outline childhood stunting -...
TRANSCRIPT

TM
Optimizing nutrition
in stunted children:
Interventions and practices
Umaporn Suthutvoravut
Faculty of Medicine Ramathibodi Hospital
Mahidol University
• Background information
• Nutrition intervention
• Practice in Thailand
• Conclusion
Outline Childhood stunting
• Short stature for age
• Indicator of chronic undernutrition
• Defined by length or height below – 2 SDs from the WHO Child Growth Standards (or an acceptable reference) median for the same age and sex
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia
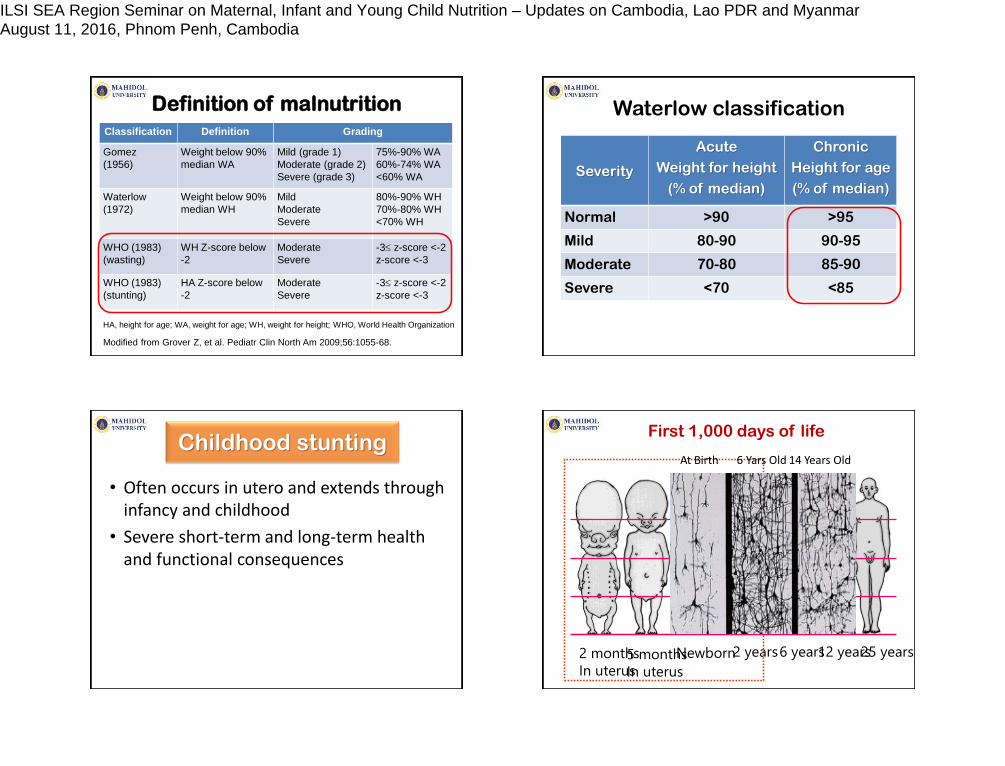
Classification Definition Grading
Gomez
(1956)
Weight below 90%
median WA
Mild (grade 1)
Moderate (grade 2)
Severe (grade 3)
75%-90% WA
60%-74% WA
<60% WA
Waterlow
(1972)
Weight below 90%
median WH
Mild
Moderate
Severe
80%-90% WH
70%-80% WH
<70% WH
WHO (1983)
(wasting)
WH Z-score below
-2
Moderate
Severe
-3 z-score <-2
z-score <-3
WHO (1983)
(stunting)
HA Z-score below
-2
Moderate
Severe
-3 z-score <-2
z-score <-3
HA, height for age; WA, weight for age; WH, weight for height; WHO, World Health Organization
Modified from Grover Z, et al. Pediatr Clin North Am 2009;56:1055-68.
Definition of malnutrition Waterlow classification
Severity
Acute
Weight for height
(% of median)
Chronic
Height for age
(% of median)
Normal >90 >95
Mild 80-90 90-95
Moderate 70-80 85-90
Severe <70 <85
Childhood stunting
• Often occurs in utero and extends through infancy and childhood
• Severe short-term and long-term health and functional consequences
2 months
In uterus 5 months
In uterus
Newborn 2 years 6 years 12 years 25 years
At Birth 6 Yars Old 14 Years Old
First 1,000 days of life
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

UNICEF Report: Critical Importance of First 1,000 Days of Life Friday, April 19, 2013 World attention is increasingly focused on the most critical period experienced by everyone on earth-the first 1,000 days of life from conception to the second birthday.
"It is difficult to think of a greater injustice than robbing a child, in the womb and in infancy, of the ability to fully develop his or her talents throughout life. This is a tragedy for the 165 million children under the age of 5 afflicted by stunting in the world today. It is a violation of their rights. It is also a huge burden for nations whose future citizens will be neither as healthy nor as productive as they could have been."
Anthony Lake, Executive Director of UNICEF
Linear growth & child development
in LMICs: Meta-analysis
• 68 studies in 29 low- and middle-income countries
• Cross-sectional and prospective studies
Sudfeld CR et al. Pediatrics 2015; 135: e1266-75.
Multivariate adjusted cross-sectional SMD in cognition per unit increase in HAZ stratified by age at measurement.
Sudfeld CR et al. Pediatrics 2015; 135: e1266-75.
+ 0.24
+ 0.09
Multivariate adjusted prospective SMD in
cognition per unit increase in HAZ.
Sudfeld CR et al. Pediatrics 2015; 135: e1266-75.
+ 0.22
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

• 5 long-standing prospective cohort studies from Brazil, Guatemala, India, Philippines, South Africa
• Poor fetal growth or stunting in the first 2 years of life leads to irreversible damage including shorter adult height, lower attained schooling, reduced adult income, decreased offspring birth weight
• Children who are undernourished in the first 2 years and put on weight rapidly later are at high risk of diet-related chronic diseases
Victora CG et al. Lancet 2008
Maternal and child undernutrition:
Consequences for adult health & human capital 40%reductionin the number of children under-5 who are stunted.
Framework of the relations between poverty, food insecurity, and other underlying and immediate causes to maternal and child undernutrition and its short-term and long-term consequences
Black RE, et al. Lancet 2008.
Maternal and child
undernutrition
Short-term consequences:
Mortality, morbidity, disability
Long-term consequences:
Adult size, intellectual ability, economic
productivity, reproductive performance,
metabolic and cardiovascular disease
Inadequate dietary
intake Disease
Inadequate care Unhealthy household environment
and lack of health services
Household food
insecurity
Income poverty: employment, self-
employment, dwelling, assets,
remittances, pensions, transfers etc
Lack of capital: financial, human,
physical, social, and natural
Social, economic, and political context
Immediate
causes
Basic
causes
Underlying
causes
Changes in stunting prevalence
between 1996-2010 in SEA countries
Bloem MW et al. Food Nutr Bull 2013;34:S8-16.
32 36 44 17 35 30 0 16 19
Globalnutritionreport.org 2015
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

Stunting rates by Gross Domestic Product
in selected ASEAN countries: 2010 data
Bloem MW et al. Food Nutr Bull 2013;34:S8-16.
Optimal
catch-up
growth
Energy
Protein
Micro-
nutrients
Treat
causes
• Depend on severity (wasted, wasted and stunted) and causes
• Estimated energy need by using ideal body weight for height or energy/kg actual body weight plus 10-50%
• Estimated protein requirement of wasted children are 9-11.5 % of total energy, depending on the rate and composition of weight gain
Energy & protein requirement
to catch up
Report of Joint WHO/FAO/UNU Expert Consultation, 2007. Nevin-Folino N (ed). Ped Manual Clin Dietetics, 2003. Sullivan PB and Goulet O (eds). EJCN 2010; 64 (Suppl 1)
Protein Amino
acids Bone growth
Growth
hormone,
zinc IGF-1*
Stimulate chondrocyte &
osteoblast
Intestinal Ca, P
absorption
25(OH)D3 1,25(OH)2D3
Renal tubular
P absorption *Insulin-like growth factor-1
Protein and bone growth
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

Dietary protein
Endogenous acid
production
Renal tubular
Ca reabsorption
Direct physico-
chemical
dissolution of bone
Cell-
mediated
bone
resorption
Urinary calcium loss
Bone loss
Protein & Energy
Vitamins: D, K, A, C
Minerals:
Ca, P, Mg, Na, K
I, Zn, Cu, Fe, F
Major nutrients for bone growth
www.bbc.co.uk
Successful nutrition
intervention
• Integrated approaches
• Combined with infection control and child development intervention
• Cover both pregnancy and post-natal periods
Nutrition interventions
• Dietary diversification
• Selection of nutrient-rich foods
• Exclusive breastfeeding 0-6 months
• Improved complementary feeding practice
• Staple food fortification eg. iron, zinc
• Multiple micronutrient supplementation
• Use of fortified food products specifically formulated for these target groups
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

Dietary diversification &
Selection of nutrient-rich food
• Food-Based Dietary Guidelines & Food Guide
• Challenges: Implementation and evaluation
• Healthy food environment and effective partnership among various sectors i.e. government, food industry/producer, agriculture, health service, nutrition, education, community
Hans de Beer. Economics & Human Biology 2012.
Dairy products and physical stature
• Systematic review and meta-analysis of controlled trials
• 12 studies: 7 randomized controlled trials and 5 non-randomized controlled trials
• Sample size 36-757 participants
• Age 3-13 years
• Country: Europe (3), USA (2), China (2), Indonesia (2), Northern Vietnam, Kenya, India
Forest plot of trials comparing height increases in supplementation groups versus usual diet or usual diet plus calorie supplement groups.
Hans de Beer. Economics & Human Biology 2012.
Additional growth of 0.4 cm/year/245 ml of milk daily
Dairy products and physical stature
0.59 cm
Lactose maldigestion (LM)
and intolerance (LI) in Thais
Subject N Test food LM(%) LI (%)
Children, 5-6 y 101 250 ml milk between
meal
15 0
250 ml milk+snack 12 0
Adolescents,13-16 y 324 250 ml milk 38 18
Adults, 18-45 y 93 250 ml milk 69 64
24
LM
125 ml milk 42
23
LM
250 ml milk+sandwich 21
29
LM
Yoghurt 15 4
Middle age, 45-60 70 Milk 57 64
40 Low lactose milk 17 36
40 Lactose-free milk 11 6
Sirichakwal PP, et al. 1989-2002
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

zinc
Catalytic Structural Regulatory
Clinical manifestation of zinc deficiency
Growth retardation (stunting)
Weight loss (wasting)
Delayed puberty
Hypogonadism & hypospermia
Poor appetite, hypogeusia, dysgeusia
Diarrhea
Impaired immunity, increase susceptibility to infection
Clinical manifestation of zinc deficiency
Skin lesions: dermatitis, erythematous, vesiculobullous, pustular, acro-orificial lesion
Glossitis, nail dystrophy, hair loss
Eye lesions: photophobia, impaired dark adaptation, blepharoconjunctivitis
Delayed wound healing
Behavioral abnormality
Low birth weight, prematurity
• Meta-analysis of randomized controlled trials
• 33 RCTs in children aged < 12 years (majority in <5-year-old children)
• Various dosage (1-20 mg/day)
• Duration 8 weeks -15 months
• Most studies provided ZnSO4
Zinc supplementation and linear
growth: Meta-analysis of RCT
Brown KH et al. Am J Clin Nutr 2002.
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

Weighted mean effect size and 95% CI (in SD units) for the effect of zinc
supplementation on children's linear growth by the subjects' mean initial
HAZ, WAZ, age, and serum zinc concentration
Brown KH et al. Am J Clin Nutr 2002.
• Systematic review and meta-analysis of randomized controlled trials
• 21 RCTs in infants (n=9), 1-5 year-old (n=6), > 6 year-old children (n=6)
• Various dosage (1-3 mg/kg/day – 3 mg/kg/week)
• Various iron preparation
• Duration 6 weeks -12 months
No effect of iron intervention on height
Vucic V et al. Nutr Rev 2013.
Strategies for prevention and control of malnutrition in Thailand
• Food/micronutrient supplementation
• Food fortification
• Food security
Food & Nutrients
• Public health measures: immunization, sanitation, water supply, deworming, growth monitoring, etc
• Community-based approaches
Public health &Community
• Food regulation
• Food and nutrition education/communication
Regulation& Education
Capacity building, Research & Development
“National food Fortification Committee” (appointed 1993 by MoPH) - Mandate : Support food fortification to improve micronutrient nutrition - Fortified product development : eg. universal salt iodization; iron, iodide, VA fortified instant noodle seasoning mix; iron and iodide in fish sauce Dietary diversification - Development and modification of Food Composition Table - Promotion of micronutrient-rich food production - Development of dietary guidelines and micronutrient-rich menu - Dietary guidelines for preparation of complementary foods from locally available raw materials for children of different age groups Development of national food-based dietary guidelines - FBDGs and Nutrition Flag - FBDGs for pregnant women - FBDGs for infants & preschool children
Food fortification and Food-based Dietary
Guidelines in Thailand
36
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

Food-Based Dietary Guidelines (FBDGs)
for Infants and Young Children, 2009
• Bureau of Health Promotion,
Ministry of Public Health
o Guidelines for antenatal care
o Guidelines for infant and young child feeding, care, immunization
o Record of growth, immunization
Maternal and child health record
Dietary guidelines: Pregnancy Dietary guidelines: Infants and young children
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia

Micronutrient supplementation
• Iodine, folic acid, iron supplementation for pregnant and lactating women : daily dose
• Iron supplementation for pre-school and school-age children : weekly dose
School milk program in Thailand
Implemented as national programs since 1992
Based on Food and Nutrition Plan aiming to provide 200 ml/day of milk to children in kindergartens and primary school for 230 days/ year
An example of inter-sectoral linkage between education, agriculture, industry, local administration and health
Creating demand for local dairy industry which has grown significantly
• Optimizing nutrition support in stunted children is essential to reduce the short- and long-term consequences of malnutrition
• Integrated approaches: nutrition intervention should be combined with other public health intervention
• Prevention of childhood stunting by proper nutrition in pregnancy and post-natal periods
Conclusion
ILSI SEA Region Seminar on Maternal, Infant and Young Child Nutrition – Updates on Cambodia, Lao PDR and MyanmarAugust 11, 2016, Phnom Penh, Cambodia