mechanism of action and morphologic changes in the … the mechanical basis of orthodontic...
TRANSCRIPT

ORIGINAL ARTICLE
Mechanism of action andmorphologic changes inthe alveolar bone in response to selective alveolardecortication–facilitated tooth movement
S. Susan Baloul,a Louis C. Gerstenfeld,b Elise F. Morgan,c Roberto S. Carvalho,d Thomas E. Van Dyke,e
and Alpdogan Kantarcif
Boston, Mass
aResidUnivebProfeMass.cAssoMass.dAssisBostoeProfeGoldmfAlpdoBiologDr. S.The aproduReprinInstituSubm0889-Copyrdoi:10
Background and Purpose: The aim of this study was to test if corticotomy-induced osteoclastogenesis andbone remodeling underlie orthodontic tooth movement and how selective alveolar decortication enhances therate of tooth movement. Materials and Methods: A total of 114 Sprague-Dawley rats were included in 3treatment groups: selective alveolar decortication alone (SADc); tooth movement alone (TM); and “combined”therapy (SADc 1 TM). Surgery was performed around the buccal and palatal aspects of the left maxillary firstmolar tooth and included 5 decortication dots on each side. Tooth movement was performed on the firstmolar using a 25-g Sentalloy spring. Measurements were done at baseline (day 0: no treatment rendered)and on days 3, 7, 14, 21, 28 and 42. Microcomputed tomography, Faxitron analyses, and quantitative real-time polymerase chain reaction (q-PCR) of expressed mRNAs were used to assess changes. Results: Thecombined group showed increased tooth movement (P 5 0.04) at 7 days compared with the tooth movementgroup with significantly decreased bone volume (62%; P 5 0.016) and bone mineral content (63%; P 5
0.015). RNA markers of osteoclastic cells and key osteoclastic regulators (M-CSF [macrophage colony-stimulating factor], RANKL [receptor activator of nuclear factor kappa-B ligand], OPG [osteoprotegerin],calcitonin receptor [CTR], TRACP-5b [tartrate-resistant acid phosphatase 5b], cathepsin K [Ctsk]) all showedexpression indicating increased osteoclastogenesis in the combined group. RNA markers of osteoblasticcells (OPN [osteopontin], BSP [bone sialoprotein], OCN [osteocalcin]) also showed increased anabolicactivity in response to the combination of alveolar decortication and tooth movement. Conclusions: The datasuggest that the alveolar decortication enhances the rate of tooth movement during the initial tooth displacementphase; this results in a coupled mechanism of bone resorption and bone formation during the earlier stages oftreatment, and this mechanism underlies the rapid orthodontic tooth movement. (Am J Orthod DentofacialOrthop 2011;139:S83-101)
ent, Department of Orthodontics and Dentofacial Orthopedics, Bostonrsity Goldman School of Dental Medicine, Boston, Mass.ssor of Orthopedic Surgery, Boston University School of Medicine, Boston,
ciate professor of Mechanical Engineering, Boston University, Boston,
tant professor, Department of Orthodontics and Dentofacial Orthopedics,n University Goldman School of Dental Medicine, Boston, Mass.ssor, Department of Periodontology and Oral Biology, Boston Universityan School of Dental Medicine, Boston, Mass.gan Kantarci, Associate Professor, Department of Periodontology and Oraly, Boston University Goldman School of Dental Medicine, Boston, Mass.Susan Baloul is the recipient of the 2010 Milo Hellman Research Award.uthors report no commercial, proprietary, or financial interest in thects or companies described in this article.t requests to: Alpdogan Kantarci, Department of Periodontology, Forsythte, 245 First Street, Cambridge, MA 02142; e-mail, [email protected], March 2010; revised and accepted, September 2010.5406/$36.00ight � 2011 by the American Association of Orthodontists..1016/j.ajodo.2010.09.026
Historically, orthodontic tooth movement was de-scribed as a site-specific bone remodeling andconsists of coupled bone resorption and bone
formation.1 The mechanical basis of orthodontictreatment is the application of force (stimuli) to the teethusing an appliance. This, in turn, leads to biologic reac-tions, including remodeling changes in the dental andperiodontal tissues.2
Biologically, tooth movement has 2 fundamentalrequirements: (1) periodontal ligament (PDL) betweenthe tooth and alveolar bone and (2) bone turnover. Inresponse to orthodontic force, the PDL mediates the mo-bility of the tooth in the alveolus.3 The bone is temporar-ily and spatially regulated, facilitating the movement ofteeth.4 Application of force during orthodontic toothmovement leads to osteoclastogenesis characterizedby tissue damage with production of inflammatory
S83

S84 Baloul et al
mediators in the PDL and alveolar process deformation.A few days after force application, the first osteoclastprogenitor cells appear at the compression sites in the al-veolar crest vasculature and marrow spaces, and the PDLspace widens. Osteoclasts appear in higher quantity atthe compression sites compared with tension sites.5
While the pathologic aspect of inflammation cer-tainly does not represent the physiologic response tothe mechanical forces by the alveolar bone during theorthodontic therapy, pathways inherent to inflammatoryprocesses regulate the bone turnover, soft and hard tis-sue reactions, and the healing process. Proinflammatorycytokines such as interleukin-6, interleukin-8, andtumor necrosis factor-a are produced at this stage,which supports the notion that the pathways of inflam-mation initiate the osteoclastogenesis during toothmovement.6,7 Osteoclastic activity is characterized bychanges in tooth-supporting tissue biomarkers of recep-tor activator of nuclear factor (RANK), RANKL, and OPGduring tooth movement. RANKL expression is increasedin response to compressive forces and mediated by pros-taglandin E2.8 RANKL mediates osteoclastogenesis andtooth movement, and its actions are antagonized byOPG. Osteoclastic activity is coupled with osteogenesis,where the type of orthodontic force determines theosteoblast recruitment and tensile strains determinethe osteogenic activity. Tensile strains stimulate theproliferation of the osteoblast progenitor cells in thePDL, leading to bone formation and inhibition of boneresorption.
Various methods have been tested to enhance therate, magnitude, and stability of the tooth movement.While the history of intentional wounding of the alveolarbone to enhance the speed of the tooth movement datesback to the late 19th century, K€ole9 reintroduced thecorticotomy procedure to orthodontic therapy. He pro-posed that by disturbing the continuity of the corticallayer, tooth movement would increase dramatically asa “bony block” with several teeth embedded. This tech-nique was not widely accepted because of its invasivenature, but it was tested in various experimental modelswith some modifications.10-12 More recently, acceleratedosteogenic orthodontics has been introduced asa combination of ideas from previous corticotomy-facilitated tooth movement, along with periodontaltherapy including alveolar bone augmentation, allowingthe selective alveolar decortication in areas of desiredtooth movement.13,14
It was proposed that the coupling between deminer-alization and remineralization during corticotomy-facilitated toothmovement therapy was due to a regionalacceleratory phenomenon and not as a net result of bony“block” movement.13 Following the observation that
April 2011 � Vol 139 � Issue 4 � Supplement 1 American
bone resorption occurs following the periosteal flap sur-gery15; rapid mineral release was hypothesized to occurduring the earlier weeks after the surgery followed by re-sorption of the bone organic matrix, release of calcium,and occurrence of localized osteoporosis. However,while the clinical protocols have been well defined andsuccessful outcomes have been reported, the biologicmechanism underlying the corticotomy-assisted toothmovement is not understood.
A recent rat model studying the biologic mechanismsunderlying the corticotomy process in vivo demon-strated that bone turnover followed the alveolar decorti-cation, suggesting that a periodontium-mediatedRegional Acceleratory Phenomenon (RAP) accompaniesthe decortication. Enhancement of the PDL activityand a dominant role by the spongiosa suggested thattooth movement could be the result of increased turn-over rate in alveolar bone.16
We have hypothesized that SADc-induced osteoclas-togenesis and bone remodeling underlie the orthodontictooth movement, where alveolar decortication enhancesthe rate of tooth movement by increasing bone remod-eling compared with conventional tooth movement.Thus, the aims are (1) to study the rate of tooth move-ment after orthodontic treatment with or withoutSADc, (2) to examine the alveolar bone structure afterorthodontic tooth movement with or without SADcusing MicroCT, (3) to analyze the osteoclastic andosteoblastic activities in selective alveolar decortication-facilitated tooth movement at the molecular level, and(4) to assess the temporal relationships in the expressionof regulatory genes that control bone formation andremodeling.
MATERIAL AND METHODS
Study design
The study included a total of 114 Sprague-Dawley(Crl:CD) rats obtained from Charles River Laboratories,Mass. The study protocol was approved by the Institu-tional Animal Use and Care Committee. All animalswere housed at the Laboratory Animal Science Centerwhere all procedures, including surgery, orthodontic ap-pliance application, orthodontic appliance removal, andeuthanasia were performed. A 12-hour light cycle wasmaintained during the period of observation, and a reg-ular hard diet was supplied. The animals were anesthe-tized intraperitoneally with a mixture of anestheticsolution (100 mg/kg of ketamine hydrochloride [KetasetIII; Injectable, 100 mg/mL, Fort Dodge Animal Health,Fort Dodge, Iowa], 4 mg/kg of xylazine hydrochloride[AnaSed; Injectable, 20 mg/mL, Lloyd Inc., Shenandoah,Iowa], and 0.9% sodium chloride solution [Hospira Inc.,
Journal of Orthodontics and Dentofacial Orthopedics

Table I. Study design*
Time(Days) Subgroup
Faxitron,Micro-CT
Molecularmarkers (RNA)
0 Baseline controls 3 33 SADc 3 3
TM 3 3SADc 1 TM 3 3
7 SADc 3 3TM 3 3
Baloul et al S85
Lake Forest, Ill]). During the surgery, animals wereclosely monitored and a heating pad was placed underthe operation field to avoid body temperature loss. Ob-servations were made at baseline (day 0: no treatmentrendered) and days 3, 7, 14, 21, 28, and 42. Table I sum-marizes the distribution of the animals among differentgroups and subgroups with the corresponding observa-tion periods; Figure 1 represents the study design andtimeline.
SADc 1 TM 3 314 SADc 3 3
TM 3 3SADc 1 TM 3 3
21 SADc 3 3TM 3 3SADc 1 TM 3 3
28 SADc 3 3TM 3 3SADc 1 TM 3 3
42 SADc 3 3TM 3 3SADc 1 TM 3 3
57 57Total 114
*Table summarizes the study design and animal numbers in eachgroup. Half of the animals were used in microcomputed tomography(MicroCT), and Faxitron analyses and the rest were used for molec-ular biology studies (RNA isolation and real-time PCR). Timeline in-cluded baseline observation, where no procedures were performed,and 3, 7, 14, 21, 28 and 42 days of active tooth movement. Nineanimals were used at each time point and 3 treatment groupswere defined: selective alveolar bone decortication only (SADc),tooth movement only (TM), and combination of selective alveolarbone decortication with tooth movement (SADc 1 TM).
Clinical procedures
Selective alveolar decortication was performed firstby making a sulcular incision from the mesial aspect ofthe maxillary left first molar, which extended 5 mm(measured by a periodontal probe) in a mesial directionfrom the tooth line-angle extending to the edentuloussoft tissue space adjacent to the molar. Full-thicknessflaps were then elevated on the buccal and palatalaspects. Using a slow-speed hand piece and a smallNo. 1/4 round bur (Buffalo Dental Manufacturing, Syos-set, NY), 5 intramedullary decortication marks—each0.25-mm wide and 0.25-mm deep corresponding tothe size of the bur—were made on both the buccal andpalatal sides under water irrigation. Drilling was donewhere the 0.25-mm bur was fully immersed into bone(for every decortication mark). Flaps were sutured withsimple interrupted bioresorbable 6–0 chromic gutsutures (ACE Surgical Supply Inc., Brockton, Mass).Primary closure was achieved for primary tissue healing.
Orthodontic tooth movement was performed on theleft side of the maxilla. The original technique was firstdescribed by Verna.17 We modified the model to achievestability over the course of the study period. Force wasapplied to the maxillary left first molar using an ultra-light (25 g) superelastic NiTi (Sentalloy) closed coilspring with eyelets (GAC International, Bohemia, NY) be-tween the left maxillary first molar and the maxillary in-cisors. A retentive groove was made using a 1/4 roundbur in a slow-speed hand piece. The groove connectedthe linear mesial angles of the first molar. Another reten-tive groove was made on the central incisors placed asclose to the gingiva as possible on the lateral surfaceof the central incisor continuing to the buccal surfaceof the incisors and ending on the lateral surface of thecontralateral incisor. A 0.010-in stainless steel ligaturewire (GAC international, Bohemia, NY) was inserted un-der the contact point of the first and second maxillaryleft molars palatal and pulled from the buccal usinga Mathieu forceps. The ligature wire was then wrappedaround the first molar under the retentive groove, andthe distal eyelet of the coil spring was engaged intothe palatal end of the ligature wire. The ligature wire
American Journal of Orthodontics and Dentofacial Orthoped
was then tied against the mesial site of the first molar se-curing the distal end of the coil spring to the mesiopala-tal angle of the first molar. Another stainless steelligature wire was inserted into the mesial eyelet ofthe coil spring, snapped between the 2 incisors, wrap-ped around the incisors in a double figure-8 tie run-ning under the retentive groove, and then tiedagainst the buccal surface of the incisors. This wasused to secure the closed coil spring against the palatalsurface of the incisors.
To ensure the stability of the ligature wire in the an-terior area, a 1.5-mm-diameter 4-mm-long titaniumminiscrew (Neuro MD screw, KLS Martin LP, Jackson-ville, Fla) was inserted through the mesial eyelet of thecoil spring palatal to the incisors into the maxillarybone, avoiding the palatal bony suture. Flowable com-posite bonding material (Henry Schein Inc., Melville,NY) was placed over the ligature wire on the mesial-buccal-distal aspects of the incisor teeth. This wasdone to prevent appliance loss and protect the animal’slips from damage by the ligature.
ics April 2011 � Vol 139 � Issue 4 � Supplement 1

Fig 1. Study design and timeline. This figure represents the total number of animals used in the study:equally divided into Group A (descriptive studies: Faxitron and MicroCT analyses) and Group B (mo-lecular biology real-time PCR studies). Furthermore, each group (A and B) was subdivided into 3 ex-perimental treatment groups: selective alveolar decortication alone (SADc), tooth movement alone(TM), and combination of selective alveolar decortication and tooth movement (SADc 1 TM). Timeline included baseline observation, where no procedures were performed, and 3, 7, 14, 21, 28 and42 days of active tooth movement. Nine animals were used at each time point (n5 3 for each treatmentgroup).
S86 Baloul et al
Prior to placement of the bonding material, the inci-sors were etched using a self-etching primer (Transbondplus, 3M Unitek, Monrovia, Calif). The bonding materialwas then light cured. This model resulted in deliveringa continuous 25-g mesial force to the left maxillary firstmolar, with an absolute anchorage resulting from theuse of the miniscrews. The 25-g continued force was mea-sured by an internal dial caliper gauge at the initial day ofthe procedure and the force was remeasured using the cal-iper gauge prior to complete removal of the appliance onthe day of sacrifice. Our measurements showed consistentforce delivery of 25 g throughout the treatment period.
Faxitron-assisted assessment of tooth movement
Two-dimensional radiographic Faxitron imaging hasbeen widely used in animal research for studying thespecimen without distortion. In this study, terminalFaxitron x-ray images (Faxitron X-Ray Corp. Wheeling,Ill) were taken after the harvest of the maxillae. Theimages were taken at 3x magnification with 35 kV for45 seconds’ exposure on XAR-5 Kodak film (Kodak,Rochester, NY). Data obtained from Faxitron imageswas analyzed using Olympus MicroSuite five software
April 2011 � Vol 139 � Issue 4 � Supplement 1 American
(Olympus, Center Valley, Pa). It consisted of the follow-ing linear variables measured from the posterior nasalspine and palatal midline (Fig 2):
1. Anterior-posterior (mesial-distal) length measure-ments
2. Transverse tooth-width measurements3. Space created by mesial movement of right first
molar (distance)4. Rate of tooth movement (distance/time, calculated
from measurements).
Microcomputed tomography
Microcomputed tomography (MicroCT) was used asa tool to study the structural changes, which occurredin bone in 3 dimensions. Samples were immersed inAccustain formalin solution 10% neutral buffered(Sigma-Aldrich Inc., St. Louis, Mo, USA) during scanningin order to minimize decomposition of the tissuethroughout the duration of the scan. Scans were per-formed using a Scanco mCT 40 system (Scanco Medical,Bassersdorf, Switzerland). Total mineral density was cal-culated by converting the grayscale output of bone
Journal of Orthodontics and Dentofacial Orthopedics

Fig 2. Faxitron analysis: A, Graphic presentation of Faxitron analysis of amount of tooth movementdistance in response to TM and SADc 1 TM during tooth movement. B, Graphic presentation ofFaxitron analysis of tooth movement rate in response to TM and SADc 1 TM during tooth movement.C, Illustration of Faxitron analysis linear lines made for measurement of tooth movement distance.D, Table showing P values.
Baloul et al S87
voxels in Hounsfield units (HU) to mineral values (mg/mL of hydroxyapatite) through the use of a calibrationphantom containing air, water, and hydroxyapatite(SB3; Gammex RMI, Middleton, Wis, USA). Total mineraldensity was defined as the average bone voxel HU valuedivided by the average HA phantom HU value multipliedby 1130 mg/mL (hydroxyapatite physical density). Thesame calibration phantom was used in each scan tonormalize mineral density measurements and to accountfor possible variability among scan sessions.
Scans were performed at a resolution of 36 mm/voxel.Samples were filtered to remove extraneous voxels usinga gaussian smoothing algorithm and individually ad-justed using a standard threshold algorithm to segmentbone and nonbone voxels.18 Adjusted MicroCT imageswere used to measure mineralized tissue surroundingthe maxillary first molar. In order to measure the mineral
American Journal of Orthodontics and Dentofacial Orthoped
bone only, with exclusion of tooth-mineral structure, a re-gion of interest was isolated using the contouring option.The bone area found in between the 5 roots of the maxil-lary first molar was defined as region of interest (ROI).Measurements of the bone (total volume) and density (vol-ume fraction andmineral density) were made directly fromthe MicroCT image data of each specimen. The followingmeasurements were obtained from the MicroCT scanning:
TV: The total volume of tissue enclosed by the con-tours that were measuredBV: The volume of the voxels that were above thethreshold (8192), that is, the volume of mineralizedtissue and therefore considered to be bone.BV/TV: Bone volume fraction: the ratio of bone vol-ume to total volume; this parameter is described asa percentage of the total volume that is bone
ics April 2011 � Vol 139 � Issue 4 � Supplement 1

Table II. Probes used in this study from Applied Biosystems*
Gene Gene Symbol UniGene ID Reference Number Primer Sequenceb-Actin Actb Rn.94978 NM_031144.2 CCTTCCTTCCTGGGTATGGAATCCTCalcitonin R Calcr Rn.10062 NM_053816.2 CCGGACTTTGACCCAACAGAAAAGGCathepsin K Ctsk Rn.5598 NM_031560.2 ATAATTAAAAACAGCTGGGGAGAAAOsteocalcin Bglap Rn.9722 NM_013414.1 CTGACAAAGCCTTCATGTCCAAGCAOsteoprotegrin Tnfrsf11b Rn.202973 NM_012870.2 CTGTGCACTCCTGGTGTTCTTGGACRANKL Tnfsf11 Rn.217570 NM_057149.1 GCCGACATCCCATCGGGTTCCCATA
*Table represents gene probes purchased from Applied Biosystems and their pertinent information, including primer sequences.
S88 Baloul et al
Ap
BMD: The average mineral density of only those vox-els above the threshold (ie, voxels that are consideredto be bone tissue)BMC: The average mass of bone mineral over thosevoxels above the threshold and therefore consideredto be bone.
RNA isolation from the alveolar bone
mRNA isolation was prepared from each animalaround the maxillary molar area harvested. The bound-aries of the collected bone area was a box-like configu-ration that measured 5 mm mesial to the maxillarymolar, the exact distal area of the molar, 5 mm palatalbone, and 5 mm buccal bone. In addition, the boxenclosed the root apex. The specimens were powderedin liquid nitrogen using a mortar and pestle. mRNAwas extracted using QIAzol Lysis Reagent (QIAGENInc., Valencia, Calif). RNeasy Lipid Tissue Mini Kit(QIAGEN Inc., Valencia, Calif) was used to purify theRNA as described by the manufacturer. Quantificationof mRNA was determined using NanoDrop 1000 (ThermoFisher Scientific, Wilmington, Del). mRNA sample integ-rity was verified by visualization of ribosomal RNA withGelstar Nucleic Acid Stain (Cambrex Bioscience RocklandInc., Rockland, Me) after denaturing RNA gel electropho-resis. mRNA samples were stored at �80�C until use.RNAse-free water (American Bioanalytical, Natick, Mass)was used for all dilutions during procedures.
Quantitative mRNA expression by q-PCR fordetection of osteoclastic and osteoblastic activity inalveolar bone
To study osteoclastic and osteoblastic activities, weanalyzed 9 markers at mRNA level by q-PCR. Themarkers were grouped by function into 3 categories:
1. Osteoclast regulation markers
� M-CSF� OPG� RANKL
ril 2011 � Vol 139 � Issue 4 � Supplement 1 American
2. Osteoclast activity markers
� TRACP 5b� Cathepsin K (Ctsk)� Calcitonin receptor (CTR)
3. Osteoblast markers
� Osteopontin (OPN)� Bone sialoprotein (BSP)� Osteocalcin (OCN)
All reagents for the q-PCR analysis were fromApplied Biosystems, and plate assays were read on anABI 7700 Sequence Detector (Applied Biosystems,Foster City, Calif). One microgram of total RNA wasused for each preparation of cDNA. All cDNA prepara-tions were generated by random hexamer priming.External and internal primers for ß-actin, CTR, Ctsk,OCN, OPG, and RANKL were purchased from commer-cial sets available from Applied Biosystems Inc. Perti-nent sequence information and amplicon sizes foreach target gene are presented in Table II. In addition,we designed our own primers and probes for themarkers, which were not available at Applied Biosys-tems. These (BSP, M-CSF, OPN, and TRACP 5b) werepurchased from either Sigma-Aldrich or Invitrogen(Table III). Each plate contained 2 negative controlsand a positive control probe. The endogenous controlb-actin was used in all experimental samples for nor-malization and quantification of each target sequence.All samples were run in triplicate. The fractional cyclenumber at which the fluorescence passed the fixedthreshold (CT values) was used for quantification byusing a comparative CT method. Sample values werenormalized to the threshold value for b-actin (Actb)for each time point: DCT 5 X CT (exp) – X CT (Actb).The CT value for baseline (day 0) was used as a referencein the following formula: DDCT 5 X CT (exp) �X CT(control day 0). The fold change in mRNA expressionfor each time point was plotted in a graph using day0 as a reference: 2�DDCT (baseline at day 0) 5 1.
Journal of Orthodontics and Dentofacial Orthopedics

Table III. Primers custom-designed and used in this study
Gene Forward Sequence Reverse SequenceBSP TGACGCTGGAAAGTTGGAGTTAG GCCTTGCCCTCTGCATCTCM-CSF CCGACACAGGCTCTTCTATTCAG CAGCCAGCAAGACTAGGATGAOPN GGAGCGGTCGGATGCTATC TCGTGGCTCTGATGTTCCATRACP 5b TGCATGACGCCAATGACAA GAGGGCACGGTCAGAGAAC
Baloul et al S89
Statistical analysis
The data for both the control and experimentalgroups were presented as means. Two independent andblinded investigators at different time points evaluatedthe Faxitron data. MicroCT measurements were repeated3 times by the same investigator at different time points.The average of the 3 measurements was reported in thefinal results. q-PCR measurements were all done intriplicate, and all assays were repeated twice. The levelof significance was P \0.05 for all data analyzed.One-way analysis of variance (ANOVA) using the effectof time, treatment, and the interaction between timeand treatment was used. When applicable, a post hocleast significant difference (LSD) test was used to identifysignificant differences between themeans. As a nonpara-metric alternative to the 1-way independent samplesANOVA, a Kruskal-Wallis test was performed. We ob-served no differences between the 2 tests. Therefore,we elected, with a consultation with statisticians, to use1-way ANOVA for our study. SPSS 16.0.1 (SPSS Inc.,Chicago, Ill) software was used for all statistical analysis.
RESULTS
Magnitude and rate of tooth movement
The impact of alveolar decortication on tooth move-ment was initially assessed via Faxitron analysis. Twovariables were measured. First, we examined the amountof tooth movement that occurred in both the toothmovement (TM) and combined (SADc 1 TM) groups.Second, we calculated the rate of tooth movement inTM and SADc 1 TM. In terms of the amount of toothmovement, our results illustrated that the SADc 1 TMgroup showed a steady increase beginning from baselineup to 21 days. The amount of tooth movement washigher at 7 days in the SADc 1 TM group comparedwith the TM group (Fig 2, A; P 5 0.04). In contrast,the TM group demonstrated a fluctuation reflectingthe typical characteristics of tooth movement phases be-ginning with an initial displacement (seen as an increasebetween 7 and 14 days), followed by a lag phase (de-crease between 14 days to 28 days), and then a continu-ous tooth movement (increase between 28 days and 48days). TM and SADc 1 TM demonstrated similar tooth
American Journal of Orthodontics and Dentofacial Orthoped
movement displacement (amount of movement andrate) between 28 and 42 days. Rate of tooth movementillustrated an early, sharp increase in the SADc 1 TMgroup compared with the TM group for the first 7days. This was significantly higher compared with theTM group (Fig 2, B; P 5 0.04). The TM group showeda similar sharp increase 7 days later (at 14 days) com-pared with the SADc1 TM group. Alveolar decorticationappears to keep the rate of tooth movement at a highsteady level during the initial force application for partof tooth movement. The TM group showed a dramaticdecrease in tooth movement rate by 21 days. The effectof alveolar decortication on tooth movement seems todiminish by 28 days; SADc 1 TM and TM groups hada similar tooth movement rate between day 28 andend of therapy at 42 days (Fig 2, D).
Structural changes in alveolar bone
In order to determine how alveolar decortication af-fects the bone during tooth movement, we next exam-ined the overall bone structure and mineral content byMicroCT. Representative MicroCT images of the first mo-lar and surrounding area are shown in Figure 3. The bonevolume, which is defined as total volume of voxels abovea density threshold, was found to be significantly de-creased (�62%) in the combined group by 14 days com-pared with the baseline, (P 5 0.016), but BV wasincreased to higher levels than baseline by 42 days(130%). In comparison, the TM group demonstrateda significant decrease (�65 %) by 21 days, 1 week afterthe SADc1 TM group (P5 0.013), and restored to levelsclose to baseline (16%) by 42 days. Selective alveolar de-cortication by itself resulted in no effect on BV until 21days (133% bone formation). Overall, there were nosignificant differences between the TM and SADc 1TM groups at any given time point regarding the BV(Fig 4, A). The SADc group showed no significantchanges in BV. In addition, MicroCT analysis showedthat SADc 1 TM resulted in a proportional and signifi-cant reduction in the overall ratio of bone volume–to–total volume (BV/TV) 7 days after treatment (�55%;P 5 0.010 vs baseline) and at 14 days (�44%; P 50.039). BV/TV was restored to baseline levels by 28days in the SADc1 TM group (18%). Tooth movement
ics April 2011 � Vol 139 � Issue 4 � Supplement 1

Fig 3. Representative MicroCT images of first molar and surrounding area in ROI. Images were ob-tained from baseline, SADc, TM, and SADc 1 TM groups during 14 days and at end of active toothmovement phase at 42 days. Top row images represent teeth from buccal side. Middle row imagesrepresent teeth from occlusal surface. Reconstructed images (bottom row) were cut at CEJ level toshow bone between 5 roots of maxillary first molar. Yellow arrows indicate space created between firstand second molars as seen in buccal and occlusal views. Yellow arrows in CEJ view depict bonechanges around roots of first molar.
S90 Baloul et al
alone demonstrated a decrease in BV/TV as well, but thechange was not statistically significant compared withthe baseline. The difference between the SADc 1 TM(�55%) and TM (�18%) groups showed a strong trendtoward statistical significance at 7 days (P 5 0.075).While there was a decrease in the BV/TV in the SADcgroup, the difference was not statistically significantcompared with the baseline. Interestingly, the SADcgroup showed a significant increase in BV/TV betweenday 28 (119%) and day 42 (122%; P5 0.045) (Fig 4,B).
To examine the mineralization associated with alve-olar decortication combined with tooth movement, weanalyzed bone mineral content (BMC) and bone mineraldensity (BMD). In terms of bone mass (BMC), the
April 2011 � Vol 139 � Issue 4 � Supplement 1 American
combined group demonstrated a decrease starting at 7days (�49%; P 5 0.056). This decrease was statisticallysignificant by 14 days (�63%; P 5 0.015) and restoredto levels greater than baseline (day 0) at 42 days (122%).Tooth movement alone exhibited a significant decreasecompared with baseline in BMC at a later stage, 21days, (�64%; P 5 0.015). The BMC was restored tolevels close to baseline by the end of the study at 42days (19%). SADc by itself did not affect the BMC whilean increase was observed at 42 days (145%) comparedwith SADc at 7 days (�6%; P 5 0.049) (Fig 4, C).
In terms of BMD, there were no statistical significantchanges among the 3 procedures at any time point. TheBMD fluctuated in response to TM and SADc1 TM, but
Journal of Orthodontics and Dentofacial Orthopedics

Fig 4. Graphic presentation of bone volume, bone volume fraction, bonemineral content and bonemineraldensity as measured by MicroCT for SADc, TM, and SADc1 TM during active tooth movement phase.
Baloul et al S91
no statistically significant changes were observed. In re-sponse to SADc alone, BMD showed a gradual increase,which reached its maximum level at 28 days (19.1%).This increase was significant when compared with 7days (�0.96%, P 5 0.012), 14 days (11.45%, P 50.008), and 21 days (13.61%, P 5 0.005) (Fig 4, D).
Molecular mechanism of osteoclastogenesis
Since selective alveolar decortication results in signif-icant therapeutically induced osteopenia16 and ourMicroCT results further confirmed that this may be themechanism in rapid tooth movement, we examined themRNA expression of the major molecules that regulatedosteoclastogenesis. M-CSF is essential for osteoclastdevelopment and regulation. Its expression increasedat 3 days in the SADc1 TM group, suggesting the pres-ence of mature osteoclasts at an early stage of SADc 1TM compared with TM alone (P 5 0.005 vs baseline).
American Journal of Orthodontics and Dentofacial Orthoped
At 14 days, the SADc 1 TM group showed a further in-crease in M-CSF expression compared with the baseline(P 5 0.001) (Fig 5, A).
RANKL is important for osteoclastogenesis; it is pres-ent during osteoclast differentiation and activity in re-sorbing bone. The SADc 1 TM group demonstrated anincreased expression of RANKL at 7 days (P 5 0.000),14 days (P 5 0.000), 21 days (P 5 0.000), and 28 days(P 5 0.00) compared with the baseline. At 28 days, theSADc1 TM group showed significant increased levels ofRANKL when compared with the TM (P 5 0.006) andSADc (P5 0.030) groups. Similarly, the TM group showedan increased expression of RANKL at 7 days (P5 0.000),14 days (P 5 0.000), 21 days (P 5 0.000), and 28 days(P 5 0.010) compared with baseline (Fig 5, B).
The temporal expression of OPG, a molecule that in-hibits osteoclast differentiation, was increased in theSADc 1 TM group during the initial 3 days (P 5 0.000).Increased expression of OPG in the SADc 1 TM group
ics April 2011 � Vol 139 � Issue 4 � Supplement 1

Fig 5. Graphic presentation of amount of relative mRNA expression levels during osteoclast regula-tion; markers studied: M-CSF, OPG, and RANKL. Levels obtained from q-PCR analysis over timecourse of active tooth movement phase for SADc, TM, and SADc1 TM. Fold change is presented rel-ative to control bone (day 0). Data presented as mean values.
S92 Baloul et al
continued to 14 days (P 5 0.000 vs baseline: day 0). Adecrease in OPG expression in the SADc 1 TM groupwas observed thereafter until the end of treatment at 42days (P 5 0.001). In contrast, TM showed a decrease inOPG expression at 3 days (P 5 0.005 vs baseline: day 0).This decrease was significant in comparison with theSADc1 TM group (P5 0.000). In addition, the TMgroupshowed an increase in OPG expression between 3 and 14days, but this was not statistically significant. However,at 21 days, the TM group demonstrated a decrease in OPGexpression (P 5 0.001 compared with the SADc 1 TM).SADc alone did not exhibit a change until 21(P 5 0.016) and 28 (P 5 0.044) days when a decreasein OPG expression was observed. OPG expression in re-sponse to SADc returned to baseline (day 0) levels by
April 2011 � Vol 139 � Issue 4 � Supplement 1 American
42 days when SADc showed statistically significanthigher levels of OPG expression compared with both TM(P 5 0.006) and SADc1 TM (P 5 0.001) (Fig 5, C).
To further study osteoclast differentiation in re-sponse to selective alveolar decortication-facilitatedtooth movement, we analyzed CTR expression. The com-bined group exhibited the highest expression at 3 days(P 5 0.000). This was significantly higher than SADcat 3 days (P 5 0.012). In the combined group, CTR ex-pression decreased at 7 days (P 5 0.001 vs 3 days) andincreased at 14 days (P 5 0.000 vs baseline: day 0). At14 days, SADc 1 TM was the highest compared withTM (P 5 0.027) and SADc (P 5 0.000). The SADc 1TM group showed a decrease at 21 days (P 5 0.021 vs14 days), an increase at 28 days (P 5 0.000 vs baseline
Journal of Orthodontics and Dentofacial Orthopedics
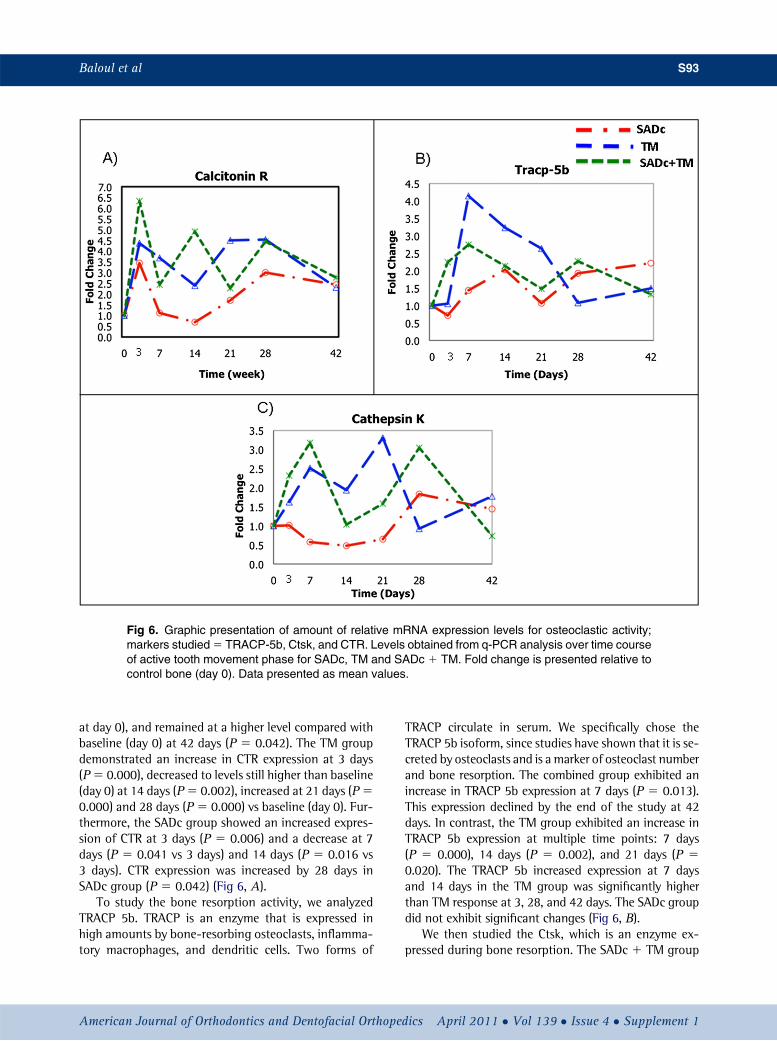
Fig 6. Graphic presentation of amount of relative mRNA expression levels for osteoclastic activity;markers studied5 TRACP-5b, Ctsk, and CTR. Levels obtained from q-PCR analysis over time courseof active tooth movement phase for SADc, TM and SADc 1 TM. Fold change is presented relative tocontrol bone (day 0). Data presented as mean values.
Baloul et al S93
at day 0), and remained at a higher level compared withbaseline (day 0) at 42 days (P 5 0.042). The TM groupdemonstrated an increase in CTR expression at 3 days(P5 0.000), decreased to levels still higher than baseline(day 0) at 14 days (P5 0.002), increased at 21 days (P50.000) and 28 days (P5 0.000) vs baseline (day 0). Fur-thermore, the SADc group showed an increased expres-sion of CTR at 3 days (P 5 0.006) and a decrease at 7days (P 5 0.041 vs 3 days) and 14 days (P 5 0.016 vs3 days). CTR expression was increased by 28 days inSADc group (P 5 0.042) (Fig 6, A).
To study the bone resorption activity, we analyzedTRACP 5b. TRACP is an enzyme that is expressed inhigh amounts by bone-resorbing osteoclasts, inflamma-tory macrophages, and dendritic cells. Two forms of
American Journal of Orthodontics and Dentofacial Orthoped
TRACP circulate in serum. We specifically chose theTRACP 5b isoform, since studies have shown that it is se-creted by osteoclasts and is a marker of osteoclast numberand bone resorption. The combined group exhibited anincrease in TRACP 5b expression at 7 days (P 5 0.013).This expression declined by the end of the study at 42days. In contrast, the TM group exhibited an increase inTRACP 5b expression at multiple time points: 7 days(P 5 0.000), 14 days (P 5 0.002), and 21 days (P 50.020). The TRACP 5b increased expression at 7 daysand 14 days in the TM group was significantly higherthan TM response at 3, 28, and 42 days. The SADc groupdid not exhibit significant changes (Fig 6, B).
We then studied the Ctsk, which is an enzyme ex-pressed during bone resorption. The SADc 1 TM group
ics April 2011 � Vol 139 � Issue 4 � Supplement 1

S94 Baloul et al
showed a higher and early upregulation of Ctsk startingat 7 days (P 5 0.010 vs baseline). A decrease was thenobserved at 14 days (P 5 0.010). This was followed byan increase in expression at 28 days (P 5 0.002). TheSADc 1 TM group demonstrated a higher Ctsk expres-sion at 28 days (P5 0.011 vs TM group) and the expres-sion went back to baseline by 42 days. In contrast, theTM group showed an upregulation in Ctsk expressionstarting at 7 days (P 5 0.017), reached its highest at21 days (P 5 0.000), and returned to baseline at 42days. The SADc group did not exhibit significant changes(Fig 6, C).
Molecular mechanisms of osteogenesis
Since previous work16 has suggested that the cortico-tomy results in an expedited coupling and remodeling ofthe bone, and limited clinical evidence has implied thatthe resorptive changes in alveolar bone have been rapidlyreversed by bone apposition.13 we wanted to study theosteoblastic activity in parallel to the osteoclastic activ-ity. MicroCT assessment supported the notion that thiscould be the case in SADc 1 TM. Therefore, to betterunderstand how the osteoblastic activity is affected inresponse to alveolar decortication with or without toothmovement, we analyzed 3 osteoblastic markers: OPN,BSP, and OCN
To study the early osteoblastic activity, we analyzedOPN. The combined group demonstrated the highestOPN expression at both 7 days (P 5 0.000) and 14days (P5 0.000) vs baseline. At 21 days, OPN expressionin the SADc 1 TM group decreased to close to baselinelevels (P5 0.001 vs 14 days). In contrast, the TM groupdemonstrated an increase in OPN at 7 days (P5 0.007).The TM group exhibited a decrease by 14 days andstayed at levels close to baseline until the end of thestudy at 42 days. Similar to the SADc 1 TM group, theSADc group showed an increased OPN at 7 days (P 50.010 vs baseline at day 0). This expression decreasedat 14 days (P5 0.046 vs 7 days) with no further changeobserved in the SADc group (Fig 7, A).
To study the intermediate osteoblastic activity asso-ciated with alveolar decortication in relation to ortho-dontic movement, we analyzed BSP expression. TheSADc 1 TM group demonstrated the highest increasein BSP expression at 14 days (P 5 0.000 vs baseline atday 0). This increase was statistically significant whencompared with TM group at 14 days (P 5 0.000). How-ever, the TM group showed an increase in BSP expres-sion at 21 days (P 5 0.000). That was statisticallysignificant compared with both SADc (P 5 0.022) andCTM (P 5 0.023) groups. The BSP expression in theTM group then decreased at 28 days (P 5 0.019 vs 21
April 2011 � Vol 139 � Issue 4 � Supplement 1 American
days). At 42 days, BSP expression was increased in theTM group (P 5 0.000 vs baseline at day 0). The SADcgroup did not show any significant changes in BSPexpression (Fig 7, B).
Finally, to study the late osteoblastic activity in re-sponse to alveolar decortication combined with ortho-dontic tooth movement, we analyzed OCN expression.At 14 days, both the TM (P 5 0.033) and SADc 1 TM(P 5 0.009) groups exhibited the highest expressioncompared with the baseline and decreased to the base-line levels for the rest of the study. Additionally, theSADc group demonstrated an increase in OCN at 21days (P 5 0.001 vs baseline at day 0); this was statisti-cally significant compared with both TM (P 5 0.029)and CTM (P 5 0.006). The SADc group then showeda decline in OCN expression at 28 days (P 5 0.014 vs21 days) and throughout the rest of the study (Fig 7, C).
DISCUSSION
Selective alveolar decortication induces a localizedincrease in turnover of alveolar spongiosa,16 suggestingthat the dramatic acceleration of demineralization andremineralization dynamics could be the mechanism un-derlying the rapid tooth movement after selective alveo-lar decortication observed in clinical reports.13 Based onthis evidence,therefore, we hypothesized that the selec-tive alveolar decortication–induced osteoclastogenesisand bone remodeling underlie the orthodontic toothmovement, and selective alveolar decortication en-hances the rate of tooth movement by increasing thebone turnover compared with the conventional toothmovement. In order to test this hypothesis, we used mor-phologic analysis, quantitative MicroCT for the struc-tural analysis, and q-PCR to analyze mRNA expressionof genes associated with both osteoclasts and osteo-blasts. Three groups were formed to investigate theresponse of alveolar bone in an experimental animalmodel: SADc alone, TM, and the combination of SADcand tooth movement (SADc 1 TM). The results sug-gested that the combined treatment group had an in-creased amount and rate of tooth movement and therewas significant reduction in bone volume and increasedosteoclastic and osteoblastic activity during the earlyhealing process, denoting a coupled bone remodelingresponse after alveolar decortication. These data furthersuggest that the coupling mechanism at an earlier timepoint can be induced by alveolar decortication withoutany pathologic consequences in alveolar bone and thatthis mechanism underlies the rapid orthodontic toothmovement phenomenon.
The migration of the teeth via orthodontic applianceshas been traditionally described as “a process in which
Journal of Orthodontics and Dentofacial Orthopedics

Fig 7. Graphic presentation of amount of relative mRNA expression levels for osteoblastic markers:OPG, BSP, and OCN. Levels obtained from q-PCR analysis over time course of active tooth movementphase for SADc, TM, and SADc1 TM. Fold change is presented relative to control bone (day 0). Datapresented as mean values.
Baloul et al S95
the application of a mechanical force induces alveolarbone resorption on the pressure side and alveolar bonedeposition on the tension side.”19 This descriptionsuggests that the mechanical force results in several dif-ferent events around the tooth that is being moved. Theresorption of the bone is accompanied by the appositionof the bone under controlled mechanical forces, wherethe tooth movement does not exceed the physiologicthreshold that the PDL fibers could withstand. Thisparadigm has dominated the understanding of themechanism of orthodontic toothmovement.More recentstudies suggest that the resorption and apposition arenot strictly sequential or independent events; they are
American Journal of Orthodontics and Dentofacial Orthoped
rather connected with each other and overlap in their ac-tion.20 This phenomenon is referred to as “coupling” andsuggests that the resorptive changes in the bone are ac-companied by the formation process in healthy tissues.21
Osteoclasts are actively involved in the osteoblastic func-tion, and the bone represents a dynamic environment.22
Since the clinical orthodontic treatment can take consid-erable time, numerous efforts have been made toenhance the rate of therapy. Increasing the magnitudeof mechanical forces and exceeding the biologic thresh-old of the tissue capacity to physiologically respond toincreased forces leads to pathologic responses such asankylosis, root resorption and hyalinization.23,24 and
ics April 2011 � Vol 139 � Issue 4 � Supplement 1

S96 Baloul et al
cessation of the tooth movement.25 Therefore, the ratio-nale for “speeding” the orthodontic tooth movementwithout increasing the force application should be basedon accelerating the turnover rate of the alveolar bone.26
A recent study has confirmed that the basic mechanismunderlying the selective alveolar decortication was thecoupling between osteoblasts and osteoclasts initiatedat the same time window after the mechanical injury.16
This work further suggested that the orthodontic toothmovement enhancement could be due to rapid turnoverof the alveolar bone when osteoclastic activity can be ini-tiated earlier. It was not clear however, if the toothmove-ment in response to surgical decortication followed thesame pattern as the conventional tooth movement ina similar sequence of phases or if different biologic path-ways were followed. The findings from the current workdemonstrate that the tooth displacement curve of themaxillary left first molar was similar to the classic toothdisplacement curve first described in response to conven-tional tooth movement.27 There was a decrease in BVduring the initial 7 days. This decrease, however, wasnot sufficient to cause any initial displacement butshould be referred as the “initial phase.” During this pe-riod, the combined group demonstrated an early “initialmovement.” MicroCT analysis of the bone volume sug-gested that the combined group, in contrast to TM,showed the most significant decrease in 7 days, corre-sponding to the initial movement observed. Thus, thecomparison of the combined group to the TMgroup sug-gested that the remodeling phase was earlier; a primarycatabolic phase in bone healing was observed ata much higher level and RAP28 occurred during thebone remodeling in association with alveolar bonedecortication. After the first week, the initial toothmove-ment occurred by 14 days in the TM group, with a de-creased activity over the next 7 days. On the otherhand, alveolar decortication results in continuity of thetooth movement that had been initiated earlier over 14days. This observation was supported by further reduc-tion in bone volume, suggesting that the bone resorptioncontinued. The lag phase in traditional tooth movementhas been associated with hyalinization in the PDL.Pressure associated with orthodontic forces on the PDLresults in permanent damage and plays a major role asa rate-limiting factor in orthodontic tooth movement.25
In our study, a lag phase after the initial displacementphase was found in conventional tooth movementgroup, which occurred between 14 and 21 days. On theother hand, the SADc1 TM group showed a continuousand steady movement without any evidence of a lagphase. The increase in toothmovement is possibly a resultof the alveolar decortication effect on tooth movement,as it was suggested that selective alveolar decortication
April 2011 � Vol 139 � Issue 4 � Supplement 1 American
led to rapid alveolar bone reaction and it might havebeen due to less hyalinization of the PDL on the alveolarwall.29 Thus, the mechanism of this technique was to“bypass” the lag phase and initiate the tooth movementearlier in comparison with the traditional tooth move-ment group and, therefore, eliminate the hyalinizationassociated with the lag phase early on.
In order to characterize the kinetics of tooth move-ment and bone response, we used several methods: Faxi-tron analysis as detailed above provided information on2D changes in spatial displacement of the teeth using ra-diographic techniques.30 Further morphologic evidenceregarding the density, mass, and bone in 3D wasobtained by MicroCT analysis.31 Indeed, this is the firststudy where these 2 techniques have been used in com-bination with other methods to assess bone structureand its mineralization during alveolar bone healingassociated with orthodontic treatment with or withoutSADc. Thus, we were able to characterize the changesin bone over time. The results suggested a significant re-duction in bone volume in response to the combinationof tooth movement, and selective alveolar decorticationsupports the notion that such an impact would result ina rapid loss of bone volume. Another important findingusing the MicroCT analysis was the observation that thebone homeostasis was restored to baseline levels with nopathologic loss of bone density, mass, and volume. Thetooth movement phase can be interpreted as a period inwhich the biologic processes involving remodeling of thePDL and alveolar bone reach their maximum.32 At thisstage, hyalinization has been eliminated and boneremodeling occurs by direct and undermining boneresorption. The total tooth displacement during ourstudy was 6.94 mm in the combined group comparedwith 5.30 mm in the traditional tooth movement group.This greater orthodontic tooth movement has been re-ported to occur in alveolar bone with loose trabeculaeand less bone resistance.33 During the tooth displace-ment phase (28 to 42 days), the combined treatmentgroup showed an increase in the mineralized bonevolume and increased bone mass, with simultaneousloss in BV and BMD. This denotes that the surgical inter-vention led to an increase in bone mineral volume andbone mineral mass. Using these qualitative assessmentsof change in alveolar bone and based on a previous re-port.6 We suggest that the coupling initiated by osteo-clastic bone resorption and accompanied byosteoblastic bone deposition is the underlying mecha-nism for rapid orthodontic tooth movement.
Characteristic changes of reversible osteopenia wereassociated with alveolar decortication in previous stud-ies.34,35 Therefore, to further elucidate the mechanismby which the alveolar decortication affects the bone
Journal of Orthodontics and Dentofacial Orthopedics

Baloul et al S97
healing during orthodontic tooth movement, molecularanalyses of osteoclastic and osteoblastic markers werecarried out. To this end, we first studied the expressionof macrophage-colony stimulating factor (M-CSF),which stimulates osteoclastic proliferation and differen-tiation and decreases osteoclast apoptosis.36 TheSADc 1 TM group displayed an initial increase in M-CSF expression at 3 days and another peak at 14 days.These levels were significantly different from the TMgroup, suggesting that the combination of surgical in-jury to the bone and mechanistic forces can lead to in-creased osteoclast proliferation and differentiation.
In order to elucidate if the alveolar decortication-mediated increase in the expression of cytokines was as-sociated with osteoclast differentiation and regulation,we then studied RANKL and OPG , which are known toregulate osteoclast differentiation and survival. RANKLis a member of the tumor necrosis factor (TNF) super-family and a membrane-residing protein on osteoblastsand their precursors, which recognize its receptor RANKonmarrowmacrophages, promoting them to assume theosteoclast phenotype.37 In addition to increasing osteo-clastogenesis by inducing osteoclast differentiation,RANKL activates osteoclasts.38 Data from our studyshowed that RANKL expression was elevated in responseto both the combined and traditional tooth movementmodalities beginning at 7 days. The combined group ex-hibited a steady increase in RANKL expression during the14 and 21 days compared with baseline (day 0), while theTM group demonstrated a peak at 14 days and a declinethereafter. This data further suggested that the increasedosteoclastic proliferation and differentiation were trans-lated into prolonged osteoclastic activity in the SADc 1TM group.
Next, we evaluated the expression for OPG, which isa soluble decoy receptor antagonist to RANK.39 Bybinding to RANKL, OPG inhibits osteoclast differentia-tion.40 OPG expression in the combined group peakedat 3 days and 14 days, suggesting a bimodal response.On the other hand, the TM group showed a decrease ofOPG expression at 3 days. These findings suggestedthat selective alveolar decortication diverts the biologicresponse to conventional tooth movement, and thecombination approach represents a unique pattern ofchallenge to the alveolar bone in which the couplingof RANKL and OPG is more rapid and simultaneouscompared with conventional tooth movement, wherean increase in RANKL was associated with decreasedOPG.
Calcitonin has an inhibitory effect on the osteoclastactivity and decreases bone resorption via theCTR.41 Several studies have recognized calcitonin asa therapeutic agent for the treatment of osteoporosis,
American Journal of Orthodontics and Dentofacial Orthoped
Paget’s disease and late-stage malignancies.36 Calcito-nin receptor is a G-protein coupled receptor present onthe osteoclasts and is a specific marker of osteoclastdifferentiation. While all treatment groups showeda significant increase in CTR compared with baseline,the SADc 1 TM group exhibited the highest expression.At 7 days, all 3 groups showed a decrease reflectingincreased osteoclastogenesis and bone resorption. TheSADc 1 TM group returned to higher levels by 14days, whereas the TM group levels decreased and theSADc group stayed at low levels. This observation wasin parallel with the fluctuating pattern observed in theMicroCT analysis and illustrates that the bone healingin the combined therapy is following a unique patternindependent of TM.
TRACP-5b has been used as a potential marker toevaluate osteoclastic activity and bone resorptionrate.42 It is secreted by osteoclasts during boneresorption.43 Studies showed that TRACP-5b was signif-icantly elevated in osteoporotic patients.44 In addition,TRACP-5b has been shown to have a significant negativecorrelation with BMD. TRACP-5b demonstrated activitythroughout our study. The combined group exhibited anosteoclastic activity at 3 days, 7 days, and 14 days, whichwas in parallel with the bone changes seen in MicroCTanalyses. Conventional toothmovement displayed a sim-ilar pattern. However, active osteoclastic activity in TMwas seen later than the SADc 1 TM group at 7 daysand 14 days, suggesting that the active bone resorptionfacilitated the earlier tooth movement in the SADc1 TMgroup.
The final marker of osteoclastic activity tested in thisstudy was Ctsk, which is predominantly expressed inosteoclasts and is a major bone extracellular bone-degrading enzyme. Ctsk represents 98% of the totalcysteine protease activity and of the collagenases ofthe matrix metalloproteinase (MMP) family.45,46 Thecombined group demonstrated high mRNA expression ofCtsk at 3 days and 7 days, indicating a high osteoclasticactivity allowing the tooth to move more rapidly. Ctskactivity decreased in the SADc 1 TM group by 14 days.The conventional tooth movement group followeda similar pattern at 3 and 7 days, while the expression at3 days was not as high as seen in the SADc1 TM group,which may explain the delay in initial toothdisplacement. Overall, the analyses of different markersof osteoclastic activity, proliferation, and differentiationdemonstrated that the osteopenic changes were inducedby selective alveolar decortication and that this impactaccounted for the rapid tooth movement. Anotherimportant finding was that the combination of surgicaldecortication injury to the alveolar bone and orthodonticforces represents a unique healing model, compared
ics April 2011 � Vol 139 � Issue 4 � Supplement 1

S98 Baloul et al
with the individual responses to these stimuli, rather thanan additive effect.
RANKL expression was decreased in both the SADc1TM and TM groups, denoting a decrease in osteoclasticactivity during the linear tooth displacement period. Inthe combined group, RANKL expression showed a de-crease during the period of 28 to 42 days. The TM groupdemonstrated a similar pattern in its lag phase between21 and 42 days. Both groups, therefore, exhibited a de-crease in osteoclast differentiation and activation duringthe tooth movement phase. The combined group re-turned to levels close to baseline, while the TM grouphad a higher expression than baseline by the end ofthe study at 42 days. Both SADc1 TM and TM exhibiteda similar pattern in OPG expression, with SADc 1 TMshowing a decreased expression at 42 days. Calcitoninreceptor data demonstrated that during the linear toothmovement, all treatment modalities led to a decreasebetween 28 and 42 days. Interestingly, the peak inCTR expression at 28 days in the SADc group paralleledthe increase seen in MicroCT parameters (BV, BV/TV,BMC, and BMD). Since CTR expression is associatedwith osteoclast formation.47 The peak activity between28 and 42 days may suggest apoptotic changes inosteoclasts and inhibition of further bone resorption.Furthermore, this signifies that alveolar decorticationalone leads to increased bone formation in the laterstages of alveolar bone healing.
Since orthodontic tooth movement is the result of anextrinsic mechanical stimulus, which aims to restore thebalance by remodeling the PDL, it is of interest to assessthe timing of the bone apposition in conjunction withthe resorption of the alveolar bone around the tooth.An increase in both catabolic and anabolic activitieshas been reported, suggesting coupled alveolar turnoverin response to selective alveolar decortication.16 There-fore, in order to explore the anabolic mechanism inresponse to tooth movement with or without alveolardecortication, it was prudent to assay osteoblasticmarkers. We began our investigation with OPN as anearly osteoblastic activity marker. OPN is a secretedphosphoprotein rich in sialic acid. It is a prominentconstituent of the extracellular matrices of mineralizedtissues such as bone and cementum.48 OPN has multipleroles in various tissues such as bone, kidney, heart,and immune tissue49,50; it is produced by oncogeniccells regardless of their origin in substantial amounts incomparison with their nontransformed cell counterparts.51
Sodek et al52 reported high levels of OPNmRNA expressionfound in mature osteoblasts at sites of bone remodeling.Our results demonstrated that the SADc 1 TM resultedin a robust increase in OPN expression at 3, 7, and 14days, while the TM group displayed an increase in OPN
April 2011 � Vol 139 � Issue 4 � Supplement 1 American
expression at significantly lower levels. The SADc groupshowed a peak in OPN expression at 3 and 7 days, andthe osteoblastic activity soon returned to baseline levelsby 14 days. The data suggested that osteoblast matura-tion was complete in response to alveolar decortications,while the increased osteoclastic activity was coupledwithhigher osteoblastic activity in the SADc 1 TM group.
In order to assess the changes in an intermediate os-teoblastic marker, we then studied BSP, another noncol-lagenous matrix protein. Similar to OPN, BSP containsa classic integrin-binding motif (RGD) for cell attach-ment.53 Its expression is restricted to mineralized con-nective tissues, and it is first expressed at the onset ofbone, cementum, and dentin formation.54 BSP has animportant role in nucleation of hydroxyapatite at themineralization front of bone.55 In addition, the expres-sion of BSP has been reported in breast, thyroid, andprostate cancers that metastasize to bone.56 Similar toOPN, we found a significant increase in BSP expressionin the SADc 1 TM group at 14 days. This was signifi-cantly different in comparison with both the traditionalTM group and the SADc group. A later peak wasobserved in the TM group at 21 days, suggesting thatthe early increase in BSP in the SADc 1 TM group ledto earlier osteoblastic activity. These data, combinedwith an earlier OPN expression increase suggests thatthe bone turnover was steady in SADc 1 TM.
To study late osteoblastic activity, we analyzed OCN,another noncollagenous protein secreted by osteoblasts,which plays an important role during the mineralizationstage and is known as a marker for mature osteoblasts.57
Our data showed an increased peak in OCN at 14 days inboth the combined and the TM groups. Therefore, bothtreatment modalities exhibited a simultaneous high rateof turnover along with initial tooth movement. Overall,these observations suggested that the selective alveolardecortication–induced osteoclastic activity is a continu-ous stimulation of osteoblast proliferation and matura-tion, and anabolic activity is directed by the catabolicresorption of the alveolar bone during orthodontic toothmovement.
The rat is considered suitable for an animal model oforthodontic tooth movement because the rat mouth islarge enough to perform surgery and place orthodonticwires.58,59 However, there are morphologic andphysiologic differences between rat and humanalveolar bone. The alveolar bone in rats is denser andexhibits no osteons. Its bone plates are void of marrowspaces. Humans have more osteoid tissue along thealveolar bone surfaces.60 Some reports showed that ratextracellular matrix has less acid mucopolysaccharides,and calcium homeostasis is controlled by the kidneysrather than in the bone. In addition, tissue development
Journal of Orthodontics and Dentofacial Orthopedics

Baloul et al S99
during tooth formation, as related to orthodontic treat-ment, appears to be faster in rats compared with hu-mans. Another limitation is the natural distal drift ofrat teeth.58 This may have led to an underestimationof the mesial molar displacement. A limitation in ourstudy design using the rat as a model was the tippingtooth movement. Tipping takes place by means of un-even distribution of stresses and strains occurring withinthe PDL. This results clinically in different rates of move-ment in both the crown and root of the tooth, leading tomovement in different directions. According to Fortin,61
the rate of crown and root movement is determined bythe center of rotation, and this is difficult to change dur-ing the tipping movement. Consequently, tipping move-ment is not a well-defined reproducible action.Measurements of the mesial molar displacement usingthe Faxitron x-ray system were performed at the crownlevel rather than the center of rotation. Therefore, thismay have caused an overestimation of our tooth dis-placement measurements. However, we performed thesame type of measurements with all samples and groupsso that the relative movements are comparable. Mean-while, in order to eliminate the shortcoming of thelack of tooth movement reactivation throughout thestudy period in our study design, we used ultralightsuperelastic NiTi closed coil spring with eyelets produc-ing a force of 25 g, which was attached to a ligature wireon the maxillary left first molar and the anterior teeth.These springs produced a constant, continuous, recipro-cal force on the anchorage teeth over a wider range ofactivation.23 Therefore, reactivation was not required.However, we still made sure that the force was constantduring the activation period by measuring with a gauge.The key point in this technique was not to violate the ac-tive range of action, which was 1 cm. This distance wasseveralfold larger than the distance between the molarand the incisor.
CONCLUSIONS
Collectively, the results demonstrate that toothmove-ment with or without alveolar decortication is a coupledprocess in which there is bone resorption followed by for-mation during bone turnover. This was demonstrated bymeans of radiographic, tomographic, and molecularmethods. The early rapid tooth movement observed inthe combined group during the initial phase of tooth dis-placement is due to the increased bone remodeling asa result of the surgical intervention. The results supportthe notion that surgically facilitated tooth movement isa process of demineralization-remineralization andsuggest that selective alveolar decortication induces a lo-calized increased turnover of alveolar spongiosa and that
American Journal of Orthodontics and Dentofacial Orthoped
demineralization-remineralization is the likely biologicmechanism underlying rapid toothmovement associatedwith selective alveolar decortication.
This study provides the first scientific evidence for therole of coupled osteoclastic and osteoblastic activity inresponse to alveolar decortication through which the or-thodontic tooth movement is enhanced. While the surgi-cal intervention during the orthodontic treatment maynot always be desired, understanding the biologic mech-anism underlying the bone turnover and the change indynamics of tooth movement as a result of the increasedbone activity are critical for designing novel treatmentmethods in the future. Therefore, the knowledge gainedfrom the current study would be useful when mechanicsare combined with biologic processes during orthodon-tic treatment.
The authors would like to acknowledge the followingmembers for their contribution to the study: Dr. TareqAl-Zeitani, Dr. Chie Hayashi, Dr. Donald Ferguson,Dr. Manish Bais, Dr. Leslie Will, and Mr. Zack Mason.
REFERENCES
1. Parfitt AM. The cellular basis of bone remodeling: the quantumconcept reexamined in light of recent advances in the cell biologyof bone. Calcified Tissue Int 1984;36:S37-45.
2. Krishnan V, Davidovitch Z. Cellular, molecular, and tissue-level re-actions to orthodontic force. Am J Orthod Dentofacial Orthop2006;129:469.e1-32.
3. de Carlos F, Cobo J, Perillan C, Garcia MA, et al. Orthodontic toothmovement afterdifferent coxib therapies. Eur JOrthod2007;29:596-9.
4. Wise GE, King GJ. Mechanisms of tooth eruption and orthodontictooth movement. J Dent Res 2008;87:414-34.
5. Kawarizadeh A, Bourauel C, Zhang D, Gotz W, Jager A. Correlationof stress and strain profiles and the distribution of osteoclastic cellsinduced by orthodontic loading in rat. Eur J Oral Sci 2004;112:140-7.
6. Alhashimi N, Frithiof L, Brudvik P, Bakhiet M. Orthodontic toothmovement and de novo synthesis of proinflammatory cytokines.Am J Orthod Dentofac Orthoped 2001;119:307-12.
7. Lee YH, Nahm DS, Jung YK, et al. Differential gene expression ofperiodontal ligament cells after loading of static compressive force.J Periodontol 2007;78:446-52.
8. Kanzaki H, Chiba M, Shimizu Y, Mitani H. Periodontal ligamentcells under mechanical stress induce osteoclastogenesis by re-ceptor activator of nuclear factor kappaB ligand up-regulationvia prostaglandin E2 synthesis. J Bone Miner Res 2002;17:210-20.
9. K€ole H. Surgical operations on the alveolar ridge to correct occlusalabnormalities. Oral Surg Med Pathol 1959;12:515-29.
10. Duker J. Experimental animal research into segmental alveolarmovement after corticotomy. J Maxillofac Surg 1975;3:81-4.
11. Anholm JM, Crites DA, Hoff R, Rathbun WE. Corticotomy-facili-tated orthodontics. CDA J 1986;14:7-11.
12. Amimoto A, Iwamoto S, Taura Y, Nakama S, Yamanouchi T. Effectsof surgical orthodontic treatment for malalignment due to theprolonged retention of deciduous canines in young dogs. J VetMed Sci 1993;55:73-9.
ics April 2011 � Vol 139 � Issue 4 � Supplement 1

S100 Baloul et al
13. Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodon-tics with alveolar reshaping: two case reports of decrowding. Int JPeriodontics Restorative Dent 2001;21:9-19.
14. Murphy KG, Wilcko MT, Wilcko WM, Ferguson DJ. Periodontal ac-celerated osteogenic orthodontics: a description of the surgicaltechnique. J Oral Maxillofac Surg 2009;67:2160-6.
15. Yaffe A, Fine N, Binderman I. Regional accelerated phenomenon inthe mandible following mucoperiosteal flap surgery. J Periodontol1994;65:79-83.
16. Sebaoun JD, Kantarci A, Turner JW, Carvalho RS, Van Dyke TE,Ferguson DJ. Modeling of trabecular bone and lamina dura fol-lowing selective alveolar decortication in rats. J Periodontol2008;79:1679-88.
17. Verna C, Zaffe D, Siciliani G. Histomorphometric study of bone re-actions during orthodontic tooth movement in rats. Bone 1999;24:371-9.
18. Otsu N. A threshold selection method from gray-scale histogram.IEEE Trans Syst Man Cybernet 1978;8:62-6.
19. Graber T, Vanarsdall RL. Orthodontics: Current principles andtechniques. St. Louis: Mosby; 2000.
20. King GJ, Keeling SD. Orthodontic bone remodeling in relation toappliance decay. Angle Orthodont 1995;65:129-40.
21. Proff P, Romer P. The molecular mechanism behind bone remod-elling: a review. Clin Oral Invest 2009;13:355-62:Epub 2009 Mar25. Review.
22. Vargervik K. Some aspects of bone formation and remodeling per-tinent to craniofacial development and reconstructive treatment.Acta Odontol Scand 1995;53:167-73.
23. van Leeuwen EJ, Maltha JC, Kuijpers-Jagtman AM. Tooth move-ment with light continuous and discontinuous forces in beagledogs. Eur J Oral Sci 1999;107:468-74.
24. van Driel WD, van Leeuwen EJ, Von den Hoff JW, Maltha JC,Kuijpers-Jagtman AM. Time-dependent mechanical behaviour ofthe periodontal ligament. Proc InstMechEngH2000;214:497-504.
25. Rygh P, Norton LA, Burstone CJ. The periodontal ligament understress: the biology of tooth movement. Boca Raton: CRC Press;1989. p. 9-12.
26. Verna C, Dalstra M, Melsen B. The rate and the type of orthodontictooth movement is influenced by bone turnover in a rat model. EurJ Orthod 2000;22:343-52.
27. Reitan K. Clinical and histologic observations on tooth movementduring and after orthodontic treatment. Am J Orthodont 1967;53:721-45.
28. Frost HM. The biology of fracture healing: an overview for clini-cians. Part I. Clin Orthop Relat Res 1989;248:283.
29. Iino S, Sakoda S, Ito G, Nishimori T, Ikeda T, Miyawaki S. Acceler-ation of orthodontic tooth movement by alveolar corticotomy inthe dog. Am J Orthodont Dentofacial Orthoped 2007;31:448.e1-8.
30. Aitchison GU. Use of a Faxitron x-ray cabinet for the rapid detectionof the end-point of decalcification. Med Lab Sci 1979;36:195-6.
31. Muller R, Ruegsegger P. Micro-tomographic imaging for the non-destructive evaluation of trabecular bone architecture. Stud HealthTech Informat 1997;40:61-79.
32. Pilon JJ, Kuijpers-Jagtman AM, Maltha JC. Magnitude of ortho-dontic forces and rate of bodily tooth movement. An experimentalstudy. Am J Orthodont Dentofacial Orthoped 1996;110:16-23.
33. Midgett RJ, Shaye R, Fruge JF Jr. The effect of altered bonemetab-olism on orthodontic tooth movement. Am J Orthod 1981;80:256-62.
34. Ashcraft MB, Southard KA, Tolley EA. The effect ofcorticosteroid-induced osteoporosis on orthodontic toothmovement. Am J Orthodont Dentofacial Orthoped 1992;102:310-9.
April 2011 � Vol 139 � Issue 4 � Supplement 1 American
35. Sidiropoulou-Chatzigiannis S, Kourtidou M, Tsalikis L. The effectof osteoporosis on periodontal status, alveolar bone and ortho-dontic tooth movement. A literature review. J Int Acad Periodont2007;9:77-84.
36. Bruzzaniti A, Baron R. Molecular regulation of osteoclast activity.Rev Endocr Metab Dis 2006;7:123-39.
37. Teitelbaum SL. Osteoclasts: what do they do and how do they doit? Am J Pathol 2007;170:427-35.
38. Lam J, Nelson CA, Ross FP, Teitelbaum SL, Fremont DH. Crys-tal structure of the TRANCE/RANKL cytokine reveals determi-nants of receptor-ligand specificity. J Clin Invest 2001;108:971-9.
39. Kostenuik PJ, Shalhoub V. Osteoprotegerin: a physiological andpharmacological inhibitor of bone resorption. Curr Pharm Des2001;7:613-35.
40. Aubin JE, Bonnelye E. Osteoprotegrin and its ligand: a newparadigm for regulation of osteoclastogenesis and bone resorp-tion. Osteoporosis Int 2000;11:905-13.
41. Becker KL, Nylen ES, White JC, Muller B, Snider RH Jr. Clinical re-view 167: Procalcitonin and the calcitonin gene family of peptidesin inflammation, infection, and sepsis: a journey from calcitoninback to its precursors. J Clin Endocrinol Metabol 2004;89:1512-25.
42. Pagani F, Francucci CM, Moro L. Markers of bone turnover: bio-chemical and clinical perspectives. J Endocrinol Invest 2005;28:8-13.
43. Halleen JM, Tiitinen SL, Ylipahkala H, Fagerlund KM, Vaananen HK.Tartrate-resistant acid phosphatase 5b (TRACP 5b) as a marker ofbone resorption. Clin Lab 2006;52:499-509.
44. Rosenbrock H, Seifert-Klauss V, Kaspar S, Busch R, Luppa PB.Changes of biochemical bone markers during the menopausaltransition. Clin Chem Lab Med 2002;40:143-51.
45. Shingleton WD, Hodges DJ, Brick P, Cawston TE. Collagenase:a key enzyme in collagen turnover. Biochem Cell Biol 1996;74:759-75.
46. Kafienah W, Bromme D, Buttle DJ, Croucher LJ, Hollander AP.Human cathepsin K cleaves native type I and II collagens at theN-terminal end of the triple helix. Biochem J 1998;331(Pt 3):727-32.
47. Granholm S, Lundberg P, Lerner UH. Calcitonin inhibits osteoclastformation in mouse haematopoetic cells independently of tran-scriptional regulation by receptor activator of NF-{kappa}B andc-Fms. J Endocrinol 2007;195:415-27.
48. McKee MD, Nanci A. Osteopontin at mineralized tissue interfacesin bone, teeth, and osseointegrated implants: ultrastructuraldistribution and implications for mineralized tissue formation,turnover, and repair. Micros Res Tech 1996;33:141-64.
49. Brown LF, Berse B, Van de Water L, et al. Expression and dis-tribution of osteopontin in human tissues: widespread associa-tion with luminal epithelial surfaces. Mol Biol Cell 1992;3:1169-80.
50. Giachelli CM, Bae N, Almeida M, Denhardt DT, Alpers CE,Schwartz SM. Osteopontin is elevated during neointima formationin rat arteries and is a novel component of human atheroscleroticplaques. J Clin Invest 1993;92:1686-96.
51. Denhardt DT, Guo X. Osteopontin: a protein with diverse func-tions. FASEB J 1993;7:1475-82.
52. Sodek J, Chen J, Nagata T, et al. Regulation of osteopontin expres-sion in osteoblasts. Ann NY Acad Sci 1995;760:223-41.
53. Oldberg A, Franzen A, Heinegard D. Cloning and sequence analysisof rat bone sialoprotein (osteopontin) cDNA reveals anArg-Gly-Asp cell-binding sequence. Proc Nat Acad Sci 1986;83:8819-23.
Journal of Orthodontics and Dentofacial Orthopedics

Baloul et al S101
54. Chen J, Shapiro HS, Sodek J. Development expression of bonesialoprotein mRNA in rat mineralized connective tissues. J BoneMiner Res 1992;7:987-97.
55. Ogata Y. Bone sialoprotein and its transcriptional regulatorymechanism. J Periodont Res 2008;43:127-35.
56. Waltregny D, Bellahcene A, de Leval X, Florkin B, Weidle U,Castronovo V. Increased expression of bone sialoprotein in bonemetastases compared with visceral metastases in human breastand prostate cancers. J Bone Miner Res 2000;15:834-43.
57. Liu Z, Luyten FP, Lammens J, Dequeker J. Molecular signaling inbone fracture healing and distraction osteogenesis. Histol Histopa-thol 1999;14:587-95.
American Journal of Orthodontics and Dentofacial Orthoped
58. Ren Y, Maltha JC, Kuijpers-Jagtman AM. The rat as a model fororthodontic tooth movement—a critical review and a proposedsolution. Eur J Orthod 2004;26:483-90.
59. Verna C, Dalstra M, Melsen B. Bone turnover rate in rats does notinfluence root resorption induced by orthodontic treatment. Eur JOrthod 2003;25:359-63.
60. Reitan K, Kvam E. Comparative behavior of human and animal tis-sue during experimental tooth movement. Angle Orthod 1971;41:1-14.
61. Fortin JM. Translation of premolars in the dog by controlling themoment-to-force ratio on the crown. Am J Orthodont 1971;59:541-51.
ics April 2011 � Vol 139 � Issue 4 � Supplement 1