pharmaceutic development issues for hepatitis b nathaniel a. brown, m.d. sr. vice president,...
TRANSCRIPT

Pharmaceutic Development Issuesfor Hepatitis B
Nathaniel A. Brown, M.D.Sr. Vice President, Hepatitis Clinical Research
Idenix Pharmaceuticals
Cambridge, MA, USA

Topics for Discussion
HBV versus HIV infection: Disease differences & implications for treatment studies
Experience with efficacy endpoints in HBV trials
Compensated liver disease
Decompensated liver disease
Pending sources of new types of clinical data
Key issues for discussion – an Industry consensus

HBV and HIV Infection:Disease Differences and Implications for Treatment Studies
2 forms of endstage HBV: decompensated cirrhosis & HCC. Both associated with HBV replication, but distinct pathogeneses
Antiviral therapy may not affect both
Chronic HBV infection can revert to low-replicative states (HBeAg and HBsAg seroconversion), spontaneously or with therapy, with minimal risk of disease progression
Treatment can be stopped in some hepatitis B patients:lifelong care, but not lifelong treatment
Chronic HBV infection generally slower than HIV to cause irreversible damage (10-50 years for HBV vs. 5-20 years for HIV), in untreated patients and after treatment-related breakthrough
HBV and HIV Infection:Disease Differences and Implications for Treatment Studies
Differences in target cells and replication templates:
- 1° target cells more regenerable for HBV than for HIV
- hepatocytes turn over; HIV infects long-term cell types
- HBV templates not maintained by cellular polymerases
- HBV polymerase fidelity 10-fold better than HIV RT
Treatment of chronic HBV infection potentially associated with clearance of replication templates over time
HBV less likely to be associated with early resistance (e.g. 3TC), and chance for loss of drug-resistant HBV templates – over time, or with switch to new antiviral Rx

Hepatitis B vs. HIV Infection:Goals for combination therapy in HBV infection
Improve efficacy – increase frequency of durable responses
OR: Improve outcomes in refractory or high-risk subgroups
Decompensated cirrhotics Transplant recipients Co-infected patients Possibly HBeAg-negative (pre-core mutant) disease
Improved efficacy must offsetcosts & potential additional toxicities of combination regimens

Efficacy Endpoints in Hepatitis B Compensated Liver Disease
Serologic:
HBeAg loss, seroconversion (gain of anti-HBe)
HBsAg loss, seroconversion (gain of anti-HBs)
ALT normalization
Serum HBV DNA levels – unamplified assays and PCR assays
Composite serologic responses: “Virologic Response”, etc
Histologic:
Necroinflammatory scoring – Knodell, Ishak, ranking
Fibrosis/cirrhosis scoring – Knodell, Ishak, ranking

HBeAg Seroconversion (HBeAg-, HBeAb+) Over 4 Years58 LAM100 Patients (Asian Multicenter Study)
0
10
20
30
40
50
60
70
80
0 52 104 156 208
Weeks of Therapy
% withResponse
All
ALT Norm
ALT >1 xULN
ALT >2 xULN
Minimal seroconversion in patients with normal ALT
HBeAg seroconversion proportionally greatest in first year

Baseline Factors and HBeAg Seroconversion Multivariate Analysis of Integrated Phase III Lamivudine Data
(Perrillo et al., Hepatology, July 2002)
A multivariate analysis used stepwise logistic regression to investigate the influence of baseline factors on HBeAg seroconversion + loss of detectable HBV DNA (hybridization assay) at week 52.
The most important pre-treatment factors, in order, were:
Treatment (p 0.001)
Baseline ALT (p 0.001)
HAI score (p 0.001)
HBV DNA values (p = 0.11)

Post-Treatment Durability of HBeAg Responses Integrated Phase III Data: LAM100 Patients, 52 Weeks of Therapy
77 76 74 77
0
10
20
30
40
50
60
70
80
90
HBeAg Loss HBeAg LossHBeAb PresentHBV DNA n.d.*
HBeAg LossHBeAb PresentHBV DNA n.d.*on 2 occasions
n=45/58 n=31/40 n=26/32 n=18/23
Percent ofPatients with
ResponseMaintained3-4 Months
Post-Rx
HBeAg Response Status at End of Therapy (Week 52)
HBeAg LossHBV DNA n.d.*
*n.d. = HBV DNA not detectable by solution hybridization

Histology as an Efficacy Endpoint in HBV Trials:Important Findings
Suppression of HBV replication ( HBV DNA) is associated with decreased necroinflammatory activity in liver
IFN and LAM trials: 3-4 point HAI reductions occurred in non-seroconverters with non-detectable HBV DNA (by hybridization)
LAM and ADV trials – some histologic worsening (including fibrosis) in placebo recipients after 1 year
Fibrosis/cirrhosis improves with antiviral Rx in some patients
Histologic stage of disease (cirrhosis vs. no cirrhosis) does not appreciably influence responses to nucleosides
Antiviral Rx associated with decreased stellate cell activation
cccDNA in liver decreases with long-term antiviral Rx

Histology as an Efficacy Endpoint: Problems
Liver bx – picture of disease, but “only a snapshot in time & space”
Waxing/waning disease, and biopsy sampling error, reduce prognostic value of liver biopsy in chronic HBV infection
Histologic scoring has wide inter- and intra-observer variation
Accounting for missing biopsy data (10-40% of total) in placebo-controlled vs. active-controlled studies
Implications for efficacy: non-inferiority, superiority
Sample size calculations problematic due to unpredictable extent of missing data and scoring imprecision
Liver biopsies uncommonly used in practice: sometimes for disease staging, but almost never to monitor response to Rx
Many investigators cannot participate in global HBV trials that require biopsies (especially in China and elsewhere in Asia)

Relationships Among Efficacy Responses in Trials
Broad relationship of efficacy endpoints evident in results of placebo-controlled lamivudine and adefovir trials
Clinical improvements (histology, ALT, etc) occurred disproportionately in patients on active antiviral treatment
Precise correlations between efficacy parameters difficult to assess
Addressed by others today
Integrated phase III lamivudine data: Serologic markers (ALT, HBV DNA) adequately predicted lack of histologic worsening at Week 52
ALT normalized or improved by 50%: HAI “worse” at W52 in only 5%
HBV DNA non-detectable or by 50%: HAI “worse” at W52 in only 9%
Efficacy Endpoints in Hepatitis B Decompensated Liver Disease
Survival
Improvement in Child-Pugh score
Improvement in bilirubin, albumin, PT, etc
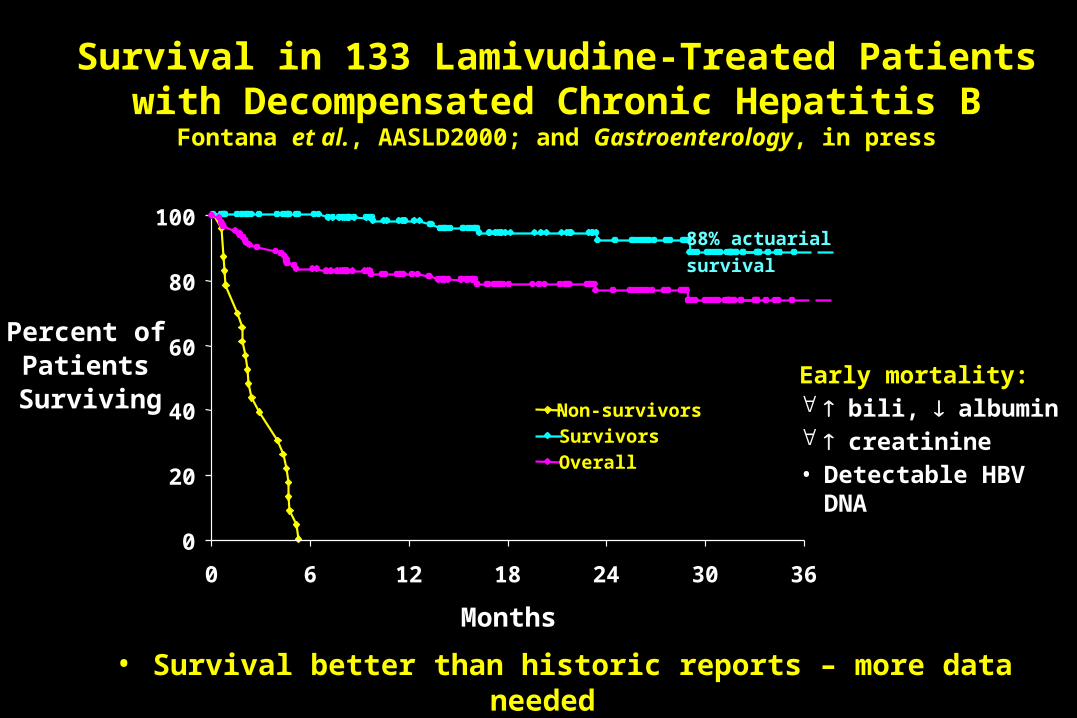
88% actuarial
survival
Non-survivorsSurvivors
Overall
Early mortality: bili, albumin creatinine• Detectable HBV DNA
0
20
40
60
80
100
0 6 12 18 24 30 36
Months
Percent of Patients
Surviving
Survival in 133 Lamivudine-Treated Patientswith Decompensated Chronic Hepatitis B
Fontana et al., AASLD2000; and Gastroenterology, in press
• Survival better than historic reports – more data needed

Child Pugh Scores70 Lamivudine-treated patients, 50 with data >6 months (Hann et al., DDW2000)
Mean/median baseline CP score 9.3/9.0
Mean/median last visit CP score 7.6/7.0
Improved by 2 points 21 (42%)
Unchanged (Changed by < 2 points) 26 (52%)
Worsened by 2 points 3 (6%)

Biochemical Changes in Lamivudine Treated Patients27 Non-Transplanted Patients (Perrillo et al., Hepatology 2001)
n= 27 n=22 n=17Baseline week 52 week 104
Median
Albumin
(g/dL)
Median
Bilirubin(mg/dL)
4
3.5
3
2.5
1.5
2
2 1

Efficacy Endpoints in HBV Trials: Conclusions
ALT & histologic responses related to HBV DNA suppression
HBV DNA suppression also associated with HBeAg responses
But immune response ( ALT pre-treatment) also required
Serologic monitoring (ALT & HBV DNA) predicts lack of histologic worsening
Clinical and biochemical signs of disease progression are rare during 1‑2 year trials in compensated patients
Some histologic deterioration seen in placebo recipients
Improvements in hepatic function seen in patients with decompensated disease – more data needed
Improved or stabilized CP scores, bilirubin, albumin Possible survival benefit in decompensated patients

Pending Sources of New Types of Clinical Data
Current nucleoside/tide comboRx trials in treatment-naïve patients: Glaxo-Gilead collaborative trials, LAM + ADV Idenix Phase IIb trial, LdT + LAM
Large clinical endpoints trial (Glaxo NUCB4006) >600 Asian patients with documented HBV cirrhosis LAM vs Placebo, sequential analysis Stopped by DSMB for efficacy on clinical disease progression
Perinatal HBV Transmission Study (Glaxo NUC30914) 25% failure rate (to vaccine + HBIg) in high-viremic mothers 3-arm randomized trial (2:2:1):
vacc + HBIg + PLA vs. vacc + HBIg + LAM vs. vacc + LAM LAM given to mothers from gestation week 32 to postnatal week 4 410 patients; 1º endpoint is HBsAg status of infant at 1 year of age

An Industry Perspective:Scientific Issues and Issues for Discussion Today
CONTRIBUTORS
•Achillion
Lisa Dunkle
•Bristol Myers Squibb
Deborah DeHertogh, Bruce Kreter,Michael Brady, Katherine Takaki
•Eli Lilly
James McGill, Margaret Wasilewski
•GlaxoSmithKline
Stephen Gardner, Fraser Gray, Lynn Condreay
•Idenix
Nat Brown, Maureen Myers, Dave Standring, George Chao
•Roche
Nigel Pluck, S. Chris Pappas
•Schering Plough
Janice Albrecht
•Triangle Pharmaceuticals
Franck Rousseau, Elsa Mondou
•Tulane University
Shobha Joshi

An Industry Perspective: Endpoint and Trial Design Issues Are Critical!
Rated “critically important” by ALL respondents: Histology as an efficacy endpoint
Active vs. placebo controls in future trials
Rated “critically” to “very” important for discussion today: HBV DNA suppression (alone) vs. short-term clinical endpoints
(HBeAg, histology, ALT)
Endpoints in HBeAg-negative (pre-core mutant) hepatitis B
Correlation between serologic and histologic endpoints
Criteria for non-inferiority vs. superiority in Phase III trials
How to deal with non-standardized HBV DNA assays
An Industry Perspective: Discussion Framework for the Issues
What are therapy goals in chronic hepatitis B? Therapeutic response endpoints Treatment discontinuation endpoints
Choices for 1 efficacy endpoint in: HBeAg+ patients (histology, HBeAg/Ab, ALT, HBV DNA) HBeAg- patients (histology, ALT, HBV DNA)
Active vs. placebo controls in future trials What 1 endpoint best discriminates between 2 active Rx’s?

An Industry Perspective: Important Scientific Issues
Virology knowledge gaps: cccDNA formation & persistence Antiviral targets other than polymerase?
Immunology knowledge gaps: Immune factors in HBV persistence vs clearance Viral suppression vs. immune effects for durable responses
(implications for antiviral Rx vs. antiviral + immunomodulator)
Clinical knowledge gaps: Undefined correlation between HBV DNA suppression and
clinical efficacy endpoints No established early determinants of long-term outcomes

A Personal Perspective:Facilitating Progress in HBV Therapeutics
DAVDP & Committee guidance: endpoint and design issues
Future HBV registration trials: Global (to ICH/FDA standards)
Most patients from Asia, some from N.America/EU/elsewhere
Most trials with active control designs (monoRx and comboRx)
Need 1° serologic endpoints for efficiency and precision
‘Clinical’ endpoints linked with HBV DNA suppression? Desirable for trials in patients with compensated liver disease
After assay standardization, HBV DNA as 1° endpoint in some circumstances? Conditional approvals, decomp, co-infected patients?
Goal: Optimize progress against severe morbidity/mortality

Q & A