payments for rural health care providers 2010 today, 68% of medically underserved communities across...
TRANSCRIPT
Payments for Rural Health Care Providers
2010
Today, 68% of medically underserved communities across the nation are in rural areas, and these communities often have trouble attracting and retaining medical professionals.
PPACA provides increased payment to rural health care providers to help
them continue to serve their communities.

Prescription Drug DiscountsEffective January 1, 2011
2010 2011
Seniors who reach the coverage gap will receive a 50% discount when buying Medicare Part D covered brand-name prescription drugs. Over the next ten
years, seniors will receive additional savings on brand-name and generic drugs until
the coverage gap is closed completely in 2020.

2010 2011
Free Preventive Care for Seniors
Effective January 1, 2011
PPACA expands Medicare provides
certain free preventive services, such as
annual wellness visits and personalized prevention plans.

2010 2011
To ensure premium dollars are spent primarily on health care, the new law generally requires that at least 85% of all premium dollars collected by insurance companies for large employer plans are spent on health care services & health care quality improvement.
Bringing Down Health Care PremiumsRebate Program Began January 1, 2011
For plans sold to individuals and small employers, at least 80% of the premium must be spent on benefits and quality improvement. If insurance companies do not meet these goals because their administrative costs or profits are too high, they must provide rebates to consumers.
2010 2011
Today, Medicare pays Medicare Advantage insurance companies over $1,000 more per person on average
than is spent per person in traditional Medicare. This results in increased
premiums for all Medicare beneficiaries, including the 77% of beneficiaries who are not currently enrolled in a Medicare Advantage
plan.
Addressing Overpayments to Insurance Companies and Strengthening Medicare Advantage
Effective January 1, 2011
The new law levels the playing field by gradually eliminating this discrepancy. People enrolled in a
Medicare Advantage plan will still receive all guaranteed Medicare benefits, and the law provides bonus payments
to Medicare Advantage plans that provide high quality care.

2010 2011
The law establishes a new Center for Medicare & Medicaid Innovation that will begin testing new ways of delivering care to patients. These new methods are expected to improve the quality of care & reduce the rate of growth in costs for Medicare, Medicaid, & the Children’s Health Insurance Program (CHIP). By January 1, 2011, DHHS will submit a national strategy for quality improvement in health care, including these programs.
Improving Health Care Quality and Efficiency
Effective no later than January 1, 2011
2010 2011
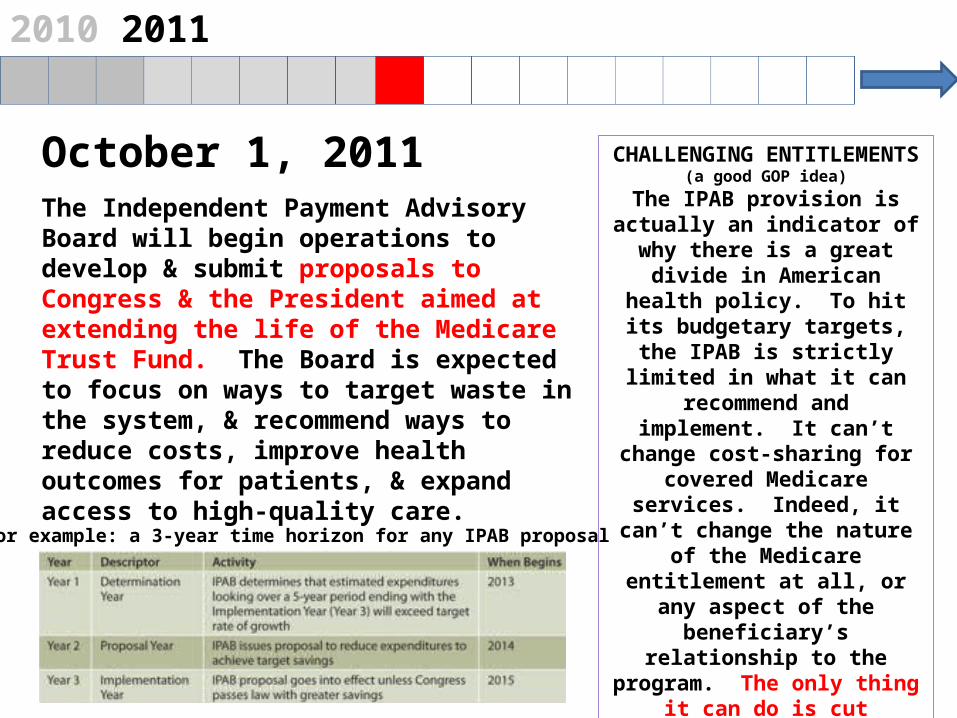
October 1, 2011The Independent Payment Advisory Board will begin operations to develop & submit proposals to Congress & the President aimed at extending the life of the Medicare Trust Fund. The Board is expected to focus on ways to target waste in the system, & recommend ways to reduce costs, improve health outcomes for patients, & expand access to high-quality care.
CHALLENGING ENTITLEMENTS(a good GOP idea)
The IPAB provision is actually an indicator of
why there is a great divide in American health
policy. To hit its budgetary targets, the
IPAB is strictly limited in what it can recommend and implement. It can’t change cost-sharing for
covered Medicare services. Indeed, it can’t change the nature of the Medicare entitlement at all, or any aspect of the
beneficiary’s relationship to the program. The only
thing it can do is cut Medicare payment rates
for those providing services to the beneficiaries.
For example: a 3-year time horizon for any IPAB proposal

2010 2011
Expands Cafeteria-Style “Flex” Plans. Creates a Simple Cafeteria Plan to provide a vehicle through which small businesses can provide tax-free benefits to their employees. This would ease the small employer’s administrative burden of sponsoring a cafeteria plan. PPACA also exempts employers who make
contributions for employees under a simple cafeteria plan from pension plan nondiscrimination requirements applicable to highly compensated and key employees.

2010 2011
New Limits to Health Flexible Savings Account Contributions.
Limits the amount of contributions that can be made to health FSAs to $2,500 per year, indexed by CPI for subsequent years. Further limits FSA payments to in-hospital & doctor-prescribed care, no more OTC coverages.
But then 2011 Also
Brings Some Tax Changes
to Individuals:
2010 2011
Increased Additional Tax for Withdrawals from Health Savings
Accounts and Archer Medical Savings Account Funds for Non-Qualified
Medical Expenses.
Increases the additional tax for HSA withdrawals prior to age 65 that are not used
for qualified medical expenses from 10 to 20%. The additional tax for Archer MSA
withdrawals not used for qualified medical expenses would increase from 15 to 20%

2010 2011
And then in 2011 There are Some Tax Changes for Businesses too:
Eliminates the Deduction for Employer Part D Subsidy. No more deduction for the
subsidy for employers who maintain prescription drug plans for their Medicare
Part D eligible retirees.The Part D Employer Subsidy was added to the 2003 Medicare Modernization Act by Republicans (without a single Democratic
vote) as a “carrot” to keep employers from dropping their retiree coverage for drugs after the new Medicare Part D program started in 2006. The idea was to hold down the reported cost of the new Medicare Part D benefit by burying a substantial part of the cost as a tax cut to businesses. We all know how well that has worked as employers have been dropping all of their health coverage for
their retirees, including Rx, like a hot potato ever since. Democrats now will phase it out via PPACA without a single GOP
vote.
2010 2011
The new Community First Choice Option
allows States to offer home & community based services to
disabled individuals through Medicaid rather than institutional care
in nursing homes.
Increase Access to Home & Community Services
Effective beginning October 1, 2011
Note: This was an idea pushed extensively by Republicans during the Bush presidency. President Bush included calls for
this 3 times in his State of the Union addresses. It will be interesting to see how many red state governors take
advantage of the option. Or if they continue to stall, hoping the entire PPACA falls on its face.

2010 2011 2012
PPACA provides incentives for physicians to join together to form “Accountable Care Organizations.” In these groups, doctors can
better coordinate patient care & improve the quality, help prevent disease & illness, & reduce unnecessary hospital
admissions. If Accountable Care Organizations provide high quality care & reduce costs to the health care system, they can
keep some of the money that they have helped save.
Encouraging Integrated Health Systems
Effective January 1, 2012
2010 2011 2012
To help understand and reduce persistent health disparities, the law requires any ongoing or new Federal health program to collect and report racial, ethnic and language data. The Secretary of Health and Human Services will use this data to help identify and reduce disparities.
Understanding and Fighting Health Disparities
Effective March, 2012

2010 2011 2012
PPACA creates a voluntary LTC insurance program (CLASS) with cash benefits to disabled adults.
Providing New, Voluntary Options for Long-Term Care Insurance
Benefit plan no later than October 1, 2012
Neither private health insurance nor Medicare cover basic LTC services. Private LTC coverage is available in the individual
insurance market, but policies have high premiums & limited benefits. Many families deplete their resources & are forced onto Medicaid for long-term care. 40% of the people who need LTC are
non-elderly with serious disabling conditionsWorking-age adults will be able to choose to have premiums
deducted from their paychecks to purchase public LTC insurance through CLASS, starting in 2012 or 2013. No one will be required to participate in CLASS. Employers may elect to enroll their workers
automatically, but if so, a worker will be able to opt out. The younger the age at which a person enrolls, the lower the premium.
Enrollees can continue to participate by paying premiums after they leave the labor force or retire. If they become disabled, enrollees
who have contributed for at least 5 years will automatically qualify for help to purchase home-based services, assisted living, or nursing
home care.

2010 2011 2012
Health care remains one of the few industries that relies on
paper records. PPACA institutes a series of changes to
standardize billing & requires health plans to begin adopting &
implementing rules for the secure, confidential, electronic
exchange of health information.
Reducing Paperwork & Administrative CostsFirst regulations effective October 1, 2012
Using electronic health records will reduce paperwork and administrative
burdens, cut costs, reduce medical errors &, most importantly, improve the quality
of care.

2010 2011 2012
The law establishes a hospital Value-Based
Purchasing program (VBP) in Original Medicare. This program offers financial
incentives to hospitals to improve the quality of care.
Hospital performance is required to be publicly
reported, beginning with measures relating to heart
attacks, heart failure, pneumonia, surgical care, &
health-care associated infections.
Linking Payment to Quality OutcomesEffective for payments for discharges occurring on or after October
1, 2012

2010 2011 2012 2013
To expand the number of Americans receiving
preventive care, PPACA provides new funding to state Medicaid programs
that choose to cover preventive services for patients at little or no
cost.
Expanding Medicaid Preventive Health Coverage
Effective January 1, 2013
2010 2011 2012 2013
Increasing Primary Care Medicaid PaymentsEffective January 1, 2013
As Medicaid programs and providers prepare to cover more patients in 2014, the Act
requires states to pay primary care physicians no less than 100 percent of Medicare payment
rates in 2013 and 2014 for primary care services. The increase is fully funded by the
federal government.
2010 2011 2012 2013
PPACA establishes a system of payment “bundling” – where hospitals, doctors, and
providers are paid a flat rate for an episode of care rather than the current fragmented
system where each service or test are billed separately to Medicare.
expanded Authority to Bundle Payments
Effective no later than January 1, 2013.
Bundle: instead, say, a surgical procedure generating multiple claims from multiple
providers, the entire team is compensated with a “bundled” payment that provides incentives to deliver health care services
more efficiently while maintaining or improving quality of care. It aligns the incentives of those delivering care, and
savings are shared between providers and the Medicare program

2010 2011 2012 2013
Under PPACA, states will receive two more years of
funding to continue coverage
for children not eligible for Medicaid.
Additional Funding for the Children’s Health Insurance Program (S-CHIP)
Effective October 1, 2013

2010 2011 2012 2013 2014
Under PPACA, most individuals will be required to obtain basic
health insurance coverage or pay
a fee to help offset the costs
of caring for uninsured
Americans.
Individual MandateEffective January 1, 2014
When President Clinton was pushing for employers to cover their workers in his 1993 bill, John Chafee of Rhode Island, along with 20 other GOP senators and
Rep. Bill Thomas of California, introduced legislation that instead
featured an individual mandate. Three of those Republican co-sponsors — Orrin Hatch of Utah, Charles Grassley of Iowa,
and Christopher Bond of Missouri — remain in the Senate today.

2010 2011 2012 2013 2014
Starting in 2014 if your employer doesn’t offer insurance, you will be able to buy insurance
directly in an Exchange -- a new transparent and competitive insurance marketplace where individuals and small businesses can buy
affordable and qualified health benefit plans. Exchanges will offer you a choice of health plans
that meet certain benefits & cost standards. Starting in 2014, Members of Congress will be getting their health care
insurance through Exchanges, and you will be able buy your insurance through Exchanges too.
Establishing Health Insurance Exchanges
Effective January 1, 2014

2010 2011 2012 2013 2014
Workers who cannot afford the coverage provided by their
employer may take whatever funds their employer might have
contributed to their insurance and use these resources to help purchase a more affordable plan
in the new health insurance Exchanges. These new
competitive marketplaces will allow individuals and small businesses to buy qualified
health benefit plans.
More Choices for WorkersEffective January 1, 2014
Starting in 2014, Members of Congress will be getting their health care insurance through Exchanges.
Former Bush Secretary of HHS, Mike Leavitt has
formed a consulting company to advise states how to use
“Exchanges” to limit health care costs as he did as Republican
governor of Utah.

It’s not hard to understand why: Utah stands with Massachusetts in having the only statewide health exchanges in operation. With minimal bureaucracy — the Utah Health Exchange operates with a $500,000 budget and two or three employees — and a maximum commitment to free-market principles, it hews closely to how many believe a marketplace ought to operate, with just the appropriate amount of government “interference,” or of you prefer “guidance.”
The Utah Exchange: National Model ???
Or … Troublesome to PPACAJust after the health care law passed, many on both sides of the aisle, in a rare exercise of bipartisanship, quickly coalesced around the Utah Health Exchange as the best-case scenario for implementing the new law.
“The Utah model is a valid model for an exchange,” Joel Ario, the DHHS official who oversees the implementation of health exchanges, has said. “But Utah will also be the first to say they have some work to do to get their model to work [under PPACA], with all the technical specifications they need to meet and how they deal with qualified plans.”

• We are given the flexibility to decide which insurers are permitted to offer their products in the Exchange. • All the law's expensive benefit mandates are waived, so that our citizens aren't forced to buy benefits through the Exchange they don't need and have a range of choice that includes more affordable plans.• The law's provisions discriminating against consumer-driven plans, such as health savings accounts, are waived.• We are given the freedom to move Medicaid beneficiaries into the exchange, or to utilize new approaches to the traditional program, instead of herding hundreds of thousands more people into today's broken Medicaid system.• Our state is reimbursed the true, full cost of the administrative burden running an Exchange will imposed on us.• A trustworthy projection is commissioned, by a research organization independent of the department, of how many people are likely to wind up in the Exchange, given the large incentives for employers to save money by off-loading their workers.
At Least a few Politicians are Acting Like Adults… Indiana Gov. Mitch Daniels Has Actually
Suggested a few Items to make PPACA Work… at Least as Far as He is Concerned

“Health Exchange” at Work
Private

2010 2011 2012 2013 2014
Americans who earn less than 133% of the poverty level ($14,000 for an individual and $29,000 for a family of four) will be eligible
to enroll in Medicaid.
Increasing Access to MedicaidEffective January 1, 2014
States will receive 100% federal funding
for the first three years to support this expanded coverage,
phasing to 90% federal funding in subsequent
years.

2010 2011 2012 2013 2014
Tax credits will become available for people with incomes above 100% and below 400% of poverty ($43,000 for an
individual or $88,000 for a family of four in 2010) who are not eligible for or offered other affordable coverage. These
individuals may also qualify for reduced cost-sharing (copayments, coinsurance, and deductibles).
PPACA Provides Tax Credits to Help Make Care More Affordable
Effective January 1, 2014
Family of Four IncomeMaximum % of Income Paid for
Health Premiums
Percent of Costs Paid for by
Insurance Plan
$22,000 - $29,000 2.0% 94%$29,000 - $33,000 3.0-4.0% 90%$33,000 - $44,000 4.0-6.3% 85%$44,000 - $55,000 6.3-8.1% 73%$55,000 - $66,000 8.1-9.5% 70%$66,000 - $77,000 9.5% 70%$77,000 - $88,000 9.8% 70%

2010 2011 2012 2013 2014
PPACA prohibits new plans and existing group
plans from imposing annual
dollar limits on the amount of
coverage an individual may
receive.
Eliminating Annual Limits on Insurance Coverage
Effective January 1, 2014
2010 2011 2012 2013 2014
The law implements strong reforms that prohibit
insurance companies from refusing to sell coverage or renew policies because
of an individual’s pre-existing conditions. Also,
in the individual and small group market, it
eliminates the ability of insurance companies to
charge higher rates due to gender or health status.
No Discrimination Due to Pre-Existing Conditions or Gender
Effective January 1, 2014

2010 2011 2012 2013 2014
The law implements the second phase of the small business tax credit for qualified small
businesses and small non-profit organizations. In this phase, the credit is up to 50% of the employer’s contribution to provide health
insurance for employees. There is also up to a 35% credit for small non-profit organizations.
Increasing Small Business Health Insurance Tax Credit
Effective January 1, 2014

2010 2011 2012 2013 2014
A new provision will tie physician payments to the quality of care they provide. Physicians will
see their payments modified so that those
who provide higher value care will receive higher
payments than those who provide lower quality
care. “Pay for Performance”
2015
Paying Physicians Based on Value Not Volume
Effective January 1, 2015
NEED MORE INFORMATION ???
WANT TO KNOW WHAT WILL HAPPEN NEXT ???
---VISIT
www.health-politics.com…for regular updates &
commentary,or e-mail Jeanne at
& ask her