perpetually perplexing pediatric patients: it’s ... · of perpetually perplexing pediatric cases....
TRANSCRIPT
470 Copyright © SLACK Incorporated
Healthy BabyPractical advice for treating newborns and toddlers.
Abstract
Managing pediatric patients with atypical
rashes and seemingly simple diagnostic ill-
nesses will continue to challenge pediatricians.
Considering the presence of an alternative di-
agnosis or more than one concomitant diag-
nosis or pathogen in the evaluation, although
we try to avoid it, may often lead to better
outcomes. Complex pediatric patients who
vex and perplex each of us are to be expected
in any outpatient general pediatric practice.
[Pediatr Ann. 2014;43(12):470-474.]
This year continued to present more of perpetually perplexing pediatric cases. Some patients were critical-
ly ill, some had peculiar skin findings, and some were just downright baffling. Inter-estingly, most patients had diagnostic and management issues that I had previously discussed in my 36 monthly columns writ-ten for Pediatric Annals.
In another bit of remarkable prescience
attributable to my Pediatric Annals articles, within the November issue of the American Academy of Pediatrics (AAP) News maga-zine,1 four headline articles and one full page advertisement discussed topics that I have also previously written in detail about: 1) “When physicians talk about safe infant sleep practices, parents listen;”2 2) “AAP group offers advice to reduce infants’ expo-sure to arsenic in rice;”3 3) “Study on helmet therapy suffers from several weaknesses”4 (this rebuttal states that helmets actually work well); 4) “U.S. releases broad plan to combat antibiotic resistance;”5 and 5) “Hemangeol TM—an FDA approved drug (propranolol) for infantile hemangioma.”6
CASE 1A 14-year-old white female pre-
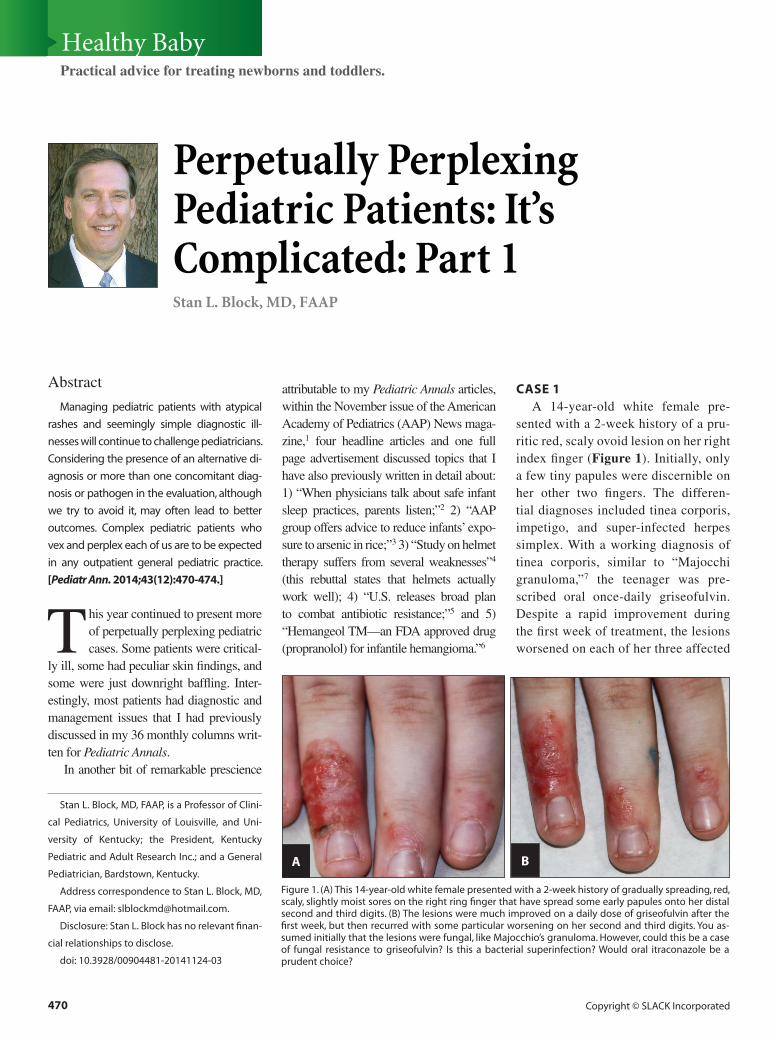
sented with a 2-week history of a pru-ritic red, scaly ovoid lesion on her right index finger (Figure 1). Initially, only a few tiny papules were discernible on her other two fingers. The differen-tial diagnoses included tinea corporis, impetigo, and super-infected herpes simplex. With a working diagnosis of tinea corporis, similar to “Majocchi granuloma,”7 the teenager was pre-scribed oral once-daily griseofulvin. Despite a rapid improvement during the first week of treatment, the lesions worsened on each of her three affected
Perpetually Perplexing Pediatric Patients: It’s Complicated: Part 1 Stan L. Block, MD, FAAP
Stan L. Block, MD, FAAP, is a Professor of Clini-
cal Pediatrics, University of Louisville, and Uni-
versity of Kentucky; the President, Kentucky
Pediatric and Adult Research Inc.; and a General
Pediatrician, Bardstown, Kentucky.
Address correspondence to Stan L. Block, MD,
FAAP, via email: [email protected].
Disclosure: Stan L. Block has no relevant finan-
cial relationships to disclose.
doi: 10.3928/00904481-20141124-03
Figure 1. (A) This 14-year-old white female presented with a 2-week history of gradually spreading, red, scaly, slightly moist sores on the right ring finger that have spread some early papules onto her distal second and third digits. (B) The lesions were much improved on a daily dose of griseofulvin after the first week, but then recurred with some particular worsening on her second and third digits. You as-sumed initially that the lesions were fungal, like Majocchio’s granuloma. However, could this be a case of fungal resistance to griseofulvin? Is this a bacterial superinfection? Would oral itraconazole be a prudent choice?
A B
PEDIATRIC ANNALS • Vol. 43, No. 12, 2014 471
Healthy Baby
fingers by the second week of therapy. Considering the reported increasing frequency of resistant Trichophyton infections, you prescribed daily oral terbinafine for 30 days.
However, the lesions continued to spread slowly over the next week, with no response to the terbinafine. On fur-ther inspection by your partner, the lesions had also become more honey-crusted and weepy—more typical of an impetigo simplex infection. She was prescribed a 10-day course of oral cephalexin, which resulted in rapid amelioration of the lesions.
Was this a primary or a secondary bacterial infection with Staphylococcus aureus? Once again, this shows that dif-ferentiating early skin lesions as caused by either fungal or bacterial pathogens based on clinical appearance is fre-quently perilous. But because growing cultures for bacteria (and also fungus) is so expensive, you are reluctant to typi-cally obtain them for simple lesions. In the future, when you are uncertain about tinea corporis versus impetigo le-sion, you may decide to consider initi-ating coverage for both pathogens, and then discontinuing the antifungal if the lesion responds substantially within 48 hours. A 7-day starter of griseofulvin is not very expensive.
CASE 2 A previously healthy 10-year-old
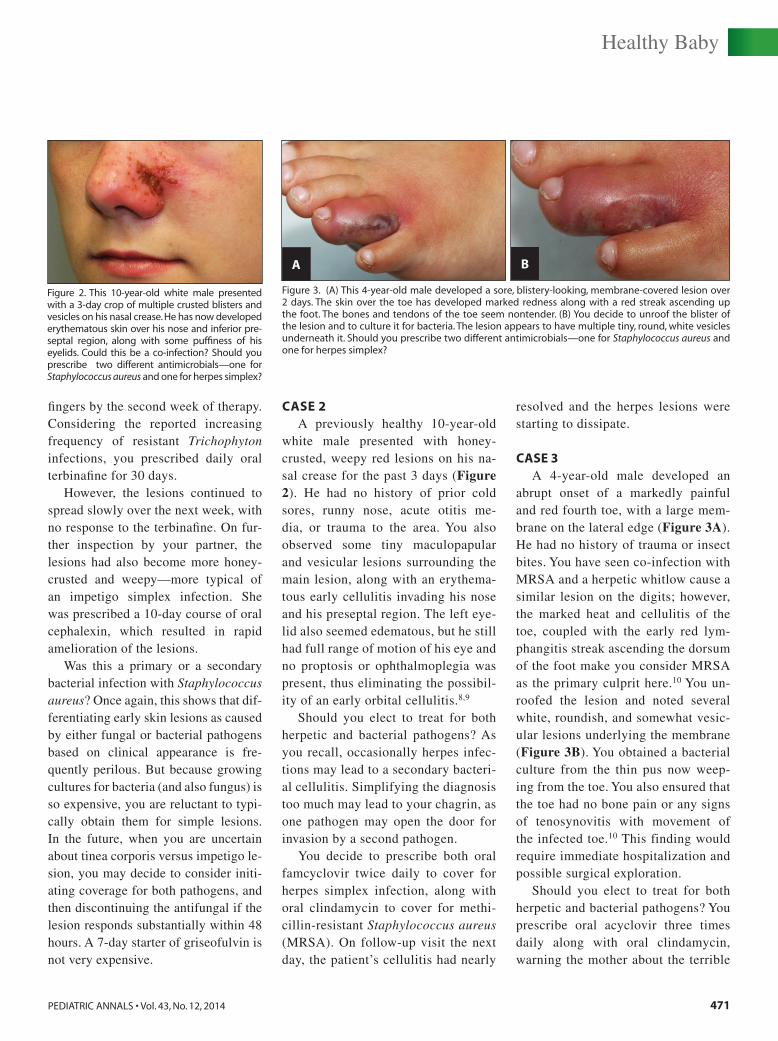
white male presented with honey-crusted, weepy red lesions on his na-sal crease for the past 3 days (Figure 2). He had no history of prior cold sores, runny nose, acute otitis me-dia, or trauma to the area. You also observed some tiny maculopapular and vesicular lesions surrounding the main lesion, along with an erythema-tous early cellulitis invading his nose and his preseptal region. The left eye-lid also seemed edematous, but he still had full range of motion of his eye and no proptosis or ophthalmoplegia was present, thus eliminating the possibil-ity of an early orbital cellulitis.8,9
Should you elect to treat for both herpetic and bacterial pathogens? As you recall, occasionally herpes infec-tions may lead to a secondary bacteri-al cellulitis. Simplifying the diagnosis too much may lead to your chagrin, as one pathogen may open the door for invasion by a second pathogen.
You decide to prescribe both oral famcyclovir twice daily to cover for herpes simplex infection, along with oral clindamycin to cover for methi-cillin-resistant Staphylococcus aureus (MRSA). On follow-up visit the next day, the patient’s cellulitis had nearly
resolved and the herpes lesions were starting to dissipate.
CASE 3 A 4-year-old male developed an
abrupt onset of a markedly painful and red fourth toe, with a large mem-brane on the lateral edge (Figure 3A). He had no history of trauma or insect bites. You have seen co-infection with MRSA and a herpetic whitlow cause a similar lesion on the digits; however, the marked heat and cellulitis of the toe, coupled with the early red lym-phangitis streak ascending the dorsum of the foot make you consider MRSA as the primary culprit here.10 You un-roofed the lesion and noted several white, roundish, and somewhat vesic-ular lesions underlying the membrane (Figure 3B). You obtained a bacterial culture from the thin pus now weep-ing from the toe. You also ensured that the toe had no bone pain or any signs of tenosynovitis with movement of the infected toe.10 This finding would require immediate hospitalization and possible surgical exploration.
Should you elect to treat for both herpetic and bacterial pathogens? You prescribe oral acyclovir three times daily along with oral clindamycin, warning the mother about the terrible
Figure 2. This 10-year-old white male presented with a 3-day crop of multiple crusted blisters and vesicles on his nasal crease. He has now developed erythematous skin over his nose and inferior pre-septal region, along with some puffiness of his eyelids. Could this be a co-infection? Should you prescribe two different antimicrobials—one for Staphylococcus aureus and one for herpes simplex?
Figure 3. (A) This 4-year-old male developed a sore, blistery-looking, membrane-covered lesion over 2 days. The skin over the toe has developed marked redness along with a red streak ascending up the foot. The bones and tendons of the toe seem nontender. (B) You decide to unroof the blister of the lesion and to culture it for bacteria. The lesion appears to have multiple tiny, round, white vesicles underneath it. Should you prescribe two different antimicrobials—one for Staphylococcus aureus and one for herpes simplex?
A B

472 Copyright © SLACK Incorporated
Healthy Baby
palatability of the liquid clindamycin. On follow-up the next day, the cel-
lulitis and lymphangitis had wors-ened, thus necessitating an immedi-ate inpatient admission for parenteral antibiotics. Your outpatient bacterial culture grew MRSA on day 3, whereas the herpes simplex culture performed at the hospital on day 2 was negative (as expected after treatment with 24 hours of oral acyclovir). He received intravenous clindamycin for 5 days; however, the acyclovir was discon-tinued on admission to the hospital. After 24 hours, the lesion had already lost any characteristics of a potential herpetic infection. The entire lesion completely resolved uneventfully over the course of the next week.
CASE 4 A puncture wound by an unknown
object and its secondary cellulitis on the hand of a 2-year-old boy had evolved over 2 days (Figure 4). For-
tunately, the stab wound seemed to be between any bone or tendons, as seen by his lack of any bone pain on palpation or any tendon pain on full range of motion of the fingers. You observed the worrisome mild swelling of the proximal phalanges. But, you have also previously seen too many of these moderately infected hand punc-ture wounds in toddlers during your career to know they need to be taken seriously. You beg the father to allow you to admit the boy to the hospital for high-dose parenteral antibiotics and probable expert surgical explora-tion, but the father declines and asks for “your best oral antibiotic.”
No pus can be expressed from com-pression of the painful lesion. After 24 hours of oral clindamycin, the child re-turns the next day. The entire hand and fingers are moderately swollen now, and the cellulitis was much more exten-sive. You insist that he be hospitalized as the only option for his care. You call
your local hand surgeon to arrange for admission and surgical exploration.
The surgeons are concerned about the severity of the infection and im-mediately arrange for a large incision, drainage, culture, and exploration of the wound. Unfortunately, the surgi-cal resident does not initiate parenter-al antibiotics on the first day postop-eratively because he has been reading that incision and drainage is adequate to manage MRSA lesions smaller than 5 cm. Fortunately, the attending sur-geon rectified this matter immediately the next day by starting intravenous vancomycin and ampicillin/sulbactam due to his high level of concern for providing broad-spectrum bacterial coverage in such a precarious wound of unknown etiology. After 1 week of parenteral therapy, the child recovered fully but the large, open wound on his palm needed management for several more weeks.
CASE 5 This patient illustrates the impor-
tance of always listening to and re-specting the perpetual “Oh by the way, doc, would you look at…” that inevi-tably occurs at the end of several visits every week.
The 2.5-year-old black male was being treated with oral amoxicillin for an episode of acute otitis media diag-nosed earlier in the week. He returned to the office today because of new-on-set fever of 101.5°F for 2 days along with marked irritability, malaise, and decreased appetite. You finish his “directed” physical examination, which is normal, and you find that his ears are improved. In light of his febrile condition, you obtain a com-plete blood count (CBC) that shows a leukocyte count of 23,500 cells/mm3 with a left shift (90% segmented neu-trophils). You are trying to decide how
Figure 4. This afebrile 2-year-old boy was stabbed by an unknown object in the third and fourth digital interspace 2 days ago, and he has now de-veloped this red, very tender, swollen cellulitis sur-rounding the puncture wound. The tendons and bones of the finger and hand appear nontender. You cannot express any pus, and you are aware that simply opening the lesion in your office will require massive interoffice forces to hold him down. You inform the father that with this type of wound infection, in your opinion, hospitalization is needed—both for exploration and for paren-teral antibiotics. The father declines, and instead demands a prescription for an oral antibiotic. You prescribe oral clindamycin 20 mg/kg/day three times per day.
Figure 5. The 2.5-year-old black male developed marked irritability and fever to 101.5°F over 2 days. He has been receiving twice daily oral amoxicillin for an acute otitis media episode diagnosed 4 days ago. His tympanic membrane seems to be improving, and you cannot find anything extraor-dinary on his physical examination. His leukocyte count is 23,500 cells/mm3. As you are trying to de-cide whether to obtain blood cultures and chest radiograph, the mother says he has developed this small hemorrhoid on his anus. How do you proceed?
PEDIATRIC ANNALS • Vol. 43, No. 12, 2014 473
Healthy Baby
far to take his evaluation, including chest radiograph, blood culture, and intramuscular ceftriaxone.
The mother requests that before you finish today, “Would you just mind peeking at his small hemor-rhoid?” Your curiosity is piqued, and you find the anal lesion shown in Fig-ure 5. You now have your diagnosis—this child had a perirectal abscess.
You arrange for transfer to your pe-diatric surgeon for incision and drain-age (I&D). But is the I&D needed? Perhaps the child would have a better outcome if merely parenteral broad-spectrum antibiotics were initiated in-stead. One recent study of perirectal abscesses found that reduced recur-rences and higher cure rates were ob-served with conservative management using only parenteral antibiotics when compared with surgical methods (62% versus 13%).11 The child underwent surgical incision and drainage and re-sponded well to the additional paren-teral antibiotics without any recurrence.
CASE 6 A 6-year old female returns to your
office today with recurrence of fever (102°F) and worsening sore throat. Af-ter being diagnosed with streptococcal pharyngitis last week, she had received 3 days of amoxicillin that has caused her to develop some hives. Amoxicil-lin was discontinued and she was pre-scribed cephalexin instead, which she has been taking for the past 4 days. You note that she still has exudates on her reddened tonsils when you can depress her tongue. You notice that she seems to have some difficulty opening her mouth fully without your help, a not uncom-mon occurrence at this age. Her physical examination is otherwise unremarkable except for some mildly tender, bilateral 2-cm anterior cervical nodes; no hepa-tosplenomegaly or rash is present.
Because of her lymphadenopathy and exudative tonsillitis, you suspect that she most likely has infectious mononucleosis. But, you remember to follow the diagnostic “rules” for any significant anterior lymphadeni-tis: first, obtain a CBC, monospot, and streptococcal antigen detection test (ADT).12 The streptococcal ADT is pointless here, as she is already re-ceiving cephalexin, a quite effective antibiotic for strep throat. Her CBC reveals, however, that her leukocyte count is 21,500 cells/mm3 with 88% segmented neutrophils—quite alarm-ingly high for a simple pharyngitis that is already being adequately treat-ed. This is your clue that something is amiss!
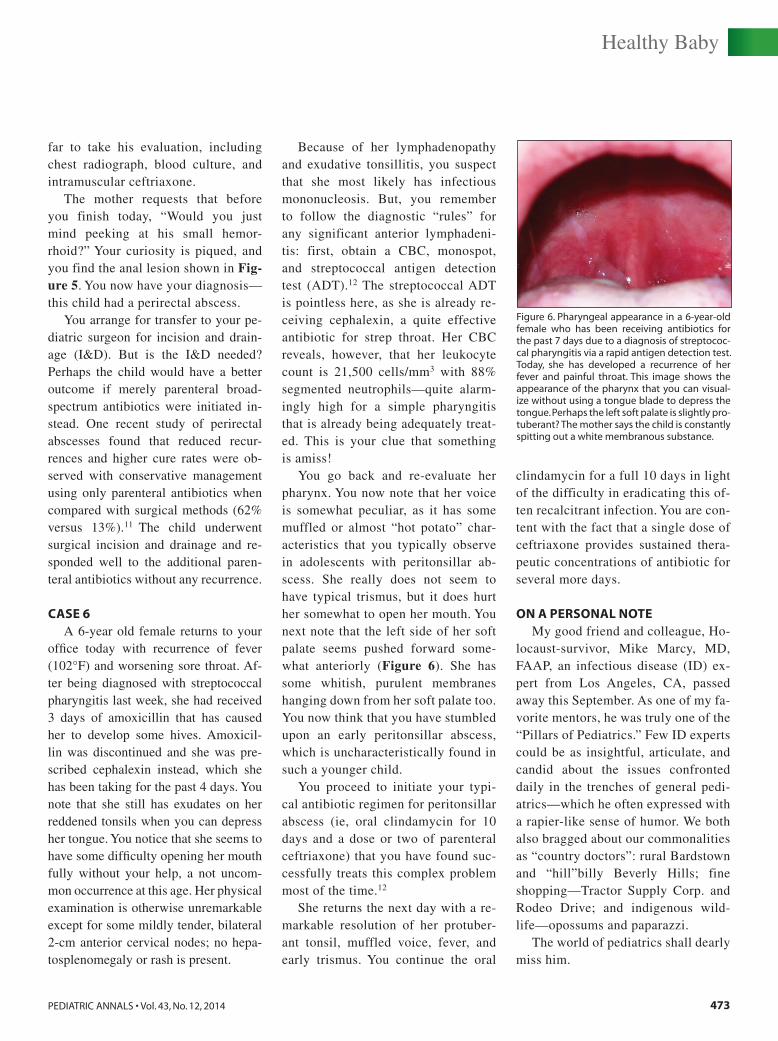
You go back and re-evaluate her pharynx. You now note that her voice is somewhat peculiar, as it has some muffled or almost “hot potato” char-acteristics that you typically observe in adolescents with peritonsillar ab-scess. She really does not seem to have typical trismus, but it does hurt her somewhat to open her mouth. You next note that the left side of her soft palate seems pushed forward some-what anteriorly (Figure 6). She has some whitish, purulent membranes hanging down from her soft palate too. You now think that you have stumbled upon an early peritonsillar abscess, which is uncharacteristically found in such a younger child.
You proceed to initiate your typi-cal antibiotic regimen for peritonsillar abscess (ie, oral clindamycin for 10 days and a dose or two of parenteral ceftriaxone) that you have found suc-cessfully treats this complex problem most of the time.12
She returns the next day with a re-markable resolution of her protuber-ant tonsil, muffled voice, fever, and early trismus. You continue the oral
clindamycin for a full 10 days in light of the difficulty in eradicating this of-ten recalcitrant infection. You are con-tent with the fact that a single dose of ceftriaxone provides sustained thera-peutic concentrations of antibiotic for several more days.
ON A PERSONAL NOTEMy good friend and colleague, Ho-
locaust-survivor, Mike Marcy, MD, FAAP, an infectious disease (ID) ex-pert from Los Angeles, CA, passed away this September. As one of my fa-vorite mentors, he was truly one of the “Pillars of Pediatrics.” Few ID experts could be as insightful, articulate, and candid about the issues confronted daily in the trenches of general pedi-atrics—which he often expressed with a rapier-like sense of humor. We both also bragged about our commonalities as “country doctors”: rural Bardstown and “hill”billy Beverly Hills; fine shopping—Tractor Supply Corp. and Rodeo Drive; and indigenous wild-life—opossums and paparazzi.
The world of pediatrics shall dearly miss him.
Figure 6. Pharyngeal appearance in a 6-year-old female who has been receiving antibiotics for the past 7 days due to a diagnosis of streptococ-cal pharyngitis via a rapid antigen detection test. Today, she has developed a recurrence of her fever and painful throat. This image shows the appearance of the pharynx that you can visual-ize without using a tongue blade to depress the tongue. Perhaps the left soft palate is slightly pro-tuberant? The mother says the child is constantly spitting out a white membranous substance.
474 Copyright © SLACK Incorporated
Healthy Baby
REFERENCES1. American Academy of Pediatrics. AAP News.
Available at: http://aapnews.aappublications.org/content/35/11.toc. Accessed November 19, 2014.
2. Block SL. Simple checklist for the full-term healthy newborn visit. Pediatr Ann. 2012;41(7):270-274.
3. Block SL. Delayed introduction of solid foods to infants: not so fast! Pediatr Ann. 2013;42(4):143-147.
4. Block SL. “Skull-duggery” and the manage-
ment of positional plagiocephaly. Pediatr Ann. 2012;41(12):497-501.
5. Block SL. Improving the diagnosis of acute otitis media: “seeing is believing.” Pediatr Ann. 2013;42(12):485-490.
6. Block SL. Treating infantile hemangiomatosis: a case study. Pediatr Ann. 2013;42(6):230-233.
7. Block SL. Nasolabial rings and things. Pediatr Ann. 2013;42(11):444-447.
8. Block SL. The many faces of facial cellulitis. Pediatr Ann. 2013;42(5):187-190.
9. Block SL. Getting an eyeful of preseptal cel-
lulitis. Pediatr Ann. 2013;42(3):99-102. 10. Block SL. What’s my line? Red streaks in pe-
diatric patients. Pediatr Ann. 2014;43(4):129-134.
11. Christison-Lagay ER, Hall JF, Wales PW, et al. Nonoperative management of peri-anal abscess in infants is associated with de-creased risk for fistula formation. Pediatrics. 2007;120(3):e548-e552.
12. Block SL. Managing cervical lymphadeni-tis—a total pain in the neck! Pediatr Ann. 2014;43(10):390-396.
ERRATUM FOR HEALTHY BABY: MANAGING CERVICAL LYMPHADENITIS—A TOTAL PAIN IN THE NECK!
The article “Managing Cervical Lymphadenitis—A Total Pain in the Neck!” by Stan L. Block, MD, FAAP, which was published in the October 2014 issue of Pediatric Annals (volume 43, number 10), has been amended to include a factual correction. An error was identi-fied subsequent to its original publication.
In Level 1 of Table 1, a punctua-tion error made the last sentence unclear.
doi: 10.3928/00904481-20141124-13
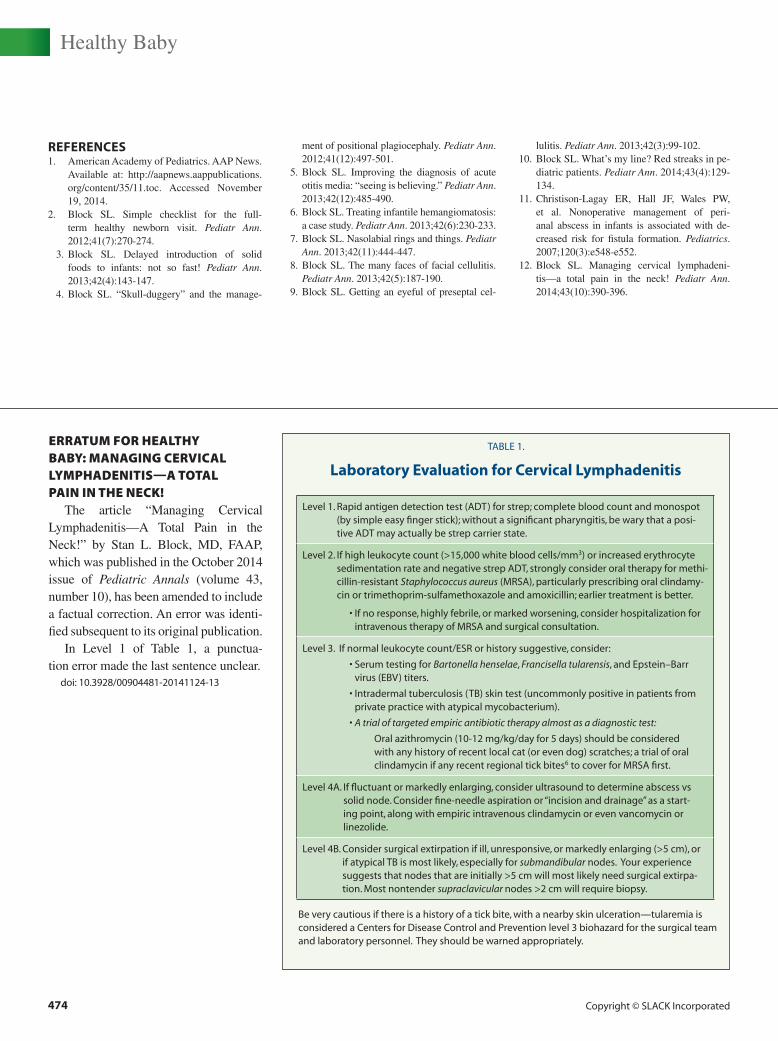
TABLE 1.
Laboratory Evaluation for Cervical Lymphadenitis
Level 1. Rapid antigen detection test (ADT) for strep; complete blood count and monospot (by simple easy finger stick); without a significant pharyngitis, be wary that a posi-tive ADT may actually be strep carrier state.
Level 2. If high leukocyte count (>15,000 white blood cells/mm3) or increased erythrocyte sedimentation rate and negative strep ADT, strongly consider oral therapy for methi-cillin-resistant Staphylococcus aureus (MRSA), particularly prescribing oral clindamy-cin or trimethoprim-sulfamethoxazole and amoxicillin; earlier treatment is better.
• If no response, highly febrile, or marked worsening, consider hospitalization for intravenous therapy of MRSA and surgical consultation.
Level 3. If normal leukocyte count/ESR or history suggestive, consider:
• Serum testing for Bartonella henselae, Francisella tularensis, and Epstein–Barr virus (EBV) titers.
• Intradermal tuberculosis (TB) skin test (uncommonly positive in patients from private practice with atypical mycobacterium).
• A trial of targeted empiric antibiotic therapy almost as a diagnostic test:
Oral azithromycin (10-12 mg/kg/day for 5 days) should be considered with any history of recent local cat (or even dog) scratches; a trial of oral clindamycin if any recent regional tick bites6 to cover for MRSA first.
Level 4A. If fluctuant or markedly enlarging, consider ultrasound to determine abscess vs solid node. Consider fine-needle aspiration or “incision and drainage” as a start-ing point, along with empiric intravenous clindamycin or even vancomycin or linezolide.
Level 4B. Consider surgical extirpation if ill, unresponsive, or markedly enlarging (>5 cm), or if atypical TB is most likely, especially for submandibular nodes. Your experience suggests that nodes that are initially >5 cm will most likely need surgical extirpa-tion. Most nontender supraclavicular nodes >2 cm will require biopsy.
Be very cautious if there is a history of a tick bite, with a nearby skin ulceration—tularemia is considered a Centers for Disease Control and Prevention level 3 biohazard for the surgical team and laboratory personnel. They should be warned appropriately.