case studies in patient safety: foundations in core ... studies in patient safety: foundations in...
TRANSCRIPT
Case Studies in Patient Safety: Foundations in Core Competencies
CONSUMERS ADVANCING PATIENT SAFETY
August 2015 Webinar

Welcome
• Dr. Knitasha Washington, FACHE, Executive Director of CAPS

Learning Objectives
• Understand how patient stories can be used to teach Safety Across the Board principles.
• Explore one story and how you can use this and similar stories in the book, Case Studies in Patient Studies: Foundations in Core Competencies, in teaching Safety Across the Board principles.
• Learn how advance training and implementation of neonatal rapid response teams improves quality and safety in maternal and child health.
• Discuss how patients and families may be invited to share stories in a manner that allows their message to be heard by your key stakeholders.

Agenda
1. Helen Haskell – An overview of the book Case Studies in Patient Safety.2. Lisa Morrise – Share, briefly, the story from the book, “The Trial Meant for You: The Lifelong Medical Journey of a Child with a Complex Congenital Condition.”3.Deborah Kilday, MSN – Detail how implementation and training of neonatal rapid response teams works to mitigate issues upon birth of a compromised infant. Discuss the importance of early identification and a team training approach to improve quality and safety in labor and delivery and neonatal emergent needs.4. Developing and using questions to prompt Safety Across the Board DiscussionHelen Haskell and Lisa Morrise and Deborah Kilday –How questions exploring safety issues were developed from the patient stories shared in the book. How you may develop similar questions.5. A family member’s perspective on consequences and using patient experience to advocate for Safety Across the Board - Lisa Morrise

Case Studies in Patient Safety
The Patient Story
• “Meeting people where they are”
• Providers rarely hear the whole story.
• The story as a source for learning.
• Finishing the story - What can be done in response?

The Trial Meant for You
• Where that title comes from.• Kirsten was born after a 38
week gestation.• I had ultrasounds and
biophysical profiles. Too much amniotic fluid, despite being too low in prior pregnancies.
• No sign of breathing, no surfactant in amniotic fluid
• Problematic delivery• Born with Pierre Robin
Sequence – recessed mandible, complete bilateral cleft palate, retro tongue base
• Immediate airway emergency

Rescued – after two hours
• I met Kirsten after two hours in the REGULAR newborn nursery.
• The Resident.
• The Nurse.
• The NICU.
• The Diagnosis.
• The rest of the story in a nutshell.

Sixteen Years Later
• Annual dinner meeting of Parent to Parent program for the NICU at Kirsten’s birth hospital.
• Introductions around the table.
• We know YOU!

Today
• 44 surgeries later, including three jaw advancement efforts.
• Tracheal malacia and stenosis from tracheotomy – requires laser reduction every 1-2 years.
• Studies Social Work at Utah State.
• We advocate for Safety Across the Board in Healthcare.

Deborah Kilday, MSN, RN
Senior Performance Partner
Quality and Safety Division
Premier, Inc.
Case Studies in Patient Studies:
Foundations in Core Competencies
Thursday, August 27, 2015

12© 2015 PREMIER, INC.
I have no actual or potential conflict of interest in relation to
this program/presentation.
Disclosure

13© 2015 PREMIER, INC.
1999 we learned that 98,000 people were dying every year
from preventable errors in hospitals ~ IOM To Err is Human
2013 it is estimated that more than 440,000 people per
year die from preventable harm in hospitals ~ Journal of Patient Safety
Preventable medical errors ranks 3rd highest killer in U.S.
only to heart disease and cancer. ~ The Leapfrog Group 2013
“We are burying a population the size of Miami every year
from medical errors that can be prevented” ~ The Leapfrog Group 2013
Preventable deaths in hospitals

14© 2015 PREMIER, INC.
Approximately 4.1 million women in the U.S. between the ages of 15
and 50 gave birth from May 2013 to May 2014.
In 2013, 18 mothers died in the U.S. for every 100,000 live births,
The U.S. has FALLEN to 64th in the world on maternal mortality.
The U.S. ranks 3rd in the world for C/S, where 30% of women have
surgical deliveries
Adverse events occur in approximately 9% of all deliveries in the US.
at a cost of $17 billion annually
Maternal mortality
Leading causes of maternal death:
1. Obstetric Hemorrhage
2. Hypertension in Pregnancy
3. Venous Thromboembolism

15© 2015 PREMIER, INC.
U.S. ranks 41st in the world for risk of newborn death ~ 24,000 deaths
Due to high infant mortality rates, the U.S. is ranked 31st as the best
place to have a baby
U.S has the highest first-day infant death rate out of all the
industrialized countries in the world deaths
Neonatal mortality
CDC/NCHS, linked birth/infant death data set

16© 2015 PREMIER, INC.
Estimated 50 - 90% of these events preventable
Just the tip of the iceberg

17© 2015 PREMIER, INC.
“Identify specific triggers for responding to changes in the
mother’s vital signs and clinical condition and develop and
use protocols and drills for responding to changes, such as
hemorrhage and pre-eclampsia. Use the drills to train staff
in the protocols, to refine local protocols, and to identify and
fix systems problems that would prevent optimal care.”
Preventing maternal death
JC SE #44 ~ 2010
18© 2015 PREMIER, INC.
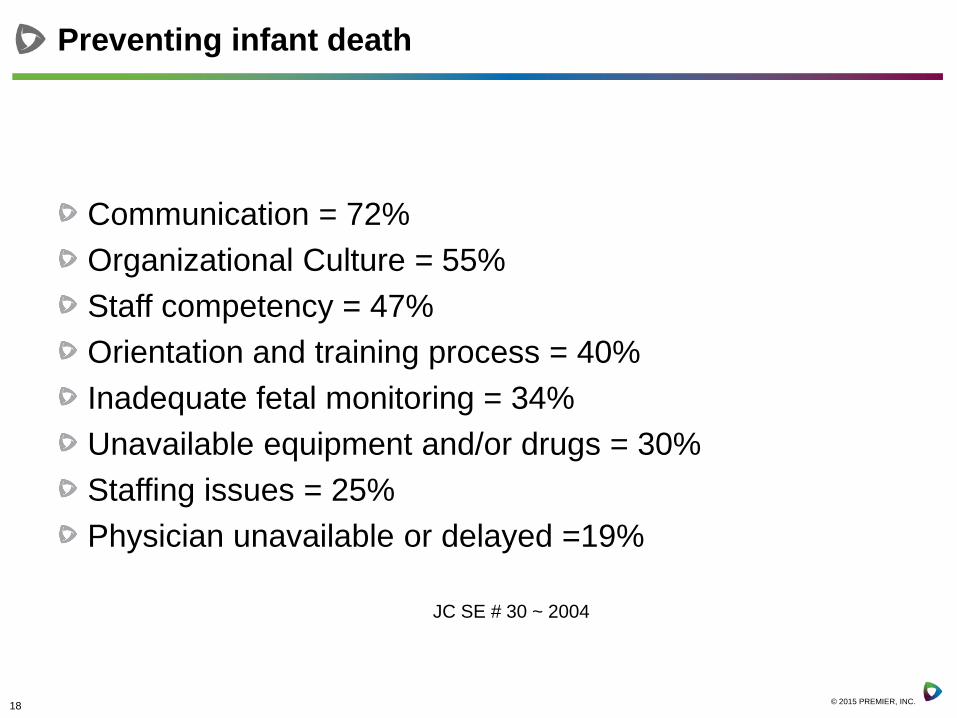
Communication = 72%
Organizational Culture = 55%
Staff competency = 47%
Orientation and training process = 40%
Inadequate fetal monitoring = 34%
Unavailable equipment and/or drugs = 30%
Staffing issues = 25%
Physician unavailable or delayed =19%
Preventing infant death
JC SE # 30 ~ 2004

19© 2015 PREMIER, INC.
Culture of safety
The root of most sentinel events involving injury and death
is a flawed delivery system
This has led many systems to develop highly reliable units
and integrate a rooted culture of safety
General safety culture concepts; Strong leadership
Multidisciplinary team interaction
Adherence to principles of evidence based medicine
Standardized policies and procedures for clinical operations
Common terminology
Timely communication
High degree of emergency readiness

20© 2015 PREMIER, INC.
Improving “Readiness, Recognition and Response”
Implementation of RRT’s as an important strategy in the
prevention of deaths is supported by research from:
Institute of Medicine
Agency for Healthcare
Quality and Research
Institute for Health
Improvement
The American Heart
Association
The Joint Commission
21© 2015 PREMIER, INC.
Practice as a Team

22© 2015 PREMIER, INC.
The Effectiveness of Combined Training Modalities on
Neonatal Rapid Response Teams
“The Effectiveness of Combined Training Modalities on Neonatal Rapid Response Teams” Clinical Simulation in Nursing, Volume 9, Issue 7 , July 2013.
Time is Life ~ Speed is Essential

23© 2015 PREMIER, INC.
Research results
Data Analysis
Increased teamwork and safety
climate
Increased knowledge
assessment scores
Increased team performance
Lessons Learned
Availability of self-inflating
versus flow inflating ambu bags
System standardization of
neonatal code carts
Assignment and management
of equipment checklists
Repair or replacement of
broken or missing equipment
Standardized team education
Practice critical events as a
team
Design of Patient- or Family-
Activated RRT
“The Effectiveness of Combined Training Modalities on Neonatal Rapid Response Teams” Clinical Simulation in Nursing, Volume 9, Issue 7 , July 2013.
24© 2015 PREMIER, INC.
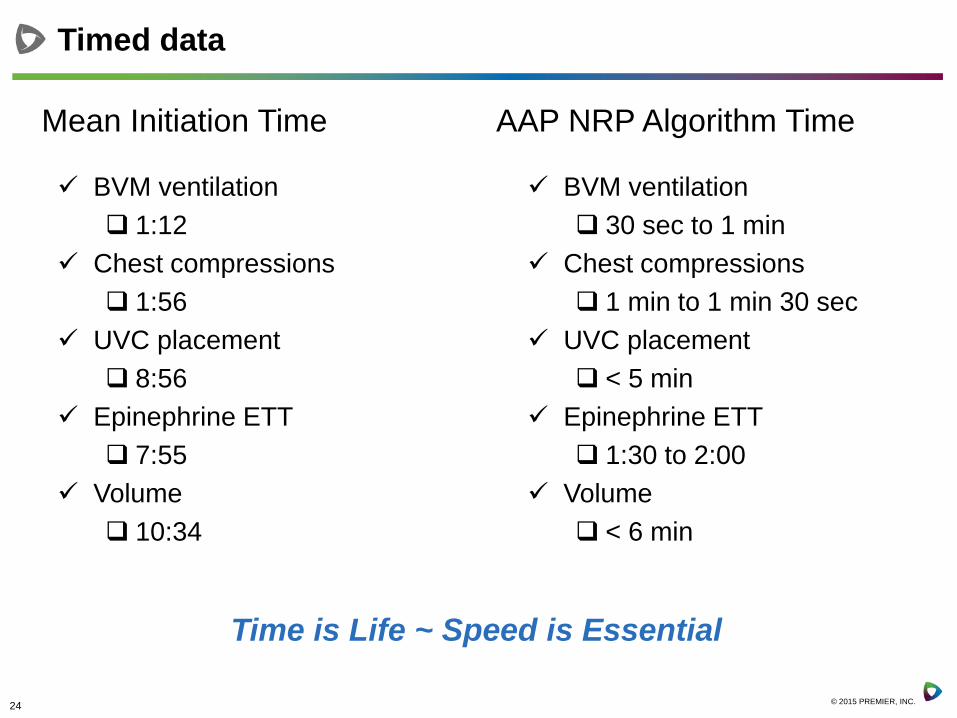
Timed data
Mean Initiation Time AAP NRP Algorithm Time
BVM ventilation
1:12
Chest compressions
1:56
UVC placement
8:56
Epinephrine ETT
7:55
Volume
10:34
BVM ventilation
30 sec to 1 min
Chest compressions
1 min to 1 min 30 sec
UVC placement
< 5 min
Epinephrine ETT
1:30 to 2:00
Volume
< 6 min
Time is Life ~ Speed is Essential

25© 2015 PREMIER, INC.
Readiness: Resources, supplies & equipment
Availability of BloodEmergency Cart
Activated TeamLaryngeal Mask
Pulse Oximeter
Medications
26© 2015 PREMIER, INC.
Common themes of opportunity
2
6

27© 2015 PREMIER, INC.
Recognition: Informed Patients and Families
Awareness of risks, signs and symptoms
How to ask for and call for help
Implement patient education strategies
Target to the educational level of the patients

28© 2015 PREMIER, INC.
You are the most important member of your healthcare
team
Understand what it means to get quality healthcare, and
how to find it
Choose a healthcare team that will partner with you
Learn about your condition and how to care for yourself
Take action if you are not getting the right care
Activated patient and family

29© 2015 PREMIER, INC.
Informed consumer

30© 2015 PREMIER, INC.
Ask questions;
How does your quality of care measure up?
What do your patients say about you?
What are barriers to care (rural communities)?
Are your doctors and nurses board-certified?
What is the organizations compliance with
accreditation for quality and safety standards?
What is your healthcare team's experience in
diagnosing and treating your type of condition?
How do you prepare for and respond to emergencies?
Is 24/7 in-house provider coverage available?
Informed consumer

31© 2015 PREMIER, INC.
Prepare for appointments and procedures
• List your visit goals with the most important ones first
• Bring a friend or family member to appointments
• Bring a list of all your medications
• Share preferences, needs, medical history and other
information
• Actively listen to what the medical team tells you
• Ask more questions
Prepare

32© 2015 PREMIER, INC.
Consumers Advancing Patient Safety - http://www.patientsafety.org/
Hospital Safety Score - http://www.hospitalsafetyscore.org/
Patient Safety America - http://patientsafetyamerica.com/
The Joint Commission - http://www.jointcommission.org/topics/speakup_brochures.aspx
Nursing Home Compare - www.medicare.gov/NHCompare
Hospital Compare - www.hospitalcompare.hhs.gov
Physician Compare - www.medicare.gov/find-a-doctor/provider-search.aspx
Home Health Compare - www.medicare.gov/homehealthcompare
Leapfrog Group - www.leapfroggroup.org
Informed Patient Institute - www.informedpatientinstitute.org
Aligning Forces for Quality - www.forces4quality.org
Partnership for Patients - http://partnershipforpatients.cms.gov/
Solutions for Patient Safety - www.solutionsforpatientsafety.org
Transforming Maternity Care - http://transform.childbirthconnection.org/resource
Council for Patient Safety - www.safehealthcareforeverywoman.org
Safe Motherhood Initiative - Maternal safety materials http://www.acog.org
Preeclampsia Foundation - www.preeclampsia.org
Premier Safety Institute - http://www.premiersafetyinstitute.org/
Premier Advisor Live Education - https://www.premierinc.com/events/
Finding quality national resources

33© 2015 PREMIER, INC.
Our ultimate goal
34© 2015 PREMIER, INC.
Questions and contact information
Deb Kilday, MSN, RN
Senior Performance Partner
Premier Inc.
Discussion
• Questions from Case Studies in Patient Safety:
– “What cognitive biases do you think might have contributed to the errors in Kirsten’s care?”
– “Should a family be told if their loved one’s events are being used for teaching? What practical and emotional effects do you think this lack of disclosure might have had on the family?”
– “Do you think disclosure of adverse events is effectively done now?”

More Discussion
• Your questions
• How do you use patient stories in illustrating Safety Across the Board concepts?
• How do you use YOUR story to advocate?

Upcoming Events
• September 24 – Linda Kenney – Supporting Patients and Providers After an Adverse Event
• October 22 – Ilene Corina – Turning Personal Tragedy into Advocacy – Meeting the Needs of Vulnerable Populations