pelvis forum. shapes of the pelvic inlet (superior aperture) – a. android – heart shaped, more...
TRANSCRIPT

Pelvis Forum

Shapes of the pelvic inlet (superior aperture) – a. Android – heart shaped, more commonly male – b. Anthropoid – rounded, more commonly male – c. Gynecoid – heart-shaped, more narrow than android,
most common female – d. Platypelloid – oval and wide, uncommon
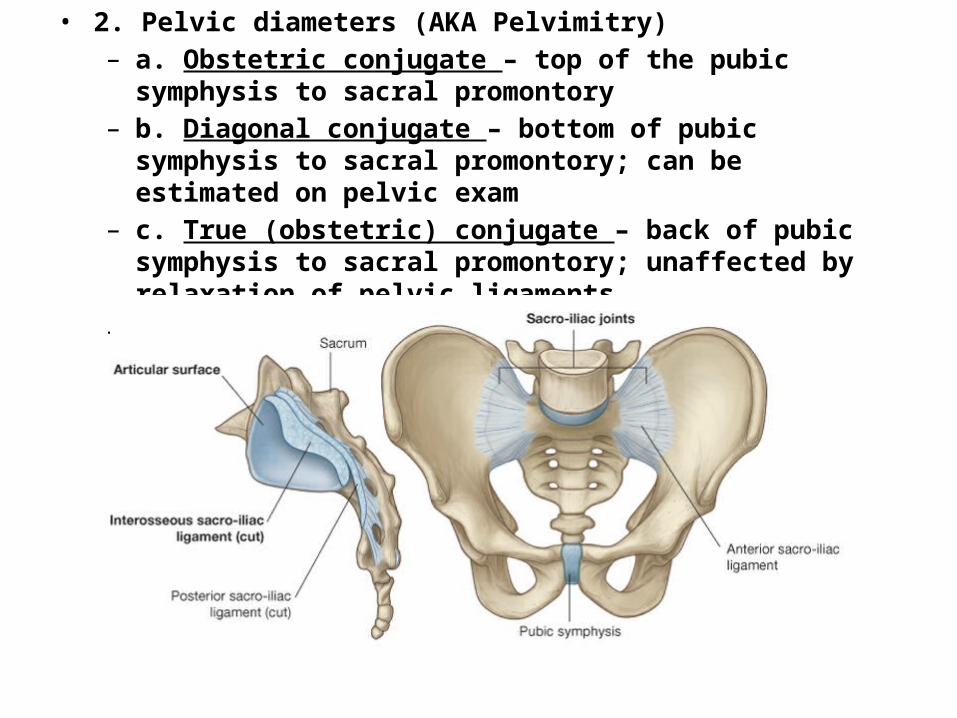
• 2. Pelvic diameters (AKA Pelvimitry) – a. Obstetric conjugate – top of the pubic symphysis to sacral
promontory – b. Diagonal conjugate – bottom of pubic symphysis to sacral
promontory; can be estimated on pelvic exam – c. True (obstetric) conjugate – back of pubic symphysis to sacral
promontory; unaffected by relaxation of pelvic ligaments – d. Interspinous distance – between ischial spines

Pelvic + Perineum Blood Supply

Pelvic and Perineum Blood Supply
Male Female

Nerve Supply

The ureter is in danger during: – a. hysterectomy – it travels inferior (under) the uterine
artery “Water under the bridge”– b. ovarectomy [ureter and ovarian vessels cross the
pelvic inlet]

Internal Iliac artery – ligation of the internal iliac artery may be used to reduce blood flow during surgery or blockage of this vessel may occur in atherosclerotic disease; significant anastomoses occur between:
– a. Uterine and Ovarian (aorta) – b. Iliolumbar/circumflex iliac and lumbar (from aorta) – c. Lateral sacral and median sacral (aorta at division to
internal iliacs) – d. Middle rectal and superior rectal (IMA) – e. Inferior gluteal and profunda femoris (femoral)

Damage to the perineal body/pelvic floor - disruption of the perineal body (episotomy) can result in dysfunction of the muscles of the levator ani and herniation of pelvic contents:
– a. Cystocele – collapse of the bladder into the anterior wall of the vagina; can occur also with injury to the supportive structures of the vagina
– b. Rectocele – anterior and inferior protrusion of the rectum – c. Enterocele – anterior and inferior protrusion of the
rectovaginal pouch


Rupture of the male urethra:
a. Recall - the superficial fascia of the abdominal wall (Scarpa’s) continues onto the penis and scrotum as Dartos fascia and into the penis as Colle’s fascia and that the deep investing fascia extends over the shaft of the penis as Buck’s fascia and over the superificial perineal muscles (external perineal fascia).
b. Lacerations of the spongy urethra + Buck’s fascia intact = urine spreads along the shaft of the penis
c. Laceration of the spongy urethra + Buck’s fascia torn = urine leaks into the superficial pouch (scrotum) along the shaft of the penis and along the anterior abdominal wall, deep to Scarpa’s fascia

Micturition
• Action potentials carried by sensory neurons from stretch receptors in the urinary bladder wall travel to the sacral segments of the spinal cord through the pelvic nerves
– a. somatic [S2-4] – voluntary relaxation of the sphincter urethrae
– b. sympathetics – inhibit the detrusor/excite the internal sphincter
– c. parasympathetics – excite the detrusor/inhibit the internal sphincter

Sacral Cord/PNS injury resulting in overflow incontinence – i. Sensory neurogenic – ii. Motor neurogenic/detrusor areflexia
Destruction of sacral spinal cord – i. Autonomous bladder – continuous dribble of urine
Spinal cord injury (cervical/thoracic/lumbar) – i. Atonic/flaccid then spastic/hyperactive
Nocturnal enuresis – i. Abnormal changes in bladder pressure? – ii. Delayed maturation of bladder; small bladder – iii. Possible link to ADH secretion? Overactive detrusor

• Rupture of the spongy urethra in males in usually the result of straddling injuries.
• Need to know the consequences of rupture to the spongy urethrae to know where the urine will accumulate
ANS Control of Male Sexual Response
• Autonomic control of: – a. Erection – parasympathetic [S2-4] for vascular
smooth muscle; pudendal [S2-4] for contraction of perineal muscles
– b. Emission – sympathetic [L1-2] for contraction of smooth muscle in ductus deferens
– c. Ejaculation – sympathetic [L1-2] for closure of internal urethral sphincter; parasympathteics [S2-4] for contraction of urethral smooth muscle and pudendal [S2-4] for contraction of perineal muscles
• Removal/ablation of the prostate endangers the prostatic plexus which carries both sympathetic [via hypogastric nerves] and parasympathetic fibers [via pelvic splanchnic nerves] to the penis
• Batson’s venous plexus: many connections exist between pelvic venous networks (e.g. prostatic) and vertebral veins and provides a route for metastasis of cancerous cells to the vertebral column, skull and brain.

Uterine prolapse: protrusion of the cervix into the vaginal – may extend to the external orifice signs/symptoms
Pelvic pain, lower back pain, constipation, dysuria, painful intercourse results from weakness/damage to:
Pelvic diaphragm > urogenital diaphragm > fascial ligaments (uterosacral, transverse cervical)
peritoneal folds (e.g. broad ligament) provide minimal support to the uterus

Pectinate Line• Above the pectinate line, the anal canal is visceral – autonomic
innervation (no “pain”!) and visceral support [lymph: inferior mesenteric nodes; arterial: inferior mesenteric artery; venous: portal system]
• b. Below the pectinate line, the anal canal is somatic – somatic innervation (pain/touch) and somatic support [lymph: superficial inguinal nodes; arterial: pudendal; venous: caval system]

Hemorrhoids• a. Internal hemorrhoids: related to internal rectal plexus and
breakdown of muscularis mucosa; prolapses can result in strangulation and/or ulceration; involves viscera and are painless
• b. External hemorrhoids: involve the external rectal plexus; somatic part of canal and therefore are painful!