patient safety & usability of medical devices part i 2004 fall ceso conference gill ginsburg,...
TRANSCRIPT

Patient Safety & Usability of Medical DevicesPart I
2004 Fall CESO Conference
Gill Ginsburg, M.A.Sc
Human Factors & Biomedical Engineer
Trillium Health Centre
Erin Barkel, B.A.Sc
Patient Safety/Risk Management Specialist
Niagara Health System

Outline – Part I
• Intro to usability
• Intro to Human Factors Engineering
• Why do users make mistakes?
• Intro to patient safety & medical error
• Canadian Adverse Events Study
• Examples

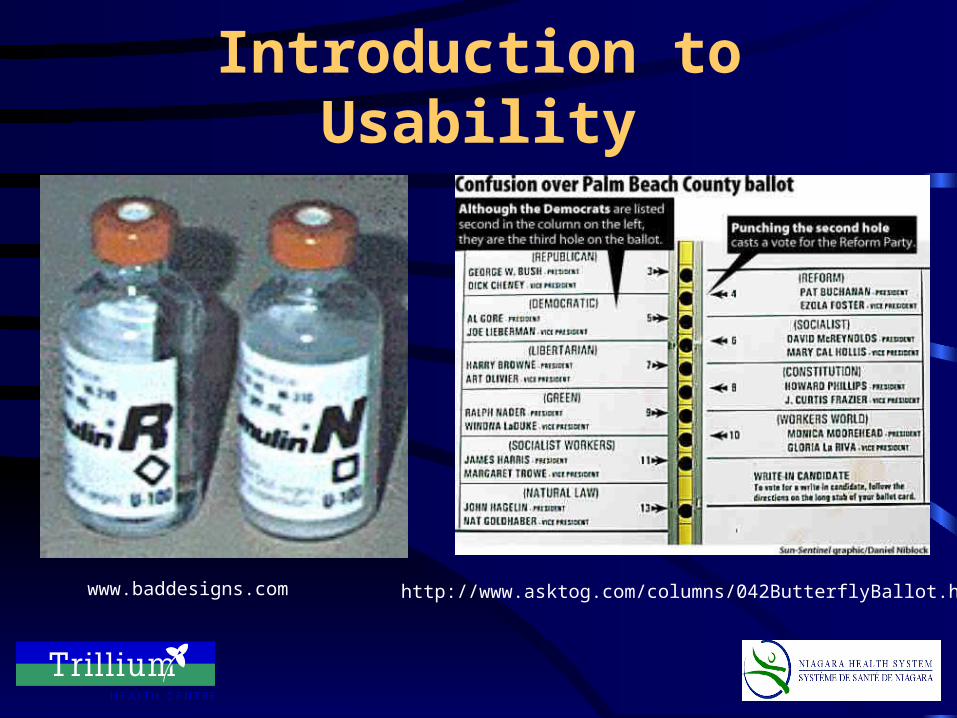
Introduction to Usability
Mike’s New CarMonsters, Inc.

Introduction to Usability
• Usability issues with Mike’s new car:– Complex dashboard
• Too many buttons / switches• Functions are not obvious• No logical grouping
– Hood is too high for Mike– Sully doesn’t fit– New & exciting features are too complicated to
use…Mike “wants his old car back”!

Introduction to Usability
www.baddesigns.com

Introduction to Usability
www.baddesigns.com
www.baddesigns.com

Introduction to Usability
www.baddesigns.com
www.baddesigns.com
X
Introduction to Usability
www.baddesigns.com http://www.asktog.com/columns/042ButterflyBallot.html

Introduction to Usability
Other Usability Examples
???

Introduction to HFE
• Human Factors Engineering (HFE) ensures that systems are easy-to-use
• Multidisciplinary: engineering, medicine, psychology, computing, statistics…etc.
• Design of systems according to Human Factors Principles…iterative process incorporating user feedback
• Evaluation of systems for usability, safety, efficiency & effectiveness

HFE Principles
Easy-to-use systems incorporate these Human Factors Principles:
•Visibility of system status•Consistency & standards•Match between system & world•Minimalist design•Minimize memory load•Informative feedback•Flexibility & efficiency
•Good error messages•Prevent errors•Clear closure•Reversible actions•Use user’s language•Users in control•Help & documentation
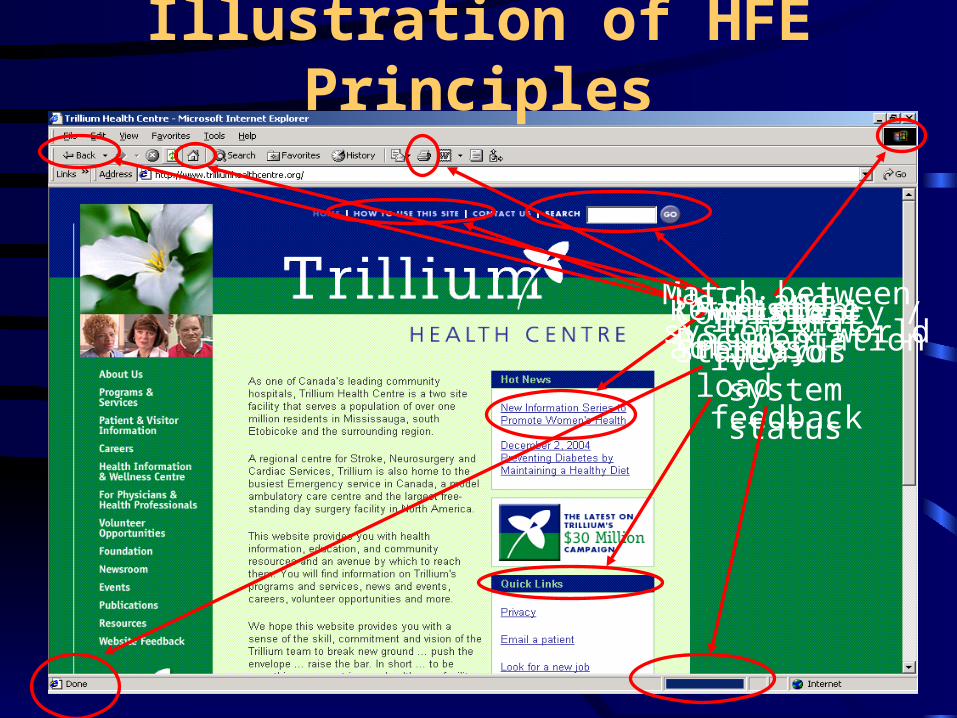
Illustration of HFE Principles
Consistency / Standards
Minimizememory load
Informative
feedback
Reversible actions
Help andDocumentation
Visibility of system status
Match betweensystem & world
An Easy-to-Use System is…• Effective
– Task completed, user’s goals met
• Efficient– Task completed quickly
without undue cognitive effort
• Easy-to-learn– System is predictable
and consistent
• Engaging– User experiences
pleasant interaction with the system
– User satisfied with how system supports completion of task
• Error tolerant– System prevents errors
and assists in error recovery

HFE Techniques to Ensure Usability of Systems
• Heuristic evaluation– How does the system violate the HFE principles?– What is the severity of the violations?
• User testing– Real users– Realistic tasks– What mistakes are made?– What is the severity of the mistakes?– Other performance measures: task completion time,
mental workload, user preference

• Observations
• Task analysis
• Work domain analysis
• Questionnaires
• Surveys
• Interviews
• Focus groups
HFE Techniques to Ensure Usability of Systems

Why do users make errors?
human error
Device iseasy-to-use
Device is not easy-to-use
DeviceUse
Work Environment•Light, noise•Distraction/Interruption•Workload
patient injury or death
User•Knowledge•Abilities•Expectations•Limitations
System•Operational requirements, procedures•Complexity•User interface characteristics
Adapted from Kaye & Crowley, 2000

Examples of Medical Error
• Incorrectly sterilizing equipment
• Administering wrong medication
• Administering wrong dose
• Administering wrong blood type
• Wrong site surgery
• Making an incorrect diagnosis
• Burning a patient

“Computers allow us to make mistakes faster than any other
invention in history”
-Unknown
Canadian Adverse Events Study
• Principal Investigators Ross Baker and Peter Norton
• Released May 2004
• Based on a review of 3,700 charts from 20 acute care facilities
• Year 2000 data
Methodology
• Nurses reviewed the charts looking for any of the 18 “triggers” that might indicate that an AE had occurred– 40.8% of charts had at least one trigger
• Charts were then reviewed by Doctors– Looking for evidence that an injury that caused
disability, death or a prolonged LOS was present
• Injury caused by “health care management”

Findings
• 1 in 13 patients will experience an AE– 255 of these AEs required an additional 1521
days in hospital– About 1 million bed days nation wide
• 5% of AEs resulted in permanent disability
• 16,500 deaths

Recommendations
• Near Miss/Close Catch Reporting– “Accident Ratio Study”
• Incident Reporting– Renewed efforts to promote incident reporting
• Using Root Cause Analysis to investigate incidents– Ask why 5x

Niagara Health System
• Last of the HSRC amalgamations, and the largest– 7 sites– 6 municipalities
• Population based of approximately 450,000

The Challenge
• Regionalization• 7 Distinct Site Cultures
– Different levels of awareness of patient safety– Different attitudes towards reporting– Different methods of reporting
• Need to standardize reporting– Consistent data set– Consistent, conscientious reporting

Standardize Data Collection
• In June 2004, 3 of 7 sites were using the Encon Incident Reporting system– The remaining 4 were using homemade forms
• Inservice sessions were run at the remaining 4 sites– As of September, all NHS sites are using Encon
Continuing Efforts
• Need for continuous inservicing– Maintain staff awareness– Develop awareness of Near Miss/Close Catch
situations– Increase visibility of Risk Management
initiatives and demonstrate accountability– Address staff fear (e.g. that reporting is
punitive)

Cautionary Note
• Increased volume is not reflective of a higher error rate– Incidents are presently under reported at most
facilities– Education of staff will lead to an increase in
reporting

Medication Safety Committee
• Part of our Service Excellence Initiative– Reporting to the “Inspiring Excellence
Council”
• Representatives from Risk Management, Pharmacy, Nursing, Human Resources and Finance
Medication Safety Committee
• First Year Goals– Increase incident reporting
• Complete/Revise the Regional Medication Administration Policy
• Provide education to frontline staff on the policy and the importance of reporting
• Work on developing the framework for a “Just Culture” (Marx, 2001)
– Creating a list of “Look-a-like, Sound-a-like” drugs in our facilities
• Implement a education strategy to reduce errors associated with these drugs
Other Projects
“Best-of-Breed”– Joint effort by Finance, Information
Technology and Biomedical Departments– Standardize purchasing – only the best
products, that are well supported and are usable, will be purchased

Projects at Trillium Health Centre
• Infusion pump selection
• Usability of bed alarms
• Usability of diagnostic imaging systems
• Incorporating human factors specifications into Request for Proposal process

• Background– Over 500 general-purpose IV pumps in hospital– Existing contract expiring– Need for “smart” features for patient safety
• Dose-error reduction
• Automated programming
– Need for standard pump across hospital
IV Pump Selection

IV Pump Selection
• 3 pumps after RFP
• Similar functionality & features
• Initial selection process not successful
• Used HFE to evaluate usability of pumps to:– Choose best pump for end users
– Enhance patient safety

• Heuristic Evaluation– Based on Human Factors principles– Revealed usability issues– Revealed information about causes of errors
• User testing– 5 clinical areas, 14 nurses & 3 anaesthetists– Realistic scenarios– Observed & recorded # of errors & severity
• Usability errors• Critical usability errors• Critical undetected usability errors
IV Pump Selection

IV Pump Selection
05
101520253035404550
Onc Surg Paeds ICU Anesth
Pump APump BPump C
Total Number of Usability Errors
IV Pump Selection
05
101520253035404550
Onc Surg Paeds ICU Anesth
Pump A
Pump B
Pump C
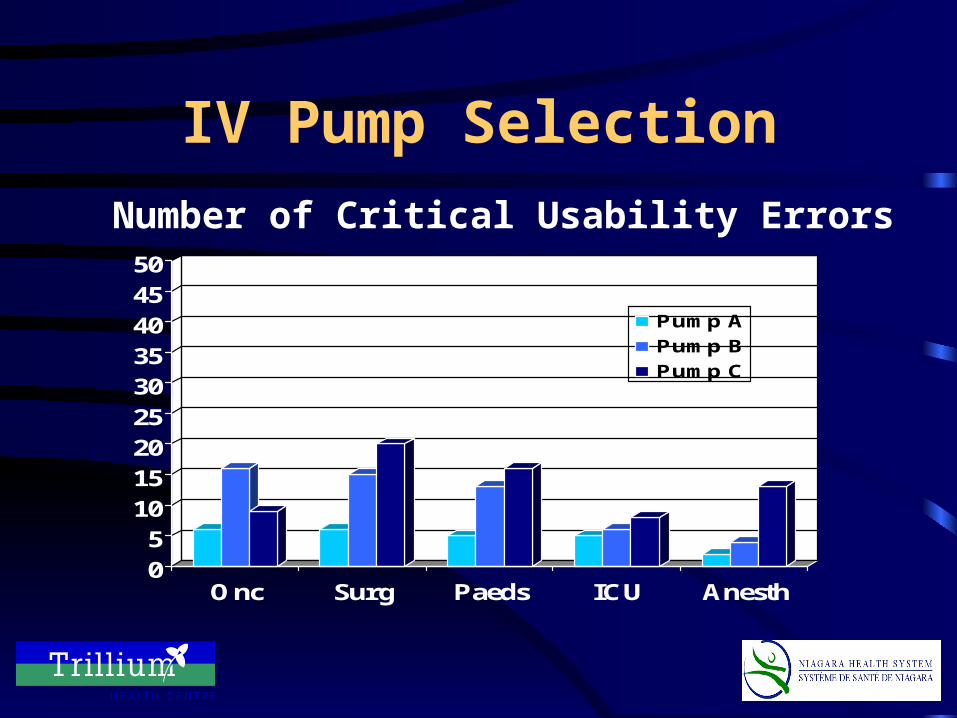
Number of Critical Usability Errors

IV Pump Selection
05
101520253035404550
Onc Surg Paeds ICU Anesth
Pump A
Pump B
Pump C
Number of Undetected Critical Usability Errors

IV Pump SelectionTotal # of Errors Across Clinical Areas

IV Pump Selection
Usability Characteristic# Participants who preferred…
Pump A Pump B Pump C
Easiest to program a basic infusion 4 5 12
Easiest to program from a drug library 8 3 5
Easiest to program from a drug calc 10 5 4
Easiest to loading a set 8 5 7
Easiest to transport 12 2 6
Most user-friendly prompts 6 5 5
Most user-friendly keypad 5 6 9
Most user-friendly display 6 6 9
Overall preference 6 5 8

IV Pump Selection
• Benefits of using HFE to evaluate usability:– Structured & objective approach– User involvement– Feedback to vendors– Customize user training– User familiarity & preference not always an
indicator of device usability

Thank you!
Gill Ginsburg
905-848-7580 x 3016
Erin Barkel
905-684-7271 x 4420
Questions?