pediatric covid-19 patients - indushospital.org.pk
TRANSCRIPT

MANAGEMENT OFPEDIATRIC
COVID-19PATIENTS
INDUS HEALTH NETWORK
indushospital the-indus-hospital The Indus Hospitalindus_hospital theindushospital

ACKNOWLEDGMENT
Dr. Samina Junejo Pediatric Infectious Diseases Consultant, Indus Hospital developed the guidelines with contribution from Dr. Samreen Sarfaraz (Consultant Adult Infectious Diseases) at the Indus Hospital. It is reviewed by Dr. Ahmer Hamid, Chair Pediatrics, Indus Hospital and Dr. Hanif kamal Pediatric Infectious Diseases, Consultant Liaquat National Hospital, Karachi.Sada Abbas, Assistant Manager, CRD helped with the designing of the guidelines.

CONTENTS
Case Definition
Diagnostic testing Prioritization
Personal Protective Equipment according to risk of COVID-19 for admitted patients
Categorization of the cases
Management of Patients with suspected/ confirmed COVID-19
Criteria for admission of COVID-19 suspected or confirmed patients
Quarantine and Isolation
Newborn Management
Annexures
1.
2.
3.
4.
5.
6.
7.
8.
9.

CASE DEFINITION OF A COVID-19 SUSPECT
PERSONAL PROTECTIVE EQUIPMENT ACCORDING TORISK OF COVID-19 FOR ADMITTED PATIENTS
May need revision as it is an evolving situation and we are now facing community transmission. Ideally every suspect based on the case definition should have a nasopharyngeal PCR for COVID-19 but as shortage of kits is a challenge, we can utilize kits according to the Tiers explained below:
Tier-1: High level of suspicion of COVID-19. Always test with a nasopharyngeal swab PCR.Tier-2: Low level of suspicion of COVID-19. Test with Nasopharyngeal swab only if there is strong physician suspicion. Usual strategy is home isolation until symptoms resolve with temperature charting. Ask to come again for re-assessment & NP swabbing, if spiking fevers or there is worsening in symptoms
Tier – 1: High level of suspicion of COVID-19
Known local transmission reported in place of residenceHistory of International travel in the last 14 daysHistory of close (15 minutes face to face contact within 1 month) or household contact with a confirmed or probable COVID-19 patientIn a patient who has daily or very frequent use of public transport associated with crowding, e.g. crowded busesIn a close (15 minutes face to face contact within 1 meter) or household contact with an asymptomatic international traveler
•••
•
•
••
Other Tier-1 Conditions:
Oncology patients (especially with low ANC less than 500) and the immunocompromised patients secondary to HIV, primary immunodeficiency.Children with chronic medical conditions who are on prolonged immunosuppressive therapy/ steroid more than 2 weeks.
•
•
•
Tier – 2: Low suspicion of COVID -19
History of inter-city travel in the last 14 daysClose (15 minutes face to face contact within 1 meter) or household contact with an asymptomatic domestic traveler
••
FEVER &COUGH/SOB
Non HCW
Patients
HCW
PERSON SITUATION NONE SURGICALMASK
N95MASK GLOVES GOWNS EYE
SHIELD
Caring for suspected/confirm patient
Suspected
Confirmed
In single room isolation
Taking care of suspected orconfirmed patient regardlessof need for suctioning
Collecting NP swab
While removing linen/waste
√
√
√
√
√√√
√√√√
√√√√
Fever or suspected respiratory infection with any of the following:
Fast breathing (in breaths/min): a. < 2 months: ≥ 60 b. 2–11 months: ≥ 50 c. 1–5 years: ≥ 40. Severe respiratory distress includes use of accessary muscles, nasal flaring, grunting in younger children Central cyanosisConfusion, agitation, restlessnessSpO2 ≤ 94% on room airBilateral or wide spread infiltrates on CXR or CXR suggestive of ARDSPaO2/FiO2 ratio less than 300 or Pa O2 less than 65 or Rising Pa Co2 General danger sign: inability to breastfeed or drink, lethargy or unconsciousness, or convulsions, excessive/inconsolable cry.Evidence of heart failure/ Myocarditis: Raised JVP, Gallop rhythm, hepatomegaly with or without the signs of shock
•
•••••••
•
Signs of shock: i. Tachycardia ii. Delayed capillary refill iii. Cold, clammy peripheries iv. Mottled skin v. Low Systolic BP … according to age vi. Urine output < 1 ml/kg/hr
SEVERE CASES
Found to have PCR +ve on respiratory secretions but having NO symptoms.
CATEGORIZATION OF THE CONFIRMEDCOVID-19 CASES
ASYMPTOMATIC CASES
Mild symptoms (low grade fever spikes with flu and cough) with no sign of pneumonia on CXR.
Patients with fever and respiratory symptoms, with a CXR showing signs of pneumonia or fulfilling criteria for admission due to other reasons e.g. high spiking fevers, excessive vomiting, dehydration etc. along with the respiratory symptoms.
Pneumonia cases showing signs of impending or established respiratory failure and/ or ARDS or having Gener-al danger signs ((Inability to feed, vomiting, lethargy, decrease in conscious level or unconsciousness, irritability, inconsolable cry, grunting)
MILD CASES
MODERATE CASES
CLINICAL CRITERIA
Bi-level (NIV or CPAP) ≥ 5 cmH2O via full face mask: PaO2/FiO2 ≤ 300 mmHg or SpO2/FiO2 ≤ 264Mild ARDS (invasively ventilated): 4 ≤ OI < 8 or 5 ≤ OSI < 7.5Moderate ARDS (invasively ventilated): 8 ≤ OI < 16 or 7.5 ≤ OSI < 12.3Severe ARDS (invasively ventilated): OI ≥ 16 or OSI ≥ 12.3
••••
Hemodynamically unstableHemodynamically stable but sick looking Sign and symptoms of pneumonia according to IMNCIDyspneaUnable to tolerate orallyProfuse vomiting or diarrhea DehydratedComplaining of decreasing urine outputListlessness/reluctance to feedImmunosuppressed (e.g. HIV, on long term steroids or immunosuppressive) Severe co-morbid: heart failure, congenital heart disease, decompensated liver disease, chronic lung disease, uncontrolled diabetes, CKD Developing superadded bacterial infection
1.2.3.4.5.6.7.8.9.10.11.
12.
Vitals: vitally unstable (R/R, H/R and BP chart is given below according to age)GCS < 15 General danger signs: lethargic, inconsolable cry, grunting, convulsionsCentral cyanosisDehydration Signs of shock: tachycardia, delayed capillary refill, cold, clammy skin, mottling Urine output < 1 ml/kg/hr. Abnormal chest findings: localized crepitation, decreased air entry, findings of effusion or wheezingSigns of heart failure (Tachycardia, raised JVP, edema, gallop rhythm, hepatomegaly)
•••••••••
SEVERE PNEUMONIAOnset: within 1 week of a known clinical insult or new or worsening respiratory symptoms.
Chest imaging (radiograph, CT scan, or lung ultrasound): bilateral opacities, not fully explained by volume overload, lobar or lung collapse, or nodules or the picture of ARDS
Origin of pulmonary infiltrates: respiratory failure not fully explained by cardiac failure or fluid overload. Need objective assessment (e.g. echocardiography) to exclude hydrostatic cause of infiltrates/edema if no risk factor present.
Oxygenation impairment in children: (references 1-3)
OI = Oxygenation Index and OSI = Oxygenation Index using SpO2. Use PaO2-based metric when available. If PaO2 not available, wean FiO2 to maintain SpO2 ≤ 97% to calculate OSI or SpO2/FiO2 ratio:
CRITERIA FOR ADMISSION OF COVID-19 SUSPECTED ORCONFIRMED PATIENTS

MANAGEMENT OF ASYMPTOMATIC CASES Can be managed in home isolation if minimum requirement of home isolation met.or Monitored institutional isolation (other than hospital) for a minimum of 14 days.Educate patient and their parents about symptoms and encourage to self-report if develops symptoms.Repeat NP PCR on day-14. If it is negative, break isolation. If NP PCR still positive on day-14, repeat NP PCR after another 5 days and break isolation if it is negative (appendix -1)
•
••
PLACEMENT
INVESTIGATIONS
MILD CASES MODERATE CASES
•
•
•
•
Should be placed in a single room, or cohorted with other positive patients, keeping a distance of 1 meter between beds.Contact and droplet precautions should be instituted.Can be sent for home isolation if minimum requirements of home isolation metIf home isolation requirements not met, can be isolated in institutions other than hospitals to decrease burden on health-care (appendix -1)
•
•
Should be placed in a single room, or cohorted with other positive patients in hospital, keeping a distance of 1 meter between beds.Contact and droplet precautions should be instituted
•••
Hydration (preferably orally)Paracetamol for fever (avoid NSAIDS)Antihistamines
(In case of oncology/immunosup-pressed first line antibiotics according to our institution protocol and for PCM or other chronic etiology add antibiotics according to physician advice)
••
••
HydrationOxygen saturation monitoring, oxygen therapy with nasal cannula (if needed)Paracetamol for fever (avoid NSAIDS)Consider treating as community acquired pneumonia (till Coronavirus RT-PCR results available) with beta-lact-am like Ampicillin or ceftriaxone in general population and Tazocin in oncology patients.
Once diagnosed as COVID pneumonia(if patient is not improving or worsening consult to ID physician)
DISCHARGECRITERIA
•
•
Retesting after resolution of symptoms or after 7 days of hospitalization whichev-er comes later (2 samples should be negative 24 hours apart) for the admit-ted patients. Improvement of symptoms and mother fully trained to take care at home in isolation and bring back after 14 days of completion to re-test.
•
•
••
•
Retesting after resolution of symptoms or after 7 days of hospitalization whichev-er comes later (2 samples should be negative 24 hours apart) for the admit-ted patientsLung imaging shows obvious improve-mentSpO2 >94% without assisted O2There are no comorbidities that require hospitalizationCaregiver is ready to look after the child at home
Note: If the patient has become asymp-tomatic after treatment but the swab is positive, the patient may be moved to home isolation

Recognize severe hypoxemic respiratory failure when a patient with respiratory distress is failing standard oxygen therapy and prepare to provide advanced oxygen/ventilator support.Endotracheal intubation should be performed by a trained and experienced provider using airborne precautions.Give empiric antimicrobials to treat suspected pathogens (preferably based on ID decisions)Do not give high-dose systemic corticosteroids or other adjunctive therapies for viral pneumonitis outside the context of clinical trialsIt is crucial to minimize the risk of aerosol generating events/procedures during airway management and take proper PPE if these procedures are necessary
•
•
••
•
Following are the Aerosol generating events during airway management:
SUGGESTED TREATMENT PROTOCOL FOR COVID-19 ARDS
AEROSOL GENERATING EVENTS
Coughing/sneezingNIV or positive pressure ventilation with inadequate seal*High flow nasal oxygen (HFNO)Delivery of nebulized/atomized medications via simple face maskCardiopulmonary resuscitation (prior to intubation)Tracheal suction (without a closed system)Tracheal extubation
•••••••
PROCEDURES VULNERABLE TO AEROSOL GENERATION
LaryngoscopyTracheal intubationBronchoscopy/GastroscopyFront-of-neck airway (FONA) procedures (including tracheostomy, cricothyroidotomy)
••••
THE FOLLOWING RECOMMENDATIONS PERTAIN TO MECHANICALLYVENTILATED PEDIATRIC PATIENTS WITH ARDS:
Implement mechanical ventilation using lower tidal volumes (4–8 mL/kg predicted body weight, PBW) and lower inspiratory pressures (plateau pressure < 30 cmH2O).
Use a conservative fluid management strategy for ARDS patients without tissue hypo perfusion. The main effect is to shorten the duration of ventilation. In patients with moderate or severe ARDS, higher PEEP instead of lower PEEP is suggested.In patients with moderate-severe ARDS (PaO2/FiO2 < 150), neuromuscular blockade by continuous infusion should not be routinely used.Avoid disconnecting the patient from the ventilator, which results in loss of PEEP and atelectasis.Use in-line catheters for airway suctioning and clamp endotracheal tube when disconnection is required (for example, transfer to a transport ventilator).
In children, a lower level of plateau pressure (< 28 cmH2O) is targeted, and lower target of pH is permitted (7.15–7.30). Tidal volumes should be adapted to disease severity: 3–6 mL/kg PBW in the case of poor respiratory system compliance, and 5–8 mL/kg PBW with better preserved compliance
1.
2.
3.4.
5.6.

Admit the patient to airborne isolation with strict PPE Give empiric antimicrobials to treat suspected pathogens (preferably based on ID decisions)In addition to other supportive measures, consider the following if no contra-indications (preferably early in course of illness <= 12th day) after COVID confirmation.If patient is not improving or getting worse then consult to ID Physician for further management.
•••
•
TREATMENT PROTOCOL FOR COVID-19SEVERE PNEUMONIA/ARDS
Separation and restriction of movement of the child who are exposed to a patient with COVID-19 to see whether they develop the infection. Quarantine may be at home or in a facility. Duration: 14 days.
•
•
QUARANTINE AND ISOLATION OF COVID SUSPECTS
DISCHARGE CRITERIA FOR SEVERE CASES
Retesting after resolution of symptoms or after 7 days of hospitalization whichever comes later (2 samples should be negative 24 hours apart) for the admitted patients No respiratory distress at rest, R.R < 30/minuteImprovement of respiratory symptomsLung imaging shows obvious improvementSpO2 >94% without assisted O2There are no comorbidities that require hospitalization
Note: If the patient has become asymptomatic after treatment symptoms but the swab is positive, the patient may be moved to home isolation.
•
•••••
Child must stay at home.Stay in a well-ventilated single room.Child should not be allowed to mingle with other children. Playing with other children should not be allowed.Eating with other children should be prohibited.Avoid gatherings and crowded spaces. Maintain a distance of at least 1 meter with family members.Perform hand hygiene frequently.Alcohol-based hand rubs can be used if hands are not visibly soiled. Use soap and water when hands are visibly soiled.
Recommendations for child under quarantine
It is difficult to isolate the child especially difficult for younger children but best way to avoid the spread in other people is isolation. Older children can easily follow the parents’ instructions.
•
QUARANTINE FACILITY LEVEL
Quarantine is used to separate and restrict the movement of well person who may have been exposed to a communicable disease to see if they become ill.
HOME QUARANTINE
Tab/SypChloroquinephosphate
10 mg/kg base stat Then 5 mg/kg base once a day
7 to 10 days GI disturbance, blurring of vision, , blood dyscrasias, headache, Cardiovascular collapse, skin reaction
G6PD deficiency, known hypersensitivity
DOSE DURATIONDRUG CONTRAINDICATIONADVERSE EFFECTS

Separation of patients infected with proven or suspected COVID-19 to prevent the spread of the infection. Isolation may be at home or in the hospital.
•
ISOLATION OF PROBABLE OR CONFIRMED COVID PATIENTS
GUIDELINES FOR HOSPITAL ISOLATION
Patients will be isolated in COVID Unit at TIH Korangi campus or other dedicated isolation areas in other INH hospitals where droplet and airborne transmission risks can be minimized.Single room is preferred.If not available, patients can be cohorted together in a dedicated ward. Maintain at least 1-meter distance between patients.Ensure either single-use or disposable or dedicated equipment (e.g. stethoscopes, blood pressure cuffs, and thermometers).If equipment needs to be shared, clean and disinfect it between use for each patient (e.g. by using ethyl alcohol 70%).Staff taking care of these patients should strictly observe contact and air-borne precautions.If negative pressure isolation is not available (as in our set up) then place in a room with ample ventila-tion. Do not place patient in a room in which air is recirculated (e.g. centrally air-conditioned area without special air handling).Ensure adequate environmental cleaning consistently and correctly.Manage laundry, food service utensils and medical waste in accordance with safe routine procedures.Avoid moving and transporting patients out of their room or area unless medically necessary.
•
••
•
•
••
•••
ISOLATION DISCONTINUATION
Patients can be moved out of isolation only when symptoms improve AND two consecutive swabs (sent one day apart) are negative.If the patient has become asymptomatic after treatment but the swab is positive, the patient may be moved to home isolation.
•
•
All healthcare workers must take the following precautions when entering the room/ward.•
Use designated portable X-ray equipment and/or other designated diagnostic equipment, whenever possible. If transport is required, use predetermined transport routes to minimize exposure for staff, other patients and visitors. The patient should use a medical mask during transport.Ensure that HCWs who are transporting patients perform hand hygiene and wear appropriate PPE.Notify the area receiving the patient of any necessary precautions as early as possible before the patient’s arrival.
Wear an N-95 mask at all times during patient care.Observe STRICT hand hygiene.Avoid touching eyes or the mask.Wear clean, long sleeve non-sterile gowns.Remove PPE before leaving the room/ward and immediately perform hand hygiene.Wear an N-95 mask at all times during patient care.

GUIDELINES FOR HOME ISOLATION:
Those with a separate room to stay in.Those with mild or asymptomatic disease.Mother or caretaker ready to take care at home safely.
•••
INDICATIONS
Home Isolation may be considered in the following patients:
Place the patient in a well-ventilated single room (i.e. with open windows and an open door). Limit the number of caregivers just mother or father.Child should not be allowed to mingle with other children. Playing with other children should not be allowed. Eating with other children should be prohibited.Limit the movement of the patient in the house and minimize shared space.Household members should stay in a different room. Ideally, assign one person who is in good health with no underlying chronic or immunocompromising conditions. Visitors should not be allowed until the patient has completely recovered and has no signs and symp-toms. Perform hand hygiene after any type of contact with patients or their immediate environment.
••••••••
•
•
A medical mask should be provided to the patient and worn as much as possible. Mouth and nose should be covered with a disposable paper tissue when coughing or sneezing and discarded after use.
••
GUIDELINES FOR HOME ISOLATION
Hand hygiene should also be performed before and after preparing food, before eating, after using the toilet and whenever hands look dirty. If hands are not visibly dirty, an alcohol-based hand rub can be used.For visibly dirty hands, use soap and water.When washing hands with soap and water, it is preferable to use disposable paper towels to dry hands. If these are not available, use clean cloth towels and replace them when they become wet. The patient must use their own towel.
CAREGIVERS
Should wear a surgical mask that covers their mouth and nose when in the same room as the patient. Masks should not be touched or handled during use. If the mask gets wet or dirty from secretions, it must be replaced immediately with a new clean, dry mask. Remove the mask using the appropriate technique – that is, do not touch the front, but instead untie it. Discard the mask immediately after use and perform hand hygiene. Avoid direct contact with body fluids, particularly oral or respiratory secretions, and stool. Use disposable gloves and a mask when providing oral or respiratory care and when handling stool, urine and other waste. Perform hand hygiene before and after removing gloves and the mask. Do not reuse masks or gloves. Use dedicated linen and eating utensils for the patient.Items should be cleaned with soap and water after use and may be re-used instead of being discarded. In the room where the patient is being cared for, clean and disinfect daily surfaces that are frequently touched, such as bedside tables, bedframes and another bedroom furniture. Regular household soap or detergent should be used first for cleaning, and then, after rinsing, regular household disinfectant containing 0.5% sodium hypochlorite (i.e. equivalent to 5000 pm or 1-part bleach to 9 parts water) should be applied.
•••
•
••
•••••
•

COVID-19 infection during pregnancy still not clear and we don’t have any evidence of vertical transmission. Newborns suspected of Covid-19 infection are those newborns born to the mothers with a history of infection between 14 days before delivery and 28 days after delivery, or the newborns directly exposed to Covid-19 positive case.
At the time of birth designated member of the neonatal team should be assigned to attend suspected / confirmed COVID-19 deliveries. It is important that the most senior person likely to be required attends in the first instance, to minimize staff exposure.Neonates should be transferred in a closed incubator. Where possible, all procedures and investiga-tions should be carried out in the single room with a minimal number of staff present.Babies requiring admission to the NICU/Neonatal unit should be assessed in a designated area by an appropriately skilled neonatal team member wearing PPE.Breastfeeding will be encouraged through supporting mothers who have been separated from their baby to express milk (EBM). Keep the baby in NICU If the mother is sick and baby need to separate from the mother, test the baby and observe for at least 24 hours if remains well and test is negative then discharge home. It is not yet clear whether COVID-19 can be transferred via breast milk.
•
•
•
•
NEWBORN MANAGEMENT
Clean and disinfect bathroom and toilet surfaces at least once daily.Regular household soap or detergent should be used first for cleaning, and then, after rinsing, regular household disinfectant containing 0.5% sodium hypochlorite should be applied.
••
CAREGIVERS
Clean the patient’s clothes, bed linen, and bath and hand towels using regular laundry soap and water or machine wash at 60–90 °C with common household detergent, and dry thoroughly. Place contaminated linen into a laundry bag. Do not shake soiled laundry and avoid contaminated materials coming into contact with skin and clothes. Gloves and protective clothing (e.g. plastic aprons) should be used when cleaning surfaces or handling clothing or linen soiled with body fluids. Perform hand hygiene before and after removing gloves.Gloves, masks and other waste generated during at-home patient care should be placed into a waste bin with a lid in the patient’s room before being disposed of as infectious waste. Avoid other types of exposure to contaminated items from the patient’s immediate environment (e.g. do not share toothbrushes, cigarettes, eating utensils, dishes, drinks, towels, washcloths or bed linen).

NEONATALMANAGEMENT FORNEONATE WITHSUSPECTED ORCONFIRMEDCOVID-19EXPOSURE
Infant born to Mother with Confirmed or Suspected COVID-19
Resuscitation in labor room Resuscitate as per NRP
Transport from Labor room or in closed incubator
CONTACT DROPLET PRECAUTIONS with N95 mask as required for aerosol generating medical procedures. Staff to wear Personal Protective
Equipment (N95 mask, reflective face shield/goggles, gown and gloves)
Always have mother perform hand hygiene and wear a surgical mask before holding infant until mother is known to be negative for COVID-19.
WELL BABY
Mother COVID-19NEGATIVE
Mother COVID-19 POSITIVE
DiscontinueDroplet/Contact
Precautions.ROUTINE
Newborn Care
Mother COVID-19NEGATIVE
Newborn COVID-19NEGATIVE
Routine NICU careTreatment of
underlying disease
Mother COVID-19POSITIVE
Newborn COVID-19POSITIVE
Droplet/Contact Precautions for14 days while in NICU If well DCwith mother on Droplet/Contactprecautions at home All newbornwith COVID +ve mother if neededto be seen in ER, they shouldbe seen in Clinic-3
NewbornCOVID-19 POSITIVE
Consult: ID specialist Droplet/ContactPrecautionsuntil dischargefrom hospital Further follow-upfor COVID-19 +venewborn will bedirected as per ID
Newborn testing forPCR COVID-19 -NPS
Newborn COVID-19NEGATIVE
Newborn COVID-19POSITIVE
Admit to COVID-19 isolation Unit.DROPLET/ CONTACT PRECAUTIONS
Monitoring for symptoms- Vital Signs per shiftCan breastfeed with surgical mask
ROOMING TOGETHER ON COVID-19 ISOLATION UNIT AT 1ST FLOOR Droplet/Contact Precautions if remains in hospital Mother CAN breastfeed with mask Can be discharged home as per routine with discharge instructions and danger signs.If baby is negative then repeat testing for the baby after 2 to 3 or after 14th days of completion of mother isolationAll newborn with COVID +ve mother or baby needed to be seen in ER, they should be seen in Clinic-3 with Droplet/Contact precautions.
•••
•
•
ADMIT TO NEONATAL ICUAdmit only in TWO Isolation rooms at 3rd floorDROPLET/CONTACT PRECAUTIONS Supportive Care, Treatment of underlying disease.Investigations: CBC, CRP, BCS, PCR COVID-19Chest X-ray Discuss feeding options with parents
SICK BABY
SYMPTOMATIC
Infant born to Mother with Confirmed or Suspected COVID-19 Or Exposed to Contact with Confirmed COVID-19 DROPLET/-CONTACT for the Staff Personal Protective Equipment (Gown,
Face mask, face shield, gloves)

1. Screening sites outside ER2. Referred from other hospital3. Unknown pnuemonia and Collapsed patients
1. Triage assessment2. Ask for COVID status
Sick
PositiveProven
SUSPECTEDDiagnosed Case
Stable
PositiveProven
Send toDedicated Facility
HomeIsolation
SUSPECTEDDiagnosed Case
Inform Local AuthorityAssessment for Home Isolation
Perform NPSSend to Home
Re-test with PCRat 24 hours
Re-test alsoNegetive
Admit in SuspectedIsolation Ward
Rist Stratly by ID
Stabilization & Testing
Home IsolationCriteria Not Met
Home IsolationCriteria Met
NegativeHigh Risk
Positive
Low Risk
Shift to ward ORto primary referral center
Inform FamilyAdvise home for 14 days
Re-test if symptomscompatible by
COVID-19 develop Admit & Manage in
COVID Isolation Unit
Annexure 1A: Pathway for the management of suspected & diagnosed COVID-19 patient at
The Indus Health Network
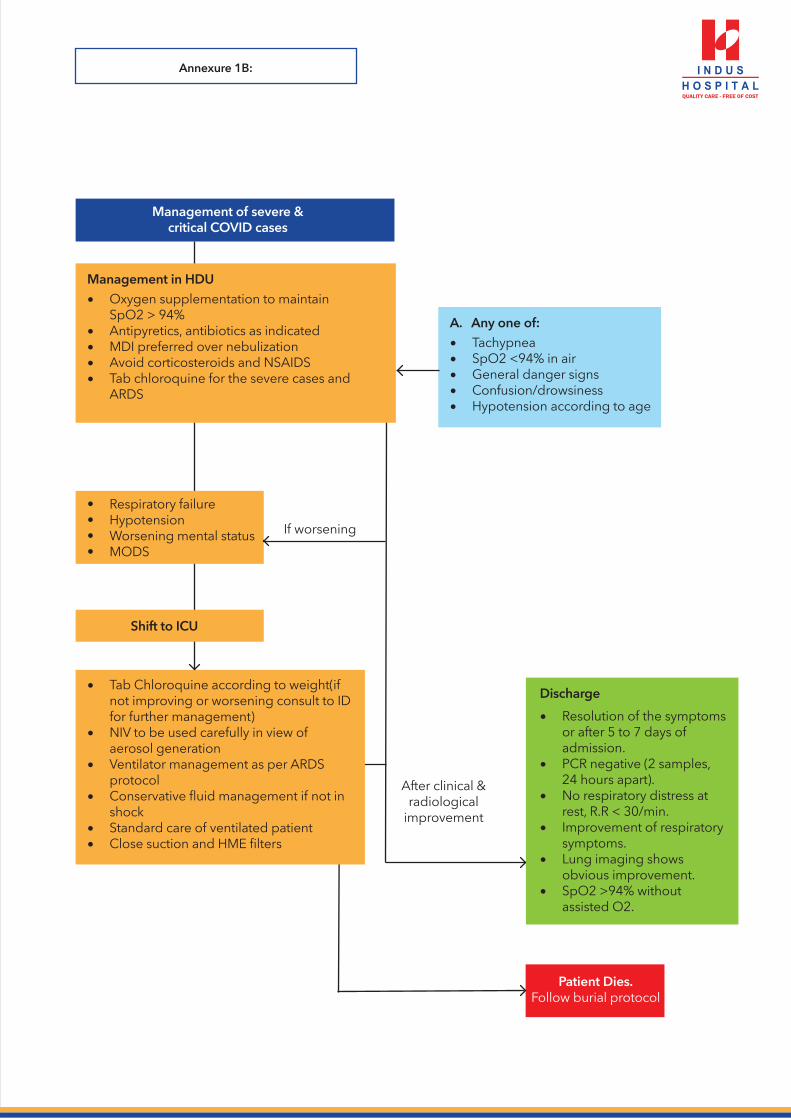
Management of severe &critical COVID cases
Annexure 1B:
Management in HDUOxygen supplementation to maintain SpO2 > 94%Antipyretics, antibiotics as indicatedMDI preferred over nebulizationAvoid corticosteroids and NSAIDSTab chloroquine for the severe cases and ARDS
•
••••
A. Any one of:TachypneaSpO2 <94% in airGeneral danger signsConfusion/drowsinessHypotension according to age
•••••
Tab Chloroquine according to weight(if not improving or worsening consult to ID for further management)NIV to be used carefully in view of aerosol generation Ventilator management as per ARDS protocolConservative fluid management if not in shockStandard care of ventilated patientClose suction and HME filters
•
•
•
•
••
Discharge
Resolution of the symptoms or after 5 to 7 days of admission.PCR negative (2 samples, 24 hours apart).No respiratory distress at rest, R.R < 30/min.Improvement of respiratory symptoms.Lung imaging shows obvious improvement.SpO2 >94% without assisted O2.
•
•
•
•
•
•
••••
Respiratory failureHypotensionWorsening mental statusMODS
Shift to ICU
After clinical &radiological
improvement
If worsening
Patient Dies.Follow burial protocol

Annexure 1C: Pathway of discontinuing isolation in COVID-19 patients
VITAL CHARTACCORDING TO AGE

Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020.
Children and Coronavirus Disease 2018 (COVID-19)-Centers for Disease Control and Prevention 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/prepare/children.html.
Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020; 579(7798):270-3.
Organization WH. Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected: Interim guidance V 1.2. 2020 [Available from: https://www.who.int/publications-detail/clinicalmanage-ment-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected.
Cortegiani A, Ingoglia G, Ippolito M, Giarratano A, Einav S. A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19. J Crit Care. 2020.
Evaluating and Testing Persons for Coronavirus Disease 2019 (COVID-19)-Centers for Disease Control and Prevention 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-crite-ria.html.
Wang L, Shi Y, Xiao T, Fu J, Feng X, Mu D, et al. Chinese expert consensus on the perinatal and neonatal management for the prevention and control of the 2019 novel coronavirus infection (First edition). Ann Transl Med. 2020;8(3):47-
Clean & Disinfect- Centers for Disease Control and Prevention 2020. Available from:https://ww-w.cdc.gov/coronavirus/2019-ncov/prepare/cleaning-disinfection.html.
1.
2.
3.
4.
5.
6.
7.
8.
REFERENCES