part 2: prognosis in penetrating brain injury - neurosurgery · each guideline section. it should...
TRANSCRIPT

Part 2: Prognosis in Penetrating Brain InjuryJ Trauma. 2001;51:S44–S86.
INTRODUCTION AND METHODOLOGYPart 2 of this document presents early clinical indicators
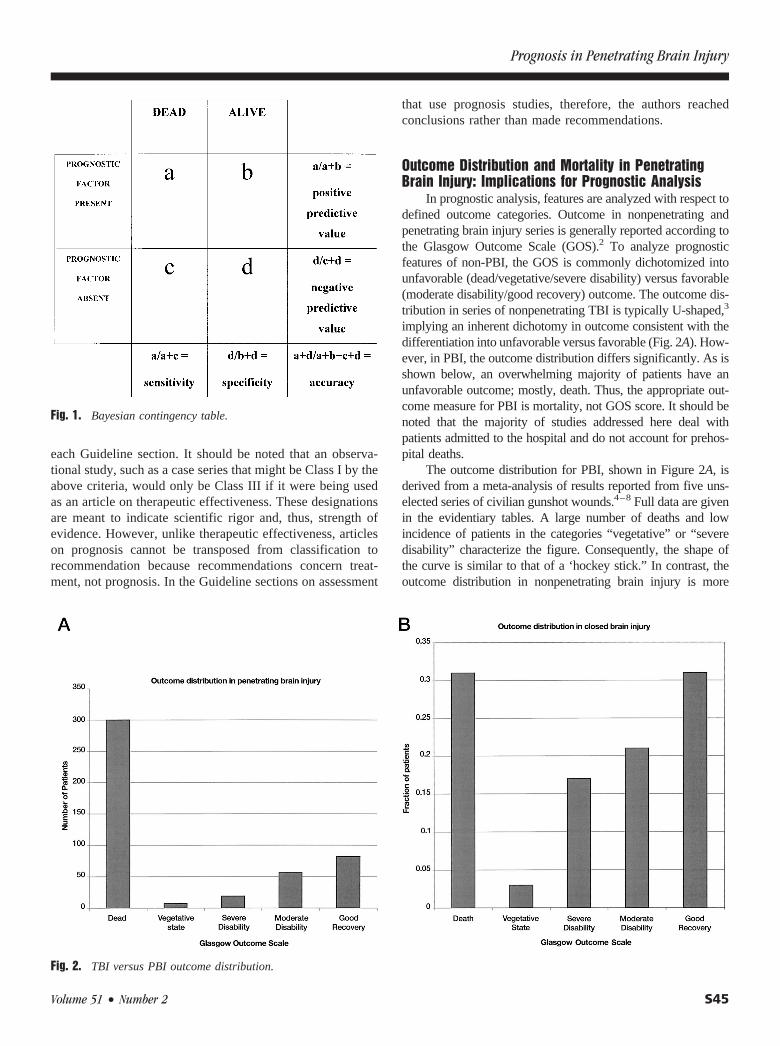
that may be prognostic of outcome among patients with pene-trating brain injury (PBI). This portion of the document is de-rived from the same principles of clinical epidemiology de-scribed in Part 1 of this Guideline’s methodology section, andevaluates the pertinent literature on prognosis in patients withPBI qualitatively. The clinical factors used to determine prog-nosis for this section of the Guideline were determined byclinical assessments derived from measures with proven reliabil-ity (e.g., pupillary reflex or Glasgow Coma Scale [GCS] score).In this context, reliability means that different people with dif-ferent backgrounds will reach the same conclusion about whatthey observe most of the time. Fortunately, good studies testingthe reliability of these measures have been carried out, and willbe discussed in the section on assessment that follows. Onlyreliable measures were included in this document. These includethe following: clinical assessments (GCS score, pupillary sizeand reactivity, intracranial pressure [ICP], and neuroimaging),factual data (demographics, e.g., age), epidemiology (cause andmode of injury and caliber of weapon), and systemic measures(hypotension, coagulopathy, respiratory depression). Demo-graphic factors such as race and gender were excluded becausethe literature lacked data on these topics. If we liken clinicalassessments to diagnostic tests, and particularly to their role aspredictors of poor outcome, we must be able to determinewhether the diagnostic test has sensitivity, specificity, and pos-itive or negative predictive value. An explanation of these fac-tors is described below in a bayesian contingency table (Fig. 1).
In a diagnostic test, sensitivity and specificity measurethe appropriateness of the test. However, in prognosis, themost important aspects of this model are positive and nega-tive predictive value. Positive predictive value represents thenumber of patients who had the clinical sign or prognosticindicator and had a poor outcome. For this to be meaningfuland useful, a minimum positive predictive value of 70% orgreater is thought to be necessary. However, this is inappro-priate in PBI, since the prevalence of death is so high. There-fore, a different and more precise measure of prediction isused, as discussed below.
To analyze prognostic parameters in nonpenetrating trau-matic brain injury (TBI), a probability of at least 70% of a givenoutcome has been used as a cut-off point in defining parametersof clinical importance.1 According to the bayesian statisticalapproach, the probability of a defined outcome in analyzingprognostic features should be viewed with respect to the ‘priorprobability,” i.e., the distribution of outcome in the populationstudied. Since the prevalence of death (the primary outcome
measure) in PBI is already above 70% in most series, whenassessing positive predictive values of various prognostic indi-cators, a cut-off point of 70% is not relevant to this population.Therefore, instead of using a high positive predictive value as thestandard of clinical importance, we used the odds ratio.
The odds ratio is an estimate of relative risk for theoutcome of interest if the studied factor is present as opposedto the factor being absent. Data from each article were usedto determine the odds ratio for each prognostic indicator. Forexample, an odds ratio of 1 indicates no increase in risk if thefactor is present, and an odds ratio of 3 indicates a three timesgreater risk of the same outcome. A 95% confidence intervalwas also calculated for each odds ratio. Clinical significancewas defined as an odds ratio whose 95% confidence intervaldid not include the number 1.
Prognosis studies (including prognosis with treatment)can have strength or weakness just like studies of therapeuticeffectiveness. In the strongest studies, the patients should:
● Be seen at a uniform time in their disease (e.g., at timeof admission to treating facility).
● Be followed prospectively for a designated block oftime (e.g., for the first 24 hours after injury).
● Have their outcomes measured definitively and reliably(e.g., death).
● Be part of a continuous or defined cohort of at least 25patients (e.g., from an ongoing, prospectively collecteddatabase).
● Be examined for extraneous prognostic variables, suchas underlying disease or age (e.g., use of appropriate statisticssuch as multivariate analysis).
Published studies that report on prognosis cannot beassessed using the same paradigm as those for therapeuticeffectiveness. Prognosis studies are observational in natureand can never be randomized controlled trials, which aremeant to compare treatments. However, for consistency inassessing “levels” of evidence in reaching conclusions aboutprognosis, the same designations (Class I, II, and III) as thosefor therapeutic effectiveness were identified. The Guidelinedevelopment group agreed on the following definitions:
● Class I—articles with all of the above characteristics.● Class II—articles exhibiting four out of the five char-
acteristics (including prospectively collected data).● Class III—articles with three or fewer of any of the
above characteristics.
Using this classification scheme, all published articleswere evaluated and are listed in the evidentiary tables within
The Journal of TRAUMA� Injury, Infection, and Critical Care
S44 August Supplement 2001
each Guideline section. It should be noted that an observa-tional study, such as a case series that might be Class I by theabove criteria, would only be Class III if it were being usedas an article on therapeutic effectiveness. These designationsare meant to indicate scientific rigor and, thus, strength ofevidence. However, unlike therapeutic effectiveness, articleson prognosis cannot be transposed from classification torecommendation because recommendations concern treat-ment, not prognosis. In the Guideline sections on assessment
that use prognosis studies, therefore, the authors reachedconclusions rather than made recommendations.
Outcome Distribution and Mortality in PenetratingBrain Injury: Implications for Prognostic Analysis
In prognostic analysis, features are analyzed with respect todefined outcome categories. Outcome in nonpenetrating andpenetrating brain injury series is generally reported according tothe Glasgow Outcome Scale (GOS).2 To analyze prognosticfeatures of non-PBI, the GOS is commonly dichotomized intounfavorable (dead/vegetative/severe disability) versus favorable(moderate disability/good recovery) outcome. The outcome dis-tribution in series of nonpenetrating TBI is typically U-shaped,3
implying an inherent dichotomy in outcome consistent with thedifferentiation into unfavorable versus favorable (Fig. 2A). How-ever, in PBI, the outcome distribution differs significantly. As isshown below, an overwhelming majority of patients have anunfavorable outcome; mostly, death. Thus, the appropriate out-come measure for PBI is mortality, not GOS score. It should benoted that the majority of studies addressed here deal withpatients admitted to the hospital and do not account for prehos-pital deaths.
The outcome distribution for PBI, shown in Figure 2A, isderived from a meta-analysis of results reported from five uns-elected series of civilian gunshot wounds.4–8 Full data are givenin the evidentiary tables. A large number of deaths and lowincidence of patients in the categories “vegetative” or “severedisability” characterize the figure. Consequently, the shape ofthe curve is similar to that of a ‘hockey stick.” In contrast, theoutcome distribution in nonpenetrating brain injury is more
Fig. 1. Bayesian contingency table.
Fig. 2. TBI versus PBI outcome distribution.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S45
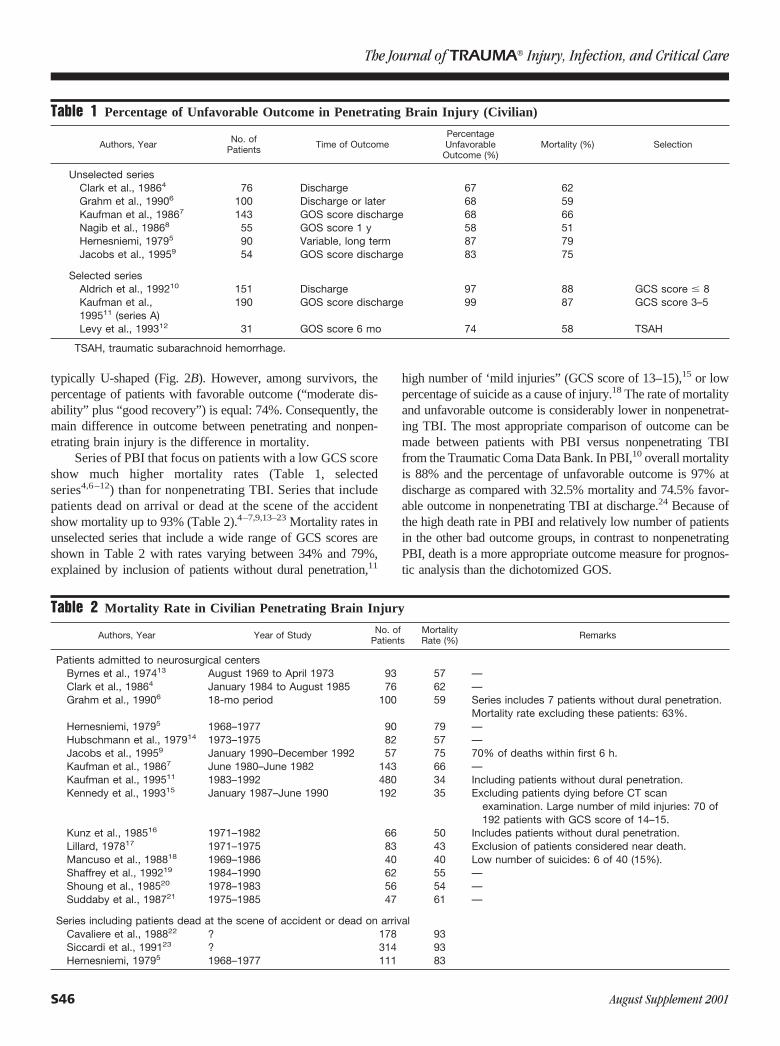
typically U-shaped (Fig. 2B). However, among survivors, thepercentage of patients with favorable outcome (“moderate dis-ability” plus “good recovery”) is equal: 74%. Consequently, themain difference in outcome between penetrating and nonpen-etrating brain injury is the difference in mortality.
Series of PBI that focus on patients with a low GCS scoreshow much higher mortality rates (Table 1, selectedseries4,6–12) than for nonpenetrating TBI. Series that includepatients dead on arrival or dead at the scene of the accidentshow mortality up to 93% (Table 2).4–7,9,13–23 Mortality rates inunselected series that include a wide range of GCS scores areshown in Table 2 with rates varying between 34% and 79%,explained by inclusion of patients without dural penetration,11
high number of ‘mild injuries” (GCS score of 13–15),15 or lowpercentage of suicide as a cause of injury.18 The rate of mortalityand unfavorable outcome is considerably lower in nonpenetrat-ing TBI. The most appropriate comparison of outcome can bemade between patients with PBI versus nonpenetrating TBIfrom the Traumatic Coma Data Bank. In PBI,10 overall mortalityis 88% and the percentage of unfavorable outcome is 97% atdischarge as compared with 32.5% mortality and 74.5% favor-able outcome in nonpenetrating TBI at discharge.24 Because ofthe high death rate in PBI and relatively low number of patientsin the other bad outcome groups, in contrast to nonpenetratingPBI, death is a more appropriate outcome measure for prognos-tic analysis than the dichotomized GOS.
Table 1 Percentage of Unfavorable Outcome in Penetrating Brain Injury (Civilian)
Authors, Year No. ofPatients Time of Outcome
PercentageUnfavorable
Outcome (%)Mortality (%) Selection
Unselected seriesClark et al., 19864 76 Discharge 67 62Grahm et al., 19906 100 Discharge or later 68 59Kaufman et al., 19867 143 GOS score discharge 68 66Nagib et al., 19868 55 GOS score 1 y 58 51Hernesniemi, 19795 90 Variable, long term 87 79Jacobs et al., 19959 54 GOS score discharge 83 75
Selected seriesAldrich et al., 199210 151 Discharge 97 88 GCS score � 8Kaufman et al.,199511 (series A)
190 GOS score discharge 99 87 GCS score 3–5
Levy et al., 199312 31 GOS score 6 mo 74 58 TSAH
TSAH, traumatic subarachnoid hemorrhage.
Table 2 Mortality Rate in Civilian Penetrating Brain Injury
Authors, Year Year of Study No. ofPatients
MortalityRate (%) Remarks
Patients admitted to neurosurgical centersByrnes et al., 197413 August 1969 to April 1973 93 57 —Clark et al., 19864 January 1984 to August 1985 76 62 —Grahm et al., 19906 18-mo period 100 59 Series includes 7 patients without dural penetration.
Mortality rate excluding these patients: 63%.Hernesniemi, 19795 1968–1977 90 79 —Hubschmann et al., 197914 1973–1975 82 57 —Jacobs et al., 19959 January 1990–December 1992 57 75 70% of deaths within first 6 h.Kaufman et al., 19867 June 1980–June 1982 143 66 —Kaufman et al., 199511 1983–1992 480 34 Including patients without dural penetration.Kennedy et al., 199315 January 1987–June 1990 192 35 Excluding patients dying before CT scan
examination. Large number of mild injuries: 70 of192 patients with GCS score of 14–15.
Kunz et al., 198516 1971–1982 66 50 Includes patients without dural penetration.Lillard, 197817 1971–1975 83 43 Exclusion of patients considered near death.Mancuso et al., 198818 1969–1986 40 40 Low number of suicides: 6 of 40 (15%).Shaffrey et al., 199219 1984–1990 62 55 —Shoung et al., 198520 1978–1983 56 54 —Suddaby et al., 198721 1975–1985 47 61 —
Series including patients dead at the scene of accident or dead on arrivalCavaliere et al., 198822 ? 178 93Siccardi et al., 199123 ? 314 93Hernesniemi, 19795 1968–1977 111 83
The Journal of TRAUMA� Injury, Infection, and Critical Care
S46 August Supplement 2001
Timing of Outcome Measure in PBIImplications for Classification of Data
Death after PBI usually occurs soon after injury. Cava-lieri et al.22 describe 95% of deaths occurring within 3 hoursand 97% within 24 hours of injury. Siccardi et al. report 92%of deaths occurring within 3 hours. In the study reported byGrahm et al.,6 77% of patients died before admission to theintensive care unit; in the study by Shaffrey et al.,19 53%.Hernesniemi5 describes 76% of all deaths occurring in thefirst 24 hours, and Jacobs et al.9 also found that 93% of deathsoccurred in the first 24 hours. The percentages of deathoccurring within 12, 24, or 48 hours after injury, as reportedin three studies, are shown in Table 3. The observation that,of the patients who die, the majority of deaths occur within
the first 24 hours (70%) implies that the majority of outcomesin any given study occurs within the first 24 to 48 hours. Forthis reason, measurement of early mortality is relevant forprognostic purposes.
Civilian versus Military Penetrating InjuriesImplications for Prognostic Analysis
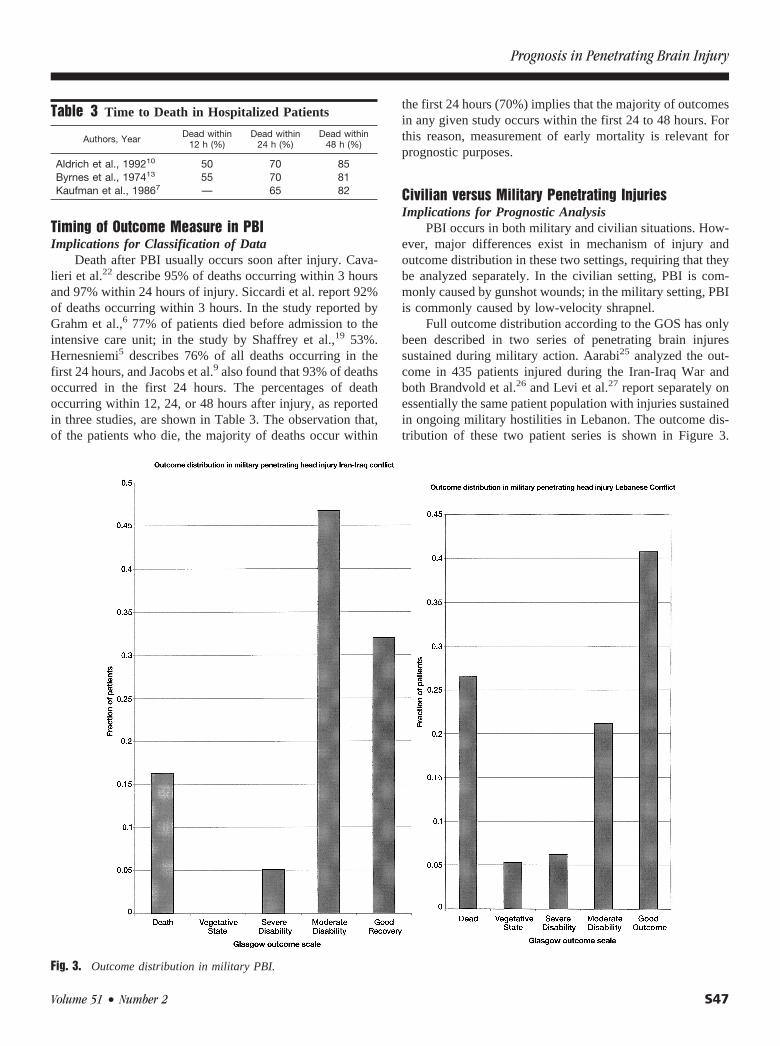
PBI occurs in both military and civilian situations. How-ever, major differences exist in mechanism of injury andoutcome distribution in these two settings, requiring that theybe analyzed separately. In the civilian setting, PBI is com-monly caused by gunshot wounds; in the military setting, PBIis commonly caused by low-velocity shrapnel.
Full outcome distribution according to the GOS has onlybeen described in two series of penetrating brain injuressustained during military action. Aarabi25 analyzed the out-come in 435 patients injured during the Iran-Iraq War andboth Brandvold et al.26 and Levi et al.27 report separately onessentially the same patient population with injuries sustainedin ongoing military hostilities in Lebanon. The outcome dis-tribution of these two patient series is shown in Figure 3.
Fig. 3. Outcome distribution in military PBI.
Table 3 Time to Death in Hospitalized Patients
Authors, Year Dead within12 h (%)
Dead within24 h (%)
Dead within48 h (%)
Aldrich et al., 199210 50 70 85Byrnes et al., 197413 55 70 81Kaufman et al., 19867 — 65 82
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S47

When comparing this figure to the composite outcome dis-tribution in penetrating brain injuries in the civilian situation(Fig. 2A), it is evident that the outcome in injuries sustainedduring military action is significantly different from civilianpenetrating brain injuries.
Military PBI series differ from civilian series in bothmechanism of injury and severity. A number of issues explainthe differences in reported outcomes between military andcivilian PBI. In civilian injuries, gunshot wounds are theprimary cause of PBI. In addition, among civilians, suicide isthe most common cause of gunshot wounds to the brain,implying contact injuries, with high-energy transmission intothe brain. A large proportion of deaths in civilian injuriesoccurs during the first few hours after injury.
In the military setting, penetrating injuries that reachmedical attention are predominantly caused by shell andshrapnel injuries. Because of the extremely damaging natureof the cerebral injuries inflicted by the high velocity of bulletscommonly found in war injuries, the majority of those suf-fering battlefield gunshot wounds to the head presumablynever reach medical care. This skews the surviving militaryPBI population toward lower velocity shrapnel wounds. Thepriorities of field triage under battle conditions means thatthere is no control for those patients who are found to have alow probability of survival and therefore are not prioritizedfor rapid transport. Although evacuation times from the frontline to military hospitals has been considerably improved inthe past two decades, the average time to arrival at thehospital is considerably longer than in civilian situations.Brandvold et al.26 describe a mean evacuation time in themilitary setting of 2.3 hours. In civilian injures, the averagetime from injury to hospital is less than 30 to 45 minutes.
Additionally, the exigencies of war mean that the deter-minants of the methods and applications of field resuscitation
and triage are difficult to control and compare with thecivilian situation. There is also a much higher likelihood ofwound contamination in the battlefield. The conditions underwhich early surgical treatment is rendered are generallyunique and more limited with respect to treatment facilities inthe civilian setting. For instance, although computed tomo-graphic (CT) scanning was generally available in civilianemergency centers in the 1970s, the first reports describingroutine use of CT scanning in the military situation date fromconflicts in the early 1980s. Also, injuries in the militarysetting occur primarily in young men in otherwise excellentphysical condition; this contrasts with the civilian setting,where a broader age range is represented.
Death rates are similarly much lower for patients whoreach care for penetrating injuries occurring in the militarysetting than in civilian penetrating brain injuries. The re-ported case fatality rate from World War II is 10% to13%.28,29 Meirowski observed a 10% mortality reportingamong 673 penetrating brain wounds from Korea. Oncomposite analysis of 2,187 consecutive penetratingwounds of the brain from Vietnam, Hammon30 describes ahospital mortality of 11%. This excludes, however, pa-tients with injuries of extreme severity in whom the man-agement policy was ‘unoperated expectant.” When thesepatients were included, an overall mortality of approxi-mately 30% was demonstrated. This rate is very similar tothe 26% mortality described in the series reporting oninjuries sustained during the Lebanese conflict. The deathrate reported by Aarabi for the Iran-Iraq War is consider-ably lower at 16.3%. However, this series concerns aselected patient population referred to a tertiary center fordefinitive treatment. The mean time from injury to arrivalat this center was 49 hours (range, 7– 450 hours).
Evidentiary Table: Outcome Distribution of Penetrating Brain Injury—Military Injuries
Authors, Year DataClass Description of Study Inclusion Criteria
Time of Outcomeand OutcomeDistribution
No.Dead
No.Vegetative
No. withSevere
Disability
No. withModerateDisability
No. withGood
RecoveryTotal
Aarabi, 199025 III Analysis of outcome in 435patients in whom full datawere available from aseries of 690 patientswith missile headwounds, sustained duringthe Iran-Iraq War,evacuated to Nemazeehospital in Shiraz.
435 of 690 patientsevacuated to Nemazeehospital with missile headwounds and duralpenetration. 255 patientswere excluded from thestudy (58 patients forinadequate information onadmission GCS score, 64patients for inadequateinformation about type ofmissile injury, and 132patients for insufficientfollow-up). Mean timefrom injury to arrival atNemazee hospital was 49hours (range, 7–450 h).
364 of the 435patients werefollowed for atleast 6 mo.
71 0 22 203 139 435
The Journal of TRAUMA� Injury, Infection, and Critical Care
S48 August Supplement 2001

Evidentiary Table. Continued.
Authors, Year DataClass Description of Study Inclusion Criteria
Time of Outcomeand OutcomeDistribution
No.Dead
No.Vegetative
No. withSevere
Disability
No. withModerateDisability
No. withGood
RecoveryTotal
Brandvold et al.,199026
III Retrospective analysis of113 patients evacuated toRambam MaimonidesMedical Center withpenetrating craniocerebralinjuries sustained inongoing military hostilitiesin Lebanon. Essentiallythe same patientpopulation as describedby Levi et al.
All patients with penetratinghead injury evacuated toRambam MaimonidesMedical Center, theprimary evacuation centerfor those wounded inIsraeli-occupied territory.Median time from injuryto arrival at RambamMaimonides MedicalCenter emergencydepartment was 2.0 h.Initially, the seriescontained 116 patients,but 3 were removed afterreview of charts, becausethere was no penetratinginjury.
Outcome atdischarge
30 6 7 24 46 113
Levi et al.,199012
III Retrospective study on 116patients with penetratinginjury, occurred duringinvolvement of Israelidefense forces inLebanon from June 1982to June 1985. Essentiallysame patient populationas described byBrandvold et al.
All patients with penetratinghead injury sustainedduring ongoing hostilitiesin Lebanon evacuated toRambam MaimonidesMedical Center. Seriesincludes patients reachingthe facility alive.
GOS scoredischarge
30 6 7 24 49 116
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S49

PROGNOSTIC INDICATORSThe following variables will be discussed in the clinical
prognostic indicator section. Unless otherwise stated, conclu-sions will discuss civilian prognostic indicators (Table 4).
ProcessOf the original 65 articles, 24 were found to have adequate
information for inclusion in this section on prognostic clinical fea-tures. Cross-referencing and expertise available among the authorsadded an additional 19 published studies. Among the 43 studiesaddressing clinical prognostic features, 5 report on the relationbetween age and outcome in civilian PBI. Nine studies address therelation between cause of injury and outcome in civilian gunshotwounds. Three studies report on the relation between mechanism ofinjury in the military setting and outcome. Three studies providedata on the prognostic value of the mode of injury. Eight studiesinvestigate the relation between caliber and outcome.
Table 4 Prognostic Indicators
Variable Type Predictor Variables
Demographics AgeEpidemiology Cause of injury
Mode of injuryCaliber of weapon
Systemic measures HypotensionCoagulation disturbancesRespiratory distress
Neurologic measures Level of consciousness and GCS scorePupillary examinationIntracranial pressure
Neuroimaging features Missile trackEvidence of increased intracranial pressurePresence of hemorrhage or mass lesion
The Journal of TRAUMA� Injury, Infection, and Critical Care
S50 August Supplement 2001

DEMOGRAPHIC FACTORS: AGEI. Conclusion
Increasing age correlates with increased mortality afterpenetrating brain injury (Class III).
II. OverviewAge has been shown to be one of the most important
prognostic factors in evaluating prognosis after nonpenetrat-ing TBI. The mean age reported in 10 civilian series thatdescribe age in PBI ranges from 25 to 35 years (Table 5).
Four series, three of which exclude patients dead onarrival, report the age distribution in decades (Table 6). Re-ported series on PBI among patients admitted to the hospital,however, include relatively few patients in older age groups.In the series by Clark et al.4 describing 76 patients withcivilian gunshot wounds, only six patients above 65 years ofage were included. Suddaby et al.21 reported on 59 patients,and only three patients were over the age of 60.
The majority of patients in those series that excludepatients dead on arrival are in the third decade (20–29 years),and only 15 patients from these two series totaling 236patients are over the age of 50. The age distribution in thoseseries that include patients dead at the scene of accident ordead on arrival have many more patients over the age of 50.
III. Process (Methodology)Of the 43 studies that address clinical prognostic fea-
tures, 5 report on the relation between age and outcome incivilian PBI. In the military setting, PBI is largely restrictedto young men; consequently, analysis of the prognostic valueof age in military PBI is impractical.
IV. Scientific FoundationOnly two studies describe a significant relation between
age and outcome. Both Kaufman et al.7 and Siccardi et al.23
show a significantly higher mortality among patients over 49
years of age (odds ratio, 3.45–11.0). Suddaby et al.21 describea slightly better outcome among patients below 40 years ofage, but the finding was not statistically significant. Simi-larly, Jacobs et al.9 report a slightly higher average ageamong patients dying (34.5 vs. 29), but the differences are notstatistically significant. Hernesiemi5 states that the influenceof age is not statistically significant despite a trend towardsunfavorable outcome and higher mortality among patientsover 45 years of age.
V. SummaryAlthough age has been shown to be one of the most
significant prognostic indicators in nonpenetrating TBI, itssignificance in PBI is not as clear. In civilian series, the meanage of patients ranges between the second and third decades.Most series have relatively few patients in the older agegroups. Although patients older than 50 constitute a relativelylow percentage of patients in most series, statistical analysisreveals that age greater than 50 is associated with an in-creased mortality.
Table 5 Mean Age in Reported Series of PenetratingBrain Injury (Civilian)
Authors, Year No. ofPatients Mean Age (y) Range (y)
Grahm et al., 19906 100 35 8–87Hubschmann et al., 197914 82 14–67Kaufman et al., 199511 190 26 2–97Kaufman et al., 199511 146 25 � 11.6 3–82Lillard, 197817 83 29.6 2–72Nagib et al., 19868 55 34 5–77Shaffrey et al., 199219 62 39 10–72Shoung et al., 198520 56 35.3 5 mo–78 ySuddaby et al., 198721 47 30.4Jacobs et al., 19959 57 32.2 4 mo–95 yHernesniemi, 19795 42Levy et al., 199312 31 35.1 � 11.61 16 mo–97 y
Table 6 Age Distribution in Penetrating Brain Injury
Age (y)
Series Including Patients Dead At the Scene of the Accidentor Dead On Arrival Series Excluding Patients Dead On Arrival
Cavalieri et al., 198822
(n � 179) (%)Siccardi et al., 199123
(n � 314) (%)Byrnes et al., 197413
(n � 93) (%)Kaufman et al., 19867
(n � 143) (%)
0–9 1 1 2 710–19 4 4 34 2020–29 21 19 43 3430–39 18 17 11 1540–49 15 16 8 1050–59 16 17 0 760–69 9 10 1 470–79 9 12 1 180–89 7 5 0 1
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S51

VI. Evidentiary Table: Age
Authors, Year Year of Study Description of Study Class Conclusions
Siccardi etal., 199123
Retrospective study of 314consecutive patients with civiliangunshot wounds, of whom 228died at the scene of the accident.
III Mortality is significantly higher among patients over 49 y ofage (p � 0.01); OR: 3.45*
Age Dead Alive�50 130 5�50 158 21
No probability analysis performed because series includespatients dead at the scene of the accident (n � 314).
Kaufman etal., 19867
January 1980–June 1982
Descriptive and prognostic(retrospective) study of 143patients with civilian gunshotinjuries.
III Survival rates related to age, being good among patientsunder 10 y of age and poorer among those over 40.
Age Dead Alive�50 18 1�50 77 47
Pprior, 66%; PPV, 95%; OR, 11.0* (n � 143).Suddaby et
al., 1987211975–1985 Retrospective analysis of 49
patients with low-velocity gunshotwounds.
III Slightly better outcome among patients below 40 y of age,but not statistically significant difference (p � 0.88).
Alive Age (y)
GOS Discharge
Mortality (Dead)Unfavorable Favorable
3 �40 6 3 616 �40 25 15 24
Pprior, 61%; PPV, 67%; OR, 1.33 (n � 49).
Jacobs et al.,19959
January 1990–December1992
Retrospective analysis of 57patients in whom full data wereavailable from 72 cases admittedfrom January 1990 to December1992 with transcranial gunshotwounds. Focus of the study is oncost and consequences.
III Average age is slightly higher among patients dying (34.5vs. 29). No statistically significant difference.
Hernesniemi,19795
1968–1977 Retrospective study of 90 patientsadmitted to neurosurgicaldepartment with penetratinggunshot wounds.
III Authors states that in this series the influence of age onoutcome is not important. However, evidence presentedsuggests higher incidence of unfavorable outcomeamong patients over 45 y of age and mortality amongpatients over 60 (n � 22) is 95%.
GOS variable, long term:Age (y) Unfavorable Favorable
�45 31 3�45 47 9
Mortality:Age (y) Dead Alive
�45 30 4�45 41 15
Pprior, 79%; PPV, 88%; OR, 2.74 (n � 90).
OR, odds ratio; PPV, positive predictive value; Pprior, prior probability (the outcome distribution in the population studied).
The Journal of TRAUMA� Injury, Infection, and Critical Care
S52 August Supplement 2001

EPIDEMIOLOGY: CAUSE OF INJURYI. Conclusion
Suicide is correlated with a higher rate of mortality thanother causes of PBI (Class II).
II. OverviewIn civilians with PBI, gunshot wounds almost always are
the cause of the injury. These gunshot wounds may be acci-dental, self-inflicted (suicide), or caused by assault/homicide.The incidence of suicide as a cause of civilian PBI variesconsiderably among the series; from 5% to 88%. Clark et al.4
report suicide to be significantly more common in Cauca-sians. An overview of the incidence of suicide in civiliangunshot wounds is given in Table 7.
In military injuries, shrapnel/shell fragments and debrispredominate over missile wounds. In the series reported byAarabi,25 86% of injuries were caused by shell fragments.The series reported by Brandvold et al.26 reported 82% highermortality after gunshot wounds then in patients with shrapnelwounds.
III. Process (Methodology)Among the 43 studies that address clinical prognostic
features, 9 report on the relation between cause of injury andoutcome among civilians with gunshot wounds. Three studiesreport on the relation between mechanism of injury in themilitary setting and outcome.
IV. Scientific FoundationCivilian Injuries
Of the nine studies reporting on the results betweensuicide and outcome, seven describe a higher mortality andpoorer outcome for patients who attempted suicide comparedwith patients injured accidentally or by assault. In the seriesreporting a relation between suicide and mortality, odds ratiosvarying from 1.63 to 5.83 were calculated. In a smallerretrospective series of 56 patients, no such relation could befound.20 In the series reported by Cavalieri et al., includingpatients dead at the scene, no relation was found betweensuicide and mortality.22
Although mortality is higher in suicide than in othercauses, there remains the possibility that in some centers,suicide is treated less aggressively than other causes of PBI.In one survey of attitudes of neurosurgeons, over 60% ofneurosurgeons responding stated that suicide patients weremuch less likely to receive aggressive resuscitation efforts
than other types of patients.31 Therefore, suicide may be asignificant indicator of poor outcome not because there aresome physiologic variables that relate to poor outcome, butbecause this method of injury changes the behavior or expec-tations of the clinicians attending the patient. It is clear fromthe clinical psychology literature that patients who recoverfrom attempted suicide frequently report relief over survivaland express gratitude to their caregivers.32 Thus, the findingthat suicide has been shown to be a predictor of poor outcomeshould not deter clinicians from intervening.
Military InjuriesAarabi25 reports no statistically significant difference in
outcome between gunshot wounds and shell injuries. Brand-vold et al.,26 however, report a statistically highly significantincreased mortality among patients with gunshot wounds,with an odds ratio of 11.05 towards mortality. These diver-gent results may be explained by patient selection. In theseries reported by Aarabi,25 the mean time to admission was49 hours. Consequently, patients with more severe injuriesmay have been excluded.
V. SummaryAlthough the reported incidence varies among series,
suicide is a major cause of PBI among civilians, predomi-nantly because of gunshot wounds to the head. Suicide isassociated with higher mortality than other causes of PBI. Inthe military setting, PBI is caused mainly by shell and shrap-nel fragments, whereas military gunshot wounds are associ-ated with poorer outcomes.
Table 7 Reported Incidence of Suicide As Cause ofInjury in Civilian Gunshot Wounds
Authors, Year No. Suicide/Total No. Percentage Suicide
Cavaliere et al., 198822 126/178 71Clark et al., 19864 35/76 46Grahm et al., 19906 63/100 63Hernesniemi, 19795 78/90 87Jacobs et al., 19959 41/57 72Kaufman et al., 19867 61/143 43Levy et al., 199312 6/31 19Lillard, 197817 15/83 18Mancuso et al., 198818 5/40 13Nagib et al., 19868 21/55 38Shaffrey et al., 199219 37/62 60Shoung et al., 198520 35/56 63Siccardi et al., 199123 217/314 69Suddaby et al., 198721 43/49 88
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S53

VI. Evidentiary Table: Cause of Injury
Authors, Year Years of Study Description of Study Class Conclusions
CivilianGrahm et al.,
19906
Prospective study over an 18-moperiod of 100 patients with civiliangunshot wounds.
II Prognostic analysis on caliber, GCS, pupils, OCR,bihemispheric versus unilateral injury, and causeof injury. Prognosis is poorer among patients whoattempted suicide.
GOS discharge or latera:Unfavorable Favorable
Suicide 47 16Assault/unknown/other 21 16Pprior, 68%; PPV, 75%; OR, 2.23.
Mortality:Dead Alive
Suicide 44 19Assault/unknown/other 16 21Pprior, 60%; PPV, 70%; OR, 3.03.b
Lillard,197817
1971–1975 Retrospective analysis in 5-y period,describing 83 patients with PBI.
III Predictors of outcome: level of consciousness,cause of injury, caliber, missile track, multilobarinvolvement. Poorer prognosis among patientswho attempted suicide.
Dead AliveSuicide 8 7Assault/accident 28 40Pprior, 43%; PPV, 53%; OR, 1.63.
Nagib et al.,19868
1978–1983 Retrospective study of prognosisand management of civiliangunshot wounds during a 5-yperiod from 1978–1983.
III Related to poorer outcome: suicide level ofconsciousness, multilobar unilateral injury,bilateral injury.
GOS score at 1 y:GOS score
of 1/2GOS score
of 3/4/5Suicide 16 5Other 13 21Pprior, 53%; PPV, 76%; OR, 5.17.b
Mortality:Dead Alive
Suicide 15 6Other 13 21Pprior, 51%; PPV, 71%; OR, 4.03b (n � 55).
Siccardi etal., 199123
Retrospective study of 314consecutive patients with civiliangunshot wounds, of whom 228died at the scene of the accident.
III Mortality is higher in suicide, age �49, bilaterallesions or multilobar unilateral lesions,intraventricular hemorrhage. Mortality inattempted suicide is 95%; in other causes, 88%.
Shoung etal., 198520
1978–1983 Retrospective study on 56 patientswith craniocerebral gunshotwounds.
III Overall mortality is 53.6%. In cases of attemptedsuicide, no significant difference in mortality inrespect to overall population.
Dead AliveSuicide 17 18Accident/assault 13 8Prior, 54%; PPV, 49%; OR, 0.58 (n � 56).
The Journal of TRAUMA� Injury, Infection, and Critical Care
S54 August Supplement 2001

VI. Continued
Authors, Year Years of Study Description of Study Class Conclusions
Hernesniemi,19795
1968–1977 Retrospective study on 90 patientsadmitted to neurosurgicaldepartment with penetratinggunshot wounds.
III Prognostic factors analyzed: age, level ofconsciousness, caliber, missile track, cause ofinjury. High percentage of suicide in this series.Outcome in suicide is unfavorable.
GOS score at 1 mo or later:Unfavorable Favorable
Suicide 69 9Other cause 9 3Pprior, 87%; PPV, 88%; OR, 2.56.
Mortality:Dead Alive
Suicide 64 14Other cause 7 5Pprior, 79%; PPV, 82%; OR, 3.27 (n � 90).
Jacobs et al.,19959
January 1990–December1992
Retrospective analysis of 57patients in whom full data wereavailable from 72 cases admittedfrom January 1990 to December1992 with transcranial gunshotwounds. The study focuses oncost and consequences.
III Relation to mortality of Caucasian race, GCS score� 4, lateral trajectory. High percentage of suicideas cause of injury (72%).
Dead AliveSuicide 35 6Other cause 8 8Pprior, 75%; PPV, 85%; OR, 5.83.b
Cavaliere etal., 198822
Retrospective study of 178 patientswith civilian gunshot wounds.
III High overall mortality (93%). Mortality even higher inlesions crossing midline and massiveintraventricular hemorrhage. No relation betweensuicide and mortality.
Dead AliveSuicide 119 7Homicide 41 2No probability analysis performed because series
included patients dead on arrival.OR, 0.83 (n � 169).
Kaufman etal., 19867
January 1980–June 1982
Descriptive and prognostic(retrospective) study on 143patients with civilian gunshotinjuries.
III Cause of injury: assault 57%, suicide 43%. Mortalityhigher in attempted suicide
Dead AliveSuicide 48 13Assault 47 35Pprior, 66%; PPV, 78%; OR, 2.75b (n � 143).
MilitaryArabi, 199025 February
1981–August1988
Analysis of outcome in 435 patients inwhom full data were available from aseries of 690 patients with missilehead wounds, sustained during theIran-Iraq War, evacuated to Nemazeehospital in Shiraz.
III Outcome:GWSShell
Bad1155
Good40259
Pprior, 18%; PPV, 22%; OR, 1.3.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S55

VI. Continued
Authors, Year Years of Study Description of Study Class Conclusions
Brandvold etal., 199026
1982–June1985
Retrospective analysis of 113patients evacuated to RambamMaimonides Medical Center withpenetrating craniocerebral injuriessustained in ongoing militaryhostilities in Lebanon.
III GOS score at discharge:Unfavorable Favorable
GSW 14 4Shrapnel injury 25 59Pprior, 38%; PPV, 78%; OR, 8.26b
Mortality:Dead Alive
GSW 13 5Shrapnel injury 16 68Pprior, 28%; PPV, 72%; OR, 11.05.*
Levi et al.,199027
Retrospective study with penetratinginjury, occurred duringinvolvement of Israeli defenseforces in Lebanon from June 1982to June 1985. Essentially samepatient population as describedunder Brandvolt et al.
III GOS score at discharge:Unfavorable Favorable
GSW 13 2Shrapnel injury 26 64Pprior, 37%; PPV, 87%; OR, 16.*
Mortality:Dead Alive
GSW 12 3Shrapnel injury 17 73Pprior, 28%; PPV, 80%; OR, 17.18.*
OCR, oculocardiac reflex; Pprior, prior probability (the outcome distribution in the population studied); PPV, positive predictive value; OR,odds ratio; GSW, gunshot wound.
a Outcome was determined at discharge; among patients who were vegetative or severely disabled at discharge, a mean follow-up of 9 mowas performed.
b Indicates that the confidence interval for the odds ratio does not include 1.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S56 August Supplement 2001
EPIDEMIOLOGY: MODE OF INJURYI. Conclusion
Perforating injuries correlate with a poorer outcomewhen compared with either penetrating or tangential braininjuries (Class III).
II. OverviewPBIs are differentiated into the following categories:
penetrating (a foreign object penetrates skull and dura andremains lodged within the intracranial cavity); tangential (aforeign object glances off the skull, often driving bone frag-ments into the brain); and perforating (a ‘through-and-through‘ injury, characterized by entry and exit wounds).Debris and bone fragments commonly are present within thebrain in this latter type of injury.
Differentiation as to the mode of injury (penetrating/tangential/perforating) is found mainly in military series. Theabsence of reports of tangential injuries in the civilian pop-ulation is remarkable. A possible explanation could be thatsuch injuries are not recognized as a penetrating type of braininjury, but are classified as compound depressed skull frac-ture and included in series of patients with depressed skullfractures. The differentiation between a compound depressedskull fracture caused by a falling object and a tangential typeof PBI caused by a projectile appears to be arbitrary.
Major differences exist between military series concern-ing the incidence of penetrating, tangential, and perforatinginjuries. Aarabi25 describes penetrating injuries in 266 of 435(61%), tangential injuries in 128 of 435 (29%), and perforat-ing injuries in 41 of 435 (9%). In the series described byBrandvold et al.,26 the majority of injuries are classified aspenetrating; only one patient having a perforating injury, and10 of 113 (9%) tangential. No studies report on the relationbetween mode of injury and other features. However, it seems
that a relation between a perforating injury and a missilewound of relatively high velocity can be inferred from theballistic data and the geometry of the calvarium.
III. Process (Methodology)Among the 43 studies addressing clinical prognostic fea-
tures, 3 provided data on the prognostic value of the mode ofinjury.
IV. Scientific FoundationAarabi25 reports lower mortality and more favorable out-
come in patients with a tangential injury, though this was notstatistically significant. Brandvold et al.26 report no signifi-cant differences between outcome in penetrating and tangen-tial types of injury. On analysis of the results reported, how-ever, a significantly lower mortality can be shown intangential types of injuries, with an odds ratio of 3.58 whencompared with penetrating injuries.
Aarabi25 reports a significantly poorer outcome in per-forating types of injuries. Odds ratios of 4.18 (unfavorableoutcome) and 3.06 (mortality) can be calculated in the pres-ence of perforating injuries when compared with the othermodes of injury. The very low incidence (only one case) ofpenetrating injuries in the series reported by Brandvold etal.26 and Levi et al.27 limits their relevance.
V. SummaryMode of injury can be divided into perforating, penetrat-
ing, and tangential. The predictive value of the mode of injuryhas been studied mainly in the military setting. Although theincidence of these modes of injury varies among studies,perforating injuries are associated with the highest mortality.There is a trend toward higher mortality in penetrating inju-ries compared with tangential injuries, although no study hasshown a statistically significant increase in mortality.
VI. Evidentiary Table: Mode of Injury
Authors, Year Years of Study Description of Study Class Conclusions
Arabi, 199025 February 1981–August 1988
Analysis of outcome in 435 patients in whomfull data were available from a series of 690patients with missile head wounds,sustained during the Iran-Iraq War,evacuated to Nemazee hospital in Shiraz.
III Not related to outcome: side of injury, retentionof foreign material, type of projectile.
Related to outcome: mode of injury and GCSadmission.
Poor outcome in 19.9% of patients withpenetrating injury; 15.6% in tangential injuryand 48.8% in perforating injury.
Brandvold etal., 199026
1982–June 1985 Retrospective analysis of 113 patientsevacuated to Rambam Maimonides MedicalCenter with penetrating craniocerebralinjuries sustained in ongoing militaryhostilities in Lebanon.
III The mode of injury was an important factor inoutcome, with shrapnel and tangentialwounds faring better than gunshot wounds.
Levi et al.,199027
Retrospective study on 116 patients withpenetrating injury, occurred duringinvolvement of Israeli defense forces inLebanon from June 1982 to June 1985.Essentially same patient population asdescribed under Brandvolt et al.
III Parameters related to outcome: GCS score,mechanism of injury, intracerebral track,multilobar involvement, transventricular injury,hypotension.
GOS score at discharge.
a Indicates that the confidence interval for the odds ratio does not include 1.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S57

EPIDEMIOLOGY: CALIBER OF WEAPONI. Conclusion
The effect of weapon caliber on outcome, independent oftotal kinetic energy, was not demonstrated in the published data.
II. OverviewThe caliber of a missile is defined as the inner diameter
of the barrel of the weapon in inches or millimeters. Theamount of energy transmitted from a missile striking the headis dependent on its mass and velocity according to the for-mula: E � 1/2 MV2. Therefore, the velocity of a bullet willhave a greater effect on the transmission of kinetic energy tothe brain than its mass or caliber.
III. Process (Methodology)Among the 43 studies addressing clinical prognostic fea-
tures, 8 investigated the relation between caliber andoutcome.
IV. Scientific FoundationThe relation between missile caliber and patient outcome
is not clear. Some studies report an increased mortality with
increasing caliber of the weapon.4,6,17 The reported differ-ences, however, are not statistically significant. The lowincidence of larger caliber injuries often precludes definiteconclusions. Grahm et al.6 report a 75% mortality in rifleinjuries compared with 67% in low-caliber pistol injuries.The number of patients with rifle injuries, however, islow (n � 4).
V. SummarySeveral studies have related outcome to the weapon caliber
but none showed statistical significance. Various factors com-plicate the analysis of the effect of caliber on the extent of injuryand outcome. There is a large preponderance of low-caliberinjuries in civilian gunshot wounds of the brain. In civiliangunshot wounds, suicide is a common cause of injury. Thiscause usually represents a close contact type of injury with highinitial velocity of the missile and variable blast effect. Velocityvaries significantly with a given caliber, depending on the cir-cumstances surrounding the injury. The extent of damage isrelated not only to caliber and velocity but to increased tissuedamage that may result from missile fragmentation or a “tum-bling effect” (yaw) resulting from the initial impact.
VI. Evidentiary Table: Caliber of Weapon
Authors, Year Year of Study Description of Study Class Conclusions
Lillard, 197817 1971–1975 Retrospective analysis in 5-y period,describing 83 patients with PBI.
III Mortality increases with caliber of weapon; shotgunwounds are particularly devastating because of blasteffect and widespread tissue disruption.
Caliber Dead Alive.22 18 31.25 2 4.32 7 4.38 4 5
Shotgun 5 3Shoung et al.,
1985201978–1983 Retrospective study on 56 patients
with craniocerebral gunshotwounds.
III Highest mortality (83%) in hunting rifle injuries. Otherwise,no relation to caliber or type of weapon.
Caliber Dead Alive6.35-mm 1 29-mm 2 1.22 6 3.38 1 1
Hunting rifle 5 1Clark et al.,
19864January 1984–
August 1985Retrospective analysis of 76
patients with civiliancraniocerebral gunshot wounds.
III In this series, preponderance of small-caliber injuries(70.9%). Tendency for patients wounded with largercaliber weapons to worse outcome: 78% mortality vs.54.5% in smaller caliber.
Hernesniemi,19795
1968–1977 Retrospective study on 90 patientsadmitted to neurosurgicaldepartment with penetratinggunshot wounds.
III No significant correlation between caliber of weapon andoutcome.
Caliber Unfavorable Favorable Dead Alive.22 22 4 20 6.25 19 0 18 1.32 23 4 20 7.38 9 0 9 0
Shotgun 3 0 2 1Airgun 1 3 1 3
The Journal of TRAUMA� Injury, Infection, and Critical Care
S58 August Supplement 2001

VI. Continued
Authors, Year Year of Study Description of Study Class Conclusions
Aldrich et al.,199210
January 1984–September1987
Prospective study on prognosis in151 patients with civilian gunshotinjuries from the Traumatic ComaData Bank.
I All patients with large-caliber injuries died (n � 4).However, there was no significant relation betweencaliber of weapon and mortality.
Caliber Dead Alive.22–.25 59 7.32–.38 38 6.41–.45 4 0
Nagib et al.,19868
1978–1983 Retrospective study on prognosisand management of civiliangunshot wounds during a 5-yperiod from 1978 to 1983.
III Caliber of bullet does not have prognostic value.
Caliber Unfavorable Favorable Dead Alive.22 21 15 19 19.357 5 4 4 5.38 6 4 6 4
Grahm et al.,19906
Prospective study over an 18-moperiod of 100 patients with civiliangunshot wounds.
II Tendency to higher percentage of unfavorable outcome inlarge caliber injuries.
GOS score at discharge or laterb:Caliber Unfavorable Favorable Dead Alive
.22–.25 18 8 17 9
.32–.38, 9-mm 11 6 11 6
.357 magnum,.44, .45
7 1 6 2
.22 rifle 3 1 3 1Siccardi et al.,
199123Retrospective study of 314
consecutive patients with civiliangunshot wounds, of whom 228died at the scene of the accident.
III The authors state that no statistically significant differencein the mortality rate exists when comparing bullets of acaliber of 7.65 mm or less with heavier missiles.Extracting data presented in the patients wounded withlarger caliber bullets.
Caliber Dead Alive7.65-mm or less 74 13�7.65-mm 22 1
a Indicates that the confidence interval for the odds ratio does not include 1.b Outcome was determined at discharge; among patients who were vegetative or severely disabled at discharge, a mean follow-up of 9 mo
was performed.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S59

SYSTEMIC MEASURES: HYPOTENSIONI. Conclusion
Hypotension is associated with increased mortality(Class III).
II. OverviewHypotension is an important secondary insult after trau-
matic brain injury. Hypotension is defined as a systolic bloodpressure of � 90 mm Hg. In nonpenetrating TBI, hypotensionis frequently observed, both at the scene of the accident33 andat hospital admission.34 In these studies, the occurrence ofhypotension is significantly related to poorer outcome.
Four studies report on the incidence of hypotension incivilian gunshot wounds to the brain.7,10,11,21 Incidences aresummarized in Table 8. The percentage of patients withhypotension at admission varies considerably from 10% to50%. The studies are unclear about how many patients withhypotension at admission were moribund. In the militaryseries of Levi et al.,27 hypotension occurred in 116 patients(19%).
III. Process (Methodology)Among the 43 studies that addressed clinical prognostic
features, 6 (5 civilian, 1 military) described the relation be-tween hypotension in PBI and outcome.
IV. Scientific FoundationIn 480 PBI patients, Kaufman et al.11 report a statistically
significant correlation between occurrence of hypotension
and mortality. In the overall population, mortality was 34%,whereas in the presence of hypotension it was 62%. Twostudies7,13 report higher mortality among patients with hypo-tension, but do not report results of statistical significance.Aldrich et al.,10 analyzing civilian gunshot injuries in 151patients, report a higher mortality among patients with hypo-tension, although statistical significance could not be demon-strated (p � 0.6). Although this paper is a Class I study, itshowed no difference in outcome when comparing those whoexperienced hypotension with those who were normotensivebecause one third of the study’s patients were excluded.Conversely, in the study by Byrnes et al.,13 higher mortalitywas noted among patients with an increased blood pressure atadmission (� 150 mm Hg).
V. SummaryHypotension correlates with increased mortality (Class
III).
VI. Evidentiary Table: Hypotension
Authors, Year Years of Study Description of Study Class Conclusions
Byrnes et al.,197413
August 1969–April 1973
Review article of 93 civilian penetratingcraniocerebral missile injuries in civildisturbances in Northern Ireland.
III Patients with PBI often had a low SBP (�90mm Hg), because of bleeding from scalp,cerebral arteries, or dural sinuses.Hypotension and hypertension (�150mm Hg) are related to poorer outcome; noexact numbers reported.
Dead (%) Alive (%)SBP � 90 mm Hg 72 28SBP 90–150 mm Hg 41 59SBP � 150 mm Hg 93 7
Kaufman et al.,19867
January 1980–June 1982
Descriptive and prognostic (retrospective) studyof 143 patients with civilian gunshot injuries.
III Hypotension (SBP � 90 mm Hg) was noted in71 of 143 patients (50%) and related topoorer outcome.
Dead AliveSBP � 90 mm Hg 55 16SBP � 90 mm Hg 40 32Pprior, 66%; PPV, 77%; OR, 2.75a (n � 143).
Table 8 Incidence of Hypotension in Penetrating BrainInjury
Authors, Year No. Hypotension/Total No.
Percentage WithHypotension
Aldrich et al., 199210 43/103 43Kaufman et al., 19867 71/143 50Kaufman et al., 199511 50/480 10Suddaby et al., 198721 5/49 10
The Journal of TRAUMA� Injury, Infection, and Critical Care
S60 August Supplement 2001

VI. Continued
Authors, Year Years of Study Description of Study Class Conclusions
Kaufman et al.,199511
Two series of patients with civilian gunshotwounds to the brain are described. Emphasisof the study is on patients with admission GCSscores of 3–5. The first series (series A)evaluates treatment results in 190 patientspresenting over a 6-y period to the Universityof Southern California. These patients weresubjected to a conservative approach. Thesecond series (series B) describes 480 patientsadmitted to Cook County Hospital in Chicagofrom 1983 through 1992. Full data are reportedonly on patients with GCS scores of 3–5(n � 146).
III Data on hypotension are given for the secondseries reported in this manuscript. Overallmortality in this series was 34%.Hypotension occurred in 10% of patientsand was related to poorer outcome(mortality 62%), statistically significant (p �0.005).
Dead Alive
SBP � 90 mm Hg 31 19
SBP � 90 mm Hg 132 298
Pprior, 34%; PPV, 62%; OR, 3.68* (n � 480b).
Levi et al.,199027
Retrospective study of 116 patients withpenetrating injury that occurred duringinvolvement of Israeli defense forces inLebanon from June 1982 to June 1985.Essentially same patient population asdescribed under Brandvolt et al.
III Overall mortality in this series was 26%.Hypotension (SBP � 90 mm Hg) was notedin 19% of patients from whom data onblood pressure were available. Mortalityamong patients with hypotension was 67%(12 of 18).
Aldrich et al.,199210
January 1984–September1987
Prospective study on prognosis in 151 patientswith civilian gunshot injuries from the TraumaticComa Data Bank.
I Hypotension was noted in 43% of patients;mortality was higher among patients withhypotension, but differences were notstatistically significant.
Dead AliveSBP � 90 mm Hg 37 7SBP � 90 mm Hg 45 14Pprior, 80%; PPV, 84%; OR, 1.64 (n � 103).
Suddaby et al.,198721
1975–1985 Retrospective analysis of 49 patients with low-velocity gunshot wounds.
III Hypotension (SBP � 90 mm Hg) was seen in5 of 48 patients (10%). Mortality was slightlyhigher in the presence of hypotension, butdifferences were not statistically significant.
Dead Alivec
SBP � 90 mm Hg 4 1SBP � 90 mm Hg 25 18Pprior, 60%; PPV, 80%; OR, 2.88 (n � 48).
SBP, systolic blood pressure; Pprior, prior probability (the outcome distribution in the population studied); PPV, positive predictive value;OR, odds ratio.
a Indicates that the confidence interval for the odds ratio does not include 1.b Data derived from article.c Mistake in original table of the article; date derived by default.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S61
SYSTEMIC MEASURES: COAGULOPATHYI. Conclusion
Coagulopathy is associated with increased mortality, par-ticularly at lower levels of the GCS (Class III).
II. OverviewCoagulopathy may complicate PBI. Coagulation studies
available include prothrombin time, thrombin time, partialthromboplastin time, fibrinogen level, fibrin degradationproducts, and platelet count. Subsequent complications, suchas intracerebral hematoma, may increase mortality.
III. ProcessAmong the 43 studies that addressed clinical prognostic
features, 2 investigated the occurrence of coagulation distur-bances in PBI and its relation to outcome.
IV. Scientific FoundationTwo studies investigated the occurrence of coagulation
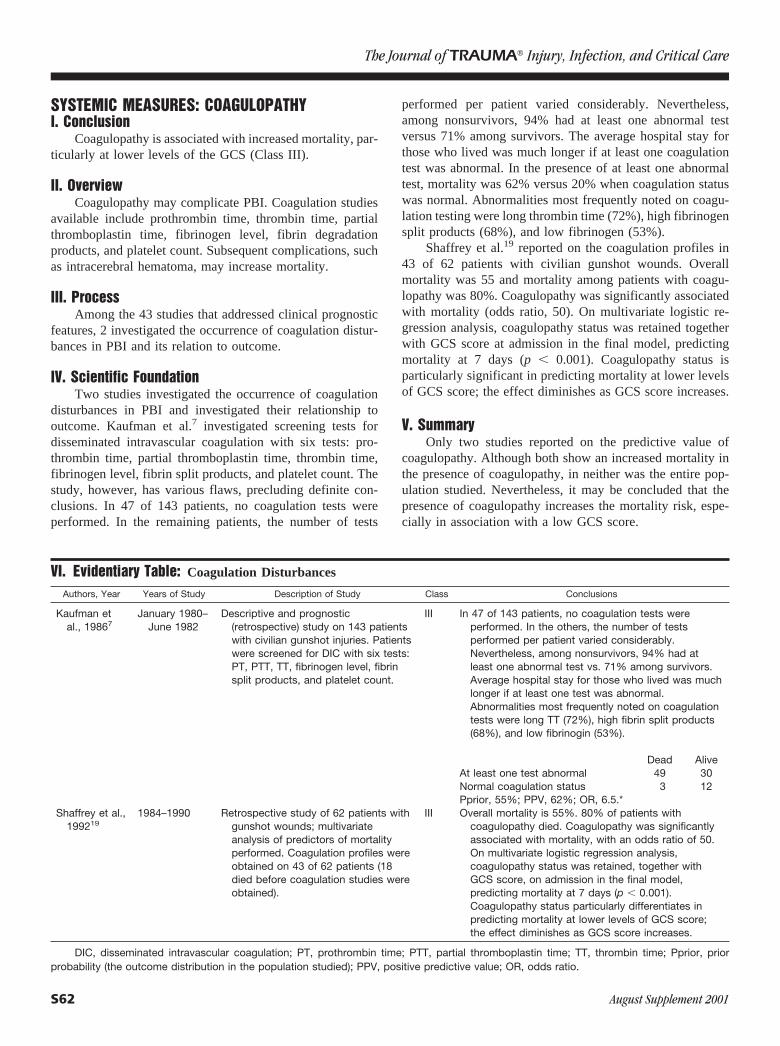
disturbances in PBI and investigated their relationship tooutcome. Kaufman et al.7 investigated screening tests fordisseminated intravascular coagulation with six tests: pro-thrombin time, partial thromboplastin time, thrombin time,fibrinogen level, fibrin split products, and platelet count. Thestudy, however, has various flaws, precluding definite con-clusions. In 47 of 143 patients, no coagulation tests wereperformed. In the remaining patients, the number of tests
performed per patient varied considerably. Nevertheless,among nonsurvivors, 94% had at least one abnormal testversus 71% among survivors. The average hospital stay forthose who lived was much longer if at least one coagulationtest was abnormal. In the presence of at least one abnormaltest, mortality was 62% versus 20% when coagulation statuswas normal. Abnormalities most frequently noted on coagu-lation testing were long thrombin time (72%), high fibrinogensplit products (68%), and low fibrinogen (53%).
Shaffrey et al.19 reported on the coagulation profiles in43 of 62 patients with civilian gunshot wounds. Overallmortality was 55 and mortality among patients with coagu-lopathy was 80%. Coagulopathy was significantly associatedwith mortality (odds ratio, 50). On multivariate logistic re-gression analysis, coagulopathy status was retained togetherwith GCS score at admission in the final model, predictingmortality at 7 days (p � 0.001). Coagulopathy status isparticularly significant in predicting mortality at lower levelsof GCS score; the effect diminishes as GCS score increases.
V. SummaryOnly two studies reported on the predictive value of
coagulopathy. Although both show an increased mortality inthe presence of coagulopathy, in neither was the entire pop-ulation studied. Nevertheless, it may be concluded that thepresence of coagulopathy increases the mortality risk, espe-cially in association with a low GCS score.
VI. Evidentiary Table: Coagulation Disturbances
Authors, Year Years of Study Description of Study Class Conclusions
Kaufman etal., 19867
January 1980–June 1982
Descriptive and prognostic(retrospective) study on 143 patientswith civilian gunshot injuries. Patientswere screened for DIC with six tests:PT, PTT, TT, fibrinogen level, fibrinsplit products, and platelet count.
III In 47 of 143 patients, no coagulation tests wereperformed. In the others, the number of testsperformed per patient varied considerably.Nevertheless, among nonsurvivors, 94% had atleast one abnormal test vs. 71% among survivors.Average hospital stay for those who lived was muchlonger if at least one test was abnormal.Abnormalities most frequently noted on coagulationtests were long TT (72%), high fibrin split products(68%), and low fibrinogin (53%).
Dead AliveAt least one test abnormal 49 30Normal coagulation status 3 12Pprior, 55%; PPV, 62%; OR, 6.5.*
Shaffrey et al.,199219
1984–1990 Retrospective study of 62 patients withgunshot wounds; multivariateanalysis of predictors of mortalityperformed. Coagulation profiles wereobtained on 43 of 62 patients (18died before coagulation studies wereobtained).
III Overall mortality is 55%. 80% of patients withcoagulopathy died. Coagulopathy was significantlyassociated with mortality, with an odds ratio of 50.On multivariate logistic regression analysis,coagulopathy status was retained, together withGCS score, on admission in the final model,predicting mortality at 7 days (p � 0.001).Coagulopathy status particularly differentiates inpredicting mortality at lower levels of GCS score;the effect diminishes as GCS score increases.
DIC, disseminated intravascular coagulation; PT, prothrombin time; PTT, partial thromboplastin time; TT, thrombin time; Pprior, priorprobability (the outcome distribution in the population studied); PPV, positive predictive value; OR, odds ratio.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S62 August Supplement 2001
SYSTEMIC MEASURES: RESPIRATORY DISTRESSI. Conclusion
Respiratory distress is associated with increased mortal-ity in PBI (Class III).
II. OverviewRespiratory distress is variously defined in the PBI litera-
ture as a respiratory rate of less than 10, apnea, or respiratorydepression; however, studies do not contain a clear and consis-tent definition for respiratory distress. A significant number ofpatients arrive at hospital already intubated, and the reasons forintubation in the field are often difficult to ascertain. For thepurpose of this section, we have chosen a respiratory rate of lessthan 10 breaths/min or impairment of the patient’s airway re-lated to a level of coma that required intubation as the criteria forour definition of respiratory distress.
III. Process (Methodology)Among the 43 studies that address clinical prognostic
features, 2 were found to contain significant data regardingthe relation between respiratory distress and outcome.
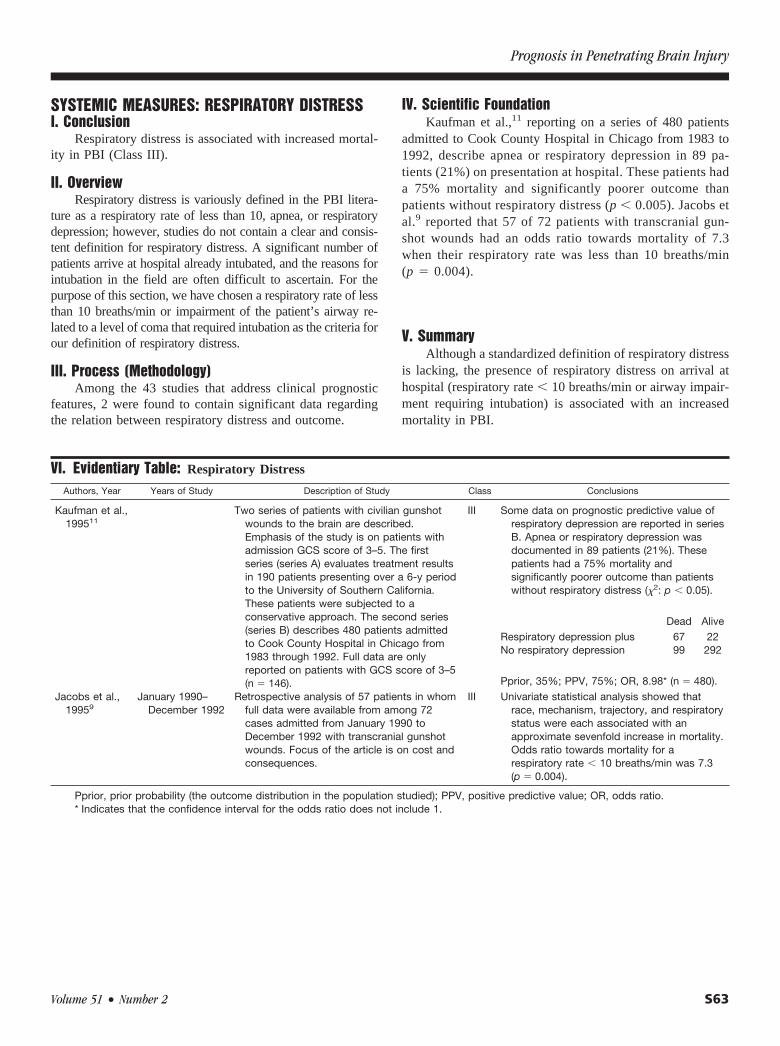
IV. Scientific FoundationKaufman et al.,11 reporting on a series of 480 patients
admitted to Cook County Hospital in Chicago from 1983 to1992, describe apnea or respiratory depression in 89 pa-tients (21%) on presentation at hospital. These patients hada 75% mortality and significantly poorer outcome thanpatients without respiratory distress (p � 0.005). Jacobs etal.9 reported that 57 of 72 patients with transcranial gun-shot wounds had an odds ratio towards mortality of 7.3when their respiratory rate was less than 10 breaths/min(p � 0.004).
V. SummaryAlthough a standardized definition of respiratory distress
is lacking, the presence of respiratory distress on arrival athospital (respiratory rate � 10 breaths/min or airway impair-ment requiring intubation) is associated with an increasedmortality in PBI.
VI. Evidentiary Table: Respiratory Distress
Authors, Year Years of Study Description of Study Class Conclusions
Kaufman et al.,199511
Two series of patients with civilian gunshotwounds to the brain are described.Emphasis of the study is on patients withadmission GCS score of 3–5. The firstseries (series A) evaluates treatment resultsin 190 patients presenting over a 6-y periodto the University of Southern California.These patients were subjected to aconservative approach. The second series(series B) describes 480 patients admittedto Cook County Hospital in Chicago from1983 through 1992. Full data are onlyreported on patients with GCS score of 3–5(n � 146).
III Some data on prognostic predictive value ofrespiratory depression are reported in seriesB. Apnea or respiratory depression wasdocumented in 89 patients (21%). Thesepatients had a 75% mortality andsignificantly poorer outcome than patientswithout respiratory distress (�2: p � 0.05).
Dead Alive
Respiratory depression plusNo respiratory depression
6799
22292
Pprior, 35%; PPV, 75%; OR, 8.98* (n � 480).
Jacobs et al.,19959
January 1990–December 1992
Retrospective analysis of 57 patients in whomfull data were available from among 72cases admitted from January 1990 toDecember 1992 with transcranial gunshotwounds. Focus of the article is on cost andconsequences.
III Univariate statistical analysis showed thatrace, mechanism, trajectory, and respiratorystatus were each associated with anapproximate sevenfold increase in mortality.Odds ratio towards mortality for arespiratory rate � 10 breaths/min was 7.3(p � 0.004).
Pprior, prior probability (the outcome distribution in the population studied); PPV, positive predictive value; OR, odds ratio.* Indicates that the confidence interval for the odds ratio does not include 1.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S63

NEUROLOGIC MEASURES: LEVEL OFCONSCIOUSNESS AND GLASGOW COMA SCALEI. Conclusions
In civilian patients, low GCS correlates with higher mor-tality and unfavorable outcome (Class I). In military injuries,fewer patients have a low GCS score. A strong correlationalso exists between low GCS score and unfavorable outcomein military series (Class III).
II. OverviewSince the introduction of the GCS in 1974 by Teasdale
and Jennett,35 this score has become widely accepted as anobjective measure of level of consciousness. Prior to thistime, various grading systems, often ill defined, were usedacross the world. In published reports on PBI before 1975,most authors distinguish four grades of consciousness: alert,drowsy, purposeful reaction to pain, and deep coma. In non-penetrating TBI, patients with a GCS score � 8 are classifiedas having severe injuries, and patients with GCS scores of 9of 12 are classified as moderate. Several studies focusedspecifically on those with severe injuries.10,11 The distribu-tions of the level of consciousness observed in the seriesreported are shown in Tables 9 and 10.
In civilian series, some variation in the severity of injuryexists, probably reflecting different admission referral poli-cies. All series are characterized by the relatively high num-ber of patients in grade 4 (approximately 35%) or with a GCSscore of 3 to 5 (38–61%) in unselected series. Few patientsare included with a GCS score of 6 to 8; the percentage ofpatients who may be considered in coma is 53% to 57%, andthe percentage of patients with a GCS score � 8 is 37% to70%. The percentage of patients with milder injuries (GCSscore of 13–15) in various series ranges from 15% to 51%. Inthe series reported by Kennedy et al.,15 51% of patients hada GCS score of 14 to 15.
The incidence of various categories of GCS score re-ported in military series is different from civilian series. Thepercentage of patients with GCS score of 3 to 5 is lower (11%and 35%) and the percentage of patients with GCS score of13 to 15 is higher (63% and 45%).
No results of interobserver reliability in the use of GCSin PBI have been reported, but there is no reason to supposethat results might be different from those observed in non-penetrating TBI. Some studies in nonpenetrating TBI dem-onstrated a high intra- and interobserver reliability in the use
of GCS, and also when applied by medical personnel withlimited experience.36–39 However, a study by Marion et al.40
suggested considerable variability in how the GCS score wasassessed. Furthermore, the use of paralytic agents and drugsor alcohol can significantly compromise the reliability of theGCS.
III. Process (Methodology)Among the 43 studies that addressed clinical prognostic
features, 8 report on the relation between level of conscious-ness and outcome in the civilian setting, 11 on relation be-tween GCS score at admission and outcome, and 4 on therelation between level of consciousness or GCS score andoutcome in military injuries.
IV. Scientific FoundationCivilian Series
All civilian studies reporting on level of consciousness orGCS score in PBI show a strong correlation between GCSscore and outcome. Mortality among patients in deep coma isuniformly high, and a mortality of 100% is reported in threeseries. In the civilian series that report both GCS and GOS,only 5 of 490 patients with GCS score of 3 to 5 had afavorable outcome. Among patients alert at hospital admis-sion, mortality is low (0–10%), and among patients with GCSscore of 13 to 15, mortality and unfavorable outcome was0%. Prognosis for patients in a coma (GCS score � 8) aresummarized in Tables 1113,14,17,20,41 and 12.6–8,25,18,26
Military SeriesAs in civilian injuries, the three military studies reporting
on GCS score and outcome in PBI show a strong correlationbetween GCS score and outcome. Both in the Iranian series25
and in the Israeli series26, a positive predictive value of 61%was calculated among patients with a GCS score � 8. Among
Table 9 Level of Consciousness in Penetrating BrainInjury
Byrnes, 1974 (n � 89)Byrnes et al., 197413
(n � 89)
Hubschmann etal., 197914
(n � 82)
Shoung etal., 198520
(n � 56)
Alert (%) 29 29 27Drowsy (%) 20 26 20Reacts to pain (%) 27 10 25Deep coma (%) 28 48 29
Table 10 GCS Score in Penetrating Brain Injury
GCS Score Aldrich et al., 199210
(n � 151)Grahm et al.,
19906 (n � 100)Kaufman et al.,19867 (n � 141)
Mancuso etal., 198818
(n � 40)
Nagib et al., 19868
(n � 55)
3–5 (%) 81 58 61 38 536–8 (%) 13 8 15 10 169–12 (%) 5 12 9 28 3113–15 (%) 22 15 25
The Journal of TRAUMA� Injury, Infection, and Critical Care
S64 August Supplement 2001

patients with a GCS score of 13 to 15, a positive predictivevalue to survival was calculated as 97% and 94%. The resultsof the study reported by Aarabi25 should, however, be inter-preted with care because it concerns a selected series ofpatients with a mean admission time of 49 hours after injury(range, 7–450 hours), which is different from most civilianseries.
V. SummaryIn civilian series, large proportions of patients are admit-
ted with a GCS score of 3 to 5. However, in military series,fewer patients have a low admission GCS score, and morehave a GCS score of 13 to 15. Nevertheless, in both civilianand military PBI, the level of consciousness as assessed bythe GCS is the strongest indicator of outcome and mortality.
VI. Evidentiary Table: Level of Consciousness
Authors, Year Year of Study Description of Study Class Conclusions
Byrnes et al.,197413
August 1969–April 1973
Review study of 93 civilianpenetrating craniocerebralmissile injuries in civildisturbances in NorthernIreland.
III Features related to outcome (dead/alive):hypotension, level of consciousness, pupilreactivity.
Dead AliveAlert 3 23Drowsy/irritable 6 12Only reacts to pain 19 5Deep Coma 25 0
Dead AliveComa� 44 5Coma– 9 35Pprior, 57%; PPV, 88%; OR, 34.2a (n � 93).
Table 11 Level of Consciousness: Predictive Value of Coma to Mortality
Authors, Year Years of Study Predictionof
Mortality ofSeries
Mortality(Deep Coma) Odds Ratio
Byrnes et al., 197413 August 1969–April 1973 Mortality 0.57 0.88 34.2Carey et al., 197241 September 1968–September 1969 Mortality 0.12 0.28 5.83Hubschmann et al., 197914 1973–1975 Mortality 0.57 0.91 114.6Lillard, 197817 1971–1975 Mortality 0.43 0.80 20Shoung et al., 198520 1978–1983 Mortality 0.45 0.83 21
Table 12 GCS Score versus Outcome: Analysis of GCS Score < 8 versus GCS Score > 9
Authors, Year Years ofStudy Prediction of Mortality of
SeriesMortality
(GCS Score � 8) Odds Ratio
Arabi, 199025 1981–1988 Unfavorable outcome 0.21 0.61 20.66Mortality 0.16 0.51 18.07
Brandvold et al., 199026 1982–1985 Unfavorable outcome 0.37 0.77 32.7Mortality 0.28 0.61 24.97
Grahm et al., 19906 ? Unfavorable outcome 0.68 0.94 240Mortality 0.59 0.85 57.8
Kaufman et al., 19867 1980–1982 Mortality 0.66 0.87 219Mancuso et al., 198818 1969–1986 Mortality 0.40 0.84 112a
Nagib et al., 19868 1978–1983 Unfavorable outcome 0.58 0.79 28.1Mortality 0.51 .073 47.6a
a 0 set to 1 calculation.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S65
VI. Continued
Authors, Year Year of Study Description of Study Class Conclusions
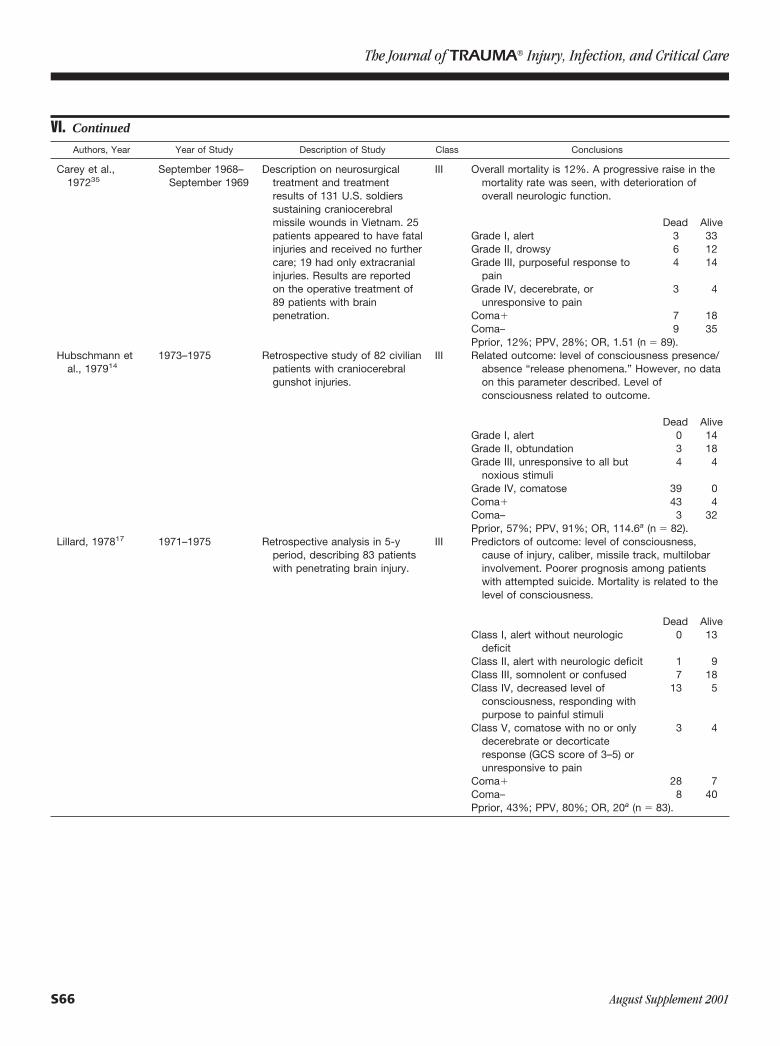
Carey et al.,197235
September 1968–September 1969
Description on neurosurgicaltreatment and treatmentresults of 131 U.S. soldierssustaining craniocerebralmissile wounds in Vietnam. 25patients appeared to have fatalinjuries and received no furthercare; 19 had only extracranialinjuries. Results are reportedon the operative treatment of89 patients with brainpenetration.
III Overall mortality is 12%. A progressive raise in themortality rate was seen, with deterioration ofoverall neurologic function.
Dead AliveGrade I, alert 3 33Grade II, drowsy 6 12Grade III, purposeful response to
pain4 14
Grade IV, decerebrate, orunresponsive to pain
3 4
Coma� 7 18Coma– 9 35Pprior, 12%; PPV, 28%; OR, 1.51 (n � 89).
Hubschmann etal., 197914
1973–1975 Retrospective study of 82 civilianpatients with craniocerebralgunshot injuries.
III Related outcome: level of consciousness presence/absence “release phenomena.” However, no dataon this parameter described. Level ofconsciousness related to outcome.
Dead AliveGrade I, alert 0 14Grade II, obtundation 3 18Grade III, unresponsive to all but
noxious stimuli4 4
Grade IV, comatose 39 0Coma� 43 4Coma– 3 32Pprior, 57%; PPV, 91%; OR, 114.6a (n � 82).
Lillard, 197817 1971–1975 Retrospective analysis in 5-yperiod, describing 83 patientswith penetrating brain injury.
III Predictors of outcome: level of consciousness,cause of injury, caliber, missile track, multilobarinvolvement. Poorer prognosis among patientswith attempted suicide. Mortality is related to thelevel of consciousness.
Dead AliveClass I, alert without neurologic
deficit0 13
Class II, alert with neurologic deficit 1 9Class III, somnolent or confused 7 18Class IV, decreased level of
consciousness, responding withpurpose to painful stimuli
13 5
Class V, comatose with no or onlydecerebrate or decorticateresponse (GCS score of 3–5) orunresponsive to pain
3 4
Coma� 28 7Coma– 8 40Pprior, 43%; PPV, 80%; OR, 20a (n � 83).
The Journal of TRAUMA� Injury, Infection, and Critical Care
S66 August Supplement 2001

VI. Continued
Authors, Year Year of Study Description of Study Class Conclusions
Shoung et al.,198520
1978–1983 Retrospective study on 56patients with craniocerebralgunshot wounds.
Level of consciousness related to mortality.
Dead AliveGrade I, alert, no neurologic deficit 2 13Grade II, drowsy 3 8Grade III, coma 9 5Grade IV, deep coma with brain stem
clinical impairment16 0
Coma� 25 5Coma– 5 21Pprior, 45%; PPV, 83%; OR, 21a (n � 56).
Hernesniemi,19795
1968–1977 Retrospective study on 90patients admitted toneurosurgical department withpenetrating gunshot wounds.
III Related to outcome are level of consciousness andmissile tract.
GOS variable, long term:Unfavorable (Dead) Favorable
5 Alive Alert10 3
Pprior, prior probability (the outcome distribution in the population studied); PPV, positive predictive value; OR, odds ratio.a Indicates that the confidence interval for the odds ratio does not include 1.
VII. Evidentiary Table: GCS Score At Admission
Authors, Year Years of Study Description of Study Class Conclusions
Arabi, 199025 February 1981–August 1988
Analysis of outcome in 435patients in whom full datawere available from a series of690 patients with missile headwounds, sustained during theIran-Iraq War, evacuated toNemazee hospital in Shiraz.
III GCS score at admission is related to outcome (GOS) and focalneurologic deficit. Selected series of patients with a meanadmission time of 49 h after injury (range, 7–450 h).
Mortality: GOS score at 6 mo or more:
Admission GCS score Dead Alive Unfavorable Favorable3–5 27 19 30 166–8 26 32 33 259–12 10 47 14 43
13–15 8 266 16 258Probability analysis GCS score � 8 vs. GCS score � 8.Unfavorable outcome: Pprior, 21%; PPV, 62%; OR, 16.15.a
Mortality: Pprior, 16%; PPV, 51%; OR, 18.07.a
Aldrich et al.,199210
January 1984–September 1987
Prospective study on prognosisamong 151 patients withcivilian gunshot injuries fromthe Traumatic Coma DataBank.
I Overall mortality 88%. Related to outcome: GCS score atadmission. GCS score after resuscitation and intensive care.
Admissions GCS score Dead Alive GOS score at discharge:
Unfavorable Favorable3–5 116 7 122 16–8 14 5 18 29–15 3 5 6 2
No probability analysis performed because patient populationstudied included only patients with GCS score � 8 ordeterioration to that level within 48 h of injury.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S67

VII. Continued
Authors, Year Years of Study Description of Study Class Conclusions
Brandvold etal., 199026
1982–June 1985 Retrospective analysis of 113patients evacuated toRambam Maimonides MedicalCenter with penetratingcraniocerebral injuriessustained in ongoing militaryhostilities in Lebanon.
III Prognostic features related to outcome: mechanism of injury, GCSscore, hypotension, CT scan characteristics, and infection.Mortality in GCS score of 2–4 is 80%, GCS score of 5–12 is 12%,GCS score of 13–15 is 6%.
GCS score: GOS score at discharge:
Unfavorable Favorable3–5 33 66–8 3 59–12 2 13
13–15 4 47Probability analysis GCS score � 8 vs. GCS score � 8.Pprior, 37%; PPV, 77%; OR, 32.7.a
Mortality:
GCS score: Dead Alive3–5 27 126–8 2 69–12 1 14
13–15 3 48Probability analysis GCS score � 8 vs. GCS score � 8.
Pprior, 28%; PPV, 62%; OR, 24.97.a
Clark et al.,19864
January 1984–August 1985
Retrospective analysis of 76patients with civiliancraniocerebral gunshotwounds.
III Overall mortality 62%. Suicide more common in Caucasian males;homicide in blacks. No patients with an admission GCS score of 3survived. Prognostic variables are GCS score, ventricular injury,bihemispheric wounds. Admission GCS score is lower amongpatients with poor outcome (3.68 � 1.3) in comparison withpatients with good outcome (9.48 � 3.2). The difference isstatistically significant (p � 0.001). No exact data reported.
Grahm et al.,19906
Not specified Prospective study over an 18-moperiod of 100 patients withcivilian gunshot wounds.
II 58% of patients had an admission GCS score of 3–5; 8%, 6–8;12%, 9–12; and 22%, 13–15. Lower GCS score is associated withpoorer prognosis. A relation was described between theadmission GCS score and abnormalities in pupillary reactivity and/or oculocephalic eye movements.
GCS score GOS discharge or laterb
Unfavorable Favorable3–5 58 06–8 6 29–12 4 8
13–15 0 22Probability analysis GCS score � 8 vs. GCS score � 8.Pprior, 68%; PPV, 97%; OR, 240.a
Mortality:
GCS score Dead Alive3–5 54 46–8 2 69–12 3 9
13–15 0 22Pprior, 59%; PPV, 85%; OR, 57.9.a
The Journal of TRAUMA� Injury, Infection, and Critical Care
S68 August Supplement 2001

VII. Continued
Authors, Year Years of Study Description of Study Class Conclusions
Kaufman etal., 19867
January 1980–June 1982
Descriptive and prognostic(retrospective) study of 143patients with civilian gunshotinjuries.
III Overall mortality is 66%. Low GCS score is related to pooroutcome, but a few unexpected recoveries are described amongpatients in whom a large debridement was performed.
GCS score Dead Alive3–5 83 36–8 10 119–11 1 12
12–15 0 21Probability analysis GCS score � 8 vs. GCS score � 8.Pprior, 66%; PPV, 87%; OR, 219.a
Kaufman etal., 199511
Two series of patients withcivilian gunshot wounds to thebrain are described. Emphasisof the study is on patients withadmission GCS score of 3–5.The first series (series A)evaluates treatment results in190 patients presenting over a6-y period to the University ofSouthern California. Thesepatients were subjected to aconservative approach. Thesecond series (series B)describes 480 patientsadmitted to Cook CountyHospital in Chicago from 1983through 1992. Full data arereported only on patients withGCS score of 3–5 (n � 146).
III Logistic regression analysis performed on series A shows admissionGCS score, TSAH, pupils to be predictive of mortality. Predictiveof morbidity are GCS score, bihemispheric injury, diffusefragmentation.
Mortality: GOS score at discharge:
GCS score Dead Alive Unfavorable Favorable3 101 5 106 04 55 7 61 15 10 12 21 1
Logistic regression analysis on series B showed relation to outcomeof GCS score, bihemispheric injury, pupil reactivity, and TSAH.
Mortality: GOS score at discharge:
GOS score at discharge Dead Alive Unfavorable Favorable3 102 4 104 24 24 6 30 05 9 1 10 0
No probability analysis performed because series includes onlypatients with GCS score of 3–5.
Kennedy etal., 199315
January 1987–June 1990
Retrospective analysis ofprognostic features among192 patients with gunshot andshotgun injuries.
III Related to outcome: GCS score, brain extrusion, but interaction withGCS score, CT scan: single-lobe injury better than multiple-lobeinjuries.
Levi et al.,199027
June 1982–June 1985
Retrospective study of 116patients with penetratinginjury; occurred duringinvolvement of Israeli defenseforces in Lebanon.
III Related to outcome: GCS score, mechanism of injury, intracerebraltrack, multilobar injury, transventricular injury, and hypotension.
Mancuso etal., 198818
1969–1986 Retrospective study of 40patients with craniocerebralgunshot wounds. Mainlydescriptive study.
III Poor outcome among patients with GCS score � 8.GCS score Dead Alive
�8 16 3�8 0 21
Pprior, 40%; PPV, 84%; OR, 112a,c
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S69

VII. Continued
Authors, Year Years of Study Description of Study Class Conclusions
Nagib et al.,19868
1978–1983 Retrospective study of prognosisand management of civiliangunshot wounds during a 5-yperiod from 1978 to 1983.
III Related to poorer outcome: suicide, level of consciousness,multilobar unilateral injury, bilateral injury.
GCS score GOS score at 1 y:
Unfavorable Favorable3–5 28 16–8 2 79–15 2 15
Probability analysis GCS score � 8 vs. GCS score � 8.Pprior, 58%; PPV, 79%; OR, 28.1.a
Mortality:
GCS score Dead Alive3–5 26 36–8 2 79–15 0 17
Pprior, 51%; PPV, 74%; OR, 47.6.a,c
Shaffrey etal., 199219
1984–1990 Retrospective study of 62patients with gunshot wounds;multivariate analysis ofpredictors of mortality isperformed.
III Overall mortality is 55%. In GCS score of 3, 87.5%; GCS score of4–7, 56.3%; GCS score � 7, 0%. Multivariate logistic regressionanalysis of clinical variables shows GCS score at admission pluscoagulopathy status to be the best predictor of mortality at 7days. Coagulopathy status makes a difference in predictedmortality at lower levels of GCS score, but its value diminishes asGCS score increases. CT scan parameters retained in the step-uplogistic regression procedure are volume of contused brain andcrossing of horizontal or sagittal plane. The odds ratio foradmission GCS score of 3 to mortality is 266; for admission GCSscore of 4–7, 49.
Suddaby etal., 198721
1975–1985 Retrospective analysis of 49patients with low-velocitygunshot wounds.
III 85% were suicide cases. Overall mortality 61%. Related to poorerprognosis: GCS score � 7 and nonreactive pupils.
Mortality: GOS score at discharge:
GCS scale Dead Alive Unfavorable Favorable�7 28 4 29 4�8 2 14 2 14
Jacobs et al.,19959
January 1990–December 1992
Retrospective analysis of 57patients in whom fill data wereavailable from 72 casesadmitted from January 1990 toDecember 1992 withtranscranial gunshot wounds.Focus of the study is on costand consequences.
III Relation to mortality of Caucasian race, GCS score � 4, lateraltrajectory. Odds ratio to unfavorable outcome in GCS score � 4 is33.7 (p � 0.003).
Pprior, prior probability (the outcome distribution in the population studied); PPV, positive predictive value; OR, odds ratio; TSAH, traumaticsubarachnoid hemorrhage.
a Indicates that the confidence interval for the odds ratio does not include 1.b Outcome was determined at discharge; among patients vegetative or severely disabled at discharge a mean follow-up of 9 mo was
performed.c 0 set to 1 for calculation.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S70 August Supplement 2001

NEUROLOGIC MEASURES: PUPILLARY SIZE ANDLIGHT REFLEXI. Conclusion
The presence of bilateral fixed and dilated pupils ishighly predictive of mortality (Class III).
II. OverviewAn abnormal pupillary light reflex may be an indirect
indicator of cerebral herniation or possible brain stem injury.Other causes of an abnormal pupillary response include directorbital trauma. Measurement of pupillary reactivity includesmeasurement of the light reflex and size of the pupils. Anoverview of the incidence of pupillary abnormalities in seriesof patients with penetrating brain injury is given in Table 13.
The series are characterized by a high percentage of patientswith fixed and dilated pupils. In the PBI literature, no studieshave been conducted that examine the interobserver or intraob-server reliability on scoring of pupillary light reflex and sizeequality of pupils. A high interobserver reliability has beenreported in the assessment of ocular signs in coma.42 In non-penetrating TBI, a relation between absence of pupillary reac-tivity and obliteration of the basal cisterns, as documented by CTscan investigation, has been demonstrated.43,44 Other authorsreporting on nonpenetrating TBI show an association of pupil-lary reactivity with the GCS score,45,46 focal lesions,46 and ahistory of early hypoxic or hypotensive insults.47 Among pa-tients with PBI, Byrnes et al.13 describe a relation betweenpupillary reactivity/size and level of consciousness. Similarly,
Grahm et al.6 report a relation between ocular signs and GCSscore (Table 14).
III. Process (Methodology)Among the 43 studies that address clinical prognostic
features, 5 report on the prognostic value of pupillary reac-tivity/size in PBI, all in civilian injuries.
IV. Scientific FoundationClinical studies investigating the prognostic value of
pupillary light reactions have examined this parameter usingvarious methodologies. No study of PBI has rigorously mea-sured the pupil size and reactivity; none give exact definitionsof pupillary inequality. Five studies report on the prognosticvalue of pupillary reactivity/size in PBI. All authors describea relation between absence of pupillary reactivity and mor-tality. Kaufman et al.,7 studying 143 patients, and Shaffrey etal.,19 in a retrospective study of 62 patients, show a strongrelation between unreactive pupils and outcome (odds ratio,44–184 for mortality in the presence of nonreactive pupils).Neither Suddaby et al.21 nor Byrnes et al.13 could demon-strate a statistically significant relation between inequality ofpupils and outcome.
V. SummaryAlthough standardized definitions are lacking, the inci-
dence of pupillary abnormalities ranges between one thirdand one half of patients admitted with PBI. Pupillary abnor-malities appear to correlate with a patient’s level of con-sciousness. Unequal or fixed and dilated pupils correlate withincreased mortality.
VI. Evidentiary Table: Pupillary Examination
Authors, Year Years of Study Description of Study Class Conclusions
Byrnes et al.,197413
August 1969–April 1973
Review of study of 93 civilians withpenetrating craniocerebral missileinjuries in civil disturbances in NorthernIreland.
III Pupillary reactivity is related to the level ofconsciousness and mortality. No multivariateanalysis was performed to determine therelative importance of pupillary reactivity vs.level of consciousness.
Pupillary reactivity/size:Dead Alive
Fixed, dilated 24 1Unequal 8 13Normal 16 31Probability analysis: nonreacting vs. one or both
reacting.Pprior, 52%; PPV, 96%; OR, 44.a
Table 13 Distribution Pupils in Penetrating BrainInjury
Byrnes et al.,197413 (%)
Series B, Kaufmanet al., 199511 (%)
Suddaby et al.,198721 (%)
Normal 50 61 53Unequal 23 9Fixed dilated 27 30 47
Table 14 Pupillary Reactivity/Size and GCS Score
Alert Drowsy Reacts to pain Deep coma
Normal 24 11 7 5Unequal 2 5 10 4Fixed, dilated 0 2 7 16
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S71
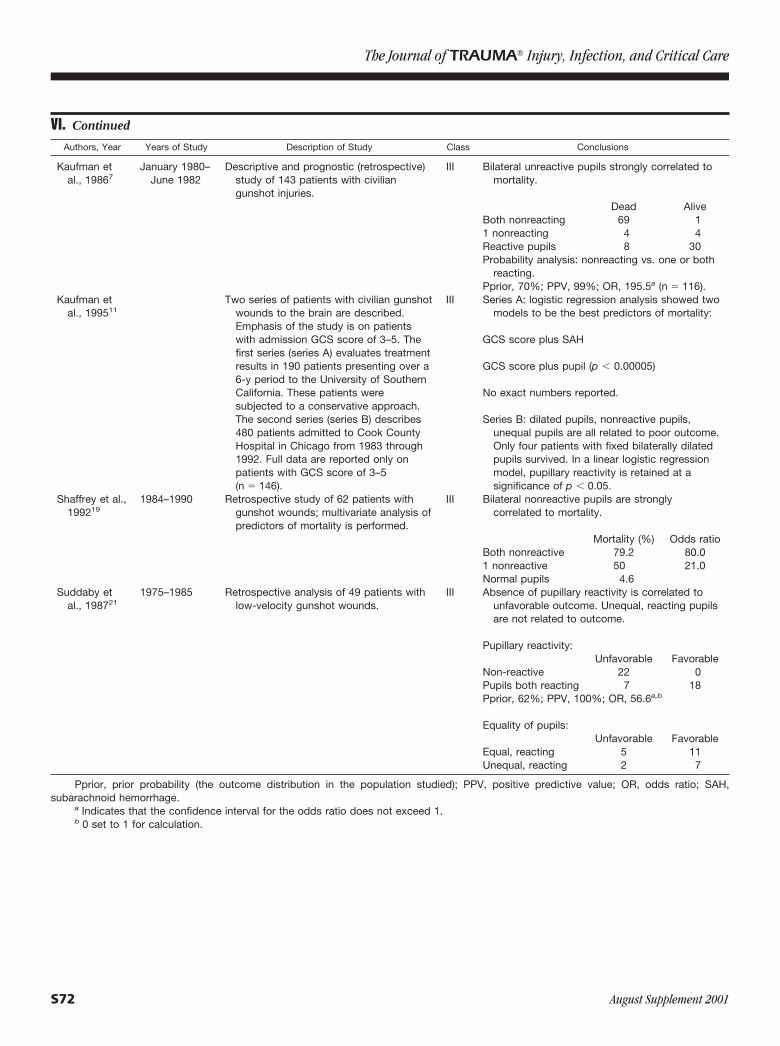
VI. Continued
Authors, Year Years of Study Description of Study Class Conclusions
Kaufman etal., 19867
January 1980–June 1982
Descriptive and prognostic (retrospective)study of 143 patients with civiliangunshot injuries.
III Bilateral unreactive pupils strongly correlated tomortality.
Dead AliveBoth nonreacting 69 11 nonreacting 4 4Reactive pupils 8 30Probability analysis: nonreacting vs. one or both
reacting.Pprior, 70%; PPV, 99%; OR, 195.5a (n � 116).
Kaufman etal., 199511
Two series of patients with civilian gunshotwounds to the brain are described.Emphasis of the study is on patientswith admission GCS score of 3–5. Thefirst series (series A) evaluates treatmentresults in 190 patients presenting over a6-y period to the University of SouthernCalifornia. These patients weresubjected to a conservative approach.The second series (series B) describes480 patients admitted to Cook CountyHospital in Chicago from 1983 through1992. Full data are reported only onpatients with GCS score of 3–5(n � 146).
III Series A: logistic regression analysis showed twomodels to be the best predictors of mortality:
GCS score plus SAH
GCS score plus pupil (p � 0.00005)
No exact numbers reported.
Series B: dilated pupils, nonreactive pupils,unequal pupils are all related to poor outcome.Only four patients with fixed bilaterally dilatedpupils survived. In a linear logistic regressionmodel, pupillary reactivity is retained at asignificance of p � 0.05.
Shaffrey et al.,199219
1984–1990 Retrospective study of 62 patients withgunshot wounds; multivariate analysis ofpredictors of mortality is performed.
III Bilateral nonreactive pupils are stronglycorrelated to mortality.
Mortality (%) Odds ratioBoth nonreactive 79.2 80.01 nonreactive 50 21.0Normal pupils 4.6
Suddaby etal., 198721
1975–1985 Retrospective analysis of 49 patients withlow-velocity gunshot wounds.
III Absence of pupillary reactivity is correlated tounfavorable outcome. Unequal, reacting pupilsare not related to outcome.
Pupillary reactivity:Unfavorable Favorable
Non-reactive 22 0Pupils both reacting 7 18Pprior, 62%; PPV, 100%; OR, 56.6a,b
Equality of pupils:Unfavorable Favorable
Equal, reacting 5 11Unequal, reacting 2 7
Pprior, prior probability (the outcome distribution in the population studied); PPV, positive predictive value; OR, odds ratio; SAH,subarachnoid hemorrhage.
a Indicates that the confidence interval for the odds ratio does not exceed 1.b 0 set to 1 for calculation.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S72 August Supplement 2001
NEUROLOGIC MEASURES: INTRACRANIALPRESSUREI. Conclusion
High ICP is predictive of higher mortality (Class II).
II. OverviewBrain injury, whether from a closed or penetrating brain
injury, is associated with increased ICP. Monitoring ICP canbe performed using intracranial pressure monitors (intrapa-renchymal or subdural) or ventriculostomy. ICP values areused not only to treat elevated ICP primarily but also inconjunction with the mean arterial pressure, to maximizecerebral perfusion pressure. Most reports give incidental in-formation regarding ICP and outcome7,13 and the frequencyof ICP monitoring is low in PBI. In the studies by Kaufmanet al.7 and Aldrich et al.,10 only 14% and 23% of patients,respectively, received ICP monitoring.
III. Process (Methodology)Among the 43 articles addressing clinical prognostic
features, 1 study reported on the prognostic value of ICP
monitoring and 1 other mentioned the use of ICP monitoringbut did not report its prognostic value.
IV. Scientific FoundationOnly a few studies report on experience with intracranial
pressure monitoring among patients with penetrating braininjury. Aldrich et al.10 found the average ICP during the first72 hours among patients who died was 62 mm Hg versus 31mm Hg in those who survived. The percentage of time thatthe ICP was � 20 mm Hg in the first 72 hours was likewisesubstantially higher in the group that died (75% vs. 26%).Linear regression analysis showed that high ICP was thesecond most important predictor of mortality.
V. SummaryFew reports provide data relating ICP and outcome.
Although there are a number of methods for reporting ICP,available data suggest that elevated ICP within the first 72hours predicts higher mortality.
VI. Evidentiary Table: Intracranial Pressure
Authors, Year Years of Study Description of Study Class Conclusions
Aldrich et al., 199210 January 1984–September 1987
Prospective study on prognosis in 151patients with civilian gunshot injuries fromthe Traumatic Coma Data Bank.
II ICP was monitored in 35 patients; high ICPwas associated with high mortality. AverageICP among patients dying during the first 72h was 62 mm Hg vs. 31 mm Hg insurvivors. Percentage of time that ICP wasgreater than 20 mm Hg in the first 72 h waslikewise substantially higher in the groupthat died (75% vs. 26%). Linear regressionanalysis showed that high ICP was thesecond most important predictor ofmortality.
Kaufman et al.,19867
January 1980–June 1982
Descriptive and prognostic (retrospectivestudy on 143 patients with civilian gunshotinjuries).
III ICP monitors were inserted in 20 patients(14%). Among patients operated fordebridement, ICP monitoring often revealedelevated pressures. No data on ICP orpredictive value of ICP reported.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S73

FEATURES ON CT SCANNINGCategories of Pathologic CT Scan Features
The prognostic significance of various pathologic fea-tures found on CT scan examination will be discussed. Thesefeatures have been divided into the following categories:
Missile Track● Bihemispheric lesions● Multilobar injuries● Ventricular involvement
Evidence of increased intracranial pressure● Cisternal effacement● Midline shift
Presence of hemorrhage or mass lesions● Intracranial hematoma● Intraventricular hemorrhage● Mass lesion/contusions● Subarachnoid hemorrhage
FEATURES ON CT SCANNINGMissile Track
● Bihemispheric lesions● Multilobar injuries● Ventricular involvement
I. ConclusionsBihemispheric lesions relate to increased mortality (Class
II). Compared with unilobar injuries, multilobar injuries arestrongly associated with mortality (Class III). Injuries with ven-tricular involvement have an increased mortality rate (Class III).
II. OverviewCT scan examination permits an accurate detection of the
path a missile has followed through the brain. The extent andlocation of resulting brain damage can be estimated, and thefindings related to outcome. Aspects of the missile trackanalyzed for prognostic value include the presence of bihemi-spheric lesions, the number of planes crossed, multilobarinvolvement, and ventricular involvement. Bihemispheric in-juries are defined as injuries in which the missile trackcrosses the midsagittal plane, causing injury to both cerebralhemispheres. The path of the missile can be described inreference to three planes: the midsagittal plane, the horizontalplane at the level of the third ventricle, and the midcoronalplane (Fig. 4). Multilobular involvement is defined as CTscan evidence of damage to more than one lobe of the cere-brum. Ventricular involvement refers to CT scan evidence ofthe missile path having penetrated the ventricular system.
The reported incidence of bihemispheric lesions in the stud-ies varies from 33% to 63%. The highest incidence is seen inthose studies including patients dead at the scene of accident or
on arrival at the hospital.22,23 It may, therefore, be concludedthat bihemispheric lesions are more common in the most se-verely injured patients. Multilobar involvement in PBI is fre-quent, with a reported incidence varying from 59% to 89%.8,21
Ventricular involvement is described less frequently in 37% ofcases in the military series reported by Brandvold et al.26 and in57% of patients with civilian brain injuries described by Clark.4
No studies report a direct relation between the missile track andother prognostic features. The study by Nagib et al.,8 however,states that all patients with bilateral lesions had a GCS score �6. An overlap exists between the number of planes crossed andthe presence of bihemispheric lesions. A trajectory through themidsagittal plane implies bihemispheric injury.
III. Process (Methodology)Of the 65 original studies, 16 were found to have ade-
quate information on the prognostic value of CT scan exam-ination. The relation between presence or absence of bihemi-spheric lesions and outcomes is described in 12 of the 65studies analyzed. Two studies additionally describe injuriescrossing the horizontal or coronal plane (i.e., lateral trajecto-
Fig. 4. CT wound profile of a penetrating brain trauma in a youngman. The entrance wound is in the right temporal region. Multipleretained bone and metal fragments are visible in the right hemi-sphere, and a small foreign body is seen in the trigone of the rightlateral ventricle. There is extensive intracerebral and intraventric-ular hematoma in association with pneumocephalus. The projectilehas crossed the sagittal, axial, and coronal planes of the cerebralhemispheres and after penetrating the parietal bone has beenstopped by the scalp. This victim was comatose at admission anddied within 2 hours.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S74 August Supplement 2001

ry). Seven studies address the relation between multilobarinjuries and mortality. The relation between a transventriculartrajectory and mortality is addressed in three studies.
IV. Scientific FoundationCT scan is used in the diagnosis of bihemispheric lesions
in most studies. In four, the results of autopsy findings wereincluded for patients who died early.11,19,22,23 All studiesreport a higher mortality among patients with bihemisphericlesions, with odds ratios varying from 1.18 to 20.05. How-ever, differences were not always statistically significant, asin the study of civilian gunshot injuries from the TraumaticComa Data Bank that compared bilateral versus unilaterallesions.10 Despite the failure to demonstrate significance inthe study by Aldrich et al., the authors describe the highestmortality occurring in the presence of large bilateral lesions(93%). Kaufman et al.11 report poorer prognosis in bihemi-spheric lesions, but an exception is made for the presence ofbifrontal lesions, with a mortality of 12% and good outcomein 30%. Two report on the relation between presence ofbihemispheric lesions and unfavorable GOS studies.6,8 Kauf-man et al.,11 reporting on 190 patients with a GCS score of 3to 5, state that on logistic regression analysis the presence ofbihemispheric lesions is also predictive of morbidity.11
Missile tracks crossing the midsagittal plane are synon-ymous with the presence of bihemispheric lesions. Two stud-ies additionally describe injuries crossing the horizontal orcoronal plane. Both Jacobs et al.9 and Shaffrey et al.19 de-scribe increased mortality when the track crosses the hori-zontal plane. Respective odds ratios for these studies towards
mortality are 8.46 and 5.4. Crossing of the midcoronal planehas not been shown to increase mortality.
Seven studies address the relation between multilobarinjuries and mortality. All authors describe a higher mortalityin the presence of multilobar injures when compared withunilobar injuries. Calculated odds ratios range from 3.27 to84.4. However, multilobar injuries are frequent in PBI; con-sequently, the positive predictive value of this parameter isnot always greatly increased with respect to prior probabili-ties in the patient population studied. For example, in thestudy by Nagib et al.,8 a positive predictive value for multi-lobar injuries can be calculated as 57%, but this should berelated to the prior probability of death of 51% occurring inthis study. Perhaps it should be better stated that the absenceof multilobar injuries, i.e., the presence of unilobar damage,is strongly correlated to survival. Calculated negative predic-tive values for mortality range from 77% to 98%.
The relation between ventricular penetration and mortal-ity is addressed in three studies. All three studies show astrong association between ventricular injury and mortality,with calculated odds ratios from 3.35 to 27.5.
V. SummaryCT scan evaluation of the missile track provides useful
prognostic data. Missile track features correlated with in-creased mortality include bihemispheric lesions, multilobarinjuries, and ventricular involvement. Although bihemi-spheric injuries are associated with an increased mortality, apossible exception may be bifrontal injuries.
VI. Evidentiary Table: Missile Track
Authors, Year Year of Study Description of Study Class Conclusions
Cavaliere etal., 198822
Not specified Retrospective study of 178 patientswith civilian gunshot wounds.
III Diagnosis of bihemispheric lesions was made by CT orautopsy. Overall mortality in this series was 93%; 95% ofthe fatally injured patients died within 3 hours; 110 of 112patients with bihemispheric injuries died.
Dead AliveBilateral injuries 110 2Unilateral injuries 56 10OR, 9.8a (n � 178).No probability analysis performed because series includes
patients dead on arrival (n � 178).
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S75
VI. Continued
Authors, Year Year of Study Description of Study Class Conclusions
Clark et al.,19864
January 1984–August 1985
Retrospective analysis of 76 patientswith civilian craniocerebral gunshotwounds.
III Diagnosis of bihemispheric lesion by CT scans. Overallmortality was 62%. Poor outcome was observed in85.7% of patients with bihemispheric lesions vs. 35.5%in-patients with unilateral lesions (�2: p � 0.0001).
GOS score discharge
Unfavorable FavorableBilateral injuries 36 6Unilateral injuries 12 22Pprior, 63%; PPV, 86%; OR, 11.0a,b
# data derived from study
Ventricular injury is associated with poorer outcomePoor outcome Good outcome
Transventricular 35 4No ventricular penetration 7 22Pprior, 62%; PPV, 90%; OR, 27.5.
Grahm etal., 19906
Not specified Prospective study over an 18 monthperiod of 100 patients with civiliangunshot wounds.
II? Results reported on 76 patients of a series of 100 in whomCT analysis was available. Overall mortality in this seriesis 62%. Presence of bihemispheric lesions is related tounfavorable outcome.
GOS score discharge or later:b
Unfavorable FavorableBilateral lesions 30 3Unilateral lesions 14 22Pprior, 64%; PPV, 91%; OR, 15.7.a
Mortality:
Dead AliveBilateral lesions 26 7Unilateral lesions 10 26
Pprior, 52%; PPV, 79%; OR, 9.66 (n � 69).Kaufman et
al., 19867January 1980–
June 1982Descriptive and prognostic
(retrospective) study of 143 patientswith civilian gunshot injuries.
III CT scanning was done on 62 patients of a series of 143,including 29 of 48 survivors and 33 of 95 patients whodied. Bihemispheric lesions, as defined by the missilepath crossing the midline was related to increasedmortality: 15% of patients with a missile tract crossingthe midline survived versus 64% with unilateral injuries.
Dead AliveBilateral lesions 17 3Unilateral or reaching
midline16 21
Pprior, 58%; PPV, 85%; OR, 7.44a (n � 57).
The Journal of TRAUMA� Injury, Infection, and Critical Care
S76 August Supplement 2001
VI. Continued
Authors, Year Year of Study Description of Study Class Conclusions
Kaufman etal., 199511
Retrospective review of two series ofpatients with civilian gunshot woundsto the brain. Emphasis of the study ison patients with admission GCSscore 3–5. The first series (series A)evaluates treatment results in 190patients presenting over a 6-yearperiod to the University of SouthernCalifornia. These patients weresubjected to a conservativeapproach. The second series (seriesB) describes 480 patients admitted toCook County Hospital in Chicagofrom 1983 through 1992. Full dataare reported on patients with GCSscore 3–5 only (n � 146).
III Bihemispheric lesions diagnosed by CT scan.Series A: Presence of bihemispheric lesions is related to
mortality (p � 0.05).
Dead AliveBihemispheric lesions 94 12No bihemispheric lesions 73 11Pprior, 88%; PPV, 89%; OR, 1.18 (n � 190).
On logistic regression analysis bihemispheric lesions werepredictive of morbidity.
Series B: Bihemispheric injuries had the worst prognosis.The exception is the presence of bifrontal lesions, with amortality of 12% and good outcome in 30%. No exactdata reported. On linear regression analysis thedifferentiation unilateral versus bihemispheric injury wasretained in the model at p � 0.05.
Lillard,197817
1971–1975 Retrospective analysis in 5-year period,describing 83 patients with PBI.
III Single lobe injuries did much better than cases when themissile crossed the midsagittal plane. Highest mortalitywas noted when both midsagittal and midcoronal planescrossed (75%). No data on CT scan reported; it remainsunclear on which basis the diagnosis of a single lobeinjury or the crossing of planes is determined.
Dead AliveCrossing midsagittal plane 15 12Unilateral injury 14 26Pprior, 43%; PPV, 55%; OR, 2.23 (n � 67).
Siccardi etal., 199123
Retrospective study of 314 consecutivepatients with civilian head wounds ofwhom 228 died at the scene of theaccident.
III Diagnosis of unilateral versus bilateral injuries made by CTscan or autopsy. Out of a series of 314 consecutivepatients with civilian gunshot wounds, 228 were dead atthe scene of accident. Mortality is higher in the presenceof bilateral or multilobar injury.
Dead AliveBilateral injuries 160 6Unilateral injuries 128 20OR, 4.17.a
Dead AliveMultilobar injury 248 14Single lobe injury 40 12OR, 5.3.a
No probability analysis performed because series includespatients dead at the scene of accident.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S77

VI. Continued
Authors, Year Year of Study Description of Study Class Conclusions
Shaffrey etal., 199219
1984–1990 Retrospective study of 62 patients withgunshot wounds; multivariateanalysis of predictors of mortality isperformed.
III Diagnosis of missile tract on CT scan (n � 40) or autopsy,18 patients dead on arrival. Overall mortality 55%. CTfeatures of prognostic significance include: crossing ofsagittal (p � 0.004) or horizontal planes (p � 0.002) andcrossing of three planes (p � 0.017). Mortality is 68% inthe presence of bihemispheric injuries, as defined bymissile tract crossing the midsagittal plane. Mortality ininjuries not crossing the midsagittal plane: 27.8%. Thedifference is statistically significant. Crossing of themidcoronal plane is not associated to increased mortality.Odds ratios for crossing sagittal, horizontal and 3 planesare resp.: 5.6,a 5.4,a and 9.3.a
Transventricular trajectory is associated with increasedmortality (p � 0.024).
Aldrich etal., 199210
January 1984–September 1987
Prospective study on prognosis in 151patients with civilian gunshot injuriesfrom the Traumatic Coma Data Bank.
I Data reported on 89 patients of the total series of 151 inwhom CT scan was available. Mortality is slightly higheramong patients with bilateral lesions, but differences arenot statistically significant. In the presence of largebilateral lesions (n � 14) mortality is 93%.
Dead AliveBilateral lesions 31 6Unilateral lesions 21 6Pprior, 81%; PPV, 84%; OR, 1.48 (n � 64).
Nagib et al.,19868
1978–1983 Retrospective study on prognosis andmanagement of civilian gunshotwounds during a 5-year period from1978 to 1983.
III Diagnosis of bilateral lesions by CT scan; the presence ofbihemispheric lesions was related to both mortality andunfavorable outcome. All patients with bilateral lesionshad a GCS score � 6. Multilobar injuries are associatedwith increased mortality and poorer outcome.
Mortality:
Dead AliveBilateral lesions 19 4Unilateral lesions 9 23Pprior, 51%; PPV, 82%; OR, 12.1.a
Dead AliveMultilobar injuries 28 21Single lobe injuries 0 6
Pprior, 51%; PPV, 57%; NPV, 100%; OR, 8a,c (n � 56).Jacobs et
al., 19959January 1990–
December 1992Retrospective analysis of 57 patients in
whom full data were available from72 cases admitted from January1990 to December 1992 withtranscranial gunshot wounds. Focuson the manuscript is on cost andconsequences.
III Diagnosis of bihemispheric lesions by CT scan;bihemispheric gunshot wounds are statisticallysignificantly more frequently observed among non-survivors (p � 0.03) with an odds ratio to mortality of 4.6.On multivariate analysis only Caucasian racial state, GCSscore � 4 and lateral trajectory remain statisticallysignificant.
Dead AliveBihemispheric injuries 24 3No bihemispheric injury 19 11Pprior, 75%; PPV, 89%; OR, 4.6.a
Dead AliveLateral trajectory 30 3No lateral trajectory 13 11Pprior, 75%; PPV, 91%; OR, 8.46a (n � 57).
The Journal of TRAUMA� Injury, Infection, and Critical Care
S78 August Supplement 2001

VI. Continued
Authors, Year Year of Study Description of Study Class Conclusions
Brandvold etal., 199026
1982–June 1985 Retrospective analysis of 113 patientsevacuated to Rambam MaimonidesMedical Center with penetratingcraniocerebral injuries sustained inongoing military hostilities inLebanon.
III Multilobar injuries have a significantly higher rate ofmortality.
Dead AliveMultilobar 29 26Unilobar 2 59Pprior, 27%; PPV, 53%; NPV, 97%; OR, 32.9.a
Transventricular injuries have an increased mortality rate.
Dead AliveTransventricular 24 18No ventricular penetration 6 65Pprior, 27%; PPV, 57%; OR, 14.4.a
Kennedy etal., 199315
January 1987–June 1990
Retrospective analysis of prognosticfeatures in 192 patients with gunshotand shotgun injuries.
III Mortality is increased in multilobar injuries among patientswith GCS score 5–13.
Dead AliveMultilobar 11 13Unilobar 1 8Pprior, 36%; PPV, 46%; NPV, 89%; OR, 6.77.
Levi et al.,199027
Prospective? Study on 116 patientswith penetrating injury, occurredduring involvement of Israeli defenseforces in Lebanon from June 1982 toJune 1985. Essentially, same patientpopulation as described underBrandvolt et al.
III Multilobar injuries are related to increased mortality andpoorer outcome.
Dead AliveMultilobar injuries 29 22Unilobar injuries 1 64Pprior, 26%; PPV, 57%; NPV, 98%; OR, 84.4.a
Shoung etal., 198520
1978–1983 Retrospective study on 56 patients withcraniocerebral gunshot wounds.
III Injuries involving two or more lobes are associated withincreased mortality.
Dead AliveMultilobar injuries 27 14Single lobe injuries 3 12Pprior, 54%; PPV, 66%; NPV, 80%; OR, 7.7.a
Suddaby etal., 198721
1975–1985 Retrospective analysis of 49 patientswith low velocity gunshot wounds.
III Injury to multiple lobes is associated with poorer outcome.
Dead AliveMultilobar injuries 19 8Single lobe injuries 8 11Pprior, 58%; PPV, 70%; NPV, 77%; OR, 3.27.a
Pprior, prior probability (the outcome distribution in the population studied); PPV, positive predictive value; OR, odds ratio; NPV, negativepredictive value.
a Indicates 95% confidence interval does not include 1.b Outcome was determined at discharge, patients vegetative or severely disabled at discharge, a mean follow-up of 9 months was performed.c Zero set to 1 for calculation.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S79

FEATURES ON CT SCANNINGEvidence of Increased Intracranial Pressure
● Cisternal effacement● Midline shift
I. ConclusionsCisternal effacement in severe PBI is associated with
increased mortality (Class I). No relation between midlineshift and outcome has been established (Class I).
II. OverviewCompression or absence of the basal cisterns on CT scan is
considered one of the most reliable indicators of raised intracra-nial pressure.48,49 Indirectly, the presence of midline shift maybe considered indicative of raised ICP because of the mass effectcausing the shift. Although the status of the basal cisterns is oneof the best studied CT scan parameters in nonpenetrating TBI, itremains ill-defined in PBI. In nonpenetrating TBI, a strongassociation has been demonstrated between the status of thebasal cisterns and pupil reactivity.43,44 None of the studies inPBI, however, investigated such a relation.
Most studies that examined the basal cisterns focused onthe perimesencephalic cisterns, describing them as absent,compressed, or open. Partial or complete obliteration of thebasal cisterns is described in 69% of patients with PBI fromthe Traumatic Coma Data Bank, in whom CT scan examina-tion was performed. This incidence is similar to reportedresults in nonpenetrating TBI.
The presence of midline shift is defined as the absolutedistance (in millimeters) that midline structures of the brain aredisplaced with respect to the midline, as determined by averag-ing the distance between the inner tables of the skull. Midlinestructures are evaluated at the level of the septum pellucidum. Inthe nonpenetrating TBI literature, a relation between midlineshift and the presence or absence of focal lesions and the GCSscore is described.50,51 No such relation has been reported in thePBI literature. The presence of midline shift is described in 40%of patients in the study by Kaufman et al.7 with PBI and in 48%
of patients in the study described by Aldrich et al.10 The higherincidence, as described by Aldrich et al., may be related todifferent definitions of degree of midline shift. In the study byAldrich et al., a midline shift of � 3 mm is the threshold versusa midline shift of � 1 cm in the study by Kaufman et al.
III. Process (Methodology)Of the 65 original studies, 16 were found to have ade-
quate information on the prognostic value of CT scan exam-ination. Among the 16 studies addressing the prognosticfeatures of CT scan examination in PBI, only 1 describes therelation between compression of basal cisterns and outcome,and only 2 describe the relation between midline shift andoutcome.
IV. Scientific FoundationThe presence of obliterated basal cisterns has a positive
predictive value of 85% to mortality among patients with PBIwho have a GCS score of 8 or less. The calculated odds ratiois 2.74. Cisternal compression is therefore related to in-creased mortality. No data are available to relate the presenceof obliterated basal cisterns to intracranial pressure in thisstudy.10 The presence of midline shift is not related to mor-tality. Neither of the two studies7 describing this parametershowed any statistical significance, and calculated odds ratioswere 0.92 and 1.21. The absence of prognostic significance ofshift in PBI may be caused by the frequent occurrence ofbihemispheric injuries.
V. SummaryCT scan characteristics considered to be associated with
increased intracranial pressure include cisternal effacementand midline shift. Because increased ICP has been correlatedwith mortality, these CT scan findings have been studied fortheir clinical import. Although cisternal effacement is asso-ciated with increased mortality, no relation between midlineshift and outcome has been established. A lack of standard-ized definitions for midline shift may contribute to the ab-sence of discernible data.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S80 August Supplement 2001

VI. Evidentiary Table: Predictive Value of CT Scan Indicators of Raised Intracranial Pressure
Authors, Year Years of Study Description of Study Class Conclusions
Aldrich et al.,199210
January 1984–September 1987
Prospective study on prognosis among151 patients with civilian gunshotinjuries from the Traumatic ComaData Bank.
I Cisternal effacement on CT scan isassociated with increased mortality.
Dead AliveObliterated cisterns 52 9Patent cisterns 19 9Pprior, 80%; PPV, 85%; OR, 2.74.
Midline shift �3 mm on CT scan is notrelated to mortality.
Dead AliveShift 34 9No shift 37 9Pprior, 80%; PPV, 79%; OR, 0.92
(n � 89).Kaufman et
al., 19867January 1980–
June 1982Descriptive and prognostic
(retrospective) study of 143 patientswith civilian gunshot injuries.
III Midline shift �1 cm on CT scan is notrelated to increased mortality.
Dead AliveShift 14 11No shift 19 18Pprior, 53%; PPV, 56%; OR, 1.21.
Pprior, prior probability (the outcome distribution in the population studied); PPV, positive predictive value; OR, odds ratio.a Indicates that the 95% confidence interval does not include 1.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S81

FEATURES ON CT SCANNINGPresence of Hemorrhage or Mass Lesions
● Intracranial hematoma● Intraventricular hemorrhage● Mass lesion/contusions● Subarachnoid hemorrhage
I. ConclusionsIntraventricular hemorrhage is strongly correlated to in-
creased mortality (Class I). Subarachnoid hemorrhage in PBIis also correlated to increased mortality (Class I).
II. OverviewIntracranial hemorrhage may take many forms in the
setting of trauma. Intracranial hematoma is defined as hyper-dense lesions on CT scanning, with a density of blood oc-curring in either the epidural or subdural space, or within theparenchyma. In PBI, focal intraparenchymal lesions or con-tusions are generally hyperdense and form a continuum withparenchymal hematoma. Hyperdensity within the ventricularsystem is consistent with intraventricular hemorrhage. Incases of subarachnoid hemorrhage, blood is within the sub-arachnoid space, either over the convexity or in the basalcisterns.
An accurate determination of the real incidence of thesefeatures is difficult because, among the various studies de-scribed, relatively few patients received CT scan examina-tions. In the study by Kaufman et al.,7 CT scans were ob-tained in only 43% of the patients, and in the study by Aldrichet al.,10 CT scans were obtained in 59%. The reported inci-dence of intracranial hematoma varies between 29% and63%. The incidence of intraventricular hemorrhage variesfrom 35% to 47%. The presence of focal lesions varies from31% to 34%, and the presence of traumatic subarachnoidhemorrhage ranges from 31% to 78%.
III. Process (Methodology)Of the 65 original studies, 16 were found to have ade-
quate information on prognostic value of CT scan examina-tion. Among the 16 studies addressing prognostic features ofCT scan examination in PBI, 6 investigated the relationbetween the presence of hemorrhage or mass lesions andoutcome. Three studies describe increased mortality in thepresence of intracranial hematoma. The predictive value ofthe presence of focal lesions is investigated in three studies.Three studies investigate the relation between intraventricularhemorrhage and mortality, and three studies correlate out-come with the presence of subarachnoid hemorrhage.
IV. Scientific FoundationTwo studies7,19 describe increased mortality in the pres-
ence of intracranial hematoma, with an odds ratio of 3.35 and4.01, respectively. Shaffrey et al.19 report a Class I study thatcorrelates increased mortality with increased volume of con-
tused brain. In the study by Mancuso et al.,18 however, thepresence of a hematoma was not related to mortality. Therelatively low percentage of patients in whom CT scan ex-aminations were performed and the differing results betweenthe studies yield inconclusive evidence concerning the pre-dictive value of intracranial hematoma.
Three studies7,8,10 investigated the relation between in-traventricular hemorrhage and mortality in PBI. All threestudies show an increased mortality in the presence of intra-ventricular hemorrhage, with odds ratios varying from 2.83 to96.9. It may therefore be concluded that the presence ofintraventricular hemorrhage is strongly correlated to in-creased mortality.
The predictive value of the presence of focal lesions isinvestigated in three studies.8,10,19 The quantification of theextent of the lesion is, however, performed differently.Whereas some authors quantify the lesion in terms of cerebralvolume (i.e., � 10% of the cerebrum), others use actualvolume of the mass lesion (i.e., � 15 mL). Both Aldrich etal.10 and Shaffrey et al.19 report increased mortality in thepresence of focal lesions, but only Shaffrey et al. reportstatistical significance (p � 0.002). In a retrospective studyon 55 civilian gunshot wounds, Nagib et al.8 could find nosuch relation. Calculated odds ratios for the three studiesranged from 0.36 to 13.22. The conflicting data do not allowdefinite conclusions concerning the prognostic significanceof the presence of focal lesions.
In nonpenetrating TBI, the presence of traumatic subarach-noid hemorrhage is correlated to mortality and unfavorableoutcome.47,52 The available data on PBI are mixed. Aldrich etal.,10 analyzing 89 patients in whom CT scan was obtained in aseries of 151 patients with civilian gunshot injuries from theTraumatic Coma Data Bank, showed a slightly increased mor-tality in the presence of traumatic subarachnoid hemorrhage(81% vs. 75%). Differences, however, were not statisticallysignificant. Similarly, Kaufman et al.11 describe a slightly in-creased mortality, but no statistical significance. Odds ratios forthese two studies are 1.44 and 1.81. However, in the Class Istudy described by Levy et al.,12 a significantly increased mor-tality was noted in 31 patients with radiologic evidence oftraumatic subarachnoid hemorrhage in a consecutive series of100 civilian patients with cerebral gunshot wounds admittedover a 12-month period. Odds ratio of mortality in this study wascalculated as 10.6. The significant predictive value of this studywas maintained when confounding effects of other variableswere excluded in a �2 hierarchical evaluation of outcome. Theabsence of significance in the other two studies describing thisparameter may be caused by the selection of patients, whichfocused on the most severely injured, with a prior probability ofmortality already of 80% and 88%.
V. SummaryThe presence of large contusions on CT scans does
correlate with increased mortality. Intraventricular hemor-rhage has been shown to be associated with increased mor-
The Journal of TRAUMA� Injury, Infection, and Critical Care
S82 August Supplement 2001

tality. Focal lesions on CT scan are defined differently invarious articles, making conclusions difficult to ascertain.Intracerebral hematoma appears to increase mortality, butstudy design flaws in the various articles prevent definitive
conclusions. The single Class I study of traumatic subarach-noid hemorrhage in PBI showed the same influence on mor-tality as in nonpenetrating TBI, whereas the two Class IIIstudies showed no significant difference.
VI. Evidentiary Table: Predictive Value of Hemorrhage or Mass Lesions
Authors, Year Years of Study Description of Study Class Conclusions
Kaufman etal., 19867
January 1980–June 1982
Descriptive and prognostic (retrospective)study of 143 patients with civiliangunshot injuries.
III The presence of intracranial hematoma (EDH �4, SDH � 27, ICH � 19) was associated withincreased mortality.
Dead AliveHematoma 25 14No hematoma 8 15Pprior, 53%; PPV, 64%; OR, 3.35.a
Intraventricular hemorrhage was stronglyassociated with increased mortality.
Dead AliveIVH 31 4No IVH 2 25Pprior, 53%; PPV, 89%; OR, 96.9a (n � 62).
Mancuso etal., 198818
1969–1986 Retrospective study of 40 patients withcraniocerebral gunshot wounds. Mainlydescriptive study.
III The presence of a hematoma (SDH or ICH) didnot effect outcome.
Dead AliveHematoma 1 5No hematoma 4 11Pprior, 24%; PPV, 17%; OR, 0.55 (n � 21).
Shaffrey et al.,199219
1984–1990 Retrospective study of 62 patients withgunshot wounds, multivariate analysis ofpredictors of mortality is performed.
I Intraventricular hemorrhage as demonstrated onCT scan correlates with increased mortality.
Dead AliveIVH 37 5No IVH 34 13Pprior, 80%; PPV, 88%; OR, 2.83a (n � 89).
Large intracranial lesions (�15 mL) correlate withincreased mortality.
Dead AliveLesion �15 mL 26 4No lesion 45 14Pprior, 80%; PPV, 87%; OR, 2.02.
Subarachnoid hemorrhage is not significantlyrelated to increased mortality.
Dead AliveSAH 56 13No SAH 15 5Pprior, 80%; PPV, 81%; OR, 1.44.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S83

VI. Continued
Authors, Year Years of Study Description of Study Class Conclusions
Nagib et al.,19868
1978–1983 Retrospective study of prognosis andmanagement of civilian gunshot woundsduring 5-y period from 1978 to 1983.
III Intraventricular hemorrhage is associated withincreased mortality and poor outcome.
Dead AliveIVH 15 4No IVH 10 26Pprior, 45%; PPV, 79%; OR, 9.75a (n � 55).
Mass lesions defined by a hematoma or focalswelling are not associated with increasedmortality or poorer outcome.
Dead AliveLesion 6 11No lesion 22 16Pprior, 51%; PPV, 35%; OR, 0.40.
Kaufman etal., 199511
1983–1994 Two series of patients with civilian gunshotwounds to the brain are described.Emphasis of the study is on patientswith admission GCS score of 3–5. Thefirst series (series A) evaluates treatmentresults in 190 patients presenting over a6-y period to the University of SouthernCalifornia. These patients weresubjected to a conservative approach.The second series (series B) describes480 patients admitted to Cook CountyHospital in Chicago from 1983 through1992. Full data are reported only onpatients with GCS score of 3–5(n � 146).
III The predictive value of SAH is investigated inseries A. SAH is correlated with increasedmortality.
Dead AliveSAH 129 15
No SAH 38 8
Pprior, 88%; PPV, 90%; OR, 1.81.
Levy et al.,199312
100 PBI patients from civilian gunshotwound, 31 with SAH on CT scan whohad angiography. One TICA found andoperated on. 68% of patients dyingwithin 48 h had SAH compared with only17% who survived.
I Presence of traumatic subarachnoid hemorrhageis significantly correlated with mortality(p � 0.01).
Dead AliveSAH 19 12No SAH 9 60Pprior, 28%; PPV, 61%; OR, 10.6.a
EDH, epidural hematoma; SDH, subdural hematoma; ICH, intracranial hemorrhage; Pprior, prior probability (the outcome distribution in thepopulation studied); PPV, positive predictive value; OR, odds ratio; IVH, intraventricular hemorrhage; SAH, subarachnoid hemorrhage; TICA,traumatic intracranial aneurysm.
a Indicates that the 95% confidence interval does not include 1.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S84 August Supplement 2001

KEY ISSUES FOR FUTURE RESEARCH INPROGNOSIS IN PBI
Of prime importance for future research into prognosticindicators is the proper data collection. Standardized defini-tions of various parameters that appear to have prognosticsignificance should be instituted among trauma centers.These include, but are not restricted to, hypotension, co-agulopathy, respiratory distress, pupillary examination, in-tracranial pressure, as well as the CT scan findings. Theseparameters should be recorded prospectively at admissionand at set intervals thereafter. A rigid set of outcomemeasures should be collected at predetermined intervalsduring the hospital and posthospital course. Only withsuch standardization will the needed data regarding thebenefit of treatment modalities and the significance ofprognostic indicators truly be known.
REFERENCES1. Guidelines for the management of severe traumatic brain injury.
Brain Trauma Foundation, American Association of NeurologicalSurgeons, Joint Section on Neurotrauma and Critical Care.J Neurotrauma. 2000;17:451–627.
2. Jennett B, Bond M. Assessment of outcome after severe braindamage. Lancet. 1975;1:480–484.
3. Maas AIR, Steyerberg EW, Murray GD, et al. Why have recenttrials of neuroprotective agents in head injury failed to showconvincing efficacy? A pragmatic analysis and theoreticalconsiderations. Neurosurgery. 199;44:1286–1298.
4. Clark CW, Muhlbauer MS, Watridge CB, et al. Analysis of 76civilian craniocerebral gunshot wounds. J Neurosurg. 1986;65:9 –14.
5. Hernesniemi J. Penetrating craniocerebral gunshot wounds incivilians. Acta Neurochir (Wien). 1979;49:199–205.
6. Grahm TW, Williams FC Jr, Harrington T, Spetzler RF. Civiliangunshot wounds to the head: a prospective study. Neurosurgery.1990;27:696–700.
7. Kaufman HH, Makela ME, Lee KF, Haid RW Jr, Gildenberg PL.Gunshot wounds to the head: a perspective. Neurosurgery. 1986;18:689–695.
8. Nagib MG, Rockswold GL, Sherman RS, Lagaard MW. Civiliangunshot wounds to the brain: prognosis and management.Neurosurgery. 1986;18:533–537.
9. Jacobs DG, Brandt CP, Piotrowski JJ, McHenry CR. Transcranialgunshot wounds: cost and consequences. Am Surg. 1995;61:647–654.
10. Aldrich EF, Eisenberg HM, Saydjari C, et al. Predictors of mortalityin severely head-injured patients with civilian gunshot wound: areport from the NIH Traumatic Coma Data Bank. Surg Neurol.1992;38:418–423.
11. Kaufman HH, Levy ML, Stone JL, et al. Patients with GlasgowComa Scale scores 3, 4, 5 after gunshot wounds to the brain.Neurosurg Clin North Am. 1995;6:701–714.
12. Levy ML, Rezai A, Masri LS, et al. The significance ofsubarachnoid hemorrhage after penetrating craniocerebral injury:correlations with angiography and outcome in civilian population.Neurosurgery. 1993;32:532–540.
13. Byrnes DP, Crockard HA, Gordon DS, Gleadhill CA. Penetratingcraniocerebral missile injuries in the civil disturbances in NorthernIreland. Br J Surg. 1974;61:169–176.
14. Hubschmann O, Shapiro K, Baden M, Shulman K. Craniocerebralgunshot injuries in civilian practice: prognostic criteria and surgicalmanagement experience with 82 cases. J Trauma. 1979;19:6–12.
15. Kennedy F, Gonzalez P, Dang C, Fleming A, Sterling-Scott R. TheGlasgow Coma Scale and prognosis in gunshot wounds to the brain.J Trauma. 1993;35:75–77.
16. Kunz U, Seidel BU, Stolke D, Dietz H. Gunshot wounds of the skullduring peacetime [in German]. Neurochirurgia. 1985;28:134–142.
17. Lillard PL. Five years experience with penetrating craniocerebralgunshot wounds. Surg Neurol. 1978;9:79–83.
18. Mancuso P, Chiaramonte I, Passanisi M, Guarnera F, Augello G,Tropea R. Craniocerebral gunshot wounds in civilians: report on 40cases. J Neurosurg Sci. 1988;32:189–194.
19. Shaffrey ME, Polin RS, Phillips CD, Germanson T, Shaffrey CI,Jane JA. Classification of civilian craniocerebral gunshot wounds: amultivariate analysis predictive of mortality. J Neurotrauma. 1992;9(suppl 1):S279–S285.
20. Shoung HM, Sichez JP, Pertuiset B. The early prognosis ofcraniocerebral gunshot wounds in civilian practice as an aid to thechoice of treatment: a series of 56 cases studied by the computerizedtomography. Acta Neurochir (Wien). 1985;74:27–30.
21. Suddaby L, Weir B, Forsyth C. The management of .22 calibergunshot wounds of the brain: a review of 49 cases. Can J NeurolSci. 1987;14:268–272.
22. Cavaliere R, Cavenago L, Siccardi D, Viale GL. Gunshot wounds ofthe brain in civilians. Acta Neurochir (Wien). 1988;94:133–136.
23. Siccardi D, Cavaliere R, Pau A, Lubinu F, Turtas S, Viale GL.Penetrating craniocerebral missile injuries in civilians: a retrospectiveanalysis of 314 cases. Surg Neurol. 1991;35:455–460.
24. Marshall LF, Maas AI, Marshall SB, et al. A multicenter trial on theefficacy of using tirilazad mesylate in cases of head injury.J Neurosurg. 1998;89:519–525, 1998.
25. Aarabi B. Surgical outcome in 435 patients who sustained missilehead wounds during the Iran-Iraq war. Neurosurgery. 1990;27:692–695.
26. Brandvold B, Levi L, Feinsod M, George ED. Penetratingcraniocerebral injuries in the Israeli involvement in the Lebaneseconflict, 1982-1985: analysis of a less aggressive surgical approach.J Neurosurg. 1990;72:15–21.
27. Levi L, Borovich B, Guilburd JN, et al. Wartime neurosurgicalexperience in Lebanon, 1982-85, I: penetrating craniocerebralinjuries. Br J Med Sci. 1990;26:548–554.
28. Small JM, Turner EA. A surgical experience of 1200 cases ofpenetrating brain wounds in battle, N.W. Europe, 1944–1945. Br JSurg. 1947; War Surgery Supplement I;62–74.
29. Matson DD. The Treatment of Acute Craniocerebral Injuries Due ToMissiles. Springfield, IL: Charles C Thomas; 1948.
30. Hammon WM, Kempe LG. Analysis of 2187 consecutive penetratingwounds of the brain from Vietnam. J Neurosurg. 1971;34:127–131.
31. Kaufman HH, Schwab K, Salazar AM. A national survey ofneurosurgical care for penetrating head injury. Surg Neurol. 1991;36:370–377.
32. Wright N, Adams KS. Changing motivation in severely suicidalpatients. Can Med Assoc J. 1986;135:1361–1363.
33. Stocchetti N, Furlan A, Volta F. Hypoxemia and arterial hypotensionat the accident scene in head injury. J Trauma. 1996;40:764–767.
34. Chesnut RM, Marshall SB, Piek J, Blunt BA, Klauber MR, MarshallCF. Early and late systemic hypotension as a frequent andfundamental source of cerebral ischemia following severe braininjury in the Traumatic Coma Data Bank. Acta Neurochir Suppl(Wien). 1993;59:121–125.
35. Teasdale G, Jennett B. Assessment of coma and impairedconsciousness: a practical scale. Lancet. 1974;2:81–84.
Prognosis in Penetrating Brain Injury
Volume 51 • Number 2 S85

36. Braakman R, Avezaat CJ, Maas AI, Roel M, Schouten HJ. Interobserver agreement in the assessment of the motor response of theGlasgow ‘coma’ scale. Clin Neurol Neurosurg. 1977;80:100–106.
37. Fielding K, Rowley G. Reliability of assessments by skilled observersusing the Glasgow Coma Scale. Aust J Adv Nurs. 1990;7:13–17.
38. Menegazzi JJ, Davis EA, Sucov AN, Paris PM. Reliability of theGlasgow Coma Scale when used by emergency physicians andparamedics. J Trauma. 1993;34:46–48.
39. Teasdale G, Knill-Jones R, van der Sande J. Observer variability inassessing impaired consciousness and coma. J Neurol NeurosurgPsychiatry. 1978;41:603–610.
40. Marion DW, Carlier PM. Problems with initial Glasgow Coma Scaleassessment caused by prehospital treatment of patients with headinjuries: results of a national survey. J Trauma. 1994;36:89–95.
41. Carey ME, Young HF, Mathis JL. The neurosurgical treatment ofcraniocerebral missile wounds in Vietnam. Surg Gynecol Obstet.1972;135:386–390.
42. van den Berge JH, Schouten HJ, Boomstra S, Van Drunen Little S,Braakman R. Interobserver agreement in assessment of ocular signsin coma. J Neurol Neurosurg Psychiatry. 1979;42:1163–1168.
43. van Dongen KJ, Braakman R, Gelpke GJ. The prognostic value ofcomputerized tomography in comatose head-injured patients.J Neurosurg. 1983;59:951–957.
44. Teasdale E, Cardoso E, Galbraith S, Teasdale G. CT scan in severediffuse head injury: physiological and clinical correlations. J NeurolNeurosurg Psychiatry. 1984;47:600–603.
45. Toutant SM, Klauber MR, Marshall LF, et al. Absent or compressedbasal cisterns on first CT scan: ominous predictors of outcome insevere head injury. J Neurosurg. 1984;61:691–694.
46. Athiappan S, Muthukumar N, Srinivasan US. Influence of basalcisterns, midline shift and pathology on outcome in head injury. AnnAcad Med Singapore. 1993;22(3 suppl):452–455.
47. Eisenberg HM, Gary HE Jr, Aldrich EF, et al. Initial CT findings in753 patients with severe head injury: a report from the NIHTraumatic Coma Data Bank. J Neurosurg. 1990;73:688–698.
48. Teasdale G, Bailey I, Bell A, et al. A randomized trial ofnimodipine in severe head injury, HIT I: British/Finnish Co-operative Head Injury Trial Group. J Neurotrauma. 1992;9(suppl2):S545–S550.
49. Klauber MR, Toutant SM, Marshall LF. A model for predictingdelayed intracranial hypertension following severe head injury.J Neurosurg. 1984;61:695–699.
50. Kotwica Z, Brzezinski J. Acute subdural haematoma in adults: ananalysis of outcome in comatose patients. Acta Neurochir (Wien).1993;121:95–99.
51. Young B, Rapp RP, Norton JA, Haack D, Tibbs PA, Bean JR. Earlyprediction of outcome in head-injured patients. J Neurosurg. 1981;54:300–303.
52. Kakarieka A, Braakman R, Schakel EH. Clinical significance of thefinding of subarachnoid blood on CT scan after head injury. ActaNeurochir (Wien). 1994;129:1–5.
The Journal of TRAUMA� Injury, Infection, and Critical Care
S86 August Supplement 2001