pardon me, i speak jive - kotaonline.orgkotaonline.org/events/conference/2016/handouts/pardon me i...
TRANSCRIPT

Pardon me, I speak Jive Utilizing Outcomes in the Clinical Practice Mike Reynolds OT, CHT
Via Christi Therapy Center at Founders Circle
Wichita KS
Question
•How do you currently assess your effectiveness in treating pt’s?
•Do you currently track your effectiveness in providing OT?
• If not…..why?

My Occupational Therapy Journey
• Began as an acute care therapist at via Christi St. Francis Hospital 2001
• Briefly specialized in inpatient cardiac, neuro, trauma
• Transitioned into inpatient burn rehabilitation
• Accepted outpatient hand therapist position, combining both acute care/acute burn with outpatient hands/outpatient burn rehabilitation.
• Built outpatient practice and transitioned into full-time outpatient hands/outpatient burn therapy
• Excepted outpatient hands position within physician office in 2011- current.
Chalking the field……..
• Observation of differing treatment methods/ practitioners • Realization I don’t really know
why I’m doing what I’m doing.. Is it evidenced based? What is evidenced based? • Too busy adding to my toolbox
without a thorough ‘cleansing’. • Consumed by learning the latest
and greatest……adding tx methods/ techniques without ever establishing a ‘baseline or pulse’ on my own outcomes.
My Journey
• CHT quest for knowledge and referrals.
• Sit back, and let them roll in…
• Ok, now what???!
• I now have the credentials, but realized I don’t speak the language.
Jive Talking
• Video
• Video explanation.
Physician ----- therapist communication barrier
Data -----vs------cookies and trinkets
How do we do this?
• We have to know our audience to speak their language.
Ultimately, we have to change our language.
We have to start speaking jive.

Research and Definitions
• “There are three kinds of lies: lies, damned lies, and statistics.”
Mark Twain
• People can make facts and numbers mean almost anything. Interpret yours so that your listeners draw the same conclusions you intend.
Supporting Research
• …Not only do clinical outcomes constitute a form of valuable evidence for informed patient health care, but they also represent the means by which we can evaluate the effectiveness of evidence-based rehabilitation.⁴⁻⁵
• Evidence based practitioner should be regarded as a clinical attitude, mindset, were approached by which health care decisions are based on the best available evidence, the practitioners clinical experience, and the patient’s values and expectations.¹
• It is through the assessment of clinical outcomes that clinicians can engage the effectiveness of their treatments and clinicians and researchers can partner to establish the evidence needed to support the use of specific medical interventions.²
Supporting Resarch cont.
• Without the objective knowledge of the patient’s perception of their own health, it is difficult to establish whether they experienced true and meaningful improvements that are important to them as result of medical intervention.²
How to speak Jive
• Although the concept a simple, collecting, analyzing, and interpreting clinical outcomes can be quite challenging.⁶⁻⁷
• To speak the language we have to look at our practice from a different angle. We MUST look to outcomes to fuel our clinical decisions.
• What do I mean by that? Lets work backwards. To reach a final destination (jive talking), we need to pack first………
• If our goal is to assess the effectiveness of a protocol or treatment, then we must have something to compare it to. I.e. a baseline consisting of previous outcomes.

Questions…
- What information do we need to know to evaluate if a treatment technique works? Protocol is better?
- How is Evidence-based practice established?
discussion
What do you need to know?
• …….if clinicians are not educated on clinical outcomes assessments, the likelihood of them incorporating outcome measures into their daily practice is relatively low.²
• Lets chalk another field….
• Definitions:
Clinician and Patient rated outcomes:
• Definition of Clinician- outcomes assessed from the clinician’s point of view and are typically represented by changes occurring at an impairment level. …. These are often characterized by clinical evaluations such as strength, range of motion, and laxity.²
• Definition of Patient- these are outcomes assessed by the patient and provide insight into the patient’s health condition from his or her own perspective. ²
• For the longest time, therapist’s relied on clinician rated outcomes to satisfy their final assessment of patient’s progress and to assist with discharge planning.
• Examples would include patient achieving a long-term goal of shoulder flexion above 130° with strength within available range measuring 4/5.
Which is most important?
•BOTH! • Patient-rated measures must be used to evaluate the
outcome of care and guide treatment, because they measure the impact of the disease or injury on the patient’s ability to perform activities and participate in life, work, and sports. Clinician-related impairment measures should primarily be used to guide treatment decision making with respect to intervention choices.⁹

• Currently, there is a greater dependence on the clinician-rated impairment measures than self-report patient-rated outcome measures in daily clinical practice.³¯⁸
• Since we all would agree that everyone in this room has a firm handle on clinician rated outcomes , let’s spend time understanding the world of patient rated outcomes.

How to Choose the Correct Patient-rated Tool • Terms:
• Validity: your findings truly represent the phenomenon you are claiming to measure.
• Reliability: the degree to which an assessment tool produces stable and consistent results.
• Standardized: use closed-ended questionnaire formats or specific protocols for implementation, provide scores that allow quantitative assessment of ability, and have been evaluated for their psychometric properties.
• Outcome Measures: used to determine the change in ability from before to after an intervention.
• Ceiling effect: the tool given is too easy that all pt.’s score very high • Floor effect: the examination is too difficult where most pt.'s score
are very low. • Is the tool you choose recognized by the American Association of
Orthopedic Surgeons? American Hand Society? • Is it ‘accepted’ as valid and reliable? • Is your tool sensitive enough to capture the data your looking for?

How to Choose the Correct Patient-rated Tool • My example: how to find an appropriate outpt UE tool that
can be:
• Easy to administer
• Simple to score
• Nationally recognized
• Locally recognized


Once you choose an outcome tool…..
• Outcome tools used for treatment decision making and documenting outcomes must have established measurement properties.⁹
• Need to Know- • Standard error of the measure (SEM). SEM=standard deviation x (1-internal
consistency coefficient of reliability coefficient)
• Minimal detectable difference (MDC). MDC= smallest detectable difference. This allows the clinician to evaluate a pt.'s response to treatment.
• Minimally clinically important difference (MCID). MCID= the smallest amount of change in a measure that is associated with change that is important or perceived as beneficial to the patient and as such isn’t index of responsiveness.
• NOTE: the MCD values can be used in the same manner as the MCID for clinical decision making
• Confidence interval (CI) : a range of values so defined that there is a specified probability that the value of a parameter lies within it.

Example
• A patient who completes the disability of the arm, shoulder and hand(DASH) measure at the initial evaluation has a score of 30/100
• What do we need to know about the Quick DASH to interpret the above?
• DASH scoring : 0–100 points, 0 = no disability
• DASH’s SEM = 7.4.
• SO…the clinician can be 90 percent confident (CI) that the patient’s score is 30 ± 7.4 points on the DASH.

Example
• Same patient retakes the DASH 3 weeks later and scores a 15/ 100
• Pt now has a 15 point improvement in DASH score
• What do we need to know about the Quick DASH to interpret the above?
• DASH scoring : 0–100 points, 0 = no disability
• DASH’s MCD= 10.5
• DASH’s MCID= 10.2
• SO…the clinician can be 90 percent confident (CI) that :
1. true change has occurred (MCD of > 10.5)
2. the pt perceives a meaningful change / improvement has occurred (MCID > 10.2).
Therapist ‘Buy-In’
• …….the true beauty and power of clinical outcomes assessment lies in collaborative efforts between clinicians. If gathered as a collective group (eg, within a single clinic, between numerous affiliated regional sites, or a national patient-based research network), the information can be pulled together, allowing for more detailed analysis, brought her generalized patient’s, and further insight into the effectiveness ( or ineffectiveness) of current clinical practices.²
• Nonetheless, it is important to consider that outcomes research requires the corporation of practicing clinicians who are willing to document their clinical records and patient now comes in a manner that allows for quantification and entry into a large database, without compromising their ability to provide efficient care.⁷

Therapist ‘Buy-In’
• ….although there are several challenges associated with the incorporation of patient rated outcomes into standard patient care, this year magnitude of the potential benefits, as related to patient care, clinical research, and professional standing within the healthcare system, far outweigh any initial inconveniences…….²

What’s it gonna take to get you to drive this baby home today..
The ‘Pitch’
• Pucker up and kiss…….the data example for our Via Christi Clinics. powerpoint


PUCKER-UP AND KISS……….
the DATA!
How do you measure
success in your clinic?
THE TRANSITION
“….there has been a significant shift in the way evidence is
used to make clinical decisions about therapeutic
interventions….more attention is needed to improve our
understanding of the accuracy of commonly used
assessments… this is the only way we can properly integrate
evidence for diagnostic accuracy of clinical test into our
practice and truly consider ourselves as evidence-based
practitioners.” (Simoneau- 2010)

GENERAL SENTIMENT
“..although in the back of our mind, we need to
prove what we’re doing is effective with
outcome measures, you’re on such a treadmill
you’re cutting corners or you just can’t do some
of the things you would like”
(some physio in Canada- 2002)

THE MEAT-
Outcome management allows the organization to define quality for itself, leading to an honest appraisal of its own practices, and to further generate means to reach target levels (luquire and Houston, 1997)
What’s needed?
Staff must facilitate a shared vision of best practice in all areas of operations.
Buy in…what’s it gonna take to get you in this baby today?!
Def: Outcome assessment is the measurement of the change that occurred, and how the type and amount of change affected the client's quality of life, life satisfaction, and occupational performance. (Bondoc -2004)
Ultimately, funding agencies and patients are more interested in performance indicators related to function and activity levels, than more traditional musculoskeletal physiotherapy outcomes such as range of movement or muscle strength. (Hefford et al 2008)
We need a common language!! In order to make comparisons and benchmark nationally/ regionally, we need it!!!
With the costs of healthcare rising, administrators and clinicians are under growing pressure to demonstrate effectiveness of therapy by using functional, activity related outcome measures. (Unsworth et al 2004)
Better education of clinicians about the value of collecting outcomes

BARRIERS
Time take to complete the
outcomes
Lack of knowledge about
the outcome measures
Seriously….more
paperwork?
Inconvenience.

BENEFITS
Facilitates communication with colleagues and
families and enhances collaborative clinical
decision making….in short, health care
providers need standardized measures to
assist with examination, prognosis, and
outcome evaluation, as described in the
elements of physical and occupational therapy
practice
(Ketelaar 2008)
The debate as to which is the most appropriate
outcome measure for musculoskeletal clinical practice
must take into account the pros and cons of various
perspectives, formats and frameworks, as well as
validity, reliability, responsiveness to change,
generalizability, and practical efficiency.
(Hefford – 2008)
Lucky for you……we already did this!

WHAT’S COOLER THAN THAT?

YEP, THAT’S A PIG HEAD..

GOD FATHER OF SOUL…I REST MY CASE
MORE LIKE THIS
NECK DISABILITY INDEX (NDI)
Used in over 300 publications, translated into 22 languages, endorsed by a number of clinical
practice guideline committees. Making the NDI the most widely used and most strongly
validated instrument for assessing suffering disability in patients with neck pain. (McDermid
2009)
Administration Burden- completion time ranges from 3-10 minutes
Developed using the Oswestry Low Back Pain Index as a template. Contains 10 items
measured on a 6-point scale from 0 (no disability) to 5 (full disability).
The numeric response for each item is summed for a score varying from 0 to 50.
Minimal Detectable Change (MDC) is accepted as 5 points.
Short term therapy goals should require a minimum of 5 points change
Clinically Important Difference (CID) is accepted as 7points.
Long-term treatment goals should be set for a minimum 7-point reduction in score to
demonstrate treatment benefits

NECK DISABILITY INDEX (NDI)
‘Normal Score’- (bunch of research here- no clearly accepted range)
Vernon and Mior 2000 suggest:
No Disability - 0-4
Mild Disability - 5-14
Moderate Disability 15-24
Complete Disability > 35
Sterling et al 2004 suggest:
No Disability - 0-8
Mild Disability - 10-28
Moderate to Severe Disability >30
LOWER EXTREMITY FUNCTIONAL SCALE
(LEFS)
LEFS- a self-reported measure designed to assess the functional status of patients
with any musculoskeletal condition related to the lower extremity.
Error associated with a given measurement = ± 5 scale points
Clinicians can be reasonably confident that an observed score is within 5 points
of the pt’s “true” score
The Minimal Detectable Change (MDC) of the LEFS is 9 scale points
Clinicians can be reasonably confident that change on the LEFS of greater than
9 points is a true changes
SO…. We can use this information to base short- and long-term goals for
functional change that are at least greater than the MDC (9 points)
MODIFIED OSWESTRY BACK PAIN DISABILITY
QUESTIONNAIRE (ODQ)
Developed by John O’Brien in 1976. First published in 1980. It is, perhaps, the most
widely used outcome measure in low back pain disability, having been translated
into several languages and used in many studies. (Page et al. 2002)
• Administration Burden - completion time ranges from 3-10 minutes – Trina (rock-
star PT @ founders)
Minimal Detectable Change- (MDC) is accepted as 6 points
SO…. We can use this information to base short- and long-term goals for
functional change that are at least greater than the MDC (6 points)

MODIFIED OSWESTRY BACK PAIN DISABILITY
QUESTIONNAIRE (ODQ)
‘Normal Score’- (bunch of research here- no clearly accepted range)
-Fairbank, J.C., & Pynsent, P.B. (2000) The Oswestry disability index. Spine, 25,
2940-2953
-0% to 20% - minimal disability
-20% to 40% - moderate disability
-40% to 60% - severe disability
-60% to 80% - crippled
-80% to 100% - bed bound (or exaggerating symptoms)
DISABILITY OF ARM SHOULDER HAND
(DASH)
….overall, the DASH is the most extensively studied tool and
has the most supporting evidence for good clinimetric quality,
with positive results for all criteria… (Schoneveld et al 2009)
Administrative burden: 5-7 minutes (secret nerd- founders circle)
Minimal Detectable Change: 10.5 points
Clinicians can be reasonably confident that change on the DASH of greater than 15 points
is a true changes
SO…. We can use this information to base short- and long-term goals for
functional change that are at least greater than the MDC (10.5 points)

EXAMPLES
DASH
LTG:
Pt will score ≤ 28 on the DASH to represent significant clinical
improvement with left UE use during self care/ mobility completion.
(X 4weeks)
www.orthopaedicscores.com

KNEE OUTCOME SURVEY
Research usability. The KOS-ADL is reliable, valid, and appropriate for
measuring change following nonsurgical and surgical interventions in a
variety of knee conditions. However, researchers should be aware that if
subjects being evaluated are highly physically active, this instrument is not
necessarily valid. (NATALIE J. COLLINS et al. 2011)
Administrative burden: 5 minutes
Minimal Detectable Change: 11.4 points
Clinicians can be reasonably confident that change on the KOS of greater than or equal to
12 points is a true change
Please use this information to base short- and long-term goals for functional change that are at
least greater than the MDC (12 points)

TINETTI
Research usability: The maximum score for gait component is
12. The maximum score for balance component is 16. Total
maximum score is 28. In general, pt’s who score below 19 are
at high risk for falls. Pt’s who score in the range of 19-24
indicate that the pt has a risk for falls. http://www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=899&Source=http%3A%2F%2Fwww%2Erehabmeasures%2Eorg%2Frehabweb%2Fallmeasures%2Easpx%3FPaged
%3DTRUE%26p%5FTitle%3DTimed%2520Backwards%2520Walk%26p%5FID%3D1136%26View%3D%257b0C859D90%252d7478%252d4C9B%252d9575%252d784C4A9A2D85%257d
%26PageView%3DShared%26PageFirstRow%3D301
Administration burden: 10 minutes.
Minimal Detectable Change: not established.

BERG BALANCE SCALE
Purpose: A 14-item objective measure designed to assess static balance and fall risk in adult populations
Description: Static and dynamic activities of varying difficulty are performed. Item-level scores range from 0-4, determined by ability to perform the assessed activity. Item scores are summed. Maximum score = 56
Administrative burden: 15 min
Minimal Detectable Change: Elderly:
(Donoghue et al, 2009; Elderly)
Berg Balance Scale Initial Score MDC
0 - 24 4.6
25 - 34 6.3
35 - 44 4.9
45 - 56 3.3
SO…. We can use this information to base short- and long-term goals for functional change that are at least greater than the MDC (see above)
OXFORD HIP SCALE
Research usability: There are 12 items in the instrument. Each of the items has 5 categories
of response. Each item is scored 1 to 5 (from least to most difficult) and the items are added
together. The minimum score is a 12 indicating least difficulty. The maximum score is a 60
indicating most difficulty
Administrative burden: 5 Minutes or less
Minimal Detectable Change: 6.11 (research based on Hip Osteoarthritis) .
SO…. We can use this information to base short- and long-term goals for
functional change that are at least greater than the MDC (7 points)

TIMED UP AND GO (TUG)
Description: The patient sits in the chair with his/her back against the chair back. On the command “go”, the patient rises from the chair, walks 3 meters at a comfortable and safe pace, turns, walks back to the chair and sits down. Timing begins at the instruction “go” and stops when the patient is seated . Scores range from 1 to 5 based on the observer's perception of the patient’s risk of falling (Mathias et al, 1986). Podsiadlo & Richardson, 1991, quantified the test by recommending timing (sec) the time between the command to start, till the buttocks touch the chair. The patient should have one practice trial that is not included in the score (Podsiadlo & Richardson, 1991). Patient must use the same assistive device each time he/she is tested to be able to compare scores
Administrative burden: <3 minutes Minimal Detectable Change: see below
Alzheimer’s Disease:
(Ries et al, 2009, Alzheimer’s Disease) MDC = 4.09 seconds
Chronic Stroke:
(Flansbjer et al, 2005) MDC (calculated from Flansbjer et al, 2005) = 2.9 seconds. Smallest Real Difference (SRD) = 23%
Parkinson's Disease:
(Dal Bello-Haas et al, 2011, PD). MDC = 4.85 seconds. (Huang et al, 2011; n = 72; mean age = 67.5 (11.6) years; mean baseline TUG = 11.8 seconds; DGI = 21.6 points; Chinese language sample, PD). MDC = 3.5 seconds. (Steffen & Seney, 2008; n = 37, mean age = 71 (12); mean H&Y score = 2 (range = 1–4); mean disease duration = 14 (6) years, PD) MDC = 11 seconds
SCI:
(Lam et al, 2007; SCI meta analysis; AIS A, B, C, D; C2-L1; only subjects able to complete the walking test were included, calculated from van Hedel 2005, Acute SCI)
Smallest Real Difference= 10.8 seconds, found to detect significant clinical change in the TUG, Smallest Real Difference % = 30%
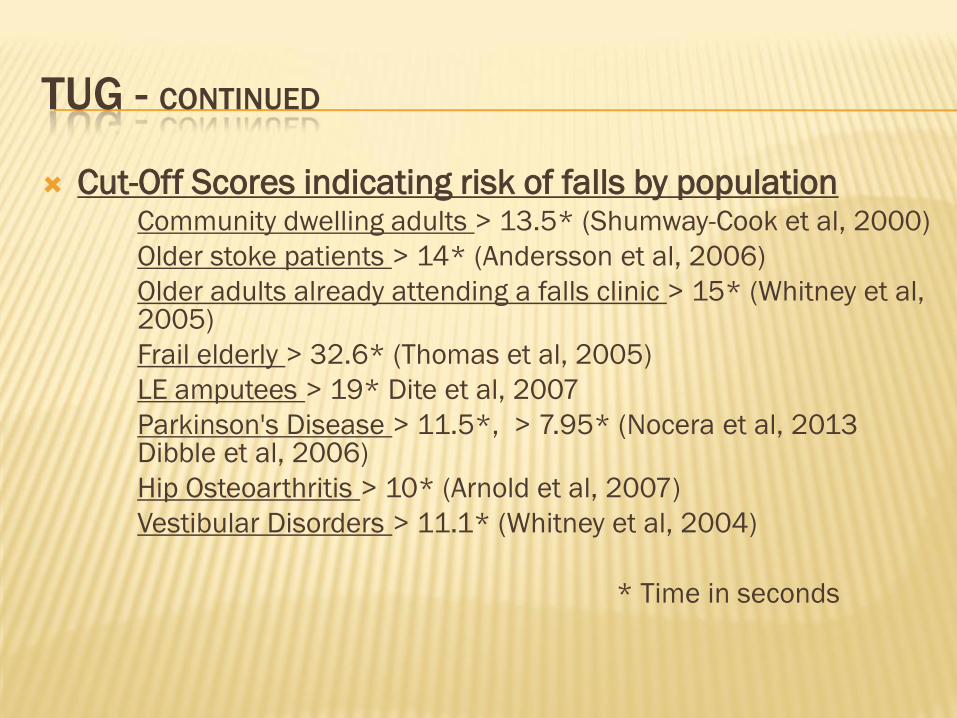
TUG - CONTINUED
Cut-Off Scores indicating risk of falls by population Community dwelling adults > 13.5* (Shumway-Cook et al, 2000)
Older stoke patients > 14* (Andersson et al, 2006)
Older adults already attending a falls clinic > 15* (Whitney et al, 2005)
Frail elderly > 32.6* (Thomas et al, 2005)
LE amputees > 19* Dite et al, 2007
Parkinson's Disease > 11.5*, > 7.95* (Nocera et al, 2013 Dibble et al, 2006)
Hip Osteoarthritis > 10* (Arnold et al, 2007)
Vestibular Disorders > 11.1* (Whitney et al, 2004)
* Time in seconds

PELVIC FLOOR INDEX
20-item questionnaire that is the short form of the 46 question PFDI
Reflects symptoms experienced over the last 3 months
Separated into three subscales:
Urinary Distress Inventory 6 (UDI-6)
Colorectal-Anal Distress Inventory 8 (CRADI-8)
Pelvic Organ Prolapse Distress Inventory 6 (POPDI-6)
Can be given in its entirety or as individual scales ·
Patient/client answers yes or no to questionnaire items and then ranks the l evel of bother of each “yes” item on a Likert-scale with 1 = “not at all,” 2 = “somewhat,” 3 = “moderately,” and 4 = “quite a bit”
No answers receive a 0
Scoring:
Scale scores- The mean value of all questions answered is then multiplied by 25 for the actual score (range 0 to 100)
Summary score- Add the scores from the 3 scales together to obtain the summary score (range 0 to 300). The higher the score the greater the perceived impact that pelvic floor dysfunction has on a patient’s life
Administrative burden: 5 minutes
Minimal Detectable Change: Not established

‘PARDON ME…I SPEAK JIVE’
Cut me some slack-jack!
Physician engagement
‘Your patient has improved to a score of 4 from and initial 17
on the NDI. This indicates Mrs. Jones now has no disability as
stated by Sterling – 2004’
‘Out of the last 15 conservative shoulder patients you’ve sent to
our clinic, they are averaging a 27% improvement on their DASH
score!’
THE FUTURE-------------
Once we have established a current ‘average’
score per diagnosis we can then:
Compare protocols
Examine impact of time until therapy intervention
Promote our benchmarks to referral sources
Use data sets for future research ideas
Utilize our data to impact prescriber tendencies (pucker-up
and kiss)
Link hospital + rehab + outpatient care services (current
LEFS research)
Ummm….now what
• What to do with all this data!!!!!
• Roeder Tool (Via Christi’s electronic database)
TKA pathway
• Via Christi completed revised TKA pathway in 2015
• Consisting of:
• Creating team of ‘Top Performers’, by using data from Roeder tool • Identified top PT’s that had least visits/pt, greatest KOS change
• Comprehensive literature review of recent publications (within past 5 years)
• Resulted in revised outpt TKA algorithm
• Rolled out education to all outpt PT’s, including accepted research findings and new scripting.
• Example: Outcome Performers- TKA powerpoint

Jive scripting- for pt.s
• “Our clinic is currently averaging 9 visits with your diagnosis, provided we see you 2x/week. Let’s set our sights at 9, but see if we can do better. “
• “So far, the pt’s I’ve seen with lateral epicondylits are needing 7 visits on average to return to their prior level of activity (provided they comply with all our recommendations).”
• Well, we’ve already used 12 visits, and have been seeing you for 6 weeks. That’s over our average. Judging on your DASH score you just completed, you are scoring below (better) than those we feel are ready to be discharged. Let’s talk more about transitioning you to a home program.”
• “Because it took you over 6 months to present to our office with your shoulder pain, I’d expect your therapy sessions to extend to 6-8 weeks.”
• “We track all our data to make sure we are providing the best care possible.”
Jive scripting- for physicians
• “Our data indicates that your referrals with shoulder pain are averaging 10 outpt visits. And that’s with an average onset to therapy evaluation of 120 days. If we can get our hands on these pt’s when they present with pain at 60 days or less, we average 6 visits. What do you think about sending them sooner.”
• “Your pt.’s are averaging 3.5 weeks in therapy for their post-op wrist fractures. That’s the shortest time compared to all our referring physicians, way to go!”
• “There is a new protocol for conservative carpal tunnel. So far, your pt.’s average 5.6 visits to improve their DASH score to below 20 points. Could we try this new technique and see if we can improve our pt outcome?”

Bibiography
1. Sackett DL, Rosenburg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312:71-72.
2. Evans TA, Lam KC. Clinical outcomes assessment in sports rehabilitation. J Sport Rehab. 2001;20:8-16.
3. Jette DU, Halbert J, Iverson C, Miceli E, Shah P. Use of standardized outcome measures in physical therapist practice: Perceptions and applications. Phys Ther .2009;89(2):125-135.
4. DeLise DC, Leasure AR. Benchmarking: measuring the outcomes of evidence-based practice. Outcomes Manag Nurs Pract. 2001;5:70-74
5. Leufer T, Cleary-Holdforth J. Evidence-based practice: Improving patient outcomes. Nurs Stand. 2009;23:35-39
6. Kraus DR, Horan FP. Outcomes roadblocks: Problems and solutions (cover story). Behav Health Mana.ge. 1997;17:22.
7. Watts JH, Clement DG, Casanova JS. Perspectives on outcomes research and practice collaboration. J Rehabil Outcome Meas. 1999;3:22-32
8. Russek L, Wooden M, Ededahl S, Bush A. attitudes towards standardized data collection.Phys Ther. 1997;7(7):714-729.3. World Health Organization. Towards a Common Language for Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization; 2002.
9. Michener LA. Patient and clinician related outcome measures for clinical decision making in rehabilitation. J Sport Rehab. 2011;20:37-45