pediatric obesity: assessment, prevention, & · pdf filegenes include leptin, leptin...
TRANSCRIPT
PEDIATRIC OBESITY:ASSESSMENT, PREVENTION, &
TREATMENT
Selma Feldman Witchel, MD
Children’s Hospital of Pittsburgh of UPMC
disclosures
Ilene Fennoy, MD, MPHProfessor of Pediatrics
Columbia University, New York
Drugs and devices unapproved by the FDA will be discussed
I have no financial or other conflicts of interest
LEARNING OBJECTIVES
At the end of this activity, participants will be able to…
Define pediatric obesity
Recognize the many factors leading to obesity
Identify the co-morbidities associated with obesity
Evaluate the pedatric patient with obesity
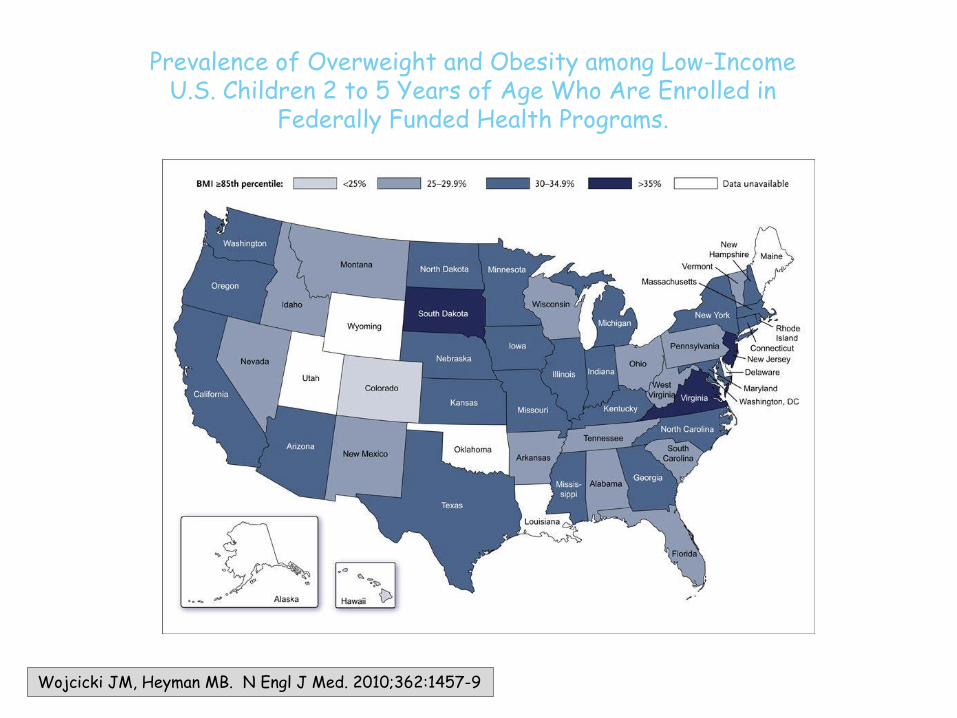
Wojcicki JM, Heyman MB. N Engl J Med. 2010;362:1457-9
Prevalence of Overweight and Obesity among Low-IncomeU.S. Children 2 to 5 Years of Age Who Are Enrolled in
Federally Funded Health Programs.
The Financial Costs of Childhood Obesity
• Incremental lifetime medical cost of an obese child relative to a normal weight child who maintains weight throughout adulthood: $16,310- $19, 350.
Finkelstein EA, et al. Pediatrics 2014;133:854
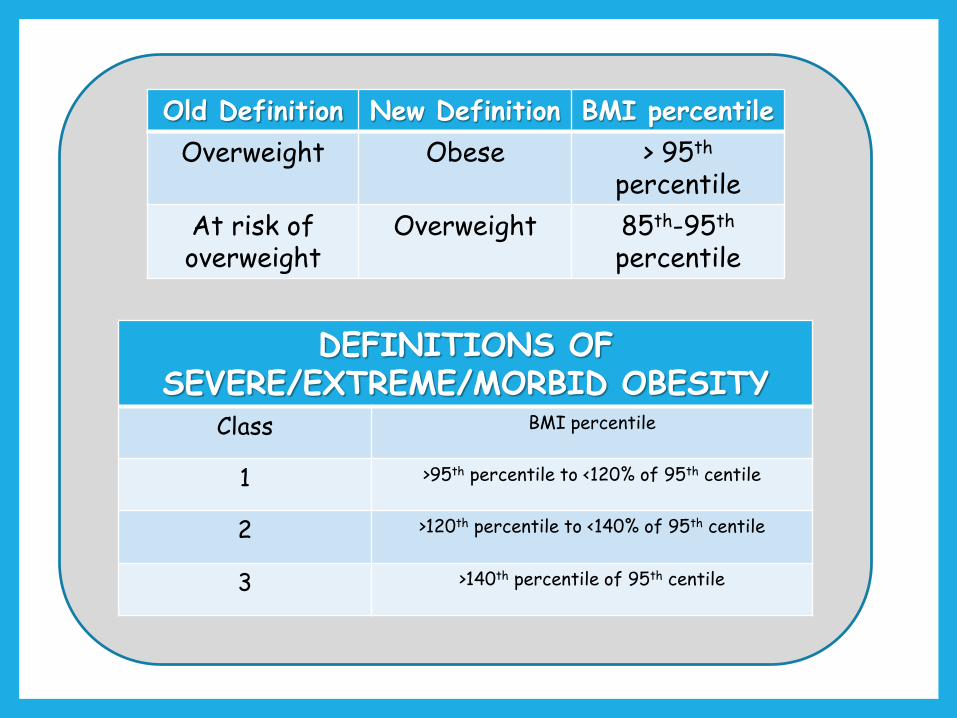
Old Definition New Definition BMI percentile
Overweight Obese > 95th
percentile
At risk of overweight
Overweight 85th-95th
percentile
DEFINITIONS OF SEVERE/EXTREME/MORBID OBESITY
Class BMI percentile
1 >95th percentile to <120% of 95th centile
2 >120th percentile to <140% of 95th centile
3 >140th percentile of 95th centile
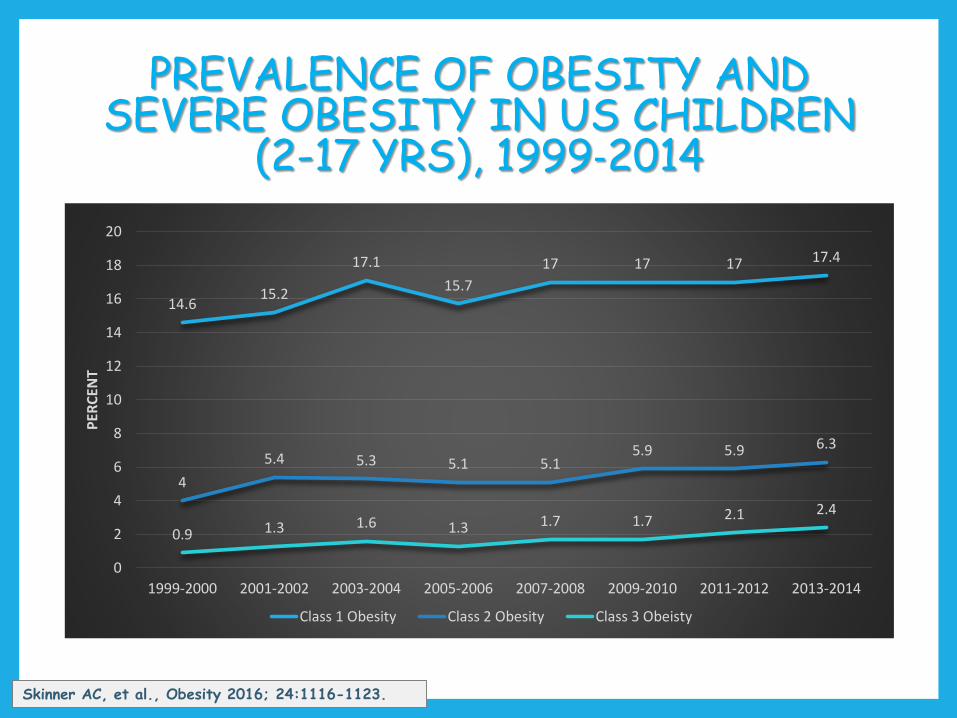
PREVALENCE OF OBESITY AND SEVERE OBESITY IN US CHILDREN
(2-17 YRS), 1999‐2014
14.615.2
17.1
15.7
17 17 17 17.4
4
5.4 5.3 5.1 5.15.9 5.9 6.3
0.9 1.3 1.6 1.3 1.7 1.7 2.1 2.4
0
2
4
6
8
10
12
14
16
18
20
1999-2000 2001-2002 2003-2004 2005-2006 2007-2008 2009-2010 2011-2012 2013-2014
PER
CEN
T
Class 1 Obesity Class 2 Obesity Class 3 Obeisty
Skinner AC, et al., Obesity 2016; 24:1116-1123.
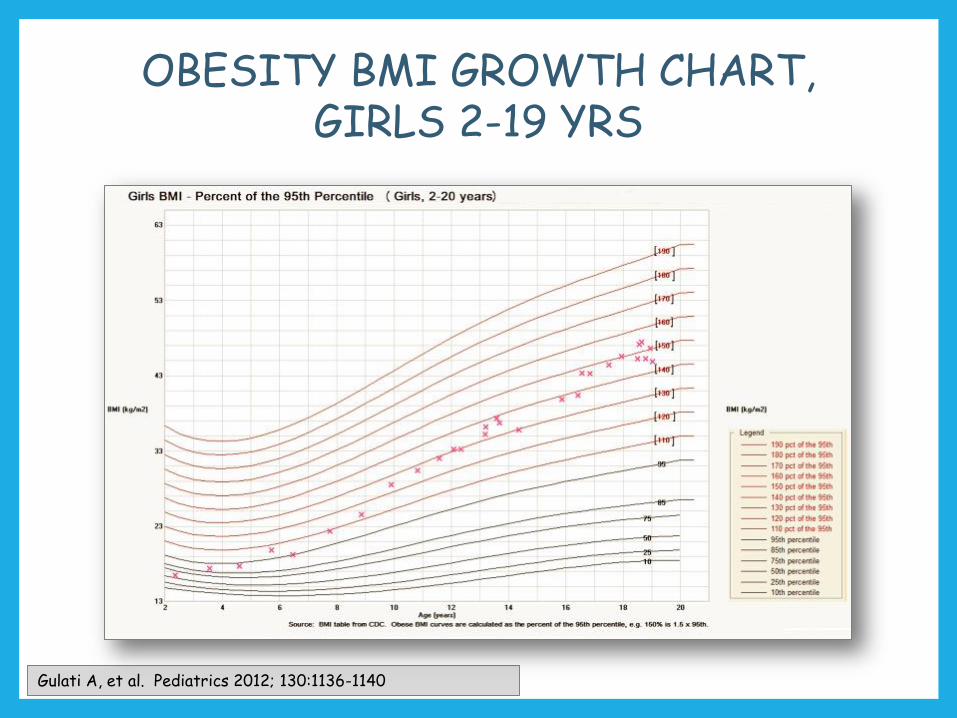
OBESITY BMI GROWTH CHART, GIRLS 2-19 YRS
Gulati A, et al. Pediatrics 2012; 130:1136-1140
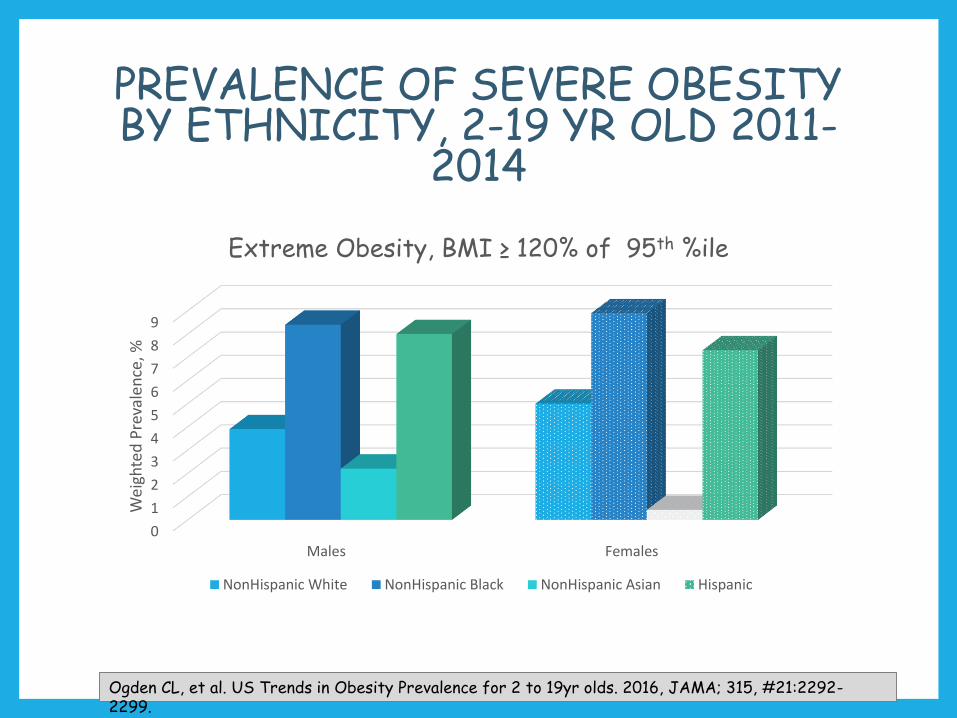
PREVALENCE OF SEVERE OBESITY BY ETHNICITY, 2-19 YR OLD 2011-
2014
0
1
2
3
4
5
6
7
8
9
Males Females
Wei
ghte
d P
reva
len
ce, %
Extreme Obesity, BMI ≥ 120% of 95th %ile
NonHispanic White NonHispanic Black NonHispanic Asian Hispanic
Ogden CL, et al. US Trends in Obesity Prevalence for 2 to 19yr olds. 2016, JAMA; 315, #21:2292-2299.
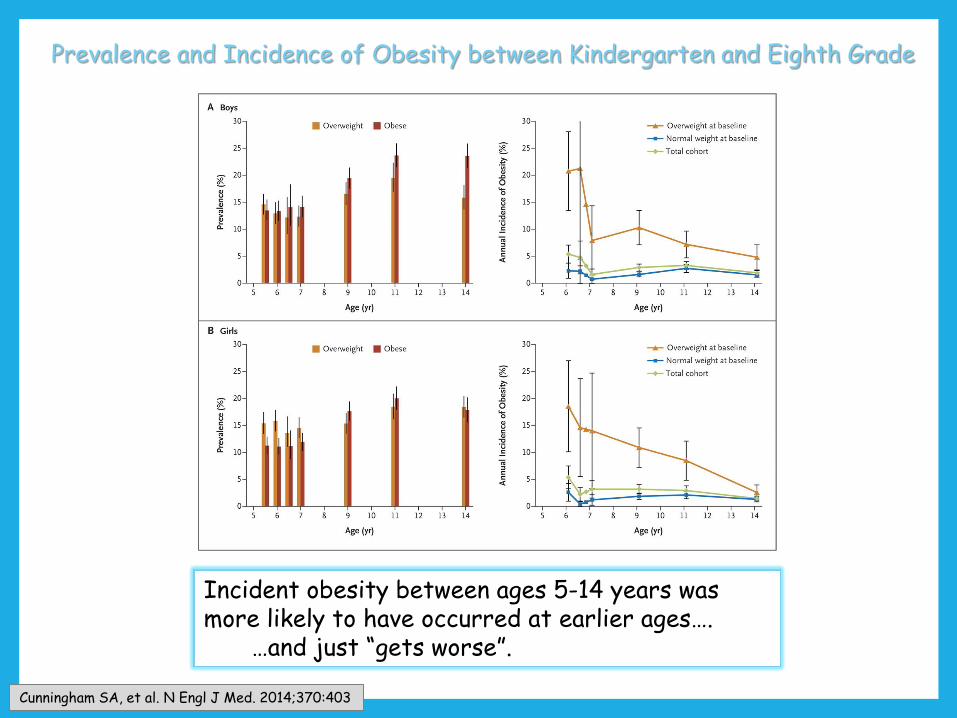
Prevalence and Incidence of Obesity between Kindergarten and Eighth Grade
Incident obesity between ages 5-14 years was more likely to have occurred at earlier ages….
…and just “gets worse”.
Cunningham SA, et al. N Engl J Med. 2014;370:403
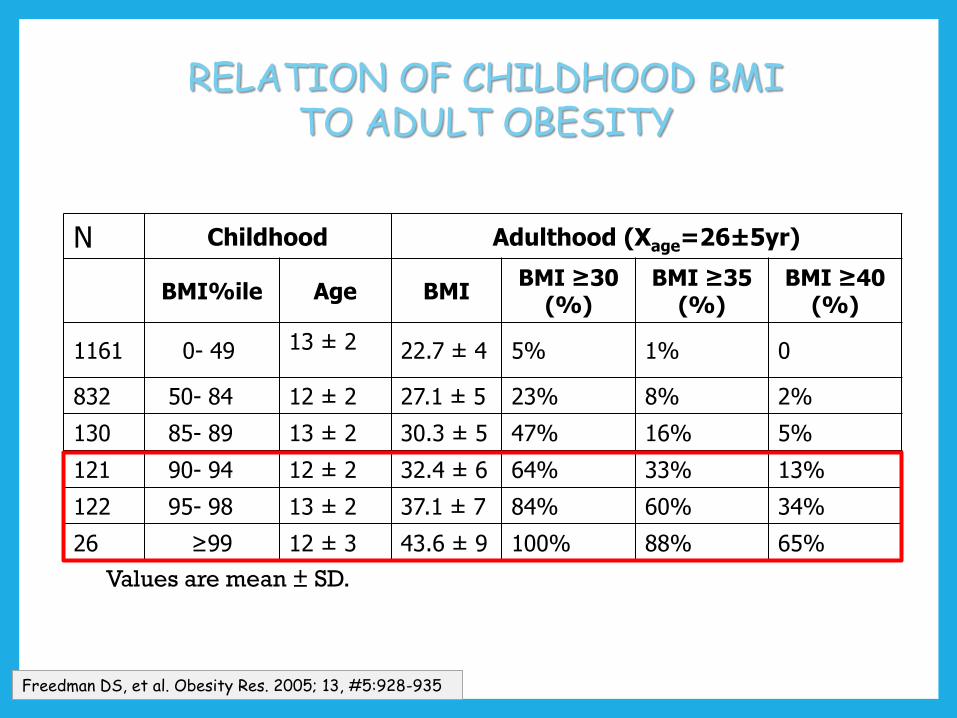
RELATION OF CHILDHOOD BMI TO ADULT OBESITY
Freedman DS, et al. Obesity Res. 2005; 13, #5:928-935
N Childhood Adulthood (Xage=26±5yr)
BMI%ile Age BMIBMI ≥30
(%)BMI ≥35
(%)BMI ≥40
(%)
1161 0- 49 13 ± 2 22.7 ± 4 5% 1% 0
832 50- 84 12 ± 2 27.1 ± 5 23% 8% 2%
130 85- 89 13 ± 2 30.3 ± 5 47% 16% 5%
121 90- 94 12 ± 2 32.4 ± 6 64% 33% 13%
122 95- 98 13 ± 2 37.1 ± 7 84% 60% 34%
26 ≥99 12 ± 3 43.6 ± 9 100% 88% 65%
Values are mean ± SD.
Risk Factors for Pediatric Obesity
Parental and family obesity
Increased intake of sugar-sweetened beverages, fast food, & processed food
Decreased physical activity
Increased screen time
Shorter sleep duration
Parental stress
Mother’s pre-pregnancy BMI & gestational weight gain
High birth weight and rapid infant weight gain
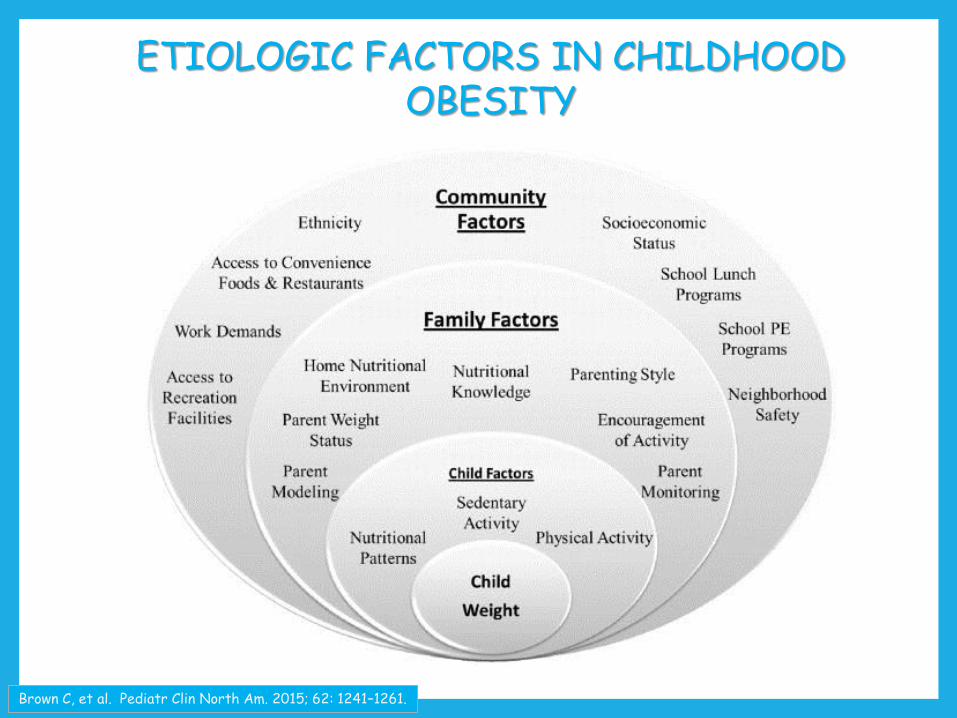
ETIOLOGIC FACTORS IN CHILDHOOD OBESITY
Brown C, et al. Pediatr Clin North Am. 2015; 62: 1241–1261.
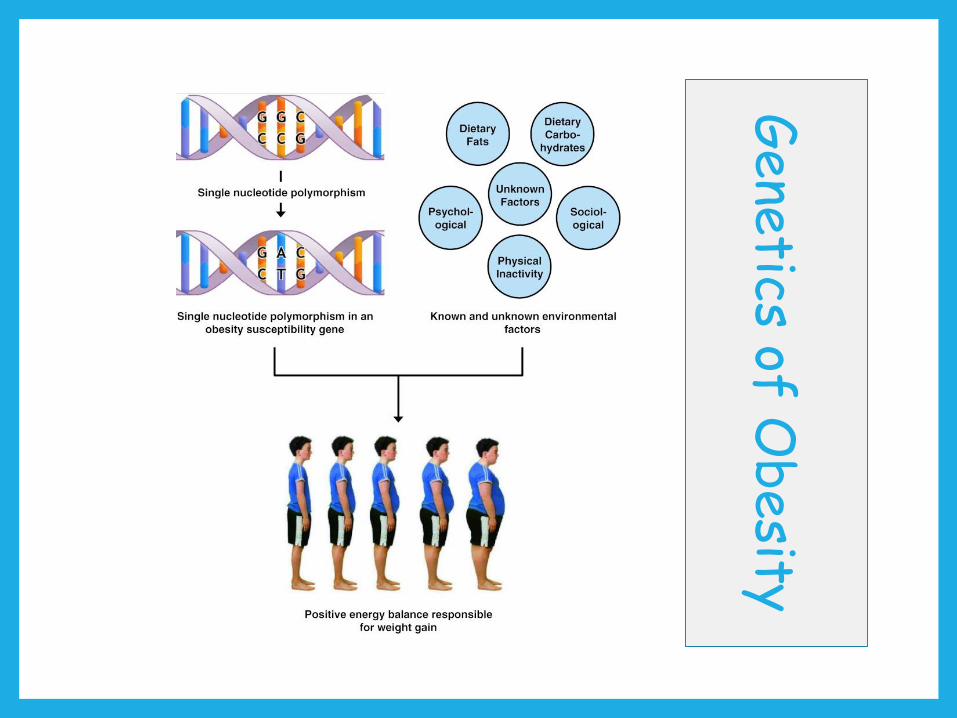
Gene
tics of Obesity
Hereditability of BMI is approximately 70%
Although monogenic obesity is rare, several genes have been associated with obesity.
Syndromes associated with obesity include Prader-Willi andBardet-Biedl Syndromes.
Genes include leptin, leptin receptor, & melanocortin 4 receptor.
Common phenotypic features include markedly increased appetite, reduced duration of satiety, & increased food-seeking behavior.
? Neurobehavioral effect
Venus of Willendorf~25,000 BCE
Obesity is not new disease
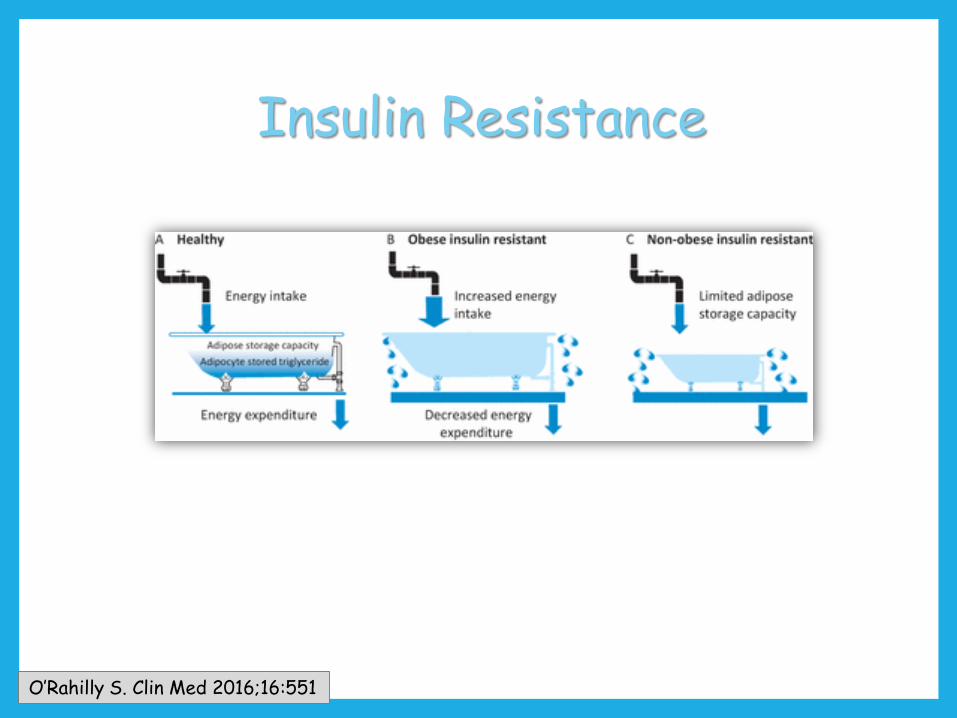
O’Rahilly S. Clin Med 2016;16:551
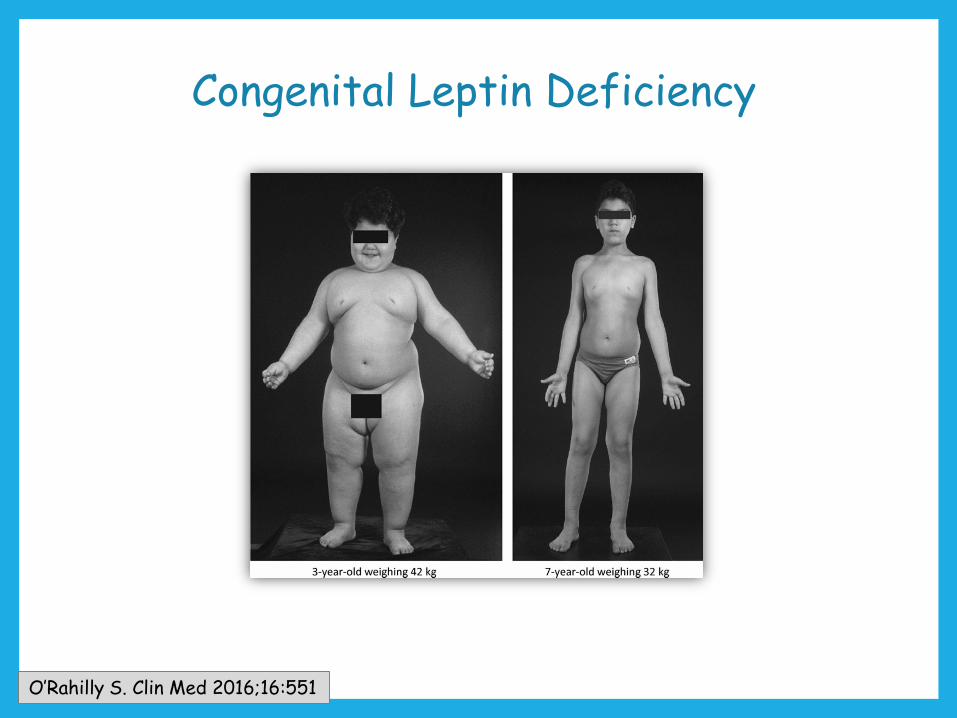
Congenital Leptin Deficiency
O’Rahilly S. Clin Med 2016;16:551

COMORBIDITIES ASSOCIATED WITH PEDIATRIC OBESITY
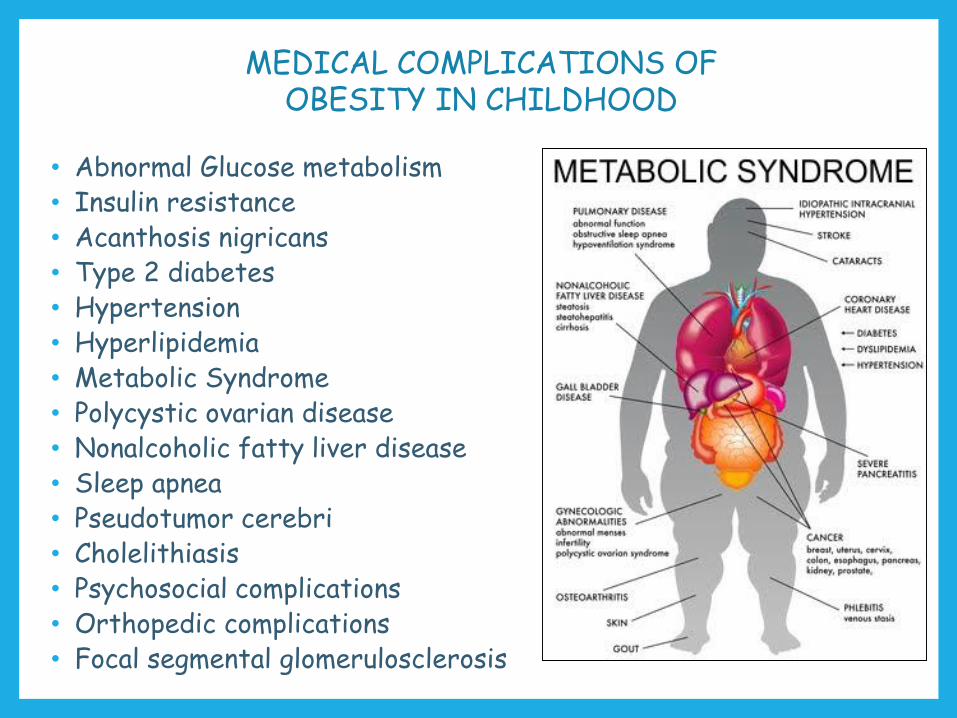
MEDICAL COMPLICATIONS OF OBESITY IN CHILDHOOD
• Abnormal Glucose metabolism• Insulin resistance• Acanthosis nigricans• Type 2 diabetes • Hypertension• Hyperlipidemia• Metabolic Syndrome• Polycystic ovarian disease• Nonalcoholic fatty liver disease• Sleep apnea• Pseudotumor cerebri• Cholelithiasis• Psychosocial complications• Orthopedic complications• Focal segmental glomerulosclerosis
0
5
10
15
20
25
30
35
Overweight Class 1 Obesity Class 2 Obesity Class 3 Obesity
Pre
vale
nce
(%
)
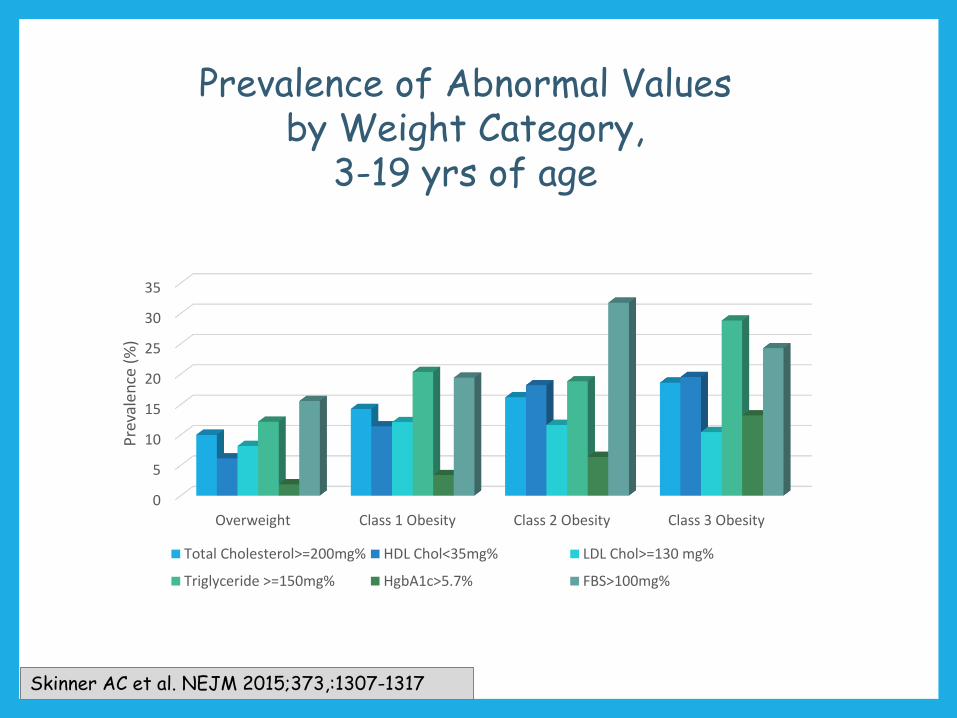
Total Cholesterol>=200mg% HDL Chol<35mg% LDL Chol>=130 mg%
Triglyceride >=150mg% HgbA1c>5.7% FBS>100mg%
Skinner AC et al. NEJM 2015;373,:1307-1317
Prevalence of Abnormal Values by Weight Category,
3-19 yrs of age
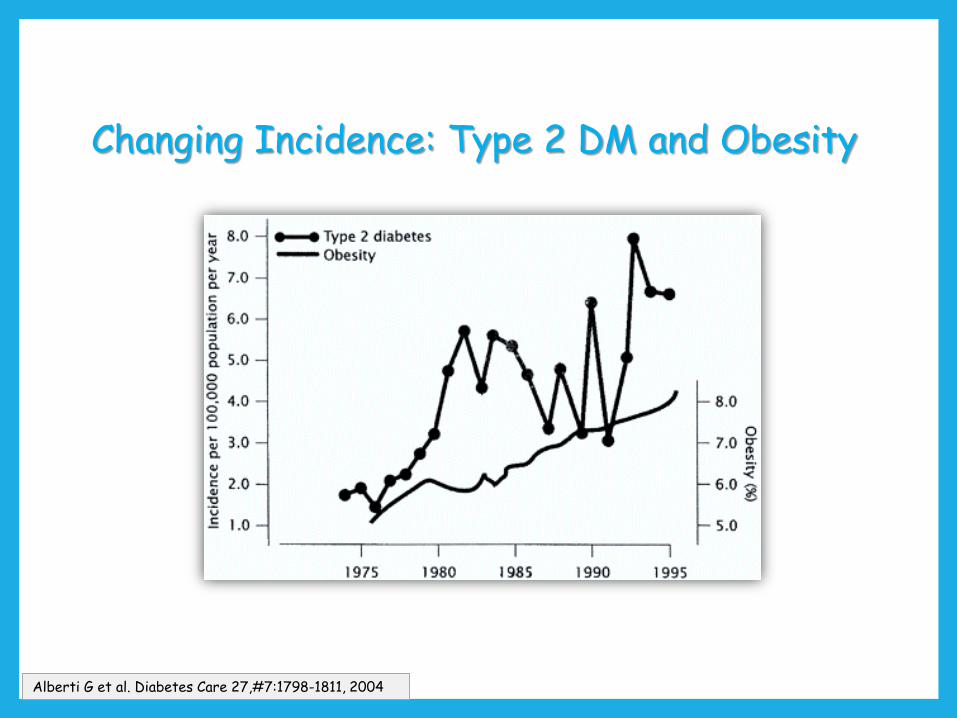
Changing Incidence: Type 2 DM and Obesity
Alberti G et al. Diabetes Care 27,#7:1798-1811, 2004
Polycystic Ovary Syndrome
Heterogeneous familial disorder characterized by hyperandrogenismand chronic anovulation.
In adolescent girls, persistent menstrual irregularity beyond 2 yearsafter menarche or primary amenorrhea with complete pubertymay suggest androgen excess
Insulin resistance and obesity are common features. But, theyshould not be used as diagnostic criteria for PCOS.
Witchel SF, et al. Horm Res Paediatr. 2015 Apr 1.Ibáñez et al. Horm Res Paediatr. (in press).
O’Rahilly S. Clin Med 2016;16:551
Insulin Resistance
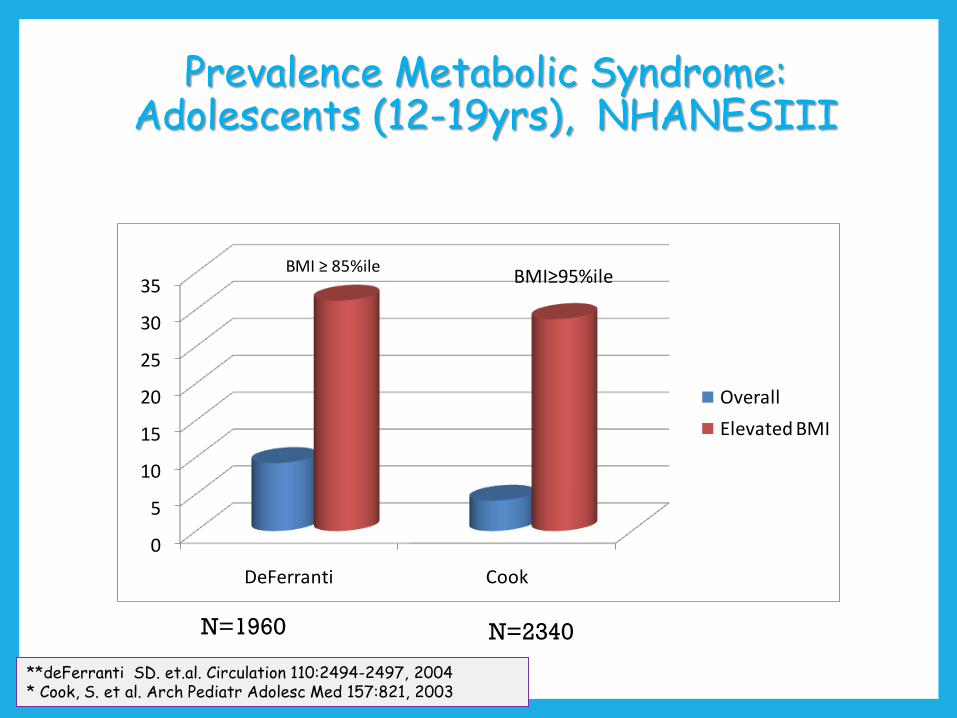
Prevalence Metabolic Syndrome: Adolescents (12-19yrs), NHANESIII
0
5
10
15
20
25
30
35
DeFerranti Cook
Overall
Elevated BMI
BMI≥95%ileBMI ≥ 85%ile
N=1960 N=2340
**deFerranti SD. et.al. Circulation 110:2494-2497, 2004* Cook, S. et al. Arch Pediatr Adolesc Med 157:821, 2003
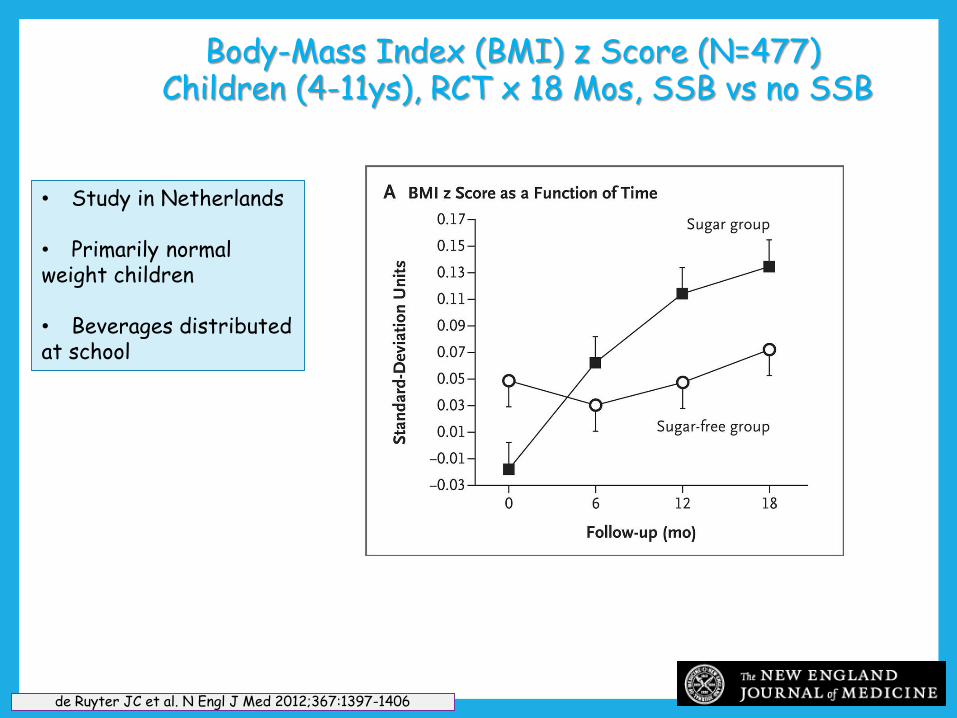
Body-Mass Index (BMI) z Score (N=477)Children (4-11ys), RCT x 18 Mos, SSB vs no SSB
de Ruyter JC et al. N Engl J Med 2012;367:1397-1406
• Study in Netherlands
• Primarily normalweight children
• Beverages distributedat school
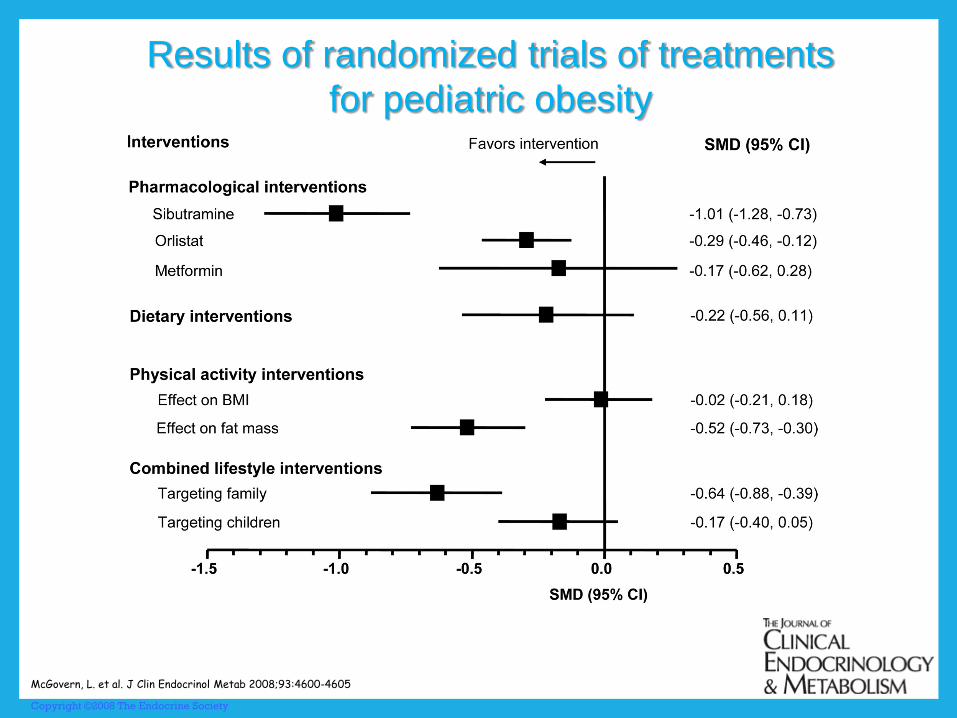
Copyright ©2008 The Endocrine Society
McGovern, L. et al. J Clin Endocrinol Metab 2008;93:4600-4605
Results of randomized trials of treatments
for pediatric obesity
Sibutramine resulted in a relevant increase in both systolic and diastolic pressure and was
withdrawn from the US market because of an increased risk of serious cardiovascular
events.
Metformin appears to have similar minimal weight loss effects as in adults and should only
be used in children aged ≥10 years.
Orlistat remains the only FDA–approved drug for treatment of childhood obesity for those
aged ≥12 years.
Rajjo T, et al J Clin Endocrinol Metab. 2017;102:763-775

Bariatric Surgery
Adjustable Gastric BandRoux-en-Y Gastric BypassSleeve Gastrectomy
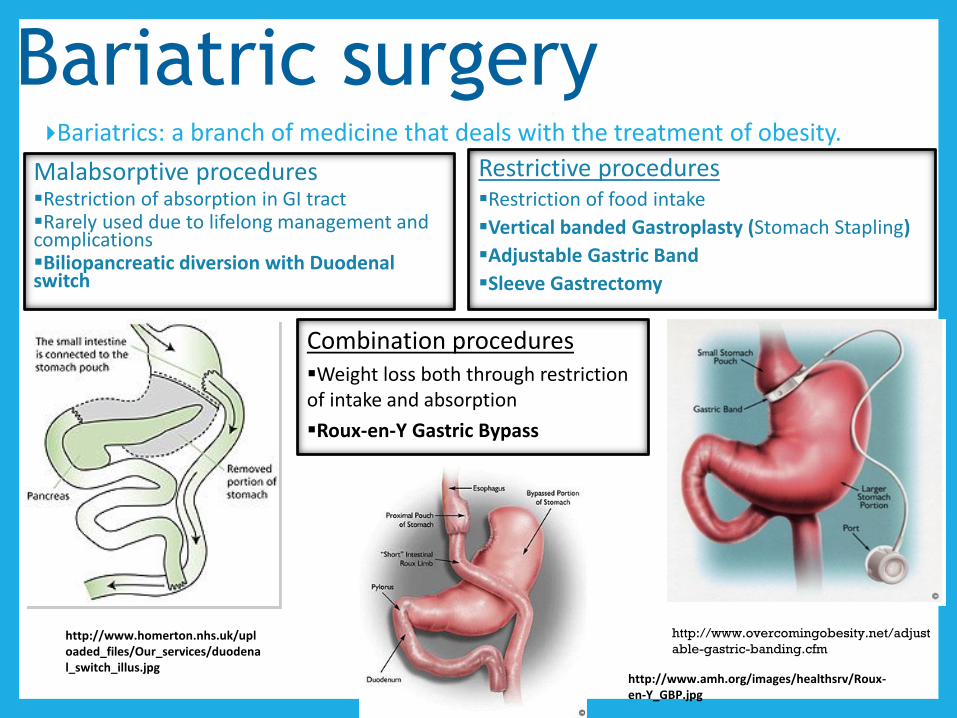
Bariatric surgeryBariatrics: a branch of medicine that deals with the treatment of obesity.
Malabsorptive proceduresRestriction of absorption in GI tractRarely used due to lifelong management and complicationsBiliopancreatic diversion with Duodenal switch
Restrictive proceduresRestriction of food intake
Vertical banded Gastroplasty (Stomach Stapling)
Adjustable Gastric Band
Sleeve Gastrectomy
Combination proceduresWeight loss both through restriction of intake and absorption
Roux-en-Y Gastric Bypass
http://www.homerton.nhs.uk/uploaded_files/Our_services/duodenal_switch_illus.jpg
http://www.amh.org/images/healthsrv/Roux-en-Y_GBP.jpg
http://www.overcomingobesity.net/adjust
able-gastric-banding.cfm
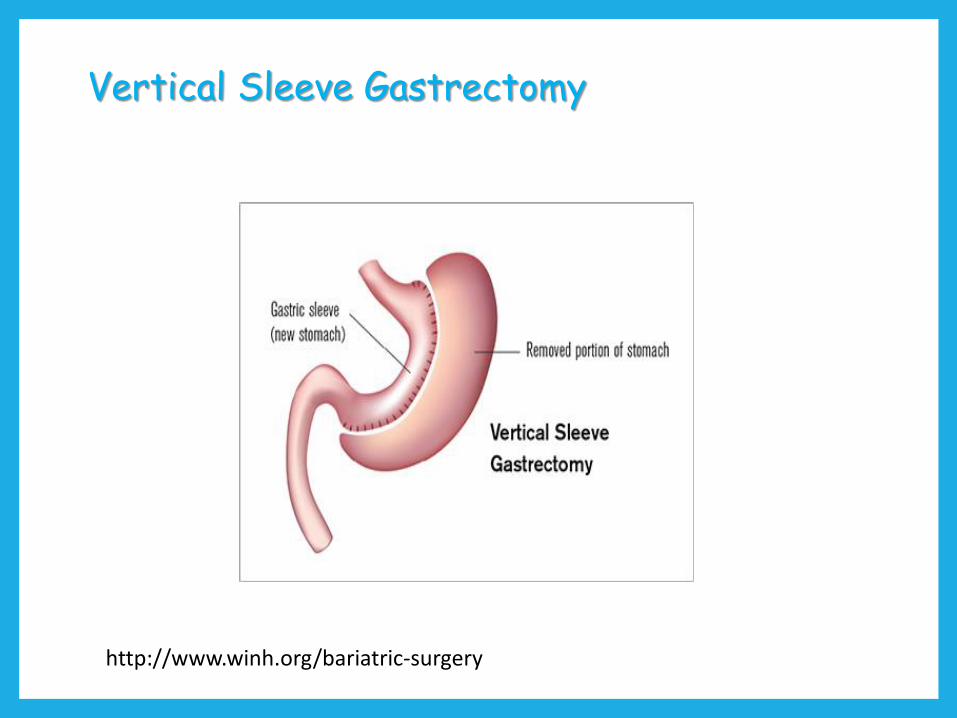
Vertical Sleeve Gastrectomy
http://www.winh.org/bariatric-surgery
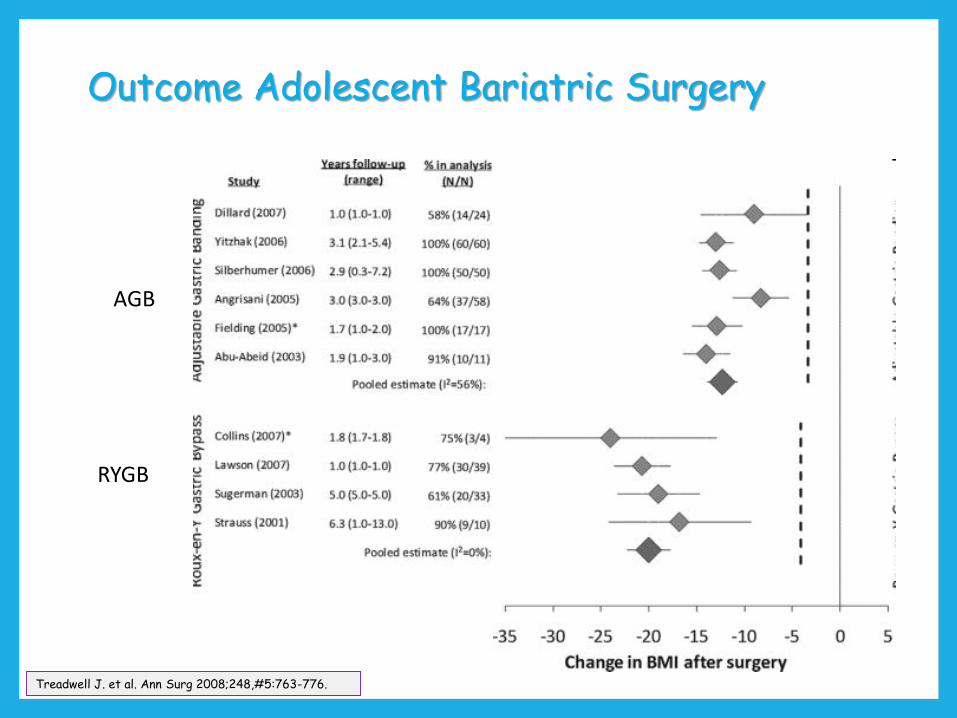
Outcome Adolescent Bariatric Surgery
Treadwell J. et al. Ann Surg 2008;248,#5:763-776.
AGB
RYGB
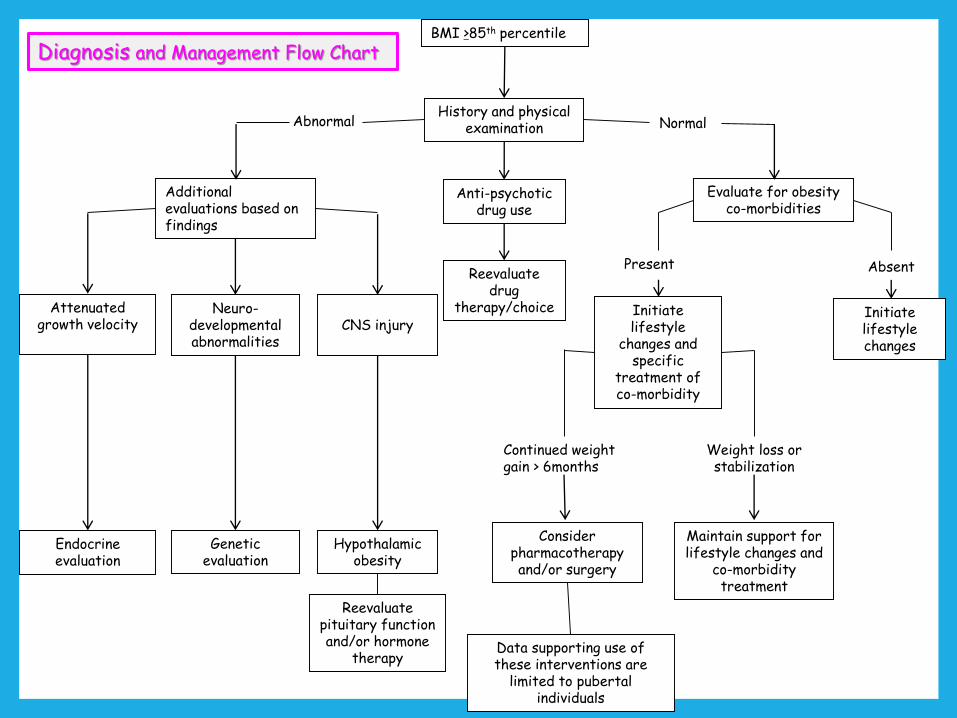
BMI >85th percentile
History and physical examination
Evaluate for obesityco-morbidities
Additional evaluations based on findings
Initiate lifestyle changes
Initiate lifestyle
changes and specific
treatment of co-morbidity
Maintain support for lifestyle changes and
co-morbidity treatment
Consider pharmacotherapy and/or surgery
Continued weight gain > 6months
Weight loss or stabilization
CNS injuryNeuro-
developmental abnormalities
Attenuated growth velocity
NormalAbnormal
Hypothalamic obesity
Genetic evaluation
Endocrine evaluation
AbsentPresent
Reevaluate pituitary function and/or hormone
therapy
Anti-psychotic drug use
Reevaluate drug
therapy/choice
Data supporting use of these interventions are
limited to pubertal individuals
Diagnosis and Management Flow Chart
Summary (1)
Childhood obesity is associated with family, community, racial, and SES factors in addition to sugared beverage intake,
physical activity level, and sedentary activity.
Obesity and extreme obesity have increased over the past 3 decades particularly among African American
and Hispanic Youth.
Obesity in childhood tracks into adult life.
Comorbidities include diabetes, hypertension, dyslipidemia, PCOS, and metabolic syndrome.
Prevalences of these comorbidities have increased in children and adolescents
Summary (2)
Lifestyle interventions focused on the family and including both dietary and physical activity changes have
therapeutic efficacy in reducing obesity but of small effect (approx. 3 to 4 Kg on average).
There are limited pharmacological agents currently available for use in the pediatric population and their efficacy above and beyond lifestyle intervention is
marginal at best.
Surgical interventions have proven to be most effective for extremely obese pediatric patients
Prevention (BMI 5th to 85th%ile)
Dietary Intake
Limit consumption of sugar sweetened beverages
Encourage 5-a-day fruits and vegetables
Physical Activity
Limit screen time to 1-2hrs/day starting age 5yrs
No TV/computer screens in bedroom
Encourage 60min moderate to vigorous physical activity/day
Eating Behaviors
Daily breakfast
Limit restaurant eating
Encourage family meals
Limit portion size
Barlow SE. Pediatrics 2007; 120, Suppl #4: S164-S192
Role of Primary Care Physician
Measure height and weight and calculate BMI at least annually
Observe for trends such as rapid weight gain
Offer anticipatory guidance about nutrition and physical activity at every well child check
Help families make better food choices
Advocate for children on local, state, and national levels
Brown C, et al. Pediatr Clin North Am. 2015; 62: 1241–1261.
Interventions
• Stage 1: Prevention+ program• General recommendations + monthly follow-up • Target: Weight maintenance
• Stage 2: Structured weight management program (failed prevention+)• Balanced macronutrient diet, • Supervised active play of 60 min/day, • Decreased screen time ≤ 1 hr/day• Target: Weight loss 1 lb/month in 2-11 yr olds, maximum 2 lbs/week in older obese children and adolescents
Barlow SE. Pediatrics 2007; 120, Suppl #4: S164-S192
Conclusions (1)
Lifestyle interventions are the cornerstone of all therapeutic interventions for obesity in childhood.
Recognition of comorbidities in children with obesity demands both a therapeutic intervention for the
comorbidity as well as targeting the obesity.
Pharmacotherapy and surgical interventions are currently recommended only for those who have failed lifestyle
approaches and continue to gain weight at an accelerated rate.
Conclusions (2)
Given our limited armamentarium for treating obesity, prevention represents the best course to
control the epidemic.
Research into non-surgical interventions to treat those children already obese is an important unmet
need.
Conclusions (3)
Successful lifestyle change requires family interventions with community advocacy to support those changes.
Shared agreements for use of physical activity spaces
Establishing/maintaining recess and gym classes
Subsidies for schools to provide healthy foods
Menu labeling in restaurants
Laws addressing food advertising to children
Food and beverage industry incentives
Brown C, et al. Pediatr Clin North Am. 2015; 62: 1241–1261.

Prevention
A collective responsibility requiring
individual
family
physician
community
corporate
government
COMMITMENT
THANK YOUSelma Feldman Witchel, MD
Pediatric Endocrinology
Children’s Hospital of Pittsburgh of UPMC
Phone: 412-692-5170
“Endocrine Wellness”