patients at risk the art & science of patient positioning™ a patient positioning injury is any...
TRANSCRIPT
PATIENTS AT RISKPATIENTS AT RISK
THE ART & SCIENCE OF PATIENT POSITIONING™
A Patient Positioning injury is any dysfunction, discomfort, or injury not related to the surgical site, they are for the most part
PREVENTABLE
Presented by: Clare Tager, BSE, MFA, [email protected]
Designed by: Candi Forney, [email protected]
THE ART & SCIENCE OF PATIENT POSITIONING™
A Patient Positioning injury is any dysfunction, discomfort, or injury not related to the surgical site, they are for the most part
PREVENTABLE
Presented by: Clare Tager, BSE, MFA, [email protected]
Designed by: Candi Forney, [email protected]




O.R. Nurses frequently do not hear....O.R. Nurses frequently do not hear....
• “Peripheral nerve injuries are a significant source of anesthesia-related liability claims….The signs of denervation resulting from acute injury appear 18 to 21 days after the event and are limited to a specific nerve distribution. Recovery from peripheral nerve injury is often slow, taking 3 to 12 months and during this time the patient may experience pain and disability.” ~Basics of Anesthesia
• “Peripheral nerve injuries are a significant source of anesthesia-related liability claims….The signs of denervation resulting from acute injury appear 18 to 21 days after the event and are limited to a specific nerve distribution. Recovery from peripheral nerve injury is often slow, taking 3 to 12 months and during this time the patient may experience pain and disability.” ~Basics of Anesthesia
“Freedom from injury related to positioning is one of a number of expected outcomes of the surgical experience.” ~ AORN Standards and Practices
“Freedom from injury related to positioning is one of a number of expected outcomes of the surgical experience.” ~ AORN Standards and Practices
“The perioperative nurse should view positioning as a specialized piece of knowledge that when applied can make a distinct difference in patient outcomes. The practice of patient positioning is rational and logical. Positioning is grounded in basic knowledge of anatomy and physiology. The perioperative nurse approaches positioning with a sense of urgency and intense thought.” -~Alexander’s Care of the Patient in Surgery
“The perioperative nurse should view positioning as a specialized piece of knowledge that when applied can make a distinct difference in patient outcomes. The practice of patient positioning is rational and logical. Positioning is grounded in basic knowledge of anatomy and physiology. The perioperative nurse approaches positioning with a sense of urgency and intense thought.” -~Alexander’s Care of the Patient in Surgery

The sequelae of improper positioning may be temporarily discomforting, permanently disabling, or may terminate in the death of the patient.
Operative position has been the direct cause of injuries to delicate nerves, skeletal and supporting structures and other organs and tissues; the sporadic reporting of such accidents in the medical literature makes one suspect that many more accidents occur, but fail to be reported. There are no reliable statistical data to reveal the incidence of complications related to body position during surgery.
~Dr. John Lincoln, Director of Anesthesia, Maine Medical Center, Complications related to Body Positions During Surgery
The sequelae of improper positioning may be temporarily discomforting, permanently disabling, or may terminate in the death of the patient.
Operative position has been the direct cause of injuries to delicate nerves, skeletal and supporting structures and other organs and tissues; the sporadic reporting of such accidents in the medical literature makes one suspect that many more accidents occur, but fail to be reported. There are no reliable statistical data to reveal the incidence of complications related to body position during surgery.
~Dr. John Lincoln, Director of Anesthesia, Maine Medical Center, Complications related to Body Positions During Surgery
Factors Leading to Injury
•Faulty Positioning of the Patient
•Undue Haste
•Failure to insist on an adequate number of personnel before a position change
•Equal=potential for injury to patient (and staff!!)
•Post Op Backache one of the most common complications!
Back PainBack Pain
Nerves at RiskNerves at Risk

Brachial PlexusBrachial Plexus

Ulnar NerveUlnar Nerve

Femoral NerveFemoral Nerve
•Example: Hyper-flexion can damage this nerve, i.e. High lithotomy, when hips are flexed too far back or low lithotomy when leg is stretched lower than the plane the abdomen.
•Example: Hyper-flexion can damage this nerve, i.e. High lithotomy, when hips are flexed too far back or low lithotomy when leg is stretched lower than the plane the abdomen.
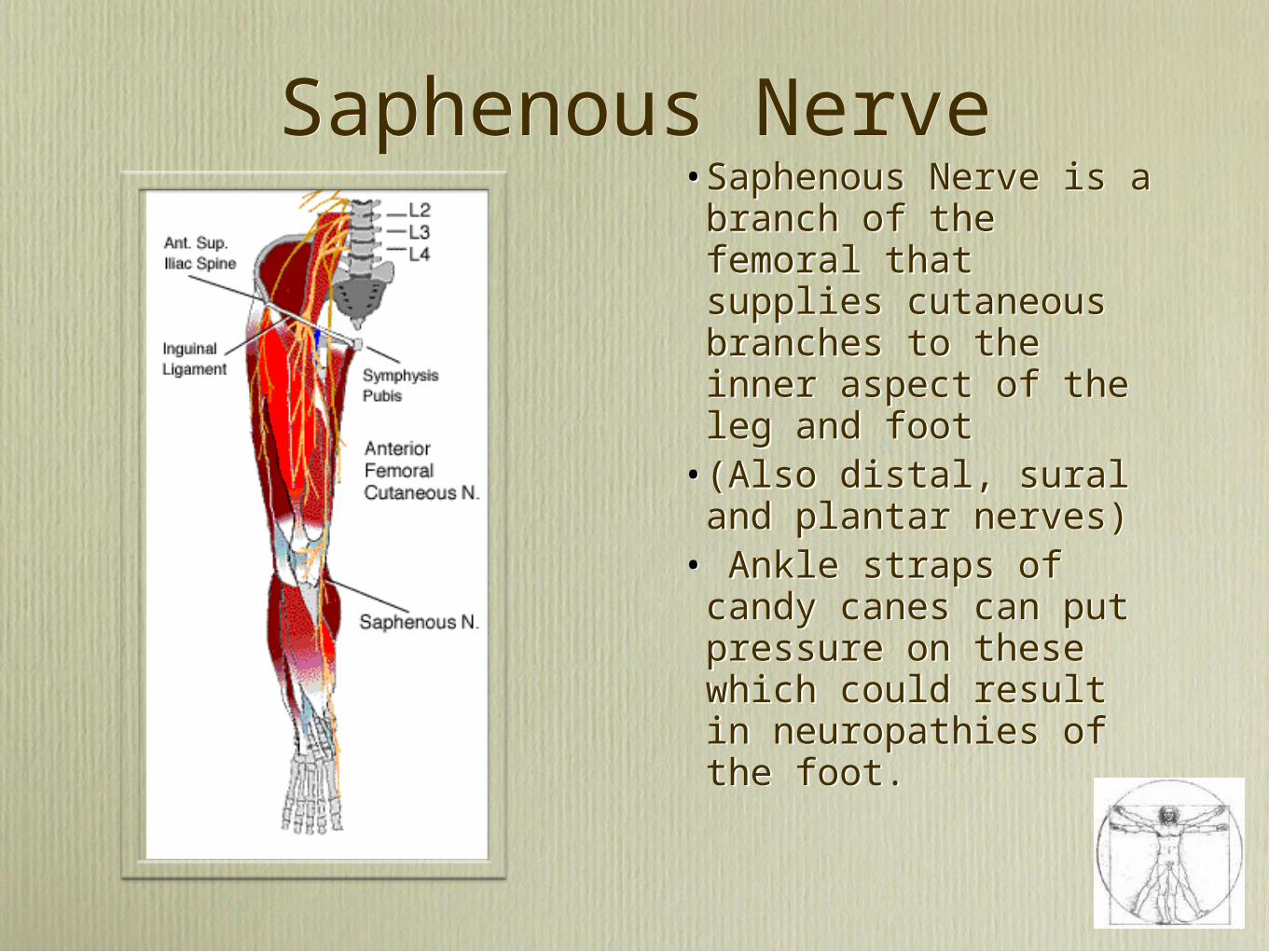
Saphenous NerveSaphenous Nerve•Saphenous Nerve is a branch of the femoral that supplies cutaneous branches to the inner aspect of the leg and foot
•(Also distal, sural and plantar nerves)
• Ankle straps of candy canes can put pressure on these which could result in neuropathies of the foot.
•Saphenous Nerve is a branch of the femoral that supplies cutaneous branches to the inner aspect of the leg and foot
•(Also distal, sural and plantar nerves)
• Ankle straps of candy canes can put pressure on these which could result in neuropathies of the foot.

Obturator NerveObturator Nerve
•Injury can occur as a result of over-abduction of legs in lithotomy.
•Patient loses sensation on inner aspect of thigh (can’t bring thighs together – gait and balance affected.
•Leg has to swing out before making contact with surface.
•Injury can occur as a result of over-abduction of legs in lithotomy.
•Patient loses sensation on inner aspect of thigh (can’t bring thighs together – gait and balance affected.
•Leg has to swing out before making contact with surface.
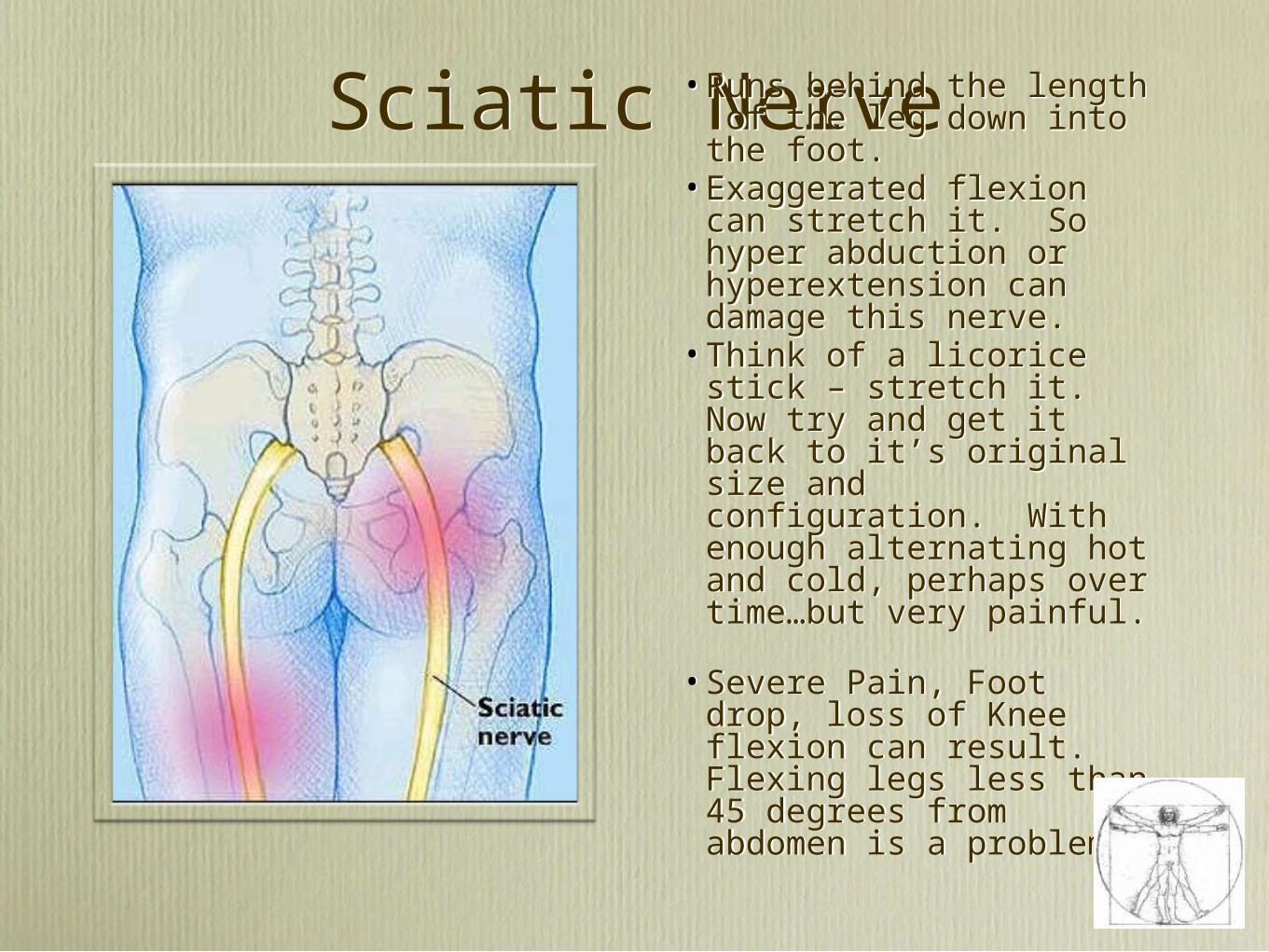
Sciatic NerveSciatic Nerve•Runs behind the length of the leg down into the foot.
•Exaggerated flexion can stretch it. So hyper abduction or hyperextension can damage this nerve.
•Think of a licorice stick – stretch it. Now try and get it back to it’s original size and configuration. With enough alternating hot and cold, perhaps over time…but very painful.
•Severe Pain, Foot drop, loss of Knee flexion can result. Flexing legs less than 45 degrees from abdomen is a problem
•Runs behind the length of the leg down into the foot.
•Exaggerated flexion can stretch it. So hyper abduction or hyperextension can damage this nerve.
•Think of a licorice stick – stretch it. Now try and get it back to it’s original size and configuration. With enough alternating hot and cold, perhaps over time…but very painful.
•Severe Pain, Foot drop, loss of Knee flexion can result. Flexing legs less than 45 degrees from abdomen is a problem
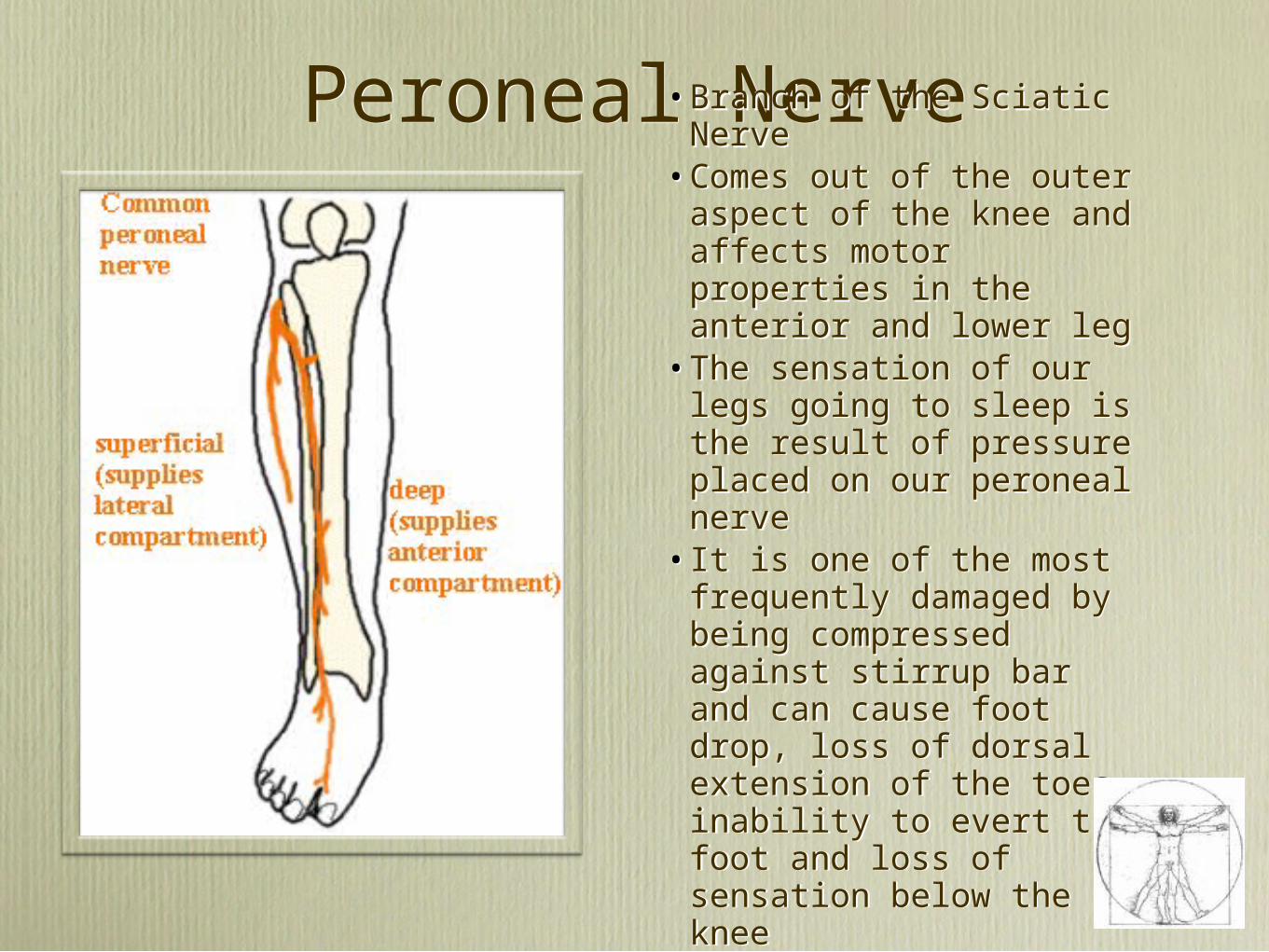
Peroneal NervePeroneal Nerve•Branch of the Sciatic
Nerve •Comes out of the outer
aspect of the knee and affects motor properties in the anterior and lower leg
•The sensation of our legs going to sleep is the result of pressure placed on our peroneal nerve
•It is one of the most frequently damaged by being compressed against stirrup bar and can cause foot drop, loss of dorsal extension of the toes, inability to evert the foot and loss of sensation below the knee
•Branch of the Sciatic Nerve
•Comes out of the outer aspect of the knee and affects motor properties in the anterior and lower leg
•The sensation of our legs going to sleep is the result of pressure placed on our peroneal nerve
•It is one of the most frequently damaged by being compressed against stirrup bar and can cause foot drop, loss of dorsal extension of the toes, inability to evert the foot and loss of sensation below the knee
PRESSURE/ ORAPU O.R. ACQUIRED PRESSURE ULCERS
PRESSURE/ ORAPU O.R. ACQUIRED PRESSURE ULCERS
• “Documented incidents for ORAPU - between 8.5% and 66%”
• “Surgical positioning affects the risk and location of skin breakdown... adding surface layers, i.e. cloth, warming blanket on top of a pressure reducing surface negates the the effect of the pressure reduction surface and produces a higher pressure reading than would be expected... Hence negativity.”
~Sharon Aronovitch, Phd., APRN,BC, CWOCN, Intraoperatively Acquired Pressure Ulcers, 1998
• “Documented incidents for ORAPU - between 8.5% and 66%”
• “Surgical positioning affects the risk and location of skin breakdown... adding surface layers, i.e. cloth, warming blanket on top of a pressure reducing surface negates the the effect of the pressure reduction surface and produces a higher pressure reading than would be expected... Hence negativity.”
~Sharon Aronovitch, Phd., APRN,BC, CWOCN, Intraoperatively Acquired Pressure Ulcers, 1998

AORN STANDARDS & PRACTICES 2008
AORN STANDARDS & PRACTICES 2008
• Capillary closure Point is 32mmhg, yet research studies found foam overlays or replacement pads ( most OR bed mattresses) do not have effective pressure reduction capabilities
• Standard OR Table pads (even new ones) may not reduce capillary interface pressure for all body types
• Pressure readings as high as 150mmhg noted during prolonged unrelieved pressure without position change
• Studies show viscoelastic overlays are effective for preventing skin changes and pressure sore formation, offering most benefit for older patient population, patients with chronic health problems, vascular disease or surgical procedures over 2 hours
• Capillary closure Point is 32mmhg, yet research studies found foam overlays or replacement pads ( most OR bed mattresses) do not have effective pressure reduction capabilities
• Standard OR Table pads (even new ones) may not reduce capillary interface pressure for all body types
• Pressure readings as high as 150mmhg noted during prolonged unrelieved pressure without position change
• Studies show viscoelastic overlays are effective for preventing skin changes and pressure sore formation, offering most benefit for older patient population, patients with chronic health problems, vascular disease or surgical procedures over 2 hours
“Pressure ulcers slow patients recovery and prolong their hospital stays, Worse, nearly 60,000 US hospital patients are estimated to die each year from complications due to hospital acquired pressure ulcers, The total annual cost for treating pressure ulcers in the US is estimated at $11 billion”
~IHI 5 Million Lives Campaign, How to Guide: Prevent Pressure Ulcers
“Pressure ulcers slow patients recovery and prolong their hospital stays, Worse, nearly 60,000 US hospital patients are estimated to die each year from complications due to hospital acquired pressure ulcers, The total annual cost for treating pressure ulcers in the US is estimated at $11 billion”
~IHI 5 Million Lives Campaign, How to Guide: Prevent Pressure Ulcers
Medicare RegulationsMedicare Regulations
•Effective October 2008, Medicare no longer reimburses for a number of hospital-acquired complications, including pressure sores.
•Aronovitch study: “Treatment of a single ulcer has been estimated to cost up to $40,000.”
•Effective October 2008, Medicare no longer reimburses for a number of hospital-acquired complications, including pressure sores.
•Aronovitch study: “Treatment of a single ulcer has been estimated to cost up to $40,000.”
RESOURCESRESOURCES
• SUZY SCOTT-WILLIAMS, RN, MSN, CWOCN
• (901) 523-8990 ext 7136, VA Medical Center Memphis, TN
• SUZY SCOTT-WILLIAMS, RN, MSN, CWOCN
• (901) 523-8990 ext 7136, VA Medical Center Memphis, TN

Anatomic Locations of Pressure UlcersAnatomic Locations of Pressure Ulcers
1.Sacrum 36.9%
2.Heel 30.3%
3. Ischium (sit bone) 8.0%
4.Elbow 6.9%
5.Malleolus (ankle bone) 6.1%
6.Trochanter (hip bone) 5.1%
7.Knee 3.0%
8.Scapula (shoulder blade) 2.4%
9.Occiput (back of head) 1.3%
Amlung SR, Miller WL, Bosley LM, Adv Skin Wound Care. 2001 Nov/Dec;14(6):297-301.
10. Amlung SR, Miller WL, Bosley LM, Adv Skin Wound Care. 2001 Nov/Dec;14(6):297-301.
1.Sacrum 36.9%
2.Heel 30.3%
3. Ischium (sit bone) 8.0%
4.Elbow 6.9%
5.Malleolus (ankle bone) 6.1%
6.Trochanter (hip bone) 5.1%
7.Knee 3.0%
8.Scapula (shoulder blade) 2.4%
9.Occiput (back of head) 1.3%
Amlung SR, Miller WL, Bosley LM, Adv Skin Wound Care. 2001 Nov/Dec;14(6):297-301.
10. Amlung SR, Miller WL, Bosley LM, Adv Skin Wound Care. 2001 Nov/Dec;14(6):297-301.
Occiput
Scapula
Elbow
Trochanter
Sacrum
Ischium
Knee
MalleolusHeel
30.3%Heels
Perioperative Pressure Ulcer (PPrU) Defined
Perioperative Pressure Ulcer (PPrU) Defined
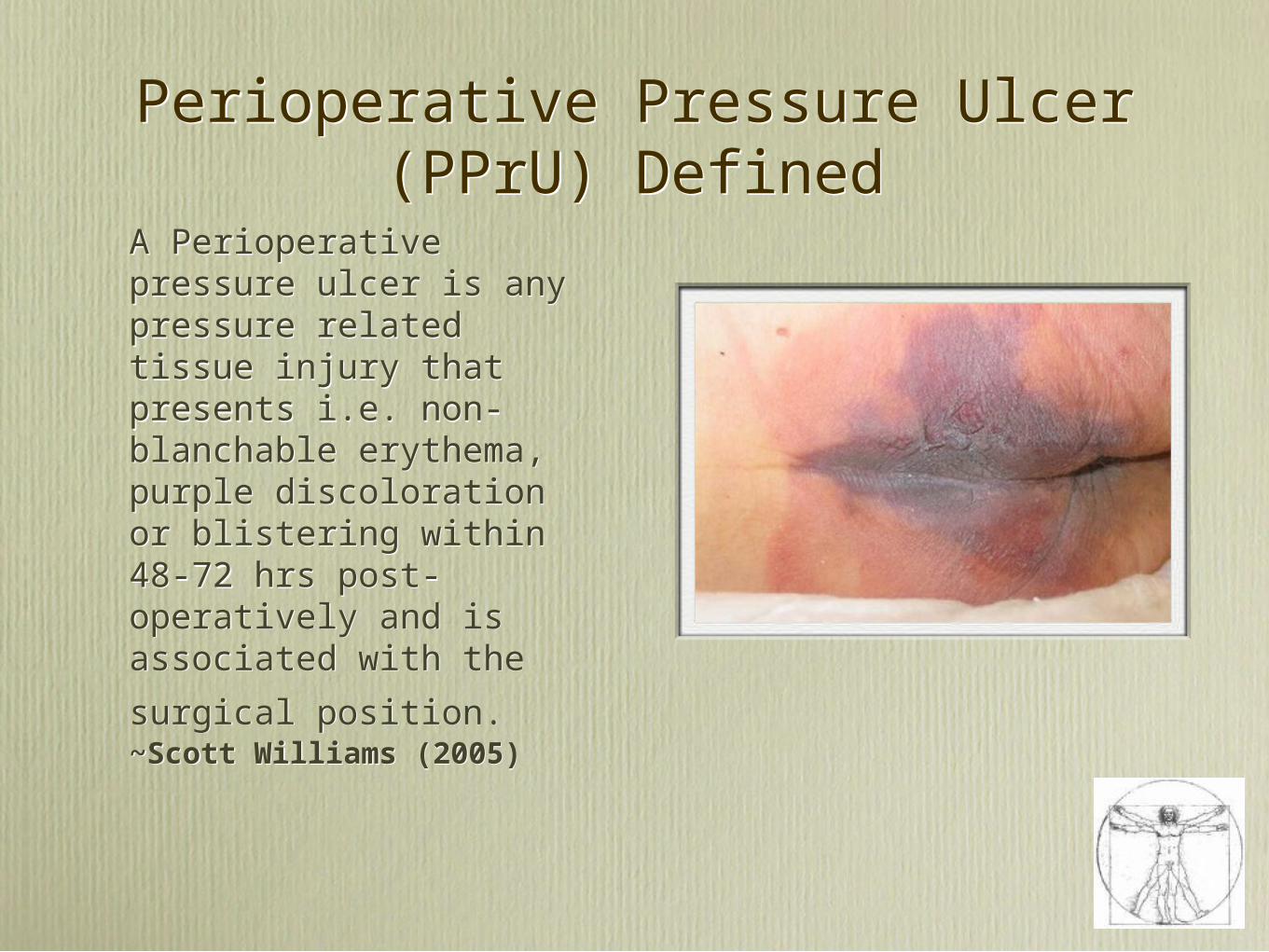
A Perioperative pressure ulcer is any pressure related tissue injury that presents i.e. non-blanchable erythema, purple discoloration or blistering within 48-72 hrs post-operatively and is associated with the
surgical position. ~Scott Williams (2005)
A Perioperative pressure ulcer is any pressure related tissue injury that presents i.e. non-blanchable erythema, purple discoloration or blistering within 48-72 hrs post-operatively and is associated with the
surgical position. ~Scott Williams (2005)

Perioperative Pressure Ulcer Prevention Program (PPUP)
Perioperative Pressure Ulcer Prevention Program (PPUP)• Assessment
• Perioperative Nursing Care Plan
• Universal Pressure Precautions
• Product Specification
• Staff Education & Awareness
• Evidence-based Best Practices
• Nursing Specialty Collaboration
• Quality Improvement
• Assessment
• Perioperative Nursing Care Plan
• Universal Pressure Precautions
• Product Specification
• Staff Education & Awareness
• Evidence-based Best Practices
• Nursing Specialty Collaboration
• Quality Improvement

Scott Triggers™Scott Triggers™• Assess pre-op for ALL
• Four Triggers
• Age over 62
• Albumin < 3.5
• ASA Score 3 or greater
• Surgery > 3 hours (time in/out of OR)
• Consider cardiac, vascular, trauma, transplants, and bariatric procedures
• 2 or more triggers=HIGH RISK SURGICAL PT
• Assess pre-op for ALL
• Four Triggers
• Age over 62
• Albumin < 3.5
• ASA Score 3 or greater
• Surgery > 3 hours (time in/out of OR)
• Consider cardiac, vascular, trauma, transplants, and bariatric procedures
• 2 or more triggers=HIGH RISK SURGICAL PT
ASA
& TIME
ALB
AGE
“Patients who are 100% over normal weight can have as much as a 40-50% increase in the mechanical work of breathing.” ~Alexander’s Care of the Patient in Surgery
“Patients who are 100% over normal weight can have as much as a 40-50% increase in the mechanical work of breathing.” ~Alexander’s Care of the Patient in Surgery
Risks Involving Morbidly Obese and Bariatric Patients

Morbidly Obese Patients Positioning Concerns
Morbidly Obese Patients Positioning Concerns
• AORN Standards and Practices• Bed must articulate and support 800 to 1000
pounds• Mattresses should not ' bottom out"• Width of legs determines whether lower legs
remain on bed or require stirrups. Check stirrup weight limit. Consider table width extenders
• Padded Sleds may be used to contain patients arms at side of body as long as no excessive pressure on arms
• Extra wide extra long safety straps ( Sheets not a good substitute) One safety strap across thighs, one over lower legs
• In Supine, a roll or wedge under right flank to relieve compression of vena cava
• AORN Standards and Practices• Bed must articulate and support 800 to 1000
pounds• Mattresses should not ' bottom out"• Width of legs determines whether lower legs
remain on bed or require stirrups. Check stirrup weight limit. Consider table width extenders
• Padded Sleds may be used to contain patients arms at side of body as long as no excessive pressure on arms
• Extra wide extra long safety straps ( Sheets not a good substitute) One safety strap across thighs, one over lower legs
• In Supine, a roll or wedge under right flank to relieve compression of vena cava

Morbidly Obese Patients Positioning Concerns
Morbidly Obese Patients Positioning Concerns
• AORN Standards and Practices• In Prone, support for the upper chest and pelvis
reduces pressure on diaphragm and inferior vena cava
• Trendelenburg should be avoided, as added weight of abdominal contents press against diaphragm, respiratory compromise, increased blood flow from lower extremities causes vascular congestion
• Lithotomy should be avoided if possible due to weight of patients thighs pressing on abdomen and raising intra-abdominal pressure, risk of circulatory complications
• Lateral position may be preferred instead of prone but nursing awareness that shifts in weight can in itself increase risk of falling
• AORN Standards and Practices• In Prone, support for the upper chest and pelvis
reduces pressure on diaphragm and inferior vena cava
• Trendelenburg should be avoided, as added weight of abdominal contents press against diaphragm, respiratory compromise, increased blood flow from lower extremities causes vascular congestion
• Lithotomy should be avoided if possible due to weight of patients thighs pressing on abdomen and raising intra-abdominal pressure, risk of circulatory complications
• Lateral position may be preferred instead of prone but nursing awareness that shifts in weight can in itself increase risk of falling

LithotomyLithotomy
The Time FactorThe Time Factor
“A recent study showed that patients in the lithotomy position sustained few injuries during the first hour of surgery, but each additional hour posed a 100-fold increase in the risk for neuropathy.” ~Dr. Mark Warner, Mayo Clinic, Department Anesthesia
“A recent study showed that patients in the lithotomy position sustained few injuries during the first hour of surgery, but each additional hour posed a 100-fold increase in the risk for neuropathy.” ~Dr. Mark Warner, Mayo Clinic, Department Anesthesia
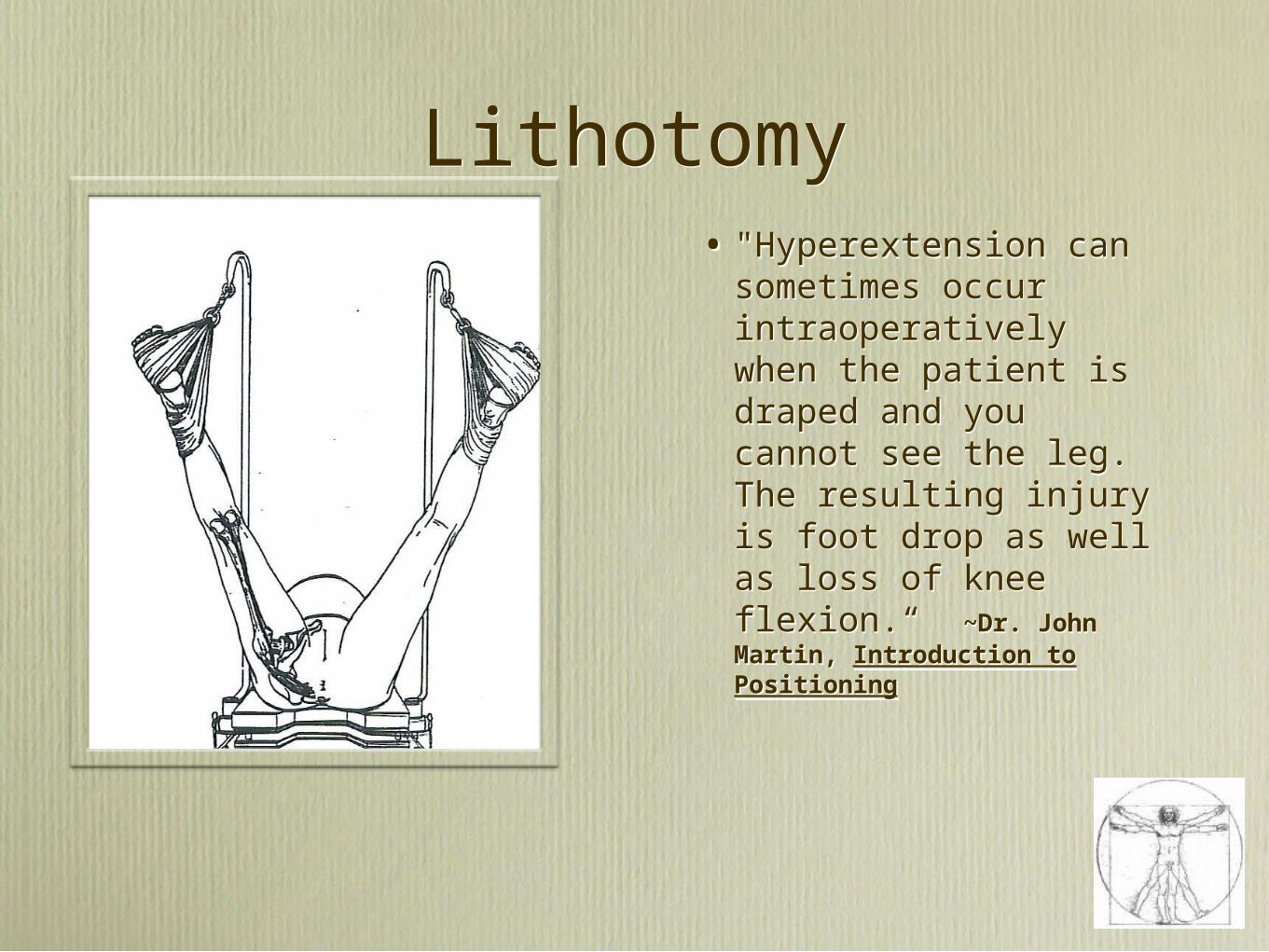
• "Hyperextension can sometimes occur intraoperatively when the patient is draped and you cannot see the leg. The resulting injury is foot drop as well as loss of knee flexion.“ ~Dr. John Martin, Introduction to Positioning
• "Hyperextension can sometimes occur intraoperatively when the patient is draped and you cannot see the leg. The resulting injury is foot drop as well as loss of knee flexion.“ ~Dr. John Martin, Introduction to Positioning
LithotomyLithotomy

• Hyperflexion = < 45 degrees from the abdomen
•Hyperextension = No flexion in knee or leg lower than the plane of the abdomen in low lithotomy
• Hyperflexion = < 45 degrees from the abdomen
•Hyperextension = No flexion in knee or leg lower than the plane of the abdomen in low lithotomy
Lithotomy Risks
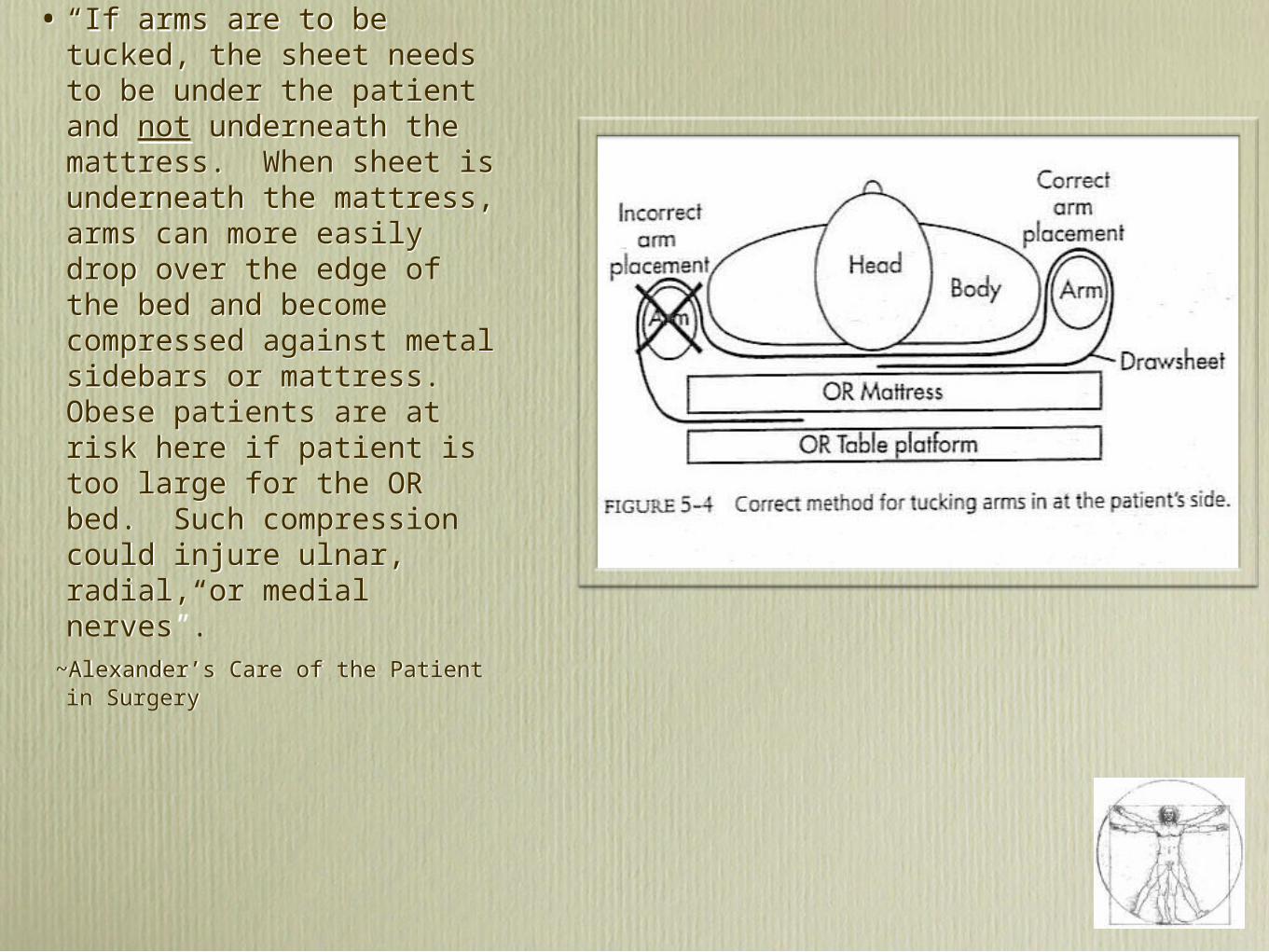
• “If arms are to be tucked, the sheet needs to be under the patient and not underneath the mattress. When sheet is underneath the mattress, arms can more easily drop over the edge of the bed and become compressed against metal sidebars or mattress. Obese patients are at risk here if patient is too large for the OR bed. Such compression could injure ulnar, radial, or medial nerves”.
~Alexander’s Care of the Patient in Surgery
• “If arms are to be tucked, the sheet needs to be under the patient and not underneath the mattress. When sheet is underneath the mattress, arms can more easily drop over the edge of the bed and become compressed against metal sidebars or mattress. Obese patients are at risk here if patient is too large for the OR bed. Such compression could injure ulnar, radial, or medial nerves”.
~Alexander’s Care of the Patient in Surgery

Stirrups
The first consideration in patient positioning is to...
FIT THE EQUIPMENT TO THE PATIENT, NOT THE PATIENT TO THE EQUIPMENT
~Dr. John Martin, Positioning in Anesthesia and Surgery
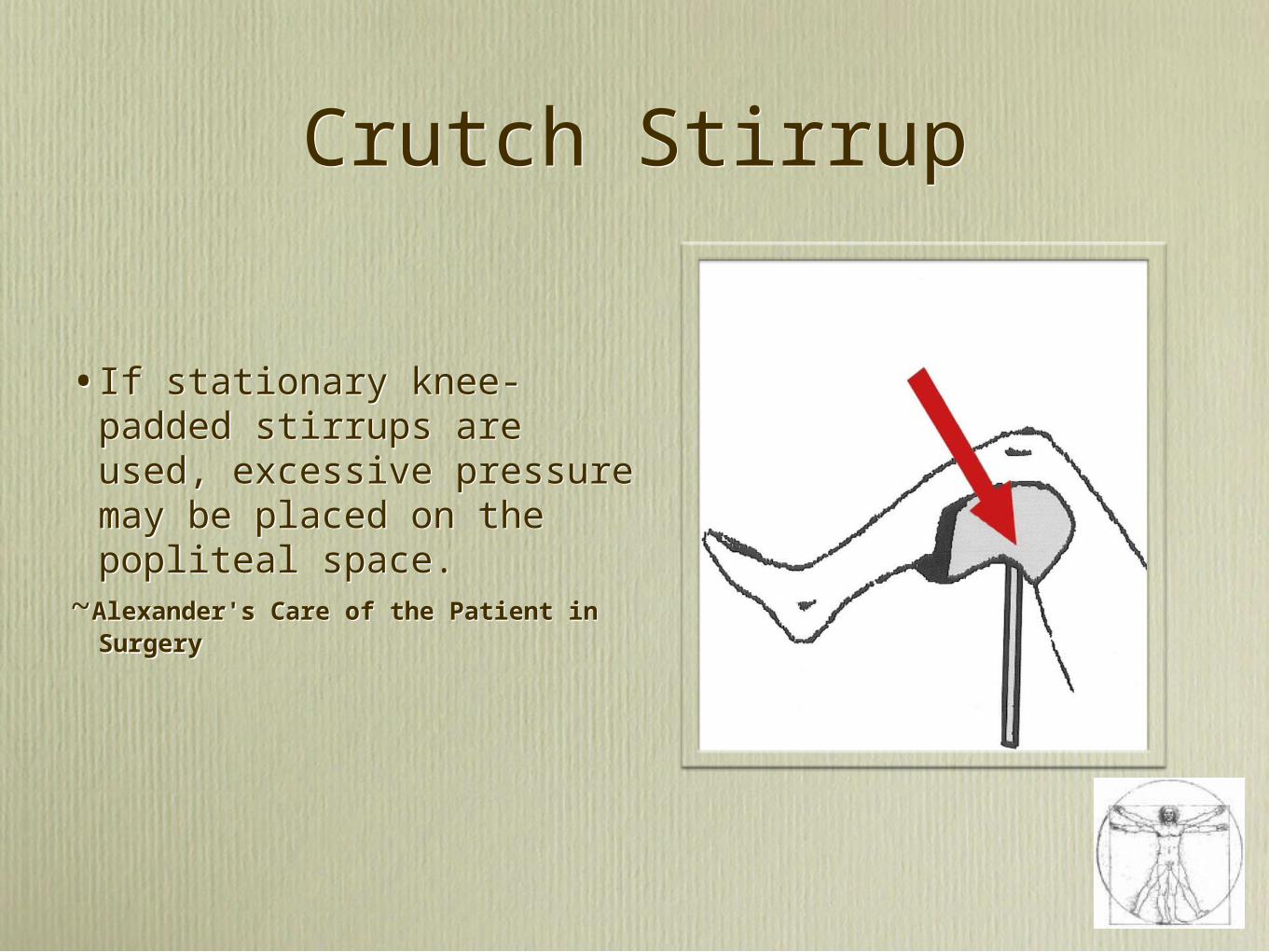
Crutch StirrupCrutch Stirrup
•If stationary knee-padded stirrups are used, excessive pressure may be placed on the popliteal space.
~Alexander's Care of the Patient in Surgery
•If stationary knee-padded stirrups are used, excessive pressure may be placed on the popliteal space.
~Alexander's Care of the Patient in Surgery

Boot StirrupBoot Stirrup
1.Place sockets at hips
2.Extend the legs if going into high lithotomy
3.Avoid over-flexion less than 45 degrees from the abdomen
4.Avoid frog-legging
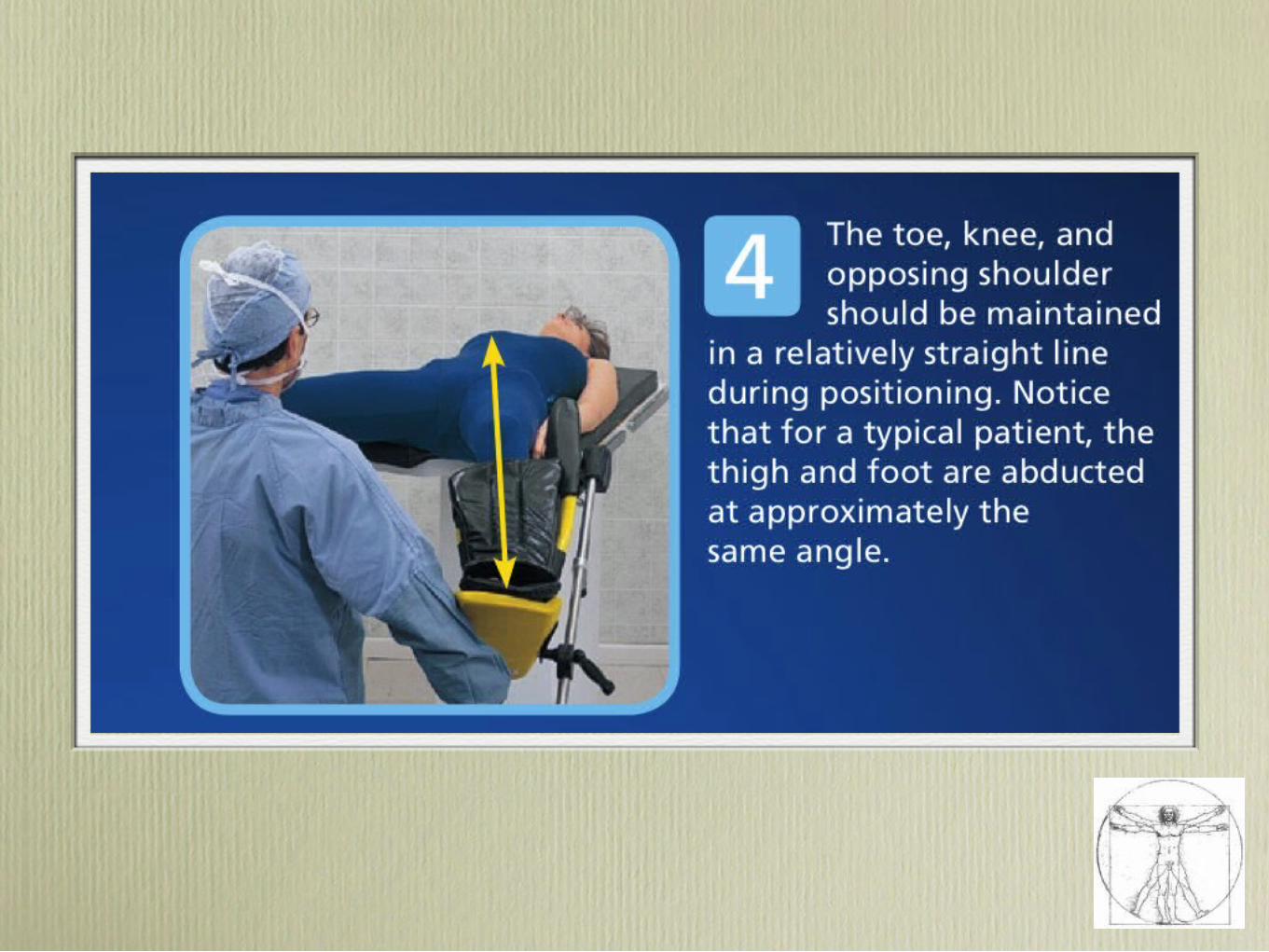
5. Line up toe, knee, opposite shoulder
1.Place sockets at hips
2.Extend the legs if going into high lithotomy
3.Avoid over-flexion less than 45 degrees from the abdomen
4.Avoid frog-legging
5. Line up toe, knee, opposite shoulder
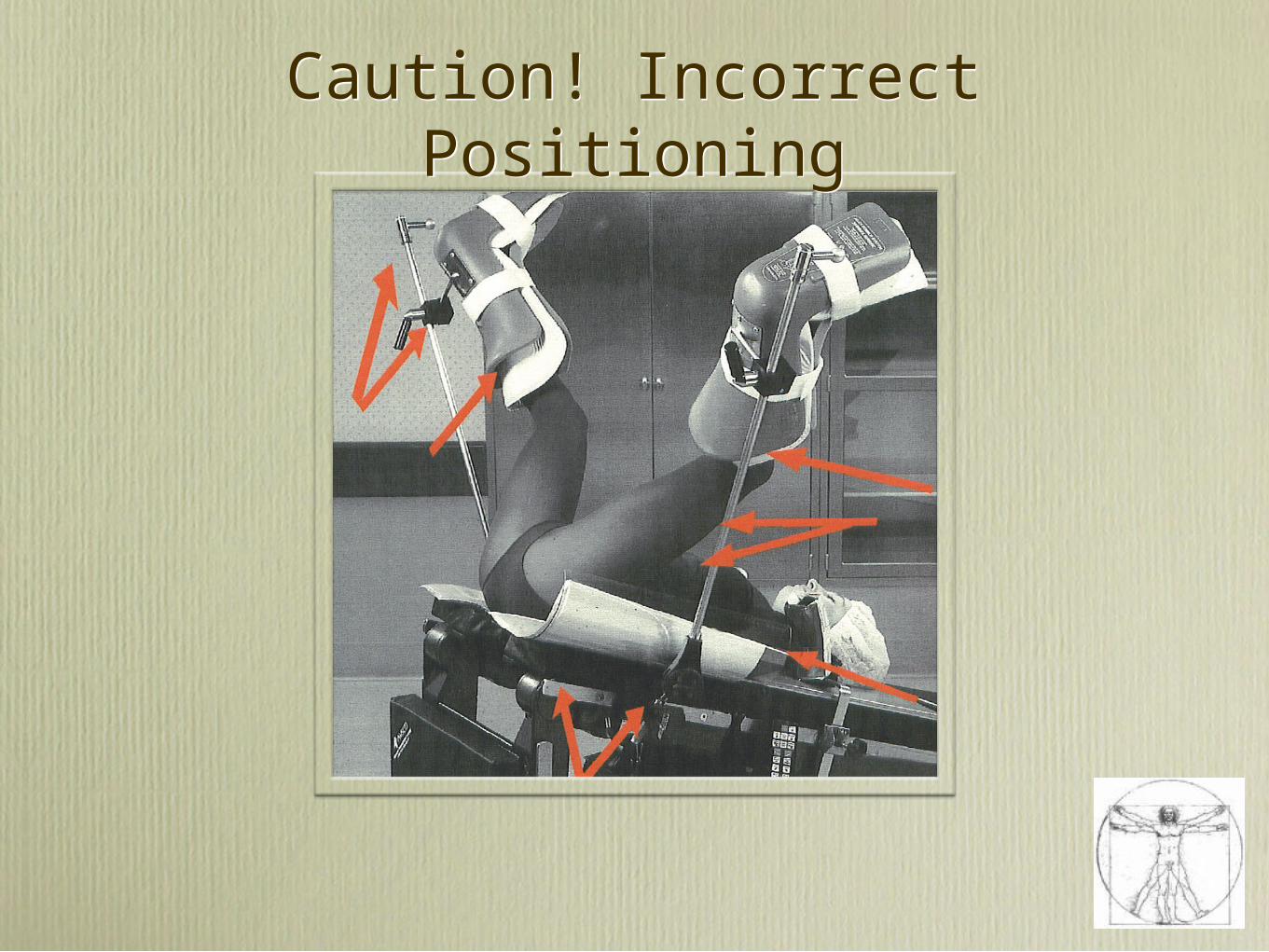
Caution! Incorrect PositioningCaution! Incorrect Positioning

Candy CanesCandy Canes
“What you do in the few minutes you have to position a patient for surgery can have lasting consequences. Candy Cane leg holders that wrap around the head of the fibula can compress the leg’s peroneal nerve. Excessively abducted hips increase the strain on the obturator nerve and can cause pain and adductor muscle dysfunction. Hip flexion increases pressure on the femoral and lateral femoral cutaneous nerves and can cause painful paresthesias.” ~Outpatient Surgery, 6 Patient Positioning Pointers, Nathan Hall, Editor, April 2008

Placement of Patients Buttocks on Edge of OR Table
Placement of Patients Buttocks on Edge of OR Table
•“The Patients Buttocks should not extend over the break of the bed to prevent pressure areas and to decrease lower back strain” ~AORN Positioning Module
•Note also, Peroneal Nerve area being compressed against the post. ~Dr. John Martin
•“The Patients Buttocks should not extend over the break of the bed to prevent pressure areas and to decrease lower back strain” ~AORN Positioning Module
•Note also, Peroneal Nerve area being compressed against the post. ~Dr. John Martin

Uncontrolled AbductionUncontrolled Abduction
• “Uncontrolled abduction of the thigh can manifest in post-operative back-ache and stretching in the groin area can manifest as an Obturator nerve injury.”
~AORN Positioning Module
• “Uncontrolled abduction of the thigh can manifest in post-operative back-ache and stretching in the groin area can manifest as an Obturator nerve injury.”
~AORN Positioning Module

Address at ACOG 2003Address at ACOG 2003
• “Avoid candy cane stirrups! I know plenty of people still use these things, but many of us are getting away from this practice. They basically just hang your leg dangling there which is not ideal for making sure the patient’s leg is safe.” He encouraged his audience of fellow Gynecologists to use boot stirrups and to do the positioning themselves adding, “make sure you feel comfortable with the positioning because you’re the one who’s going to be in court if there is a problem.” ~Dr. William Hurd, Professor of Gynecology, Wright State University, Dayton, Ohio, ACOG
• “Avoid candy cane stirrups! I know plenty of people still use these things, but many of us are getting away from this practice. They basically just hang your leg dangling there which is not ideal for making sure the patient’s leg is safe.” He encouraged his audience of fellow Gynecologists to use boot stirrups and to do the positioning themselves adding, “make sure you feel comfortable with the positioning because you’re the one who’s going to be in court if there is a problem.” ~Dr. William Hurd, Professor of Gynecology, Wright State University, Dayton, Ohio, ACOG

AORN Standards 2009 LithotomyAORN Standards 2009 Lithotomy
• Stirrups placed at even height
• Patients buttocks should be even with the lower break of the procedure bed and positioned in a manner that securely supports the sacrum on the bed surface
• Legs moved slowly and simultaneously into holders to prevent lumbosacral strain
• To maintain hemodynamic status, legs slowly returned to bed
• Arms extended less than 90 degree
• Stirrups placed at even height
• Patients buttocks should be even with the lower break of the procedure bed and positioned in a manner that securely supports the sacrum on the bed surface
• Legs moved slowly and simultaneously into holders to prevent lumbosacral strain
• To maintain hemodynamic status, legs slowly returned to bed
• Arms extended less than 90 degree

AORN Standards 2009 LithotomyAORN Standards 2009 Lithotomy
• Arms tucked only if surgically necessary with elbows padded and palms facing in toward body
• Support should be provided over the largest surface area of the leg positioner
• Legs should not rest against stirrup posts
• Scrubbed personnel should not lean against patients thighs
• Patient should be in the lithotomy position for the shortest time possible
• Arms tucked only if surgically necessary with elbows padded and palms facing in toward body
• Support should be provided over the largest surface area of the leg positioner
• Legs should not rest against stirrup posts
• Scrubbed personnel should not lean against patients thighs
• Patient should be in the lithotomy position for the shortest time possible

1885 TRENDELENBURG1885 TRENDELENBURG

Staff Seeking Solutions
" It is definitely an uncomfortable position as the blood pools in your head. Even the surgeon commented ‘We do this to our patients?’ If you have never been positioned Trendelenburg, I suggest you try it. In our peri-op classes we included many positions for our new staff members to practice and to experience but not Trendelenburg; now it will be on the list."
~Claudia Campese RN CNOR Nurse Educator, New Hanover Regional Medical Center, Wilmington NC

•“Any variation of Trendelenburg’s position should be maintained only as long as necessary” - Alexander’s Care of the Patient in Surgery
•“Any variation of Trendelenburg’s position should be maintained only as long as necessary” - Alexander’s Care of the Patient in Surgery
Trendelenburg RisksTrendelenburg Risks• Excessive pressure on clavicle =
compression on B-Plexus
• Morrell Closed Claims: B-Plexus injury results from shoulder braces and Trendelenburg
• Patients with history of heart failure especially at risk
• Gravitational blood flow away from surgical field masks blood loss.
• Cerebral blood flow may fall as pressure rises
• Trendelenburg can equal visual loss related to decrease venous return from head
~ AORN Standards & Practices 2009
• Excessive pressure on clavicle = compression on B-Plexus
• Morrell Closed Claims: B-Plexus injury results from shoulder braces and Trendelenburg
• Patients with history of heart failure especially at risk
• Gravitational blood flow away from surgical field masks blood loss.
• Cerebral blood flow may fall as pressure rises
• Trendelenburg can equal visual loss related to decrease venous return from head
~ AORN Standards & Practices 2009

Alexander’s TrendelenburgAlexander’s Trendelenburg
• CONSIDERATIONS
• Sliding in Trendelenburg: Issues
• Steeper degrees of Trendelenburg with new OR tables
• Robotics
• CONSIDERATIONS
• Sliding in Trendelenburg: Issues
• Steeper degrees of Trendelenburg with new OR tables
• Robotics
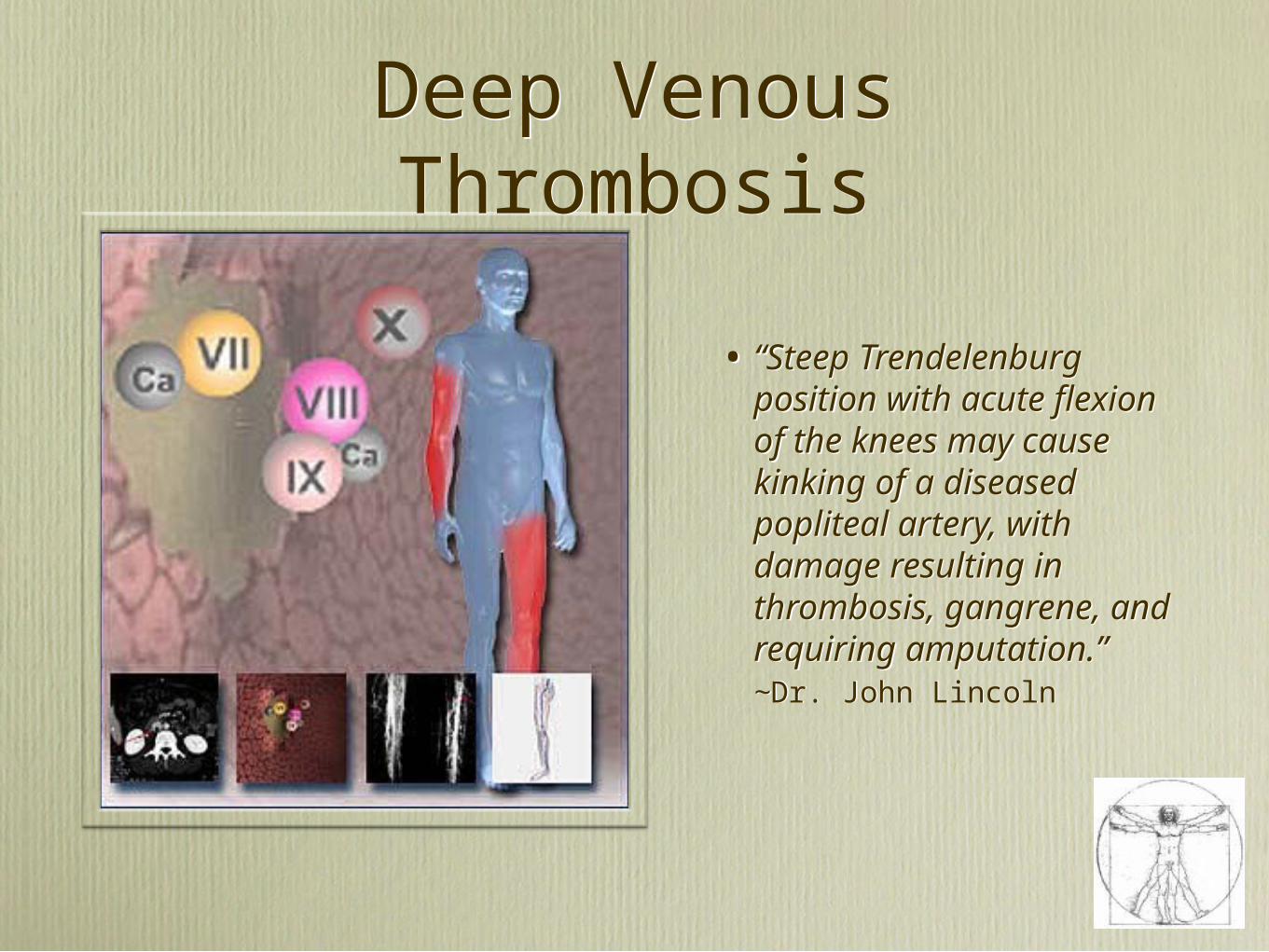
• “Steep Trendelenburg position with acute flexion of the knees may cause kinking of a diseased popliteal artery, with damage resulting in thrombosis, gangrene, and requiring amputation.” ~Dr. John Lincoln
• “Steep Trendelenburg position with acute flexion of the knees may cause kinking of a diseased popliteal artery, with damage resulting in thrombosis, gangrene, and requiring amputation.” ~Dr. John Lincoln
Deep Venous ThrombosisDeep Venous Thrombosis

Alexander’s ProneAlexander’s Prone

Spinal FrameSpinal Frame
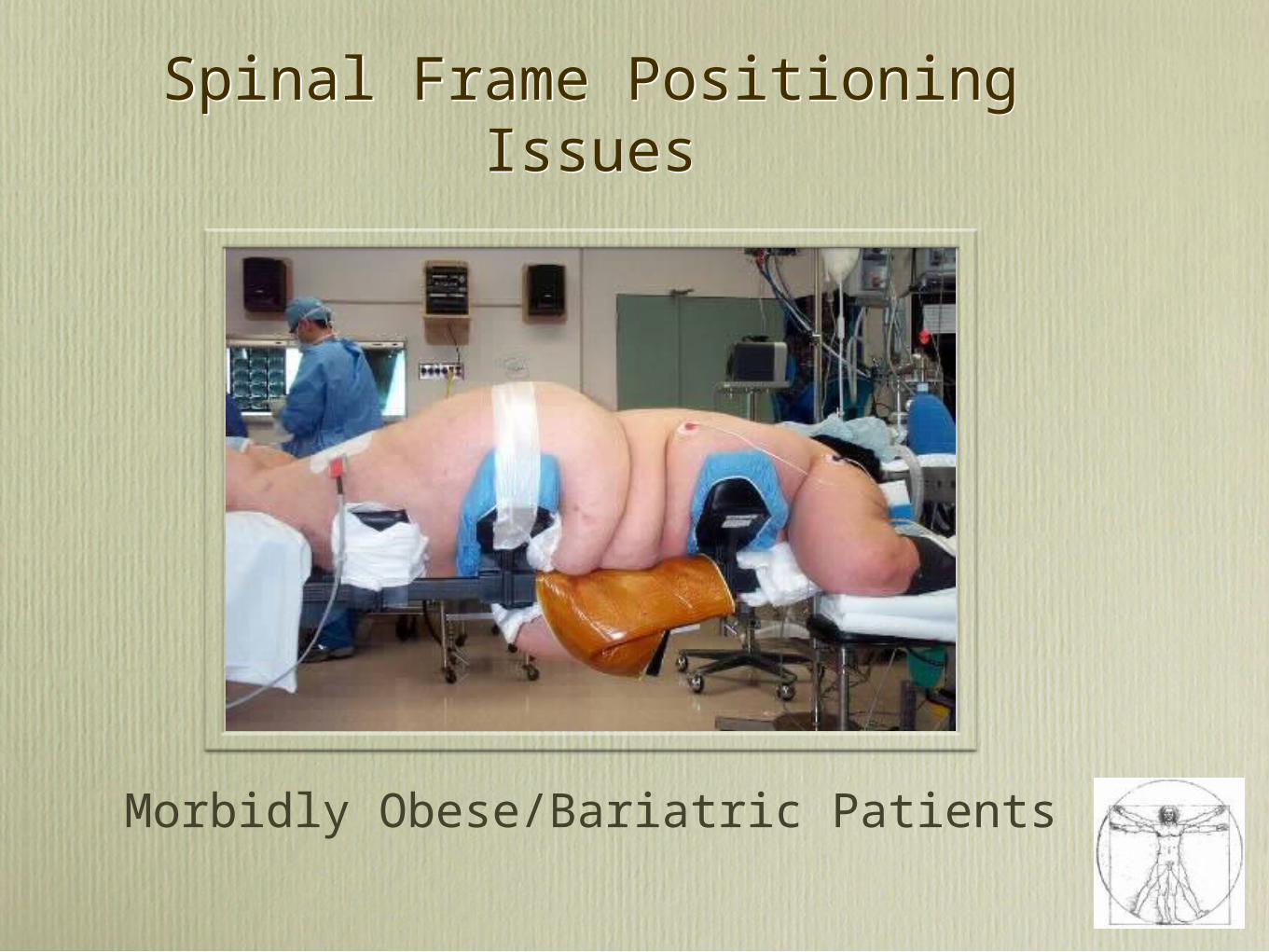
Spinal Frame Positioning IssuesSpinal Frame Positioning Issues
Morbidly Obese/Bariatric Patients

Spine Frame Positioning Issues
Spine Frame Positioning Issues
• Imaging
• Visual Access
• Decompressed Abdomen
• Pressure Management
• Skin Sheer & Maceration
• Face
• Large Patients
• Pediatrics
• Brachial Plexus
• Breasts
• Imaging
• Visual Access
• Decompressed Abdomen
• Pressure Management
• Skin Sheer & Maceration
• Face
• Large Patients
• Pediatrics
• Brachial Plexus
• Breasts
The Prone Positioning of Patients on Operating Room Equipment: Intraoperative Complications
~Helen Manson, Professor of Anesthesia, UK
The Prone Positioning of Patients on Operating Room Equipment: Intraoperative Complications
~Helen Manson, Professor of Anesthesia, UK
• Cardiopulmonary: Pressure on abdomen compresses inferior vena cava and femoral veins,…. Support surfaces that minimize intraabdominal pressure are essential
• Respiratory: High airway pressures and large tidal volumes need to ventilate a patient improperly positioned can have severe side effects. The patient who is supported with the abdomen FREE FROM PRESSURE will have improved ventilation and oxygenation
• Neurological: Careful positioning of the neck and head support in a neutral postion are ESSENTIAL to prevent neurological injury while prone. Use of Chest Rolls led to increased venous pressure which .. decreased the perfusion pressure in the spinal cord, causing Ischemia. CASE: Pt had fatal ischemic stroke after being positioned prone with head rotated during spine surgery
• Case: Postoperative Paraplegia due to cervical spine injury attributed to neck positioning during prone spine surgery
• Cardiopulmonary: Pressure on abdomen compresses inferior vena cava and femoral veins,…. Support surfaces that minimize intraabdominal pressure are essential
• Respiratory: High airway pressures and large tidal volumes need to ventilate a patient improperly positioned can have severe side effects. The patient who is supported with the abdomen FREE FROM PRESSURE will have improved ventilation and oxygenation
• Neurological: Careful positioning of the neck and head support in a neutral postion are ESSENTIAL to prevent neurological injury while prone. Use of Chest Rolls led to increased venous pressure which .. decreased the perfusion pressure in the spinal cord, causing Ischemia. CASE: Pt had fatal ischemic stroke after being positioned prone with head rotated during spine surgery
• Case: Postoperative Paraplegia due to cervical spine injury attributed to neck positioning during prone spine surgery

The Prone Positioning of Patients on Operating Room Equipment: Intraoperative Complications
~Helen Manson, Professor of Anesthesia, UK
The Prone Positioning of Patients on Operating Room Equipment: Intraoperative Complications
~Helen Manson, Professor of Anesthesia, UK• Patient support devices that minimize abdominal compression and maintain neck and body in NEUTRAL position can help prevent these neurological complications
• Nerve: Peripheral nerve injury one of the most frequent causes of morbidity Compression of lateral femoral cutaneous nerve a common complication. Support devices that minimize pressure are key
• Skin: Prone patients at high risk for pressure ulcer development Iliac bony prominences common area for pressure ulcers . The prolonged nature of these spinal procedures increase likelihood of shearing and pressure injury
• Pressure: Prone positioning may inadvertently damage breast tissue, resulting in chest wall pain, breast tenderness or bleeding of nipples Longitudinal positioning frames or rolls can damage breast tissue by direct compression, Rupturing of implants also noted
• Ocular: Compared with Supine and lateral positioning, there is a ten fold increase in eye injury associated with surgery while prone. In addition to Corneal abrasions, POVL Postoperative visual loss is associated with spinal surgery. 67% of all cases of POVL registered on ASA Registry occurred after spine surgery. ASA has a task force set up on post operative blindness due to prone positioining
• Patient support devices that minimize abdominal compression and maintain neck and body in NEUTRAL position can help prevent these neurological complications
• Nerve: Peripheral nerve injury one of the most frequent causes of morbidity Compression of lateral femoral cutaneous nerve a common complication. Support devices that minimize pressure are key
• Skin: Prone patients at high risk for pressure ulcer development Iliac bony prominences common area for pressure ulcers . The prolonged nature of these spinal procedures increase likelihood of shearing and pressure injury
• Pressure: Prone positioning may inadvertently damage breast tissue, resulting in chest wall pain, breast tenderness or bleeding of nipples Longitudinal positioning frames or rolls can damage breast tissue by direct compression, Rupturing of implants also noted
• Ocular: Compared with Supine and lateral positioning, there is a ten fold increase in eye injury associated with surgery while prone. In addition to Corneal abrasions, POVL Postoperative visual loss is associated with spinal surgery. 67% of all cases of POVL registered on ASA Registry occurred after spine surgery. ASA has a task force set up on post operative blindness due to prone positioining
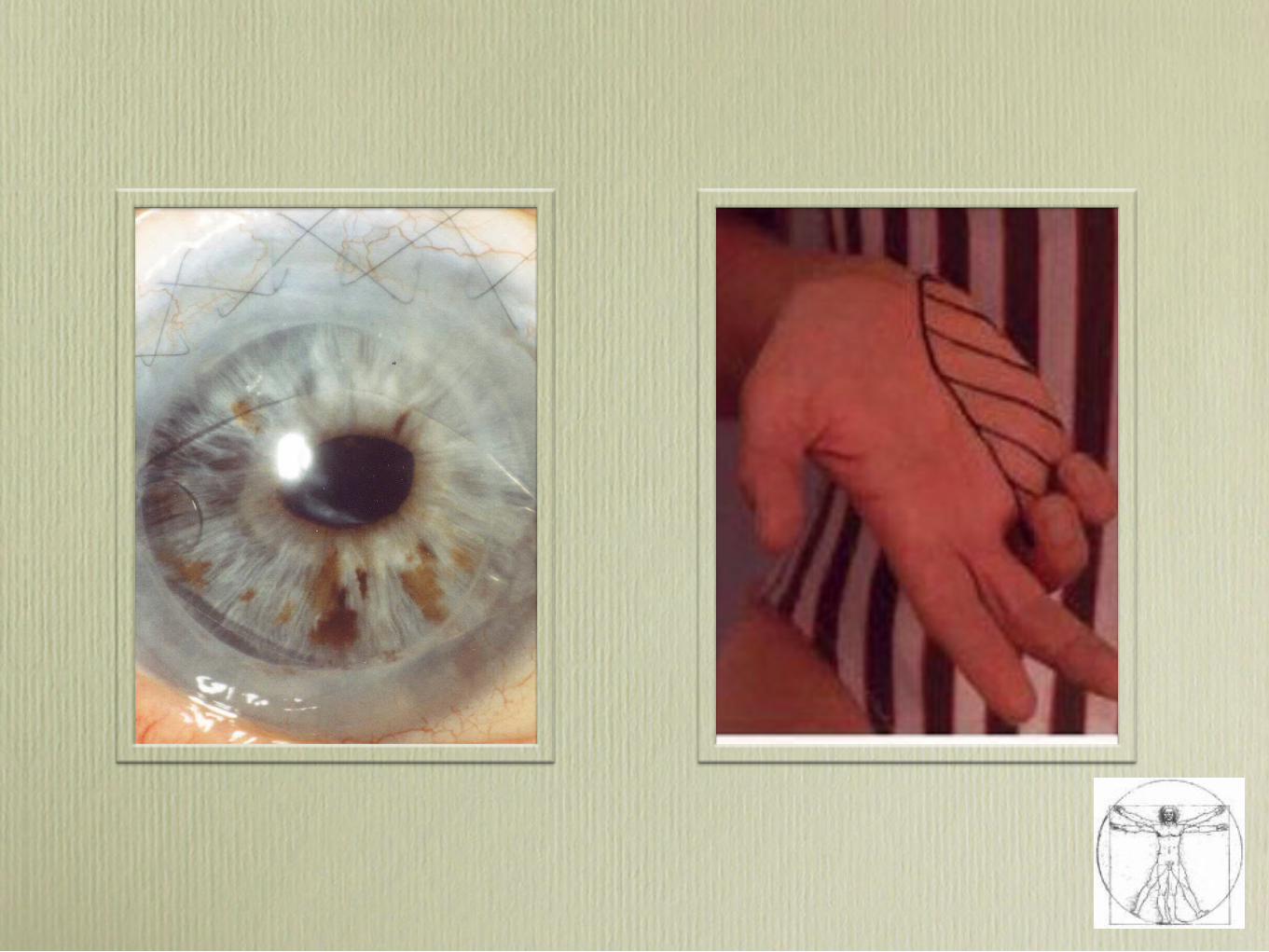
Nerve damage from Coronary Artery Bypass Surgery can Affect Arm Functioning
~Dr. Joseph Episcopio, Senior Attending Physician in Internal Medicine, Lehigh Valley, PA
Nerve damage from Coronary Artery Bypass Surgery can Affect Arm Functioning
~Dr. Joseph Episcopio, Senior Attending Physician in Internal Medicine, Lehigh Valley, PA
One seldom discussed complication is injury to the brachial plexus nerve which should be considered when the patient complains of acute onset of shoulder pain, weakness and/or paralysis following the surgical procedure.
•Brachial plexus injury • Patient experience intense pain and discomfort • Delay in return to employment(uncompensated)• Possible permanent disability.
•Emergence of Emotional involvement • Depression• Anxiety
One seldom discussed complication is injury to the brachial plexus nerve which should be considered when the patient complains of acute onset of shoulder pain, weakness and/or paralysis following the surgical procedure.
•Brachial plexus injury • Patient experience intense pain and discomfort • Delay in return to employment(uncompensated)• Possible permanent disability.
•Emergence of Emotional involvement • Depression• Anxiety
Mr. Thompson, 62 year retired pharmacist was admitted to Methodist Medical in
Memphis, Tennessee in 1982 for a coronary bypass.....
Mr. Thompson, 62 year retired pharmacist was admitted to Methodist Medical in
Memphis, Tennessee in 1982 for a coronary bypass.....
•Pain
•Discomfort
•Emotional Involvment
•Depression
•Anxiety
•This gentleman was my Dad...
•Pain
•Discomfort
•Emotional Involvment
•Depression
•Anxiety
•This gentleman was my Dad...
Patient Advocacy…You are the voice for
the voiceless
Patient Advocacy…You are the voice for
the voiceless