periodontal indices final
TRANSCRIPT

1
GOOD MORNING
2
PERIODONTAL INDICES
SUBMITTED BY: SHEKHAR KUMAR MANDAL Roll no: 26 BDS IV
GUIDED BY: DR. NAVRAJ LAMDARI
DR. LAL BABU KAMAIT DEPARTMENT OF PERIODONTICS COLLEGE OF MEDICAL SCIENCES, BHARATPUR NEPAL

3
CONTENTS
REFERENCESCONCLUSIONRECENT ADVANCES IN PERIODONTAL INDICESGINGIVAL AND PERIODONTAL DISEASE INDICESORAL HYGIENE AND PLAQUE INDEXOBJECTIVES AND USES OF INDEXIDEAL REQUISITES OF AN INDEXCLASSIFICATION OF INDEXDEFINITIONSINTRODUCTION

4
INTRODUCTION
“UNLESS YOU CAN COUNT IT, WEIGH IT OR EXPRESS IT IN A QUANTITATIVE FASHION, YOU HAVE
SCARCELY BEGUN TO THINK ABOUT THE DISEASE IN A SCIENTIFIC FASHION”
-LORD KELVIN

5
DEFINITIONS
• “Epidemiological indices are attempts to quantitate clinical condition on
graduated scale, thereby facilitating comparison among populations examined
by the same criteria and methods”. – Irving Glickman
According to Russell A.L , an index is defined as ‘A numerical value describing the relative status of the population on a graduated scale with definite upper and lower limits which is designed to permit and facilitate comparison with other population classified with the same criteria and the method”

6
“An index is an expression of clinical observation in numeric values. It is used to
describe the status of the individual or group with respect to a condition being
measured. The use of numeric scale and a standardized method for interpreting
observations of a condition results in an index score that is more consistent and
less subjective than a word description of that condition”. – Esther M Wilkins

7
IDEAL REQUISITES OF AN INDEX
IDEAL REQUISITES OF INDEX
CLARITY SIMPLICITY
OBJECTIVITY
VALIDITYRELIABILI
TYSENSITIVI
TY
ACCEPTABILITY
QUANTIFIABILITY
SPECIFICITY

8
OBJECTIVES
FOR INDIVIDUAL PATIENT
• Recognize an oral problem
• Effectiveness of present oral
hygiene practices
• Motivation in preventive and
professional care for control
and elimination of diseases
IN RESEARCH
• Determine base line data before
experimental factors are
introduced
• Measure the effectiveness of
specific agents for prevention
control or treatment of oral
condition
IN COMMUNITY
• Shows prevalence and incidence
of a condition
• Assess the need of the
community
• Compare the effects of a
community program and evaluate
the results

9
Based on the direction in which their scores can fluctuate:
• Measures condition that can be changed e.g. periodontal index
Reversible index:
• Measures conditions that will not change e.g. dental caries
Irreversible index:
CLASSIFICATION OF INDEX

10
•Depending upon the extent to which areas of oral cavity are measured :
Full mouth indices:
•Patient’s entire periodontium or dentition is measured. •e.g. OHI
Simplified indices:
•Measure only a representative sample of the dental apparatus.•e.g. OHI-S

11
According to the entity which they measure
• “d” decay portion of the dmf index is the best example of disease index
Disease index :
• Measuring gingival or sulcular bleeding are essentially examples of symptom indices
Symptom index :
•“f” filled portion of dmft index is the best example for treatment index
Treatment index :

12
General indices :
•index that measures the presence or absence of a condition. e.g. plaque index
Simple index:
•index that measures all the evidence of a condition, past and present. e.g. dmf index
Cumulative index:

13
INDICES USED FOR ORAL HYGIENE ASSESSMENT
• Oral hygiene index
• Simplified oral hygiene index
• Patient hygiene performance
• Turesky, Gilmore, Glickman modification of the Quigley Hein plaque index

14
ORAL HYGIENE INDEX (OHI)
• Developed in 1960 by John C. Green and Jack R. Vermillion in order to classify
and assess oral hygiene status.
• Simple and sensitive method for assessing group or individual oral hygiene
quantitatively.
• Composed of 2 components:
• Debris index (DI)
• Calculus index (CI)

15
RULES OF ORAL HYGIENE INDEX
1 Only fully erupted permanent teeth are scored.
2 Third molars and incompletely erupted teeth are not scored because of the wide variations in heights of clinical crowns.
3 The buccal and lingual debris scores are both taken on the tooth in a segment having the greatest surface area covered by debris.
4 The buccal and lingual calculus scores are both taken on the tooth in a segment having the greatest surface area covered by supragingival and subgingival calculus.

0 – No debris or stain present1 – Soft debris covering not more than 1/3rd the tooth surface, or presence of extrinsic stains without other debris regardlessof the area covered
2 – Soft debris covering more than 1/3rd, but not more than 2/3rd,of the exposed tooth surface
3 – Soft debris covering more than 2/3rd of the exposed tooth surface
DEBRIS INDEX CRITERIA

17
SCORE CRITERIA0 No calculus present
1 Supragingival calculus covering not more than 1/3 of the exposed tooth surface
2 Supragingival calculus covering more than 1/3 but not more than 2/3 the exposed tooth surface or presence of individual flecks of subgingival calculus around the cervical portion of the tooth or both.
3 Supragingival calculus covering more than 2/3 the exposed tooth surface or a continuous heavy band of subgingival calculus around the cervical portion of tooth or both.Supragingival
calculusSubgingival
calculus
CALCULUS INDEX CRITERIA

18
CALCULATION• Debris Index (DI) =( Buccal Score+ Lingual Score) / NO. OF SEG
• Calculus Index (CI) =( Buccal Score+ Lingual Score) / NO. OF SEG
• Oral Hygiene Index= DI+CI
• DI and CI range from 0-6
• Maximum score for all segments can be 36 for debris or calculus
• OHI range from 0-12
• Higher the OHI, poorer is the oral hygiene of patient

19
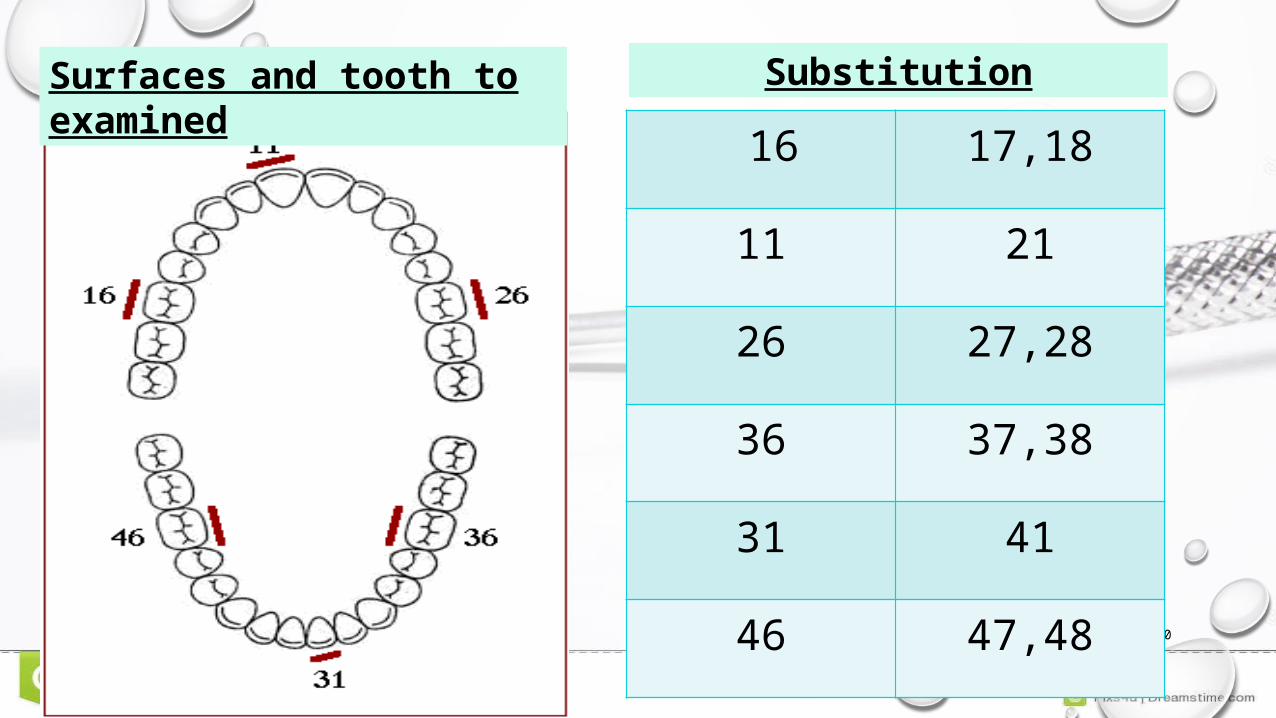
SIMPLIFIED ORAL HYGIENE INDEX• Developed by John C Greene and Jack R Vermillion in 1964 as OHI was time
consuming and required more decision making
• Only fully erupted permanent teeth are scored
• Natural teeth with full crown restorations and surfaces reduced in height by caries or trauma are not scored
• An alternate tooth is then examined if missing
20
16 17,18
11 21
26 27,28
36 37,38
31 41
46 47,48
Surfaces and tooth to examined
Substitution

21
DI –S and CI-S• Good -0.0-0.6• Fair – 0.7-1.8• Poor – 1.9 -3.0
OHI –S•Good - 0.0-1.2•Fair – 1.3- 3.0•Poor – 3.0 -6.0
INTERPRETATIONCALCULATION• DI –S = Total score/No of
surfaces
• CI-S = Total score/ No of surfaces
• OHI -S= DI-S+ CI-S

USES• Widely used in epidemiological studies of periodontal diseases.
• Useful in evaluation of dental health education programs
• Evaluating the efficacy of tooth brushes.
• Evaluate an individual’s level of oral cleanliness.
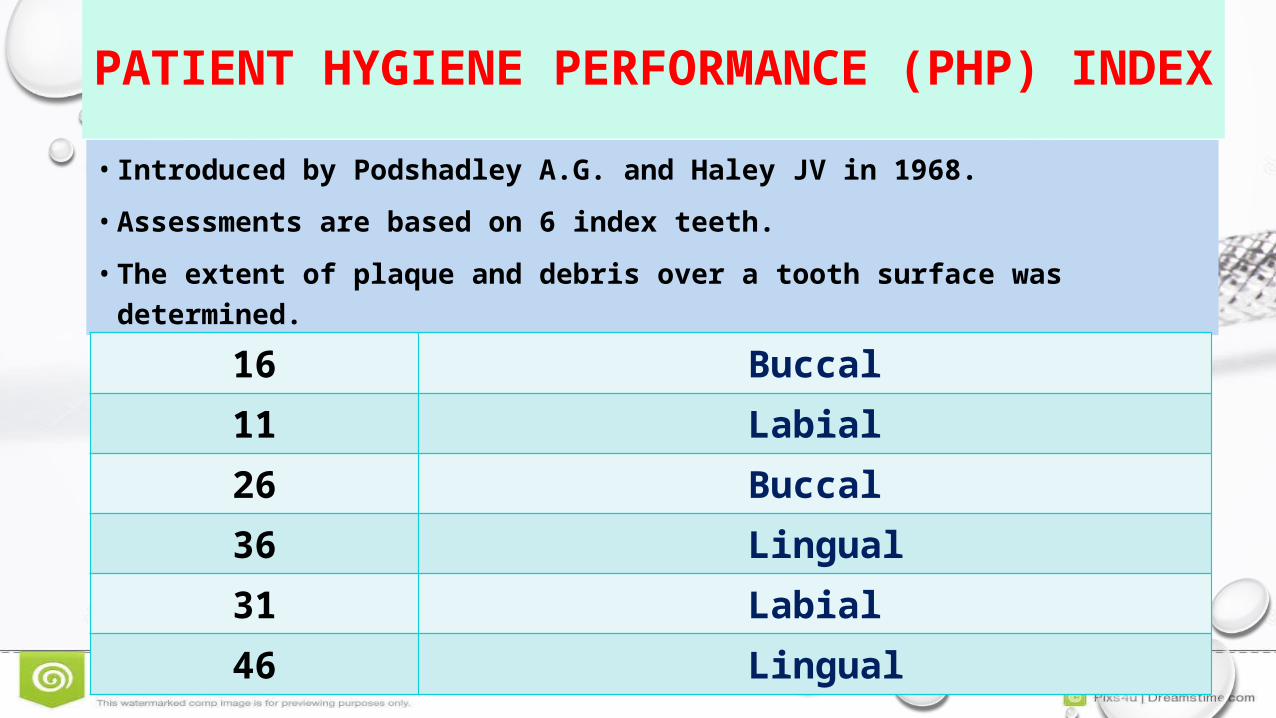
PATIENT HYGIENE PERFORMANCE (PHP) INDEX
• Introduced by Podshadley A.G. and Haley JV in 1968.
• Assessments are based on 6 index teeth.
• The extent of plaque and debris over a tooth surface was determined.
23
16 Buccal11 Labial26 Buccal36 Lingual31 Labial46 Lingual
24
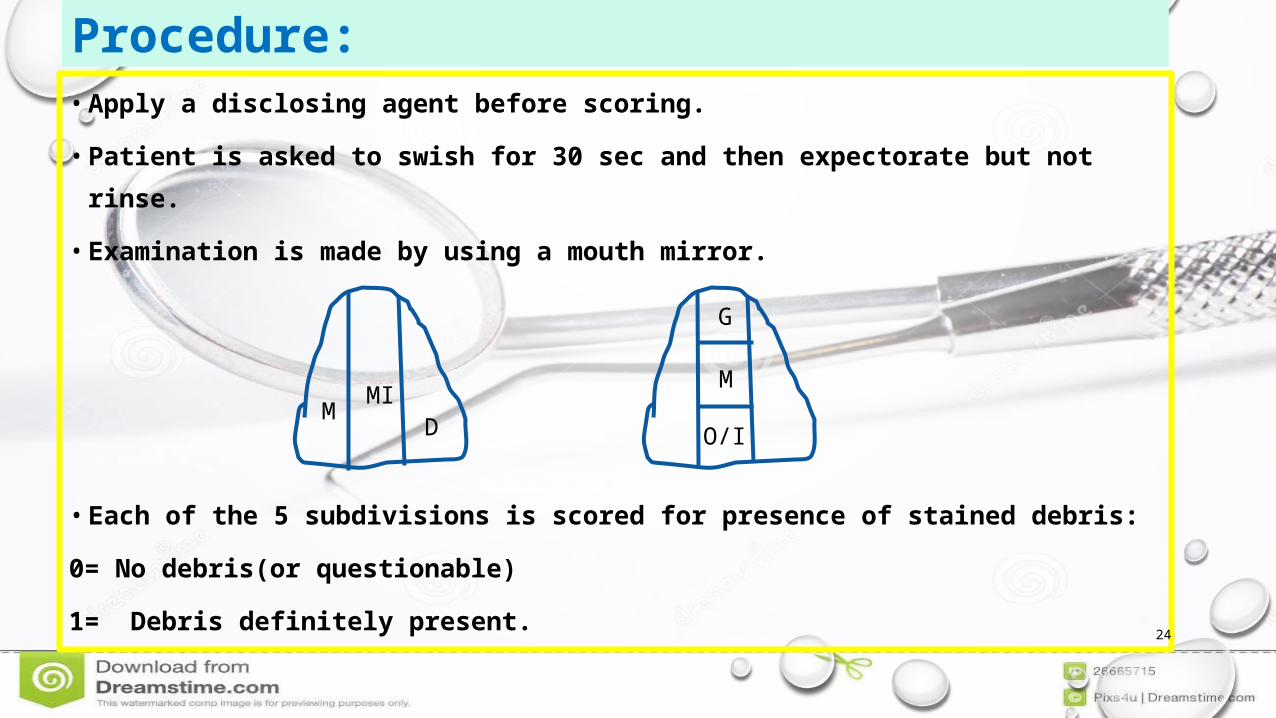
• Apply a disclosing agent before scoring.
• Patient is asked to swish for 30 sec and then expectorate but not rinse.
• Examination is made by using a mouth mirror.
• Each of the 5 subdivisions is scored for presence of stained debris:
0= No debris(or questionable)
1= Debris definitely present.
M MID
M
O/I
G
Procedure:

• Debris score for individual tooth:
• Add the scores for each of the 5 subdivisions.
• PHP index for an individual= (Total score for all the teeth /the number of teeth examined)
Debris score for 1 tooth = 4/5 = 0.8
1
1
1 1
0
Rating scoresExcellent : 0 (no debris)Good : 0.1-1.7Fair : 1.8 – 3.4Poor : 3.5 – 5.0

PLAQUE INDEX
• Silness and Loe in 1964
• Assesses only thickness of plaque at the cervical
margin of the tooth closest to the gums
• All four surfaces are examined
• Distal
• Mesial
• Lingual
• Buccal
12
2416
44
32
36

27
SCORING CRITERIAScore Criteria
0 No Plaque
1
A film of plaque adhering to the free gingival margin and adjacent area of tooth the plaque may be seen in situ only after application of disclosing solution or by using probe on tooth surface
2Moderate accumulation of soft deposits within the gingival pocket, or the tooth and gingival margin which can be seen with the naked eye
3Abundance of soft matter within the gingival pocket and/or on the tooth and gingival margin
28
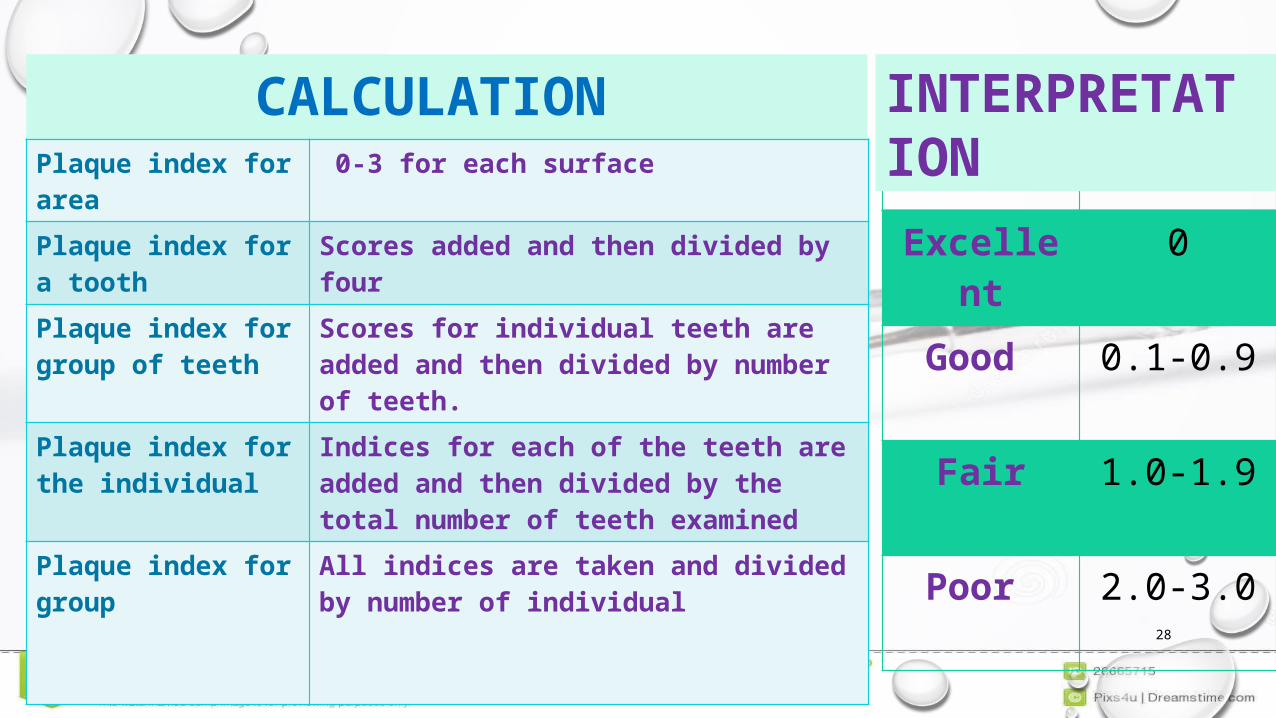
CALCULATION Plaque index for area 0-3 for each surface
Plaque index for a tooth
Scores added and then divided by four
Plaque index for group of teeth
Scores for individual teeth are added and then divided by number of teeth.
Plaque index for the individual
Indices for each of the teeth are added and then divided by the total number of teeth examined
Plaque index for group All indices are taken and divided by number of individual
Rating Scores
Excellent
0
Good 0.1-0.9
Fair 1.0-1.9
Poor 2.0-3.0
INTERPRETATION

29
USES
• Reliable technique for evaluating both mechanical anti plaque procedures and
chemical agents
• Used in longitudinal studies and clinical trials

30
ADVANTAGE•Good validity and reproducibility•Can be used as full mouth or simplified
DRAWBACK
•Subjectivity in estimating plaque

31
Turesky, Gilmore, Glickman modification of the Quigley-Hein plaque index
• Quigley and Hein in 1962 reported a plaque measurement that focused on the
gingival third of the tooth surface.
• Only facial surfaces of the anterior teeth were examined after using basic
fuchsin mouthwash as a disclosing agent.
• Quigley - Hein plaque index was modified by Turesky, Gilmore and Glickman in
1970.

32
SCORE
CRITERIA
0 No plaque
1 Separate flecks of plaque at the cervical margin of tooth
2 Thin continuous band of plaque ( up to 1 mm
3 Band of plaque wider than 1 mm but covering less than 1/3rd of the crown of the tooth.
4 Plaque covering at least 1/3rd but less than 2/3rd of the crown of the tooth
5 Plaque covering 2/3rd or more of the crown of the tooth

33
• Plaque is assessed on the labial, buccal and lingual surfaces of all the teeth after
using a disclosing agent.
• The scores of the gingival 1/3rd area was also redefined.
• Provides a comprehensive method for evaluating anti plaque procedures such
as tooth brushing, flossing as well as chemical anti plaque agents.
• The index is based on a numerical score of 0 to 5

O’LEARY INDEX(plaque control record)
• O' leary T, Drake R, Naylor in1972
• Method of recording the presence of the plaque on individual tooth surfaces
• Suitable disclosing solution such as Bismarck brown, Diaplac or similar is painted on all exposed tooth surfaces..
• The operator (using an explorer or a tip of a probe) examines each stained surface for soft accumulations at the dentogingival junction. When found, they are recorded by making a dash/red colour in the appropriate spaces on the record form

Calculation PLAQUE INDEX =The number of plaque containing surfaces The total number of available surfaces
Since plaque is stained ,identification and record making is easyAlso aids in patient education
DrawbackRecords only the presence or absence of plaque

BLEEDING POINT INDEX
• Provides an evaluation of gingival inflammation around each tooth in patient’s mouth• Bleeding on probing recorded on distal ,facial ,mesial and gingival surface• Calculation=(no of bleeding surface/total no of tooth surface)*100•Demonstrates gingival inflammation characterized by gingival bleeding rather than presence of microbial plaque

37
GINGIVAL AND PERIODONTAL DISEASE INDICES
• GINGIVAL INDEX
• PERIODONTAL INDEX
• CPITN
• COMMUNITY PERIODONTAL INDEX

38
GINGIVAL INDEX
• Developed by Loe and Silness in 1963.
• One of the most widely accepted and used gingival indices.
• Assess the severity of gingivitis and its location in 4 possible areas.
• Mesial
• Lingual
• Distal
• Facial
• 0nly qualitative changes are assessed.

39
:
• All surfaces of all teeth or selected teeth or selected surface of all teeth or
selected teeth are scored.
• The selected teeth as the index teeth are 16,12,24,36,32,44.
• The teeth and gingiva are first dried with a blast of air and/or cotton rolls.
• The tissues are divided into 4 gingival scoring units: Disto facial papilla, Facial
margin, Mesio facial papilla and Entire lingual margin.
• A blunt periodontal probe is used to assess the bleeding potential of the tissues.
METHOD

SCORE CRITERIA
0 Absence of inflammation/normal gingiva
1Mild inflammation, slight
change in color, slight edema, no bleeding on
probing
2Moderate inflammation,
moderate glazing, redness, edema and hypertrophy.
bleeding on probing
3
Severe inflammation, marked redness and
hypertrophy ulceration. Tendency to spontaneous
bleeding.
40

41
CALCULATION AND INTERPRETATION• If the scores around each tooth are totaled
and divided by the number of surfaces per
tooth examined (4), the gingival index score
for the tooth is obtained.
• Totaling all of the scores per tooth and
dividing by the number of teeth examined
provides the gingival index score for
individual.
INTERPRETATION:0.1 - 1.0 : mild gingivitis
1.1 – 2.0 : moderate gingivitis
2.1 – 3.0 : severe gingivitis

42
MODIFIED GINGIVAL INDEX
• Developed by Lobene, Weatherford, Ross, Lamm and Menaker in 1986.
• Assess the prevalence and severity of gingivitis.
• Strictly based on non invasive approach i.e. visual examination only without
any probing.
• To obtain MGI , labial and lingual surfaces of the gingival margins and the
interdental papilla of all erupted teeth except 3rd molars are examined and
scored.

43
0 • Normal (absence of inflammation)
1• Mild inflammation (slight change in
color, little change in texture) of any portion of the gingival unit
2 • Mild inflammation of the entire gingival unit
3• Moderate inflammation (moderate
glazing, redness, edema, and/or hypertrophy) of the gingival unit.
4• Severe inflammation (marked
redness and edema/hypertrophy, spontaneous bleeding, or ulceration) of the gingival unit.
SCORE CRITERIA

44
RUSELL’S PERIODONTAL INDEX
• Developed by Rusell AI in 1956.
• It was once widely used in epidemiological surveys but not used much now
because of introduction of new periodontal indices and refinement of criteria.
• The RPI is reported to be useful among large populations, but it is of limited use
for individuals or small groups.

45
• All the teeth are examined in this index.
• Russell chose the scoring values as 0,1,2,4,6,8 in order to relate the stage of
the disease in an epidemiological survey to the clinical conditions observed.
• The Russell’s rule states that “ when in doubt assign the lower score.”
METHOD

46
FIELD STUDIES CLINICAL STUDIES / RADIOGRAPHIC FINDINGS0 Negative. Neither overt inflammation in the
investing tissues nor loss of function due to destruction of supporting bone.
Radiographic appearance is essentially normal.
1 Mild gingivitis. An overt area of inflammation in the free gingiva does not circumscribe the tooth
2 Gingivitis. Inflammation completely circumscribe the tooth, but there is no apparent break in the epithelial attachment
4 Used only when radiographs are available. There is early notch like resorption of alveolar crest.6 Gingivitis with pocket formation. The
epithelial attachment is broken and there is a pocket. There is no interference with normal masticatory function; the tooth is firm in its socket and has not drifted.
There is horizontal bone loss involving the entire alveolar crest, up to half of the length of the tooth root.
8 Advanced destruction with loss of masticatory function. The tooth may be loose, may have drifted, may sound dull on percussion with metallic instrument, or may be depressible in its socket.
There is advanced bone loss involving more than half of the tooth root, or a definite intrabony pocket with widening of periodontal ligament. There may be root resorption or rarefaction at the apex.

47
CALCULATION AND INTERPRETATION
• RPI score per person = Sum of individual scores
No of teeth present
Clinical Condition Individual ScoresClinical normally supportive tissue
0.0-0.2
Simple gingivitis 0.3-0.9Beginning destructive periodontal diseases
1.0-1.9
Established destructive periodontal disease
2.0-4.9
Terminal disease 5.0-8.0

48
COMMUNITY PERIODONTAL INDEX OF TREATMENT NEEDS
• The community periodontal index of treatment needs (CPITN) was introduced by
JUKKA AINAMO for joint working committee of the WHO and FDI in 1982.
• Developed primarily to survey and evaluate periodontal treatment needs rather than
determining past and present periodontal status i.e. recession of the gingival margin
and alveolar bone.
• Treatment needs implies that the CPITN assesses only those conditions potentially
responsive to treatment, but not non treatable or irreversible conditions.

49
The mouth is divided into sextants :
17- 14 13- 23 24- 27
47 – 44 43- 33 34 – 37
• The 3rd molars are not included, except where they are functioning in place of 2nd molars.
• The treatment need in a sextant is recorded only if there are 2 or more teeth present in a
sextant and not indicated for extraction.
• If only one tooth remains in a sextant, then the tooth is included in the adjoining sextant.
Procedure :

50
Probing depth is recorded either on all the teeth in a sextant or only on certain
indexed teeth as recommended by who for epidemiological surveys.
For adults aged > 20 yrs:
• 10 index teeth are taken into account :17 16 11 26 37 47 46 31 36 37.
• The molars are examined in pairs and only one score the highest score is
recorded.

51
For young people up to 19 yrs:
• Only 6 index teeth are examined : 16 11 26 46 31 36
• The second molars are excluded at these ages because of the high frequency
of false pockets (non inflammatory tooth eruption associated).
• When examining children less than 15 yrs, pockets are not recorded although
probing for bleeding and calculus are carried out as a routine.

52
First described by WHO.
Designed for 2 purposes :
• measurement of pockets.
• detection of sub-gingival calculus.
Weighs : 5 gms
Working force: 20-25 gms
CPITN probe
CPITN-E PROBE
CPITN-C PROBE

53
CODE
CRITERIA TREATMENT NEEDS
0 Healthy periodontium
TN-0 No need of treatment
1 Bleeding observed during / after probing
TN-1 Self care
2 Calculus or other plaque retentive factors seen or felt during probing
TN-2 Professional care
3 Pathological pocket 4-5 mm. gingival margin situated on black band of the probe.
TN-2 Scaling and root planning
4 Pathological pocket 6mm or more. Black band of the probe not visible
TN-3 Complex therapy by specially trained personnel

54
ADVANTAGE• Simplicity
• Speed
• International uniformity
LIMITATIONS• Doesnot record the position of
gingiva
• Doesn’t provide assessment of past periodontal breakdown

COMMUNITY PERIODONTAL INDEX (CPI)Based on modification of CPITNModification is done by including “loss of attachment” and
eliminating “treatment needs” category.
CPI scoring criteria is same as CPITN and done with CPITN-C probe

56
Code Criteria 0 loss of attachment 0-3 mm, CEJ not visible
1 loss of attachment 4-5mm 2 loss of attachment 6-8mm 3 loss of attachment 9-11mm 4 loss of attachment 12mm or more X excluded sextant 9 not recorded
Codes and Criteria for Loss of attachment includes:

BY SCHOUR & MASSLER, (1944) • To count number of gingival unit affected with gingivitis that is
correlated with severity of gingival inflammation. • The facial surface of gingiva around a tooth divided into three
units: Papillary gingiva (P),
Marginal gingiva (M), and Attached gingiva (A).
• Usually central incisor to second premolars are examined.
PAPILLARY MARGINAL ATTACHMENT INDEX(PMA)

PAPILLARY COMPONENT (P)
• 0= NORMAL; NO INFLAMMATION.
• 1+= MILD PAPILLARY ENGORGEMENT; SLIGHT INCREASE IN SIZE.
• 2+= OBVIOUS INCREASE IN SIZE OF GINGIVAL PAPILLA; HEMORRHAGE ON PRESSURE.
• 3+= EXCESSIVE INCREASE IN SIZE WITH SPONTANEOUS HEMORRHAGE.
• 4+= NECROTIC PAPILLA.
• 5+= ATROPHY AND LOSS OF PAPILLA (THROUGH INFLAMMATION).

MARGINAL COMPONENT(M)• 0= Normal; no inflammation visible.
• 1+= Engorgement; slight increase in size; no bleeding.
• 2+= Obvious engorgement; bleeding upon pressure.
• 3+= Swollen collar; spontaneous hemorrhage; beginning infiltration into attached gingivae.
• 4+= Necrotic gingivitis.
• 5+= Recession of the free marginal gingiva below the CEJ due to inflammatory changes.
ATTACHED COMPONENT(A) 0= Normal; pale rose; stippled.
1+= slight engorgement with loss of stippling; change in color may or may not be present.
2+=obvious engorgement of attached gingivae with marked increase in redness. Pocket formation present.
3+=advanced periodontitis. Deep pockets evident.

61
CALCULATION:
P M A INDEX SCORE PER PERSON = P + M + A
USES:On clinical trailsOn individual patientFor epidemiological surveys

• FIRST INTRODUCED BY RAMFJORD IN 1959
• COMPOSED OF THREE COMPONENTS:
I. PLAQUE COMPONENT,
II. CALCULUS COMPONENT AND
III. GINGIVAL & PERIODONTAL COMPONENET.
• ALL THE THREE COMPONENTS WILL BE SCORED SEPARATELY USING SIX RAMFJORD SELECTED TEETH.
16 21 24 44 41 36
PERIODONTAL DISEASE INDEX (PDI)

PLAQUE COMPONENT:Scoring is done after staining with Bismark Brown solution.Score Criteria
0 No plaque
1 Plaque present on some but not on all interproximal, buccal, and lingual surfaces of the tooth
2 Plaque present on all interproximal, buccal, and lingual surfaces,but covering less than one half of these surfaces
3 Plaque extending over all interproximal, buccal and lingual surfaces, and covering more than one half of these surfaces

Plaque Score = Total scores No. of teeth examined
CALCULATION:

CALCULUS COMPONENT:SCORING CRITERIA:
SCORE
CRITERIA
0 No calculus
1 Supragingival calculus extending only slightly below the free gingival margin (not more than 1 mm
2 Moderate amount of supragingival and sub gingival calculus or sub- gingival calculus alone.
3 An abundance of supra gingival and sub gingival calculus

CALCULATION:
CALCULUS SCORE = TOTAL SCORES
NO. OF SURFACES EXAMINED

GINGIVAL AND PERIODONTAL COMPONENT.
• Gingival status is scored first.• Gingival status and crevice depth is recorded in relation to CEJ• All areas (m, d, b, l) is scored . • Only fully erupted teeth are scored . • There is no substitution for excluded teeth.

68
SCORE CRITERIA0 Absence of signs of inflammation1 Mild to moderate inflammatory gingival changes not
extending around the tooth2 Mild to moderately severe gingivitis extending all
around the tooth
3 severe gingivitis characterized by marked redness, swelling, tendency to bleed, and ulceration
4 gingival crevice in any of 4 measured areas(M,D,B,L) extending apically to CEJ but not more than 3mm
5 gingival crevice in any of 4 measured areas(M,D,B,L) extending apically to CEJ between 3-6mm
6 gingival crevice in any of 4 measured areas(M,D,B,L) extending apically more than 6mm from CEJ

CALCULATION
PDI score = Total of individual tooth scores (PS+CS+GPS) Number of tooth examined

70
RECENT ADVANCES IN PERIODONTAL INDICES
• BASIC PERIODONTAL EXAMINATION (BPE) INDEX• GENETIC SUSCEPTIBILITY INDEX FOR PERIODONTAL DISEASE• PERIODONTAL SCREENING AND RECORDING (PSR) INDEX

• Developed by British Society of Periodontology in 1986• Derived from the community periodontal index of
treatment needs (cpitn)• Simple and rapid screening tool that is used to
indicate the level of examination needed and to provide basic guidance on treatment need• Not a diagnostic tool
71
BASIC PERIODONTAL EXAMINATION (BPE) INDEX

72

• Genetic markers denote susceptibility toward disease manifestation and it would be useful to exploit the information hidden into them and to derive a Genetic Susceptibility Index (GSI)• Single Nucleotide Polymorphisms (SNP’s) in genes
encoding molecules of the host defense system are assessed and an association is established between SNP and disease status
73
GENETIC SUSCEPTIBILITY INDEX FOR PERIODONTAL DISEASE

• Introduced in 1992 by American Academy of Periodontology (AAP) and American Dental Association(ADA)• Endorsed by the World Health Organization (WHO)• Adaptation of the Community Periodontal Index of Treatment
needs (CPITN)• Used to measure gingival bleeding upon probing, calculus on
a tooth, and periodontal pocket depth in each sextant of the oral cavity 74
PERIODONTAL SCREENING AND RECORDING (PSR) INDEX

CALCULATING PSR
• Highest score in a sextant is recorded as the PSR score for the sextant.• Only one score is recorded for each sextant of the
oral cavity.• A WHO/CPITN/PSR probe is used to examine each
tooth individually75

ADVANTAGES
• Introducing a simplified screening method that met legal dental recording requirements.• Early detection of periodontal disease and it
serves as an aid in monitoring the periodontal status of patients
76
LIMITATIONS
• Limited use of the PSR system in children due to inability to differentiate pseudo-pockets• Does not measure epithelial attachment,
the severity of periodontal disease may be underestimated with its use
77

• Used to measure pocket depths.• A pocket measuring probe/ Williams probe is
used.• Main components to record: - Pocket depth (mm) - Mobility - Recession (mm) - Bleeding on probing - Furcation
DPC – DETAILED PERIODONTAL CHART

• Two blunt instruments are used to asses a tooth’s mobility.
e.g end of mirror and probe
• To quantify mobility, Millers index of mobility is used:
MOBILITY
GRADE MOBILITYGrade 0
Normal physiological mobility (<1mm)
Grade 1
Movement up to 1mm in horizontal plane
Grade 2
Movement greater than 1mm in horizontal plane
Grade 4
Severe mobility greater than 2mm or vertical mobility

• The furcation is the point at which the two roots divide.
• A pocket measuring probe is used (naber’s probe)
Ramfjord and Ash furcation index:
FURCATION
GRADE MOBILITYGrade 0 No clinical furcation involvedGrade 1 Bone loss up to 1/3 widthGrade 2 Bone loss up to 2/3 widthGrade 4 Through and through defect
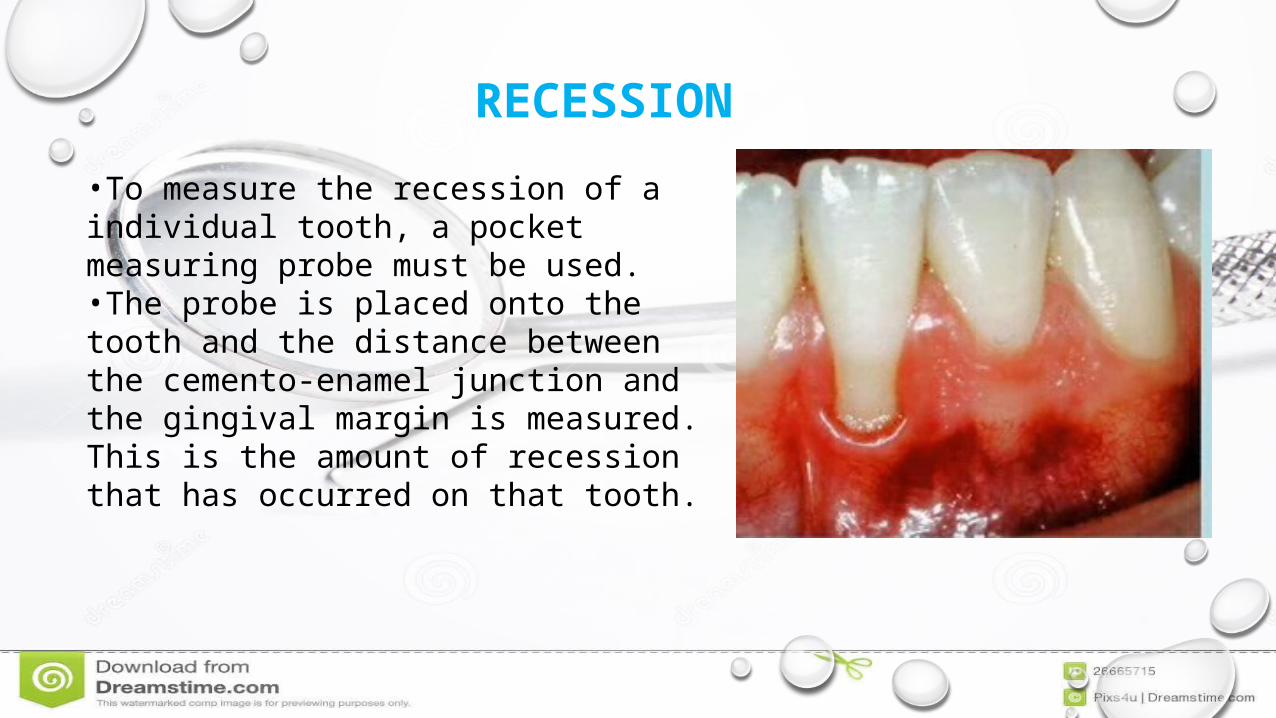
RECESSION•To measure the recession of a individual tooth, a pocket measuring probe must be used.•The probe is placed onto the tooth and the distance between the cemento-enamel junction and the gingival margin is measured. This is the amount of recession that has occurred on that tooth.

• THE POCKET MEASURING PROBE IS INSERTED INTO THE GINGIVAL CREVICE.
• THE DISTANCE FROM THE BASE OF THE POCKET AND THE GINGIVAL MARGIN IS MEASURED.
• IN ADDITION, IF THE SITE BLEEDS ON PROBING, CIRCLE THE SCORE IN RED AND IF THE SITE HAS SUPPURATION (PUS) CIRCLE THE SCORE IN BLUE OR BLACK.
BASELINE POCKET DEPTH
BASELINE POCKET DEPTH + RECESSION = CAL

• The DPC allows the operator to find sites in the mouth requiring attention.• Sites with pockets greater than 5mm will require RSD.• Subsequent pocket depths and cal can be measured after
treatment to assess the success of treatment.
WHAT HAPPENS FROM THE RESULTS OF THE DPC??

84
Dental diseases are the most prevalent and most neglected of all the chronic diseases of mankind.One of the major problems in studying dental diseases and its factors is the development of a suitable and practicable method for recording and classifying the occurrence and severity of the disease.Dental indices and scoring methods are used in clinical practice and community programs to determine and recoRd the state of health of individual and group
CONCLUSION

85
REFERENCES• Essentials of Public health dentistry 5E, Soben Peter
• Carranza's Clinical Periodontology, 12E (2015) , Newman, Takei, Klokkevold, Carranza
• Https://www.mah.se/capp/methods-and-indices/oral-hygiene-indices/simplified-oral-hygiene-index--ohi-s/
• Dhingra k, vandana k l; indices for measuring periodontitis: a literature review. international dental journal. 2011;

86
THANK YOU