perioperative use of arginine-supplemented diets: a ... · perioperative use of...
TRANSCRIPT

COLLECTIVE REVIEW
Perioperative Use of Arginine-supplemented Diets:A Systematic Review of the EvidenceJohn W Drover, MD, FRCSC, Rupinder Dhaliwal, RD, Lindsay Weitzel, PhD, Paul E Wischmeyer, MD,Juan B Ochoa, MD, FACS, Daren K Heyland, MD, FRCPC, MSC
Infections are the most frequent cause of morbidity aftersurgery and up to 54% of all hospital-acquired infectionsoccur in high-risk surgical populations.1 Infections result inprolongation of hospital stay2 and increased health carecosts by up to $10 billion per year in the United Statesalone.3 Multifaceted efforts to prevent infection are an es-sential component of any surgical practice.4
Surgical stress predisposes patients to immune dysfunc-tion, placing them at higher risk of infection, risks that areincreased even more if the patient is malnourished beforesurgical insult.5 Various nutrient and nutritional strategieshave been studied to evaluate their effect on immune functionand clinical outcomes. One pharmaconutrient that has beenthe center of much debate in the literature is arginine andarginine-supplemented nutritional formulas.6-9 Arginine is anamino acid involved in multiple metabolic processes. It is aprecursor of the formation of polyamines and hydroxypro-line, which is important for connective tissue repair, and isthe precursor for the formation of nitric oxide, an impor-tant signaling molecule.10 In addition to these vital roles,arginine is an essential metabolic substrate for immunecells and required for normal lymphocyte function.11
Arginine deficiency after surgical stress was reportedmore than 30 years ago, although the mechanisms behindthis have until recently remained unknown.11,12 More than20 years ago, supraphysiologic concentrations of argininewere added to the diets of critically ill and surgical patients.These diets were aimed at “enhancing immune function”and also contained increased amounts of omega-3 fattyacids, nucleotides, and other nutrients. These nutrients
were eventually incorporated into commercial diets with-out a rigorous evaluation of their individual effects or sideeffects in different patient populations. In 2001, Heylandand others reported a meta-analysis suggesting that thesearginine-supplemented diets were not beneficial in criti-cally ill patients and could even potentially adversely affectoutcomes in this population.9 In contrast, patients under-going elective surgery appeared to exhibit a benefit, with apossible decreased rate of infection. The treatment effect ofthese diets was systematically different in critically ill pa-tients compared with elective surgery patients, and it be-came apparent that a dedicated meta-analysis should bedone separately for patients undergoing elective surgery.Although subsequent meta-analyses have recently beendone,13,14 they were limited in scope, not including all per-tinent articles, included unpublished and duplicate publi-cations, and combined studies with different study designsin evaluating the role of perioperative nutrition. The pur-pose of this review is to provide an up-to-date systematicreview on all studies of arginine-supplemented diets inelective surgical patients. With a larger database, we mightbe able to shed some light on the perioperative role of suchdiets.
METHODSStudy identificationWe conducted a systematic review of the published litera-ture to identify all relevant trials. Using text word or MeSHheadings containing “randomized,” “blind,” “clinicaltrial,” “nutrition,” “arginine,” “glutamine,” “omega-3 fattyacids,” “fish oil,” “nucleotides,” “immune,” “immunonu-trition,” we performed computerized searches for relevantarticles on MEDLINE, EMBASE, BIIOSIS, CINAHLelectronic databases Cochrane Controlled Trials Registerfrom 1990 to March 2010. We also searched our personalfiles and reference lists of review articles and original stud-ies. There were no language restrictions.
Study selection criteriaCitations were classified as primary studies, review articles,or other. All primary studies were retrieved and reviewedindependently. We included primary studies if they wererandomized clinical trials (RCTs); studied elective surgical
Disclosure Information: Dr Heyland received a research grant as the prin-cipal investigator and an honorarium as a speaker for Nestle. Dr Ochoa wasa paid consultant for Nestle until July 2010, and receives a salary as MedicalScientific Director for Nestle since July 2010. All other authors have noth-ing to disclose.
Received August 12, 2010; Revised October 1, 2010; Accepted October 26,2010.From the Departments of Surgery (Drover) and Medicine (Heyland), ClinicalEvaluation Research Unit (Dhaliwal, Heyland), Kingston, Ontario, Canada,Department of Anesthesiology, University of Colorado School of Medicine,Aurora, CO (Weitzel, Wischmeyer), Department of Surgery, University ofPittsburgh, Pittsburgh, PA (Ochoa).Correspondence address: Daren Keith Heyland, MD, FRCPC, MSc, Angada4, Kingston General Hospital, 76 Stuart Street, Kingston, Ontario K7L 2V7,Canada. email: [email protected]
385© 2011 by the American College of Surgeons ISSN 1072-7515/11/$36.00Published by Elsevier Inc. doi:10.1016/j.jamcollsurg.2010.10.016

in adults; compared enteral nutrition supplemented witharginine with or without other immune-modulating agentswith standard enteral nutrition; and included clinically im-portant outcomes such as mortality, infectious complica-tions, and hospital length of stay.
To select studies with the greatest validity with respect torelative treatment effect, we included only RCTs. We ex-cluded the studies reporting only nutritional or immuno-logical outcomes. We defined elective surgical patients asthose undergoing a scheduled surgical procedure whetherthey were cared for in a critical care environment or not.We excluded studies of critically ill patients who underwenturgent or emergent operations (ie, trauma, ruptured aneu-rysms, etc.).
Using a scoring system that we have used in previousstudies,15 we scored the methodological quality of individ-ual studies considering the extent to which randomizationwas concealed, if the study was double-blinded and theanalysis was based on the intention-to-treat principle andother key features of high-quality studies, and abstractednecessary data in duplicate and independently. Disagree-ment in the individual scores of each of the categories (ie, 0,1, or 2) was resolved by consensus (see Appendix, availableonline only, for methodological scoring tool). We at-tempted to contact the authors of included studies andrequested additional information not contained in pub-lished articles.
Data synthesisAmong the primary outcomes of interest was the numberof patients with new infectious complications. We useddefinitions of infectious complications as defined by theoriginal authors, which usually included pneumonia, intra-abdominal abscess, sepsis, line sepsis, wound infection,anastomotic leak, fistula formation, and urinary tract in-fection. We included only infectious complications whenwe could abstract the number of patients with such com-plications. Secondary outcomes included hospital length ofstay and mortality. We combined data from all studies toestimate the pooled risk ratio (RR) with 95% confidenceintervals for death and infectious complications and overallweighted mean difference (WMD) with 95% confidenceintervals for hospital length of stay.
All analyses, except the test for asymmetry, were con-ducted using Review Manager 5.16 Pooled RRs were calcu-lated using the Mantel-Haenszel estimator and WMDswere estimated by the inverse variance approach. The ran-dom effects model of DerSimonian and Laird was used toestimate variances for the Mantel-Haenszel and inversevariance estimators.17 RRs are undefined and excluded forstudies with no event in either arm. When only 1 group has0 events then ½ was added to each cell to allow estimation.The presence of heterogeneity was tested by a weightedMantel-Haenszel chi-square test and quantified by the I2
statistic as implemented in Review Manager 5.18 The pos-sibility of publication bias was assessed by generating fun-nel plots and testing asymmetry of outcomes using meth-ods proposed by Rucker and colleagues.19 We consideredp ! 0.05 to be statistically significant.
We combined experimental arms for the purposes of theoverall analysis for studies that randomized patients tomore than 2 groups of interest. On review of the data set,we identified 2 studies that had used considerable amountsof glycine in an effort to create isonitrogenous enteral for-mulas in the control groups.20,21 To explore whether thisamino acid supplementation affected the results of themeta-analysis, a sensitivity analysis was undertaken by re-peating the analysis with these studies excluded.
Earlier hypotheses testingIn addition to the primary outcomes of interest in theoverall patient groups, a priori, we identified 4 questions orsubgroup analysis that we wished to explore within thecontext of the data set. The first was an analysis by type ofsurgery. As a larger number of studies were done in thecontext of gastrointestinal (GI) surgery, we planned tocompare studies that principally enrolled patients havingGI surgery and those having other surgical procedures. Sec-ond, within the group of patients having GI surgery, thereseemed to be 2 different cohorts. We compared outcomesfor those having only upper GI surgery with those studiesthat included only patients having lower GI surgery withthose with mixed upper and lower GI surgery. Third, manyformulations of arginine-supplemented diets have beenstudied. These have varying concentrations of arginine,and contain different additional supplemental agents. Themost frequently used product in these studies is Impact(Nestle, Inc). We compared studies that used Impact in theexperimental group with those that used other arginine-supplemented formulations. Finally, one of the outstand-ing issues for perioperative supplementation is whether it ismore important to give the supplements before or after thesurgery, or both. Unfortunately, there has been no consis-tent study design used to answer this question. We groupedlike studies based on whether the experimental diet was
Abbreviations and AcronymsGI " gastrointestinalMDSC " myeloid-derived suppressor cellsRCT " randomized clinical trialsRR " risk ratioWMD " weighted mean difference
386 Drover et al Arginine Supplementation in Surgical Patients J Am Coll Surg
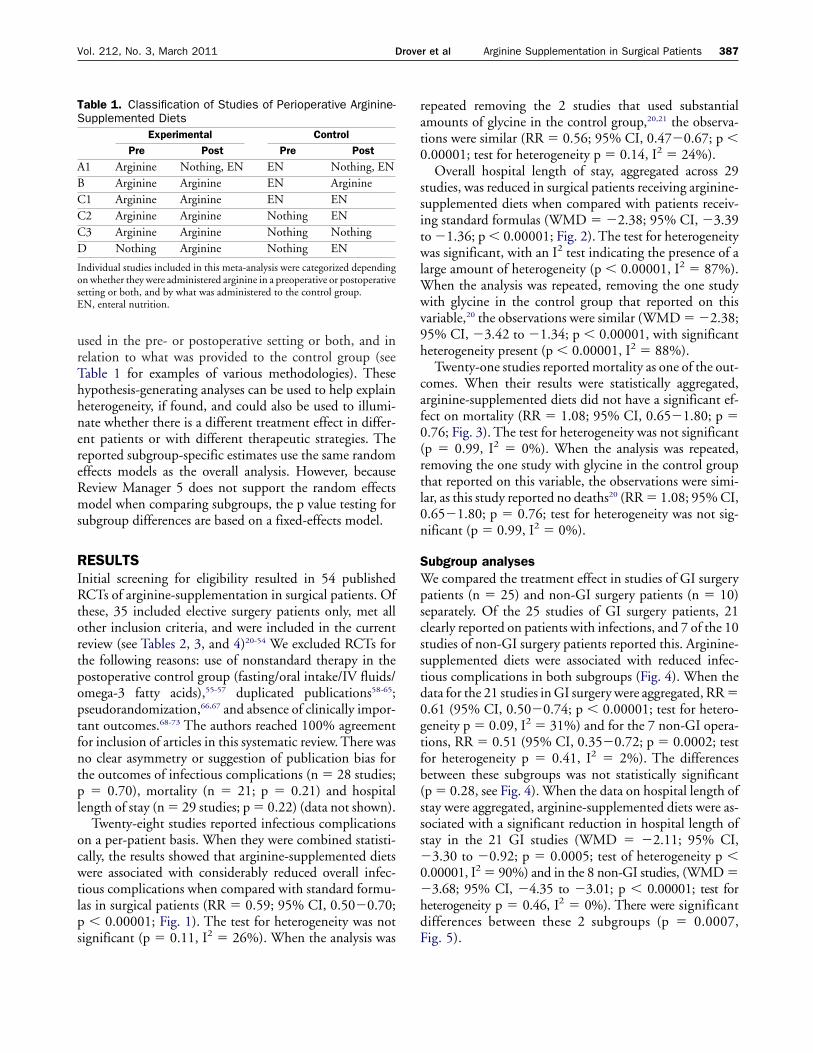
used in the pre- or postoperative setting or both, and inrelation to what was provided to the control group (seeTable 1 for examples of various methodologies). Thesehypothesis-generating analyses can be used to help explainheterogeneity, if found, and could also be used to illumi-nate whether there is a different treatment effect in differ-ent patients or with different therapeutic strategies. Thereported subgroup-specific estimates use the same randomeffects models as the overall analysis. However, becauseReview Manager 5 does not support the random effectsmodel when comparing subgroups, the p value testing forsubgroup differences are based on a fixed-effects model.
RESULTSInitial screening for eligibility resulted in 54 publishedRCTs of arginine-supplementation in surgical patients. Ofthese, 35 included elective surgery patients only, met allother inclusion criteria, and were included in the currentreview (see Tables 2, 3, and 4)20-54 We excluded RCTs forthe following reasons: use of nonstandard therapy in thepostoperative control group (fasting/oral intake/IV fluids/omega-3 fatty acids),55-57 duplicated publications58-65;pseudorandomization,66,67 and absence of clinically impor-tant outcomes.68-73 The authors reached 100% agreementfor inclusion of articles in this systematic review. There wasno clear asymmetry or suggestion of publication bias forthe outcomes of infectious complications (n " 28 studies;p " 0.70), mortality (n " 21; p " 0.21) and hospitallength of stay (n " 29 studies; p " 0.22) (data not shown).
Twenty-eight studies reported infectious complicationson a per-patient basis. When they were combined statisti-cally, the results showed that arginine-supplemented dietswere associated with considerably reduced overall infec-tious complications when compared with standard formu-las in surgical patients (RR " 0.59; 95% CI, 0.50#0.70;p ! 0.00001; Fig. 1). The test for heterogeneity was notsignificant (p " 0.11, I2 " 26%). When the analysis was
repeated removing the 2 studies that used substantialamounts of glycine in the control group,20,21 the observa-tions were similar (RR " 0.56; 95% CI, 0.47#0.67; p !0.00001; test for heterogeneity p " 0.14, I2 " 24%).
Overall hospital length of stay, aggregated across 29studies, was reduced in surgical patients receiving arginine-supplemented diets when compared with patients receiv-ing standard formulas (WMD " #2.38; 95% CI, #3.39to #1.36; p ! 0.00001; Fig. 2). The test for heterogeneitywas significant, with an I2 test indicating the presence of alarge amount of heterogeneity (p ! 0.00001, I2 " 87%).When the analysis was repeated, removing the one studywith glycine in the control group that reported on thisvariable,20 the observations were similar (WMD " #2.38;95% CI, #3.42 to #1.34; p ! 0.00001, with significantheterogeneity present (p ! 0.00001, I2 " 88%).
Twenty-one studies reported mortality as one of the out-comes. When their results were statistically aggregated,arginine-supplemented diets did not have a significant ef-fect on mortality (RR " 1.08; 95% CI, 0.65#1.80; p "0.76; Fig. 3). The test for heterogeneity was not significant(p " 0.99, I2 " 0%). When the analysis was repeated,removing the one study with glycine in the control groupthat reported on this variable, the observations were simi-lar, as this study reported no deaths20 (RR " 1.08; 95% CI,0.65#1.80; p " 0.76; test for heterogeneity was not sig-nificant (p " 0.99, I2 " 0%).
Subgroup analysesWe compared the treatment effect in studies of GI surgerypatients (n " 25) and non-GI surgery patients (n " 10)separately. Of the 25 studies of GI surgery patients, 21clearly reported on patients with infections, and 7 of the 10studies of non-GI surgery patients reported this. Arginine-supplemented diets were associated with reduced infec-tious complications in both subgroups (Fig. 4). When thedata for the 21 studies in GI surgery were aggregated, RR "0.61 (95% CI, 0.50#0.74; p ! 0.00001; test for hetero-geneity p " 0.09, I2 " 31%) and for the 7 non-GI opera-tions, RR " 0.51 (95% CI, 0.35#0.72; p " 0.0002; testfor heterogeneity p " 0.41, I2 " 2%). The differencesbetween these subgroups was not statistically significant(p " 0.28, see Fig. 4). When the data on hospital length ofstay were aggregated, arginine-supplemented diets were as-sociated with a significant reduction in hospital length ofstay in the 21 GI studies (WMD " #2.11; 95% CI,#3.30 to #0.92; p " 0.0005; test of heterogeneity p !0.00001, I2 " 90%) and in the 8 non-GI studies, (WMD "#3.68; 95% CI, #4.35 to #3.01; p ! 0.00001; test forheterogeneity p " 0.46, I2 " 0%). There were significantdifferences between these 2 subgroups (p " 0.0007,Fig. 5).
Table 1. Classification of Studies of Perioperative Arginine-Supplemented Diets
Experimental ControlPre Post Pre Post
A1 Arginine Nothing, EN EN Nothing, ENB Arginine Arginine EN ArginineC1 Arginine Arginine EN ENC2 Arginine Arginine Nothing ENC3 Arginine Arginine Nothing NothingD Nothing Arginine Nothing EN
Individual studies included in this meta-analysis were categorized dependingon whether they were administered arginine in a preoperative or postoperativesetting or both, and by what was administered to the control group.EN, enteral nutrition.
387Vol. 212, No. 3, March 2011 Drover et al Arginine Supplementation in Surgical Patients

Table2.
Random
izedS
tudiesEvaluating
PreoperativeN
utritionin
ElectiveS
urgeryPatients
Firstauthor,
yearPopulation
Methodsscore
blinding
InterventionM
ortalityInfections
Hospitalstay,
d
Experimental
Control
Experimental
Control
Experimental
Control
Experimental
Control
n%
n%
n%
n%
Preoperativearginine
versusnoarginine
Wachtler,1995
50U
GIsurgery
(n"
40)5
YesIm
pactpreop$
5d
%hospital
foodIsoenergetic
supplement
preop%
hospitalfood
2/2010
2/2010
5/2025
5/2025
NR
NR
McC
arter,199827
UG
Icancer(n"
51)7
Yes1)Form
ulaw
/arginine750
mL/d
$7
dpreop
2)Formula
with
arginine%
omega-3
fattyacids(Im
pact)$
7d
preop
3)Standardform
ula$
7d
preop1)1/142)0/13
703)0/11
01)4/142)5/13
29383)2/11
181)15
&2.4
2)17&
3.73)13
&1.7
Braga,2002
34C
olorectalcancer(n
"200)
12N
o2)Im
pactpreop1
L/d$
5d
3)IsoC/IsoN
formula
preop1
L/d$
5d
2)0/503)0/50
2)6/5012
3)16/5032
2)9.5&
2.93)12
&4.5
Braga,2002
35U
GIand
LGIcancer
malnourished
(n"
150)
11N
o2)Im
pactpreop$
7d
%EN
standardpostop
3)IsoC/IsoN
standardEN
postop2)1/50
23)2/50
42)8/50
163)12/50
242)13.2
&3.5
3)15.3&
4.1
Gianotti,2002
37U
GI
%LG
Icancer!
10%w
eightloss(n
"305)
8N
o1)Im
pactpreop$
5d
3)None
pre/postop1)1/102
3)1/1021
1)14/10214
3)31/10230
1)11.6&
4.73)14
&7.7
Xu,2006
43C
olorectalandgastric
GIcancer(n
"60)
11N
oIm
pactpreop,standardEN
postopIsoC
/IsoNstandard
ENform
ulapostop
NR
NR
NR
NR
9&
3.212
&3.7
Okam
oto,200953
Gastric
cancerpatients(n
"60)
10N
oIm
pactpreop$
7d
%standard
postopStandard
ENpreop
$7
d%
standardpostop
NR
NR
2/307
8/3028
23.8&
16.625
&10.6
Perioperativearginine
versuspreoperativestandard
andpostoperative
arginine
Giger,2007
51Stom
ach,pancreascancer(n
"46)
10N
o1)Im
pactx5
dpreop
%7d
postop2)Im
pactPlus$
2dpreop
%7
dpostop
3)Impact$
7dpostop
1)1/142)0/17
3)0/151)2/142)5/17
3)10/151)13.7
&2.3
2)14.1&
1.33)23.1
&3.6
EN,enteralnutrition;G
I,gastrointestinal;IsoN,isonitrogenous;IsoC
,isocaloric;LGI,low
ergastrointestinal;N
R,notreported;postop,postoperative;preop,preoperative;U
GI,
uppergastrointestinal.M
cCarter
27:D
ataforgroups1
and2
combined
inthe
meta-analysis.
Braga
34,3
5:Data
forGroup
1(receiving
Impactperioperatively)show
nin
comparison
C2.
Gianotti 3
7:Data
forGroup
2(receiving
Impactperioperatively)show
nin
comparison
C3.
388DroveretalArginineSupplementationinSurgicalPatientsJAmCollSurg

Table3.
Random
izedS
tudiesEvaluating
PerioperativeArginine
inElective
Surgery
PatientsC
:Perioperative
arginine
Firstauthor,
yearPopulation
Methodsscore
blindingIntervention
experimentalcontrol
Mortality
experimental
control,n
(%)
Infectionsexperim
entalcontrol,
n(%
)H
ospitalstay(d)
Experimentalcontrol
C1:Perioperative
arginineversusperioperative
standard
Braga,1999
28Stom
ach,pancreas,colorectalcancer(n
"206)
12Yes
Impactpreop
%standard
ENpostop
IsoC/IsoN
ENpreop
%standard
ENpostop
0/102(0)
1/104(14)
14/102(14)
31/104(30)
11.1&
4.4(102)
12.9&
4.6(104)
Senkal,199929
UG
Icancer(n"
178)11Yes
Impactpre-
%postop
StandardEN
pre-%
postopIsoN
/IsoCN
RN
R10/78
(13)18/76
(24)22.2
&4.1
(78)25.8
&3.8
(76)
Snyderman,1999
30H
eadand
neckcancer(n
"136)
8Yes
Impactpre-
%postop
StandardEN
formulas
pre-andpost(m
ainlyreplete)
0/82(0)
0/47(0)
19/82(23)
19/47(40)
15.3&
9.1(82)
17.4&
11.9(47)
Tepaske,2001
32C
ardiacsurgery
(n"
50)7
YesIm
pact5#10
dpre-
%postop
StandardIsoC
al/IsoN5#
10d
preop1/23
(4)1/22
(5)4/23
(17)12/22
(55)7.5
(IQR
7#108)
9.6&
5.39.5
(IQR
6#12)
11.7&
12
vanB
okhorst-De
vanderSchueren,2001
33
Head
andneck
cancer,m
alnourished(n
"56)
6Yes
1)Arginine
formula
(12.5g/L)Pre-
%postop
2)StandardEN
pre%
post1)2/17
(12)2)1/15
(7)N
RN
R1)31
&23
2)46&
30
Finco,200742
Colon
disease(n
"28)
9N
oIm
pact%low
-fiberdiet750
mL/d,6
dpre
%3
dpost
StandardEN
%low
-fiberdiet$
6d
pre-%
3d
standardpost-EN
NR
NR
NR
NR
7.7&
2.36.8
&1.6
Sakurai,200745
Esophagectomy
(n"
30)6
No
Impact3
dpre-
%14
dpost
IsoCEnsure
3d
pre%
14d
postN
RN
RN
RN
R26.6
&14
31.3&
1.6
Tepaske,2007
22C
ardiopulmonary
bypass(n
"70)
10Yes
1)Impact5#
10d
pre%
postop2)Im
pact%glycine,
5#10
dpre-
%postop
3)IsoC/IsoV
olControl
5#10
dpreop
NR
NR
1)4/24(17)
2)5/22(23)
12/24(50)
1)6.5(IQ
R6-8)
2)7(IQ
R6-13)
8(IQ
R6-10)
Celik,2009
54G
YNcancer(n
"50)
8N
oIm
pactpreop$
2days
%7
dpostop
StandardEN
pre-%
postop0/25
(0)0/25
(0)1/25
(4)7/25
(28)4.1
&1.3
7.8&
1.2
C2:Perioperative
arginineversusnothing
preoperativeand
postoperativestandard
vanB
okhorst-De
vanderSchueren,2001
33
Head
andneck
cancer,m
alnourished(n
"49)
6Yes
1)Arginine
formula
(12.5g/L)pre-
%postop
3)StandardIsoC
al/IsoNEN
postoponly
1)2/17(12)
3)0/17(0)
NR
NR
1)31&
233)41
&32
Braga,2002
35U
GIand
LGIcancer,
malnourished
(n"
150)11N
o1)Im
pactpreop$
7d
%Im
pactpostop3)IsoC
/IsoNEN
postop1)0/50
(0)3)2/50
(4)1)5/50
(10)3)12/50
(24)1)12
&3.8
3)15.3&
4.1
C3:Perioperative
arginineversusnone
Braga,2002
34C
olorectalcancer(n"
200)12N
o1)Im
pactpreop1
L/d$
5d
%postop
4)None
pre-/postop1)1/50
(2)4)1/50
(2)1)5/50
(10)4)15/50
(30)1)9.8
&3.1
4)12.2&
3.9
Gianotti,2002
37U
GI
%LG
Icancer!
10%w
eightloss(n"
305)8
No
2)Impactpreop
$5
d%
postop3)N
onepre-/postop
2)2/101(2)
3)1/102(1)
2)16/101(16)
3)31/102(30)
2)12.2&
4.13)14
&7.7
EN,enteralnutrition;G
YN,gynecological;IQ
R,interquartilerange;IsoN
,isonitrogenous;IsoC,isocaloric;IsoVol,isovolem
ic;LGI,low
ergastrointestinal;NR
,notreported;postop,postoperative;preop,preoperative;U
GI,uppergastrointestinal.
14:Snyderman
30:D
ataforgroups1
and2
combined
(Impactpre
%post)and
compared
with
groups3and
4com
bined(standard
pre%
post).15a:van
BokhorstD
evan
derSchueren33:D
ataforG
roup3
(controlnothingpreop
andEN
postop)appearsinC
2.Tepaske
22:G
roups1and
2com
binedin
them
eta-analysis.C
elik54:Infection
datanotincluded
inm
eta-analysisasonlyreported
aswound
infection,nottotalnumberofinfections.
vanB
okhorstDe
vanderSchueren
33:D
ataforG
roup2
(ControlEN
pre-andpostop)appearsin
C1.
Braga
35:D
ataforG
roup2
(Impactpreop
andstandard
postop)appearsinA
1.G
ianotti 37:D
ataforG
roup1
(Impactpreop)appearsin
A1.
389 Vol.212,No.3,March2011DroveretalArginineSupplementationinSurgicalPatients

Table4.
Random
izedS
tudiesEvaluating
PostoperativeArginine
inElective
Surgery
Patients
Firstauthor,
yearPopulation
MethodsScore
Blinding
InterventionM
ortality,n
(%)
Infections,n
(%)
Hospitalstay,
d
Experimental
Control
Experimental
Control
Experimental
Control
Experimental
Control
Postoperativearginine
versusstandard
Daly,1990
21U
GIsurgery
(n"
30)4
No
Arginine
25g/d
with
modular
feedpostop
Glycine
43g/d
modularfeed
postopN
RN
R10/16
(63)9/14
(64)N
RN
R
Daly,1992
23U
GIcancer(n
"85),32%
weightloss
'10%
10N
oIm
pactviaN
CJ
postopO
smolite
HN
viaN
CJ
non-IsoN
postop2/41
(5)0/44
(0)5/41
(12)13/44
(30)18.8
&11.1
(41)20.4
&9.6
(44)
Daly,1995
24Esophageal,pancreatic
andgastric
cancer(n"
60),37%!
10%usualw
eightloss
9Yes
1)Impactpostop
andas
outpatient2)Im
pactpostopsm
allbowel
3)Traum
acalpostopand
asoutpatient
4)Traum
acalpostopsm
allbow
elIsoN/IsoC
1/30(3)
2/30(7)
1/30(10)
9/30(30)
16&
0.9(30)
22&
2.9(30)
Braga,1996
20Pancreatic,gastric
cancer(n"
60),50%w
ithw
eightloss'
10%
9N
oIm
pactpostopSam
eEN
formula
w/o
arginineand
omega-3
fattyacids,w
ithglycine
%om
ega-6fatty
acidsIsoNpostop
0/20(0)
0/20(0)
2/20(10)
3/20(15)
13.2&
6.1(20)
15.5&
3.5(20)
Schilling,199625
GIcancer(upperand
lower)(n
"45),body
massindex
23#24
6N
oIm
pactpostopvia
nasojejunalFresubin
(StandardEN
)vianasojejunalpostop
NR
NR
3/14(21)
6/14(43)
14.7&
4(14)
20.3&
13(14)
Senkal,199726
UG
Icancer(n"
154)N
RIndex
98#100
8Yes
Impact(m
in3.0
L/day)viajejunum
postopStandard
EN(m
in3.0
L/day)via
jejunumIsoC
/IsoN
postop
3/77(4)
2/77(3)
17/77(22)
24/77(31)
27&
2.3(77)
30.6&
3.1(77)
Gianotti,2000
36Pancreatic
duodenectomy,40%
,m
alnourished(n
"212)
10N
o1)Im
pactpostop2)Standard
ENform
ulapostop
2/71(3)
1/73(1)
6/71(8)
11/73(15)
15.4&
5.417
&6.1
Riso,2000
31H
eadand
neckcancer(n
"44)
6N
oN
utrisonIntensive
(6.25g
arginine/L)postopN
utrisonProtein
PlusIsoC/
IsoNpostop
NR
NR
NR
NR
25&
11.6(23)
28&
12.6(21)
Jiang,200138
UpperG
Isurgery(n
"120)
7Yes
Impactpostop
(fromday
1#11)
IsoC/IsoN
standardEN
postopN
RN
R0/60
(0)2/58
(3)13.1
&2.5
14.5&
3
Postoperativearginine
versusstandard
deLuis,2002
39H
eadand
neckcancer(n
"47)
10Yes
Arginine-enhanced
EN%
fiberpostopIsocal/IsoN
%fiberPostop
3m
onths3/23
(13)3
months
2/24(8)
5/23(22)
4/24(17)
NR
NR
deLuis,2004
40H
eadand
neckcancer(n"
90)9
YesA
rginine-enhancedEN
%fiberpostop
Isocal/IsoN%
fiberpostopN
RN
R2/45
(4)4/45
(9)25.8
&15
35.0&
24.6
Farreras,200541
Gastric
cancer(n"
66)9
YesIm
pactpostopIsosource
postop1/30
2/302/30
(7)9/30
(30)13
(mean)
11#22
(range)15
(mean)
10#22
(range)
Lobo,200644
Resection
forpancreas,stomach,
esophagealcancer(n"
120)8
YesStresson
feedw
/arginine,glutam
ine,omega-3
PUFA
postop
IsoC/IsoN
control(Nutrison
highprotein)postop
6/54(11)
At30
d32/54
(59)A
t4y
6/54(11)
At30
d33/54
(61.1)A
t4y
24/54(44)
24/54(44)
14.5(12#
23)17.5
(13#23)
deLuis,2007
49H
eadand
neckcancer(n
"72)
8N
oEN
dietw/arginine
8.5g/L
postopIsoC
/IsoNpostop
NR
NR
2/35(6)
2/37(5)
27.9&
2128.2
&12
Casas-R
odero,2008
48O
ralandlaryngealcancer(n
"44)
7N
o1)EN
w/arginine
postop2)EN
w/arginine%
omega-3
PUFA
postop
IsoC/IsoN
postopN
RN
RN
RN
R1)22.5
&10.0
2)18.6&
7.818.3
&7.5
Klek,2008
46Pancreatic
andgastric
cancerresections(n
"196)
6Yes
Reconvan
20m
L/hd1;50
mL/h
d2;75
mL/h
d3,
100m
L/huntild
7postop
Peptisorb,same
scheduleas
experimentalgroup
postop
1/92(1)
ITT
1/98(1)
1/91(1)
ITT
1/98(2)
21/92(23)
23/91(25)
12.9&
8.012.4
&5.9
Klek,2008
47Pancreatic
andgastric
cancerR
esections(n"
205)9
No
Stressonw
/arginine,glutam
ine,omega-3
PUFA
postop
Peptisorbpostop
1/52(2)
1/53(2)
13/52(25)
15/53(28)
13.1&
4.112.4
&3.9
(continued).
390DroveretalArginineSupplementationinSurgicalPatientsJAmCollSurg

Outcomes were also analyzed separately for studies ofupper GI operations only (n " 18), lower GI operationsonly (n " 2), and studies of mixed (both upper and lowerGI surgery) (n " 5). When the 16 trials of patients withupper GI surgery only that reported on infectious com-plications were aggregated, patients receiving arginine-supplemented diets experienced fewer infectious com-plications than those receiving standard diet therapies(RR " 0.69; 95% CI, 0.55#0.87; p " 0.002; test forheterogeneity p " 0.15, I2 " 27%). In the one study oflower GI surgery, RR " 0.34 (95% CI, 0.17#0.68, p "0.002; test for heterogeneity not applicable). In the 4 stud-ies of mixed GI surgery, RR " 0.49 (95% CI, 0.36#0.66;p ! 0.00001; test for heterogeneity p " 0.99, I2 " 0%).Differences between these subgroups were not statisticallysignificant (p " 0.06, see Fig. 4).
When the data on hospital length of stay were aggre-gated, arginine-supplemented diets were associated with asignificant reduction in hospital length of stay in the 14upper GI studies (WMD " #2.12, 95% CI, #3.85 to#0.39; p " 0.02; test of heterogeneity p ! 0.00001, I2 "93%) and in the 5 studies of upper and lower GI studies(WMD " #2.36; 95% CI, #3.09 to #1.64; p !0.00001, test of heterogeneity p " 0.66, I2 " 0%). Whenthe data from the 2 studies of lower GI studies were aggre-gated, arginine-supplemented diets had no effect on hospi-tal length of stay (WMD " #0.74; 95% CI, #3.92 to#2.45; p " 0.65; test for heterogeneity p " 0.002, I2 "90%). There were significant differences between thesesubgroups (p " 0.004, Fig. 5).
We compared the data from the trials that used Impact(n " 23) with those that used other formulations (n " 12).The use of Impact was associated with a greater reductionof infectious complications in the 21 trials that reported onoutcomes (RR " 0.49; 95% CI, 0.41#0.58; p ! 0.00001;test of heterogeneity p " 0.74, I2 " 0%) than the use ofother formulations in the 7 trials (RR " 0.95; 95% CI,0.75#1.21; p " 0.68; test of heterogeneity p " 0.98, I2 "0%). The differences between these 2 subgroups was statis-tically significant (p ! 0.0001, see Fig. 4). When the dataon hospital length of stay were aggregated and compared,the 21 studies using Impact formulas were associated witha statistically significant reduction (WMD " #2.62; 95%CI, #3.65 to #1.59; p ! 0.00001; test for heterogeneityp ! 0.00001; I2 " 87%) compared with the 8 studiesusing non-Impact formulas (WMD " #0.89; 95% CI,#3.21 to #1.44; p " 0.45; test for heterogeneity p "0.05; I2 " 49%). Differences between the subgroups weresignificant (p ! 0.00001, see Fig. 5).
Finally, patients who were fed the arginine-supplemented diets preoperatively only (7 trials), thoseTa
ble
4.C
ontin
ued
Firs
tau
thor
,ye
arPo
pula
tion
Met
hods
Scor
eB
lindi
ng
Inte
rven
tion
Mor
talit
y,n
(%)
Infe
ctio
ns,
n(%
)H
ospi
tals
tay,
d
Expe
rimen
tal
Con
trol
Expe
rimen
tal
Con
trol
Expe
rimen
tal
Con
trol
Expe
rimen
tal
Con
trol
deLu
is,20
0952
Hea
dan
dne
ckca
ncer
(n"
72)
10 Yes
ENdi
etw
/arg
inin
epo
stop
ENIs
oC/I
soN
post
opN
RN
RN
RN
RPo
stop
stay
24.3
&14
Post
opst
ay36
.1&
27
Schi
lling
,25
Bra
ga,2
0G
iano
tti3
6:d
ata
only
show
nfo
rgro
upre
ceiv
ing
Impa
ctve
rsus
stan
dard
ente
ralf
orm
ula,
noda
tash
own
forg
roup
rece
ivin
gPN
only
.EN
,ent
eral
nutr
ition
;IT
T,in
tent
totr
eat;
isoN
,iso
nitr
ogen
ous;
isoC
,iso
calo
ric;L
GI,
low
erga
stro
inte
stin
al;N
R,n
otre
port
ed;p
osto
p,po
stop
erat
ive;
preo
p,pr
eope
rativ
e;PU
FA,
poly
unsa
tura
ted
fatt
yac
id;U
GI,
uppe
rgas
troi
ntes
tinal
;PN
,par
ente
raln
utrit
ion.
Dal
y24
grou
ps1
and
2co
mbi
ned
and
com
pare
dw
ithgr
oups
3an
d4
com
bine
d.G
iano
tti3
6:D
ata
only
show
nfo
rgro
upre
ceiv
ing
Impa
ctve
rsus
stan
dard
ente
ralf
orm
ula,
noda
tash
own
forg
roup
rece
ivin
gPN
only
.C
asas
-Rod
ero4
8:B
oth
expe
rimen
talg
roup
swer
eco
mbi
ned
inm
eta-
anal
ysis.
Kle
k46:D
ata
forg
roup
srec
eivi
ngPN
are
nots
how
n.
391Vol. 212, No. 3, March 2011 Drover et al Arginine Supplementation in Surgical Patients

who received an arginine-supplemented diet both pre- andpostoperatively (13 trials), and those who received thearginine-supplemented diet postoperatively (n " 18) wereanalyzed separately. In all subgroups, patients experiencedfewer infectious complications if they were fed thearginine-supplemented diets (see Fig. 4). There was a sta-tistically significant difference across groups, suggesting agreater treatment effect with the perioperative administra-tion of arginine-supplemented diets (perioperative: RR "0.46; 95% CI, 0.36#0.59; p ! 0.00001, test for hetero-geneity p " 0.89; I2 " 0%; preoperative: RR " 0.57; 95%CI, 0.37#0.88; p " 0.01, test for heterogeneity p " 0.24;I2 " 26%, and postoperative: RR " 0.78; 95% CI,0.64#0.95; p " 0.01, test for heterogeneity p " 0.52; I2 "0%, the test of significance between subgroups, p " 0.03,see Fig. 4). Arginine-supplemented diets were associatedwith a significant reduction in hospital length of stay in the11 studies of perioperative intervention (WMD " #2.38;95% CI, #3.44 to #1.32; p ! 0.0001, test for heteroge-neity p ! 0.0001; I2 " 74%) and in the 14 studies ofpostoperative intervention only (WMD " #2.23; 95%CI, #3.80 to #0.65; p " 0.006; test for heterogeneity p !
0.00001; I2 " 85%), but there was no significant effect in6 studies of preoperative intervention (WMD " #1.38;95% CI, #3.49 to 0.73; p " 0.20; test for heterogeneityp ! 0.00001; I2 " 87%). There were significant differ-ences between the subgroups, again suggesting a greaterbenefit to the perioperative administration of arginine-supplemented diets (p " 0.001, see Fig. 5).
DISCUSSIONWe have systematically reviewed all RCTs evaluatingthe effect of perioperative administration of arginine-supplemented diets in elective surgical patients. We found35 eligible RCTs in elective surgery patients for consider-ation. When statistically aggregated, there is a substantialreduction in infectious complications and shorter hospitallength of stay associated with the use of these specialtydiets, with no overall effect on mortality compared withstandard care. These findings are insensitive to the use ofglycine in the control diets and are consistent with earliermeta-analyses on more limited samples of RCTs than wereincluded in our comprehensive analysis.9,13
Figure 1. Effect of arginine-supplemented diets on infections. Events, number of patients with infections; Total, totalnumber of patients in group; M-H, Random, Mantzel-Haenzel Random effects.
392 Drover et al Arginine Supplementation in Surgical Patients J Am Coll Surg

Figure 3. Effect of arginine-supplemented diets on mortality. Events, number of patients that died; Total, total number ofpatients in group; M-H, Random, Mantzel-Haenzel Random effects.
Figure 2. Effect of arginine-supplemented diets on hospital length of stay. Mean, mean hospital length of stay; SD,standard deviation; Total, total number of patients in group; IV, Random, inverse variance, random effects.
393Vol. 212, No. 3, March 2011 Drover et al Arginine Supplementation in Surgical Patients

Admittedly, there is considerable heterogeneity in ouranalysis of arginine-supplemented diets, particularly in theevaluation of their effect on hospital length of stay. Thisheterogeneity is likely due to differences in patients, prac-tice patterns, health care systems, study designs, treatmentdiets, and other methodologies across all studies. Becauseof the presence of heterogeneity, we pursued severalhypothesis-generating subgroup analyses. We first demon-strated that the treatment effect of arginine-supplementeddiets seems to be consistent across all types of GI andnon-GI operations. There might be a greater reduction inhospital length of stay associated with these diets in thenon-GI surgery patients compared with GI surgery (reduc-tion of 3.7 versus 2.1 days). However, this observationshould by no means diminish enthusiasm for using theseproducts in GI surgery because they are associated with an
average reduction of 2 days in hospital, which can translateinto considerable cost savings for institutions and healthcare systems.74-76 There was no substantial reductionin hospital length of stay associated with arginine-supplemented diets in lower GI surgery. However, the riskratio was similar to that of other GI operations, but therewere only 2 studies of lower GI surgery and the findingswere not statistically significant. We conclude thatarginine-supplemented diets should be prescribed to allpatients undergoing elective surgery with substantial risk ofinfectious complications.
We then explored the potential benefits of the differentarginine-supplemented formulas by analyzing the RCTsthat used Impact in the experimental arm and comparedwith RCTs that used other formulas.The treatment effect islarge and statistically significant in the group of RCTs that
Figure 4. Results of subgroup analyses examining the effect of arginine-supplemented diets oninfection. Numbers in parentheses indicate number of studies. RR, risk ratio; p values: refer to thedifferences in the effect of arginine-supplemented diets on infections between subgroups (gas-trointestinal [GI] versus non-GI studies, p " 0.28; lower GI, upper GI, and mixed GI studies, p "0.06; Impact versus non-Impact studies; p ! 0.0001; preoperative, perioperative, and postop-erative; p " 0.03).
394 Drover et al Arginine Supplementation in Surgical Patients J Am Coll Surg

used Impact, and aggregation of the data from the RCTs ofother formulations showed no substantial reduction in in-fectious complications or hospital length of stay. Impactcontains a combination of arginine, omega-3 fatty acids,and nucleotides, but it is hard to make generalizationsabout the formulations used in the non-Impact RCTs, ex-cept that no 2 studies used the same formulation. It isdifficult to ascertain the exact amount of arginine deliveredin these studies, but it was generally of a lower concentra-tion than is found in Impact. Three of the studies supple-mented with some amount of omega-3 fats, 1 study used aformula with RNA, and 2 studies also used formulas withglutamine.
The only inference from these data is that infectiouscomplications are reduced with use of Impact and notother arginine formulations. It is possible that the specificcombination of nutrients in Impact is necessary and these
nutrients can interact to produce benefit. In addition, it isnot possible to say what the optimal combination or dosageof specialized nutrients is from this data set. Because theclinical benefit observed relates to a substantial reductionof infections, one might postulate (at least in part) thatthese diets work by improving the immune response aftersurgery.
A causal relationship has been shown to exist betweenphysical injury (surgery and trauma) and the predisposi-tion for infectious complications to develop in these pa-tients.11 This increased infectious risk has been hypothe-sized to be related to an acquired arginine-deficient state,which leads to substantial immune dysfunction. Recentinvestigations suggest that arginine metabolism is inti-mately regulated by the immune system.11 Soon after phys-ical injury (surgery or trauma), an accumulation of imma-ture cells of myeloid origin has been discovered in the
Figure 5. Results of subgroup analyses examining the effect of arginine-supplemented diets onhospital length of stay. p Values: refer to the differences in the effect of arginine-supplementeddiets on hospital length of stay between subgroups (gastrointestinal [GI] versus non-GI studies;p " 0.0007; lower GI, upper GI, and mixed GI studies; p " 0.004; Impact versus non-Impactstudies; p ! 0.00001; preoperative, perioperative, and postoperative; p " 0.001).
395Vol. 212, No. 3, March 2011 Drover et al Arginine Supplementation in Surgical Patients

circulation and lymph tissue. These cells express arginase 1,which efficiently depletes arginine. Coupled with poor ar-ginine intake and inadequate endogenous generation, argi-nase 1 serves to create a state of arginine deficiency. Anincreasing amount of evidence has accumulated in the last10 years to demonstrate that suppression of T-lymphocytefunction can be caused through arginine depletion by my-eloid cells expressing arginase 1, giving these cells the namemyeloid-derived suppressor cells (MDSC).77 Several clinicalstudies suggest that use of arginine supplementation alongwith omega-3 fatty acids restores T-lymphocyte function,including CD4 counts and interleukin-2 production.78,79
We speculate that arginine-supplemented diets can over-come arginine deficiency caused by MDSC through thesynergistic effect of several components. First, arginine issupplemented in supraphysiologic quantities, helping in-crease systemic arginine availability. Second, omega-3 fattyacids can “blunt” upregulation of MDSC and arginase 1,the enzyme responsible for arginine destruction.80-82 In ad-dition, vitamin A (and vitamin A analogues) has beenshown under certain circumstances to induce maturationof MDSC and a decrease in arginase 1 expression.83,84 Ad-ditional investigation will be necessary to test thesepossibilities.
Finally, we explored a priori the question of whetherproviding the specialized formula is better done before sur-gical insult, after the surgical insult, or both. We observedthat all 3 strategies are associated with a substantial reduc-tion in infectious complications. Both perioperative andpostoperative use of these diets were associated with a re-duction in hospital length of stay and, used in the preop-erative setting, were not associated with a substantial reduc-tion in hospital length of stay (WMD " #1.38, 95%, CI,#3.49 to 0.73; p " 0.20). In addition, when we comparedthe estimates of treatment effect across these 3 subgroups,we observed that the largest treatment effect was associatedwith the perioperative administration of the arginine-supplemented diets. We are cautious not to overstate thesefindings, as this comparison is an indirect comparison ofstudies—we are comparing RRs across 3 subgroups. Thereis only 1 head-to-head study that compares perioperativeadministration of arginine-supplemented diets with post-operative use only.51 In this study of 46 patients with stom-ach or pancreas cancer, use of perioperative arginine dietswas associated with a reduction in infection (RR " 0.34;95% CI, 0.16#0.71; p " 0.004) and a reduction in hos-pital length of stay (WMD " #9.18; 95% CI, #11 to#7.26; p ! 0.00001) compared with the group that justreceived arginine-supplemented diets in the postoperativephase. Although this hypothesis warrants additional inves-tigation, it appears, based on these results, that use of
arginine-supplemented diets in both the pre- and postop-erative phase are superior to either phase alone. That is notto say that use in the preoperative only or postoperativephase only is not worthwhile. It means that we can expect agreater treatment effect if we use them both before and aftersurgery.
We would like to acknowledge some of the limitations ofthis review. The studies included in this review, althoughRCTs and of reasonable methodological quality (as evi-denced by an average scoring of 8.2 of a maximum of 14),cover a span of almost 2 decades. Recent advances in dis-charge management (affecting hospital length of stay), glu-cose and antibiotic therapy (affecting infection control),and surgery (eg, minimally invasive surgery) could affectresults from later studies. Some of the included studies hadsmall samples sizes (n ! 100) with more than 1 interven-tion and/or control group, and in other studies the sameintervention was used in varying settings, ie, pre-, post-,and/or perioperatively. Although we have separated thesevarying interventions into the various subgroups, the ap-propriateness of the study design in some cases is question-able. Lastly, many studies, despite reporting a reduction ininfectious morbidity, failed to report data related to infec-tions in a clear, meaningful way, and these studies had to bedeleted from our analyses. Despite these limitations, thestrong signals for a reduction in infections from our anal-yses cannot be ignored.
In conclusion, in this review we have demonstratedsome clinical evidence that use of nutrition therapy con-taining arginine and omega-3 fatty acids used both pre-and postoperatively in high-risk elective surgical patients isassociated with a substantial reduction in infection andshorter length of hospital stay. Efforts to implement the useof these diets in the perioperative setting are worthwhile.These efforts will result in considerable reduction in mor-bidity for our patients and substantial reductions in costsfor the health care system.
Author Contributions
Study conception and design: Drover, Dhaliwal, Weitzel, Wis-chmeyer, Ochoa, Heyland
Acquisition of data: Wischmeyer, Drover, Heyland, DhaliwalAnalysis and interpretation of data: Dhaliwal, HeylandDrafting of manuscript: Drover, HeylandCritical revision: Wischmeyer, Dhaliwal, Ochoa
Acknowledgment: We would like to thank Sarah Maddenand Gina Haeussner for their assistance with abstraction andchecking of data and Mr Andrew Day for his assistance withthe statistical analysis.
396 Drover et al Arginine Supplementation in Surgical Patients J Am Coll Surg
REFERENCES
1. Richards MJ, Edwards JR, Culver DH, et al. Nosocomial infec-tions in combined medical-surgical intensive care units in theUnited States. Infection Control Hosp Epidemiol 2000;21:510–515.
2. de Lissovoy G, Fraeman K, Hutchins V, et al. Surgical site infec-tion: incidence and impact on hospital utilization and treatmentcosts. Am J Infect Control 2009;37:387–397.
3. Scott RD II. The direct medical healthcare costs of healthcareassociated infections in us hospitals and the benefits of preven-tion. Available at: http://www.cdc.gov/ncidod/dhqp/pdf/Scott_CostPaper.pdf. Accessed April 13, 2010.
4. American College of Surgeons, National Surgical Quality Im-provement Program. About ACS NSQIP: Program Overview.Available at: http://www.acsnsqip.org/main/aboutacs/about_overview.jsp. Accessed April 30, 2010.
5. Garth AK, Newsome CM, Simmance N, et al. Nutritional sta-tus, nutrition practices and post-operative complications in pa-tients with gastrointestinal cancer. J Hum Nutr Diet 2010;23:393–401.
6. Jones NE, Heyland DK. Pharmaconutrition: a new emergingparadigm. Curr Opin Gastroenterol 2008;24:215.
7. Dupertuis YM, Meguid MM, Pichard C. Advancing from im-munonutrition to a pharmaconutrition: a gigantic challenge.Curr Opin Clin Nutr Metab Care 2009;12:398–403.
8. Ochoa JB. Separating pharmaconutrition from classic nutri-tion goals: a necessary step. Crit Care Med 2008;36:347–348.
9. Heyland DK, Novak F, Drover JW, et al. Should immunonutri-tion become routine in critically ill patients? A systematic reviewof the evidence. JAMA 2001;286:944–953.
10. Morris SM Jr. Recent advances in arginine metabolism. CurrOpin Clin Nutr Metab Care 2004;7:45–51.
11. Popovic PJ, Zeh HJ 3rd, Ochoa JB. Arginine and immunity. JNutr 2007;137[Suppl]:1681S#1686S.
12. Ochoa JB, Makarenkova V, Bansal V. A rational use of immuneenhancing diets: when should we use dietary arginine supple-mentation? Nutr Clin Pract 2004;19:216–225.
13. Waitzberg DL, Saito H, Plank LD, et al. Postsurgical infectionsare reduced with specialized nutrition support. World J Surg2006;30:1592–1604.
14. Marik PE, Zaloga GP. Immunonutrition in high-risk surgicalpatients: a systematic review and analysis of the literature. JPENJ Parent Enteral Nutr 2010;34:378–386.
15. Heyland DK, MacDonald S, Keefe L, et al. Total parenteralnutrition in the critically ill patient: a meta-analysis. JAMA1998;280:2013–2019.
16. Review Manager (RevMan). Version 5.0. Copenhagen: TheNordic Cochrane Center, The Cochrane Collaboration; 2008.
17. DerSimonian R, Laird N. Meta-analysis in clinical trials. Con-trol Clin Trials 1986;7:177–188.
18. Higgins JPT, Thompson SG. Quantifying heterogeneity in ameta-analysis. Stat Med 2002;21:1539–1558.
19. Rucker G, Schwarzer G, Carpenter J. Arcsine test for publica-tion bias in meta-analyses with binary outcomes. Stat Med2008;27:746–763.
20. Braga M, Vignali A, Gianotti L, et al. Immune and nutritionaleffects of early enteral nutrition after major abdominal opera-tions. Eur J Surg 1996;162:105–112.
21. Daly JM, Reynolds J, Sigal RK, et al. Effect of dietary proteinand amino acids on immune function. Crit Care Med 1990;18[Suppl]:S86#S93.
22. Tepaske R, te Velthuis H, Oudemans-van Straaten HM, et al.Glycine does not add to the beneficial effects of perioperativeoral immune-enhancing nutrition supplements in high-risk car-diac surgery patients. JPEN J Parenter Enteral Nutr 2007;31:173–180.
23. Daly JM, Lieberman MD, Goldfine J, et al. Enteral nutritionwith supplemental arginine, RNA, and omega-3 fatty acids inpatients after operation: immunologic, metabolic, and clinicaloutcome. Surgery 1992;112:56–67.
24. Daly JM, Weintraub FN, Shou J, et al. Enteral nutrition duringmultimodality therapy in upper gastrointestinal cancer patients.Ann Surg 1995;221:327–338.
25. Schilling J, Vranjes N, Fierz W, et al. Clinical outcome andimmunology of postoperative arginine, omega-3 fatty acids, andnucleotide-enriched enteral feeding: a randomized prospectivecomparison with standard enteral and low calorie/low fat i.v.solutions. Nutrition 1996;12:423–429.
26. Senkal M, Mumme A, Eickhoff U, et al. Early postoperativeenteral immunonutrition: clinical outcome and cost-comparison analysis in surgical patients. Crit Care Med 1997;25:1489–1496.
27. McCarter MD, Gentilini OD, Gomez ME, et al. Preoperativeoral supplement with immunonutrients in cancer patients.JPEN J Parenter Enteral Nutr 1998;22:206–211.
28. Braga M, Gianotti L, Radaelli G, et al. Perioperative immunonu-trition in patients undergoing cancer surgery: results of a random-ized double-blind phase 3 trial. Arch Surg 1999;134:428–433.
29. Senkal M, Zumtobel V, Bauer KH, et al. Outcome and cost-effectiveness of perioperative enteral immunonutrition in pa-tients undergoing elective upper gastrointestinal tract surgery: aprospective randomized study. Arch Surg 1999;134:1309–1316.
30. Snyderman CH, Kachman K, Molseed L, et al. Reduced post-operative infections with an immune-enhancing nutritionalsupplement. Laryngoscope 1999;109:915–921.
31. Riso S, Aluffi P, Brugnani M, et al. Postoperative enteral immu-nonutrition in head and neck cancer patients. Clin Nutr 2000;19:407–412.
32. Tepaske R, Velthuis H, Oudemans-van Straaten HM, et al. Ef-fect of preoperative oral immune-enhancing nutritional supple-ment on patients at high risk of infection after cardiac surgery: arandomised placebo-controlled trial. Lancet 2001;358:696–701.
33. van Bokhorst-De Van Der Schueren MA, Quak JJ, vonBlomberg-van der Flier BM, et al. Effect of perioperative nutri-tion, with and without arginine supplementation, on nutri-tional status, immune function, postoperative morbidity, andsurvival in severely malnourished head and neck cancer patients.Am J Clin Nutr 2001;73:323–332.
34. Braga M, Gianotti L, Vignali A, et al. Preoperative oral arginineand n-3 fatty acid supplementation improves the immunometa-bolic host response and outcome after colorectal resection forcancer. Surgery 2002;132:805–814.
35. Braga M, Gianotti L, Nespoli L, et al. Nutritional approach inmalnourished surgical patients: a prospective randomized study.Arch Surg 2002;137:174–180.
36. Gianotti L, Braga M, Gentilini O, et al. Artificial nutrition afterpancreaticoduodenectomy. Pancreas 2000;21:344–351.
397Vol. 212, No. 3, March 2011 Drover et al Arginine Supplementation in Surgical Patients

37. Gianotti L, Braga M, Nespoli L, et al. A randomized controlledtrial of preoperative oral supplementation with a specialized dietin patients with gastrointestinal cancer. Gastroenterology 2002;122:1763–1770.
38. Jiang ZM, Gu ZY, Chen FL, et al. The role of immune enhancedenteral nutrition on plasma amino acid, gut permeability andclinical outcome (a randomized, double blind, controlled,multi-center clinical trial with 120 cases). Zhongguo Yi Xue KeXue Yuan Xue Bao 2001;23:515–518.
39. de Luis DA, Aller R, Izaola O, et al. Postsurgery enteral nutritionin head and neck cancer patients. Eur J Clin Nutr 2002;56:1126–1129.
40. de Luis DA, Izaola O, Cuellar L, et al. Randomized clinical trialwith an enteral arginine-enhanced formula in early postsurgicalhead and neck cancer patients. Eur J Clin Nutr 2004;58:1505–1508.
41. Farreras N, Artigas V, Cardona D, et al. Effect of early postop-erative enteral immunonutrition on wound healing in patientsundergoing surgery for gastric cancer. Clin Nutr 2005;24:55–65.
42. Finco C, Magnanini P, Sarzo G, et al. Prospective randomizedstudy on perioperative enteral immunonutrition in laparoscopiccolorectal surgery. Surg Endosc 2007;21:1175–1179.
43. Xu J, Zhong Y, Jing D, et al. Preoperative enteral immunonu-trition improves postoperative outcome in patients with gastro-intestinal cancer. World J Surg 2006;30:1284–1289.
44. Lobo DN, Williams RN, Welch NT, et al. Early postoperativejejunostomy feeding with an immune modulating diet in pa-tients undergoing resectional surgery for upper gastrointestinalcancer: a prospective, randomized, controlled, double-blindstudy. Clin Nutr 2006;25:716–726.
45. Sakurai Y, Masui T, Yoshida I, et al. Randomized clinical trial ofthe effects of perioperative use of immune-enhancing enteralformula on metabolic and immunological status in patients un-dergoing esophagectomy. World J Surg 2007;31:2150–2157;discussion 2158#2159.
46. Klek S, Kulig J, Sierzega M, et al. Standard and immunomodu-lating enteral nutrition in patients after extended gastrointesti-nal surgery—a prospective, randomized, controlled clinicaltrial. Clin Nutr 2008;27:504–512.
47. Klek S, Kulig J, Sierzega M, et al. The impact of immunostimu-lating nutrition on infectious complications after upper gastro-intestinal surgery: a prospective, randomized, clinical trial. AnnSurg 2008;248:212–220.
48. Casas-Rodera P, Gomez-Candela C, Benitez S, et al. Immu-noenhanced enteral nutrition formulas in head and neck cancersurgery: a prospective, randomized clinical trial. Nutr Hosp2008;23:105–110.
49. de Luis DA, Izaola O, Cuellar L, et al. Clinical and biochemicaloutcomes after a randomized trial with a high dose of enteralarginine formula in postsurgical head and neck cancer patients.Eur J Clin Nutr 2007;61:200–204.
50. Wachtler P, Axel Hilger R, Konig W, et al. Influence of a pre-operative enteral supplement on functional activities of periph-eral leukocytes from patients with major surgery. Clin Nutr1995;14:275–282.
51. Giger U, Buchler M, Farhadi J, et al. Preoperative immunonu-trition suppresses perioperative inflammatory response in pa-tients with major abdominal surgery—a randomized controlledpilot study. Ann Surg Oncol 2007;14:2798–2806.
52. De Luis DA, Izaola O, Cuellar L, et al. High dose of arginineenhanced enteral nutrition in postsurgical head and neck cancer
patients. A randomized clinical trial. Eur Rev Med PharmacolSci 2009;13:279–283.
53. Okamoto Y, Okano K, Izuishi K, et al. Attenuation of the sys-temic inflammatory response and infectious complications aftergastrectomy with preoperative oral arginine and omega-3 fattyacids supplemented immunonutrition. World J Surg 2009;33:1815–1821.
54. Celik JB, Gezginç K, Ozçelik K, et al. The role of immunonu-trition in gynecologic oncologic surgery. Eur J Gynaecol Oncol2009;30:418–421.
55. Heslin MJ, Latkany L, Leung D, et al. A prospective, random-ized trial of early enteral feeding after resection of upper gastro-intestinal malignancy. Ann Surg 1997;226:567–577; discussion577#580.
56. Helminen H, Raitanen M, Kellosalo J. Immunonutrition inelective gastrointestinal surgery patients. Scand J Surg 2007;96:46–50.
57. de Luis DA, Izaola O, Aller R, et al. A randomized clinical trialwith oral immunonutrition (omega3-enhanced formula vs.arginine-enhanced formula) in ambulatory head and neck can-cer patients. Ann Nutr Metab 2005;49:95–99.
58. Braga M, Gianotti L, Cestari A, et al. Gut function and immuneand inflammatory responses in patients perioperatively fed withsupplemented enteral formulas. Arch Surg 1996;131:1257–1264.
59. Gianotti L, Braga M, Fortis C, et al. A prospective, randomizedclinical trial on perioperative feeding with an arginine-, omega-3fatty acid-, and RNA-enriched enteral diet: effect on host re-sponse and nutritional status. JPEN J Parenter Enteral Nutr1999;23:314–320.
60. Gianotti L BM, Vignali A, Bisagni P, et al. Route and composi-tion of postoperative nutritioal support: impact on immune-metabolic response and postoperative outcome. Riv Ital NutrParenterale Enterale 1998;19:173–182.
61. Braga M, Gianotti L, Vignali A, et al. Artificial nutrition aftermajor abdominal surgery: impact of route of administration andcomposition of the diet. Crit Care Med 1998;26:24–30.
62. Braga M, Gianotti L, Vignali A, et al. Immunonutrition in gas-tric cancer surgical patients. Nutrition 1998;14:831–835.
63. Braga M, Vignali A, Gianotti L, et al. Benefits of early postop-erative enteral feeding in cancer patients. Infusionsther Transfu-sionsmed 1995;22:280–284.
64. Gianotti L, Braga M, Vignali A, et al. Effect of route of deliveryand formulation of postoperative nutritional support in patientsundergoing major operations for malignant neoplasms. ArchSurg 1997;132:1222–1229.
65. Di Carlo V, Gianotti L, Balzano G, et al. Complications ofpancreatic surgery and the role of perioperative nutrition. DigSurg 1999;16:320–326.
66. Takeuchi H, Ikeuchi S, Kawaguchi Y, et al. Clinical significanceof perioperative immunonutrition for patients with esophagealcancer. World J Surg 2007;31:2160–2167.
67. Horie H, Okada M, Kojima M, et al. Favorable effects of pre-operative enteral immunonutrition on a surgical site infection inpatients with colorectal cancer without malnutrition. Surg To-day 2006;36:1063–1068.
68. Slotwinski R. Anti-inflammatory response to early enteral im-munonutrition in malnourished patients after pancreaticoduo-denectomy. Centr Eur J Immunol 2007;32:138–146.
69. Kemen M, Senkal M, Homann HH, et al. Early postoperativeenteral nutrition with arginine-omega-3 fatty acids and ribonu-cleic acid-supplemented diet versus placebo in cancer patients:
398 Drover et al Arginine Supplementation in Surgical Patients J Am Coll Surg

an immunologic evaluation of Impact. Crit Care Med1995;23:652–659.
70. Wu GH, Zhang YW, Wu ZH. Modulation of postoperativeimmune and inflammatory response by immune-enhancingenteral diet in gastrointestinal cancer patients. World J Gas-troenterol 2001;7:357–362.
71. de Luis DA, Izaola O, Cuellar L, et al. Effect of c-reactive proteinand interleukins blood levels in postsurgery arginine-enhancedenteral nutrition in head and neck cancer patients. Eur J ClinNutr 2003;57:96–99.
72. de Luis DA, Arranz M, Aller R, et al. Immunoenhanced enteralnutrition, effect on inflammatory markers in head and neckcancer patients. Eur J Clin Nutr 2005;59:145–147.
73. Loi C, Zazzo JF, Delpierre E, et al. Increasing plasma glutaminein postoperative patients fed an arginine-rich immune-enhancing diet—a pharmacokinetic randomized controlledstudy. Crit Care Med 2009;37:501–509.
74. Braga M, Gianotti L. Preoperative immunonutrition: cost-benefit analysis. JPEN J Parenter Enteral Nutr 2005;29[Suppl]:S57#S61.
75. Braga M, Gianotti L, Gentilini O, et al. Early postoperativeenteral nutrition improves gut oxygenation and reduces costscompared with total parenteral nutrition. Crit Care Med 2001;29:242–248.
76. Strickland A, Brogan A, Krauss J, et al. Is the use of specializednutritional formulations a cost-effective strategy? A national
database evaluation. JPEN J Parenter Enteral Nutr2005;29[Suppl]:S81–S91.
77. Makarenkova VP, Bansal V, Matta BM, et al. CD11b%/Gr-1%myeloid suppressor cells cause T cell dysfunction after traumaticstress. J Immunol 2006;176:2085–2094.
78. Nieves C Jr, Langkamp-Henken B. Arginine and immunity:a unique perspective. Biomed Pharmacother 2002;56:471–482.
79. Moore FA. Effects of immune-enhancing diets on infectiousmorbidity and multiple organ failure. JPEN J Parenter EnteralNutr 2001;25[Suppl]:S36#S42.
80. Whiting CV, Bland PW, Tarlton JF. Dietary n-3 polyunsatu-rated fatty acids reduce disease and colonic proinflammatorycytokines in a mouse model of colitis. Inflamm Bowel Dis 2005;11:340–349.
81. Almallah YZ, Richardson S, O’Hanrahan T, et al. Distal procto-colitis, natural cytotoxicity, and essential fatty acids. Am J Gas-troenterol 1998;93:804–809.
82. Bansal V, Syres KM, Makarenkova V, et al. Interactions betweenfatty acids and arginine metabolism: implications for the designof immune-enhancing diets. JPEN J Parenter Enteral Nutr2005;29[Suppl]:S75#S80.
83. Mehta K. Retinoic acid—a player that rules the game of life anddeath in neutrophils. Indian J Exp Biol 2002;40:874–881.
84. Kuwata T, Wang IM, Tamura T, et al. Vitamin A deficiency inmice causes a systemic expansion of myeloid cells. Blood2000;95:3349–3356.
399Vol. 212, No. 3, March 2011 Drover et al Arginine Supplementation in Surgical Patients

Appendix 1Methodological Scoring Tool
Score0 1 2
Randomization — Not concealed or not sure Concealed randomizationAnalysis Other — Intention to treatBlinding Not blinded Single blind Double blindedPatient selection Selected patients or unable to tell Consecutive eligible patients —Comparability of groups at baseline No or not sure Yes —Extent of follow-up !100% 100% —Treatment protocol Poorly described Reproducibly described —Co-interventions Not described Described but not equal or not sure Well-described and all equalOutcomes Not described Partially described Objectively defined
399.e1 Drover et al Arginine Supplementation in Surgical Patients J Am Coll Surg