per-patient-per-month drug costs in medicare part d protected classes
TRANSCRIPT
Per-patient-per-month Drug Costs inMedicare Part D Protected ClassesLisa Mucha,1 Neal A. Masia2 and Kirsten J. Axelsen2
1 Thomson Medstat, Cambridge, Massachusetts, USA2 Pfizer Inc., New York, New York, USA
Abstract Objective: The objective of this study was to estimate the per-patient-per-month(PPPM) costs of medications in the six Medicare Part D protected classes based onfindings among Medicare and dual eligible beneficiaries with drug coverage beforethe enactment of the benefit.
Design: Data were from the Thomson Medstat MarketScan1 Medicare andMedicaid claims databases. The study sample was constructed by identifyingpatients who were enrolled either in Medicare or dually in Medicare and Medicaid.PPPM costs were calculated for each protected class. Drugs covered under Part Bwere excluded.
Outcomes measure: PPPM aggregated costs within each class.
Results: The classes in which generic formulations are available (antidepressants andanticonvulsants) show low PPPM costs ($US45.31 and $US50.97, respectively). Themost expensive class is the antiretrovirals ($US829.73). This class is the costliest forall dual eligible patients including those aged 64 years and under. Among the dualeligibles aged 65 years and older, the immunosuppressants are the most expensiveclass. The same result is seen qualitatively in the Medicare group.
Conclusions: PPPM costs are not uniformly high among the protected classes. Theclaims data in this study allowed a ‘real world’ check of how much the protectedclasses may impact the finances of Part D. There are differences within the classesbetween the dual eligible and Medicare patients, and also within the dual eligibles byage. This is an important message to policy makers that a change to the structure of theprotected classes in Part D may have differential effects across classes and also withinclasses.
Introduction
The Medicare Modernization Act of 2003(Public Law 108–173) created a voluntary out-patient prescription drug benefit for Medicarebeneficiaries.[1] This landmark legislation bringsabout a long desired benefit to Medicare recipients.
‘‘With the Medicare Act of 2003, our govern-ment is finally bringing prescription drug coverageto the seniors of America.’’[2]
Referred to as Part D, this benefit covers elderlyand disabled individuals enrolled in Medicare ordually in Medicare and Medicaid. Patients arerequired to enrol themselves into this coverage,
ORIGINAL RESEARCH Pharmacoeconomics 2006; 24 Suppl. 3: 79–841170-7690/06/0003-0079/$39.95/0
� 2006 Adis Data Information BV. All rights reserved.

and as of June 2006, 38.2 millionMedicare patientshad an outpatient prescription drug benefit throughPart D.[3]
Part D plans were directed to create a formularythat includes at least two drugs from each coveredtherapeutic class of drugs. Regulatory guidancefrom the Centers for Medicare and MedicaidServices for the 2006 plan year specified six‘protected’ classes of drugs for Medicare Part Dplans. This guidance requires plan formularies toinclude ‘all or substantially all’ US FDA-approvedmedications in these classes. The six protectedclasses are: antidepressants, antipsychotics, antic-onvulsants, antiretrovirals, immunosuppressantsand antineoplastics. Maintaining the security ofthese six classes is an important issue as theMedicare Prescription Drug Simplification Act of2006, section 112, requires healthcare plans toextend the protection until 2008.[4] The rationalebehind the selection of these six classes was basedon a review of formularies of comparable drugprogrammes such as Medicaid and the FederalEmployees Health Benefit Program. The results ofthis review showed that patients taking drugs inthese classes required uninterrupted utilisation forclinical reasons. As a result of the high cost ofhealthcare, including drugs, for some of thediseases within these classes, there was alsoconcern about a resulting lack of formularycoverage among Part D plans. Therefore all or‘substantially all’ drugs in these six classes mustbe provided to plan enrollees. The phrase‘substantially all’ allows for some exceptions,such as permission to put a prior authorisationon specific branded agents, and that not allmultisource brands or extended release forms ofdrugs have to be included.[5]
From a public policy standpoint, it is of interestto understand the economic burden associatedwith the six protected classes. The objectiveof this study was to estimate the per-patient-per-month (PPPM) costs of medications in thesesix protected classes based on findings amongMedicare beneficiaries that had prescription drugcoverage before enactment of the Part Dprogramme.
Data and Methods
Data were from the Thomson Medstat Market-Scan1 2004 Medicare and Medicaid claimsdatabases. The Medicare database consists ofclaims from retired employees who have bothMedicare coverage and supplemental coveragefrom the employer they retired from. Thesupplemental coverage provided by the employerprovides benefits to the retiree, such as outpatientprescription drug coverage, which Medicaredoes not. The database does not identify thespecific carrier of the prescription drug cover-age that employers provided to their Medicareretirees. The Medicaid database reflects thehealthcare service use of individuals coveredby Medicaid programmes in eight geographicallydispersed states. Only those enrollees with aprescription drug benefit were considered for theanalysis. Both databases include the representa-tion of care delivered by fee-for-service andmanaged care plans. Both the Medicare-coveredportion of payment (represented as coordinationof benefits amount), the employer, and theMedicaid-paid portion are included in thesedatabases.
The study sample was constructed by identify-ing patients who were enrolled either in Medicareor dually in Medicare and Medicaid. During 2004,the Medicare database incorporated healthservices data for approximately 1.4 millionbeneficiary years. The Medicaid databasecontained a similar number of years linked toindividuals who were flagged as dually eligible.Patients taking one or more drugs within any of thesix protected classes were identified via therelevant National Drug Codes on their pharmacyclaims for that year. Drugs that may be coveredunder Medicare Part B were not included in thisanalysis. Patients who had multiple claims withinthe same class were counted once. Patients whohad claims in more than one class were countedonce in each class.
PPPM costs were calculated for each protectedclass. Costs were aggregated within each class,including patient-paid and plan-paid amounts.
80 Mucha et al.
� 2006 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2006; 24 Suppl. 3
These costs provided the numerators for the PPPMcalculations. Denominators were defined as theaggregated patient months for only those individ-uals who filled a drug within a particular class. Thisresulted in six different denominators, one for eachprotected class.
Results
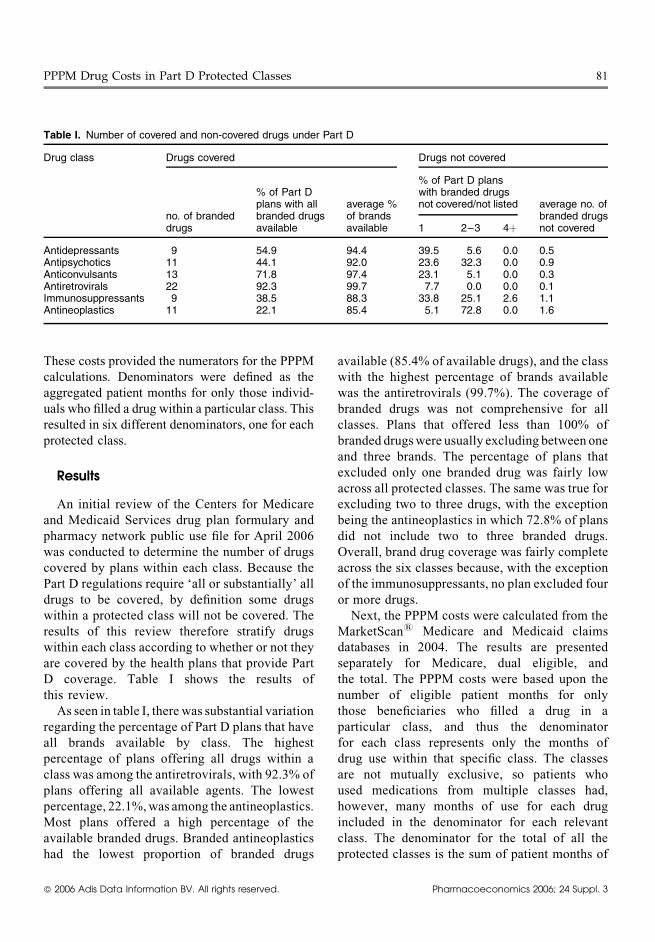
An initial review of the Centers for Medicareand Medicaid Services drug plan formulary andpharmacy network public use file for April 2006was conducted to determine the number of drugscovered by plans within each class. Because thePart D regulations require ‘all or substantially’ alldrugs to be covered, by definition some drugswithin a protected class will not be covered. Theresults of this review therefore stratify drugswithin each class according to whether or not theyare covered by the health plans that provide PartD coverage. Table I shows the results ofthis review.
As seen in table I, there was substantial variationregarding the percentage of Part D plans that haveall brands available by class. The highestpercentage of plans offering all drugs within aclass was among the antiretrovirals, with 92.3% ofplans offering all available agents. The lowestpercentage, 22.1%,was among the antineoplastics.Most plans offered a high percentage of theavailable branded drugs. Branded antineoplasticshad the lowest proportion of branded drugs
available (85.4% of available drugs), and the classwith the highest percentage of brands availablewas the antiretrovirals (99.7%). The coverage ofbranded drugs was not comprehensive for allclasses. Plans that offered less than 100% ofbranded drugswere usually excluding between oneand three brands. The percentage of plans thatexcluded only one branded drug was fairly lowacross all protected classes. The same was true forexcluding two to three drugs, with the exceptionbeing the antineoplastics in which 72.8% of plansdid not include two to three branded drugs.Overall, brand drug coverage was fairly completeacross the six classes because, with the exceptionof the immunosuppressants, no plan excluded fouror more drugs.
Next, the PPPM costs were calculated from theMarketScan1 Medicare and Medicaid claimsdatabases in 2004. The results are presentedseparately for Medicare, dual eligible, andthe total. The PPPM costs were based upon thenumber of eligible patient months for onlythose beneficiaries who filled a drug in aparticular class, and thus the denominatorfor each class represents only the months ofdrug use within that specific class. The classesare not mutually exclusive, so patients whoused medications from multiple classes had,however, many months of use for each drugincluded in the denominator for each relevantclass. The denominator for the total of all theprotected classes is the sum of patient months of
PPPM Drug Costs in Part D Protected Classes 81
Table I. Number of covered and non-covered drugs under Part D
Drug class Drugs covered Drugs not covered
no. of brandeddrugs
% of Part Dplans with allbranded drugsavailable
average %of brandsavailable
% of Part D planswith branded drugsnot covered/not listed average no. of
branded drugsnot covered1 2–3 4þ
Antidepressants 9 54.9 94.4 39.5 5.6 0.0 0.5Antipsychotics 11 44.1 92.0 23.6 32.3 0.0 0.9Anticonvulsants 13 71.8 97.4 23.1 5.1 0.0 0.3Antiretrovirals 22 92.3 99.7 7.7 0.0 0.0 0.1Immunosuppressants 9 38.5 88.3 33.8 25.1 2.6 1.1Antineoplastics 11 22.1 85.4 5.1 72.8 0.0 1.6
� 2006 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2006; 24 Suppl. 3
drug use in each class. The denominators are asfollows:� Antidepressants: 8 107 740� Antipsychotics: 3 335 406� Anticonvulsants: 6 482 993� Antiretrovirals: 201 430� Immunosuppressants: 82 188� Antineoplastics: 2 923 864� Total of all six classes: 21 133 621
The total PPPM for each class is representedfollowed by stratification between dual eligiblepatients and Medicare-only beneficiaries.
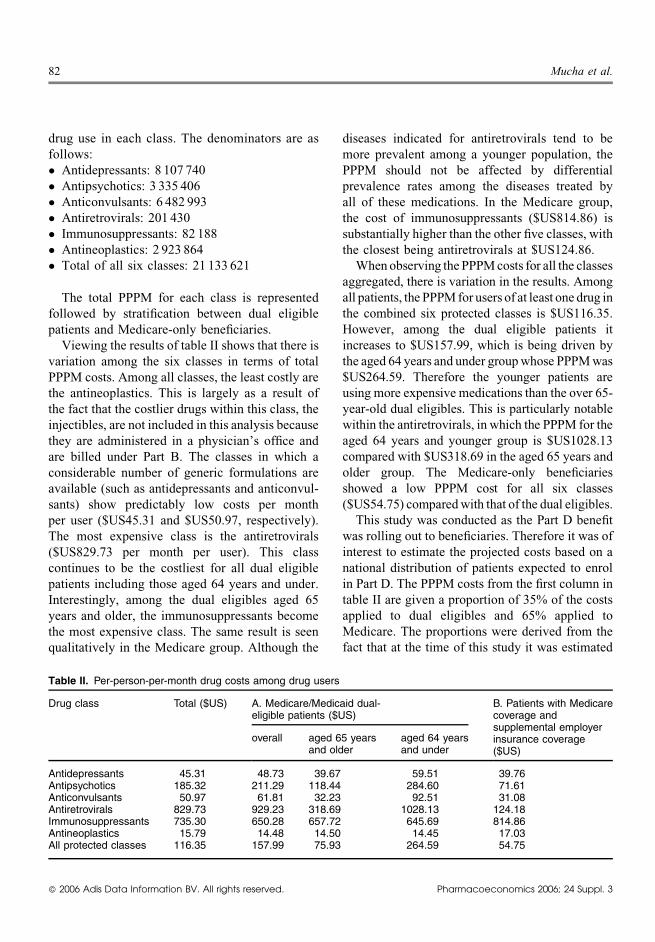
Viewing the results of table II shows that there isvariation among the six classes in terms of totalPPPM costs. Among all classes, the least costly arethe antineoplastics. This is largely as a result ofthe fact that the costlier drugs within this class, theinjectibles, are not included in this analysis becausethey are administered in a physician’s office andare billed under Part B. The classes in which aconsiderable number of generic formulations areavailable (such as antidepressants and anticonvul-sants) show predictably low costs per monthper user ($US45.31 and $US50.97, respectively).The most expensive class is the antiretrovirals($US829.73 per month per user). This classcontinues to be the costliest for all dual eligiblepatients including those aged 64 years and under.Interestingly, among the dual eligibles aged 65years and older, the immunosuppressants becomethe most expensive class. The same result is seenqualitatively in the Medicare group. Although the
diseases indicated for antiretrovirals tend to bemore prevalent among a younger population, thePPPM should not be affected by differentialprevalence rates among the diseases treated byall of these medications. In the Medicare group,the cost of immunosuppressants ($US814.86) issubstantially higher than the other five classes, withthe closest being antiretrovirals at $US124.86.
When observing thePPPMcosts for all the classesaggregated, there is variation in the results. Amongall patients, the PPPMfor users of at least one drug inthe combined six protected classes is $US116.35.However, among the dual eligible patients itincreases to $US157.99, which is being driven bythe aged 64 years and under groupwhose PPPMwas$US264.59. Therefore the younger patients areusing more expensive medications than the over 65-year-old dual eligibles. This is particularly notablewithin the antiretrovirals, in which the PPPM for theaged 64 years and younger group is $US1028.13compared with $US318.69 in the aged 65 years andolder group. The Medicare-only beneficiariesshowed a low PPPM cost for all six classes($US54.75) comparedwith that of the dual eligibles.
This study was conducted as the Part D benefitwas rolling out to beneficiaries. Therefore it was ofinterest to estimate the projected costs based on anational distribution of patients expected to enrolin Part D. The PPPM costs from the first column intable II are given a proportion of 35% of the costsapplied to dual eligibles and 65% applied toMedicare. The proportions were derived from thefact that at the time of this study it was estimated
82 Mucha et al.
Table II. Per-person-per-month drug costs among drug users
Drug class Total ($US) A. Medicare/Medicaid dual-eligible patients ($US)
B. Patients with Medicarecoverage andsupplemental employerinsurance coverage($US)
overall aged 65 yearsand older
aged 64 yearsand under
Antidepressants 45.31 48.73 39.67 59.51 39.76Antipsychotics 185.32 211.29 118.44 284.60 71.61Anticonvulsants 50.97 61.81 32.23 92.51 31.08Antiretrovirals 829.73 929.23 318.69 1028.13 124.18Immunosuppressants 735.30 650.28 657.72 645.69 814.86Antineoplastics 15.79 14.48 14.50 14.45 17.03All protected classes 116.35 157.99 75.93 264.59 54.75
� 2006 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2006; 24 Suppl. 3
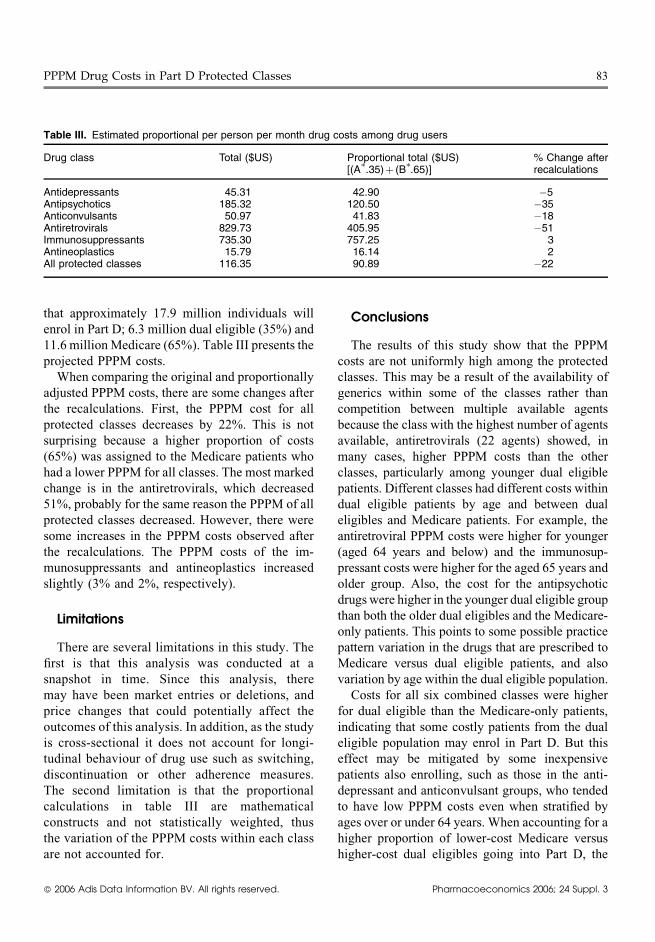
that approximately 17.9 million individuals willenrol in Part D; 6.3 million dual eligible (35%) and11.6 millionMedicare (65%). Table III presents theprojected PPPM costs.
When comparing the original and proportionallyadjusted PPPM costs, there are some changes afterthe recalculations. First, the PPPM cost for allprotected classes decreases by 22%. This is notsurprising because a higher proportion of costs(65%) was assigned to the Medicare patients whohad a lower PPPM for all classes. The most markedchange is in the antiretrovirals, which decreased51%, probably for the same reason the PPPM of allprotected classes decreased. However, there weresome increases in the PPPM costs observed afterthe recalculations. The PPPM costs of the im-munosuppressants and antineoplastics increasedslightly (3% and 2%, respectively).
Limitations
There are several limitations in this study. Thefirst is that this analysis was conducted at asnapshot in time. Since this analysis, theremay have been market entries or deletions, andprice changes that could potentially affect theoutcomes of this analysis. In addition, as the studyis cross-sectional it does not account for longi-tudinal behaviour of drug use such as switching,discontinuation or other adherence measures.The second limitation is that the proportionalcalculations in table III are mathematicalconstructs and not statistically weighted, thusthe variation of the PPPM costs within each classare not accounted for.
Conclusions
The results of this study show that the PPPMcosts are not uniformly high among the protectedclasses. This may be a result of the availability ofgenerics within some of the classes rather thancompetition between multiple available agentsbecause the class with the highest number of agentsavailable, antiretrovirals (22 agents) showed, inmany cases, higher PPPM costs than the otherclasses, particularly among younger dual eligiblepatients. Different classes had different costs withindual eligible patients by age and between dualeligibles and Medicare patients. For example, theantiretroviral PPPM costs were higher for younger(aged 64 years and below) and the immunosup-pressant costs were higher for the aged 65 years andolder group. Also, the cost for the antipsychoticdrugs were higher in the younger dual eligible groupthan both the older dual eligibles and the Medicare-only patients. This points to some possible practicepattern variation in the drugs that are prescribed toMedicare versus dual eligible patients, and alsovariation by age within the dual eligible population.
Costs for all six combined classes were higherfor dual eligible than the Medicare-only patients,indicating that some costly patients from the dualeligible population may enrol in Part D. But thiseffect may be mitigated by some inexpensivepatients also enrolling, such as those in the anti-depressant and anticonvulsant groups, who tendedto have low PPPM costs even when stratified byages over or under 64 years. When accounting for ahigher proportion of lower-cost Medicare versushigher-cost dual eligibles going into Part D, the
PPPM Drug Costs in Part D Protected Classes 83
Table III. Estimated proportional per person per month drug costs among drug users
Drug class Total ($US) Proportional total ($US)[(A
�.35)þ (B
�.65)]
% Change afterrecalculations
Antidepressants 45.31 42.90 �5Antipsychotics 185.32 120.50 �35Anticonvulsants 50.97 41.83 �18Antiretrovirals 829.73 405.95 �51Immunosuppressants 735.30 757.25 3Antineoplastics 15.79 16.14 2All protected classes 116.35 90.89 �22
� 2006 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2006; 24 Suppl. 3

PPPM costs declined for four out of six protectedclasses.
When viewing the average wholesale prices foragents included within the six protected classes,there are some high-cost drugs and also low-costgenerics within the classes. The presence of high-cost drugs, however, may lead to concern thatprotecting these classes may lead to an increasedburden on Part D. But the presence of high-costdrugs within a protected class does not necessarilymean that a high number of patients will beprescribed these drugs with the resulting budgetimplications. First, the underlying prevalence ofthe disease they are indicated for should be takeninto account. Then, as the results of this studyshow, actual drug claims should be reviewed toobserve the scope of utilisation of high-cost drugs.What is often lost in this issue is the mitigatingpresence of lower-cost drugs, whether they aregeneric formulations or simply lower-cost brandeddrugs. Often many patients are on the lower-cost agents.
The claims data in this study allowed a ‘realworld’ check of how much the protected classesmay impact the finances of Part D by showing thePPPM costs of each class and all classes combined.The results showed that although there aresome high costs that additional research shouldbe conducted on to determine the causes of thesecosts, there are a number of classes in which thePPPM costs are relatively low. Also, interestingly,it showed that there are differences within theclasses between the dual eligible and Medicarepatients, and also some differences within the dualeligibles by a single age stratification. This is animportant message to policy makers that a changeto the structure of the protected classes in Part Dmay have differential effects across classes and
also within classes. It also leads to the question thatif this differential is seen in drug costs, would awholesale change to other types of Medicarecoverage show differential results in costs amongpatients with the diseases these protected drugs areindicated for. Future research needs to beconducted to determine whether these cost differ-ences within and across protected classes continueto be shown once the Part D claims data are readyto analyse.
Acknowledgements
This work was performed at Thomson Medstat.
References1. Medicare Program; Medicare Prescription Drug Benefit.
Federal Register 2005 Jan 28; 70 (18): 4193–5852. President George W. Bush, White House press release; 8
December 20033. Over 38 million people with Medicare now receiving pre-
scription drug coverage. HHS press release, 14 June 2006[online]. Available from URL: http://hhs.gov/news/press/2006pres/20060614.html [Accessed 2006 Aug 9]
4. Section-by-section of the Medicare Prescription Drug Sim-plification Act of 2006 [online]. Available from URL:http://www.senate.gov/�finance/press/Bpress/2005press/prb042706a.pdf [Accessed 2006 Aug 9]
5. Why is CMS requiring ‘all or substantially all’ of the drugsin the antidepressant, antipsychotic, anticonvulsant, antic-ancer, immunosuppressant and HIV/AIDS categories[online]. Available from URL: http://www.cms.hhs.gov/PrescriptionDrugCovContra/Downloads/Formulary-GuidanceAllorSubAll.pdf [Accessed 2006 Aug 9]
Correspondence and offprints: Lisa Mucha, PhD,Thomson Medstat, 125 Cambridge Park Drive,Cambridge, MA 02140, USA.e-mail: [email protected]
84 Mucha et al.
� 2006 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2006; 24 Suppl. 3