perioperative chemotherapy for colorectal cancer ... en...jy douillard m ducreux a falcone a grothey...
TRANSCRIPT
Perioperative chemotherapy for
colorectal cancer livermetastases:
what is the optimal strategy?
Prof Eric Van Cutsem, MD, PhD
Digestive Oncology
Leuven, Belgium [email protected]
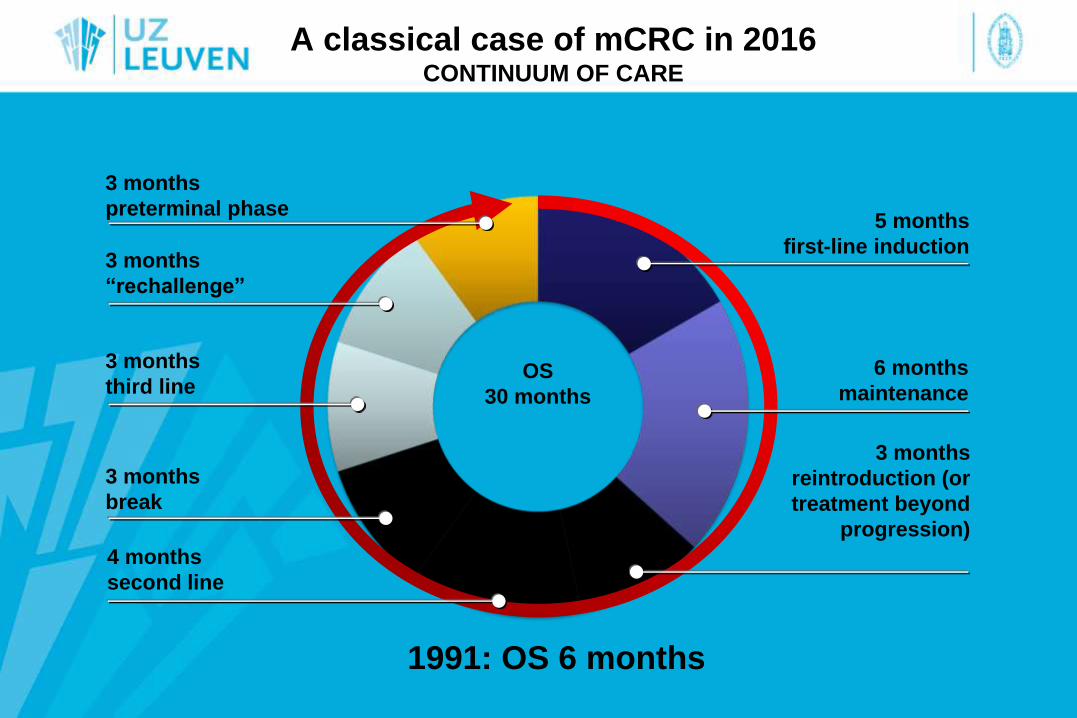
OS
30 months
A classical case of mCRC in 2016 CONTINUUM OF CARE
5 months
first-line induction
3 months
reintroduction (or
treatment beyond
progression)
3 months
“rechallenge”
3 months
break
6 months
maintenance
4 months
second line
3 months
third line
3 months
preterminal phase
1991: OS 6 months
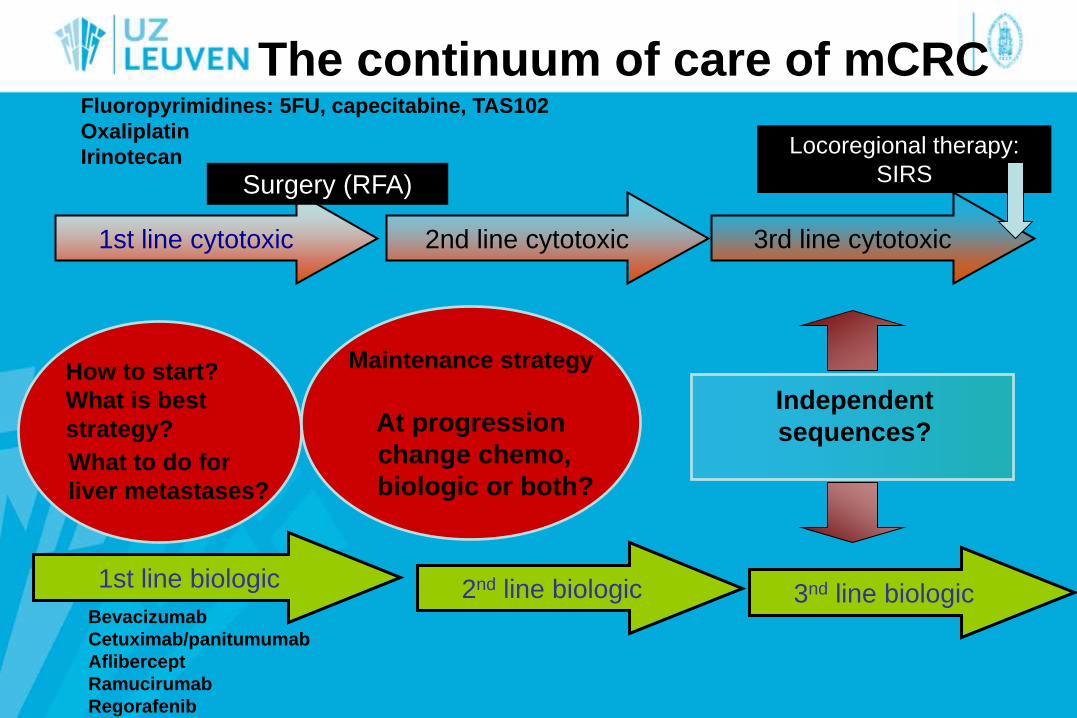
The continuum of care of mCRC
1st line cytotoxic 3rd line cytotoxic 2nd line cytotoxic
1st line biologic 2nd line biologic
Maintenance strategy
At progression
change chemo,
biologic or both?
Independent
sequences?
Fluoropyrimidines: 5FU, capecitabine, TAS102
Oxaliplatin
Irinotecan
Bevacizumab
Cetuximab/panitumumab
Aflibercept
Ramucirumab
Regorafenib
How to start?
What is best
strategy?
What to do for
liver metastases?
Locoregional therapy:
SIRS Surgery (RFA)
3nd line biologic
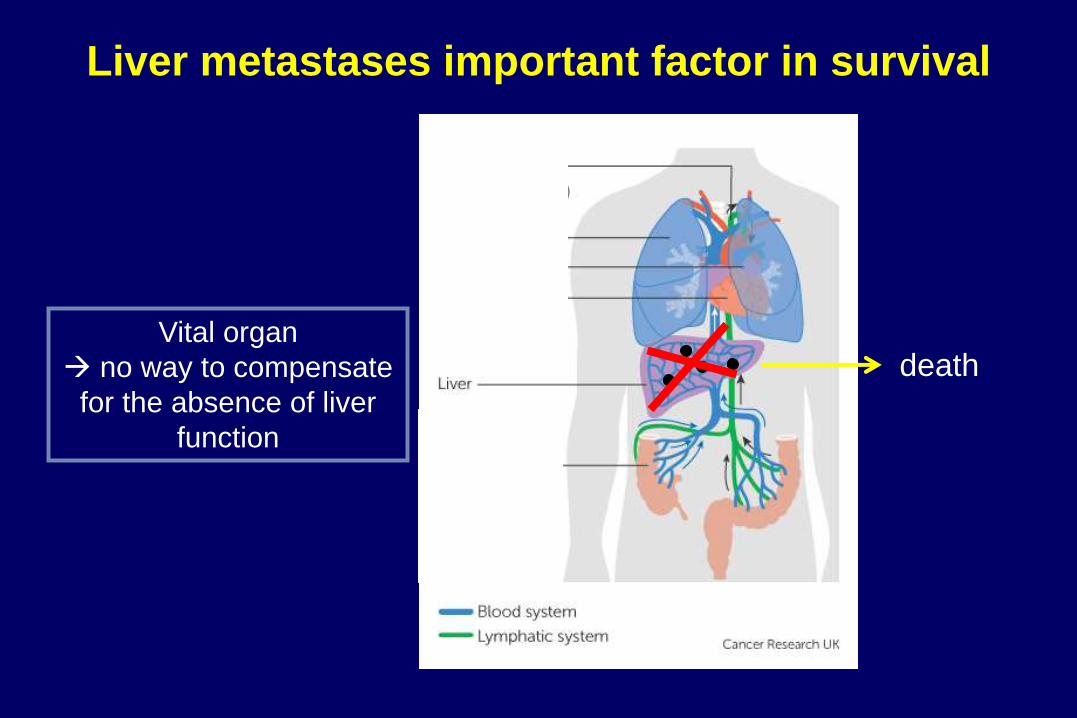
Liver metastases important factor in survival
death Vital organ
no way to compensate
for the absence of liver
function
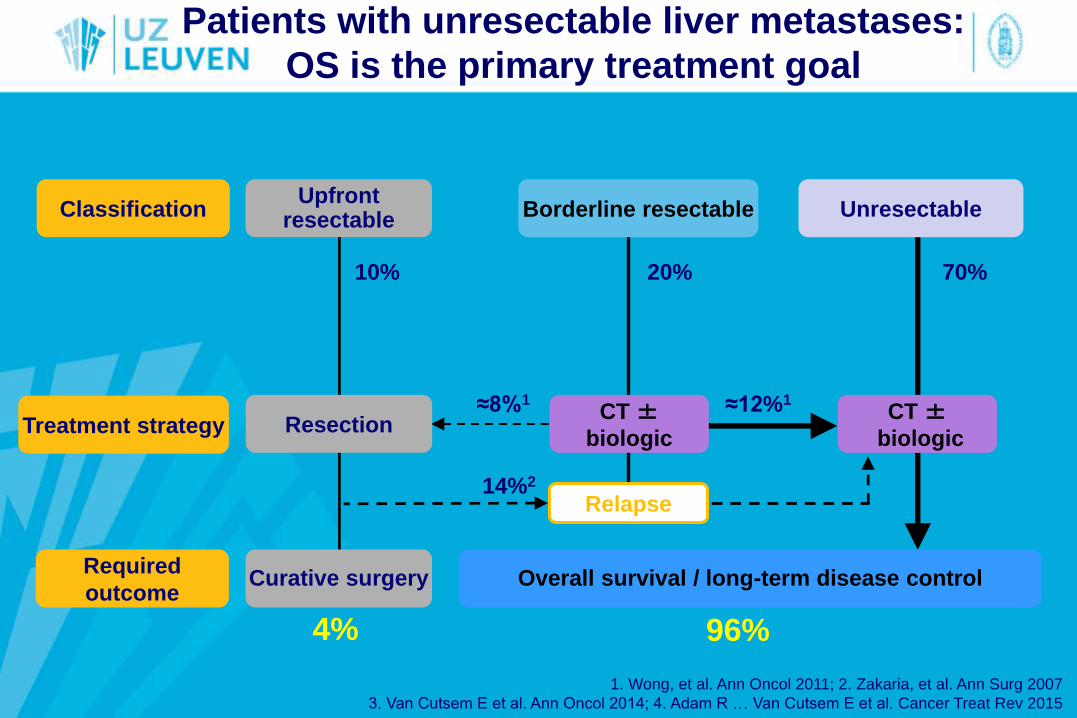
Patients with unresectable liver metastases:
OS is the primary treatment goal
Resection
Overall survival / long-term disease control
Treatment strategy
Required
outcome Curative surgery
10% 20% 70%
Classification Upfront
resectable Borderline resectable Unresectable
CT ±
biologic
CT ±
biologic
≈12%1 ≈8%1
Relapse 14%2
4% 96%
1. Wong, et al. Ann Oncol 2011; 2. Zakaria, et al. Ann Surg 2007
3. Van Cutsem E et al. Ann Oncol 2014; 4. Adam R … Van Cutsem E et al. Cancer Treat Rev 2015
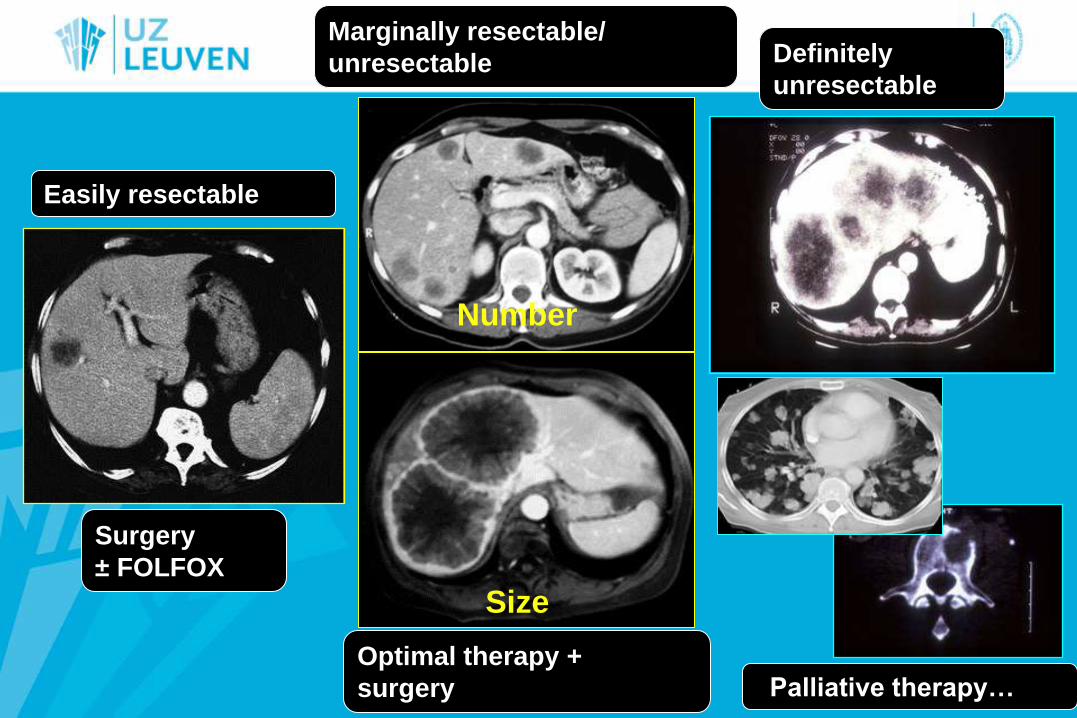
Easily resectable
Marginally resectable/
unresectable
Number
Size
Definitely
unresectable
Surgery
± FOLFOX
Optimal therapy +
surgery Palliative therapy…
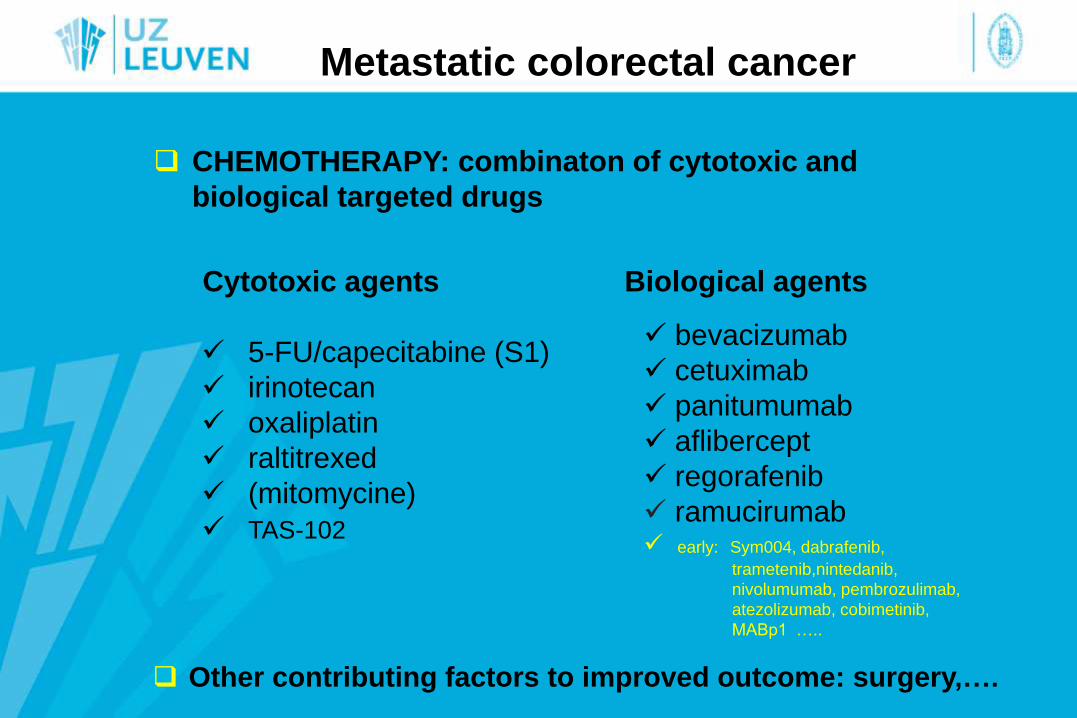
Metastatic colorectal cancer
CHEMOTHERAPY: combinaton of cytotoxic and
biological targeted drugs
Cytotoxic agents Biological agents
5-FU/capecitabine (S1)
irinotecan
oxaliplatin
raltitrexed
(mitomycine)
TAS-102
bevacizumab
cetuximab
panitumumab
aflibercept
regorafenib
ramucirumab early: Sym004, dabrafenib,
trametenib,nintedanib,
nivolumumab, pembrozulimab,
atezolizumab, cobimetinib,
MABp1 …..
Other contributing factors to improved outcome: surgery,….
ESMO consensus on mCRC 2016
Chairs: Co-Chairs of working groups
E Van Cutsem A Sobrero Advanced mCRC
D Arnold R Adam Local and ablative treatment, oligometastasis
A Cervantes H Van Krieken Molecular Pathology and Biomarkers
Contributors
D Aderka
E Aranda
A Bardelli
A Benson
G Bodoky
F Ciardiello
A D’Hoore
A Diaz Rubio
JY Douillard
M Ducreux
A Falcone
A Grothey
T Gruenberger
K Haustermans
V Heinemann
P Hoff
K Köhne
R Labianca
P Laurent-Puig
B Ma
T Maughan
K Muro
N Normanno
P Österlund
W Oyen
D Papamichael
G Pentheroudakis
P Pfeiffer
T Price
C Punt
J Ricke
A Roth
R Salazar
W Scheithauer
HJ Schmoll
J Tabernero
J Taieb
S Tejpar
H Wassan
T Yoshino
A Zaanan

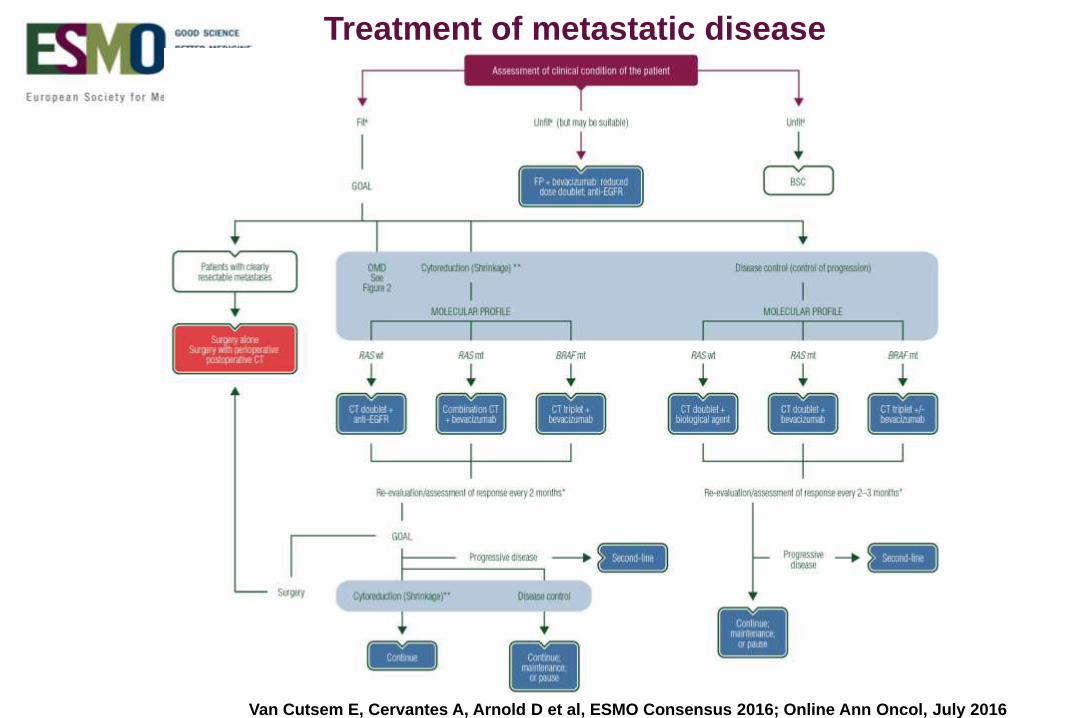
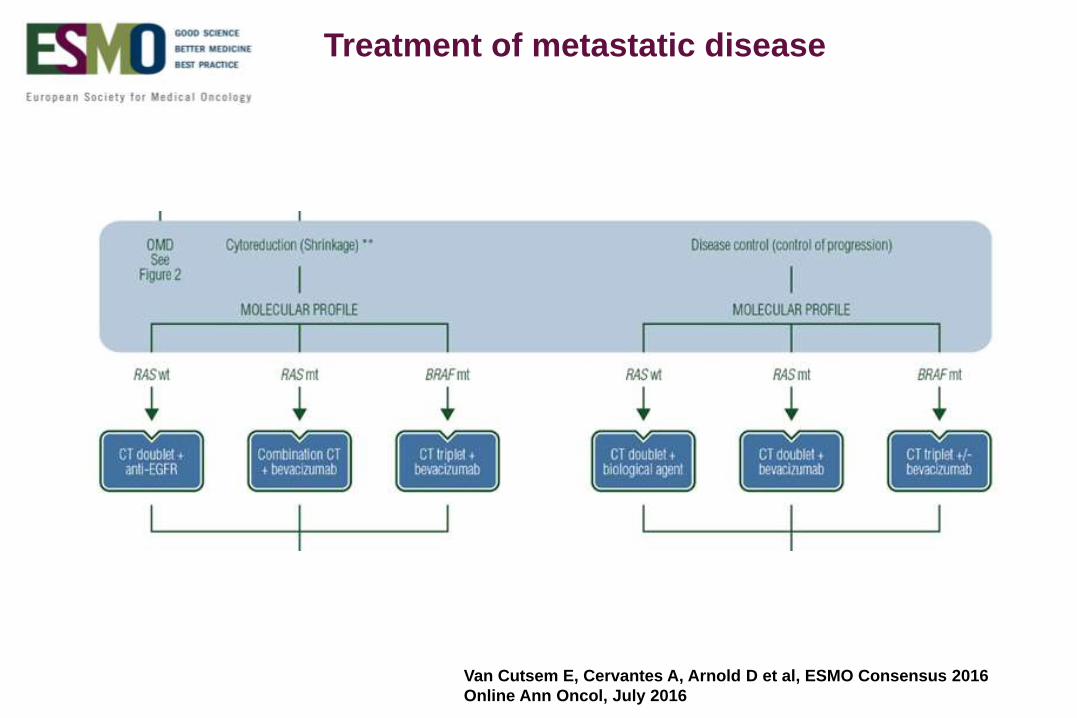
Treatment of metastatic disease
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016; Online Ann Oncol, July 2016
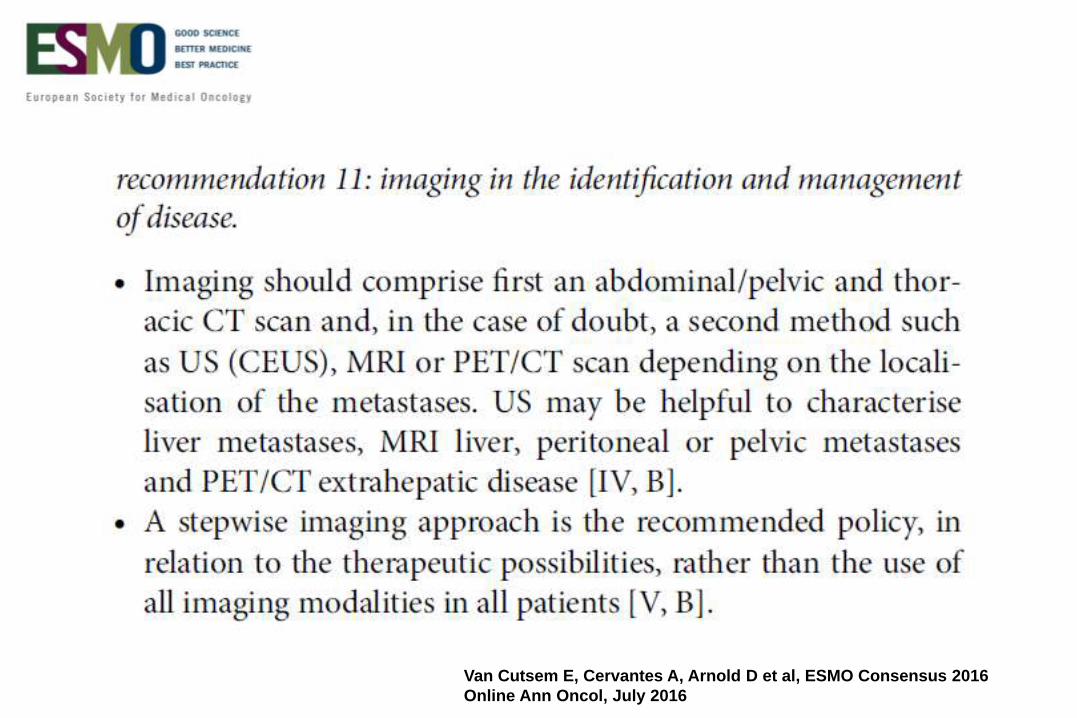
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
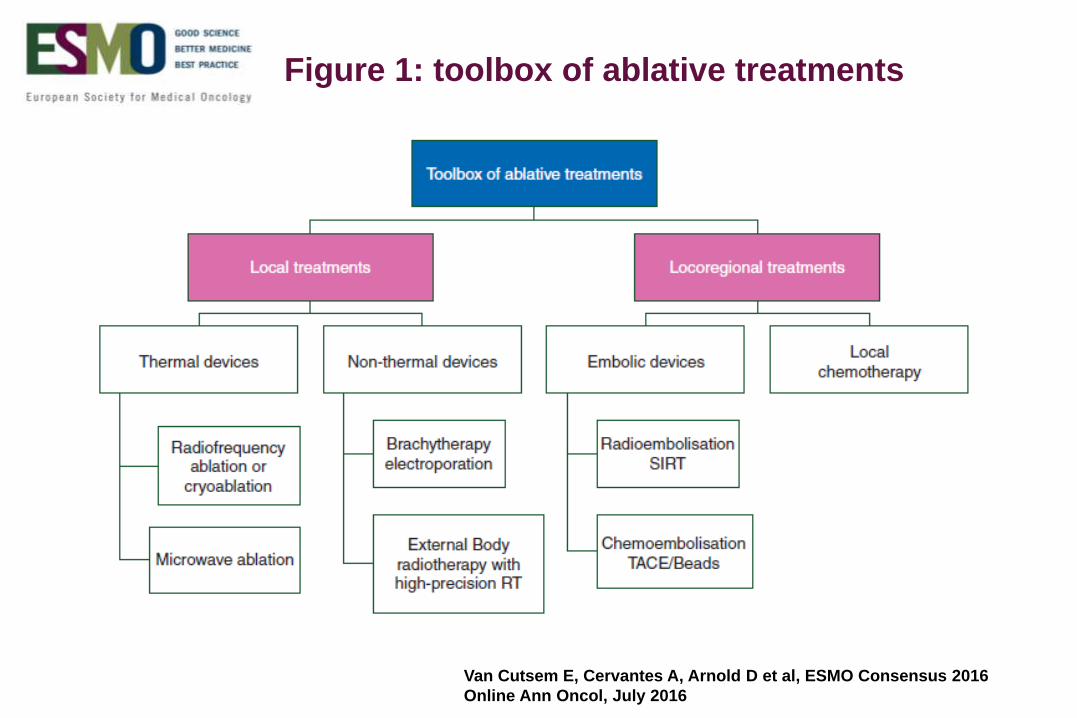
Figure 1: toolbox of ablative treatments
Recommendation 12: perioperative treatment.
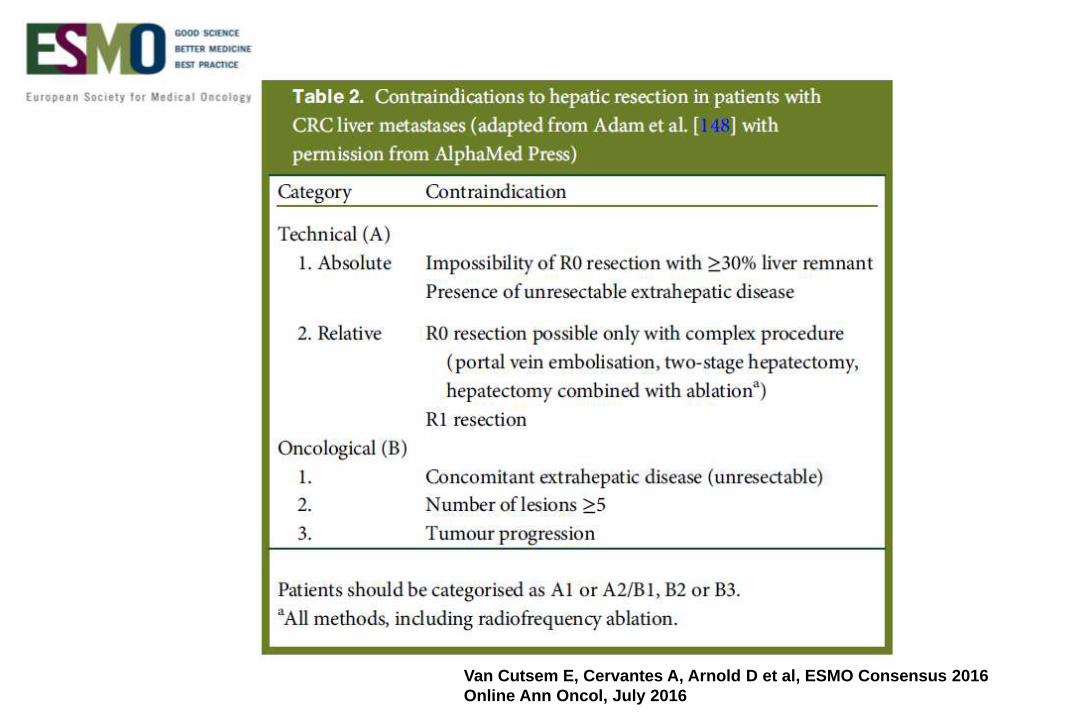
Both technical criteria for resection and prognostic considerations
define the need for systemic perioperative therapy [IV, B].
In patients with clearly resectable disease and favourable prognostic
criteria, perioperative treatment may not be necessary and upfront
resection is justified [I, C; consensus >75%].
In patients with technically resectable disease where the prognosis
is unclear or probably unfavourable, perioperative combination
chemotherapy (FOLFOX or CAPOX) should be administered [I, B;
consensus >75%].
Targeted agents should not be used in resectable patients where the
indication for perioperative treatment is prognostic in nature [II, E].
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Local and ablative treatment
(including surgery)
recommendation 12: perioperative treatment.
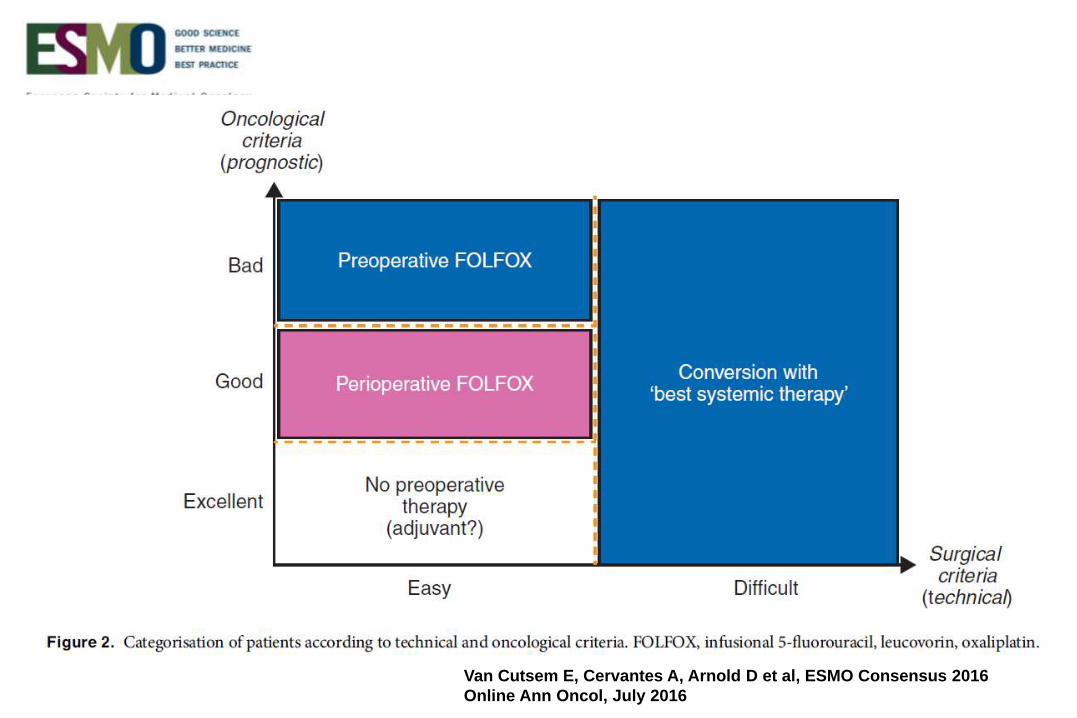
In situations where the criteria for prognosis and resectability are not sharply defined,
perioperative therapy should be considered (as part of a continuum of treatment option)
[IV, B] (Figure 2). Patients with synchronous onset of metastases should be allocated to
this group and therapeutic pathway.
In patients with favourable oncological and technical (surgical) criteria, who have not
received perioperative chemotherapy, there is no strong evidence to support the use of
adjuvant chemotherapy [II, C], whereas patients with unfavourable criteria may benefit
from adjuvant treatment [III, B].
In patients who have not received any previous chemotherapy, adjuvant treatment with
FOLFOX or CAPOX is recommended (unless patients were previously recently
exposed to oxaliplatin-based adjuvant chemotherapy) [IV, B].
Decision-making should include patients’ characteristics and preferences [IV, B].
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Local and ablative treatment
(including surgery)
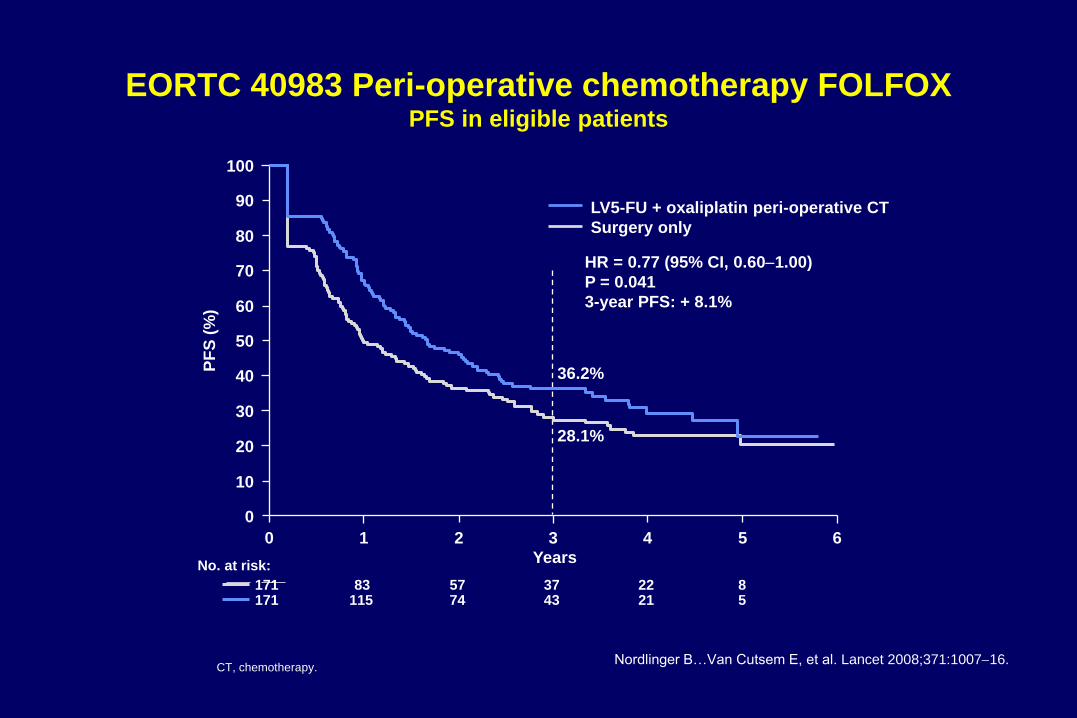
EORTC 40983 Peri-operative chemotherapy FOLFOX PFS in eligible patients
Nordlinger B…Van Cutsem E, et al. Lancet 2008;371:100716. CT, chemotherapy.
HR = 0.77 (95% CI, 0.601.00)
P = 0.041
3-year PFS: + 8.1%
28.1%
36.2%
Years
0 1 2 3 4 5 6
0
10
20
30
40
50
60
70
80
90
100
No. at risk:
171 83 57 37 22 8 171 115 74 43 21 5
PF
S (
%)
LV5-FU + oxaliplatin peri-operative CT
Surgery only
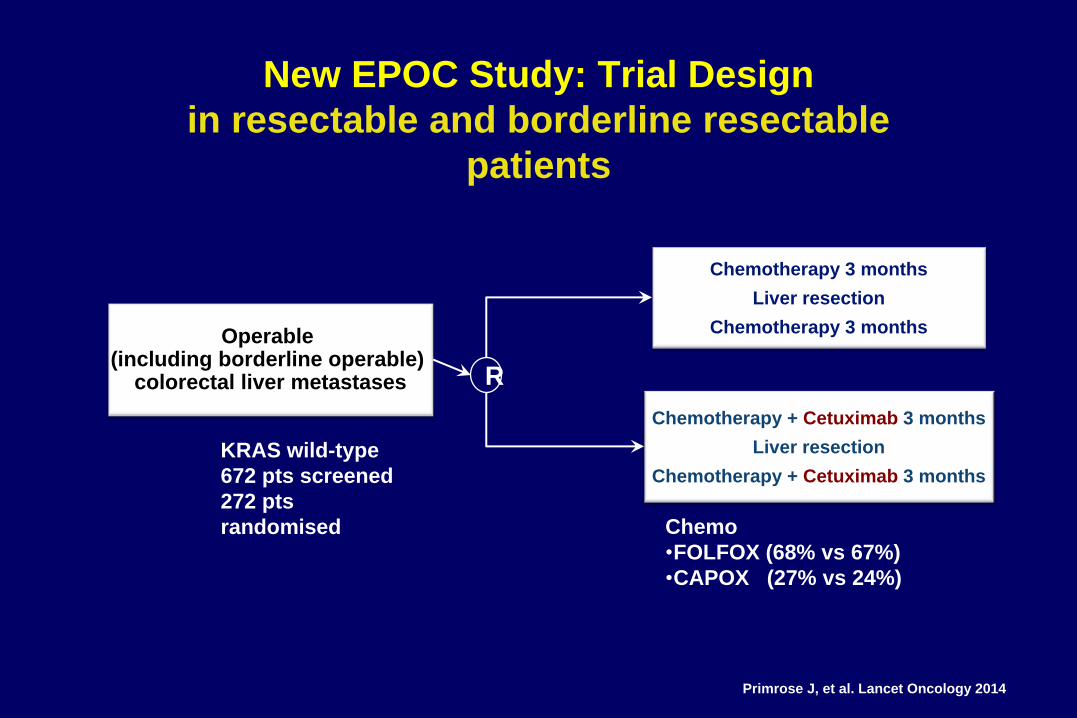
New EPOC Study: Trial Design
in resectable and borderline resectable
patients
Chemotherapy 3 months
Liver resection
Chemotherapy 3 months Operable (including borderline operable)
colorectal liver metastases
Chemotherapy + Cetuximab 3 months
Liver resection
Chemotherapy + Cetuximab 3 months
R
Primrose J, et al. Lancet Oncology 2014
Chemo
•FOLFOX (68% vs 67%)
•CAPOX (27% vs 24%)
KRAS wild-type
672 pts screened
272 pts
randomised
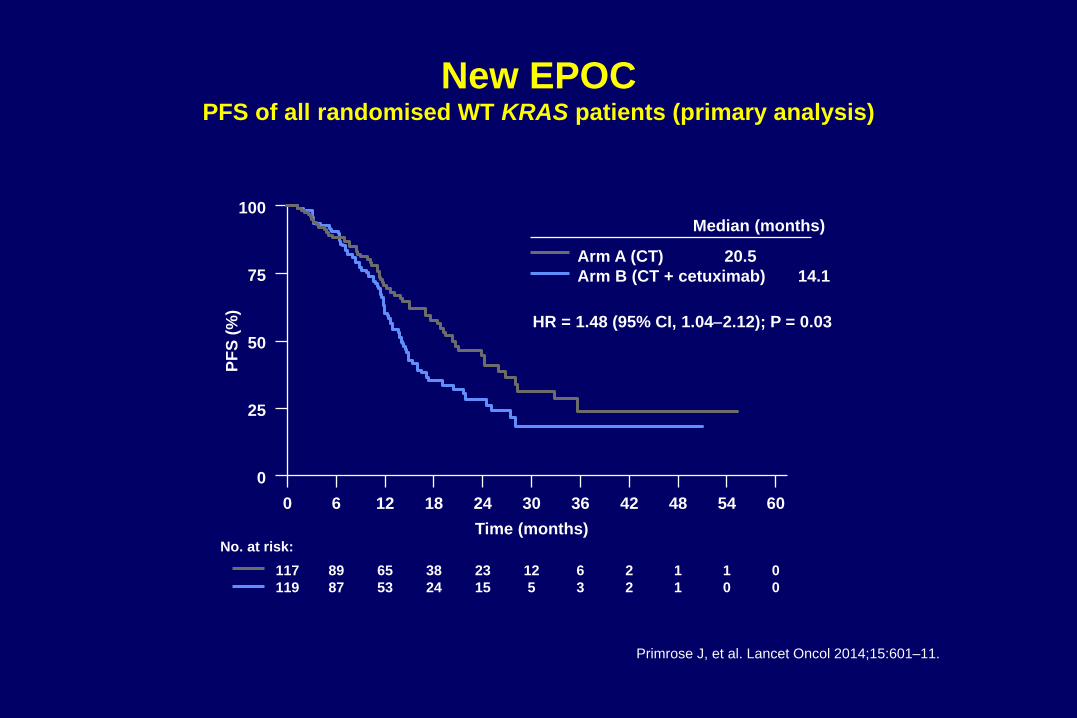
New EPOC PFS of all randomised WT KRAS patients (primary analysis)
Primrose J, et al. Lancet Oncol 2014;15:601–11.
60 54 48 42 36 30 24 18 12 6 0
0
25
50
75
100
HR = 1.48 (95% CI, 1.042.12); P = 0.03
Arm A (CT) 20.5
Arm B (CT + cetuximab) 14.1
0
0
1
0
1
1
2
2
6
3
12
5
23
15
38
24
65
53
89
87
117
119
Time (months) No. at risk:
PF
S (
%)
Median (months)
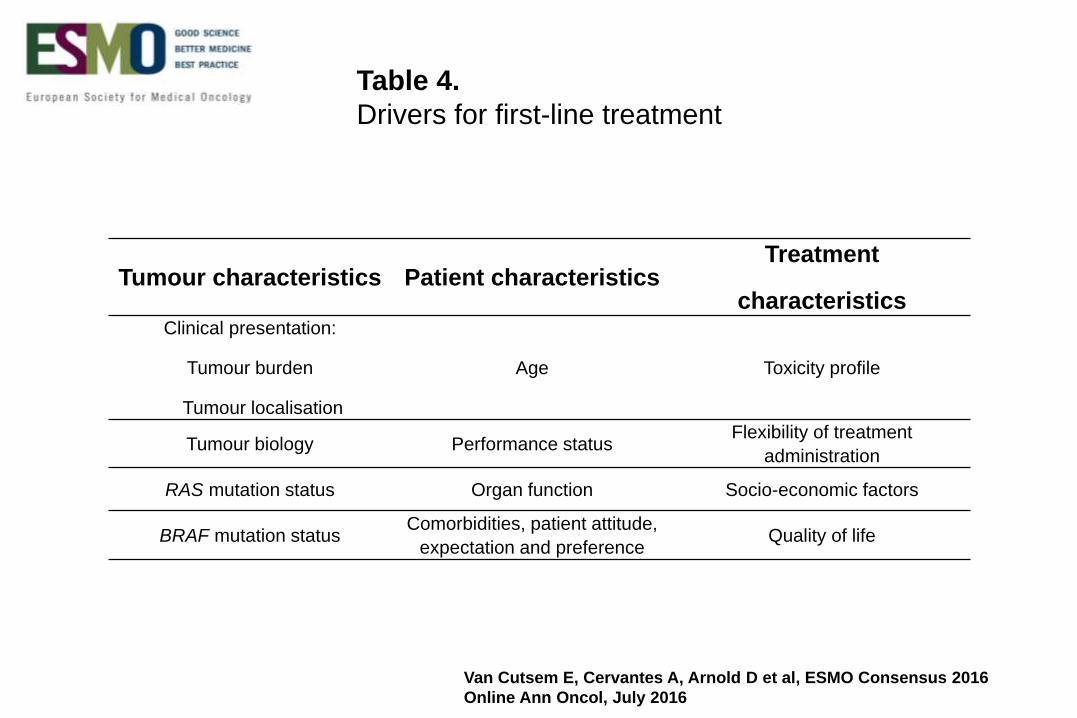
Tumour characteristics Patient characteristics Treatment
characteristics Clinical presentation:
Tumour burden
Tumour localisation
Age Toxicity profile
Tumour biology Performance status Flexibility of treatment
administration
RAS mutation status Organ function Socio-economic factors
BRAF mutation status Comorbidities, patient attitude,
expectation and preference Quality of life
Table 4.
Drivers for first-line treatment
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
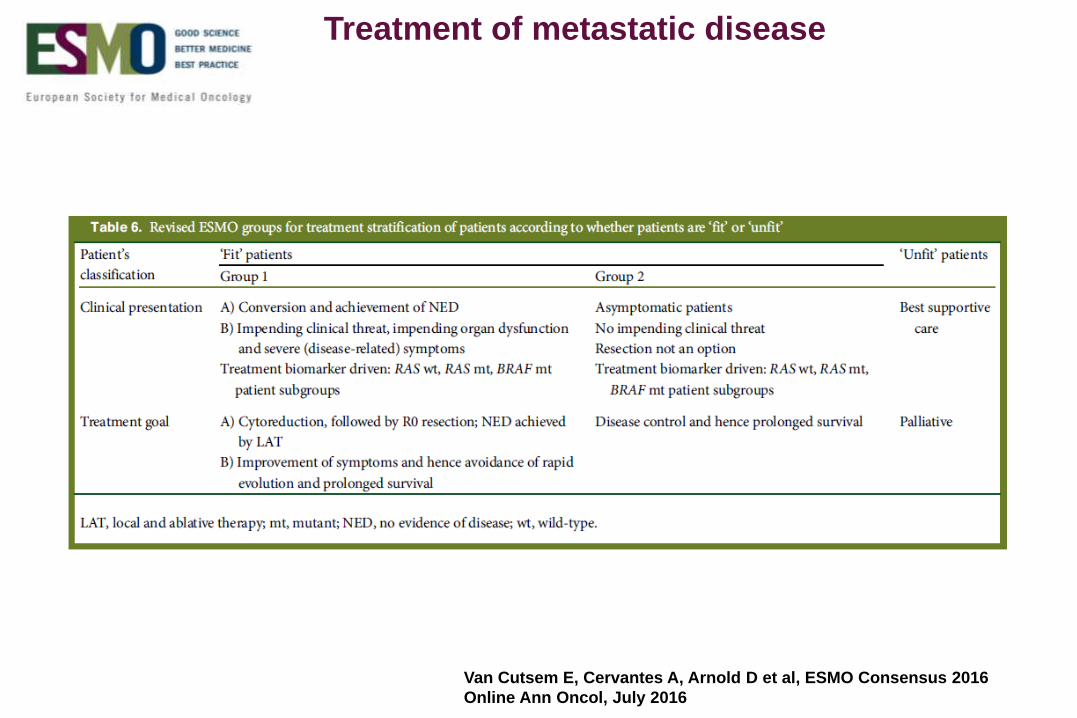
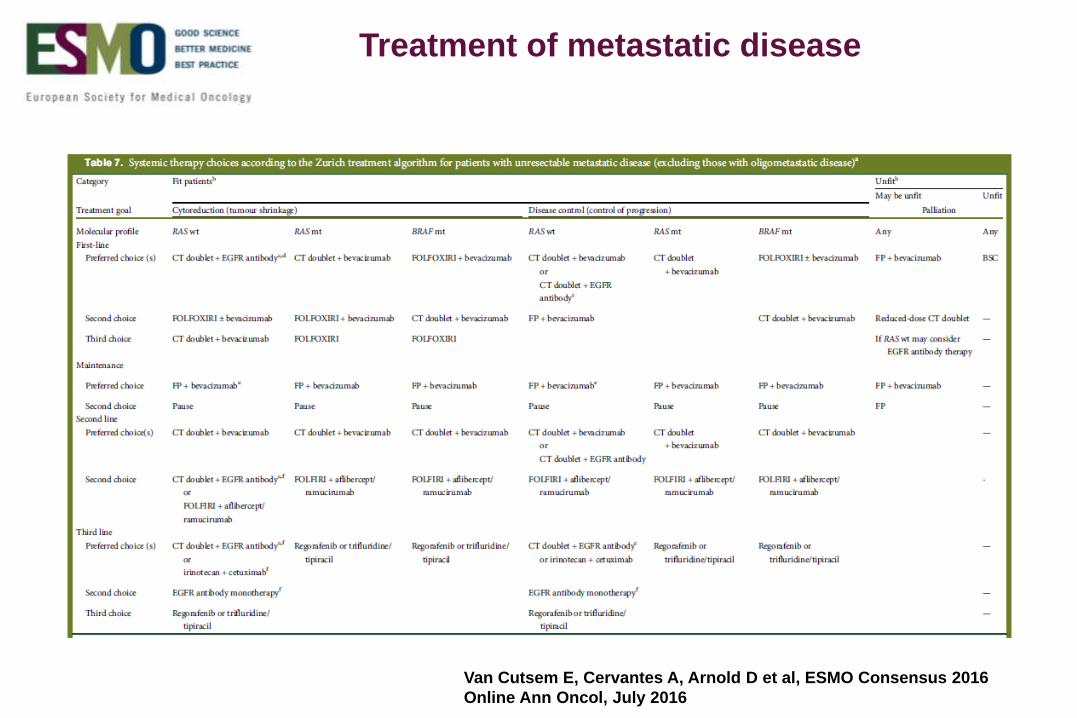
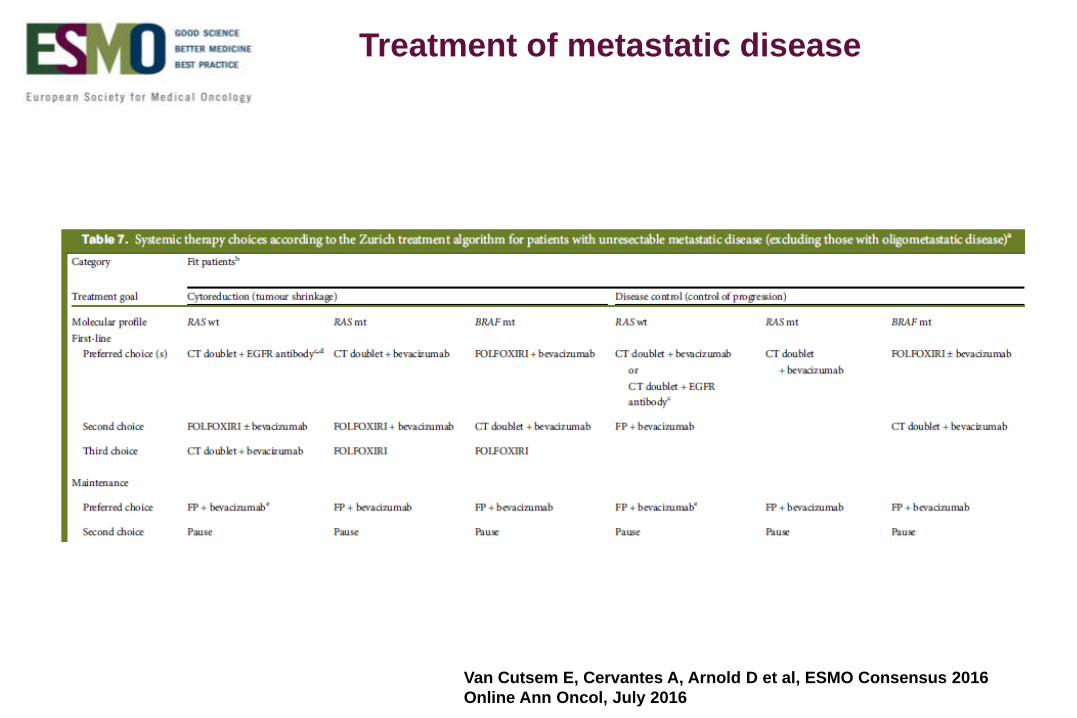
Treatment of metastatic disease
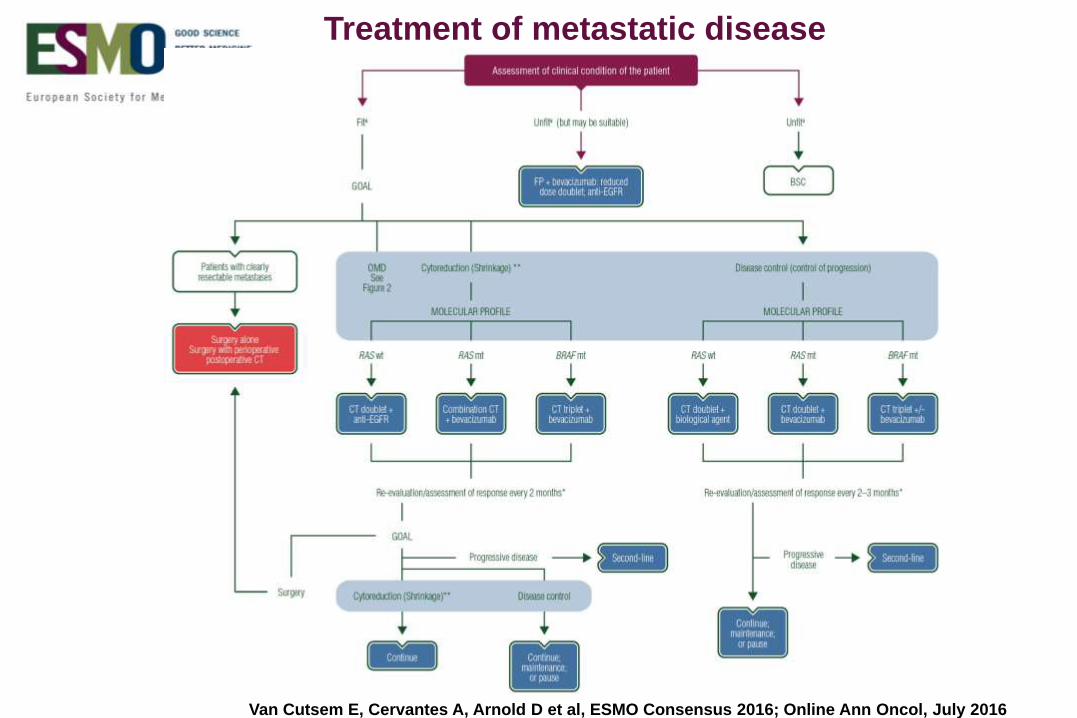
Treatment of metastatic disease
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016; Online Ann Oncol, July 2016
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Treatment of metastatic disease
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Treatment of metastatic disease
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Treatment of metastatic disease
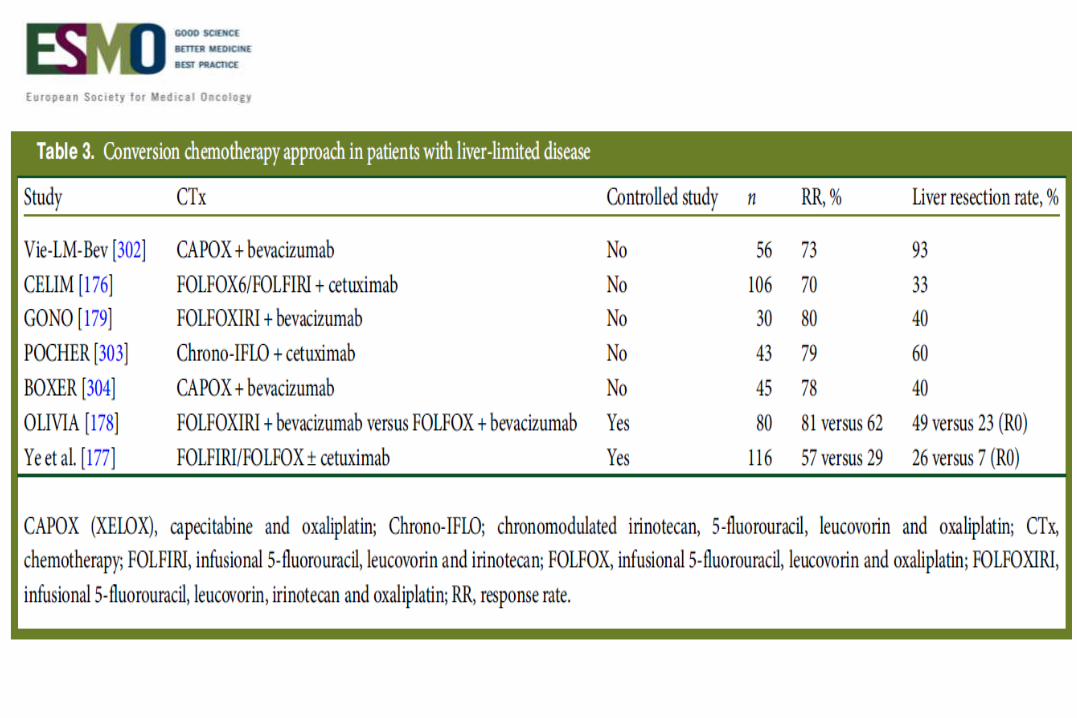
Recommendation 13: conversion therapy.
In potentially resectable patients (if conversion is the goal), a regimen leading to high
RRs and/or a large tumour size reduction (shrinkage) is recommended [II, A].
There is uncertainty surrounding the best combination to use as only few trials have
addressed this specifically:
In patients with RAS wild-type disease, a cytotoxic doublet plus an anti-EGFR
antibody seems to have the best benefit risk/ratio, although the combination of
FOLFOXIRI plus bevacizumab may also be considered and, to a lesser extent, a
cytotoxic doublet plus bevacizumab [II, A].
In patients with RAS-mutant disease: a cytotoxic doublet plus bevacizumab or
FOLFOXIRI plus bevacizumab [II, A].
Patients must be re-evaluated regularly in order to prevent the overtreatment of
resectable patients as the maximal response is expected to be achieved after 12–16
weeks of therapy in most patients.
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
Local and ablative treatment
(including surgery)
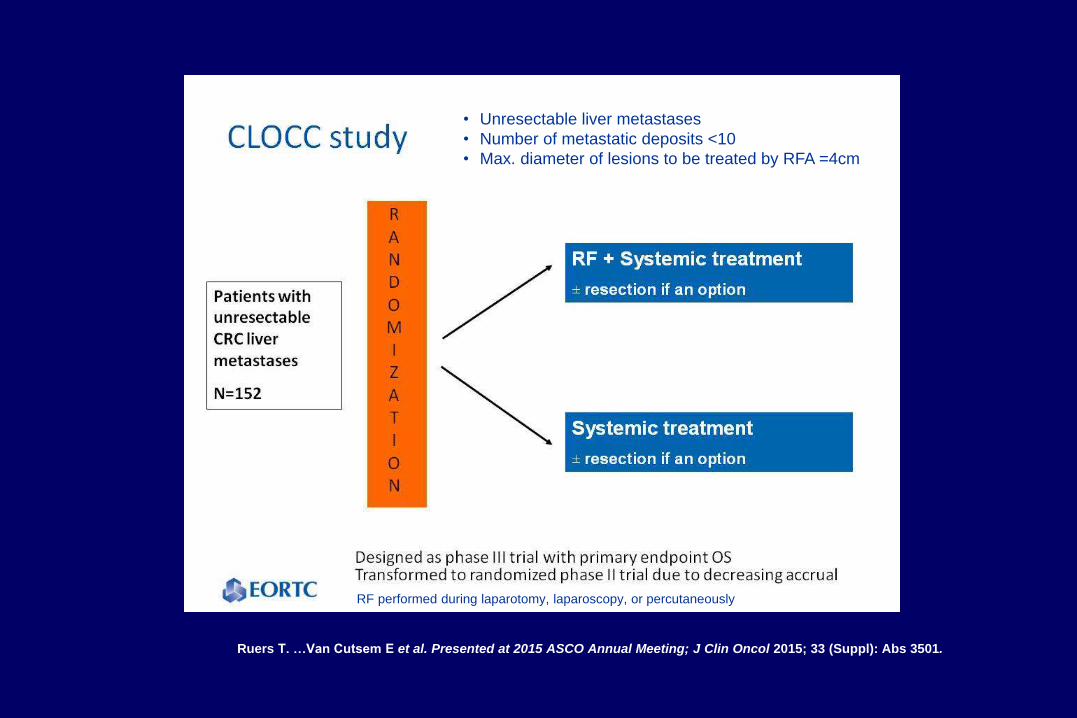
Ruers T. …Van Cutsem E et al. Presented at 2015 ASCO Annual Meeting; J Clin Oncol 2015; 33 (Suppl): Abs 3501.
• Unresectable liver metastases
• Number of metastatic deposits <10
• Max. diameter of lesions to be treated by RFA =4cm
RF performed during laparotomy, laparoscopy, or percutaneously
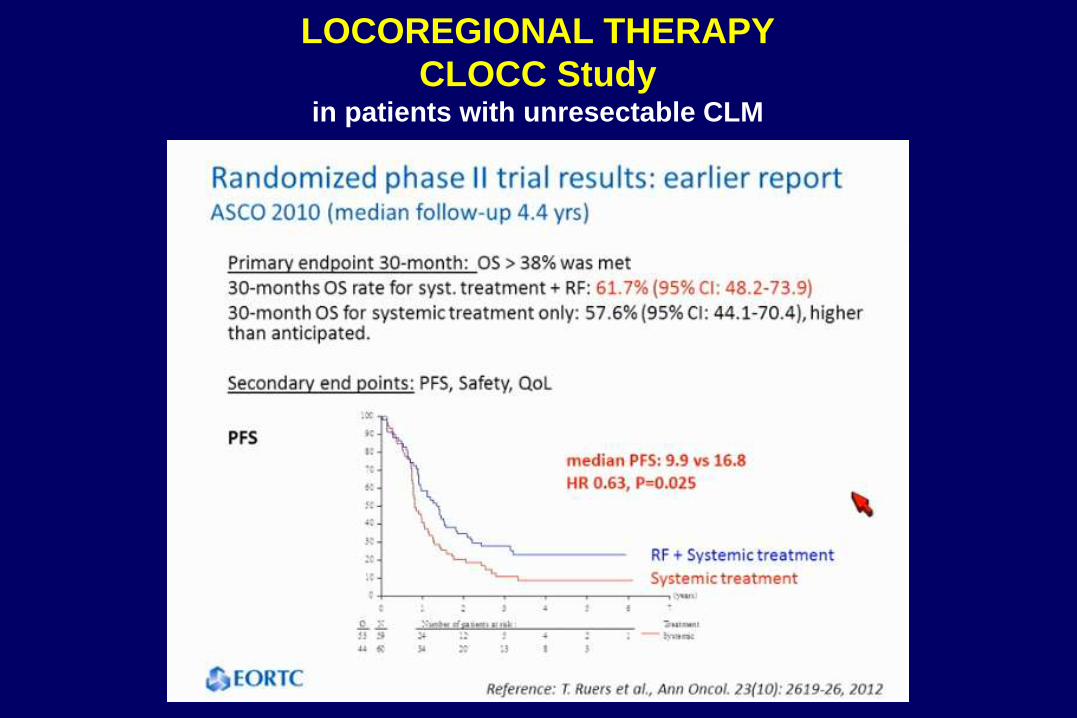
LOCOREGIONAL THERAPY
CLOCC Study in patients with unresectable CLM
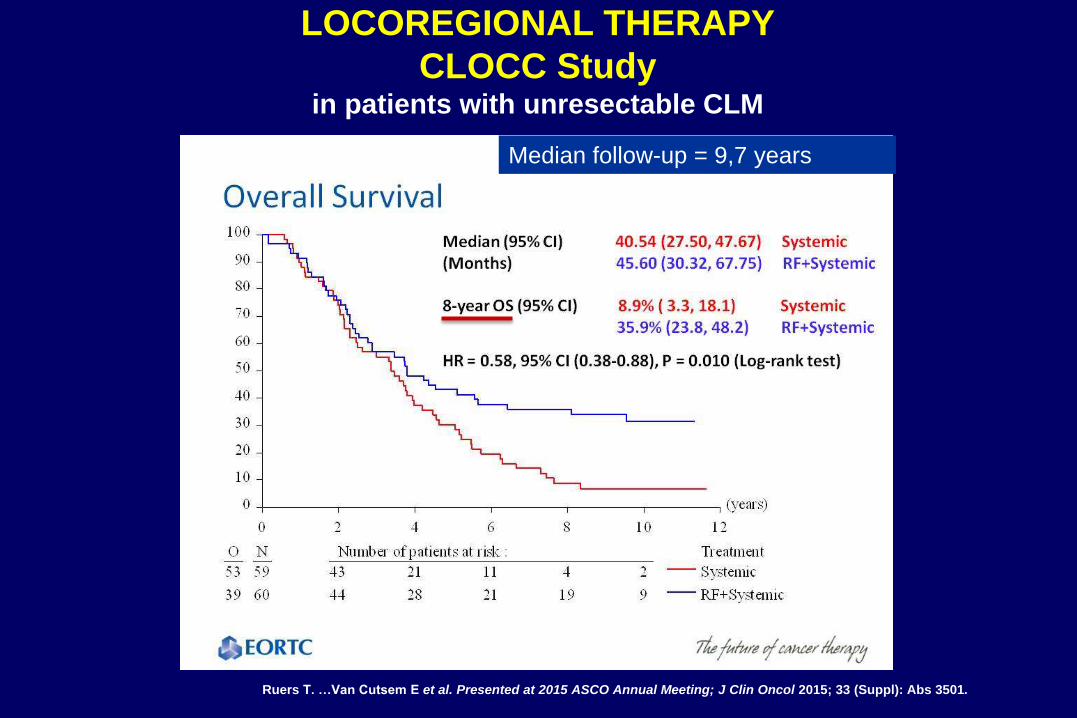
Median follow-up = 9,7 years
Ruers T. …Van Cutsem E et al. Presented at 2015 ASCO Annual Meeting; J Clin Oncol 2015; 33 (Suppl): Abs 3501.
LOCOREGIONAL THERAPY
CLOCC Study in patients with unresectable CLM
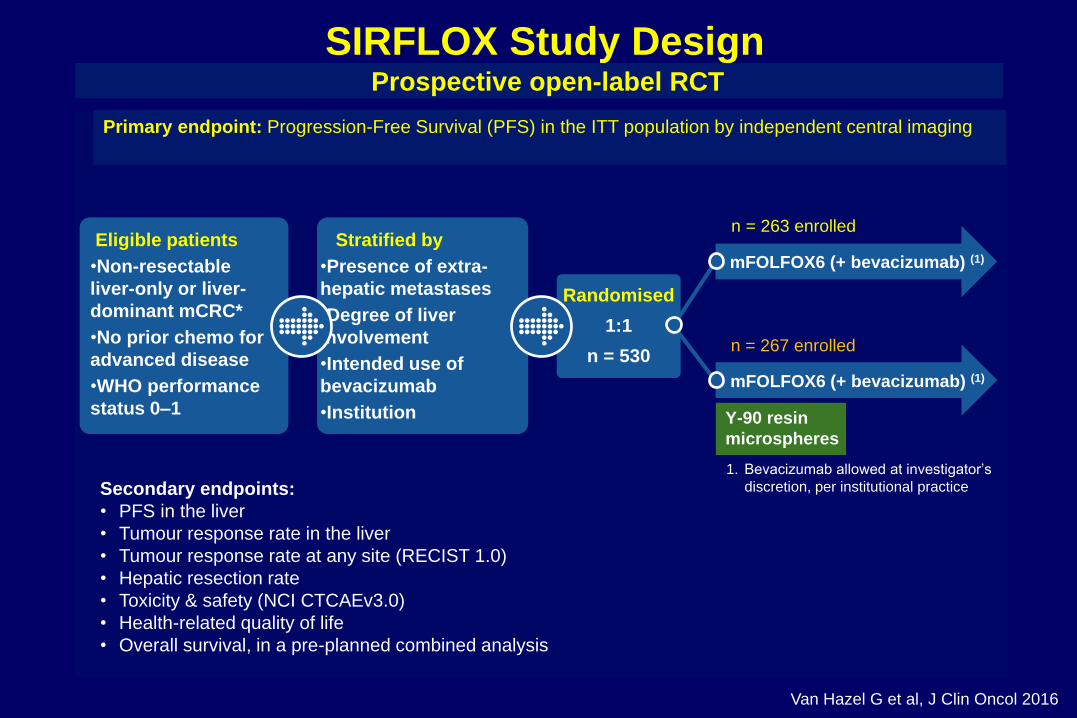
SIRFLOX Study Design Prospective open-label RCT
Primary endpoint: Progression-Free Survival (PFS) in the ITT population by independent central imaging
1. Bevacizumab allowed at investigator’s
discretion, per institutional practice
Stratified by
•Presence of extra-
hepatic metastases
•Degree of liver
involvement
•Intended use of
bevacizumab
•Institution
Randomised
1:1
n = 530
Eligible patients
•Non-resectable
liver-only or liver-
dominant mCRC*
•No prior chemo for
advanced disease
•WHO performance
status 0–1
mFOLFOX6 (+ bevacizumab) (1)
Y-90 resin
microspheres
n = 263 enrolled
n = 267 enrolled
mFOLFOX6 (+ bevacizumab) (1)
Secondary endpoints:
• PFS in the liver
• Tumour response rate in the liver
• Tumour response rate at any site (RECIST 1.0)
• Hepatic resection rate
• Toxicity & safety (NCI CTCAEv3.0)
• Health-related quality of life
• Overall survival, in a pre-planned combined analysis
Van Hazel G et al, J Clin Oncol 2016
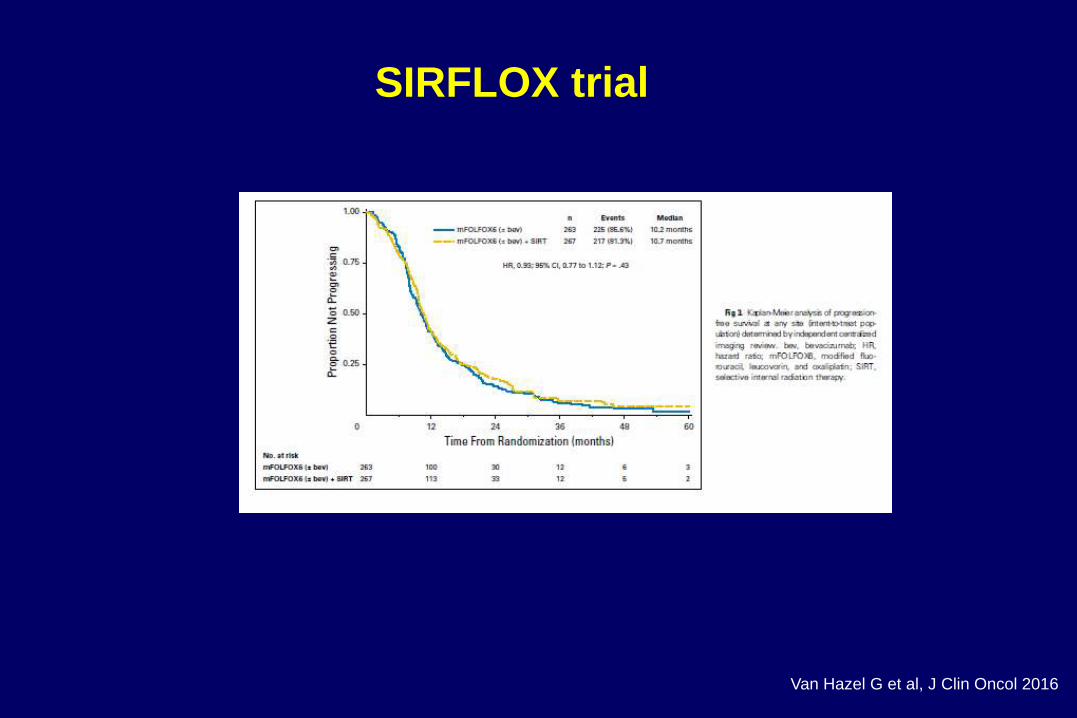
SIRFLOX trial
Van Hazel G et al, J Clin Oncol 2016
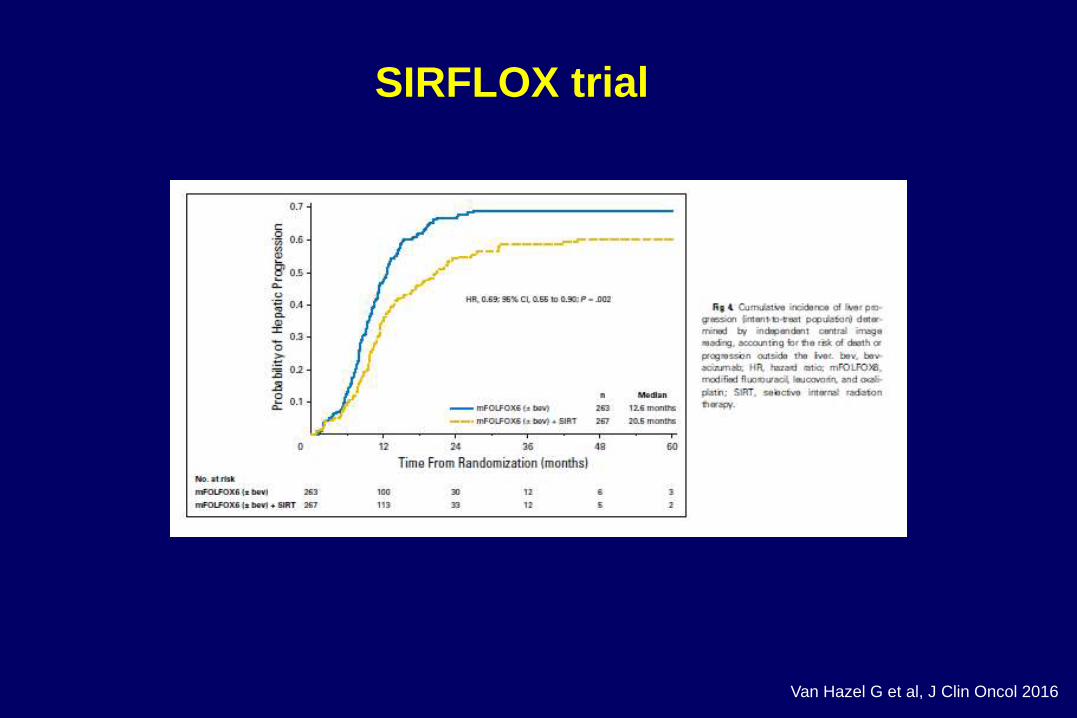
SIRFLOX trial
Van Hazel G et al, J Clin Oncol 2016
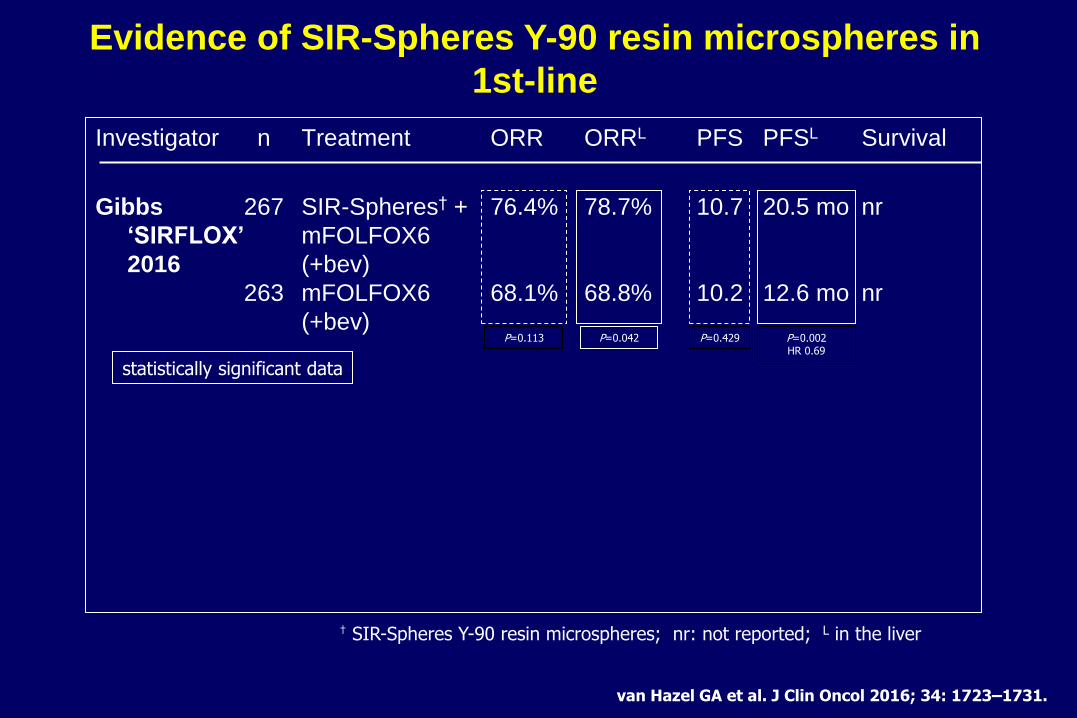
Investigator n Treatment ORR ORRL PFS PFSL Survival
Gibbs 267 SIR-Spheres† + 76.4% 78.7% 10.7 20.5 mo nr
‘SIRFLOX’ mFOLFOX6
2016 (+bev)
263 mFOLFOX6 68.1% 68.8% 10.2 12.6 mo nr
(+bev)
P=0.042 P=0.429
statistically significant data
† SIR-Spheres Y-90 resin microspheres; nr: not reported; L in the liver
van Hazel GA et al. J Clin Oncol 2016; 34: 1723–1731.
P=0.002 HR 0.69
P=0.113
Evidence of SIR-Spheres Y-90 resin microspheres in
1st-line
Recommendation 16: Embolisation
For patients with liver-limited disease failing the available
chemotherapeutic options
Radioembolisation with yttrium-90 microspheres should be considered
[II, B] Chemoembolisation may be also considered as a treatment option [IV,
B].
Radioembolisation (and chemoembolisation) of CLM in earlier
treatment lines may be interesting as “consolidation treatment” but
should be limited to clinical trials.
Local and ablative treatment
Van Cutsem E, Cervantes A, Arnold D et al, ESMO Consensus 2016
Online Ann Oncol, July 2016
SCENARIO 1: Asymptomatic CRC and resectable
synchronous CRCLM:
No strong evidence on best scenario
Expert recommendation: chemotherapy first – 4-6 cycles
But: LiverMetsSurvey: 5 y survival: 42 vs 47 % for CT first
vs Surgery of primary first
For mid and low rectal primary tumours:
* RT is often needed
* One-stage surgery should not be performed, unless
limited hepatic disease and ‘easy’ to resect primary
Synchronous liver metastases:
clinical scenarios
SCENARIO 2: Asymptomatic CRC and non-resectable
synchronous CRCLM:
Most frequently observed scenario
Chemotherapy first (expert opinion): optimal
chemotherapy (doublets or triplets + biologicals)
But: LiverMetsSurvey: no 5 y survival difference: 31 vs 33%
for CT first vs Surgery of primary first
One-stage surgery should not be performed
If metastases become resectable: experts recommend
reverse approach: liver first
LiverMetsSurvey: 5 y survival 42 % for reverse strategy vs
33% for colon first and 28% for one stage surgery
RT: either before starting CT or in window between CT and
surgery
Synchronous liver metastases:
clinical scenarios
SCENARIO 3: Symptomatic CRC and resectable
synchronous CRCLM:
No strong evidence on best scenario
More difficult for rectal cancer than colon cancer (where
often resection of the primary tumour is adviced)
Bleeding: start with CT or RT
Obstruction: derivative colostomy for rectal cancer if not
resectable
Results with stents have been poor
Expert recommendation: chemotherapy first – 4-6 cycles
For mid and low rectal primary tumours:
* RT is often needed
* One-stage surgery should not be performed, unless
limited hepatic disease and ‘easy’ to resect primary
Synchronous liver metastases:
clinical scenarios
SCENARIO 4: Symptomatic CRC and non-resectable
synchronous CRCLM:
Aim: make the liver metastases resectable
Bleeding: start with CT or RT
Obstruction: derivative colostomy for rectal cancer if not
resectable
Results with stents have been poor
Chemotherapy first (expert opinion): optimal
chemotherapy (doublets or triplets + biologicals)
One-stage surgery should not be performed
If metastases become resectable: experts recommend
reverse approach: liver first (unless primary is still very
symptomatic)
RT: either before starting CT or in window between CT and
surgery
Synchronous liver metastases:
clinical scenarios
