palexia sr product information aust r 165332, … · palexia® sr product information aust r...
TRANSCRIPT

1
PALEXIA® SR PRODUCT INFORMATION AUST R 165332, 165346, 165347, 165356, 165357, 229737 NAME OF THE MEDICINE PALEXIA® SR 25 mg tapentadol (as hydrochloride) sustained release tablets PALEXIA® SR 50 mg tapentadol (as hydrochloride) sustained release tablets PALEXIA® SR 100 mg tapentadol (as hydrochloride) sustained release tablets PALEXIA® SR 150 mg tapentadol (as hydrochloride) sustained release tablets PALEXIA® SR 200 mg tapentadol (as hydrochloride) sustained release tablets PALEXIA® SR 250 mg tapentadol (as hydrochloride) sustained release tablets DESCRIPTION PALEXIA® SR sustained release tablets contain tapentadol hydrochloride (HCl) which is a centrally acting synthetic analgesic combining mu agonist and noradrenaline re-uptake inhibition activity in a single molecule. Tapentadol is a white to off-white powder; freely soluble in water and methanol, and soluble in ethanol. The pKa1 is 9.36 and pKa2 is 10.37 determined in 0.15 M KCl solution. The partition coefficient is defined as the ratio of the equilibrium concentrations of a single neutral molecular species in a 1-octanol/aqueous buffered solution 2-phase system. The value of log P for tapentadol hydrochloride in 1-octanol/water is 2.89 ± 0.01. The chemical name for tapentadol HCl is 3-[(1R,2R)-3-(dimethylamino)-1-ethyl-2-methylpropyl]phenol monohydrochloride. The molecular weight of tapentadol HCl is 257.80, and the empirical formula is C14H23NOHCl. The structural formula of tapentadol HCl (CAS number: 175591-09-0) is:
PALEXIA® SR tablets contain 25, 50, 100, 150, 200 or 250 mg tapentadol (as hydrochloride). Excipients in the tablet core (all strengths) are: hypromellose 100,000 mPa-s, microcrystalline cellulose, colloidal anhydrous silica and magnesium stearate. Excipients in the film coating are: hypromellose 6 mPa-s, lactose, talc, macrogol 6000, titanium dioxide (E171), propylene glycol (50, 100, 150, 200 and 250 mg tablets only), macrogol 400 (25 mg tablets only), iron oxide yellow (E172) (25, 100, 150, 200 and 250 mg tablets only), iron oxide red (E172) (25, 150, 200 and 250 mg tablets only), and iron oxide black (E172) (250 mg tablets only). PHARMACOLOGY Pharmacodynamics Tapentadol is a centrally acting synthetic analgesic combining opioid and non-opioid activity in a single molecule. It has 18 times less binding affinity than morphine to the
. HCl
N
OH
(R)(R)
2
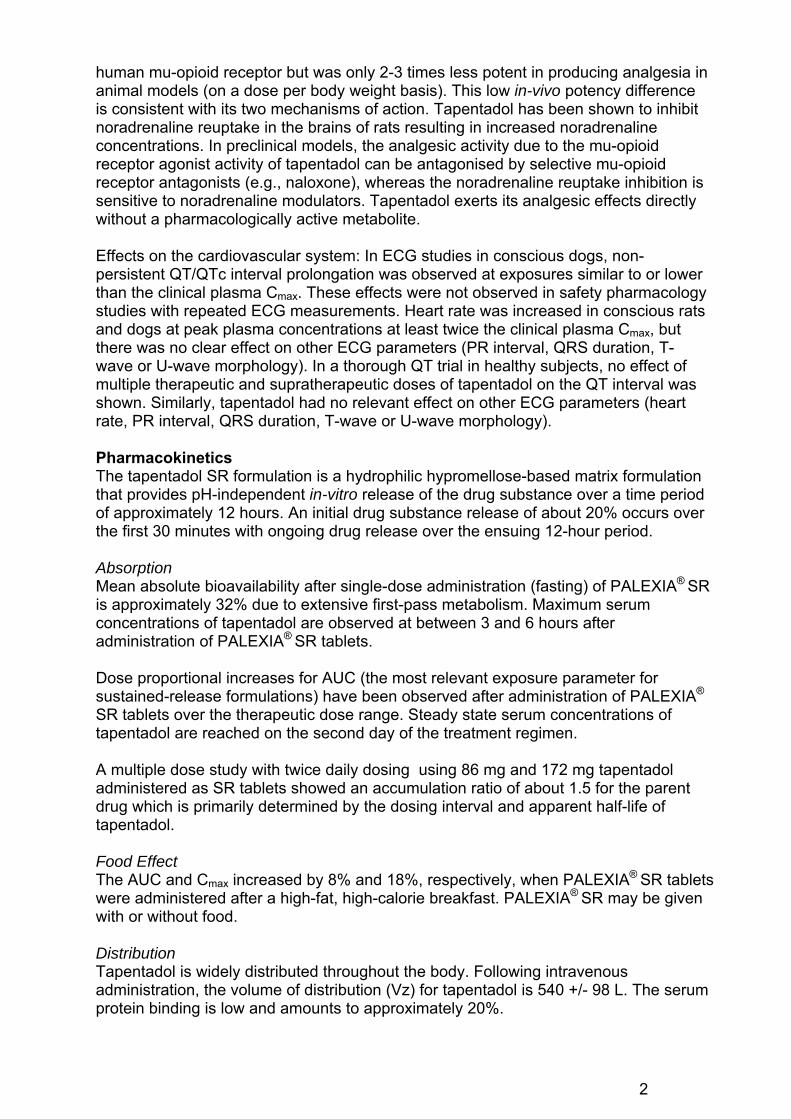
human mu-opioid receptor but was only 2-3 times less potent in producing analgesia in animal models (on a dose per body weight basis). This low in-vivo potency difference is consistent with its two mechanisms of action. Tapentadol has been shown to inhibit noradrenaline reuptake in the brains of rats resulting in increased noradrenaline concentrations. In preclinical models, the analgesic activity due to the mu-opioid receptor agonist activity of tapentadol can be antagonised by selective mu-opioid receptor antagonists (e.g., naloxone), whereas the noradrenaline reuptake inhibition is sensitive to noradrenaline modulators. Tapentadol exerts its analgesic effects directly without a pharmacologically active metabolite. Effects on the cardiovascular system: In ECG studies in conscious dogs, non-persistent QT/QTc interval prolongation was observed at exposures similar to or lower than the clinical plasma Cmax. These effects were not observed in safety pharmacology studies with repeated ECG measurements. Heart rate was increased in conscious rats and dogs at peak plasma concentrations at least twice the clinical plasma Cmax, but there was no clear effect on other ECG parameters (PR interval, QRS duration, T-wave or U-wave morphology). In a thorough QT trial in healthy subjects, no effect of multiple therapeutic and supratherapeutic doses of tapentadol on the QT interval was shown. Similarly, tapentadol had no relevant effect on other ECG parameters (heart rate, PR interval, QRS duration, T-wave or U-wave morphology). Pharmacokinetics The tapentadol SR formulation is a hydrophilic hypromellose-based matrix formulation that provides pH-independent in-vitro release of the drug substance over a time period of approximately 12 hours. An initial drug substance release of about 20% occurs over the first 30 minutes with ongoing drug release over the ensuing 12-hour period. Absorption Mean absolute bioavailability after single-dose administration (fasting) of PALEXIA® SR is approximately 32% due to extensive first-pass metabolism. Maximum serum concentrations of tapentadol are observed at between 3 and 6 hours after administration of PALEXIA® SR tablets. Dose proportional increases for AUC (the most relevant exposure parameter for sustained-release formulations) have been observed after administration of PALEXIA®
SR tablets over the therapeutic dose range. Steady state serum concentrations of tapentadol are reached on the second day of the treatment regimen. A multiple dose study with twice daily dosing using 86 mg and 172 mg tapentadol administered as SR tablets showed an accumulation ratio of about 1.5 for the parent drug which is primarily determined by the dosing interval and apparent half-life of tapentadol. Food Effect The AUC and Cmax increased by 8% and 18%, respectively, when PALEXIA® SR tablets were administered after a high-fat, high-calorie breakfast. PALEXIA® SR may be given with or without food. Distribution Tapentadol is widely distributed throughout the body. Following intravenous administration, the volume of distribution (Vz) for tapentadol is 540 +/- 98 L. The serum protein binding is low and amounts to approximately 20%.

3
Metabolism and Elimination In humans, the metabolism of tapentadol is extensive. About 97% of the parent compound is metabolised. The major pathway of tapentadol metabolism is conjugation with glucuronic acid to produce glucuronides. After oral administration approximately 70% (55% glucuronide and 15% sulfate of tapentadol) of the dose is excreted in urine in the conjugated form. Uridine diphosphate glucuronyl transferase (UGT) is the primary enzyme involved in the glucuronidation (mainly UGT1A6, UGT1A9 and UGT2B7 isoforms). A total of 3% of drug was excreted in urine as unchanged drug. Tapentadol is additionally metabolised to N-desmethyl tapentadol (13%) by CYP2C9 and CYP2C19 and to hydroxy tapentadol (2%) by CYP2D6, which are further metabolised by conjugation. Therefore, drug metabolism mediated by cytochrome P450 system is of less importance than phase 2 conjugation. None of the metabolites contributes to the analgesic activity. Tapentadol and its metabolites are excreted almost exclusively (99%) via the kidneys. The terminal half-life is on average 5-6 hours after oral administration. The total clearance is 1530 +/- 177 ml/min. Elderly patients The mean exposure (AUC) to tapentadol was similar in elderly subjects compared to young adults, with a 16% lower mean Cmax observed in the elderly subject group compared to young adult subjects. Renal Impairment AUC and Cmax of tapentadol were comparable in subjects with varying degrees of renal function (from normal to severely impaired). In contrast, increasing exposure (AUC) to tapentadol-O-glucuronide was observed with increasing degree of renal impairment. In subjects with mild, moderate, and severe renal impairment, the AUC of tapentadol-O-glucuronide was 1.5-, 2.5-, and 5.5-fold higher compared with normal renal function, respectively. Hepatic Impairment Administration of tapentadol resulted in higher exposures and serum levels to tapentadol in subjects with impaired hepatic function compared to subjects with normal hepatic function. The ratios of tapentadol pharmacokinetic parameters for the mild and moderate hepatic impairment groups in comparison to the normal hepatic function group were 1.7 and 4.2, respectively, for AUC; 1.4 and 2.5, respectively, for Cmax; and 1.2 and 1.4, respectively, for t1/2. The rate of formation of tapentadol-O-glucuronide was lower in subjects with increased liver impairment. Pharmacokinetic Interactions Tapentadol is mainly metabolised by Phase 2 glucuronidation, and only a small amount is metabolised by Phase 1 oxidative pathways. As glucuronidation is a high capacity/low affinity system, any clinically relevant interactions caused by Phase 2 metabolism are unlikely to occur. This has been evidenced by clinical pharmacokinetic drug-drug interaction studies with probe drugs naproxen and probenecid with increases in AUC of tapentadol by 17% and 57%, respectively. No changes in the pharmacokinetic parameters of tapentadol were observed when paracetamol and acetylsalicylic acid were given concomitantly. Tapentadol was shown to be a weak inhibitor of human CYP2D6 activity in vitro but at

4
concentrations 180- to 1400-fold higher than maximum concentrations in humans. In vitro induction experiments in human hepatocytes showed that CYP1A2, CYP2C9, and CYP3A4 activities were not markedly induced. Thus in vitro studies did not reveal any potential of tapentadol to either inhibit or induce cytochrome P450 enzymes. Tapentadol is an inducer of CYP1A, CYP2B and CYP2E in rats in vivo. The potential clinical relevance of this finding is unknown. The pharmacokinetics of tapentadol were not affected when gastric pH or gastrointestinal motility were increased by omeprazole and metoclopramide, respectively. Plasma protein binding of tapentadol is low (approximately 20%). Therefore, the likelihood of pharmacokinetic drug-drug interactions by displacement from the protein binding site is low. CLINICAL TRIALS Osteoarthritis and low back pain The efficacy and safety of PALEXIA® SR in the treatment of moderate to severe chronic pain has been investigated in three pivotal Phase III randomised, double-blind, active- and placebo-controlled, parallel-group, multicentre studies; two in patients with moderate to severe chronic pain from osteoarthritis of the knee (clinical trials KF5503/11 and KF5503/12) and one in patients with moderate to severe chronic low back pain (clinical trial KF5503/23). These pain conditions were chosen as they usually present with moderate to severe pain that is often treated with opioids. In three studies, subjects were initially randomised to receive PALEXIA® SR (50 mg twice daily), placebo or oxycodone CR (10 mg twice daily) for the first 3 days. Subjects were then titrated upwards over the following 3 weeks (increments of PALEXIA® SR 50 mg, oxycodone CR 10 mg, or placebo twice daily) to achieve a stable optimum dose. Subjects were allowed paracetamol as rescue medication during the titration period. Subjects received the following maximum (minimum) doses: PALEXIA® SR 250 mg (100 mg) twice daily, oxycodone CR 50 mg (20 mg) twice daily, or placebo twice daily. The study drug was taken with or without food. To enter the 12-week maintenance period, subjects had to be on a stable dose of the study drug for the last 3 days of the titration period without any rescue medication. If needed, subjects could request controlled adjustment of their dose based on their individual analgesia requirements and/or tolerability experience however adjustments were to be kept to a minimum during the maintenance period. All three studies had the same primary endpoints - change from baseline of the average pain intensity over the 12-week maintenance period of the daily pain intensity on an 11-point numerical rating scale (NRS), and change from baseline of the average pain intensity over the last week of the maintenance period at Week 12 of the daily pain intensity on an 11-point NRS. Secondary endpoints included 30% and 50% responder rates and Patient Global Impression of Change scale. The results for these endpoints for all three studies are summarised in Table 1.
5
Meta-analysis of pivotal studies A pre-specified meta-analysis of the data generated in the above three clinical trials was undertaken. The two main objectives of the meta-analysis were to assess the superior safety of PALEXIA® SR compared to oxycodone CR with regards to constipation (gastrointestinal tolerability), and to assess the non-inferior efficacy of PALEXIA® SR compared to oxycodone CR. PALEXIA® SR was superior to oxycodone CR with regards to constipation, nausea and vomiting (gastrointestinal tolerability) (p<0.001). The non-inferiority of PALEXIA® SR to oxycodone CR in relation to the primary endpoint (change from baseline of the average pain intensity over the 12-week maintenance period or at Week 12) (using LOCF) was also demonstrated (both p-values ≤ 0.001) (Table 1).

6
Table 1. Meta-analysis of data generated in studies KF5503/11, KF5503/12 and KF5503/23 (ITT, LOCF); non-inferior efficacy of PALEXIA® SR compared to oxycodone CR.
KF5503/11 (n=1023), Osteoarthritis KF5503/12 (n=987), Osteoarthritis KF5503/23 (n=958), Lower back pain Meta-analysis
Placebo (n=336)
PALEXIA®
SR (n=344)
Oxycodone CR
(n=342)
Placebo (n=336)
PALEXIA®
SR (n=319)
Oxycodone CR
(n=331)
Placebo (n=316)
PALEXIA®
SR (n=312)
Oxycodone CR
(n=323)
Placebo (n=991)
PALEXIA®
SR (n=978)
Oxycodone CR
(n=999) Baseline pain
Mean (SD) 7.2 (1.29) 7.4 (1.35) 7.2 (1.29) 7.3 (1.12) 7.3 (1.09) 7.3 (1.10) 7.6 (1.32) 7.5 (1.32) 7.5 (1.22) 7.4 (1.25) 7.4 (1.26) 7.3 (1.21)
Wk 12 maintenance
Mean (SD) 5.0 (2.61) 4.4 (2.48) 4.7 (2.35) 4.8 (2.47) 4.5 (2.48) 5.0 (2.44) 5.5 (2.57) 4.6 (2.66) 4.6 (2.56) 5.1 (2.56) 4.5 (2.54) 4.8 (2.45)
LS Means diff from placebo Baseline vs
Wk 12a
-0.7 (0.18) -0.3 (0.18) -0.3 (0.18) 0.2 (0.18) -0.8 (0.19) -0.9 (0.19) -0.6 (0.11) -0.3 (0.11)
p-value 95% CIb
<0.001 (-1.04, -0.33)
0.069 (-0.68, 0.02)
0.152
(-0.61, 0.09) 0.279
(-0.16, 0.54)
<0.001 (-1.22, -0.47)
<0.001 (-1.24, -0.49)
<0.001
(-0.80, -0.39) 0.002
(-0.53, -0.12)
Overall maintenance
Mean (SD) 5.1 (2.48) 4.4 (2.40) 4.7 (2.26) 5.0 (2.24) 4.7 (2.28) 5.1 (2.29) 5.5 (2.46) 4.7 (2.52) 4.6 (2.38) 5.2 (2.40) 4.6 (2.40) 4.8 (2.32)
LS Means diff from placebo Baseline vs
overalla
-0.7 (0.17) -0.3 (0.17) -0.2 (0.16) 0.1 (0.16) -0.7 (0.18) -0.8 (0.18) -0.5 (0.10) -0.3 (0.10)
p-value 95% CIb
<0.001 (-1.00, –0.33)
0.049 (-0.67, -0.00)
0.135
(-0.55, 0.07) 0.421
(-0.18, 0.44)
<0.001 (-1.06, -0.35)
<0.001 (-1.16, -0.46)
<0.001
(-0.73, -0.34) <0.001
(-0.52, -0.14)
30% responder
rate 35.9% 43.0%c 24.9%c 40.9% 41.1% 26.0%d 27.1% 39.7%c 36.5% 34.8% 41.3%c 27.0%d
50% responder
rate 24.3% 32.0%c 17.3%d 27.0% 31.0% 22.1% 18.9% 27.0%c 17.4% 23.5% 30.1%c 20.8%
PGIC assessment of very much improved &
much improved
35.5% 58.5%c 47.0%c 43.2% 56.0%c 42.5% 32.7% 55.5%c 60.0%c 37.4% 56.7%c 49.8%c
a: Change from baseline in average pain intensity scores based on numerical rating scale (NRS)a, ITT population; LOCF = last observation carried forward Average pain scores are the averages of all scores recorded during the baseline period or during each time period (Week 12 of maintenance or overall maintenance). b: Test for no difference between treatment from ANCOVA model with factor(s) treatment, pooled centre and baseline pain intensity as covariate (type III SS) unadjusted p-value. c:Indicates statistically significant over placebo d: Indicates statistical significance of placebo over active LS = least square
7
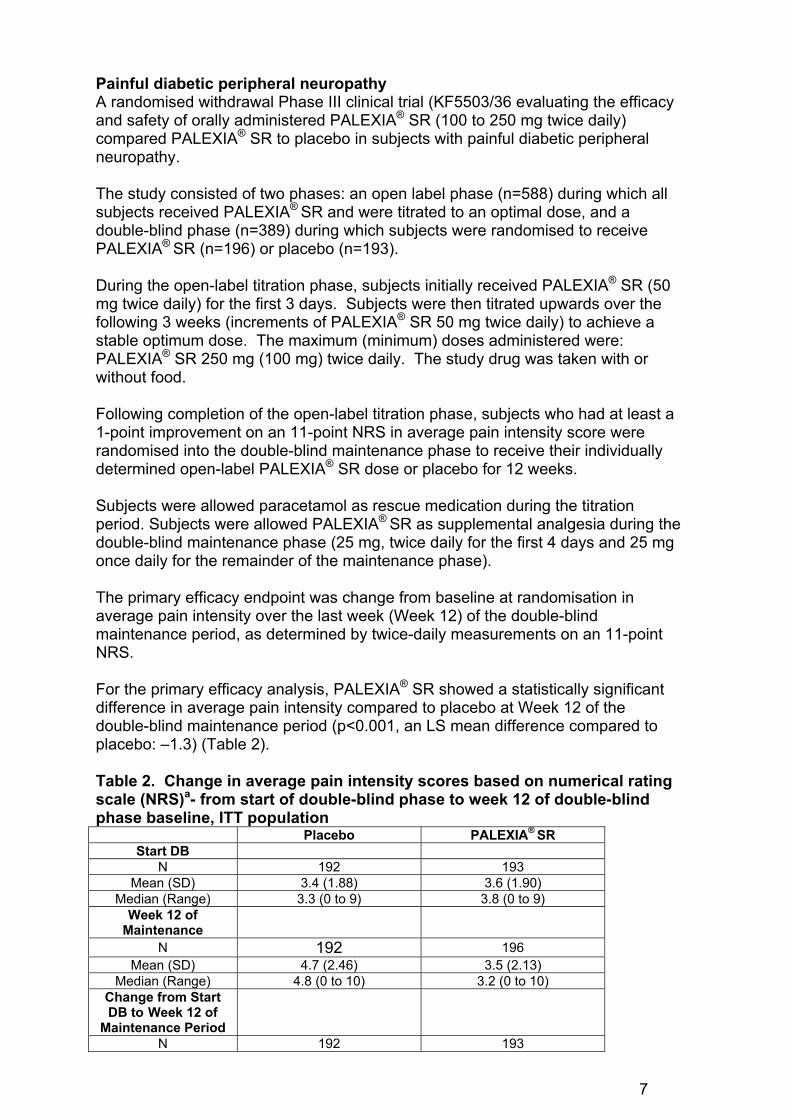
Painful diabetic peripheral neuropathy A randomised withdrawal Phase III clinical trial (KF5503/36 evaluating the efficacy and safety of orally administered PALEXIA® SR (100 to 250 mg twice daily) compared PALEXIA® SR to placebo in subjects with painful diabetic peripheral neuropathy. The study consisted of two phases: an open label phase (n=588) during which all subjects received PALEXIA® SR and were titrated to an optimal dose, and a double-blind phase (n=389) during which subjects were randomised to receive PALEXIA® SR (n=196) or placebo (n=193). During the open-label titration phase, subjects initially received PALEXIA® SR (50 mg twice daily) for the first 3 days. Subjects were then titrated upwards over the following 3 weeks (increments of PALEXIA® SR 50 mg twice daily) to achieve a stable optimum dose. The maximum (minimum) doses administered were: PALEXIA® SR 250 mg (100 mg) twice daily. The study drug was taken with or without food. Following completion of the open-label titration phase, subjects who had at least a 1-point improvement on an 11-point NRS in average pain intensity score were randomised into the double-blind maintenance phase to receive their individually determined open-label PALEXIA® SR dose or placebo for 12 weeks. Subjects were allowed paracetamol as rescue medication during the titration period. Subjects were allowed PALEXIA® SR as supplemental analgesia during the double-blind maintenance phase (25 mg, twice daily for the first 4 days and 25 mg once daily for the remainder of the maintenance phase). The primary efficacy endpoint was change from baseline at randomisation in average pain intensity over the last week (Week 12) of the double-blind maintenance period, as determined by twice-daily measurements on an 11-point NRS. For the primary efficacy analysis, PALEXIA® SR showed a statistically significant difference in average pain intensity compared to placebo at Week 12 of the double-blind maintenance period (p<0.001, an LS mean difference compared to placebo: –1.3) (Table 2). Table 2. Change in average pain intensity scores based on numerical rating scale (NRS)a- from start of double-blind phase to week 12 of double-blind phase baseline, ITT population
Placebo PALEXIA® SR Start DB
N 192 193 Mean (SD) 3.4 (1.88) 3.6 (1.90)
Median (Range) 3.3 (0 to 9) 3.8 (0 to 9) Week 12 of
Maintenance
N 192 196 Mean (SD) 4.7 (2.46) 3.5 (2.13)
Median (Range) 4.8 (0 to 10) 3.2 (0 to 10) Change from Start DB to Week 12 of
Maintenance Period
N 192 193

8
Mean (SD) 1.3 (2.41) -0.1 (1.69) Median (Range) 1.0 (-7 to 9) -0.1 (-7 to 5)
LS Mean Change 1.4 0.0 LS Mean
Difference versus Placebo (SE)
-1.3 (0.20)
95% CI (verses Placebo)
(-1.70, -0.92)
p value (versus Placebo)b
<0.001
a: LOCF=last observation carried forward b: Test for no treatment difference based on the ANCOVA model with treatment, country, dose category and prior opioid use as factors and Start DB pain intensity as a covariate. Average pain scores are the averages of all scores recorded during the 72-hour period before randomisation or during each week. Daily pain intensity is the average of pain scores over a 24-hour period, starting from time of randomization. DB=double-blind
Cancer pain A randomised withdrawal active and placebo controlled double-blind Phase III trial (KF5503/15 evaluated the efficacy and safety of orally administered PALEXIA® SR tablets given twice daily over 4 weeks (Maintenance Phase) in subjects with moderate to severe chronic malignant tumour-related pain in comparison to placebo. The study consisted of two phases: a titration phase (n= 505) where subjects were randomised to receive PALEXIA® SR (n = 345) or morphine PR (n= 160) and were titrated to an optimal dose, and a maintenance phase (n = 328). Subjects who received PALEXIA® SR in the titration phase were re-randomised to PALEXIA® SR (n=107) or placebo (n=112) in the maintenance phase. Subjects who received morphine PR in the titration phase continued to take morphine PR (n = 109) in the maintenance phase. During the titration phase, subjects initially received PALEXIA® SR (100mg twice daily) or morphine PR (40mg twice daily) for the first 3 days. Subjects were then titrated upwards over the following 2 weeks (increments of PALEXIA® SR 50mg or morphine PR 20mg twice daily at minimum 3-day intervals). The maximum (minimum) doses administered were: PALEXIA® SR 250mg (100 mg) twice daily or morphine PR 100mg (40mg) twice daily. The mean (standard deviation [sd]) daily dose was 276.1 mg (66.66 mg) for PALEXIA® SR and 101.8 mg (29.06) for morphine PR. Following completion of the titration phase, subjects who had met the stabilisation criteria (mean pain intensity <5 points/day (11-point NRS)) and mean consumption of rescue medication ≤ 20 mg morphine IR per day) during the last 3 days of the titration phase were re-randomised into the maintenance phase to receive their individually determined titration phase dose of PALEXIA® SR or placebo for 4 weeks. A similar percentage of subjects in the Palexia® SR (216/279 [77%]) and morphine PR (107/129 [83%]) treatment groups completed the titration phase and met the stabilisation criteria. Subjects were allowed morphine IR (10 mg) as rescue medication during the titration phase. No maximum dose was defined. The primary efficacy endpoint was the proportion of subjects classified as responders at the end of the 4 week maintenance phase. Responders were
9
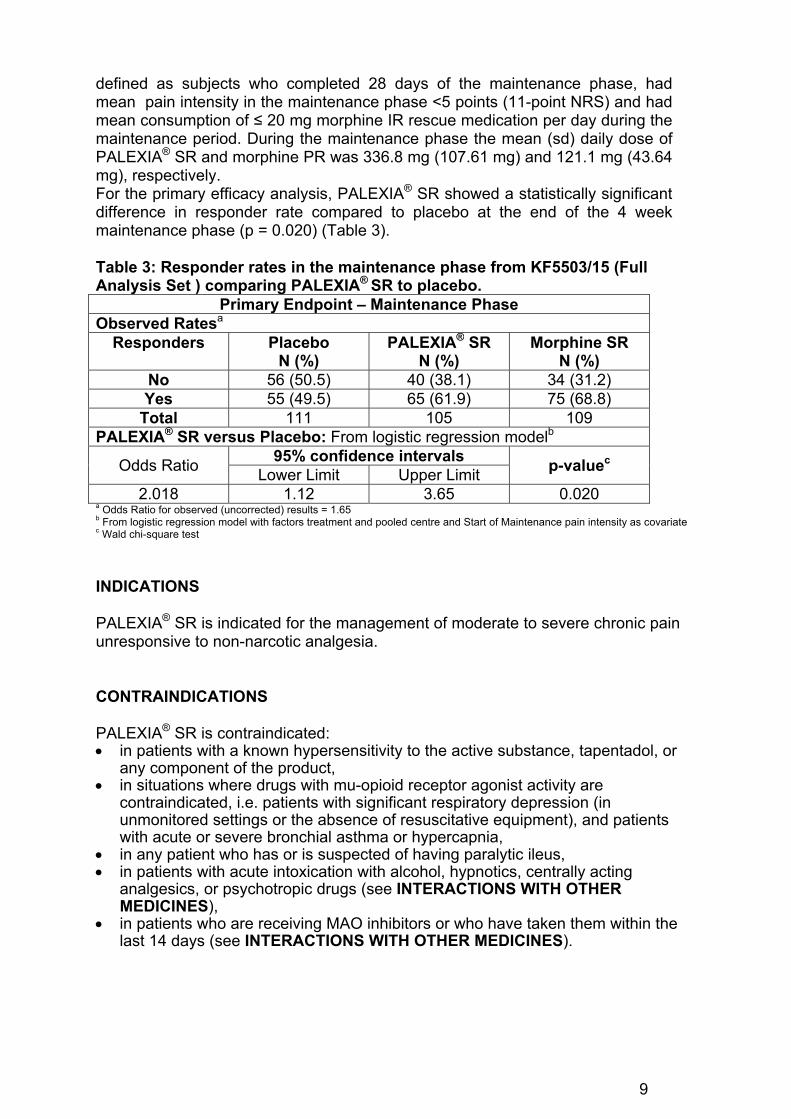
defined as subjects who completed 28 days of the maintenance phase, had mean pain intensity in the maintenance phase <5 points (11-point NRS) and had mean consumption of ≤ 20 mg morphine IR rescue medication per day during the maintenance period. During the maintenance phase the mean (sd) daily dose of PALEXIA® SR and morphine PR was 336.8 mg (107.61 mg) and 121.1 mg (43.64 mg), respectively. For the primary efficacy analysis, PALEXIA® SR showed a statistically significant difference in responder rate compared to placebo at the end of the 4 week maintenance phase (p = 0.020) (Table 3). Table 3: Responder rates in the maintenance phase from KF5503/15 (Full Analysis Set ) comparing PALEXIA® SR to placebo.
Primary Endpoint – Maintenance Phase Observed Ratesa
Responders Placebo N (%)
PALEXIA® SR N (%)
Morphine SR N (%)
No 56 (50.5) 40 (38.1) 34 (31.2) Yes 55 (49.5) 65 (61.9) 75 (68.8)
Total 111 105 109 PALEXIA® SR versus Placebo: From logistic regression modelb
Odds Ratio 95% confidence intervals
p-valuec Lower Limit Upper Limit
2.018 1.12 3.65 0.020 a Odds Ratio for observed (uncorrected) results = 1.65 b From logistic regression model with factors treatment and pooled centre and Start of Maintenance pain intensity as covariate c Wald chi-square test
INDICATIONS PALEXIA® SR is indicated for the management of moderate to severe chronic pain unresponsive to non-narcotic analgesia. CONTRAINDICATIONS PALEXIA® SR is contraindicated: in patients with a known hypersensitivity to the active substance, tapentadol, or
any component of the product, in situations where drugs with mu-opioid receptor agonist activity are
contraindicated, i.e. patients with significant respiratory depression (in unmonitored settings or the absence of resuscitative equipment), and patients with acute or severe bronchial asthma or hypercapnia,
in any patient who has or is suspected of having paralytic ileus, in patients with acute intoxication with alcohol, hypnotics, centrally acting
analgesics, or psychotropic drugs (see INTERACTIONS WITH OTHER MEDICINES),
in patients who are receiving MAO inhibitors or who have taken them within the last 14 days (see INTERACTIONS WITH OTHER MEDICINES).
10
PRECAUTIONS
Potential for Abuse As with other drugs that have mu-opioid receptor agonist activity, PALEXIA® SR has a potential for abuse. This should be considered when prescribing or dispensing PALEXIA® SR in situations where there is concern about an increased risk of misuse, abuse, or diversion. Drugs that have mu-opioid receptor agonist activity may be abused by crushing, chewing, snorting or injecting the product. Such practices pose a significant risk to the abuser and may result in overdose or death. All patients treated with drugs that have mu-opioid receptor agonist activity should be carefully monitored for signs of abuse and addiction. Drug Dependence Tolerance: Repeated administration of opioids may lead to tolerance. Tolerance is the need for increasing doses of opioids to maintain a defined effect such as analgesia, in the absence of disease progression or other external factors. Withdrawal symptoms: Withdrawal symptoms could occur after abrupt discontinuation of treatment with tapentadol (see DOSAGE and ADMINISTRATION). In a study conducted over 12 months, 22.4% of patients given PALEXIA® SR had objective signs of opioid withdrawal compared with 27.3% given oxycodone CR when assessed between 2 - 5 days after the last dose of study drug. Only 4.8% of patients given PALEXIA® SR and 4.5% given oxycodone CR were considered by investigators to have moderate withdrawal. No subjects had moderately severe or severe withdrawal. Respiratory Depression At high doses or in mu-opioid receptor agonist sensitive patients, PALEXIA® SR may produce dose-related respiratory depression. Therefore, PALEXIA® SR should be administered with caution to patients with impaired respiratory functions. Alternative non-mu-opioid receptor agonist analgesics should be considered and PALEXIA® SR should be employed only under careful medical supervision at the lowest effective dose in such patients. If respiratory depression occurs, it should be treated as any mu-opioid receptor agonist-induced respiratory depression (see OVERDOSAGE). Head Injury and Increased Intracranial Pressure Like other drugs with mu-opioid receptor agonist activity, PALEXIA® SR should not be used in patients who may be particularly susceptible to the intracranial effects of carbon dioxide retention such as those with evidence of increased intracranial pressure, impaired consciousness, or coma. Analgesics with mu-opioid receptor agonist activity may obscure the clinical course of patients with head injury. PALEXIA® SR should be used with caution in patients with head injury and brain tumors. Seizures PALEXIA® SR has not been systematically evaluated in patients with a seizure disorder, and such patients were excluded from clinical studies. However, like other analgesics with mu-opioid receptor agonist activity PALEXIA® SR should be prescribed with care in patients with a history of a seizure disorder or any condition that would put the patient at risk of seizures.

11
Renal Impairment For patients with mild or moderate renal impairment, no dosage adjustment is recommended (see DOSAGE AND ADMINISTRATION). PALEXIA® SR has not been studied in controlled efficacy studies in patients with severe renal impairment, therefore use in this population is not recommended (see DOSAGE AND ADMINISTRATION and also Pharmacokinetics). Hepatic Impairment For patients with mild hepatic impairment, no dosage adjustment is recommended (see DOSAGE AND ADMINISTRATION). A study of tapentadol (PALEXIA® IR) in subjects with hepatic impairment showed higher serum concentrations than in those with normal hepatic function. PALEXIA® SR should be used with caution in patients with moderate hepatic impairment (see DOSAGE AND ADMINISTRATION and also Pharmacokinetics). PALEXIA® SR has not been studied in patients with severe hepatic impairment and, therefore, use in this population is not recommended (see DOSAGE AND ADMINISTRATION and also Pharmacokinetics). Use in Pancreatic/Biliary Tract Disease Drugs with mu-opioid receptor agonist activity may cause spasm of the sphincter of Oddi. PALEXIA® SR should be used with caution in patients with biliary tract disease, including acute pancreatitis. Effect on fertility There were no apparent effects on the fertility of male rats at intravenous doses up to 12 mg/kg/day, although histopathology analyses were not conducted. In female rats, the numbers of corpora lutea and implantations were reduced, and pre- and post-implantation losses were increased, at intravenous tapentadol doses associated with maternal toxicity. The clinical relevance of these findings is unknown. Use in pregnancy (Category C) There are no adequate and well controlled studies of tapentadol in pregnant women. PALEXIA® SR should be used during pregnancy only if the potential benefit justifies the potential risk to the foetus. The effect of tapentadol on labour and delivery in humans is unknown. PALEXIA® SR is not recommended for use in women during and immediately prior to labour and delivery. Due to the mu-opioid receptor agonist activity of tapentadol, neonates whose mothers have been taking tapentadol should be monitored for respiratory depression. Tapentadol crosses the placenta in pregnant rats. Tapentadol was evaluated for teratogenic effects in rats and rabbits following intravenous and subcutaneous administration during organogenesis. Embryofetal toxicity such as delays in skeletal maturation and cerebral ventricular dilation was observed in rats concomitant with maternal toxicity at subcutaneous doses of 10 mg/kg/day or greater (plasma AUC exposure less than maximum anticipated clinical exposure). Subcutaneous administration of tapentadol to rabbits revealed embryofoetal toxicity at doses of 10-

12
24 mg/kg/day (AUC exposure 1 to 2 fold the maximum anticipated human exposure), along with reduced foetal viability, skeletal delays and other variations, and multiple malformations including gastroschisis/thoracogastroschisis, amelia/phocomelia and cleft palate at 10-24 mg/kg/day, and ablepharia, encephalopathy and spina bifida at 24 mg/kg/day. There were no teratogenic effects observed in similar studies conducted in rats and rabbits via the intravenous route (up to 15 mg/kg/day) Embryofoetal toxicity, including malformations, may be secondary to maternal toxicity in these species. Use in lactation There is limited information on the excretion of tapentadol in breast milk. Tapentadol is excreted into milk in lactating rats following oral dosing. Oral tapentadol administration to rats during lactation resulted in increased postnatal pup mortality, at doses lower than those associated with maternal toxicity (exposure (AUC) less than maximum anticipated clinical exposure). The potential relevance to humans is unknown. Physicochemical and available pharmacodynamic/toxicological data on tapentadol point to excretion in breast milk and risk to the suckling child cannot be excluded. PALEXIA® SR should not be used during breast feeding. Paediatric use PALEXIA® SR is not recommended for use in children below 18 years of age due to insufficient data on safety and efficacy in this population. Use in the elderly (persons aged 65 years and over) In general, recommended dosing for elderly patients with normal renal and hepatic function is the same as for younger adult patients with normal renal and hepatic function. Because elderly patients are more likely to have decreased renal and hepatic function, care should be taken in dose selection as recommended (see DOSAGE AND ADMINISTRATION and also Pharmacokinetics). Carcinogenicity Tapentadol was administered to rats (diet) and mice (oral gavage) for two years. A significant trend towards increased hepatocellular tumours (adenoma and carcinoma) was observed in mice at oral doses of 100 mg/kg/day or greater. A dose-related increased incidence of hepatocellular hypertrophy (but not tumours) was observed in rats at dietary doses of 125 mg/kg/day or greater. Exposures (plasma AUC) in both species were less than that at the maximum recommended clinical dose. These findings may derive from adaptive changes following hepatic enzyme induction. The potential clinical relevance is unknown. Genotoxicity Tapentadol did not induce gene mutations in bacteria, but was clastogenic at cytotoxic concentrations in an in vitro chromosomal aberration test with metabolic activation in Chinese hamster V79 cells in 1 of 2 assays. The one positive result for tapentadol was not confirmed in vivo in rats, using the two endpoints of chromosomal aberration and unscheduled DNA synthesis at extrapolated exposures (AUC) similar to the maximum anticipated human exposure. The weight of evidence indicates that tapentadol presents no significant genotoxic potential at clinical doses.

13
Effects on Ability to Drive and Use Machines Like drugs with mu-opioid receptor agonist activity, PALEXIA® SR may have a major influence on the ability to drive and use machines, due to the fact that it may adversely affect central nervous system functions (see ADVERSE EFFECTS). This has to be expected especially at the beginning of treatment, at any change of dosage as well as in connection with alcohol or tranquilizers (see INTERACTIONS WITH OTHER MEDICINES). Patients should be cautioned as to whether driving or use of machines is permitted. INTERACTIONS WITH OTHER MEDICINES Tapentadol is mainly metabolised by glucuronidation, a system with a very high capacity which is not easily saturated even in disease. As therapeutic concentrations of drugs that are subject to glucuronidation are generally well below the concentrations needed for potential inhibition of glucuronidation, the risk of clinically relevant interaction between these drugs is generally low. The following substances have been included in a set of interaction studies without any clinically significant finding: paracetamol, acetylsalicylic acid, naproxen, probenecid, omeprazole and metoclopramide (see Pharmacokinetics). Only a small amount of tapentadol is metabolised by oxidative pathways (see Pharmacokinetics). Tapentadol was shown to be a weak inhibitor of human CYP2D6 activity in vitro but at concentrations 180- to 1400-fold higher than maximum concentrations in humans. In vitro induction experiments in human hepatocytes showed that CYP1A2, CYP2C9, and CYP3A4 activities were not markedly induced. Thus in vitro studies did not reveal any potential of tapentadol to either inhibit or induce cytochrome P450 enzymes. Tapentadol is an inducer of CYP1A, CYP2B and CYP2E in rats in vivo. The potential clinical relevance of this finding is unknown. Mu-opioid agonists/antagonists There is no clinical data on the concomitant use of PALEXIA® SR with mixed opioid agonist/antagonists or partial mu-opioid agonists. As with pure mu-opioid agonists, the analgesic effect provided by the mu-opioid component of PALEXIA® SR may be theoretically reduced in such circumstances. Therefore, care should be taken when combining PALEXIA® SR with these medicinal products. CNS depressants Patients receiving other mu-opioid receptor agonist analgesics, general anesthetics, phenothiazines, other tranquilizers, sedatives, hypnotics or other CNS depressants (including alcohol and illicit drugs) concomitantly with PALEXIA® SR may exhibit an additive CNS depression. Interactive effects resulting in respiratory depression, hypotension, profound sedation, or coma may result if these drugs are taken in combination with PALEXIA® SR. When such combined therapy is contemplated, the reduction of dose of one or both agents should be considered. Monoamine oxidase (MAO) inhibitors PALEXIA® SR is contraindicated in patients who are receiving monoamine oxidase (MAO) inhibitors or who have taken them within the last 14 days due to potential additive effects on noradrenaline levels which may result in adverse cardiovascular events (see CONTRAINDICATIONS).

14
Serotonin Syndrome PALEXIA® SR is a centrally acting synthetic analgesic combining mu-agonist and noradrenaline re-uptake inhibition activity A causal relationship between tapentadol and serotonin syndrome has not been established. However, in isolated cases there have been reports of serotonin syndrome in a temporal connection with the therapeutic use of tapentadol in combination with serotoninergic medicinal products such as selective serotonin re-uptake inhibitors (SSRIs), serotonin and noradrenaline reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), MAOIs and triptans. Signs of serotonin syndrome may include confusion, agitation, fever, sweating, ataxia, hyperreflexia, myoclonus and diarrhoea. Withdrawal of the serotonergic drugs usually brings about a rapid improvement. Treatment depends on the nature and severity of the symptoms. ADVERSE EFFECTS Treatment emergent adverse events in the double-blind Phase 2/3 studies (osteoarthritis, low back pain, diabetic peripheral neuropathy) In the pooled Phase 2/3 PALEXIA® SR studies, the percentage of subjects administered PALEXIA® SR with at least 1 TEAE was 71.7%. This was higher when compared with the placebo group (54.5%) and lower than the oxycodone CR group (86.3%) (Table 4). Compared with oxycodone CR there was better gastrointestinal tolerability with PALEXIA® SR. The incidence of nausea (19.5%), vomiting (7.4%) and constipation (13.6%) was lower with PALEXIA® SR than oxycodone CR (36.1%, 19.8% and 31.5%, respectively) (Table 4). PALEXIA® SR also had a beneficial safety profile over that of oxycodone CR for somnolence (11.3% vs 16.3%), dizziness (13.7% vs 19.8%), and pruritus (4.9% vs 12.4%). This suggests that the adverse event profile for PALEXIA® SR is similar to those of other opioid agonists, while at the same time exhibiting a lower incidence of a number of adverse events. The majority of subjects in all treatment groups in the pooled all Phase 2/3 PALEXIA® SR studies experienced TEAEs that were mild to moderate in intensity. Less subjects in the all PALEXIA® SR group reported severe adverse events compared to those in the oxycodone CR group. Table 4. TEAEs in at least 5% of subjects in any pooled treatment group (all studies) (PALEXIA® SR formulation Phase 2/3 studies integrated summary of safety: safety analysis set)a
System organ class/preferre
d term
Placebo (n=1498)
n (%)
All PALEXIA® SR
(n=3613) n (%)
All oxycodone CR
(n=1472) n (%)
Number (n (%)) of
subjects with TEAE
817 (54.5) 2589 (71.7) 1271 (86.3)
Gastrointestinal disorders
370 (24.7) 1464 (40.5) 952 (64.7)
Nausea 128 ( 8.5) 704 (19.5) 531 (36.1) Constipation 85 ( 5.7) 493 (13.6) 464 (31.5)

15
Vomiting 44 ( 2.9) 269 ( 7.4) 292 (19.8) Dry mouth 26 ( 1.7) 217 ( 6.0) 66 ( 4.5) Diarrhoea 78 ( 5.2) 199 ( 5.5) 78 ( 5.3) Nervous system
disorders 288 (19.2) 1308 (36.2) 662 (45.0)
Dizziness 77 ( 5.1) 495 (13.7) 291 (19.8) Headache 170 (11.3) 427 (11.8) 174 (11.8)
Somnolence 44 ( 2.9) 408 (11.3) 240 (16.3) General
disorders and administratio
n site conditions
138 ( 9.2) 583 (16.1) 290 (19.7)
Fatigue 48 ( 3.2) 253 ( 7.0) 139 ( 9.4) Skin and
subcutaneous tissue
disorders
80 ( 5.3) 481 (13.3) 332 (22.6)
Pruritus 20 ( 1.3) 176 ( 4.9) 183 (12.4) Hyperhidrosis 16 ( 1.1) 160 ( 4.4) 75 ( 5.1)
a: This summary of clinical safety includes clinical studies that vary in design (controlled dose adjustment, fixed dose, and open label) and subject population (lower back pain, pain due to OA, and pain due to peripheral neuropathy). Studies included: KF5503/09, KF5503/10, KF5503/19, KF5503/20, KF5503/24, KF5503/11, KF5503/12, KF5503/23, KF5503/36 MedDRA version 11.0 was used for coding. TEAE = treatment emergent adverse events; MedDRA = Medical Dictionary for Regulatory Activities; N, n = number of subjects (total, per category).
Treatment emergent adverse events in the double-blind Phase III cancer pain studies The safety analyses for the pooled Phase III cancer trials (KF5503/15 and KF5503/16) were performed for the titration phases and maintenance phases separately. All groups could receive rescue medication (morphine IR). For the titration phase, the percentage of subjects administered PALEXIA® SR with at least 1 TEAE was 52.0% compared to 64.0% for those administered morphine PR. Compared to morphine PR, there was better gastrointestinal tolerability with PALEXIA® SR. The incidence of nausea (12.3%), vomiting (7.0%), dry mouth (1.5%) and constipation (13.5%) was lower with PALEXIA® SR than morphine PR (22.2%, 14.3%, 5.8%, and 16.4% respectively) (Table 5). For the maintenance phase, the percentage of subjects administered PALEXIA® SR with at least 1 TEAE was 62.0%. This was higher when compared with the placebo group (57.1%) and lower than the morphine PR group (64.6%). Compared to morphine PR, there was better gastrointestinal tolerability with PALEXIA® SR (30.7% versus 27.3% respectively) (Table 5). The incidence of diarrhoea (0.8%) was lower with PALEXIA® SR than morphine PR (6.3%) (Table 5). During the titration and maintenance phases, the intensity of TEAEs was mild or moderate in most subjects in all treatment groups. There was no notable difference between the groups, or any notable differences for each of the system organ classes or TEAEs with the exception of neoplasms benign, malignant and unspecified in the maintenance phase. The higher incidence of neoplasms in the

16
PALEXIA® SR group was classified as unrelated to tapentadol and due to the underlying disease. Table 5: TEAEs in at least 5% of subjects in titration and maintenance phases of pooled Phase III cancer pain trials - (KF5503/15 and KF5503/16a – safety analysis set).
System Organ Class/preferred term
Placebo (n) %
PALEXIA® SR (n) %
Morphine PR (n) %
Titration phase - n=400 n=189
Number (n (%)) of subjects with TEAE
- 208 (52.0) 121 (64.0)
Gastrointestinal disorders
- 120 (30.0) 84 (44.4)
Constipation - 54 (13.5) 31 (16.4) Nausea - 49 (12.3) 42 (22.2) Vomiting - 28 (7.0) 27 (14.3)
Dry mouth - 6 (1.5) 11 (5.8) Nervous system
disorders - 57 (14.3) 28 (14.8)
Dizziness - 21 (5.3) 11 (5.8) Somnolence - 16 (4.0) 12 (6.3)
Maintenance phase n=126 n=121 n=127 Number (n (%)) of
subjects with TEAE 72 (57.1) 75 (62.0) 82 (64.6)
Gastrointestinal disorders
40 (31.7) 33 (27.3) 39 (30.7)
Nausea 19 (15.1) 17 (14.0) 14 (11.0) Constipation 13 (10.3) 13 (10.7) 14 (11.0)
Vomiting 4 (3.2) 10 (8.3) 9 (7.1) Diarrhoea 5 (4.0) 1 (0.8) 8 (6.3)
Neoplasms benign, malignant and
unspecified (including cysts and polyps)
8 (6.3) 15 (12.4) 6 (4.7)
Neoplasm malignant 6 (4.8) 11 (9.1) 5 (3.9) Metabolism and
nutrition disorders 9 (7.1) 10 (8.3) 9 (7.1)
Decreased appetite 7 (5.6) 8 (6.6) 8 (6.3) Skin and
subcutaneous tissue disorder
2 (1.6) 7 (5.8) 13 (10.2)
Hyperhidrosis 1 (0.8) 4 (3.3) 7 (5.5) a This study was terminated due to poor recruitment and an FDA recall of rescue medication
The following adverse drug reactions (ADRs) were reported from clinical trials performed with PALEXIA® SR: Very Common (≥ 1/10) Nervous system disorders: Dizziness, Somnolence, Headache Gastrointestinal disorders: Nausea, Constipation
17
Common (1/100 to <1/10) Metabolism and nutrition disorders: Decreased appetite Psychiatric disorders: Anxiety, Depressed mood, Sleep disorder,
Nervousness, Restlessness Nervous system disorders: Disturbance in attention, Tremor, Muscle contractions involuntary Vascular disorders: Flushing Respiratory, thoracic and mediastinal disorders: Dyspnoea Gastrointestinal disorders: Vomiting, Diarrhoea, Dyspepsia Skin and subcutaneous tissue disorders: Pruritus, Hyperhidrosis, Rash General disorders and administration site conditions: Asthenia, Fatigue, Feeling of body
temperature change, Mucosal dryness, Oedema
Uncommon (1/1,000 to <1/100) Immune system disorders: Drug hypersensitivity Metabolism and nutrition disorders: Weight decreased Psychiatric disorders: Disorientation, Confusional state,
Agitation, Perception disturbances, Abnormal dreams, Euphoric mood
Nervous system disorders: Depressed level of consciousness, Memory impairment, Mental impairment, Syncope, Sedation, Balance disorder, Dysarthria, Hypoaesthesia, Paraesthesia
Eye disorders: Visual disturbance Cardiac disorders: Heart rate increased, Heart rate
decreased, palpitations Vascular disorders: Blood pressure decreased Gastrointestinal disorders: Abdominal discomfort Skin and subcutaneous tissue disorders: Urticaria Renal and urinary disorders: Urinary hesitation, Pollakiuria Reproductive system and breast disorders: Sexual dysfunction General disorders and administration site conditions: Drug withdrawal syndrome, Feeling
abnormal, Irritability Rare (1/10,000 to <1/1,000) Psychiatric disorders: Drug dependence, Thinking abnormal Nervous system disorders: Convulsion, Presyncope, Coordination abnormal Respiratory, thoracic and mediastinal disorders: Respiratory depression Gastrointestinal disorders: Impaired gastric emptying General disorders and administration site conditions: Feeling drunk, Feeling of relaxation Treatment emergent adverse events with prolonged treatment

18
A total of 894 subjects with moderate to severe pain from low back pain or osteoarthritis of the knee or hip were treated with a flexible dosing regimen of PALEXIA® SR (100 mg to 250 mg twice daily) in a 1 year safety study (KF5503/24). The overall TEAE profile for prolonged treatment did not differ from the profile observed in short-term treatment. The overall incidence of TEAEs was lower in the PALEXIA® SR group (85.7%) compared to oxycodone CR (20 mg to 50 mg) (90.6%). The most common TEAEs (incidence >10% in either treatment group) were constipation, nausea, vomiting, somnolence, dizziness, headache, fatigue and pruritus. Subjects administered PALEXIA® SR had a lower incidence of constipation, nausea, vomiting, dizziness, fatigue and pruritus compared to oxycodone CR (22.6% vs 38.6%, 18.1% vs 33.2%, 7.0% vs 13.5%, 14.8% vs 19.3%, 9.7% vs 10.3%, and 5.4% vs 10.3% respectively). Post marketing experience In addition to adverse events reported in clinical trials, the following adverse events have been observed during post approval use of PALEXIA®. As these events are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Suicidal ideation has been reported during post approval use of PALEXIA®. Post-marketing rare events of angioedema, anaphylaxis and anaphylactic shock have been reported. DOSAGE AND ADMINISTRATION As with many centrally acting analgesic medications, the dosing regimen should be individualised according to the severity of pain being treated, the previous treatment experience and the ability to monitor the patient. PALEXIA® SR should be taken twice daily, approximately every 12 hours. PALEXIA® SR should be taken whole with sufficient liquid. PALEXIA® SR may be administered with or without food. Initiation of therapy a) Initiation of therapy in patients currently not taking opioid analgesics:
Patients should start treatment with single doses of 50 mg PALEXIA® SR administered twice daily.
b) Initiation of therapy in patients currently taking opioid analgesics: When switching from opioids to PALEXIA® SR and choosing the initial dose, the nature of the previous medication, administration and the mean daily dose should be taken into account.
Titration and maintenance After initiation of therapy the dose should be titrated individually to a level that provides adequate analgesia and minimizes side effects under the close supervision of the prescribing physician.

19
Experience from clinical trials has shown that a titration regimen in increments of 50 mg PALEXIA® SR twice daily every 3 days was appropriate to achieve adequate pain control in most of the patients. For dose adjustments 25 mg PALEXIA® SR may also be used. Total daily doses of PALEXIA® SR tablets greater than 500 mg tapentadol have not been studied and are therefore not recommended. Discontinuation of treatment Withdrawal symptoms could occur after abrupt discontinuation of treatment with tapentadol. When a patient no longer requires therapy with tapentadol, it may be advisable to taper the dose gradually to prevent symptoms of withdrawal (see PRECAUTIONS). Renal Impairment No dosage adjustment is recommended in patients with mild or moderate renal impairment (see Pharmacokinetics). PALEXIA® SR has not been studied in controlled efficacy studies in patients with severe renal impairment, and its use is not recommended. A pharmacokinetic study showed an increased level of an inactive metabolite in subjects with renal impairment (see PRECAUTIONS and also Pharmacokinetics). Hepatic Impairment No dosage adjustment is recommended in patients with mild hepatic impairment (see Pharmacokinetics). PALEXIA® SR should be used with caution in patients with moderate hepatic impairment. Treatment in these patients should be initiated at 25 mg or 50 mg PALEXIA® SR and not be administered more frequently than once every 24 hours. Further treatment should reflect maintenance of analgesia with acceptable tolerability (see PRECAUTIONS and also Pharmacokinetics). PALEXIA® SR has not been studied in patients with severe hepatic impairment and, therefore, use in this population is not recommended (see PRECAUTIONS and also Pharmacokinetics). Elderly Patients (persons aged 65 years and over) In general, recommended dosing for elderly patients with normal renal and hepatic function is the same as for younger adult patients with normal renal and hepatic function. Because elderly patients are more likely to have decreased renal and hepatic function, care should be taken in dose selection as recommended (see PRECAUTIONS and also Pharmacokinetics). Paediatric Patients PALEXIA® SR is not recommended for use in children below 18 years of age due to insufficient data on safety and efficacy in this population (see PRECAUTIONS). OVERDOSAGE Experience with PALEXIA® SR overdose is very limited. Preclinical data suggest that symptoms similar to those of other centrally acting analgesics with mu-opioid receptor agonist activity are to be expected upon intoxication with tapentadol. In

20
the clinical setting, these symptoms may include miosis, vomiting, cardiovascular collapse, consciousness disorders up to coma, convulsions and respiratory depression up to respiratory arrest. Management of overdose should be focused on treating symptoms of mu-opioid receptor agonism. Primary attention should be given to re-establishment of a patent airway and institution of assisted or controlled ventilation when overdose of PALEXIA® SR is suspected. Pure opioid antagonists such as naloxone, are specific antidotes to respiratory depression resulting from opioid overdose. Respiratory depression following an overdose may outlast the duration of action of the opioid antagonist. Administration of an opioid antagonist is not a substitute for continuous monitoring of airway, breathing, and circulation following an opioid overdose. If the response to opioid antagonists is suboptimal or only brief in nature, an additional antagonist should be administered as directed by the manufacturer of the product. Gastrointestinal decontamination may be considered in order to eliminate unabsorbed drug. Gastrointestinal decontamination with activated charcoal or by gastric lavage may be considered within 2 hours after intake. Before attempting gastrointestinal decontamination, care should be taken to secure the airway. Contact the Poisons Information Centre on 131 126 for further advice on overdosage management. PRESENTATION AND STORAGE CONDITIONS There are six (6) distinct strengths of PALEXIA® SR sustained release tablets: PALEXIA SR 25 mg tapentadol (as hydrochloride) sustained release
tablets: slightly brownish-orange film-coated oblong shaped tablets with Grünenthal logo engraving on one side and “H9” engraving on the other side
PALEXIA SR 50 mg tapentadol (as hydrochloride) sustained release tablets: white film-coated oblong shaped tablets with Grünenthal logo engraving on one side and “H1” engraving on the other side.
PALEXIA SR 100 mg tapentadol (as hydrochloride) sustained release tablets: pale yellow film-coated oblong shaped tablets with Grünenthal logo engraving on one side and “H2” engraving on the other side.
PALEXIA SR 150 mg tapentadol (as hydrochloride) sustained release tablets: pale pink film-coated oblong shaped tablets with Grünenthal logo engraving on one side and “H3” engraving on the other side.
PALEXIA SR 200 mg tapentadol (as hydrochloride) sustained release tablets: pale orange film-coated oblong shaped tablets with Grünenthal logo engraving on one side and “H4” engraving on the other side.
PALEXIA SR 250 mg tapentadol (as hydrochloride) sustained release tablets: brownish red film-coated oblong shaped tablets with Grünenthal logo engraving on one side and “H5” engraving on the other side.
Blister Packs of 7, 10, 14, 20, 28, 30, 40, 50, 56, 60, 90, 100 tablets.

21
Not all tablet strengths or pack sizes may be available. PALEXIA SR 25 mg, 50 mg, 100 mg, 150 mg, 200 mg and 250 mg sustained release tablets have a shelf-life of 36 months when stored below 30C. Protect from light. NAME AND ADDRESS OF SPONSOR Seqirus Pty Ltd ABN 26 160 735 035 63 Poplar Road Parkville, VIC 3052 Australia POISON SCHEDULE OF THE MEDICINE Controlled Drug, S8 Date of first inclusion in the Australian Register of Therapeutic Goods: 19 January 2011 Date of most recent amendment: 27 March 2017 PALEXIA® is a registered trademark of Grünenthal GmbH, used under licence.