parkinsonismi (atipici ?): inquadramento clinico · parkinsonismi (atipici ?): inquadramento...
TRANSCRIPT
Parkinsonismi (Atipici ?):inquadramento clinico
Seminario UNIVA, 3 Luglio 2013, Lamezia Terme
Paolo BaroneCenter for Neurodegenerative Diseases
University of Salerno, Italy

Le sindromi parkinsoniane

Segni che suggeriscono un parkinsonismo atipico
Motori• instabilità precoce con cadute• rapida progressione• risposta alla levo-dopa assente,
povera, non mantenuta• segni piramidali• segni cerebellari• disartria e disfagia precoci
Oculomotori• paralisi sopranucleare• rallentamento dei saccadici• difficoltà ad iniziare i saccadici
Cognitivo-comportamentali• demenza precoce• allucinazioni visive non indotte da
trattamento• aprassia• disturbi corticali sensitivi
Vegetativi• disturbi vegetativi precoci non
imputabili al trattamento (ipotensione ortostatica, impotenza, disturbi urinari)

Parkinsonismi Atipici: criteri diagnostici
• MSA: Gilman et al. - J. Neurol. Sci. 1999-
Gilman et al- Neurology 2008
• PSP: Litvan et al. - Neurology 1996
• CBD: Litvan et al. - Neurology 1997
• DLBD: McKeith et al. - Neurology 2005
Classification of parkinsonian syndromes in a community
• Idiopathic PD ~ 85% of all PS cases
• Drug-induced parkinsonism (DIP) 7% - 9%
• MSA-P ~ 2.5%
• PSP ~ 2.0%
• Vascular parkinsonism ~ 3%
• PS due to MPTP, CO, Mn, recurrent head trauma is extremely rare
• No new cases of postencephalitic parkinsonism since l960s
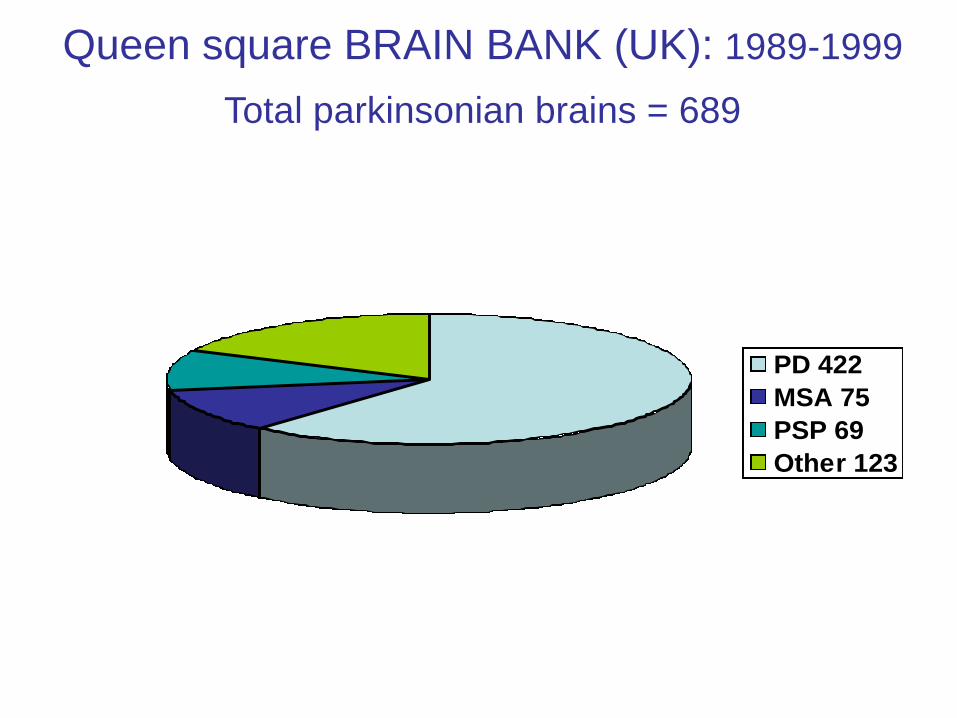
PD 422
MSA 75
PSP 69
Other 123
Queen square BRAIN BANK (UK): 1989-1999
Total parkinsonian brains = 689

Patologie Rare: problema di denominazione
MSA Schrag et al 1999
• Prevalenza 4.4 10-5
• Incidenza 0.5 10-5/yr
PSP Schrag et al 1999
• Prevalenza 6.4 10-5
• Incidenza 1.14 10-5/yr
Quadro anatomo-patologico
che dovrebbe definire
un gruppo di malattie (ed in vivo ?)
Un segno/sintomo che definisce
una malattia (patognomonico ?)
DCB

Adams et al 1961
SND
Dejerine & Thomas 1900
OPCA
Graham & Oppenheimer 1969
MSA = OPCA = SDS = SND
Spillantini et al 1998
MSA =
α-Synucleino-
pathie
Papp, Kahn,
Lantos 1989
GCI
Shy & Drager 1960
SDS

Fattori di rischio per MSA
• Maggior rischio di MSA per esposizione occupazionale a:– Solventi organici
– Monomeri plastici
– Pesticidi
– Metalli (Nee et al, 1991)
• Abitudine al fumo meno comune negli MSA rispetto ai controlli (Vanacore et al, 2000)
• Genetica– Limitata al Giappone (?)

parahydroxybenzoate-polyprenyl transferase
CoQ10
2013

Homozygous mutation (M78V-V343A/M78V-V343A) and
compound heterozygous mutations (R337X/V343A) in COQ2
in multiplex families
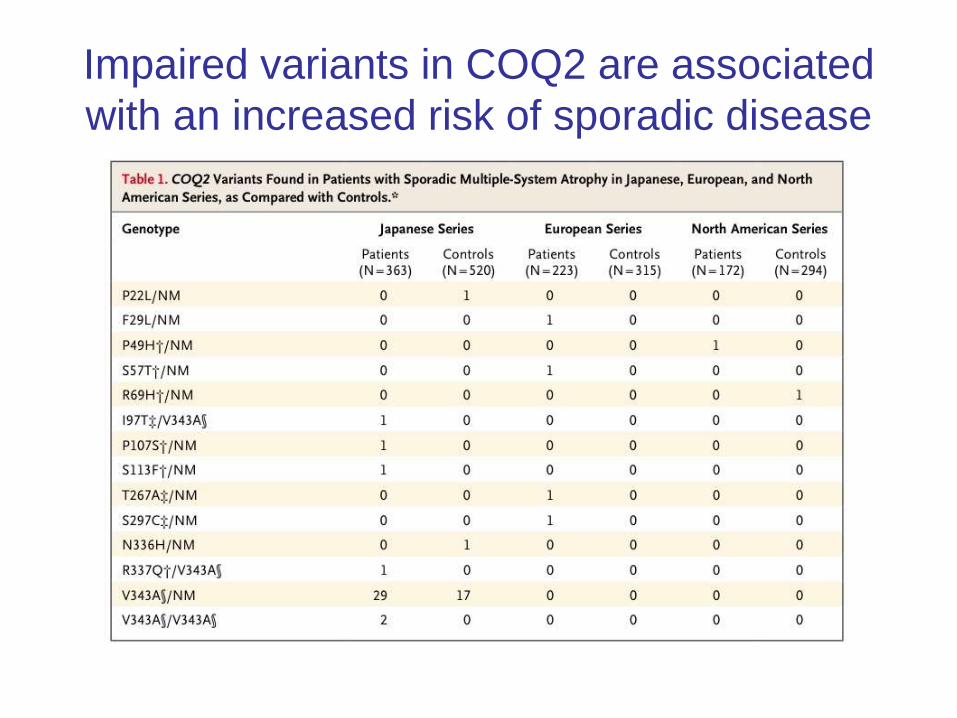
Impaired variants in COQ2 are associated
with an increased risk of sporadic disease

Caratteristiche cliniche della MSA
Parkinsonismo 80% Rigidità Acinesia asimmetrica Tremore a riposo Distonie
Segni cerebellari 40% Coordinazione Atassia marcia Tremore intenzionale Nistagmo
Disturbi vegetativi 96% Impotenza Incontinenza urinaria Ritenzione urinaria Ipotensione posturale Sincopi ricorrenti
Segni piramidali 54% Iperreflessia
Babinski

European MSA-SG Registry

Clinical presentation
Age at disease onsetWenning et al, Brain 1994
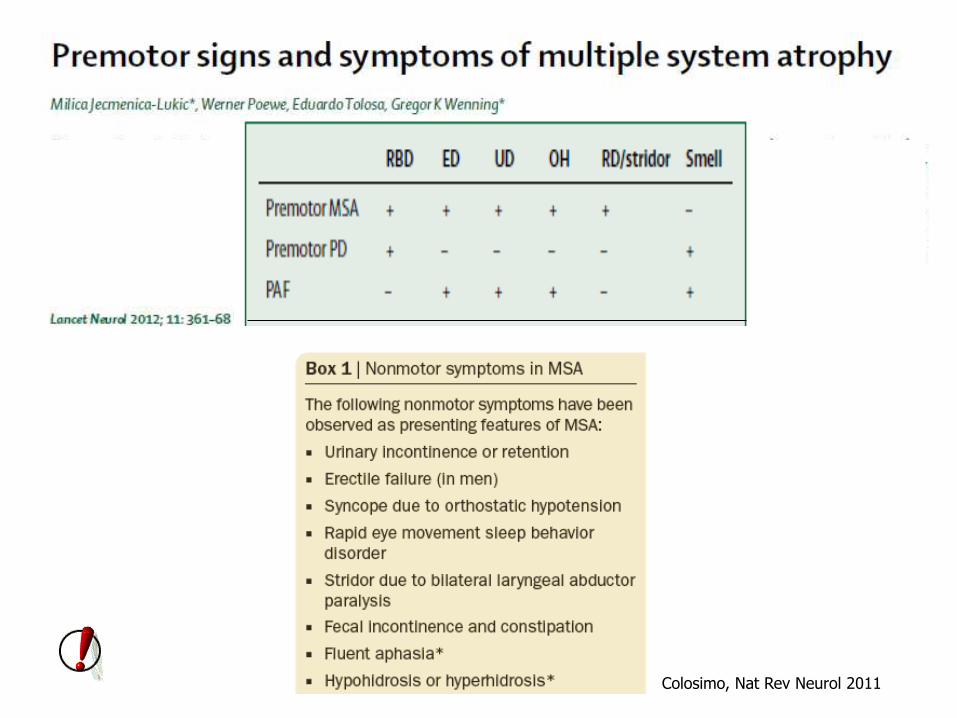
Colosimo, Nat Rev Neurol 2011
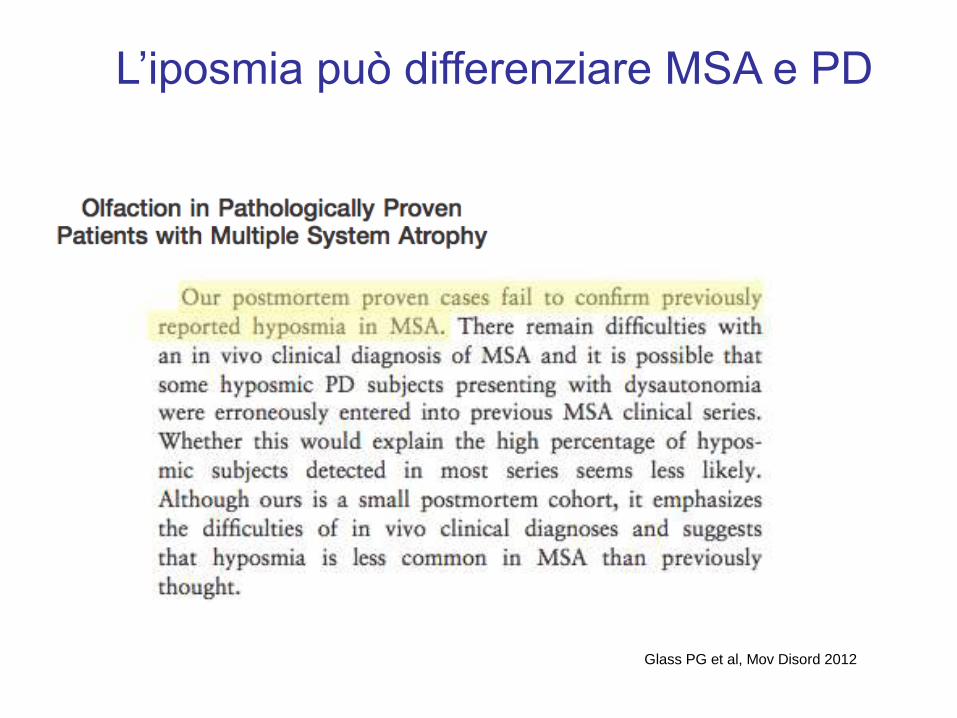
Glass PG et al, Mov Disord 2012
L’iposmia può differenziare MSA e PD

Dysautonomia Parkinsonism L-Doparesponse(duration)
Ataxia Babinski Hyper-reflexia
Europe 78% 87% 38% (3) 63% 28% 43%
Austria 67% 95% 32% (3) 92% 38% 38%
Denmark 87% 100% 40% (3.5) 53% 27% 33%
England 87% 85% 27% (3) 84% 48% 56%
France 86% 90% 18% (3) 71% 30% 59%
Germany 80% 86% 26% (4) 71% 14% 25%
Israel 78% 86% 55% (3) 56% 59% 37%
Italy 88% 100% 45% (2) 58% 33% 73%
Portugal 46%* 100% 45% (2) 39% 15% 62%
Spain 74% 49%* - 71% 14% 34%
Sweden 87% 80% 67% (5.5) 40% 7% 13%
Clinical presentation in Europe

Gilman et al, J Neural Transm 2005
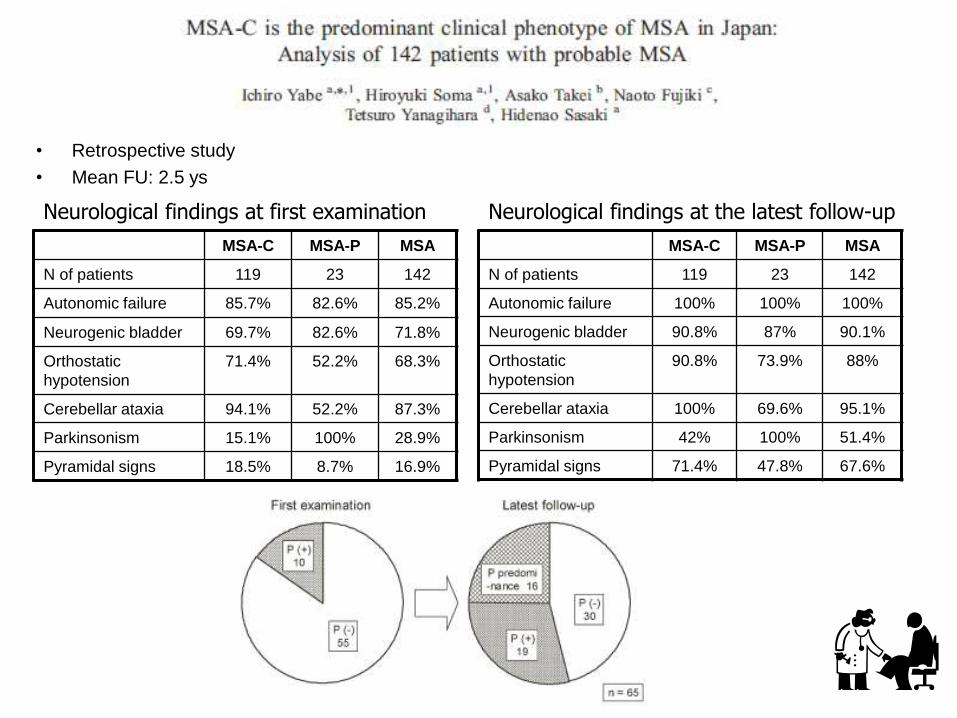
• Retrospective study
• Mean FU: 2.5 ys
MSA-C MSA-P MSA
N of patients 119 23 142
Autonomic failure 85.7% 82.6% 85.2%
Neurogenic bladder 69.7% 82.6% 71.8%
Orthostatic
hypotension
71.4% 52.2% 68.3%
Cerebellar ataxia 94.1% 52.2% 87.3%
Parkinsonism 15.1% 100% 28.9%
Pyramidal signs 18.5% 8.7% 16.9%
MSA-C MSA-P MSA
N of patients 119 23 142
Autonomic failure 100% 100% 100%
Neurogenic bladder 90.8% 87% 90.1%
Orthostatic
hypotension
90.8% 73.9% 88%
Cerebellar ataxia 100% 69.6% 95.1%
Parkinsonism 42% 100% 51.4%
Pyramidal signs 71.4% 47.8% 67.6%
Neurological findings at first examination Neurological findings at the latest follow-up
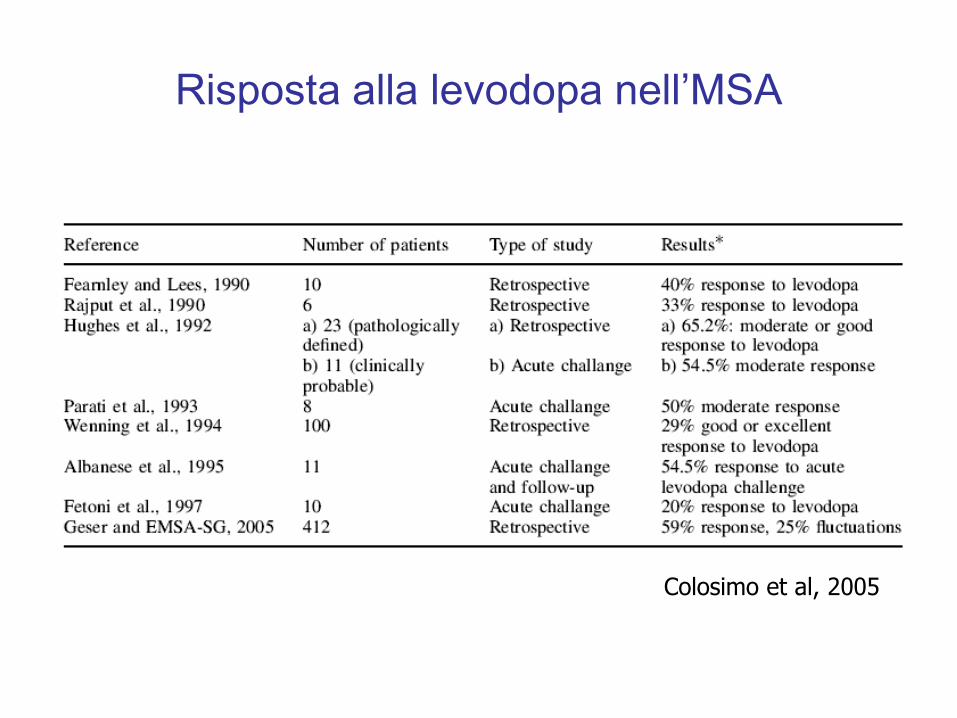
Risposta alla levodopa nell’MSA
Colosimo et al, 2005
Wenning et al, submitted
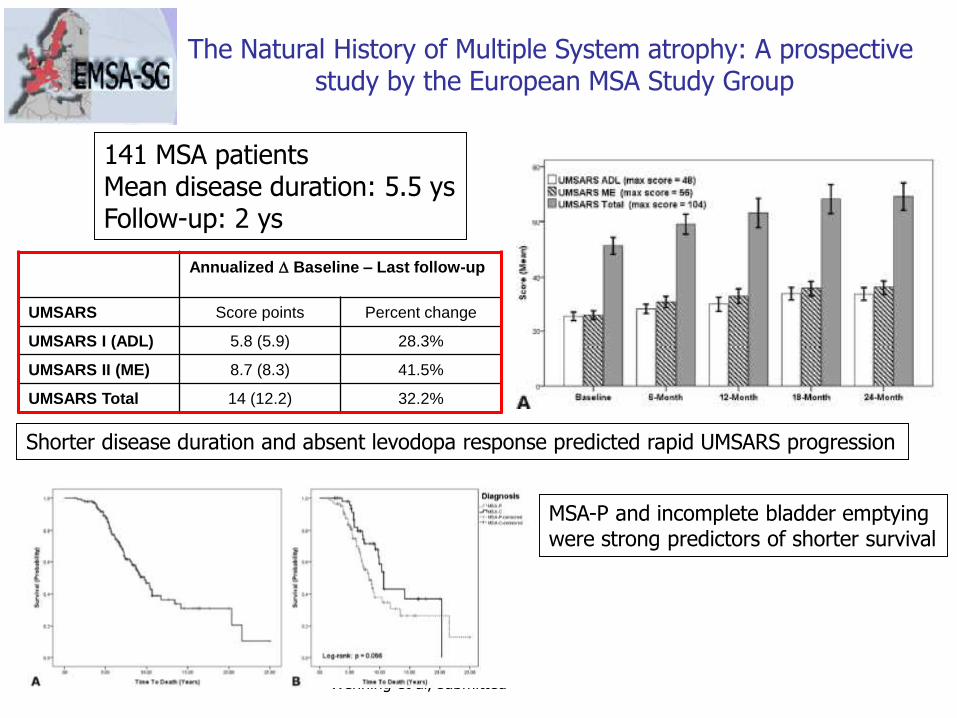
The Natural History of Multiple System atrophy: A prospective study by the European MSA Study Group
141 MSA patientsMean disease duration: 5.5 ysFollow-up: 2 ys
Annualized D Baseline – Last follow-up
UMSARS Score points Percent change
UMSARS I (ADL) 5.8 (5.9) 28.3%
UMSARS II (ME) 8.7 (8.3) 41.5%
UMSARS Total 14 (12.2) 32.2%
Shorter disease duration and absent levodopa response predicted rapid UMSARS progression
MSA-P and incomplete bladder emptying were strong predictors of shorter survival

Wenning et al, submitted

Caveat: La disautonomia nell’ MSA può comparire
molto tardivamente
Petrovic et al, Mov Disord 2012
(4 casi di MSA confermati antomo-patologicamente)

Petrovic et al, Mov Disord 2012
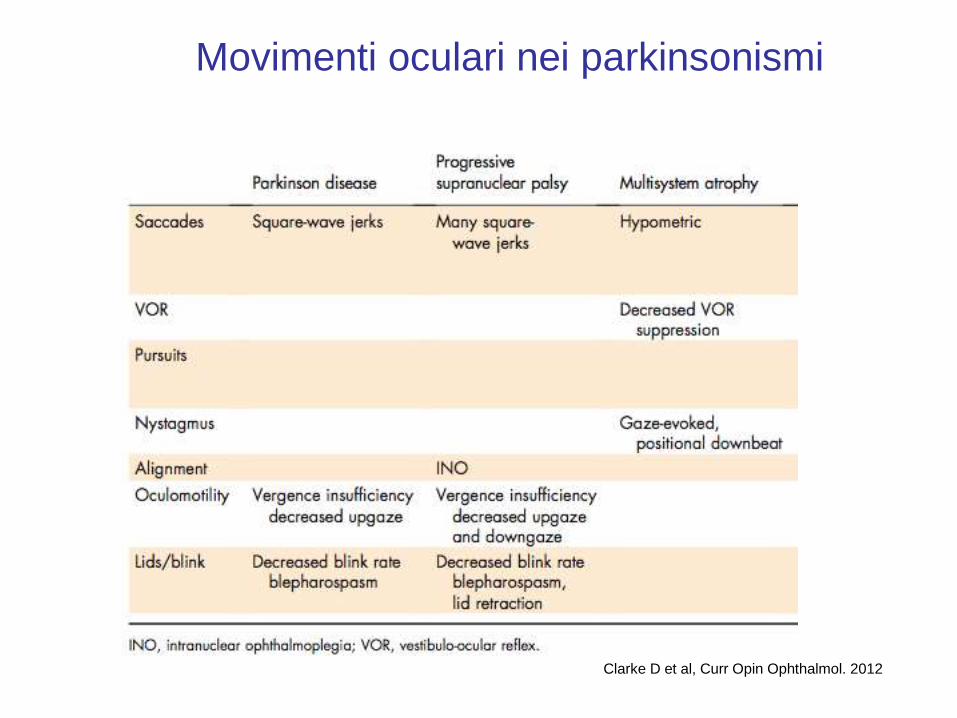
Clarke D et al, Curr Opin Ophthalmol. 2012
Movimenti oculari nei parkinsonismi


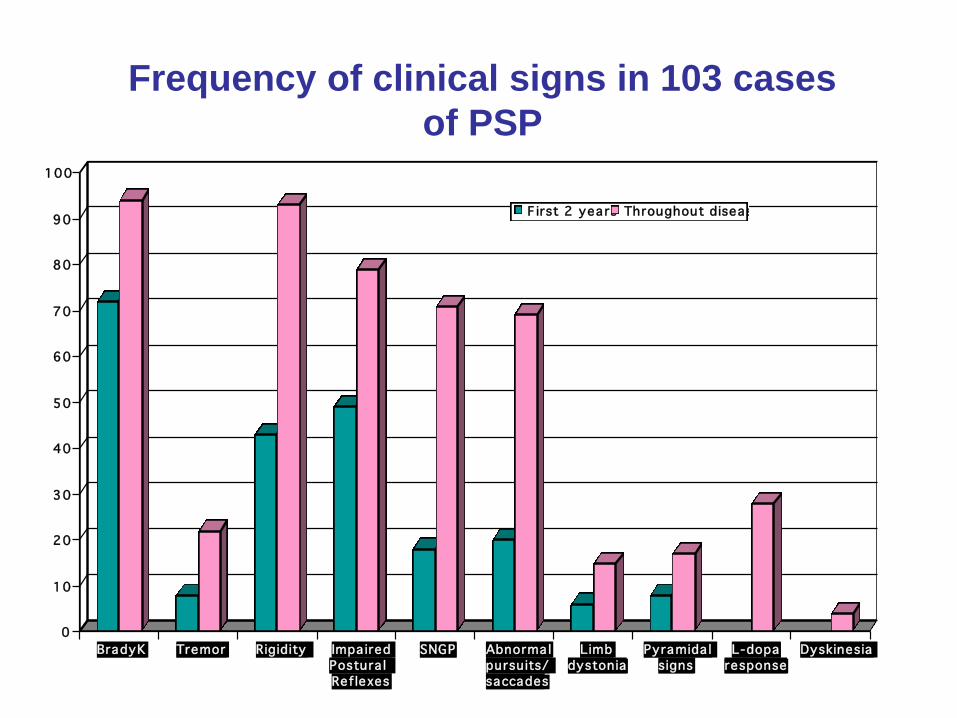
0
10
20
30
40
50
60
70
80
90
100
Falls Cognitive
dysfunction
Visual
Sypmtoms
Dysphagia Speech
disturbance
Asymmetric
onset
First 2 years Throughout disease
Frequency of symptoms reported in 103
cases of PSP
0
10
20
30
40
50
60
70
80
90
100
BradyK Tremor Rigidity Impa ired
Postura l
Ref lexes
SNGP Abnorma l
pursuits/
saccades
Limb
dystonia
Pyramida l
signs
L-dopa
response
Dyskinesia
F irst 2 yea rs Throughout disease
Frequency of clinical signs in 103 cases
of PSP
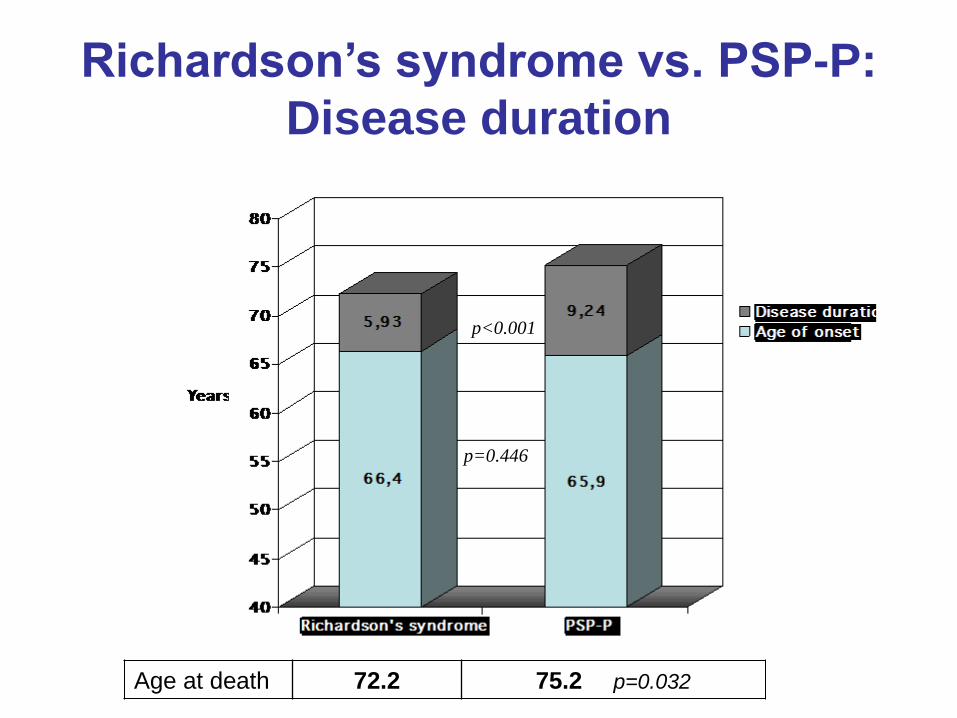
Richardson’s syndrome vs. PSP-P:
Disease duration
p=0.446
p<0.001
Age at death 72.2 75.2 p=0.032

n=25 n=18
0.0
0.2
0.4
0.6
0.8
1.0
2N4R 2N3R 1N4R 1N3R 0N4R 0N3R
Series1 Series2
Richardson’s syndrome vs. PSP-P:
Tau isoforms
R-τ RS PSP-P
2N 4R
2N 3R
1N 4R
1N 3R
0N 4R
0N 3R *
*
*
* p<0.05 RS PSP-P

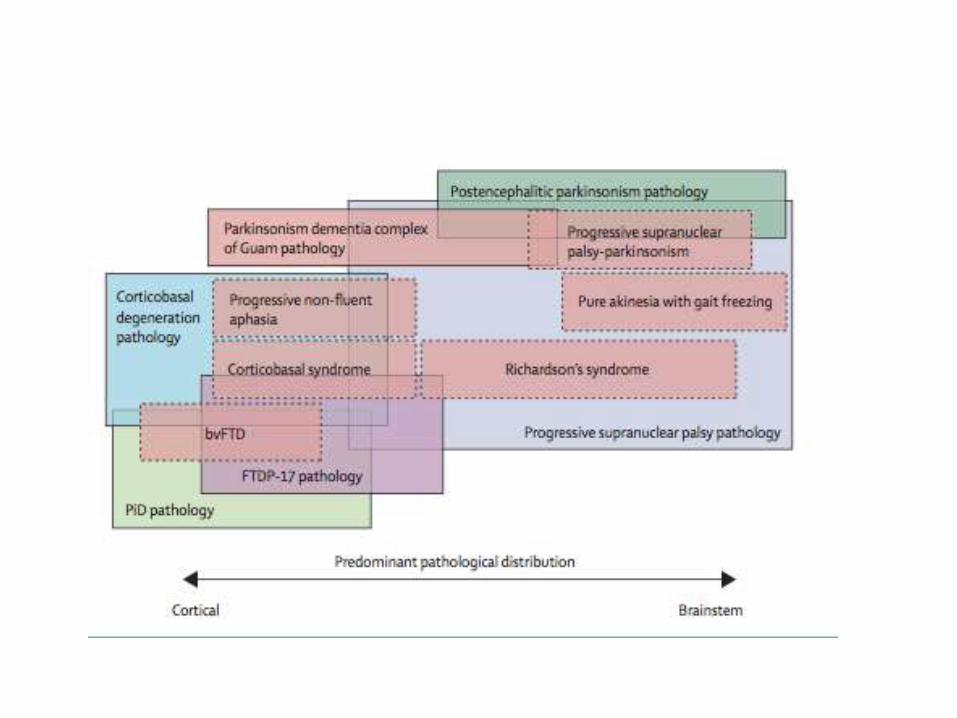
Typical and “atypical” PSP
Four clinical phenotypes were identified
• Richardson’s syndrome PSP-RS
• Parkinsonism PSP-P
• Pure akenesia with gait freezing PSP-PAGF
• Progressive non-fluent aphasia PSP-PNFA

SPM clearly demonstrated a bilateral frontotemporal hypoperfusion
involving the IFG and the STG. In this patient, a significant
hypoperfusion was also detected in the rectal gyrus of both
cerebral hemispheres.

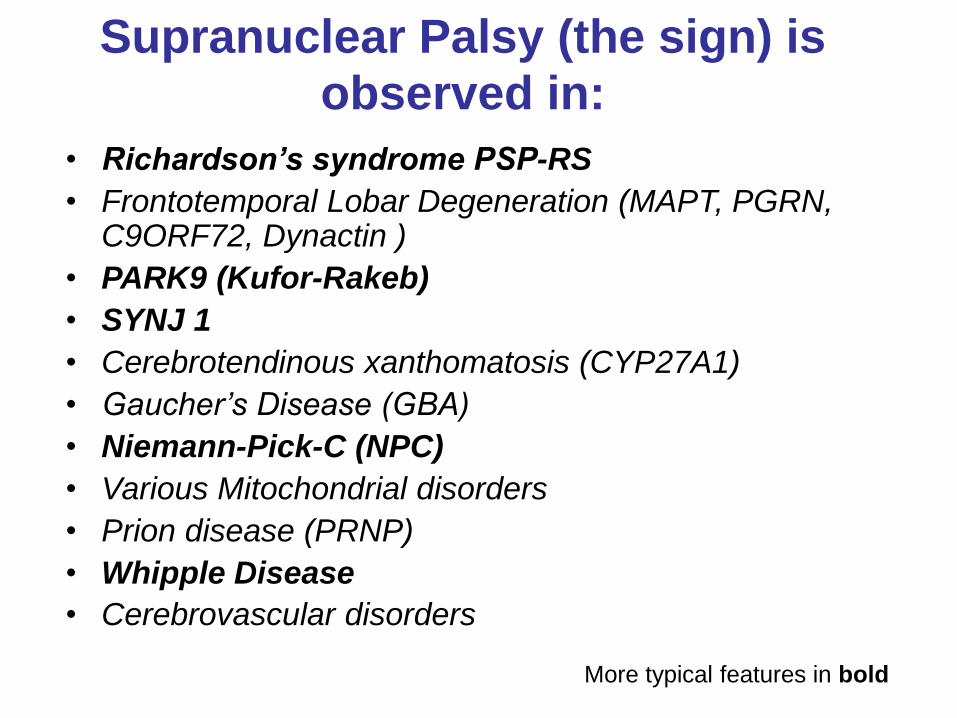
Supranuclear Palsy (the sign) is
observed in:
• Richardson’s syndrome PSP-RS
• Frontotemporal Lobar Degeneration (MAPT, PGRN, C9ORF72, Dynactin )
• PARK9 (Kufor-Rakeb)
• SYNJ 1
• Cerebrotendinous xanthomatosis (CYP27A1)
• Gaucher’s Disease (GBA)
• Niemann-Pick-C (NPC)
• Various Mitochondrial disorders
• Prion disease (PRNP)
• Whipple Disease
• Cerebrovascular disorders
More typical features in bold


CONTROL
CONTROLCONTROL
Quadri et al, 2013


CASO 1, donna di 77 anni
-Esordio a 72 anni con rigidità e dolenzia al braccio dx; A 74 anni cadute
CASO 2, donna di 68 anni
- Esordio a 65 anni con disturbo del linguaggio. Progressione negli anni e comparsa di
sindrome parkinsoniana bradicinetico-rigida.
CASO 3, Donna, 63 anni
- Esordio a 59 anni con rallentamento motorio generalizzato e “limitazione funzionale” del
braccio dx
CASO 4, Donna, 59 anni
- Esordio 9 mesi prima con distonia, movimenti involontari e alterato controllo del braccio sin.
CASO 5, Donna, 74 anni
- Esordio 1 mese prima con alterazione del linguaggio, delle funzioni cognitive e della marcia

Case #1: diagnosis

Case #2: diagnosis
“My left hand goes first...”

“Is your hand moving?”
“No...”
Case #3: diagnosis

Case #4: diagnosis

Case #5: diagnosis

Case #5: diagnosis
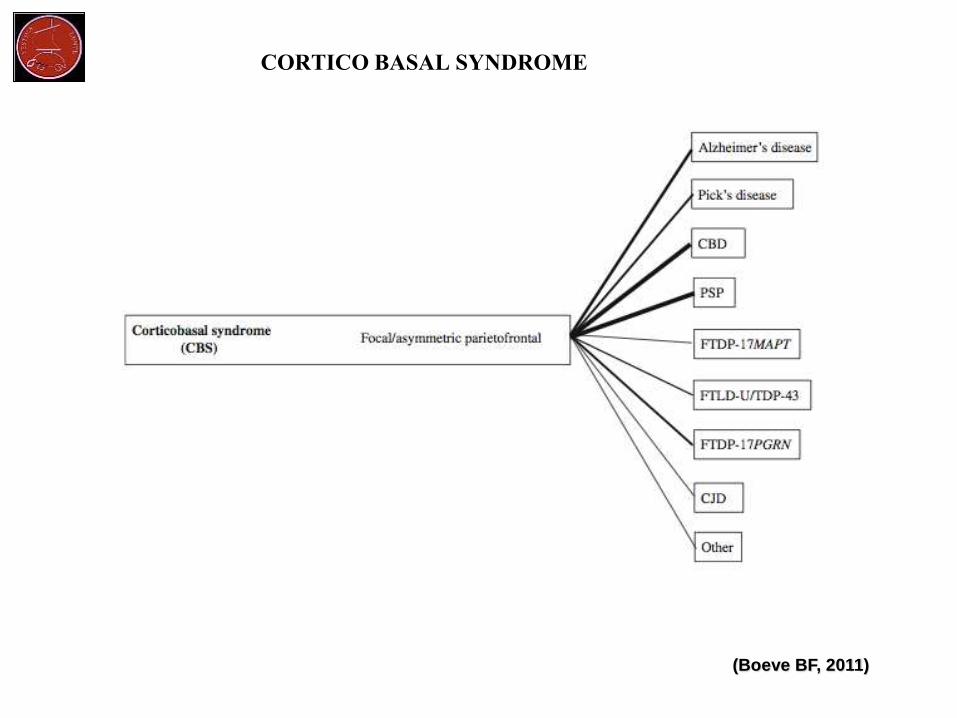
CORTICO BASAL SYNDROME
(Boeve BF, 2011)
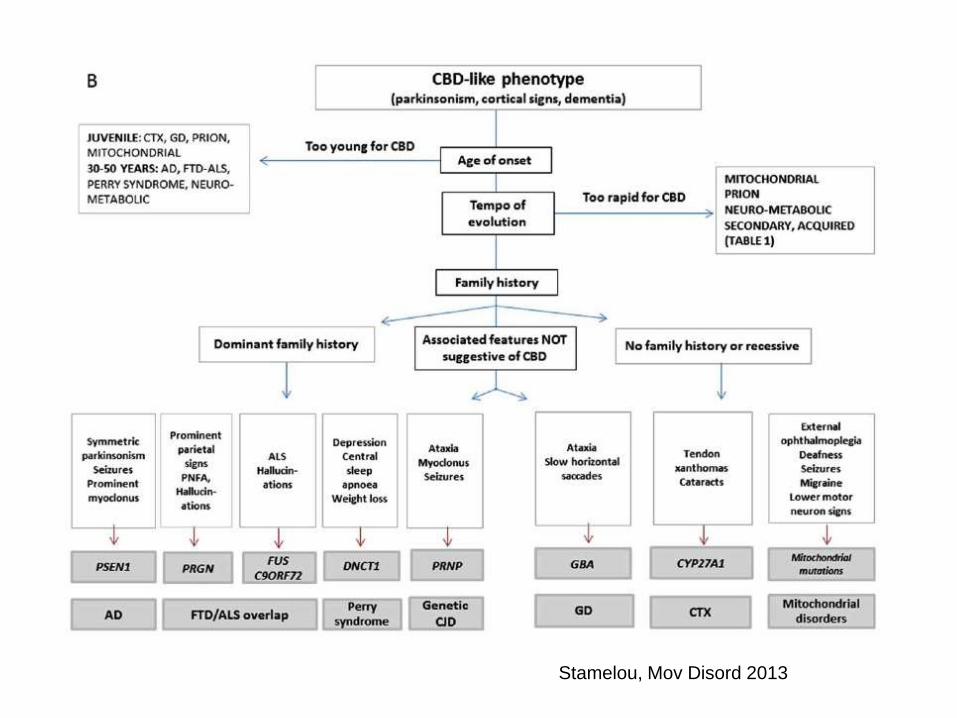
Stamelou, Mov Disord 2013

Aerts MB et al, Practical Neurology 2012

Stamelou, Mov Disord 2013

Stamelou, Mov Disord 2013

Lee W et al, Mov Disord 2012

Lipp et al, Arch Neurol 2009
Lipp et al, Arch Neurol 2009

68 MSA patientsFollow-up: 10 months
Damon-Perriere et al, 2012

Pinkhardt EH et al, J Neurol 2009
Target
Saccadi anticipatorie
Rappresenta il rapporto tra il
movimento reale e quello aspettato
(quanto è più vicino al volare unitario,
tanto più il movimento è continuo)