pediatric obesity and the early childhood obesity prevention collaborative presenters: jolene smith,...
TRANSCRIPT
Pediatric Obesity and the
Early Childhood Obesity Prevention Collaborative
Presenters:
•Jolene Smith, Executive Director, FIRST 5 Santa
Clara County
•Daniel Delgado, MD, FAAP
Pediatric Healthy Lifestyle Center,
Santa Clara County Health and Hospital System
•Jo Seavey-Hultquist, FIRST 5 Santa Clara County,
Performance Management Liaison
•Michelle Wexler, FIRST 5 Santa Clara County,
Performance Management Liaison
www.first5kids.org2
Why Should We Care About Pediatric Obesity?
• Daniels, SR. Future Child. 2006 Spring;16(1):47-67.
“the possibility has even been raised that the increasing prevalence and severity of childhood obesity may reverse the modern era's steady increase in life expectancy, with today's youth on average living less healthy and ultimately shorter lives than their parents-the first such reversal in lifespan in modern history. Such a possibility, he concludes, makes obesity in children an issue of utmost public health concern.”
www.first5kids.org3
Goals of Today’s Talk
• Clarify the extent of the obesity epidemic on a national & state level
• Educate on the health problems that pediatric obesity causes
• Clarify what the “epidemic” means on the front lines – at the patient level
• Not to scare you but call you to legislative action
www.first5kids.org4
Clarify the terms: a word about BMI & tracking an epidemic
• Body Mass Index: weight (kg) ÷ height (cm) ÷ height (cm) x 10,000
• BMI is a proxy for weight for height and overweight/obesity
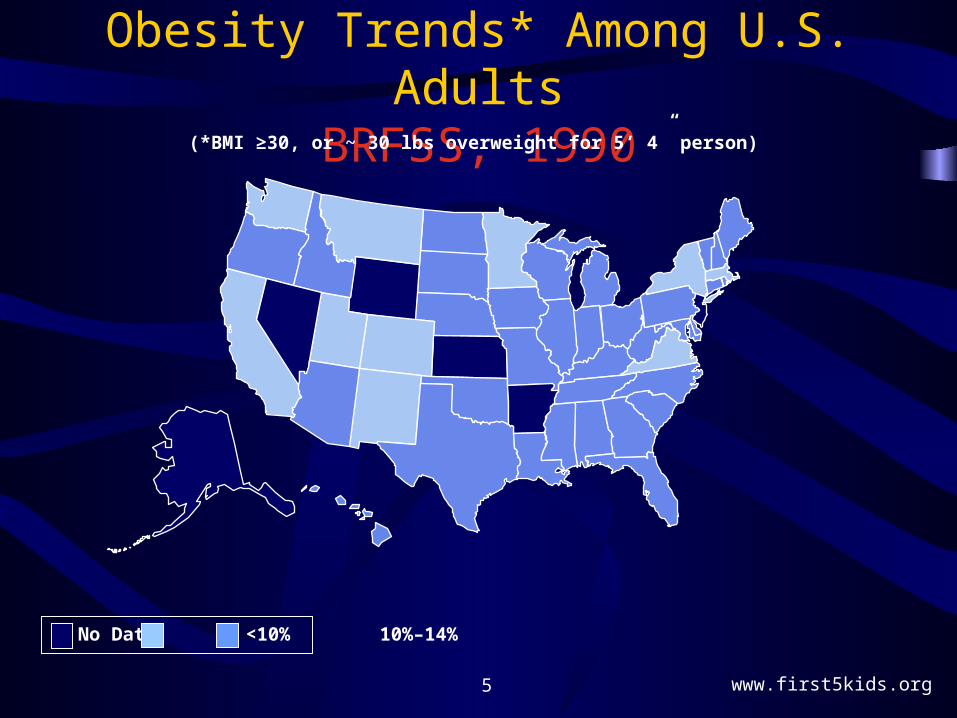
• In 1990, NO STATES had obesity prevalence rates above 20 percent
www.first5kids.org5
Obesity Trends* Among U.S. AdultsBRFSS, 1990
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14%
www.first5kids.org6
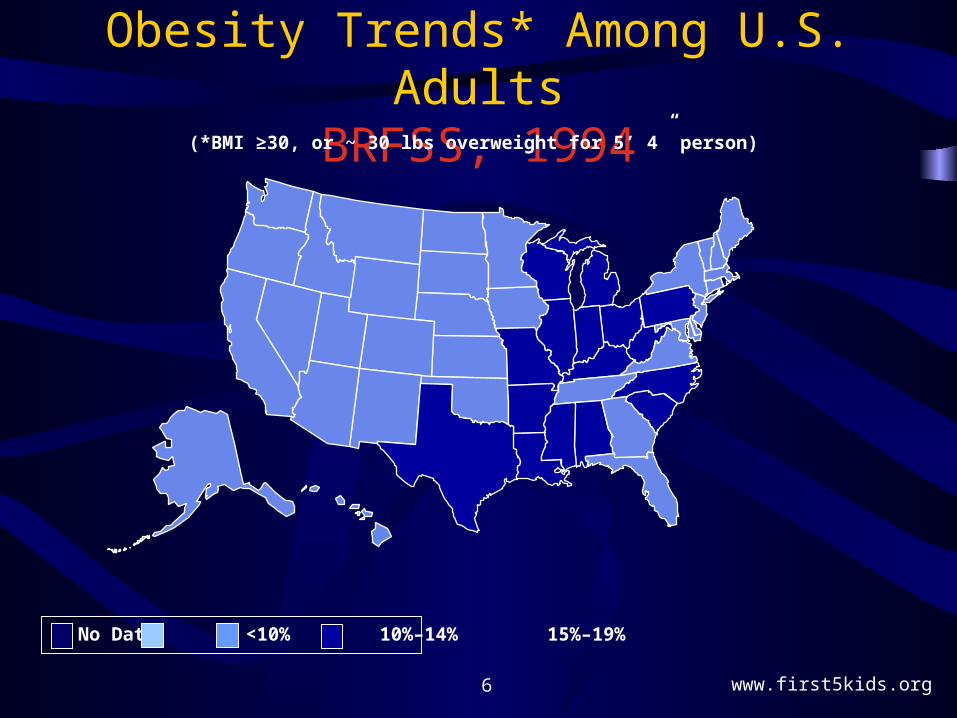
Obesity Trends* Among U.S. AdultsBRFSS, 1994
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%
www.first5kids.org7
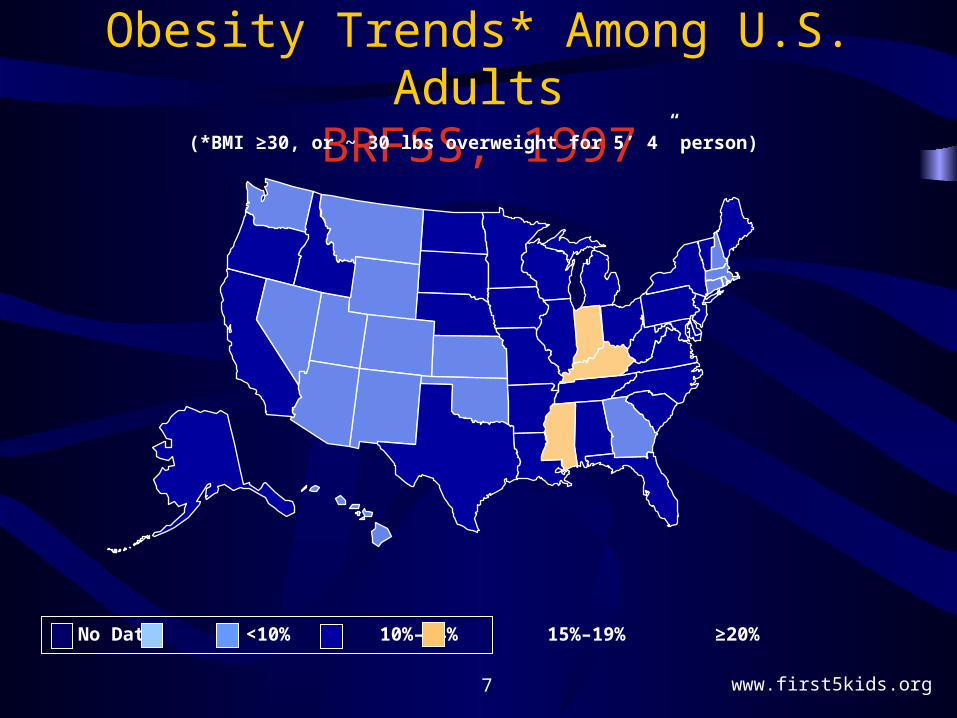
Obesity Trends* Among U.S. AdultsBRFSS, 1997
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% ≥20%
www.first5kids.org8
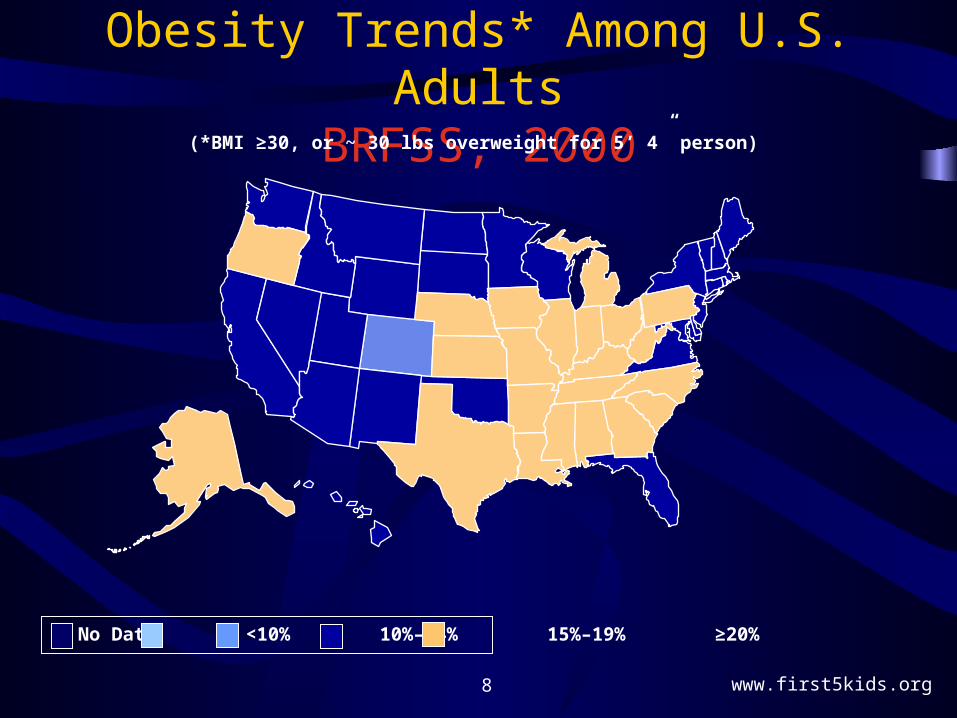
Obesity Trends* Among U.S. AdultsBRFSS, 2000
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% ≥20%
www.first5kids.org9
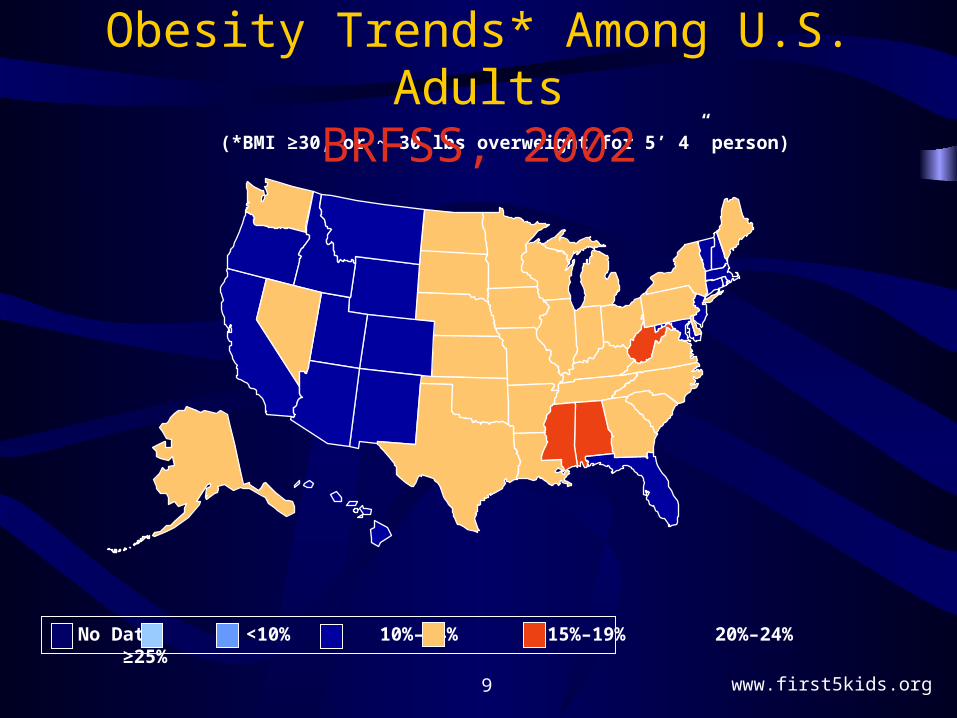
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
Obesity Trends* Among U.S. AdultsBRFSS, 2002
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%

www.first5kids.org10
Obesity Trends* Among U.S. AdultsBRFSS, 2005
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25 %–29% ≥30%
What about California children?
Data from Children’s Health and Disability Prevention (CHDP) - Pediatric Nutrition
Surveillance System (PedNSS)
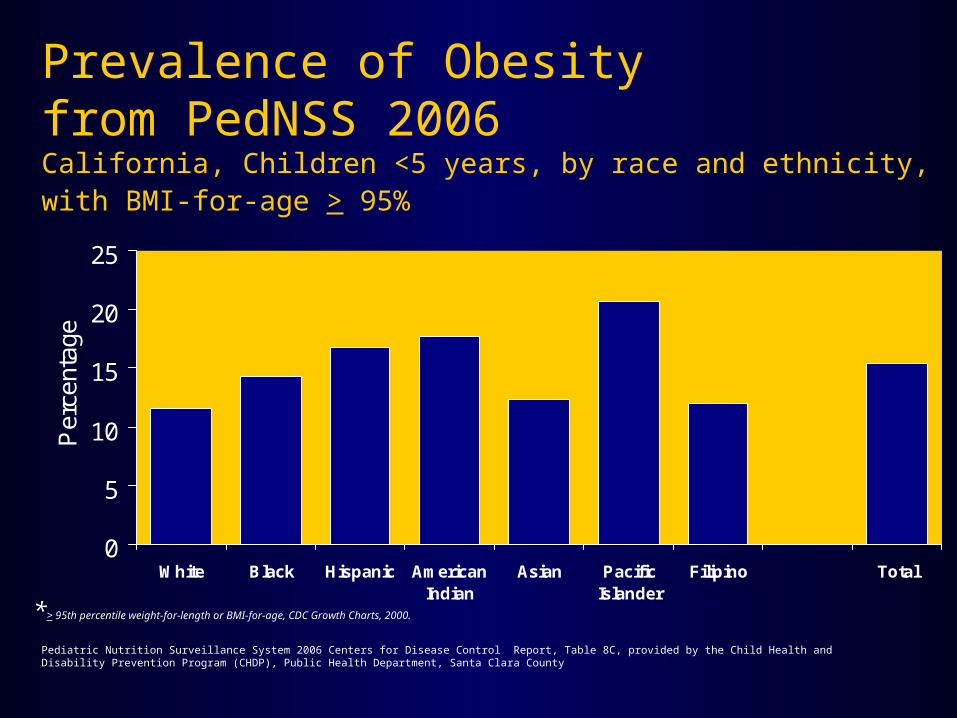
Prevalence of Obesityfrom PedNSS 2006California, Children <5 years, by race and ethnicity, with BMI-for-age > 95%
Pediatric Nutrition Surveillance System 2006 Centers for Disease Control Report, Table 8C, provided by the Child Health and Disability Prevention Program (CHDP), Public Health Department, Santa Clara County
0
5
10
15
20
25
White Black Hispanic AmericanIndian
Asian PacificIslander
Filipino Total
Per
cent
age
*> 95th percentile weight-for-length or BMI-for-age, CDC Growth Charts, 2000.
www.first5kids.org13
So do kids grow out of it?
• The NIH Institute of Child Health and Human Development Study of Early Child Care and Youth Development looked at 1042 healthy children in 10 locations
• Born in 1991, their growth reflects the secular trend of increasing overweight/obesity in the US population
www.first5kids.org14
So do kids grow out of it? NO!
• BMI > 85% once between 24-54 months old were 5 times more likely to be overweight at age 12
• 60% of overweight preschoolers were overweight at age 12
• 80% of overweight elementary school kids were overweight at age 12
• Pervasive message: prevention starts EARLY– Nader, PR, et al. Identifying Risk for Obesity in Early Childhood. Pediatrics 2006;
118: e594-e601
www.first5kids.org15
What does obesity mean for kids?
• Kids now present with adult disease states that were unheard of 10 years ago
• Seeing not only earlier progression to disease but also more severe disease
• Pediatric obesity effects current quality of life
www.first5kids.org16
Diseases seen in obese children
• Neurologic
– Headaches• Increased incidence
– Obstructive Sleep Apnea (OSA)• 90% of obese kids that snore have some component of OSA
• 50% of OSA children also have ADHD symptoms
• Many need tonsillectomies/adenoidectomies

www.first5kids.org17
Diseases seen in obese children
• Cardiovascular
– Obese kids (BMI >95%) have risk of hypertension (BP’s = 95% or above)
• 8% of 2-5 year olds• 11% of 6-10 year olds• 20% of 11-15 year olds• 20% of 16-19 year olds
– J. Pediatr. 2006; 148: 195-200.

www.first5kids.org18
Diseases seen in obese children
• Gastroenterologic
– Non-alcoholic Fatty Liver Disease (NAFLD)• Excess fat storage in liver (think foie gras)
• Is related to insulin resistance (certain ethnicities at risk)
• 38% of PHLC kids that had labs had elevated liver enzymes
– Non-alcoholic steatohepatitis (NASH)• Inflammation/scarring due to fatty liver
• Up to 20% of NASH may progress to cirrhosis
www.first5kids.org19
Diseases seen in obese children
• Endocrine Disorders
– Precocious Puberty• Treated as older by peers and family
– Polycystic Ovarian Syndrome• Infertility
– Insulin Resistance/Pre-diabetes• Irregular menses, liver dysfunction

www.first5kids.org20
Diseases seen in obese children
• Orthopedic
– Slipped Capital Femoral Epiphysis (SCFE)• Growth plate shears at the femur; leads to pinning
– Blount’s disease• Crushing of growth plate at knees
www.first5kids.org21
Diseases seen in obese children
• Psychologic/Psychiatric
– Depression
– Diminished self-esteem
– Eating disorders • Up to 50% of adults in self-help weight loss program had
findings of Binge Eating Disorder
www.first5kids.org22
Diseases seen in obese children
• Pulmonary
– Pulmonary hypertension• End result of untreated OSA, leads to right-sided heart failure
– Increased allergen sensitivity
– Asthma • Worse in both in incidence and severity
www.first5kids.org23
Could one disease lead to another?
• “Overweight kids in Harlem twice as likely to suffer from asthma” J of Urban Health
• Chicken or egg?– Overweight exposed to more allergens since
they spend more time indoors– Asthma kids less active to avoid flares and thus
gain weight
www.first5kids.org24
Could one disease lead to another?
• Sedentary lifestyle -> more allergen sensitivity
enlarged adenoids and tonsils
increased OSA/apnea -> morning sleepiness
less time to eat b-fast & increase in weight
ADHD symptoms -> more homework time
less play -> increase in weight -> worse asthma/allergies -> worse apnea
The downward spiral
www.first5kids.org25
The Pervasive Message?
• All organ systems are related!
• Obese children are complicated patients
• Pediatricians are ill-prepared to deal with these medical problems
www.first5kids.org26
Why Should We Care About Pediatric Obesity?
• Indeterminable cost to society in the future– Already needing to start kids on diabetes meds– Generic Metformin: $600-$1,200 per year– Echocardiograms, liver biopsies, sleep studies– It is all on the tax dollar
• Future issues of rationing care• Which diabetics should we dialyze?• Which NASH kids should get a liver transplant?
www.first5kids.org27
Typical day at the PLMC
• 8 y.o. (163 lb) & 10 y.o. (220 lb) Latina sisters, both insulin resistant (IR) and abnormal lipid panels
• 8 y.o. (105 lb) Latina, IR, no weight gain x 2 months, active now, says she’s happy
• 15 y.o (237 lb) Latina, IR, on metformin, 6 lb wt loss in 2 months
www.first5kids.org28
Typical day at the PLMC
• 6 y.o. (70 lb) Latina, acanthosis, labs pending• 12 y.o. (143 lb) Latina, IR, gained 10 lbs in 2
months, not ready to change lifestyle, started metformin at visit for borderline sugar
• 11 y.o. (180 lb) Latino, at charter school 7am-5pm everyday. 4 hours of PE a week. IR, fatty liver, metformin candidate
• 4 y.o. (55 lb) Latina, mom now concerned• 11 y.o. (121 lb) Filipina, Fam Hx diabetes, labs
pending, likely IR
www.first5kids.org29
Typical day at the PLMC
• 10 y.o. (150 lb) Latina, IR, mom diabetic, recently cut back soda
• 13 y.o. (181 lb) Latina, nl labs, + wt loss but frustrated not faster, poor body image
• 10 y.o. (155 lb) Latina, IR, OSA, likely NAFLD, liver US pending, metformin candidate
• 9 y.o. (121 lb) Latino, likely IR, labs pending, 4 hours of videogames every afternoon
www.first5kids.org30
Early Childhood Obesity Prevention Collaborative
• Co-Chaired by Dr. Daniel Delgado, and FIRST 5• Charged with developing a strategic plan that
incorporates interventions which will address the issue of early childhood obesity
• Sub-group: Policy Workgroup Chaired by Santa Clara County Supervisor Ken Yeager
• Generated ideas for policy approaches to early childhood obesity
www.first5kids.org31
Call to Action
Provide subsidies to small stores so that they can price healthier foods cheaper than unhealthy foods
Tax or fee on fast food sales and have the fee monies be used for obesity prevention programs
Advocate for health insurance plans to cover obesity prevention in clinical practice and breastfeeding/lactation services
Have preschool and child care licensing/ certification contingent upon meeting and implementing nutritional and physical activity guidelines
Create policies that regulate advertising/marketing of unhealthy foods to young children
Early Childhood Obesity Prevention Collaborative:Potential Legislative Strategies
www.first5kids.org32
Call to Action
Continued changes needed in school lunch offerings; re-do current nutritional guidelines
Junk Food Tax or even better “Diabetes Prevention Tax” on unhealthy foods (high fructose corn syrup)
Junk food-free school campuses Mandatory everyday PE in schools Mandatory play before homework in after-school programs Legislation so that insurance companies will pay for
obesity treatment/lifestyle modification visits; currently not a reimbursed visit
Examine legislation to mandate changes in medical education
Other School-Age Potential Legislative Strategies
www.first5kids.org33
Call to Action
Stop serving soda/high fructose corn syrup drinks at family functions
Soda = beer/tequila. It’s a drink for adults only. Have your kids play as soon as they get home &
before doing their homework, especially in winter Buy a kid a bike, not videogames Eat dinner as a family
Strategies for Change on a Personal Level
www.first5kids.org34
Contact Information
Jolene Smith, FIRST 5 (408) 260-3701
Dr. Dan Delgado,
Pediatric Healthy Lifestyle Center (408) 817-1406
Jo Seavey-Hultquist, FIRST 5 (408) 260-3720
Michelle Wexler, FIRST 5 (408) 260-3730