palliation of malignant dysphagia3
TRANSCRIPT

Palliation of Malignant Dysphagia
Jason Klapman, MD FASGEDirector of EndoscopyMoffitt Cancer Center
Tampa, FL
Definition
To Palliate-From the Latin Palliatus-to cloak or conceal. To palliate a disease is to treat it partially and
insofar as possible, but not cure it completely. Easing the severity of a pain or a disease without
removing the cause

OUTLINE Methods of Palliation Endoscopic Management of TE Fistulas

Methods of Palliation
Dilation Ablation Radiation Stenting

Endoscopic dilation
Temporary relief of dysphagia Balloon or polyvinyl Bougies Goal to 15-16mm will allow most foods Need for repeat sessions Associated procedure risks
Aspiration Perforation

Ablation Methods
Nd:YAG laser APC PDT CRYO

Nd:YAG
Neodymium-yttrium-aluminum-garnet Fleisher et al. Am J Surg. 1982
A new palliative approach for esophageal cancer Fulgurating the esophageal cancer to make a
larger lumen. Generally requires multiple sessions Can be challenging at the cervical esophagus or
GE junction Risk of perforation is up to 7%*
Lightdale et al. GIE Dec1995

APC
Argon Plasma Coagulation Monopolar, non-contact method causes tissue
coagulation Main complication is bleeding Most useful in combination therapy
CONSORT 1a trial Rupinski et al. Am J of Gastro Sept 2011 93 pt’s randomized to APC with HDR,PDT or APC alone Time to first dysphagia recurrence was 88,59 and 35days
respectively APC with HDR fewest complications and highest QoL
PDT
Photodynamic Therapy Uses a photosensitizing agent in combination with laser
exposure to ablate malignant tissue Porfiner sodium (Photofrin) is the only photosensitizing agent
available in US More effective than other ablative techniques
Lightdale et al. GIE Dec 1995 Multicenter randomized trial of PDT vs. Nd:Yag laser for palliation of esophageal cancer
PDT equally efficacious and better tumor response Easier to perform Less complications than Nd:Yag (1% vs 7%)
Use is limited by photosensitivity and high cost
Cryotherapy
Used for early or superficial recurrent esophageal cancer
Not routinely used for palliation

Radiation
High-dose Brachytherapy (HDR) Localized treatment with high-dose radiation with sparing of the
surrounding structures Depth of 1cm and length adjustable to tumor length
Timing of Brachytherapy As Monotherapy? Before or after Stenting? In combination with
esophageal stenting or other modalities? HDR as Monotherapy
Homs et al. Lancet 2004 Brachytherapy better for long term palliation for patients with life
expectancy >3months but less than 6 months Stenting better for patients with <3months life expectancy
HDR combination therapy CONSORT 1a showed benefit in combination with APC Berquist et al. Dis Esophagus Jul 2012
Combined stent insertion and HDR pilot study 12 patients received stent insertion and then single dose of 12Gy Relief of dysphagia in 10/11 Median survival was 6.6months
Hirdes et al. GIE Aug 2012 Combination of Biodegradable stent and single-dose
brachytherapy Brachy 12Gy first then stent placement 19 patients 28 complications in 17patients (mainly pain and vomiting) causing
premature ending of study

Esophageal Stenting
ASGE Guidelines GIE March 2013 Esophageal Stenting should be the preferred method
for palliation of malignant dysphagia and Fistulae Provides immediate and durable relief in the majority
of patients

Esophageal Stents Types
Plastic or Metal Fully Covered Partially covered Uncovered Biodegradable
Choosing a stent
Majority are Metal stents Most SEMS are equally effective in relieving
symptoms, have similar complication rates No study has been done comparing all types of metal
stents Choice usually determined by perceived ease of
placement and personal experience of endoscopist
Low incidence of migration is the holy grail!!
Choosing a stent (con’t)
Stent characteristics Delivery systems Deployment patterns Expansile force Foreshortening characteristics Removability

Available Esophageal Stents (U.S.) Boston Scientific
Polyflex -strong expansile force,removable 16-21mm 9-12-15cm length Ultraflex- distal and proximal release option, most flexible, least expansile force
(partially or uncovered) 18 or 23 mm, 10,12,15cm lengths Wallflex-, no foreshortening, smooth delivery vs. Ultraflex, lasso loop
(fully/partially) 18 or 23mm 10,12,15cm Cook Endoscopy
Evolution-no shortening, recapturable, lasso loop, distal release only(fully18,20 -8,10,12cm or partially 20mm, 8,10,12.5,15
Z stent - no shortening, short bare wire at ends, has anti-reflux valve option (fully, partially, anti-reflux)18mm, 8,10,12,14
Merrit Medical EndoTek Alimaxx-E-non-foreshortening, fully covered, lasso loop, distal release only
multiple sizes 12-22mm 7,10,12cm lengths EndoMaxx-non-forshortening,fully covered,Metal loop, 19,23mm ,7,10,12,15cm
Endochoice-Bonastent- Fully covered, Hook/Cross technology, Non-foreshortening, retrieval lasso-18mm 6-16cm length
TaeWoong- Niti-S TTS, fully covered ,lasso loop 18mm, 6-15cm ,(
Non-TTS placement
A stiff 0.035 guidewire for stability, over which stent is deployed
Remove endoscope leaving wire in place Back load stent over wire and advance through
stricture Can place endoscope alongside stent to observe
deployment if desired (No fluoroscopy needed) Choose stent that is 4cm longer than tumor to
allow for 2cm above and below tumor for stability

Non-TTS placement

TTS placement
Niti-s esophageal stent 10.5 fr diameter deployment system Use therapeutic upper scope Proximal release
After stent placement
Starts clears and slowly advance to soft foods
Give post stent diet instructions-tailor it to the size of stent
Analgesics prn for pain

Complications
Chest pain Bleeding Perforation Aspiration Severe GERD Dysphagia: tumor ingrowth, migration, food
impaction, device malposition Tracheal Esophageal (TE) Fistula formation
OUTLINE Methods of Palliation Endoscopic Management of TE Fistulas
Case History 65 y.o definitive chemo XRT for proximal
squamous cell esophageal cancer Developed non-malignant XRT stricture 6mos
post treatment Underwent serial dilations ( 3 over 6 weeks
w/limited improvement) Feedings mainly through G-tube Presented with worsening dysphagia and cough
and CXR c/w pneumonia
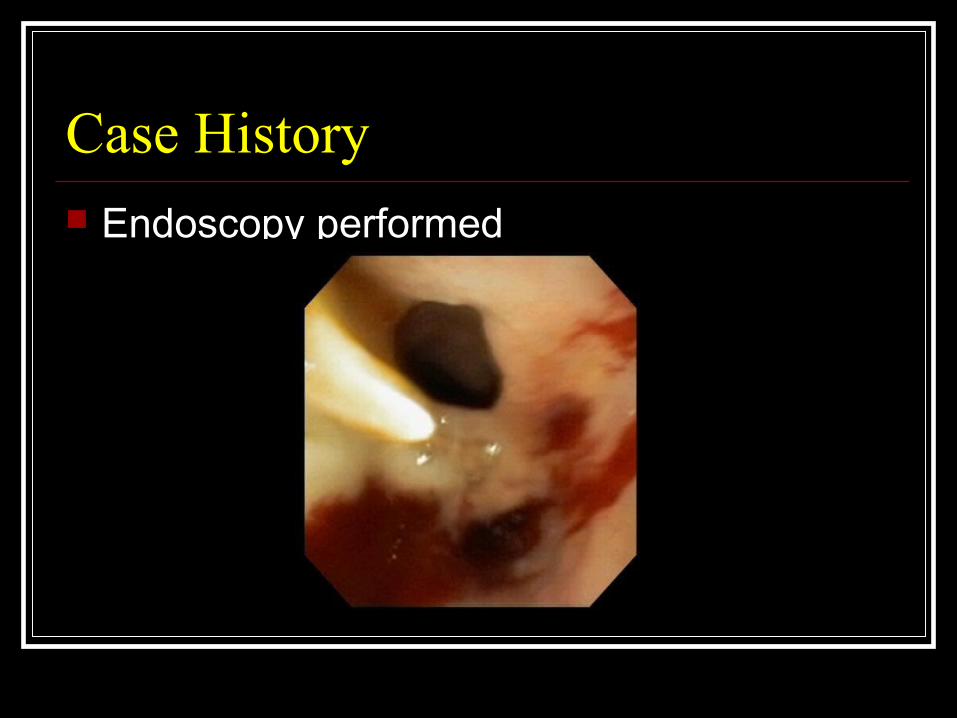
Case History Endoscopy performed

Management of TE Fistula
Etiology Malignant vs. Benign Pre-treatment vs. during treatment
Risk factors Previous radiation Location (never distal) In situ esophageal Stent

Endoscopic options
Placement of a fully covered esophageal stent is the preferred treatment

TTS stent insertion for TE-Fistula
Stenting for TE-Fistula
Success rate is 70%-85% (consider double stenting)
Leave stent in for 4-6 weeks and re-evaluate Unsuccessful
Consider re-stenting Clipping (OTSC) +/- stenting Fibrin Glue application +/- Clipping +/-stenting Surgery bypass or mucus fistula

Summary
Palliation in esophageal cancer has one primary goal To allow patients to maintain oral intake and improve quality of
life Multiple palliative options are available which
may be used as monotherapy, in combination, or sequentially. Endoscopic stenting is now the preferred initial treatment
modality for both palliation of dysphagia and treatment of TE-fistula
Choosing the right stent involves many factors including physician preference, esophageal stricture characteristics and location, and patients clinical scenario
Thank You!!