pennsylvania. agitation after traumatic brain injury · demonstrate some aggressive behaviors...
TRANSCRIPT
Authors:Lisa A. Lombard, MDRoss D. Zafonte, DO
Affiliations:From the Department of PhysicalMedicine and Rehabilitation,University of Pittsburgh, TheUniversity of Pittsburgh MedicalCenter–Institute for Rehabilitationand Research, Pittsburgh,Pennsylvania.
Correspondence:All correspondence and requests forreprints should be addressed to RossD. Zafonte, DO, University ofPittsburgh, Rehabilitation, KaufmannMedical Building, 3471 Fifth Avenue,Suite 201, Pittsburgh, PA 15213.
0894-9115/05/8410-0797/0American Journal of PhysicalMedicine & RehabilitationCopyright © 2005 by LippincottWilliams & Wilkins
DOI: 10.1097/01.phm.0000179438.22235.08
Agitation After Traumatic BrainInjuryConsiderations and Treatment Options
ABSTRACT
Lombard LA, Zafonte RD: Agitation after traumatic brain injury: Considerationsand treatment options. Am J Phys Med Rehabil 2005;84:797–812.
Posttraumatic agitation is a challenging problem for acute and rehabilitation staff,persons with traumatic brain injury, and their families. Specific variables forevaluation and care remain elusive. Clinical trials have not yielded a strongfoundation for evidence-based practice in this arena. This review seeks toevaluate the present literature (with a focus on the decade 1995–2005) andemploy previous clinical experience to deliver a review of the topic. We willdiscuss definitions, pathophysiology, evaluation techniques, and treatment regi-mens. A recommended approach to the evaluation and treatment of the personwith posttraumatic agitation will be presented. The authors hope that this reviewwill spur discussion and assist in facilitating clinical care paradigms and researchprograms.
Key Words: Traumatic Brain Injury, Agitation, Delirium, Behavior
One of the more frustrating aspects of care of persons with traumatic braininjury (TBI) is in the management of the agitated patient; agitated patients mayresist direct care, be disruptive on the unit, or even pose a physical risk tothemselves, family, or staff. A specific definition of agitation remains elusive;some have described it as a variation of delirium. It may include inappropriatevocalizing, intolerance of medical management or equipment, and directed ordiffuse aggressive behaviors. Careful consideration of environmental factorsshould be given before medicating a person with agitation. When medicationsare eventually pursued to modulate behavior, measurement of agitation with anobjective tool is highly recommended in determining the success of treatment.
DEFINITIONS/SCOPEThe Rancho Los Amigos scale1 describes agitation as a component of the
fourth stage of recovery; however, some patients are noted to progress fromlocalized responses to confusion and consciousness without any stage of ag-gression. Agitation does seem to correlate with lower cognitive status, as foundby Corrigan and Mysiw2 in an examination of 18 persons with TBI. Ten of the18 patients were found to be agitated. In a study of 28 persons with brain injurydue to stroke, trauma, or anoxia in a rehabilitation facility, 39% were found to
October 2005 Agitation After Traumatic Brain Injury 797
INVITED REVIEW
Brain Injury

demonstrate some aggressive behaviors within thefirst week of admission. There was a significantcorrelation between these behaviors and severity ofinjury and disorientation to time and place.3 In astudy that used a strict definition of agitation, only11 of 100 rehabilitation inpatients with severe TBIwere found to be agitated, and 35 were determinedto experience restlessness. In the majority of per-sons with agitation, the symptoms resolved withina week.4 In contrast, a more recent study5 exam-ined agitation in a cohort of 158 persons with TBIin an inpatient rehabilitation setting; 50% of theirsample experienced agitation, but it typically lasted�10 days. No difference was noted in agitationwith regard to sex.
Some of the variation in the reports of fre-quency of posttraumatic agitation may be a resultof a lack of consensus of the specific definition ofthe term. A group in 1997 attempted to determineclinicians’ definitions of agitation; a survey wasperformed of members of the Brain Injury SpecialInterest Group of the American Academy of Phys-ical Medicine and Rehabilitation.6 The factors ofphysical aggression, explosive anger, increased psy-chomotor activity, impulsivity, verbal aggression,disorganized thinking, perceptual disturbances,and reduced ability to maintain or appropriatelyshift attention were noted by �50% of respondentsto be either “very important” or “essential” to thedefinition of agitation. There was no consensus asto whether agitation was, by its nature, limited tothe period before clearing posttraumatic amnesiaor if it could extend past that time and thus be achronic issue. The unification of the definition ofagitation is highly recommended; the ability tocompare or replicate studies depends on a commonlanguage describing this condition.
We suggest that posttraumatic agitation bedefined as a state of aggression during posttrau-matic amnesia. This state occurs in the absence ofother physical, medical, or psychiatric causes. Itcan be manifested by intermittent or continuousverbal or physical behaviors and can be identifiedby a score of �22 on the Agitated Behavior Scale.7
Akathisia, which can be seen during recoveryfrom TBI, carries a more standardized definition.8
It describes a constant sense of inner restlessness,which may or may not be manifested in motoractivity, ranging from bouncing legs and fidgetinghands to pacing behaviors. It is not limited to braininjury specifically; it has been reported as an extra-pyramidal side effect from ingestion of neurolepticmedications.9 As akathisia does not require thepresence of aggression, it is thus not synonymouswith agitation, although certainly could be a com-ponent of it.
PATHOPHYSIOLOGY
Like definitions of agitation, the specificpathophysiology of posttraumatic aggression re-mains poorly understood. In determining anatomicareas associated with this behavior, three specificsubtypes of aggression have been defined: socialaggression, predatory aggression, and defensive ag-gression.10 In contrast with social and predatoryaggressions, which are associated with more goal-directed acts, defensive aggression is most similarto behaviors seen in persons with TBI, in which theresponse is to a perceived threat, real or otherwise.In cats, the hypothalamus, periaquaductal gray,and limbic structures, such as the amygdala, hip-pocampus, and septal area, have been associatedwith this defensive rage.11 In one case report, a14-yr-old boy with a history of aggression who hadmurdered was found to have a cystic lesion lateralto the right amygdala.12 Temporal lobe epilepsy hasbeen, on rare occasions, associated with interictalaggression; a radiographic survey of persons with ahistory of both temporal lobe epilepsy and aggres-sion revealed a subgroup of patients with signifi-cant amygdala and peri-amygdala atrophy.13 Theimportance of subclinical seizures in disorders ofaggression may be underappreciated.14
From a neurochemical perspective, regulationof aggression seems to be primarily dependent onthe balance of serotonin and dopamine. Exposureto a confrontational situation results in increaseddopamine and decreased serotonin in normalrats.15 5HT-1b knockout mice demonstrate disin-hibition and increased aggression toward othermice.16 Apomorphine, a dopamine agonist, can in-duce aggression in nonaggressive mice, and ad-ministration of a D2 inhibitory agent decreasesaggressive behaviors in high-aggressive strains ofmice.17 However, we do not suggest regular use ofpotent D2 inhibitors in the treatment of posttrau-matic agitation, as it is fraught with the potentialto slow neural recovery (see section on antipsy-chotic agents below).
In humans, particularly low cerebrospinalfluid levels of 5-hydroxyindolacetic acid, a majormetabolite of serotonin, were found in male pris-oners incarcerated for impulsive, aggressivecrimes.18 Nitric oxide seems to have effects onaggression, as well; male mice that lack the neu-ronal nitric oxide synthase gene have significantlydecreased serotonin turnover and clinically dem-onstrate greater intraspecies aggression.19
Dopamine is also implicated in akathisia,which, as stated above, often accompanies post-traumatic agitation. Dopamine transporter geneknockout mice (DAT�/�) demonstrate increasedextracellular dopamine and locomotion but showno increase in aggression.20 In a positron emission
798 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10
tomographic study in humans, administration of apotent D1 receptor antagonist resulted in transientakathisia in both normal controls and schizo-phrenic patients when receptor occupancy reached45–59%. Similar results were seen after adminis-tration of a D2 receptor antagonist.21
To our knowledge, no study has identified aspecific site or mechanism to account for posttrau-matic agitation in humans; it is likely a compli-cated combination of structural lesions, biochem-ical deficits, and external factors that lead to thiscondition.
MONITORING OF AGITATIONWhen determining a treatment plan for an
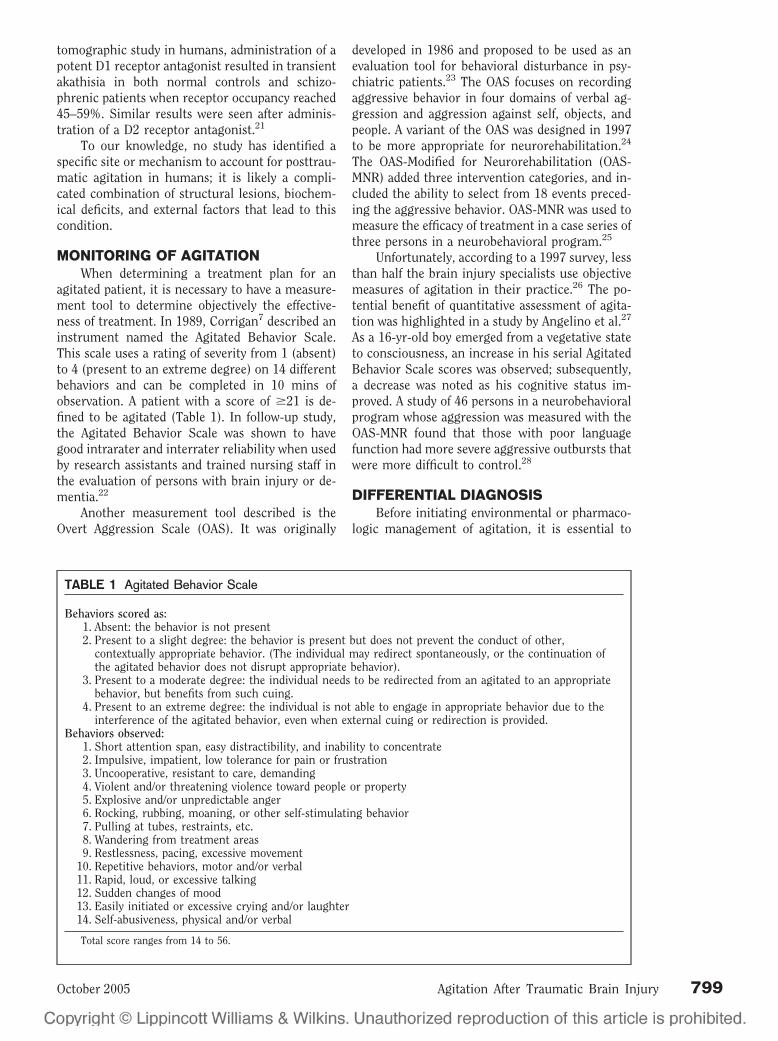
agitated patient, it is necessary to have a measure-ment tool to determine objectively the effective-ness of treatment. In 1989, Corrigan7 described aninstrument named the Agitated Behavior Scale.This scale uses a rating of severity from 1 (absent)to 4 (present to an extreme degree) on 14 differentbehaviors and can be completed in 10 mins ofobservation. A patient with a score of �21 is de-fined to be agitated (Table 1). In follow-up study,the Agitated Behavior Scale was shown to havegood intrarater and interrater reliability when usedby research assistants and trained nursing staff inthe evaluation of persons with brain injury or de-mentia.22
Another measurement tool described is theOvert Aggression Scale (OAS). It was originally
developed in 1986 and proposed to be used as anevaluation tool for behavioral disturbance in psy-chiatric patients.23 The OAS focuses on recordingaggressive behavior in four domains of verbal ag-gression and aggression against self, objects, andpeople. A variant of the OAS was designed in 1997to be more appropriate for neurorehabilitation.24
The OAS-Modified for Neurorehabilitation (OAS-MNR) added three intervention categories, and in-cluded the ability to select from 18 events preced-ing the aggressive behavior. OAS-MNR was used tomeasure the efficacy of treatment in a case series ofthree persons in a neurobehavioral program.25
Unfortunately, according to a 1997 survey, lessthan half the brain injury specialists use objectivemeasures of agitation in their practice.26 The po-tential benefit of quantitative assessment of agita-tion was highlighted in a study by Angelino et al.27
As a 16-yr-old boy emerged from a vegetative stateto consciousness, an increase in his serial AgitatedBehavior Scale scores was observed; subsequently,a decrease was noted as his cognitive status im-proved. A study of 46 persons in a neurobehavioralprogram whose aggression was measured with theOAS-MNR found that those with poor languagefunction had more severe aggressive outbursts thatwere more difficult to control.28
DIFFERENTIAL DIAGNOSISBefore initiating environmental or pharmaco-
logic management of agitation, it is essential to
TABLE 1 Agitated Behavior Scale
Behaviors scored as:1. Absent: the behavior is not present2. Present to a slight degree: the behavior is present but does not prevent the conduct of other,
contextually appropriate behavior. (The individual may redirect spontaneously, or the continuation ofthe agitated behavior does not disrupt appropriate behavior).
3. Present to a moderate degree: the individual needs to be redirected from an agitated to an appropriatebehavior, but benefits from such cuing.
4. Present to an extreme degree: the individual is not able to engage in appropriate behavior due to theinterference of the agitated behavior, even when external cuing or redirection is provided.
Behaviors observed:1. Short attention span, easy distractibility, and inability to concentrate2. Impulsive, impatient, low tolerance for pain or frustration3. Uncooperative, resistant to care, demanding4. Violent and/or threatening violence toward people or property5. Explosive and/or unpredictable anger6. Rocking, rubbing, moaning, or other self-stimulating behavior7. Pulling at tubes, restraints, etc.8. Wandering from treatment areas9. Restlessness, pacing, excessive movement
10. Repetitive behaviors, motor and/or verbal11. Rapid, loud, or excessive talking12. Sudden changes of mood13. Easily initiated or excessive crying and/or laughter14. Self-abusiveness, physical and/or verbal
Total score ranges from 14 to 56.
October 2005 Agitation After Traumatic Brain Injury 799

address other causes of acute mental statuschanges. Other factors may either contribute to orbe misdiagnosed as posttraumatic agitation. Infec-tions are very common in trauma patients and maylead to delirium. Rapid catecholamine release, asoccurs in hypoglycemic or hypoxic states, can re-sult in aggressive behaviors. Although its exactcause is unclear, “sundowning” may cause in-creased confusion in afternoons or evenings inpatients with dementia.
Drug and alcohol abuse are common co-mor-bidities with TBI. Acute alcohol withdrawal, hall-marked by hypertension, tachycardia, hallucina-tions, disorientation, and agitation, can occur aslate as 72 hrs after the last drink.29 Delirium tre-mens can be managed with benzodiazepines. Thetiming of opioid withdrawal is dependent on thepharmacology of the agent used. Heroin with-drawal symptoms peak at 24–48 hrs after last in-gestion, whereas methadone withdrawal can occurin 3 days. Restlessness, abdominal pain, yawning,and piloerection may be seen. Although hallucina-tions and other mental status changes are rare,persons experiencing these symptoms may becomeagitated and violent in attempts to resume theirdrug of abuse. Withdrawal from benzodiazepinesmay be recognized by hypertension, tachycardia,diaphoresis, tremors, hyperthermia, and seizures;symptoms may begin in 2–7 days and can last aslong as 3 wks. A slow taper of a long-acting ben-zodiazepine can be helpful in reducing symp-toms.30
Epilepsy can be a common complication afterTBI, but focal seizures may not be easily recog-nized; in a study by Vespa et al.,14 22% of personswith TBI screened with electroencephalography inthe intensive care unit (ICU) setting had seizures,and 52% of those were not apparent clinically.Those in a postictal state may be confused and bemisdiagnosed as having intermittent agitation. Asdescribed above, epilepsy arising from the mesialtemporal lobe may be associated with confusion oranxiety and is typically followed by a confusedpostictal period.
Endocrine dysfunction is both a common and,likely, an underdiagnosed consequence of TBI.31
Hyperthyroidism alone may result in significantanxiety and agitation;32,33 however, persons withTBI are more likely to be hypothyroidal after inju-ry.34,35 One case report describes a TBI inpatientwith persistent agitation, hyponatremia, and ortho-stasis. The patient was diagnosed with primaryadrenal insufficiency, and his ability to participatein therapies improved after treatment.36 Hypona-tremia has, in a few occasions, been associated withdelirium in both ICU37 and elderly hospitalizedpopulations.37 In persons with TBI, it seems that
isolated hyponatremia can be seen with a decreasein cognitive function.38
ENVIRONMENTAL CAUSES ANDTREATMENT
Acute care hospitals, especially in ICU set-tings,39 can be very noisy, distractible environ-ments. Constant stimulation in the form of fre-quent assessment of vital signs, audible alarms,around-the-clock medication administration, con-stant lighting, and ambient hallway noise can re-sult in “ICU syndrome,” an acute confusional stateseen even in those without primary brain patholo-gy.40 Although many of these distractions are nec-essary, every attempt should be made to reducestimulation, especially at nighttime.
In the rehabilitation setting, there is oftenmore flexibility in scheduling rest breaks, restora-tion of day and night patterns, and ensuring a quietnight environment. Therapies and meals may bescheduled in an isolated area. Persons with akathi-sia pose additional needs; many of these patientsbenefit from movement and may be calmed bybeing wheeled or walked around the unit. Directphysical restraints, such as vest or wrist restraints,and intravenous lines may create an additionalsource of irritation. When possible, restraintsshould be minimized, or changed to noncontactrestraints, such as netted beds to prevent falls andone-to-one staff supervision to prevent intravenouslines, gastrostomy tubes, and cervical collars frombeing pulled. Protectors or binders should be con-sidered when clinically feasible. Patients with re-straints do need to be monitored closely by staff; arecent recall of a particular brand of netted bedshighlights the potential dangers of equipmentwhen patients are left unattended.41 Maximal re-duction of lines, urinary catheters, and nasogastrictubes should be attempted as soon as possible, aspotentially hazardous consequences may resultfrom manipulation of lines by the patient.42 Bind-ers and other covers for lines provide a barrier forthe patient, which may allow for reduction of re-straint needs. Simple environmental alterationsmay reduce unwanted behaviors; in one study, theinitiation of a staff education program regardingagitation and the placement of patients on a sched-uled toileting program resulted in fewer verbaloutbursts in a heterogeneous population in a long-term care facility.43
In addition to external factors, persons withTBI have innately disturbed sleep cycles. In onesurvey of persons admitted to inpatient rehabilita-tion after TBI, 50% described difficulty sleeping.44
Interestingly, they found that the more severe theinjury, the less likely the patient reported sleepdisturbance. Sleep-disordered breathing seems tobe the most common disturbance noted in acute
800 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10
TBI.45,46 Careful monitoring of sleep cycles andquality of sleep is indicated in all persons with TBI.
Pain is a well-recognized cause of agitation indemented elders.47,48 Persons with TBI have manypotential pain generators: musculoskeletal inju-ries, spasticity, heterotopic bone, and iatrogeniccauses, such as lines, tracheostomies, and gastros-tomy tubes. Many associated injuries may be ini-tially undiagnosed.49 The inability to voice paincomplaints may lead to frustration and agitation.Regular monitoring of pain control, either by pa-tient reports or by observation of behaviors is anessential component of agitation management.However, as opioids can be sedating, they should beused judiciously in this population.
BEHAVIORAL MODIFICATIONIn addition to the above environmental alter-
ations, structured behavioral programs may also beconsidered. Prigatano et al.50 provided an excellentmodel from which to base a behavioral program inthe treatment of psychiatric disorders after TBI.They introduced the “ICAR” model: information,whereby patients or families, or both, are providedwith objective information regarding the patient’scognitive status; contingencies, whereby patientsmay suffer ramifications from engaging in unde-sirable behaviors; improving self-awareness,whereby various techniques are suggested to en-courage self-monitoring of performance; relation-ship, whereby the psychotherapeutic relationshipis used in conjunction with cognitive rehabilita-tion. Although there are aspects of this model thatcertainly would be of limited utility in persons withsignificant cognitive or communication impair-ments, there are some aspects that may aide con-trol of behaviors in persons with TBI-related agi-tation.
MEDICATIONSAs several studies suggest that agitation in
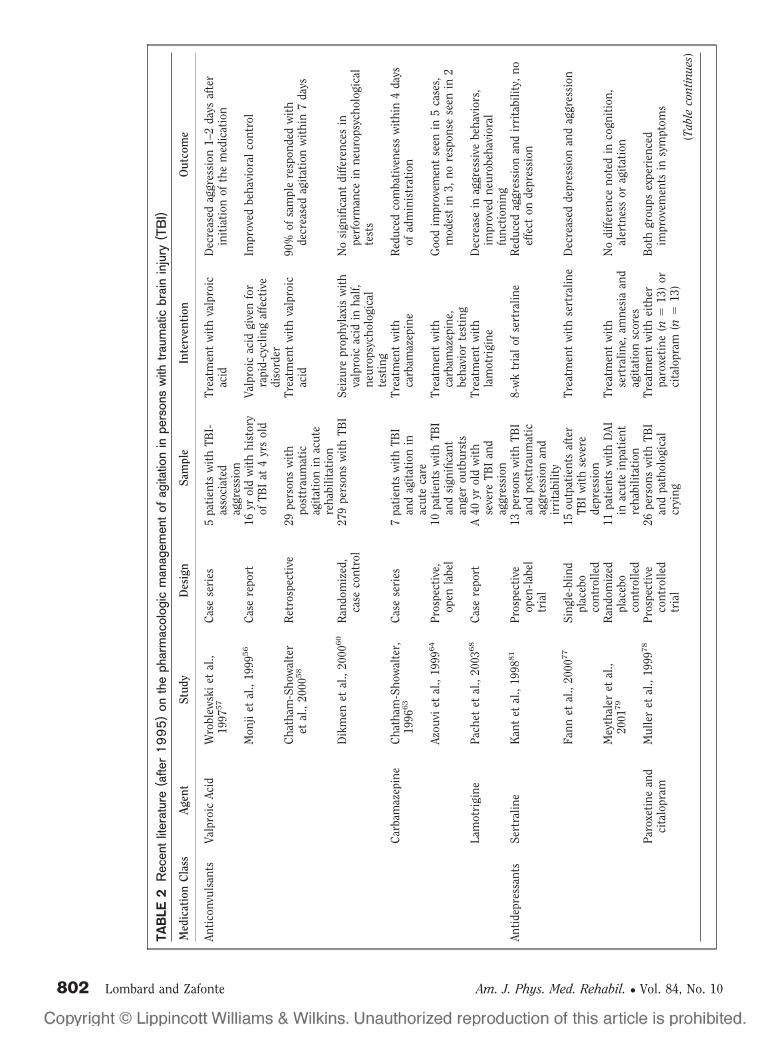
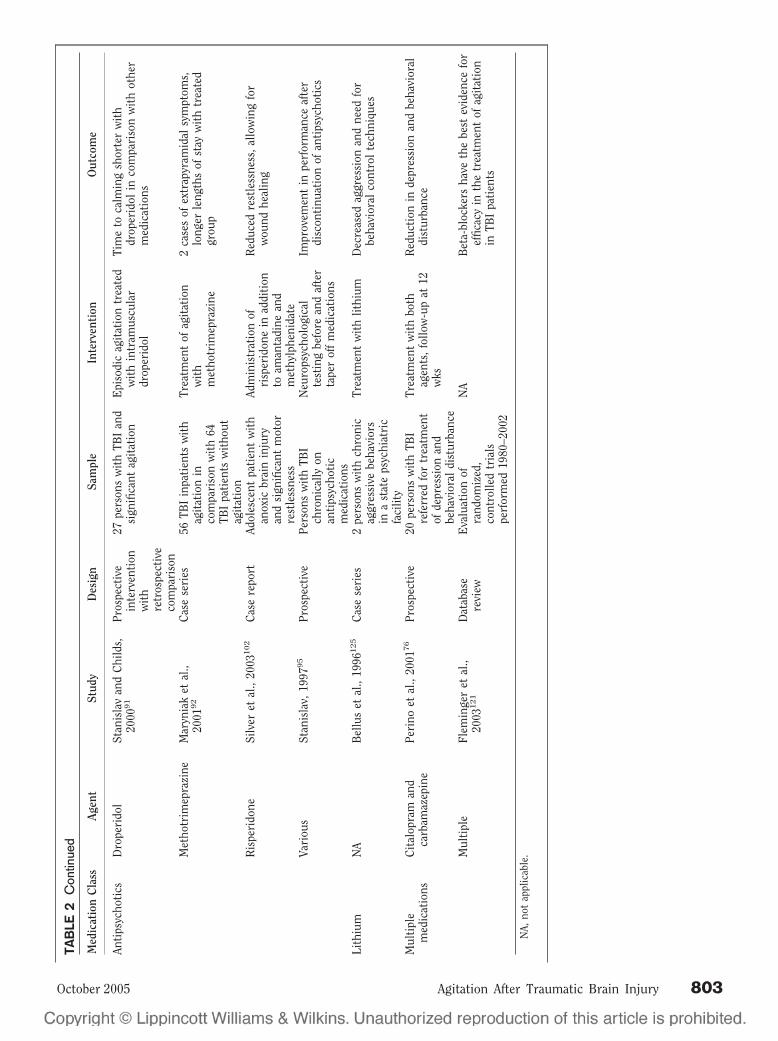
most cases may be time-limited to �10 days,4,5 aconvincing argument could be made to “ride thestorm” of agitation and wait for the recovery pro-cess to resolve the behavioral issues without thepotential risks of medication side effects. However,with potential risk of injury to the patient or staffmembers and the current climate of pressure toshorten rehabilitation days, pharmacologic mea-sures can be considered in persons with agitationrefractory to environmental or behavioral modifi-cations (as mentioned in “ENVIRONMENTALCAUSES AND TREATMENT”). A summary of theliterature of the past 10 yrs (published after 1995)of medications used for TBI-related agitation canbe found in Table 2.
AnticonvulsantsOne of the more commonly recognized anti-
convulsants in the control of behavior is valproicacid; it has long been used for the treatment ofmania in bipolar disorder.51 Although it has beensuggested by some as a treatment for dementia-related agitation,52–54 a recent Cochrane databasereview suggests that its sedative side effects out-weigh any potential benefit in this population.55
Monji et al.56 reported success in the treatment ofa rapid cycling affective disorder with valproic acidin a 16-yr-old patient with a history of TBI at 4 yrsof age. In a study of five patients with TBI-relatedaggression who failed multiple pharmacologictreatments, valproic acid did reduce the undesir-able behaviors.57 Valproic acid was shown to beefficacious in the treatment of agitation within aweek of administration in 26 of 29 persons admit-ted to an inpatient brain injury rehabilitationunit.58 Although valproic acid has been shown tohave some effects on cognition in epileptics andnormal controls,59 no significant effects on neuro-psychological testing were seen in a double-blindedstudy of 279 persons with TBI who were given themedication for posttraumatic seizure prophylax-is.60 One of the benefits of valproic acid is thepotential for a rapid load (10–20 mg/kg/day). Itsmaximum dose is limited mainly by hepatotoxicity,thrombocytopenia, and medication toxicity. Onestudy does suggest that persons with TBI maydemonstrate increased metabolism of valproic acid,and thus this population may require higher dos-es.61
Another anticonvulsant used in the TBI popu-lation is carbamazepine, which although maycause some motor slowing, has effects of question-able clinical significance on cognitive tasks in onestudy.62 Chatham-Showalter63 described the suc-cessful use of carbamazepine in a series of sevenacute inpatients with combativeness after TBI re-fractory to other medications. In another study,carbamazepine was found to significantly improveAgitated Behavior Scale scores without alterationof Mini-Mental Status Examination scores in eightof ten patients treated; particular areas of improve-ment cited were in irritability and disinhibition.64
Its major side effects include hyponatremia, renalfailure, and in rare cases, aplastic anemia. Al-though dosing level is to therapeutic effect, serumlevels should be monitored to avoid toxicity. Gaba-pentin has been reported to be helpful in modulat-ing agitation related to dementia.65,66 However, acase series reported paradoxical effects in two per-sons with TBI treated with gabapentin for neuro-pathic pain.67 Other similar membrane-stabilizingagents, such as lamotrigine,68 may be of use in
October 2005 Agitation After Traumatic Brain Injury 801
TAB
LE2
Rec
entl
itera
ture
(afte
r1
99
5)
onth
eph
arm
acol
ogic
man
agem
ento
fag
itatio
nin
pers
ons
with
traum
atic
brai
nin
jury
(TB
I)
Med
icat
ion
Cla
ssA
gent
Stud
yD
esig
nSa
mpl
eIn
terv
enti
onO
utco
me
Anti
conv
ulsa
nts
Valp
roic
Acid
Wro
blew
ski
etal
.,19
9757
Cas
ese
ries
5pa
tien
tsw
ith
TBI-
asso
ciat
edag
gres
sion
Trea
tmen
tw
ith
valp
roic
acid
Dec
reas
edag
gres
sion
1–2
days
afte
rin
itia
tion
ofth
em
edic
atio
n
Mon
jiet
al.,
1999
56
Cas
ere
port
16yr
old
wit
hhi
stor
yof
TBI
at4
yrs
old
Valp
roic
acid
give
nfo
rra
pid-
cycl
ing
affe
ctiv
edi
sord
er
Impr
oved
beha
vior
alco
ntro
l
Cha
tham
-Sho
wal
ter
etal
.,20
0058
Ret
rosp
ecti
ve29
pers
ons
wit
hpo
sttr
aum
atic
agit
atio
nin
acut
ere
habi
litat
ion
Trea
tmen
tw
ith
valp
roic
acid
90%
ofsa
mpl
ere
spon
ded
wit
hde
crea
sed
agit
atio
nw
ithi
n7
days
Dik
men
etal
.,20
0060
Ran
dom
ized
,ca
seco
ntro
l27
9pe
rson
sw
ith
TBI
Seiz
ure
prop
hyla
xis
wit
hva
lpro
icac
idin
half,
neur
opsy
chol
ogic
alte
stin
g
No
sign
ifica
ntdi
ffere
nces
inpe
rfor
man
cein
neur
opsy
chol
ogic
alte
sts
Car
bam
azep
ine
Cha
tham
-Sho
wal
ter,
1996
63
Cas
ese
ries
7pa
tien
tsw
ith
TBI
and
agit
atio
nin
acut
eca
re
Trea
tmen
tw
ith
carb
amaz
epin
eR
educ
edco
mba
tive
ness
wit
hin
4da
ysof
adm
inis
trat
ion
Azou
viet
al.,
1999
64
Pros
pect
ive,
open
labe
l10
pati
ents
wit
hTB
Ian
dsi
gnifi
cant
ange
rou
tbur
sts
Trea
tmen
tw
ith
carb
amaz
epin
e,be
havi
orte
stin
g
Goo
dim
prov
emen
tse
enin
5ca
ses,
mod
est
in3,
nore
spon
sese
enin
2
Lam
otri
gine
Pach
etet
al.,
2003
68
Cas
ere
port
A40
yrol
dw
ith
seve
reTB
Ian
dag
gres
sion
Trea
tmen
tw
ith
lam
otri
gine
Dec
reas
ein
aggr
essi
vebe
havi
ors,
impr
oved
neur
obeh
avio
ral
func
tion
ing
Anti
depr
essa
nts
Sert
ralin
eK
ant
etal
.,19
9881
Pros
pect
ive
open
-lab
eltr
ial
13pe
rson
sw
ith
TBI
and
post
trau
mat
icag
gres
sion
and
irri
tabi
lity
8-w
ktr
ial
ofse
rtra
line
Red
uced
aggr
essi
onan
dir
rita
bilit
y,no
effe
cton
depr
essi
on
Fann
etal
.,20
0077
Sing
le-b
lind
plac
ebo
cont
rolle
d
15ou
tpat
ient
saf
ter
TBI
wit
hse
vere
depr
essi
on
Trea
tmen
tw
ith
sert
ralin
eD
ecre
ased
depr
essi
onan
dag
gres
sion
Mey
thal
eret
al.,
2001
79
Ran
dom
ized
plac
ebo
cont
rolle
d
11pa
tien
tsw
ith
DAI
inac
ute
inpa
tien
tre
habi
litat
ion
Trea
tmen
tw
ith
sert
ralin
e,am
nesi
aan
dag
itat
ion
scor
es
No
diffe
renc
eno
ted
inco
gnit
ion,
aler
tnes
sor
agit
atio
n
Paro
xeti
nean
dci
talo
pram
Mul
ler
etal
.,19
9978
Pros
pect
ive
cont
rolle
dtr
ial
26pe
rson
sw
ith
TBI
and
path
olog
ical
cryi
ng
Trea
tmen
tw
ith
eith
erpa
roxe
tine
(n�
13)
orci
talo
pram
(n�
13)
Bot
hgr
oups
expe
rien
ced
impr
ovem
ents
insy
mpt
oms
(Tab
leco
ntin
ues)
802 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10
TAB
LE2
Con
tinue
d
Med
icat
ion
Cla
ssA
gent
Stud
yD
esig
nSa
mpl
eIn
terv
enti
onO
utco
me
Anti
psyc
hoti
csD
rope
rido
lSt
anis
lav
and
Chi
lds,
2000
91
Pros
pect
ive
inte
rven
tion
wit
hre
tros
pect
ive
com
pari
son
27pe
rson
sw
ith
TBI
and
sign
ifica
ntag
itat
ion
Epi
sodi
cag
itat
ion
trea
ted
wit
hin
tram
uscu
lar
drop
erid
ol
Tim
eto
calm
ing
shor
ter
wit
hdr
oper
idol
inco
mpa
riso
nw
ith
othe
rm
edic
atio
ns
Met
hotr
imep
razi
neM
aryn
iak
etal
.,20
0192
Cas
ese
ries
56TB
Iin
pati
ents
wit
hag
itat
ion
inco
mpa
riso
nw
ith
64TB
Ipa
tien
tsw
itho
utag
itat
ion
Trea
tmen
tof
agit
atio
nw
ith
met
hotr
imep
razi
ne
2ca
ses
ofex
trap
yram
idal
sym
ptom
s,lo
nger
leng
ths
ofst
ayw
ith
trea
ted
grou
p
Ris
peri
done
Silv
eret
al.,
2003
102
Cas
ere
port
Adol
esce
ntpa
tien
tw
ith
anox
icbr
ain
inju
ryan
dsi
gnifi
cant
mot
orre
stle
ssne
ss
Adm
inis
trat
ion
ofri
sper
idon
ein
addi
tion
toam
anta
dine
and
met
hylp
heni
date
Red
uced
rest
less
ness
,al
low
ing
for
wou
ndhe
alin
g
Vari
ous
Stan
isla
v,19
9795
Pros
pect
ive
Pers
ons
wit
hTB
Ich
roni
cally
onan
tips
ycho
tic
med
icat
ions
Neu
rops
ycho
logi
cal
test
ing
befo
rean
daf
ter
tape
rof
fm
edic
atio
ns
Impr
ovem
ent
inpe
rfor
man
ceaf
ter
disc
onti
nuat
ion
ofan
tips
ycho
tics
Lith
ium
NA
Bel
lus
etal
.,19
96125
Cas
ese
ries
2pe
rson
sw
ith
chro
nic
aggr
essi
vebe
havi
ors
ina
stat
eps
ychi
atri
cfa
cilit
y
Trea
tmen
tw
ith
lithi
umD
ecre
ased
aggr
essi
onan
dne
edfo
rbe
havi
oral
cont
rol
tech
niqu
es
Mul
tipl
em
edic
atio
nsC
ital
opra
man
dca
rbam
azep
ine
Peri
noet
al.,
2001
76
Pros
pect
ive
20pe
rson
sw
ith
TBI
refe
rred
for
trea
tmen
tof
depr
essi
onan
dbe
havi
oral
dist
urba
nce
Trea
tmen
tw
ith
both
agen
ts,
follo
w-u
pat
12w
ks
Red
ucti
onin
depr
essi
onan
dbe
havi
oral
dist
urba
nce
Mul
tipl
eFl
emin
ger
etal
.,20
03121
Dat
abas
ere
view
Eva
luat
ion
ofra
ndom
ized
,co
ntro
lled
tria
lspe
rfor
med
1980
–200
2
NA
Bet
a-bl
ocke
rsha
veth
ebe
stev
iden
cefo
ref
ficac
yin
the
trea
tmen
tof
agit
atio
nin
TBI
pati
ents
NA,
not
appl
icab
le.
October 2005 Agitation After Traumatic Brain Injury 803

TBI-related agitation; however, no studies beyondcase reports have been reported.
Antidepressant AgentsBefore the advent of selective-serotonin re-
uptake inhibitors (SSRIs), tricyclic antidepressantswere the most commonly used medication in thepharmacological treatment of both idiopathic de-pression and mood disorders related to organicbrain disease.69,70 In TBI, specifically, tricyclic an-tidepressants with predominantly noradrenergicaction (e.g., protriptyline and desipramine) haveshown some efficacy in the treatment of hy-poarousal.71,72 Other tricyclic antidepressants thatdemonstrate greater affinity for serotonergic recep-tors (e.g., amitriptyline and imipramine) have asignificant sedative side effect profile and thus havesome potential to reduce aggression. An early casereport described the successful treatment of a pa-tient with frontal lobe damage and aggression withamitriptyline.73 It seems that the cause of the ag-itation may determine success with this medica-tion; in a study by Mysiw et al.,74 12 out of 17agitated persons with TBI in posttraumatic amne-sia responded well to amitriptyline, whereas two ofthree patients out of posttraumatic amnesia failedto respond. Despite these successes, due to itssedative and cardiac effects and potential reductionof seizure threshold,75 its utility is limited in theTBI population.
SSRIs offer the appeal of a more benign side-effect profile than with tricyclic antidepressants.They have been shown to be efficacious in thetreatment of depression in persons with TBI.76,77
An additional use for this class is in the treatmentof emotional lability.78 Equivocal results were ob-tained in a small study of sertraline for hypoarousalin TBI patients.79 A case series of two patients withagitation associated with Huntington’s diseaseshowed that sertraline was helpful in reducing ir-ritability and aggressive behaviors.80 In 13 outpa-tients with TBI, treatment with sertraline for 8 wksreduced irritability and aggression, but it had noeffect on depressive symptoms.81 One major draw-back of this class is that, at least for its antidepres-sant effects, �2 wks is needed for effectiveness; thiswould be an unacceptable amount of time to waitfor the control of severe agitation. Unlike the tri-cyclic agents, it seems that SSRIs may not have assignificant of an effect on seizure frequency; in astudy of 100 persons with epilepsy, five developedincreased seizure frequency, but all returned tobaseline with adjustments in seizure medica-tions.82
A newer phenylpiperazine serotonergic agentcommonly used for sleep-cycle regulation in TBI istrazodone. It has been shown in some studies todecrease agitation and aggressive behaviors in both
persons with dementia83,84 and progressive su-pranuclear palsy.85 However, a recent CochraneDatabase Study questions its efficacy in elderlydemented patients.86 Starting dose can be 50–100mg, with results of increased sleep usually seen by150 mg. Care must be given when using this med-ication in those who are also taking SSRIs to avoidpotential serotonin syndrome. Other side effectsattributed to this medication include anticholin-ergic symptoms and priapism.87
Buspirone, as a serotonergic and weak dopa-minergic agent, is known to have significant anxi-olytic properties without sedation. Levine88 ini-tially reported incidental findings of improvementin agitation in three persons with TBI who weregiven this medication; this has been supported inlater studies.89,90 As buspirone may induce sei-zures, care should be taken in its use with personswith TBI.
Antipsychotic AgentsTypical antipsychotic agents have often been
used for the immediate control of aggression oragitation in TBI patients; in the case of haloperidol,it can be given intravenously, intramuscularly, ororally, and it has a rapid onset of action. Intramus-cular administration of droperidol, another mem-ber of the butyrophenone class, was found to befaster and superior in controlling acute episodes ofagitation when compared with haloperidol, diphen-hydramine, or lorazepam.91 Maryniak et al.92 de-scribe their successful use of scheduled oralmethotrimeprazine, from the older phenothiazineclass of antipsychotics, in persons with TBI admit-ted to their inpatient rehabilitation unit; it hadbeen used in almost half of their agitated inpatients(n � 56), with only two persons experiencing sideeffects of extrapyramidal symptoms and paradoxi-cal akathisia. Although those treated with metho-trimeprazine had longer periods of posttraumaticamnesia and lengths of stay, the authors assert thatthe patients with agitation as a group are typicallymore seriously injured than those without behav-ioral issues.
There is, however, some concern with the useof typical antipsychotic agents in persons with TBI.Research by Feeney et al.93 showed that haloperidolslowed motor recovery in an animal model of TBI.In a study of humans, although haloperidol did notchange eventual rehabilitation outcome, its usewas associated with a longer period of time inposttraumatic amnesia.94 Improvements in neuro-psychological test results were seen in a populationof adults with TBI after a taper off chronic typicalantipsychotic agents.95 As with any patient group,neuroleptic malignant syndrome has been reportedin the administration of antipsychotic agents topersons with TBI;96–98 presenting symptoms can
804 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10

include significant fever, leukocytosis, and musclestiffness and can carry a mortality rate of �10%.99
Treatment is with dantrolene and beta-blockers.Persons receiving these medications are also sub-ject to extrapyramidal side effects of tardive dyski-nesia and Parkinsonism, which could form lifelongsources of disability.
The source of these adverse effects seems to bethe typical antipsychotics’ particular affinity forblocking the D2 dopamine receptor; a newer gen-eration of neuroleptics, termed atypical antipsy-chotics, has less D2 receptor activity and more5HT-2a activity, theoretically reducing some of theundesirable effects and alpha adrenergic blockade.In an animal study evaluating the effects of anti-psychotic agents on cognitive function after TBI,haloperidol was shown to increase Morris watermaze time, whereas olanzapine did not.100 In anearly study of the oldest atypical antipsychotic,clozapine, nine persons with TBI demonstratingrage and aggression were given this medication;three responded favorably and three had mild im-provements in behavior, but two patients devel-oped seizures.101 Frequent blood draws for evalua-tion of agranulocytosis are required for patients onclozapine. Risperidone, in combination with meth-ylphenidate and amantadine, was shown to de-crease restlessness in a 15-yr-old patient with an-oxic brain injury.102 However, the powerfuladrenergic and D2 blockade of this agent may raiseconcerns. In addition, a recent study in an animalmodel of TBI has suggested that at high doses,risperidone has a cognitive effect similar to halo-peridol (A. Kline, personal communication, unpub-lished data, 2005).
BenzodiazepinesBenzodiazepines remain a core medication for
sedation in the ICU and for surgical procedures.Short-acting agents (e.g., midazolam, lorazepam)and long-acting agents (e.g., diazepam, clonaz-epam) exist in both enteral and parenteral forms,allowing for a range of administrations. Short-acting benzodiazepines are commonly used in thetreatment of acute mania and other psychiatricemergencies and, in one study, have been shown tobe superior to haloperidol in the treatment of mo-tor agitation in this population.103 Their utility inthe treatment of acute alcohol withdrawal has beendiscussed earlier. In addition, benzodiazepineshave been shown to be efficacious in the treatmentof neuroleptic-induced akathisia.104,105
In brain injury, the effects of benzodiazepinesare more complex. Early and daily administrationof diazepam significantly impaired motor recoveryin rats with cortical lesions; later administration indiazepam-naı̈ve injured rats produced a transient
reoccurrence of hemiparesis.106 In eight personswith a distant history of stroke, light sedation withmidazolam resulted in reemergence of strokesymptoms.107 Benzodiazepines are thus consideredby some to be in the group of potentially detrimen-tal medications in persons with stroke108 and braininjury.109,110 Benzodiazepine administration mayresult in paradoxical agitation in a small subpopu-lation of patients, particularly in the elderly; it canbe successfully treated with flumazneil.111,112 El-derly patients who take benzodiazepines regularlyhave lower functional status than those who donot.113 By its nature, this class of medicationscauses an amnestic effect and may increase confu-sion in those emerging from posttraumatic amne-sia. It is not without any utility in this population;as an agent that potentiates the GABAA receptor, italso can be used as a treatment for spasticity. Inaddition, a case report by Caradoc-Davies114 sug-gested it has potential use in the treatment ofmutism in persons with TBI. It is the authors’opinion that, outside of their utility in the treat-ment of alcohol withdrawal, benzodiazepinesshould be used in emergency situations only andnot be utilized in frequent dosing for the treatmentof agitation.
Beta-BlockersAs a frequently used medication for the treat-
ment of hyperadrenergic states after TBI, beta-blockers may also help in the reduction of agita-tion. Early studies suggest that atenolol can behelpful in the treatment of alcohol withdrawal,with reduction of agitation and anxiety and in morerapid normalization of vital signs.115 Beta-blockadehas also been shown to be efficacious in managingakathisia due to either neuroleptic agents116–118 orto Parkinson’s disease;116 lipophilic beta-blockers,such as propranolol and metoprolol, were particu-larly effective, suggesting a central mode of ac-tion.116,118 In persons with dementia, low-dose pro-pranolol monotherapy was shown to decreaseagitation, aggression, and wandering behaviors.119
Pindolol was reported to reduce violent behaviorsin 8 of 13 inpatients with TBI in a double-blind,placebo-controlled trial, and in some, it reducedcare needs due to improved behavioral manage-ment.120 A Cochrane database review of studiesexamining medications in the treatment of post-traumatic agitation found that beta-blockers hadthe best evidence for efficacy.121 The major limit-ing factor in the administration of beta-blockers ishypotension and bradycardia, but as many patientsmay present with aspects of hyperadrenergia, thesemedications may serve to treat two clinical prob-lems at once.
October 2005 Agitation After Traumatic Brain Injury 805

LithiumLithium carbonate has long been a mainstay
treatment of mania and bipolar disease.122 Al-though specific details of its method of action areunknown, it is recognized to primarily alter so-dium transport and increase intracellular metabo-lism of catecholamines. However lithium doesseem to have some dopamine blocking effects, as itseems to inhibit the response to apomorphine in ananimal model.123 Cohn et al.124 published one ofthe earliest reports of its use in persons with braininjury; they successfully treated a 12-yr-old boywho exhibited agitated and hypomanic behaviorswith a 6-mo course of lithium. Two adults withbrain injury–related aggression so severe they wereadmitted to a state psychiatric facility displayedreductions in frequency of outbursts and in othermedication needs when placed on lithium.125 Inthe rehabilitation setting, a group of ten TBI pa-tients with severe aggression were administeredlithium; although five of these persons had signif-icant improvement measured by improved partici-pation in rehabilitation, three had significant sideeffects that required discontinuation.126 Silver etal.127 have suggested that lithium use in TBI bereserved for those whose aggression is related tomanic effects and for those whose recurrent irrita-bility is related to cyclic mood disorders.
Lithium should be started at 300 mg twice aday and titrated by serum levels and side effects. Itstoxicity level (�1.4 mEq/liter) is very close to itstherapeutic range (0.6–1.2 mEq/liter), and thus,levels should be closely monitored. Significant ad-verse reactions to lithium are often related to highserum levels and may include movement disorders,ranging from tremor to dystonia, seizures, hypo-thyroidism, bradycardia, and vomiting. Those withcentral nervous system dysfunction may beuniquely sensitive to lithium’s side effects;128 thus,the difficulties in managing this medication oftendetract from its potential utility in the treatment ofagitated TBI patients.
NeurostimulantsAlthough it would seem that the administra-
tion of neurostimulant medications might becounterproductive in the management of agitatedTBI patients, it seems that they do have a role. Inhumans, dopaminergic agents, such as amantadineand bromocriptine, have been shown to be effica-cious in the treatment of low-level states129,130 andin increasing the rate of both motoric and cogni-tive recovery.131,132 Bromocriptine has been sug-gested as a treatment of TBI-induced akathisia intwo case reports;133,134 however, it may causemovement disorders as a side effect. In an earlystudy, amantadine was shown to reduce agitationin 7 of 19 persons with dementia. However, adverse
effects of overactivity, anxiety, and visual halluci-nations were seen in eight of the test subjects.135
Studies performed on the brain injury populationhave demonstrated its utility in the treatment ofsevere impairments of consciousness129,136,137 andin the enhancement of higher-level cognitive func-tion.131,138,139 Amantadine’s utility as a mood-sta-bilizing agent was shown in several small caseseries in persons with agitation due toTBI.137,140,141 Because of this potential to both en-hance recovery and control undesirable behaviors,it has been identified by experts in brain injuryrehabilitation as a preferred agent for the treat-ment of agitation.26 Methylphenidate has beenshown to help with concentration and processingdeficits after TBI.142,143 In one randomized, place-bo-controlled study of 38 persons with chronicTBI-related anger, 30 mg daily of methylphenidatesignificantly reduced these behaviors.144
Other Agents and ModalitiesThere are a number of promising treatment
avenues that merit further study. As stated above,there is a paucity of literature examining the po-tential benefits of newer anticonvulsant agents,such as lamotrigine and levetiracetam. As a com-bination SSRI and norepinephrine reuptake inhib-itor, duloxetine may also have benefits as both aneurostimulant and a mood-stabilizing agent.
A 1995 case report described the successfultreatment of severe agitation unresponsive to phar-macologic measures with electroconvulsive ther-apy. A course of six brief-pulse treatments resultedin improved participation in self-care skills andresponse to medication.145 Although this treat-ment certainly should not be first-line manage-ment, further studies to investigate its potentialuse in intractable posttraumatic agitation are inorder.
An additional treatment that has demonstratedpromise in other arenas is magnesium. It has beenshown as an effective treatment for mania in per-sons with bipolar disorder.146–148 It may have ben-efits beyond behavioral management; magnesiumhas been shown to have neuroprotective propertiesin acute TBI. Three studies in rats showed im-proved behavioral149 and motoric150,151 recoverywhen magnesium was administered acutely afterinjury. A potential mechanism was suggested byUstun et al.;152 magnesium reduced the typicaldecline of the antioxidants superoxide dismutaseand glutathione peroxidase in a model of braininjury in rabbits.
Alternative medications also remain under-ex-amined treatments in persons with TBI. Lavenderoil as aromatherapy has been suggested as an agentto reduce anxiety and agitation. In one study ofnormal subjects in a randomized, controlled de-
806 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10
sign, lavender oil added to bath water reducedanger and frustration levels.153 In persons withagitation related to dementia, the literature exam-ining lavender has been equivocal; although onestudy found modestly positive results,154 two oth-ers found no improvement in behavior.155,156
APPROACH TO AGITATIONICU
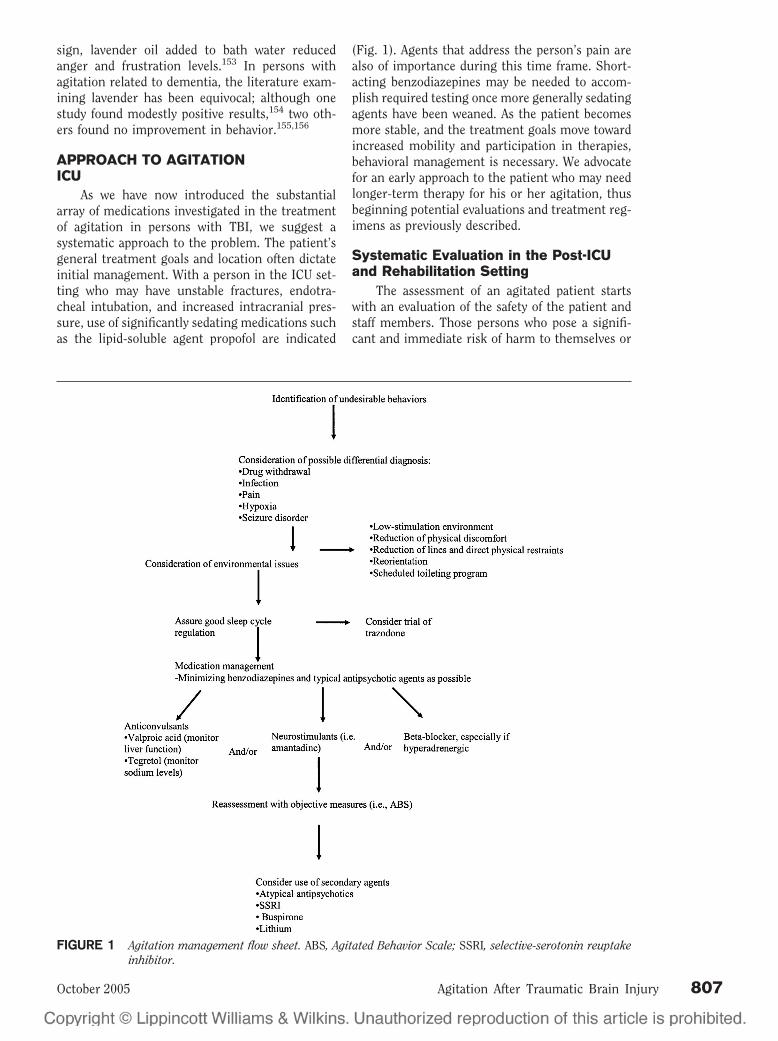
As we have now introduced the substantialarray of medications investigated in the treatmentof agitation in persons with TBI, we suggest asystematic approach to the problem. The patient’sgeneral treatment goals and location often dictateinitial management. With a person in the ICU set-ting who may have unstable fractures, endotra-cheal intubation, and increased intracranial pres-sure, use of significantly sedating medications suchas the lipid-soluble agent propofol are indicated
(Fig. 1). Agents that address the person’s pain arealso of importance during this time frame. Short-acting benzodiazepines may be needed to accom-plish required testing once more generally sedatingagents have been weaned. As the patient becomesmore stable, and the treatment goals move towardincreased mobility and participation in therapies,behavioral management is necessary. We advocatefor an early approach to the patient who may needlonger-term therapy for his or her agitation, thusbeginning potential evaluations and treatment reg-imens as previously described.
Systematic Evaluation in the Post-ICUand Rehabilitation Setting
The assessment of an agitated patient startswith an evaluation of the safety of the patient andstaff members. Those persons who pose a signifi-cant and immediate risk of harm to themselves or
FIGURE 1 Agitation management flow sheet. ABS, Agitated Behavior Scale; SSRI, selective-serotonin reuptakeinhibitor.
October 2005 Agitation After Traumatic Brain Injury 807

others and who cannot be redirected will need to bemanaged with rapidly acting pharmacologicagents, such as lorazepam. If there is no urgentsafety issue, some consideration can be given to thepossible differential diagnosis of the behavioral dis-turbance. A detailed patient history should be per-formed, with special attention to drug and alcoholuse and psychiatric conditions. Vital signs, labora-tory values, electroencephalograms, and radiologicevaluation should be performed as appropriate. Theimportance of reducing sensory stimulation in anacutely agitated patient cannot be overemphasized;excess staff members should be excused from thenearby area, television sets should be turned off,and lighting should be dimmed as possible. Evalu-ation of sleep-cycle regulation should be givencareful consideration; in our acute inpatient TBIunit, the nursing staff records the number of hoursslept for all patients. If the sleep cycle is disrupted,and environmental interventions (such as reducingcaffeine intake and minimizing naps during theday) are ineffective, trazodone should be consid-ered. Adequate pain medication should be given asappropriate.
Treatment in the Post-ICU andRehabilitation Setting
In the absence of response to behavioral andenvironmental modification, pharmacology for themanagement of agitation may be considered. Theclass of medication initially selected partially de-pends on potential secondary benefits. If the pa-tient is also experiencing hyperadrenergia, beta-blockers are likely to be a good choice. Personswith deficits in attention and concentration maybenefit from amantadine. Anticonvulsants, partic-ularly carbamazepine and valproic acid, are effec-tive for severe agitation. Other agents, such asatypical antipsychotics and SSRIs also may be con-sidered, particularly if the patient has additionalpsychiatric co-morbidities. Frequent use of “emer-gency” medications is an indication of poor generalcontrol of agitation. Lastly, it is important to useobjective measures, such as the Agitated BehaviorScale, to monitor success of treatment.
CONCLUSIONSThis review represents the thoughts of the
authors based on their experiences and review ofthe literature. Additional research is certainlyneeded to elucidate many aspects of agitation afterTBI. The pathophysiology of agitation in both ananatomic and a neurochemical basis remainslargely a mystery. Likewise, more investigationinto the safety of atypical antipsychotic agentsneeds to be pursued, starting with further animalstudies. As mentioned above, several other medica-tions, such as newer antiepileptics and antidepres-
sant therapies, show some initial promise for thetreatment of agitation. There is a general paucity ofrandomized, controlled clinical trials even for themost commonly used medications. Finally, the va-lidity and applicability of human studies depend ona common language describing agitation and com-mon objective measurement tools. The importanceof effective management of persons with agitationafter TBI has the potential to reduce morbidity andstaffing needs and to improve safety, participationin rehabilitation, and overall function.
REFERENCES1. Gouvier WD, Blanton PD, LaPorte KK, et al: Reliability and
validity of the Disability Rating Scale and the Levels ofCognitive Functioning Scale in monitoring recovery fromsevere head injury. Arch Phys Med Rehabil 1987;68:94–7
2. Corrigan JD, Mysiw WJ: Agitation following traumatichead injury: Equivocal evidence for a discrete stage ofcognitive recovery. Arch Phys Med Rehabil 1988;69:487–92
3. Galski T, Palasz J, Bruno RL, et al: Predicting physical andverbal aggression on a brain trauma unit. Arch Phys MedRehabil 1994;75:380–3
4. Brooke MM, Questad KA, Patterson DR, et al: Agitationand restlessness after closed head injury: A prospectivestudy of 100 consecutive admissions. Arch Phys Med Re-habil 1992;73:320–3
5. Kadyan V, Mysiw WJ, Bogner JA, et al: Gender differencesin agitation after traumatic brain injury. Am J Phys MedRehabil 2004;83:747–52
6. Fugate LP, Spacek LA, Kresty LA, et al: Definition ofagitation following traumatic brain injury: I. A survey ofthe Brain Injury Special Interest Group of the AmericanAcademy of Physical Medicine and Rehabilitation. ArchPhys Med Rehabil 1997;78:917–23
7. Corrigan JD: Development of a scale for assessment ofagitation following traumatic brain injury. J Clin ExpNeuropsychol 1989;11:261–77
8. Sachdev P: The development of the concept of akathisia: Ahistorical overview. Schizophr Res 1995;16:33–45
9. Miller CH, Fleischhacker WW: Managing antipsychotic-induced acute and chronic akathisia. Drug Saf 2000;22:73–81
10. Albert DJ, Chew GL: The septal forebrain and the inhibi-tory modulation of attack and defense in the rat: A review.Behav Neural Biol 1980;30:357–88
11. Siegel A, Schubert KL, Shaikh MB: Neurotransmittersregulating defensive rage behavior in the cat. NeurosciBiobehav Rev 1997;21:733–42
12. Martinius J: Homicide of an aggressive adolescent boy withright temporal lesion: A case report. Neurosci BiobehavRev 1983;7:419–22
13. van Elst LT, Woermann FG, Lemieux L, et al: Affectiveaggression in patients with temporal lobe epilepsy: A quan-titative MRI study of the amygdala. Brain 2000;123(pt2):234–43
14. Vespa PM, Nuwer MR, Nenov V, et al: Increased incidenceand impact of nonconvulsive and convulsive seizures aftertraumatic brain injury as detected by continuous electro-encephalographic monitoring. J Neurosurg 1999;91:750–60
15. van Erp AM, Miczek KA: Aggressive behavior, increasedaccumbal dopamine, and decreased cortical serotonin inrats. J Neurosci 2000;20:9320–5
16. Bouwknecht JA, Hijzen TH, van der Gugten, J, et al:Absence of 5-HT(1B) receptors is associated with impaired
808 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10
impulse control in male 5-HT(1B) knockout mice. BiolPsychiatry 2001;49:557–68
17. Nikulina EM, Kapralova NS: Role of dopamine receptors inthe regulation of aggression in mice: Relationship to ge-notype. Neurosci Behav Physiol 1992;22:364–9
18. Linnoila M, Virkkunen M, Scheinin M, et al: Low cerebro-spinal fluid 5-hydroxyindoleacetic acid concentration dif-ferentiates impulsive from nonimpulsive violent behavior.Life Sci 1983;33:2609–14
19. Chiavegatto S, Nelson RJ: Interaction of nitric oxide andserotonin in aggressive behavior. Horm Behav 2003;44:233–41
20. Spielewoy C, Roubert C, Hamon M, et al: Behaviouraldisturbances associated with hyperdopaminergia in do-pamine-transporter knockout mice. Behav Pharmacol2000;11:279–90
21. Farde L: Selective D1- and D2-dopamine receptor blockadeboth induces akathisia in humans: A PET study with[11C]SCH 23390 and [11C]raclopride. Psychopharmacol-ogy (Berl) 1992;107:23–9
22. Bogner JA, Corrigan JD, Stange M, et al: Reliability of theAgitated Behavior Scale. J Head Trauma Rehabil 1999;14:91–6
23. Yudofsky SC, Silver JM, Jackson W, et al: The Overt Ag-gression Scale for the objective rating of verbal and phys-ical aggression. Am J Psychiatry 1986;143:35–9
24. Alderman N, Knight C, Morgan C: Use of a modifiedversion of the Overt Aggression Scale in the measurementand assessment of aggressive behaviours following braininjury. Brain Inj 1997;11:503–23
25. Alderman N, Davies JA, Jones C, et al: Reduction of severeaggressive behaviour in acquired brain injury: Case studiesillustrating clinical use of the OAS-MNR in the manage-ment of challenging behaviours. Brain Inj 1999;13:669–704
26. Fugate LP, Spacek LA, Kresty LA, et al: Measurement andtreatment of agitation following traumatic brain injury: II.A survey of the Brain Injury Special Interest Group of theAmerican Academy of Physical Medicine and Rehabilita-tion. Arch Phys Med Rehabil 1997;78:924–8
27. Angelino E, Miglioretti M, Zotti AM: Agitation assessmentin severe traumatic brain injury: Methodological and clin-ical issues. Brain Inj 2002;16:269–75
28. Alderman N, Knight C, Henman C: Aggressive behaviourobserved within a neurobehavioural rehabilitation service:Utility of the OAS-MNR in clinical audit and applied re-search. Brain Inj 2002;16:469–89
29. Bayard M, McIntyre J, Hill KR, et al: Alcohol withdrawalsyndrome. Am Fam Physician Mar 15, 2004;69(6):1443–50
30. Olmedo R, Hoffman RS: Withdrawal syndromes. EmergMed Clin North Am 2000;18:273–88
31. Dimopoulou I, Tsagarakis S, Theodorakopoulou M, et al:Endocrine abnormalities in critical care patients withmoderate-to-severe head trauma: Incidence, pattern andpredisposing factors. Intensive Care Med 2004;30:1051–7
32. Burger AG, Philippe J: Thyroid emergencies. BaillieresClin Endocrinol Metab 1992;6:77–93
33. Demet MM, Ozmen B, Deveci A, et al: Depression andanxiety in hyperthyroidism. Arch Med Res 2002;33:552–6
34. Tenedieva VD, Potapov AA, Gaitur EI, et al: Thyroid hor-mones in comatose patients with traumatic brain injury.Acta Neurochir Suppl 2000;76:385–91
35. Agha A, Rogers B, Mylotte D, et al: Neuroendocrine dys-function in the acute phase of traumatic brain injury. ClinEndocrinol (Oxf) 2004;60:584–91
36. Webster JB, Bell KR: Primary adrenal insufficiency follow-ing traumatic brain injury: A case report and review of theliterature. Arch Phys Med Rehabil 1997;78:314–8
37. Aldemir M, Ozen S, Kara IH, et al: Predisposing factors for
delirium in the surgical intensive care unit. Crit Care2001;5:265–70
38. Atchison JW, Wachendorf J, Haddock D, et al: Hyponatre-mia-associated cognitive impairment in traumatic braininjury. Brain Inj 1993;7:347–52
39. Kahn DM, Cook TE, Carlisle CC, et al: Identification andmodification of environmental noise in an ICU setting.Chest 1998;114:535–40
40. Granberg Axell AI, Malmros CW, Bergbom IL, et al: Inten-sive care unit syndrome/delirium is associated with ane-mia, drug therapy and duration of ventilation treatment.Acta Anaesthesiol Scand 2002;46:726–31
41. Food and Drug Administration announcement. March 25,2005
42. Zafonte RD, Hammond FD, Rahimi R: Air embolism in theagitated traumatic brain injury patient: An unusual com-plication. Brain Inj 1996;10:759–61
43. Engst C, Chhokar R, Robinson D, et al: Implementation ofa scheduled toileting program in a long term care facility:Evaluating the impact on injury risk to caregiving staff.AAOHN J 2004;52:427–35
44. Clinchot DM, Bogner J, Mysiw WJ, et al: Defining sleepdisturbance after brain injury. Am J Phys Med Rehabil1998;77:291–5
45. Castriotta RJ, Lai JM: Sleep disorders associated with trau-matic brain injury. Arch Phys Med Rehabil 2001;82:1403–6
46. Webster JB, Bell KR, Hussey JD, et al: Sleep apnea inadults with traumatic brain injury: A preliminary investi-gation. Arch Phys Med Rehabil 2001;82:316–21
47. Buffum MD, Miaskowski C, Sands L, et al: A pilot study ofthe relationship between discomfort and agitation in pa-tients with dementia. Geriatr Nurs 2001;22:80–5
48. Zieber CG, Hagen B, Armstrong-Esther C, et al: Pain andagitation in long-term care residents with dementia: Use ofthe Pittsburgh Agitation Scale. Int J Palliat Nurs 2005;11:71–8
49. Irving MH, Irving PM: Associated injuries in head injuredpatients. J Trauma 1967;7:500–11
50. Prigatano GP, Borgaro S, Caples H: Non-pharmacologicalmanagement of psychiatric disturbances after traumaticbrain injury. Int Rev Psychiatry 2003;15:371–9
51. Bowden CL: Valproate. Bipolar Disord 2003;5:189–202
52. Narayan M, Nelson JC: Treatment of dementia with behav-ioral disturbance using divalproex or a combination ofdivalproex and a neuroleptic. J Clin Psychiatry 1997;58:351–4
53. Porsteinsson AP, Tariot PN, Erb R, et al: Placebo-con-trolled study of divalproex sodium for agitation in demen-tia. Am J Geriatr Psychiatry 2001;9:58–66
54. Porsteinsson AP, Tariot PN, Jakimovich LJ, et al: Valproatetherapy for agitation in dementia: Open-label extension ofa double-blind trial. Am J Geriatr Psychiatry 2003;11:434–40
55. Lonergan ET, Cameron M, Luxenberg J: Valproic acid foragitation in dementia. Cochrane Database Syst Rev 2004;2:CD003945
56. Monji A, Yoshida I, Koga H, et al: Brain injury-inducedrapid-cycling affective disorder successfully treated withvalproate. Psychosomatics. 1999;40:448–9
57. Wroblewski BA, Joseph AB, Kupfer J, et al: Effectiveness ofvalproic acid on destructive and aggressive behaviours inpatients with acquired brain injury. Brain Inj 1997;11:37–47
58. Chatham-Showalter PE, Kimmel DN: Agitated symptomresponse to divalproex following acute brain injury. J Neu-ropsychiatry Clin Neurosci 2000;12:395–7
59. Massagli TL: Neurobehavioral effects of phenytoin, car-bamazepine, and valproic acid: Implications for use in
October 2005 Agitation After Traumatic Brain Injury 809
traumatic brain injury. Arch Phys Med Rehabil 1991;72:219–26
60. Dikmen SS, Machamer JE, Winn HR, et al: Neuropsycho-logical effects of valproate in traumatic brain injury: Arandomized trial. Neurology 2000;54:895–902
61. Anderson GD, Awan AB, Adams CA, et al: Increases inmetabolism of valproate and excretion of 6beta-hydroxy-cortisol in patients with traumatic brain injury. Br J ClinPharmacol 1998;45:101–5
62. Smith KR Jr, Goulding PM, Wilderman D, et al: Neurobe-havioral effects of phenytoin and carbamazepine in pa-tients recovering from brain trauma: A comparative study.Arch Neurol 1994;51:653–60
63. Chatham-Showalter PE: Carbamazepine for combative-ness in acute traumatic brain injury. J NeuropsychiatryClin Neurosci 1996;8:96–9
64. Azouvi P, Jokic C, Attal N, et al: Carbamazepine in agita-tion and aggressive behaviour following severe closed-head injury: Results of an open trial. Brain Inj 1999;13:797–804
65. Herrmann N, Lanctot K, Myszak M: Effectiveness of gaba-pentin for the treatment of behavioral disorders in demen-tia. J Clin Psychopharmacol 2000;20:90–3
66. Roane DM, Feinberg TE, Meckler L, et al: Treatment ofdementia-associated agitation with gabapentin. J Neuro-psychiatry Clin Neurosci 2000;12:40–3
67. Childers MK, Holland D: Psychomotor agitation followinggabapentin use in brain injury. Brain Inj 1997;11:537–40
68. Pachet A, Friesen S, Winkelaar D, et al: Beneficial behav-ioural effects of lamotrigine in traumatic brain injury.Brain Inj 2003;17:715–22
69. Lipsey JR, Robinson RG, Pearlson GD, et al: Nortriptylinetreatment of post-stroke depression: A double-blind study.Lancet 1984;1:297–300
70. Wroblewski BA, Joseph AB, Cornblatt RR: Antidepressantpharmacotherapy and the treatment of depression in pa-tients with severe traumatic brain injury: A controlled,prospective study. J Clin Psychiatry 1996;57:582–7
71. Wroblewski B, Glenn MB, Cornblatt R, et al: Protriptylineas an alternative stimulant medication in patients withbrain injury: A series of case reports. Brain Inj 1993;7:353–62
72. Reinhard DL, Whyte J, Sandel ME: Improved arousal andinitiation following tricyclic antidepressant use in severebrain injury. Arch Phys Med Rehabil 1996;77:80–3
73. Jackson RD, Corrigan JD, Arnett JA: Amitriptyline foragitation in head injury. Arch Phys Med Rehabil 1985;66:180–1
74. Mysiw WJ, Jackson RD, Corrigan JD: Amitriptyline forpost-traumatic agitation. Am J Phys Med Rehabil 1988;67:29–33
75. Wroblewski BA, McColgan K, Smith K, et al: The incidenceof seizures during tricyclic antidepressant drug treatmentin a brain-injured population. J Clin Psychopharmacol1990;10:124–8
76. Perino C, Rago R, Cicolini A, et al: Mood and behaviouraldisorders following traumatic brain injury: Clinical evalu-ation and pharmacological management. Brain Inj 2001;15:139–48
77. Fann JR, Uomoto JM, Katon WJ: Sertraline in the treat-ment of major depression following mild traumatic braininjury. J Neuropsychiatry Clin Neurosci 2000;12:226–32
78. Muller U, Murai T, Bauer-Wittmund T, et al: Paroxetineversus citalopram treatment of pathological crying afterbrain injury. Brain Inj 1999;13:805–11
79. Meythaler JM, Depalma L, Devivo MJ, et al: Sertraline toimprove arousal and alertness in severe traumatic braininjury secondary to motor vehicle crashes. Brain Inj 2001;15:321–31
80. Ranen NG, Lipsey JR, Treisman G, et al: Sertraline in the
treatment of severe aggressiveness in Huntington’s dis-ease. J Neuropsychiatry Clin Neurosci 1996;8:338–40
81. Kant R, Smith-Seemiller L, Zeiler D: Treatment of aggres-sion and irritability after head injury. Brain Inj 1998;12:661–6
82. Kanner AM, Kozak AM, Frey M: The use of sertraline inpatients with epilepsy: Is it safe? Epilepsy Behav 2000;1:100–5
83. Lebert F, Stekke W, Hasenbroekx C, et al: Frontotemporaldementia: A randomised, controlled trial with trazodone.Dement Geriatr Cogn Disord 2004;17:355–9
84. Sultzer DL, Gray KF, Gunay I, et al: A double-blind com-parison of trazodone and haloperidol for treatment ofagitation in patients with dementia. Am J Geriatr Psychi-atry 1997;5:60–9
85. Schneider LS, Gleason RP, Chui HC: Progressive supranu-clear palsy with agitation: Response to trazodone but notto thiothixine or carbamazepine. J Geriatr PsychiatryNeurol 1989;2:109–12
86. Martinon-Torres G, Fioravanti M, Grimley EJ: Trazodonefor agitation in dementia. Cochrane Database Syst Rev2004;4:CD004990
87. Saenz de Tejada I, Ware JC, Blanco R, et al: Pathophysi-ology of prolonged penile erection associated with traz-odone use. J Urol 1991;145:60–4
88. Levine AM: Buspirone and agitation in head injury. BrainInj 1988;2:165–7
89. Gualtieri CT: Buspirone for the behavior problems of pa-tients with organic brain disorders. J Clin Psychopharma-col 1991;11:280–1
90. Ratey JJ, Leveroni CL, Miller AC, et al: Low-dose buspironeto treat agitation and maladaptive behavior in brain-in-jured patients: Two case reports. J Clin Psychopharmacol1992;12:362–4
91. Stanislav SW, Childs A: Evaluating the usage of droperidolin acutely agitated persons with brain injury. Brain Inj2000;14:261–5
92. Maryniak O, Manchanda R, Velani A: Methotrimeprazinein the treatment of agitation in acquired brain injurypatients. Brain Inj 2001;15:167–74
93. Feeney DM, Gonzalez A, Law WA: Amphetamine, haloper-idol, and experience interact to affect rate of recovery aftermotor cortex injury. Science 1982;217:855–7
94. Rao N, Jellinek HM, Woolston DC: Agitation in closed headinjury: Haloperidol effects on rehabilitation outcome. ArchPhys Med Rehabil 1985;66:30–4
95. Stanislav SW: Cognitive effects of antipsychotic agents inpersons with traumatic brain injury. Brain Inj 1997;11:335–41
96. Kadyan V, Colachis SC, Depalma MJ, et al: Early recogni-tion of neuroleptic malignant syndrome during traumaticbrain injury rehabilitation. Brain Inj 2003;17:631–7
97. Vincent FM, Zimmerman JE, Van Haren, J: Neurolepticmalignant syndrome complicating closed head injury.Neurosurgery 1986;18:190–3
98. Wilkinson R, Meythaler JM, Guin-Renfroe S: Neurolepticmalignant syndrome induced by haloperidol followingtraumatic brain injury. Brain Inj 1999;13:1025–31
99. Persing JS: Neuroleptic malignant syndrome: An overview.S D J Med 1994;47:51–5
100. Wilson MS, Gibson CJ, Hamm RJ: Haloperidol, but notolanzapine, impairs cognitive performance after traumaticbrain injury in rats. Am J Phys Med Rehabil 2003;82:871–9
101. Michals ML, Crismon ML, Roberts S, et al: Clozapineresponse and adverse effects in nine brain-injured pa-tients. J Clin Psychopharmacol 1993;13:198–203
102. Silver BV, Collins L, Zidek KA: Risperidone treatment ofmotor restlessness following anoxic brain injury. Brain Inj2003;17:237–44
810 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10
103. Wyant M, Diamond BI, O’Neal, E, et al: The use of mida-zolam in acutely agitated psychiatric patients. Psycho-pharmacol Bull 1990;26:126–9
104. Hirose S, Ashby CR: Immediate effect of intravenous diaz-epam in neuroleptic-induced acute akathisia: An open-label study. J Clin Psychiatry 2002;63:524–7
105. Bartels M, Heide K, Mann K, et al: Treatment of akathisiawith lorazepam: An open clinical trial. Pharmacopsychia-try 1987;20:51–3
106. Schallert T, Hernandez TD, Barth TM: Recovery of func-tion after brain damage: Severe and chronic disruption bydiazepam. Brain Res 1986;379:104–11
107. Lazar RM, Fitzsimmons BF, Marshall RS, et al: Reemer-gence of stroke deficits with midazolam challenge. Stroke2002;33:283–5
108. Goldstein LB: Common drugs may influence motor recov-ery after stroke: The Sygen In Acute Stroke Study Inves-tigators. Neurology 1995;45:865–71
109. Goldstein LB: Prescribing of potentially harmful drugs topatients admitted to hospital after head injury. J NeurolNeurosurg Psychiatry 1995;58:753–5
110. Goldstein LB: Basic and clinical studies of pharmacologiceffects on recovery from brain injury. J Neural TransplantPlast 1993;4:175–92
111. Rodrigo CR: Flumazenil reverses paradoxical reaction withmidazolam. Anesth Prog 1991;38:65–8
112. Weinbroum AA, Szold O, Ogorek D, et al: The midazolam-induced paradox phenomenon is reversible by flumazenil:Epidemiology, patient characteristics and review of theliterature. Eur J Anaesthesiol 2001;18:789–97
113. Ried LD, Johnson RE, Gettman DA: Benzodiazepine expo-sure and functional status in older people. J Am GeriatrSoc 1998;46:71–6
114. Caradoc-Davies TH: Traumatic mutism in severe headinjury relieved by oral diazepam. Disabil Rehabil 1996;18:482–4
115. Gottlieb LD: The role of beta blockers in alcohol with-drawal syndrome. Postgrad Med 1988;Spec No:169–74
116. Adler LA, Angrist B, Weinreb H, et al: Studies on the timecourse and efficacy of beta-blockers in neuroleptic-in-duced akathisia and the akathisia of idiopathic Parkinson’sdisease. Psychopharmacol Bull 1991;27:107–11
117. Dumon JP, Catteau J, Lanvin F, et al: Randomized, double-blind, crossover, placebo-controlled comparison of pro-pranolol and betaxolol in the treatment of neuroleptic-induced akathisia. Am J Psychiatry 1992;149:647–50
118. Zubenko GS, Lipinski JF, Cohen BM, et al: Comparison ofmetoprolol and propranolol in the treatment of akathisia.Psychiatry Res 1984;11:143–9
119. Shankle WR, Nielson KA, Cotman CW: Low-dose propran-olol reduces aggression and agitation resembling that as-sociated with orbitofrontal dysfunction in elderly de-mented patients. Alzheimer Dis Assoc Disord 1995;9:233–7
120. Greendyke RM, Berkner JP, Webster JC, et al: Treatment ofbehavioral problems with pindolol. Psychosomatics 1989;30:161–5
121. Fleminger S, Greenwood RJ, Oliver DL: Pharmacologicalmanagement for agitation and aggression in people withacquired brain injury. Cochrane Database Syst Rev 2003;1:CD003299
122. Geddes JR, Burgess S, Hawton K, et al: Long-term lithiumtherapy for bipolar disorder: Systematic review and meta-analysis of randomized controlled trials. Am J Psychiatry2004;161:217–22
123. Fazli-Tabaei S, Yahyavi SH, Zarrindast MR: Effects of lith-ium carbonate on apomorphine-induced sniffing behav-iour in rats. Pharmacol Toxicol 2002;91:135–9
124. Cohn CK, Wright JR, DeVaul RA: Post head trauma syn-
drome in an adolescent treated with lithium carbonate:Case report. Dis Nerv Syst 1977;38:630–1
125. Bellus SB, Stewart D, Vergo JG, et al: The use of lithium inthe treatment of aggressive behaviours with two brain-injured individuals in a state psychiatric hospital. BrainInj 1996;10:849–60
126. Glenn MB, Wroblewski B, Parziale J, et al: Lithium car-bonate for aggressive behavior or affective instability inten brain-injured patients. Am J Phys Med Rehabil 1989;68:221–6
127. Silver J, Youdofsky S, Anderson K : Textbook of TraumaticBrain Injury. Washington, DC, American Psychiatric Pub-lishing, 2005
128. Moskowitz A, Altshuler L: Increased sensitivity to lithium-induced neurotoxicity after stroke: A case report. J ClinPsychopharmacol 1991;11;272–3
129. Zafonte RD, Watanabe T, Mann NR: Amantadine: A poten-tial treatment for the minimally conscious state. Brain Inj1998;12:617–21
130. Passler MA, Riggs RV: Positive outcomes in traumaticbrain injury-vegetative state: Patients treated with bro-mocriptine. Arch Phys Med Rehabil 2001;82:311–5
131. Meythaler JM, Brunner RC, Johnson A, et al: Amantadineto improve neurorecovery in traumatic brain injury-asso-ciated diffuse axonal injury: A pilot double-blind random-ized trial. J Head Trauma Rehabil 2002;17:300–13
132. Powell JH, al-Adawi, S, Morgan J, et al: Motivational def-icits after brain injury: Effects of bromocriptine in 11patients. J Neurol Neurosurg Psychiatry 1996;60:416–21
133. Stewart JT: Akathisia following traumatic brain injury:Treatment with bromocriptine. J Neurol Neurosurg Psy-chiatry 1989;52:1200–1
134. Silver BV, Yablon SA: Akathisia resulting from traumaticbrain injury. Brain Inj 1996;10:609–14
135. Muller HF, Dastoor DP, Klingner A, et al: Amantadine insenile dementia: Electroencephalographic and clinical ef-fects. J Am Geriatr Soc 1979;27:9–16
136. Edby K, Larsson J, Eek M, et al: Amantadine treatment ofa patient with anoxic brain injury. Childs Nerv Syst 1995;11:607–9
137. Rosati DL: Early polyneuropharmacologic intervention inbrain injury agitation. Am J Phys Med Rehabil 2002;81:90–3
138. Arciniegas DB, Frey KL, Anderson CA, et al: Amantadinefor neurobehavioural deficits following delayed post-hy-poxic encephalopathy. Brain Inj 2004;18:1309–18
139. Wu TS, Garmel GM: Improved neurological function afterAmantadine treatment in two patients with brain injury. JEmerg Med 2005;28:289–92
140. Chandler MC, Barnhill JL, Gualtieri CT: Amantadine forthe agitated head-injury patient. Brain Inj 1988;2:309–11
141. Nickels JL, Schneider WN, Dombovy ML, et al: Clinical useof amantadine in brain injury rehabilitation. Brain Inj1994;8:709–18
142. Whyte J, Hart T, Schuster K, et al: Effects of methylpheni-date on attentional function after traumatic brain injury: Arandomized, placebo-controlled trial. Am J Phys Med Re-habil 1997;76:440–50
143. Whyte J, Hart T, Vaccaro M, et al: Effects of methylpheni-date on attention deficits after traumatic brain injury: Amultidimensional, randomized, controlled trial. Am JPhys Med Rehabil 2004;83:401–20
144. Mooney GF, Haas LJ: Effect of methylphenidate on braininjury-related anger. Arch Phys Med Rehabil 1993;74:153–60
145. Kant R, Bogyi AM, Carosella NW, et al: ECT as a thera-peutic option in severe brain injury. Convuls Ther 1995;11:45–50
146. Heiden A, Frey R, Presslich O, et al: Treatment of severe
October 2005 Agitation After Traumatic Brain Injury 811

mania with intravenous magnesium sulphate as a supple-mentary therapy. Psychiatry Res 1999;89:239–46
147. Chouinard G, Beauclair L, Geiser R, et al: A pilot study ofmagnesium aspartate hydrochloride (Magnesiocard) as amood stabilizer for rapid cycling bipolar affective disorderpatients. Prog Neuropsychopharmacol Biol Psychiatry1990;14:171–80
148. Giannini AJ, Nakoneczie AM, Melemis SM, et al: Magne-sium oxide augmentation of verapamil maintenance ther-apy in mania. Psychiatry Res 2000;93:83–7
149. Hoane MR, Barth TM: The behavioral and anatomicaleffects of MgCl2 therapy in an electrolytic lesion model ofcortical injury in the rat. Magnes Res. 2001;14:51–63
150. Heath DL, Vink R: Magnesium sulphate improves neuro-logic outcome following severe closed head injury in rats.Neurosci Lett 1997;228:175–8
151. Vink R, O’Connor, CA, Nimmo AJ, et al: Magnesium at-tenuates persistent functional deficits following diffusetraumatic brain injury in rats. Neurosci Lett 2003;336:41–4
152. Ustun ME, Duman A, Ogun CO, et al: Effects of nimodipineand magnesium sulfate on endogenous antioxidant levelsin brain tissue after experimental head trauma. J Neuro-surg Anesthesiol 2001;13:227–32
153. Morris N: The effects of lavender (Lavendula angustifo-lium) baths on psychological well-being: Two exploratoryrandomised control trials. Complement Ther Med 2002;10:223–8
154. Holmes C, Hopkins V, Hensford C, et al: Lavender oil as atreatment for agitated behaviour in severe dementia: Aplacebo controlled study. Int J Geriatr Psychiatry 2002;17:305–8
155. Gray SG, Clair AA: Influence of aromatherapy on medica-tion administration to residential-care residents with de-mentia and behavioral challenges. Am J Alzheimers DisOther Demen 2002;17:169–74
156. Snow LA, Hovanec L, Brandt J: A controlled trial of aro-matherapy for agitation in nursing home patients withdementia. J Altern Complement Med 2004;10:431–7
812 Lombard and Zafonte Am. J. Phys. Med. Rehabil. ● Vol. 84, No. 10