personalizzazione della terapia medica · personalizzazione della terapia medica francesco massari...
TRANSCRIPT

Personalizzazione della terapia medica
Francesco MassariU.O.C. di Oncologia Medica d.U.
Azienda Ospedaliera Universitaria Integrata – Verona
2nd YOUNG SPECIALIST RENAL CARE – Verona, 06 Marzo 2015

The quest for precision cancer medicine
The Right Dose ofThe Right Dose of
The Right Drug forThe Right Drug for
The Right Indication forThe Right Indication for
The Right Patient atThe Right Patient at
The Right TimeThe Right Time
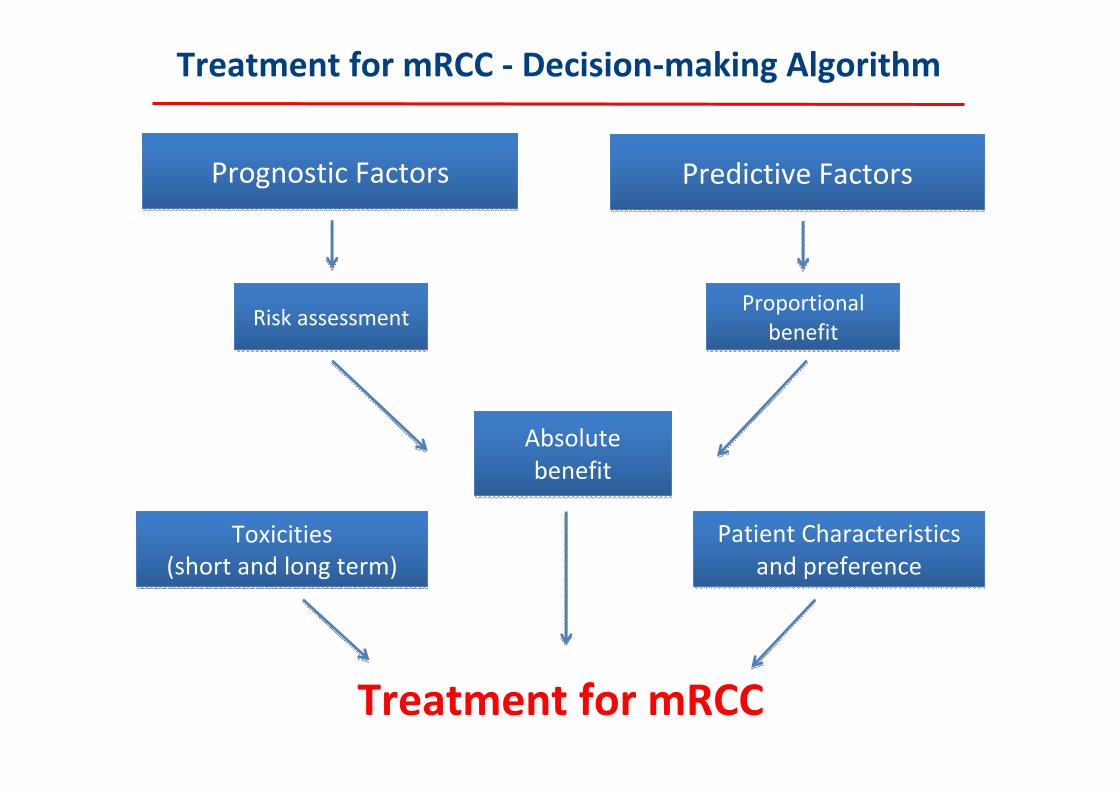
Treatment for mRCC ‐ Decision‐making Algorithm
Prognostic FactorsPrognostic Factors Predictive FactorsPredictive Factors
Risk assessmentRisk assessment Proportional benefit
Proportional benefit
Absolute benefitAbsolute benefit
Toxicities (short and long term)
Toxicities (short and long term)
Patient Characteristics and preference
Patient Characteristics and preference
Treatment for mRCC

Precision Medicine: Prognostic and Predictive Factors
Definition Aim
Prognostic Factors
Provide information on outcome regardless of therapy
To spare unnecessary treatments
Predictive Factors
Provide information on probability of benefit or toxicity from a specific therapy
To spare ineffective treatments

Prognostic Factors in mRCC
Patient Factors
Performance StatusSymptoms
ProinflammatoryMarkers
IL‐6ESR
NeutrophiliaThrombocytosis
C‐reactive proteinTumor Burden
Prior nephrectomySites of metastasesBone MetastasesLDHAnemiaCalciumSodium
Treatment‐relatedFactors
Prior therapyPrior radiotherapy
Disease‐free intervalDiagnosis to treatment interval
Patient X
Patient Y
Patient Z
SURVIVAL

Necrosi tumorale
Tempo dalla diagnosi al trattamento
LDHN° siti
metastaticiTerapie di
combinazione
Sedi di metastasi
Emoglobina Nefrectomia
Presenza di neutrofili intratumorali
Calo ponderaleNetrofilia
IstotipoSintomi
Età
Invasione del grasso perirenale
Grading
Presenza di segni di Infiammazione
Differenziazione sarcomatoide
Ipercalcemia
MultifocalitàPregressa chemioterapia
Albumina basale SessoTNM
Tempo alla metastatizzazione
Livelli TSH
Basso n° CD57+ intratumorali
Piastrinosi
Fosfatasi alcalina
Precedente RT
Dimensioni tumore
Metastasectomia
Trombosi cavaleKPS/ECOG
Courtesy of M. Santoni

Necrosi tumorale
Tempo dalla diagnosi al trattamento
LDHN° siti
metastatici
Terapie di combinazione
Sedi di metastasi
Emoglobina
Nefrectomia
Presenza di neutrofili intratumorali
Calo ponderale
Netrofilia
Istotipo
Sintomi
Età
Invasione del grasso perirenale
Grading
Presenza di segni di Infiammazione
Differenziazione sarcomatoide
Ipercalcemia Multifocalità
Pregressa chemioterapia
Albumina basale Sesso
TNM
Tempo alla metastatizzazione
Livelli TSH Basso n° CD57+ intratumorali
Piastrinosi
Fosfatasi alcalina
Precedente RT
Dimensioni tumore
Metastasectomia
Livello/presenza Trombosi cavale
Alterazioniematochimiche
Caratteristiche del tumore
Stadiazione Trattamento Paziente
KPS/ECOG
Courtesy of M. Santoni

Risk Criteria Can Provide Prognostic Information
Risk Criteria for VGFR‐targeted therapy(Prognostic factors for poor OS)
KPS <80Diagnosis to therapy <1 year
Hemoglobin < lower limit of normalCorrected calcium > upper limit of normal
Neutrophils > upper limit of normalPlatelets > upper limit of normal
0 factors: Favourable risk1‐2 factors: Intermediate risk
≥3 factors: Poor risk
Heng DYC et al. J Clin Oncol. 2009;27:5794‐9.
Heng Prognostic Model [Targeted Agents Age]

Favorable 43 mons
Intermediate 23 mons
Poor 8 mons

IMDC in non‐clear cell RCC
Kroeger et al., Cancer 2013

IMDC in 2nd line targeted therapy
Ko et al., GU Cancer Symposium 2014

Risk Stratification does not predict response to therapy
Predictive biomarkers are needed to better guide treatment selection
Favourable Intermediate Poor
Retrospective analysis of patients with mRCC treated with initial anti‐VEGF therapy
Stratification of patients who had PD as best response by Heng risk group
Heng DY et al. J Clin Oncol. 2011;29(suppl 7):305.

Category Markers
Adhesion molecules cadherin‐6, E‐cadherin, MUC1‐EMA, ICAM‐1, VCAM‐1, ELAM‐1, KSA)
Inducers of immune‐suppression
HLA class 1, IL‐6, IL‐8, IP‐10, MIG, MIP1, B7‐H1, B7‐H4, CD44
Growth factors receptors VEGFR‐3, TGFR‐II
Hypoxia‐induced molecules CAIX, CAXII, CXCR‐4, HIF‐1, VEGF, IGF‐I
Markers of proliferation Ki‐67, PCNA, Ag‐NORs
Cell cycle regulatory proteins p53, bcl‐2, PTEN, cyclin A, Akt, p27
Others VHL, mTOR, ribosomal protein S6, survivin, IMP3, caveolin‐1, PCR, vimentin, fascin, seric amiloide A, NGAL, IGF‐1
Table courtesy of G. Tortora

Renal cell carcinoma
Primary refractory10‐20%
Late relapsing10‐13%
Poor risk15‐25%
Intermediaterisk
50‐70%
Good risk10‐20%
Clear cell RCC 70%
Non‐Clear cell RCC 30%
Papillary type I 9%
Papillary type II 6%
Chromophobe 4‐5%
Oncocytoma 3‐5%
Xp11 traslocation
Associated to neuroblastoma
Tubulocystic
Neuroendocr. tumors
Mesenchymal
Ducts of Bellini <1%
Tubulo‐papillary
t(6,11) traslocation
Mucinous tubular
Her. leiomyomathosis
Unclassified
Tubulocystic
«Poor»poor risk45%
Interm. poor risk40%
«Good»poor risk 15%
PrognosisResponse to TKIs
Slow progressor
Courtesy of M. Santoni
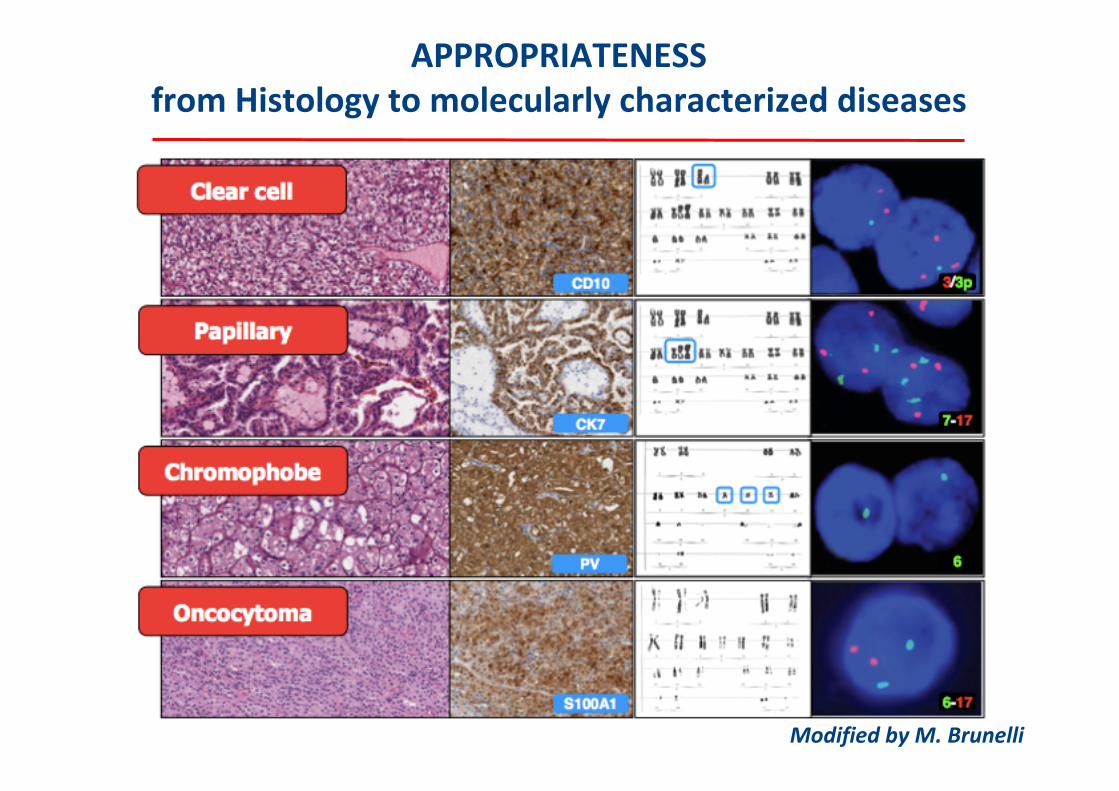
APPROPRIATENESSfrom Histology to molecularly characterized diseases
Modified by M. Brunelli

RCC ‐ HISTOTYPES
• New renal histotypes:
• CLEAR CELL PAPILLARY RCC
• TUBULOCYSTIC CARCINOMA
• ACQUIRED CYSTIC DISEASE (ACD)‐ASSOCIATED RCC
• TANSLOCATION RENAL CELL CARCINOMAs
• THYROID‐LIKE FOLLICULAR CARCINOMA
• Hybrid oncocytic chromophobic tumor
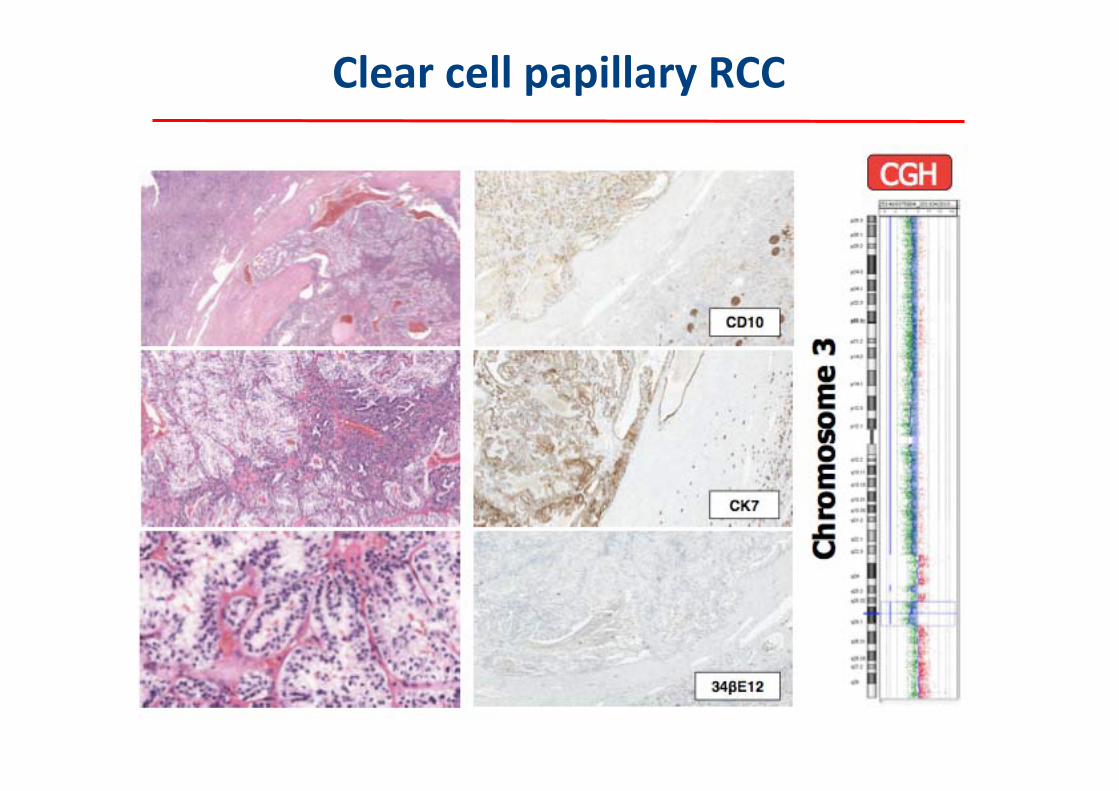
Clear cell papillary RCC

Promise: Progress in Genome Sequencing
Pasche B, Absher D. JAMA. 2011;305:1596.
MR Stratton et al. Nature 458, 719‐724 (2009) doi:10.1038/nature07943
Circos Plots

Promise: Progress in Genome Sequencingc ‐ RCC
The Cancer Genome Atlas Research Network; Nature 2013, doi:10.1038/nature12222

Linehan WM, et al. In: Cancer: Principles and Practice of Oncology. 2006:1139‐1140.
BHD = Birt‐Hogg‐Dubé
FH = Fumarate hydratase
VHL = von Hippel‐Lindau
Clear cell (75%)
Gene: VHL
Papillary Type 2 (10%)
Gene: FH
Papillary Type 1 (5%)
Gene: C‐Met
Chromophobe (5%)
Gene: BHD
Other
Gene expression
A lot of new genes: SEDT2, PBRM1, BAP1, KMD61, NF2…

Promise: Progress in Genome Sequencing ‐ RCC
AA Hakimi et al. Nature Genetics 2013, 45(8), 849‐850

BAP1 and PBRM1 are mutually exclusive
Peña‐Llopis S et al. Nat Genetics 2012

BAP1 activity in RCC
Santoni M, Massari F ‐ submitted
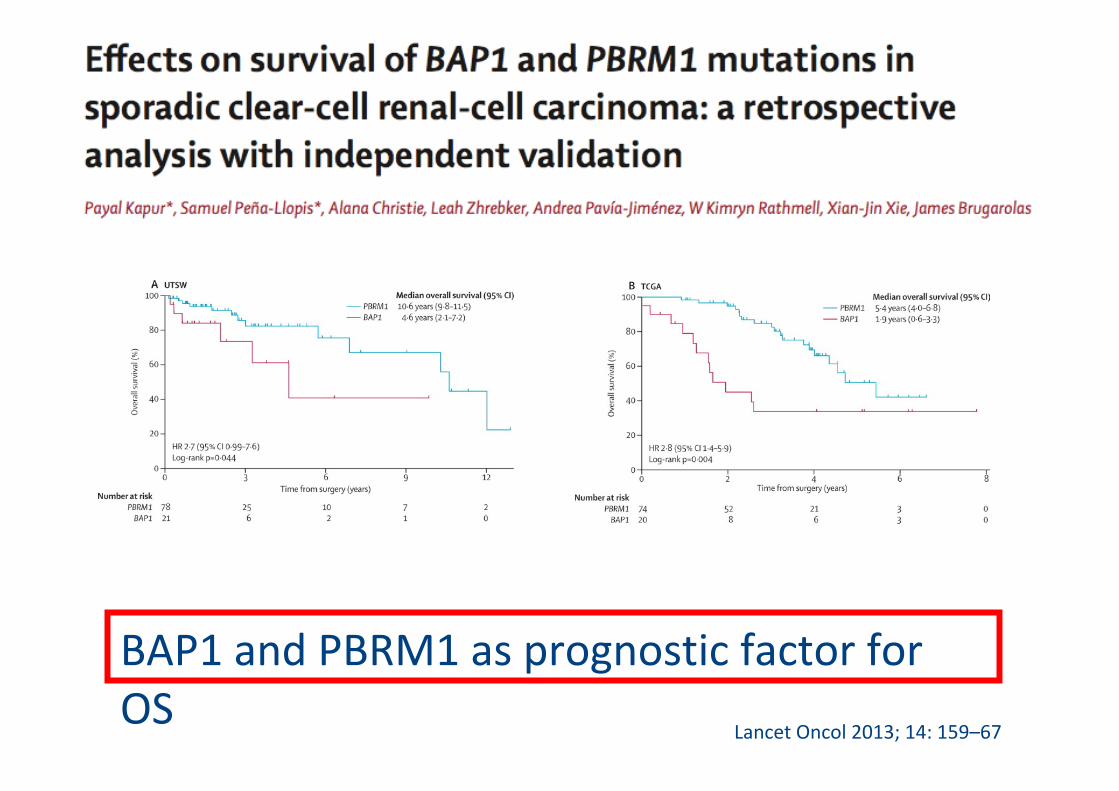
Lancet Oncol 2013; 14: 159–67
BAP1 and PBRM1 as prognostic factor for OS

Genomic signatures are coming for RCC
Escudier at 2014 ASCO Annual Meeting

From Precision Oncology to Personalized Cancer Medicine
“If it were not for the great variability among individuals, medicine might have well been a science and not an art”
Sir William Osler, 1892

Treatment for mRCC ‐ Decision‐making Algorithm
Prognostic FactorsPrognostic Factors Predictive FactorsPredictive Factors
Risk assessmentRisk assessment Proportional benefit
Proportional benefit
Absolute benefitAbsolute benefit
Toxicities (short and long term)
Toxicities (short and long term)
Patient Characteristics and preference
Patient Characteristics and preference
Treatment for mRCC
Patient Characteristics
Patient Characteristics

Treatment for cancer: the elements of the risk/benefit equation
Modified by PF Conte

Cancer and Comorbidities: A Complex Relationship
Modified by PF Conte
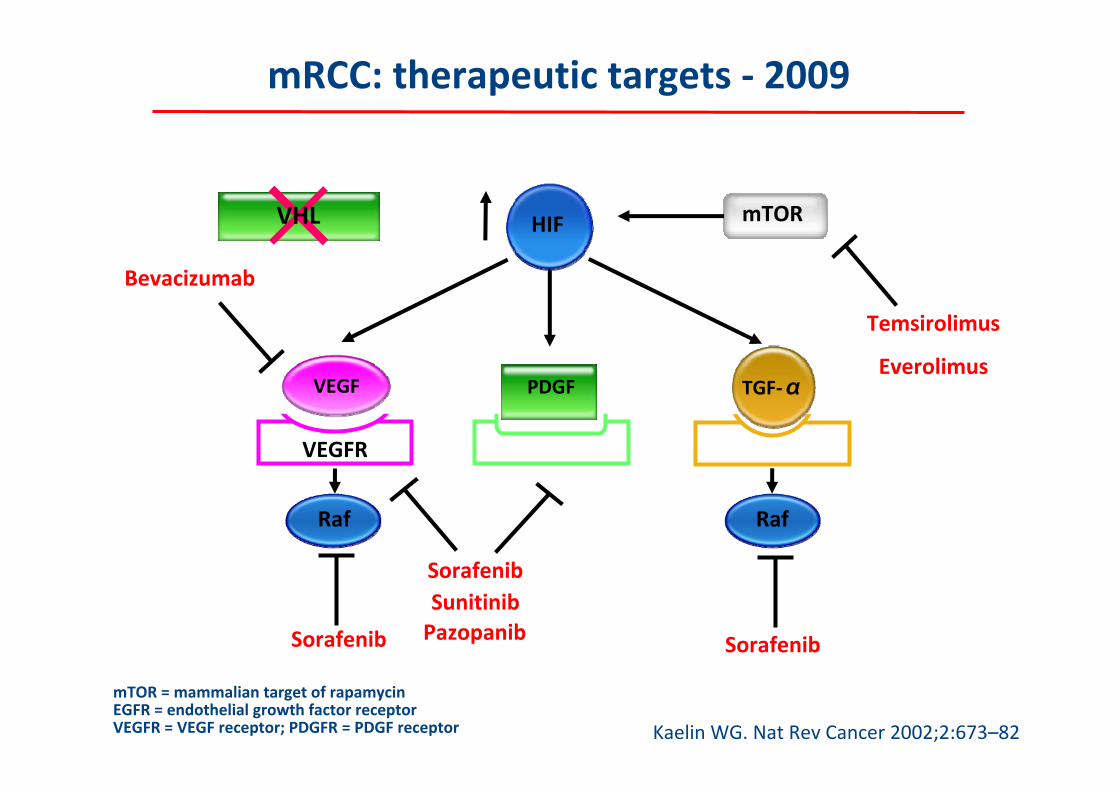
mRCC: therapeutic targets ‐ 2009
Kaelin WG. Nat Rev Cancer 2002;2:673–82
VHL HIF=
VEGFR EGFRPDGFR
Raf
mTOR
SorafenibSunitinibPazopanib SorafenibSorafenib
Temsirolimus
Everolimus
Bevacizumab
mTOR = mammalian target of rapamycinEGFR = endothelial growth factor receptorVEGFR = VEGF receptor; PDGFR = PDGF receptor
Raf
PDGFVEGF TGF‐α

mRCC: therapeutic targets ‐ 2015
Santoni M. et al, Int J Cancer 2013

IMMUNOTHERAPY
The host’s immune function:
1. can control tumor growth
2. can be stimulated
•Melanoma
•Renal cell carcinoma
mRCC: Targeted Immunotherapy
Massari F, Santoni M, Ciccarese C and Santini D, EOBT 2015 ‐ submitted

PD‐1 Blockade as a Strategy for Cancer Immunotherapy
Okazaki T. et al, Nat Immunol 2013, 14:1212–1218

Blocking PD‐1/PD‐1L in RCC tumor microenvironment
Massari F, Santoni M, Ciccarese C. et al, Cancer Treat Rev 2015
CLINICAL ACTIVITY AND SAFETY OF ANTI‐PROGRAMMED DEATH‐1 (PD‐1) (BMS‐
936558/MDX‐1106/ONO‐4538) IN PATIENTS (PTS) WITH PREVIOUSLY TREATED, METASTATIC
RENAL CELL CARCINOMA (MRCC)
• BMS‐936558 is a fully human monoclonal antibody that blocks the PD‐1 co‐inhibitory receptor expressed by activated T cells.
• In the initial portion of a phase 1 study, BMS‐936558 showed promising activity in pts with various solid tumors, including mRCC.
McDermott DF et al, ESMO 2012, abs 784O

Topalian SL, NEJM 2012

CTLA‐4 pathway PD‐1 pathway
Expressed only on T‐lymphocytesExpressed on T, B‐lymphocytes, NK
cells
Ligands: B7.1 (CD80), B7.2 (CD86)Ligands: PD‐L1 (B7‐H1), PD‐L2 (B7‐
DC)
Ligands expressed only on APC cellsLigands expressed on APC and
tumour cells
CTLA‐4 blockade increases CD4+ and CD8+ T cells proliferation
PD‐1/PD‐L1 blockade especially increases CD8+ T cells proliferation
(> CD4+ T cells)
Massari F, Santoni M, Ciccarese C. et al, Cancer Treat Rev 2015

Does PD‐L1 expression alone reliably predict responders?
PROBABLY NOT!!
Massari F, Santoni M, Ciccarese C. et al, Cancer Treat Rev 2015

Issues With PD‐L1 as a Biomarker
• PD‐L1 negativity an unreliable biomarker
Assays are technically difficult, imperfect; results may
differ depending on the antibody/assay (tumor vs
immune cells)
5% expression, tumor heterogeneity, and inducible gene
= sampling error (false negative)
Archived tissue different than recent biopsy
• PD‐L1 expression may be less relevant for combination
therapies
• PD‐L1 expression might be constitutive (no immune
infiltrate)

BMS Phase III Study
Eligibility criteria
• Advanced clear cell or a component of clear cell mRCC
• Progression on or after most recent therapy and within 6 months of study enrollment
• 1 or 2 prior anti‐VEGF• NO prior mTOR inhibitor
Nivolumab 3 mg/Kg IV Q 2wks
Everolimus 10 mg/day PO
RANDOMISATION
N= 822
Primary end point: Overall Survival

Hypoxia triggers increase in cMET expression and activity:
Cell invasion and migration
Cell proliferation
Cell survival
Inhibition of cMET may help overcome acquired resistance to the VEGF pathway
Dual inhibitors of cMET and VEGFr2 such as Cabozantinib are active
MET and Acquired Resistance to VEGFMET and Acquired Resistance to VEGF‐‐targeted Therapies targeted Therapies
Aftab DT et al. Clin Transl Oncol, 2011; 13: 703‐9

Lancet Oncol 2013; 14: 81–87
Patients with localised renal‐cell carcinoma and the MET polymorphism rs11762213 might have an increased risk of recurrence after nephrectomy

cMET expression in clear cell RCC
Courtesy of Bin Teh

CABOZANTINIB (XL 184) CABOZANTINIB (XL 184) in Patients with Metastatic, Refractory RCC
Choueiri T et al. J Clin Oncol 30, 2012 (suppl; abst 4504)
Relapsed or refractory mRCC (N= 25)
• No limit on prior therapies• ECOG PS 0‐1• Measurable disease
CABOZANTINIB140 mg daily(+ single dose rosiglitazone)
Rationale:‐ Drug‐drug interaction study at Phase 1 defined MTD (140 mg)‐ Dose reductions could be employed to optimize tolerability
Study endpoints:‐ Safety and tolerability of cabozantinib‐ Antitumor activity of cabozantinib

Choueiri T et al. J Clin Oncol 30, 2012 (suppl; abst 4504)
CABOZANTINIB (XL 184) CABOZANTINIB (XL 184) in Patients with Metastatic, Refractory RCC

METEOR Study
Primary end point: PFS
Eligibility criteria
• Advanced clear cell or a component of clear cell mRCC
• Progression on or after most recent therapy and within 6 months of study enrollment
• 1 or 2 prior anti‐VEGF• NO prior mTOR inhibitor
Cabozantinib 60 mg/day PO
Everolimus 10 mg/day PO
RANDOMISATION
N= 650

ALLIACE/CALGB Phase II study
Primary end point: PFS
Eligibility criteria
• Locally advanced or metastatic RCC
• No prior systemic treatment
Cabozantinib 60 mg/day PO
Sunitinib 50 mg/day (4/6w)
RANDOMISATION

Treatment for mRCC ‐ Decision‐making Algorithm
Prognostic FactorsPrognostic Factors Predictive FactorsPredictive Factors
Risk assessmentRisk assessment Proportional benefit
Proportional benefit
Absolute benefitAbsolute benefit
Toxicities (short and long term)
Toxicities (short and long term)
Patient Characteristics and preference
Patient Characteristics and preference
Treatment for mRCC
Patient’s preferencePatient’s preference

Who are our patients?

Conclusions
Personalized cancer medicine requires diagnostic and therapeutic options developed according to the individual tumor and patient characteristics, acknowledging that:
•not all the patients require the BEST treatment;
•the BEST treatment is not necessarely so for all the patients;
•the tradeoff between efficacy and toxicity is quite individual