part 1 - framing the discussion on sterile...
TRANSCRIPT
Page
Part 1 - Framing the Discussion on Sterile Surfaces
The Importance of Antimicrobial Incise Drapes and Sterile Surface in
Managing the Risk of Surgical Wound Infections
Patrick J. Parks M.D. Ph.D.
3M Health Care
St.Paul, Minnesota
Commercial Identification
“Povacrylex”– 3M™DuraPrep™ Surgical Solution (Iodine Povacrylex [0.7% available iodine] and Isopropyl
Alcohol, 74% w/w) Patient Preoperative Skin Preparation “Antimicrobial Impregnated Incise Drape”
– 3M™ Ioban™2 Antimicrobial Incise Drape “Ethanol/Chlorhexidine”
– ChloraPrep® (Chlorhexidine Gluconate 2% w/v and Isopropyl Alcohol 70% v/v) Antiseptic Skin Prep. ChloraPrep is a registered trademark of Allegiance Corporation [Enturia product, now part of Cardinal Health]
“Cyanoacrylate”– InteguSeal Microbial Sealant is a registered trademark of Kimberly-Clark Worldwide, Inc.
Betadine® Solution– Betadine® Solution is a registered trademark of The Purdue Frederick Company.
IF commercial labels appear, they appear as they are given in the cited literature. All data presented have appeared or are scheduled to appear in peer-reviewed
publications.
3M, DuraPrep, Ioban, and Steri-Drape are trademarks of 3M.

Page
Outline
Framing the discussion
– The relationship of contamination to infection
• Sources of infection
• Local factors
• Implants as a special case
• Biofilm formation
Reducing contamination and infection
• Antisepsis
• Sterile surface formation
Future
Wound Contamination and Wound Infection
“It ought to be axiomatic by now that reducing bacterial contamination reduces infection.”*
* Raahave,D., Wound contamination and postoperative infection. A review. Dan. Med. Bulletin (1991) 38:481-485.
Defining the Risk of Surgical Site Infection
==
Dose of Bacterial Contamination
Virulence
Resistance of the host (patient)
XRisk of Surgical Site Infections
Resistance of the host (patient)+ Antibiotics+ Local factors
SSI improved from 14.3% to 8.7%
Forbes et al.,J Am Coll Surg (2008) 207:336-341.

Page
Host Defenses
“Adequacy of host immune defenses is the primary factor determining whether wound contamination progresses into a clinical infection.”*
* Sessler, D.I., “Nonpharmacologic prevention of surgical wound infection.” Anesthesiol.Clin.(2006) 24:279-297.
Resistance of the Host
“Local” factors– Under control of SURGEON
Avoid seroma
Avoid tissue necrosis
Minimal trauma to tissue
– Inherent PATIENT risk factors Neumayer,L. et al. J.Am.Coll.Surg.(2007) 204:1178-
1187
Genetic factors (vit D receptor, MMP1 in THR failure) Malik, MHA et al. Ann.Rheum.Dis.(2007) 66:116-1120.
Defining the Risk of Surgical Site Infection:All surgeries

Page
Sources of Wound Contamination and Routes of Transmission
Patient’s skin
Theatre personnel
Instruments
Adjacent area Floor
Ventilation
Wound
Theatre air
Body, incisionand wound drapes
Watertightclothing
Gloves
Clothing
Masks
Mouthhands
Body
Source of Bacteria
Where do bacteria come from?Air Whyte et al., J. Hosp. Infect. (1991) 18:93-107.
Brown,A.R., et al., J.Hosp.Infect.(2001) 48:117-131.Edminston, CE et al., Surgery (2005) 138:573-582.
Staff skin Huebner,J. Annu.Rev.Med. (1999) 50:223-236.
Patient skin vonEiff, et al., Eur.J.Clin.Microbiol.Infect.Dis. (1999) 18:843-846.
Brown,A.R., et al., J.Hosp.Infect.(2001) 48:117-131. (ultraclean air systems present)
Garvin,K.L. and Urban,J.A., Total hip infectionsin Musculoskeletal Infections (2003) pp. 241-293.
Defining the Risk of Surgical Site Infection:Source of Organisms
Clean and Clean Contaminated surgery:Skin organisms are a major source of infecting organisms.*
*Taylor,G.J. et al., Perioperative wound infection in elective orthopaedic surgery. J.Hosp.Infec.(1990) 16:241-247.
Contaminated surgery“There was no significant correlation between intraoperative
tissue bacterial density and subsequent wound infection, or contaminating and infecting bacteria.*”
*Becker,G.D., Welch, W.D. Quantitative bacteriology of intraoperative wound tissue in contaminated surgery. Head Neck. (1990) 12:293-297.
Page
Skin Microbiology
Humans carry between 100 (“2 logs”) and100 000 (“5 logs”) organisms per sq cm on their skin
Number depends on site on body and individual Most common organisms include
– Staph. Epidermidis (coagulase neg staph)– Staph. Aureus– Propionibacterium species (anaerobe)
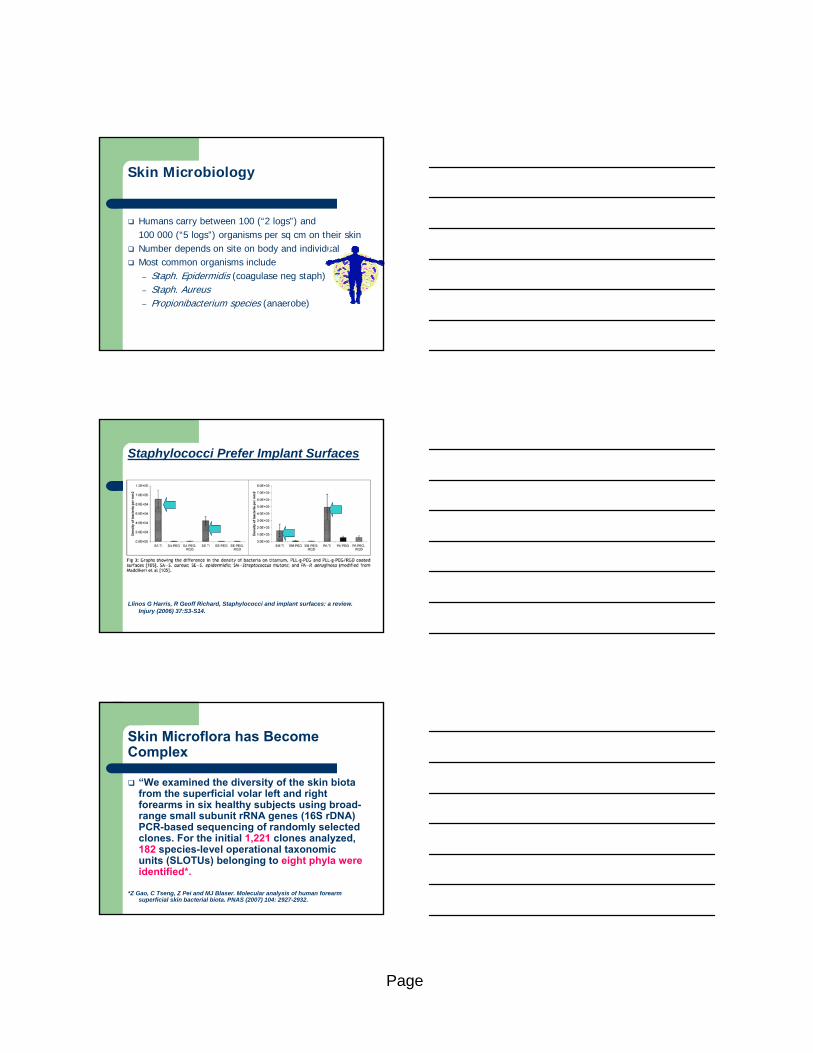
Staphylococci Prefer Implant Surfaces
Llinos G Harris, R Geoff Richard, Staphylococci and implant surfaces: a review. Injury (2006) 37:S3-S14.
Skin Microflora has Become Complex
“We examined the diversity of the skin biota from the superficial volar left and right forearms in six healthy subjects using broad-range small subunit rRNA genes (16S rDNA) PCR-based sequencing of randomly selected clones. For the initial 1,221 clones analyzed, 182 species-level operational taxonomic units (SLOTUs) belonging to eight phyla were identified*.
*Z Gao, C Tseng, Z Pei and MJ Blaser. Molecular analysis of human forearm superficial skin bacterial biota. PNAS (2007) 104: 2927-2932.

Page
Skin Biofilm Forming Bacteria are Common
Multiple biofilm forming bacteria, some previously unknown!– Lysobacter species
KE Dempsye, MP Riggion, A Lennon, VE Hannah, G Ramage, D Allan and J Bagg. Identification of bacteria on the surface of clinically infected and non-infected prosthetic hip joints removed during revision arthroplasties by 16S rRNA gene sequencing and by microbiological culture Arthritis Research & Therapy (2007) 9: 1-11.
Biofilms
All bacteria make biofilm
Foreign & devitalized tissue can succumb to biofilm formation if exposed to bacteria
Slide courtesy of Dr. Ed McPherson, USC Orthopaedics
Costergan, W. MSIS 2000
Characteristics
Biofilms
Biofilms– Sugars (Extracellular polysaccharides)
– Proteins (Bacterial and Host)Planktonic bacteria Planktonic bacteria

Page
Infection in Implant SurgeryMolecular measurement methods are critical!
“Our results indicate that the incidence of prosthetic jointinfection is grossly underestimated by current culture detection methods*.”
*Tunney,M.M., et al., Detection of prosthetic hip infection at revision arthroplasty by immunofluorescence microscopy and PCR amplification of the bacterial
16S rRNA gene. J.Clin.Microbiol. (1999) 37:3281-3290.
Where incidence is correct (Norway, Sweden, Denmark), impact may be underestimated.
– Infection during first implantation increases risk of failure ofrevision*.
*Anguita-Alosno,P. et al., Prosthetic joint infection. Expert Rev.AntiInfect.Ther. (2005) 3: 797-804.
Implant Infection Summary:
There is NO minimum critical density for infection since:– Each patient has a unique immune system
– Each patient has different risk factors
– Surgery is different for each patient
– Bacteria have different levels of virulence
– Bacteria may form biofilms
– Common pathogens (staph) preferentially attach to common implant materials
Outline
Framing the discussion
The relationship of contamination to infection
Sources of infection-patient skin
Local factors-host response
Implants as a special case-high morbidity
Biofilm formation-common critical factor
Reducing contamination and infection
Antisepsis
Sterile surface formation
Future
Page
Part 2 - Antisepsis and the Reduction of Wound Bacterial Count
Skin Microbiology:Risk of Surgical Site Infections
==
Dose of Bacterial Contamination
Virulence
Resistance of the host (patient)
X
Reducing Contamination:
There are two ways to reduce local contamination– Antibiotics
– Antiseptics
Page
25
SG
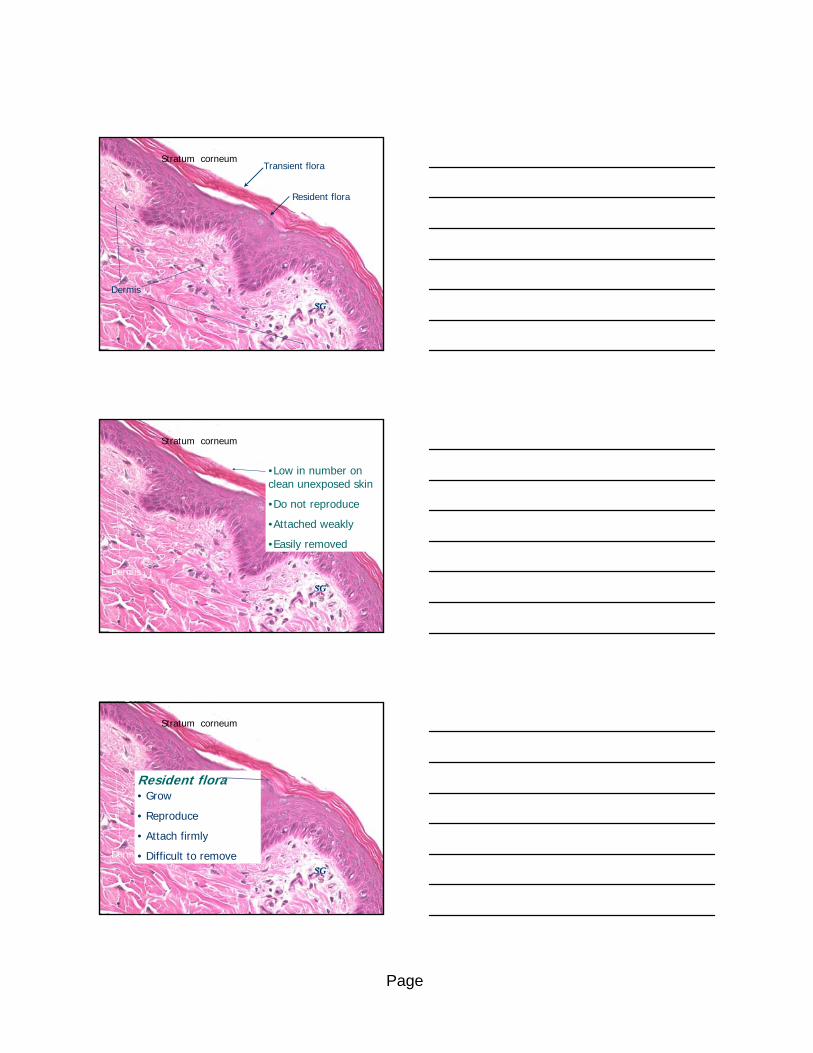
Stratum corneum
Dermis
Transient flora
Resident flora
26
SG
Stratum corneum
Dermis
Transient flora•Low in number on clean unexposed skin
•Do not reproduce
•Attached weakly
•Easily removed
27
SG
Stratum corneum
Dermis
Resident flora• Grow
• Reproduce
• Attach firmly
• Difficult to remove
Page
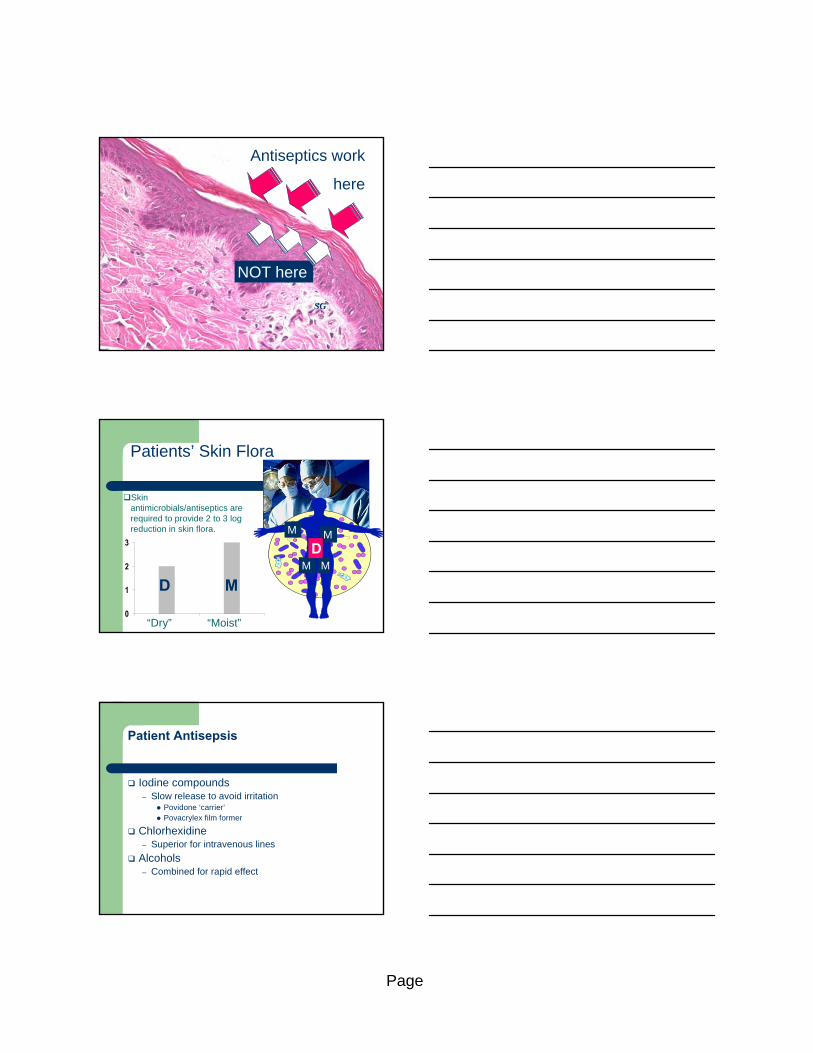
28
SG
Dermis
Antiseptics work
here
NOT here
Patients’ Skin Flora
Skin antimicrobials/antiseptics are required to provide 2 to 3 log reduction in skin flora.
0
1
2
3
“Dry” “Moist”
M
MM
M
D M
D
Patient Antisepsis
Iodine compounds– Slow release to avoid irritation
Povidone ‘carrier’ Povacrylex film former
Chlorhexidine– Superior for intravenous lines
Alcohols– Combined for rapid effect

Page
Skin Flora Counts after Chlorhexidine/Alcohol Preparation
“Skin preparation with ethanol/ chlorhexidine is unable to suppress the physiological skin flora for the duration of a heart operation*.”
*KÜHME,T, et al., Wound contamination in cardiac surgery. A systematic quantitative and qualitative study of bacterial growth in sternal wounds in cardiac surgery patients APMIS (2007) 115, 1001–1007.
Skin Flora Counts AFTER Isopropyl Alcohol
1
10
100
1000
10000
100000
1000000
1 10 100 1000 10000 100000 1000000 10000000
CFUs per square cm BEFORE skin preparation
CF
Us
per
sq c
m A
FT
ER
pre
p
Acceptable antiseptic
action
STAPH EPIDERMIDIS CFUs AFTER Iodophor
1
10
100
1000
10000
1 10 100 1000 10000 100000 1000000 10000000
CFUs per sq cm BEFORE skin preparationCF
Us
per
sq c
m A
FT
ER
(S
epi
)
Acceptable antisepsis
A.B. Cronquist, K. Jakob, L.Lai, P. Dellla Latta, and E.L. Larson. “Relationship between skin microbial counts and surgical site infection after neurosurgery.” Clin.Infect. Dis 33, no. 8(2001): 1302-08. Keywords: clinical study/infection/ioban/postoperative/PP
io009/skin preparation/skin
Page
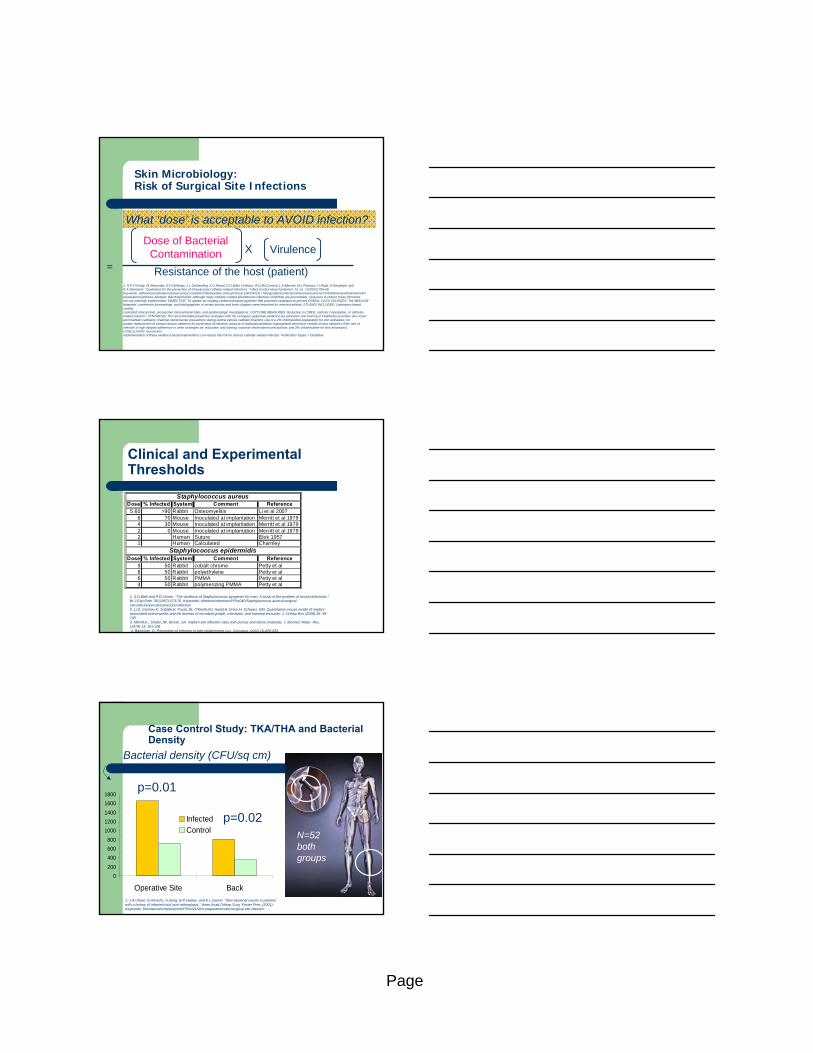
Skin Microbiology:Risk of Surgical Site Infections
==
Dose of Bacterial Contamination Virulence
Resistance of the host (patient)
X
What ‘dose’ is acceptable to AVOID infection?
1. N.P.O'Grady, M.Alexander, E.P.Dellinger, J.L.Gerberding, S.O.Heard, D.G.Maki, H.Masur, R.D.McCormick, L.A.Mermel, M.L.Pearson, I.I.Raad, A.Randolph, and R.A.Weinstein. "Guidelines for the prevention of intravascular catheter-related infections." Infect.Control Hosp.Epidemiol. 23, no. 12(2002):759-69.Keywords: adherence/catheters/central venous catheter/chlorhexidine clinical/clinical trial/Clinical Trials/guideline/infection/infections/outcome PPio062/review/Risk/skin/skin preparation/synthesis Abstract: BACKGROUND: Although many catheter-related bloodstream infections (CRBSIs) are preventable, measures to reduce these infectionsare not uniformly implemented. OBJECTIVE: To update an existing evidenced-based guideline that promotes strategies to prevent CRBSIs. DATA SOURCES: The MEDLINE database, conference proceedings, and bibliographies of review articles and book chapters were searched for relevant articles. STUDIES INCLUDED: Laboratory-based studies,controlled clinical trials, prospective interventional trials, and epidemiologic investigations. OUTCOME MEASURES: Reduction in CRBSI, catheter colonization, or catheter-related infection. SYNTHESIS: The recommended preventive strategies with the strongest supportive evidence are education and training of healthcare providers who insert and maintain catheters; maximal sterile barrier precautions during central venous catheter insertion; use of a 2% chlorhexidine preparation for skin antisepsis; noroutine replacement of central venous catheters for prevention of infection; and use of antiseptic/antibiotic-impregnated short-term central venous catheters if the rate of infection is high despite adherence to other strategies (ie, education and training, maximal sterile barrier precautions, and 2% chlorhexidine for skin antisepsis). CONCLUSION: Successfulimplementation of these evidence-based interventions can reduce the risk for serious catheter-related infection. Publication Types: • Guideline
Clinical and Experimental Thresholds
Dose % Infected System Comment Reference5.60 >90 Rabbit Osteomyelitis Li et al 2007
6 70 Mouse Inoculated at implantation Merritt et al 19794 30 Mouse Inoculated at implantation Merritt et al 19792 0 Mouse Inoculated at implantation Merritt et al 19792 Human Suture Elek 19571 Human Calculated Charnley
Dose % Infected System Comment Reference9 50 Rabbit cobalt chrome Petty et al8 50 Rabbit polyethylene Petty et al6 50 Rabbit PMMA Petty et al4 50 Rabbit polymerizing PMMA Petty et al
Staphylococcus aureus
Staphylococcus epidermidis
1. S.D.Elek and P.D.Conen. "The virulence of Staphylococcus pyogenes for man. A study of the problem of wound infections." Br.J.Exp.Path. 38,(1957):573-76. Keywords: infection/infections/PPss040/Staphylococcus aureus/surgicalsite infection/virulence/wound infection2..Li,D, Gromov,K, Soballe,K, Puzas,JE, O'Keefe,RJ, Awad,H, Drissi,H, Schwarz, EM. Quantitative mouse model of implant associated osteomyelitis and the kinetics of microbial growth, osteolysis, and humoral immunity. J. Orthop.Res (2008) 26: 96-105.3. Merritt,K., Shafer,JW, Brown, SA. Implant site infection rates with porous and dense materials. J. Biomed. Mater. Res. (1979) 13: 101-108.4. Bannister, G, Prevention of infection in joint replacement Curr. Orthopaed. (2002) 16:426-433
Case Control Study: TKA/THA and Bacterial Density
N=52 both groups
0
200
400
600
800
1000
1200
1400
1600
1800
Operative Site Back
InfectedControl
p=0.01
p=0.02
Bacterial density (CFU/sq cm)
1. J.A.Urban, S.Hinrichs, H.Song, B.P.Hasley, and K.L.Garvin. "Skin bacterial counts in patients with a history of infected total joint arthroplasty.“ Amer.Acad.Orthop.Surg. Poster Pres.,(2001).Keywords: biomaterials/implant/joint/PPio021/skin preparation/skin/surgical site infection
Page
Outline
Framing the discussion The relationship of contamination to infection
Sources of infection-patient skin Local factors-host response Implants as a special case-high morbidity Biofilm formation-common critical factor
Reducing contamination and infection Antisepsis
Antisepsis does NOT form sterile surfaceThreshold for infection ~100 organisms (per sq
cm) Sterile surface formation
Future
Part 3 - Levels of Evidence Supporting Sterile Surface Value
Levels of Evidence for Antiseptics
In vitro – Kill rate
– Minimum bacteriocidal level
– Minimum inhibitory (bacteriostatic) level
– Bacterial capture/immobilization
In vivo– Reduction in wound contamination rate
– Reduction in surgical site infection rate

Page
In Vitro Kill Rate: Povacrylex
Organisms placed on top of dried Povacrylex film (% Microbial kill)
MBCs for Povacrylex and Betadine
Povacrylex Solution
Povacrylex
Bacterial ImmobilizationNatural consequence of film formation
Povacrylex Solution + Bacteria Povacrylex Solution Control
Page
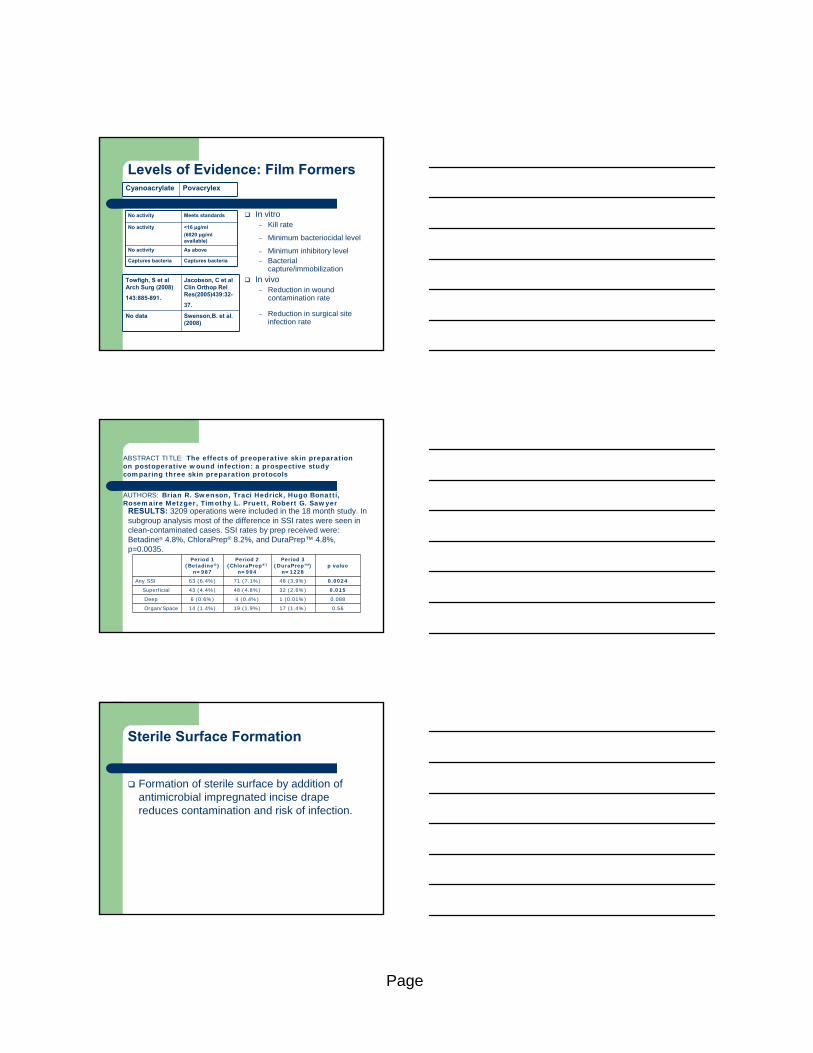
Levels of Evidence: Film Formers
In vitro – Kill rate
– Minimum bacteriocidal level
– Minimum inhibitory level– Bacterial
capture/immobilization
In vivo– Reduction in wound
contamination rate
– Reduction in surgical site infection rate
Cyanoacrylate Povacrylex
No activity Meets standards
No activity <16 μg/ml
(6020 μg/mlavailable)
No activity As above
Captures bacteria Captures bacteria
Towfigh, S et al Arch Surg (2008)
143:885-891.
Jacobson, C et al Clin Orthop Rel Res(2005)439:32-
37.
No data Swenson,B. et al. (2008)
ABSTRACT TITLE: The effects of preoperative skin preparation on postoperative wound infection: a prospective study comparing three skin preparation protocols
AUTHORS: Brian R. Swenson, Traci Hedrick, Hugo Bonatti, Rosemaire Metzger, Timothy L. Pruett, Robert G. Sawyer
RESULTS: 3209 operations were included in the 18 month study. In subgroup analysis most of the difference in SSI rates were seen in clean-contaminated cases. SSI rates by prep received were: Betadine® 4.8%, ChloraPrep® 8.2%, and DuraPrep™ 4.8%, p=0.0035.
Period 1(Betadine®)
n=987
Period 2(ChloraPrep®)
n=994
Period 3(DuraPrep™)
n=1228p value
Any SSI 63 (6.4%) 71 (7.1%) 48 (3.9%) 0.0024
Superficial 43 (4.4%) 48 (4.8%) 32 (2.6%) 0.015
Deep 6 (0.6%) 4 (0.4%) 1 (0.01%) 0.088
Organ/Space 14 (1.4%) 19 (1.9%) 17 (1.4%) 0.56
Sterile Surface Formation
Formation of sterile surface by addition of antimicrobial impregnated incise drape reduces contamination and risk of infection.

Page
Skin Microbiology:Risk of Surgical Site Infections
==
Dose of Bacterial Contamination
Virulence
Resistance of the host (patient)
X
900 prosthetic joint infections in >12,000 patients.
MRSA 28% of infections.
Lipsky, BA et al. Inf Ctl Hosp Epidemiol. (2007) 28:1290-1298.
Skin Microbiology:Risk of Surgical Site Infections
Skin Microbiology:Risk of SSI
With Antimicrobial impregnated incise Drape
Staph Aureus
↓ MRSA
Coagulase neg Staph.
Corynebacterium sp.
Without Antimicrobial impregnated incise Drape
Staph Aureus
MRSA
Coagulase neg Staph.
Corynebacterium sp.
Hemolytic strep. sp
E. faecalis
Enterococcus spp.
Proteus mirabilis
Burholdia cep.*Dohmen, PM Influence of skin flora and preventive measures on
surgical site infection during cardiac surgery. Surg. Infec. (Larchmt) (2006) 7 Suppl 1: S13-S17.

Page
Sterile Surface Formationand Virulence
Use of an iodophor impregnated incise drape – Reduces density of MRSA in wounds
– Reduces density of multiple ‘less virulent’pathogens
Antimicrobial Impregnated Incise Drape Reduces Wound Contamination
Fairclough, J.A. et al., The prevention of wound contamination by skin organisms by the pre-operative application of an iodophor impregnated plastic adhesive drape. J Int Med Res. 1986;14(2):105-9.
Jacobson, C. et al., Prevention of wound contamination using DuraPrep solution plus Ioban2 drapes. Clin Orthop Relat Res. (2005)439:32-7.
Meta-Analysis References
Hagen KS, Teston-Auran J. A comparison of two skin preps used in cardiac surgical procedures. AORN J (1995) 62: 393-402.
Pinheiro SMC,Mafra S, Couto BRGM, Starling CAF. Woven drape versus adhesive drape impregnated with PVPI: comparison of surgical infections incidence. S54, SHEA 1997 Meeting Abstract.
Segal CG and Anderson JJ. Preoperative skin preparation of cardiac patients. AORN J (2002) 76: 821-828.
Dewan PA, VanRu AM, Robinson RG, Skeggs GB, Fergus M. The use of an iodophor impregnated plastic drape in abdominal surgery- a controlled clinical trial. Aust NZ J Surg (1987) 57: 859-863.
Yoshimura Y, Kubo S, Hirohaski K, et al. Plastic iodophor drape during liver surgery: operative use of an iodophor impregnated adhesive drape to prevent wound infection during high risk surgery. World J Surg (2003) 27: 685-688.
Dahlin LG, Granfeldt H, Hultkvist H. A multimodel approach for reducing wound infections after sternotomy. Interactive Cardiovasc. Thor. Surg. (2004) 3: 206-210.

Page
Meta-Analysis: Antimicrobial Impregnated Incise Drape Reduces Risk
Outline
Framing the discussion Reducing contamination and infection AntisepsisAntisepsis does NOT form sterile surfaceThreshold for infection ~100 organisms (per sq cm)
Sterile surface formation-REDUCES Exposure to virulent strains (MRSA) Exposure to multiple organisms with different virulence levelsWound contaminationRisk of surgical site infection
Future
Future
“Prediction is difficult…………especially the future.” (Neils Bohr)
Vaccination against most common pathogens
Antimicrobial impregnated incise drapes containing different or multiple antiseptics
Reduction in wound damage through– Incise drape modification to improve healing
– Minimal incision/invasive surgery
Page
Summary
Wound contamination is important in reducing risk of infection for high morbidity surgery:
– Implant/indwelling devices
Risk of infection is the result of a balance of factors
– Local host response– Bacterial virulence– Bacterial contamination
Timely antibiotics can reduce contamination and infection
Antiseptics are critical but incomplete Sterile surface formation can reduce risk of
wound contamination and wound infection
Patrick J. Parks M.D. Ph.D. Credentials
M.D. School of Medicine 1978
Case Western Reserve University
Cleveland, Ohio
Ph.D. Department of Biomedical Engineering 1977
(bio materials track)
Case Western Reserve University
Cleveland, Ohio
B.S.Ch. E. Department of Chemical Engineering 1972
University of Pittsburgh
Pittsburgh, Pennsylvania
Education
Acknowledgements
Egil Lingaas M.D.Ph.D. Shelley-Ann Walters MS Stat David O’Sullivan, Ph.D. Laura Lyden Karen Zaruba Ken Kato, Ph.D.
Page
Thank you