peninsula shaped craniectomy for delayed … · peninsula shaped craniectomy for delayed...
TRANSCRIPT

Tiirkish Neiirosiirgery 8: 82 - 86, 1998 Erdiiiçler: Delayed Syiioslosis
Peninsula Shaped Craniectomy for DelayedHolocalvarial Synostosis
Geç Basvuran Holokalvaryal Sinostozlarda Yarimada SeklindeKraniyektomi
PAMIR ERDINÇLERi MEHMET YASAR KA YNARi BÜLENT CANBAZi NEJAT ÇIPLAK,
ALI ÇETIN SARIOGLUi CENGIZ KUDA Y
Istanbul University Cerrahpasa Medical FacuIty Department of Neurosurgery (PE, AÇS, CK),and Institute of Neurological Sciences (MYK, BC, NÇ)1 Istanbul, Turkey
Abstract: Delayed holocalvarial synostosis is anuncommon form of craniosynostosis. We report in thisartiele two children with delayed holocalvarial synostosis.Neurological examination was normal but skull X-raysshowed diffuse digital impressio and synostosis of allcalvarial sutures in both patients. The patients wereoperated with a modified pi craniectomy technique whichrelaxes entire calvarium in coronal, axial and sagittalplans. Control X-rays after surgery showed relief of digitalimpressio in both patients.
Key Word s: Craniosynostosis, digital impressio,surgery
INTRODUCTION
Most of the different types of craniosynostosishave known to be apparent at birth. Oxycephaly canhave a clinical manifestation lateri by the age of two,with signs of increased intracranial pressure (lep).Reddy et aL. (12) focused attention on patients withdelayed and progressive multiple suturecraniosynostosis. They concluded that the patientexhibiting these ra re situations is distinctlyuncommon than the other types of craniosynostosis.
82
Özet: Tüm kalvaryal sütürleri kapsayan geç ortaya çikansinostozlar kranyosinostozun nadir görülen birdurumudur. Bu makalede gecikmis holokalvaryalsinostoz bulgulari ile basvuran iki çocuk hastasunulmustur. Nörolojik muayenelerinde bir özelliksaptanmayan olgularin kranyografilerinde yaygindövülmüs bakir manzarasi ve tüm kalvaryal sütürlerdesinostoz saptandi. Hastalar, tüm kalvaryumu koronal,aksiyal ve sajital planlarda serbestlestirecek sekilde,modifiye pi kranyektomi teknigi kullanilarak ameliyatedildiler. Kontrol kranyografileri iki olguda da dövülmüsbakir manzarasinda azalma gösterdi.
Anahtar Sözcükler: Cerrahi, dövülmüs bakir manzarasiikranyosinostoz
Recently, we have operated two patients withdelayed holocalvarial synostosis. We discuss in thisarticle the clinical and radiological pictures ofdelayed holocalvarial synostosis and our surgicaltechnique for management.
REPORT OF CASES
The first patient was a 5-year-old boy. He wasreferred to our unit due to headache and
dolicocephalic skull shape. Neurological examination
Tiirkish Neiirosiirgery 8: 82 - 86, 1998
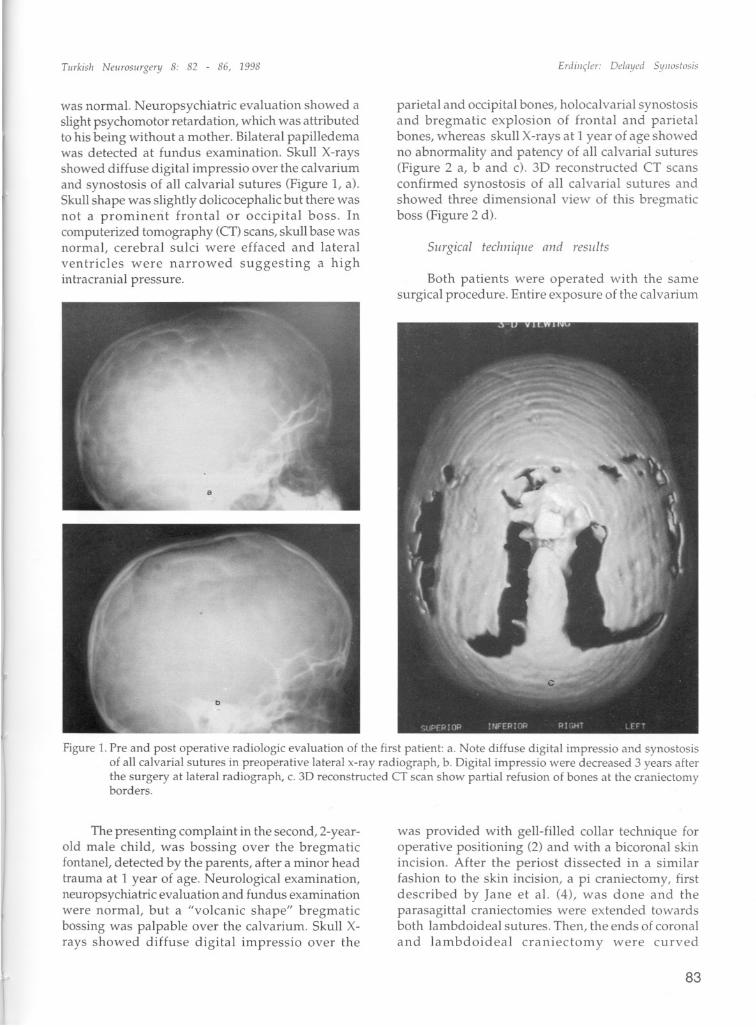
was normaL. Neuropsychiatric evaIuation showed aslight psychomotor retardation, which was attributedto his being without a mother. Bilateral papiHedemawas detected at fundus examination. Skull X-raysshowed diffuse digital impressio over the calvariumand synostosis of all calvarial sutures (Figure 1, a).Skull shape was slightly dolicocephalic but there wasnot a prominent frontal or occipital boss. Incomputerized tomography (CT)seans, skull base wasnormal, cerebral sulci were effaced and lateralventricles were narrowed suggesting a highintracranial pressure.
Erdiiiç/er: Delnyed 51/11o;;lo:,i:,
pari eta iand occipital bones, holocalvarial synostosisand bregmatic explosion of frontal and parietalbones, whereas skull X-rays at 1 year of age showedno abnormality and patency of all calvarial sutures(Figure 2 a, b and c). 3D reconstructed CT seansconfirmed synostosis of all calvarial sutures andshowed three dimensional view of this bregmaticboss (Figure 2 d).
Siirgical techniqiie and results
Both patients were operated with the samesurgical procedure. Entire exposure of the calvarium
Figure 1. Pre and post operatiye radiologic evaiuation of the first patient: a. Note diffuse digital impressio and synostosisof aIl calvarial surures in preoperative lateral x-ray radiograph, b. Oigital impressio were decreased 3 years afterthe surgery at lateral radiograph, c. 30 reconstructed CT sean show partial refusion of bones at the craniectomyborders.
The presenting complaint in the second, 2-yearold male chil d, was bossing over the bregmaticfontane!, detected by the parents, after a minor headtrauma at 1 year of age. Neurological examination,neuropsychiatric evaluation and fundus examinationwere normal, but a "volcanic shape" bregmaticbossing was palpable over the calvarium. Skull Xray s showed diffuse digital impressio over the
was provided with gell-filled coHar technique foroperative positioning (2) and with a bicoronal skinincision. After the periost dissected in asimilarfashion to the ski n incision, a pi craniectomy, firstdescribed by Jane et aL. (4), was done and theparasagittal craniectomies were extended towardsboth lambdoideal sutures. Then, the ends of coranaland lambdoideal craniectomy were curved
83

Tiirkish Neiirosiirgery 8: 82 - 86, 1998 Erriiliçler: Delnyeri Syiiostosis
Figure 2. Pre and post operative radiologic evaIuation of the second patient: a. Antero-posterior radiograph of second patientat 1 year of age show no any abnormality; b, c. Antero-posterior and lateral radiograph of the same patient sho\Vsdigital impressio over the parietal and occipital bones, holocalvarial synostosis and bregmatic bossing, 1 year after,d. Three dimensional view of the volcano shaped bregmatic boss and synostosis of all calvarial sutures are well seenin 3D reconstructed CT scan, e. Digital impressio were completely disappeared 4 months af ter the surgery in skull xrays, f. 3D reconstructed CT scan shows the craniectomy size and the created peninsula shaped parietal bones.
84

Tiirkish Neiirosiirgery 8: 82 - 86, 1998
respectively posteriarly and anteriorly and thus,large "peninsula shaped" parietal bones werecreated. The bregmatic boss in the second patient wasleft in place like an island in the bregmatic part ofthe craniectomy flap in order to avoid any possibledamage to the superior sagittal sinus.
Postoperative course was uneventful in bothpatients, except a decrease in hematocrit levels whichdidnot necessitate blood transfusion. Skull X-raysand 30 reconstructed CT scans of the first patientshowed the craniectomy size and partiallyresynostosed frontal and parietal bones, 3 years afterthe surgery (Figure 1 b and c). The digital impressiowere decreased and the patient had no any othercomplaints and he had a normal performance at theschooL.The second patient showed a dramaticallydecrease of digital impressio in skull X-rays at theend of four months after the operation (Figure 2 e).The 30 reconstructed CT scans show ed the extent of
the craniectomy to the both lambdoideal sutures(Figure 2 f). The bregmatic boss completelydisappeared at the end of 18 months after surgery.
DISCUSSION
Various attempts have been made in the pastto better understand the pathogenesis ofcraniosynostosis. The role of the skull base forprogramming the future aspect of craniofacialgrowth is now widely accepted (l0,11,15). The resultsof premature fusion of sutures are in part manifestedby an abnormal cosmetic appearance, and on theother hand, by various neurological complaints suchas increased ICP and related psychomotorretardation, epilepsy or neuro-ophtalmological signs0,6, 13, 14). The two patients in this artiele had nocosmeticdeformity except a bregmatic bossing in one.
As seen in CT and 30 reconstructed CT scans,there was no involvement of skull base or facial bones
in our patients as in 4 cases reported by Reddy et aL.(2). Zygomatic angle which seems to be non-affectedin 30 CT scans was the indirect sign of the absenceof basal synostosis (9). This situation must bereserved for patients in whom craniosynostosis wasmanifested at birth. In delayed holocalvarialsynostosis, most of the calvarial suture fusion takesplace after the facial and basal skull development iscompleted (l2). Head shapes were normal in onepatient, but slightly dolicocephalic in the other,suggesting a first attempt of sagittal suture. Oelayedholocalvarial synostosis must be differentiated from
Erdil/çler: Deloyed Syl/ostas;s
oxycephaly. Marchac et aL. (8) call oxycephaly theresult of a rather Iate elosure of the coronal suture
and announce that they have never see n oxycephalyin children young er than 2 or 3 years of age. Althougha round skull is sometimes seen, a pointedappearance of the vault, a short orbital roof andresultant exophtalmus, absence of fronto-nasal angleare considered as the keywords of this anomaly (6,8). These features were absent in our patients. In thesecond case, an "explosion" of the bregmatic fontanelafter first year of age was the alerting sign of ananomaly. Ifs probably a herniation of the brain froma single opening of all sutures synostosed calvarium.This event reflect the high capacity of the brain togrow in the first years of life and does not reflectoxycephaly.
The surgical conection of craniosynostosis hasevolved from simple removal of the suture to thevarious applications of cranio-facial principles forbetter esthetic and cosmetic results (3,5,14,17). LInearcraniectomy techniques are generally proposed forscaphocephaly in infancy (14,16). The treatmentprocedure proposed by Reddy et aL. (12) forholocalvarial synostosis was calvarial reshaping andcreation of new sutures by morcellation craniectomy.The important factors for better relaxation of the braincan be created in a multitude of ways e.g. vaultreconstruction utilizing split cranial bone grafts andjudicious use of plates or transposition techniquessuch as advocated by Marchac and Renier (7). Wehave programmed our procedure not only for thecreation of new sutures by linear craniectomy butalso for the relaxation of the brain by extending thecraniectomy as far as the temporal fossa as describedabove. The extending "peninsula shaped" parietalbones to both of the coronal and lambdoideal sutures
and to the temporal fossa, as we have done correctlyin the second case, is an important factor for betterrelaxation of the brain. The neck of the "peninsulashaped" parietal bones must be left in the squamosalpart of the temporal bone in order to give amalleability even if in the face of thickened bones atlater ages. We have observed preoperatively, therelaxation of the brain manifested by amplitudeaugmented brain pulses, immediately after the en tirecraniectomy was achieved in both cases.
This minimalist approach is safe, does not needany fixation or reshaping and allows a completerelaxation of the brain in coronal, sagittal and axialplans.
85

Tiirkish Neiirosiirgery 8: 82 - 86, 1998
Correspondence: Pamir ErdinçlerPK 19, 34312Kocamustafapasa, Istanbul, TurkeyTel: 212-5876585Fax: 212-2732477
REFERENCES
1. Anderson FM: Treatment of coronal and metopicsynostosis: 107 cases. Neurosurgery 8:143-149,1981
2. Francel PC, Beii A, Jane JA: Operative positioningundergoing repair of craniosynostosis. Neurosurgery35:304-306, 1994
3. Hoffman HJ, Mohr G: Lateral canthal advancement ofthe supraorbital margin. A new corrective techniquein the treatment of coronal synostosis. J Neurosurg45:376-381, 1976
4. Jane JA, Edgerton MT, Futrell JW: Immedia te correctionof sagittal synostosis. J Neurosurg 49:705-710,1978
5. Lannelongue M: De la craniectomie dans lamicrocephalie. CR Acad Sci 110:1382-1385, 1890
6. Marchac D, Renier D: Craniofacial surgery forcraniosynostosis. Scand J Plast Reconstr Surg 15:235243, 1981
7. Marchac D, Renier D: Scaphocephaly, in Marchac D,Renier D (eds), Craniofacial Surgery for
86
Erdiiiç/er: Delayeri Syiiostosis
Craniosynostosis, Boston: Little Brown & Company,1982:88-92
8. Marchac D, Renier D, Jones BM: Experience with the"floating forehead". Br J Plast Surg 41:1-15, 1988
9. McCarthy JG, Coccaro PJ, Epstein F, Converse JM:Early skeletal release in the infant with craniofacialdysostosis: The role of the sphenozygomatic suture.Plast Reconstr Surg 62:335-346, 1978
10. Moss ML: The pathogenesis of premature cranialstenosis in man. Acta Anat 37:351-370, 1959
11. Moss ML: Functional anatomy of cranial synostosis.Child's Brain 1:22-33, 1975
12. Reddy K, Hoffman H, Armstrong D: Delayed andprogressive multiple suture craniosynostosis.Neurosurgery 26:442-448, 1990
13. Renier D, Sainte-Rose C, Marchac D: Intracranialpressure in craniostenosis. J Neurosurg 57:370-377,1982
14. Shillito J, Matson DD: Craniosynostosis: a review of519 surgical patients. Pediatrics 41:829-842,1968
15. Smith DW, Töndury G: Origin of the calvaria and itssutures. Am J Dis Child 132:662-666, 1978
16. Stein Sc, Schut L:Management of scaphocephaly. SurgNeurol 7:153-155, 1977
17. Tessier P: Relationship of craniostenoses to craniofacialdysostoses and to faciostenoses. A study of therapeuticimplications. Plast Recostr Surg 48:224-237, 1971