pediatrics 2014 keeney 493 9
DESCRIPTION
pediatricTRANSCRIPT
Dexamethasone for Acute Asthma Exacerbations inChildren: A Meta-analysis
abstractBACKGROUND AND OBJECTIVE: Dexamethasone has been proposed asan equivalent therapy to prednisone/prednisolone for acute asthmaexacerbations in pediatric patients. Although multiple small trialsexist, clear consensus data are lacking. This systematic review andmeta-analysis aimed to determine whether intramuscular or oraldexamethasone is equivalent or superior to a 5-day course of oralprednisone or prednisolone. The primary outcome of interest wasreturn visits or hospital readmissions.
METHODS: A search of PubMed (Medline) through October 19, 2013, byusing the keywords dexamethasone or decadron and asthma or statusasthmaticus identified potential studies. Six randomized controlled trialsin the emergency department of children #18 years of age comparingdexamethasone with prednisone/prednisolone for the treatment ofacute asthma exacerbations were included. Data were abstracted by4 authors and verified by a second author. Two reviewers evaluatedstudy quality independently and interrater agreement was assessed.
RESULTS: There was no difference in relative risk (RR) of relapse be-tween the 2 groups at any time point (5 days RR 0.90, 95% confidenceinterval [CI] 0.46–1.78, Q = 1.86, df = 3, I2 = 0.0%, 10–14 days RR 1.14,95% CI 0.77–1.67, Q = 0.84, df = 2, I2 = 0.0%, or 30 days RR 1.20, 95% CI0.03–56.93). Patients who received dexamethasone were less likely toexperience vomiting in either the emergency department (RR 0.29,95% CI 0.12–0.69, Q = 3.78, df = 3, I2 = 20.7%) or at home (RR 0.32, 95%CI 0.14–0.74, Q = 2.09, df = 2, I2 = 4.2%).
CONCLUSIONS: Practitioners should consider single or 2-dose regi-mens of dexamethasone as a viable alternative to a 5-day course ofprednisone/prednisolone. Pediatrics 2014;133:493–499
AUTHORS: Grant E. Keeney, MD,a Matthew P. Gray, MD,a
Andrea K. Morrison, MD, MS,a Michael N. Levas, MD,a
Elizabeth A. Kessler, MD, MS,a Garick D. Hill, MD, MS,a MarcH. Gorelick, MD, MSCE,a Jeffrey L. Jackson, MD, MPHb,c
Departments of aPediatrics, and bGeneral Internal Medicine,Medical College of Wisconsin, Milwaukee, Wisconsin; andcZablocki VAMC, Milwaukee, Wisconsin
KEY WORDSdexamethasone, prednisone, prednisolone, asthma, statusasthmaticus
ABBREVIATIONSCI—confidence intervalED—emergency departmentIM—intramuscularPO—per osRR—relative risk
Dr Gorelick conceptualized the study; Drs Gray, Keeney,Morrison, Levas, Kessler and Hill conceptualized and designedthe study, designed the data collection instruments, coordinatedand supervised data collection, and drafted the initialmanuscript; Dr Jackson participated in study design, carriedout the initial analyses, and reviewed and revised themanuscript; and all authors approved the final manuscript assubmitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-2273
doi:10.1542/peds.2013-2273
Accepted for publication Dec 4, 2013
Address correspondence to Grant E. Keeney, MD, Department ofPediatrics, Medical College of Wisconsin, 999 North 92nd St,Milwaukee, WI 53226. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: Supported by the National Center for AdvancingTranslational Sciences, National Institutes of Health, throughgrant 8UL1TR000055. Its contents are solely the responsibility ofthe authors and do not necessarily represent the official viewsof the National Institutes of Health. Funded by the NationalInstitutes of Health (NIH).
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
PEDIATRICS Volume 133, Number 3, March 2014 493
REVIEW ARTICLE
at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from

Asthma affects .6 million children inthe United States, making it the mostcommon chronic disease of childhood.1,2
As such, asthma accounts for 2% ofall ambulatory care and emergencydepartment (ED) visits by patients,18years of age.3 Asthma is a chronic in-flammatory disease characterized byairway edema, bronchoconstrictionand airway hyperresponsiveness. Inaddition to bronchodilators, cortico-steroids are the cornerstone of therapyfor acute asthma exacerbations. Theysystemically reduce inflammation, de-crease mucus production, and enhancethe effects of b-agonists.2 National andinternational guidelines advise earlyadministration of systemic cortico-steroids for moderate or severe exac-erbations and for mild exacerbationsthat do not immediately and completelyrespond to short-acting b-agonists.1,4
Current treatment regimens consist oforal prednisone or prednisolone takenonceor twicedaily for5days.Oral (PO)orintramuscular (IM) dexamethasone hasbeen proposed as an equivalent therapy.Potential advantages include a longerhalf-life requiring a shorter course, in-creased compliance with a single dose,and less vomiting with dexamethasone.Althoughmultiplesmall trialsexist, clearconsensus data are lacking.
OBJECTIVE
Thepurpose of this systematic reviewandmeta-analysis of randomized clinicaltrials is to determine whether PO or IMdexamethasone is equivalent or superiorto a 5-day course of oral prednisone orprednisolone. The primary outcome ofinterest was unscheduled return visits(clinic visit, ED visit, orhospital admission)foracuteasthmaexacerbation inpediatricpatients. Secondary outcomes includedvomiting in the ED and vomiting at home.
METHODS
Trials were identified using PubMed (Med-line)withsearchtermsof“dexamethasone”
OR “decadron” AND “asthma” OR “sta-tus asthmaticus” in all search fields,including only human trials withoutlanguage restriction. The final searchwas conducted on October 19, 2013.
Studies were included in the meta-analysis if they were a randomized con-trolled trial of treatment of acute asthmaexacerbation in either an ambulatory orED setting comparing dexamethasonewith prednisone or prednisolone inchildren #18 years of age. Patientshospitalized during the initial study en-counter were not included in the analy-sis of return visits. Articles wereexcluded at the title and abstract phaseby 2 authors (M.L. and G.H.). Referencelists from review articles and thosestudies included in the meta-analysiswere reviewed by hand without identifi-cation of additional articles meetingcriteria.
Data were abstracted by 4 authors (G.K.,M.P.G., A.M., M.L.) and all data were ver-ifiedby a secondauthor. Abstracted dataincluded subject characteristics (age inmonths, gender, ethnicity), asthma se-verity score, treatment characteristics(number of albuterol treatments in theED), adverse effects (vomiting), andclinical outcomes (hospitalization dur-ing initial ED visit, asthma score at EDdischarge, subjective improvement, andrelapse rate as defined by an un-scheduled visit to a clinic, ED, or a hos-pitalization). Outcomes were extractedas either dichotomous or continuousvariables based on study report.
Study quality of the included trials wasassessed using the Cochrane risk ofbias tool, the 6-question instrumentcreated and validated by Jadad andcolleagues, and 2 additional items de-scribing the presence of industrysponsorship in the trial and whetherintent to treat analysis was performed.5,6
Two reviewers (G.H. and E.K.) evaluatedstudy quality independently.
Data were pooled using a fixed-effectsmodel. Relapse rates were reported
at different time intervals and combinedformeta-analysisonlywhensimilar timeintervals were reported (5 days, 10–14days, and 30 days). Differences betweengroups were tested using randomeffects meta-regression.7 Heterogeneitywas assessed using the I2 method.8 Weassessed for small study effects (pub-lication bias) using the methods ofPeters et al9 for dichotomous outcomesand Egger et al10 for continuous out-comes. We examined the potential forundue influence of any given study bylooking at the percentage of total weightto the final pooled results for each studyand by examining meta-influence plots.Potential sources of heterogeneity wereexplored by using stratified analysis. Allanalyseswere performed by using Stataversion 12.1 (Stata Corp, College StationTX). This studywas supported by a grantfrom the National Center for AdvancingTranslational Sciences, National Insti-tutes of Health.
RESULTS
Our search identified 667 articles. Ap-plication of inclusion and exclusion cri-teria resulted in 6 studies that wereincluded in our analysis (Fig 1).11–16 Allof the included studies were performedin EDs and had a mean of 171 partic-ipants (range 15–272). All studies butone (Gordon et al12) defined relapse asan unplanned clinic visit, return ED visit,or an unplanned hospital admissionrelated to their initial asthma exacerba-tion. Dexamethasone was given as a sin-gle IM dose in 3 studies,12,14,15 as a singleoral dose in 1 study,11 and as multipleoral doses in 2 studies13,16 (Table1). In-cluded studies were from the UnitedStates (n = 5) and Canada (n = 1). Allstudies were among children witha mean age of 53.2 (95% confidence in-terval [CI] 41.5–64.9) months. Partic-ipants were mostly boys (63.5%). One ofthe studies included a predominantlyHispanic population (80%).12 Among theremaining studies, participants were
494 KEENEY et al at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from
34.7% white and 37.9% African Ameri-can. Study quality ranged from 3 to 8 onthe Jadad scale (Table 1) and assess-ments using the results of the Cochranerisk of bias tool are presented in Table 2.Interrateragreementwas excellent witha k of 0.90.
In comparing the group receiving dexa-methasone to prednisone, there were nodifferencesatbaseline inage(44.4vs56.7months, P= .66), proportion of boys (63.6vs 65.8, P= .37), or initial asthma severityscore (standardized mean 3.5 vs 3.1, P =.22, 4 studies). There were no differencesin the likelihood of improvement inasthma scores during the initial ED visitbetween groups (relative risk [RR] 1.01,95% CI 0.93–1.10, Q = 0.38, df = 2, I2 =0.0%), the number of albuterol treat-ments received in the ED (2.5, 95% CI1.8–3.2 vs 2.7, 95% CI 1.9–3.5, P for dif-ference = .87, 4 studies), or in post-treatment asthma severity scores (RR1.38, 95% CI 0.0–2.81 vs 1.27, 95% CI0.0–2.71,P fordifference=0.78). Therewasno difference in the average amount ofimprovement in asthma scores between
groups (standard mean difference2.56, 95% CI 2.27–2.84 vs 2.30, 95% CI2.03–2.56, P for difference = 0.56).There was no difference in rates ofhospitalization during the initial EDvisit (RR 0.91, 95% CI 0.66–1.26, Q = 1.68,df = 4, I2 = 0.0%).
In the dexamethasone group, there wasa 6.6% (95% CI 0.3% –10.0%) relapserate by 5 days, increasing to 13.8%(95% CI 11.3–16.4) by 2 weeks (Fig 2). Inthe prednisone/prednisolone groupthe 5-day relapse rate was 3.6% (95% CI1.1%–6.2%), increasing to 11.9% (95%CI 0.9%–14.4%) by 2 weeks. There wasno difference in relapse rate betweenthe 2 groups at any time point (5 daysRR 0.90, 95% CI 0.46–1.78, Q = 1.86, df =3, I2 = 0.0%, 10–14 days RR 1.14, 95% CI0.77–1.67, Q = 0.84, df = 2, I2 = 0.0%, or30 days RR 1.20, 95% CI 0.03–56.93),although the 30-day relapse rate wasreported in only 1 study.
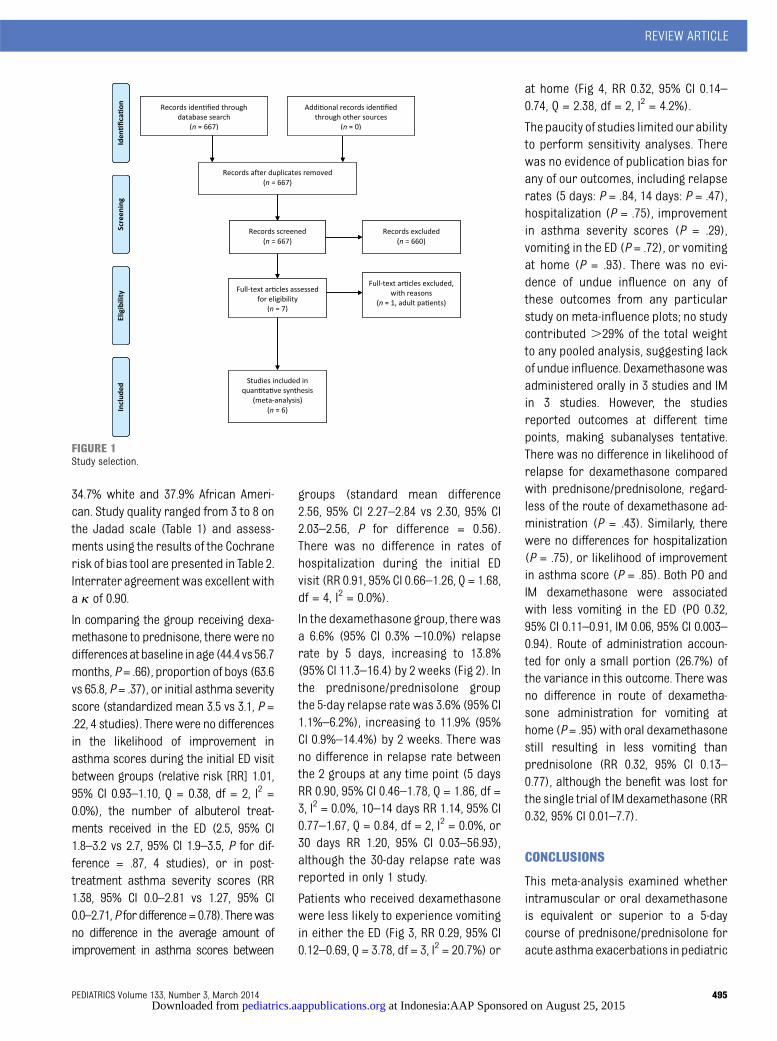
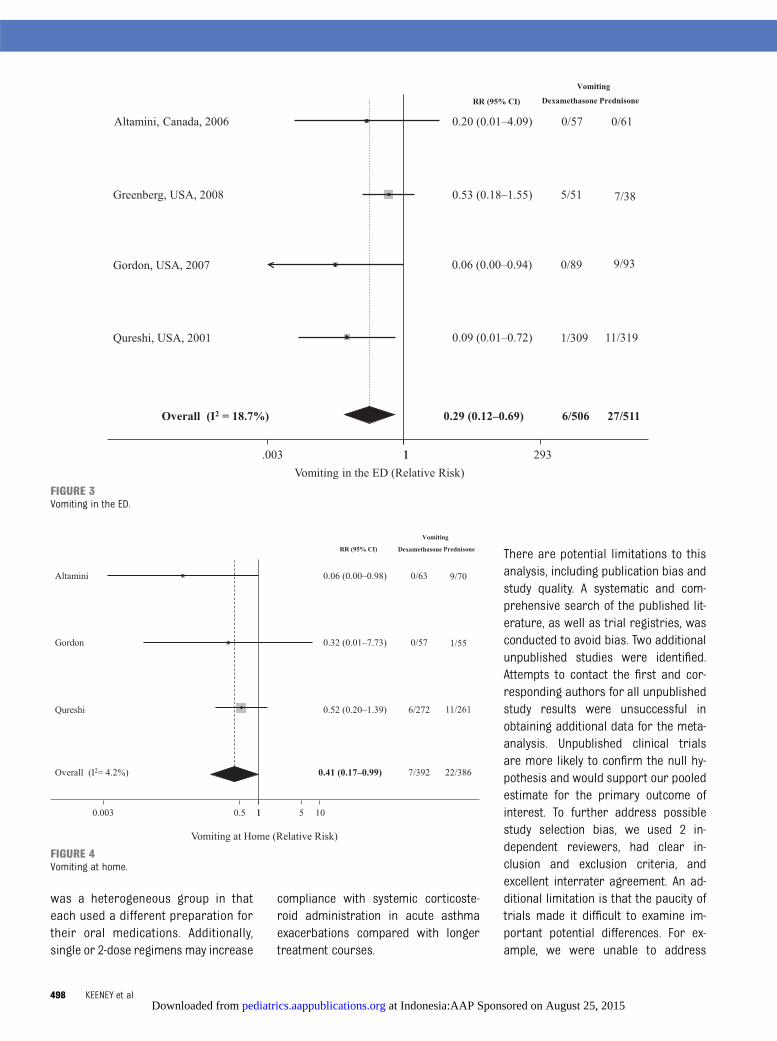
Patients who received dexamethasonewere less likely to experience vomitingin either the ED (Fig 3, RR 0.29, 95% CI0.12–0.69, Q = 3.78, df = 3, I2 = 20.7%) or
at home (Fig 4, RR 0.32, 95% CI 0.14–0.74, Q = 2.38, df = 2, I2 = 4.2%).
The paucity of studies limited ourabilityto perform sensitivity analyses. Therewas no evidence of publication bias forany of our outcomes, including relapserates (5 days: P = .84, 14 days: P = .47),hospitalization (P = .75), improvementin asthma severity scores (P = .29),vomiting in the ED (P = .72), or vomitingat home (P = .93). There was no evi-dence of undue influence on any ofthese outcomes from any particularstudy on meta-influence plots; no studycontributed .29% of the total weightto any pooled analysis, suggesting lackof undue influence. Dexamethasone wasadministered orally in 3 studies and IMin 3 studies. However, the studiesreported outcomes at different timepoints, making subanalyses tentative.There was no difference in likelihood ofrelapse for dexamethasone comparedwith prednisone/prednisolone, regard-less of the route of dexamethasone ad-ministration (P = .43). Similarly, therewere no differences for hospitalization(P = .75), or likelihood of improvementin asthma score (P = .85). Both PO andIM dexamethasone were associatedwith less vomiting in the ED (PO 0.32,95% CI 0.11–0.91, IM 0.06, 95% CI 0.003–0.94). Route of administration accoun-ted for only a small portion (26.7%) ofthe variance in this outcome. There wasno difference in route of dexametha-sone administration for vomiting athome (P= .95) with oral dexamethasonestill resulting in less vomiting thanprednisolone (RR 0.32, 95% CI 0.13–0.77), although the benefit was lost forthe single trial of IM dexamethasone (RR0.32, 95% CI 0.01–7.7).
CONCLUSIONS
This meta-analysis examined whetherintramuscular or oral dexamethasoneis equivalent or superior to a 5-daycourse of prednisone/prednisolone foracute asthma exacerbations in pediatric
FIGURE 1Study selection.
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 3, March 2014 495 at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from

TABLE1
Included
Studies
Author
Interventiona
Comparisona
InclusionCriteria
ExclusionCriteria
JadadScore
SingleIM
dose
Gries,2000
14Dexamethasone
1.7mg/kg
(max
36mg)
IM3
1dose
Prednisone
orprednisolone
1mg/kg
(max
20mg)
POtwicedaily
35d
Age6mo-7y,previous
historyofasthma,
mild
tomoderateasthmaexacerbation
Useofsteroidinprevious
2wk,severe
asthmaexacerbation(requiring
hospitalization),fever
.101,or
documentedRSVinfection
3
Gordon,20071
2Dexamethasone
0.6mg/kg
(max
15mg)
IM3
1dose
Prednisolone
2mg/kg
(max
50mg)
POdaily
35d
Age18
mo-7y,previous
historyof
asthma,mild
tomoderate
asthmaexacerbation
Useofsteroidinprevious
month,allergy
tosteroid,TB
orvaricella
exposure,
previous
enrollm
ent,major
coexisting
illness,O2saturation,
88%on
room
air,pectus
excavatum,orneed
forIV
4
Klig,19971
5Dexamethasone
0.3mg/kg
(max
15mg)
IM3
1dose
Prednisone
2mg/kg
(max
100mg)
PO3
1dose
then
1mg/kg
POdaily
32d
Age3–16
y,previous
historyof
asthma,mild
tomoderate
asthmaexacerbation
Useofsteroidinprevious
month,oxygen
saturation#
95%on
room
air,
significant
recent
hospitalizationfor
asthmaor
ICUstay
inthepastyear,
7dofprednisone
inpastyear,or
major
coexistingillness
3
SingleOralDose
Altamimi,2006
11Dexamethasone
0.6m
g/kg
(max
18mg)
PO3
1dose,
placeboPO
twicedaily
35d
Prednisone
orprednisolone
1mg/kg
(max
30mg)
PO3
1dose,then
1mg/kg
POtwicedaily
35d
Age2–16
y,previous
historyof
asthmaandmild
tomoderate
asthmaexacerbation
Useofsteroidinprevious
2wk,complete
recovery
after1bronchodilator,historyof
previous
intubationor
PICU
admission,
major
coexistingillness,history
ofacute
allergicreaction,activevaricella,orHSVinfections
8
MultipleOralDoses
Greenberg,2008
13Dexamethasone
0.6mg/kg
(max
16mg)
POonce
daily
32d
Prednisone
2mg/kg
(max
80mg)
PO3
1dose,then1mg/kg
(max
30mg)
POtwicedaily
34d
Age2–18
y,previous
historyof
asthma,andacuteexacerbation
asthma
Useofsteroidinprevious
month,history
ofintubation,varicella
exposure,
possibleforeignbody
aspiration,
major
coexistingillness,significant
respiratorydistress,previousenrollm
ent,
notelephoneforfollow-up,or
$2episodes
ofem
esisaftersteroiddose
inED
4
Qureshi,2001
16Dexamethasone
0.6m
g/kg
(max
16mg)
POonce
daily
32d
Prednisone
orprednisolone
2mg/kg
(max
60mg)
PO3
1dose,then
1mg/kg
(max
60mg)
POdaily
34d
Age2–18
y,previous
historyof
asthma,acuteexacerbation,
andrequired
atleast2b-agonist
treatm
entsinED
Useofsteroidinprevious
4wk,history
ofintubation,varicella
exposure,
concurrent
stridor,concernfor
intrathoracicforeignbody,m
ajor
coexisting
illness,orneed
forimmediateairw
ayintervention
3
HSV,herpes
simplex
virus;max,m
aximum
;RSV,respiratory
syncytialvirus;TB,tuberculosis.
aFirstdose
ofmedicationprovided
intheED.
496 KEENEY et al at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from

patients discharged to home from theED. Fixed effects methods increase thechance of finding differences. Finding nodifferences in a fixed effects model isa more conservative choice when com-paring2different treatmentoptions. Thepooled results failed to demonstratea statistically significant difference be-tween the 2 therapies for the primaryoutcome of relapse rate to clinic, ED, orhospitalization, suggesting that the 2therapies are equivalent.
Our decision to combine studies with dif-ferent routes and dosing of dexamethasone
was an effort to increase generalizability.A subgroup analysis failed to show sta-tistically significant differences regard-lessof thefollow-upperiods.The4studiesthat reported 5-day follow-up relapserates all used a single dose of IM or POdexamethasone.11,12,14,15 Five days was themost common follow-up duration and isthe most clinically relevant period inwhich to detect treatment failure. This issupported by the fact that 5-day coursesof oral corticosteroids have not beenshown to be superior to 3-day courses foroutpatient management of children with
acute exacerbations.17 There was no dif-ference detected in studies reporting re-currence rates at 5, 10 to 14, or 30 days’follow-up.
Significantly fewer patients receivingdexamethasone vomited in the ED or athome after discharge. This finding hasclinical significance for improving pa-tient and parental satisfaction. Thelower rate of vomiting with dexameth-asone possibly reflects a difference inpalatability that has been shown inprevious studies.18,19 However, the groupof studies that used oral dexamethasone
TABLE 2 Cochrane Risk of Bias Quality Assessment
Study Allocation SequenceAdequate
Allocation Concealed Blinding ofParticipants
Blinding ofOutcomes
Outcome Data AdequatelyAddressed
Free From SelectiveOutcome Reporting
Free From OtherProblems
Altamimi11 Yes Yes Yes Yes No Unclear YesGordon12 Yes Yes No No Yes No Yesa
Qureshi16 No No No No Yes Unclear Yesa
Greenberg13 Uncleara Uncleara Yes Unclear No Unclear YesGries14 Unclear Unclear No No Yesa Unclear YesKlig15 Unclear Unclear No No Yes Unclear Yesa Disagreement between reviewers.
FIGURE 2Relapse rates.
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 3, March 2014 497 at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from
was a heterogeneous group in thateach used a different preparation fortheir oral medications. Additionally,single or 2-dose regimens may increase
compliance with systemic corticoste-roid administration in acute asthmaexacerbations compared with longertreatment courses.
There are potential limitations to thisanalysis, including publication bias andstudy quality. A systematic and com-prehensive search of the published lit-erature, as well as trial registries, wasconducted to avoid bias. Two additionalunpublished studies were identified.Attempts to contact the first and cor-responding authors for all unpublishedstudy results were unsuccessful inobtaining additional data for the meta-analysis. Unpublished clinical trialsare more likely to confirm the null hy-pothesis and would support our pooledestimate for the primary outcome ofinterest. To further address possiblestudy selection bias, we used 2 in-dependent reviewers, had clear in-clusion and exclusion criteria, andexcellent interrater agreement. An ad-ditional limitation is that the paucity oftrials made it difficult to examine im-portant potential differences. For ex-ample, we were unable to address
FIGURE 3Vomiting in the ED.
FIGURE 4Vomiting at home.
498 KEENEY et al at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from

whether IM and PO dexamethasone areequally effective, whether a single oraldexamethasone dose is equivalent tomultiple doses, and whether there aredifferences in efficacy and palatabilitybetween different formulations of oral
prednisone/prednisolone. Furthermore,all our results are based on ED-basedstudies, and it is unclear whether thiswould translate to the ambulatory clinicsetting. Future research should focus onthese important questions.
Based on our findings, emergency physi-cians should consider single or 2-dosedexamethasone regimens over 5-dayprednisone/prednisolone regimensfor the treatment of acute asthmaexacerbations.
REFERENCES
1. National Asthma Education and PreventionProgram. Expert panel report 3 (EPR-3):Guidelines for the diagnosis and manage-ment of asthma-summary report 2007.J Allergy Clin Immunol. 2007;120(suppl 5):S94–S138
2. Scarfone RJ, Friedlaender E. Corticosteroidsin acute asthma: past, present, and future.Pediatr Emerg Care. 2003;19(5):355–361
3. Akinbami LJ, Moorman JE, Garbe PL, SondikEJ. Status of childhood asthma in theUnited States, 1980–2007. Pediatrics. 2009;123(suppl 3):S131–S145
4. Papadopoulos NG, Arakawa H, Carlsen KH,et al. International consensus on (ICON)pediatric asthma. Allergy. 2012;67(8):976–997
5. Higgins J, Altman D, Sterne A. Chapter 8:Assessing risk of bias in included studies.In: Higgings J, Green S, eds. Cochranehandbook for systematic reviews of inter-ventions, version 5.1.0 [updated March2011]. The Cochrane Collaboration; 2011.Available at: www.cochrane-handbook.org.Accessed May 12, 2013
6. Jadad AR, Moore RA, Carroll D, et al.Assessing the quality of reports of ran-domized clinical trials: is blinding neces-sary? Control Clin Trials. 1996;17(1):1–12
7. Sharp S. Meta-analysis regression. StataTech Bull. 1998;42:16–22
8. Higgins JP, Thompson SG, Deeks JJ, AltmanDG. Measuring inconsistency in meta-analyses.BMJ. 2003;327(7414):557–560
9. Peters JL, Sutton AJ, Jones DR, Abrams KR,Rushton L. Comparison of two methods todetect publication bias in meta-analysis.JAMA. 2006;295(6):676–680
10. Egger M, Davey Smith G, Schneider M,Minder C. Bias in meta-analysis detected bya simple, graphical test. BMJ. 1997;315(7109):629–634
11. Altamimi S, Robertson G, Jastaniah W, et al.Single-dose oral dexamethasone in theemergency management of children withexacerbations of mild to moderate asthma.Pediatr Emerg Care. 2006;22(12):786–793
12. Gordon S, Tompkins T, Dayan PS. Random-ized trial of single-dose intramusculardexamethasone compared with predniso-lone for children with acute asthma.Pediatr Emerg Care. 2007;23(8):521–527
13. Greenberg RA, Kerby G, Roosevelt GE. Acomparison of oral dexamethasone withoral prednisone in pediatric asthma exac-erbations treated in the emergency de-partment. Clin Pediatr (Phila). 2008;47(8):817–823
14. Gries DM, Moffitt DR, Pulos E, Carter ER. Asingle dose of intramuscularly adminis-tered dexamethasone acetate is as effec-tive as oral prednisone to treat asthmaexacerbations in young children. J Pediatr.2000;136(3):298–303
15. Klig JE, Hodge D III, Rutherford MW. Symp-tomatic improvement following emergencydepartment management of asthma: a pilotstudy of intramuscular dexamethasoneversus oral prednisone. J Asthma. 1997;34(5):419–425
16. Qureshi F, Zaritsky A, Poirier MP. Compar-ative efficacy of oral dexamethasone ver-sus oral prednisone in acute pediatricasthma. J Pediatr. 2001;139(1):20–26
17. Chang AB, Clark R, Sloots TP, et al. A 5- versus3-day course of oral corticosteroids forchildren with asthma exacerbations who arenot hospitalised: a randomised controlledtrial. Med J Aust. 2008;189(6):306–310
18. Kim MK, Yen K, Redman RL, Nelson TJ,Brandos J, Hennes HM. Vomiting of liquidcorticosteroids in children with asthma.Pediatr Emerg Care. 2006;22(6):397–401
19. Mitchell JC, Counselman FL. A taste comparisonof three different liquid steroid preparations:prednisone, prednisolone, and dexamethasone.Acad Emerg Med. 2003;10(4):400–403
REVIEW ARTICLE
PEDIATRICS Volume 133, Number 3, March 2014 499 at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2013-2273; originally published online February 10, 2014; 2014;133;493Pediatrics
A. Kessler, Garick D. Hill, Marc H. Gorelick and Jeffrey L. JacksonGrant E. Keeney, Matthew P. Gray, Andrea K. Morrison, Michael N. Levas, ElizabethDexamethasone for Acute Asthma Exacerbations in Children: A Meta-analysis
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2013-2273; originally published online February 10, 2014; 2014;133;493Pediatrics
A. Kessler, Garick D. Hill, Marc H. Gorelick and Jeffrey L. JacksonGrant E. Keeney, Matthew P. Gray, Andrea K. Morrison, Michael N. Levas, ElizabethDexamethasone for Acute Asthma Exacerbations in Children: A Meta-analysis
http://pediatrics.aappublications.org/content/133/3/493.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from

ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/133/3/493.full.htincluding high resolution figures, can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/133/3/493.full.htat:This article cites 18 articles, 4 of which can be accessed free
Citations
ml#related-urlshttp://pediatrics.aappublications.org/content/133/3/493.full.htThis article has been cited by 4 HighWire-hosted articles:
Rs)3Peer Reviews (PPost-Publication
http://pediatrics.aappublications.org/cgi/eletters/133/3/493
R has been posted to this article: 3One P
Subspecialty Collections
btopichttp://pediatrics.aappublications.org/cgi/collection/asthma_suAsthma
gy_subhttp://pediatrics.aappublications.org/cgi/collection/pulmonoloPulmonology
_subhttp://pediatrics.aappublications.org/cgi/collection/toxicologyToxicology
ogy_subhttp://pediatrics.aappublications.org/cgi/collection/pharmacolPharmacologythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on August 25, 2015pediatrics.aappublications.orgDownloaded from