pathophysiology and management of meningococcal … · cme septicaemia – i promised, for example...
TRANSCRIPT

CM E Sept icaem ia ndash I
promised for example by exacerbationof hypoxia due to lung injury sequentialmultiple organ failure follows Organdysfunction in sepsis is covered in moredetail in the accompanying article bySinger
Conclusion
Whilst an infecting organism mayproduce toxins which injure tissuesdirectly this is often inadequate toexplain the clinico-pathologicalsequelae in severe sepsis Instead thedominant role in pathogenesis may liewith components of the host immuneresponse to infection The highlyconserved responses of the innateimmune system comprise sequentialactivation and amplification of humoraland cellular antimicrobial defencemechanisms which can escape thecontrol of anti-inflammatory regulationinadvertently causing injury to the hostFurther understanding of the immuno-pathogenesis of severe sepsis mayunveil new opportunities for therapeuticintervention
References
1 Rangel-Frausto MS The epidemiology ofbacterial sepsis Review Infect Dis ClinNorth Am 199913299ndash312 vii
2 Morrison DC Ryan JL Endotoxins anddisease mechanisms Annu Rev Med198738417ndash32
3 Medshitov R Janeway C Innate immun-ity N Engl J Med 2000343338ndash44
4 Sriskandan S Cohen J Gram-positivesepsis Mechanisms and differences fromgram-negative sepsis Infect Dis Clin NorthAm 199913397ndash412
5 Bernal A Proft T Fraser JD Posnett DNSuperantigens in human disease J ClinImmunol 199919149ndash57
6 Takeuchi O Hoshino K Kawai T Sanjo Het al Differential roles of TLR2 and TLR4in recognition of gram-negative andgram-positive bacterial cell wall compo-nents Immunity 199911443ndash51
7 Brown EJ Lindberg FP Leucocyteadhesion molecules in host defenceagainst infection Review Ann Med199628201ndash8
8 Mammen EF The haematologica lmanifestations of sepsis J AntimicrobChemother 199841(Suppl A)17ndash24
9 Haeney MR The role of the complementcascade in sepsis J Antimicrob Chemother199841(Suppl A)41ndash6
10 van der Poll T van Deventer SJCytokines and anticytokines in the
436 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
pathogenesis of sepsis Review Infect DisClin North Am 199913413ndash26 ix
11 Mathiak G Szewczyk D Abdullah FOvadia P Rabinovici R Platelet-activat-ing factor (PAF) in experimental andclinical sepsis Shock 19977391ndash404
12 Parratt JR Nitric oxide in sepsis andendotoxaemia J Antimicrob Chemother199841(Suppl A)31ndash9
13 Dinarello CA Cytokines as endogenouspyrogens J Infect Dis 1999179(Suppl2)S294ndash304
14 Brady AJ Nitric oxide myocardial failure
and septic shock Int J Cardiol 199550269ndash72
15 Thijs LG Groeneveld AB Hack CEMultiple organ failure in septic shockCurr Top Microbiol Immunol 1996216209ndash37
Address for correspondence Professor JCohen Hammersmith Hospital Du CaneRoad London W12 0NNE-mail jcohenicacuk
Pathophysiology and management of
meningococcal septicaemia
Neisseria meningitidis (meningococcus) isa major infection risk globally In theUK it is the leading cause of death frominfection in childhood1 with a mortalityaround 102 Most deaths frommeningococcal infection are due to thedevelopment of fulminant septicshock23 Yet N meningitidis is a frequentcommensal of the human upperrespiratory tract Carriage rates increasefrom less than 1 in infancy to amaximum of 25 in adolescencedeclining to around 10 in adulthood
The meningococcus is a Gram-negative diplococcus Pathogenicmeningococci possess a polysaccharidecapsule differences in the structure ofwhich form the basis of separation intosubgroups The lack of suitable vaccinesfor all the meningococcal serogroups isbecause of a high level of geneticdiversity caused by intraspecies re-combination and transformation Asingle mutation or genetic exchange
may lead to an outbreak of clinicaldisease if associated with a change inan immunologically important surfaceantigen
Epidemiology
Meningococcal disease is endemicworldwide Serogroups B and C pre-dominate in the UK with an incidence of5ndash6 per 10000024 In sub-SaharanAfrica serogroup A predominates incyclical epidemics every eight years andcan affect up to 1000 per 100000 ofthe population5 The reasons forregional variation in disease-causingserogroups are not well defined
Immunopathology
Transmission
Transmission is by close contact orrespiratory droplet spread
Colonisation and invasion of nasopharyngeal epithelium
The risk of colonisation may beenhanced by disrupt ion of therespiratory epithelial cell layer byirritants (such as cigarette smoke) or bya preceding viral illness for exampleinfluenza A6 Binding to epithelial cells isestablished by pili78 and outermembrane proteins9 Certain outer
Nazima Pathan BSc MRCP MRCPCH Clinical Research Fellow
Simon Nadel MRCP MRCPCH Consultant Paediatric Intensive Care Unit
Michael Levin PhD FRCP FRCPCH Professor of Paediatrics
Imperial College School of Medicine at St Maryrsquos Hospital London
J R Coll Physicians Lond 200034436ndash44
CM E Septicaem ia ndash I
membrane proteins act as immuno-globulin (Ig)A1 proteases which aidsurviva l of meningococci in themucosa10 In addition the organismdisplays a high level of antigenicvariation during the invasion process1112
that may help it to evade host immunemechanisms
Survival in the bloodstream
The IgA1 proteases reduce the effective-ness of humoral immunity as cleavedinactive IgA1 monomers may competi-tively inhibit binding of IgG and IgM13The polysaccharide capsule providesprotection from both phagocytosis andcomplement mediated lysis14ndash16 Certainsialic acid residues on the capsuleactivate Factor H which has aninhibitory effect on C3b activation in thecomplement system1718
Endotoxin release
Once in the bloodstream the meningo-coccus triggers an intense inflammatoryresponse of which endotoxin is thoughtto be a primary mediator16 Themeningococcus presents an over-whelming immune challenge due torelease of endotoxin-rich membraneblebs from viable bacteria in the blood-stream19 This together with the abilityto grow to high numbers results inhigher concentrations of endotoxinthan in any other infection
Host defence against meningococcal infection
Genetic variation in the host responseto meningococcal infection may play animportant role in the risk of invasivedisease
Complement mediated bacterial lysisis an early step in prevention ofinfection18 This is highlighted by theincreased risk of meningococcal infec-tion in individuals with complementdeficiencies particularly those of theterminal components of the membraneattack pathway and properdindeficiency20ndash22 However the populationattributable risk from these deficienciesis less than 12324 suggesting that
many different factors are important indetermining infection and severity ofdisease Furthermore mannose bindinglectin which binds to the bacterialcapsule also initia tes complementactivation25 and genetic polymor-phisms in this pathway increasesusceptibility to meningococcaldisease26
Mutations in the promoter region ofthe tumour necrosis factor (TNF)-a geneare associated with increased severityand mortality in meningococcaldisease27 Individuals with a poly-morphism associated with high TNF-asecretion have higher mortality Levelsof TNF-a and other pro-inflammatorycytokines such as interleukin (IL)-1b arestrongly associated with diseaseseverity and correlate with endotoxinlevels28ndash30
A key feature of meningococcalsepticaemia is disseminated intra-vascular coagulation (DIC) Levels of thefibrinolysis inhib itor plasminogenactivator inhibitor (PAI)-1 are increasedin response to endotoxin challenge31Levels of PAI-1 in meningococcal sepsiscorrelate with disease severity32 withthe highest levels found in fatalcases3132 A genetic polymorphism inthe PAI-1 gene promoter region associ-ated with increased PAI-1 production ispresent in a significantly higher propor-tion of patients with severe fatalmeningococcal septicaemia than inthose with meningitis or mild disease33
Clinical pathophysiology
The pathophysiology of meningococcalsepticaemia has four majorcomponents3435
capillary leak
intravascular thrombosis (coagu-lopathy)
myocardial dysfunction
metabolic derangements
Capillary leak
A major feature of meningococcal infec-tion is increased vascular permeabilityThe concomitant leakage of plasmafrom the intravascular space leads to
hypovolaemia and reduced preload36This may initially be compensated by anincrease in heart rate and cardiaccontractility but these mechanisms maybe insufficient if the process continueswith resultant impaired tissue perfusion
Coagulopathy
Coagulopathy in meningococcalsepticaemia is characterised by raisedprothrombin and partial thromboplastintimes increased levels of fibrin degra-dation products reduced coagulationfactors and thrombocytopenia Insevere disease this leads to the clinicalpicture of purpura fulminans Thereappears to be an imbalance in the pro-coagulant and anticoagulant pathwaysLevels of anticoagulant factors arereduced including protein C3738 proteinS tissue factor pathway inhibitor andantithrombin I II39 The procoagulantpathway is upregulated with expressionof tissue factor40 and PAI31
Myocardial dysfunction
Acute myocardial dysfunction refractoryto colloid replacement and inotropes isa consistent feature of severe and fatalcases of meningococcal septicaemia41Myocardial failure is associated withdisease severity and prognosis36Studies using invasive monitoring inboth adult humans and animal modelshave shown that cardiac dysfunction insepsis is due to intrinsic depression ofcontractility rather than to reducedmyocardial perfusion4243 Bacterialendotoxin released into plasma leads tothe release of many pro-inflammatorysubstances which inhibit myocardialcontractility including ILs TNF oxygenfree radicals eicosanoids plateletactivating factor and nitric oxide44ndash47 Inaddition the abnormal metabolicenvironment and low circulatingvolume may contribute to acutemyocardial failure
Metabolic derangements
Impaired tissue perfusion leads tometabolic acidosis secondary toimpaired oxidative phosphorylation In
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 437
CM E Sept icaem ia ndash I
addition there is often marked hypo-kalaemia hypocalcaemia and hypo-magnesaemia48ndash52 The mechanisms leadingto these derangements are not clearlydefined
Clinical presentation andmanagement of meningococcal septicaemia
Consequences of meningococcal infectionrange from transient bacteraemia to multi-organ failure refractory shock and death34Other important sequelae include coagu-lopathy and purpura fulminans occasionallynecessitating amputation of digits or limbsEarly recognition and intervention canreduce the risk of death from meningococcalinfection The guidelines for managementpresented below represent the practice of adepartment with extensive clin ical andresearch experience in meningococcal infec-tion The major principles of treatment areelimination of bacteria using antibiotics andcorrection of disordered physiology
Initial assessment
Care should be taken to adhere to advancedlife support guidelines with regard to main-taining support of the airway breathing andcirculation Resuscitation should be guidedby the primary survey of these functionsManagement depends on whether shock orraised intracranial pressure predominates atpresentation as shown in Fig 153
Antibiotics
Although penicillin resistance is rare a third-generation cephalosporin should be givenas soon as the diagnosis of meningococcalinfection is suspected54 This should not bedelayed by diagnostic procedures
Respiratory support
Initially high flow oxygen by face maskshould be given Patients requiring large vol-umes of fluid to restore circulating volume(gt40 mlkg) should be electively intubatedas there is a significant risk of pulmonaryoedema Intubation should be performed ifthere is deterioration in neurological status(Glasgow Coma Score lt8) and in patientswith raised intracranial pressure
438 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
Fig 1 Validated algorithm for the emergency management of meningococcal disease in children (reprinted with permission of the authors (based on a previous version published in Ref 53)) Note This protocol will be distributed in leaflet form bythe Meningitis Research Foundation
CM E Septicaem ia ndash I
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 439
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
CM E Sept icaem ia ndash I
Circulatory support
Early and aggressive fluid resuscitationhas been shown to improve survival55A reduced circulating volume at presen-tation may make it difficult to establishvascular access In order to maintaintissue perfusion and oxygenationcardiac output must be maintainedusing inotropes in severe disease
Initially a 20 mlkg bolus of fluidshould be given56 This may beadequate in mild cases but all patientsshould be carefully monitored fordeterioration due to ongoing capillaryleak Further fluid boluses may berequired using clinical and laboratorysigns to assess the fluid resuscitationThese include capillary refill time heartrate urine output central venouspressure blood pressure and the degreeof metabolic acidosis The optimal fluid
for resuscitation is still debated5758 It islikely that colloidal solutions remain inthe circulation longer than crystalloidsNo artificial colloid solution has beenadequately assessed in children withsepsis and 45 human albumin solu-tion remains our preferred resuscitationfluid
In cases of shock unresponsive to 40mlkg of fluid dilute solutions ofdopamine andor dobutamine may begiven through a peripheral cannulauntil central vascular access is obtainedContinued myocardial dysfunction maynecessitate infusion of adrenaline ornoradrenaline once central access isobtained59
Metabolic corrections
Hypoglycaemia is common and requiresrapid correction Severe shock is often
associated with metabolic acidosiswhich may be partially corrected bycirculating volume and cardiovascularresuscitation The metabolic acidosis inmeningococcal septicaemia is paradoxi-cally associated with hypokalaemiaoften profound and requires closemonitoring and correction Similarlycalcium and magnesium levelscommonly fall and should be correctedin order to improve myocardialperformance
Coagulation support
DIC is a common feature of meningo-coccal septicaemia Depletion of coagu-lation factors fibrinogen and anti-coagulant proteins may be corrected byadministration of fresh frozen plasmaThis may be given as boluses in place of albumin in continuing shockCryoprecipitate is not routinely recom-mended except in severe and persistenthypofibrinogenaemia Platelet adminis-tration may exacerbate and continuethe process of DIC Thrombocytopeniais not routinely corrected unless associ-ated with spontaneous haemorrhageor a platelet count below 20000mm3Heparin does not help to reverseischaemia in sepsis60 Prostacyclin hasbeen anecdotally useful to reversesevere peripheral vasoconstriction inmeningococcal sepsis There is how-ever a risk of severe hypotension andprostacyclin should be considered onlyafter shock has been controlled withvolume replacement and inotropes
Management of raised intracranialpressure in meningococcal infection
Raised intracranial pressure may occurin isolation due to meningitis or coexistwith septic shock This may cause diag-nostic difficulties as the signs may besimilar to shock and impaired brainperfusion Clinical features includedeteriorating levels of consciousnesspupilla ry dilatation or changes inpupillary reflexes hypertension andbradycardia Papilloedema is a late sign
Patients with elevated bloodpressure relative bradycardia anddeteriorating consciousness should be
440 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
Anti inflammatory
Anti-TNF monoclonal antibody Adult sepsis trials ndash mortality reduction not significant
Anti-LPS monoclonal antibody Phase III trial in meningococcal sepsis ndash no benefit
NOS inhibition Adult sepsis trials mdash mortality reduction not significant
rBPI21 A Phase III trial evaluating rBPI21 in children with meningococcal sepsis has been completed Results will be published soon
Recombinant HDL Phase II trial pending
Fibrinolyticantithrombotic
t-PA streptokinase Anecdotal reports ndash no placebo controlled trials
Protein C Data on placebo controlled trial to be released thisyear
Activated protein C A Phase III trial evaluating recombinant human activated Protein C was stopped prematurely due toa significant beneficial effect on mortality and morbidity of the drug over placebo The safety andefficacy of this drug in meningococcal disease is currently being evaluated
Antithrombin III Data on placebo controlled trial to be released thisyear
Other
Haemofiltration
Anecdotal reports mdash no placebo controlled trialsECMO
ECMO = extracorporeal membrane oxygenation HDL = high-density lipoprotein LPS = lipopolysaccharide NOS = nitric oxide synthase rBPI21 = recombinant bactericidalpermeability increasing protein TNF = tumour necrosis factor t-PA = tissue plasminogenactivator
Table 1 Novel therapies for septic shock
CM E Septicaem ia ndash I
treated for raised intracranial pressurewith mannitol frusemide and electiveintubation In addition standardneurointensive care practice such asnursing the patient at 30deg to thehorizontal and with the head midlineshould be maintained
Normal computed tomography (CT)scans do not exclude raised intracranialpressure Thus treatment for raisedintracranial pressure should be initiatedon clinical grounds without awaiting CTresults Lumbar puncture should beavoided in patients with a clinical diag-nosis of meningococcal disease due tothe risks associated with concomitantcoagulopathy intracranial hyper-tension and cardiac and respiratoryinsufficiency
New therapeutic possibilities(Table 1)
Patients with meningococcal infectionhave been given many experimentaltreatments including anti-inflammatoryanti-endotoxin strategies (Fig 2) and
anticoagulantfibrinolytic therapies (Fig3) Until the results of placebo-controlledtrials are available these treatmentsshould be restricted to units specificallyundertaking research in the disease
There have been reports of the useof tissue plasminogen activator andstreptokinase protein C and heparin inpatients with purpura fulminanssecondary to sepsis61ndash64 These agentscarry a significant risk of haemorrhage
Until their role in sepsis is determinedby properly controlled studies routineuse of these agents cannot berecommended65
In experimental models of shockvarious anti-cytokine and anti-endotoxin strategies have seemedpromising but have failed to reducemortality in randomised controlledtrials They included administration ofanti-TNF monoclonal antibodies66 and
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 441
Fig 3 Targets for novel anticoagulant fibr inolytic therapies in meningococcal sepsis Dotted arrows represent anticoagulant solid arrowsprocoagulant (ATIII = antithrombin III FDP = fibrinogen degradation product PAI = plasminogen activator inhibitor TNF = tumour necrosisfactor t-PA = tissue plasminogen activator TFPI = tissue factor plasminogen inhibitor)
Meningococcal endotoxinCD14(LPSreceptor)
Inflammatorycells
Monoclonal anti-TNF
Reactive oxygen species NO
Proinflammatory cytokines(including TNF-a IL-1b)
NOS inhibitors
rBPI21Monoclonal anti-LPS
Fig 2 Targets for novel anti- inflammatory therapies in sepsis(IL = interleukin LPS = lipopolysaccharide NO = nitric oxide NOS = NO synthase rBPI21 = recombinant bactericidal permeabilityincreasing protein TNF = tumour necrosis factor)
CM E Sept icaem ia ndash I
anti-endotoxin (HA-1A) monoclonalantibody67 A trial of the anti-endotoxinagent recombinant bactericidalpermeability increasing protein(rBPI21)68 has been recently completedand the results will be published soonPreliminary data suggest that recombi-nant high-density lipoprotein has anti-endotoxin properties6970 and furtherinvestigation of its clinical benefit isbeing undertaken
Prevention
Community prevention of secondarycases
Chemoprophylaxis for householdcontacts is recommended Other indi-viduals having close physical contactsuch as in day-care centres or kissingcontacts should also receive prophy-lactic treatment Rifampicin is the drugof choice Ciprofloxacin and ceftriaxoneare good but unlicensed alternatives
Medical staff prophylaxis
Chemoprophylaxis is recommended formedical personnel exposed to oralsecretions such as during intubationOther hospital and laboratory personneldo not have an increased risk ofinfection and prophylaxis is notrecommended
Vaccination
At present unconjugated polysaccha-ride vaccines for serogroups A C W-135and Y are available These confer effec-
tive protection for up to three years inchildren over two years old69 The groupB meningococcal polysaccharide closelymimics a human neuronal adhesionmolecule70 and is non-immunogenic Anumber of outer membrane proteinvaccines have been developed whichhave shown efficacy in outbreaks tospecific strains7172 There is currently novaccine that protects against the largenumber of group B strains circulating inthe UK
The introduction in 1999 of a massvaccination programme using a protein-conjugated group C polysaccharideshould reduce the incidence ofmeningococcal disease in the UK by40 However there remains concernthat this vaccine may lead to a shifttowards a higher incidence of group Bdisease Public awareness of thecontinued need for vigilance earlyidentification and management of thedisease is therefore of great importance
Acknowledgements
The authors are grateful to Dr S Faustfor help in construction of the coagula-tion pathway algorithm (Fig 3) also Dr TAli for helpful advice Dr N Pathan isfunded by a British Heart FoundationJunior Research Fellowship
R eferences
1 Platt MJ Child health statistical review1997 Arch Dis Child 199777542ndash8
2 Invasive meningococcal infectionsCommun Dis Rep CDR Wkly 199555
3 Riordan FA Marzouk O Thomson APSills JA Hart CA The changing presenta-
tions of meningococcal disease Eur JPediatr 1995154472ndash4
4 Ramsay M Kaczmarski E Rush MMallard R et al Changing patterns ofcase ascertainment and trends inmeningococcal disease in England andWales Commun Dis Rep CDR Rev19977R49ndash54
5 Lapeyssonnie L La meacuteningite ceacutereacutebro-spinale en Afrique Bull WHO 196328(Suppl 1)3ndash114
6 Moore PS Hierholzer J DeWitt W GouanK et al Respiratory viruses andmycoplasma as cofactors for epidemicgroup A meningococcal meningitis JAMA19902641271ndash5
7 Virji M Kayhty H Ferguson DJAlexandrescu C et al The role of pili inthe interactions of pathogenic Neisseriawith cultured human endothelial cellsMol Microbiol 199151831ndash41
8 Stephens DS McGee ZA Melly MAHoffman LH Gregg CR Attachment ofpathogenic Neisseria to human mucosalsurfaces role in pathogenesis Infection198210192ndash5
9 de Vries FP Cole R Dankert J Frosch Mvan Putten JP Neisseria meningitidisproducing the Opc adhesin bindsepithelial cell proteoglycan receptorsMol Microbiol 1998271203ndash12
10 Vitovski S Read RC Sayers JR Invasiveisolates of Neisseria meningitidis possessenhanced immunoglobulin A1 proteaseactivity compared to colonizing strainsFASEB J 199913331ndash7
11 Nassif X So M Interaction of pathogenicneisseriae with nonphagocytic cells ClinMicrobiol Rev 19958376ndash88
12 de Vries FP Van Der Ende A van PuttenJP Dankert J Invasion of primarynasopharyngeal epithelial cells byNeisseria meningitidis is controlled byphase variation of multiple surface anti-gens Infect Immun 1996642998ndash3006
13 Mulks MH Plaut AG IgA protease pro-duction as a characteristic distinguishingpathogenic from harmless neisseriaceaeN Engl J Med 1978299973ndash6
14 Virji M Makepeace K Peak IR FergusonDJ et al Opc- and pilus-dependent inter-actions of meningococci with humanendothelial cells molecular mechanismsand modulation by surface polysaccha-rides Mol Microbiol 199518741ndash54
15 Vogel U Hammerschmidt S Frosch MSialic acids of both the capsule and thesialylated lipooligosaccharide of Neisseriameningitis serogroup B are prerequisitesfor virulence of meningococci in theinfant rat Med Microbiol Immunol (Berl)199618581ndash7
16 Klein NJ Ison CA Peakman M Levin Met al The influence of capsulation andlipooligosaccharide structure onneutrophil adhesion molecule expres-sion and endothelial injury by Neisseriameningitidis J Infect Dis 1996173172ndash9
17 Estabrook MM Griffiss JM Jarvis GASialylation of Neisseria meningitidislipooligosaccharide inhibits serum
442 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
copy Meningococcal septicaemia has a 10 mortality overall in the UK
copy The major features of meningococcal septicaemia include capillary leak
coagulopathy myocardial dysfunction and metabolic derangements
copy Management should begin with attent ion to airway breathing and circulation
problems
copy Lumbar puncture should not be performed acutely in patients w ith a clinical
diagnosis of meningococcal disease
copy Mass vaccination against group C disease should reduce the incidence of
meningococcal disease by 40 in the UK how ever no vaccination exists for
serogroup B so there is a need for continued vigilance
Key Points
CM E Septicaem ia ndash I
bactericidal activity by masking lacto-N-neotetraose Infect Immun 1997654436ndash44
18 Jarvis GA Vedros NA Sialic acid of groupB Neisseria meningitidis regulates alterna-tive complement pathway activationInfect Immun 198755174ndash80
19 Andersen BM Endotoxin release fromNeisseria meningitidis Relationshipbetween key bacterial characteristics andmeningococcal disease Review Scand JInfect Dis 198964(Suppl)1ndash43
20 Peter G Weigert MB Bissel AR Gold R etal Meningococcal meningitis in familialdeficiency of the fifth component ofcomplement Pediatrics 198167882ndash6
21 Herva E Leinonen M Kayhty H MakelaPH Vetoniemi-Korhonen SL Recurrentmeningococcal meningitis due to partialcomplement defects and poor anti-meningococcal antibody response JInfect 1983655ndash60
22 Sjoholm AG Braconier JH Soderstrom CProperdin deficiency in a family withfulminant meningococcal infections ClinExp Immunol 198250291ndash7
23 Ross SC Densen P Complementdeficiency states and infection epidemi-ology pathogenesis and consequencesof neisserial and other infections in animmune deficiency Medicine (Baltimore)198463243ndash73
24 Ernst T Spath PJ Aebi C Schaad UBBianchetti MG Screening for comple-ment deficiency in bacterial meningitisActa Paediatr 1997861009ndash10
25 Jack DL Dodds AW Anwar N Ison CA etal Activation of complement bymannose-binding lectin on isogenicmutants of Neisseria meningitidisserogroup B J Immunol 19981601346ndash53
26 Hibberd ML Sumiya M Summerfield JABooy R Levin M Association of variantsof the gene for mannose-binding lectinwith susceptibility to meningococca ldisease Lancet 19993531049ndash53
27 Nadel S Newport MJ Booy R Levin MVariation in the tumor necrosis factor-alpha gene promoter region may beassociated with death from meningococ-cal disease J Infect Dis 1996174878ndash80
28 Waage A Halstensen A Espevik TAssociation between tumour necrosisfactor in serum and fatal outcome inpatients with meningococcal diseaseLancet 1987i355ndash7
29 Gardlund B Sjolin J Nilsson A Roll M etal Plasma levels of cytokines in primaryseptic shock in humans correlation withdisease severity J Infect Dis 1995172296ndash301
30 Brandtzaeg P Kierulf P Gaustad PSkulberg A et al Plasma endotoxin as apredictor of multiple organ failure anddeath in systemic meningococca ldisease J Infect Dis 1989159195ndash204
31 Brandtzaeg P Joo GB Brusletto B KierulfP Plasminogen activator inhibitor 1 and2 alpha-2-antiplasmin plasminogenand endotoxin levels in systemic
meningococca l disease Thromb Res199057271ndash8
32 Kornelisse RF Hazelzet JA Savelkoul HFHop WC et al The relationship betweenplasminogen activator inhibitor-1 andproinflammatory and counterinflamma-tory mediators in children with meningo-cocca l septic shock J Infect Dis19961731148ndash56
33 Westendorp RG Hottenga JJ SlagboomPE Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococ-cal septic shock Lancet 1999354561ndash3
34 Flaegstad T Kaaresen PI Stokland TGutteberg T Factors associated with fataloutcome in childhood meningococcaldisease Acta Paediatr 1995841137ndash42
35 LeClerc F Beuscart R Guillo is BDiependaele JF et al Prognostic factorsof severe infectious purpura in childrenIntensive Care Med 198511140ndash3
36 Mercier JC Beaufils F Hartmann JFAzema D Hemodynamic patterns ofmeningococcal shock in children CritCare Med 19881627ndash33
37 Fijnvandraat K Peters M Derkx B VanDeventer S ten Cate JW Endotoxininduced coagulation activation andprotein C reduction in meningococcalseptic shock Prog Clin Biol Res1994388247ndash54
38 Fijnvandraat K Derkx B Peters M BijlmerR et al Coagulation activation and tissuenecrosis in meningococcal septic shockseverely reduced protein C levels predicta high mortality Thromb Haemost19957315ndash20
39 Brandtzaeg P Sandset PM Joo GBOvstebo R et al The quantitative associ-ation of plasma endotoxin antithrombinprotein C extrinsic pathway inhibitor andfibrinopeptide A in systemic meningococ-cal disease Thromb Res 198955459ndash70
40 Heyderman RS Klein NJ Daramola OAHammerschmidt S et al Induction ofhuman endothelial tissue factor expres-sion by Neisseria meningitidis the influ-ence of bacterial killing and adherenceto the endothelium Microb Pathog199722265ndash74
41 Monsalve F Rucabadol L Salvador ABonastre J et al Myocardial depressionin septic shock caused by meningococcalinfection Crit Care Med 1984121021ndash3
42 Cunnion RE Schaer GL Parker MMNatanson C Parrillo JE The coronarycirculation in human septic shockCirculation 198673637ndash44
43 Dhainaut JF Huyghebaert MF MonsallierJF Lefevre G et al Coronary hemo-dynamics and myocardial metabolism oflactate free fatty acids glucose andketones in patients with septic shockCirculation 198775533ndash41
44 Parrillo JE Burch C Shelhamer JH ParkerMM et al A circulating myocardialdepressant substance in humans withseptic shock J Clin Invest 1985761539ndash53
45 Hazelzet JA van der Voort E LindemansJ ter Heerdt PJ Neijens HJ Relation
between cytokines and routinelaboratory data in children with septicshock and purpura Intensive Care Med199420371ndash4
46 van Deuren M van der Ven-Jongekrijg JBartelink AK van Dalen R et alCorrelation between proinflammatorycytokines and antiinflammatorymediators and the severity of disease inmeningococcal infections J Infect Dis1995172433ndash9
47 Visser JJ Scholten RJ Hoekman K Nitricoxide synthesis in meningococcal menin-gitis Ann Intern Med 1994120345ndash6
48 Khilnani P Electrolyte abnormalities incritically ill children Crit Care Med199220241ndash50
49 Chernow B Calcium does it have atherapeutic role in sepsis Crit Care Med199018895ndash6
50 Gauthier B Trachtman H Di Carmine FUrivetsky M et al Hypocalcemia andhypercalcitoninemia in critically illchildren Crit Care Med 1990181215ndash9
51 Mauger DC Hypokalaemia as a consis-tent feature of fulminant meningococcalsepticaemia Aust Paediatr J 1971784ndash6
52 Weisinger JR Bellorin-Font E Magnesiumand phosphorus Lancet 1998352391ndash6
53 Pollard AJ Britto J Nadel S de Munter Cet al Emergency management ofmeningococcal disease Arch Dis Child199980290ndash6
54 Neu HC Cephalosporins in the treatmentof meningitis Drugs 198734(Suppl2)135ndash53
55 Carcillo JA Davis AL Zaritsky A Role ofearly fluid resuscitation in pediatric septicshock JAMA 19912661242ndash5
56 Dula DJ Lutz P Vogel MF Weaver BNRapid flow rates for the resuscitation ofhypovolemic shock Ann Emerg Med198514303ndash6
57 Nadel S De Munter C Britto J Levin MHabibi P Albumin saint or sinner ArchDis Child 199879384ndash5
58 Human albumin administration in criti-cally ill patients systematic review ofrandomised controlled trials CochraneInjuries Group Albumin Reviewers BrMed J 1998317235ndash40
59 Tobin JR Wetzel RC Shock and multi-organ failure In Rogers MC (ed)Textbook of pediatric intensive careBaltimore Williams and Wilkins1996555ndash605
60 Haneberg B Gutterberg TJ Moe PJOsterud B et al Heparin for infants andchildren with meningococcal septicemiaResults of a randomized therapeutic trialNIPH Ann 1983643ndash7
61 Zenz W Muntean W Zobel G GrubbauerHM Gallistl S Treatment of fulminantmeningococcemia with recombinanttissue plasminogen activator ThrombHaemost 199574802ndash3
62 Keeley SR Matthews NT Buist M Tissueplasminogen activator for gangrene infulminant meningococcaemia Lancet19913371359
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 443
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F

CM E Septicaem ia ndash I
membrane proteins act as immuno-globulin (Ig)A1 proteases which aidsurviva l of meningococci in themucosa10 In addition the organismdisplays a high level of antigenicvariation during the invasion process1112
that may help it to evade host immunemechanisms
Survival in the bloodstream
The IgA1 proteases reduce the effective-ness of humoral immunity as cleavedinactive IgA1 monomers may competi-tively inhibit binding of IgG and IgM13The polysaccharide capsule providesprotection from both phagocytosis andcomplement mediated lysis14ndash16 Certainsialic acid residues on the capsuleactivate Factor H which has aninhibitory effect on C3b activation in thecomplement system1718
Endotoxin release
Once in the bloodstream the meningo-coccus triggers an intense inflammatoryresponse of which endotoxin is thoughtto be a primary mediator16 Themeningococcus presents an over-whelming immune challenge due torelease of endotoxin-rich membraneblebs from viable bacteria in the blood-stream19 This together with the abilityto grow to high numbers results inhigher concentrations of endotoxinthan in any other infection
Host defence against meningococcal infection
Genetic variation in the host responseto meningococcal infection may play animportant role in the risk of invasivedisease
Complement mediated bacterial lysisis an early step in prevention ofinfection18 This is highlighted by theincreased risk of meningococcal infec-tion in individuals with complementdeficiencies particularly those of theterminal components of the membraneattack pathway and properdindeficiency20ndash22 However the populationattributable risk from these deficienciesis less than 12324 suggesting that
many different factors are important indetermining infection and severity ofdisease Furthermore mannose bindinglectin which binds to the bacterialcapsule also initia tes complementactivation25 and genetic polymor-phisms in this pathway increasesusceptibility to meningococcaldisease26
Mutations in the promoter region ofthe tumour necrosis factor (TNF)-a geneare associated with increased severityand mortality in meningococcaldisease27 Individuals with a poly-morphism associated with high TNF-asecretion have higher mortality Levelsof TNF-a and other pro-inflammatorycytokines such as interleukin (IL)-1b arestrongly associated with diseaseseverity and correlate with endotoxinlevels28ndash30
A key feature of meningococcalsepticaemia is disseminated intra-vascular coagulation (DIC) Levels of thefibrinolysis inhib itor plasminogenactivator inhibitor (PAI)-1 are increasedin response to endotoxin challenge31Levels of PAI-1 in meningococcal sepsiscorrelate with disease severity32 withthe highest levels found in fatalcases3132 A genetic polymorphism inthe PAI-1 gene promoter region associ-ated with increased PAI-1 production ispresent in a significantly higher propor-tion of patients with severe fatalmeningococcal septicaemia than inthose with meningitis or mild disease33
Clinical pathophysiology
The pathophysiology of meningococcalsepticaemia has four majorcomponents3435
capillary leak
intravascular thrombosis (coagu-lopathy)
myocardial dysfunction
metabolic derangements
Capillary leak
A major feature of meningococcal infec-tion is increased vascular permeabilityThe concomitant leakage of plasmafrom the intravascular space leads to
hypovolaemia and reduced preload36This may initially be compensated by anincrease in heart rate and cardiaccontractility but these mechanisms maybe insufficient if the process continueswith resultant impaired tissue perfusion
Coagulopathy
Coagulopathy in meningococcalsepticaemia is characterised by raisedprothrombin and partial thromboplastintimes increased levels of fibrin degra-dation products reduced coagulationfactors and thrombocytopenia Insevere disease this leads to the clinicalpicture of purpura fulminans Thereappears to be an imbalance in the pro-coagulant and anticoagulant pathwaysLevels of anticoagulant factors arereduced including protein C3738 proteinS tissue factor pathway inhibitor andantithrombin I II39 The procoagulantpathway is upregulated with expressionof tissue factor40 and PAI31
Myocardial dysfunction
Acute myocardial dysfunction refractoryto colloid replacement and inotropes isa consistent feature of severe and fatalcases of meningococcal septicaemia41Myocardial failure is associated withdisease severity and prognosis36Studies using invasive monitoring inboth adult humans and animal modelshave shown that cardiac dysfunction insepsis is due to intrinsic depression ofcontractility rather than to reducedmyocardial perfusion4243 Bacterialendotoxin released into plasma leads tothe release of many pro-inflammatorysubstances which inhibit myocardialcontractility including ILs TNF oxygenfree radicals eicosanoids plateletactivating factor and nitric oxide44ndash47 Inaddition the abnormal metabolicenvironment and low circulatingvolume may contribute to acutemyocardial failure
Metabolic derangements
Impaired tissue perfusion leads tometabolic acidosis secondary toimpaired oxidative phosphorylation In
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 437
CM E Sept icaem ia ndash I
addition there is often marked hypo-kalaemia hypocalcaemia and hypo-magnesaemia48ndash52 The mechanisms leadingto these derangements are not clearlydefined
Clinical presentation andmanagement of meningococcal septicaemia
Consequences of meningococcal infectionrange from transient bacteraemia to multi-organ failure refractory shock and death34Other important sequelae include coagu-lopathy and purpura fulminans occasionallynecessitating amputation of digits or limbsEarly recognition and intervention canreduce the risk of death from meningococcalinfection The guidelines for managementpresented below represent the practice of adepartment with extensive clin ical andresearch experience in meningococcal infec-tion The major principles of treatment areelimination of bacteria using antibiotics andcorrection of disordered physiology
Initial assessment
Care should be taken to adhere to advancedlife support guidelines with regard to main-taining support of the airway breathing andcirculation Resuscitation should be guidedby the primary survey of these functionsManagement depends on whether shock orraised intracranial pressure predominates atpresentation as shown in Fig 153
Antibiotics
Although penicillin resistance is rare a third-generation cephalosporin should be givenas soon as the diagnosis of meningococcalinfection is suspected54 This should not bedelayed by diagnostic procedures
Respiratory support
Initially high flow oxygen by face maskshould be given Patients requiring large vol-umes of fluid to restore circulating volume(gt40 mlkg) should be electively intubatedas there is a significant risk of pulmonaryoedema Intubation should be performed ifthere is deterioration in neurological status(Glasgow Coma Score lt8) and in patientswith raised intracranial pressure
438 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
Fig 1 Validated algorithm for the emergency management of meningococcal disease in children (reprinted with permission of the authors (based on a previous version published in Ref 53)) Note This protocol will be distributed in leaflet form bythe Meningitis Research Foundation
CM E Septicaem ia ndash I
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 439
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
CM E Sept icaem ia ndash I
Circulatory support
Early and aggressive fluid resuscitationhas been shown to improve survival55A reduced circulating volume at presen-tation may make it difficult to establishvascular access In order to maintaintissue perfusion and oxygenationcardiac output must be maintainedusing inotropes in severe disease
Initially a 20 mlkg bolus of fluidshould be given56 This may beadequate in mild cases but all patientsshould be carefully monitored fordeterioration due to ongoing capillaryleak Further fluid boluses may berequired using clinical and laboratorysigns to assess the fluid resuscitationThese include capillary refill time heartrate urine output central venouspressure blood pressure and the degreeof metabolic acidosis The optimal fluid
for resuscitation is still debated5758 It islikely that colloidal solutions remain inthe circulation longer than crystalloidsNo artificial colloid solution has beenadequately assessed in children withsepsis and 45 human albumin solu-tion remains our preferred resuscitationfluid
In cases of shock unresponsive to 40mlkg of fluid dilute solutions ofdopamine andor dobutamine may begiven through a peripheral cannulauntil central vascular access is obtainedContinued myocardial dysfunction maynecessitate infusion of adrenaline ornoradrenaline once central access isobtained59
Metabolic corrections
Hypoglycaemia is common and requiresrapid correction Severe shock is often
associated with metabolic acidosiswhich may be partially corrected bycirculating volume and cardiovascularresuscitation The metabolic acidosis inmeningococcal septicaemia is paradoxi-cally associated with hypokalaemiaoften profound and requires closemonitoring and correction Similarlycalcium and magnesium levelscommonly fall and should be correctedin order to improve myocardialperformance
Coagulation support
DIC is a common feature of meningo-coccal septicaemia Depletion of coagu-lation factors fibrinogen and anti-coagulant proteins may be corrected byadministration of fresh frozen plasmaThis may be given as boluses in place of albumin in continuing shockCryoprecipitate is not routinely recom-mended except in severe and persistenthypofibrinogenaemia Platelet adminis-tration may exacerbate and continuethe process of DIC Thrombocytopeniais not routinely corrected unless associ-ated with spontaneous haemorrhageor a platelet count below 20000mm3Heparin does not help to reverseischaemia in sepsis60 Prostacyclin hasbeen anecdotally useful to reversesevere peripheral vasoconstriction inmeningococcal sepsis There is how-ever a risk of severe hypotension andprostacyclin should be considered onlyafter shock has been controlled withvolume replacement and inotropes
Management of raised intracranialpressure in meningococcal infection
Raised intracranial pressure may occurin isolation due to meningitis or coexistwith septic shock This may cause diag-nostic difficulties as the signs may besimilar to shock and impaired brainperfusion Clinical features includedeteriorating levels of consciousnesspupilla ry dilatation or changes inpupillary reflexes hypertension andbradycardia Papilloedema is a late sign
Patients with elevated bloodpressure relative bradycardia anddeteriorating consciousness should be
440 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
Anti inflammatory
Anti-TNF monoclonal antibody Adult sepsis trials ndash mortality reduction not significant
Anti-LPS monoclonal antibody Phase III trial in meningococcal sepsis ndash no benefit
NOS inhibition Adult sepsis trials mdash mortality reduction not significant
rBPI21 A Phase III trial evaluating rBPI21 in children with meningococcal sepsis has been completed Results will be published soon
Recombinant HDL Phase II trial pending
Fibrinolyticantithrombotic
t-PA streptokinase Anecdotal reports ndash no placebo controlled trials
Protein C Data on placebo controlled trial to be released thisyear
Activated protein C A Phase III trial evaluating recombinant human activated Protein C was stopped prematurely due toa significant beneficial effect on mortality and morbidity of the drug over placebo The safety andefficacy of this drug in meningococcal disease is currently being evaluated
Antithrombin III Data on placebo controlled trial to be released thisyear
Other
Haemofiltration
Anecdotal reports mdash no placebo controlled trialsECMO
ECMO = extracorporeal membrane oxygenation HDL = high-density lipoprotein LPS = lipopolysaccharide NOS = nitric oxide synthase rBPI21 = recombinant bactericidalpermeability increasing protein TNF = tumour necrosis factor t-PA = tissue plasminogenactivator
Table 1 Novel therapies for septic shock
CM E Septicaem ia ndash I
treated for raised intracranial pressurewith mannitol frusemide and electiveintubation In addition standardneurointensive care practice such asnursing the patient at 30deg to thehorizontal and with the head midlineshould be maintained
Normal computed tomography (CT)scans do not exclude raised intracranialpressure Thus treatment for raisedintracranial pressure should be initiatedon clinical grounds without awaiting CTresults Lumbar puncture should beavoided in patients with a clinical diag-nosis of meningococcal disease due tothe risks associated with concomitantcoagulopathy intracranial hyper-tension and cardiac and respiratoryinsufficiency
New therapeutic possibilities(Table 1)
Patients with meningococcal infectionhave been given many experimentaltreatments including anti-inflammatoryanti-endotoxin strategies (Fig 2) and
anticoagulantfibrinolytic therapies (Fig3) Until the results of placebo-controlledtrials are available these treatmentsshould be restricted to units specificallyundertaking research in the disease
There have been reports of the useof tissue plasminogen activator andstreptokinase protein C and heparin inpatients with purpura fulminanssecondary to sepsis61ndash64 These agentscarry a significant risk of haemorrhage
Until their role in sepsis is determinedby properly controlled studies routineuse of these agents cannot berecommended65
In experimental models of shockvarious anti-cytokine and anti-endotoxin strategies have seemedpromising but have failed to reducemortality in randomised controlledtrials They included administration ofanti-TNF monoclonal antibodies66 and
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 441
Fig 3 Targets for novel anticoagulant fibr inolytic therapies in meningococcal sepsis Dotted arrows represent anticoagulant solid arrowsprocoagulant (ATIII = antithrombin III FDP = fibrinogen degradation product PAI = plasminogen activator inhibitor TNF = tumour necrosisfactor t-PA = tissue plasminogen activator TFPI = tissue factor plasminogen inhibitor)
Meningococcal endotoxinCD14(LPSreceptor)
Inflammatorycells
Monoclonal anti-TNF
Reactive oxygen species NO
Proinflammatory cytokines(including TNF-a IL-1b)
NOS inhibitors
rBPI21Monoclonal anti-LPS
Fig 2 Targets for novel anti- inflammatory therapies in sepsis(IL = interleukin LPS = lipopolysaccharide NO = nitric oxide NOS = NO synthase rBPI21 = recombinant bactericidal permeabilityincreasing protein TNF = tumour necrosis factor)
CM E Sept icaem ia ndash I
anti-endotoxin (HA-1A) monoclonalantibody67 A trial of the anti-endotoxinagent recombinant bactericidalpermeability increasing protein(rBPI21)68 has been recently completedand the results will be published soonPreliminary data suggest that recombi-nant high-density lipoprotein has anti-endotoxin properties6970 and furtherinvestigation of its clinical benefit isbeing undertaken
Prevention
Community prevention of secondarycases
Chemoprophylaxis for householdcontacts is recommended Other indi-viduals having close physical contactsuch as in day-care centres or kissingcontacts should also receive prophy-lactic treatment Rifampicin is the drugof choice Ciprofloxacin and ceftriaxoneare good but unlicensed alternatives
Medical staff prophylaxis
Chemoprophylaxis is recommended formedical personnel exposed to oralsecretions such as during intubationOther hospital and laboratory personneldo not have an increased risk ofinfection and prophylaxis is notrecommended
Vaccination
At present unconjugated polysaccha-ride vaccines for serogroups A C W-135and Y are available These confer effec-
tive protection for up to three years inchildren over two years old69 The groupB meningococcal polysaccharide closelymimics a human neuronal adhesionmolecule70 and is non-immunogenic Anumber of outer membrane proteinvaccines have been developed whichhave shown efficacy in outbreaks tospecific strains7172 There is currently novaccine that protects against the largenumber of group B strains circulating inthe UK
The introduction in 1999 of a massvaccination programme using a protein-conjugated group C polysaccharideshould reduce the incidence ofmeningococcal disease in the UK by40 However there remains concernthat this vaccine may lead to a shifttowards a higher incidence of group Bdisease Public awareness of thecontinued need for vigilance earlyidentification and management of thedisease is therefore of great importance
Acknowledgements
The authors are grateful to Dr S Faustfor help in construction of the coagula-tion pathway algorithm (Fig 3) also Dr TAli for helpful advice Dr N Pathan isfunded by a British Heart FoundationJunior Research Fellowship
R eferences
1 Platt MJ Child health statistical review1997 Arch Dis Child 199777542ndash8
2 Invasive meningococcal infectionsCommun Dis Rep CDR Wkly 199555
3 Riordan FA Marzouk O Thomson APSills JA Hart CA The changing presenta-
tions of meningococcal disease Eur JPediatr 1995154472ndash4
4 Ramsay M Kaczmarski E Rush MMallard R et al Changing patterns ofcase ascertainment and trends inmeningococcal disease in England andWales Commun Dis Rep CDR Rev19977R49ndash54
5 Lapeyssonnie L La meacuteningite ceacutereacutebro-spinale en Afrique Bull WHO 196328(Suppl 1)3ndash114
6 Moore PS Hierholzer J DeWitt W GouanK et al Respiratory viruses andmycoplasma as cofactors for epidemicgroup A meningococcal meningitis JAMA19902641271ndash5
7 Virji M Kayhty H Ferguson DJAlexandrescu C et al The role of pili inthe interactions of pathogenic Neisseriawith cultured human endothelial cellsMol Microbiol 199151831ndash41
8 Stephens DS McGee ZA Melly MAHoffman LH Gregg CR Attachment ofpathogenic Neisseria to human mucosalsurfaces role in pathogenesis Infection198210192ndash5
9 de Vries FP Cole R Dankert J Frosch Mvan Putten JP Neisseria meningitidisproducing the Opc adhesin bindsepithelial cell proteoglycan receptorsMol Microbiol 1998271203ndash12
10 Vitovski S Read RC Sayers JR Invasiveisolates of Neisseria meningitidis possessenhanced immunoglobulin A1 proteaseactivity compared to colonizing strainsFASEB J 199913331ndash7
11 Nassif X So M Interaction of pathogenicneisseriae with nonphagocytic cells ClinMicrobiol Rev 19958376ndash88
12 de Vries FP Van Der Ende A van PuttenJP Dankert J Invasion of primarynasopharyngeal epithelial cells byNeisseria meningitidis is controlled byphase variation of multiple surface anti-gens Infect Immun 1996642998ndash3006
13 Mulks MH Plaut AG IgA protease pro-duction as a characteristic distinguishingpathogenic from harmless neisseriaceaeN Engl J Med 1978299973ndash6
14 Virji M Makepeace K Peak IR FergusonDJ et al Opc- and pilus-dependent inter-actions of meningococci with humanendothelial cells molecular mechanismsand modulation by surface polysaccha-rides Mol Microbiol 199518741ndash54
15 Vogel U Hammerschmidt S Frosch MSialic acids of both the capsule and thesialylated lipooligosaccharide of Neisseriameningitis serogroup B are prerequisitesfor virulence of meningococci in theinfant rat Med Microbiol Immunol (Berl)199618581ndash7
16 Klein NJ Ison CA Peakman M Levin Met al The influence of capsulation andlipooligosaccharide structure onneutrophil adhesion molecule expres-sion and endothelial injury by Neisseriameningitidis J Infect Dis 1996173172ndash9
17 Estabrook MM Griffiss JM Jarvis GASialylation of Neisseria meningitidislipooligosaccharide inhibits serum
442 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
copy Meningococcal septicaemia has a 10 mortality overall in the UK
copy The major features of meningococcal septicaemia include capillary leak
coagulopathy myocardial dysfunction and metabolic derangements
copy Management should begin with attent ion to airway breathing and circulation
problems
copy Lumbar puncture should not be performed acutely in patients w ith a clinical
diagnosis of meningococcal disease
copy Mass vaccination against group C disease should reduce the incidence of
meningococcal disease by 40 in the UK how ever no vaccination exists for
serogroup B so there is a need for continued vigilance
Key Points
CM E Septicaem ia ndash I
bactericidal activity by masking lacto-N-neotetraose Infect Immun 1997654436ndash44
18 Jarvis GA Vedros NA Sialic acid of groupB Neisseria meningitidis regulates alterna-tive complement pathway activationInfect Immun 198755174ndash80
19 Andersen BM Endotoxin release fromNeisseria meningitidis Relationshipbetween key bacterial characteristics andmeningococcal disease Review Scand JInfect Dis 198964(Suppl)1ndash43
20 Peter G Weigert MB Bissel AR Gold R etal Meningococcal meningitis in familialdeficiency of the fifth component ofcomplement Pediatrics 198167882ndash6
21 Herva E Leinonen M Kayhty H MakelaPH Vetoniemi-Korhonen SL Recurrentmeningococcal meningitis due to partialcomplement defects and poor anti-meningococcal antibody response JInfect 1983655ndash60
22 Sjoholm AG Braconier JH Soderstrom CProperdin deficiency in a family withfulminant meningococcal infections ClinExp Immunol 198250291ndash7
23 Ross SC Densen P Complementdeficiency states and infection epidemi-ology pathogenesis and consequencesof neisserial and other infections in animmune deficiency Medicine (Baltimore)198463243ndash73
24 Ernst T Spath PJ Aebi C Schaad UBBianchetti MG Screening for comple-ment deficiency in bacterial meningitisActa Paediatr 1997861009ndash10
25 Jack DL Dodds AW Anwar N Ison CA etal Activation of complement bymannose-binding lectin on isogenicmutants of Neisseria meningitidisserogroup B J Immunol 19981601346ndash53
26 Hibberd ML Sumiya M Summerfield JABooy R Levin M Association of variantsof the gene for mannose-binding lectinwith susceptibility to meningococca ldisease Lancet 19993531049ndash53
27 Nadel S Newport MJ Booy R Levin MVariation in the tumor necrosis factor-alpha gene promoter region may beassociated with death from meningococ-cal disease J Infect Dis 1996174878ndash80
28 Waage A Halstensen A Espevik TAssociation between tumour necrosisfactor in serum and fatal outcome inpatients with meningococcal diseaseLancet 1987i355ndash7
29 Gardlund B Sjolin J Nilsson A Roll M etal Plasma levels of cytokines in primaryseptic shock in humans correlation withdisease severity J Infect Dis 1995172296ndash301
30 Brandtzaeg P Kierulf P Gaustad PSkulberg A et al Plasma endotoxin as apredictor of multiple organ failure anddeath in systemic meningococca ldisease J Infect Dis 1989159195ndash204
31 Brandtzaeg P Joo GB Brusletto B KierulfP Plasminogen activator inhibitor 1 and2 alpha-2-antiplasmin plasminogenand endotoxin levels in systemic
meningococca l disease Thromb Res199057271ndash8
32 Kornelisse RF Hazelzet JA Savelkoul HFHop WC et al The relationship betweenplasminogen activator inhibitor-1 andproinflammatory and counterinflamma-tory mediators in children with meningo-cocca l septic shock J Infect Dis19961731148ndash56
33 Westendorp RG Hottenga JJ SlagboomPE Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococ-cal septic shock Lancet 1999354561ndash3
34 Flaegstad T Kaaresen PI Stokland TGutteberg T Factors associated with fataloutcome in childhood meningococcaldisease Acta Paediatr 1995841137ndash42
35 LeClerc F Beuscart R Guillo is BDiependaele JF et al Prognostic factorsof severe infectious purpura in childrenIntensive Care Med 198511140ndash3
36 Mercier JC Beaufils F Hartmann JFAzema D Hemodynamic patterns ofmeningococcal shock in children CritCare Med 19881627ndash33
37 Fijnvandraat K Peters M Derkx B VanDeventer S ten Cate JW Endotoxininduced coagulation activation andprotein C reduction in meningococcalseptic shock Prog Clin Biol Res1994388247ndash54
38 Fijnvandraat K Derkx B Peters M BijlmerR et al Coagulation activation and tissuenecrosis in meningococcal septic shockseverely reduced protein C levels predicta high mortality Thromb Haemost19957315ndash20
39 Brandtzaeg P Sandset PM Joo GBOvstebo R et al The quantitative associ-ation of plasma endotoxin antithrombinprotein C extrinsic pathway inhibitor andfibrinopeptide A in systemic meningococ-cal disease Thromb Res 198955459ndash70
40 Heyderman RS Klein NJ Daramola OAHammerschmidt S et al Induction ofhuman endothelial tissue factor expres-sion by Neisseria meningitidis the influ-ence of bacterial killing and adherenceto the endothelium Microb Pathog199722265ndash74
41 Monsalve F Rucabadol L Salvador ABonastre J et al Myocardial depressionin septic shock caused by meningococcalinfection Crit Care Med 1984121021ndash3
42 Cunnion RE Schaer GL Parker MMNatanson C Parrillo JE The coronarycirculation in human septic shockCirculation 198673637ndash44
43 Dhainaut JF Huyghebaert MF MonsallierJF Lefevre G et al Coronary hemo-dynamics and myocardial metabolism oflactate free fatty acids glucose andketones in patients with septic shockCirculation 198775533ndash41
44 Parrillo JE Burch C Shelhamer JH ParkerMM et al A circulating myocardialdepressant substance in humans withseptic shock J Clin Invest 1985761539ndash53
45 Hazelzet JA van der Voort E LindemansJ ter Heerdt PJ Neijens HJ Relation
between cytokines and routinelaboratory data in children with septicshock and purpura Intensive Care Med199420371ndash4
46 van Deuren M van der Ven-Jongekrijg JBartelink AK van Dalen R et alCorrelation between proinflammatorycytokines and antiinflammatorymediators and the severity of disease inmeningococcal infections J Infect Dis1995172433ndash9
47 Visser JJ Scholten RJ Hoekman K Nitricoxide synthesis in meningococcal menin-gitis Ann Intern Med 1994120345ndash6
48 Khilnani P Electrolyte abnormalities incritically ill children Crit Care Med199220241ndash50
49 Chernow B Calcium does it have atherapeutic role in sepsis Crit Care Med199018895ndash6
50 Gauthier B Trachtman H Di Carmine FUrivetsky M et al Hypocalcemia andhypercalcitoninemia in critically illchildren Crit Care Med 1990181215ndash9
51 Mauger DC Hypokalaemia as a consis-tent feature of fulminant meningococcalsepticaemia Aust Paediatr J 1971784ndash6
52 Weisinger JR Bellorin-Font E Magnesiumand phosphorus Lancet 1998352391ndash6
53 Pollard AJ Britto J Nadel S de Munter Cet al Emergency management ofmeningococcal disease Arch Dis Child199980290ndash6
54 Neu HC Cephalosporins in the treatmentof meningitis Drugs 198734(Suppl2)135ndash53
55 Carcillo JA Davis AL Zaritsky A Role ofearly fluid resuscitation in pediatric septicshock JAMA 19912661242ndash5
56 Dula DJ Lutz P Vogel MF Weaver BNRapid flow rates for the resuscitation ofhypovolemic shock Ann Emerg Med198514303ndash6
57 Nadel S De Munter C Britto J Levin MHabibi P Albumin saint or sinner ArchDis Child 199879384ndash5
58 Human albumin administration in criti-cally ill patients systematic review ofrandomised controlled trials CochraneInjuries Group Albumin Reviewers BrMed J 1998317235ndash40
59 Tobin JR Wetzel RC Shock and multi-organ failure In Rogers MC (ed)Textbook of pediatric intensive careBaltimore Williams and Wilkins1996555ndash605
60 Haneberg B Gutterberg TJ Moe PJOsterud B et al Heparin for infants andchildren with meningococcal septicemiaResults of a randomized therapeutic trialNIPH Ann 1983643ndash7
61 Zenz W Muntean W Zobel G GrubbauerHM Gallistl S Treatment of fulminantmeningococcemia with recombinanttissue plasminogen activator ThrombHaemost 199574802ndash3
62 Keeley SR Matthews NT Buist M Tissueplasminogen activator for gangrene infulminant meningococcaemia Lancet19913371359
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 443
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F

CM E Sept icaem ia ndash I
addition there is often marked hypo-kalaemia hypocalcaemia and hypo-magnesaemia48ndash52 The mechanisms leadingto these derangements are not clearlydefined
Clinical presentation andmanagement of meningococcal septicaemia
Consequences of meningococcal infectionrange from transient bacteraemia to multi-organ failure refractory shock and death34Other important sequelae include coagu-lopathy and purpura fulminans occasionallynecessitating amputation of digits or limbsEarly recognition and intervention canreduce the risk of death from meningococcalinfection The guidelines for managementpresented below represent the practice of adepartment with extensive clin ical andresearch experience in meningococcal infec-tion The major principles of treatment areelimination of bacteria using antibiotics andcorrection of disordered physiology
Initial assessment
Care should be taken to adhere to advancedlife support guidelines with regard to main-taining support of the airway breathing andcirculation Resuscitation should be guidedby the primary survey of these functionsManagement depends on whether shock orraised intracranial pressure predominates atpresentation as shown in Fig 153
Antibiotics
Although penicillin resistance is rare a third-generation cephalosporin should be givenas soon as the diagnosis of meningococcalinfection is suspected54 This should not bedelayed by diagnostic procedures
Respiratory support
Initially high flow oxygen by face maskshould be given Patients requiring large vol-umes of fluid to restore circulating volume(gt40 mlkg) should be electively intubatedas there is a significant risk of pulmonaryoedema Intubation should be performed ifthere is deterioration in neurological status(Glasgow Coma Score lt8) and in patientswith raised intracranial pressure
438 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
Fig 1 Validated algorithm for the emergency management of meningococcal disease in children (reprinted with permission of the authors (based on a previous version published in Ref 53)) Note This protocol will be distributed in leaflet form bythe Meningitis Research Foundation
CM E Septicaem ia ndash I
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 439
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
CM E Sept icaem ia ndash I
Circulatory support
Early and aggressive fluid resuscitationhas been shown to improve survival55A reduced circulating volume at presen-tation may make it difficult to establishvascular access In order to maintaintissue perfusion and oxygenationcardiac output must be maintainedusing inotropes in severe disease
Initially a 20 mlkg bolus of fluidshould be given56 This may beadequate in mild cases but all patientsshould be carefully monitored fordeterioration due to ongoing capillaryleak Further fluid boluses may berequired using clinical and laboratorysigns to assess the fluid resuscitationThese include capillary refill time heartrate urine output central venouspressure blood pressure and the degreeof metabolic acidosis The optimal fluid
for resuscitation is still debated5758 It islikely that colloidal solutions remain inthe circulation longer than crystalloidsNo artificial colloid solution has beenadequately assessed in children withsepsis and 45 human albumin solu-tion remains our preferred resuscitationfluid
In cases of shock unresponsive to 40mlkg of fluid dilute solutions ofdopamine andor dobutamine may begiven through a peripheral cannulauntil central vascular access is obtainedContinued myocardial dysfunction maynecessitate infusion of adrenaline ornoradrenaline once central access isobtained59
Metabolic corrections
Hypoglycaemia is common and requiresrapid correction Severe shock is often
associated with metabolic acidosiswhich may be partially corrected bycirculating volume and cardiovascularresuscitation The metabolic acidosis inmeningococcal septicaemia is paradoxi-cally associated with hypokalaemiaoften profound and requires closemonitoring and correction Similarlycalcium and magnesium levelscommonly fall and should be correctedin order to improve myocardialperformance
Coagulation support
DIC is a common feature of meningo-coccal septicaemia Depletion of coagu-lation factors fibrinogen and anti-coagulant proteins may be corrected byadministration of fresh frozen plasmaThis may be given as boluses in place of albumin in continuing shockCryoprecipitate is not routinely recom-mended except in severe and persistenthypofibrinogenaemia Platelet adminis-tration may exacerbate and continuethe process of DIC Thrombocytopeniais not routinely corrected unless associ-ated with spontaneous haemorrhageor a platelet count below 20000mm3Heparin does not help to reverseischaemia in sepsis60 Prostacyclin hasbeen anecdotally useful to reversesevere peripheral vasoconstriction inmeningococcal sepsis There is how-ever a risk of severe hypotension andprostacyclin should be considered onlyafter shock has been controlled withvolume replacement and inotropes
Management of raised intracranialpressure in meningococcal infection
Raised intracranial pressure may occurin isolation due to meningitis or coexistwith septic shock This may cause diag-nostic difficulties as the signs may besimilar to shock and impaired brainperfusion Clinical features includedeteriorating levels of consciousnesspupilla ry dilatation or changes inpupillary reflexes hypertension andbradycardia Papilloedema is a late sign
Patients with elevated bloodpressure relative bradycardia anddeteriorating consciousness should be
440 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
Anti inflammatory
Anti-TNF monoclonal antibody Adult sepsis trials ndash mortality reduction not significant
Anti-LPS monoclonal antibody Phase III trial in meningococcal sepsis ndash no benefit
NOS inhibition Adult sepsis trials mdash mortality reduction not significant
rBPI21 A Phase III trial evaluating rBPI21 in children with meningococcal sepsis has been completed Results will be published soon
Recombinant HDL Phase II trial pending
Fibrinolyticantithrombotic
t-PA streptokinase Anecdotal reports ndash no placebo controlled trials
Protein C Data on placebo controlled trial to be released thisyear
Activated protein C A Phase III trial evaluating recombinant human activated Protein C was stopped prematurely due toa significant beneficial effect on mortality and morbidity of the drug over placebo The safety andefficacy of this drug in meningococcal disease is currently being evaluated
Antithrombin III Data on placebo controlled trial to be released thisyear
Other
Haemofiltration
Anecdotal reports mdash no placebo controlled trialsECMO
ECMO = extracorporeal membrane oxygenation HDL = high-density lipoprotein LPS = lipopolysaccharide NOS = nitric oxide synthase rBPI21 = recombinant bactericidalpermeability increasing protein TNF = tumour necrosis factor t-PA = tissue plasminogenactivator
Table 1 Novel therapies for septic shock
CM E Septicaem ia ndash I
treated for raised intracranial pressurewith mannitol frusemide and electiveintubation In addition standardneurointensive care practice such asnursing the patient at 30deg to thehorizontal and with the head midlineshould be maintained
Normal computed tomography (CT)scans do not exclude raised intracranialpressure Thus treatment for raisedintracranial pressure should be initiatedon clinical grounds without awaiting CTresults Lumbar puncture should beavoided in patients with a clinical diag-nosis of meningococcal disease due tothe risks associated with concomitantcoagulopathy intracranial hyper-tension and cardiac and respiratoryinsufficiency
New therapeutic possibilities(Table 1)
Patients with meningococcal infectionhave been given many experimentaltreatments including anti-inflammatoryanti-endotoxin strategies (Fig 2) and
anticoagulantfibrinolytic therapies (Fig3) Until the results of placebo-controlledtrials are available these treatmentsshould be restricted to units specificallyundertaking research in the disease
There have been reports of the useof tissue plasminogen activator andstreptokinase protein C and heparin inpatients with purpura fulminanssecondary to sepsis61ndash64 These agentscarry a significant risk of haemorrhage
Until their role in sepsis is determinedby properly controlled studies routineuse of these agents cannot berecommended65
In experimental models of shockvarious anti-cytokine and anti-endotoxin strategies have seemedpromising but have failed to reducemortality in randomised controlledtrials They included administration ofanti-TNF monoclonal antibodies66 and
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 441
Fig 3 Targets for novel anticoagulant fibr inolytic therapies in meningococcal sepsis Dotted arrows represent anticoagulant solid arrowsprocoagulant (ATIII = antithrombin III FDP = fibrinogen degradation product PAI = plasminogen activator inhibitor TNF = tumour necrosisfactor t-PA = tissue plasminogen activator TFPI = tissue factor plasminogen inhibitor)
Meningococcal endotoxinCD14(LPSreceptor)
Inflammatorycells
Monoclonal anti-TNF
Reactive oxygen species NO
Proinflammatory cytokines(including TNF-a IL-1b)
NOS inhibitors
rBPI21Monoclonal anti-LPS
Fig 2 Targets for novel anti- inflammatory therapies in sepsis(IL = interleukin LPS = lipopolysaccharide NO = nitric oxide NOS = NO synthase rBPI21 = recombinant bactericidal permeabilityincreasing protein TNF = tumour necrosis factor)
CM E Sept icaem ia ndash I
anti-endotoxin (HA-1A) monoclonalantibody67 A trial of the anti-endotoxinagent recombinant bactericidalpermeability increasing protein(rBPI21)68 has been recently completedand the results will be published soonPreliminary data suggest that recombi-nant high-density lipoprotein has anti-endotoxin properties6970 and furtherinvestigation of its clinical benefit isbeing undertaken
Prevention
Community prevention of secondarycases
Chemoprophylaxis for householdcontacts is recommended Other indi-viduals having close physical contactsuch as in day-care centres or kissingcontacts should also receive prophy-lactic treatment Rifampicin is the drugof choice Ciprofloxacin and ceftriaxoneare good but unlicensed alternatives
Medical staff prophylaxis
Chemoprophylaxis is recommended formedical personnel exposed to oralsecretions such as during intubationOther hospital and laboratory personneldo not have an increased risk ofinfection and prophylaxis is notrecommended
Vaccination
At present unconjugated polysaccha-ride vaccines for serogroups A C W-135and Y are available These confer effec-
tive protection for up to three years inchildren over two years old69 The groupB meningococcal polysaccharide closelymimics a human neuronal adhesionmolecule70 and is non-immunogenic Anumber of outer membrane proteinvaccines have been developed whichhave shown efficacy in outbreaks tospecific strains7172 There is currently novaccine that protects against the largenumber of group B strains circulating inthe UK
The introduction in 1999 of a massvaccination programme using a protein-conjugated group C polysaccharideshould reduce the incidence ofmeningococcal disease in the UK by40 However there remains concernthat this vaccine may lead to a shifttowards a higher incidence of group Bdisease Public awareness of thecontinued need for vigilance earlyidentification and management of thedisease is therefore of great importance
Acknowledgements
The authors are grateful to Dr S Faustfor help in construction of the coagula-tion pathway algorithm (Fig 3) also Dr TAli for helpful advice Dr N Pathan isfunded by a British Heart FoundationJunior Research Fellowship
R eferences
1 Platt MJ Child health statistical review1997 Arch Dis Child 199777542ndash8
2 Invasive meningococcal infectionsCommun Dis Rep CDR Wkly 199555
3 Riordan FA Marzouk O Thomson APSills JA Hart CA The changing presenta-
tions of meningococcal disease Eur JPediatr 1995154472ndash4
4 Ramsay M Kaczmarski E Rush MMallard R et al Changing patterns ofcase ascertainment and trends inmeningococcal disease in England andWales Commun Dis Rep CDR Rev19977R49ndash54
5 Lapeyssonnie L La meacuteningite ceacutereacutebro-spinale en Afrique Bull WHO 196328(Suppl 1)3ndash114
6 Moore PS Hierholzer J DeWitt W GouanK et al Respiratory viruses andmycoplasma as cofactors for epidemicgroup A meningococcal meningitis JAMA19902641271ndash5
7 Virji M Kayhty H Ferguson DJAlexandrescu C et al The role of pili inthe interactions of pathogenic Neisseriawith cultured human endothelial cellsMol Microbiol 199151831ndash41
8 Stephens DS McGee ZA Melly MAHoffman LH Gregg CR Attachment ofpathogenic Neisseria to human mucosalsurfaces role in pathogenesis Infection198210192ndash5
9 de Vries FP Cole R Dankert J Frosch Mvan Putten JP Neisseria meningitidisproducing the Opc adhesin bindsepithelial cell proteoglycan receptorsMol Microbiol 1998271203ndash12
10 Vitovski S Read RC Sayers JR Invasiveisolates of Neisseria meningitidis possessenhanced immunoglobulin A1 proteaseactivity compared to colonizing strainsFASEB J 199913331ndash7
11 Nassif X So M Interaction of pathogenicneisseriae with nonphagocytic cells ClinMicrobiol Rev 19958376ndash88
12 de Vries FP Van Der Ende A van PuttenJP Dankert J Invasion of primarynasopharyngeal epithelial cells byNeisseria meningitidis is controlled byphase variation of multiple surface anti-gens Infect Immun 1996642998ndash3006
13 Mulks MH Plaut AG IgA protease pro-duction as a characteristic distinguishingpathogenic from harmless neisseriaceaeN Engl J Med 1978299973ndash6
14 Virji M Makepeace K Peak IR FergusonDJ et al Opc- and pilus-dependent inter-actions of meningococci with humanendothelial cells molecular mechanismsand modulation by surface polysaccha-rides Mol Microbiol 199518741ndash54
15 Vogel U Hammerschmidt S Frosch MSialic acids of both the capsule and thesialylated lipooligosaccharide of Neisseriameningitis serogroup B are prerequisitesfor virulence of meningococci in theinfant rat Med Microbiol Immunol (Berl)199618581ndash7
16 Klein NJ Ison CA Peakman M Levin Met al The influence of capsulation andlipooligosaccharide structure onneutrophil adhesion molecule expres-sion and endothelial injury by Neisseriameningitidis J Infect Dis 1996173172ndash9
17 Estabrook MM Griffiss JM Jarvis GASialylation of Neisseria meningitidislipooligosaccharide inhibits serum
442 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
copy Meningococcal septicaemia has a 10 mortality overall in the UK
copy The major features of meningococcal septicaemia include capillary leak
coagulopathy myocardial dysfunction and metabolic derangements
copy Management should begin with attent ion to airway breathing and circulation
problems
copy Lumbar puncture should not be performed acutely in patients w ith a clinical
diagnosis of meningococcal disease
copy Mass vaccination against group C disease should reduce the incidence of
meningococcal disease by 40 in the UK how ever no vaccination exists for
serogroup B so there is a need for continued vigilance
Key Points
CM E Septicaem ia ndash I
bactericidal activity by masking lacto-N-neotetraose Infect Immun 1997654436ndash44
18 Jarvis GA Vedros NA Sialic acid of groupB Neisseria meningitidis regulates alterna-tive complement pathway activationInfect Immun 198755174ndash80
19 Andersen BM Endotoxin release fromNeisseria meningitidis Relationshipbetween key bacterial characteristics andmeningococcal disease Review Scand JInfect Dis 198964(Suppl)1ndash43
20 Peter G Weigert MB Bissel AR Gold R etal Meningococcal meningitis in familialdeficiency of the fifth component ofcomplement Pediatrics 198167882ndash6
21 Herva E Leinonen M Kayhty H MakelaPH Vetoniemi-Korhonen SL Recurrentmeningococcal meningitis due to partialcomplement defects and poor anti-meningococcal antibody response JInfect 1983655ndash60
22 Sjoholm AG Braconier JH Soderstrom CProperdin deficiency in a family withfulminant meningococcal infections ClinExp Immunol 198250291ndash7
23 Ross SC Densen P Complementdeficiency states and infection epidemi-ology pathogenesis and consequencesof neisserial and other infections in animmune deficiency Medicine (Baltimore)198463243ndash73
24 Ernst T Spath PJ Aebi C Schaad UBBianchetti MG Screening for comple-ment deficiency in bacterial meningitisActa Paediatr 1997861009ndash10
25 Jack DL Dodds AW Anwar N Ison CA etal Activation of complement bymannose-binding lectin on isogenicmutants of Neisseria meningitidisserogroup B J Immunol 19981601346ndash53
26 Hibberd ML Sumiya M Summerfield JABooy R Levin M Association of variantsof the gene for mannose-binding lectinwith susceptibility to meningococca ldisease Lancet 19993531049ndash53
27 Nadel S Newport MJ Booy R Levin MVariation in the tumor necrosis factor-alpha gene promoter region may beassociated with death from meningococ-cal disease J Infect Dis 1996174878ndash80
28 Waage A Halstensen A Espevik TAssociation between tumour necrosisfactor in serum and fatal outcome inpatients with meningococcal diseaseLancet 1987i355ndash7
29 Gardlund B Sjolin J Nilsson A Roll M etal Plasma levels of cytokines in primaryseptic shock in humans correlation withdisease severity J Infect Dis 1995172296ndash301
30 Brandtzaeg P Kierulf P Gaustad PSkulberg A et al Plasma endotoxin as apredictor of multiple organ failure anddeath in systemic meningococca ldisease J Infect Dis 1989159195ndash204
31 Brandtzaeg P Joo GB Brusletto B KierulfP Plasminogen activator inhibitor 1 and2 alpha-2-antiplasmin plasminogenand endotoxin levels in systemic
meningococca l disease Thromb Res199057271ndash8
32 Kornelisse RF Hazelzet JA Savelkoul HFHop WC et al The relationship betweenplasminogen activator inhibitor-1 andproinflammatory and counterinflamma-tory mediators in children with meningo-cocca l septic shock J Infect Dis19961731148ndash56
33 Westendorp RG Hottenga JJ SlagboomPE Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococ-cal septic shock Lancet 1999354561ndash3
34 Flaegstad T Kaaresen PI Stokland TGutteberg T Factors associated with fataloutcome in childhood meningococcaldisease Acta Paediatr 1995841137ndash42
35 LeClerc F Beuscart R Guillo is BDiependaele JF et al Prognostic factorsof severe infectious purpura in childrenIntensive Care Med 198511140ndash3
36 Mercier JC Beaufils F Hartmann JFAzema D Hemodynamic patterns ofmeningococcal shock in children CritCare Med 19881627ndash33
37 Fijnvandraat K Peters M Derkx B VanDeventer S ten Cate JW Endotoxininduced coagulation activation andprotein C reduction in meningococcalseptic shock Prog Clin Biol Res1994388247ndash54
38 Fijnvandraat K Derkx B Peters M BijlmerR et al Coagulation activation and tissuenecrosis in meningococcal septic shockseverely reduced protein C levels predicta high mortality Thromb Haemost19957315ndash20
39 Brandtzaeg P Sandset PM Joo GBOvstebo R et al The quantitative associ-ation of plasma endotoxin antithrombinprotein C extrinsic pathway inhibitor andfibrinopeptide A in systemic meningococ-cal disease Thromb Res 198955459ndash70
40 Heyderman RS Klein NJ Daramola OAHammerschmidt S et al Induction ofhuman endothelial tissue factor expres-sion by Neisseria meningitidis the influ-ence of bacterial killing and adherenceto the endothelium Microb Pathog199722265ndash74
41 Monsalve F Rucabadol L Salvador ABonastre J et al Myocardial depressionin septic shock caused by meningococcalinfection Crit Care Med 1984121021ndash3
42 Cunnion RE Schaer GL Parker MMNatanson C Parrillo JE The coronarycirculation in human septic shockCirculation 198673637ndash44
43 Dhainaut JF Huyghebaert MF MonsallierJF Lefevre G et al Coronary hemo-dynamics and myocardial metabolism oflactate free fatty acids glucose andketones in patients with septic shockCirculation 198775533ndash41
44 Parrillo JE Burch C Shelhamer JH ParkerMM et al A circulating myocardialdepressant substance in humans withseptic shock J Clin Invest 1985761539ndash53
45 Hazelzet JA van der Voort E LindemansJ ter Heerdt PJ Neijens HJ Relation
between cytokines and routinelaboratory data in children with septicshock and purpura Intensive Care Med199420371ndash4
46 van Deuren M van der Ven-Jongekrijg JBartelink AK van Dalen R et alCorrelation between proinflammatorycytokines and antiinflammatorymediators and the severity of disease inmeningococcal infections J Infect Dis1995172433ndash9
47 Visser JJ Scholten RJ Hoekman K Nitricoxide synthesis in meningococcal menin-gitis Ann Intern Med 1994120345ndash6
48 Khilnani P Electrolyte abnormalities incritically ill children Crit Care Med199220241ndash50
49 Chernow B Calcium does it have atherapeutic role in sepsis Crit Care Med199018895ndash6
50 Gauthier B Trachtman H Di Carmine FUrivetsky M et al Hypocalcemia andhypercalcitoninemia in critically illchildren Crit Care Med 1990181215ndash9
51 Mauger DC Hypokalaemia as a consis-tent feature of fulminant meningococcalsepticaemia Aust Paediatr J 1971784ndash6
52 Weisinger JR Bellorin-Font E Magnesiumand phosphorus Lancet 1998352391ndash6
53 Pollard AJ Britto J Nadel S de Munter Cet al Emergency management ofmeningococcal disease Arch Dis Child199980290ndash6
54 Neu HC Cephalosporins in the treatmentof meningitis Drugs 198734(Suppl2)135ndash53
55 Carcillo JA Davis AL Zaritsky A Role ofearly fluid resuscitation in pediatric septicshock JAMA 19912661242ndash5
56 Dula DJ Lutz P Vogel MF Weaver BNRapid flow rates for the resuscitation ofhypovolemic shock Ann Emerg Med198514303ndash6
57 Nadel S De Munter C Britto J Levin MHabibi P Albumin saint or sinner ArchDis Child 199879384ndash5
58 Human albumin administration in criti-cally ill patients systematic review ofrandomised controlled trials CochraneInjuries Group Albumin Reviewers BrMed J 1998317235ndash40
59 Tobin JR Wetzel RC Shock and multi-organ failure In Rogers MC (ed)Textbook of pediatric intensive careBaltimore Williams and Wilkins1996555ndash605
60 Haneberg B Gutterberg TJ Moe PJOsterud B et al Heparin for infants andchildren with meningococcal septicemiaResults of a randomized therapeutic trialNIPH Ann 1983643ndash7
61 Zenz W Muntean W Zobel G GrubbauerHM Gallistl S Treatment of fulminantmeningococcemia with recombinanttissue plasminogen activator ThrombHaemost 199574802ndash3
62 Keeley SR Matthews NT Buist M Tissueplasminogen activator for gangrene infulminant meningococcaemia Lancet19913371359
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 443
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F
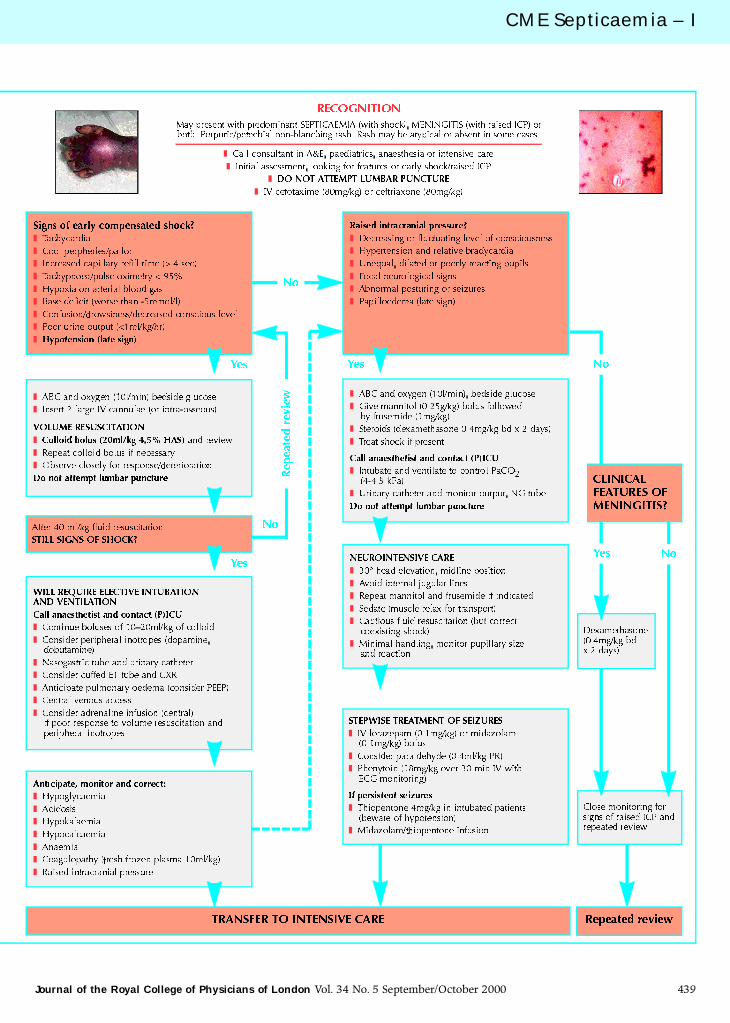
CM E Septicaem ia ndash I
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 439
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
z
CM E Sept icaem ia ndash I
Circulatory support
Early and aggressive fluid resuscitationhas been shown to improve survival55A reduced circulating volume at presen-tation may make it difficult to establishvascular access In order to maintaintissue perfusion and oxygenationcardiac output must be maintainedusing inotropes in severe disease
Initially a 20 mlkg bolus of fluidshould be given56 This may beadequate in mild cases but all patientsshould be carefully monitored fordeterioration due to ongoing capillaryleak Further fluid boluses may berequired using clinical and laboratorysigns to assess the fluid resuscitationThese include capillary refill time heartrate urine output central venouspressure blood pressure and the degreeof metabolic acidosis The optimal fluid
for resuscitation is still debated5758 It islikely that colloidal solutions remain inthe circulation longer than crystalloidsNo artificial colloid solution has beenadequately assessed in children withsepsis and 45 human albumin solu-tion remains our preferred resuscitationfluid
In cases of shock unresponsive to 40mlkg of fluid dilute solutions ofdopamine andor dobutamine may begiven through a peripheral cannulauntil central vascular access is obtainedContinued myocardial dysfunction maynecessitate infusion of adrenaline ornoradrenaline once central access isobtained59
Metabolic corrections
Hypoglycaemia is common and requiresrapid correction Severe shock is often
associated with metabolic acidosiswhich may be partially corrected bycirculating volume and cardiovascularresuscitation The metabolic acidosis inmeningococcal septicaemia is paradoxi-cally associated with hypokalaemiaoften profound and requires closemonitoring and correction Similarlycalcium and magnesium levelscommonly fall and should be correctedin order to improve myocardialperformance
Coagulation support
DIC is a common feature of meningo-coccal septicaemia Depletion of coagu-lation factors fibrinogen and anti-coagulant proteins may be corrected byadministration of fresh frozen plasmaThis may be given as boluses in place of albumin in continuing shockCryoprecipitate is not routinely recom-mended except in severe and persistenthypofibrinogenaemia Platelet adminis-tration may exacerbate and continuethe process of DIC Thrombocytopeniais not routinely corrected unless associ-ated with spontaneous haemorrhageor a platelet count below 20000mm3Heparin does not help to reverseischaemia in sepsis60 Prostacyclin hasbeen anecdotally useful to reversesevere peripheral vasoconstriction inmeningococcal sepsis There is how-ever a risk of severe hypotension andprostacyclin should be considered onlyafter shock has been controlled withvolume replacement and inotropes
Management of raised intracranialpressure in meningococcal infection
Raised intracranial pressure may occurin isolation due to meningitis or coexistwith septic shock This may cause diag-nostic difficulties as the signs may besimilar to shock and impaired brainperfusion Clinical features includedeteriorating levels of consciousnesspupilla ry dilatation or changes inpupillary reflexes hypertension andbradycardia Papilloedema is a late sign
Patients with elevated bloodpressure relative bradycardia anddeteriorating consciousness should be
440 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
Anti inflammatory
Anti-TNF monoclonal antibody Adult sepsis trials ndash mortality reduction not significant
Anti-LPS monoclonal antibody Phase III trial in meningococcal sepsis ndash no benefit
NOS inhibition Adult sepsis trials mdash mortality reduction not significant
rBPI21 A Phase III trial evaluating rBPI21 in children with meningococcal sepsis has been completed Results will be published soon
Recombinant HDL Phase II trial pending
Fibrinolyticantithrombotic
t-PA streptokinase Anecdotal reports ndash no placebo controlled trials
Protein C Data on placebo controlled trial to be released thisyear
Activated protein C A Phase III trial evaluating recombinant human activated Protein C was stopped prematurely due toa significant beneficial effect on mortality and morbidity of the drug over placebo The safety andefficacy of this drug in meningococcal disease is currently being evaluated
Antithrombin III Data on placebo controlled trial to be released thisyear
Other
Haemofiltration
Anecdotal reports mdash no placebo controlled trialsECMO
ECMO = extracorporeal membrane oxygenation HDL = high-density lipoprotein LPS = lipopolysaccharide NOS = nitric oxide synthase rBPI21 = recombinant bactericidalpermeability increasing protein TNF = tumour necrosis factor t-PA = tissue plasminogenactivator
Table 1 Novel therapies for septic shock
CM E Septicaem ia ndash I
treated for raised intracranial pressurewith mannitol frusemide and electiveintubation In addition standardneurointensive care practice such asnursing the patient at 30deg to thehorizontal and with the head midlineshould be maintained
Normal computed tomography (CT)scans do not exclude raised intracranialpressure Thus treatment for raisedintracranial pressure should be initiatedon clinical grounds without awaiting CTresults Lumbar puncture should beavoided in patients with a clinical diag-nosis of meningococcal disease due tothe risks associated with concomitantcoagulopathy intracranial hyper-tension and cardiac and respiratoryinsufficiency
New therapeutic possibilities(Table 1)
Patients with meningococcal infectionhave been given many experimentaltreatments including anti-inflammatoryanti-endotoxin strategies (Fig 2) and
anticoagulantfibrinolytic therapies (Fig3) Until the results of placebo-controlledtrials are available these treatmentsshould be restricted to units specificallyundertaking research in the disease
There have been reports of the useof tissue plasminogen activator andstreptokinase protein C and heparin inpatients with purpura fulminanssecondary to sepsis61ndash64 These agentscarry a significant risk of haemorrhage
Until their role in sepsis is determinedby properly controlled studies routineuse of these agents cannot berecommended65
In experimental models of shockvarious anti-cytokine and anti-endotoxin strategies have seemedpromising but have failed to reducemortality in randomised controlledtrials They included administration ofanti-TNF monoclonal antibodies66 and
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 441
Fig 3 Targets for novel anticoagulant fibr inolytic therapies in meningococcal sepsis Dotted arrows represent anticoagulant solid arrowsprocoagulant (ATIII = antithrombin III FDP = fibrinogen degradation product PAI = plasminogen activator inhibitor TNF = tumour necrosisfactor t-PA = tissue plasminogen activator TFPI = tissue factor plasminogen inhibitor)
Meningococcal endotoxinCD14(LPSreceptor)
Inflammatorycells
Monoclonal anti-TNF
Reactive oxygen species NO
Proinflammatory cytokines(including TNF-a IL-1b)
NOS inhibitors
rBPI21Monoclonal anti-LPS
Fig 2 Targets for novel anti- inflammatory therapies in sepsis(IL = interleukin LPS = lipopolysaccharide NO = nitric oxide NOS = NO synthase rBPI21 = recombinant bactericidal permeabilityincreasing protein TNF = tumour necrosis factor)
CM E Sept icaem ia ndash I
anti-endotoxin (HA-1A) monoclonalantibody67 A trial of the anti-endotoxinagent recombinant bactericidalpermeability increasing protein(rBPI21)68 has been recently completedand the results will be published soonPreliminary data suggest that recombi-nant high-density lipoprotein has anti-endotoxin properties6970 and furtherinvestigation of its clinical benefit isbeing undertaken
Prevention
Community prevention of secondarycases
Chemoprophylaxis for householdcontacts is recommended Other indi-viduals having close physical contactsuch as in day-care centres or kissingcontacts should also receive prophy-lactic treatment Rifampicin is the drugof choice Ciprofloxacin and ceftriaxoneare good but unlicensed alternatives
Medical staff prophylaxis
Chemoprophylaxis is recommended formedical personnel exposed to oralsecretions such as during intubationOther hospital and laboratory personneldo not have an increased risk ofinfection and prophylaxis is notrecommended
Vaccination
At present unconjugated polysaccha-ride vaccines for serogroups A C W-135and Y are available These confer effec-
tive protection for up to three years inchildren over two years old69 The groupB meningococcal polysaccharide closelymimics a human neuronal adhesionmolecule70 and is non-immunogenic Anumber of outer membrane proteinvaccines have been developed whichhave shown efficacy in outbreaks tospecific strains7172 There is currently novaccine that protects against the largenumber of group B strains circulating inthe UK
The introduction in 1999 of a massvaccination programme using a protein-conjugated group C polysaccharideshould reduce the incidence ofmeningococcal disease in the UK by40 However there remains concernthat this vaccine may lead to a shifttowards a higher incidence of group Bdisease Public awareness of thecontinued need for vigilance earlyidentification and management of thedisease is therefore of great importance
Acknowledgements
The authors are grateful to Dr S Faustfor help in construction of the coagula-tion pathway algorithm (Fig 3) also Dr TAli for helpful advice Dr N Pathan isfunded by a British Heart FoundationJunior Research Fellowship
R eferences
1 Platt MJ Child health statistical review1997 Arch Dis Child 199777542ndash8
2 Invasive meningococcal infectionsCommun Dis Rep CDR Wkly 199555
3 Riordan FA Marzouk O Thomson APSills JA Hart CA The changing presenta-
tions of meningococcal disease Eur JPediatr 1995154472ndash4
4 Ramsay M Kaczmarski E Rush MMallard R et al Changing patterns ofcase ascertainment and trends inmeningococcal disease in England andWales Commun Dis Rep CDR Rev19977R49ndash54
5 Lapeyssonnie L La meacuteningite ceacutereacutebro-spinale en Afrique Bull WHO 196328(Suppl 1)3ndash114
6 Moore PS Hierholzer J DeWitt W GouanK et al Respiratory viruses andmycoplasma as cofactors for epidemicgroup A meningococcal meningitis JAMA19902641271ndash5
7 Virji M Kayhty H Ferguson DJAlexandrescu C et al The role of pili inthe interactions of pathogenic Neisseriawith cultured human endothelial cellsMol Microbiol 199151831ndash41
8 Stephens DS McGee ZA Melly MAHoffman LH Gregg CR Attachment ofpathogenic Neisseria to human mucosalsurfaces role in pathogenesis Infection198210192ndash5
9 de Vries FP Cole R Dankert J Frosch Mvan Putten JP Neisseria meningitidisproducing the Opc adhesin bindsepithelial cell proteoglycan receptorsMol Microbiol 1998271203ndash12
10 Vitovski S Read RC Sayers JR Invasiveisolates of Neisseria meningitidis possessenhanced immunoglobulin A1 proteaseactivity compared to colonizing strainsFASEB J 199913331ndash7
11 Nassif X So M Interaction of pathogenicneisseriae with nonphagocytic cells ClinMicrobiol Rev 19958376ndash88
12 de Vries FP Van Der Ende A van PuttenJP Dankert J Invasion of primarynasopharyngeal epithelial cells byNeisseria meningitidis is controlled byphase variation of multiple surface anti-gens Infect Immun 1996642998ndash3006
13 Mulks MH Plaut AG IgA protease pro-duction as a characteristic distinguishingpathogenic from harmless neisseriaceaeN Engl J Med 1978299973ndash6
14 Virji M Makepeace K Peak IR FergusonDJ et al Opc- and pilus-dependent inter-actions of meningococci with humanendothelial cells molecular mechanismsand modulation by surface polysaccha-rides Mol Microbiol 199518741ndash54
15 Vogel U Hammerschmidt S Frosch MSialic acids of both the capsule and thesialylated lipooligosaccharide of Neisseriameningitis serogroup B are prerequisitesfor virulence of meningococci in theinfant rat Med Microbiol Immunol (Berl)199618581ndash7
16 Klein NJ Ison CA Peakman M Levin Met al The influence of capsulation andlipooligosaccharide structure onneutrophil adhesion molecule expres-sion and endothelial injury by Neisseriameningitidis J Infect Dis 1996173172ndash9
17 Estabrook MM Griffiss JM Jarvis GASialylation of Neisseria meningitidislipooligosaccharide inhibits serum
442 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
copy Meningococcal septicaemia has a 10 mortality overall in the UK
copy The major features of meningococcal septicaemia include capillary leak
coagulopathy myocardial dysfunction and metabolic derangements
copy Management should begin with attent ion to airway breathing and circulation
problems
copy Lumbar puncture should not be performed acutely in patients w ith a clinical
diagnosis of meningococcal disease
copy Mass vaccination against group C disease should reduce the incidence of
meningococcal disease by 40 in the UK how ever no vaccination exists for
serogroup B so there is a need for continued vigilance
Key Points
CM E Septicaem ia ndash I
bactericidal activity by masking lacto-N-neotetraose Infect Immun 1997654436ndash44
18 Jarvis GA Vedros NA Sialic acid of groupB Neisseria meningitidis regulates alterna-tive complement pathway activationInfect Immun 198755174ndash80
19 Andersen BM Endotoxin release fromNeisseria meningitidis Relationshipbetween key bacterial characteristics andmeningococcal disease Review Scand JInfect Dis 198964(Suppl)1ndash43
20 Peter G Weigert MB Bissel AR Gold R etal Meningococcal meningitis in familialdeficiency of the fifth component ofcomplement Pediatrics 198167882ndash6
21 Herva E Leinonen M Kayhty H MakelaPH Vetoniemi-Korhonen SL Recurrentmeningococcal meningitis due to partialcomplement defects and poor anti-meningococcal antibody response JInfect 1983655ndash60
22 Sjoholm AG Braconier JH Soderstrom CProperdin deficiency in a family withfulminant meningococcal infections ClinExp Immunol 198250291ndash7
23 Ross SC Densen P Complementdeficiency states and infection epidemi-ology pathogenesis and consequencesof neisserial and other infections in animmune deficiency Medicine (Baltimore)198463243ndash73
24 Ernst T Spath PJ Aebi C Schaad UBBianchetti MG Screening for comple-ment deficiency in bacterial meningitisActa Paediatr 1997861009ndash10
25 Jack DL Dodds AW Anwar N Ison CA etal Activation of complement bymannose-binding lectin on isogenicmutants of Neisseria meningitidisserogroup B J Immunol 19981601346ndash53
26 Hibberd ML Sumiya M Summerfield JABooy R Levin M Association of variantsof the gene for mannose-binding lectinwith susceptibility to meningococca ldisease Lancet 19993531049ndash53
27 Nadel S Newport MJ Booy R Levin MVariation in the tumor necrosis factor-alpha gene promoter region may beassociated with death from meningococ-cal disease J Infect Dis 1996174878ndash80
28 Waage A Halstensen A Espevik TAssociation between tumour necrosisfactor in serum and fatal outcome inpatients with meningococcal diseaseLancet 1987i355ndash7
29 Gardlund B Sjolin J Nilsson A Roll M etal Plasma levels of cytokines in primaryseptic shock in humans correlation withdisease severity J Infect Dis 1995172296ndash301
30 Brandtzaeg P Kierulf P Gaustad PSkulberg A et al Plasma endotoxin as apredictor of multiple organ failure anddeath in systemic meningococca ldisease J Infect Dis 1989159195ndash204
31 Brandtzaeg P Joo GB Brusletto B KierulfP Plasminogen activator inhibitor 1 and2 alpha-2-antiplasmin plasminogenand endotoxin levels in systemic
meningococca l disease Thromb Res199057271ndash8
32 Kornelisse RF Hazelzet JA Savelkoul HFHop WC et al The relationship betweenplasminogen activator inhibitor-1 andproinflammatory and counterinflamma-tory mediators in children with meningo-cocca l septic shock J Infect Dis19961731148ndash56
33 Westendorp RG Hottenga JJ SlagboomPE Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococ-cal septic shock Lancet 1999354561ndash3
34 Flaegstad T Kaaresen PI Stokland TGutteberg T Factors associated with fataloutcome in childhood meningococcaldisease Acta Paediatr 1995841137ndash42
35 LeClerc F Beuscart R Guillo is BDiependaele JF et al Prognostic factorsof severe infectious purpura in childrenIntensive Care Med 198511140ndash3
36 Mercier JC Beaufils F Hartmann JFAzema D Hemodynamic patterns ofmeningococcal shock in children CritCare Med 19881627ndash33
37 Fijnvandraat K Peters M Derkx B VanDeventer S ten Cate JW Endotoxininduced coagulation activation andprotein C reduction in meningococcalseptic shock Prog Clin Biol Res1994388247ndash54
38 Fijnvandraat K Derkx B Peters M BijlmerR et al Coagulation activation and tissuenecrosis in meningococcal septic shockseverely reduced protein C levels predicta high mortality Thromb Haemost19957315ndash20
39 Brandtzaeg P Sandset PM Joo GBOvstebo R et al The quantitative associ-ation of plasma endotoxin antithrombinprotein C extrinsic pathway inhibitor andfibrinopeptide A in systemic meningococ-cal disease Thromb Res 198955459ndash70
40 Heyderman RS Klein NJ Daramola OAHammerschmidt S et al Induction ofhuman endothelial tissue factor expres-sion by Neisseria meningitidis the influ-ence of bacterial killing and adherenceto the endothelium Microb Pathog199722265ndash74
41 Monsalve F Rucabadol L Salvador ABonastre J et al Myocardial depressionin septic shock caused by meningococcalinfection Crit Care Med 1984121021ndash3
42 Cunnion RE Schaer GL Parker MMNatanson C Parrillo JE The coronarycirculation in human septic shockCirculation 198673637ndash44
43 Dhainaut JF Huyghebaert MF MonsallierJF Lefevre G et al Coronary hemo-dynamics and myocardial metabolism oflactate free fatty acids glucose andketones in patients with septic shockCirculation 198775533ndash41
44 Parrillo JE Burch C Shelhamer JH ParkerMM et al A circulating myocardialdepressant substance in humans withseptic shock J Clin Invest 1985761539ndash53
45 Hazelzet JA van der Voort E LindemansJ ter Heerdt PJ Neijens HJ Relation
between cytokines and routinelaboratory data in children with septicshock and purpura Intensive Care Med199420371ndash4
46 van Deuren M van der Ven-Jongekrijg JBartelink AK van Dalen R et alCorrelation between proinflammatorycytokines and antiinflammatorymediators and the severity of disease inmeningococcal infections J Infect Dis1995172433ndash9
47 Visser JJ Scholten RJ Hoekman K Nitricoxide synthesis in meningococcal menin-gitis Ann Intern Med 1994120345ndash6
48 Khilnani P Electrolyte abnormalities incritically ill children Crit Care Med199220241ndash50
49 Chernow B Calcium does it have atherapeutic role in sepsis Crit Care Med199018895ndash6
50 Gauthier B Trachtman H Di Carmine FUrivetsky M et al Hypocalcemia andhypercalcitoninemia in critically illchildren Crit Care Med 1990181215ndash9
51 Mauger DC Hypokalaemia as a consis-tent feature of fulminant meningococcalsepticaemia Aust Paediatr J 1971784ndash6
52 Weisinger JR Bellorin-Font E Magnesiumand phosphorus Lancet 1998352391ndash6
53 Pollard AJ Britto J Nadel S de Munter Cet al Emergency management ofmeningococcal disease Arch Dis Child199980290ndash6
54 Neu HC Cephalosporins in the treatmentof meningitis Drugs 198734(Suppl2)135ndash53
55 Carcillo JA Davis AL Zaritsky A Role ofearly fluid resuscitation in pediatric septicshock JAMA 19912661242ndash5
56 Dula DJ Lutz P Vogel MF Weaver BNRapid flow rates for the resuscitation ofhypovolemic shock Ann Emerg Med198514303ndash6
57 Nadel S De Munter C Britto J Levin MHabibi P Albumin saint or sinner ArchDis Child 199879384ndash5
58 Human albumin administration in criti-cally ill patients systematic review ofrandomised controlled trials CochraneInjuries Group Albumin Reviewers BrMed J 1998317235ndash40
59 Tobin JR Wetzel RC Shock and multi-organ failure In Rogers MC (ed)Textbook of pediatric intensive careBaltimore Williams and Wilkins1996555ndash605
60 Haneberg B Gutterberg TJ Moe PJOsterud B et al Heparin for infants andchildren with meningococcal septicemiaResults of a randomized therapeutic trialNIPH Ann 1983643ndash7
61 Zenz W Muntean W Zobel G GrubbauerHM Gallistl S Treatment of fulminantmeningococcemia with recombinanttissue plasminogen activator ThrombHaemost 199574802ndash3
62 Keeley SR Matthews NT Buist M Tissueplasminogen activator for gangrene infulminant meningococcaemia Lancet19913371359
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 443
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F

CM E Sept icaem ia ndash I
Circulatory support
Early and aggressive fluid resuscitationhas been shown to improve survival55A reduced circulating volume at presen-tation may make it difficult to establishvascular access In order to maintaintissue perfusion and oxygenationcardiac output must be maintainedusing inotropes in severe disease
Initially a 20 mlkg bolus of fluidshould be given56 This may beadequate in mild cases but all patientsshould be carefully monitored fordeterioration due to ongoing capillaryleak Further fluid boluses may berequired using clinical and laboratorysigns to assess the fluid resuscitationThese include capillary refill time heartrate urine output central venouspressure blood pressure and the degreeof metabolic acidosis The optimal fluid
for resuscitation is still debated5758 It islikely that colloidal solutions remain inthe circulation longer than crystalloidsNo artificial colloid solution has beenadequately assessed in children withsepsis and 45 human albumin solu-tion remains our preferred resuscitationfluid
In cases of shock unresponsive to 40mlkg of fluid dilute solutions ofdopamine andor dobutamine may begiven through a peripheral cannulauntil central vascular access is obtainedContinued myocardial dysfunction maynecessitate infusion of adrenaline ornoradrenaline once central access isobtained59
Metabolic corrections
Hypoglycaemia is common and requiresrapid correction Severe shock is often
associated with metabolic acidosiswhich may be partially corrected bycirculating volume and cardiovascularresuscitation The metabolic acidosis inmeningococcal septicaemia is paradoxi-cally associated with hypokalaemiaoften profound and requires closemonitoring and correction Similarlycalcium and magnesium levelscommonly fall and should be correctedin order to improve myocardialperformance
Coagulation support
DIC is a common feature of meningo-coccal septicaemia Depletion of coagu-lation factors fibrinogen and anti-coagulant proteins may be corrected byadministration of fresh frozen plasmaThis may be given as boluses in place of albumin in continuing shockCryoprecipitate is not routinely recom-mended except in severe and persistenthypofibrinogenaemia Platelet adminis-tration may exacerbate and continuethe process of DIC Thrombocytopeniais not routinely corrected unless associ-ated with spontaneous haemorrhageor a platelet count below 20000mm3Heparin does not help to reverseischaemia in sepsis60 Prostacyclin hasbeen anecdotally useful to reversesevere peripheral vasoconstriction inmeningococcal sepsis There is how-ever a risk of severe hypotension andprostacyclin should be considered onlyafter shock has been controlled withvolume replacement and inotropes
Management of raised intracranialpressure in meningococcal infection
Raised intracranial pressure may occurin isolation due to meningitis or coexistwith septic shock This may cause diag-nostic difficulties as the signs may besimilar to shock and impaired brainperfusion Clinical features includedeteriorating levels of consciousnesspupilla ry dilatation or changes inpupillary reflexes hypertension andbradycardia Papilloedema is a late sign
Patients with elevated bloodpressure relative bradycardia anddeteriorating consciousness should be
440 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
Anti inflammatory
Anti-TNF monoclonal antibody Adult sepsis trials ndash mortality reduction not significant
Anti-LPS monoclonal antibody Phase III trial in meningococcal sepsis ndash no benefit
NOS inhibition Adult sepsis trials mdash mortality reduction not significant
rBPI21 A Phase III trial evaluating rBPI21 in children with meningococcal sepsis has been completed Results will be published soon
Recombinant HDL Phase II trial pending
Fibrinolyticantithrombotic
t-PA streptokinase Anecdotal reports ndash no placebo controlled trials
Protein C Data on placebo controlled trial to be released thisyear
Activated protein C A Phase III trial evaluating recombinant human activated Protein C was stopped prematurely due toa significant beneficial effect on mortality and morbidity of the drug over placebo The safety andefficacy of this drug in meningococcal disease is currently being evaluated
Antithrombin III Data on placebo controlled trial to be released thisyear
Other
Haemofiltration
Anecdotal reports mdash no placebo controlled trialsECMO
ECMO = extracorporeal membrane oxygenation HDL = high-density lipoprotein LPS = lipopolysaccharide NOS = nitric oxide synthase rBPI21 = recombinant bactericidalpermeability increasing protein TNF = tumour necrosis factor t-PA = tissue plasminogenactivator
Table 1 Novel therapies for septic shock
CM E Septicaem ia ndash I
treated for raised intracranial pressurewith mannitol frusemide and electiveintubation In addition standardneurointensive care practice such asnursing the patient at 30deg to thehorizontal and with the head midlineshould be maintained
Normal computed tomography (CT)scans do not exclude raised intracranialpressure Thus treatment for raisedintracranial pressure should be initiatedon clinical grounds without awaiting CTresults Lumbar puncture should beavoided in patients with a clinical diag-nosis of meningococcal disease due tothe risks associated with concomitantcoagulopathy intracranial hyper-tension and cardiac and respiratoryinsufficiency
New therapeutic possibilities(Table 1)
Patients with meningococcal infectionhave been given many experimentaltreatments including anti-inflammatoryanti-endotoxin strategies (Fig 2) and
anticoagulantfibrinolytic therapies (Fig3) Until the results of placebo-controlledtrials are available these treatmentsshould be restricted to units specificallyundertaking research in the disease
There have been reports of the useof tissue plasminogen activator andstreptokinase protein C and heparin inpatients with purpura fulminanssecondary to sepsis61ndash64 These agentscarry a significant risk of haemorrhage
Until their role in sepsis is determinedby properly controlled studies routineuse of these agents cannot berecommended65
In experimental models of shockvarious anti-cytokine and anti-endotoxin strategies have seemedpromising but have failed to reducemortality in randomised controlledtrials They included administration ofanti-TNF monoclonal antibodies66 and
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 441
Fig 3 Targets for novel anticoagulant fibr inolytic therapies in meningococcal sepsis Dotted arrows represent anticoagulant solid arrowsprocoagulant (ATIII = antithrombin III FDP = fibrinogen degradation product PAI = plasminogen activator inhibitor TNF = tumour necrosisfactor t-PA = tissue plasminogen activator TFPI = tissue factor plasminogen inhibitor)
Meningococcal endotoxinCD14(LPSreceptor)
Inflammatorycells
Monoclonal anti-TNF
Reactive oxygen species NO
Proinflammatory cytokines(including TNF-a IL-1b)
NOS inhibitors
rBPI21Monoclonal anti-LPS
Fig 2 Targets for novel anti- inflammatory therapies in sepsis(IL = interleukin LPS = lipopolysaccharide NO = nitric oxide NOS = NO synthase rBPI21 = recombinant bactericidal permeabilityincreasing protein TNF = tumour necrosis factor)
CM E Sept icaem ia ndash I
anti-endotoxin (HA-1A) monoclonalantibody67 A trial of the anti-endotoxinagent recombinant bactericidalpermeability increasing protein(rBPI21)68 has been recently completedand the results will be published soonPreliminary data suggest that recombi-nant high-density lipoprotein has anti-endotoxin properties6970 and furtherinvestigation of its clinical benefit isbeing undertaken
Prevention
Community prevention of secondarycases
Chemoprophylaxis for householdcontacts is recommended Other indi-viduals having close physical contactsuch as in day-care centres or kissingcontacts should also receive prophy-lactic treatment Rifampicin is the drugof choice Ciprofloxacin and ceftriaxoneare good but unlicensed alternatives
Medical staff prophylaxis
Chemoprophylaxis is recommended formedical personnel exposed to oralsecretions such as during intubationOther hospital and laboratory personneldo not have an increased risk ofinfection and prophylaxis is notrecommended
Vaccination
At present unconjugated polysaccha-ride vaccines for serogroups A C W-135and Y are available These confer effec-
tive protection for up to three years inchildren over two years old69 The groupB meningococcal polysaccharide closelymimics a human neuronal adhesionmolecule70 and is non-immunogenic Anumber of outer membrane proteinvaccines have been developed whichhave shown efficacy in outbreaks tospecific strains7172 There is currently novaccine that protects against the largenumber of group B strains circulating inthe UK
The introduction in 1999 of a massvaccination programme using a protein-conjugated group C polysaccharideshould reduce the incidence ofmeningococcal disease in the UK by40 However there remains concernthat this vaccine may lead to a shifttowards a higher incidence of group Bdisease Public awareness of thecontinued need for vigilance earlyidentification and management of thedisease is therefore of great importance
Acknowledgements
The authors are grateful to Dr S Faustfor help in construction of the coagula-tion pathway algorithm (Fig 3) also Dr TAli for helpful advice Dr N Pathan isfunded by a British Heart FoundationJunior Research Fellowship
R eferences
1 Platt MJ Child health statistical review1997 Arch Dis Child 199777542ndash8
2 Invasive meningococcal infectionsCommun Dis Rep CDR Wkly 199555
3 Riordan FA Marzouk O Thomson APSills JA Hart CA The changing presenta-
tions of meningococcal disease Eur JPediatr 1995154472ndash4
4 Ramsay M Kaczmarski E Rush MMallard R et al Changing patterns ofcase ascertainment and trends inmeningococcal disease in England andWales Commun Dis Rep CDR Rev19977R49ndash54
5 Lapeyssonnie L La meacuteningite ceacutereacutebro-spinale en Afrique Bull WHO 196328(Suppl 1)3ndash114
6 Moore PS Hierholzer J DeWitt W GouanK et al Respiratory viruses andmycoplasma as cofactors for epidemicgroup A meningococcal meningitis JAMA19902641271ndash5
7 Virji M Kayhty H Ferguson DJAlexandrescu C et al The role of pili inthe interactions of pathogenic Neisseriawith cultured human endothelial cellsMol Microbiol 199151831ndash41
8 Stephens DS McGee ZA Melly MAHoffman LH Gregg CR Attachment ofpathogenic Neisseria to human mucosalsurfaces role in pathogenesis Infection198210192ndash5
9 de Vries FP Cole R Dankert J Frosch Mvan Putten JP Neisseria meningitidisproducing the Opc adhesin bindsepithelial cell proteoglycan receptorsMol Microbiol 1998271203ndash12
10 Vitovski S Read RC Sayers JR Invasiveisolates of Neisseria meningitidis possessenhanced immunoglobulin A1 proteaseactivity compared to colonizing strainsFASEB J 199913331ndash7
11 Nassif X So M Interaction of pathogenicneisseriae with nonphagocytic cells ClinMicrobiol Rev 19958376ndash88
12 de Vries FP Van Der Ende A van PuttenJP Dankert J Invasion of primarynasopharyngeal epithelial cells byNeisseria meningitidis is controlled byphase variation of multiple surface anti-gens Infect Immun 1996642998ndash3006
13 Mulks MH Plaut AG IgA protease pro-duction as a characteristic distinguishingpathogenic from harmless neisseriaceaeN Engl J Med 1978299973ndash6
14 Virji M Makepeace K Peak IR FergusonDJ et al Opc- and pilus-dependent inter-actions of meningococci with humanendothelial cells molecular mechanismsand modulation by surface polysaccha-rides Mol Microbiol 199518741ndash54
15 Vogel U Hammerschmidt S Frosch MSialic acids of both the capsule and thesialylated lipooligosaccharide of Neisseriameningitis serogroup B are prerequisitesfor virulence of meningococci in theinfant rat Med Microbiol Immunol (Berl)199618581ndash7
16 Klein NJ Ison CA Peakman M Levin Met al The influence of capsulation andlipooligosaccharide structure onneutrophil adhesion molecule expres-sion and endothelial injury by Neisseriameningitidis J Infect Dis 1996173172ndash9
17 Estabrook MM Griffiss JM Jarvis GASialylation of Neisseria meningitidislipooligosaccharide inhibits serum
442 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
copy Meningococcal septicaemia has a 10 mortality overall in the UK
copy The major features of meningococcal septicaemia include capillary leak
coagulopathy myocardial dysfunction and metabolic derangements
copy Management should begin with attent ion to airway breathing and circulation
problems
copy Lumbar puncture should not be performed acutely in patients w ith a clinical
diagnosis of meningococcal disease
copy Mass vaccination against group C disease should reduce the incidence of
meningococcal disease by 40 in the UK how ever no vaccination exists for
serogroup B so there is a need for continued vigilance
Key Points
CM E Septicaem ia ndash I
bactericidal activity by masking lacto-N-neotetraose Infect Immun 1997654436ndash44
18 Jarvis GA Vedros NA Sialic acid of groupB Neisseria meningitidis regulates alterna-tive complement pathway activationInfect Immun 198755174ndash80
19 Andersen BM Endotoxin release fromNeisseria meningitidis Relationshipbetween key bacterial characteristics andmeningococcal disease Review Scand JInfect Dis 198964(Suppl)1ndash43
20 Peter G Weigert MB Bissel AR Gold R etal Meningococcal meningitis in familialdeficiency of the fifth component ofcomplement Pediatrics 198167882ndash6
21 Herva E Leinonen M Kayhty H MakelaPH Vetoniemi-Korhonen SL Recurrentmeningococcal meningitis due to partialcomplement defects and poor anti-meningococcal antibody response JInfect 1983655ndash60
22 Sjoholm AG Braconier JH Soderstrom CProperdin deficiency in a family withfulminant meningococcal infections ClinExp Immunol 198250291ndash7
23 Ross SC Densen P Complementdeficiency states and infection epidemi-ology pathogenesis and consequencesof neisserial and other infections in animmune deficiency Medicine (Baltimore)198463243ndash73
24 Ernst T Spath PJ Aebi C Schaad UBBianchetti MG Screening for comple-ment deficiency in bacterial meningitisActa Paediatr 1997861009ndash10
25 Jack DL Dodds AW Anwar N Ison CA etal Activation of complement bymannose-binding lectin on isogenicmutants of Neisseria meningitidisserogroup B J Immunol 19981601346ndash53
26 Hibberd ML Sumiya M Summerfield JABooy R Levin M Association of variantsof the gene for mannose-binding lectinwith susceptibility to meningococca ldisease Lancet 19993531049ndash53
27 Nadel S Newport MJ Booy R Levin MVariation in the tumor necrosis factor-alpha gene promoter region may beassociated with death from meningococ-cal disease J Infect Dis 1996174878ndash80
28 Waage A Halstensen A Espevik TAssociation between tumour necrosisfactor in serum and fatal outcome inpatients with meningococcal diseaseLancet 1987i355ndash7
29 Gardlund B Sjolin J Nilsson A Roll M etal Plasma levels of cytokines in primaryseptic shock in humans correlation withdisease severity J Infect Dis 1995172296ndash301
30 Brandtzaeg P Kierulf P Gaustad PSkulberg A et al Plasma endotoxin as apredictor of multiple organ failure anddeath in systemic meningococca ldisease J Infect Dis 1989159195ndash204
31 Brandtzaeg P Joo GB Brusletto B KierulfP Plasminogen activator inhibitor 1 and2 alpha-2-antiplasmin plasminogenand endotoxin levels in systemic
meningococca l disease Thromb Res199057271ndash8
32 Kornelisse RF Hazelzet JA Savelkoul HFHop WC et al The relationship betweenplasminogen activator inhibitor-1 andproinflammatory and counterinflamma-tory mediators in children with meningo-cocca l septic shock J Infect Dis19961731148ndash56
33 Westendorp RG Hottenga JJ SlagboomPE Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococ-cal septic shock Lancet 1999354561ndash3
34 Flaegstad T Kaaresen PI Stokland TGutteberg T Factors associated with fataloutcome in childhood meningococcaldisease Acta Paediatr 1995841137ndash42
35 LeClerc F Beuscart R Guillo is BDiependaele JF et al Prognostic factorsof severe infectious purpura in childrenIntensive Care Med 198511140ndash3
36 Mercier JC Beaufils F Hartmann JFAzema D Hemodynamic patterns ofmeningococcal shock in children CritCare Med 19881627ndash33
37 Fijnvandraat K Peters M Derkx B VanDeventer S ten Cate JW Endotoxininduced coagulation activation andprotein C reduction in meningococcalseptic shock Prog Clin Biol Res1994388247ndash54
38 Fijnvandraat K Derkx B Peters M BijlmerR et al Coagulation activation and tissuenecrosis in meningococcal septic shockseverely reduced protein C levels predicta high mortality Thromb Haemost19957315ndash20
39 Brandtzaeg P Sandset PM Joo GBOvstebo R et al The quantitative associ-ation of plasma endotoxin antithrombinprotein C extrinsic pathway inhibitor andfibrinopeptide A in systemic meningococ-cal disease Thromb Res 198955459ndash70
40 Heyderman RS Klein NJ Daramola OAHammerschmidt S et al Induction ofhuman endothelial tissue factor expres-sion by Neisseria meningitidis the influ-ence of bacterial killing and adherenceto the endothelium Microb Pathog199722265ndash74
41 Monsalve F Rucabadol L Salvador ABonastre J et al Myocardial depressionin septic shock caused by meningococcalinfection Crit Care Med 1984121021ndash3
42 Cunnion RE Schaer GL Parker MMNatanson C Parrillo JE The coronarycirculation in human septic shockCirculation 198673637ndash44
43 Dhainaut JF Huyghebaert MF MonsallierJF Lefevre G et al Coronary hemo-dynamics and myocardial metabolism oflactate free fatty acids glucose andketones in patients with septic shockCirculation 198775533ndash41
44 Parrillo JE Burch C Shelhamer JH ParkerMM et al A circulating myocardialdepressant substance in humans withseptic shock J Clin Invest 1985761539ndash53
45 Hazelzet JA van der Voort E LindemansJ ter Heerdt PJ Neijens HJ Relation
between cytokines and routinelaboratory data in children with septicshock and purpura Intensive Care Med199420371ndash4
46 van Deuren M van der Ven-Jongekrijg JBartelink AK van Dalen R et alCorrelation between proinflammatorycytokines and antiinflammatorymediators and the severity of disease inmeningococcal infections J Infect Dis1995172433ndash9
47 Visser JJ Scholten RJ Hoekman K Nitricoxide synthesis in meningococcal menin-gitis Ann Intern Med 1994120345ndash6
48 Khilnani P Electrolyte abnormalities incritically ill children Crit Care Med199220241ndash50
49 Chernow B Calcium does it have atherapeutic role in sepsis Crit Care Med199018895ndash6
50 Gauthier B Trachtman H Di Carmine FUrivetsky M et al Hypocalcemia andhypercalcitoninemia in critically illchildren Crit Care Med 1990181215ndash9
51 Mauger DC Hypokalaemia as a consis-tent feature of fulminant meningococcalsepticaemia Aust Paediatr J 1971784ndash6
52 Weisinger JR Bellorin-Font E Magnesiumand phosphorus Lancet 1998352391ndash6
53 Pollard AJ Britto J Nadel S de Munter Cet al Emergency management ofmeningococcal disease Arch Dis Child199980290ndash6
54 Neu HC Cephalosporins in the treatmentof meningitis Drugs 198734(Suppl2)135ndash53
55 Carcillo JA Davis AL Zaritsky A Role ofearly fluid resuscitation in pediatric septicshock JAMA 19912661242ndash5
56 Dula DJ Lutz P Vogel MF Weaver BNRapid flow rates for the resuscitation ofhypovolemic shock Ann Emerg Med198514303ndash6
57 Nadel S De Munter C Britto J Levin MHabibi P Albumin saint or sinner ArchDis Child 199879384ndash5
58 Human albumin administration in criti-cally ill patients systematic review ofrandomised controlled trials CochraneInjuries Group Albumin Reviewers BrMed J 1998317235ndash40
59 Tobin JR Wetzel RC Shock and multi-organ failure In Rogers MC (ed)Textbook of pediatric intensive careBaltimore Williams and Wilkins1996555ndash605
60 Haneberg B Gutterberg TJ Moe PJOsterud B et al Heparin for infants andchildren with meningococcal septicemiaResults of a randomized therapeutic trialNIPH Ann 1983643ndash7
61 Zenz W Muntean W Zobel G GrubbauerHM Gallistl S Treatment of fulminantmeningococcemia with recombinanttissue plasminogen activator ThrombHaemost 199574802ndash3
62 Keeley SR Matthews NT Buist M Tissueplasminogen activator for gangrene infulminant meningococcaemia Lancet19913371359
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 443
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F

CM E Septicaem ia ndash I
treated for raised intracranial pressurewith mannitol frusemide and electiveintubation In addition standardneurointensive care practice such asnursing the patient at 30deg to thehorizontal and with the head midlineshould be maintained
Normal computed tomography (CT)scans do not exclude raised intracranialpressure Thus treatment for raisedintracranial pressure should be initiatedon clinical grounds without awaiting CTresults Lumbar puncture should beavoided in patients with a clinical diag-nosis of meningococcal disease due tothe risks associated with concomitantcoagulopathy intracranial hyper-tension and cardiac and respiratoryinsufficiency
New therapeutic possibilities(Table 1)
Patients with meningococcal infectionhave been given many experimentaltreatments including anti-inflammatoryanti-endotoxin strategies (Fig 2) and
anticoagulantfibrinolytic therapies (Fig3) Until the results of placebo-controlledtrials are available these treatmentsshould be restricted to units specificallyundertaking research in the disease
There have been reports of the useof tissue plasminogen activator andstreptokinase protein C and heparin inpatients with purpura fulminanssecondary to sepsis61ndash64 These agentscarry a significant risk of haemorrhage
Until their role in sepsis is determinedby properly controlled studies routineuse of these agents cannot berecommended65
In experimental models of shockvarious anti-cytokine and anti-endotoxin strategies have seemedpromising but have failed to reducemortality in randomised controlledtrials They included administration ofanti-TNF monoclonal antibodies66 and
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 441
Fig 3 Targets for novel anticoagulant fibr inolytic therapies in meningococcal sepsis Dotted arrows represent anticoagulant solid arrowsprocoagulant (ATIII = antithrombin III FDP = fibrinogen degradation product PAI = plasminogen activator inhibitor TNF = tumour necrosisfactor t-PA = tissue plasminogen activator TFPI = tissue factor plasminogen inhibitor)
Meningococcal endotoxinCD14(LPSreceptor)
Inflammatorycells
Monoclonal anti-TNF
Reactive oxygen species NO
Proinflammatory cytokines(including TNF-a IL-1b)
NOS inhibitors
rBPI21Monoclonal anti-LPS
Fig 2 Targets for novel anti- inflammatory therapies in sepsis(IL = interleukin LPS = lipopolysaccharide NO = nitric oxide NOS = NO synthase rBPI21 = recombinant bactericidal permeabilityincreasing protein TNF = tumour necrosis factor)
CM E Sept icaem ia ndash I
anti-endotoxin (HA-1A) monoclonalantibody67 A trial of the anti-endotoxinagent recombinant bactericidalpermeability increasing protein(rBPI21)68 has been recently completedand the results will be published soonPreliminary data suggest that recombi-nant high-density lipoprotein has anti-endotoxin properties6970 and furtherinvestigation of its clinical benefit isbeing undertaken
Prevention
Community prevention of secondarycases
Chemoprophylaxis for householdcontacts is recommended Other indi-viduals having close physical contactsuch as in day-care centres or kissingcontacts should also receive prophy-lactic treatment Rifampicin is the drugof choice Ciprofloxacin and ceftriaxoneare good but unlicensed alternatives
Medical staff prophylaxis
Chemoprophylaxis is recommended formedical personnel exposed to oralsecretions such as during intubationOther hospital and laboratory personneldo not have an increased risk ofinfection and prophylaxis is notrecommended
Vaccination
At present unconjugated polysaccha-ride vaccines for serogroups A C W-135and Y are available These confer effec-
tive protection for up to three years inchildren over two years old69 The groupB meningococcal polysaccharide closelymimics a human neuronal adhesionmolecule70 and is non-immunogenic Anumber of outer membrane proteinvaccines have been developed whichhave shown efficacy in outbreaks tospecific strains7172 There is currently novaccine that protects against the largenumber of group B strains circulating inthe UK
The introduction in 1999 of a massvaccination programme using a protein-conjugated group C polysaccharideshould reduce the incidence ofmeningococcal disease in the UK by40 However there remains concernthat this vaccine may lead to a shifttowards a higher incidence of group Bdisease Public awareness of thecontinued need for vigilance earlyidentification and management of thedisease is therefore of great importance
Acknowledgements
The authors are grateful to Dr S Faustfor help in construction of the coagula-tion pathway algorithm (Fig 3) also Dr TAli for helpful advice Dr N Pathan isfunded by a British Heart FoundationJunior Research Fellowship
R eferences
1 Platt MJ Child health statistical review1997 Arch Dis Child 199777542ndash8
2 Invasive meningococcal infectionsCommun Dis Rep CDR Wkly 199555
3 Riordan FA Marzouk O Thomson APSills JA Hart CA The changing presenta-
tions of meningococcal disease Eur JPediatr 1995154472ndash4
4 Ramsay M Kaczmarski E Rush MMallard R et al Changing patterns ofcase ascertainment and trends inmeningococcal disease in England andWales Commun Dis Rep CDR Rev19977R49ndash54
5 Lapeyssonnie L La meacuteningite ceacutereacutebro-spinale en Afrique Bull WHO 196328(Suppl 1)3ndash114
6 Moore PS Hierholzer J DeWitt W GouanK et al Respiratory viruses andmycoplasma as cofactors for epidemicgroup A meningococcal meningitis JAMA19902641271ndash5
7 Virji M Kayhty H Ferguson DJAlexandrescu C et al The role of pili inthe interactions of pathogenic Neisseriawith cultured human endothelial cellsMol Microbiol 199151831ndash41
8 Stephens DS McGee ZA Melly MAHoffman LH Gregg CR Attachment ofpathogenic Neisseria to human mucosalsurfaces role in pathogenesis Infection198210192ndash5
9 de Vries FP Cole R Dankert J Frosch Mvan Putten JP Neisseria meningitidisproducing the Opc adhesin bindsepithelial cell proteoglycan receptorsMol Microbiol 1998271203ndash12
10 Vitovski S Read RC Sayers JR Invasiveisolates of Neisseria meningitidis possessenhanced immunoglobulin A1 proteaseactivity compared to colonizing strainsFASEB J 199913331ndash7
11 Nassif X So M Interaction of pathogenicneisseriae with nonphagocytic cells ClinMicrobiol Rev 19958376ndash88
12 de Vries FP Van Der Ende A van PuttenJP Dankert J Invasion of primarynasopharyngeal epithelial cells byNeisseria meningitidis is controlled byphase variation of multiple surface anti-gens Infect Immun 1996642998ndash3006
13 Mulks MH Plaut AG IgA protease pro-duction as a characteristic distinguishingpathogenic from harmless neisseriaceaeN Engl J Med 1978299973ndash6
14 Virji M Makepeace K Peak IR FergusonDJ et al Opc- and pilus-dependent inter-actions of meningococci with humanendothelial cells molecular mechanismsand modulation by surface polysaccha-rides Mol Microbiol 199518741ndash54
15 Vogel U Hammerschmidt S Frosch MSialic acids of both the capsule and thesialylated lipooligosaccharide of Neisseriameningitis serogroup B are prerequisitesfor virulence of meningococci in theinfant rat Med Microbiol Immunol (Berl)199618581ndash7
16 Klein NJ Ison CA Peakman M Levin Met al The influence of capsulation andlipooligosaccharide structure onneutrophil adhesion molecule expres-sion and endothelial injury by Neisseriameningitidis J Infect Dis 1996173172ndash9
17 Estabrook MM Griffiss JM Jarvis GASialylation of Neisseria meningitidislipooligosaccharide inhibits serum
442 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
copy Meningococcal septicaemia has a 10 mortality overall in the UK
copy The major features of meningococcal septicaemia include capillary leak
coagulopathy myocardial dysfunction and metabolic derangements
copy Management should begin with attent ion to airway breathing and circulation
problems
copy Lumbar puncture should not be performed acutely in patients w ith a clinical
diagnosis of meningococcal disease
copy Mass vaccination against group C disease should reduce the incidence of
meningococcal disease by 40 in the UK how ever no vaccination exists for
serogroup B so there is a need for continued vigilance
Key Points
CM E Septicaem ia ndash I
bactericidal activity by masking lacto-N-neotetraose Infect Immun 1997654436ndash44
18 Jarvis GA Vedros NA Sialic acid of groupB Neisseria meningitidis regulates alterna-tive complement pathway activationInfect Immun 198755174ndash80
19 Andersen BM Endotoxin release fromNeisseria meningitidis Relationshipbetween key bacterial characteristics andmeningococcal disease Review Scand JInfect Dis 198964(Suppl)1ndash43
20 Peter G Weigert MB Bissel AR Gold R etal Meningococcal meningitis in familialdeficiency of the fifth component ofcomplement Pediatrics 198167882ndash6
21 Herva E Leinonen M Kayhty H MakelaPH Vetoniemi-Korhonen SL Recurrentmeningococcal meningitis due to partialcomplement defects and poor anti-meningococcal antibody response JInfect 1983655ndash60
22 Sjoholm AG Braconier JH Soderstrom CProperdin deficiency in a family withfulminant meningococcal infections ClinExp Immunol 198250291ndash7
23 Ross SC Densen P Complementdeficiency states and infection epidemi-ology pathogenesis and consequencesof neisserial and other infections in animmune deficiency Medicine (Baltimore)198463243ndash73
24 Ernst T Spath PJ Aebi C Schaad UBBianchetti MG Screening for comple-ment deficiency in bacterial meningitisActa Paediatr 1997861009ndash10
25 Jack DL Dodds AW Anwar N Ison CA etal Activation of complement bymannose-binding lectin on isogenicmutants of Neisseria meningitidisserogroup B J Immunol 19981601346ndash53
26 Hibberd ML Sumiya M Summerfield JABooy R Levin M Association of variantsof the gene for mannose-binding lectinwith susceptibility to meningococca ldisease Lancet 19993531049ndash53
27 Nadel S Newport MJ Booy R Levin MVariation in the tumor necrosis factor-alpha gene promoter region may beassociated with death from meningococ-cal disease J Infect Dis 1996174878ndash80
28 Waage A Halstensen A Espevik TAssociation between tumour necrosisfactor in serum and fatal outcome inpatients with meningococcal diseaseLancet 1987i355ndash7
29 Gardlund B Sjolin J Nilsson A Roll M etal Plasma levels of cytokines in primaryseptic shock in humans correlation withdisease severity J Infect Dis 1995172296ndash301
30 Brandtzaeg P Kierulf P Gaustad PSkulberg A et al Plasma endotoxin as apredictor of multiple organ failure anddeath in systemic meningococca ldisease J Infect Dis 1989159195ndash204
31 Brandtzaeg P Joo GB Brusletto B KierulfP Plasminogen activator inhibitor 1 and2 alpha-2-antiplasmin plasminogenand endotoxin levels in systemic
meningococca l disease Thromb Res199057271ndash8
32 Kornelisse RF Hazelzet JA Savelkoul HFHop WC et al The relationship betweenplasminogen activator inhibitor-1 andproinflammatory and counterinflamma-tory mediators in children with meningo-cocca l septic shock J Infect Dis19961731148ndash56
33 Westendorp RG Hottenga JJ SlagboomPE Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococ-cal septic shock Lancet 1999354561ndash3
34 Flaegstad T Kaaresen PI Stokland TGutteberg T Factors associated with fataloutcome in childhood meningococcaldisease Acta Paediatr 1995841137ndash42
35 LeClerc F Beuscart R Guillo is BDiependaele JF et al Prognostic factorsof severe infectious purpura in childrenIntensive Care Med 198511140ndash3
36 Mercier JC Beaufils F Hartmann JFAzema D Hemodynamic patterns ofmeningococcal shock in children CritCare Med 19881627ndash33
37 Fijnvandraat K Peters M Derkx B VanDeventer S ten Cate JW Endotoxininduced coagulation activation andprotein C reduction in meningococcalseptic shock Prog Clin Biol Res1994388247ndash54
38 Fijnvandraat K Derkx B Peters M BijlmerR et al Coagulation activation and tissuenecrosis in meningococcal septic shockseverely reduced protein C levels predicta high mortality Thromb Haemost19957315ndash20
39 Brandtzaeg P Sandset PM Joo GBOvstebo R et al The quantitative associ-ation of plasma endotoxin antithrombinprotein C extrinsic pathway inhibitor andfibrinopeptide A in systemic meningococ-cal disease Thromb Res 198955459ndash70
40 Heyderman RS Klein NJ Daramola OAHammerschmidt S et al Induction ofhuman endothelial tissue factor expres-sion by Neisseria meningitidis the influ-ence of bacterial killing and adherenceto the endothelium Microb Pathog199722265ndash74
41 Monsalve F Rucabadol L Salvador ABonastre J et al Myocardial depressionin septic shock caused by meningococcalinfection Crit Care Med 1984121021ndash3
42 Cunnion RE Schaer GL Parker MMNatanson C Parrillo JE The coronarycirculation in human septic shockCirculation 198673637ndash44
43 Dhainaut JF Huyghebaert MF MonsallierJF Lefevre G et al Coronary hemo-dynamics and myocardial metabolism oflactate free fatty acids glucose andketones in patients with septic shockCirculation 198775533ndash41
44 Parrillo JE Burch C Shelhamer JH ParkerMM et al A circulating myocardialdepressant substance in humans withseptic shock J Clin Invest 1985761539ndash53
45 Hazelzet JA van der Voort E LindemansJ ter Heerdt PJ Neijens HJ Relation
between cytokines and routinelaboratory data in children with septicshock and purpura Intensive Care Med199420371ndash4
46 van Deuren M van der Ven-Jongekrijg JBartelink AK van Dalen R et alCorrelation between proinflammatorycytokines and antiinflammatorymediators and the severity of disease inmeningococcal infections J Infect Dis1995172433ndash9
47 Visser JJ Scholten RJ Hoekman K Nitricoxide synthesis in meningococcal menin-gitis Ann Intern Med 1994120345ndash6
48 Khilnani P Electrolyte abnormalities incritically ill children Crit Care Med199220241ndash50
49 Chernow B Calcium does it have atherapeutic role in sepsis Crit Care Med199018895ndash6
50 Gauthier B Trachtman H Di Carmine FUrivetsky M et al Hypocalcemia andhypercalcitoninemia in critically illchildren Crit Care Med 1990181215ndash9
51 Mauger DC Hypokalaemia as a consis-tent feature of fulminant meningococcalsepticaemia Aust Paediatr J 1971784ndash6
52 Weisinger JR Bellorin-Font E Magnesiumand phosphorus Lancet 1998352391ndash6
53 Pollard AJ Britto J Nadel S de Munter Cet al Emergency management ofmeningococcal disease Arch Dis Child199980290ndash6
54 Neu HC Cephalosporins in the treatmentof meningitis Drugs 198734(Suppl2)135ndash53
55 Carcillo JA Davis AL Zaritsky A Role ofearly fluid resuscitation in pediatric septicshock JAMA 19912661242ndash5
56 Dula DJ Lutz P Vogel MF Weaver BNRapid flow rates for the resuscitation ofhypovolemic shock Ann Emerg Med198514303ndash6
57 Nadel S De Munter C Britto J Levin MHabibi P Albumin saint or sinner ArchDis Child 199879384ndash5
58 Human albumin administration in criti-cally ill patients systematic review ofrandomised controlled trials CochraneInjuries Group Albumin Reviewers BrMed J 1998317235ndash40
59 Tobin JR Wetzel RC Shock and multi-organ failure In Rogers MC (ed)Textbook of pediatric intensive careBaltimore Williams and Wilkins1996555ndash605
60 Haneberg B Gutterberg TJ Moe PJOsterud B et al Heparin for infants andchildren with meningococcal septicemiaResults of a randomized therapeutic trialNIPH Ann 1983643ndash7
61 Zenz W Muntean W Zobel G GrubbauerHM Gallistl S Treatment of fulminantmeningococcemia with recombinanttissue plasminogen activator ThrombHaemost 199574802ndash3
62 Keeley SR Matthews NT Buist M Tissueplasminogen activator for gangrene infulminant meningococcaemia Lancet19913371359
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 443
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F

CM E Sept icaem ia ndash I
anti-endotoxin (HA-1A) monoclonalantibody67 A trial of the anti-endotoxinagent recombinant bactericidalpermeability increasing protein(rBPI21)68 has been recently completedand the results will be published soonPreliminary data suggest that recombi-nant high-density lipoprotein has anti-endotoxin properties6970 and furtherinvestigation of its clinical benefit isbeing undertaken
Prevention
Community prevention of secondarycases
Chemoprophylaxis for householdcontacts is recommended Other indi-viduals having close physical contactsuch as in day-care centres or kissingcontacts should also receive prophy-lactic treatment Rifampicin is the drugof choice Ciprofloxacin and ceftriaxoneare good but unlicensed alternatives
Medical staff prophylaxis
Chemoprophylaxis is recommended formedical personnel exposed to oralsecretions such as during intubationOther hospital and laboratory personneldo not have an increased risk ofinfection and prophylaxis is notrecommended
Vaccination
At present unconjugated polysaccha-ride vaccines for serogroups A C W-135and Y are available These confer effec-
tive protection for up to three years inchildren over two years old69 The groupB meningococcal polysaccharide closelymimics a human neuronal adhesionmolecule70 and is non-immunogenic Anumber of outer membrane proteinvaccines have been developed whichhave shown efficacy in outbreaks tospecific strains7172 There is currently novaccine that protects against the largenumber of group B strains circulating inthe UK
The introduction in 1999 of a massvaccination programme using a protein-conjugated group C polysaccharideshould reduce the incidence ofmeningococcal disease in the UK by40 However there remains concernthat this vaccine may lead to a shifttowards a higher incidence of group Bdisease Public awareness of thecontinued need for vigilance earlyidentification and management of thedisease is therefore of great importance
Acknowledgements
The authors are grateful to Dr S Faustfor help in construction of the coagula-tion pathway algorithm (Fig 3) also Dr TAli for helpful advice Dr N Pathan isfunded by a British Heart FoundationJunior Research Fellowship
R eferences
1 Platt MJ Child health statistical review1997 Arch Dis Child 199777542ndash8
2 Invasive meningococcal infectionsCommun Dis Rep CDR Wkly 199555
3 Riordan FA Marzouk O Thomson APSills JA Hart CA The changing presenta-
tions of meningococcal disease Eur JPediatr 1995154472ndash4
4 Ramsay M Kaczmarski E Rush MMallard R et al Changing patterns ofcase ascertainment and trends inmeningococcal disease in England andWales Commun Dis Rep CDR Rev19977R49ndash54
5 Lapeyssonnie L La meacuteningite ceacutereacutebro-spinale en Afrique Bull WHO 196328(Suppl 1)3ndash114
6 Moore PS Hierholzer J DeWitt W GouanK et al Respiratory viruses andmycoplasma as cofactors for epidemicgroup A meningococcal meningitis JAMA19902641271ndash5
7 Virji M Kayhty H Ferguson DJAlexandrescu C et al The role of pili inthe interactions of pathogenic Neisseriawith cultured human endothelial cellsMol Microbiol 199151831ndash41
8 Stephens DS McGee ZA Melly MAHoffman LH Gregg CR Attachment ofpathogenic Neisseria to human mucosalsurfaces role in pathogenesis Infection198210192ndash5
9 de Vries FP Cole R Dankert J Frosch Mvan Putten JP Neisseria meningitidisproducing the Opc adhesin bindsepithelial cell proteoglycan receptorsMol Microbiol 1998271203ndash12
10 Vitovski S Read RC Sayers JR Invasiveisolates of Neisseria meningitidis possessenhanced immunoglobulin A1 proteaseactivity compared to colonizing strainsFASEB J 199913331ndash7
11 Nassif X So M Interaction of pathogenicneisseriae with nonphagocytic cells ClinMicrobiol Rev 19958376ndash88
12 de Vries FP Van Der Ende A van PuttenJP Dankert J Invasion of primarynasopharyngeal epithelial cells byNeisseria meningitidis is controlled byphase variation of multiple surface anti-gens Infect Immun 1996642998ndash3006
13 Mulks MH Plaut AG IgA protease pro-duction as a characteristic distinguishingpathogenic from harmless neisseriaceaeN Engl J Med 1978299973ndash6
14 Virji M Makepeace K Peak IR FergusonDJ et al Opc- and pilus-dependent inter-actions of meningococci with humanendothelial cells molecular mechanismsand modulation by surface polysaccha-rides Mol Microbiol 199518741ndash54
15 Vogel U Hammerschmidt S Frosch MSialic acids of both the capsule and thesialylated lipooligosaccharide of Neisseriameningitis serogroup B are prerequisitesfor virulence of meningococci in theinfant rat Med Microbiol Immunol (Berl)199618581ndash7
16 Klein NJ Ison CA Peakman M Levin Met al The influence of capsulation andlipooligosaccharide structure onneutrophil adhesion molecule expres-sion and endothelial injury by Neisseriameningitidis J Infect Dis 1996173172ndash9
17 Estabrook MM Griffiss JM Jarvis GASialylation of Neisseria meningitidislipooligosaccharide inhibits serum
442 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
copy Meningococcal septicaemia has a 10 mortality overall in the UK
copy The major features of meningococcal septicaemia include capillary leak
coagulopathy myocardial dysfunction and metabolic derangements
copy Management should begin with attent ion to airway breathing and circulation
problems
copy Lumbar puncture should not be performed acutely in patients w ith a clinical
diagnosis of meningococcal disease
copy Mass vaccination against group C disease should reduce the incidence of
meningococcal disease by 40 in the UK how ever no vaccination exists for
serogroup B so there is a need for continued vigilance
Key Points
CM E Septicaem ia ndash I
bactericidal activity by masking lacto-N-neotetraose Infect Immun 1997654436ndash44
18 Jarvis GA Vedros NA Sialic acid of groupB Neisseria meningitidis regulates alterna-tive complement pathway activationInfect Immun 198755174ndash80
19 Andersen BM Endotoxin release fromNeisseria meningitidis Relationshipbetween key bacterial characteristics andmeningococcal disease Review Scand JInfect Dis 198964(Suppl)1ndash43
20 Peter G Weigert MB Bissel AR Gold R etal Meningococcal meningitis in familialdeficiency of the fifth component ofcomplement Pediatrics 198167882ndash6
21 Herva E Leinonen M Kayhty H MakelaPH Vetoniemi-Korhonen SL Recurrentmeningococcal meningitis due to partialcomplement defects and poor anti-meningococcal antibody response JInfect 1983655ndash60
22 Sjoholm AG Braconier JH Soderstrom CProperdin deficiency in a family withfulminant meningococcal infections ClinExp Immunol 198250291ndash7
23 Ross SC Densen P Complementdeficiency states and infection epidemi-ology pathogenesis and consequencesof neisserial and other infections in animmune deficiency Medicine (Baltimore)198463243ndash73
24 Ernst T Spath PJ Aebi C Schaad UBBianchetti MG Screening for comple-ment deficiency in bacterial meningitisActa Paediatr 1997861009ndash10
25 Jack DL Dodds AW Anwar N Ison CA etal Activation of complement bymannose-binding lectin on isogenicmutants of Neisseria meningitidisserogroup B J Immunol 19981601346ndash53
26 Hibberd ML Sumiya M Summerfield JABooy R Levin M Association of variantsof the gene for mannose-binding lectinwith susceptibility to meningococca ldisease Lancet 19993531049ndash53
27 Nadel S Newport MJ Booy R Levin MVariation in the tumor necrosis factor-alpha gene promoter region may beassociated with death from meningococ-cal disease J Infect Dis 1996174878ndash80
28 Waage A Halstensen A Espevik TAssociation between tumour necrosisfactor in serum and fatal outcome inpatients with meningococcal diseaseLancet 1987i355ndash7
29 Gardlund B Sjolin J Nilsson A Roll M etal Plasma levels of cytokines in primaryseptic shock in humans correlation withdisease severity J Infect Dis 1995172296ndash301
30 Brandtzaeg P Kierulf P Gaustad PSkulberg A et al Plasma endotoxin as apredictor of multiple organ failure anddeath in systemic meningococca ldisease J Infect Dis 1989159195ndash204
31 Brandtzaeg P Joo GB Brusletto B KierulfP Plasminogen activator inhibitor 1 and2 alpha-2-antiplasmin plasminogenand endotoxin levels in systemic
meningococca l disease Thromb Res199057271ndash8
32 Kornelisse RF Hazelzet JA Savelkoul HFHop WC et al The relationship betweenplasminogen activator inhibitor-1 andproinflammatory and counterinflamma-tory mediators in children with meningo-cocca l septic shock J Infect Dis19961731148ndash56
33 Westendorp RG Hottenga JJ SlagboomPE Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococ-cal septic shock Lancet 1999354561ndash3
34 Flaegstad T Kaaresen PI Stokland TGutteberg T Factors associated with fataloutcome in childhood meningococcaldisease Acta Paediatr 1995841137ndash42
35 LeClerc F Beuscart R Guillo is BDiependaele JF et al Prognostic factorsof severe infectious purpura in childrenIntensive Care Med 198511140ndash3
36 Mercier JC Beaufils F Hartmann JFAzema D Hemodynamic patterns ofmeningococcal shock in children CritCare Med 19881627ndash33
37 Fijnvandraat K Peters M Derkx B VanDeventer S ten Cate JW Endotoxininduced coagulation activation andprotein C reduction in meningococcalseptic shock Prog Clin Biol Res1994388247ndash54
38 Fijnvandraat K Derkx B Peters M BijlmerR et al Coagulation activation and tissuenecrosis in meningococcal septic shockseverely reduced protein C levels predicta high mortality Thromb Haemost19957315ndash20
39 Brandtzaeg P Sandset PM Joo GBOvstebo R et al The quantitative associ-ation of plasma endotoxin antithrombinprotein C extrinsic pathway inhibitor andfibrinopeptide A in systemic meningococ-cal disease Thromb Res 198955459ndash70
40 Heyderman RS Klein NJ Daramola OAHammerschmidt S et al Induction ofhuman endothelial tissue factor expres-sion by Neisseria meningitidis the influ-ence of bacterial killing and adherenceto the endothelium Microb Pathog199722265ndash74
41 Monsalve F Rucabadol L Salvador ABonastre J et al Myocardial depressionin septic shock caused by meningococcalinfection Crit Care Med 1984121021ndash3
42 Cunnion RE Schaer GL Parker MMNatanson C Parrillo JE The coronarycirculation in human septic shockCirculation 198673637ndash44
43 Dhainaut JF Huyghebaert MF MonsallierJF Lefevre G et al Coronary hemo-dynamics and myocardial metabolism oflactate free fatty acids glucose andketones in patients with septic shockCirculation 198775533ndash41
44 Parrillo JE Burch C Shelhamer JH ParkerMM et al A circulating myocardialdepressant substance in humans withseptic shock J Clin Invest 1985761539ndash53
45 Hazelzet JA van der Voort E LindemansJ ter Heerdt PJ Neijens HJ Relation
between cytokines and routinelaboratory data in children with septicshock and purpura Intensive Care Med199420371ndash4
46 van Deuren M van der Ven-Jongekrijg JBartelink AK van Dalen R et alCorrelation between proinflammatorycytokines and antiinflammatorymediators and the severity of disease inmeningococcal infections J Infect Dis1995172433ndash9
47 Visser JJ Scholten RJ Hoekman K Nitricoxide synthesis in meningococcal menin-gitis Ann Intern Med 1994120345ndash6
48 Khilnani P Electrolyte abnormalities incritically ill children Crit Care Med199220241ndash50
49 Chernow B Calcium does it have atherapeutic role in sepsis Crit Care Med199018895ndash6
50 Gauthier B Trachtman H Di Carmine FUrivetsky M et al Hypocalcemia andhypercalcitoninemia in critically illchildren Crit Care Med 1990181215ndash9
51 Mauger DC Hypokalaemia as a consis-tent feature of fulminant meningococcalsepticaemia Aust Paediatr J 1971784ndash6
52 Weisinger JR Bellorin-Font E Magnesiumand phosphorus Lancet 1998352391ndash6
53 Pollard AJ Britto J Nadel S de Munter Cet al Emergency management ofmeningococcal disease Arch Dis Child199980290ndash6
54 Neu HC Cephalosporins in the treatmentof meningitis Drugs 198734(Suppl2)135ndash53
55 Carcillo JA Davis AL Zaritsky A Role ofearly fluid resuscitation in pediatric septicshock JAMA 19912661242ndash5
56 Dula DJ Lutz P Vogel MF Weaver BNRapid flow rates for the resuscitation ofhypovolemic shock Ann Emerg Med198514303ndash6
57 Nadel S De Munter C Britto J Levin MHabibi P Albumin saint or sinner ArchDis Child 199879384ndash5
58 Human albumin administration in criti-cally ill patients systematic review ofrandomised controlled trials CochraneInjuries Group Albumin Reviewers BrMed J 1998317235ndash40
59 Tobin JR Wetzel RC Shock and multi-organ failure In Rogers MC (ed)Textbook of pediatric intensive careBaltimore Williams and Wilkins1996555ndash605
60 Haneberg B Gutterberg TJ Moe PJOsterud B et al Heparin for infants andchildren with meningococcal septicemiaResults of a randomized therapeutic trialNIPH Ann 1983643ndash7
61 Zenz W Muntean W Zobel G GrubbauerHM Gallistl S Treatment of fulminantmeningococcemia with recombinanttissue plasminogen activator ThrombHaemost 199574802ndash3
62 Keeley SR Matthews NT Buist M Tissueplasminogen activator for gangrene infulminant meningococcaemia Lancet19913371359
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 443
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F

CM E Septicaem ia ndash I
bactericidal activity by masking lacto-N-neotetraose Infect Immun 1997654436ndash44
18 Jarvis GA Vedros NA Sialic acid of groupB Neisseria meningitidis regulates alterna-tive complement pathway activationInfect Immun 198755174ndash80
19 Andersen BM Endotoxin release fromNeisseria meningitidis Relationshipbetween key bacterial characteristics andmeningococcal disease Review Scand JInfect Dis 198964(Suppl)1ndash43
20 Peter G Weigert MB Bissel AR Gold R etal Meningococcal meningitis in familialdeficiency of the fifth component ofcomplement Pediatrics 198167882ndash6
21 Herva E Leinonen M Kayhty H MakelaPH Vetoniemi-Korhonen SL Recurrentmeningococcal meningitis due to partialcomplement defects and poor anti-meningococcal antibody response JInfect 1983655ndash60
22 Sjoholm AG Braconier JH Soderstrom CProperdin deficiency in a family withfulminant meningococcal infections ClinExp Immunol 198250291ndash7
23 Ross SC Densen P Complementdeficiency states and infection epidemi-ology pathogenesis and consequencesof neisserial and other infections in animmune deficiency Medicine (Baltimore)198463243ndash73
24 Ernst T Spath PJ Aebi C Schaad UBBianchetti MG Screening for comple-ment deficiency in bacterial meningitisActa Paediatr 1997861009ndash10
25 Jack DL Dodds AW Anwar N Ison CA etal Activation of complement bymannose-binding lectin on isogenicmutants of Neisseria meningitidisserogroup B J Immunol 19981601346ndash53
26 Hibberd ML Sumiya M Summerfield JABooy R Levin M Association of variantsof the gene for mannose-binding lectinwith susceptibility to meningococca ldisease Lancet 19993531049ndash53
27 Nadel S Newport MJ Booy R Levin MVariation in the tumor necrosis factor-alpha gene promoter region may beassociated with death from meningococ-cal disease J Infect Dis 1996174878ndash80
28 Waage A Halstensen A Espevik TAssociation between tumour necrosisfactor in serum and fatal outcome inpatients with meningococcal diseaseLancet 1987i355ndash7
29 Gardlund B Sjolin J Nilsson A Roll M etal Plasma levels of cytokines in primaryseptic shock in humans correlation withdisease severity J Infect Dis 1995172296ndash301
30 Brandtzaeg P Kierulf P Gaustad PSkulberg A et al Plasma endotoxin as apredictor of multiple organ failure anddeath in systemic meningococca ldisease J Infect Dis 1989159195ndash204
31 Brandtzaeg P Joo GB Brusletto B KierulfP Plasminogen activator inhibitor 1 and2 alpha-2-antiplasmin plasminogenand endotoxin levels in systemic
meningococca l disease Thromb Res199057271ndash8
32 Kornelisse RF Hazelzet JA Savelkoul HFHop WC et al The relationship betweenplasminogen activator inhibitor-1 andproinflammatory and counterinflamma-tory mediators in children with meningo-cocca l septic shock J Infect Dis19961731148ndash56
33 Westendorp RG Hottenga JJ SlagboomPE Variation in plasminogen-activator-inhibitor-1 gene and risk of meningococ-cal septic shock Lancet 1999354561ndash3
34 Flaegstad T Kaaresen PI Stokland TGutteberg T Factors associated with fataloutcome in childhood meningococcaldisease Acta Paediatr 1995841137ndash42
35 LeClerc F Beuscart R Guillo is BDiependaele JF et al Prognostic factorsof severe infectious purpura in childrenIntensive Care Med 198511140ndash3
36 Mercier JC Beaufils F Hartmann JFAzema D Hemodynamic patterns ofmeningococcal shock in children CritCare Med 19881627ndash33
37 Fijnvandraat K Peters M Derkx B VanDeventer S ten Cate JW Endotoxininduced coagulation activation andprotein C reduction in meningococcalseptic shock Prog Clin Biol Res1994388247ndash54
38 Fijnvandraat K Derkx B Peters M BijlmerR et al Coagulation activation and tissuenecrosis in meningococcal septic shockseverely reduced protein C levels predicta high mortality Thromb Haemost19957315ndash20
39 Brandtzaeg P Sandset PM Joo GBOvstebo R et al The quantitative associ-ation of plasma endotoxin antithrombinprotein C extrinsic pathway inhibitor andfibrinopeptide A in systemic meningococ-cal disease Thromb Res 198955459ndash70
40 Heyderman RS Klein NJ Daramola OAHammerschmidt S et al Induction ofhuman endothelial tissue factor expres-sion by Neisseria meningitidis the influ-ence of bacterial killing and adherenceto the endothelium Microb Pathog199722265ndash74
41 Monsalve F Rucabadol L Salvador ABonastre J et al Myocardial depressionin septic shock caused by meningococcalinfection Crit Care Med 1984121021ndash3
42 Cunnion RE Schaer GL Parker MMNatanson C Parrillo JE The coronarycirculation in human septic shockCirculation 198673637ndash44
43 Dhainaut JF Huyghebaert MF MonsallierJF Lefevre G et al Coronary hemo-dynamics and myocardial metabolism oflactate free fatty acids glucose andketones in patients with septic shockCirculation 198775533ndash41
44 Parrillo JE Burch C Shelhamer JH ParkerMM et al A circulating myocardialdepressant substance in humans withseptic shock J Clin Invest 1985761539ndash53
45 Hazelzet JA van der Voort E LindemansJ ter Heerdt PJ Neijens HJ Relation
between cytokines and routinelaboratory data in children with septicshock and purpura Intensive Care Med199420371ndash4
46 van Deuren M van der Ven-Jongekrijg JBartelink AK van Dalen R et alCorrelation between proinflammatorycytokines and antiinflammatorymediators and the severity of disease inmeningococcal infections J Infect Dis1995172433ndash9
47 Visser JJ Scholten RJ Hoekman K Nitricoxide synthesis in meningococcal menin-gitis Ann Intern Med 1994120345ndash6
48 Khilnani P Electrolyte abnormalities incritically ill children Crit Care Med199220241ndash50
49 Chernow B Calcium does it have atherapeutic role in sepsis Crit Care Med199018895ndash6
50 Gauthier B Trachtman H Di Carmine FUrivetsky M et al Hypocalcemia andhypercalcitoninemia in critically illchildren Crit Care Med 1990181215ndash9
51 Mauger DC Hypokalaemia as a consis-tent feature of fulminant meningococcalsepticaemia Aust Paediatr J 1971784ndash6
52 Weisinger JR Bellorin-Font E Magnesiumand phosphorus Lancet 1998352391ndash6
53 Pollard AJ Britto J Nadel S de Munter Cet al Emergency management ofmeningococcal disease Arch Dis Child199980290ndash6
54 Neu HC Cephalosporins in the treatmentof meningitis Drugs 198734(Suppl2)135ndash53
55 Carcillo JA Davis AL Zaritsky A Role ofearly fluid resuscitation in pediatric septicshock JAMA 19912661242ndash5
56 Dula DJ Lutz P Vogel MF Weaver BNRapid flow rates for the resuscitation ofhypovolemic shock Ann Emerg Med198514303ndash6
57 Nadel S De Munter C Britto J Levin MHabibi P Albumin saint or sinner ArchDis Child 199879384ndash5
58 Human albumin administration in criti-cally ill patients systematic review ofrandomised controlled trials CochraneInjuries Group Albumin Reviewers BrMed J 1998317235ndash40
59 Tobin JR Wetzel RC Shock and multi-organ failure In Rogers MC (ed)Textbook of pediatric intensive careBaltimore Williams and Wilkins1996555ndash605
60 Haneberg B Gutterberg TJ Moe PJOsterud B et al Heparin for infants andchildren with meningococcal septicemiaResults of a randomized therapeutic trialNIPH Ann 1983643ndash7
61 Zenz W Muntean W Zobel G GrubbauerHM Gallistl S Treatment of fulminantmeningococcemia with recombinanttissue plasminogen activator ThrombHaemost 199574802ndash3
62 Keeley SR Matthews NT Buist M Tissueplasminogen activator for gangrene infulminant meningococcaemia Lancet19913371359
Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000 443
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F
CM E Sept icaem ia ndash I
63 Smith OP White B Vaughan D RaffertyM et al Use of protein-C concentrateheparin and haemodiafiltration inmeningococcus-induced purpurafulminans Lancet 19973501590ndash3
64 Kreuz W Veldman A Escuriola-Ettingshausen C Schneider W Beeg TProtein-C concentrate for meningococcalpurpura fulminans letter commentLancet 1998351986ndash7
65 Finn A Booy R Levin M Nadel S Faust SInfectious purpura fulminans cautionneeded in the use of protein C Br JHaematol 1999106253ndash4
66 Cohen J Monoclonal antibody to TNFalpha in septic shock letter Lancet19983511731
67 McCloskey RV Straube RC Sanders CSmith SM Smith CR Treatment of septicshock with human monoclonal antibodyHA-1A A randomized double-blindplacebo-controlled trial CHESS TrialStudy Group Ann Intern Med 19941211ndash5
68 Giroir BP Quint PA Barton P Kirsch EA etal Preliminary evaluation of recombi-nant amino-terminal fragment of humanbacteric ida l permeab ility -increasingprotein in children with severe meningo-coccal sepsis Lancet 19973501439ndash43
69 Lepow ML Beeler J Randolph MSamuelson JS Hankins WA Reacto-genicity and immunogenicity of a quadri-valent combined meningococcal poly-saccharide vaccine in children J Infect Dis19861541033ndash6
70 Finne J Leinonen M Makela PHAntigenic similarities between braincomponents and bacteria causingmeningitis Implica tions for vaccinedevelopment and pathogenesis Lancet1983ii355ndash7
71 de Moraes JC Perkins BA Camargo MCHidalgo NT et al Protective efficacy of aserogroup B meningococcal vaccine inSao Paulo Brazil Lancet 19923401074ndash8
72 Costa EA Effectiveness of meningococcalvaccine in Brazil Int J Epidemiol 199726681ndash4
Address for correspondence Professor MLevin Department of Paediatrics ImperialCollege School of Medicine Norfolk PlaceLondon W2 1PG
444 Journal of the Royal College of Physicians of London Vol 34 No 5 SeptemberOctober 2000
CM E Diabetes SAQs
Answers to CME SAQs included in JRCPL JulyAugust2000
Q1 Q2 Q3 Q4a) F a) T a) F a) Fb) F b) T b) F b) Fc) T c) T c) T c) Td) T d) F d) T d) Fe) F e) T e) T e) F
Q5 Q6 Q7 Q8a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) F c) T c) Fd) F d) T d) F d) Te) T e) F e) T e) F
Q9 Q10 Q11 Q12a) F a) F a) F a) Fb) F b) T b) T b) Fc) T c) T c) T c) Td) F d) F d) T d) Fe) F e) F e) T e) F
Q13 Q14 Q15 Q16a) T a) T a) T a) Tb) T b) T b) F b) Fc) F c) F c) T c) Td) F d) F d) F d) Te) T e) T e) T e) F
Q17 Q18 Q19 Q20a) F a) T a) F a) Tb) T b) F b) F b) Fc) F c) F c) T c) Fd) T d) T d) T d) Te) F e) T e) F e) F