported
less intense pain
Acupuncture versus no treat-
ment
Satisfaction with pain relief Outcome not reported
Acupuncture versus no treat-
ment
Sense of control in labour Outcome not reported
Acupuncture versus no treat-
ment
Satisfaction with childbirth ex-
perience
Outcome not reported
94Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
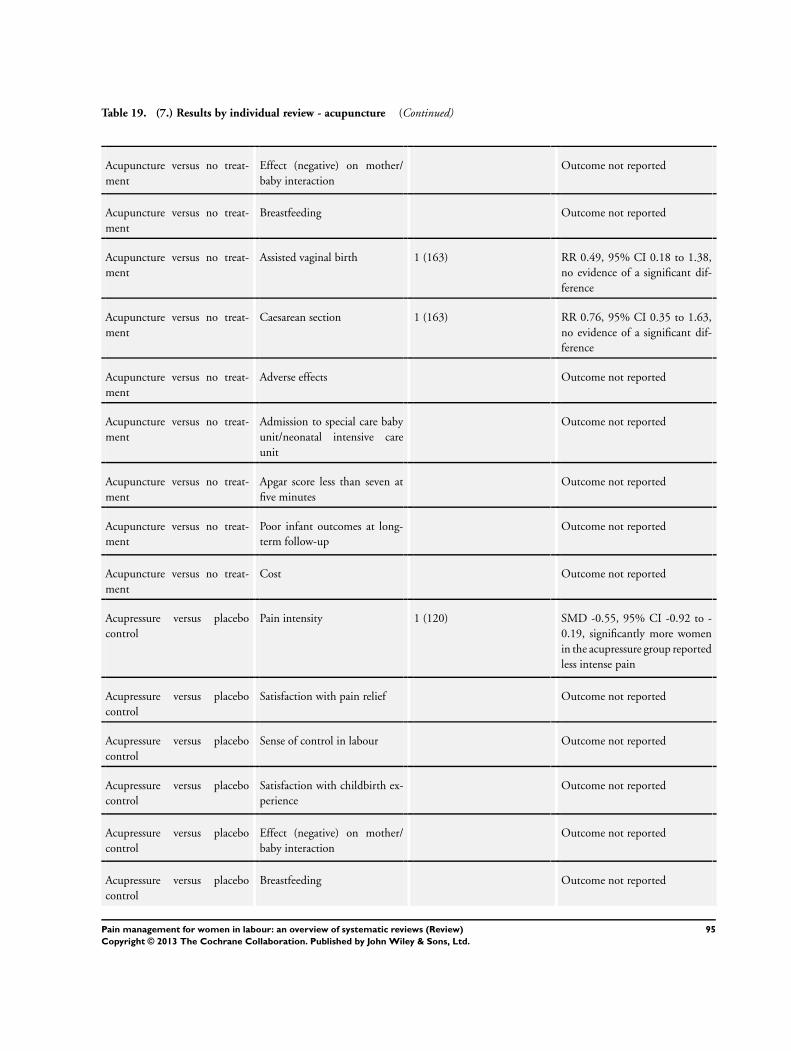
Table 19. (7.) Results by individual review - acupuncture (Continued)
Acupuncture versus no treat-
ment
Effect (negative) on mother/
baby interaction
Outcome not reported
Acupuncture versus no treat-
ment
Breastfeeding Outcome not reported
Acupuncture versus no treat-
ment
Assisted vaginal birth 1 (163) RR 0.49, 95% CI 0.18 to 1.38,
no evidence of a significant dif-
ference
Acupuncture versus no treat-
ment
Caesarean section 1 (163) RR 0.76, 95% CI 0.35 to 1.63,
no evidence of a significant dif-
ference
Acupuncture versus no treat-
ment
Adverse effects Outcome not reported
Acupuncture versus no treat-
ment
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Acupuncture versus no treat-
ment
Apgar score less than seven at
five minutes
Outcome not reported
Acupuncture versus no treat-
ment
Poor infant outcomes at long-
term follow-up
Outcome not reported
Acupuncture versus no treat-
ment
Cost Outcome not reported
Acupressure versus placebo
control
Pain intensity 1 (120) SMD -0.55, 95% CI -0.92 to -
0.19, significantly more women
in the acupressure group reported
less intense pain
Acupressure versus placebo
control
Satisfaction with pain relief Outcome not reported
Acupressure versus placebo
control
Sense of control in labour Outcome not reported
Acupressure versus placebo
control
Satisfaction with childbirth ex-
perience
Outcome not reported
Acupressure versus placebo
control
Effect (negative) on mother/
baby interaction
Outcome not reported
Acupressure versus placebo
control
Breastfeeding Outcome not reported
95Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 19. (7.) Results by individual review - acupuncture (Continued)
Acupressure versus placebo
control
Assisted vaginal birth Outcome not reported
Acupressure versus placebo
control
Caesarean section 1 (120) RR 0.24, 95% CI 0.11 to 0.54,
significantly fewer women in the
acupressure group had caesarean
section
Acupressure versus placebo
control
Adverse effects Outcome not reported
Acupressure versus placebo
control
Admission to special care baby
unit/neonatal intensive care
Outcome not reported
Acupressure versus placebo
control
Apgar score less than seven at
five minutes
Outcome not reported
Acupressure versus placebo
control
Poor infant outcomes at long-
term follow-up
Outcome not reported
Acupressure versus placebo
control
Cost Outcome not reported
Acupressure versus combined
control
Pain intensity 2 (322) SMD -0.42, 95% CI -0.65 to -
0.18, significantly more women
in the acupressure group reported
less intense pain
Acupressure versus combined
control
Satisfaction with pain relief Outcome not reported
Acupressure versus combined
control
Sense of control in labour Outcome not reported
Acupressure versus combined
control
Satisfaction with childbirth ex-
perience
1 (211) MD 4.80, 95% CI -2.29 to 11.
89, no evidence of a significant
difference
Acupressure versus combined
control
Effect (negative) on mother/
baby interaction
Outcome not reported
Acupressure versus combined
control
Breastfeeding Outcome not reported
Acupressure versus combined
control
Assisted vaginal birth 1 (222) RR 0.81, 95% CI 0.39 to 1.67,
no evidence of a significant dif-
ference
96Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 19. (7.) Results by individual review - acupuncture (Continued)
Acupressure versus combined
control
Caesarean section 1 (212) RR 0.48, 95% CI 0.22 to 1.04,
no evidence of a significant dif-
ference
Acupressure versus combined
control
Adverse effects Outcome not reported
Acupressure versus combined
control
Admission to special care baby
unit/neonatal intensive care
Outcome not reported
Acupressure versus combined
control
Apgar score less than seven at
five minutes
1 (120) No infant in either group had an
Apgar score less than seven at five
minutes
Acupressure versus combined
control
Poor infant outcomes at long-
term follow-up
Outcome not reported
Acupressure versus combined
control
Cost Outcome not reported
7.2. Acupuncture versus a dif-
ferent type of acupuncture
(no studies)
7.3.Acupuncture versus ster-
ile water injection (1study,
128 women)
Outcome No. of studies (no. women) Results
Acupuncture versus sterile wa-
ter injection
Pain intensity Outcome not reported
Acupuncture versus sterile wa-
ter injection
Satisfaction with pain relief 1 (128) MD 18.60, 95% CI 11.54 to 25.
66, significantly more women in
the sterile water group were more
satisfied with pain relief
Acupuncture versus sterile wa-
ter injection
Sense of control in labour Outcome not reported
Acupuncture versus sterile wa-
ter injection
Satisfaction with childbirth ex-
perience
Outcome not reported
Acupuncture versus sterile wa-
ter injection
Effect (negative) on mother/
baby interaction
Outcome not reported
Acupuncture versus sterile wa-
ter injection
Breastfeeding Outcome not reported
97Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
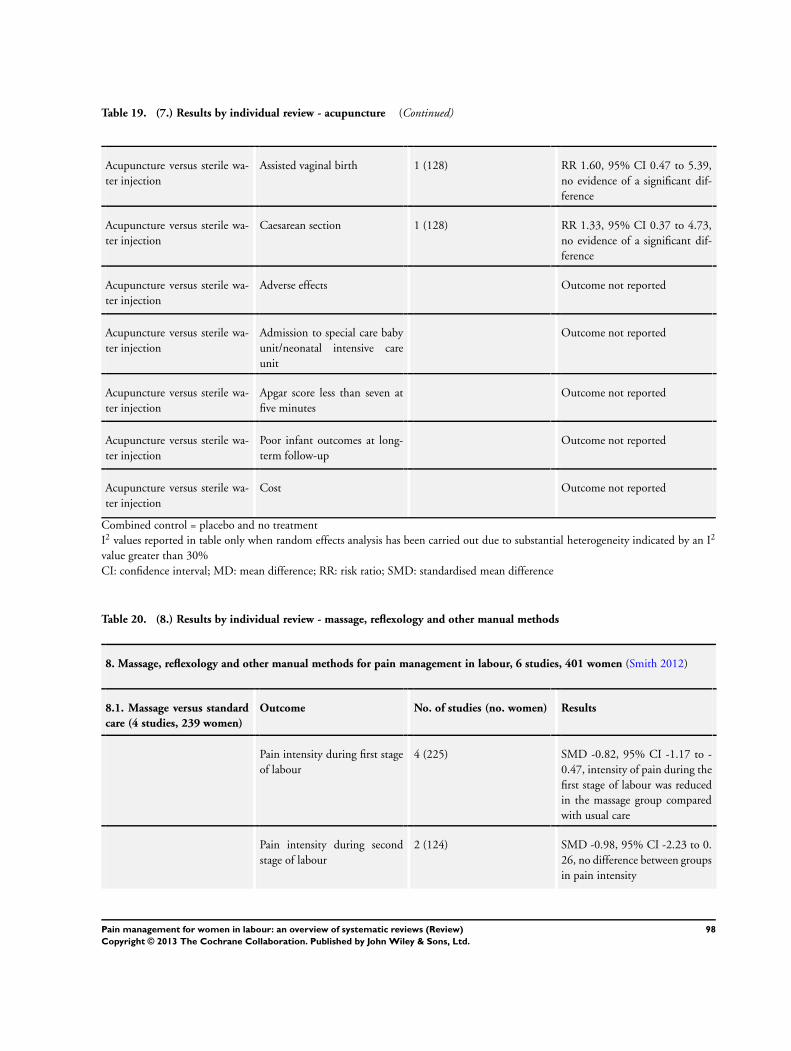
Table 19. (7.) Results by individual review - acupuncture (Continued)
Acupuncture versus sterile wa-
ter injection
Assisted vaginal birth 1 (128) RR 1.60, 95% CI 0.47 to 5.39,
no evidence of a significant dif-
ference
Acupuncture versus sterile wa-
ter injection
Caesarean section 1 (128) RR 1.33, 95% CI 0.37 to 4.73,
no evidence of a significant dif-
ference
Acupuncture versus sterile wa-
ter injection
Adverse effects Outcome not reported
Acupuncture versus sterile wa-
ter injection
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Acupuncture versus sterile wa-
ter injection
Apgar score less than seven at
five minutes
Outcome not reported
Acupuncture versus sterile wa-
ter injection
Poor infant outcomes at long-
term follow-up
Outcome not reported
Acupuncture versus sterile wa-
ter injection
Cost Outcome not reported
Combined control = placebo and no treatment
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; MD: mean difference; RR: risk ratio; SMD: standardised mean difference
Table 20. (8.) Results by individual review - massage, reflexology and other manual methods
8. Massage, reflexology and other manual methods for pain management in labour, 6 studies, 401 women (Smith 2012)
8.1. Massage versus standard
care (4 studies, 239 women)
Outcome No. of studies (no. women) Results
Pain intensity during first stage
of labour
4 (225) SMD -0.82, 95% CI -1.17 to -
0.47, intensity of pain during the
first stage of labour was reduced
in the massage group compared
with usual care
Pain intensity during second
stage of labour
2 (124) SMD -0.98, 95% CI -2.23 to 0.
26, no difference between groups
in pain intensity
98Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 20. (8.) Results by individual review - massage, reflexology and other manual methods (Continued)
Pain intensity during third stage
of labour
2 (122) SMD -1.03, 95% CI -2.17 to 0.
11, no difference between groups
in pain intensity
Satisfaction with pain relief 2 (110) Results not combined for 2 stud-
ies due to heterogeneity
Sense of control in labour 1 (40) MD -6.10, 95% CI -13.11 to 0.
91, no difference between groups
in sense of control in labour
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 2 (105) RR 0.46, 95% CI 0.14 to 1.50,
no evidence of a significant dif-
ference between groups
Caesarean section 2 (105) RR 0.73, 95% CI 0.24 to 2.22,
no evidence of a significant dif-
ference between groups
Adverse effects for women and
infants
Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
1 (44) RR 1.93, 95% CI 0.13 to 28.79,
no evidence of a significant dif-
ference between groups
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
8.2. One manual method ver-
sus different manual method
(no studies)
8.3. Massage versus music (1
study, 101 women)
Outcome No. of studies (no. women) Results
99Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 20. (8.) Results by individual review - massage, reflexology and other manual methods (Continued)
Pain intensity - number of
women reporting severe pain
1 (101) RR 0.40, 95% CI 0.18 to 0.
89, significantly fewer women in
the massage group reported se-
vere pain compared to the music
group
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
Caesarean section Outcome not reported
Adverse effects for women and
infants
Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
8.3. Massage versus breathing
exercises (1 study, 28 women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
100Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 20. (8.) Results by individual review - massage, reflexology and other manual methods (Continued)
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
Caesarean section Outcome not reported
Adverse effects for women and
infants
Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; MD: mean difference; RR: risk ratio; SMD: standardised mean difference
Table 21. (9.) Results by individual review - TENS
9. Transcutaneous electrical nerve stimulation (TENS) for pain management in labour, 17 studies, 1455 women (Dowswell
2009)
9.1. TENS versus placebo
or standard care (17 studies,
1455 women)
Outcome No. of studies (no. women) Results
TENS (to the back) versus
placebo/usual care
Pain intensity - number of
women reporting severe pain
during labour
2 (147) Average RR 0.67, 95% CI 0.32
to 1.40 (random effects; hetero-
geneity: I2 = 49%, Tau2 = 0.18,
Chi2 test for heterogeneity P = 0.
16), no evidence of a significant
difference
TENS (to the back) versus
placebo/usual care
Pain intensity - pain scores 2 (299) Average SMD -1.01, 95% CI -3.
00 to 0.97 (random effects: het-
101Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 21. (9.) Results by individual review - TENS (Continued)
erogeneity: I2 = 93%, Tau2 = 1.
92, Chi2 test for heterogeneity P
= 0.0002), no evidence of a sig-
nificant difference
TEN (to the back) versus
placebo/usual care
Satisfaction with pain relief 5 (452) RR 1.25, 95% CI 0.98 to 1.60,
no evidence of a significant dif-
ference
TENS (to the back) versus usual
care
Sense of control in labour 1 (24) Data not analysed (standard de-
viations inconsistent)
TENS (to the back) versus usual
care
Satisfaction with childbirth ex-
perience
1 (24) Data not analysed (standard de-
viations inconsistent)
TENS (to the back)
versus placebo/usual care
Effect (negative) on mother/
baby interaction
Outcome not reported
TENS (to the back)
versus placebo/usual care
Breastfeeding Outcome not reported
TENS (to the back) versus
placebo/usual care
Assisted vaginal birth 7 (840) RR 0.82, 95% CI 0.56 to 1.19,
no evidence of a significant dif-
ference
TENS (to the back) versus
placebo/usual care
Caesarean section 8 (868) RR 1.35, 95% CI 0.84 to 2.17,
no evidence of a significant dif-
ference
TENS (to the back) versus con-
trol
Adverse effects for infants (fetal
distress)
1 (200) RR 0.33, 95% CI 0.01 to 8.09,
no evidence of a significant dif-
ference
TENS (to the back)
versus placebo/usual care
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
TENS (to the back)
versus placebo/usual care
Apgar score less than seven at
five minutes
Outcome not reported
TENS (to the back)
versus placebo/usual care
Poor infant outcomes at long-
term follow-up
Outcome not reported
TENS (to the back)
versus placebo/usual care
Cost Outcome not reported
TENS (to acupuncture points)
versus placebo
Pain intensity - number of
women reporting severe pain
during labour
2 (290) RR 0.41, 95% CI 0.31 to 0.
54, significantly fewer women in
TENS group reported severe pain
102Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 21. (9.) Results by individual review - TENS (Continued)
compared with controls
TENS (to acupuncture points)
versus control (no pain relief )
Satisfaction with pain relief 1 (90) RR 4.10, 95% CI 1.81 to 9.
29, significantly more women in
TENS group were satisfied with
pain relief compared with con-
trols
TENS (to acupuncture points)
versus placebo/control (no
treatment)
Sense of control in labour Outcome not reported
TENS (to acupuncture points)
versus placebo/control (no
treatment)
Satisfaction with childbirth ex-
perience
Outcome not reported
TENS (to acupuncture points)
versus placebo/control (no
treatment)
Effect (negative) on mother/
baby interaction
Outcome not reported
TENS (to acupuncture points)
versus placebo/control (no
treatment)
Breastfeeding Outcome not reported
TENS (to acupuncture points)
versus placebo
Assisted vaginal birth 1 (100) RR 4.50, 95% CI 1.02 to 19.
79, significantly more women in
TENS group had assisted vaginal
births
TENS (Limoge current to cra-
nium) versus placebo
Assisted vaginal birth 1 (20) RR 0.67, 95% CI 0.14 to 3.17,
no evidence of a significant dif-
ference
TENS (to acupuncture points)
versus placebo
Caesarean section 1 (100) RR 1.50, 95% CI 0.26 to 8.60,
no evidence of a significant dif-
ference
TENS (Limoge current to cra-
nium) versus placebo
Caesarean section 1 (20) RR 1.00, 95% CI 0.07 to 13.87,
no evidence of a significant dif-
ference
TENS (to acupuncture points)
versus placebo
Adverse effects for infants (fetal
distress)
1 (100) RR 1.00, 95% CI 0.06 to 15.55)
, no evidence of a significant dif-
ference
TENS (to acupuncture points)
versus placebo/control (no
treatment)
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
103Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 21. (9.) Results by individual review - TENS (Continued)
TENS (to acupuncture points)
versus placebo/control (no
treatment)
Apgar score less than seven at
five minutes
Outcome not reported
TENS (to acupuncture points)
versus placebo/control (no
treatment)
Poor infant outcomes at long-
term follow-up
Outcome not reported
TENS (to acupuncture points)
versus placebo/control (no
treatment)
Cost Outcome not reported
9.2. TENS versus a different
type of TENS (no studies)
9.3. TENS versus sterile water
injection (1 study, 22 women)
Outcome No. of studies (no. women) Results
Pain intensity - pain score
measured using visual analogue
scale (VAS) in labour
1 (22) SMD 5.45, 95% CI 3.49 to 7.42,
women in the TENS group more
likely to have a higher mean pain
score than women in the ster-
ile water group, “The study mea-
sured pain on a scale with scores
recorded in millimetres, it was
not clear how the 10 cm scale was
labelled and the reported stan-
dard deviations are much smaller
than would be expected with this
type of scale, therefore results
should be interpreted with cau-
tion”
Satisfaction with pain relief Outcome not reported
Sense of control in labour 1 (22) Data not suitable for analysis
Satisfaction with childbirth ex-
perience
1 (22) Data not suitable for analysis
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
104Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 21. (9.) Results by individual review - TENS (Continued)
Caesarean section 1 (22) RR 7.62, 95% CI 0.46 to 126.
40, no evidence of a significant
difference
Adverse effects Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; RR: risk ratio; SMD: standardised mean difference
Table 22. (1.) Results by individual review - inhaled analgesia
1. Inhaled analgesia for pain management in labour, 26 studies, 2967 women (Klomp 2012)
1.1. Inhaled analgesia versus
placebo control/no treatment
(9 studies, 1495 women)
Outcome No. of studies (no. women) Results
Pain intensity during the first
stage of labour (severe/extreme
pain)
2 (310) Average RR 0.06, 95% CI 0.01
to 0.34, (random effects: hetero-
geneity: I2 = 51%, Tau2 = 1.08,
Chi2 test for heterogeneity P =0.
15), significantly fewer women in
the inhaled analgesia group expe-
rienced severe pain
Pain intensity during the first
stage of labour (VAS 0-10 after
one hour)
1 (509) MD -3.50, 95% CI -3.75 to -3.
25, mean pain score was signifi-
cantly lower in the inhaled anal-
gesia group
Satisfaction with pain relief Outcome not reported
105Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 22. (1.) Results by individual review - inhaled analgesia (Continued)
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 1 (200) RR 1.50, 95% CI 0.44 to 5.15,
no evidence of a significant dif-
ference between groups
Caesarean section 3 (465) RR 1.20, 95% CI 0.75 to 1.91,
no evidence of a significant dif-
ference between groups
Adverse effects for women
(vomiting)
2 (619) RR 9.05, 95% CI 1.18 to 69.
32, significantly more women in
the inhaled analgesia group expe-
rienced vomiting
Adverse effects for women (nau-
sea)
1 (509) RR 43.10, 95% CI 2.63 to 706.
74, significantly more women in
the inhaled analgesia group expe-
rienced nausea (very wide CI)
Adverse effects for women
(dizziness)
1 (509) RR 113.98, 95% CI 7.09
to 1833.69, significantly more
women in the inhaled analgesia
group experienced dizziness (ex-
tremely wide CI)
Adverse effects for women
(drowsiness)
1 (509) RR 77.59, 95% CI 4.80 to 1254.
96, significantly more women in
the inhaled analgesia group ex-
perienced drowsiness (extremely
wide CI)
Adverse effects for infants
(neonatal asphyxia)
1 (110) RR 1.11, 95% CI 0.26 to 4.73,
no significant difference between
groups
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
106Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
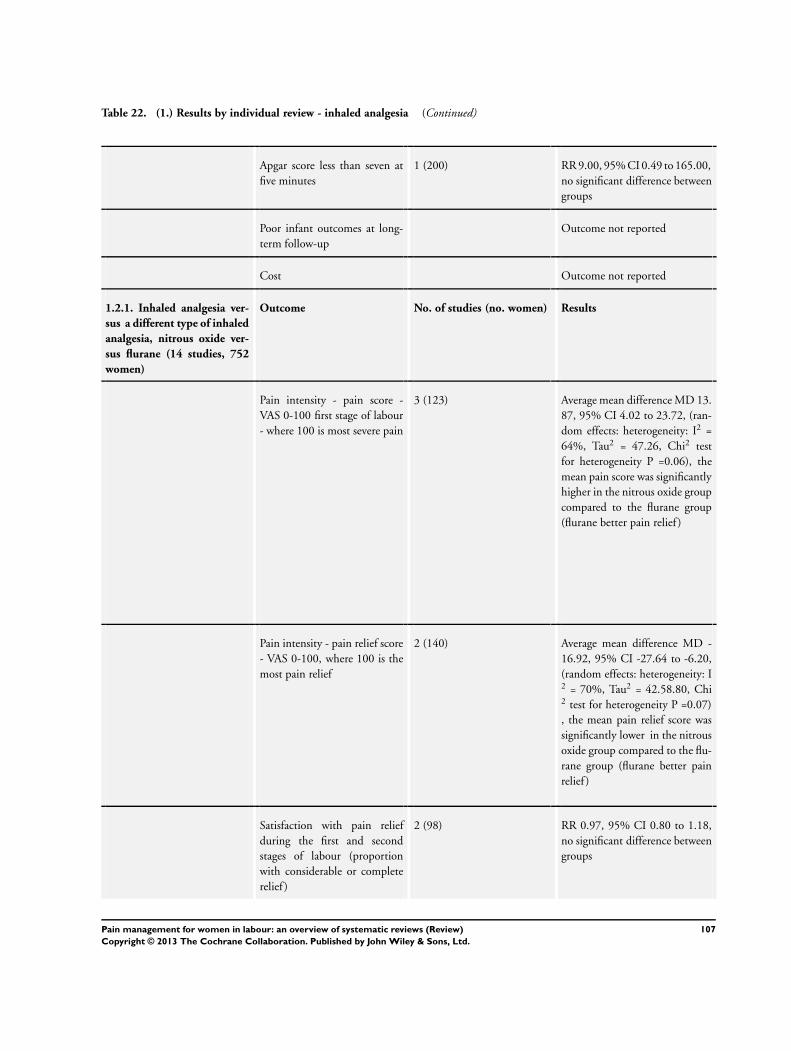
Table 22. (1.) Results by individual review - inhaled analgesia (Continued)
Apgar score less than seven at
five minutes
1 (200) RR 9.00, 95% CI 0.49 to 165.00,
no significant difference between
groups
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
1.2.1. Inhaled analgesia ver-
sus a different type of inhaled
analgesia, nitrous oxide ver-
sus flurane (14 studies, 752
women)
Outcome No. of studies (no. women) Results
Pain intensity - pain score -
VAS 0-100 first stage of labour
- where 100 is most severe pain
3 (123) Average mean difference MD 13.
87, 95% CI 4.02 to 23.72, (ran-
dom effects: heterogeneity: I2 =
64%, Tau2 = 47.26, Chi2 test
for heterogeneity P =0.06), the
mean pain score was significantly
higher in the nitrous oxide group
compared to the flurane group
(flurane better pain relief )
Pain intensity - pain relief score
- VAS 0-100, where 100 is the
most pain relief
2 (140) Average mean difference MD -
16.92, 95% CI -27.64 to -6.20,
(random effects: heterogeneity: I2 = 70%, Tau2 = 42.58.80, Chi2 test for heterogeneity P =0.07)
, the mean pain relief score was
significantly lower in the nitrous
oxide group compared to the flu-
rane group (flurane better pain
relief )
Satisfaction with pain relief
during the first and second
stages of labour (proportion
with considerable or complete
relief )
2 (98) RR 0.97, 95% CI 0.80 to 1.18,
no significant difference between
groups
107Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 22. (1.) Results by individual review - inhaled analgesia (Continued)
Satisfaction with pain relief
during the second stage of
labour (proportion with good
or excellent pain relief )
4 (323) RR 0.89, 95% CI 0.78 to 1.01,
no significant difference between
groups
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 5 (371) RR 0.74, 95% CI 0.51 to 1.05,
there were fewer assisted vaginal
births in the nitrous oxide group,
although this difference did not
reach statistical significance
Caesarean section 1 (98) Not estimable - no CS in either
group
Adverse effects for women (am-
nesia)
4 (281) Average RR 0.26, 95% CI 0.03
to 2.38, (random effects: hetero-
geneity: I2 = 74%, Tau2 = 2.76,
Chi2 test for heterogeneity P =
0.02), there was less amnesia re-
ported in the nitrous oxide group,
although this difference did not
reach statistical significance
Adverse effects for women
(drowsiness)
1 (80) Not estimable - no drowsiness in
either group
Adverse effects for women
(drowsiness), VAS 0-100 mm
2 (57) MD -12.97, 95% CI -22.33 to
-3.62, significantly lower mean
drowsiness score with nitrous ox-
ide compared to flurane group,
(nitrous oxide better)
Adverse effects for women
(dizziness)
2 (204) RR 0.80, 95% CI 0.40 to 1.61,
no evidence of a significant dif-
ference between groups
108Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 22. (1.) Results by individual review - inhaled analgesia (Continued)
Adverse effects for women (nau-
sea)
6 (378) RR 3.30, 95% CI 1.64 to 6.63,
significantly more women in the
nitrous oxide group experienced
nausea compared to the flurane
group
Adverse effects for women
(vomiting)
4 (261) RR 2.66, 95% CI 1.06 to 6.70,
significantly more women in the
nitrous oxide group experienced
vomiting compared to the flurane
group
Adverse effects for women
(blood loss)
2 (185) MD 6.00, 95% CI -32.91 to 44.
91, no significant difference be-
tween groups in blood loss
Adverse effects for infants (neu-
rologic and adaptive capacity
score NACS <35 at 2 hours af-
ter delivery)
3 (170) RR 1.45, 95% CI 0.91 to 2.33,
more babies in the nitrous oxide
group had a NACS score of <35,
although this difference did not
reach statistical significance
Admission to special care baby
unit/neonatal intensive care
Outcome not reported
Apgar score less than seven at
five minutes
6 (409) RR 0.22, 95% CI 0.01 to 4.47,
no significant difference between
groups (N.B. 5 of trials had no
babies with Apgar score less than
seven at five minutes)
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
1.2.2. Inhaled analgesia of
one strength versus a differ-
ent strength (2 studies, 625
women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Satisfaction with pain relief
during the first stage of labour
(good to complete pain relief )
1 (501) RR 1.05, 95% CI 0.94 to 1.
17, no significant difference be-
tween 50% and 70% nitrous ox-
ide groups
109Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 22. (1.) Results by individual review - inhaled analgesia (Continued)
Satisfaction with pain relief
during the second stage of
labour (good to complete relief )
1 (501) RR 0.97, 95% CI 0.87 to 1.
08, no significant difference be-
tween 50% and 70% nitrous ox-
ide groups
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 1 (501) RR 0.83, 95% CI 0.61 to 1.
14, fewer assisted vaginal births
in the 50% nitrous oxide group,
although this difference did not
reach statistical significance
Caesarean section 1 (501) RR 0.31, 95% CI 0.06 to 1.
53, fewer caesarean sections in
the 50% nitrous oxide group, al-
though this difference did not
reach statistical significance
Adverse effects for women
(vomiting)
1 (501) RR 1.29, 95% CI 0.86 to 1.94,
less vomiting reported in the 70%
nitrous oxide group, although
this difference did not reach sta-
tistical significance
Adverse effects for women
(postpartum haemorrhage)
1 (501) RR 0.80, 95% CI 0.38 to 1.70,
fewer women experienced post-
partum haemorrhage in the 50%
nitrous oxide group, although
this difference did not reach sta-
tistical significance
Adverse effects for women (hy-
poxaemia)
1 (501) RR 1.00, 95% CI 0.07 to 14.
21, no significant difference be-
tween 50% and 70% nitrous ox-
ide groups
Adverse effects for infants Outcome not reported
110Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 22. (1.) Results by individual review - inhaled analgesia (Continued)
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
1.2.3. Inhaled analgesia using
one type of delivery system
versus a different system (2
studies, 75 women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Nitrous oxide alone versus ni-
trous oxide with nasal supple-
ment
Satisfaction with pain relief
during the first stage of labour
(considerable to complete pain
relief )
1 (42) RR 1.18, 95% CI 0.94 to 1.48,
no significant difference between
groups
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
Methoxyflurane us-
ing Penthrane Analgizer versus
methoxyflurane using Cyprane
inhaler
Caesarean section 1 (26) RR 2.60, 95% CI 0.12 to 58.48,
no significant difference between
groups
Nitrous oxide alone versus ni-
trous oxide with nasal supple-
ment
Adverse effects for women
(vomiting)
1 (49) RR 1.76, 95% CI 0.77 to 4.
00, more vomiting reported in
the nitrous oxide alone group,
although this difference did not
reach statistical significance
111Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
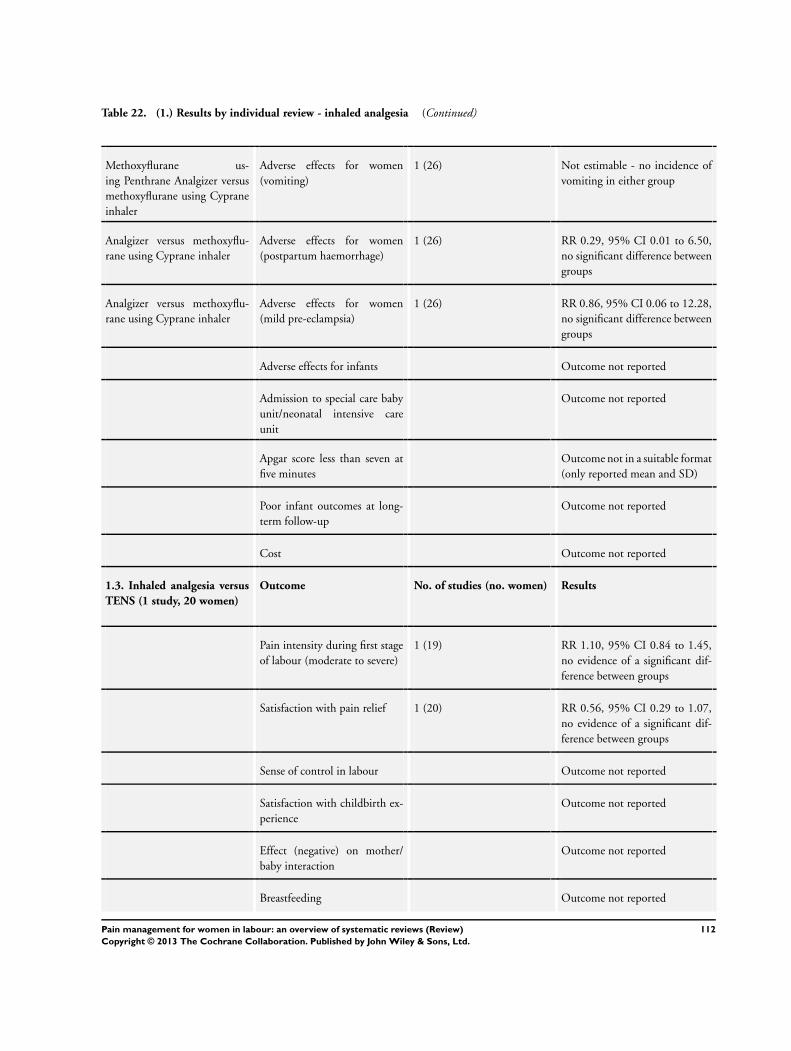
Table 22. (1.) Results by individual review - inhaled analgesia (Continued)
Methoxyflurane us-
ing Penthrane Analgizer versus
methoxyflurane using Cyprane
inhaler
Adverse effects for women
(vomiting)
1 (26) Not estimable - no incidence of
vomiting in either group
Analgizer versus methoxyflu-
rane using Cyprane inhaler
Adverse effects for women
(postpartum haemorrhage)
1 (26) RR 0.29, 95% CI 0.01 to 6.50,
no significant difference between
groups
Analgizer versus methoxyflu-
rane using Cyprane inhaler
Adverse effects for women
(mild pre-eclampsia)
1 (26) RR 0.86, 95% CI 0.06 to 12.28,
no significant difference between
groups
Adverse effects for infants Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not in a suitable format
(only reported mean and SD)
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
1.3. Inhaled analgesia versus
TENS (1 study, 20 women)
Outcome No. of studies (no. women) Results
Pain intensity during first stage
of labour (moderate to severe)
1 (19) RR 1.10, 95% CI 0.84 to 1.45,
no evidence of a significant dif-
ference between groups
Satisfaction with pain relief 1 (20) RR 0.56, 95% CI 0.29 to 1.07,
no evidence of a significant dif-
ference between groups
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
112Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 22. (1.) Results by individual review - inhaled analgesia (Continued)
Assisted vaginal birth Outcome not reported
Caesarean section Outcome not reported
Adverse effects for women and
infants
Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported in this for-
mat
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
CI: confidence interval; RR: risk ratio
Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
2. Parenteral opioids for maternal pain management in labour, 57 studies (Ullman 2010)
2.1. Parenteral opioids versus
placebo or no treatment (3
studies 226 women)
Outcome No. of studies (no. women) Results
IM pethidine versus placebo Maternal pain relief 30 minutes
after drug administration, de-
fined as a reduction in visual
analogue scale (VAS) score of at
least 40 mm
1 (50) RR 25.00, 95% CI 1.56 to 400.
54, significantly more women in
the pethidine group had a greater
reduction in pain score, CI very
wide
IM pethidine versus placebo Maternal satisfaction 30 min-
utes after administration of
study drug
1 (50) RR 7.00, 95% CI 0.38 to 128.
87, no evidence of a significant
difference
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
113Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
Breastfeeding Outcome not reported
IM pethidine versus placebo Assisted vaginal birth 1 (50) RR 0.86, 95% CI 0.34 to 2.19,
no evidence of a significant dif-
ference
IM pethidine versus placebo Caesarean section 1 (50) RR 0.83, 95% CI 0.29 to 2.38,
no evidence of a significant dif-
ference
IM pethidine versus placebo Adverse effects for women -
Nausea and vomiting
2 (166) RR 1.47, 95% CI 0.65 to 3.31,
no evidence of a significant dif-
ference
IM pethidine versus placebo Adverse effects for infants -
Neonatal resuscitation
1 (50) RR 1.67, 95% CI 0.45 to 6.24,
no evidence of a significant dif-
ference
IM pethidine versus placebo Admission to special care baby
unit/neonatal intensive care
unit
1 (50) RR 1.00, 95% CI 0.07 to 15.12,
no evidence of a significant dif-
ference
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at follow-
up
Outcome not reported
Cost Outcome not reported
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Pain intensity No. of studies (no. women) Results
IM meptazinol versus IM pethi-
dine
Assessment of analgesic effect
measured at 3 to 5 days post-
partum (not defined how mea-
sured)
1 (801) RR 1.01, 95% CI 0.91 to 1.12,
no evidence of a significant dif-
ference
Pain intensity one hour after
drug administration - rated as
severe on five-point scale
2 (239) average RR 1.11, 95% CI 0.69
to 1.80 (random effects; hetero-
geneity: I2 = 43%, Tau2 = 0.08,
Chi2 test for heterogeneity P = 0.
18), no evidence of a significant
difference
114Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
PCA (IM) meptazinol versus
PCA (IM) pethidine
Pain scores measured one day
postpartum
1 (10) MD -17.60, 95% CI -49.93 to
14.73, no evidence of a signifi-
cant difference
IM diamorphine + prochlor-
perazine versus IM pethidine +
prochlorperazine
Global assessment of pain relief
evaluated at 24 hours - rated as
‘fair’ or ‘poor’ pain relief
1 (133) RR 0.88, 95% CI 0.67 to 1.16,
no evidence of a significant dif-
ference
Pain intensity rated as moder-
ate or severe one hour after drug
administration
1 (133) RR 0.85, 95% CI 0.72 to 1.01,
no evidence of a significant dif-
ference
IM tramadol versus IM pethi-
dine
Pain intensity (defined in dis-
parate ways in studies) - rated as
‘poor’ pain relief
4 (243) RR 1.56, 95% CI 1.10 to 2.21,
significantly more women had
poor pain relief with tramadol
compared with pethidine
IM dihydrocodeine versus IM
pethidine
Pain intensity rate as ‘poor’ pain
relief one hour after drug ad-
ministration
1 (138) RR 1.09, 95% CI 0.64 to 1.86,
no evidence of a significant dif-
ference
IM pentazocine versus pethi-
dine
Pain intensity rated as ‘good’ or
‘very good’ pain relief at birth
2 (253) RR 1.08, 95% CI 0.92 to 1.27,
no evidence of a significant dif-
ference
IM nalbuphine versus pethi-
dine
Number of women reported as
being ‘free of pain’
1 (40) RR 6.00, 95% CI 0.79 to 45.42,
no evidence of a significant dif-
ference
Pain intensity at 30 minutes,
rated as severe
1 (295) RR 0.86, 95% CI 0.59 to 1.26,
no evidence of a significant dif-
ference
Pain intensity at 60 minutes
(VAS), at peak of contraction
1 (72) MD -8.00, 95% CI -18.55 to 2.
55, no evidence of a significant
difference
IM morphine versus pethidine Number of women rating their
pain relief as ‘poor’
1 (90) RR 1.22, 95% CI 0.56 to 2.66,
no evidence of a significant dif-
ference
IM pentazocine versus IM
pethilorfan
Number of women reporting
‘no pain relief ’ at one hour
1 (69) RR 1.22, 95% CI 0.77 to 1.95,
no evidence of a significant dif-
ference
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Satisfaction with pain relief No. of studies (no. women) Results
115Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
PCA (IM) meptazinol versus
PCA (IM) pethidine
Satisfied with mode of admin-
istration
1 (10) RR 1.00, 95% CI 0.71 to 1.41,
no evidence of a significant dif-
ference
IM pentazocine versus pethi-
dine
Pain relief reported as “poor” or
“partial relief ”
3 (365) RR 1.23, 95% CI 0.74 to 2.05,
no evidence of a significant dif-
ference
IM nalbuphine versus pethi-
dine
Maternal satisfaction with anal-
gesia at 24 hours; numbers dis-
satisfied
1 (72) RR 0.73, 95% CI 0.55 to 0.96,
significantly fewer women in the
nalbuphine group were dissatis-
fied with pain relief
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Satisfation with childbirth ex-
perience
Outcome not reported
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Sense of control in labour Outcome not reported
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Effect on mother/baby inter-
action
Outcome not reported
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Breastfeeding Outcome not reported
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Assisted vaginal birth No. of studies (no. women) Results
IM meptazinol versus IM pethi-
dine
Assisted vaginal birth 3 (1266) RR 1.00, 95% CI 0.81 to 1.22,
no evidence of a significant dif-
ference
Diamor-
phine + prochloprerazine versus
pethidine + prochloprerazine
Assisted vaginal birth 1 (133) RR 0.96, 95% CI 0.46 to 2.02,
no evidence of a significant dif-
ference
IM tramadol versus pethidine Assisted vaginal birth 3 (260) RR 0.56. 95% CI 0.12 to 2.56,
no evidence of a significant dif-
ference
IM pentazocine versus pethi-
dine
Assisted vaginal birth 1 (94) RR 5.22, 95% CI 0.63 to 42.97,
no evidence of a significant dif-
ference
116Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
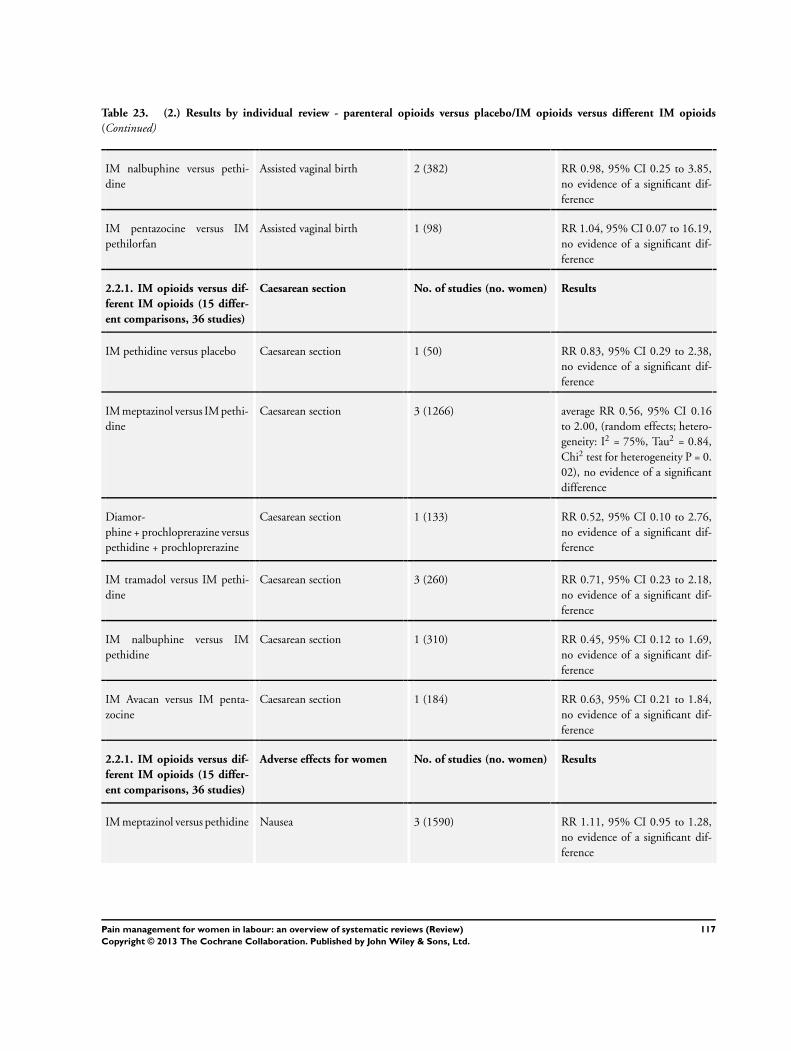
Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
IM nalbuphine versus pethi-
dine
Assisted vaginal birth 2 (382) RR 0.98, 95% CI 0.25 to 3.85,
no evidence of a significant dif-
ference
IM pentazocine versus IM
pethilorfan
Assisted vaginal birth 1 (98) RR 1.04, 95% CI 0.07 to 16.19,
no evidence of a significant dif-
ference
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Caesarean section No. of studies (no. women) Results
IM pethidine versus placebo Caesarean section 1 (50) RR 0.83, 95% CI 0.29 to 2.38,
no evidence of a significant dif-
ference
IM meptazinol versus IM pethi-
dine
Caesarean section 3 (1266) average RR 0.56, 95% CI 0.16
to 2.00, (random effects; hetero-
geneity: I2 = 75%, Tau2 = 0.84,
Chi2 test for heterogeneity P = 0.
02), no evidence of a significant
difference
Diamor-
phine + prochloprerazine versus
pethidine + prochloprerazine
Caesarean section 1 (133) RR 0.52, 95% CI 0.10 to 2.76,
no evidence of a significant dif-
ference
IM tramadol versus IM pethi-
dine
Caesarean section 3 (260) RR 0.71, 95% CI 0.23 to 2.18,
no evidence of a significant dif-
ference
IM nalbuphine versus IM
pethidine
Caesarean section 1 (310) RR 0.45, 95% CI 0.12 to 1.69,
no evidence of a significant dif-
ference
IM Avacan versus IM penta-
zocine
Caesarean section 1 (184) RR 0.63, 95% CI 0.21 to 1.84,
no evidence of a significant dif-
ference
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Adverse effects for women No. of studies (no. women) Results
IM meptazinol versus pethidine Nausea 3 (1590) RR 1.11, 95% CI 0.95 to 1.28,
no evidence of a significant dif-
ference
117Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
IM meptazinol versus pethidine Vomiting 3 (1589) RR 1.25, 95% CI 1.06 to 1.
47, significantly more women re-
ported vomiting with meptazinol
compared with pethidine
IM meptazinol versus pethidine Maternal sleepiness 3 (1590) average RR 0.55, 95% CI 0.28
to 1.07, (random effects; het-
erogeneity: I2 = 44%, Tau2 =
0.18, Chi2 test for heterogene-
ity P = 0.17), fewer women re-
ported sleepiness in the meptazi-
nol group, although the differ-
ence did not reach statistical sig-
nificance
PCA IM meptazinol versus
PCA IM pethidine
Nausea score in labour (rated 1
day after delivery)
1 (10) MD -8.00, 95% CI -48.70 to 32.
70, no evidence of a significant
difference
PCA IM meptazinol versus
PCA IM pethidine
Drowsiness score in labour
(rated 1 day after delivery)
1 (10) MD 5.60, 95% CI -28.19 to 39.
39, no evidence of a significant
difference
IM diamorphine + prochlor-
perazine versus IM pethidine +
prochlorperazine
Vomiting 1 (133) RR 0.39, 95% CI 0.17 to 0.
86, number of women vomiting
significantly lower with diamor-
phine compared with pethidine
IM diamorphine + prochlor-
perazine versus IM pethidine +
prochlorperazine
Maternal sleepiness (one hour
after study drug administra-
tion)
1 (133) RR 0.93, 95% CI 0.52 to 1.66,
no evidence of a significant dif-
ference
IM tramadol versus pethidine Nausea and vomiting 6 (454) Average RR 0.97, 95% CI 0.34
to 2.76, (random effects; hetero-
geneity: I2 = 72%, Tau2 = 1.09,
Chi2 test for heterogeneity P = 0.
003), no evidence of a significant
difference
IM tramadol versus pethidine Maternal sleepiness 5 (409) RR 0.57, 95% CI 0.33 to 0.97,
(random effects; heterogeneity: I2 = 72%, Tau2 = 0.24, Chi2 test
for heterogeneity P = 0.007), sig-
nificantly fewer women in the
tramadol group reported sleepi-
ness
118Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
IM tramadol + triflupromazine
versus pethidine + triflupro-
mazine
Nausea 1 (40) RR 0.82, 95% CI 0.13 to 5.25,
no evidence of a significant dif-
ference
IM tramadol + triflupromazine
versus pethidine + triflupro-
mazine
Vomiting 1 (40) RR 0.40, 95% CI 0.02 to 9.35,
no evidence of a significant dif-
ference
IM tramadol + triflupromazine
versus pethidine + triflupro-
mazine
Maternal sleepiness 1 (40) RR 2.86, 95% CI 0.68 to 12.12,
sleepiness was more frequently
reported by women who re-
ceived tramadol, though no sta-
tistically significant difference be-
tween groups was detected
IM dihydrocodeine versus IM
pethidine
Nausea and vomiting 1 (138) RR 0.87, 95% CI 0.40 to 1.88,
no evidence of a significant dif-
ference
IM dihydrocodeine versus IM
pethidine
Maternal sleepiness 1 (138) RR 0.67, 95% CI 0.43 to 1.04,
no evidence of a significant dif-
ference
IM pentazocine versus IM
pethidine
Nausea 3 (391) RR 0.46, 95% CI 0.24 to 0.90,
fewer women in the pentazocine
group reported nausea compared
to the pethidine group
IM pentazocine versus IM
pethidine
Vomiting 1 (73) RR 0.92, 95% CI 0.27 to 3.14,
no evidence of a significant dif-
ference
IM pentazocine versus IM
pethidine
Maternal sleepiness 3 (391) RR 1.00, 95% CI 0.89 to 1.12,
no evidence of a significant dif-
ference
IM nalbuphine versus IM
pethidine
Nausea 1 (301) RR 0.62, 95% CI 0.42 to 0.91,
fewer women in the nalbuphine
group reported nausea compared
to the pethidine group
IM nalbuphine versus IM
pethidine
Vomiting 1 (301) RR 0.41, 95% CI 0.22 to 0.76,
fewer women in the nalbuphine
group reported vomiting com-
pared to the pethidine group
IM nalbuphine versus IM
pethidine
Nausea and vomiting 1 (72) RR 0.41, 95% CI 0.18 to 0.94,
fewer women in the nalbuphine
group reported both nausea and
119Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
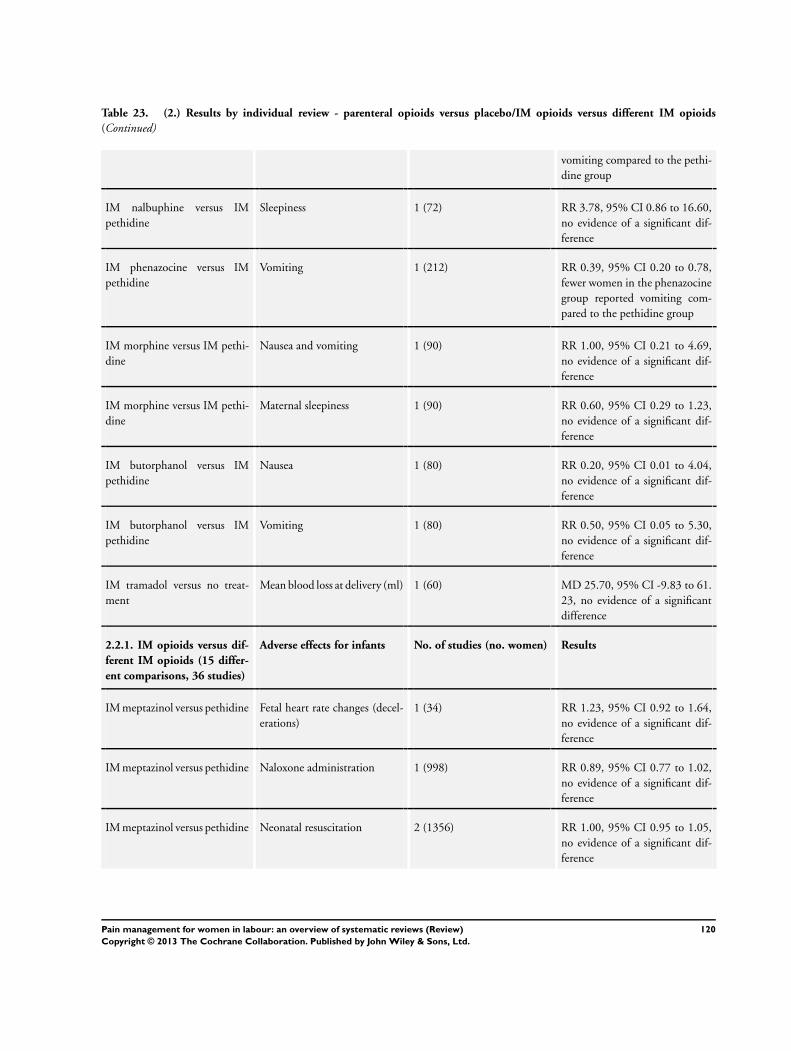
Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
vomiting compared to the pethi-
dine group
IM nalbuphine versus IM
pethidine
Sleepiness 1 (72) RR 3.78, 95% CI 0.86 to 16.60,
no evidence of a significant dif-
ference
IM phenazocine versus IM
pethidine
Vomiting 1 (212) RR 0.39, 95% CI 0.20 to 0.78,
fewer women in the phenazocine
group reported vomiting com-
pared to the pethidine group
IM morphine versus IM pethi-
dine
Nausea and vomiting 1 (90) RR 1.00, 95% CI 0.21 to 4.69,
no evidence of a significant dif-
ference
IM morphine versus IM pethi-
dine
Maternal sleepiness 1 (90) RR 0.60, 95% CI 0.29 to 1.23,
no evidence of a significant dif-
ference
IM butorphanol versus IM
pethidine
Nausea 1 (80) RR 0.20, 95% CI 0.01 to 4.04,
no evidence of a significant dif-
ference
IM butorphanol versus IM
pethidine
Vomiting 1 (80) RR 0.50, 95% CI 0.05 to 5.30,
no evidence of a significant dif-
ference
IM tramadol versus no treat-
ment
Mean blood loss at delivery (ml) 1 (60) MD 25.70, 95% CI -9.83 to 61.
23, no evidence of a significant
difference
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Adverse effects for infants No. of studies (no. women) Results
IM meptazinol versus pethidine Fetal heart rate changes (decel-
erations)
1 (34) RR 1.23, 95% CI 0.92 to 1.64,
no evidence of a significant dif-
ference
IM meptazinol versus pethidine Naloxone administration 1 (998) RR 0.89, 95% CI 0.77 to 1.02,
no evidence of a significant dif-
ference
IM meptazinol versus pethidine Neonatal resuscitation 2 (1356) RR 1.00, 95% CI 0.95 to 1.05,
no evidence of a significant dif-
ference
120Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
PCA IM meptazinol versus
PCA IM pethidine
Naloxone administration 1 (10) RR 1.00, 95% CI 0.08 to 11.93,
no evidence of a significant dif-
ference
IM diamorphine + prochlorpre-
razine versus IM pethidine +
prochlorprerazine
Neonatal resuscitation 1 (133) RR 1.21, 95% CI 0.73 to 2.02,
no evidence of a significant dif-
ference
IM tramadol versus pethidine Neonatal respiratory distress 1 (59) RR 2.26, 95% CI 0.64 to 7.89,
no evidence of a significant dif-
ference
IM pentazocine + promazine
versus IM pethidine + pro-
mazine
Naloxone administration 1 (85) RR 0.49, 95% CI 0.09 to 2.53,
no evidence of a significant dif-
ference
IM nalbuphine versus IM
pethidine
Naloxone administration 1 (72) RR 6.63, 95% CI 0.35 to 123.
93, no evidence of a significant
difference
IM nalbuphine versus IM
pethidine
Neonatal neuro-behavioural 2-
4 hours postnatal
1 (72) MD -3.70, 95% CI -6.14 to
-1.26, babies of women who
received nalbuphine had lower
scores than babies born to women
in the pethidine group
IM butorphanol versus IM
pethidine
Neonatal resuscitation 1 (80) RR 0.33, 95% CI 0.01 to 7.95,
no evidence of a significant dif-
ference
IM butorphanol versus IM
pethidine
Naloxone administration 1 (80) RR 0.33, 95% CI 0.01 to 7.95,
no evidence of a significant dif-
ference
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Admission to special care
baby unit
No. of studies (no. women) Results
IM meptazinol versus pethidine 1 (199) RR 0.88, 95% CI 0.48 to 1.63,
no evidence of a significant dif-
ference
IM diamorphine + prochlorpre-
razine versus IM pethidine +
prochlorprerazine
1 (133) RR 0.58, 95% CI 0.21 to 1.64,
no evidence of a significant dif-
ference
IM tramadol versus IM pethi-
dine
1 (59) RR 2.26, 95% CI 0.64 to 7.89,
no evidence of a significant dif-
ference
121Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 23. (2.) Results by individual review - parenteral opioids versus placebo/IM opioids versus different IM opioids
(Continued)
IM nalbuphine versus IM
pethidine
1 (299) RR 1.07, 95% CI 0.61 to 1.89,
no evidence of a significant dif-
ference
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Apgar score less than seven at
five minutes
No. of studies (no. women) Results
IM meptazinol versus IM pethi-
dine
3 (616) RR 0.49, 95% CI 0.05 to 5.37,
no evidence of a significant dif-
ference
IM diamorphine + prochlorpre-
razine versus IM pethidine +
prochlorprerazine
1 (133) RR 0.35, 95% CI 0.04 to 3.27,
no evidence of a significant dif-
ference
IM pentazocine versus IM
pethidine
1 (62) RR 0.23, 95% CI 0.01 to 4.54,
no evidence of a significant dif-
ference
IM nalbuphine versus IM
pethidine
1 (72) RR 0.47, 95% CI 0.04 to 4.99,
no evidence of a significant dif-
ference
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Poor infant outcomes at fol-
low-up
Outcome not reported
2.2.1. IM opioids versus dif-
ferent IM opioids (15 differ-
ent comparisons, 36 studies)
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; IML intramuscular; MD: mean difference; RR: risk ratio
Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention
Parenteral opioids for maternal pain management in labour, 57 studies (Ullman 2010)
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Pain intensity No. of studies (no. women) Results
122Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
IV fentanyl versus IV pethidine Mean pain score one hour after
drug administration
1 (105) MD -0.20, 95% CI -0.34 to -0.
06, the mean pain score in the IV
fentanyl group was significantly
lower than the mean pain score
in the IV pethidine group
IV butorphanol versus IV
pethidine
Women’s reported mean pain
relief score (not defined)
1 (80) MD 0.67, 95% CI 0.25 to 1.09,
the mean pain relief score was sig-
nificantly higher for the IV bu-
torphanol group compared to the
IV pethidine group
IV butorphanol versus IV
pethidine
Pain score one hour after drug
administration (10-point scale)
1 (80) MD -0.60, 95% CI -1.02 to -0.
18, the mean pain score in the
IV butorphanol group was signif-
icantly lower than the mean pain
score in the IV pethidine group
PCA pentazocine versus PCA
pethidine
Self-reported pain score during
labour
1 (23) SMD -0.76, 95% CI -1.62 to 0.
09, no evidence of a significant
difference
PCA remifentanil versus PCA
pethidine
Mean pain scores at one hour
after drug administration (a vi-
sual analogue scale (VAS) rang-
ing from 0 (“no pain”) to 10 cm
(“worst imaginable pain”)
2 (122) average MD -8.59, 95% CI -27.
61 to 10.44 (random effects; het-
erogeneity: I2 = 62%, T2 = 136.
73, Chi2 test for heterogeneity P
= 0.10), no evidence of a signifi-
cant difference
PCA nalbuphine versus PCA
pethidine
Pain score recorded in labour 1 (60) SMD -0.51, 95% CI -1.02 to 0.
00, no evidence of a significant
difference
PCA fentanyl versus PCA alf-
tentanil
Mean pain scores at 4-6 cm cer-
vical dilatation
1 (21) MD -12.80, 95% CI -32.12 to
6.52, no evidence of a significant
difference
PCA fentanyl versus PCA
pethidine
Mean pain scores at one hour
after drug administration (a vi-
sual analogue scale (VAS) rang-
ing from 0 (“no pain”) to 10 cm
(“worst imaginable pain”)
1 (107) MD -0.65, 95% CI -1.56 to 0.
26, no evidence of a significant
difference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Satisfaction with pain relief No. of studies (no. women) Results
123Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
IV phenazocine versus IV pethi-
dine
Satisfaction with pain relief
(women with fair or poor relief )
1 (194) RR 0.72, 95% CI 0.48 to 1.10,
no evidence of a significant dif-
ference
IV morphine versus IV pethi-
dine
Women satisfied with analgesia
3 days postpartum
1 (141) RR 0.87, 95% CI 0.78 to 0.98,
significantly fewer women in the
IV morphine group were satisfied
with pain relief
PCA nalbuphine versus PCA
pethidine
Measured in the postnatal pe-
riod (rated good or excellent)
1 (60) RR 1.29, 95% CI 0.88 to 1.89,
no evidence of a significant dif-
ference
PCA fentanyl versus PCA alf-
tentanil
Satisfaction with pain relief as
“adequate” or “good” within 6
hours of giving birth
1 (23) RR 1.56, 95% CI 0.93 to 2.60,
no evidence of a significant dif-
ference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Sense of control in labour Outcome not reported
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Satisfaction with childbirth
experience
No. of studies (no. women) Results
PCA remifentanil versus PCA
pethidine
Satisfaction with childbirth ex-
perience
1 (68) MD 1.10, 95% CI 0.46 to 1.74,
no evidence of a significant dif-
ference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Effect on mother/baby inter-
action
Outcome not reported
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Breastfeeding No. of studies (no. women) Results
PCA pentazocine versus PCA
pethidine
Breastfeeding at discharge 1 (23) RR 1.00, 95% CI 0.85 to 1.17,
no evidence of a significant dif-
ference between groups
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Assisted vaginal birth No. of studies (no. women) Results
IV butorphanol versus IV
pethidine
Assisted vaginal birth 1 (200) RR 1.30, 95% CI 0.60 to 2.83,
no evidence of a significant dif-
ference
124Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
PCA remifentanil versus PCA
pethidine
Assisted vaginal birth 2 (97) RR 0.96, 95% CI 0.46 to 2.00,
no evidence of a significant dif-
ference
PCA fentanyl versus PCA
pethidine
Assisted vaginal birth 1 (81) RR 0.57, 95% CI 0.22 to 1.49,
no evidence of a significant dif-
ference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Caesarean Section No. of studies (no. women) Results
IV fentanyl versus IV pethidine Caesarean section 1 (105) RR 1.14, 95% CI 0.24 to 5.40,
no evidence of a significant dif-
ference
IV nalbuphine versus IV pethi-
dine
Caesarean section 1 (28) RR 5.00, 95% CI 0.26 to 95.61,
no evidence of a significant dif-
ference
IV butorphanol versus IV
pethidine
Caesarean section 1 (200) RR 0.80, 95% CI 0.22 to 2.89,
no evidence of a significant dif-
ference
IV fentanyl versus IV butor-
phanol
Caesarean section 1 (100) RR 0.80, 95% CI 0.23 to 2.81,
no evidence of a significant dif-
ference
PCA pentazocine versus PCA
pethidine
Caesarean section 1 (29) RR 0.36, 95% CI 0.02 to 8.07,
no evidence of a significant dif-
ference
PCA remifentanil versus PCA
pethidine
Caesarean section 2 (97) RR 1.81, 95% CI 0.60 to 5.46,
no evidence of a significant dif-
ference
PCA fentanyl versus PCA alf-
tentanil
Caesarean section 1 (23) RR 1.64, 95% CI 0.33 to 8.03,
no evidence of a significant dif-
ference
PCA fentanyl versus PCA
pethidine
Caesarean section 1 (81) RR 0.25, 95% CI 0.03 to 2.34,
no evidence of a significant dif-
ference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Adverse effects for women No. of studies (no. women) Results
125Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
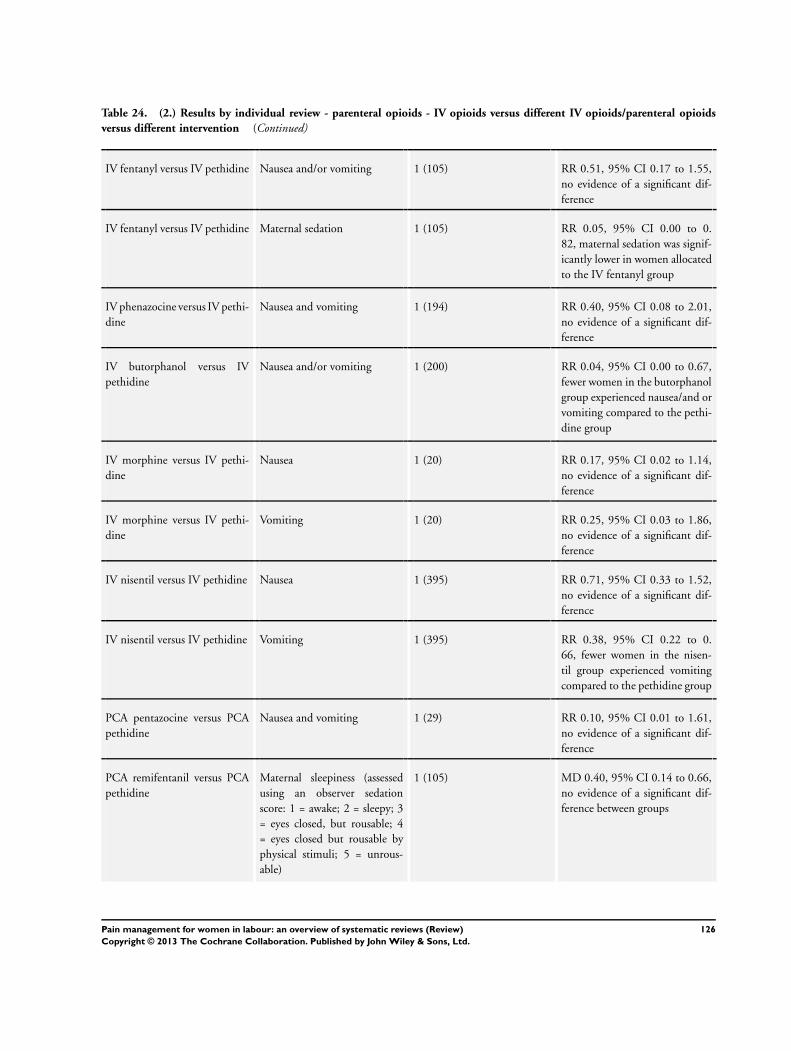
Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
IV fentanyl versus IV pethidine Nausea and/or vomiting 1 (105) RR 0.51, 95% CI 0.17 to 1.55,
no evidence of a significant dif-
ference
IV fentanyl versus IV pethidine Maternal sedation 1 (105) RR 0.05, 95% CI 0.00 to 0.
82, maternal sedation was signif-
icantly lower in women allocated
to the IV fentanyl group
IV phenazocine versus IV pethi-
dine
Nausea and vomiting 1 (194) RR 0.40, 95% CI 0.08 to 2.01,
no evidence of a significant dif-
ference
IV butorphanol versus IV
pethidine
Nausea and/or vomiting 1 (200) RR 0.04, 95% CI 0.00 to 0.67,
fewer women in the butorphanol
group experienced nausea/and or
vomiting compared to the pethi-
dine group
IV morphine versus IV pethi-
dine
Nausea 1 (20) RR 0.17, 95% CI 0.02 to 1.14,
no evidence of a significant dif-
ference
IV morphine versus IV pethi-
dine
Vomiting 1 (20) RR 0.25, 95% CI 0.03 to 1.86,
no evidence of a significant dif-
ference
IV nisentil versus IV pethidine Nausea 1 (395) RR 0.71, 95% CI 0.33 to 1.52,
no evidence of a significant dif-
ference
IV nisentil versus IV pethidine Vomiting 1 (395) RR 0.38, 95% CI 0.22 to 0.
66, fewer women in the nisen-
til group experienced vomiting
compared to the pethidine group
PCA pentazocine versus PCA
pethidine
Nausea and vomiting 1 (29) RR 0.10, 95% CI 0.01 to 1.61,
no evidence of a significant dif-
ference
PCA remifentanil versus PCA
pethidine
Maternal sleepiness (assessed
using an observer sedation
score: 1 = awake; 2 = sleepy; 3
= eyes closed, but rousable; 4
= eyes closed but rousable by
physical stimuli; 5 = unrous-
able)
1 (105) MD 0.40, 95% CI 0.14 to 0.66,
no evidence of a significant dif-
ference between groups
126Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
PCA remifentanil versus PCA
pethidine
Nausea and vomiting 2 (119) RR 0.95, 95% CI 0.61 to 1.49,
no evidence of a significant dif-
ference
PCA nalbuphine versus PCA
pethidine
Nausea and vomiting 1 (59) RR 0.68, 95% CI 0.30 to 1.54,
no evidence of a significant dif-
ference
PCA fentanyl versus PCA alf-
tentanil
Nausea 1 (23) RR 2.73, 95% CI 0.66 to 11.30,
no evidence of a significant dif-
ference
PCA fentanyl versus PCA
pethidine
Maternal sleepiness 1 (107) MD -0.06, 95% CI -0.25 to 0.
13, no evidence of a significant
difference
PCA fentanyl versus PCA
pethidine
Nausea and vomiting 1 (102) RR 0.87, 95% CI 0.55 to 1.37,
no evidence of a significant dif-
ference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Adverse effects for infants No. of studies (no. women) Results
IV fentanyl versus IV pethidine Naloxone administration 1 (105) RR 0.16, 95% CI 0.02 to 1.28,
no evidence of a significant dif-
ference
IV fentanyl versus IV pethidine Babies requiring resuscitation/
ventilatory support
1 (105) RR 1.03, 95% CI 0.46 to 2.32,
no evidence of a significant dif-
ference
IV fentanyl versus IV pethidine Neurobehavioural score (1-2
hours after delivery)
1 (105) MD 1.30, 95% CI 0.15 to 2.45,
no evidence of a significant dif-
ference
IV fentanyl versus IV pethidine Neurobehavioural score (2-24
hours after delivery)
1 (105) MD 0.90, 95% CI -0.42 to 2.
22, no evidence of a significant
difference
IV fentanyl versus IV butor-
phanol
Babies requiring ventilatory
support
1 (100) RR 11.00, 95% CI 0.62 to 193.
80, no evidence of a significant
difference
IV fentanyl versus IV butor-
phanol
Naloxone required 1 (100) RR 1.75, 95% CI 0.81 to 3.80,
no evidence of a significant dif-
ference
127Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
IV fentanyl versus IV butor-
phanol
Neurobehavioural score (2-4
hours after delivery)
1 (100) MD 0.00, 95% CI -1.61 to 1.
61, no evidence of a significant
difference
IV fentanyl versus IV butor-
phanol
Neurobehavioural score (24-36
hours after delivery)
1 (100) MD -0.50, 95% CI -1.62 to 0.
62, no evidence of a significant
difference
PCA remifentanil versus PCA
pethidine
Naloxone administration 2 (56) RR 0.30, 95% CI 0.01 to 6.47,
no evidence of a significant dif-
ference
PCA remifentanil versus PCA
pethidine
Neurobehavioural score (15
minutes post delivery)
1 (56) MD 0.20, 95% CI -0.93 to 1.
33, no evidence of a significant
difference
PCA remifentanil versus PCA
pethidine
Neurobehavioural score (2
hours after delivery)
1 (59) MD 0.60, 95% CI -0.66 to 1.
86, no evidence of a significant
difference
PCA fentanyl versus PCA alf-
tentanil
Naloxone required 1 (24) RR 2.36, 95% CI 0.53 to 10.55,
no evidence of a significant dif-
ference
PCA fentanyl versus PCA
pethidine
Neurobehavioural score (15
minutes post delivery)
1 (63) MD -0.90, 95% CI -2.31 to 0.
51, no evidence of a significant
difference
PCA fentanyl versus PCA
pethidine
Neurobehavioural score (2
hours post delivery)
1 (64) MD -0.50, 95% CI -1.95 to 0.
95, no evidence of a significant
difference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Admission to special care
baby unit/neonatal intensive
care unit
No. of studies (no. women) Results
PCA remifentanil versus PCA
pethidine
1 (17) RR 0.30, 95% CI 0.01 to 6.47,
no evidence of a significant dif-
ference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Apgar score less than seven at
five minutes
No. of studies (no. women) Results
IV fentanyl versus IV pethidine 1 (105) RR 0.38, 95% CI 0.02 to 9.12,
no evidence of a significant dif-
ference
128Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
IV butorphanol versus IV
pethidine
2 (230) RR 1.00, 95% CI 0.06 to 15.77,
no evidence of a significant dif-
ference
IV fentanyl versus IV butor-
phanol
1 (100) RR 1.20, 95% CI 0.39 to 3.68,
no evidence of a significant dif-
ference
PCA remifentanil versus PCA
pethidine
1 (17) RR 0.13, 95% CI 0.01 to 2.16,
no evidence of a significant dif-
ference
PCA nalbuphine versus PCA
pethidine
1 (41) RR 0.42, 95% CI 0.02 to 9.76,
no evidence of a significant dif-
ference
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Poor infant outcomes at fol-
low-up
Outcome not reported
2.2.2. IV opioids versus dif-
ferent IV opioids (12 compar-
isons, 17 studies)
Cost Outcome not reported
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Pain intensity No. of studies (no. women) Results
Opioids (IM pethidine; IM tra-
madol) versus TENS
Pain relief reported as com-
plete, excellent or moderate at
30 minutes after analgesia (1
study), time point not reported
in the other study
2 (290) average RR 1.15, 95% CI 0.81
to 1.61 (random effects; hetero-
geneity: I2 = 64%, T2 = 0.04, Chi2 test for heterogeneity P = 0.10)
, no evidence of a significant dif-
ference
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Satisfaction with pain relief No. of studies (no. women) Results
Opioids (IV pethidine; IM
pethidine) versus TENS
Maternal satisfaction with anal-
gesia measured post delivery
(rated as good)
2 (104) RR 1.23, 95% CI 0.79 to 1.92,
no evidence of a significant dif-
ference
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Sense of control in labour Outcome not reported
129Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
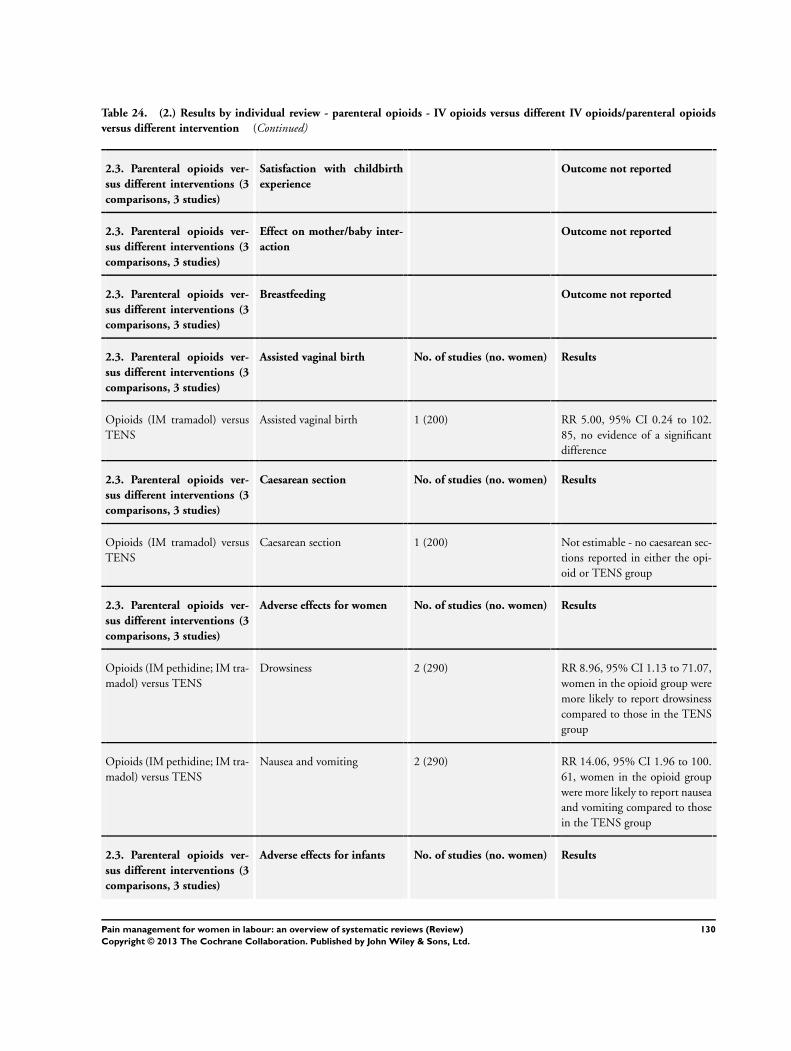
Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Satisfaction with childbirth
experience
Outcome not reported
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Effect on mother/baby inter-
action
Outcome not reported
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Breastfeeding Outcome not reported
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Assisted vaginal birth No. of studies (no. women) Results
Opioids (IM tramadol) versus
TENS
Assisted vaginal birth 1 (200) RR 5.00, 95% CI 0.24 to 102.
85, no evidence of a significant
difference
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Caesarean section No. of studies (no. women) Results
Opioids (IM tramadol) versus
TENS
Caesarean section 1 (200) Not estimable - no caesarean sec-
tions reported in either the opi-
oid or TENS group
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Adverse effects for women No. of studies (no. women) Results
Opioids (IM pethidine; IM tra-
madol) versus TENS
Drowsiness 2 (290) RR 8.96, 95% CI 1.13 to 71.07,
women in the opioid group were
more likely to report drowsiness
compared to those in the TENS
group
Opioids (IM pethidine; IM tra-
madol) versus TENS
Nausea and vomiting 2 (290) RR 14.06, 95% CI 1.96 to 100.
61, women in the opioid group
were more likely to report nausea
and vomiting compared to those
in the TENS group
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Adverse effects for infants No. of studies (no. women) Results
130Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
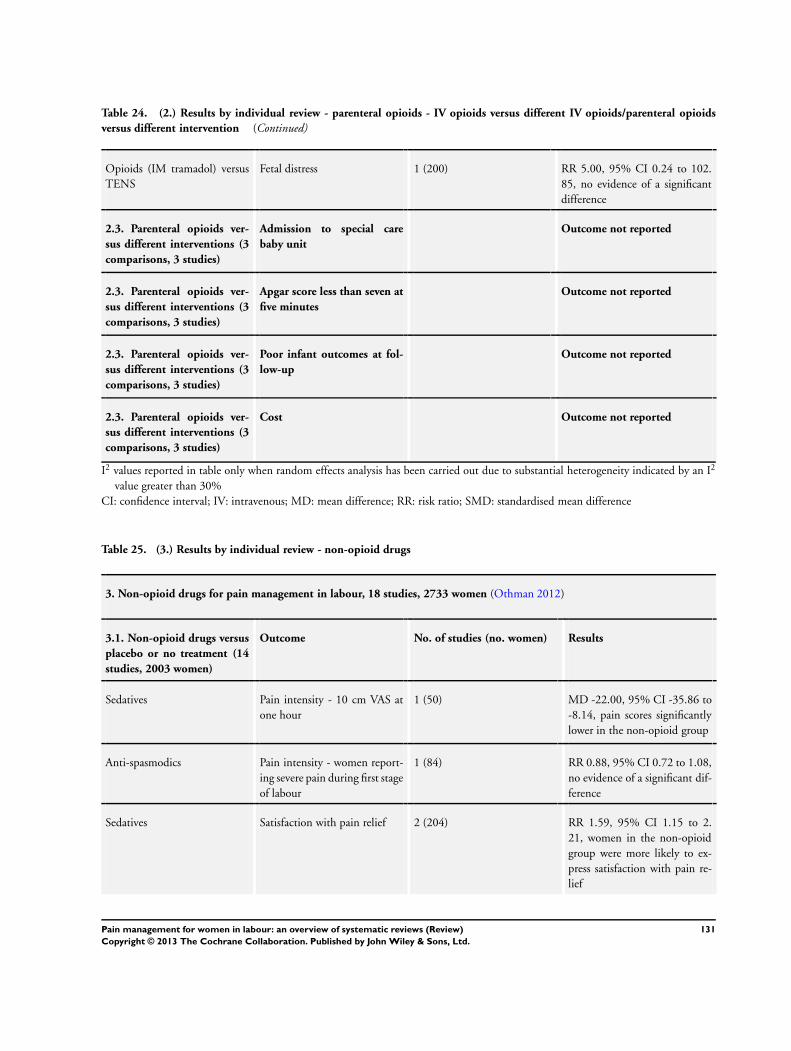
Table 24. (2.) Results by individual review - parenteral opioids - IV opioids versus different IV opioids/parenteral opioids
versus different intervention (Continued)
Opioids (IM tramadol) versus
TENS
Fetal distress 1 (200) RR 5.00, 95% CI 0.24 to 102.
85, no evidence of a significant
difference
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Admission to special care
baby unit
Outcome not reported
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Apgar score less than seven at
five minutes
Outcome not reported
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Poor infant outcomes at fol-
low-up
Outcome not reported
2.3. Parenteral opioids ver-
sus different interventions (3
comparisons, 3 studies)
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; IV: intravenous; MD: mean difference; RR: risk ratio; SMD: standardised mean difference
Table 25. (3.) Results by individual review - non-opioid drugs
3. Non-opioid drugs for pain management in labour, 18 studies, 2733 women (Othman 2012)
3.1. Non-opioid drugs versus
placebo or no treatment (14
studies, 2003 women)
Outcome No. of studies (no. women) Results
Sedatives Pain intensity - 10 cm VAS at
one hour
1 (50) MD -22.00, 95% CI -35.86 to
-8.14, pain scores significantly
lower in the non-opioid group
Anti-spasmodics Pain intensity - women report-
ing severe pain during first stage
of labour
1 (84) RR 0.88, 95% CI 0.72 to 1.08,
no evidence of a significant dif-
ference
Sedatives Satisfaction with pain relief 2 (204) RR 1.59, 95% CI 1.15 to 2.
21, women in the non-opioid
group were more likely to ex-
press satisfaction with pain re-
lief
131Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 25. (3.) Results by individual review - non-opioid drugs (Continued)
Anti-histamines Satisfaction with pain relief 1 (223) RR 1.80, 95% CI 1.16 to 2.
79, 1 trial, women in the non-
opioid group were more likely
to express satisfaction with pain
relief
Sense of control Outcome not reported
Sedatives Satisfaction with childbirth ex-
perience
1 (40) RR 2.16, 95% CI 1.34 to 3.
47, women in the non-opioid
group were more likely to ex-
press satisfaction with the child-
birth experience
Effect (negative) on mother/
baby interaction
Outcome not reported
Sedatives Breastfeeding (no definition of
what was meant by breastfeed-
ing provided in the study)
1 (198) RR 0.65, 95% CI 0.36 to 1.17,
no evidence of a significant dif-
ference
Anti-spasmodics Assisted vaginal birth 1 (84) RR 0.45, 95% CI 0.09 to 2.35,
no evidence of a significant dif-
ference
Sedatives Assisted vaginal birth 3 (417) RR 0.93, 95% CI 0.84 to 1.03,
no evidence of a significant dif-
ference
Anti-histamines Assisted vaginal birth 1 (49) RR 3.12, 95% CI 0.13 to 73.
04, no evidence of a significant
difference
Sedatives Caesarean section 2 (203) RR 3.62, 95% CI 0.40 to 32.
65, no evidence of a significant
difference
Anti-spasmodics Adverse effects for women (Re-
ported adverse effects included
nausea, vomiting, drowsiness,
tachycardia, headache, blurred
vision, dryness of the mouth,
difficulty in micturition, weak-
ness of the legs, hypotension
and atonic postpartum haemor-
rhage)
1 (84) RR 7.27, 95% CI 0.95 to 55.
61, no evidence of a significant
difference
132Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 25. (3.) Results by individual review - non-opioid drugs (Continued)
Sedatives Adverse effects for women (Re-
ported adverse effects included
nausea, vomiting, drowsiness,
tachycardia, headache, blurred
vision, dryness of the mouth,
difficulty in micturition, weak-
ness of the legs, hypotension
and atonic postpartum haemor-
rhage)
3 (216) RR 1.26, 95% CI 0.67 to 2.35,
no evidence of a significant dif-
ference
Sedatives Adverse effects for infants 2 (387) RR 0.85, 95% CI 0.46 to 1.54,
no evidence of a significant dif-
ference
Anti-histamines Adverse effects for infants Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Sedative-analgesics Apgar score less than seven at
five minutes
3 (259) RR 1.16, 95% CI 0.55 to 2.45,
no evidence of a significant dif-
ference
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
3.2. Non-opioid drugs versus
different type of non-opioid
drug (2 studies, 562 women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Sedatives versus anti-histamines Satisfaction with pain relief 1 (157) RR 1.52, 95% CI 1.06 to 2.
17, women in the sedative-anal-
gesic group more likely to ex-
press satisfaction with pain re-
lief
Anti-histamine versus different
anti-histamine
Satisfaction with pain relief 1 (289) RR 1.21, 95% CI 1.02 to
1.43, women in the hydrox-
yzine + meperidine group were
more likely to express satisfac-
tion with pain relief when com-
pared to the promethazine +
meperidine group
133Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 25. (3.) Results by individual review - non-opioid drugs (Continued)
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Anti-histamine versus different
anti-histamine
Assisted vaginal birth 1 (289) RR 0.82, 95% CI 0.64 to 1.03,
no evidence of a significant dif-
ference
Caesarean section Outcome not reported
Adverse effects for women Outcome not reported
Sedatives versus anti-histamines Adverse effects for infants 1 (157) RR 0.89, 95% CI 0.06, 14.00,
no evidence of a significant dif-
ference
Admission to special care baby
unit/neonatal intensive care
Outcome not reported
Anti-histamine versus different
anti-histamine
Apgar score less than seven at
five minutes
1 (289) RR 1.85, 95% CI 0.17 to 20.
21, no evidence of a significant
difference
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
3.2. Non-opioid drug versus
same non-opioid drug of a
different dose (1 study, 28
women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Sedatives Satisfaction with pain relief 1 (19) RR 0.22, 95% CI 0.04 to 1.33,
no evidence of a significant dif-
ference
Sense of control in labour Outcome not reported
134Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
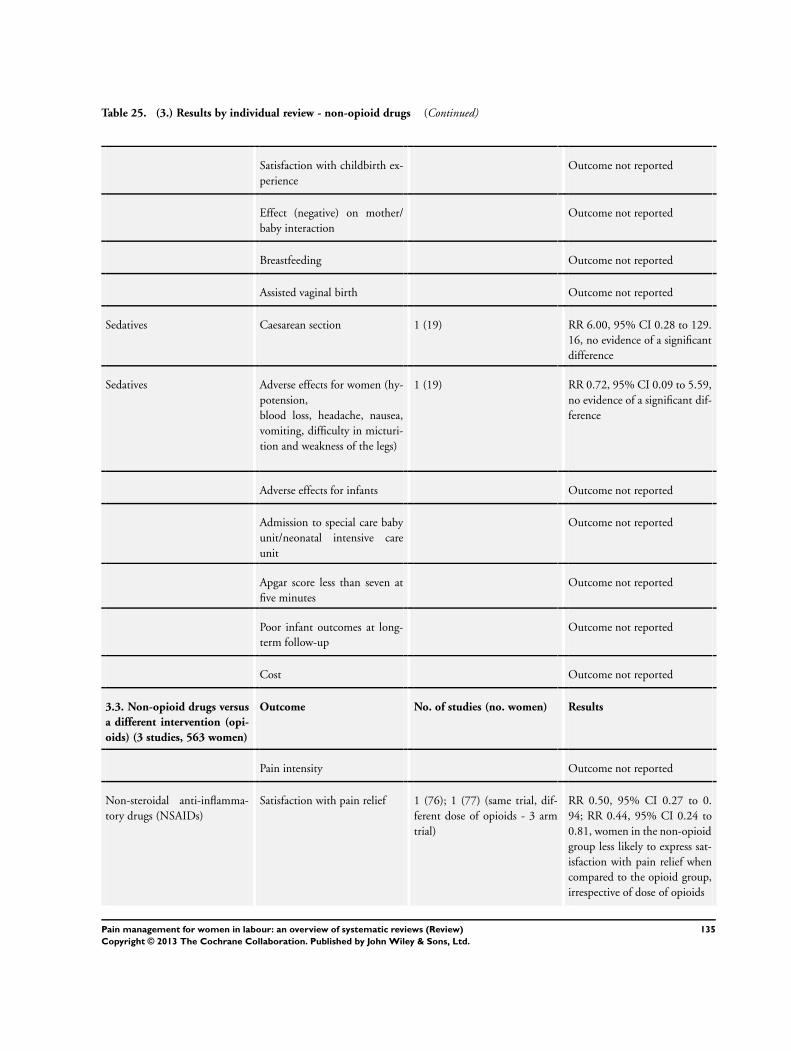
Table 25. (3.) Results by individual review - non-opioid drugs (Continued)
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
Sedatives Caesarean section 1 (19) RR 6.00, 95% CI 0.28 to 129.
16, no evidence of a significant
difference
Sedatives Adverse effects for women (hy-
potension,
blood loss, headache, nausea,
vomiting, difficulty in micturi-
tion and weakness of the legs)
1 (19) RR 0.72, 95% CI 0.09 to 5.59,
no evidence of a significant dif-
ference
Adverse effects for infants Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
3.3. Non-opioid drugs versus
a different intervention (opi-
oids) (3 studies, 563 women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Non-steroidal anti-inflamma-
tory drugs (NSAIDs)
Satisfaction with pain relief 1 (76); 1 (77) (same trial, dif-
ferent dose of opioids - 3 arm
trial)
RR 0.50, 95% CI 0.27 to 0.
94; RR 0.44, 95% CI 0.24 to
0.81, women in the non-opioid
group less likely to express sat-
isfaction with pain relief when
compared to the opioid group,
irrespective of dose of opioids
135Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 25. (3.) Results by individual review - non-opioid drugs (Continued)
Anti-histamines Satisfaction with pain relief 1 (223) RR 0.73, 95% CI 0.54 to 0.
98, women in the non-opioid
group less likely to express sat-
isfaction with pain relief when
compared to the opioid group
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Anti-histamines Assisted vaginal birth 1 (48) RR 1.00, 95% CI 0.07 to 15.
08, no evidence of a significant
difference
Caesarean section Outcome not reported
NSAIDs Adverse effects for women (nau-
sea and vomiting)
1 (76); 1 (77) (same trial, dif-
ferent dose of opioids - 3 arm
trial)
RR 0.64, 95% CI 0.33 to 1.26;
RR 0.54 95% CI 0.29 to 1.03,
no evidence of a significant dif-
ference, irrespective of dose of
opioids
Adverse effects for infants Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; MD: mean difference; RR: risk ratio
136Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 26. (4.) Results by individual review - local anaesthetic nerve block
4. Local anaesthetic nerve block for pain management in labour, 12 studies, 1549 women (Novikova 2012)
4.1. Local anaesthetic nerve
block versus placebo (1 study,
200 women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
PCB with 2% lidocaine versus
PCB with distilled water
Satisfaction with pain relief (de-
gree of pain relief rated as excel-
lent/complete)
1 (198) RR 32.31, 95% CI 10.60 to 98.
54, more women in the lidocaine
group were satisfied with pain re-
lief
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
Caesarean section Outcome not reported
Adverse effects for women and
infants (mother - giddiness,
sweating, tingling of lower
limbs; baby- bradycardia)
1 (200) RR 29.00, 95% CI 1.75 to 479.
61, significantly more side-effects
in mothers and babies in the li-
docaine group
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
4.2. Local anaesthetic nerve
block versus opioids (2 stud-
ies, 129 women)
Outcome No. of studies (no. women) Results
137Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
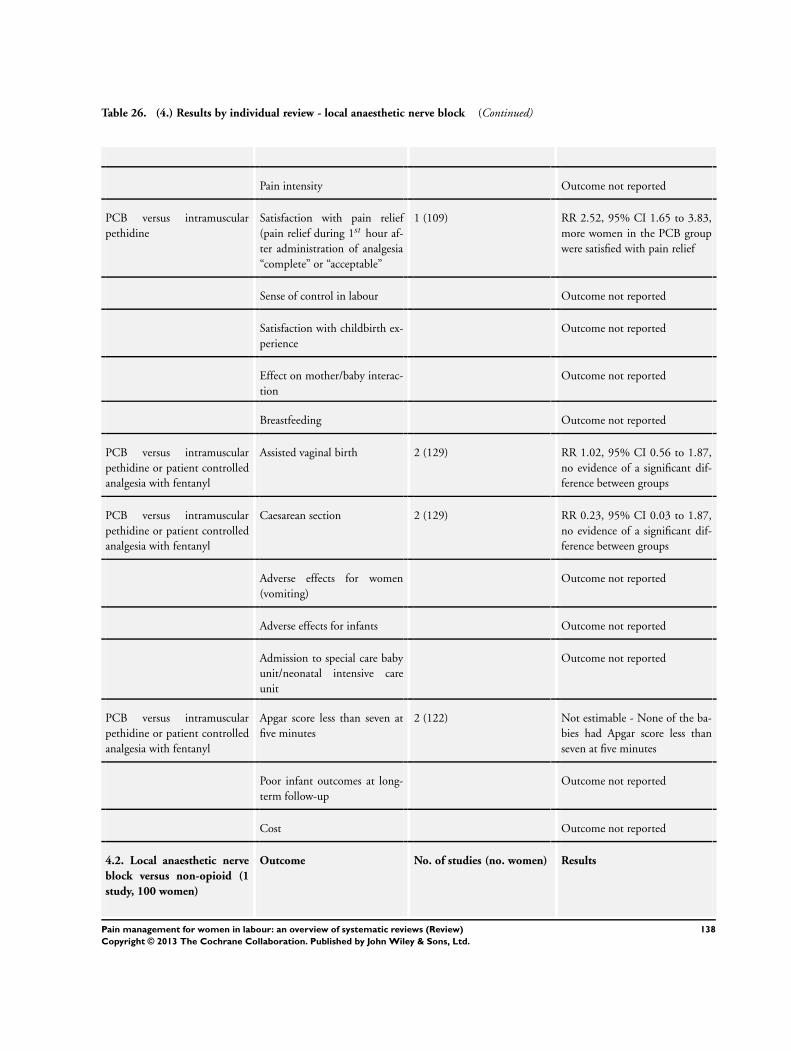
Table 26. (4.) Results by individual review - local anaesthetic nerve block (Continued)
Pain intensity Outcome not reported
PCB versus intramuscular
pethidine
Satisfaction with pain relief
(pain relief during 1st hour af-
ter administration of analgesia
“complete” or “acceptable”
1 (109) RR 2.52, 95% CI 1.65 to 3.83,
more women in the PCB group
were satisfied with pain relief
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
PCB versus intramuscular
pethidine or patient controlled
analgesia with fentanyl
Assisted vaginal birth 2 (129) RR 1.02, 95% CI 0.56 to 1.87,
no evidence of a significant dif-
ference between groups
PCB versus intramuscular
pethidine or patient controlled
analgesia with fentanyl
Caesarean section 2 (129) RR 0.23, 95% CI 0.03 to 1.87,
no evidence of a significant dif-
ference between groups
Adverse effects for women
(vomiting)
Outcome not reported
Adverse effects for infants Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
PCB versus intramuscular
pethidine or patient controlled
analgesia with fentanyl
Apgar score less than seven at
five minutes
2 (122) Not estimable - None of the ba-
bies had Apgar score less than
seven at five minutes
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
4.2. Local anaesthetic nerve
block versus non-opioid (1
study, 100 women)
Outcome No. of studies (no. women) Results
138Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 26. (4.) Results by individual review - local anaesthetic nerve block (Continued)
Pain intensity Outcome not reported
PCB versus intramuscular
promethazine
Satisfaction with pain relief (ex-
cellent or complete relief )
1 (100) RR 1.11, 95% CI 0.67 to 1.84,
no evidence of a significant dif-
ference between groups
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
PCB versus intramuscular
promethazine
Caesarean section 1 (100) RR 2.00, 95% CI 0.19 to 21.36,
no evidence of a significant dif-
ference between groups
Adverse effects for women Outcome not reported
Adverse effects for infants Outcome not reported
Admission to special care baby
unit/neonatal intensive care
unit
Outcome not reported
PCB versus intramuscular
promethazine
Apgar score less than seven at
five minutes
1 (100) Not estimable - None of the ba-
bies had Apgar score less than
seven at five minutes
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
4.3. Local anaesthetic nerve
block versus different dose/
agent or timing of anaesthetic
nerve block (8 studies, 1120
women)
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
139Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 26. (4.) Results by individual review - local anaesthetic nerve block (Continued)
PCB 1% lidocaine versus 2%
chloroprocaine
Satisfaction with pain relief -
(proportion with unsatisfactory
pain relief )
1 (60) RR 2.81, 95% CI 0.31 to 25.48,
no evidence of a significant dif-
ference between groups
PCB 0.25% bupivacaine versus
2% chloroprocaine or 1% car-
bacaine
Satisfaction with pain relief
during the second stage of
labour (proportion with good
or excellent pain relief )
2 (332) RR 0.93, 95% CI 0.85 to 1.00,
no evidence of a significant dif-
ference between groups
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
PCB 1% lidocaine versus 2%
chloroprocaine
Assisted vaginal birth 1 (60) RR 0.57, 95% CI 0.29 to 1.14,
no evidence of a significant dif-
ference between groups
PCB 1% lidocaine versus 2%
chloroprocaine
Caesarean section 1 (58) RR 1.00, 95% CI 0.15 to 6.63,
no evidence of a significant dif-
ference between groups
PCB 0.25% bupivacaine versus
1% carbacaine
Adverse effects for women
(slight dizziness after injection)
1 (285) RR 0.30, 95% CI 0.03 to 2.89,
no evidence of a significant dif-
ference between groups
Adverse effects for infants Outcome not reported
Admission to special care baby
unit/neonatal intensive care
Outcome not reported
PCB 0.25% bupivacaine versus
2% chloroprocaine
Apgar score less than seven at
five minutes
1 (47) RR 0.32, 95% CI 0.01 to 7.48,
no evidence of a significant dif-
ference between groups
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
CI: confidence interval; RR: risk ratio
140Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 27. (5.) Results by individual review - epidural
5. Epidural versus non-epidural or no analgesia in labour, 38 studies, 9658 women (Anim-Somuah 2011)
5.1. Epidural versus non-
epidural/no analgesia
Outcome No. of studies (no. women) Results
Pain intensity (during whole of
labour), using visual analogue
score (VAS) 0 to 10, where 0
represents no pain and 10 worst
pain
3 (1166 women) Average mean difference (MD)
-3.36, 95% CI -5.41 to -1.31
(random effects: heterogeneity:
I2 = 98%, Tau2 = 3.14, Chi2 test
for heterogeneity P <0.00001),
a significant reduction in pain
intensity for women receiving
epidural
Pain intensity (in the first stage
of labour) VAS
4 (589 women) Average mean difference (MD)
-16.35, 95% CI -25.11 to -7.
58 (random effects: heterogene-
ity: I2 = 87%, Tau2 = 65.03,
Chi2 test for heterogeneity P <0.
0001), a significant reduction in
pain intensity for women receiv-
ing epidural
Pain intensity (in the second
stage of labour) VAS
3 (559 women) Average mean difference (MD)
-25.29, 95% CI -40.48 to -10.
11 (random effects: heterogene-
ity: I2 = 96%, Tau2 = 162.74,
Chi2 test for heterogeneity P <0.
00001), a significant reduction
in pain intensity for women re-
ceiving epidural
Maternal satisfaction with pain
relief - dichotomous data: the
proportion of women rating
their satisfaction with analgesia
as excellent, very good, good af-
ter delivery in each group
7 (2929 women) Average RR 1.31, 95% CI 0.84
to 2.05 (random effects: hetero-
geneity: I2 = 100%, Tau2 = 0.
36, Chi2 test for heterogeneity
P <0.00001), no evidence of a
significant difference
Maternal satisfaction with pain
relief - continuous data
2 (272 women) Average standardised mean dif-
ference (SMD) 0.10, 95% CI
-0.49 to 0.70 (random effects:
heterogeneity: I2 = 62%, Tau2 =
0.12, Chi2 test for heterogene-
ity P = 0.10), no evidence of a
significant difference
141Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
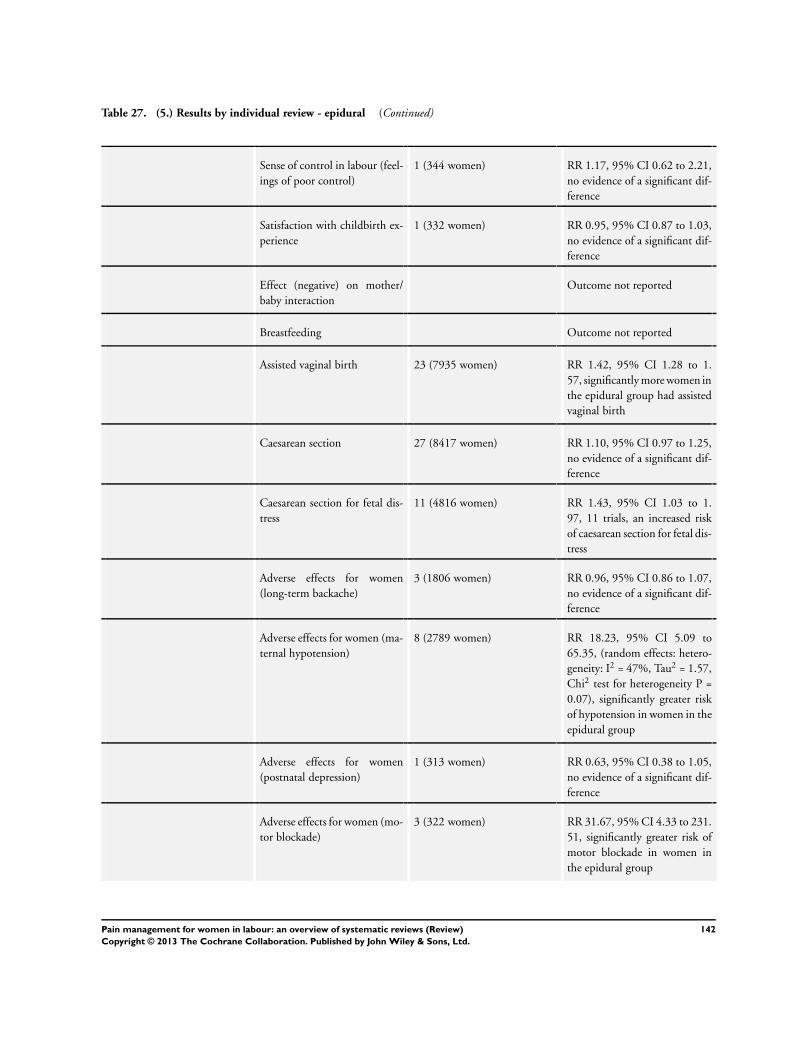
Table 27. (5.) Results by individual review - epidural (Continued)
Sense of control in labour (feel-
ings of poor control)
1 (344 women) RR 1.17, 95% CI 0.62 to 2.21,
no evidence of a significant dif-
ference
Satisfaction with childbirth ex-
perience
1 (332 women) RR 0.95, 95% CI 0.87 to 1.03,
no evidence of a significant dif-
ference
Effect (negative) on mother/
baby interaction
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 23 (7935 women) RR 1.42, 95% CI 1.28 to 1.
57, significantly more women in
the epidural group had assisted
vaginal birth
Caesarean section 27 (8417 women) RR 1.10, 95% CI 0.97 to 1.25,
no evidence of a significant dif-
ference
Caesarean section for fetal dis-
tress
11 (4816 women) RR 1.43, 95% CI 1.03 to 1.
97, 11 trials, an increased risk
of caesarean section for fetal dis-
tress
Adverse effects for women
(long-term backache)
3 (1806 women) RR 0.96, 95% CI 0.86 to 1.07,
no evidence of a significant dif-
ference
Adverse effects for women (ma-
ternal hypotension)
8 (2789 women) RR 18.23, 95% CI 5.09 to
65.35, (random effects: hetero-
geneity: I2 = 47%, Tau2 = 1.57,
Chi2 test for heterogeneity P =
0.07), significantly greater risk
of hypotension in women in the
epidural group
Adverse effects for women
(postnatal depression)
1 (313 women) RR 0.63, 95% CI 0.38 to 1.05,
no evidence of a significant dif-
ference
Adverse effects for women (mo-
tor blockade)
3 (322 women) RR 31.67, 95% CI 4.33 to 231.
51, significantly greater risk of
motor blockade in women in
the epidural group
142Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 27. (5.) Results by individual review - epidural (Continued)
Adverse effects for women
(headache)
3 (1198 women) RR 0.96, 95% CI 0.81 to 1.15,
no evidence of a significant dif-
ference
Adverse effects for women (nau-
sea and vomiting)
12 (3187 women) Average RR 0.95, 95% CI 0.72
to 1.27, random effects: hetero-
geneity: I2 = 49%, Tau2 = 0.09,
Chi2 test for heterogeneity P =
0.03), no evidence of a signifi-
cant difference
Adverse effects for women (it-
ching)
3 (230 women) RR 1.46, 95% CI 0.51 to 4.16,
no evidence of a significant dif-
ference
Adverse effects for women
(fever)
6 (2741 women) RR 3.34, 95% CI 2.63 to 4.23,
significantly greater risk of fever
in women in the epidural group
Adverse effects for women
(shivering)
1 (20 women) RR 5.00, 95% CI 0.27 to 92.
62, no evidence of a significant
difference
Adverse effects for women
(drowsiness)
4 (641 women) Average RR 0.55, 95% CI 0.07
to 4.26, random effects: hetero-
geneity I2 = 94%, Tau2 = 3.47,
Chi2 test for heterogeneity P <
0.00001), no evidence of a sig-
nificant difference
Adverse effects for women (uri-
nary retention)
3 (283 women) RR 17.05, 95% CI 4.82 to 60.
39, significantly greater risk of
urinary retention in women in
the epidural group
Adverse effects for women
(catheterization during labour)
2 (1103 women) RR 1.81, 95% CI 0.44 to 7.46,
no evidence of a significant dif-
ference
Adverse effects for women (mal-
position)
4 (673 women) RR 1.40, 95% CI 0.98 to 1.99,
no evidence of a significant dif-
ference
Adverse effects for women (sur-
gical amniotomy)
2 (211 women) Average RR 1.03, 95% CI 0.74
to 1.43, random effects: hetero-
geneity I2 = 81%, Tau2 = 0.05,
Chi2 test for heterogeneity P =
0.02, no evidence of a signifi-
cant difference
143Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 27. (5.) Results by individual review - epidural (Continued)
Adverse effects for infants (aci-
dosis pH less than 7.2)
7 (3643 women) RR 0.80, 95% CI 0.68 to 0.
94, neonates of women who
had epidural had a significantly
lower risk of acidosis
Adverse effects for infants (aci-
dosis pH less than 7.15)
2 (382 women) RR 0.95, 95% CI 0.50 to 1.79,
no evidence of a significant dif-
ference
Adverse effects for infants
(naloxone administration)
10 (2645 women) RR 0.15, 95% CI 0.10 to 0.
23, neonates of women who
had epidural had a significantly
lower risk of requiring naloxone
Adverse effects for infants
(meconium staining of liquor)
5 (2295 women) RR 1.01, 95% CI 0.84 to 1.21,
no evidence of a significant dif-
ference
Admission to special care baby
unit/neonatal intensive care
unit
7 (3125 women) RR 1.19, 95% CI 0.94 to 1.50,
no evidence of a significant dif-
ference
Apgar score less than seven at
five minutes
18 (6898 women) RR 0.80, 95% CI 0.54 to 1.20,
no evidence of a significant dif-
ference
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
I2 values reported in table only when random effects analysis has been carried out due to substantial heterogeneity indicated by an I2
value greater than 30%
CI: confidence interval; MD: mean difference; RR: risk ratio
Table 28. (6.) Results by individual review - combined spinal epidural
6. Combined spinal-epidural versus epidural in labour, 27 studies, 3303 women (Simmons 2012)
Combined spinal-epidural
versus traditional epidural
Outcome No. of studies (no. women) Results
Pain intensity - time from first
injection to effective analgesia
in minutes
2 (129) MD -2.87, 95% CI -5.07 to -0.
67, CSE had a faster onset time of
effective pain relief from time of
injection (approximately 3 min-
144Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
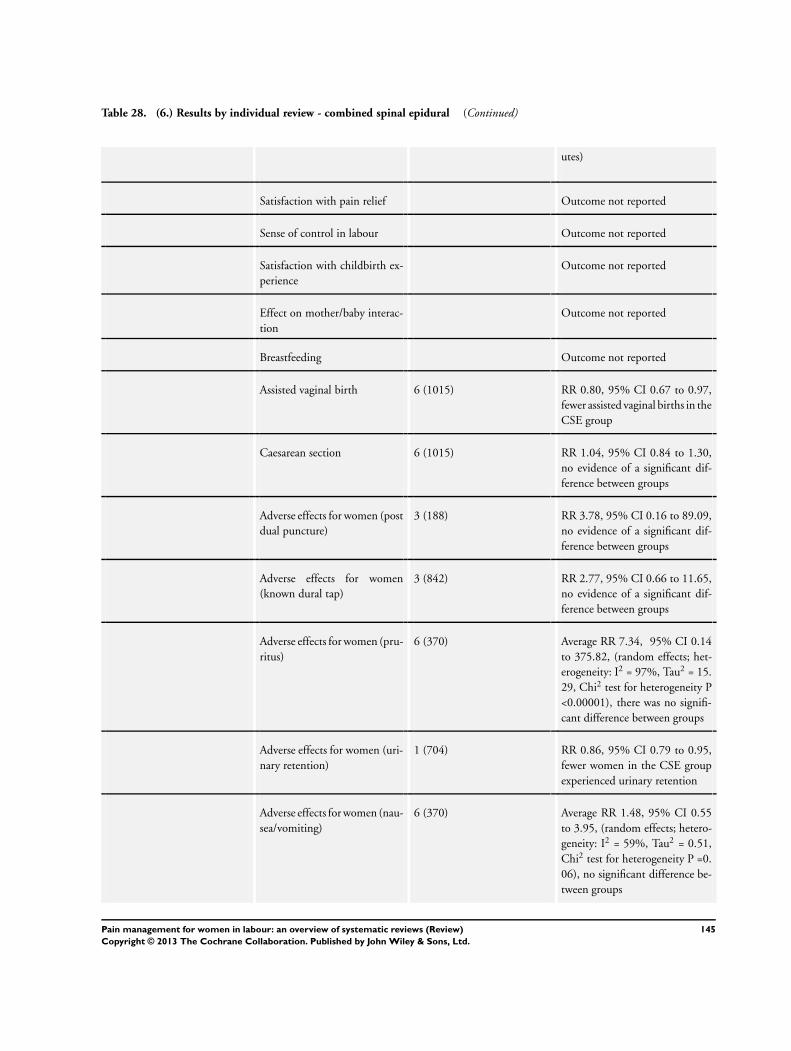
Table 28. (6.) Results by individual review - combined spinal epidural (Continued)
utes)
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 6 (1015) RR 0.80, 95% CI 0.67 to 0.97,
fewer assisted vaginal births in the
CSE group
Caesarean section 6 (1015) RR 1.04, 95% CI 0.84 to 1.30,
no evidence of a significant dif-
ference between groups
Adverse effects for women (post
dual puncture)
3 (188) RR 3.78, 95% CI 0.16 to 89.09,
no evidence of a significant dif-
ference between groups
Adverse effects for women
(known dural tap)
3 (842) RR 2.77, 95% CI 0.66 to 11.65,
no evidence of a significant dif-
ference between groups
Adverse effects for women (pru-
ritus)
6 (370) Average RR 7.34, 95% CI 0.14
to 375.82, (random effects; het-
erogeneity: I2 = 97%, Tau2 = 15.
29, Chi2 test for heterogeneity P
<0.00001), there was no signifi-
cant difference between groups
Adverse effects for women (uri-
nary retention)
1 (704) RR 0.86, 95% CI 0.79 to 0.95,
fewer women in the CSE group
experienced urinary retention
Adverse effects for women (nau-
sea/vomiting)
6 (370) Average RR 1.48, 95% CI 0.55
to 3.95, (random effects; hetero-
geneity: I2 = 59%, Tau2 = 0.51,
Chi2 test for heterogeneity P =0.
06), no significant difference be-
tween groups
145Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 28. (6.) Results by individual review - combined spinal epidural (Continued)
Adverse effects for women (hy-
potension)
6 (1002) Average RR 0.81, 95% CI 0.65
to 1.02, no significant difference
between groups
Adverse effects for women
(headache)
1 (79) RR 1.03, 0.07 to 15.83, no
significant difference between
groups
Adverse effects for women (se-
dation)
1 (79) RR 1.03, 0.46 to 2.31, no signif-
icant difference between groups
Adverse effects for infants Outcome not reported in suitable
format
Admission to special care baby
unit/neonatal intensive care
1 (704) RR 0.63, 95% CI 0.29 to 1.37,
no significant difference between
groups
Apgar score less than seven at
five minutes
3 (842) RR 2.10, 95% CI 0.63 to 6.97,
no evidence of a significant dif-
ference between groups
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
Combined spinal-epidural
versus low-dose epidural
Outcome No. of studies (no. women) Results
Pain intensity - time from first
injection to effective analgesia
in minutes
5 (461) Average Mean difference MD -
5.42, 95% CI -7.26 to -3.59,
(random effects; heterogeneity: I2 = 77%, Tau2 = 3.27, Chi2 test
for heterogeneity P =0.002), CSE
had a faster onset time of effective
pain relief from time of injection
(approximately 6 minutes)
Pain intensity - number of
women with effective analgesia
10 minutes after first injection
1 (101) RR 1.94, 95% CI 1.49 to 2.54,
more women in the CSE group
had effective analgesia
146Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 28. (6.) Results by individual review - combined spinal epidural (Continued)
Satisfaction with pain relief 7 (520) RR 1.01, 95% CI 0.98 to 1.05,
no significant difference between
groups
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 11 (1612) RR 1.07, 95% CI 0.88 to 1.30,
no evidence of a significant dif-
ference between groups
Caesarean section 15 (1960) RR 0.97, 95% CI 0.82 to 1.16,
no evidence of a significant dif-
ference between groups
Adverse effects for women (post
dual puncture)
9 (701) RR 1.68, 95% CI 0.42 to 6.81,
no evidence of a significant dif-
ference between groups
Adverse effects for women
(known dural tap)
6 (1326) RR 0.81, 95% CI 0.22 to 2.98,
no evidence of a significant dif-
ference between groups
Adverse effects for women
(number of women requiring
blood patch for post dural
puncture headache)
7 (531) RR 2.22, 95% CI 0.51 to 9.64,
no evidence of a significant dif-
ference between groups
Adverse effects for women (pru-
ritus)
11 (959) Average RR 1.80, 95% CI 1.22
to 2.65, (random effects; hetero-
geneity: I2 = 84%, Tau2 = 0.26,
Chi2 test for heterogeneity P <0.
00001), more women in the CSE
group had pruritus
Adverse effects for women (uri-
nary retention)
4 (964) RR 1.05, 95% CI 0.94 to 1.16,
no evidence of a significant dif-
ference between groups
147Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
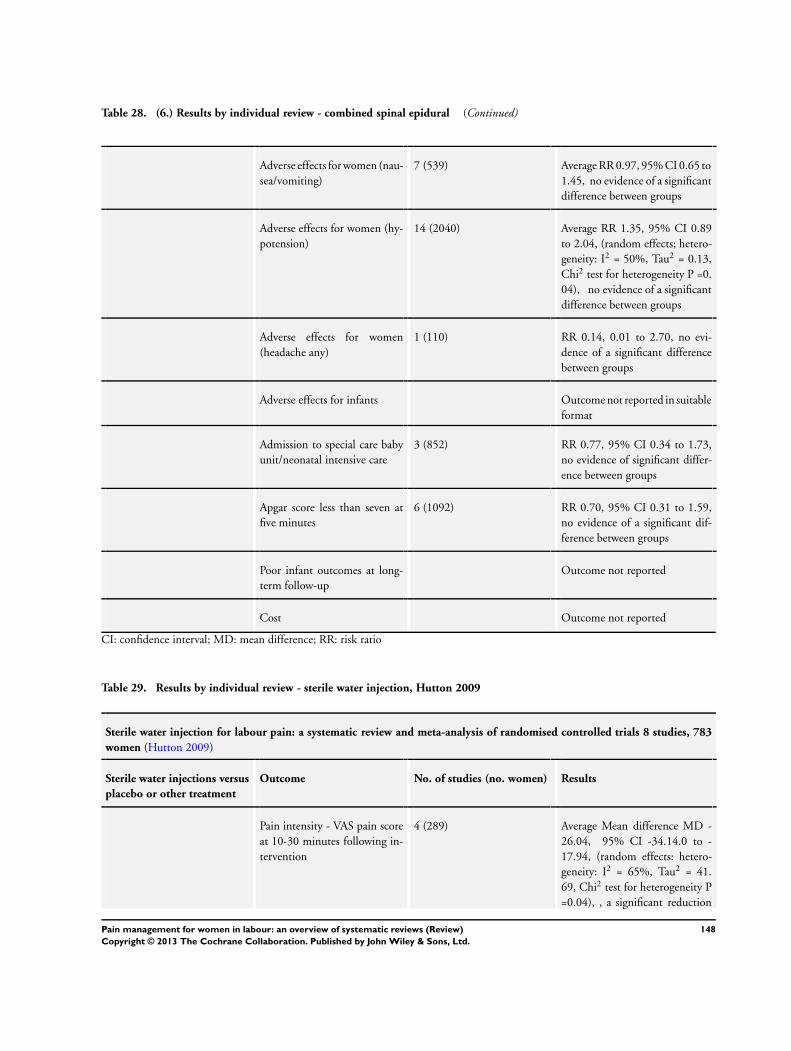
Table 28. (6.) Results by individual review - combined spinal epidural (Continued)
Adverse effects for women (nau-
sea/vomiting)
7 (539) Average RR 0.97, 95% CI 0.65 to
1.45, no evidence of a significant
difference between groups
Adverse effects for women (hy-
potension)
14 (2040) Average RR 1.35, 95% CI 0.89
to 2.04, (random effects; hetero-
geneity: I2 = 50%, Tau2 = 0.13,
Chi2 test for heterogeneity P =0.
04), no evidence of a significant
difference between groups
Adverse effects for women
(headache any)
1 (110) RR 0.14, 0.01 to 2.70, no evi-
dence of a significant difference
between groups
Adverse effects for infants Outcome not reported in suitable
format
Admission to special care baby
unit/neonatal intensive care
3 (852) RR 0.77, 95% CI 0.34 to 1.73,
no evidence of significant differ-
ence between groups
Apgar score less than seven at
five minutes
6 (1092) RR 0.70, 95% CI 0.31 to 1.59,
no evidence of a significant dif-
ference between groups
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
CI: confidence interval; MD: mean difference; RR: risk ratio
Table 29. Results by individual review - sterile water injection, Hutton 2009
Sterile water injection for labour pain: a systematic review and meta-analysis of randomised controlled trials 8 studies, 783
women (Hutton 2009)
Sterile water injections versus
placebo or other treatment
Outcome No. of studies (no. women) Results
Pain intensity - VAS pain score
at 10-30 minutes following in-
tervention
4 (289) Average Mean difference MD -
26.04, 95% CI -34.14.0 to -
17.94, (random effects: hetero-
geneity: I2 = 65%, Tau2 = 41.
69, Chi2 test for heterogeneity P
=0.04), , a significant reduction
148Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 29. Results by individual review - sterile water injection, Hutton 2009 (Continued)
in pain score of the sterile water
group compared with the placebo
or other intervention group
Pain intensity - Pain intensity -
VAS pain score at 45-60 min-
utes following intervention
5 (542) Average Mean difference MD -
36.27, 95% CI -50.80 to -21.
74, (random effects: heterogene-
ity: I2 = 94%, Tau2 = 255.58,
Chi2 test for heterogeneity P <=
0.00001), a significant reduction
in pain score of the sterile water
group compared with the placebo
or other intervention group
Pain intensity - Pain intensity -
VAS pain score at 90-120 min-
utes following intervention
5 (488) Average Mean difference MD -
27.74, 95% CI -39.03 to -16.
45, (random effects: heterogene-
ity: I2 = 86%, Tau2 = 135.71,
Chi2 test for heterogeneity P <=
0.00001), a significant reduction
in pain score of the sterile water
group compared with the placebo
or other intervention group
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth Outcome not reported
Caesarean section 8 (828) RR 0.51, 95% CI 0.30 to 0.87,
significantly fewer caesarean sec-
tions in the sterile water group
compared with the placebo or
other intervention group
Side effects for mother Outcome not reported
Side effects for baby Outcome not reported
149Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
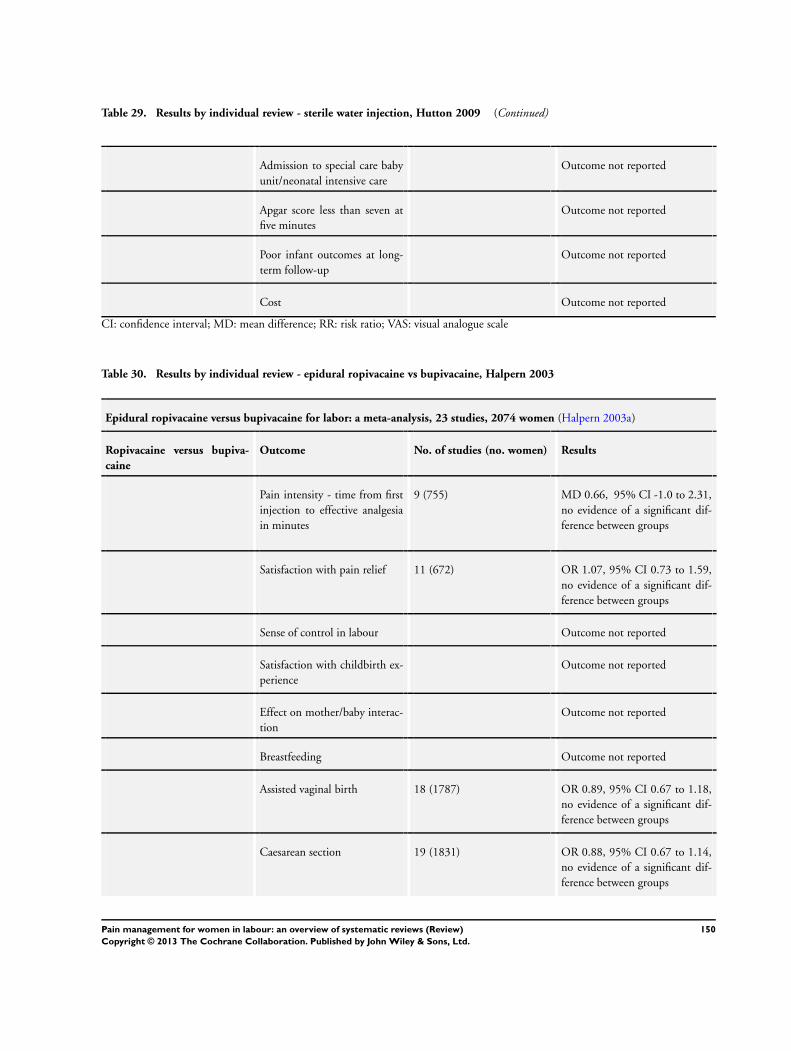
Table 29. Results by individual review - sterile water injection, Hutton 2009 (Continued)
Admission to special care baby
unit/neonatal intensive care
Outcome not reported
Apgar score less than seven at
five minutes
Outcome not reported
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
CI: confidence interval; MD: mean difference; RR: risk ratio; VAS: visual analogue scale
Table 30. Results by individual review - epidural ropivacaine vs bupivacaine, Halpern 2003
Epidural ropivacaine versus bupivacaine for labor: a meta-analysis, 23 studies, 2074 women (Halpern 2003a)
Ropivacaine versus bupiva-
caine
Outcome No. of studies (no. women) Results
Pain intensity - time from first
injection to effective analgesia
in minutes
9 (755) MD 0.66, 95% CI -1.0 to 2.31,
no evidence of a significant dif-
ference between groups
Satisfaction with pain relief 11 (672) OR 1.07, 95% CI 0.73 to 1.59,
no evidence of a significant dif-
ference between groups
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
Assisted vaginal birth 18 (1787) OR 0.89, 95% CI 0.67 to 1.18,
no evidence of a significant dif-
ference between groups
Caesarean section 19 (1831) OR 0.88, 95% CI 0.67 to 1.14,
no evidence of a significant dif-
ference between groups
150Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 30. Results by individual review - epidural ropivacaine vs bupivacaine, Halpern 2003 (Continued)
Side effects for mother (hy-
potension)
9 (615) OR 1.04, 95% CI 0.60 to 1.8,
no evidence of a significant dif-
ference between groups
Side effects for mother (nausea
or vomiting)
7 (888) OR 0.88, 95% CI 0.59 to 1.29,
no evidence of a significant dif-
ference between groups
Side effects for baby Outcome not reported in suitable
format
Admission to special care baby
unit/neonatal intensive care
Outcome not reported
Apgar score less than seven at
five minutes
15 (1550) OR 0.99, 95% CI 0.49 to 2.0,
no evidence of a significant dif-
ference between groups
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
CI: confidence interval; MD: mean difference; OR: odds ratio
Table 31. Results by individual review - intrathecal opioids - Mardirosoff 2002
Fetal bradycardia due to intrathecal opioids for labour analgesia: a systematic review, 24 studies, 3513 women (Mardirosoff
2002)
Intrathecal opioids versus
non-intrathecal opioids
Outcome No. of studies (no. women) Results
Pain intensity Outcome not reported
Satisfaction with pain relief Outcome not reported
Sense of control in labour Outcome not reported
Satisfaction with childbirth ex-
perience
Outcome not reported
Effect on mother/baby interac-
tion
Outcome not reported
Breastfeeding Outcome not reported
151Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Table 31. Results by individual review - intrathecal opioids - Mardirosoff 2002 (Continued)
Assisted vaginal birth 15 (2831) RR 0.94, 95% CI 0.83 to 1.07,
no evidence of a significant dif-
ference between groups
Caesarean section 17 (2954) RR 1.03, 95% CI 0.87 to 1.21,
no evidence of a significant dif-
ference between groups
Opioids in controls Adverse effects for women (pru-
ritus)
9 (1308) Average RR 1.71, 95% CI 0.97 to
3.02, no evidence of a significant
difference between groups
No opioids in controls Adverse effects for women (pru-
ritus)
11 (855) RR 29.6, 95% CI 13.6 to 64.
6, significantly more pruritus in
women in the intrathecal opioid
group
Adverse effects for infants (fetal
heart rate abnormalities)
17 (2081) RR 1.17, 95% CI 0.87 to 1.57,
no evidence of a significant dif-
ference between groups
Adverse effects for infants (fetal
bradycardia within 1 hour)
9 (927) OR 1.81, 95% CI 1.04 to 3.14,
significant increase in fetal brady-
cardia with intrathecal opioids
Admission to special care baby
unit/neonatal intensive care
Outcome not reported
Apgar score less than seven at
five minutes
11 (1623) OR 1.17, 95% CI 0.44 to 3.11,
no evidence of a significant dif-
ference between groups
Poor infant outcomes at long-
term follow-up
Outcome not reported
Cost Outcome not reported
CI: confidence interval; OR: odds ratio; RR: risk ratio
Table 32. Summary of outcomes reported in Cochrane systematic reviews - pharmacological interventions
Inhaled analgesia
(Klomp 2012)
Parenteral
opioids review (
Ullman 2010)
Non-opioid
drugs (Othman
2012)
Local anaesthetic
nerve blocks (
Novikova 2012)
Epidural (Anim-
Somuah 2011)
Combined
spinal epidural (
Simmons 2012)
152Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 32. Summary of outcomes reported in Cochrane systematic reviews - pharmacological interventions (Continued)
Pain intensity 9/26
trials (26%) re-
ported this out-
come
Significant find-
ings observed for
4 comparisons (7
studies)
28/57
trials (49%) re-
ported this out-
come
Significant find-
ings observed for
5 comparisons (8
studies)
2/18 trials (11%)
reported this
outcome
Significant find-
ings observed for
1 comparison (1
study)
NOT
REPORTED
7/38 trials (18%)
reported this
outcome
Significant find-
ings observed for
3 comparisons (7
studies)
8/27
trials (30%) re-
ported this out-
come
Significant find-
ings observed for
3 comparisons (8
studies)
Satisfaction with
pain relief
8/26 trials (31%)
reported this
outcome
No differences
observed
between groups
12/57 trials
(21%)
reported this
outcome
Significant find-
ings observed for
2 comparisons (2
studies)
9/18 trials (50%)
reported this
outcome
Significant find-
ings observed for
5 comparisons (7
studies)
6/12
trials (50%) re-
ported this out-
come
Significant find-
ings observed for
2 comparisons (2
studies)
9/38 trials (24%)
reported this
outcome
No differences
observed
between groups
7/27
trials (26%) re-
ported this out-
come
No differences
observed
between groups
Sense of control
in labour
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
1/38 trials (3%)
reported this
outcome
No differences
observed
between groups
NOT
REPORTED
Satisfaction with
childbirth expe-
rience
NOT
REPORTED
1/57
trial (1.75%) re-
ported this out-
come
No differences
observed
between groups
1/18 trials (6%)
reported this
outcome
Significant find-
ings observed for
1 comparison (1
study)
NOT
REPORTED
1/38 trials (3%)
reported this
outcome
No differences
observed
between groups
NOT
REPORTED
Effect on
mother/baby in-
teraction
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
Breastfeeding NOT
REPORTED
2/57
trials (3.5%) re-
ported this out-
come
No differences
observed
between groups
1/18 trials (6%)
reported this
outcome
No differences
observed
between groups
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
153Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 32. Summary of outcomes reported in Cochrane systematic reviews - pharmacological interventions (Continued)
Assisted vaginal
birth
7/26
trials (27%) re-
ported this out-
come
No differences
observed
between groups
17/57 trials
(30%)
reported this
outcome
No differences
observed
between groups
7/18 trials (39%)
reported this
outcome
No differences
observed
between groups
3/12
trials (25%) re-
ported this out-
come
No differences
observed
between groups
23/38
trials (60%) re-
ported this out-
come
Signifi-
cant findings ob-
served for 1 com-
parison (23 stud-
ies)
17/27
trials (63%) re-
ported this out-
come
Significant find-
ings observed for
1 comparison (6
studies)
Caesarean
section
6/26
trials (23%) re-
ported this out-
come
No differences
observed
between groups
20/57 trials
(35%)
Reported this
outcome
No differences
observed
between groups
3/18
trials (17%) re-
ported this out-
come
No differences
observed
between groups
4/12
trials (33%) re-
ported this out-
come
No differences
observed
between groups
27/38
trials (71%) re-
ported this out-
come
No differences
observed
between groups
21/27
trials (78%) re-
ported this out-
come
No differences
observed
between groups
Adverse effects
for women
16/26
trials (62%) re-
ported this out-
come
Significant find-
ings observed for
7 comparisons (9
studies)
35/57
trials (62%) re-
ported this out-
come
Significant find-
ings observed for
14 comparisons
(27 studies)
6/18 trials (33%)
reported this
outcome
No differences
observed
between groups
2/12 trials (17%)
reported this
outcome
Significant find-
ings observed for
1 comparison (1
study)
21/38
trials (55%) re-
ported this out-
come
Significant find-
ings observed for
4 comparisons
(12 studies)
16/27
trials (60%) re-
ported this out-
come
Significant find-
ings observed for
2 comparisons
(12 studies)
Adverse effects
for infants
4/26
trials (15%) re-
ported this out-
come
No differences
observed
between groups
17/57
trials (30%) re-
ported this out-
come
Significant find-
ings observed for
1 comparison (1
study)
5/18 trials (28%)
reported this
outcome
No differences
observed
between groups
1/12 trials (8%)
reported this
outcome
Significant find-
ings observed for
1 comparison (1
study)
18/38
trials (47%) re-
ported this out-
come
Significant find-
ings observed for
2 comparisons
(15 studies)
NOT
REPORTED
Admission to
special care baby
unit/neonatal in-
tensive care unit
NOT
REPORTED
6/57 trials (10%)
reported this
outcome
No differences
observed
between groups
NOT
REPORTED
NOT
REPORTED
7/38 trials (18%)
reported this
outcome
No differences
observed
between groups
4/27
trials (15%) re-
ported this out-
come
No differences
observed
between groups
154Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 32. Summary of outcomes reported in Cochrane systematic reviews - pharmacological interventions (Continued)
Apgar score less
than seven at five
minutes
7/26
trials (27%) re-
ported this out-
come
No differences
observed
between groups
12/57
trials (21%) re-
ported this out-
come
No differences
observed
between groups
4/18 trials (22%)
reported this
outcome
No differences
observed
between groups
4/12 trials (33%)
reported this
outcome
No differences
observed
between groups
18/38
trials (47%) re-
ported this out-
come
No differences
observed
between groups
9/27
trials (33%) re-
ported this out-
come
No differences
observed
between groups
Poor infant out-
comes at long-
term follow-up
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
Cost NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
NOT
REPORTED
Table 33. Summary of outcomes reported in Cochrane systematic reviews - non-pharmacological interventions
Hypnosis (
Madden
2012
Biofeed-
back
(Barragán
2011)
Sterile wa-
ter
injection (
Derry
2012)
Immer-
sion in wa-
ter (Cluett
2009)
Aro-
mather-
apy (Smith
2011c)
Relaxation
techniques
(Smith
2011b)
Acupunc-
ture
or acupres-
sure
(Smith
2011a)
Massage,
reflexology
&
other man-
ual meth-
ods (Smith
2012)
TENS
(Dowswell
2009)
Pain inten-
sity
1/7 trials
(14%) re-
ported this
outcome
Signif-
icant find-
ings ob-
served for
1 compari-
son
(1 study) -
but
this was a
quasi-
RCT
NOT RE-
PORTED
3/7 trials
(43%) re-
ported this
outcome
Signif-
icant find-
ings ob-
served for
10 com-
parisons (3
studies)
4/12 trials
(33%) re-
ported this
outcome
Signif-
icant find-
ings ob-
served for
10 com-
parisons (1
study)
NOT RE-
PORTED
5/11 trials
(45%) re-
ported this
outcome
Significant
findings
observed
for 3 com-
parisons (3
studies)
7/13 trials
(54%) re-
ported this
outcome
Significant
findings
observed
for 3 com-
parison (4
studies)
5/6 trials
(83%) re-
ported this
outcome
Significant
findings
observed
for 2 com-
parisons (5
studies)
10/17 tri-
als
(59%) re-
ported this
outcome
Significant
findings
observed
for 2 com-
parisons (3
studies)
Satisfac-
tion with
pain relief
1/7 trials
(14%) re-
ported this
outcome
No differ-
ences ob-
NOT RE-
PORTED
NOT RE-
PORTED
NOT ) NOT RE-
PORTED
3/11 trials
(27%) re-
ported this
outcome
Significant
3/13 trials
(23%) re-
ported this
outcome
Significant
2/6 trials
(33%) re-
ported this
outcome
6/17 trials
(35%) re-
ported this
outcome
Significant
155Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 33. Summary of outcomes reported in Cochrane systematic reviews - non-pharmacological interventions (Continued)
served be-
tween
groups
findings
observed
for 2 com-
parisons (2
studies)
findings
observed
for 2 com-
parisons (2
studies)
No differ-
ences ob-
served be-
tween
groups
findings
observed
for 1 com-
parison (1
study)
Sense of
control in
labour
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
1/6 trials
(17%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
Satisfac-
tion
with child-
birth expe-
rience
2/7 trials
(28%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
1/12 trial
(8%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
2/11 trials
(18%) re-
ported this
outcome
Significant
findings
observed
for 1 com-
parison (1
study)
1/13 trials
(7%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
Effect on
mother/
baby inter-
action
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
Breastfeed-
ing
1/7 trials
(14%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
3/12 trials
(25%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
As-
sisted vagi-
nal birth
3/7 trials
(43%) re-
ported this
outcome
No differ-
ences ob-
2/4 trials
(50%) re-
ported this
outcome
No differ-
ences ob-
6/7 trials
(86%) re-
ported this
outcome
No differ-
ences ob-
8/12 trials
(67%) re-
ported this
outcome
No differ-
ences ob-
2/2 trials
(100%) re-
ported this
outcome
No differ-
ences ob-
3/11 trials
(27%) re-
ported this
outcome
Significant
findings
7/13 trials
(54%) re-
ported this
outcome
Signif-
icant find-
2/6 trials
(33%) re-
ported this
outcome
No differ-
11/17 tri-
als
(65%) re-
ported this
outcome
156Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
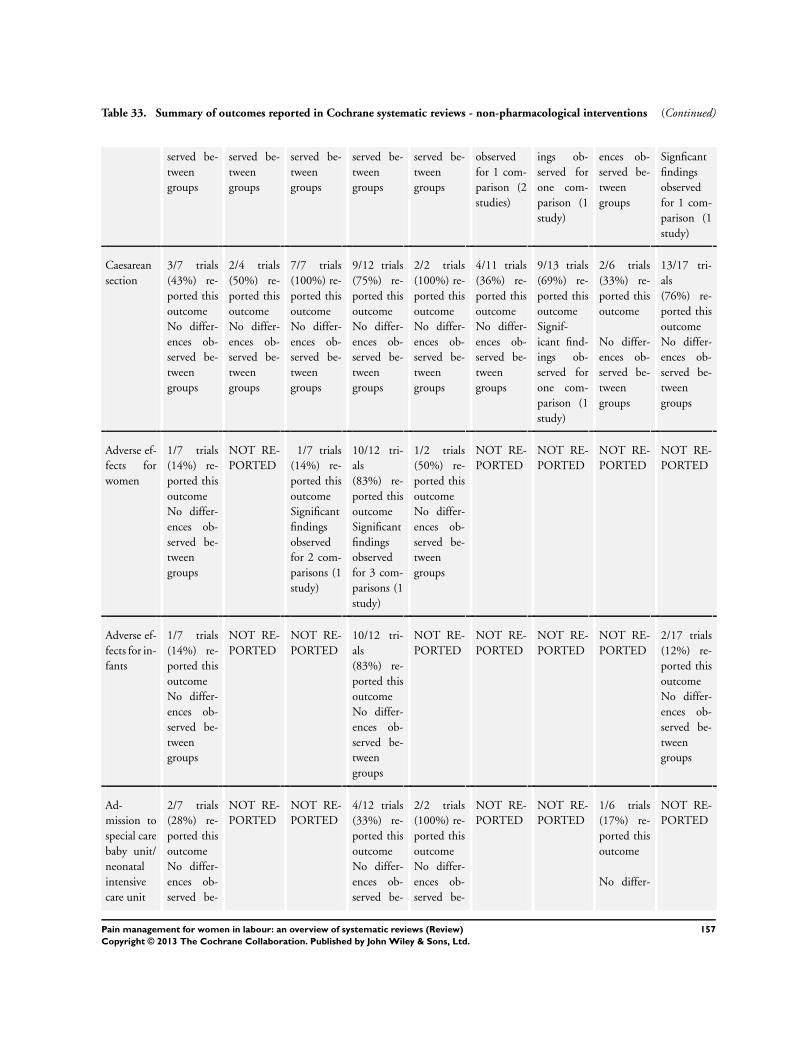
Table 33. Summary of outcomes reported in Cochrane systematic reviews - non-pharmacological interventions (Continued)
served be-
tween
groups
served be-
tween
groups
served be-
tween
groups
served be-
tween
groups
served be-
tween
groups
observed
for 1 com-
parison (2
studies)
ings ob-
served for
one com-
parison (1
study)
ences ob-
served be-
tween
groups
Signficant
findings
observed
for 1 com-
parison (1
study)
Caesarean
section
3/7 trials
(43%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
2/4 trials
(50%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
7/7 trials
(100%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
9/12 trials
(75%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
2/2 trials
(100%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
4/11 trials
(36%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
9/13 trials
(69%) re-
ported this
outcome
Signif-
icant find-
ings ob-
served for
one com-
parison (1
study)
2/6 trials
(33%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
13/17 tri-
als
(76%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
Adverse ef-
fects for
women
1/7 trials
(14%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
1/7 trials
(14%) re-
ported this
outcome
Significant
findings
observed
for 2 com-
parisons (1
study)
10/12 tri-
als
(83%) re-
ported this
outcome
Significant
findings
observed
for 3 com-
parisons (1
study)
1/2 trials
(50%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
Adverse ef-
fects for in-
fants
1/7 trials
(14%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
10/12 tri-
als
(83%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
2/17 trials
(12%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
Ad-
mission to
special care
baby unit/
neonatal
intensive
care unit
2/7 trials
(28%) re-
ported this
outcome
No differ-
ences ob-
served be-
NOT RE-
PORTED
NOT RE-
PORTED
4/12 trials
(33%) re-
ported this
outcome
No differ-
ences ob-
served be-
2/2 trials
(100%) re-
ported this
outcome
No differ-
ences ob-
served be-
NOT RE-
PORTED
NOT RE-
PORTED
1/6 trials
(17%) re-
ported this
outcome
No differ-
NOT RE-
PORTED
157Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 33. Summary of outcomes reported in Cochrane systematic reviews - non-pharmacological interventions (Continued)
tween
groups
tween
groups
tween
groups
ences ob-
served be-
tween
groups
Apgar
score less
than seven
at five min-
utes
1/7 trials
(14%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
7/12 trials
(58%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
5/13 trials
(38%) re-
ported this
outcome
No differ-
ences ob-
served be-
tween
groups
NOT RE-
PORTED
NOT RE-
PORTED
Poor
infant out-
comes at
long-term
follow-up
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
Cost NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
NOT RE-
PORTED
RCT: randomised controlled trial
A P P E N D I C E S
Appendix 1. Search strategies for non-Cochrane reviews
Database of Abstracts of Reviews of Effects (The Cochrane Library 2011, Issue 2 of 4)
#1 MeSH descriptor Labor Pain explode all trees
#2 labor or labour or birth or childbirth
#3 pain or analges*
#4 MeSH descriptor Analgesia, Obstetrical explode all trees
#5 (#2 AND #3)
#6 (#1 OR #4 OR #5)
MEDLINE (via OVID) (1966 to 31 May 2011)
1. (“review” or “review academic” or “review tutorial”).pt.
2. (medline or medlars or embase or pubmed).tw,sh.
3. (scisearch or psychinfo or psycinfo).tw,sh.
4. (psychlit or psyclit).tw,sh.
5. cinahl.tw,sh.
6. ((hand adj2 search$) or (manual$ adj2 search$)).tw,sh.
158Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

7. (electronic database$ or bibliographic database$ or computeri?ed database$ or online database$).tw,sh.
8. (pooling or pooled or mantel haenszel).tw,sh.
9. (retraction of publication or retracted publication).pt.
10. (peto or dersimonian or der simonian or fixed effect).tw,sh.
11. or/2-10
12. 1 and 11
13. meta-analysis.pt.
14. meta-analysis.sh.
15. (meta-analys$ or meta analys$ or metaanalys$).tw,sh.
16. (systematic$ adj5 review$).tw,sh.
17. (systematic$ adj5 overview$).tw,sh.
18. (quantitativ$ adj5 review$).tw,sh.
19. (quantitativ$ adj5 overview$).tw,sh.
20. (quantitativ$ adj5 synthesis$).tw,sh.
21. (methodologic$ adj5 review$).tw,sh.
22. (methodologic$ adj5 overview$).tw,sh.
23. (integrative research review$ or research integration).tw.
24. or/13-23
25. 12 or 24
26. exp Labor Pain/
27. exp Analgesia, Obstetrical/
28. (labor or labour or childbirth or birth).mp. and (pain* or analges*).tw.
29. exp Anesthesia, Obstetrical/
30. 26 or 27 or 28 or 29
31. 25 and 30
EMBASE (via NHS Evidence Health Information Resources) (1980 to 31 May 2011)
1. exp REVIEW/
2. (medline OR medlars OR embase OR pubmed).af
3. (psycinfo OR psychinfo).af
4. cinahl.af
5. (((hand adj2 search$) OR (manual$ ADJ search$))).ti,ab
6. (((electronic ADJ database$) OR (bibliographic ADJ database$))).ti,ab
7. ((pooled ADJ analys$) OR (pooling)).ti,ab
8. (peto OR dersimonian OR (fixed ADJ effect) OR mantel AND haenszel).ti,ab
9. RETRACTED ARTICLE/
10. (scisearch OR psychlit OR psyclit).af
11. 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10
12. 1 AND 11
13. exp META ANALYSIS/
14. meta?analys$.af
15. (systematic$ adj5 review$).af
16. (systematic$ adj5 overview$).af
17. (quantitativ$ adj5 review$).af
18. (quantitativ$ adj5 overview$).af
19. (methodologic$ adj5 review$).af
20. (methodologic$ adj5 overview$).af
21. ((integrative adj5 research adj5 review$) OR (research adj5 integration)).ti,ab
22. (quantitativ$ adj5 synthesi$).af
23. 13 OR 14 OR 15 OR 16 OR 17 OR 18 OR 19 OR 20 OR 21 OR 22
24. 12 OR 23
25. exp LABOR PAIN/
26. exp OBSTETRIC ANALGESIA/
27. exp OBSTETRIC ANESTHESIA/
159Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

28. ((labor OR labour OR birth OR childbirth) AND (pain* OR analges*)).ti,ab
29. 25 OR 26 OR 27 OR 28
30. 24 AND 29
Systematic review search filters (lines 1-25 in the MEDLINE search and 1-24 in the EMBASE search) taken from the Clinical Evidence
website. The EMBASE filter was adapted for the NHS Evidence Health Information Resources version of EMBASE.
W H A T ’ S N E W
Last assessed as up-to-date: 31 October 2011.
Date Event Description
20 May 2013 Amended Number of new (6) and updated (9) Cochrane reviews corrected in the Abstract. NIHR acknowledge-
ment added
C O N T R I B U T I O N S O F A U T H O R S
James Neilson and Zarko Alfirevic conceived the idea of the overview. Leanne Jones, Mohammad Othman and Therese Dowswell
assessed review eligibility and carried out all data extraction and data entry. Therese Dowswell and Leanne Jones co-authored initial
drafts of the overview. James Neilson, Zarko Alfirevic, Simon Gates, Mary Newburn, Sue Jordan and Tina Lavender commented on
draft versions of the protocol and the final overview.
D E C L A R A T I O N S O F I N T E R E S T
None known.
S O U R C E S O F S U P P O R T
Internal sources
• The University of Liverpool, UK.
External sources
• National Institute for Health Research, UK.
Cochrane-NHS Engagement Project No: 10/4000/02
160Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

N O T E S
In future updates the relaxation techniques and manual methods reviews will be split into separate reviews on yoga, music, audio and
massage and reflexology, respectively.
I N D E X T E R M S
Medical Subject Headings (MeSH)
Acupuncture Analgesia; Administration, Inhalation; Analgesia, Epidural [adverse effects; methods]; Analgesia, Obstetrical [adverse
effects; ∗methods]; Analgesics [administration & dosage; adverse effects]; Cesarean Section [utilization]; Immersion; Labor Pain
[∗therapy]; Massage; Patient Satisfaction; Relaxation Therapy [methods]; Review Literature as Topic
MeSH check words
Female; Humans; Pregnancy
161Pain management for women in labour: an overview of systematic reviews (Review)
Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.