perspectives fall 2013 - optum · pdf fileplans must focus on sales and retention solutions,...
TRANSCRIPT

Cracking the code with new approaches to care delivery and operations
Perspectives
FALL
201
3
Eric MurphyPresident, Payer Solutions, Optum
2
Perspectives
In recent months, we have all been witness to the introduction of ACA and, along with it, a spectrum of competitive, socioeconomic, demographic and government-mandated changes that impact growth, quality and performance strategies. It’s clear that in our current environment, tackling the complexities of our health care system can feel daunting at times, which is why I find it intriguing — and fitting — that we’ve entitled this edition of Perspectives, “Cracking the code with new approaches to care delivery and operations.”
Through this continuum of change, each of us has before us an extraordinary opportunity to make decisions that positively affect the health of our communities and our organizations.
At Optum, we recognize the challenges and new market realities that health plans face. We remain committed to understanding the implications of these changes, and bringing together the brightest minds in health care to discuss how we can meet these challenges head-on and turn strategies into concrete, tactical initiatives.
Enjoy this issue of Perspectives and the insights provided. We hope it serves as a valuable resource to you and your colleagues.
Best regards,
FALL
201
3

Health plans need to transform back office to achieve consumer engagement goals4
3
Plans must provide population health incentives to promote provider risk sharing 9

4
Health plans need to transform back office to achieve consumer engagement goals

5
M any health plans recognize
that their future growth will come
from participating in health care
exchanges and adopting new
business models, but what they
may not have considered is that streamlining their current
back-office operations is essential to realizing that growth
faster and in a manner that builds their relationships
with consumers.
“As the health care market changes in a dynamic fashion,
plans need to focus their attention on their back-office
strategy, on levers that can be pulled by payers to optimize
costs, and on metrics, such as auto-adjudication rates, in
order to fund new initiatives and transformation,” according
to Jim Mapes, senior vice president, Optum, who spoke
Oct. 29 in an Optum webinar, “Transform the Back Office
to Better Engage Consumers on the Front Line.”
Shifting resources from claims to communication
Plans need to find a new paradigm “so that the investments
we make, which include the true time that we spend and
the capital we have on an annualized basis, are focused on
the consumer and on those growth drivers,” Mapes said.
Without a big-picture strategy for the business, he explained,
plans are not going to be able to move forward during
post-health care reform changes, which include accountable
care organizations, value-based delivery and compensation
models, consumer- and individual-based customized care,
and state exchanges. Under this new paradigm, plans must
reexamine the market dynamics that are at play:
• Focus on clinical quality
• Medicaid privatization
• Market consolidation
• Consumer health revolution
• Operational efficiency
• Health benefit exchanges
• Aligning network and incentives
• Payer/provider convergence
These market factors are pushing plans toward three
key areas: 1) population and consumer management;
2) acceleration of automation; and 3) operations and
administrative results. If plans do not move in these
directions, Mapes asserted, they are unlikely to survive in
future market models.
Population and consumer management
Payers need to focus on ensuring growth and financial
success in a consumer-driven marketplace, according to
Mapes. “Consumer engagement is key to moving forward.
When competing in an exchange, plans need to ensure
that the consumer’s first experience is a great experience,”
he said. Plans must focus on sales and retention solutions,
innovatively retool benefits administration and product
management as well as financial risk management, and
communicate with consumers in a clear manner.
Acceleration of automation
“Delivering on goals takes a lot of hard work, but focusing
on automation and data integration will allow plans to
do real-time claims adjudication, provide benefit design
flexibility and facilitate clinical quality/accountable care
integration,” Mapes stated. “Plans need to be able to
turn on a dime when regulatory changes are made, and
automation and technology are the foundation for that
ability. These are becoming the table stakes — the pipes and
wires for building a house.”
Expert presenters
Jim Mapes, Senior Vice
President, Optum
Clay Heinz, Vice President,
Optum
When competing in an exchange, plans
need to ensure that the consumer’s first
experience is a great experience.
— Jim Mapes Senior Vice President, Optum

6
Operations and administration results
Plans also need “a laser-like focus on cost and deployment
strategies, with benefits delivered at a price that keeps them
in business,” Mapes said. Core administration and business
services, payment integrity and claims accuracy, and ICD-10
support solutions can create cost reductions and drive efficiencies,
he noted. “In the past, prompt payment and delivering and
responding accurately to claim inquiries were enough, but now
the stakes are going up. Transparent models make timeliness and
accuracy apparent to everyone and being able to deliver is critically
important,” he said, noting that the results — “true, bottom-line
unit costs and unit price results” — are what need attention.
He further explained that the “truth is in the numbers” when
it comes to claims adjudication. Plans need to reduce their
current operational and administrative costs to less than $10 per
member, per month (PMPM), which can only be achieved through
automation, because auto-adjudication is eight to 10 times less
expensive than manual adjudication. Failing to pursue automation
in this area “leaves a lot of costs on the table and leaves a lot
of dollars on the table from a health care standpoint,”
Mapes emphasized.
He cited an American Medical Association statistic stating that
if claims are paid accurately, an estimated $43 billion1 in cost
savings can be achieved by the industry, and noted that anti-fraud
programs can save 1 percent of medical expense and increase
profitability by roughly 16.7 percent.2 He also remarked that
payment integrity and payment accuracy “can fund a lot of
the initiatives that are needed for a consumer approach”
(see Figure 1).
Payment Accuracy
ProcessAutomation
Consumerismand Population
Health
Your members wantto know::
How do I manage by plan?
How do I manage by health?
How do I manage my money?
Onboarding conciergeprovides:
• Proactive member services
• Designated navigator for your member
• Channels of communication members prefer
• Provider directory
• Completion of health risk assessment
• Appointment scheduling
• Follow-up after doctor visits
• Prescription monitoring
• Microsites specific to member care
• Assistance with bills and claims • EFT payment option• Ways to save solutions
Figure 1Transformation levers
Part of cracking the code to achieving consumer engagement is
understanding what the back office needs to look like, how to set
the transformational drivers in motion — such as payment accuracy
and process automation — and what the strategy will be for
taking the cost and accuracy of delivering health plan benefits to a
new level, according to Jim Mapes, senior vice president, Optum.
“Without the first two, you cannot tackle consumer engagement
and population health,” he said.
Plans need to reduce their current operational and administrative costs to less than
$10 per member, per month (PMPM), which can only be achieved through automation,
because auto-adjudication is eight to 10 times less expensive than manual adjudication.
— Jim Mapes Senior Vice President, Optum
7
Payment Accuracy
ProcessAutomation
Consumerismand Population
Health
Your members wantto know::
How do I manage by plan?
How do I manage by health?
How do I manage my money?
Onboarding conciergeprovides:
• Proactive member services
• Designated navigator for your member
• Channels of communication members prefer
• Provider directory
• Completion of health risk assessment
• Appointment scheduling
• Follow-up after doctor visits
• Prescription monitoring
• Microsites specific to member care
• Assistance with bills and claims • EFT payment option• Ways to save solutions
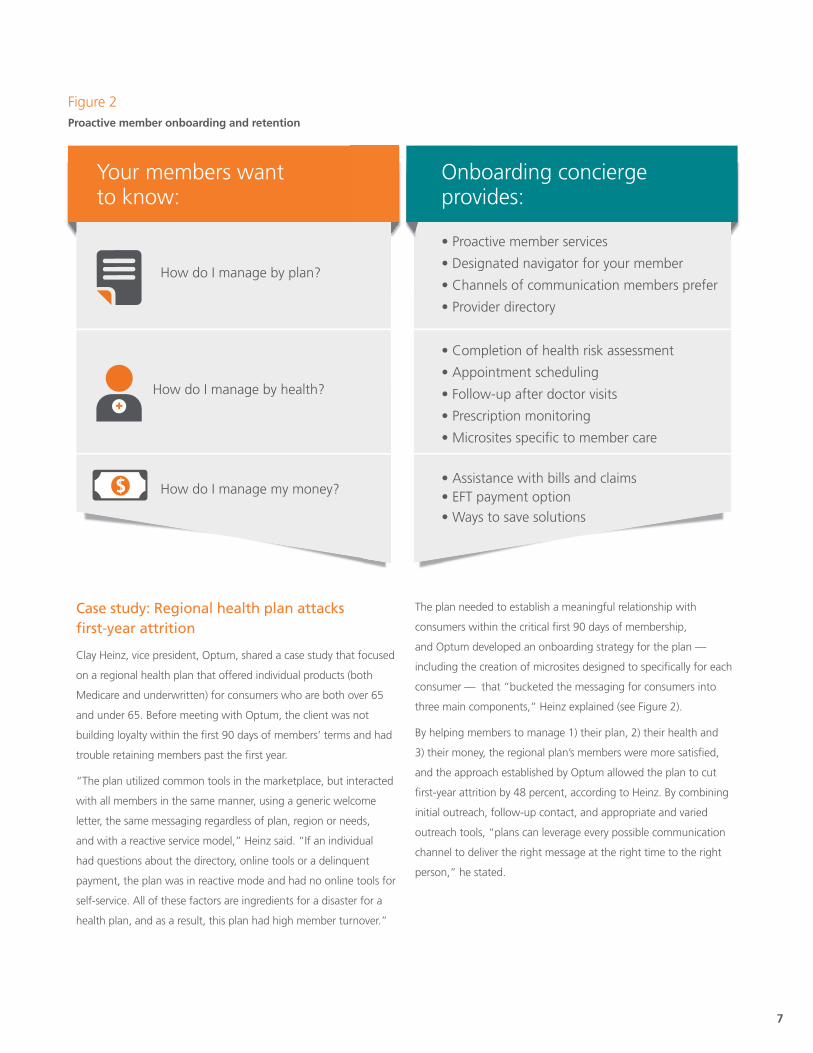
Figure 2Proactive member onboarding and retention
Case study: Regional health plan attacks first-year attrition
Clay Heinz, vice president, Optum, shared a case study that focused
on a regional health plan that offered individual products (both
Medicare and underwritten) for consumers who are both over 65
and under 65. Before meeting with Optum, the client was not
building loyalty within the first 90 days of members’ terms and had
trouble retaining members past the first year.
“The plan utilized common tools in the marketplace, but interacted
with all members in the same manner, using a generic welcome
letter, the same messaging regardless of plan, region or needs,
and with a reactive service model,” Heinz said. “If an individual
had questions about the directory, online tools or a delinquent
payment, the plan was in reactive mode and had no online tools for
self-service. All of these factors are ingredients for a disaster for a
health plan, and as a result, this plan had high member turnover.”
The plan needed to establish a meaningful relationship with
consumers within the critical first 90 days of membership,
and Optum developed an onboarding strategy for the plan —
including the creation of microsites designed to specifically for each
consumer — that “bucketed the messaging for consumers into
three main components,” Heinz explained (see Figure 2).
By helping members to manage 1) their plan, 2) their health and
3) their money, the regional plan’s members were more satisfied,
and the approach established by Optum allowed the plan to cut
first-year attrition by 48 percent, according to Heinz. By combining
initial outreach, follow-up contact, and appropriate and varied
outreach tools, “plans can leverage every possible communication
channel to deliver the right message at the right time to the right
person,” he stated.

8
Want to learn more?
Visit optum.com
or call 1-800-765-6807.
How Optum can helpPartner with Optum to transform your back office to ensure growth and financial
success in a consumer-driven marketplace with a strategy focused on:
• Improved payment accuracy
• Accelerated administrative automation and real-time data
• Proactive member onboarding and retention
He added that satisfied customers are:
• 87 percent more likely to renew.3
• 83 percent more likely to recommend.4
• 43 percent more likely to purchase other products.5
“There has been a paradigm shift to really engage consumers, so
plans need to change to become trusted advisors and co-navigators
with the members,” he said. “Plans don’t want to just be a card in
the member’s wallet anymore.”
Mapes also noted that the most important factors plans need
to consider to enable migration to a new business model are
leveraging data to focus on cost structure and back-office
automation, looking at where the plan needs or wants to be in
three to five years, and determining where to invest capital.
“Being able to deliver from a PMPM standpoint by initiating
projects that create true cost take-out, such as automation,
eliminating redundancy, working with vendors and looking at
globalization, will be necessary as plans refocus their attention on
getting new members and retaining them,” Mapes concluded.
“These levers have to be pulled to be more forward-thinking and
build relationships with consumers. The time to act is now.”
Plans don’t want to just be a card
in the member’s wallet anymore.
— Clay HeinzVice President, Client Practice, Optum
1. American Medical Association, 2013 National Health Insurer Report Card (NHIRC)
2. Optum estimates based on client experience
3. J.D. Power and Associates 2012 study
4. ibid.
5. ibid.
9
Plans must provide population health incentives to promote provider risk sharing

DDuring the past several years, the delivery
of health care has changed dramatically.
These changes, which stem from
government-mandated health insurance
as well as competitive, socioeconomic and
demographic forces, have a direct impact
on health plans’ growth strategies, care
management approaches, and cost and
quality initiatives. Among these initiatives is risk sharing, which calls
for all health care stakeholders to take on more risk in order to
improve health outcomes.
To encourage physicians and hospitals to participate in integrated
risk-sharing models that advance population health management,
health plans will need to develop incentives that are both significant
enough to ensure stakeholder buy-in and simple enough that they
can be implemented in a reasonable and timely manner, according
to Dr. Scott Howell, senior national medical director, Optum.
“There are hundreds of ways to design population health
management programs, but if risk-adjustment model incentives are
minor and bonuses get paid out 18 months later, providers will not
be interested,” Howell said, adding that regardless of how plans
design their programs, they have to first acknowledge that the
status quo in health care is long gone.
“Over the past three years, we have seen one of the most
transformational periods in medicine. Right now, plans are under
exceptional pressures, which include changes in Medicare risk-
adjustment models, sequestration and performance standards,”
he said, “so models have to be extremely fine-tuned to meet cost,
quality and performance goals while firing on all cylinders.”
Howell noted that various factors — from geography to health
information technology (HIT) adoption rates — contribute to success
or failure in meeting important performance measures. “According
to an analysis of key community benchmarks from Optum,1 health
care today is ‘both local and uneven,’” said Howell.
Geographic differences evident for three key measures
To demonstrate the inconsistencies in care, cost and population
health, Howell turned to Optum data, which tracks certain
health care indicators as a way to identify key enablers of better
performance. To understand certain quality benchmarks, the data
set includes avoidable hospitalizations, hospital readmissions and
medication adherence rates. “From a quality-of-care perspective,
looking at large data sets is crucial for understanding geographic
trends,” comments Howell.
Optum data shows the following:
• Avoidable hospitalizations: Commercial data reveals that
avoidable hospitalization rates are lowest in the West, the
Midwest and the Northeast, while the highest rates can be
found in the South and certain rural and urban regions. These
higher rates are associated with chronic illness, low economic
resources and poor patient health behaviors.
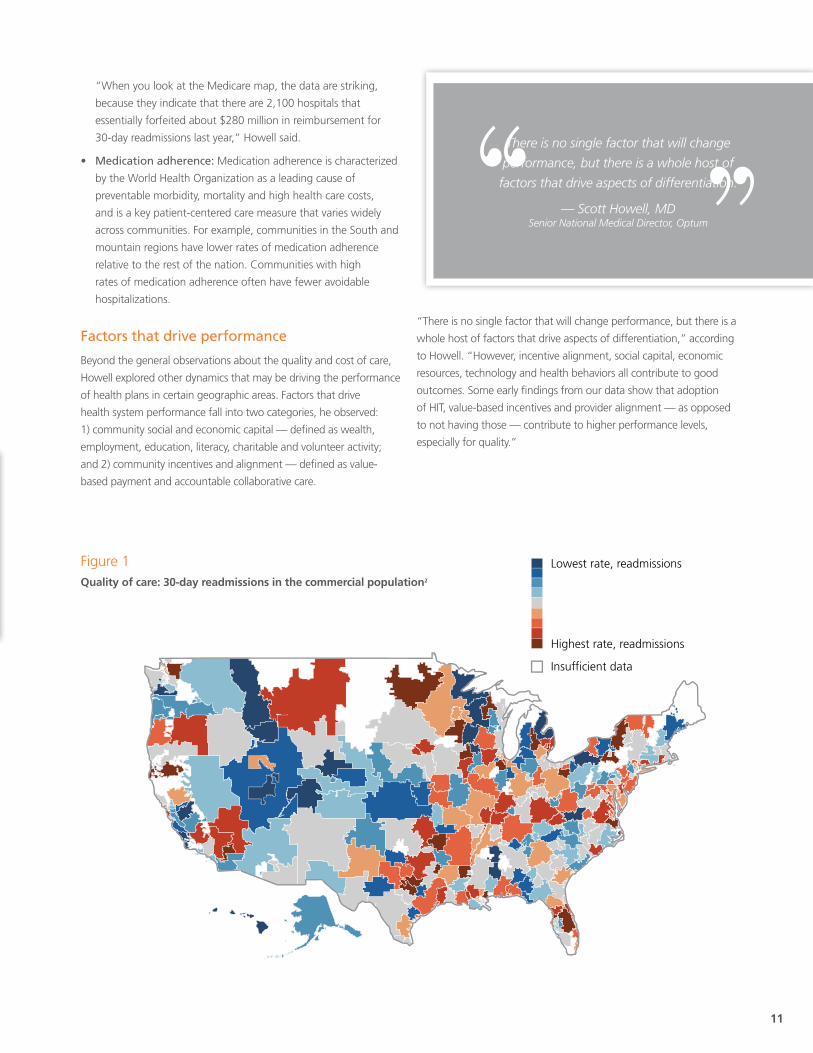
• Hospital readmissions: For 30-day hospital readmissions in
the commercial population, the highest and lowest rates are
less centralized. Among the Medicare population, 18 percent
of patients are readmitted within 30 days, while just 8 percent
of commercial plan patients are readmitted within 30 days
(see Figure 1). The highest rates for readmission for Medicare
patients are concentrated in the Appalachian and Ohio Valley
regions, as well as in the states of Mississippi and Louisiana.
10
Expert presenters
Scott Howell, MD, Senior National Medical Director, Optum
There are hundreds of ways to design population
health management programs, but if risk-adjustment
model incentives are minor and bonuses get paid out
18 months later, providers will not be interested.
— Scott Howell, MD Senior National Medical Director, Optum
11
4,000
3,500
3,000
2,500
2,000
1,500
1,000
500
0
Rat
e p
er 1
,000
per
yea
r
0.170.35
0.550.75
0.951.15
1.351.55
1.751.95
2.152.35
2.552.75
2.953.15
3.353.35
3.753.95
4.154.35
4.685.73
6.737.73
8.739.72
HCC Risk Score
ER Visits
Hospital Admits
Member-centric, collaborative approach
Where Population health managements �t
Retrospective Services Prospective ServicesAcuisition & Retention Population Health Management
Population Health Management
Improving member care and quality of life within an itegrated manner using a framework that leverages best practice advanced analytic capabilities to provide a holistic view of your population and provide the right intervention at the right time to drive member and provider behavior.
Operations & Administration
AttributionCMS Payment Projection & Bid Support
Renue Reconciliation
Retrieval & ReviewsHospital Data Capture Chart Reviews
AttestationsRAPS & EDPS Submissions
Population SegmentationRisk & Quality SegmentationStars Measures
Population SegmentationRisk & Quality SegmentationStars Measures
Analytics & Reporting
Retrieval, Review &
Submission
Care Gap Analysis
RADVClaims Verification (CV)Internal Data Validation
OIG Audits
Marketing ConsultationProvider Training & EducationMember Outreach
ComplianceProvider & Member
Engagement
Sales & Marketing
Benefit Design
Pricing & Underwriting
Network Mgmt.
Health Mgmt.
Quality Improvement
Claims & Payments Mgmt.
ConstituentService
Corporate Admin
Percent of Providers Who Have Population Health Initiatives Completed or Underway
Clinical Integration Initiatives
High-Risk PatientManagement Programs
ReadmissionsReduction Programs
31%
57%
28%
50%
33%
73%
0
10
20
30
40
50
60
70
80PhysiciansHospitals
11: Map: Quality: 30-day Readmissions Commercial population(HR R s >4,000 members )
Highest rate, readmissions
Insufficient data
Lowest rate, readmissionsFigure 1Quality of care: 30-day readmissions in the commercial population2
“When you look at the Medicare map, the data are striking,
because they indicate that there are 2,100 hospitals that
essentially forfeited about $280 million in reimbursement for
30-day readmissions last year,” Howell said.
• Medication adherence: Medication adherence is characterized
by the World Health Organization as a leading cause of
preventable morbidity, mortality and high health care costs,
and is a key patient-centered care measure that varies widely
across communities. For example, communities in the South and
mountain regions have lower rates of medication adherence
relative to the rest of the nation. Communities with high
rates of medication adherence often have fewer avoidable
hospitalizations.
Factors that drive performance
Beyond the general observations about the quality and cost of care,
Howell explored other dynamics that may be driving the performance
of health plans in certain geographic areas. Factors that drive
health system performance fall into two categories, he observed:
1) community social and economic capital — defined as wealth,
employment, education, literacy, charitable and volunteer activity;
and 2) community incentives and alignment — defined as value-
based payment and accountable collaborative care.
“There is no single factor that will change performance, but there is a
whole host of factors that drive aspects of differentiation,” according
to Howell. “However, incentive alignment, social capital, economic
resources, technology and health behaviors all contribute to good
outcomes. Some early findings from our data show that adoption
of HIT, value-based incentives and provider alignment — as opposed
to not having those — contribute to higher performance levels,
especially for quality.”
There is no single factor that will change
performance, but there is a whole host of
factors that drive aspects of differentiation.
— Scott Howell, MD Senior National Medical Director, Optum

12
“Looking at how a very large data set maps out, you can see
where health plan performance is, what types of interventions
are sophisticated and where there are good outcomes,” he says,
“and it all points to a high level of HIT adoption and value-based
incentives.”
However, in individual communities and regions that are not high
performers and that do not have some of the high-performance
drivers in place, providers may not be quite ready to take on more
responsibility for the care of populations.
In a Harris Interactive multi-stakeholder survey commissioned by
Optum in late 2013, 1,602 physicians and 400 hospitals were
asked questions to determine their readiness to take on more
accountability for managing patient care and dollars, improve
population health management and manage population health
initiatives. Although some physicians (34 percent) and hospitals
(43 percent) said they were adequately prepared to take greater
responsibility for managing patient care, only 16 percent of
physicians and 30 percent of hospitals were similarly prepared to
take greater financial risk for that care, Howell explained.
Further, the survey shows that when you add consumers into the
equation (3,400 consumers were surveyed), their perception of
health care delivery in their communities does not always match
up with the doctors and facilities providing that care. For example,
Howell pointed out that although 38 percent of consumers stated
that health care is coordinated in their communities, only 22 percent
of physicians and 29 percent of hospitals thought that was true.
And when asked whether they thought patients received needed
preventive care, 51 percent of physicians thought they did, while
only 35 percent of consumers thought so.
Integrated risk adjustment drivers must be in place
To drive population health management, which Howell defines as
“improving member care and quality of life in an integrated manner
using a framework that leverages best practice analytic capabilities
to provide a holistic view of your population and provide the
right intervention at the right time to drive member and provider
behavior,” providers need to implement such population health
initiatives as clinical integration, high-risk patient management and
readmission reduction programs.
Surprisingly, the survey results show that only one-third of providers
have implemented population health initiatives or have them
underway (see Figure 2). Hospitals are further along in meeting
those goals. This delta in implementation rates is likely due to
hospitals having greater incentives in place to do so and in providers’
“wait-and-see” approach to developing value-based payment
capabilities, said Howell.
The factors behind this provider reluctance to adopt value-based
opportunities stem from concerns over complexity, administrative
costs and increased risk without adequate reward, according to
Howell. “The marginal aspect of this situation is determining how
much of a reward you need to provide to move forward on the risk
front,” he said. “You can’t add risk without enough reward to keep
the lights on. Also, providers want to keep things simple so they can
understand the targets; plans need to design value-based programs
with this information in mind.”
Although some physicians (34 percent) and hospitals (43 percent) said they were adequately prepared
to take greater responsibility for managing patient care, only 16 percent of physicians and 30 percent
of hospitals were similarly prepared to take greater financial risk for that care.
— Scott Howell, MD Senior National Medical Director, Optum
...In individual communities and regions that are
not high performers and that do not have some
of the high-performance drivers in place,
providers may not be quite ready to take on more
responsibility for the care of populations.
— Scott Howell, MD Senior National Medical Director, Optum

13
4,000
3,500
3,000
2,500
2,000
1,500
1,000
500
0
Rat
e p
er 1
,000
per
yea
r
0.170.35
0.550.75
0.951.15
1.351.55
1.751.95
2.152.35
2.552.75
2.953.15
3.353.35
3.753.95
4.154.35
4.685.73
6.737.73
8.739.72
HCC Risk Score
ER Visits
Hospital Admits
Member-centric, collaborative approach
Where Population health managements �t
Retrospective Services Prospective ServicesAcuisition & Retention Population Health Management
Population Health Management
Improving member care and quality of life within an itegrated manner using a framework that leverages best practice advanced analytic capabilities to provide a holistic view of your population and provide the right intervention at the right time to drive member and provider behavior.
Operations & Administration
AttributionCMS Payment Projection & Bid Support
Renue Reconciliation
Retrieval & ReviewsHospital Data Capture Chart Reviews
AttestationsRAPS & EDPS Submissions
Population SegmentationRisk & Quality SegmentationStars Measures
Population SegmentationRisk & Quality SegmentationStars Measures
Analytics & Reporting
Retrieval, Review &
Submission
Care Gap Analysis
RADVClaims Verification (CV)Internal Data Validation
OIG Audits
Marketing ConsultationProvider Training & EducationMember Outreach
ComplianceProvider & Member
Engagement
Sales & Marketing
Benefit Design
Pricing & Underwriting
Network Mgmt.
Health Mgmt.
Quality Improvement
Claims & Payments Mgmt.
ConstituentService
Corporate Admin
Percent of Providers Who Have Population Health Initiatives Completed or Underway
Clinical Integration Initiatives
High-Risk PatientManagement Programs
ReadmissionsReduction Programs
31%
57%
28%
50%
33%
73%
0
10
20
30
40
50
60
70
80PhysiciansHospitals
11: Map: Quality: 30-day Readmissions Commercial population(HR R s >4,000 members )
Highest rate, readmissions
Insufficient data
Lowest rate, readmissionsFigure 2Population health management: Are providers ready to manage population health initiatives?3
A member-centric, collaborative approach is ideal, he noted. “Plans
need to surround the member in an interactive and integrative
manner,” he said, adding that Optum collaborates with a health
plan’s quality and clinical teams and works with its disease
management and other program staff to drive programs toward a
prospective service model. Prospective services include:
• Analytics and reporting (population segmentation, risk and
quality segmentation, Stars measures implementation)
• Care gap analysis (HEDIS/Stars, HQPAF, chronic condition
management, in-home assessments)
• Provider and member engagement (market consultation,
provider training and education, member outreach)
“Looking at the current state of the nation, it is important to
integrate population health, cost measures and quality initiatives
to drive change moving forward,” Howell says. “As seen in these
data, we are not there yet, but we need to start heading in that
direction…to move the needle on risk management, he advises. “It
is going to be important to ramp up from where we are today, so
that five years from now, the whole industry will be willing to take
more risks based on outcomes and performance.”
Surprisingly, the survey results show that only
one-third of providers have implemented population
health initiatives or have them underway.
— Scott Howell, MD Senior National Medical Director, Optum

14
Want to learn more?
Visit optum.com
or call 1-800-765-6807.
How Optum can helpOptum helps health plans improve care by the accuracy, thoroughness and
timeliness of their reporting through outsourced services that include a clinical
orientation. Our solution set helps you:
• Implement an integrated risk and quality program.
• Review and collect information through retrospective data capture.
• Submit and manage data transactions.
• Manage risk adjustment analytics and reporting.
• Prospectively engage with providers and members.
1 The Optum Labs Community Measures Project provides new data and analyses on the performance of the health care system in 306
communities across the United States; its results underscore that health care today is both local and uneven. The Optum Labs Community
Measures Project evaluates the local cost of care for commercially-insured and Medicare populations, utilization of health care services
(including analyses that pinpoint potentially avoidable care and excessive use), and quality of care. It uses a portfolio of measures that are
well validated and capture a range of outcomes across points of care and health care conditions. Performance measures include readmission
rates, physician compliance with chronic care guidelines and patient medication adherence. Population health is captured in measures of life
expectancy and prevalence of disease.
2 Commercial claims as analyzed by Optum
3 Multi-stakeholder Study, October 2013 conducted for The Optum Institute by Harris Interactive
15
Clay Heinz, Vice President, Client Practice, Optum
Heinz is responsible for developing new business concepts at Optum. As vice president of Client Practice, he lends his expertise and innovation to payers, providers, employers and government entities in the health care marketplace. His mission is to empower consumers to make better health care decisions. Prior to joining Optum, Heinz worked for Extend Health, where he developed work force readiness, ranging from the development of training to licensing and appointments. He also managed relationships with several health plan payer partners, ensuring compliance, policy reconciliation and systems integration.
Scott Howell, MD, Senior National Medical Director, Optum
Howell is responsible for risk adjustment, quality performance and predictive modeling. Prior to Optum, he was the regional chief medical officer (RCMO) for the Northeast Region of AmeriChoice, Inc., focusing on the Medicaid and Dual SNPs populations. He also served as the medical director for managed care at the AIDS Healthcare Foundation along with having responsibility for international consulting in Russia, Ukraine, Guatemala, Honduras and Haiti.
Jim Mapes, Senior Vice President, Optum
Mapes is focused on delivering technology and services-based solutions to hospitals, payers, physicians, life sciences companies and other key players in health care. He is responsible for all facets of the business including global strategy, finance, executive leadership, operations and business development. He has more than 25 years of experience in developing client relationships and deploying a unique combination of business, clinical and technology solutions for the health care industry. Mapes has worked in various Fortune 50 firms as a technology executive and business leader.
Perspectives
Expert presenters
Fall 2013
Biographies

optum.com
13625 Technology Drive, Eden Prairie, MN 55344
OptumTM and its respective marks are trademarks of Optum, Inc. All other brand or product names are trademarks or registered marks of their respective owner. Because we are continuously improving our products and services, Optum reserves the right to change specifications without prior notice. Optum is an equal opportunity employer.
OPTPRJ2881_Print 12/13 © 2013 Optum, Inc. All rights reserved.
Cracking the code with new approaches to care delivery and operations
Perspectives
FALL
201
3
Visit optum.com
or call 1-800-765-6807.