perioperative fluid management in pediatric patient
TRANSCRIPT

Perioperative Fluid Management
In Pediatric Patient
Arie Utariani
Department of Anesthesiology & Reanimation
Faculty of Medicine, Airlangga University
Surabaya

Physiology
- Percentage of body water exceeds that of adult.
- Expanded extracellular space which contracts during
first week of life :
1. Increasing glomerular filtration rate
2. Physiologic diuresis occurs with loss of about 10%
of total body weight
3. Some SGA / dysmature infants may not have
expanded extracelllar space
- By 6 months of age, healthy infants have kidney function
that is almost normal.
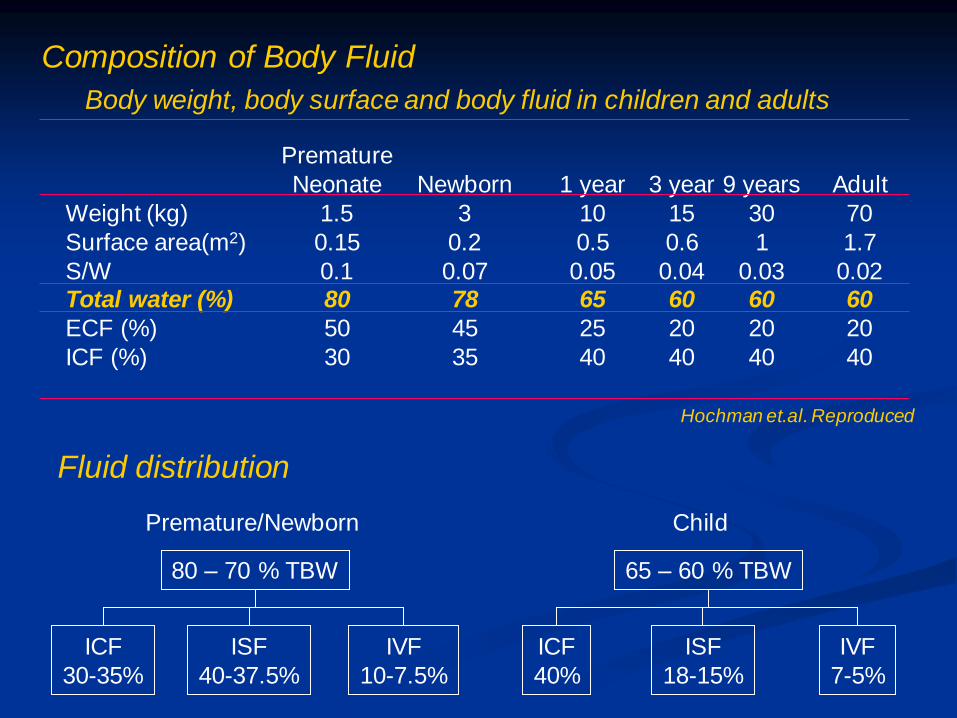
Body weight, body surface and body fluid in children and adults
Weight (kg)
Surface area(m2)
S/W Total water (%)
ECF (%)
ICF (%)
Premature
Neonate
1.5
0.15
0.1 80
50
30
Newborn
3
0.2
0.07 78
45
35
1 year
10
0.5
0.05 65
25
40
3 year
15
0.6
0.04 60
20
40
9 years
30
1
0.03 60
20
40
Adult
70
1.7
0.02 60
20
40
Hochman et.al. Reproduced
Premature/Newborn
80 – 70 % TBW
ICF
30-35%
ISF
40-37.5%
IVF
10-7.5%
Child
65 – 60 % TBW
ICF
40%
ISF
18-15%
IVF
7-5%
Fluid distribution
Composition of Body Fluid
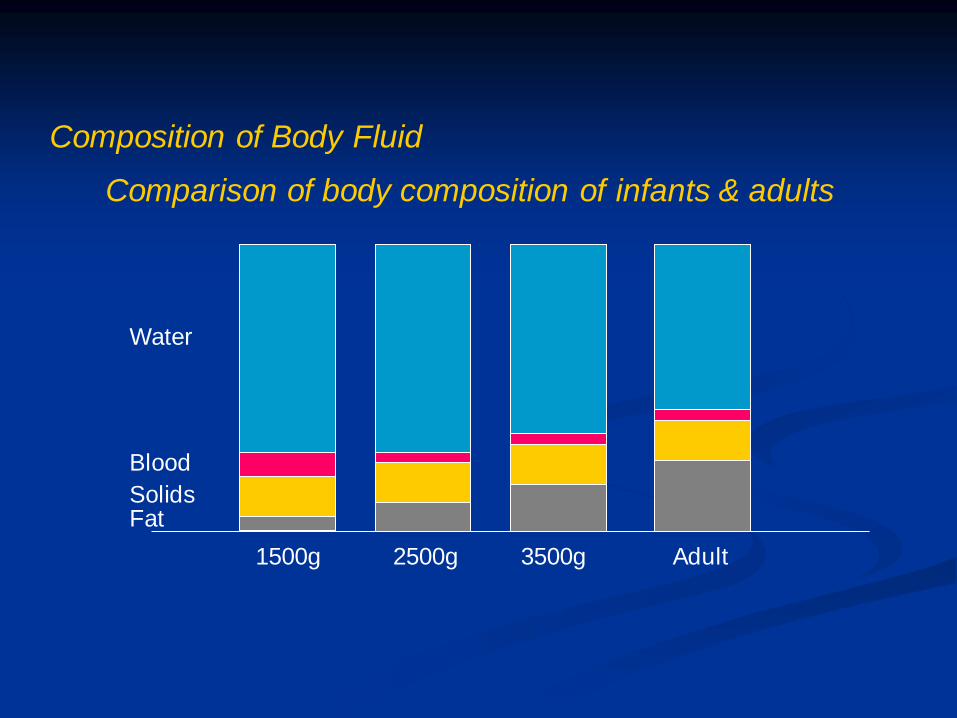
1500g 2500g 3500g Adult
Water
Blood
Solids Fat
Comparison of body composition of infants & adults
Composition of Body Fluid
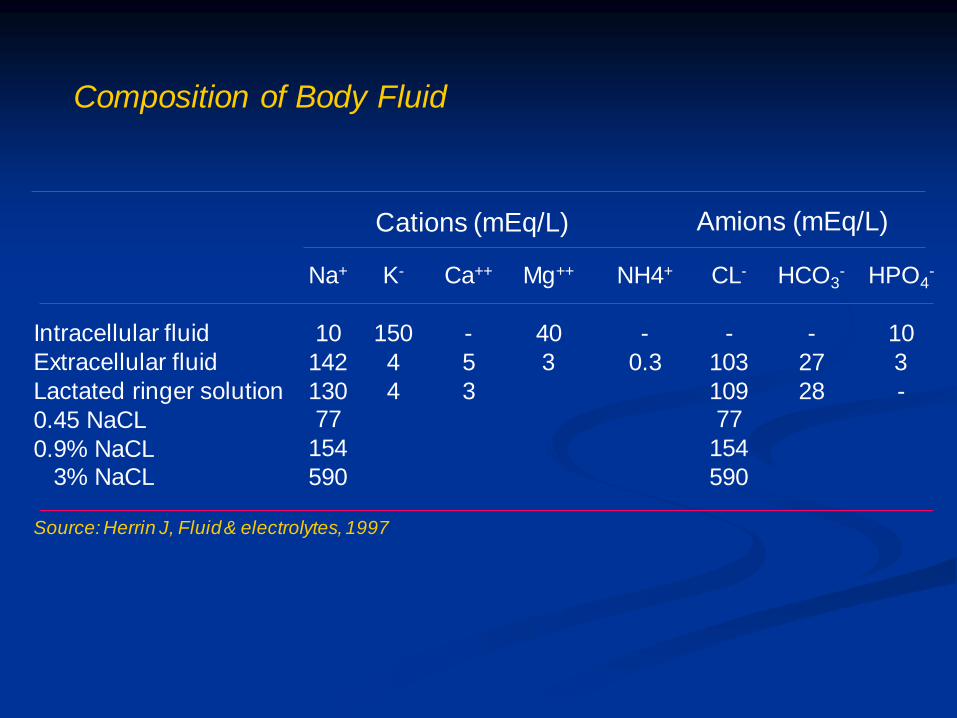
Composition of Body Fluid
Intracellular fluid
Extracellular fluid
Lactated ringer solution
0.45 NaCL
0.9% NaCL 3% NaCL
Na+
10
142
130 77
154
590
K-
150
4
4
Ca++
-
5
3
NH4+
-
0.3
CL-
-
103
109 77
154
590
HCO3-
-
27
28
HPO4-
10
3
-
Cations (mEq/L) Amions (mEq/L)
Source: Herrin J, Fluid & electrolytes, 1997
Mg++
40
3

Composition of Body Fluid
Source
Gastric
Pancreas Bile
Illeostomy
Diarrhea
Sweat
Blood Urine
Na+
50
140 130
130
50
50
140 0-100
K+(mEq/L)
10-15
5 5
15-20
35
5
4-5 20-100
CI-(mEq/L)
150
50-100 100
120
40
55
100 70-100
HCO3-
0
100 40
25-30
50
0
25 0
pH
1
9 8
8
Alkaline
7.4 4.5-8.5
Osmolality
(mOsm/L)
300
300 300
300
285-295 50-1400
Source: Herrin J, Fluid & electrolytes, 1997
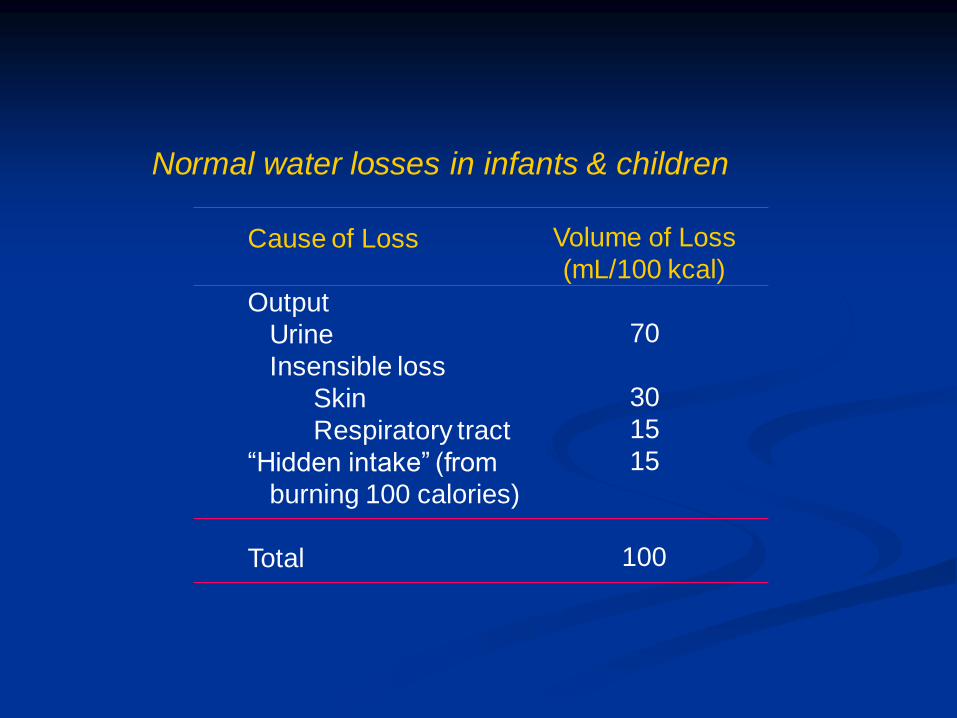
Cause of Loss
Output
Urine
Insensible loss
Skin
Respiratory tract
“Hidden intake” (from
burning 100 calories)
Total
Volume of Loss
(mL/100 kcal)
70
30
15
15
100
Normal water losses in infants & children

Perioperative fluid management
I. Maintenance
II. Deficit
III. Replacement
How should be given ?
What kind of fluid ?
How much ?

I. MAINTENANCE
1. Maintenance fluid and caloric requirements of neonate /
newborn
Age
Day 1
Day 2
Day 3
Day 4
Day 5
Vol (mL/kg/day)
50 – 80
80 – 100
100 – 120
120 – 150
150
Energy (KCal/kg/day)
40 – 50
50 – 70
70 -90
90 – 110
110 – 120

Weight (kg)
<10
10-20
>20
Day
100mL/kg
1000mL + 50 mL/kg
1500 ml + 20 mL/kg
Hour
4mL/kg
40mL + 2 mL/kg
60 mL + 1 mL/kg
Maintenance fluid requirements
2. Hourly and Daily Maintenance Fluid Requirements
of Children
For example :
a 25 kg child would required
1000 ml + 500 ml + 100 ml = 1600 ml
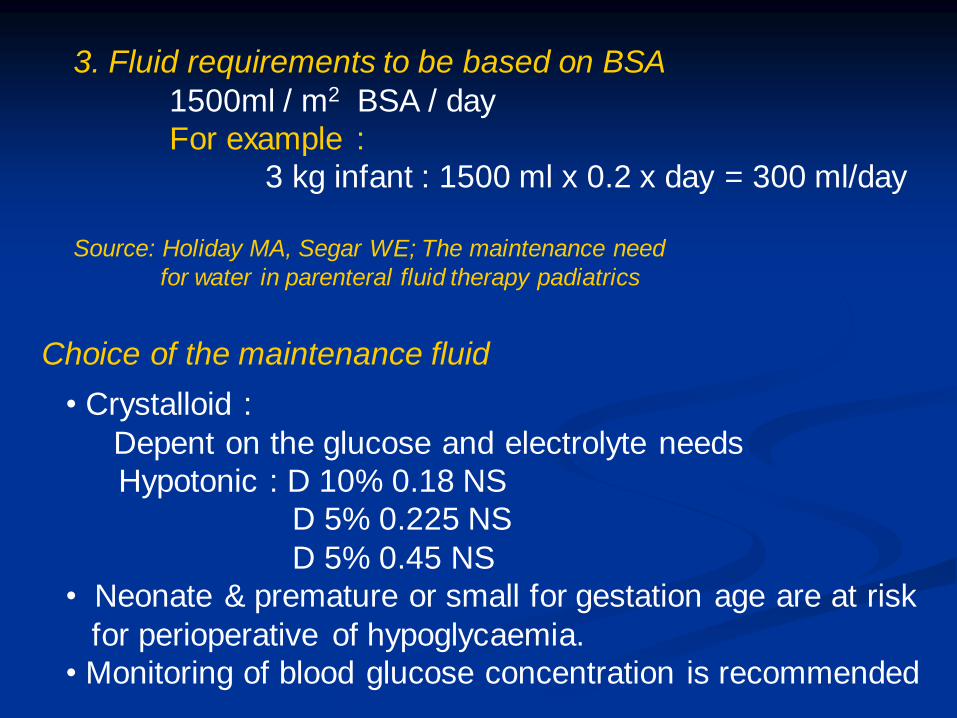
3. Fluid requirements to be based on BSA
1500ml / m2 BSA / day
For example :
3 kg infant : 1500 ml x 0.2 x day = 300 ml/day
Source: Holiday MA, Segar WE; The maintenance need
for water in parenteral fluid therapy padiatrics
Choice of the maintenance fluid
• Crystalloid :
Depent on the glucose and electrolyte needs
Hypotonic : D 10% 0.18 NS
D 5% 0.225 NS
D 5% 0.45 NS
• Neonate & premature or small for gestation age are at risk
for perioperative of hypoglycaemia.
• Monitoring of blood glucose concentration is recommended

II. DEFICIT
Preoperative fluid deficits :
Maintenance + fluid deficit
1. Fasting period
2. Hydration
3. Electrolyte imbalance
Solids
4
6
8
Age
< 6 months
6-36 months
> 36 months
Clear liquids
2
3
3
Fasting time (Hours)
1. Fasting period
Fasting (NPO) guidelines for children and adults

Replacement of fasting
Hourly fluid requirement x length of fasting (hours)
For example : a 5 kg child
5 kg x 4ml/kg/h x 4 h = 80 ml
Given : 50% in the first hour
25% in the second and third hour
Choice of fasting fluid : Crystalloid fluid
- Hypotonic solution
- Isotonic solution

Clinical findings
% body weight loss
Estimation fluid defisit
Pulse
Blood pressure
Respiration
Skin turgor
Mucous membranes
Peripheral perfusion
Urine
Mild
4-5%
40-50ml/kg
Normal
Normal
Normal
Normal
Moist
Normal
Reduced
Moderate
6-9%
60-90 ml/kg
↑, Weak
Normal of low
Deep
↓
Dry
Poor
Oliguria
Severe
>10%
100-110 ml/kg
↑↑, feeble
Reduced
Deep & rapid
↓ ↓
Very dry
Poor, cool, extremitas
Marked oliguria
Assessment of the degree of dehydration
2. Hydration :
Source: Nelson W

Management of dehidration
a. Estimated fluid deficit
b. Rehydration
For example : a 10 kg child is assessed to severe
dehydration with an estimated 10%
Dehydration 10%, 10 kg
EFD : 100 ml x 10 = 1000 ml
Initial fluid resusitation : 20ml/kg (20-30’)
Reassess the clinical state
Improved Non improvement
First 8h : 50% rest fluid deficit +
fluid maintenance
Second 16h : 50% rest fluid deficit +
fluid maintenance
Repeat : 20 ml/kg/20-30’
Resassess
- Respiration
- Circulation
- Mental status
Choice of the fluid :
Rehydration : Isotonic crystalloid
Maintenance : Hypotonic crystalloid

20
40
60
80
100
120
140
160
H+
K+
Cl+
K+
Na+
HCO3
Cl+
Cl+ K+
HCO3 Na+
Stomach Small bowel Diarrhea
Electrolyte composition of stomach, small bowel and diarrhea
3. Electrolyte im balance

Electrolytes
Sodium : 3-4 mEq/kg/day
Potassium : 2-3 mEq/kg/day
Chloride : 2-3 mEq/kg/day
Calcium : 150-500 mg/kg/day
Phosphorus : 0.5-2 mmol/kg/day
Magnesium : 0.25-0.5 mEq/kg/day
Maintenance electrolyte requirement in children
Source : J Allan Paschall
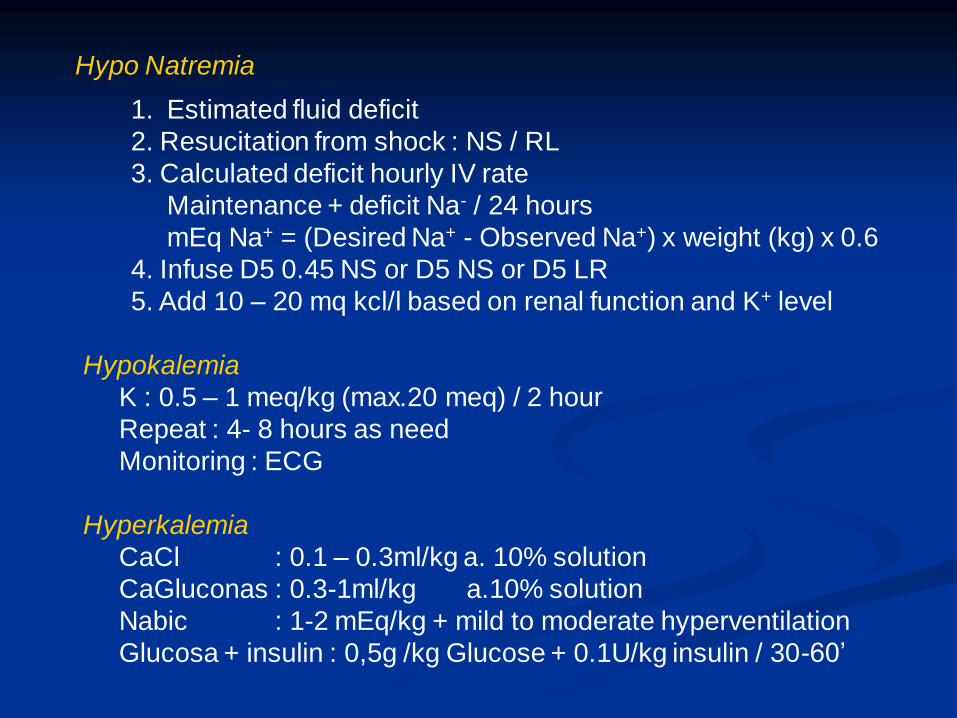
Hypo Natremia
1. Estimated fluid deficit
2. Resucitation from shock : NS / RL
3. Calculated deficit hourly IV rate
Maintenance + deficit Na- / 24 hours
mEq Na+ = (Desired Na+ - Observed Na+) x weight (kg) x 0.6
4. Infuse D5 0.45 NS or D5 NS or D5 LR
5. Add 10 – 20 mq kcl/l based on renal function and K+ level
Hypokalemia
K : 0.5 – 1 meq/kg (max.20 meq) / 2 hour
Repeat : 4- 8 hours as need
Monitoring : ECG
Hyperkalemia
CaCl : 0.1 – 0.3ml/kg a. 10% solution
CaGluconas : 0.3-1ml/kg a.10% solution
Nabic : 1-2 mEq/kg + mild to moderate hyperventilation
Glucosa + insulin : 0,5g /kg Glucose + 0.1U/kg insulin / 30-60’
III. REPLACEMENT
Intraoperative fluid management
- Maintenance
- Replacement
Replacement
- Third space lossess
- On going lossess

1. First hour, hydrating solution:
Age ≤ 3 year : 25ml/kg, plus item 3
Age ≥ 4 year :15 ml/kg, plus item 3
2. All other hours basic hourly fluid plus item 3 below
Maintenance fluid = 4 mL/kg
Maintenance + trauma = basic hourly fluid
4 mL/kg + mild trauma (2 mL/kg) = 6 mL/kg
4 mL/kg + moderate trauma (4 mL/kg) = 8 mL/kg
4 mL/kg + maximal trauma (6 mL/kg) = 10 mL/kg
3. Blood replacement with 3:1 volume replacement with crystalloid
or colloid, or blood
Guidelines for intraoperative fluids in pediatric patiens
From: Berry Reproduced
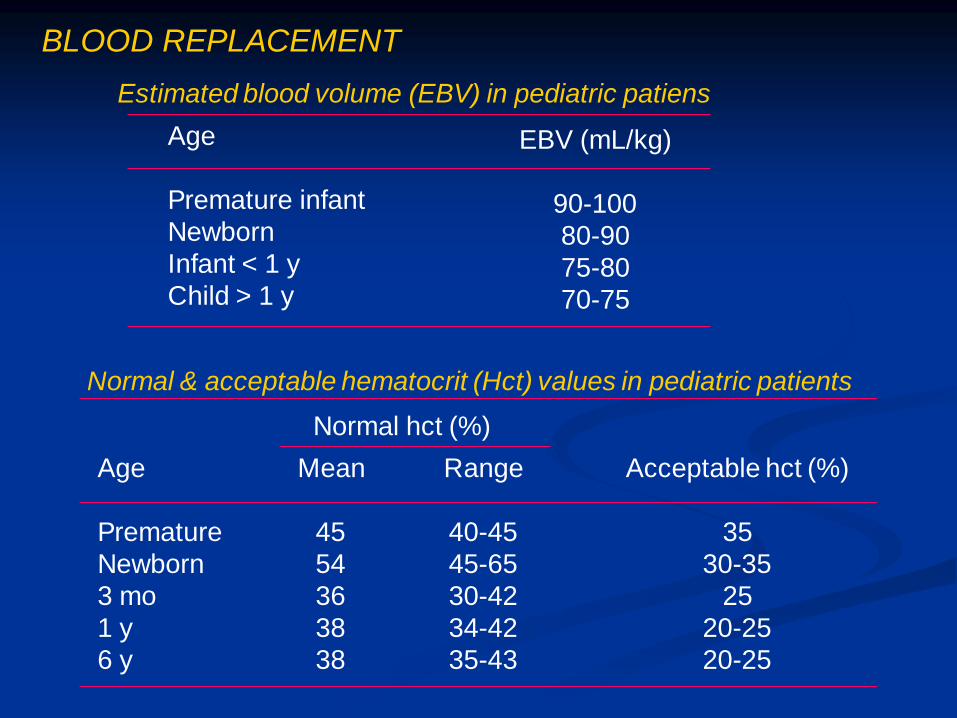
Age
Premature infant
Newborn
Infant < 1 y
Child > 1 y
EBV (mL/kg)
90-100
80-90
75-80
70-75
Estimated blood volume (EBV) in pediatric patiens
BLOOD REPLACEMENT
Age
Premature
Newborn
3 mo
1 y
6 y
Mean
45
54
36
38
38
Range
40-45
45-65
30-42
34-42
35-43
Acceptable hct (%)
35
30-35
25
20-25
20-25
Normal hct (%)
Normal & acceptable hematocrit (Hct) values in pediatric patients
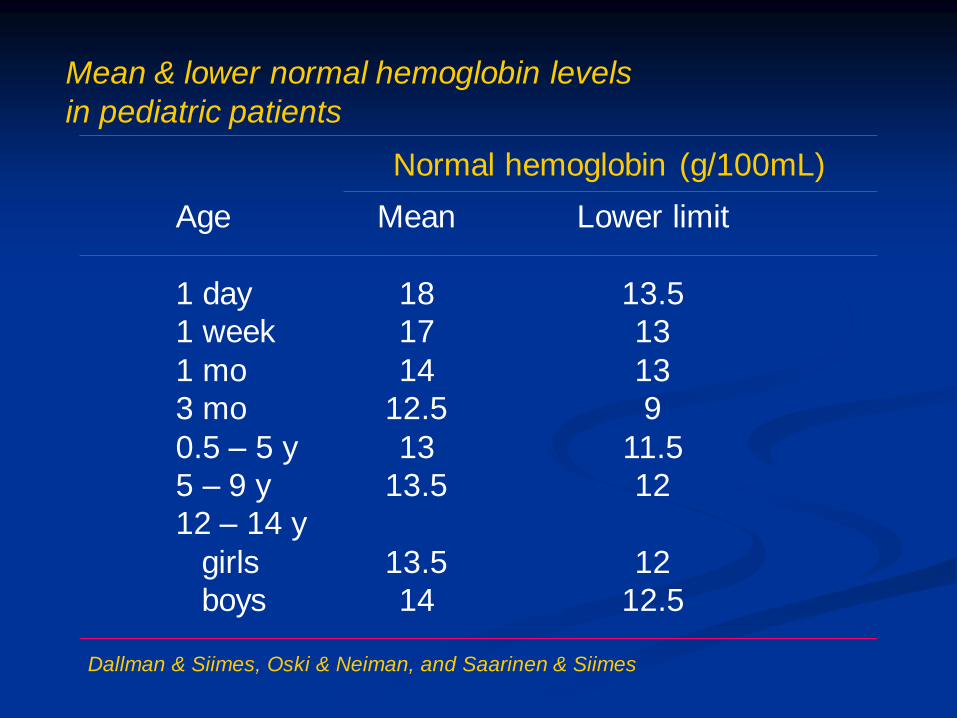
Age
1 day
1 week
1 mo
3 mo
0.5 – 5 y
5 – 9 y
12 – 14 y
girls
boys
Mean
18
17
14
12.5
13
13.5
13.5
14
Lower limit
13.5
13
13
9
11.5
12
12
12.5
Normal hemoglobin (g/100mL)
Mean & lower normal hemoglobin levels
in pediatric patients
Dallman & Siimes, Oski & Neiman, and Saarinen & Siimes

1. Blood required =
Hct 1 – Hct 2
Hct 3
X EBV
2. Blood required (PRC) = (Hct 1 – Hct 2) x body weight (kg) x 1.5
(WB) = (Hct 1 – Hct 2) x body weight (kg) x 2.5
Hct1 : Haematocrit before transfusion, the measured
haematocrit
Hct2 : Haematocrit required after transfusion, the desired
haematocrit
Hct3 : Haematocrit of the blood to be given (60% if packed cells)
EBV : Estimated blood volume
BLOOD REPLACEMENT TO USE HAEMOTOCRIT LEVEL
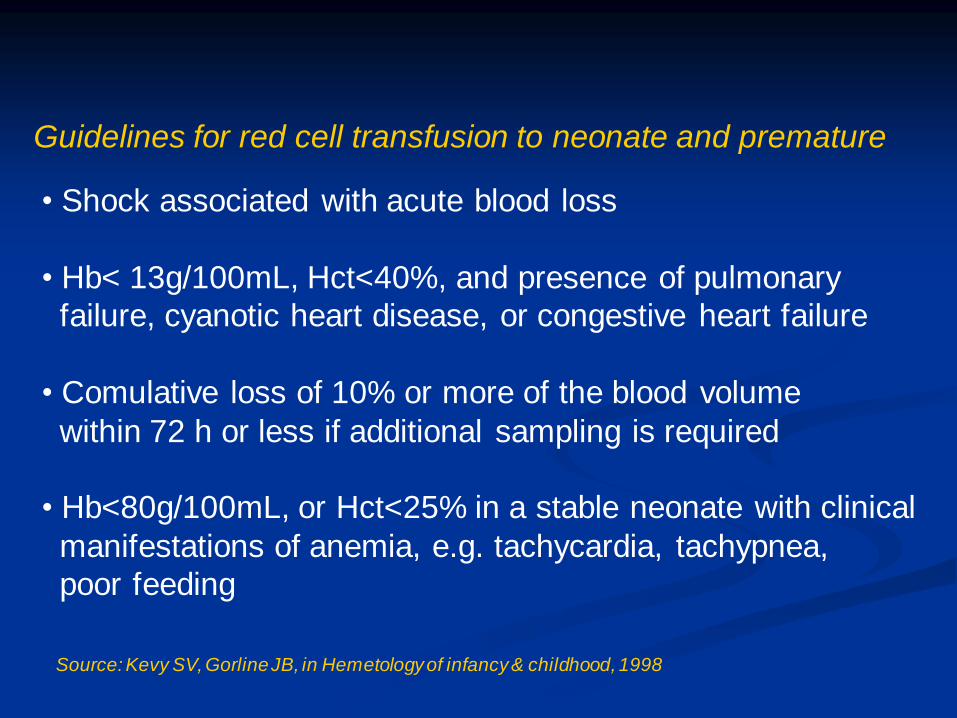
Guidelines for red cell transfusion to neonate and premature
• Shock associated with acute blood loss
• Hb< 13g/100mL, Hct<40%, and presence of pulmonary
failure, cyanotic heart disease, or congestive heart failure
• Comulative loss of 10% or more of the blood volume
within 72 h or less if additional sampling is required
• Hb<80g/100mL, or Hct<25% in a stable neonate with clinical
manifestations of anemia, e.g. tachycardia, tachypnea,
poor feeding
Source: Kevy SV, Gorline JB, in Hemetology of infancy & childhood, 1998

Postoperative Fluid Management
• Maintenance fluid
• Replacement of fluid deficit
• Replacement of other losses
- Chest tube
- Nasogastric tube
- Weeping incision
- Continous slow bleeding
• Correction of electrolyte inbalance
• Maintenance fluid requirement on the first most operation
day are decreased to 2/3 of the usual daily amount

Conclusion
• Fluid therapy for pediatric patients must be based on the knowledge
of the fluid and electrolyte needs in healthy infants and children
on physiologic responses to the surgical procedure
• Formula for fluid therapy are guidelines that need to be revaluated
according the patients response
• Even more than in the adult, improper fluid management in
infants and children can cause life threatening consequences
• The inadverten administration of a seemingly minuscule excess
of fluid may couse problems.
For example :
100 ml fluid in full term neonate is comparable to 1 to 2
liter excess in an dault
