transvascular aortic valve replacement planning: … are manufacturer s guidelines for sizing for...
TRANSCRIPT

557
WE
DN
ESD
AY
DisclosuresDisclosures
N�None
TAVR vs. TAVITAVR vs. TAVI
�TAVR = Transcatheter Aortic Valve ReplacementReplacement
�TAVI = Transcatheter Aortic Valve Implantation
�TAVI seems to have won out in the literature
Objectivesj
�Introduction to TAVR/TAVIIntroduction to TAVR/TAVI�Familiarization with available and soon to be available valvessoon to be available valves�Review measurements performed on preoperative CT scanspreoperative CT scans�Review potential complications�Highlight developing applications
Aortic Stenosis
�Slowly develops but rapidly progresses after�Slowly develops, but rapidly progresses after symptom onset� 50% mortality within 2y of symptom onsety y y p
�Severe aortic stenosis defined as any of the Following:� Aortic Valve Area < 0.8 cm2
M A ti V l G di t 40 H� Mean Aortic Valve Gradient > 40 mmHg� Peak Aortic Jet Velocity > 4 m/sec
Aortic Stenosis
�Surgical replacement typically offers a low�Surgical replacement typically offers a low mortality cure�Up to 30 % of patients w/ AS are not surgicalUp to 30 % of patients w/ AS are not surgical
candidates�First transcatheter valve placed using an antigrade transeptal approach by Cribier and co-workers in 2002
�Currently, over 60,000 valves have been placed in over 40 countries
Transvascular Aortic Valve Replacement Planning:What Radiologists Need to Know Gregory D.N. Pearson, MD, PhD

558
WE
DN
ESD
AY
TAVI: how does it work?TAVI: how does it work?
N Engl J Med 2011; 364:2187-2198 N Engl J Med 2011; 364:2187-2198
Floroscopypy
N Engl J Med 2011; 364:2187-2198
Transapical approach
Edwards SAPIEN ValveEdwards SAPIEN Valve
http://www.edwards.com/products/transcathetervalve/pages/sapienthv.aspx
PARTNERPARTNER�Cohort A (Non-Surgical Patients � TAVR vs. V l l l t ) O t 2010Valvuloplasty) Oct. 2010
�Transcatheter Aortic-Valve Implantation for AorticTranscatheter Aortic Valve Implantation for Aortic Stenosis in Patients Who Cannot Undergo Surgery
�Cohort B (TAVR vs. Surgery in High Risk Patients) June 2011
�Transcatheter versus Surgical Aortic-Valve Replacement in High-Risk Patients
N Engl J Med 2010;363:1597-1607. N Engl J Med 2011; 364:2187-2198

559
WE
DN
ESD
AY
Cohort A (Non-Surgical Patients)Cohort A (Non Surgical Patients) � Multi-Center (21 centers, 17 in US)
� 358 patients with:� Severe Aortic Stenosis:
� Aortic Valve Area < 0.8 cm2
� Mean Aortic Valve Gradient > 40 mmHg� Mean Aortic Valve Gradient > 40 mmHg� Peak Aortic Jet Velocity > 4 m/sec
� Predicted > 50% mortality or severe morbidity at 30 days after potential surgery
E l i� Exclusion: � Bicuspid valve; LVEF < 20%; AV annulus < 18 mm or > 25 mm� Severe MR or AR; TIA/CVA within 6 mo; Severe renal insufficiency
� Randomized: � TAVR or Valvuloplasty
� Follow up at 30 days and 1 year� Follow-up at 30 days and 1 year
N Engl J Med 2010;363:1597-1607.
Cohort A (Non-Surgical Patients)Cohort A (Non Surgical Patients) 30 Days 1 Year
TAVRN=179
StndTxt N=179
P value
| TAVRN=179
StndTxt N=179
P value
Death (any cause) 9 5 0.41 | 55 89 <0.001
Death (CV cause) 8 3 0.22 | 35 75 <0.001
Re-Hospitalization 10 18 0.17 | 40 79 <0.001
Stroke 12 3 0.03 | 19 8 0.04|Any Death or Stroke 15 7 0.12 | 59 90 0.001
Vascular 55 9 <0.001 | 58 13 <0.001Complication
|Major Bleeding 30 7 <0.001 | 40 20 <0.001
N Engl J Med 2010;363:1597-1607.
Cohort A (Non-Surgical Patients)Cohort A (Non Surgical Patients)
�Summary
� At 1 year, TAVR showed significantly lower risk of death from CV and any cause� # needed to treat to prevent 1 death from AS = 5� # needed to treat to prevent 1 death or re-hospitalization = 3
� TAVR had Significantly more:� Strokes� Major Vascular Complications
M j Bl di� Major Bleeding
� TAVR patients experienced significant improvement symptoms� Based NYHA class I or II at 30 days 6 months and 1 year (all P < 0 001)� Based NYHA class I or II at 30 days, 6 months and 1 year (all P < 0.001)
N Engl J Med 2010;363:1597-1607.
Cohort B: High-Risk PatientsCohort B: High Risk Patients �Multicenter (25 centers, 22 in US)
�699 patients with:� Severe Aortic Stenosis (same criteria as Cohort A)� Severe Aortic Stenosis (same criteria as Cohort A)� High-Risk for Operative Complications:� Co-Existing conditions associated with > 15% risk of death w/n 30 days of
procedurep
�Randomized into:� Standard treatment: Surgical Replacement (N = 351)Standard treatment: Surgical Replacement (N 351)� TAVR (N = 348)� These were further split based on degree of PAD:
� Transfemoral approach (N = 244)pp ( )� Transapical approach (N = 104)
N Engl J Med 2011; 364:2187-2198
Cohort B: High-Risk PatientsCohort B: High Risk Patients � Primary endpoint was Death from any cause at 1 year
� TAVR = 24.2 % versus Surgical = 26.8% (P = 0.44)� Served to prove �Non-Inferiority� of TAVR in this High-Risk Population (P
0.001)
� TAVR again showed increased risk of Stroke at 30 days and 1 year� 30 days: 5 5% vs 2 4% (P = 0 04)30 days: 5.5% vs 2.4% (P 0.04)� 1 year: 8.3% vs 4.3% (P = 0.04)
C bi d i k f D th d St k t diff t (TAVR� Combined risk of Death and Stroke were not different (TAVR vsSurgery)� 30 Days: 6.9% vs 8.2%� 1 year: 26.5% vs 28.0%
N Engl J Med 2011; 364:2187-2198
Cohort B: High-Risk PatientsCohort B: High Risk Patients � TAVR had higher rates of Major Vascular Complications:
� 11.0% vs 3.2% (P<0.001)( )
� Surgery had higher rates of Major Bleeding and New-Onset A-Fib� 9.3% vs 19.5% (P<0.001) and 8.6% vs16.0% (P=0.006)
� TAVR had shorter ICU stay (3d vs 5d) & index hospitalization (8d vs 12d)
� At 30 days TAVR showed a significant reduction in NYHA symptomsAt 30 days, TAVR showed a significant reduction in NYHA symptoms � (Grade I or II), but this difference equalized at 1 year follow up
� At 1 year, TAVR had better valve function (Gradient and Valve Area)
� Significantly more aortic regurgitation after TAVR:� 30 Days: 12.2% vs 0.9%� 1 Year: 6 8% vs 1 9%1 Year: 6.8% vs 1.9%
N Engl J Med 2011; 364:2187-2198

560
WE
DN
ESD
AY
Company Valve Trials sizes annulus routes Femoral I t dIntroducerdiameter
Edwards Sapien PARTNER 23 mm26 mm
18-22 mm21-25 mm
Femoralapical
22 fr24 fr26 mm 21 25 mm apical 24 fr
Edwards Sapien XT PARTNER II 20 mm23 mm
16-19 mm18-21 mm
FemoralApical
ti16 fr
f26 mm29 mm
22-25 mm25-27 mm
aortic 18 fr20 fr
Edwards Sapien III 20 mm23 mm
16-19 mm18-21 mm
FemoralApical
14 fr14 fr
26 mm29 mm
22-25 mm25-27 mm
paortic 14 fr
16 frMedtronic CoreValve SURTAVI 23 mm
26 mm18-20 mm20 23 mm
FemoralApical
18 fr26 mm29 mm31 mm
20-23 mm23-26 mm26-29 mm
ApicalAorticSubclav.
Direct Flow Direct DISCOVER 25 mm 19-24 mm Femoral 18 frFlow SALUS 27 mm 22-26 mm 18 fr
Medtronic CoreValveMedtronic CoreValve
Valve comparison
Sapien valve CoreValve
Valve comparison
p
�Balloon expandable �Self-expanding�Round annulus�Annular valve
�Oval annulus�Supraannular valve
�Lower pacemaker risk (5 9%)
p�Higher pacemaker risk (22 5%)risk (5.9%) risk (22.5%)
Anatomy: how do we size valves?Anatomy: how do we size valves?
Preoperative imaging�Cardiac Catheterization�Cardiac Catheterization�Transthoracic and/or transesophageal echo�Cardiac CTCardiac CT�Gated, with systolic and diastolic phases�No � blockade
�Chest/Abdomen/Pelvis CT�Aortic runoff--with fast scanner can be performed
with same bolus as cardiac CTwith same bolus as cardiac CT
Schultz et al (Euro Heart Journal)Schultz et al. (Euro Heart Journal)� Three Dimensional Evaluation of the Aortic Annulus Using Multislice
CT: Are Manufacturer�s Guidelines for Sizing for Percutaneous Aortic Valve Replacement Helpful?Valve Replacement Helpful?
� 75 pts being evaluated for TAVR including a CT for pre-op planning� Only 50 received the valve (25 were too small / large for valve)
� Cardiologist picked valve based on:g p� Gender, body height, weight� LVOT and Aortic root on TTE and Aortography
� CT was performed and various measurements were obtained to find:� What was the best match between the cardiologist choice and manufacturer
European Heart Journal (2010) 31, 849�856
561
WE
DN
ESD
AY
MeasurementsRadiologists Cardiologists
http://sckhsmg2008.blogspot.com/2011/05/simple-echocardiography-views.html
European Heart Journal (2010) 31, 849�856
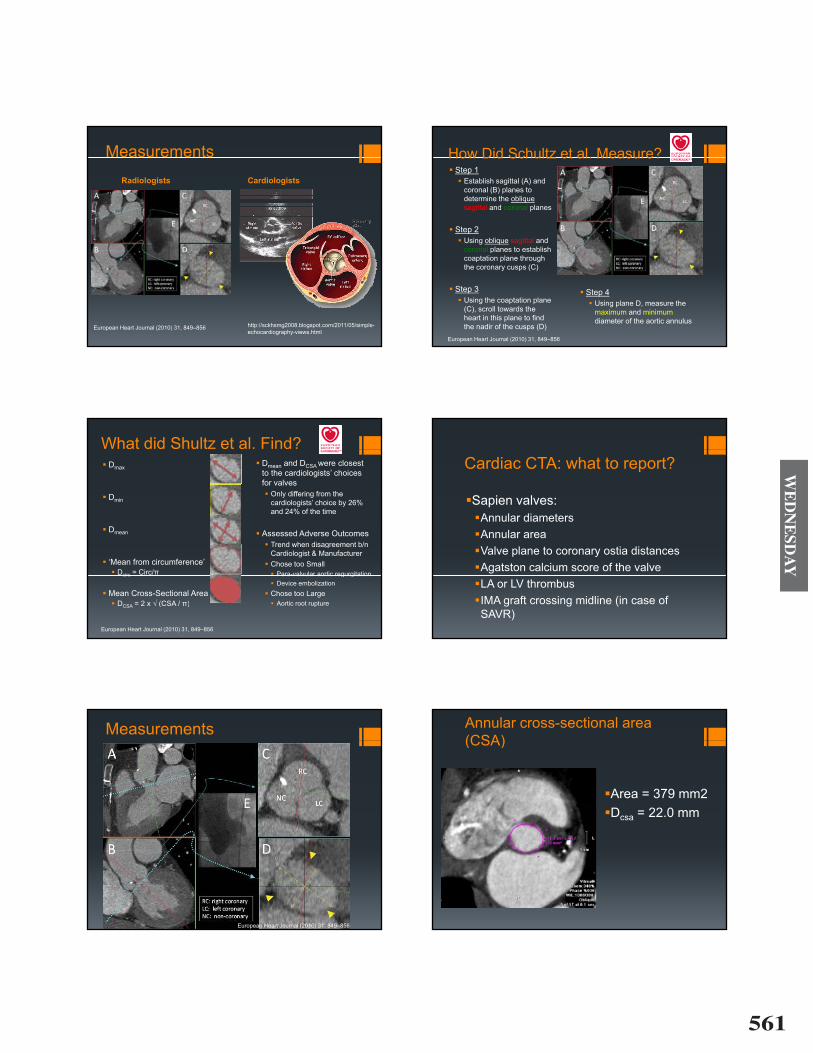
How Did Schultz et al. Measure?How Did Schultz et al. Measure?� Step 1
� Establish sagittal (A) and coronal (B) planes tocoronal (B) planes to determine the obliquesagittal and coronal planes
� Step 2� Using oblique sagittal and
coronal planes to establish pcoaptation plane through the coronary cusps (C)
� Step 3� Using the coaptation plane
(C), scroll towards the h t i thi l t fi d
� Step 4� Using plane D, measure the
maximum and minimumheart in this plane to find the nadir of the cusps (D)
diameter of the aortic annulus
European Heart Journal (2010) 31, 849�856
What did Shultz et al. Find?� Dmax � Dmean and DCSA were closest
to the cardiologists� choices f l
� Dmin
for valves� Only differing from the
cardiologists� choice by 26% and 24% of the time
� Dmean
and 24% of the time
� Assessed Adverse Outcomes� Trend when disagreement b/n
� �Mean from circumference� � Dcirc = Circ/�
� Trend when disagreement b/n Cardiologist & Manufacturer
� Chose too Small� Para-valvular aortic regurgitationcirc
� Mean Cross-Sectional Area� DCSA = 2 x � (CSA / �)
Para valvular aortic regurgitation� Device embolization
� Chose too Large� Aortic root ruptureCSA ( )
European Heart Journal (2010) 31, 849�856
Cardiac CTA: what to report?
�Sapien valves:�Annular diameters�Annular area�Valve plane to coronary ostia distances�Agatston calcium score of the valve�LA or LV thrombus�IMA graft crossing midline (in case of SAVR)
Measurements
European Heart Journal (2010) 31, 849�856
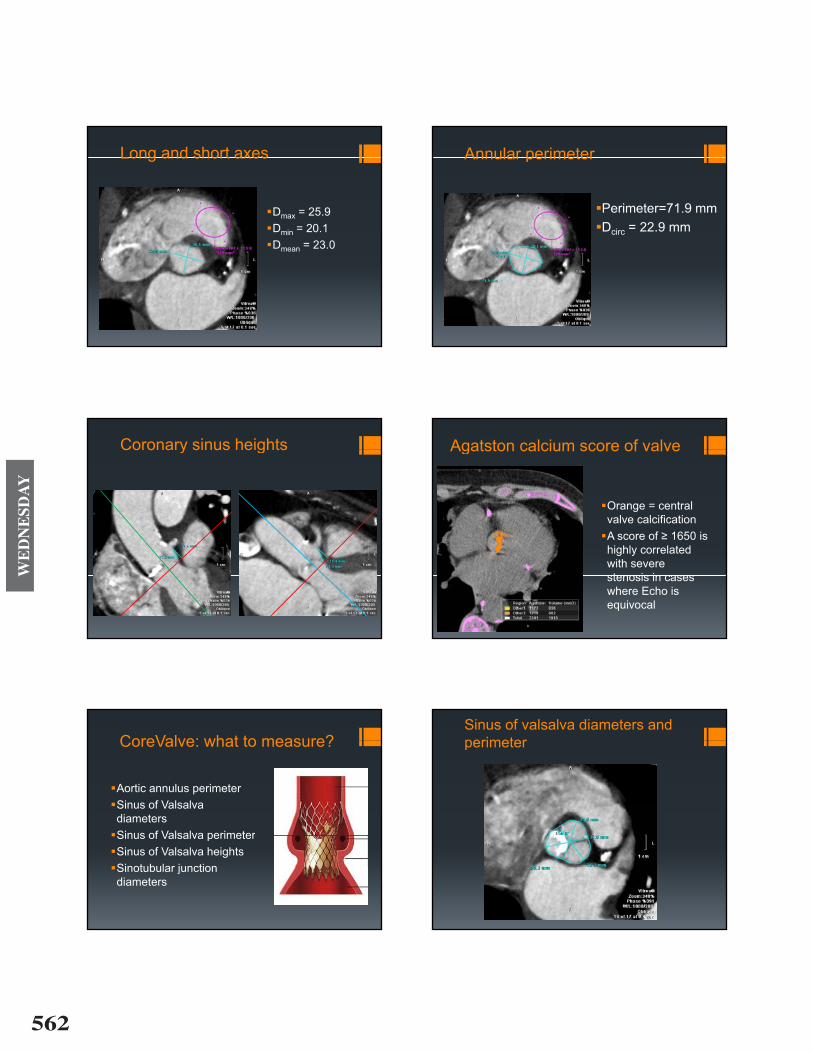
Annular cross-sectional area (CSA)(CSA)
�Area = 379 mm2�Dcsa = 22.0 mm
562
WE
DN
ESD
AY
Long and short axesLong and short axes
�Dmax = 25.9�Dmin = 20.1�Dmean = 23.0
Annular perimeterAnnular perimeter
�Perimeter=71.9 mm�Dcirc = 22.9 mm
Coronary sinus heightsCoronary sinus heights Agatston calcium score of valveAgatston calcium score of valve
�Orange = central valve calcification
�A score of � 1650 is highly correlated with severe stenosis in casesstenosis in cases where Echo is equivocalequivocal
CoreValve: what to measure?CoreValve: what to measure?
�Aortic annulus perimeter�Sinus of Valsalva�Sinus of Valsalva diameters
�Sinus of Valsalva perimeter�Sinus of Valsalva perimeter�Sinus of Valsalva heights�Sinotubular junction�Sinotubular junction diameters
Sinus of valsalva diameters and perimeterperimeter

563
WE
DN
ESD
AY
Sinus of Valsalva heightsSinus of Valsalva heights Sinotubular junction diametersSinotubular junction diameters
CoreValve: what to measure?CoreValve: what to measure?
�Ascending aortic diameters�Ascending aortic diameters �3 cm above valve plane�For 23 mm valve, must be less than 34 mm
�4 cm above valve plane�For 26 mm valve, must be less than 40 mm
�For 29 and 31 mm valves, must be less than 43 mm
CoreValve: what to measure?CoreValve: what to measure?
�Aortic angulation�Aortic angulation�Coronal viewF f l/ b l i t b�For femoral/subclavian access, must be <70°
�For transaortic access must be >30°�For transaortic access, must be >30
Aortic angulationAortic angulation
564
WE
DN
ESD
AY
Chest/abd/pelvis CT: what toChest/abd/pelvis CT: what to report?
�Porcelain aorta�Aneurysms�Minimal diameters�Aorta�Common iliacs�External iliacs�External iliacs�Common femorals
�Comorbid disease�Comorbid disease� tumors
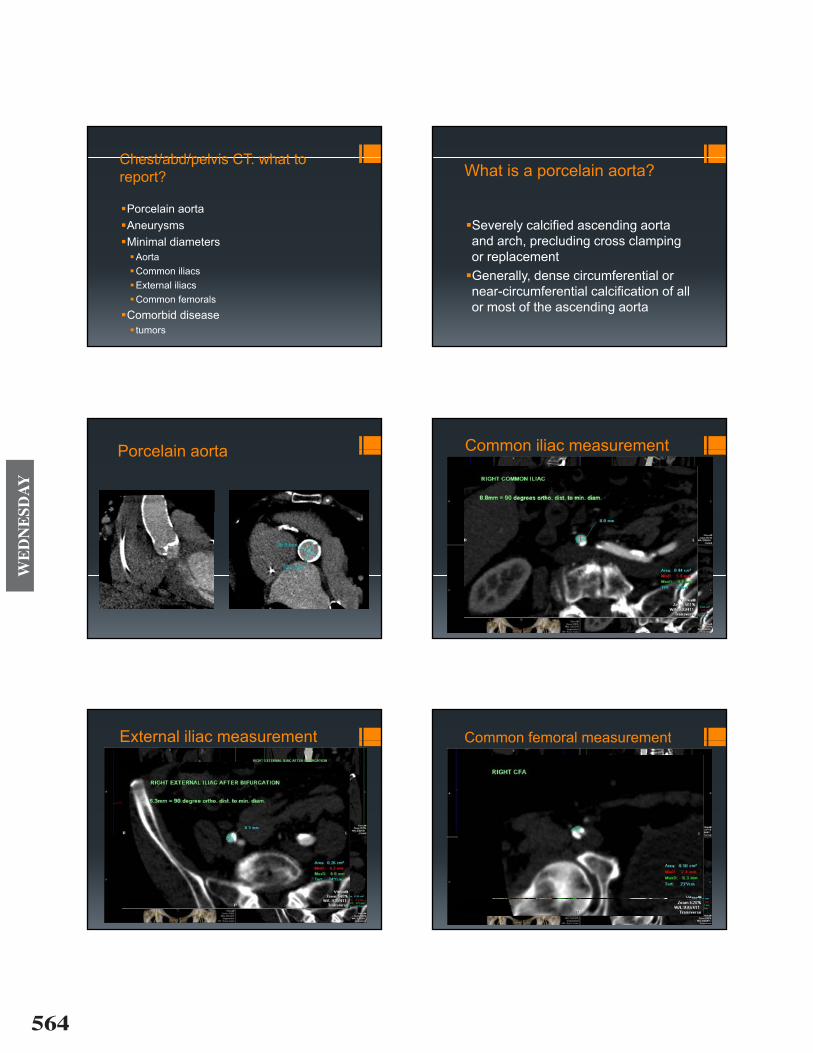
What is a porcelain aorta?
S l l ifi d di t�Severely calcified ascending aorta and arch, precluding cross clamping
l tor replacement�Generally, dense circumferential or near-circumferential calcification of all or most of the ascending aorta
Porcelain aortaPorcelain aorta Common iliac measurementCommon iliac measurement
External iliac measurementExternal iliac measurement Common femoral measurementCommon femoral measurement
565
WE
DN
ESD
AY
Comorbid disease: PEComorbid disease: PE What are we doing at Columbiag� Standard here is to use TEE to obtain annulus measurements
� CTA cardiac� CTA cardiac � To assess aortic annulus size (End Diastole and Systole)� To assess annulus to coronary ostia distance (�jailing the artery�)
T d f V l l ifi ti� To assess degree of Valve calcification
� CTA Chest/Abdomen/Pelvis� To assess Aorta calcification� Assess the iliac and femoral artery anatomy� Best to have a � 8 mm vascular access to accommodate the loading system
ComplicationsComplications
�Stroke�Para-valvular aortic regurgitationg g�Heart block�Vascular injuryVascular injury�Device migration
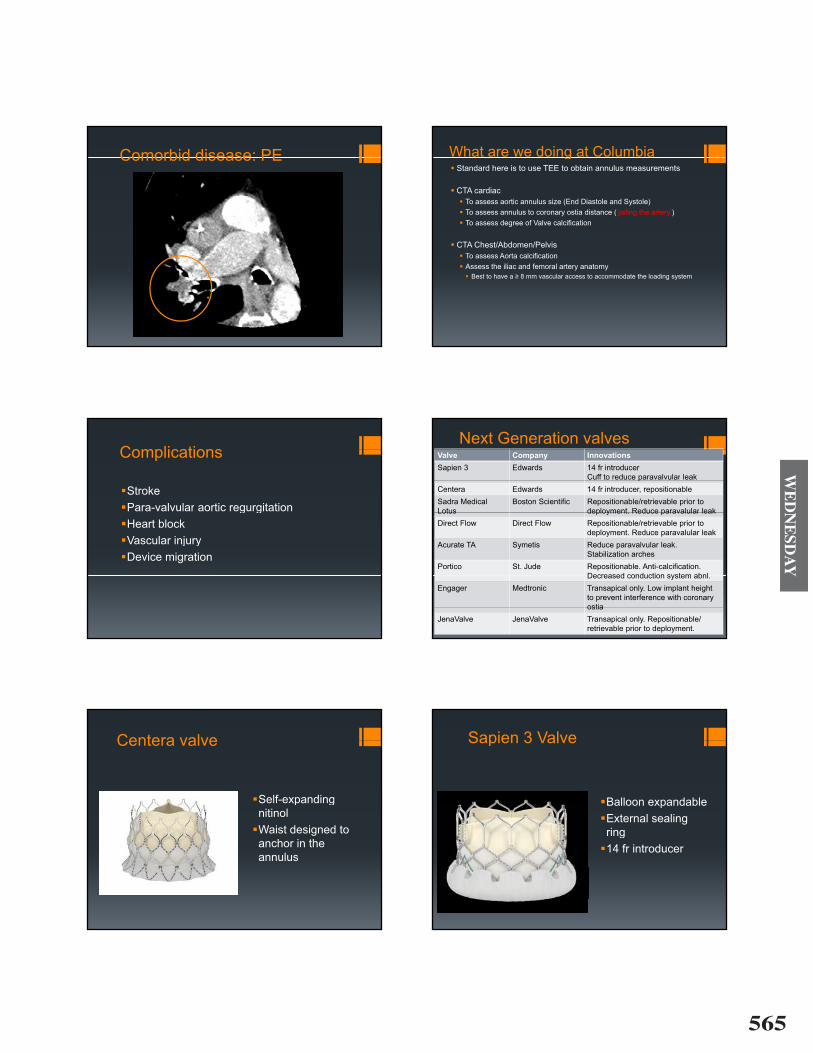
Next Generation valvesValve Company InnovationsSapien 3 Edwards 14 fr introducer
Cuff to reduce paravalvular leakpCentera Edwards 14 fr introducer, repositionableSadra MedicalLotus
Boston Scientific Repositionable/retrievable prior to deployment Reduce paravalular leakLotus deployment. Reduce paravalular leak
Direct Flow Direct Flow Repositionable/retrievable prior to deployment. Reduce paravalular leak
Acurate TA Symetis Reduce paravalvular leakAcurate TA Symetis Reduce paravalvular leak.Stabilization arches
Portico St. Jude Repositionable. Anti-calcification. Decreased conduction system abnlDecreased conduction system abnl.
Engager Medtronic Transapical only. Low implant height to prevent interference with coronary ostiaostia
JenaValve JenaValve Transapical only. Repositionable/ retrievable prior to deployment.
Centera valveCentera valve
�Self-expanding p gnitinol
�Waist designed to ganchor in the annulus
Sapien 3 ValveSapien 3 Valve
�Balloon expandableBalloon expandable�External sealing ringring
�14 fr introducer
566
WE
DN
ESD
AY
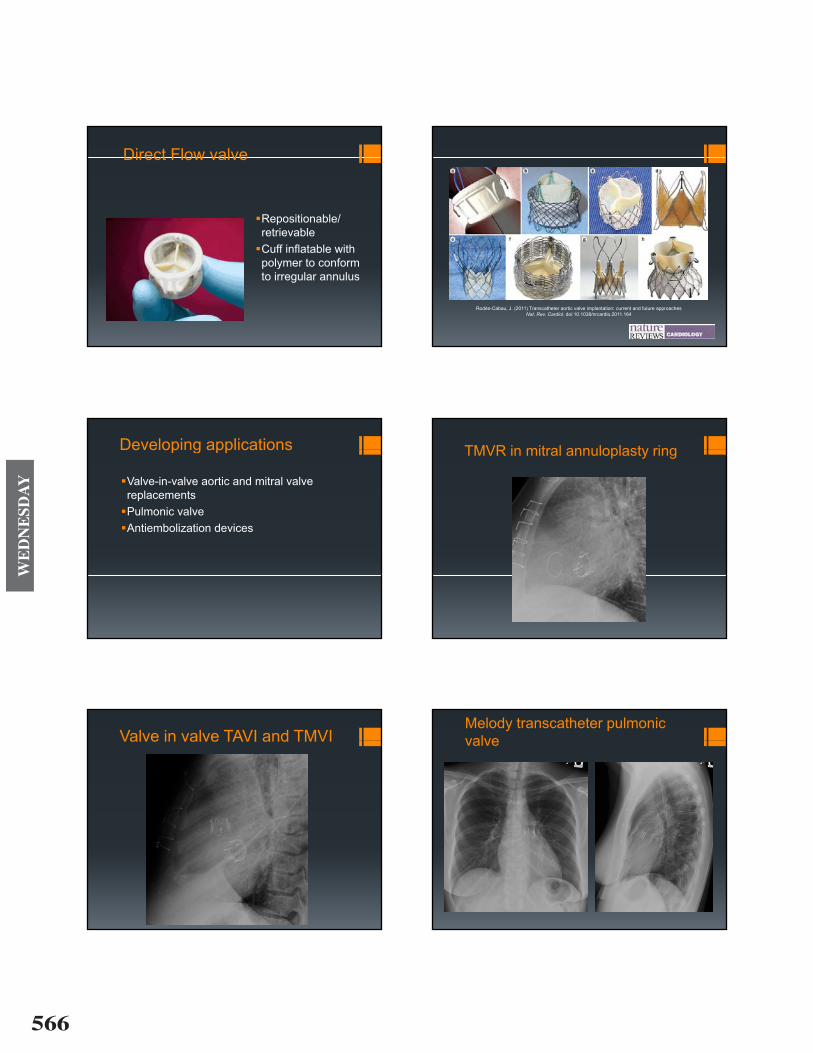
Direct Flow valveDirect Flow valve
�Repositionable/Repositionable/ retrievable
�Cuff inflatable withCuff inflatable with polymer to conform to irregular annulus
Images of emerging transcatheter valve technology (valves with first-in-man data). a | Direct Flow Medical® valve (Direct Flow Medical, Santa Rosa, CA, USA). Permission obtained from Direct Flow Medical. b | HLT valve (Heart
Leaflet Technologies, Maple Grove, MN, USA). ©2011 HLT, Inc. a Bracco Group Co. c | Innovare valve (BraileLeaflet Technologies, Maple Grove, MN, USA). ©2011 HLT, Inc. a Bracco Group Co. c | Innovare valve (BraileBiomedical, São José do Rio Preto, Brazil). Courtesy of Diego Gaia, Federal University of São Paulo, Brazil. d | JenaValve® (JenaValve Technology, Munich, Germany). Permission obtained from JenaValve Technology. e |
Portico® valve (St-Jude Medical, St Paul, MN, USA). f | Sadra® Lotus Medical valve (Boston Scientific SciMedInc, Maple Grove, MN, USA). ©2011 Boston Scientific Corporation or its affiliates. All rights reserved. Used with permission of Boston Scientific Corporation. g | Symetis® Accurate valve (Symetis SA, Lausanne, Switzerland).
Permission obtained from Symetis. h | Engager® valve (Medtronic Inc., Minneapolis, MN, USA). ©2010 Medtronic, Inc. Image provided by Medtronic, Inc
Rodés-Cabau, J. (2011) Transcatheter aortic valve implantation: current and future approachesNat Rev Cardiol doi:10.1038/nrcardio 2011.164Nat. Rev. Cardiol. doi:10.1038/nrcardio.2011.164
Developing applicationsDeveloping applications
�Valve in valve aortic and mitral valve�Valve-in-valve aortic and mitral valve replacements
�Pulmonic valve�Pulmonic valve�Antiembolization devices
TMVR in mitral annuloplasty ringTMVR in mitral annuloplasty ring
Valve in valve TAVI and TMVIValve in valve TAVI and TMVIMelody transcatheter pulmonic valvevalve

567
WE
DN
ESD
AY
MRI safety
Ed d S i diti l 6�Edwards Sapien conditional 6�Edwards Sapien XT conditional 5�Medtronics Core Valve conditional 5�Direct Flow conditional 5Direct Flow conditional 5
�the list�, MRISafety.com
Special ThanksSpecial Thanks
�Dr. Mark Escudero�TAVR imaging teamTAVR imaging team�Dr. Anna Rozenshtien�Dr. Belinda D�Souza�Dr. Todd Pulerwitz�Dr. Andrew Einstein
�Other members of the TAVR team�Dr. Susheel Kodali �Dr. Omar Kahlique