perceptual and response interference in alzheimer’s
TRANSCRIPT

Clinical Neurophysiology 124 (2013) 2389–2396
Contents lists available at SciVerse ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
Perceptual and response interference in Alzheimer’s disease and mildcognitive impairment
1388-2457/$36.00 � 2013 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.http://dx.doi.org/10.1016/j.clinph.2013.05.014
⇑ Corresponding authors. Addresses: Department of Neurology, Institute ofGeriatrics and Gerontology, Chinese PLA General Hospital, Fuxing Road 28, Beijing100853, PR China. Tel./fax: +86 10 8862 6308 (X. Zhang), Brainnetome Center,Institute of Automation, Chinese Academy of Sciences, Beijing 100190, China. Tel.:+86 10 8261 4469; fax: +86 10 6255 1993 (T. Jiang).
E-mail addresses: [email protected] (X. Zhang), [email protected](T. Jiang).
1 These authors contributed equally to this work.
Pan Wang a,1, Xin Zhang b,c,1, Yong Liu b,c, Sainan Liu a, Bo Zhou a, Zengqiang Zhang a, Hongxiang Yao d,Xi Zhang a,⇑, Tianzi Jiang b,c,e,f,⇑a Department of Neurology, Institute of Geriatrics and Gerontology, Chinese PLA General Hospital, Beijing 100853, Chinab Brainnetome Center, Institute of Automation, Chinese Academy of Sciences, Beijing 100190, Chinac National Laboratory of Pattern Recognition, Institute of Automation, Chinese Academy of Sciences, Beijing 100190, Chinad Department of Radiology, Chinese PLA General Hospital, Beijing 100853, Chinae Key Laboratory for NeuroInformation of Ministry of Education, School of Life Science and Technology, University of Electronic Science and Technology of China, Chengdu 610054,Chinaf The Queensland Brain Institute, The University of Queensland, Brisbane, QLD 4072, Australia
a r t i c l e i n f o h i g h l i g h t s
Article history:Accepted 22 May 2013Available online 17 June 2013
Keywords:Alzheimer’s diseasePerceptual processesResponse processesFlanker taskEvent-related potential
� Patients with cognitive impairment, such as Alzheimer’s disease (AD) and mild cognitive impairment(MCI), are more distracted than normal controls (NC) by irrelevant information.
� Interference process subjected to conflicts happens not only at the response level but also at the per-ceptual level as demonstrated in the work, and subjects of MCI and AD present interference at distinctstages.
� The alterations of N2 are larger than those of P300 in the task and N2 demonstrates more sensitive tothe deterioration of cognitive impairment than P300.
a b s t r a c t
Objectives: The ability to resolve conflicts is indispensable to the function of daily life and decreases withcognitive decline. We hypothesized that subjects with different levels of cognitive impairment exhibit dif-ferent conflict resolution performances and may be susceptible to interference effects at different stages.Methods: Sixteen normal controls (NC), 15 mild cognitive impairment (MCI) and seven Alzheimer’s dis-ease (AD) patients were recruited to perform in a modified Eriksen flanker task.Results: We observed that the AD and MCI patients exhibited smaller accuracy rate and longer responsetime compared to NC subjects. Longer N2 and P300 latencies were observed in the AD group. Furthermore,the MCI group showed a longer latency than the NC group in the P300 latency. The magnitude of the per-ceptual and response interference effects was larger in the AD group than the other groups, and the MCIgroup significantly differed from the NC group at the perceptual level.Conclusion: The ability to resolve conflict decreased with impaired cognition and the perceptual andresponse interference effects may be useful in distinguishing MCI and AD.Significance: The perceptual or response interference effect may potentially be employed as a useful non-invasive probe for the clinical diagnosis of MCI and AD.� 2013 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved.
1. Introduction
In cognitive psychology, information processing occurs at sev-eral distinct levels, including stimulus encoding, target detection,response selection, and response execution (Koch et al., 2010). The-oretically, conflicts may initiate processes at any or all of these lev-els (Eriksen and Schultz, 1979; van Veen et al., 2001). Kornblumand colleagues showed that interference tasks involved conflictsnot only at the response level but also at the perceptual level

2390 P. Wang et al. / Clinical Neurophysiology 124 (2013) 2389–2396
(Kornblum et al., 1990; Kornblum, 1994). Perceptual conflict oc-curs when the presence of task-irrelevant perceptual informationhas a negative impact on the processing of task-relevant percep-tual information, and response conflict occurs when simultaneousneural signals support competing response alternatives (Kornb-lum, 1994).
Alzheimer’s disease (AD), an age-related neurological degenera-tive disorder characterized by early cognitive and behavioral prob-lems, is of great interest for researchers. Mild cognitive impairment(MCI) is the transitional stage from normal aging to AD and do notyet encompass the definition of dementia (Morris et al., 2001; Pet-ersen, 2004). Amnesic MCI (aMCI) is a subtype of MCI and is char-acterized by the main complaint of memory deterioration. It isconsidered a transitional stage between normal aging and AD,and patients show a high rate of progression from this state tothe fully fledged disease (Petersen et al., 2001; Scheltens et al.,2002). The participants in our study all received a diagnosis ofaMCI.
Studies investigating the neuropsychology of AD have typicallybeen primarily focused on cognitive impairments as they relate tomemory function. Recently, a growing number of studies have ana-lyzed impairments in conflict resolution and have found that con-flict resolution ability is reduced in patients with AD (Casey et al.,2000; Castel et al., 2007; Fernandez-Duque and Black, 2006; Gam-boz et al., 2010; Mahoney et al., 2010). However, few studies haveexplored conflict resolution ability in multiple impaired groups,nor have they studied differences in perceptual and response con-flict resolution among AD, MCI patients and normal controls (NC).To clarify the difference, we used the event-related potential (ERP)to measure brain response. ERP reveals potential functional brainabnormalities that are not detectable during clinical or behavioralexaminations (Zhang et al., 2002). It shows promising applicationsfor the evaluation of cognitive processes and consists of a series ofpositive and negative voltage deflections, which are referred to ascomponents. ERP components have been associated with sensory,cognitive, executive and motor events. The N2 and the P300 arethe most frequently recorded potentials and are also the mostprominent potentials indicating changes related to cognitiveimpairment and conflict resolution (Bennys et al., 2007). The N2 re-flects the level of conflict presented by a stimulus. The more nega-tive the N2 was, the higher the level of conflict became(Danielmeier et al., 2009; Forster et al., 2011). The P300 is elicitedby a response to deviant stimuli. Its amplitude is considered to be amanifestation of the brain activity that regulates attention to anincoming stimulus when its representation is updated (Polich,2007). This study used N2 and P300 amplitude differences to indi-cate differences in cognitive functioning among the three groups intheir ability to confront and handle conflicts.
In this study, a modified flanker task (Eriksen and Eriksen,1974) was employed and it required participants to make judg-ments about the central target stimulus while ignoring distract-ers. In this task, there were four conditions: target-alone (none),congruent, neutral and incongruent. By comparing the target-alone with the neutral condition, ‘‘perceptual’’ interference canbe studied because these stimuli differ only in the presence offlankers. By comparing the incongruent stimuli with the neutralstimuli, ‘‘response’’ interference can be studied because thesetwo stimuli are not perceptually different but differ in that incon-gruent flankers prime a particular response, whereas neutralflankers do not.
We hypothesized that subjects with different levels of cognitiveimpairment display different conflict resolution performances andmay be susceptible to interferences at different stages. To addressit, 16 NC, 15 MCI and seven AD patients were recruited to conductthe task. Next, we investigated the perceptual interference byevaluating the difference between the neutral and target-alone
stimulus and response interference by assessing the difference be-tween the neutral and incongruent stimuli.
2. Methods
2.1. Subjects
This study was approved by the Medical Ethics Committee ofthe PLA general hospital. All of the participants were recruited byan advertisement (http://www.301ad.com.cn, Chinese version),and written consent forms were obtained from the subjects or theirlegal guardians. Moreover, all subjects were not treated with anymedication that might influence their cognition during the task.They were right-handed and performed a battery of neuropsycho-logical tests that included the Mini-Mental State Examination(MMSE), Clinical Dementia Rating (CDR) (Morris, 1993) and Activ-ities of Daily Living scale (ADL). The demographic and neuropsy-chological details for the participants are listed in Table 1.
The recruited AD patients fulfilled the following inclusion crite-ria: (1) diagnosed with the National Institute of Neurological andCommunicative Disorders and Stroke and the Alzheimer’s Diseaseand Related Disorders Association criteria for probable AD; (2)CDR = 1; (3) were not receiving nootropic drugs such as anticholin-esterase inhibitors; (4) were able to perform the neuropsychologi-cal test. The diagnostic criteria for MCI was as stated in Petersenet al. (1999) including: (1) memory complaints, lasting at least6 months; (2) CDR = 0.5; (3) intact functional status andADL < 26; and (4) lack of dementia. Meanwhile, the AD and MCI pa-tients also met the core clinical criteria for probable AD dementiaand MCI as described in the recently published recommendationof the new diagnostic criteria (Albert et al., 2011; McKhann et al.,2011; Sperling et al., 2011). The criteria for the NC subjects com-prised the following: (1) normal general physical status; (2)CDR = 0; and (3) no memory complaints. Structural MRI imageswere recorded and analyzed with voxel-based morphometry(VBM) to quantify the differences between subjects’ brains thatcorrespond to the groups. There were no significant differencesin the parietal and frontal lobes among the three groups.
Excluding conditions for this study were as follows: (1) meta-bolic conditions such as hypothyroidism or vitamin B12 or folicacid deficiencies; (2) psychiatric disorders such as schizophreniaor depression; (3) infarction or brain hemorrhaging as indicatedby MR/CT imaging; or (4) Parkinsonian syndrome, epilepsy andother nervous system diseases. In addition, patients with a metallicforeign body were excluded from the study.
2.2. Task
The stimulus display was administered by EEvoke (AdvancedNeuro Technology (ANT) software BV, 2004). Participants werepositioned roughly parallel to a CRT monitor and responded to astimulus using their thumbs to click on a control pad held withtwo hands. The left hand was used to respond to a centered arrowfacing to the left, and the right hand was used to respond to a cen-tered arrow facing to the right. They were instructed to focus onthe task and to respond to a stimulus quickly and correctly. The re-sponse window was set to be the same as the inter-stimulusinterval.
Before the actual task, a practice test of 15 events was per-formed. The task was separated into three blocks of the samelength, with 100 stimuli for each block, as depicted in Fig. 1A.The task was composed of four conditions, with each conditionconsisting of 25 events that were placed in a random order. Asshown in Fig. 1B, the stimulus of the target-alone consisted of noneof the flankers, the neutral stimulus with ‘‘ + ’’ flanker, the congru-
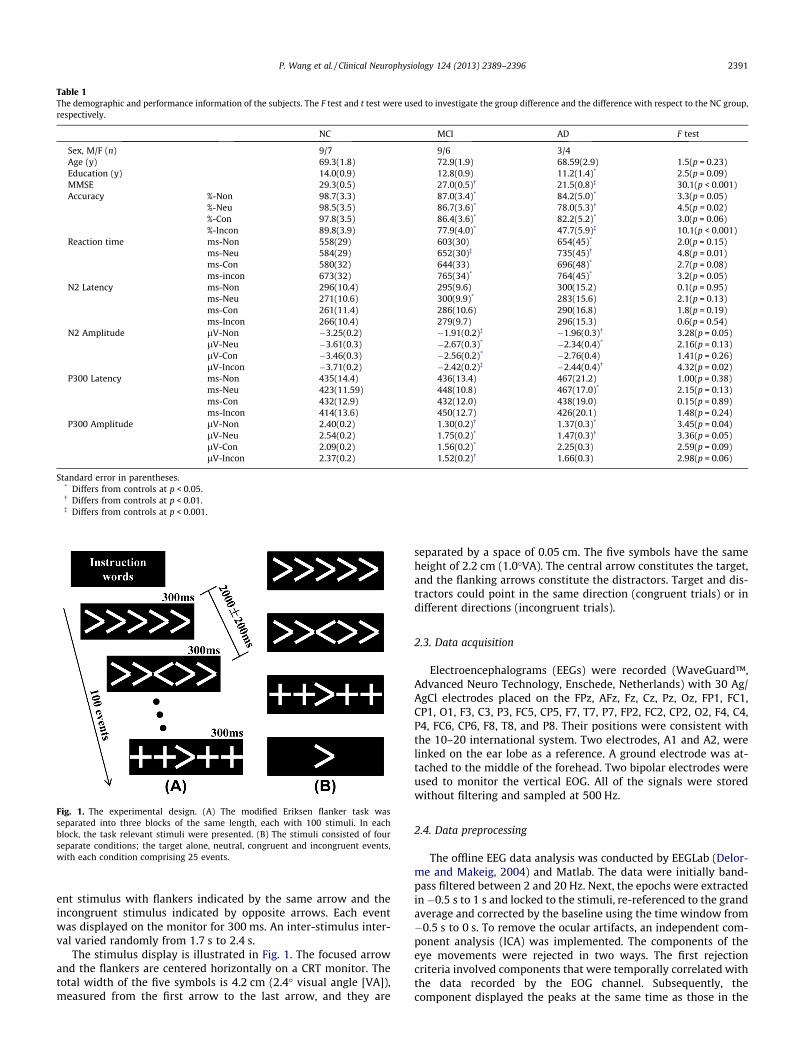
Table 1The demographic and performance information of the subjects. The F test and t test were used to investigate the group difference and the difference with respect to the NC group,respectively.
NC MCI AD F test
Sex, M/F (n) 9/7 9/6 3/4Age (y) 69.3(1.8) 72.9(1.9) 68.59(2.9) 1.5(p = 0.23)Education (y) 14.0(0.9) 12.8(0.9) 11.2(1.4)* 2.5(p = 0.09)MMSE 29.3(0.5) 27.0(0.5)� 21.5(0.8)� 30.1(p < 0.001)Accuracy %-Non 98.7(3.3) 87.0(3.4)* 84.2(5.0)* 3.3(p = 0.05)
%-Neu 98.5(3.5) 86.7(3.6)* 78.0(5.3)� 4.5(p = 0.02)%-Con 97.8(3.5) 86.4(3.6)* 82.2(5.2)* 3.0(p = 0.06)%-Incon 89.8(3.9) 77.9(4.0)* 47.7(5.9)� 10.1(p < 0.001)
Reaction time ms-Non 558(29) 603(30) 654(45)* 2.0(p = 0.15)ms-Neu 584(29) 652(30)� 735(45)� 4.8(p = 0.01)ms-Con 580(32) 644(33) 696(48)* 2.7(p = 0.08)ms-incon 673(32) 765(34)* 764(45)* 3.2(p = 0.05)
N2 Latency ms-Non 296(10.4) 295(9.6) 300(15.2) 0.1(p = 0.95)ms-Neu 271(10.6) 300(9.9)* 283(15.6) 2.1(p = 0.13)ms-Con 261(11.4) 286(10.6) 290(16.8) 1.8(p = 0.19)ms-Incon 266(10.4) 279(9.7) 296(15.3) 0.6(p = 0.54)
N2 Amplitude lV-Non �3.25(0.2) �1.91(0.2)� �1.96(0.3)� 3.28(p = 0.05)lV-Neu �3.61(0.3) �2.67(0.3)* �2.34(0.4)* 2.16(p = 0.13)lV-Con �3.46(0.3) �2.56(0.2)* �2.76(0.4) 1.41(p = 0.26)lV-Incon �3.71(0.2) �2.42(0.2)� �2.44(0.4)� 4.32(p = 0.02)
P300 Latency ms-Non 435(14.4) 436(13.4) 467(21.2) 1.00(p = 0.38)ms-Neu 423(11.59) 448(10.8) 467(17.0)* 2.15(p = 0.13)ms-Con 432(12.9) 432(12.0) 438(19.0) 0.15(p = 0.89)ms-Incon 414(13.6) 450(12.7) 426(20.1) 1.48(p = 0.24)
P300 Amplitude lV-Non 2.40(0.2) 1.30(0.2)� 1.37(0.3)* 3.45(p = 0.04)lV-Neu 2.54(0.2) 1.75(0.2)* 1.47(0.3)� 3.36(p = 0.05)lV-Con 2.09(0.2) 1.56(0.2)* 2.25(0.3) 2.59(p = 0.09)lV-Incon 2.37(0.2) 1.52(0.2)� 1.66(0.3) 2.98(p = 0.06)
Standard error in parentheses.* Differs from controls at p < 0.05.� Differs from controls at p < 0.01.� Differs from controls at p < 0.001.
Fig. 1. The experimental design. (A) The modified Eriksen flanker task wasseparated into three blocks of the same length, each with 100 stimuli. In eachblock, the task relevant stimuli were presented. (B) The stimuli consisted of fourseparate conditions; the target alone, neutral, congruent and incongruent events,with each condition comprising 25 events.
P. Wang et al. / Clinical Neurophysiology 124 (2013) 2389–2396 2391
ent stimulus with flankers indicated by the same arrow and theincongruent stimulus indicated by opposite arrows. Each eventwas displayed on the monitor for 300 ms. An inter-stimulus inter-val varied randomly from 1.7 s to 2.4 s.
The stimulus display is illustrated in Fig. 1. The focused arrowand the flankers are centered horizontally on a CRT monitor. Thetotal width of the five symbols is 4.2 cm (2.4� visual angle [VA]),measured from the first arrow to the last arrow, and they are
separated by a space of 0.05 cm. The five symbols have the sameheight of 2.2 cm (1.0�VA). The central arrow constitutes the target,and the flanking arrows constitute the distractors. Target and dis-tractors could point in the same direction (congruent trials) or indifferent directions (incongruent trials).
2.3. Data acquisition
Electroencephalograms (EEGs) were recorded (WaveGuard™,Advanced Neuro Technology, Enschede, Netherlands) with 30 Ag/AgCl electrodes placed on the FPz, AFz, Fz, Cz, Pz, Oz, FP1, FC1,CP1, O1, F3, C3, P3, FC5, CP5, F7, T7, P7, FP2, FC2, CP2, O2, F4, C4,P4, FC6, CP6, F8, T8, and P8. Their positions were consistent withthe 10–20 international system. Two electrodes, A1 and A2, werelinked on the ear lobe as a reference. A ground electrode was at-tached to the middle of the forehead. Two bipolar electrodes wereused to monitor the vertical EOG. All of the signals were storedwithout filtering and sampled at 500 Hz.
2.4. Data preprocessing
The offline EEG data analysis was conducted by EEGLab (Delor-me and Makeig, 2004) and Matlab. The data were initially band-pass filtered between 2 and 20 Hz. Next, the epochs were extractedin�0.5 s to 1 s and locked to the stimuli, re-referenced to the grandaverage and corrected by the baseline using the time window from�0.5 s to 0 s. To remove the ocular artifacts, an independent com-ponent analysis (ICA) was implemented. The components of theeye movements were rejected in two ways. The first rejectioncriteria involved components that were temporally correlated withthe data recorded by the EOG channel. Subsequently, thecomponent displayed the peaks at the same time as those in the

2392 P. Wang et al. / Clinical Neurophysiology 124 (2013) 2389–2396
EOG were removed. The second criteria relied on the topography.The component of the eye movements demonstrated a spatialweight located at the frontal channels. After its removal, theremaining components were then back-projected onto the EEGchannels. We then designated N2 as the negative peak from200 ms to 350 ms on the electrodes at F3, Fz and F4 (Folstein andVan Petten, 2008), and P300 as the positive peak from 300 ms to550 ms on the electrodes at P3, Pz and P4 (Polich, 2007). The laten-cies of the N2 and P300, respectively, corresponded to the latenciesof the maximum peaks of the N2 and P300 measured from stimu-lus onset.
2.5. Statistical analysis
The statistics were performed by the R software (R Develop-ment Core Team, 2011). Two-sample two-tailed t tests were con-ducted to evaluate the group differences between two of thethree groups. As the median of the population was more robust,it was more appropriate to use the median rather than the meanto determine an ‘‘average’’; thus, the median response time and re-sponse accuracy were analyzed using a multivariate analysis ofcovariance (MANCOVA). For this analysis, the diagnosis (AD, MCI,and NC) was the between-subject factor and the conditions (tar-get-alone, neutral, congruent and incongruent) were a within-sub-ject factor, with age and the Mini-Mental State Examination(MMSE) being included as covariates (Krueger et al., 2009).
When a significant multivariate main effect was detected withMANCOVA, additional univariate ANCOVAs were performed to elu-cidate differences in either the response times or accuracy with abetween-subject factor group with any two of three possible levelsand a within-subject factor with any two of four levels. If there wasa significant multivariate Group � Condition interaction effect, fur-ther ANCOVAs were conducted to investigate the interaction witha two-level group factor and a two-level condition factor. For alltests, the alpha level was set at 5%. By the same principle, theERP components were also analyzed by MANCOVA (p < 0.05). Inthis study, the accuracy and response time were replaced witheither the amplitude or latency of N2 and P300.
3. Results
3.1. Subjects and statistical results
The mean values for each of the cognitive and flanker measureswere completed by the AD, MCI and NC subjects and are displayedin Table 1. The AD, MCI and NC group did not statistically differ inage (F2,35 = 1.49, p = 0.23); however, the number of years of educa-tion in the AD group was slightly smaller than that of the NC group(p = 0.09). For the clinical measures, in particular, the scores of theMMSE, the MCI patients performed better than the AD patients(p < 0.001) but performed poorer than the NC (p = 0.01).
3.2. Performance
In terms of accuracy, a group effect (F2,29 = 6.4, p = 0.005) indi-cated that there were significant differences among the threegroups. The accuracy of the MCI group was higher than that ofthe AD group and lower than that of the NC group. A significant con-dition effect (F3,248 = 21.9, p < 0.001) was also observed. Comparedwith other stimuli, more errors were made in response to the incon-gruent stimuli by all of the groups. Because a Group � Conditioninteraction (F6,248 = 9, p < 0.001) was found in the multivariate anal-ysis (Fig. 2A), two comparisons were used to test the Group � Per-ceptual and Group � Response conflict interaction. Although nosignificant Group � Perceptual conflict interaction was found
(F2,108 = 0.6, p = 0.5), a Group � Response conflict interaction wasobserved (F2,108 = 7.2, p = 0.002). Further testing showed that theresponse interference effect was larger in the AD group than inthe MCI and NC groups (F1,62 = 7.2, p = 0.009 and F1,65 = 19.8,p < 0.001, respectively), while the effect was not significantly differ-ent between the MCI and NC groups.
For the response time, a group effect (F2,32 = 2.8, p = 0.07) indi-cated that there were no significant differences among the groups,while the condition effect (F3,96 = 24.2, p < 0.001) indicated that theresponses were slower in the incongruent stimuli compared withthe other stimulus types. The Group � Condition interaction(F6,96 = 2.5, p = 0.02) plot of the response time is shown in Fig. 2B.Moreover, we found no significant Group � Response conflictinteraction (F2,32 = 3.3, p = 0.06) and the Group � Perceptual con-flict interaction (F2,32 = 8.6, p = 0.001) showed that the perceptualinterference effect was larger in the AD group than in the MCI(F1,18 = 4.4, p = 0.05) nearly and NC groups (F1,19 = 19.7, p < 0.001)significantly.
3.3. ERPs
The averaged ERPs of every condition are shown in Fig. 2C–F.Representative waveforms only at the Cz electrode are shown forbrevity. After conducting an MANCOVA analysis, the N2 latencyshowed a significant condition effect (F3,99 = 5.4, p = 0.002). Fur-thermore, the latencies of the MCI group were longer than thoseof the NC group, and although the latencies of the AD group werealso longer than those of the NC group, they were not significant(Fig. 3A). In Fig. 3C, the Group � Condition interaction effects weresignificant (F6,99 = 2.4, p = 0.03). Further analysis showed that theeffect was significant between the MCI and NC groups as comparedwith the target-alone and the neutral conditions (F1,28 = 5.7,p = 0.02) and between the MCI and AD compared to the neutraland the incongruent effect (F1,18 = 6.7, p = 0.02).
For the N2 amplitude, there was a condition effect (F6,99 = 6.4,p < 0.001). Further testing showed that the amplitudes evoked bythe neutral stimuli were higher than the target-alone stimuli(F1,33 = 10.4, p = 0.003). A group main effect also existed in the N2amplitude (F2,33 = 3.8, p = 0.03). As depicted in Fig. 3B, the effectappeared between the NC and MCI groups (p < 0.001) and betweenNC and AD groups (p < 0.05); however, no Group � Condition ef-fects were found (Fig. 3D).
The multivariate P300 latency analysis demonstrated a nearlysignificant Group � Condition effect (F6,99 = 2.1, p = 0.06), as shownin Fig. 3E. Further testing showed that the effect showed nearly sig-nificant differences between the AD and MCI subjects from theneutral to the incongruent condition (F1,18 = 3.1, p = 0.09).
For the P300 amplitude, a group effect (F2,33 = 3.9, p = 0.03) wasfound in all of the conditions. Further t testing showed that thegroup effect showed differences between the NC and MCI patients(p < 0.001) and between the NC and AD patients (p < 0.05); how-ever, no Group � Condition effects were observed (Fig. 3F).
4. Discussion
This study explored the ability to resolve conflicts among personswith different levels of cognition impairment using a flanker taskand investigated whether these groups demonstrated any interfer-ence effects. The two levels, perceptual and response, were exam-ined here. Perceptual and response are two necessary processesthat occur during conflict resolution. The behavioral and ERP datawere recorded to study the interference effect. Perceptual conflictoccurs when the presence of task-irrelevant perceptual informationhas a negative impact upon the processing of task-relevantperceptual information, and response conflict occurs when
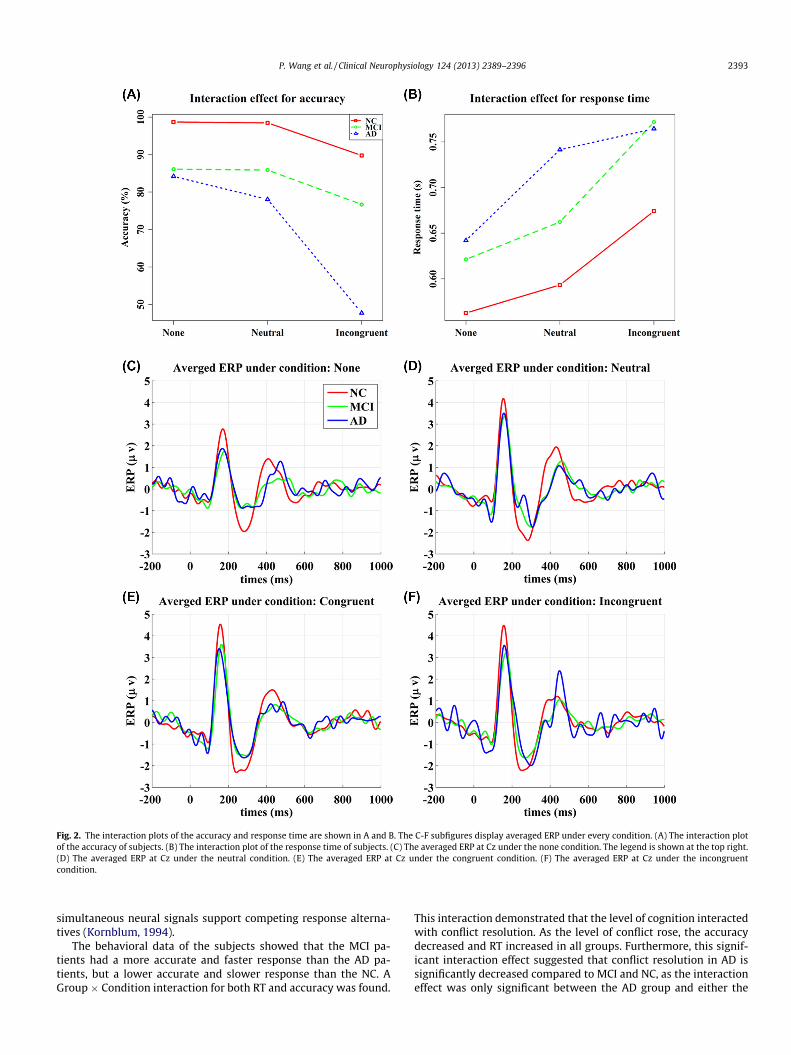
Fig. 2. The interaction plots of the accuracy and response time are shown in A and B. The C-F subfigures display averaged ERP under every condition. (A) The interaction plotof the accuracy of subjects. (B) The interaction plot of the response time of subjects. (C) The averaged ERP at Cz under the none condition. The legend is shown at the top right.(D) The averaged ERP at Cz under the neutral condition. (E) The averaged ERP at Cz under the congruent condition. (F) The averaged ERP at Cz under the incongruentcondition.
P. Wang et al. / Clinical Neurophysiology 124 (2013) 2389–2396 2393
simultaneous neural signals support competing response alterna-tives (Kornblum, 1994).
The behavioral data of the subjects showed that the MCI pa-tients had a more accurate and faster response than the AD pa-tients, but a lower accurate and slower response than the NC. AGroup � Condition interaction for both RT and accuracy was found.
This interaction demonstrated that the level of cognition interactedwith conflict resolution. As the level of conflict rose, the accuracydecreased and RT increased in all groups. Furthermore, this signif-icant interaction effect suggested that conflict resolution in AD issignificantly decreased compared to MCI and NC, as the interactioneffect was only significant between the AD group and either the
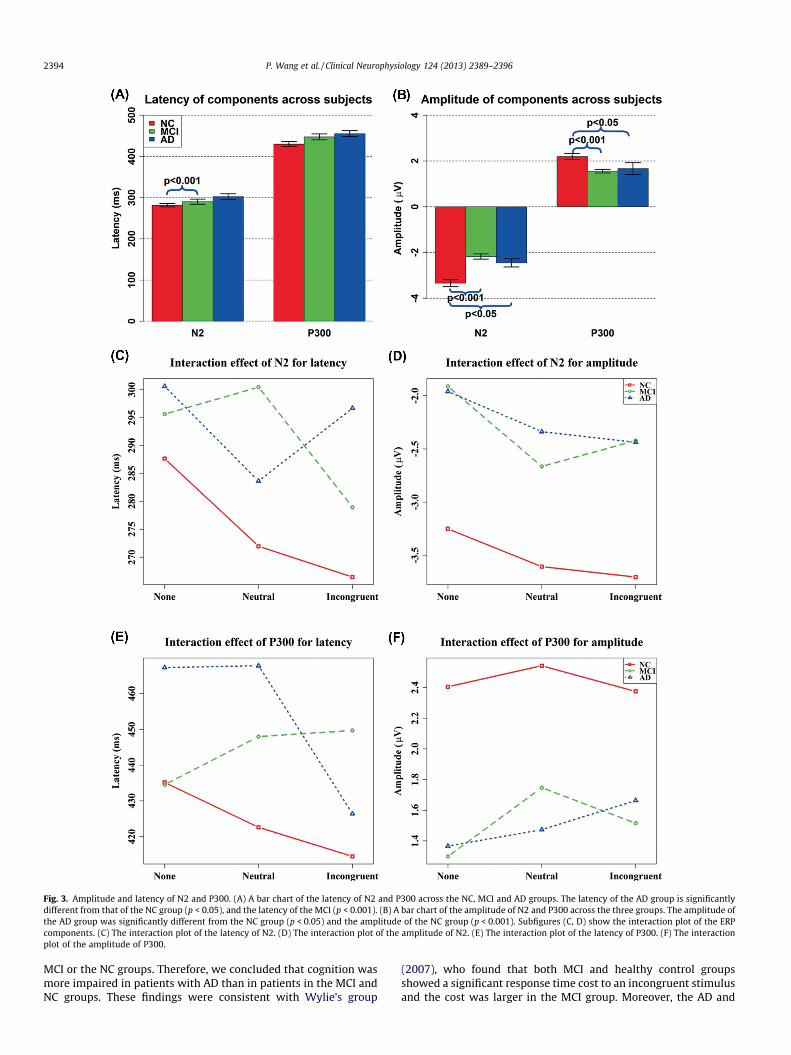
Fig. 3. Amplitude and latency of N2 and P300. (A) A bar chart of the latency of N2 and P300 across the NC, MCI and AD groups. The latency of the AD group is significantlydifferent from that of the NC group (p < 0.05), and the latency of the MCI (p < 0.001). (B) A bar chart of the amplitude of N2 and P300 across the three groups. The amplitude ofthe AD group was significantly different from the NC group (p < 0.05) and the amplitude of the NC group (p < 0.001). Subfigures (C, D) show the interaction plot of the ERPcomponents. (C) The interaction plot of the latency of N2. (D) The interaction plot of the amplitude of N2. (E) The interaction plot of the latency of P300. (F) The interactionplot of the amplitude of P300.
2394 P. Wang et al. / Clinical Neurophysiology 124 (2013) 2389–2396
MCI or the NC groups. Therefore, we concluded that cognition wasmore impaired in patients with AD than in patients in the MCI andNC groups. These findings were consistent with Wylie’s group
(2007), who found that both MCI and healthy control groupsshowed a significant response time cost to an incongruent stimulusand the cost was larger in the MCI group. Moreover, the AD and

P. Wang et al. / Clinical Neurophysiology 124 (2013) 2389–2396 2395
MCI patients encountered greater difficulty in resolving conflictthan the healthy elder controls (van Deursen et al., 2009; Wylieet al., 2007).
The N2 component was typically evoked prior to the motor re-sponse, suggesting a link to the cognitive processes of stimulusevaluation, selective attention and conscious discrimination (Hillet al., 2002). Comparison of the N2 latency and amplitude revealedthat the AD group significantly elicited smaller N2 amplitudes andslower N2 responses than both the NC and MCI groups. Theseobservations are consistent with several previous studies (Bennyset al., 2007; Papaliagkas et al., 2011; Tachibana et al., 1996). Thedifferences in the amplitude and response time might reflect thereduced speed and efficiency of conflict detection in AD and MCIpatients. The ERP results indicated that the MCI and AD groups’worse conflict resolving performances could be attributed to eitheran impairment of neural processing or inefficient frontal neuralfunctioning during conflict resolution. Based on the behavioraland ERP data, we conclude that the conflict resolving performanceis correlated with cognitive levels and that the ability of resolvingconflict is partially impaired in AD and MCI patients comparedwith NC subjects.
Previous studies have proposed that the P300 component is suf-ficiently sensitive to detect early stages of cognitive impairment(Ashford et al., 2011; Bennys et al., 2007; Polich and Corey-Bloom,2005). In contrast, our study found changes in N2 that were largerthan those of P300. One reason for this discrepancy may be thatmost previous studies employed an auditory oddball task, whereaswe used a flanker task in this study. The flanker task covers strate-gic monitoring and the immediate control of motor response witha larger N2, while the oddball task reflects neural reactions tounpredictable, but recognizable, events with a larger P300. Becausethe flanker task is related to executive function, we conclude thatN2 is more sensitive than P300 in evaluating the interference effectdue to the impairment of cognitive function.
In addition, N2 activation in the frontal brain regions is relatedto conflict monitoring (Botvinick et al., 2004; Kerns et al., 2004);however, P300 activation in the central-parietal regions is corre-lated with attention control processing (Liotti et al., 2000). A num-ber of studies have implicated early and significant changes inexecutive function and early neurobiological changes in the frontallobes of AD or MCI patients (Baddeley et al., 2001; Duke and Kasz-niak, 2000; Perry and Hodges, 1999; Royall et al., 2002). Neuroim-aging studies of early AD and MCI have found increased prefrontalactivity during cognitive tasks compared with normal elder controlsubjects (Agosta et al., 2012; Pariente et al., 2005). Thus, the N2component of ERP could be of high diagnostic value for the earlydiagnosis of AD and MCI.
In a cognitive task, there will be several perceptual or cognitiveprocesses where conflict interference effects may occur. A numberof independent mental systems in the brain are involved in thecognition of a human being. If the outputs of the systems areincongruent, an interference effect occurs and additional resourcesare required to resolve the conflict, which may have a negative ef-fect on the subject’s performance (De Houwer, 2003; Kim et al.,2011; Nassauer and Halperin, 2003; Sugg and McDonald, 1994).
We hypothesized that, if response deficiency presented itself,then AD patients would show a larger response interference effectthan either patients with MCI or the NC group. The accuracy inincongruent trials declined dramatically in AD patients when com-pared to the neutral condition or to the MCI or the NC group; thus,the response interference effect was larger in the AD group. As thetime spent making correct responses was a more meaningful mea-sure for depicting subjects’ speed, only response times in correcttrials were analyzed in this study. However, there was no signifi-cant group difference in RT in response conflict trials betweenthe groups. However, subjects’ RTs depended upon their accuracy.
Fig. 2A showed that the accuracy of the AD in incongruent trialswas only 50%. This lower accuracy, which was nearly equal to ran-dom chance, might imply that the AD patients did not have suffi-cient cognitive capabilities to successfully resolve the conflict.Thus, we propose that the AD patients pressed either the right orthe left button randomly without identifying the targeting accu-rately. Combining their much lower accuracy and their RTs, whichwere only equal to those of the MCI group, we could infer that re-sponse conflict was impaired more seriously in AD. There were nosignificant differences between the MCI and NC groups. The ERP re-sults showed that the difference in the N2 latency between theneutral and target-alone stimuli was more significant in the MCIthan in the NC group. In addition, the difference in the N2 andP300 latencies between the neutral and incongruent stimuli wasmore significant in the AD group than in the MCI group. Thus,the MCI subjects demonstrated a stronger perceptual interferenceduring conflict resolution than the NC subjects, and the AD patientsexhibited the strongest perceptual interference. The AD patientsrevealed a significantly higher level of interference in the responsethan both the MCI and NC; however, the MCI patients did not differfrom the NC.
Flanker-induced interference may attribute to perceptual pro-cessing (Duncan and Humphreys, 1989; Eriksen and Schultz,1979; Smid et al., 1991). The interference results in slow perfor-mance under neutral flankers due to the additional time requiredto recognize the central target. Compared with the NC subjects, pa-tients with AD or MCI were more distracted by the irrelevant infor-mation at the perceptual level, as demonstrated by their increasedresponse time and N2 latency. In addition to effects on the percep-tual level, the interference effect may result from the response le-vel. When a greater number of flankers appear compared with thetarget, the response activation is initially due to the flankers and,subsequently, from the target. The reaction times will be delayedby the incongruent flankers due to a conflict between the flankerand target-based response. At this level, the AD patients are moredistracted. Thus, compared with the NC, we speculate that patientsat the early stage of cognition impairment are susceptible to theinterference mainly from the perception level and patients at thelater stage are susceptible to both the perception and the responselevel.
Although our reported results demonstrate a legitimate study,we recognize the limitations. First, we included a relatively smallnumber, particularly in the AD group. However, our results weresignificant overall, indicating that the group differences were suffi-ciently large. In addition, the ocular movements recorded duringthe ERP were unavoidable in the elder patients with cognitiveimpairment. Thus, we introduced an additional step to removethe noise. Although the method of removing the noise in this studyhas been employed in previous studies, the results should still becarefully interpreted.
We conclude that subjects with AD and MCI are more distractedthan NC by irrelevant information. In addition, subjects with ADhave conflict interference on both levels (perceptual and response),and MCI demonstrate at the perceptual level. Thus, the differentlevels of interference may be a predictor in distinguishing ADand MCI.
Acknowledgements
This work was partially supported by the National Key Basic Re-search and Development Program (973) (Grant No.2011CB707800), the Natural Science Foundation of China (GrantNos. 60831004, 81270020, 81101082), the Specific Healthcare Re-search Project (Grant No. 13BJZ50) and PLA General Hospital Scien-tific Innovation Fund (Grant No. 12KMM19).
2396 P. Wang et al. / Clinical Neurophysiology 124 (2013) 2389–2396
References
Agosta F, Pievani M, Geroldi C, Copetti M, Frisoni GB, Filippi M. Resting state fMRI inAlzheimer’s disease: beyond the default mode network. Neurobiol Aging2012;33:1564–78.
Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. Thediagnosis of mild cognitive impairment due to Alzheimer’s disease:recommendations from the National Institute on Aging-Alzheimer’sAssociation workgroups on diagnostic guidelines for Alzheimer’s disease.Alzheimers Dement 2011;7:270–9.
Ashford JW, Coburn KL, Rose TL, Bayley PJ. P300 energy loss in aging andAlzheimer’s disease. J Alzheimers Dis 2011;26(Suppl. 3):229–38.
Baddeley AD, Baddeley HA, Bucks RS, Wilcock GK. Attentional control in Alzheimer’sdisease. Brain 2001;124:1492–508.
Bennys K, Portet F, Touchon J, Rondouin G. Diagnostic value of event-relatedevoked potentials N200 and P300 subcomponents in early diagnosis ofAlzheimer’s disease and mild cognitive impairment. J Clin Neurophysiol2007;24:405–12.
Botvinick MM, Cohen JD, Carter CS. Conflict monitoring and anterior cingulatecortex: an update. Trends Cogn Sci 2004;8:539–46.
Casey BJ, Thomas KM, Welsh TF, Badgaiyan RD, Eccard CH, Jennings JR, et al.Dissociation of response conflict, attentional selection, and expectancy withfunctional magnetic resonance imaging. Proc Natl Acad Sci U S A2000;97:8728–33.
Castel AD, Balota DA, Hutchison KA, Logan JM, Yap MJ. Spatial attention andresponse control in healthy younger and older adults and individuals withAlzheimer’s disease: evidence for disproportionate selection impairments in theSimon task. Neuropsychology 2007;21:170–82.
Danielmeier C, Wessel JR, Steinhauser M, Ullsperger M. Modulation of the error-related negativity by response conflict. Psychophysiology 2009;46:1288–98.
De Houwer J. On the role of stimulus-response and stimulus-stimulus compatibilityin the stroop effect. Mem Cognit 2003;31:353–9.
Delorme A, Makeig S. EEGLAB: an open source toolbox for analysis of single-trialEEG dynamics including independent component analysis. J Neurosci Methods2004;134:9–21.
Duke LM, Kaszniak AW. Executive control functions in degenerative dementias: acomparative review. Neuropsychol Rev 2000;10:75–99.
Duncan J, Humphreys GW. Visual search and stimulus similarity. Psychol Rev1989;96:433–58.
Eriksen BA, Eriksen CW. Effects of noise letters upon the identification of a targetletter in a nonsearch task. Percept Psychophys 1974;16:143–9.
Eriksen CW, Schultz DW. Information processing in visual search: a continuous flowconception and experimental results. Percept Psychophys 1979;25:249–63.
Fernandez-Duque D, Black SE. Attentional networks in normal aging andAlzheimer’s disease. Neuropsychology 2006;20:133–43.
Folstein JR, Van Petten C. Influence of cognitive control and mismatch on the N2component of the ERP: a review. Psychophysiology 2008;45:152–70.
Forster SE, Carter CS, Cohen JD, Cho RY. Parametric manipulation of the conflictsignal and control-state adaptation. J Cogn Neurosci 2011;23:923–35.
Gamboz N, Zamarian S, Cavallero C. Age-related differences in the attentionnetwork test (ANT). Exp Aging Res 2010;36:287–305.
Hill H, Strube M, Roesch-Ely D, Weisbrod M. Automatic vs. controlled processes insemantic priming–differentiation by event-related potentials. Int JPsychophysiol 2002;44:197–218.
Kerns JG, Cohen JD, MacDonald 3rd AW, Cho RY, Stenger VA, Carter CS. Anteriorcingulate conflict monitoring and adjustments in control. Science2004;303:1023–6.
Kim C, Kroger JK, Kim J. A functional dissociation of conflict processing withinanterior cingulate cortex. Hum Brain Mapp 2011;32:304–12.
Koch I, Gade M, Schuch S, Philipp AM. The role of inhibition in task switching: areview. Psychonom Bull Rev 2010;17:1–14.
Kornblum S, Hasbroucq T, Osman A. Dimensional overlap: cognitive basis forstimulus-response compatibility – a model and taxonomy. Psychol Rev1990;97:253–70.
Kornblum S. The way irrelevant dimensions are processed depends on what theyoverlap with: the case of Stroop- and Simon-like stimuli. Psychol Res1994;56:130–5.
Krueger CE, Bird AC, Growdon ME, Jang JY, Miller BL, Kramer JH. Conflict monitoringin early frontotemporal dementia. Neurology 2009;73:349–55.
Liotti M, Woldorff MG, Perez R, Mayberg HS. An ERP study of the temporal course ofthe Stroop color-word interference effect. Neuropsychologia 2000;38:701–11.
Mahoney JR, Verghese J, Goldin Y, Lipton R, Holtzer R. Alerting, orienting, andexecutive attention in older adults. J Int Neuropsychol Soc 2010;16:877–89.
McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack Jr CR, Kawas CH, et al. Thediagnosis of dementia due to Alzheimer’s disease: recommendations from theNational Institute on Aging-Alzheimer’s Association workgroups on diagnosticguidelines for Alzheimer’s disease. Alzheimers Dement 2011;7:263–9.
Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules.Neurology 1993;43:2412–4.
Morris JC, Storandt M, Miller JP, McKeel DW, Price JL, Rubin EH, et al. Mild cognitiveimpairment represents early-stage Alzheimer disease. Arch Neurol2001;58:397–405.
Nassauer KW, Halperin JM. Dissociation of perceptual and motor inhibitionprocesses through the use of novel computerized conflict tasks. J IntNeuropsychol Soc 2003;9:25–30.
Papaliagkas VT, Kimiskidis VK, Tsolaki MN, Anogianakis G. Cognitive event-relatedpotentials: longitudinal changes in mild cognitive impairment. ClinNeurophysiol 2011;122:1322–6.
Pariente J, Cole S, Henson R, Clare L, Kennedy A, Rossor M, et al. Alzheimer’s patientsengage an alternative network during a memory task. Ann Neurol2005;58:870–9.
Perry RJ, Hodges JR. Attention and executive deficits in Alzheimer’s disease. Acritical review. Brain 1999;122:383–404.
Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Mild cognitiveimpairment: clinical characterization and outcome. Arch Neurol1999;56:303–8.
Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC, Rabins PV, et al. Current conceptsin mild cognitive impairment. Arch Neurol 2001;58:1985–92.
Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med2004;256:183–94.
Polich J, Corey-Bloom J. Alzheimer’s disease and P300: review and evaluation of taskand modality. Curr Alzheimer Res 2005;2:515–25.
Polich J. Updating P300: an integrative theory of P3a and P3b. Clin Neurophysiol2007;118:2128–48.
R Development Core Team. R: a language and environment for statisticalcomputing. Austria, Vienna: R Development Core Team; 2011.
Royall DR, Palmer R, Mulroy AR, Polk MJ, Roman GC, David JP, et al. Pathologicaldeterminants of the transition to clinical dementia in Alzheimer’s disease. ExpAging Res 2002;28:143–62.
Scheltens P, Fox N, Barkhof F, De Carli C. Structural magnetic resonance imaging inthe practical assessment of dementia: beyond exclusion. Lancet Neurol2002;1:13–21.
Smid HG, Lamain W, Hogeboom MM, Mulder G, Mulder LJ. Psychophysiologicalevidence for continuous information transmission between visual search andresponse processes. J Exp Psychol Hum Percept Perform 1991;17:696–714.
Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, et al. Towarddefining the preclinical stages of Alzheimer’s disease: recommendations fromthe National Institute on Aging-Alzheimer’s Association workgroups ondiagnostic guidelines for Alzheimer’s disease. Alzheimers Dement2011;7:280–92.
Sugg MJ, McDonald JE. Time course of inhibition in color-response and word-response versions of the Stroop task. J Exp Psychol Hum Percept Perform1994;20:647–75.
Tachibana H, Takeda M, Okuda B, Kawabata K, Nishimura H, Kodama N, et al.Multimodal evoked potentials in Alzheimer’s disease and Binswanger’s disease.J Geriatr Psychiatry Neurol 1996;9:7–12.
van Deursen JA, Vuurman EF, Smits LL, Verhey FR, Riedel WJ. Response speed,contingent negative variation and P300 in Alzheimer’s disease and MCI. BrainCogn 2009;69:592–9.
van Veen V, Cohen JD, Botvinick MM, Stenger VA, Carter CS. Anterior cingulatecortex, conflict monitoring, and levels of processing. Neuroimage2001;14:1302–8.
Wylie SA, Ridderinkhof KR, Eckerle MK, Manning CA. Inefficient response inhibitionin individuals with mild cognitive impairment. Neuropsychologia2007;45:1408–19.
Zhang X, Wang Y, Li S, Huang X, Cui L. Early detection of cognitive impairment inpatients with obstructive sleep apnea syndrome: an event-related potentialstudy. Neurosci Lett 2002;325:99–102.