performance salvatore hospital 2009 laquila eq
TRANSCRIPT

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 1/18
Performance of the San SalvatoreRegional Hospital in the 2009L’Aquila Earthquake
H. John Price,a) Adriano De Sortis,b) and Marko Schotanus,c) M.EERI
The San Salvatore Hospital in Coppito was closed shortly after the 6 April
2009 L’Aquila earthquake, even though the buildings on its campus experienced
only limited and localized structural damage. The decision to close part or all of an essential facility such as a hospital can be easily made in the heat of the
moment after a disaster, but reopening even portions of such a facility is far
more complex and raises a large number of operational issues. A documented pre-established program for post-event safety inspections, as well as training in
its implementation for both on-site and backup personnel, is vital to the contin-ued operation of any essential facility. While continued operation after an event
may be the targeted goal, it may not actually be fully achieved, in particular for older facilities, and some disruption is to be expected. Management of realistic
expectations is a vital part of the program for post-event safety inspections.[DOI: 10.1193/1.3673595]
INTRODUCTION
The 6 April 2009 L’Aquila earthquake, Mw¼ 6.3, occurred at 3:32 a.m. in the centralvalley area of the Abruzzo region of Italy. The epicenter of the earthquake was approxi-mately 4 km south of the site of the San Salvatore Hospital, the centralized emergency
treatment facility for the region most heavily impacted by this seismic event. Some hoursfollowing the earthquake the hospital was ordered closed as a precautionary measure and
patients, including earthquake casualties, were transferred to other hospitals that were gen-erally a significant distance away. Reportedly, this is the only regional facility of this type
and size within about 50 km or more. In the following days a tent hospital was erected at the site, but its capacity and capabilities were a very small fraction of those of the closed fa-
cility. The closure of the hospital received much attention in the press (e.g., Pennella 2009),
as the campus had only been officially inaugurated in 2000 and had generally been expected to perform well in a significant seismic event.
The authors visited the subject site on 18 April 2009, 12 days after the main April 6
event. The team had access to all areas of this medium-large regional hospital, except as
specifically noted. Our guide for the visit was the on-site Engineering/Facilities Manager,whose responsibilities included the central plant and utilities throughout all of the buildings.
a) Curry Price Court, 444 Camino Del Rio S, Suite 201, San Diego, CA 92108 b) Department of Civil Protection, Via Vitorchiano 2, 00189, Rome, Italyc) Rutherford & Chekene, 55 Second Street, Suite 600, San Francisco, CA 94105
239
Earthquake Spectra, Volume 28, No. 1, pages 239–256, February 2012; VC 2012, Earthquake Engineering Research Institute

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 2/18
The authors were particularly fortunate in that this facility had been the subject of signif-
icant prior review and documentation. This provided a unique insight into the subject hospi-
tal prior to the recent seismic event. The Italian Department of Civil Protection and Applied Technology Council (ATC) of Redwood City, California, had undertaken inspections of
this specific facility in 2002 and 2003 as part of a seismic study (ATC 2000 and 2003).Approximately half of the photographed content of ATC-51-2 (ATC 2003) was based on
this specific hospital (see Figure 1), and considerable additional documentation and photo-graphs were available from that effort. The report prepared by ATC for the Department of
Civil Protection in 2003 deals with the bracing and anchorage of nonstructural components.The second author on this paper, Adriano De Sortis, participated in both the 2003 site
inspections and in the post-earthquake review of the hospital. The other authors, Marko
Schotanus and H. John Price, through their affiliations with ATC, were well-informed about
the buildings before their post-earthquake inspections. (Price, as ATC president and
Figure 1. Example page from ATC-51-2, which uses the San Salvatore Hospital as an exampleto illustrate the recommendations for bracing and anchoring nonstructural components in Italianhospitals (ATC 2003, p. 49).
PRICE, DE SORTIS, AND SCHOTANUS240

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 3/18
Schotanus through Rutherford & Chekene, who contracted with ATC for the earlier report).
The relationship between ATC and the Department of Civil Protection was fundamental to
the authors obtaining site access at an early stage.
DESCRIPTION OF THE HOSPITAL
The San Salvatore Hospital (see Figure 2) is a centralized regional emergency treatment facility with over 500 beds, serving a community of about 100,000 inhabitants in an area of
approximately 1,800 km2 (700 mi2). It is located on the outskirts of the town of Coppito, a
few kilometers from L’Aquila, the administrative center of the Abruzzo region.
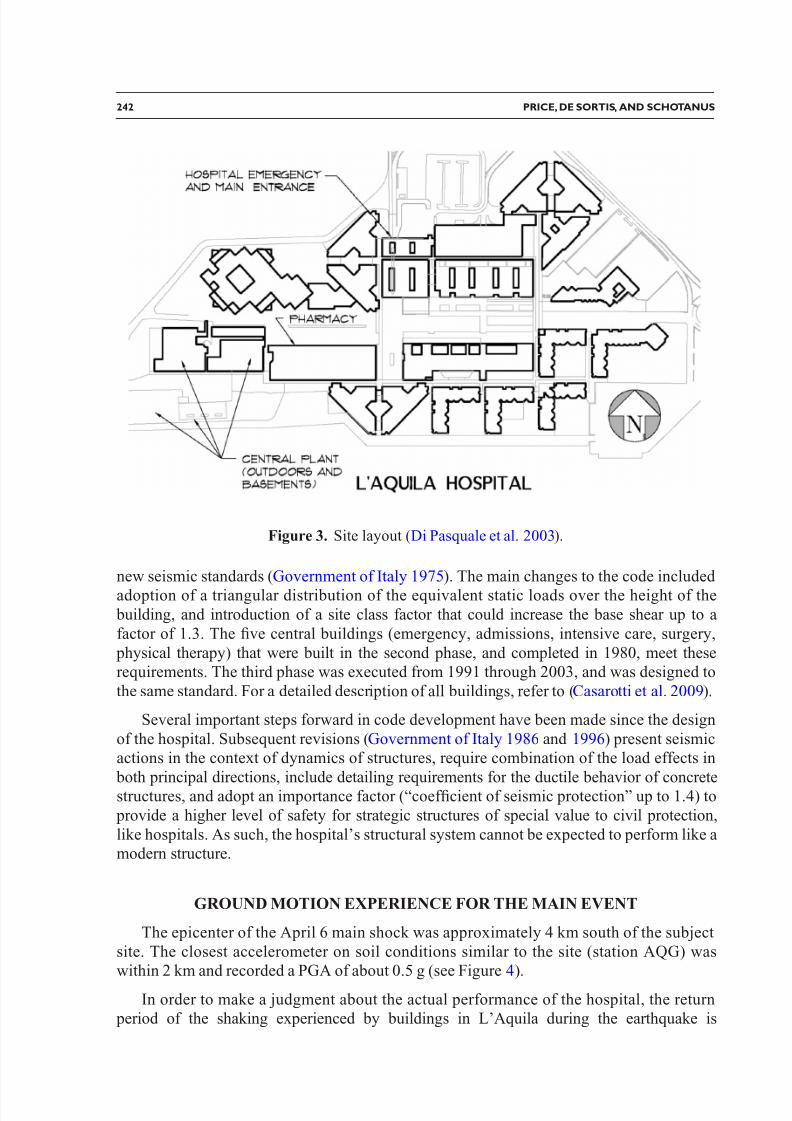
The hospital campus comprises approximately 14 buildings (see Figure 3) with separa-
tion joints between and within some of them, resulting in several more independent struc-
tural units. The structural units are three- to five-story reinforced concrete frames, with infillhollow clay block walls and brick masonry veneer exteriors, both unreinforced and not
designed as part of the structural system.
Though the hospital was officially inaugurated in 2000, the original design by Marcello
Vittorini was completed in 1967. As such, the structure was originally designed for lateralseismic forces equal to 7% of its seismic weight, the subject municipality having been clas-
sified as “intermediate” on the scale of the then three zones of Italian seismic zonation(Government of Italy 1962). In accordance with these provisions, the lateral loads were
applied statically and distributed according to the tributary mass of each level. The concrete
elements were verified using allowable stress design to resist the maximum load effects in-dependently for each direction, without special detailing requirements for ductile response.
Compared to a current building code approach, the design base shear of 0.07 g correspondsto a design ground motion of approximately 0.6 g (assuming a load reduction factor of 5,
and a conversion factor of 1.7 from allowable stress design load combinations).
The hospital campus was reportedly built in three phases between 1972 and 2003. Thefirst phase, consisting of two buildings, started construction in 1972 and was designed in
accordance with the 1962 seismic provisions. Following adoption of new seismic require-ments (Government of Italy 1974), the design was updated in 1975 in accordance with the
Figure 2. Aerial view of the campus of the San Salvatore Hospital (Di Pasquale et al. 2003).
PERFORMANCE OF THE SAN SALVATORE REGIONAL HOSPITAL IN THE 2009 L’AQUILA EARTHQUAKE 241
8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 4/18
new seismic standards (Government of Italy 1975). The main changes to the code included
adoption of a triangular distribution of the equivalent static loads over the height of the building, and introduction of a site class factor that could increase the base shear up to a
factor of 1.3. The five central buildings (emergency, admissions, intensive care, surgery,
physical therapy) that were built in the second phase, and completed in 1980, meet theserequirements. The third phase was executed from 1991 through 2003, and was designed to
the same standard. For a detailed description of all buildings, refer to (Casarotti et al. 2009).
Several important steps forward in code development have been made since the design
of the hospital. Subsequent revisions (Government of Italy 1986 and 1996) present seismicactions in the context of dynamics of structures, require combination of the load effects in
both principal directions, include detailing requirements for the ductile behavior of concretestructures, and adopt an importance factor (“coefficient of seismic protection” up to 1.4) to
provide a higher level of safety for strategic structures of special value to civil protection,
like hospitals. As such, the hospital’s structural system cannot be expected to perform like amodern structure.
GROUND MOTION EXPERIENCE FOR THE MAIN EVENT
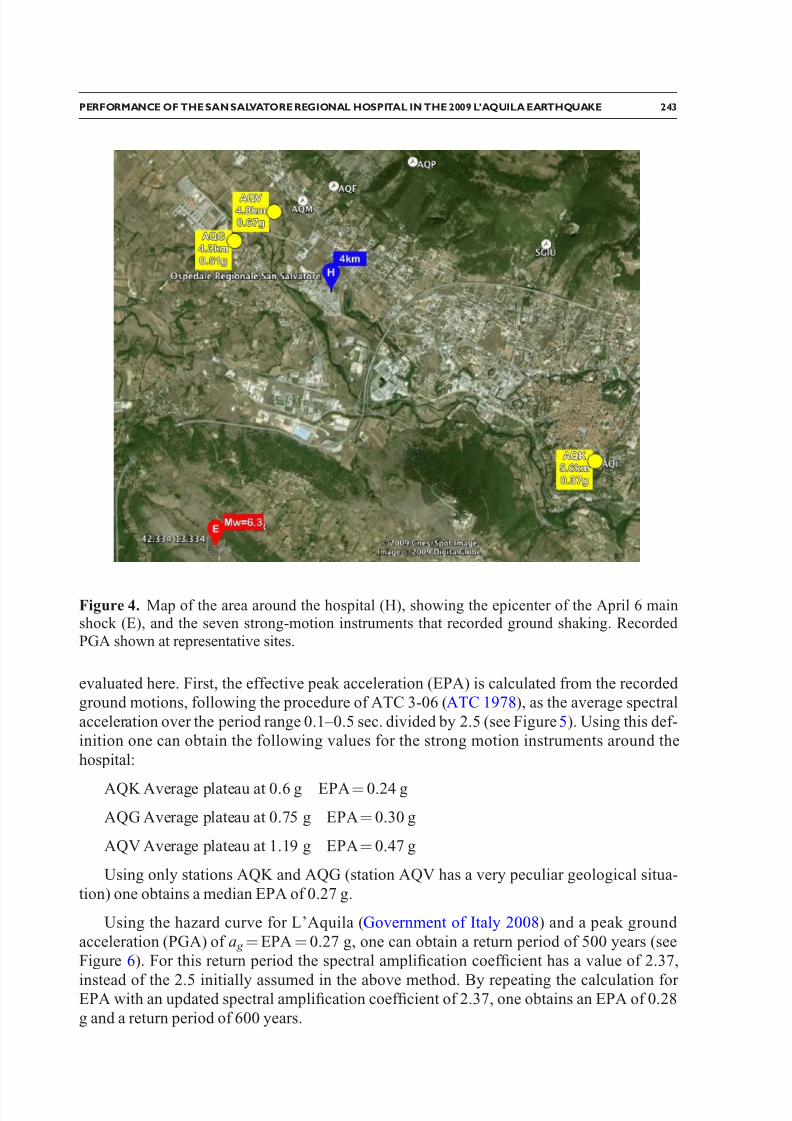
The epicenter of the April 6 main shock was approximately 4 km south of the subject
site. The closest accelerometer on soil conditions similar to the site (station AQG) waswithin 2 km and recorded a PGA of about 0.5 g (see Figure 4).
In order to make a judgment about the actual performance of the hospital, the return period of the shaking experienced by buildings in L’Aquila during the earthquake is
Figure 3. Site layout (Di Pasquale et al. 2003).
PRICE, DE SORTIS, AND SCHOTANUS242
8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 5/18
evaluated here. First, the effective peak acceleration (EPA) is calculated from the recorded ground motions, following the procedure of ATC 3-06 (ATC 1978), as the average spectral
acceleration over the period range 0.1–0.5 sec. divided by 2.5 (see Figure 5). Using this def-inition one can obtain the following values for the strong motion instruments around the
hospital:
AQK Average plateau at 0.6 g EPA¼ 0.24 g
AQG Average plateau at 0.75 g EPA¼ 0.30 g
AQV Average plateau at 1.19 g EPA¼ 0.47 g
Using only stations AQK and AQG (station AQV has a very peculiar geological situa-
tion) one obtains a median EPA of 0.27 g.
Using the hazard curve for L’Aquila (Government of Italy 2008) and a peak ground
acceleration (PGA) of a g ¼EPA¼ 0.27 g, one can obtain a return period of 500 years (seeFigure 6). For this return period the spectral amplification coefficient has a value of 2.37,
instead of the 2.5 initially assumed in the above method. By repeating the calculation for EPA with an updated spectral amplification coefficient of 2.37, one obtains an EPA of 0.28
g and a return period of 600 years.
Figure 4. Map of the area around the hospital (H), showing the epicenter of the April 6 mainshock (E), and the seven strong-motion instruments that recorded ground shaking. Recorded PGA shown at representative sites.
PERFORMANCE OF THE SAN SALVATORE REGIONAL HOSPITAL IN THE 2009 L’AQUILA EARTHQUAKE 243

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 6/18
Six hundred years exceeds the 475-year return period traditionally used for design in building standards. The measured seismic shaking (plateau of the calculated effective
ground motion spectrum in the range of 0.6 to 0.75 g) corroborates that the original designground motion (elastic spectral ordinate equal to 0.6 g, as discussed above) was likely
exceeded.
PERFORMANCE OF THE HOSPITAL
On-site staff (including the facility management staff members Mauro Tursini and
Fabrizio Andreassi) reported that no deaths or injuries occurred at the hospital as a result of
the earthquake shaking. The earthquake occurred at approximately 3:30 a.m. local time, soit can be presumed that very few people were in or immediately outside of the various build-
ings and that a normal nightshift scenario was in progress. The shaking caused most hospi-tal central utility supplies to switch over to their on-site emergency backup systems. This
occurred successfully within the planned operational standards. The hospital continued tooperate for several hours (with some, but not all, operating rooms) after the initial seismic
event and to accept casualties brought in during the initial hours, even though processing of
the new emergency admissions was hindered by masonry debris that had fallen from the building above the access portico of the emergency and main entrance (see Figure 7).
A safety evaluation in the early morning identified significant structural damage.
Though sufficient enough to warrant shoring and/or permanent remediation, only portionsof three buildings were noted to be affected, as described in the following section. Nonethe-less, all buildings on the hospital campus were closed as a precautionary measure. Patients,
Figure 5. Response spectra for recorded ground motions at stations AQK, AQG, and AQV,and calculated effective ground motion spectrum.
PRICE, DE SORTIS, AND SCHOTANUS244

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 7/18
including new admissions, were transferred to other hospitals. Within 12 hours of this deci-
sion, a field hospital was erected at the site, but its capacity and capabilities were only afraction of those of the closed facility.
The evacuated hospital remained fully closed until the end of May 2009, when the first
departments where reopened. By the end of July, all departments moved back into the reop-ened hospital buildings, though occupying only a limited portion of the total space. Most
pre-earthquake services were resumed at this time, including outpatient treatment.
The hospital received a e47 million insurance payout, part of which has been assigned
to repair and retrofit of the structure.
PERFORMANCE OF THE STRUCTURAL SYSTEM
Generally, the concrete framing of the hospital buildings performed adequately,especially if one compares the ground motion intensity to the design loads, with significant
damage limited to isolated columns in three structural units on the campus.
Several lower-level columns (four to eight in total) comprising the entry portico of the main entrance and emergency entrance (see Figure 3) suffered partial failure without collapse or noticeable deflection at the tops of these frame elements. The concrete cover at
Figure 6. Hazard curves and short-period spectral amplification coefficient for L’Aquila, based on Government of Italy (2008).
PERFORMANCE OF THE SAN SALVATORE REGIONAL HOSPITAL IN THE 2009 L’AQUILA EARTHQUAKE 245

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 8/18
these locations spalled, the inner concrete core of the column appeared to have a slight
offset, and the vertical reinforcement was exposed and buckled (see Figure 8). Column tiereinforcement was not observed and appears to be either very widely spaced or to have
been omitted, at least at these locations. Our reviews to date indicate that, at least, a level of column tie reinforcement consistent with the 1967 design of the hospital had been intended.
The reconnaissance team could not approach closer than about 10 feet (or stop for a close
Figure 7. Location of collapsed masonry infill and veneer from above the entrance portico (thedebris had been cleared away at the time of visit).
Figure 8. Column damage at the main entrance of the structure (see Figures 3 and 7 for location).
PRICE, DE SORTIS, AND SCHOTANUS246

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 9/18
detailed observation) as the area had been designated as a crime scene by the relevant
branch of the police force. The portico could be considered something of a soft-story condi-
tion, as the levels above it had significant infill masonry.
A series of lower-level columns in a second building containing the pharmacy (seeFigure 3) suffered damage typical of short-column behavior. Approximately six columns
were thus affected, but even in the worst case a considerable vertical load capacity remained
after the earthquake. The concrete cover spalled off, exposing the tie reinforcement, and inthe worst cases there was some cracking to the core concrete. No collapse or noticeable
deflection had occurred. The short-column condition arose because of infill masonry between the columns, capped by a rigid precast concrete wall cap. Due to the secured nature
of the pharmacy, interior access to view this damage was not possible, but interior photoshave been provided by Mauro Tursini (see Figure 9).
Finally, poor structural detailing of certain seismic joints led to local damage at one
column supporting the elevated corridor structure that connects the buildings on the hospitalcampus. Frequently, seismic separations were not achieved by bringing separate-
but-adjacent vertical members up from a common footing, but rather, by having adjacent
upper-level portions of the building supported on a common wall or a common column. Inthe case of one narrow column this caused local damage to the column and a loss of bearing
(see Figure 10).
Elsewhere, the structural joint detailing made use of half-joints in beams and slabs,
similar to those often used in bridge construction (see Figure 13). These types of joints per-
formed erratically and generally lacked adequate joint seating material. Bridge construction, by comparison, typically has sophisticated and expensive bridge bearings at such joints.
Figure 9. (a) Short column damage at the first floor pharmacy. The operating rooms above had been taken out of service, and (b) damage to a column in the pharmacy due to a short-columneffect caused by infill masonry (Photos courtesy of Mauro Tursini, 2009).
PERFORMANCE OF THE SAN SALVATORE REGIONAL HOSPITAL IN THE 2009 L’AQUILA EARTHQUAKE 247

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 10/18
At the level of seismic shaking experienced by the hospital structure, it seems reasona-
ble to conclude that the primary lateral resistance was provided by unreinforced hollow clay
tile infill masonry. The majority of this infill was generally undamaged (though some had minor cracking). The concrete frame did not perform well in the locations where it, rather
than the infill, resisted the lateral load (see above). It would seem that structural damage to
the concrete columns was the primary reason for the closure of the hospital, rather than non-structural damage (see sections below).
PERFORMANCE OF NONSTRUCTURAL COMPONENTS
It was generally observed that from a seismic engineering point of view, the joints
between adjacent buildings and structural units were poorly detailed and constructed. Some
joints were likely intended to only be expansion/contraction joints, and even as such could have been better configured (see Figures 11, 12 and 13). Because of this style of detailing,
and because the joint width (capacity) of the exterior brick veneer and the interior hollowclay tile infill and plaster was generally less than that between the concrete structural ele-
ments, there was localized damage to the exterior veneer and interior infill and plaster,including local collapse of some exterior veneer. In one instance, a 30 to 50 mm-thick layer
of plaster over a seismic separation joint at one end of a stairway created both a falling and
tripping hazard. To the extent that pounding occurred, adjacent floors and the roof wereconstructed at the same elevation.
As noted above, the major nonstructural issues were related to the exterior masonry
veneer. This unreinforced veneer was often poorly detailed at movement joints. The ties between the exterior veneer and the interior infill and concrete frame elements were widelyspaced. Nevertheless, only a few panels of veneer were dislodged and fell outward. In these
Figure 10. Damage to a separation joint that occurred over a shared column.
PRICE, DE SORTIS, AND SCHOTANUS248

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 11/18
instances, it appeared that only a limited number of ties had been used between the exterior
veneer and interior infill. Other than over the emergency entry roadway (see Figure 7), these
local collapses generally occurred in exterior zones of the facility with little traffic below
them. Had the seismic event occurred during a time of the day when the facility was at maximum occupancy, injuries and fatalities may well have occurred.
Most areas of the hospital had a metal ceiling system and fallen sections were veryinfrequent, with none in hallways or treatment rooms (see Figure 14a). The ceiling was
distorted in limited areas. This ceiling system performed very well.
There was very little damage to interior building finish elements. One section of
suspended fluorescent lights was dislodged (see Figure 14b). Based on the widespread
Figure 11. (a) Damage to interior partition walls, and (b) localized damage to infill walls adja-cent to a separation joint.
Figure 12. (a) Veneer dislodged by pounding at joints, and (b) interior falling hazard (plaster over seismic joint).
PERFORMANCE OF THE SAN SALVATORE REGIONAL HOSPITAL IN THE 2009 L’AQUILA EARTHQUAKE 249

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 12/18
observation of little (often no) movement of shelf and desk contents within the buildings, it
seems reasonable to describe local shaking as moderate, rather than severe.
Medical equipment in the hospital generally escaped damage, even though much of it
was unsecured on shelves, stands, and operating room trolleys (see Figure 15). No overhead
mounted equipment appeared to have fallen (see Figure 16a). Major imaging and operatingequipment typically comes from manufacturers with substantial standard anchorage require-ments. All of this equipment anchorage performed well and most such equipment was still
operational. On-site medical staff reported that certain calibration-sensitive classes of equip-ment would likely require significant recalibration or adjustment before it could be recom-
missioned (MRI, focused radiation therapy equipment, etc; see Figure 16b). In general, a
Figure 14. (a) Isolated ceiling damage, shelf and desk contents still in place, and (b) one sectionof suspended fluorescent lights dislodged.
Figure 13. (a) Building half-joint at stairwell, plaster over seismic joint dislodged, and (b) ma-sonry veneer collapse adjacent to seismic half-joint due to inadequate separation. Note also thelimited veneer ties to interior infill.
PRICE, DE SORTIS, AND SCHOTANUS250

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 13/18
majority of the medical equipment on trolleys and shelves is typically unrestrained in hospi-tals, and work processes seem to require this to be the case. Nevertheless, such trolley tops
and all shelves could readily have a 15 to 25 mm lip or offset buffers that would aid restraint, and certain trolleys that require signing out for use could have a home station
tether system.
The central plant and building utility provision of the hospital typically performed to thedesired standard. Emergency systems kicked in with flawless operation. Since beinginspected by ATC in 2003, several components of this plant had been adequately retrofitted
and restrained. This effort appeared to have been performed by the on-site facility manager
on an ad-hoc basis, rather than a systemic requirement from administration. Most of the
heavier components at risk of overturning had been restrained (see Figure 17b). Several
Figure 15. (a) Operating room and unsecured equipment, little of which damage and (b) operat-ing room recovery area, one out of eight stations had equipment fall.
Figure 16. (a) Overhead mounted equipment in good condition, and (b) imaging equipment adequately restrained, but may have interior calibration issues.
PERFORMANCE OF THE SAN SALVATORE REGIONAL HOSPITAL IN THE 2009 L’AQUILA EARTHQUAKE 251

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 14/18
lighter components in the cooling tower yard had not been anchored, and were slightly dis-
placed but still operational (see Figure 17c). At the level of shaking experienced, the
attached utility pipes provided the needed restraint without failure, but this may not beappropriate at high levels of shaking.
In the backup medical nitrogen facility, about 60% of the heavy nitrogen bottles wererestrained at the time of the earthquake (see Figure 17a). The balance of these cylinders fell
and rolled about, most fortunately missing the glass-fronted control system of this needed medical gas. This situation indicates just how difficult a housekeeping task it is to have all
potential missiles restrained at all times. The on-site facilities staff obviously understood theseismic risk and generally did very well in limiting exposure.
Reportedly, all elevators were still fully operational after the shaking and were onlytaken out of service when the facility was closed.
DISCUSSION AND CONCLUSIONS
San Salvatore Hospital was considered an essential facility and, as such, was expected by many to be functional after a significant seismic event such as the one that occurred on 6
April 2009.
CONCLUSIONS AND QUESTIONS THAT COULD APPLY TO HOSPITALS
GENERALLY, NOT JUST THIS FACILITY
Decisions to close part or all of an essential facility such as a hospital can be easily
made in the heat of the moment after an earthquake. Sometimes such decisions may be based on local political factors (not least of all, the appearance of doing something quickly
to protect safety) and may be made without appropriate technical and professional input regarding realistic safety concerns. Decisions to re-open portions of such a facility are far
more complex and raise a large number of operational issues that are not likely routinewithin the hospital’s operation.
The U.S.-Italy collaborative program reports (ATC 2000, 2002, 2003) contain acomprehensive set of recommended practices to help hospital operators improve the seismic
Figure 17. (a) Loose gas cylinders, (b) retrofit of tall elevated tank since 2003, and (c) unse-cured lightweight equipment displaced but operational.
PRICE, DE SORTIS, AND SCHOTANUS252

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 15/18
safety of their facilities and prepare for a seismic event. The on-site, case-specific experi-
ence at the San Salvatore Hospital confirmed the validity of these recommendations, which
include, among other items:
1. Seismic vulnerability assessments of structural and nonstructural components;
2. Mitigation of hazards and reorganization of health functions;
3. Development of post-earthquake inspection procedure and preparation, and;
4. Training.
While the general topic of seismic vulnerability assessments (the first recommendationabove) has been advanced in both the United States and in Italy, no site-specific building-
specific assessments of this hospital campus were reported to have been performed before
the earthquake besides the inspections that occurred within the scope of the U.S.-Italycollaborative project. As insights into potential vulnerabilities continuously change with the
advancement of research and through lessons learned from earthquake occurrences, hospitaloperators should reassess the need for the reevaluation of their buildings on a regular basis.
Regarding the second recommendation, specific on-site mitigation of hazards appeared to be limited to nonstructural items, as described earlier in this paper, rather than to the
structures themselves. The post-event reorganization of health functions was well planned and well executed, although in a rapidly deployed tent hospital format.
At a national level, the development of Italian post-earthquake inspection procedures is
well advanced. The initial screening process strikes a somewhat different balance from cur-rent U.S. practice in the offset between speed and scope. The somewhat more comprehen-
sive Italian inspection and documentation process necessarily makes the process less rapid.However, at the local level (hospital campus specific), preparation for post-earthquake
inspections is much less structured. The experience in L’Aquila confirms that a documented
pre-established program for post-event safety inspections (structural and nonstructural com- ponents), as well as training in its implementation for both on-site and backup personnel
(ATC 2002), is vital to the continued operation of any essential facility. The program should include options to allow the continued operation of undamaged portions of a facility while
restricting access to damaged portions. Duplicate off-site copies of this documentation need
to be maintained. The authors would refer readers to the comprehensive treatment of thesubject matter in those reports. Though oftentimes a centralized agency will be in charge of
post-earthquake inspections, hospital operators may wish to develop programs for private
inspection of their buildings to permit rapid, individualized emergency response that isfocused on reoccupation and resumption of operations as soon as it is safely possible. In
addition to the ATC documents, San Francisco’s Building Occupancy Resumption Program(BORP) provides valuable guidance (City and County of San Francisco 2006).
Community expectations need to be appropriately managed both before and after anearthquake event, especially regarding the serviceability and continued operation of an
essential facility. There needs to be an understanding that some damage at the facility is to
be expected and is normal. It is noted that even though the current Italian seismic code con-tains requirements for the operational continuity of hospitals, the design-level ground shak-
ing for that particular limit state has a return period of less than 100 years (a level of shaking
PERFORMANCE OF THE SAN SALVATORE REGIONAL HOSPITAL IN THE 2009 L’AQUILA EARTHQUAKE 253

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 16/18
lower that that experienced in this event). Thus operational continuity after a rare event is
not a strict design requirement for new hospitals. While many people may expect continued
post-event operation, that goal may not actually be fully achieved and some disruption is to be expected. Plans need to exist to manage housekeeping disruptions (local dust, debris,
fallen contents, etc). The existence and implementation of the post-event safety inspectionsis an integral part of this management of expectations. Management of realistic expectations
is also vital to the continued operation of an essential facility.
CONCLUSIONS THAT MAY BE SPECIFIC TO THIS HOSPITAL, BUT ALSO
AFFECT OTHERS
Considerations of the ease and reliability of the needed post-event structural inspectionswill be a factor. Fortunately the L’Aquila hospital’s reinforced concrete (and infill masonry)structural system was highly exposed and readily inspected—this was largely a reliable
rapid visual inspection, at that.
By contrast, inspections of structural joints in a multistory steel-frame building would
not be easily accomplished, given the fireproofing and ceiling systems that would impact visual access to the critical areas. Further visual inspection, even if the steel were exposed,
would not be rapid, and visual methods might not be appropriate or sufficiently accurate.
Access routes to and around hospitals and other essential facilities require special atten-
tion, and perhaps even upgraded design standards. Aside from structural design to ensurecontinued access to the facility, this topic would also benefit from some basic planning
issues. For example, why run the major access route to the facility under or through another building, especially where it may create a potential soft-story hazard? Likewise, access
routes within the facility require both planning and structural design attention.
Aside from limited and localized structural damage to portions of three buildings, the
most noticeable systemic problem at this facility relates to its seismic separation joints,which did not perform adequately, most noticeably affecting the exterior and interior
finishes and the inadequately anchored exterior veneer. Local exterior veneer collapses
were the result of inadequate anchorage of the veneer and pounding of the veneer across
seismic movement joints (as a result of the poor detailing of those joints).Utility systems performed well and backup emergency utility systems operated as
planned. With appropriate implementation, current seismic design technologies and under-standing appear to be adequate to accomplish the continued performance of utility systems
after an event with levels of shaking like this one.
Closing a large regional hospital for any reason has significant impacts. Geographic
diversity among hospital facilities would provide some diversification of risk, includingseismic risk.
Based on the level of contents displacement within the facility, which would be
described as slight-to-moderate, it may be that an appropriate description of the seismicshaking experienced by the facility is significant, but nevertheless moderate. More intenseshaking seems possible and should be considered when reviewing our observations reported
PRICE, DE SORTIS, AND SCHOTANUS254

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 17/18
in this paper. The fundamental question remains: What would the performance be at more
intense levels of seismic shaking?
ACKOWLEDGEMENTS
Special thanks are due to on-site facility management staff Mauro Tursini and Fabrizio
Andreassi for giving the authors a tour through the relevant areas of the facility, and for pro-viding valuable information on building history and post-earthquake performance. David
Alexander (CESPRO, University of Florence), Mersedeh Jorjani (historic preservationresearcher), Khalid Mosalam (University of California, Berkeley), and Fausto Marincioni
(Marche Polytechnic University) were part of the team visiting the hospital, and the authors
are grateful for their input and discussion. The authors thank Bill Holmes, Susan Tubessing,
and Marjorie Green for including them in the EERI reconnaissance team. Funding from
the U.S. National Science Foundation, under contract #CMMI-0758529, is gratefullyacknowledged.
REFERENCES
Applied Technology Council (ATC), 1978. Tentative Provisions for the Development of Seismic
Regulations for Buildings, Tech. Rep. ATC 3-06 , Redwood City, CA.
Applied Technology Council (ATC), 2000. U.S.-Italy Collaborative Recommendations for
Improved Seismic Safety of Hospitals in Italy, Tech. Rep. ATC-51, Redwood City, CA.
Applied Technology Council (ATC), 2002. Recommended U.S.-Italy Collaborative Procedures
for Earthquake Emergency Response Planning for Hospitals in Italy, Tech. Rep. ATC-51-1,Redwood City, CA.
Applied Technology Council (ATC), 2003. Recommended U.S.-Italy Collaborative Guidelines
for Bracing and Anchoring Nonstructural Components in Italian Hospitals, Tech. Rep. ATC-51-2, Redwood City, CA.
City and County of San Francisco, 2006. Emergency Operations Plan: Building Occupancy
Resumption Program (BORP), Department of Building Inspection, San Francisco, CA,http://www.sfdbi.org=index.aspx?page=60.
Casarotti, C., Pavese, A., and Peloso, S., 2009. 2.8 Seismic response of the San Salvatore Hospi-tal of Coppito (L’Aquila) during the earthquake of April 6 th 2009, Progettazione Sismica 3
159–172.
Di Pasquale, G., Bearzi, V., De Sortis, A., Gatti, F., and Martini A, 2003. ATC-51-2 Project Support Documents, revised 5 June 2003, Applied Technologies Council (ATC), Redwood City, CA.
Government of Italy, 1962. Provvedimenti per l’edilizia con particolari prescrizioni per le zonesismiche, Law No. 1684, Gazzetta Ufficiale della Repubblica Italiana No. 326 , Rome.
Government of Italy, 1974. Provvedimenti per le costruzioni con particolari prescrizioni per lezone sismiche, Law No. 64, Gazzetta Ufficiale della Repubblica Italiana No.76 , Rome.
Government of Italy, 1975. Disposizioni concernenti l’applicazione delle norme tecniche per lecostruzioni in zone sismiche, Decree of the Ministry of Public Works No. 40, Gazzetta Uffi-
ciale della Repubblica Italiana No. 93, Rome.
Government of Italy, 1986. Norme tecniche relative alle costruzioni antisismiche, Decree of theMinistry of Public Works, 24 January 1986, Gazzetta Ufficiale della Repubblica Italiana No.
108, Rome.
PERFORMANCE OF THE SAN SALVATORE REGIONAL HOSPITAL IN THE 2009 L’AQUILA EARTHQUAKE 255

8/10/2019 Performance Salvatore Hospital 2009 LAquila EQ
http://slidepdf.com/reader/full/performance-salvatore-hospital-2009-laquila-eq 18/18
Government of Italy, 1996. Norme tecniche per zona sismica, Decree of the Ministry of PublicWorks, 16 January 1996, Gazzetta Ufficiale della Repubblica Italiana No. 29, Rome.
Government of Italy, 2008. Approvazione delle nuove norme tecniche per le costruzioni, Decreeof the Ministry of Public Works, 14 January 2008, Gazzetta Ufficiale della Repubblica Ital-
iana N.29, Rome.
Pennella, P., 2009. Il nuovo ospedale nato gia vecchio, Il Tempo, 9 April 2009.
(Received 16 December 2009; accepted 8 April 2011)
PRICE, DE SORTIS, AND SCHOTANUS256