peripheral arterial disease claudication and critical limb...
TRANSCRIPT

1
ClaudicationClaudication and Critical and Critical Limb IschemiaLimb Ischemia
Endovascular Treatment of Peripheral Arterial DiseaseEndovascular Treatment of Peripheral Arterial Disease
Jason Wollmuth, MD, FACCJason Wollmuth, MD, FACCHeart Center CardiologyHeart Center Cardiology
Peripheral Arterial DiseasePeripheral Arterial Disease
Affects ~20% of adults older than 55Affects ~20% of adults older than 55Estimated 27 million in the US and EuropeEstimated 27 million in the US and Europe~50% are asymptomatic~50% are asymptomaticPrevalence increases with age, smoking, Prevalence increases with age, smoking, diabetesdiabetesIncidence of symptomatic PAD between 1 and Incidence of symptomatic PAD between 1 and 3.6 per 1000 population3.6 per 1000 populationIncidence 2Incidence 2--fold higher in menfold higher in menIn patients with asymptomatic disease, 5In patients with asymptomatic disease, 5--10% 10% will develop symptoms in 5 yearswill develop symptoms in 5 years
Peripheral Arterial DiseasePeripheral Arterial Disease
Critical leg ischemia most frequent in DMCritical leg ischemia most frequent in DMOne fifth of people with PAD have typical One fifth of people with PAD have typical symptomssymptomsOneOne--third with atypical leg symptomsthird with atypical leg symptomsDespite relatively slow and low rate of Despite relatively slow and low rate of local complications, patients with PAD local complications, patients with PAD have 5 year mortality rates of 25have 5 year mortality rates of 25--30% 30% (mainly from coronary or cerebral vascular (mainly from coronary or cerebral vascular disease)disease)
SymptomsSymptoms
Intermittent Intermittent claudicationclaudication–– Calf pain most commonCalf pain most common–– Buttock/hip pain with proximal diseaseButtock/hip pain with proximal disease–– Ankle/foot pain with distal diseaseAnkle/foot pain with distal disease
Critical limb ischemiaCritical limb ischemia–– Rest pain, ulceration, gangreneRest pain, ulceration, gangrene–– Indicates severe, often multilevel arterial diseaseIndicates severe, often multilevel arterial disease
Acute arterial occlusionAcute arterial occlusion–– Trauma, thrombosis, embolismTrauma, thrombosis, embolism
Differential DiagnosisDifferential Diagnosis
PADPADNeurogenicNeurogenic pseudoclaudicationpseudoclaudicationVenous Venous claudicationclaudicationSkeletal muscle metabolic abnormalitiesSkeletal muscle metabolic abnormalitiesArterial entrapment syndromesArterial entrapment syndromesThromboangiitisThromboangiitis obliteransobliteransFibromuscularFibromuscular dysplasiadysplasiaExtravascularExtravascular compressioncompression
Physical FindingsPhysical Findings
Subcutaneous atrophySubcutaneous atrophyHair lossHair lossPallorPallorCoolnessCoolnessDependent Dependent ruborruborBrittle toenailsBrittle toenailsDecreased/absent pulsesDecreased/absent pulsesbruitsbruits
2
Diagnostic ModalitiesDiagnostic ModalitiesAnkleAnkle--Brachial Index (ABI) = Highest ankle Brachial Index (ABI) = Highest ankle pressure/Highest brachial pressurepressure/Highest brachial pressure–– Normal 0.9 to 1.3Normal 0.9 to 1.3–– 0.71 0.71 –– 0.9 0.9 –– mild obstructionmild obstruction–– 0.41 0.41 –– 0.7 0.7 –– moderate obstructionmoderate obstruction–– <0.4 <0.4 –– severe obstructionsevere obstruction
Should also be measured after exerciseShould also be measured after exercise–– If no drop in ABI after exercise likely not PADIf no drop in ABI after exercise likely not PAD–– 20 mm Hg drop considered significant20 mm Hg drop considered significant
BP below 90 mm Hg BP below 90 mm Hg –– intermittent intermittent claudicationclaudication, , below 60 mm Hg below 60 mm Hg c/wc/w rest painrest painABI may underestimate disease in calcified, ABI may underestimate disease in calcified, noncompressiblenoncompressible arteries (often ABI>1.5)arteries (often ABI>1.5)
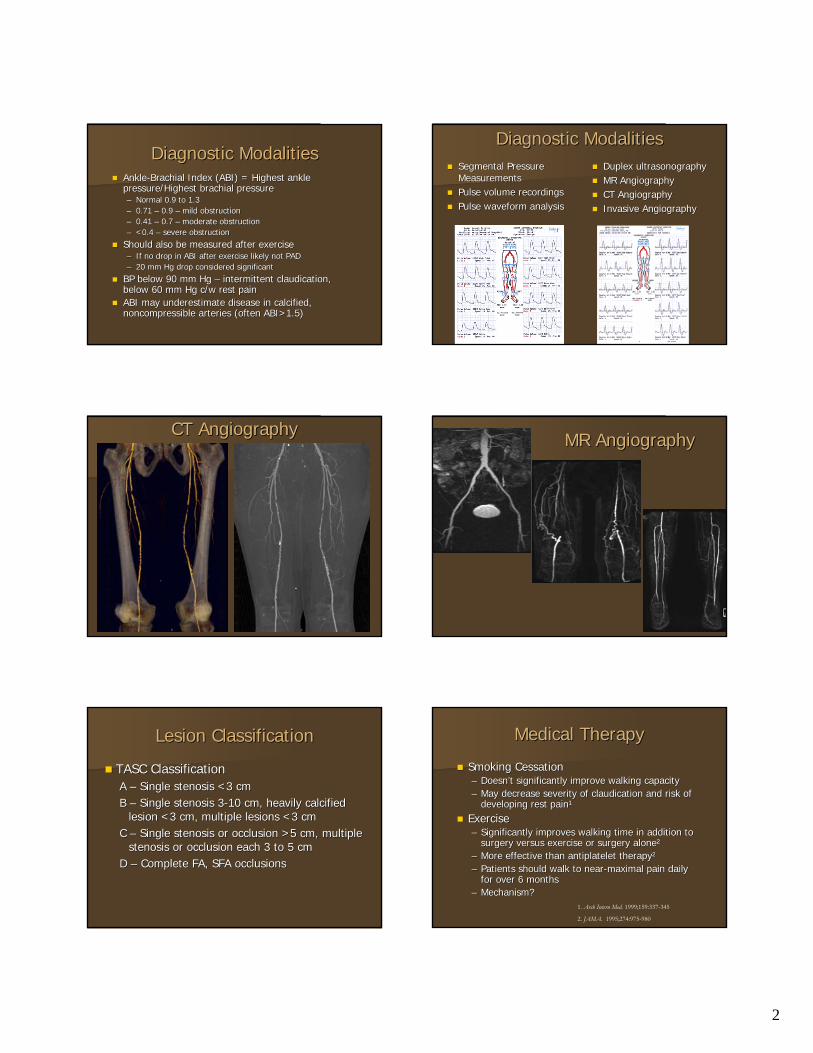
Diagnostic ModalitiesDiagnostic ModalitiesSegmental Pressure Segmental Pressure MeasurementsMeasurementsPulse volume recordings Pulse volume recordings Pulse waveform analysisPulse waveform analysis
Duplex Duplex ultrasonographyultrasonographyMR AngiographyMR AngiographyCT AngiographyCT AngiographyInvasive AngiographyInvasive Angiography
CT AngiographyCT AngiographyMR AngiographyMR Angiography
Lesion ClassificationLesion Classification
TASC ClassificationTASC ClassificationA A –– Single stenosis <3 cmSingle stenosis <3 cmB B –– Single stenosis 3Single stenosis 3--10 cm, heavily calcified 10 cm, heavily calcified
lesion <3 cm, multiple lesions <3 cmlesion <3 cm, multiple lesions <3 cmC C –– Single stenosis or occlusion >5 cm, multiple Single stenosis or occlusion >5 cm, multiple
stenosis or occlusion each 3 to 5 cmstenosis or occlusion each 3 to 5 cmD D –– Complete FA, SFA occlusionsComplete FA, SFA occlusions
Medical TherapyMedical Therapy
Smoking CessationSmoking Cessation–– DoesnDoesn’’t significantly improve walking capacityt significantly improve walking capacity–– May decrease severity of May decrease severity of claudicationclaudication and risk of and risk of
developing rest paindeveloping rest pain¹¹
ExerciseExercise–– Significantly improves walking time in addition to Significantly improves walking time in addition to
surgery versus exercise or surgery alonesurgery versus exercise or surgery alone²²–– More effective than antiplatelet therapyMore effective than antiplatelet therapy²²–– Patients should walk to nearPatients should walk to near--maximal pain daily maximal pain daily
for over 6 monthsfor over 6 months–– Mechanism?Mechanism?
1. Arch Intern Med. 1999;159:337-345
2. JAMA. 1995;274:975-980

3
Medical TherapyMedical TherapyStatinsStatins–– 4S trial 4S trial –– significantly less new significantly less new claudicationclaudication in in
patients treated with patients treated with statinsstatins (3.6 (3.6 vsvs 2.3%)2.3%)¹¹–– Improved walking timeImproved walking time²²
PentoxifyllinePentoxifylline –– no significant benefit found in no significant benefit found in metameta--analysisanalysisCilostazolCilostazol –– phosphodiesterasephosphodiesterase 3 inhibitor3 inhibitor–– Significantly improved walking timesSignificantly improved walking times³³–– Inhibits platelet aggregation and Inhibits platelet aggregation and vasodilatesvasodilates
1. Am J Cardiol. 1998;88:333-5.
2. Circulation. 2003;108:1481-6.
3. Am J Cardiol. 2002;90:1314-9.
Surgical TreatmentSurgical Treatment
Considered gold standard against which Considered gold standard against which percutaneous treatments measuredpercutaneous treatments measuredPrimary recommendation for Type D lesions, Primary recommendation for Type D lesions, failed endovascular therapyfailed endovascular therapyLongLong--term patency rates dependent on graft term patency rates dependent on graft typetype¹¹–– PTFE grafts PTFE grafts –– patency rate ~60% at 4 yearspatency rate ~60% at 4 years
Decreased OR time, hospital stays, infections. Preserve Decreased OR time, hospital stays, infections. Preserve SVG SVG
–– SVGs SVGs –– patency rate ~80% at 4 yearspatency rate ~80% at 4 yearsRisks Risks –– wound infection, MI, death. wound infection, MI, death. PeriPeri--op op mortality historically higher than for mortality historically higher than for percutaneous treatmentpercutaneous treatment
J Cardiovasc Surg. 2004;3:193-201.
Surgery versus Percutaneous Surgery versus Percutaneous TherapyTherapy
Historically, PTA used in patients with Historically, PTA used in patients with lifestyle limiting lifestyle limiting claudicationclaudication and surgery and surgery for patients with rest pain and critical limb for patients with rest pain and critical limb ischemiaischemiaPTA increasingly used in CLIPTA increasingly used in CLITechnological advances leading to more Technological advances leading to more aggressive percutaneous approaches with aggressive percutaneous approaches with improved outcomesimproved outcomes
Percutaneous TherapyPercutaneous Therapy
Favorable predictors of benefit from endovascular Favorable predictors of benefit from endovascular procedures include intermittent procedures include intermittent claudicationclaudication, proximal , proximal location, short lesions, stenosis rather than occlusion, location, short lesions, stenosis rather than occlusion, good distal rungood distal run--off, lack of residual stenosis after off, lack of residual stenosis after treatmentstreatmentsBalloon AngioplastyBalloon Angioplasty–– Equivalent risk of longEquivalent risk of long--term failure compared to PTFE term failure compared to PTFE
bypass grafts and roughly twice the risk of venous bypass bypass grafts and roughly twice the risk of venous bypass graftsgrafts¹¹
–– MetaMeta--analysis revealed patency rates of 59% at 1 year and analysis revealed patency rates of 59% at 1 year and 45% at 5 years45% at 5 years²²
1. Med Decision Making. 1994;14:71-81
2. J Vasc Interv Radiol. 1995;6:843-9.
StentsStentsInitially used to treat suboptimal PTA or related Initially used to treat suboptimal PTA or related complicationscomplications11stst stents were balloon expandable with poor clinical stents were balloon expandable with poor clinical outcomes (4 year patency rates 37outcomes (4 year patency rates 37--52%)52%)–– Significant Significant intimalintimal hyperplasia and external compressionhyperplasia and external compression–– No improvement over balloon angioplasty aloneNo improvement over balloon angioplasty alone
Improved outcomes with selfImproved outcomes with self--expanding and expanding and nitinolnitinolstents. stents. –– NickelNickel--titanium alloy with titanium alloy with superelasticitysuperelasticity and thermal shape and thermal shape
memory ideal for SFA/memory ideal for SFA/poplitealpopliteal–– SMART stent SMART stent –– primary patency 75primary patency 75--84% at 1 year, 6084% at 1 year, 60--84% 84%
at 2 years. Fracture rate >15%at 2 years. Fracture rate >15%–– Improved fracture rate with next generation stents Improved fracture rate with next generation stents
((LifestentLifestent, , ZilverZilver PTX, Leipzig)PTX, Leipzig)–– RESILIENT trial RESILIENT trial -- multicenter trial multicenter trial LifestentLifestent vs. PTA vs. PTA -- 206 pt206 pt
11°° patency 79.5 with stenting versus 37.6% with PTA. patency 79.5 with stenting versus 37.6% with PTA. Primary patency 78% at 2 yearsPrimary patency 78% at 2 yearsFracture rate 3.8% at 18 months Fracture rate 3.8% at 18 months FDA approval 2/09 for SFAFDA approval 2/09 for SFA
DrugDrug--eluting Stentseluting Stents
DES (SMART stent, Cordis, sirolimusDES (SMART stent, Cordis, sirolimus--eluting) eluting) have shown mixed resultshave shown mixed resultsSIRROCCO 1 Trial (36 patients)SIRROCCO 1 Trial (36 patients)¹¹–– 66--month data restenosis 0% versus 17%month data restenosis 0% versus 17%–– 1818--month data, restenosis 0% with slowmonth data, restenosis 0% with slow--eluting eluting
stents, 33% with faststents, 33% with fast--eluting stents, and 29% with eluting stents, and 29% with BMSBMS
–– 2424--months, DES >40% with BMS 47%months, DES >40% with BMS 47%SIRROCCO 2 Trial (57 patients)SIRROCCO 2 Trial (57 patients)²²–– 6 month data similar to SIRROCCO 16 month data similar to SIRROCCO 1–– 18 month pooled data showed (mean stent diameter) 18 month pooled data showed (mean stent diameter)
early advantage was lostearly advantage was lost1. Circulation. 2002;106:505-9
2. TCT, 2003

4
ZilverZilver PTXPTX
Paclitaxel eluding selfPaclitaxel eluding self--expanding stentexpanding stentZilverZilver PTX trial PTX trial –– pts randomized to pts randomized to ZilverZilver PTX vs. PTX vs. angioplasty with second randomization (angioplasty with second randomization (ZilverZilver PTX PTX vsvsZilverZilver BMS) in pts with suboptimal PTABMS) in pts with suboptimal PTA–– EventEvent--free survival (death, TLR, amputation, worsening free survival (death, TLR, amputation, worsening
claudicationclaudication) ) -- 86.6% vs. 77.6%86.6% vs. 77.6%–– Vessel Patency at 2 yearsVessel Patency at 2 years
PTA PTA -- 57.8%57.8% ZilverZilver PTX PTX –– 74.8%74.8%Provisional stentingProvisional stentingZilverZilver BMS BMS –– 62.7% 62.7% ZilverZilver PTX PTX –– 81.2%81.2%
–– Fracture rate 0.9%Fracture rate 0.9%
FDA approved 10/11FDA approved 10/11Duration of antiplatelet therapy?Duration of antiplatelet therapy?
StentStent--graftsgraftsInitial Initial ““homehome--mademade”” from balloon expandable stents and from balloon expandable stents and vascular graftsvascular grafts–– High complication rates, 20% early occlusion, high restenosis High complication rates, 20% early occlusion, high restenosis
rates (<20% at 3 years)rates (<20% at 3 years)
Current endovascular grafts more promising, now made Current endovascular grafts more promising, now made with PTFE and with PTFE and nitinolnitinolOnly Gore VIABAHN Only Gore VIABAHN endoprosthesisendoprosthesis with data in peerwith data in peer--reviewed literaturereviewed literature–– 3 year patency rates ~80% (1200 limbs, 9.53 year patency rates ~80% (1200 limbs, 9.5--13.9 cm), higher 13.9 cm), higher
than synthetic graft bypassthan synthetic graft bypass¹¹–– KedoraKedora, et al. 100 patents randomized to , et al. 100 patents randomized to ViabahnViabahn stent vs. femstent vs. fem--
pop bypass with synthetic graft. 1pop bypass with synthetic graft. 1°° patency rate (74%) and 2 patency rate (74%) and 2 °°patency (84%) same in both groupspatency (84%) same in both groups
–– Ideal lesions Ideal lesions -- >1 cm of healthy vessel proximal and distal to >1 cm of healthy vessel proximal and distal to lesion, no lesion, no poplitealpopliteal lesions, at least 1 open lower leg vessel, no lesions, at least 1 open lower leg vessel, no significant calcificationsignificant calcification
–– ?thrombosis risk, collaterals?thrombosis risk, collaterals 1. J Cardiovasc Surg. 2004;3:193-201.
2. J Vasc Surg. 2007;45:10-16.
Directional AtherectomyDirectional AtherectomySilverhawkSilverhawk Plaque Excision Device (Fox Hollow Plaque Excision Device (Fox Hollow Technologies)Technologies)–– FDA approved in June 2003 for peripheral vasculatureFDA approved in June 2003 for peripheral vasculature–– Single center reportsSingle center reports
Univ. Arizona Univ. Arizona –– patency patency -- 11°° 68%, 2 68%, 2 °° 73% at 10 months73% at 10 monthsColumbia Columbia –– patency patency -- 1 1 °° 58%, 2 58%, 2 °° 83% at 18 months83% at 18 monthsCleveland Clinic Cleveland Clinic –– patency patency –– 1 1 °° 43%, 2 43%, 2 °° 57% at 1 year57% at 1 yearSouth Florida South Florida –– patency patency –– 1 1 °° 62%, 2 62%, 2 °° 76% at 1 year76% at 1 yearIowa Iowa -- patency patency –– 1 1 °° 10% at 1 year10% at 1 year
–– TALON Registry TALON Registry –– 19 centers, 601 patients, 1258 19 centers, 601 patients, 1258 lesionslesions
Target lesion revascularization free Target lesion revascularization free –– 90% at 6 months, 80% 90% at 6 months, 80% at 1 yearat 1 year
–– Limb salvage rates universally > 70%Limb salvage rates universally > 70%–– No randomizedNo randomized--controlled trials currentlycontrolled trials currently
SilverhawkSilverhawk atherectomyatherectomy
Crosser CTO catheterCrosser CTO catheterHigh frequency mechanical vibration @20,000 High frequency mechanical vibration @20,000 cycles/sec for crossing cycles/sec for crossing CTOCTO’’ssPATRIOT trial PATRIOT trial –– 84% success crossing wire resistant 84% success crossing wire resistant CTOCTO’’ss, no perforations, no perforations
Novel TherapiesNovel Therapies
Re-entry catheters
Distal protection devices

5
Antiplatelet Therapy after PTAAntiplatelet Therapy after PTA
ASA, ASA, dipyridamoledipyridamole, and , and ticlopidineticlopidine have all have all been shown superior to placebobeen shown superior to placeboNo comparative studies No comparative studies Patients with PAD in CAPRIE had a 24 % Patients with PAD in CAPRIE had a 24 % relative risk reduction in CVA, MI or relative risk reduction in CVA, MI or vascular deathvascular deathMost interventionalist treating with ASA Most interventionalist treating with ASA indefinitely and plavix for one monthindefinitely and plavix for one month
Case #1Case #1
62 62 yoyo male with RLE male with RLE exertionalexertionalclaudicationclaudication and stable anginaand stable anginaRisk factors Risk factors –– FH CAD, HTN, tobacco FH CAD, HTN, tobacco abuseabuseABI at rest 0.54 on RLE, left leg normalABI at rest 0.54 on RLE, left leg normalReferred for LE angiogram, coronary Referred for LE angiogram, coronary angiogramangiogram
Abdominal aorta
Left common iliac artery
Left external iliac artery
Left common femoral artery
6
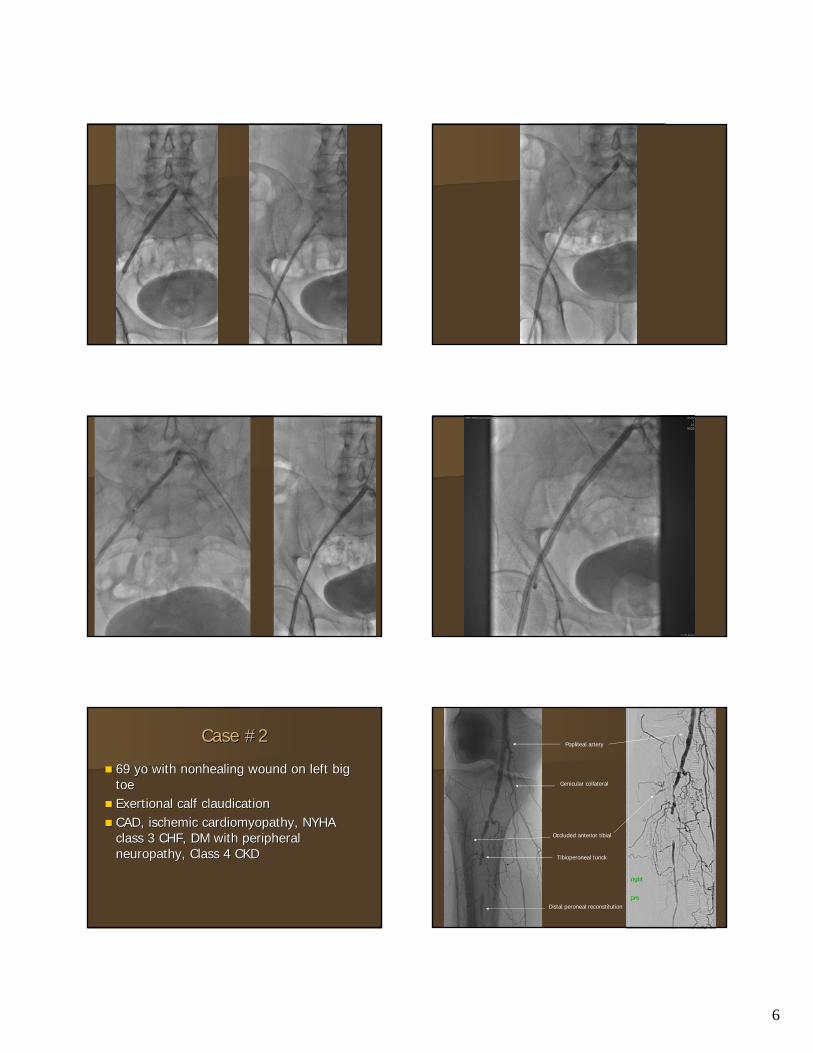
Case #2Case #2
69 69 yoyo with with nonhealingnonhealing wound on left big wound on left big toetoeExertionalExertional calf calf claudicationclaudicationCAD, ischemic cardiomyopathy, NYHA CAD, ischemic cardiomyopathy, NYHA class 3 CHF, DM with peripheral class 3 CHF, DM with peripheral neuropathy, Class 4 CKDneuropathy, Class 4 CKD
Popliteal artery
Genicular collateral
Occluded anterior tibial
Tibioperoneal tunck
Distal peroneal reconstitution
7
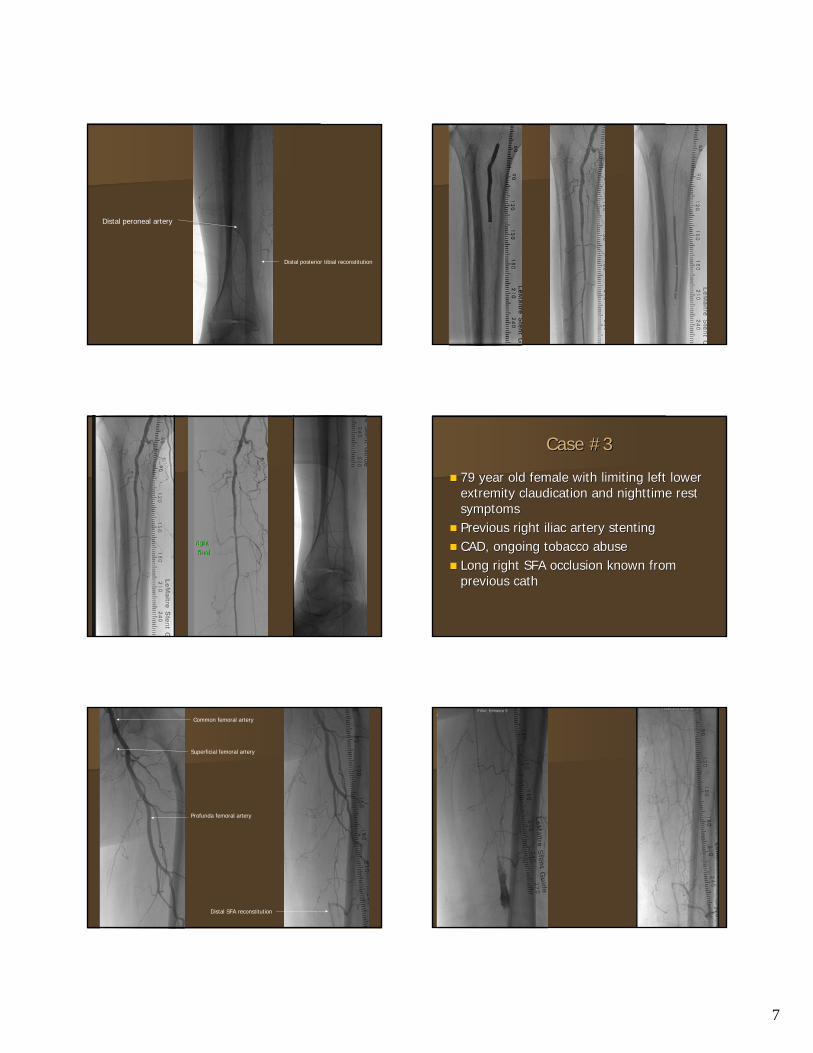
Distal peroneal artery
Distal posterior tibial reconstitution
Case #3Case #3
79 year old female with limiting left lower 79 year old female with limiting left lower extremity extremity claudicationclaudication and nighttime rest and nighttime rest symptomssymptomsPrevious right iliac artery stentingPrevious right iliac artery stentingCAD, ongoing tobacco abuseCAD, ongoing tobacco abuseLong right SFA occlusion known from Long right SFA occlusion known from previous cathprevious cath
Common femoral artery
Profunda femoral artery
Superficial femoral artery
Distal SFA reconstitution

8
Case #4Case #4
80 year old with bilateral non80 year old with bilateral non--healing foot healing foot ulcersulcersDM with severe neuropathyDM with severe neuropathyEvaluated by orthopedist who Evaluated by orthopedist who recommended amputationrecommended amputationPalpable femoral and Palpable femoral and poplitealpopliteal pulses pulses bilaterally without pulses in feetbilaterally without pulses in feet
Peroneal artery
Anterior tibial artery
Dorsalis pedis artery
Plantar artery

9
Anterior tibial artery
Peroneal artery
Dorsalis pedis arteryPlantar artery
Case 5Case 572 72 yoyo with DM, HTN, with DM, HTN, hyperlipidemiahyperlipidemia, CRI, , CRI, ongoing tobacco abuse ongoing tobacco abuse Underwent Underwent aortobifemoralaortobifemoral bypass for AAA and bypass for AAA and bilateral iliac stenosis in 1/2009bilateral iliac stenosis in 1/2009Developed severe limiting Developed severe limiting claudicationclaudication several several months latermonths laterLE ultrasound revealed markedly elevated peak LE ultrasound revealed markedly elevated peak velocities at velocities at anastamoticanastamotic sites (>6 sites (>6 m/sm/s on right, on right, >3 >3 m/sm/s on left, rest ABI 0.61 on right, 0.89 on on left, rest ABI 0.61 on right, 0.89 on left)left)

10
Intervention Intervention -- LeftLeft Intervention Intervention -- RightRight
Case # 6Case # 6
82 year old Madras cowboy with left calf 82 year old Madras cowboy with left calf claudicationclaudicationCAD with multiple CAD with multiple PCIPCI’’ss, chronic stable , chronic stable angina, HTN, angina, HTN, hyperlipidemiahyperlipidemia, ongoing , ongoing tobacco usetobacco useAbsent left pedal pulses, 2+ Absent left pedal pulses, 2+ onrightonrightABI 0.67 on leftABI 0.67 on leftMRA showed focal distal left SFA MRA showed focal distal left SFA stenosisstenosis
SFA

11
PRE POST-ATHERECTOMY
Case #6Case #6
86 year old with left calf 86 year old with left calf claudicationclaudicationRisk factors Risk factors –– DM, previous smoking DM, previous smoking history, history, hyperlipidemiahyperlipidemia, known CAD, known CADAbnormal Abnormal ABIABI’’ssMRA showing diffuse distal SFA and MRA showing diffuse distal SFA and poplitealpopliteal diseasedisease