pharmacogenetics of slco1b1: population genetics and
TRANSCRIPT

Department of Clinical PharmacologyUniversity of Helsinki
Finland
PHARMACOGENETICS OF SLCO1B1:POPULATION GENETICS AND EFFECT ON STATINS
Marja Pasanen
ACADEMIC DISSERTATION
To be presented, with the permission of the Medical Faculty of the University ofHelsinki, for public examination in Lecture hall 3 of Biomedicum Helsinki,
Haartmaninkatu 8, on December 19th, 2008, at 12 noon.
Helsinki 2008

Supervisors: Docent Mikko Niemi, MD, PhDDepartment of Clinical PharmacologyUniversity of HelsinkiHelsinki, Finland
Professor Pertti Neuvonen, MD, PhDDepartment of Clinical PharmacologyUniversity of HelsinkiHelsinki, Finland
Reviewers: Docent Reijo Laaksonen, MD, PhDScience CenterTampere University HospitalTampere, FinlandandZora Biosciences OyEspoo, Finland
Docent Miia Turpeinen, MD, PhDDepartment of Pharmacology and ToxicologyUniversity of OuluOulu, Finland
Opponent: Professor Timo Strandberg, MD, PhDDepartment of Health Sciences/GeriatricsUniversity of OuluOulu, Finland
ISBN 978-952-92-4677-9 (paperback)ISBN 978-952-10-5090-9 (PDF, http://ethesis.helsinki.fi)Helsinki 2008Yliopistopaino

”It is unthinkable that selecting drugs for individual patients remains an empirical exercise.”Giacomini et al. Nature 2007
TABLE OF CONTENTS
4
TABLE OF CONTENTS
TABLE OF CONTENTS................................................................................................................. 4
ABBREVIATIONS AND DEFINITIONS .................................................................................... 6
LIST OF ORIGINAL PUBLICATIONS ...................................................................................... 9
ABSTRACT ..................................................................................................................................... 10
INTRODUCTION........................................................................................................................... 12
REVIEW OF THE LITERATURE ............................................................................................. 141. Pharmacokinetic principles of drug action.............................................................................. 14
1.1 Principles of drug metabolism........................................................................................... 142. Membrane transporters............................................................................................................. 15
2.1 General aspects ................................................................................................................... 152.2 Role of transporters in drug disposition............................................................................ 162.3 Transporter pharmacogenetics........................................................................................... 182.4 Influx transporters and their pharmacogenetics................................................................ 192.5 Efflux transporters and their pharmacogenetics ............................................................... 212.6 Transporter-mediated drug-drug interactions ................................................................... 232.7 OATP1B1............................................................................................................................ 26
2.7.1 Structure and function................................................................................................. 262.7.2 Substrates..................................................................................................................... 272.7.3 Inhibitors...................................................................................................................... 302.7.4 SLCO1B1 pharmacogenetics ...................................................................................... 30
3. CYP enzymes and their pharmacogenetics ............................................................................. 354. Cholesterol homeostasis ........................................................................................................... 36
4.1 Cholesterol synthesis.......................................................................................................... 384.2 Cholesterol absorption........................................................................................................ 394.3 Cholesterol elimination and bile acid metabolism ........................................................... 394.4 Plasma noncholesterol sterols............................................................................................ 40
5. HMG-CoA reductase inhibitors (statins) ................................................................................ 425.1 Pharmacodynamics and clinical use.................................................................................. 425.2 Pharmacokinetic properties................................................................................................ 44
5.2.1 Fluvastatin.................................................................................................................... 445.2.2 Pravastatin.................................................................................................................... 465.2.3 Simvastatin .................................................................................................................. 465.2.4 Rosuvastatin................................................................................................................. 475.2.5 Atorvastatin ................................................................................................................. 47
5.3 Adverse effects ................................................................................................................... 495.4 Pharmacogenetics ............................................................................................................... 51
AIMS OF THE STUDY ................................................................................................................. 53

TABLE OF CONTENTS
5
MATERIALS AND METHODS .................................................................................................. 541. Population genetic studies (I, II) .............................................................................................. 54
1.1 Subjects and study design .................................................................................................. 541.2 Blood sampling and genomic DNA extraction................................................................. 541.3 Genotyping.......................................................................................................................... 541.4 Population genetics and statistical analyses...................................................................... 56
2. Pharmacokinetic and pharmacodynamic studies (III–VI)...................................................... 582.1 Subjects ............................................................................................................................... 58
2.1.1 Genotyping .................................................................................................................. 582.2 Study design........................................................................................................................ 582.3 Blood sampling................................................................................................................... 602.4 Quantification of plasma statins ........................................................................................ 602.5 Quantification of plasma sterols ........................................................................................ 612.6 Pharmacokinetic calculations ............................................................................................ 612.7 Pharmacodynamic variables .............................................................................................. 612.8 Statistical analysis .............................................................................................................. 62
3. Ethical considerations............................................................................................................... 62
RESULTS......................................................................................................................................... 631. SLCO1B1 allele frequencies .................................................................................................... 63
1.1 Finnish population (I)......................................................................................................... 631.2 Global analysis (II) ............................................................................................................. 63
2. Effect of SLCO1B1 polymorphism on statin pharmacokinetics............................................ 672.1 Fluvastatin (III) ................................................................................................................... 672.2 Pravastatin (III) ................................................................................................................... 672.3 Simvastatin (IV) ................................................................................................................. 672.4 Rosuvastatin (V) ................................................................................................................. 682.5 Atorvastatin (V).................................................................................................................. 68
3. Effect of SLCO1B1 polymorphism on statin pharmacodynamics (VI)................................. 704. Effect of SLCO1B1 polymorphism on cholesterol homeostasis (VI).................................... 70
DISCUSSION .................................................................................................................................. 711. Methodological considerations ................................................................................................ 71
1.1 Population genetic studies.................................................................................................. 711.2 Pharmacokinetic and pharmacodynamic studies.............................................................. 71
2. Population genetics of SLCO1B1 ............................................................................................ 733. Role of SLCO1B1 polymorphism in statin pharmacokinetics and pharmacodynamics....... 744. Role of SLCO1B1 polymorphism in cholesterol homeostasis ............................................... 775. Clinical implications................................................................................................................. 78
CONCLUSIONS ............................................................................................................................. 80
ACKNOWLEDGEMENTS........................................................................................................... 81
REFERENCES................................................................................................................................ 83
ORIGINAL PUBLICATIONS....................................................................................................105

ABBREVIATIONS AND DEFINITIONS
6
ABBREVIATIONS AND DEFINITIONS
3’UTR 3’-untranslated regionABC ATP-binding cassetteACAT Acyl-coenzyme A:cholesterol acyltransferaseACE Angiotensin-converting enzymeACU154 O-glucuronide of PKI116AMOVA Analysis of molecular varianceANOVA Analysis of varianceApo ApolipoproteinASBT Apical sodium dependent bile acid transporterATP Adenosine triphosphateAUC Area under the concentration-time curveAUC0-t AUC from time 0 to t hoursAUC0- AUC from time 0 to infinityBamet Bile acid-cisplatin derivativeBCRP Breast cancer resistance proteinBMI Body mass indexBQ-123 Cyclic-pentapeptideBSEP Bile salt export pumpBSP Bromosulphophtaleinc.DNA Coding deoxyribonucleic acidCA Cholic acidCDCA Chenodeoxycholic acidCEPH Fondation Jean Dausset – Centre d’Étude du Polymorphisme HumainCHD Coronary heart diseaseCHO Chinese hamster ovaryCI Confidence intervalCK Creatine kinaseCL ClearanceCLH Hepatic clearanceCLH,int Hepatic intrinsic clearanceCLH,int,all Overall hepatic intrinsic clearanceCmax Peak concentrationCNS Central nervous systemCoA Coenzyme ACOS1 A cell line used to transfect cells, name derived from the cells being CV-1
(simian) in Origin, and carrying the SV40 genetic materialCV Coefficient of variationCYP Cytochrome P450CYP7A1 Cholesterol 7 -hydroxylaseCYP8B1 Sterol 12 -hydroxylase

ABBREVIATIONS AND DEFINITIONS
7
DADLE (D-Ala2, D-Leu5)-enkephalindbSNP NCBI single nucleotide polymorphism databaseDHEAS Dehydroepiandrosterone sulphateDNA Deoxyribonucleic acidDPDPE (D-penicillamine2,5)-enkephalinEI Intestinal extraction ratioEH Hepatic extraction ratioEDTA Ethylenediaminetetraacetic acidf FemaleF Oral bioavailabilityFDA Food and Drug AdministrationFGF-19 Fibroblast growth factor-19FST Fixation indexfu Unbound fraction of drugFXR Farnesoid X receptorg.DNA Genomic deoxyribonucleic acidGLC Gas-liquid chromatographyHDL High-density lipoproteinHEK293 Human embryonic kidney cellsHeLa Human cervical carcinoma cells, name derived from Henrietta LacksHGDP Human Genome Diversity ProjectHIV Human immunodeficiency virusHMG 3-hydroxy-3-methylglutarylHMG-CoAR HMG-CoA reductaseIBABP Ileal bile acid binding proteinIDL Intermediate-density lipoproteinke Elimination rate constantKm Michaelis-Menten kinetic constantLCL Lymphoblastoid cell lineLC-MS-MS Liquid chromatography–tandem mass spectrometryLD Linkage disequilibriumLDL Low-density lipoproteinLDL-C LDL-cholesterolLST Liver-specific transporterLXR Liver X receptorm MaleMATE Multidrug and toxin extrusion transporterMCF-7 Michigan Cancer Foundation breast cancer cell lineMDCKII Madin-Darby canine kidney strain II cellsMDR1 Multidrug resistance transportermRNA Messenger ribonucleic acidMGB Minor groove binderMRP Multidrug resistance-associated protein

ABBREVIATIONS AND DEFINITIONS
8
NAN Non-AustronesianNCBI National Center for Biotechnology InformationNPC1L1 Niemann-Pick C1-like 1 proteinNTCP Sodium-dependent taurocholate co-transporting proteinOAT Organic anion transporterOATP Organic anion-transporting polypeptideOCT Organic cation transporterOCTN Organic cation/carnitine transporterOST Organic solute transporterPAH Para-aminohippuric acidPCR Polymerase chain reactionPEPT Peptide transporterPSinflux Permeability of cell membrane from outside to insidePSefflux Permeability of cell membrane from inside to outsidePRIMO Prediction du Risque Musculaire en ObservationnelPXR Pregnane X receptorSD Standard deviationSEM Standard error of the meanSHP Small heterodimer partnerSLC Solute carrierSLCO Solute carrier organic anion transporterSNP Single nucleotide polymorphismSREBP Sterol regulatory element binding proteint½ Elimination half-lifetmax Time to peak concentrationUGT Uridine diphosphate-glucuronosyltransferaseUNG Uracil-N-glycosylaseURAT Urate transporterVd Volume of distributionVLDL Very-low-density lipoproteinQH Hepatic blood flow

LIST OF ORIGINAL PUBLICATIONS
9
LIST OF ORIGINAL PUBLICATIONS
This thesis work is based on the following original publications, which are referred to in the textby the Roman numerals I–VI.
I Pasanen MK, Backman JT, Neuvonen PJ, Niemi M. Frequencies of singlenucleotide polymorphisms and haplotypes of organic anion transportingpolypeptide 1B1 SLCO1B1 gene in a Finnish population. Eur J Clin Pharmacol2006; 62:409-15.
II Pasanen MK, Neuvonen PJ, Niemi M. Global analysis of genetic variation inSLCO1B1. Pharmacogenomics 2008; 9:19-33.
III Niemi M, Pasanen MK, Neuvonen PJ. SLCO1B1 polymorphism and sex affect thepharmacokinetics of pravastatin but not fluvastatin. Clin Pharmacol Ther 2006;80:356-66.
IV Pasanen MK, Neuvonen M, Neuvonen PJ, Niemi M. SLCO1B1 polymorphismmarkedly affects the pharmacokinetics of simvastatin acid. PharmacogenetGenomics 2006; 16:873-9.
V Pasanen MK, Fredrikson H, Neuvonen PJ, Niemi M. Different effects ofSLCO1B1 polymorphism on the pharmacokinetics of atorvastatin and rosuvastatin.Clin Pharmacol Ther 2007; 82:726-33.
VI Pasanen MK, Miettinen TA, Gylling H, Neuvonen PJ, Niemi M. Polymorphism ofthe hepatic influx transporter OATP1B1 is associated with increased cholesterolsynthesis rate. Pharmacogenet Genomics 2008; 18:921-6.
These original publications are reproduced with the permission of their copyright holders. Inaddition, some unpublished material has been presented.

ABSTRACT
10
ABSTRACT
Wide interindividual and interethnic variability exists in the plasma concentrations of thecholesterol-lowering drugs HMG-CoA reductase inhibitors (statins) in their efficacy and risk ofadverse effects. The risk of muscle toxicity as an adverse effect of statin therapy is known toincrease along with elevated plasma statin concentrations.
Organic anion-transporting polypeptide 1B1 (OATP1B1) is an uptake transporter located on thebasolateral (sinusoidal) membrane of human hepatocytes, encoded by the gene SLCO1B1.OATP1B1 facilitates the hepatic uptake of many endogenous and foreign compounds, such asoestrogen conjugates, bile acids and statins. Taking into consideration the known interindividualand interethnic differences in the disposition of many OATP1B1 substrates, particularly statins,and its functional role in the pharmacokinetics of many drugs, it is important to characterize thediversity of the SLCO1B1 gene in various ethnic groups and to investigate the effects ofSLCO1B1 polymorphism on statin disposition and response.
The frequencies of SLCO1B1 sequence variations were studied in a population of 468 healthyFinnish volunteers and globally in various ethnic populations. DNA samples from theparticipants were genotyped for the presence of single nucleotide polymorphisms (SNPs) inSLCO1B1 and the results were analysed using population genetic methods. Secondly, the effectsof SLCO1B1 genotypes on the pharmacokinetics and pharmacodynamics of fluvastatin,pravastatin, simvastatin, rosuvastatin and atorvastatin, and on cholesterol homeostasis, werestudied in a prospective genotype panel study with 32 healthy volunteers. The subjects ingesteda single dose of each investigated statin in five different phases. Blood samples were collectedbefore statin administration and up to 48 hours thereafter to determine the concentrations ofplasma statins, statin metabolites, cholesterol and noncholesterol sterols.
Functionally significant variants in the SLCO1B1 gene were detected at varying frequencies indifferent populations. Genetic variation in SLCO1B1 was generally similar to that observed forother autosomal markers, although selective pressure may have acted on SLCO1B1, favouringlow-activity variants in the north. The frequency of the low-activity c.521T>C variant allele was24% (95% CI, 18–32%) in Native American populations, 20% (95% CI, 15–25%) in the MiddleEast, 18% (95% CI, 14–23%) in Europe, 12% (95% CI, 9.5–15%) in East Asia, 9.4% (95% CI,6.9–13%) in Central/South Asia and 1.9% (95% CI, 0.7–4.8%) in Sub-Saharan Africa. Nocarriers of the c.521T>C SNP were found in Oceania. The frequency of the homozygous variantc.521CC genotype was around 2% in Caucasians and around 4% in the Finnish population. Thegreatest genetic diversity was seen in African populations and SLCO1B1 diversity was generallyfar greater within than between populations.
The SLCO1B1 genotype significantly affected the pharmacokinetics of most of the statinsinvestigated. The mean area under the plasma concentration-time curve (AUC) of simvastatinacid, atorvastatin, pravastatin and rosuvastatin was 3.2-, 2.4-, 1.9- and 1.7-fold, respectively, insubjects with the SLCO1B1 c.521CC variant genotype compared with subjects with the c.521TT

ABSTRACT
11
control genotype (P < 0.05). The SLCO1B1 genotype had no significant effect on the plasmaconcentrations of fluvastatin. Despite the considerable effect on the pharmacokinetics of statins,the response to a single dose of any of the statins studied was not affected by the SLCO1B1genotype. Interestingly, the SLCO1B1 variant genotype was associated with an increasedbaseline cholesterol synthesis rate, as indicated by a 40% higher desmosterol to cholesterol ratioin subjects with the c.521CC genotype than in those with the c.521TT genotype (P = 0.043). Inagreement, there was a tendency toward higher plasma concentrations of absolute desmosteroland lathosterol, as well as lathosterol to cholesterol ratios, and lower plasma concentrations ofcholesterol absorption markers in subjects with the variant genotype.
In conclusion, the low-activity SLCO1B1 c.521T>C variant occurs at varying frequencies indifferent ethnic groups and is relatively common in non-African populations. Geneticallyimpaired activity of the hepatic influx transporter OATP1B1, due to the presence of thec.521T>C SNP, leads to elevated plasma concentrations of many but not all statins, thusincreasing the risk for muscle toxicity. The SLCO1B1 genotype may partially explain whyindividual patients respond differently to various statins and may help to identify subjects whoare at higher risk of developing statin-induced myopathy.

INTRODUCTION
12
INTRODUCTION
Several studies in different populations indicate a continuous positive relationship betweenblood cholesterol concentrations and coronary heart disease (CHD) risk (Rose and Shipley1986, Stamler et al. 1993), with no threshold below which a lower cholesterol concentration isnot associated with lower risk (Chen et al. 1991). The 3-hydroxy-3-methyl-glutaryl coenzyme A(HMG-CoA) reductase inhibitors (statins) are essential drugs in the treatment ofhypercholesterolaemia (LaRosa et al. 1999). They effectively lower cholesterol levels andconsistently and significantly reduce mortality and morbidity in patients with and without ahistory of coronary artery disease (Scandinavian Simvastatin Survival Study Group 1994,Shepherd et al. 1995, Sacks et al. 1996, Baigent et al. 2005). Statins are among the mostprescribed drugs worldwide and the number is increasing, as the need for lipid-lowering therapygrows together with increase in cardiovascular morbidity, metabolic syndrome and obesity.Careful assessment of cost-effectiveness, safety and tolerability is essential. The treatment ofhypercholesterolaemia is usually lifelong and patients often have other concomitant diseases andmedications, all of which together with the genetic background increase the risk for adverseeffects. Although statins are fairly well-tolerated, especially in monotherapy, they can causemyopathy and even rhabdomyolysis as a rare adverse effect (Thompson et al. 2003). The muscletoxicity of statins is a dose- and concentration-dependent phenomenon (Bradford et al. 1991,Dujovne et al. 1991), and the risk of toxity increases when the plasma concentrations of statinsare increased, often due to drug interactions or inherited defects in proteins affecting statindisposition (Staffa et al. 2002, Thompson et al. 2003, Neuvonen et al. 2006). Furthermore,considerable interindividual variability is evident in the response to statin therapy (Pazzucconi etal. 1995).
Plasma membrane transporters have been implicated as important determinants of intestinalabsorption and hepatobiliary clearance, especially of hydrophilic statins. Multiple organic anion-transporting polypeptide (OATP) family members are capable of statin transport, and some ofthem are abundant in the liver, where they may be involved in the hepatic uptake of statins fromthe sinusoidal blood (Abe et al. 1999, Niemi 2007). OATP1B1 is an uptake transporter locatedin the basolateral (sinusoidal) membrane of human hepatocytes and involved in the hepaticuptake of a broad array of endogenous and foreign compounds, such as oestrogen conjugates,bile acids and statins (Hsiang et al. 1999, König et al. 2000). Several single nucleotidepolymorphisms (SNPs) in the gene encoding OATP1B1, solute carrier organic anion transporter(SLCO1B1), have been discovered (Tirona et al. 2001, König et al. 2006). Some of them, inparticular the nonsynonymous sequence variation c.521T>C (Val174Ala), have been associatedwith reduced activity of OATP1B1 in vitro (Tirona et al. 2001, Iwai et al. 2004, Kameyama etal. 2005, Nozawa et al. 2005), and increased plasma concentrations of pravastatin, rosuvastatin,pitavastatin, repaglinide and fexofenadine in vivo in humans (Nishizato et al. 2003, Mwinyi etal. 2004, Niemi et al. 2004, 2005a,b, Chung et al. 2005, Lee et al. 2005a). The frequency of thepolymorphisms in SLCO1B1 appears to be heavily dependent on ethnic background (Tirona etal. 2001, Lee et al. 2005a).

INTRODUCTION
13
Access into the liver is an important step in the elimination of many endogenous compoundsand xenobiotics, including most drugs. Since statins exert their cholesterol-lowering effects byinhibiting the HMG-CoA reductase in the hepatocytes, reduced OATP1B1-mediated uptake intothe liver due to genetic polymorphism in the encoding SLCO1B1 gene may both reduce theirefficacy and increase their peripheral plasma concentrations, thus enhancing the risk of systemicadverse effects, such as myopathy (Niemi et al. 2004).
Characterization of genetic variation in transporter genes is an important step towardsunderstanding individual variation in drug response and developing personalized and safer drugtherapy. Given the known interindividual and interethnic differences in drug dispositioninvolving the OATP1B1 transporter, especially in statin therapy, and the functional role ofOATP1B1 in the pharmacokinetics of many clinically important drugs, we investigatedSLCO1B1 polymorphism in several populations and its role in statin pharmacokinetics, statinpharmacodynamics and cholesterol synthesis.
REVIEW OF THE LITERATURE
14
REVIEW OF THE LITERATURE
1. Pharmacokinetic principles of drug action
After oral administration, drugs pass through the intestinal wall and enter the portal bloodcirculation. The portal blood takes the drugs into the liver, after which they reach the systemiccirculation and are distributed to the target sites. Drugs are eliminated from the body bymetabolism and excretion, usually via the liver into the bile or via the kidneys into the urine.Drug pharmacokinetics is concerned with the stages of a drug in the body, i.e. absorption,distribution, metabolism and excretion, while pharmacodynamics refers to the biological effectsof a drug on the body. Drug efficacy and response are determined by a complex interplay ofmultiple processes regulating drug pharmacokinetics and pharmacodynamics (Rowland andTozer 1995).
The rate and extent of intestinal absorption of a drug are dependent on its physicochemicalproperties and on active transport processes. The distribution occurs initially into highlyperfused tissues and is dependent on the ability of the drug to penetrate biological membranes,either by filtration, passive or facilitated diffusion, or active transport. Most drugs are lipophiliccompounds and must be biotransformed into more hydrophilic forms to be excreted from thebody (Meyer 1996). The extent of renal and hepatobiliary excretion is partly determined by theexpression of uptake and efflux transporters in the clearance organs (Shitara et al. 2006).
1.1 Principles of drug metabolism
The liver is the major organ of drug metabolism, in which enzymes located in the endoplasmicreticulum and cytoplasm of hepatocytes catalyse drug biotransformation. Other organs, e.g. thegut, kidneys, lung and skin, can also contribute to drug metabolism (Krishna and Klotz 1994).An orally administered drug can begin to be biotransformed in the gastrointestinal tract byenterocytes and in the liver after passing through the portal circulation (first-pass metabolism),which can considerably decrease the oral bioavailability of many drugs (Shen et al. 1997). Drugbiotransformation is often divided into two phases, including phase I functionalization andphase II conjugation reactions. Phase I enzymes insert a functional group in their substrate,usually by oxidation, reduction and hydrolysis reactions, leading generally to metabolites lessactive than the parent drug (Josephy et al. 2005). These reactions are mainly catalysed bycytochrome P450 (CYP) enzymes. Phase II reactions are usually conjugation reactions, in whichdrugs or their metabolites are conjugated with endogenous molecules to produce more water-soluble compounds in order to facilitate their excretion (Josephy et al. 2005). Phase II enzymesinclude uridine diphosphate-glucuronosyltransferases (UGTs), sulphotransferases andglutathione transferases (Cribb et al. 2005). Some drugs can also be directly excreted after eitherphase I or phase II reactions, or even nonmetabolized (Krishna and Klotz 1994). Transportersexpressed in plasma membranes facilitate the import of drugs into metabolizing cells and exportof the drug metabolites produced (Shitara et al. 2006).

REVIEW OF THE LITERATURE
15
2. Membrane transporters
2.1 General aspects
In addition to the physicochemical properties of a compound such as charge, molecular size,lipophilicity and solubility, carrier-mediated processes or transporters also affect thetransmembrane passage of substrates. Transporters are usually separated into two major classes- uptake and efflux transporters (Table 1, Figure 1); it has been estimated that approximately2000 genes encode transport proteins in humans (Giacomini and Sugiyama 2006). The polarizedexpression of transporters in targeted organs such as the intestine, kidney and liver and thedynamic interplay between uptake and efflux transporters, often with overlapping substratecapabilities, in the cell membrane of epithelial cells, together determine the direction and extentof flow of a number of xenobiotic and endobiotic substances (Kerb 2006). Moreover, theirexpression on the interfaces of different parts of the body contributes to the maintenance ofseveral important structural barriers, e.g. the blood-brain barrier and the blood-placental barrier(Graff and Pollack 2004, Syme et al. 2004, Mölsä et al. 2005). Transporters mediate importantphysiologic functions via influx and efflux of endogenous substrates such as amino acids, bileacids, steroids, sugars, lipids and hormones that are critical for normal homeostasis. They alsoplay a significant role in mediating the absorption, tissue distribution and elimination of manyenvironmental toxins and drugs (Ho and Kim 2005, Shitara et al. 2006).
Figure 1. Classification of the solute carriers (SLCs), ATP-binding cassette (ABC) transportersand channels in the plasma membrane. Adapted and modified from Petzinger and Geyer(2006).

REVIEW OF THE LITERATURE
16
2.2 Role of transporters in drug disposition
In the gut, drug absorption from the intestinal lumen is facilitated by uptake transporters andlimited by efflux transporters, both expressed in the brush-border membrane of enterocytes(Figure 2). Following uptake, drugs are translocated via the basolateral membrane into the portalblood circulation by efflux transporters such as the multidrug resistance-associated proteins(MRPs). Many drugs also pass through the enterocytes by passive diffusion and some drugsalready undergo extensive metabolism in the enterocytes (Kullak-Ublick et al. 2004, Glaeser etal. 2007, Meier et al. 2007).
Figure 2. Drugs pass through the intestinal wall to portal blood via transcellular andparacellular diffusion, and via uptake and efflux transporters located in the luminal brush-border membrane and basolateral membrane, respectively. Some drugs undergo metabolism,mainly by CYP3A4, in the enterocytes.
Uptake transporters expressed on the basolateral (sinusoidal) membrane of hepatocytes facilitatethe influx of compounds into the liver (Figure 3). Drugs taken into the hepatocytes oftenundergo metabolic transformation and/or conjugation, or they may be excreted unchanged (Pangand Rowland 1977). Transport of the drugs and their metabolites out of the hepatocyte via thecanalicular membrane into the bile or via the basolateral membrane back into the portal bloodmay be mediated by efflux transporters (Shitara et al. 2006). Hepatic clearance can be describedby the following equation (Pang and Rowland 1977, Yamazaki et al. 1996):
allint,,HuH
allint,,HuHH CLfQ
CLfQCL
where CLH, QH, fu and CLH,int,all represent the hepatic clearance, hepatic blood flow, the unboundfraction of drug in blood and overall hepatic intrinsic clearance, including uptake, metabolismand biliary excretion, respectively.

REVIEW OF THE LITERATURE
17
CLH,int,all can be described by the following equation:
int,Hefflux
int,Hinfluxallint,,H CLPS
CLPSCL
where PSinflux and PSefflux are the membrane permeabilities across the sinusoidal membrane fromthe outside to the inside and from the inside to the outside of cells, respectively, and CLH,int
represents the intrinsic clearance for the metabolism and biliary excretion of the unbound drugs.The uptake of drugs via the sinusoidal membrane (PSinflux), which is partly mediated bytransporters, is a determinant of the net hepatic clearance (CLH,int,all) regardless of the otherprocesses (CLH,int and PSefflux). Therefore, hepatic clearance (CLH) may be affected when theuptake clearance of drugs is altered, even if the drug finally undergoes metabolism. On the otherhand, the excretion of drugs via the bile canalicular membrane, which is also partly mediated bytransporters, is a determinant of the net hepatic clearance (CLH,int,all), unless PSefflux is negligiblylow compared with CLH,int. When PSefflux << CLH,int, hepatic uptake predominantly determinesoverall hepatic clearance (CLH,int,all = PSinflux) and the hepatic clearance is uptake-limited. Onthe other hand, when PSefflux >> CLH,int, all processes affect the overall hepatic clearance. Whena drug is lipophilic with rapid membrane permeability, transport from the outside of the cells tothe inside and in the opposite direction, is symmetric (PSinflux = PSefflux). In this case, the overallintrinsic clearance equals the exact intrinsic clearance (CLH,int,all = CLH,int) (Shitara et al. 2005,2006).
Figure 3. Drug elimination in the liver involves uptake into hepatocytes via transporters and/orpassive diffusion, followed by metabolism and efflux to the bile or blood.

REVIEW OF THE LITERATURE
18
In the kidney, drugs are excreted in the urine as a net result of glomerular filtration, tubularsecretion and reabsorption (Inui et al. 2000, Dresser et al. 2001). Glomerular filtration is simplyultrafiltration of drugs and xenobiotics not bound to macromolecules (plasma proteins). Severalactive mechanisms, including transporters, are involved in the tubular secretion of compoundsinto the urine (Figure 4). Some drugs are returned to the systemic circulation via drugreabsorption, which is also mainly mediated by transporters. Tubular secretion and drugreabsorption can be inhibited by coadministered drugs (Koepsell and Endou 2004).
Figure 4. Drug elimination in the kidney occurs by glomerular filtration and secretion at theproximal tubules. Some drugs may return to the systemic circulation via drug reabsorption.Transporters are involved in tubular secretion and reabsorption.
2.3 Transporter pharmacogenetics
Recent studies have shown increasing evidence that nucleotide sequence variation(polymorphism) in drug transporters plays a major role in interindividual differences in drugdisposition. Polymorphism leading to functional changes in drug transporters can affect thepharmacokinetics and subsequent pharmacodynamics and toxicological effects of drugs. It canalso affect susceptibility to certain diseases (Ho and Kim 2005). Although detailed informationon genetic variability in drug transporter genes is available, our knowledge on identifying thosegenetic variants that have functional significance and how they contribute to interindividualvariability in drug response is still limited (Kerb 2006).

REVIEW OF THE LITERATURE
19
There are many mechanisms by which polymorphism can affect transporter phenotype.Common polymorphisms include tandem repeated segments, large (copy number variants) andsmall segmental deletions/insertions/duplications and substitutions (SNPs). SNPs are anexceedingly common form of polymorphism that may account for approximately 90% of allknown sequence variation (Collins et al. 1998). Functional SNPs that lead to changes in geneexpression occur in all regions of the genome. SNPs in the coding (exonic) regions oftransporter genes can be nonsynonymous, meaning that they lead to a change in encoded aminoacids, or synonymous (no amino acid change). Although both kinds of SNPs can have an impacton transporter activity, it is widely accepted that nonsynonymous SNPs are more likely to havefunctional consequences. Nonsynonymous SNPs can lead to protein misfolding, polarity shift orimproper phosphorylation. SNPs in the noncoding regions of transporter genes are lesspredictable and include variants in the intronic, promoter and 3’-untranslated region (3’UTR).These variants can affect the splicing or regulation of transporter genes. SNPs in the promoterregion may modify transporter expression by altering the binding sites for transcription factors(Chorley et al. 2008, Gradhand and Kim 2008).
2.4 Influx transporters and their pharmacogenetics
Influx (uptake) transporters facilitate the entry of drugs into cells. Uptake transporters includethe organic anion-transporting polypeptides (OATPs, SLCO), organic anion transporters (OATs,SLC22A), organic cation transporters (OCTs, SLC22A), organic cation/carnitine transporters(OCTNs, SLC22A), peptide transporters (PEPTs, SLC15A) and sodium-dependent taurocholatecotransporting protein (NTCP, SLC10A1) (Ho and Kim 2005, Zair et al. 2008). Multidrug andtoxin extrusion transporter 1 (MATE1, SLC47A1) and multidrug and toxin extrusion transporter2-K (MATE2-K, SLC47A2) also participate into the uptake of compounds into the cell(Tanihara et al. 2007). All of these transporters belong to the superfamily of solute carriers(SLCs) (Hagenbuch and Meier 2004, Hediger et al. 2004, Seithel et al. 2008a).
OATPs (rodents: Oatps; human: OATPs) are sodium-independent uptake transporters thatmediate the influx of a variety of amphipathic compounds. Their transport mechanism iselectroneutral exchange, coupling the cellular uptake of organic compounds with the efflux ofneutralizing anions such as bicarbonate, glutathione or glutathione-S-conjugates (Satlin et al.1997, Li et al. 1998, 2000). OATPs have been identified at least in the intestine, liver, kidney,lung, testis, placenta and blood-brain barrier, and their substrates include endogenous substancessuch as bile salts, steroid conjugates and thyroid hormones, as well as several xenobiotics suchas statins (Seithel et al. 2008a). OATP1B1 (previously known as OATP-C, OATP2, liver-specific transporter 1; LST-1), OATP1B3 (previously known as OATP8 and LST-2) andOATP2B1 (previously known as OATP-B) are expressed in the sinusoidal membrane ofhepatocytes and participate in the active uptake of compounds from the portal blood into theliver. These three transporters have overlapping substrate selectivity, including endogenouscompounds and several therapeutic drugs (Hagenbuch and Meier 2004, Niemi 2007). OATP2B1and OATP1A2 are also expressed in the brush-border membrane of enterocytes, indicating apossible role in the active absorption of drugs from the intestine (Meier et al. 2007). OATP4C1

REVIEW OF THE LITERATURE
20
is localized in the basolateral membrane of proximal tubule cells and may thus mediate theuptake of substrates from blood into the kidney (Niemi 2007). Information on the othermembers of the OATP family is limited. Numerous genetic polymorphisms in at least theOATP1B1- and OATP1B3-encoding genes SLCO1B1 and SLCO1B3 have been identified, someassociated with altered transport function. OATPs can be inhibited by cyclosporine, rifampicin,gemfibrozil and macrolides (Niemi 2007).
OATs are multispecific anion-exchange transporters expressed in a variety of tissues, at least inthe kidney, liver, brain and placenta (Koepsell and Endou 2004). Seven members of thistransporter family have been identified (OAT1–6 and URAT1), and they mediate mostly theuptake of organic anions of relatively small molecular weight. OATs are mainly important renaluptake transporters, although OAT2 and OAT5 are localized in the liver, and OAT4 is expressedin the brush-border membrane of the kidney (involved in the efflux from renal tubules into theurine). OAT4 is also expressed on the fetal-facing surface of the placenta and is thought to playa role in the placental uptake of fetal-derived compounds (Rizwan and Burckhardt 2007, Zhouand You 2007). URAT1 (urate transporter 1) mediates the uptake of urate in the proximal tubulecells in the kidneys. OATs can be inhibited by certain cephalosporin antibiotics and probenecid(Dresser et al. 2001, Shitara et al. 2005). Several SNPs specific for certain ethnic groups havebeen reported in the OATs, especially in OAT2. However, no certain effect of these SNPs ontransport function, substrate specificity or expression has been found (Zair et al. 2008).
OCTs and OCTNs transport organic cations such as endogenous amines and several drugs.OCTs act as electrogenic uniporters that mediate facilitated diffusion in either direction. OCT1is primarily expressed in the sinusoidal membranes of hepatocytes and, to a lesser extent, inintestinal cells. OCT2 is highly expressed in the kidney and is important for the renal tubularexcretion of many drugs (Inui et al. 2000, Dresser et al. 2001, Koepsell and Endou 2004). Over200 SNPs have been identified in the SLC22A1 gene encoding OCT1. Some of these have beenassociated with altered transport function, e.g. reduced uptake of the OCT1 substrate metformin(Shu et al. 2008, Zair et al. 2008). A number of genetic variants have been also identified in theSLC22A2 gene encoding OCT2, some associated with altered uptake of substrate drugs(Leabman et al. 2002, Zair et al. 2008).
OCTN1 is a pH-dependent cation transporter, while OCTN2 transports carnitine in addition tocations (Yabuuchi et al. 1999, Koepsell and Endou 2004). OCTNs have been found in thekidney, liver, intestine, brain, heart, skeletal muscle and placenta (Koepsell et al. 2007). Geneticvariants of the OCTN1 and OCTN2 genes have been associated with inflammatory boweldisease (Cucchiara et al. 2007). Furthermore, the c.150C>T SNP in the OCTN1 has been shownto alter the renal transport of the antiepileptic drug gabapentin (Urban et al. 2008).
PEPTs are proton-coupled peptide transporters, located in the intestinal and renal cellmembranes. PEPT1 is mainly expressed in the apical membrane of enterocytes in theduodenum, jejunum and ileum (Meier et al. 2007), and PEPT1 and PEPT2 are both expressed inrenal epithelial cells (Brandsch et al. 2008). They mediate the uptake of peptides produced byprotein digestion (di- and tripeptides), as well as structurally related compounds such as ß-

REVIEW OF THE LITERATURE
21
lactam antibiotics and angiotensin-converting enzyme (ACE) inhibitors (Terada and Inui 2004,Shitara et al. 2006). Over 40 polymorphisms have been identified in the SLC15A1 geneencoding PEPT1 (Anderle et al. 2006). These SNPs do not significantly affect the transporterfunction of PEPT1.
NTCP is primarily a bile salt and bile salt derivative transporter exclusively expressed in theliver (Hagenbuch and Meier 1994). It also appears to transport certain drugs, such asrosuvastatin (Ho et al. 2006). NTCP transport is dependent on the sodium gradient. Bile salttransporters, such as NTCP, can be used for the targeting of chemotherapeutic agents tohepatocellular carcinomas by using bile salt derivatives coupled with cytostatic agents (Briz etal. 2002).
MATEs are kidney-specific antiporters localized in the brush-border membrane of renal cells.They form the human orthologue of the bacterial multidrug and toxin extrusion family and act totransport drugs and other xenobiotics across the tubular cells, both anions and cations, to excretethem out of the body (Tanihara et al. 2007). No published data on MATE1 or MATE-Kpolymorphisms are currently available (Zair et al. 2008).
2.5 Efflux transporters and their pharmacogenetics
Efflux transporters limit the entry of drugs or enhance their removal from the cell in varioustissues. They often work against high concentration gradients. The main efflux transporterscurrently identified are multidrug resistance transporter 1 (MDR1), the canalicular bile saltexport pump (BSEP), the MRP family and breast cancer resistance protein (BCRP). These areall members of the adenosine triphosphate (ATP)-binding cassette (ABC) superfamily, whichuses energy from ATP hydrolysis to mediate substrate translocation across biologic membranes(Ho and Kim 2005, Gradhand and Kim 2008). In humans, at least 49 members of thistransporter superfamily have been identified and subdivided into seven subfamilies(http://nutrigene.4t.com/humanabc.htm).
MDR1 (also known as P-glycoprotein) is encoded by the ABCB1 gene. The clinical importanceof MDR1 was first recognized in cancer chemotherapy, where high levels of expression andactivity of MDR1 caused pleiotropic resistance of cancer cells to chemotherapeutic agents(Gottesman et al. 1996). MDR1 is also expressed in the epithelial cells of various organs with anexcretory or barrier function: the liver, kidneys and small intestine, and the endothelial cells ofthe blood-brain, blood-testes and blood-placental barriers. It can thus inhibit drug absorptionfrom the gastrointestinal tract and enhance drug excretion into the bile and urine, as well asprotect the brain, testis and placenta by limiting their exposure to drugs (Fromm 2004, Mölsä etal. 2005). The known drug substrates, inhibitors and inducers of MDR1 are structurally diverse,and its substrate specificity overlaps with that of CYP3A4 (Kim et al. 1999). Both CYP3A4 andMDR1 are coexpressed in tissues such as intestinal enterocytes and hepatocytes, and it has beensuggested that MDR1 and CYP3A4 function together to limit oral drug bioavailability (Kim etal. 1999, Kivistö et al. 2004a). The wide variety of MDR1 substrates includes cytotoxic agents,
REVIEW OF THE LITERATURE
22
protease inhibitors, immunosuppressants, steroids, statins, calcium channel blockers, beta-blockers, antihistamines, anticonvulsants and antidepressants (Leschziner et al. 2007). Inaddition, MDR1 has been implicated in the regulation of entry of enveloped viruses (e.g. humanimmunodeficiency virus (HIV)-1 and influenza virus) into cells (Raviv et al. 2000).
Various polymorphisms have been identified in the MDR1 gene, some associated withdifferences in MDR1 expression and function (Kroetz et al. 2003, Leschziner et al. 2007). Oneof the most characterized sequence variations in MDR1 is the synonymous c.3435C>T SNP,which is relatively common in Caucasians (40–50%) and affects protein expression level andefflux activity (Maeda and Sugiyama 2008). MDR1 polymorphism has been also associatedwith susceptibility to renal cell carcinoma, Parkinson’s disease, inflammatory bowel disease andrefractory epilepsy (Bohan and Boyer 2002, Lockhart et al. 2003, Sakaeda et al. 2004).
BSEP, encoded by the gene ABCB11, mediates the canalicular secretion of bile salts inhepatocytes. It is also expressed in the human testis and several other tissues to a smaller extent(Noe et al. 2002, Stieger et al. 2007). Polymorphism in the ABCB11 gene encoding BSEP hasbeen associated with functional defects of BSEP-mediated canalicular bile salt secretion andcholestasis (Stieger et al. 2007).
MRPs, encoded by the ABCC gene family, are organic anion efflux pumps located in varioustissues, e.g. liver, intestine, kidney, brain and placenta. At least nine members in the MRPfamily have been identified but the tissue distribution and function of most of the MRPs remainto be established (Borst et al. 2007). MRP1 and MRP3 are typically localized in the basolateralmembrane of polarized human cells, whereas MRP2 is largely found in the apical domain. Theexpression of MRP2 in hepatocytes plays an important role in the biliary excretion ofendogenous and exogenous compounds (Keppler et al. 1997, Nies and Keppler 2007). MRP4and MRP5 are ubiquitous transporter proteins; MRP4 is localized both in the basolateral andapical domains and MRP5 mainly in the basolateral domain of polarized cells (Borst et al.2007). MRPs have overlapping, but not identical, substrate specificities and are involved in atleast the transport of bile salts, bilirubin glucuronides, steroid hormones, and both unconjugatedand conjugated drugs. MRP4 and MRP5 are also capable of transporting nucleoside andnucleotide analogues used in antiviral therapies and chemotherapy (Borst et al. 2007). For someMRPs, transport appears to be dependent on reduced glutathione (Faber et al. 2003, Haimeur etal. 2004, Gradhand and Kim 2008).
At least 16 nonsynonymous SNPs have been found in the ABCC1 gene encoding MRP1, someassociated with altered membrane expression or function. Genetic deficiency of MRP2 (ABCC2)is associated with Dubin-Johnson syndrome, and certain ABCC2 SNPs apparently affectsubstrate pharmacokinetics. Considerably less information is available on genetic variation inthe MRP3-encoding gene ABCC3, and the few nonsynonymous and synonymous SNPs foundhave not been associated with changes in transporter expression, localization or function(Gradhand and Kim 2008). The available information on genetic variability in MRP4 and MRP5is still very limited (Gradhand and Kim 2008).

REVIEW OF THE LITERATURE
23
BCRP is an efflux transporter expressed in the intestine, liver, placenta and blood-brain barrier(Allen and Schinkel 2002). Structurally, it is a half-transporter that needs to form homodimers tobe functional (Henriksen et al. 2005). BCRP facilitates e.g. the removal of drugs from the liverand limits drug entry into the central nervous system (CNS). Initially, it was cloned from humanMCF-7 (Michigan Cancer Foundation) breast cancer cells as a multidrug resistance transporter(Doyle et al. 1998). Many chemotherapeutic agents are BCRP substrates, as are manyantibiotics, antivirals and other therapeutic drugs. The endogenous substrates of BCRP includesulphated conjugates, such as oestrone-3-sulphate (Suzuki et al. 2003, Gradhand and Kim 2008).Interestingly, BCRP expression in the liver appears to be higher in men than in women (Merinoet al. 2005). The clinical importance of the nonsynonymous SNPs identified in the ABCG2 geneencoding BCRP is uncertain (Gradhand and Kim 2008).
2.6 Transporter-mediated drug-drug interactions
Most transporters accept multiple drugs as their substrates and clinically relevant drug-druginteractions may occur through inhibition or induction of transporter-mediated influx or efflux(Meier et al. 1997, Kerb 2006). This can affect the tissue distribution of transporter substratedrugs and lead to altered plasma concentrations and pharmacological activity (Ho and Kim2005, Kitamura et al. 2008a). The total effect is dependent on the type and localization of thetransporter inhibited or induced (Handschin and Meyer 2003).
The inhibition of transporters is a complex process and can involve multiple mechanisms. Forexample, different drugs can inhibit MDR1 by competing for the drug-binding sites of thetransporter, by blocking the ATP hydrolysis process or by both of these mechanisms (Lin andYamazaki 2003). Furthermore, many transporters and CYP enzymes share overlapping tissueexpression and substrate capacities, which can also lead to drug-drug interactions. Induction ofseveral drug transporters is mediated by the same nuclear receptors that regulate CYP geneexpression. The expression of drug disposition genes is under the transcriptional control ofmembers of the nuclear receptor 1 family of transcription factors, including the constitutiveandrostane receptor, pregnane X receptor (PXR) and farnesoid X receptor (FXR) (Handschinand Meyer 2003, Tirona and Kim 2005).
Known examples of interactions involving drug transporters include elevated plasmaconcentrations of digoxin and the central opioid effects of loperamide when used concomitantlywith MDR1 inhibitors (quinidine, verapamil, cyclosporine, clarithromycin, talinolol,atorvastatin) (Kim et al. 1999), and elevated serum levels of penicillin, ACE inhibitors andantiviral drugs when co-administered with probenecid, inhibiting OAT-mediated secretion in thetubular kidney cells (Ho and Kim 2005).

REVIEW OF THE LITERATURE
24
Table 1. Drug transporters belonging to the SLC and ABC transporter families, their tissue distributionand selected substrates.Family Member Tissue distribution Cellular
localizationExamples of substrates Important roles
SLCO OATP1A2 Brain, kidney,liver, intestine
Basolateral Fexofenadine, indomethacin,hormone conjugates,eicosanoids, rosuvastatin, bilesalts
CNS distribution,intestinalabsorption
OATP1B1 Liver Basolateral Statins, benzylpenicillin,rifampicin, irinotecan (SN-38),methotrexate, bilirubin, bilesalts, eicosanoids, hormoneconjugates, fexofenadine,troglitazone
Hepatic uptake
OATP1B3 Liver Basolateral Digoxin, methotrexate,rifampicin, bile salts,eicosanoids, hormone conjugates
Hepatic uptake
OATP2B1 Liver, intestine,placenta, kidney,skin, heart
Basolateral Digoxin, benzylpenicillin,hormone conjugates,rosuvastatin
Hepatic uptake,intestinalabsorption
OATP4C1 Kidney Basolateral Digoxin, methotrexate,sitagliptin, thyroid hormones
Renal uptakefrom blood
SLC22 OAT1 Kidney, brain,placenta
Basolateral Cidofovir, PAH, acyclovir,tetracycline, methotrexate,salicylate
Renal uptakefrom blood
OAT2 Kidney, liver Basolateral Salicylate, tetracyclins,zidovudine, methotrexate
Renal uptakefrom blood,hepatic uptake
OAT3 Kidney, brain,skeletal muscle
Basolateral Cimetidine, PAH, methotrexate,salicylate, valacyclovir,tetracycline, oestrone sulphate
Renal uptakefrom blood
OAT4 Kidney, placenta ApicalBasolateral
Salicylate, PAH, tetracycline Renal uptakefrom blood, renalsecretion intourine
OCT1 Liver, brain, smallintestine
Basolateral Cimetidine, corticosteroids,quinidine, quinine, midazolam,verapamil, clonidine, prazosin,procainamide, acyclovir
Hepatic uptake
OCT2 Kidney, brain,small intestine
Basolateral Amantadine, choline, dopamine,histamine, norepinephrine,serotonin, metformin, quinidine
Renal uptakefrom blood
OCT3 Placenta, liver,adrenal, heart,brain, skeletalmuscle, intestine
Unknown Cimetidine, epinephrine,histamine, norepinephrine,
Hepatic uptake

REVIEW OF THE LITERATURE
25
Table 1. (continued)Family Member Tissue distribution Cellular
localizationExamples of substrates Important roles
SLC15 PEPT1 Small intestine,kidney, liver
Apical Dipeptides, tripeptides, ß-lactamantibiotics, ACE inhibitors
Intestinalabsorption, renaluptake from urine
PEPT2 Kidney, brain, lung,mammary gland
Apical Renal uptake fromurine
ABCB MDR1 Kidney, liver, brain,small intestine,placenta
Apical Digoxin, cyclosporine,paclitaxel, vinca alkaloids,doxorubicin, HIV-1 proteaseinhibitors, statins, loperamide,erythromycin, fexofenadine
Limiting oralabsorption, limitingCNS distribution,renal secretion intourine, biliarysecretion
BSEP Liver Apical Vinblastine, tamoxifen, bile salts Biliary secretion
ABCC MRP1 Ubiquitous Basolateral Vinca alkaloids, methotrexate,etoposide
Transport into thebloodstream
MRP2 Liver, kidney, smallintestine
Apical Vinca alkaloids, methotrexate,pravastatin, ampicillin,ceftriaxone, cisplatin, irinotecan,hormone conjugates, bile salts
Biliary excretion,renal secretion intourine
MRP3 Liver, kidney, smallintestine
Basolateral Doxorubicin, vincristine,methotrexate, cisplatin, bile salts
Transport into thebloodstream
MRP4 Ubiquitous 6-Mercaptopurine,azathiopurine, adefovir,methotrexate, bile salts
MRP5 Ubiquitous 6-Mercaptopurine, adefovir
ABCG BCRP Placenta, liver,small intestine
Apical Mitoxantrone, doxorubicin,topotecan, zidovudine,methotrexate, irinotecan (SN-38)
Limiting oralabsorption, limitingfetal exposure,biliary excretion
See text for references.ACE, angiotensin-converting enzyme; CNS, central nervous system; HIV-1, human immunodeficiency virus-1; PAH,para-aminohippuric acid

REVIEW OF THE LITERATURE
26
2.7 OATP1B1
Genes encoding the OATP uptake transporters form a large family of solute carrier organicanion transporters (SLCO) within the SLC superfamily (Hagenbuch and Meier 2004). OATPs inthe OATP/SLCO superfamily are subdivided into families indicated by a number for > 40%amino acid sequence identity (e.g. OATP1/SLCO1), into subfamilies indicated by a letter for >60% amino acid sequence identity (e.g. OATP1B/SLCO1B) and into individual genes and geneproducts indicated by an additional number (e.g. OATP1B1/SLCO1B1), according to thephylogenetic relationships and chronology of identification (Hagenbuch and Meier 2004).OATP1A2 (previously known as OATP-A) was the first member to be described, followed bythe discovery of OATP1B1 in 1999 (Kullak-Ublick et al. 1995, Abe et al. 1999, Hsiang et al.1999, König et al. 2000). Today, 36 mammalian OATPs and 11 human OATPs have beenidentified (Hagenbuch and Meier 2003, Mikkaichi et al. 2004). OATP1B1, encoded by the geneSLCO1B1, is one of the main sodium-independent bile acid and organic anion transporters in theliver (Hsiang et al. 1999, König et al. 2000). In a recent study, OATP1B1 was also found at themessenger ribonucleic acid (mRNA) level in small intestinal enterocytes (Glaeser et al. 2007).
2.7.1 Structure and function
OATP1B1 is a 691-amino acid glycoprotein with 12 putative membrane-spanning domains(currently accepted structure based on hydropathy analyses) and a large fifth extracellular loop(Hagenbuch and Meier 2003, Chang et al. 2005). Common to all OATP proteins, OATP1B1carries N-glycosylation sites in extracellular loops 2 and 5 and the OATP ‘superfamilysignature’ D-X-RW-(I, V)-GAWW-X-G-(F, L)-L at the border between extracellular loop 3 andtransmembrane domain 6. OATP1B1 shares 80% amino acid identity with OATP1B3(Hagenbuch and Meier 2003). Its apparent molecular mass is 84 kDa, which is reduced afterdeglycosylation to 54 kDa (König et al. 2000). Its almost exclusive expression in the humanliver suggests that it plays a crucial role in the hepatic uptake and clearance of amphipathicorganic compounds. The mechanism of substrate transport is not completely understood,although it has been suggested that OATPs translocate their substrates through a central,positively charged pore in a so-called rocker-switch type of mechanism (Meier-Abt et al. 2005).This transport is independent of sodium, chloride and potassium gradients, membrane potentialand ATP levels. The phosphorylation state of at least the rat Oatp1a1 is important for transport,since extracellular ATP reduces Oatp1a1-mediated bromosulphophtalein (BSP) transport in rathepatocytes via phosphorylation of intracellular serine residues (Glavy et al. 2000). No high-resolution structures are currently known for OATP1B1, but one recent study using three-dimensional quantitative structure-activity relationship models showed that OATP1B1substrates produce a pharmacophore containing two hydrogen bond acceptors, one hydrogenbond donor and two hydrophobic regions (Hagenbuch and Meier 2004). In another study using ameta-pharmacophore approach combining limited datasets from different laboratories, cell typesand species, a meta-model for OATP1B1 was generated in which the hydrophobic features arecentrally located and hydrogen bond features located at the extremities (Chang et al. 2005).

REVIEW OF THE LITERATURE
27
2.7.2 Substrates
In general, OATP substrates appear to be anionic amphipathic molecules with a rather highmolecular weight (> 450) and a high degree of albumin binding under physiological conditions(Hagenbuch and Meier 2004). A variety of endogenous compounds such as bile acids, steroidconjugates, bilirubin glucuronides, thyroid hormones, eicosanoids, cyclic peptides and BSP aresubstrates of OATP1B1. Substrate drugs include the ACE inhibitors enalapril and temocapril,the angiotensin II receptor antagonists olmesartan and valsartan, the antifungal agentcaspofungin, the antibiotics rifampicin and benzylpenicillin, methotrexate, the endothelinreceptor antagonists atrasentan and bosentan, troglitazone sulphate, the active SN-38 metaboliteof the anticancer agent irinotecan, fexofenadine, the glucuronide of the cholesterol-loweringdrug ezetimibe and the statins atorvastatin, cerivastatin, fluvastatin, pitavastatin, pravastatin,rosuvastatin and simvastatin acid (Table 2). The pharmacokinetics of repaglinide has beenassociated with OATP1B1 transport function, although there is no in vitro evidence showingthat it is an OATP1B1 substrate (Niemi et al. 2005a,b, Kalliokoski et al. 2008b). In addition, thenatural toxins microcystin and phalloidin are substrates of OATP1B1 (Hagenbuch and Meier2003). Reports on unbound bilirubin being a substrate of OATP1B1 are somewhat controversial,since it has been shown to be transported by this transporter in both HEK293 (human embryonickidney) cells and Xenopus laevis oocytes, but no transport was observed in another study withHeLa (human cervical carcinoma) and HEK293 cells (Cui et al. 2001, Briz et al. 2003, Wang etal. 2003).

REVIEW OF THE LITERATURE
28
Table 2. OATP1B1 substrates.Molecule Km (µM) Transporter expression
systemReferences
ACU154 + MDCKII Takada et al. 2004Atorvastatin 12 HEK293 Kameyama et al. 2005Atrasentan + HeLa Katz et al. 2006Bamet-UD2 10 Oocyte Briz et al. 2002Bamet-R2 10 Oocyte Briz et al. 2002Benzylpenicillin + HEK293 Tamai et al. 2001Bilirubin (unconjugated) 0.0076 Oocyte Briz et al. 2003Bilirubin monoglucuronide 0.1 HEK293 Cui et al. 2001Bisglucuronosyl bilirubin 0.3 HEK293 Cui et al. 2001Bosentan 44 CHO Treiber et al. 2007Bromosulphophtalein 0.1 HEK293 Cui et al. 2001
0.3 Oocyte Kullak-Ublick et al. 20012.4 MDCKII Kopplow et al. 2005+ COS1 van der Deure et al. 2008
BQ-123 + Oocyte Kullak-Ublick et al. 2001Caspofungin + HeLa Sandhu et al. 2005Cerivastatin 3-18 Human hepatocytes Shitara et al. 2003
+ HEK293 Kameyama et al. 2005Cholate 11 HEK293 Cui et al. 2001Cholecystokinin octapeptide + HEK293 Hirano et al. 2004Cholyltaurine + HEK293 König et al. 2000DADLE 111 Rat hepatocytes Nozawa et al. 2003Demethylphalloidin 39 HEK293 Fehrenbach et al. 2003
17 Oocyte Meier-Abt et al. 2004DHEAS + Oocyte Abe et al. 1999
22 HEK293 Cui et al. 2001DPDPE + Oocyte Kullak-Ublick et al. 2001
+ Oocyte Abe et al. 2001Enalapril 262 HEK293 Liu et al. 2006E217ßG + Oocyte Abe et al. 1999
8.2 HEK293 König et al. 20009.7 Oocyte Nakai et al. 20013.7 Oocyte Tamai et al. 20018.2 HEK293 Cui et al. 200128 MDCKII Sasaki et al. 20028.3 HEK293 Hirano et al. 2004
E1S + Oocyte Abe et al. 19990.2 HEK293 Tamai et al. 20005.3 Oocyte Tamai et al. 200113 HEK293 Cui et al. 20010.5 HEK293 Hirano et al. 2004+ MDCKII Kopplow et al. 2005+ COS1 van der Deure et al. 2008
Ezetimibe glucuronide + HEK293 Oswald et al. 2008Fexofenadine + MDCKII Matsushima et al. 2008

REVIEW OF THE LITERATURE
29
Table 2. (continued)Molecule Km (µM) Transporter expression
systemReferences
Fluvastatin 2.4 MDCKII Kopplow et al. 200531 Oocyte Deng et al. 2008
Glycocholate + Oocyte Kullak-Ublick et al. 2001Irinotecan (SN-38 metabolite) + Oocyte Nozawa et al. 2005
+ HEK293 Nozawa et al. 2005Leukotriene C4 + Oocyte Abe et al. 1999Leukotriene E4 + Oocyte Abe et al. 1999Methotrexate + Oocyte Abe et al. 2001Microcystin-LR 7 Oocyte Fischer et al. 2005Olmesartan 43 Oocyte Nakagomi-Hagihara et al. 2006
13 HEK293 Yamada et al. 2007Pitavastatin 3.0 HEK293 Hirano et al. 2004
6.7 Oocyte Deng et al. 2008Pravastatin 35 HEK293 Hsiang et al. 1999
12 Oocyte Nakai et al. 200124 MDCKII Sasaki et al. 200286 HEK293 Kameyama et al. 200558 Oocyte Deng et al. 2008
Prostaglandin E2 + Oocyte Abe et al. 1999+ HEK293 Tamai et al. 2000
Rifampicin 13 Oocyte Vavricka et al. 20021.5 HeLa Tirona et al. 2003
Rosuvastatin 7.3 Oocytes Brown et al. 20018.5 Oocyte Schneck et al. 2004
Simvastatin + HEK293 Kameyama et al. 2005Taurolithocholate 3-sulphate + MDCKII Sasaki et al. 2002Taurocholate 34 HEK293c18 Hsiang et al. 1999
14 Oocyte Abe et al. 199910 HEK293 Cui et al. 2001
Temocapril + HEK293 Maeda et al. 2006aThyroid hormonesthyroxine + HEK293c18 Hsiang et al. 1999thyroxine 3.0 Oocyte Abe et al. 1999triiodothyronine 2.7 Oocyte Abe et al. 1999Iodothyronine sulphates + COS1 van der Deure et al. 2008Troglitazone sulphate + Oocyte Nozawa et al. 2004bThromboxane B2 + Oocyte Abe et al. 1999Valsartan 1.4 HEK293 Yamashiro et al. 2006+ Indicates that the molecule is a substrate but the Km value is unknownACU154, O-glucuronide of PKI116 (selective inhibitor of tyrosine kinase activity, Novartis Basel); BQ-123,cyclic-pentapeptide (cyclo[D-Trp-D-Asp-L-Pro-D-Val-L-Leu]); Bamet-R2, bile acid-cisplatin derivative [cis-diamine-chloro-cholylglycinate-platinum(II)]; Bamet-UD2, bile acid-cisplatin derivative [cis-diamine-bisursodeoxycholate-platinum(II)]; CHO, Chinese hamster ovary; DADLE, [D-Ala2, D-Leu5]-enkephalin (opioidpeptide analogue); DHEAS, dehydroepiandrosterone sulphate; DPDPE, [D-penicillamine2,5]-enkephalin (opioid-receptor antagonist); E217ßG, oestradiol-17ß-D-glucuronide; E1S, oestrone-3-sulphate; HEK293, humanembryonic kidney cells; HeLa, human cervical carcinoma cells; Km; Michaelis-Menten kinetic constant;MDCKII, Madin-Darby canine kidney strain II cells; oocyte, Xenopus laevis oocyte

REVIEW OF THE LITERATURE
30
2.7.3 Inhibitors
The immunosuppressive drug cyclosporine markedly increases the plasma concentrations ofseveral OATP1B1 substrates, such as statins and repaglinide (Arnadottir et al. 1993, Regazzi etal. 1993, Olbricht et al. 1997, Muck et al. 1999, Park et al. 2001, Åsberg et al. 2001, Simonsonet al. 2004, Kajosaari et al. 2005, Hirano et al. 2006). Although inhibition of CYP3A4 mayexplain the effects of cyclosporine on its substrate drugs simvastatin, lovastatin, atorvastatin andcerivastatin, it does not adequately explain its effect on the pharmacokinetics of rosuvastatin,pitavastatin and pravastatin, which are not significantly metabolized by CYP3A4 (Neuvonen etal. 2006). It is widely agreed that inhibition of OATP1B1-mediated hepatic uptake of substratedrugs contributes to these clinically observed drug interactions (Shitara et al. 2003). Gemfibroziland its glucuronide metabolite also inhibit OATP1B1 and significantly increase the plasmaconcentrations of several OATP1B1 substrate drugs including simvastatin acid (Backman et al.2000), lovastatin acid (Kyrklund et al. 2001), cerivastatin (Backman et al. 2002), pravastatin(Kyrklund et al. 2003), repaglinide (Niemi et al. 2003b), rosuvastatin (Schneck et al. 2004) andatorvastatin (Backman et al. 2005). Rifampicin, a strong inducer of drug-metabolizing enzymes,has increased the expression of OATP1B1 in cultured human hepatocytes in vitro (Niemi et al.2003a, Jigorel et al. 2006). This may explain the slight decrease in plasma pravastatinconcentrations when administered concomitantly with rifampicin (Kyrklund et al. 2004). On theother hand, rifampicin is a relatively potent inhibitor of OATP1B1 and OATP1B3 in vitro(Vavricka et al. 2002). In addition, the antimicrobial drugs clarithromycin, erythromycin,roxithromycin and telithromycin as well as the HIV protease inhibitors indinavir, ritonavir andsaquinavir have been identified as OATP1B1 inhibitors in vitro (Campbell et al. 2004, Hirano etal. 2006, Seithel et al. 2007).
2.7.4 SLCO1B1 pharmacogenetics
The SLCO1B1 gene is located in chromosome 12 (gene locus 12p12). A large number of SNPs,both nonsynonymous and synonymous, have been discovered in the SLCO1B1 gene, and severalof these affect transport function in vitro and in vivo (Figure 5). Most of the SNPs associatedwith altered transport function span the transmembrane domains or extracellular loop 5 ofOATP1B1. In vitro experimental systems expressing mutated OATP1B1 have been used todemonstrate the effects of SNPs on the uptake clearance of OATP1B1 (Table 3) (Tirona et al.2001, Iwai et al. 2004, König et al. 2006). The effects of certain SLCO1B1 polymorphisms ontransport function appear to be substrate-dependent (Tirona et al. 2001).
REVIEW OF THE LITERATURE
31
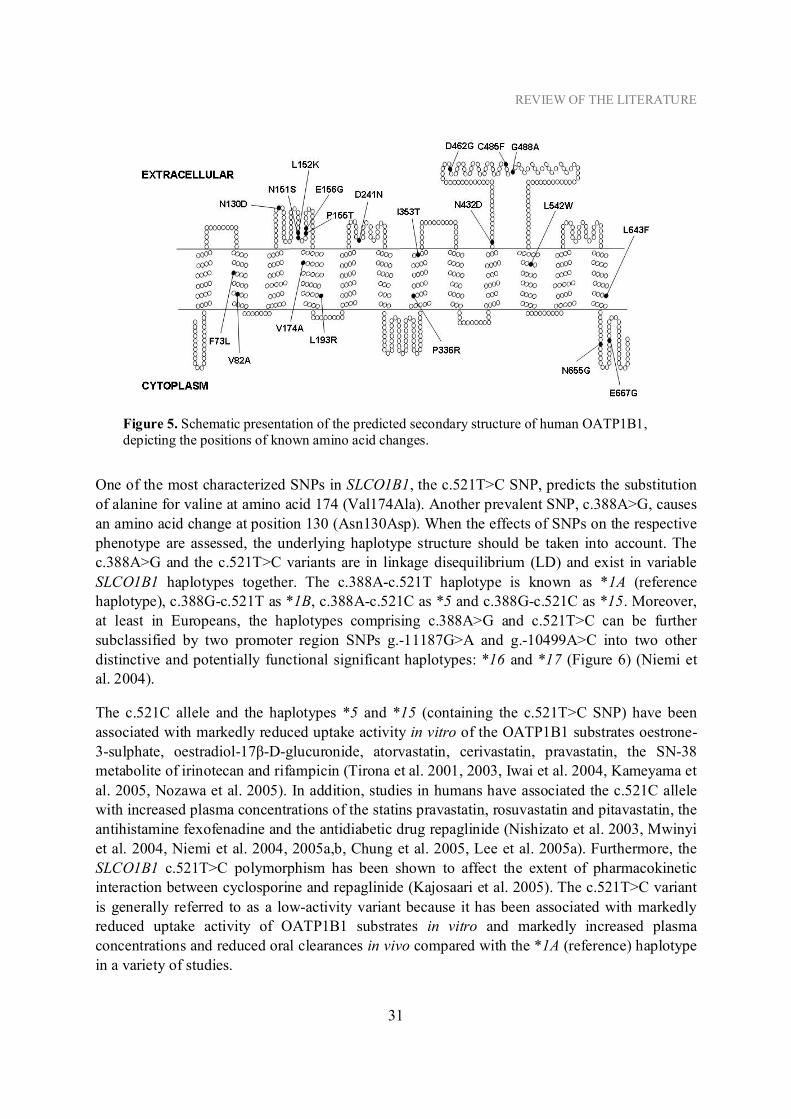
Figure 5. Schematic presentation of the predicted secondary structure of human OATP1B1,depicting the positions of known amino acid changes.
One of the most characterized SNPs in SLCO1B1, the c.521T>C SNP, predicts the substitutionof alanine for valine at amino acid 174 (Val174Ala). Another prevalent SNP, c.388A>G, causesan amino acid change at position 130 (Asn130Asp). When the effects of SNPs on the respectivephenotype are assessed, the underlying haplotype structure should be taken into account. Thec.388A>G and the c.521T>C variants are in linkage disequilibrium (LD) and exist in variableSLCO1B1 haplotypes together. The c.388A-c.521T haplotype is known as *1A (referencehaplotype), c.388G-c.521T as *1B, c.388A-c.521C as *5 and c.388G-c.521C as *15. Moreover,at least in Europeans, the haplotypes comprising c.388A>G and c.521T>C can be furthersubclassified by two promoter region SNPs g.-11187G>A and g.-10499A>C into two otherdistinctive and potentially functional significant haplotypes: *16 and *17 (Figure 6) (Niemi etal. 2004).
The c.521C allele and the haplotypes *5 and *15 (containing the c.521T>C SNP) have beenassociated with markedly reduced uptake activity in vitro of the OATP1B1 substrates oestrone-3-sulphate, oestradiol-17 -D-glucuronide, atorvastatin, cerivastatin, pravastatin, the SN-38metabolite of irinotecan and rifampicin (Tirona et al. 2001, 2003, Iwai et al. 2004, Kameyama etal. 2005, Nozawa et al. 2005). In addition, studies in humans have associated the c.521C allelewith increased plasma concentrations of the statins pravastatin, rosuvastatin and pitavastatin, theantihistamine fexofenadine and the antidiabetic drug repaglinide (Nishizato et al. 2003, Mwinyiet al. 2004, Niemi et al. 2004, 2005a,b, Chung et al. 2005, Lee et al. 2005a). Furthermore, theSLCO1B1 c.521T>C polymorphism has been shown to affect the extent of pharmacokineticinteraction between cyclosporine and repaglinide (Kajosaari et al. 2005). The c.521T>C variantis generally referred to as a low-activity variant because it has been associated with markedlyreduced uptake activity of OATP1B1 substrates in vitro and markedly increased plasmaconcentrations and reduced oral clearances in vivo compared with the *1A (reference) haplotypein a variety of studies.

REVIEW OF THE LITERATURE
32
Studies on the effect of the c.388A>G SNP and the *1B haplotype on OATP1B1 activity arecontroversial. In one in vitro study, the c.388G allele was associated with reduced transportactivity of OATP1B1 towards rifampicin (Tirona et al. 2003), but this reduction in in vitroactivity has not been seen in studies with other OATP1B1 substrates (Tirona et al. 2001, Iwai etal. 2004, Kameyama et al. 2005, Nozawa et al. 2005). On the other hand, the *1B haplotype hasbeen associated with increased activity of OATP1B1 in vivo and the plasma concentrations ofpravastatin and repaglinide have been approximately 30–35% lower in carriers of the *1Bhaplotype than in individuals with the *1A/*1A genotype (Mwinyi et al. 2004, Maeda et al.2006a, Kalliokoski et al. 2008a). In one in vivo study, the area under the plasma concentration-time curve (AUC) of ezetimibe was approximately 50% lower in subjects with the *1Bhaplotype compared with those with the *1A/*1A genotype (Oswald et al. 2008). Further studiesare required to clarify the effects of the c.388A>G SNP on drug pharmacokinetics in vivo inhumans, but it could be considered as a high-activity variant, at least for some substrates (Liu etal. 2006). The effects of the SLCO1B1 polymorphism on statins are further discussed in thecontext of the pharmacogenomics of statins.
Other, less studied, potentially functional SLCO1B1 variants have also been identified. Thec.467A>G (p.Glu156Gly), c.1058T>C (p.Ile353Thr), c.1463G>C (p.Gly488Ala) andc.1964A>G (p.Asp655Gly) SNPs have been associated with reduced transport function ofOATP1B1 in vitro but, except for the c.1463G>C variant with an allele frequency of 9% inAfrican-Americans, these SNPs are very rare (Tirona et al. 2001). In addition, the SLCO1B1c.578T>G variant (p.Leu193Arg) located in the fourth transmembrane helix has been associatedwith significant defects in protein maturation and in transport function, but it was found in onlyone liver sample in one study (Michalski et al. 2002). In this study, the c.463C>A (SLCO1B1*4)variant was also associated with reduced transport activity in the OATP1B1 substratetaurocholate, but no effect on transport function was seen with the other substrates tested (BSPor oestradiol-17 -D-glucuronide). The nonsynonymous c.1929A>C SNP (p.Leu643Phe) doesnot apparently affect hepatic OATP1B1 expression or transport function (Seithel et al. 2008b).Very few data on the effects of promoter region SNPs on OATP1B1 transport function areavailable. The g.-11187A>G SNP has been associated with reduced OATP1B1 activity in vivo(Niemi et al. 2004). In addition, the g.-11110T>G, g.-10499A>C and g.-314T>C allelefrequencies have been studied in Chinese, Malay and Indian populations, but no published dataon their functionality are available (Jada et al. 2007).
It is becoming evident that the incidence of sequence variations in the SLCO1B1 gene is heavilydependent on the ethnic background. A few studies had investigated the frequencies ofSLCO1B1 SNPs in individual populations before I undertook studies on this thesis. Thec.521T>C variant showed an allele frequency of approximately 10–15% in Asian populations,10–20% in Caucasians and 1–2% in African-American populations. The c.388A>G SNPshowed an allele frequency of approximately 30–45% in Caucasians, 70–80% in African-American/Sub-Saharan African populations and 60–90% in Asian populations (Tirona et al.2001, Nozawa et al. 2002, Niemi et al. 2004, Lee et al. 2005a, Jada et al. 2007). AmongJapanese subjects, most of the c.521C alleles had been reported to be part of the *15 haplotype.

REVIEW OF THE LITERATURE
33
However, it was unclear what the frequency was of *15 compared with the *5 haplotype inother populations. In addition, the frequencies of other, potentially functional, SNPs had beenpoorly elucidated in any population.
A few studies have shown that the carriers of the sequence variations SLCO1B1 c.388A>G andc.521T>C are more susceptible to higher levels of unconjugated bilirubin and it has beensuggested that these variations could reduce the normal functional rate of unconjugated bilirubinelimination (Ieiri et al. 2004, Huang et al. 2005). In addition, the c.388A>G SNP was found tobe a risk factor for severe hyperbilirubinaemia amongst neonates in another study (Huang et al.2004). Moreover, the SLCO1B1 C.521T>C SNP has been associated with increased levels ofthyroid hormone sulphates (van der Deure et al. 2008).
Figure 6. Schematic representation of functionally distinctive SLCO1B1 haplotypes.

Table 3. Nonsynonymous sequence variations in the SLCO1B1 gene.Variant allele frequency (%) Function
Location Nucleotide change Amino acid change Europeansa Africansb East Asiansc In vitro In vivo ReferencesExon 2 c.217T>C p.Phe73Leu 0-2 0 0 Unknown 1–5Exon 3 c.245T>C p.Val82Ala 0-2 0 0 Unknown 1–6Exon 4 c.388A>G p.Asn130Asp 30-45 72-81 62-86 1–4, 6–13Exon 4 c.452A>G p.Asn151Ser 0 0 0-4 Unknown Unknown 3, 4, 7, 8, 14Exon 4 c.455G>A p.Arg152Lys 0 0 0 Unknown Unknown 1, 2, 4, 5, 8Exon 4 c.463C>A p.Pro155Thr 13-23 2-10 0-3 1, 3–6, 10Exon 4 c.467A>G p.Glu156Gly 0-2 0 0 Unknown 1–5Exon 5 c.521T>C p.Val174Ala 15-20 1-4 8-16 1, 3–8, 10–12, 15Exon 5 c.578T<G p.Leu193Arg <0.3 Unknown Unknown Unknown 16Exon 6 c.721G>A p.Asp241Asn 0 0 0 Unknown Unknown 1, 2, 5Exon 8 c.1007C>G p.Pro336Arg 0 0 1 Unknown 3, 4, 14, 17Exon 8 c.1058T>C p.Ile353Thr 0-2 0 0 Unknown 1–5Exon 9 c.1294A>G p.Asn432Asp 0-1 0 0 Unknown 1–5Exon 10 c.1385A>G p.Asp462Gly 0-1 0 0 Unknown 1, 3–5Exon 10 c.1454G>T p.Cys485Phe 0 0 1 Unknown Unknown 1, 3, 4, 14Exon 10 c.1463G>C p.Gly488Ala 0 2-9 0 Unknown 1–6Exon 11 c.1628T>G p.Leu543Trp 0 Unknown <1 Unknown Unknown 14, 18Exon 14 c.1929A>C p.Leu643Phe 3-9 5-7 1 5, 6, 10, 14Exon 14 c.1964A>G p.Asp655Gly 0-2 0 0 Unknown 1, 3–5Exon 14 c.2000A>G p.Glu667Gly 0-2 0-34 0 Unknown 1, 3–51. Tirona et al. 2001; 2. Tirona et al. 2003; 3. Nishizato et al. 2003; 4. Jada et al. 2007; 5. Mwinyi et al. 2008; 6. Thompson et al. 2005; 7. Iida et al. 2001; 8.Nozawa et al. 2002; 9. Mwinyi et al. 2004; 10. Niemi et al. 2004; 11. Chung et al. 2005; 12. Lee et al. 2005a; 13. Maeda et al. 2006b; 14. Seithel et al. 2008b;15. Niemi et al. 2005b; 16. Michalski et al. 2002; 17. Kameyama et al. 2005; 18. Morimoto et al. 2004
Indicates unchanged transporter function; Indicates reduced transporter activity; Indicates increased transporter activityThe variant allele frequency is the range of values from different populations in the referenced articles.a Includes Europeans and European-Americans.b Includes Sub-Saharan Africans and African-Americans.c Includes the Chinese and Japanese.

REVIEW OF THE LITERATURE
35
3. CYP enzymes and their pharmacogenetics
The CYP enzymes are a superfamily of haem-containing monooxygenases located in theendoplasmic reticulum and involved in the metabolism of a large number of organic compounds(Wrighton and Stevens 1992, Lewis 2004). Over 2700 individual members of this enzymefamily are known to exist. The CYP enzymes were named after their characteristic peakabsorption wavelength (450 nm), seen when the reduced form of the enzyme is bound to carbonmonoxide (Omura and Sato 1962). The degree of similarity in amino acid sequence divides theCYP enzymes into families indicated by a number showing > 40% identity with each other (e.g.CYP3), into subfamilies indicated by a letter showing > 55% amino acid sequence identity (e.g.CYP3A) and into individual enzymes in which the specific gene is indicated by a number (e.g.CYP3A4) (Nebert and Russell 2002).
In humans, 57 CYP enzymes have been identified, most present in families CYP1–CYP4. TheCYP1, CYP2 and CYP3 families predominantly participate in the metabolism of exogenouscompounds, whereas the other CYP families are mainly involved in endogenous metabolism(Lewis 2004). CYP enzymes play a major role in human drug metabolism, mainly catalysingoxidation reactions in the liver in order to make drugs less active and thus more readilyexcretable. However, sometimes the metabolite formed can also be more toxic or the drug canbe metabolically activated (prodrug) (Meyer 1996, Riley 2001).
The endogenous role of CYP enzymes in humans concerns mainly the biosynthesis anddegradation of prostaglandins, steroids, fatty acids, eicosanoids, bile acids and vitamin D3. Anumber of CYP enzymes are also involved in the key stages of cholesterol metabolism (Nebertand Russell 2002). Substantial interindividual and intraindividual variability is seen in CYPactivity, and it can be affected by environmental influences including drug interactions(inhibition or induction by concomitant medications), genetic variability (polymorphisms) andphysiological as well as disease determinants (Zanger et al. 2008).
The CYP2C subfamily comprises CYP2C8, CYP2C9, CYP2C18 and CYP2C19, whichcollectively account for the metabolism of about 20% of clinically described drugs (Nebert andRussell 2002). The CYP2C18 protein has not been found in any human tissue, despite highlevels of CYP2C18 mRNA expression (Läpple et al. 2003). Other members of the CYP2Csubfamily play major roles in the metabolism of various clinically important drugs. CYP2C9 isthe most abundant CYP2C isoform in both the liver and intestine and it comprises about 17% ofthe total liver CYP content (Läpple et al. 2003). CYP2C9 substrates include many weakly acidiccompunds such as warfarin, tolbutamide, losartan, glimepiride, several nonsteroidal anti-inflammatory drugs, fluvastatin and rosuvastatin. Other statins are not known to be CYP2C9substrates. CYP2C9 is inhibited by sulphaphenazole, amiodarone and several azole antifungals,and induced by rifampicin, dexamethasone and barbiturates (Miners and Birkett 1998). AllCYP2C enzymes are genetically polymorphic and several sequence variations in CYP2C9 havebeen described, many of them associated with impaired enzymatic activity. The two mostcommon variant alleles are CYP2C9*2 (p.Arg144Cys) and CYP2C9*3 (p.Ile359Leu), with anallele frequency of approximately 10% and 8%, respectively, in Caucasians. The CYP2C9

REVIEW OF THE LITERATURE
36
polymorphism is of clinical relevance, e.g. in warfarin treatment (Daly 2003, Zanger et al.2008).
The CYP3A subfamily accounts for approximately 30–40% of the total CYP content in thehuman liver and is involved in the metabolism of over 50% of all drugs. The CYP3A subfamilycomprises the CYP3A4, CYP3A5, CYP3A7 and CYP3A43 enzymes. CYP3A4 is the mostabundant CYP enzyme in both the liver and intestine and is the most important drug-metabolizing enzyme in humans (Nebert and Russell 2002, Wrighton et al. 2000). CYP3A5 isexpressed mainly in the liver but also in extrahepatic tissues such as the intestine and lung(Kivistö et al. 1996a,b). CYP3A5 substrate specifity largely overlaps that of CYP3A4, but thecatalytic activity of CYP3A5 is usually smaller. Substrates of CYP3A include atorvastatin,simvastatin, midazolam, triazolam, cyclosporine A, erythromycin and several calcium channelblockers (Wrighton et al. 2000). The expression of CYP3A5 is largely polymorphic; only 20%of Caucasians are CYP3A5*1 carriers and express significant amounts of the metabolizingenzyme, while the CYP3A5*3 genotype that produces a nonfunctional protein is common in allethnic groups (Lamba et al. 2002, Daly 2003). Several CYP3A4 variant alleles have been found,but they occur at low frequencies and their contribution in determining CYP3A4 activityappears negligible (Lamba et al. 2002, Zanger et al. 2008).
4. Cholesterol homeostasis
Cholesterol is a major component of mammalian cell membranes modulating fluidity andmaintaining the barrier between the cell and the environment. Cholesterol is also essential fortissue growth, bile acid synthesis in the liver, vitamin D production in the skin and steroidhormone synthesis in the adrenal glands, ovaries and testes (Brown and Goldstein 1986). Thetransport of cholesterol in the circulatory system is facilitated by lipoproteins. Lipoproteins arespherical particles with a hydrophobic core of esterified cholesterol and triglycerides and asurrounding hydrophilic shell of apolipoproteins (apos), phospholipids and unesterifiedcholesterol. Plasma lipoproteins can be divided according to their density in ultracentrifugationinto chylomicrons (< 95 g/ml), very-low-density lipoprotein (VLDL; 0.95–1.006 g/ml),intermediate-density lipoprotein (IDL; 1.006–1.019 g/ml), low-density lipoprotein (LDL; 1.019–1.063 g/ml) and high-density lipoprotein (HDL; 1.063–1.210 g/l). The apolipoproteins (A, B, C,E) serve as structural proteins, cofactors for enzymes and ligands for cell surface receptors oflipoprotein particles, and as raw material for production of lipoproteins. Lipoprotein receptors,prototypically LDL receptors located on the surfaces of cells, bind LDL and carry cholesterolinto the cells by receptor-mediated endocytosis, where it is used by the cell or stored in the formof cytoplasmic cholesteryl ester droplets (Brown and Goldstein 1983, Brown and Goldstein1986, Martini and Pallottini 2007).
In humans, cholesterol is acquired either by de novo synthesis or by absorption from the diet.Accumulation of cholesterol in tissues due to increased dietary intake is generally prevented byseveral feedback responses down-regulating absorption or synthesis of cholesterol or enhancingcholesterol excretion (Gylling and Miettinen 1992). High cholesterol intake exceeding the

REVIEW OF THE LITERATURE
37
capacity of adaptive changes in cholesterol metabolism generally increases the serum levels oftotal cholesterol and LDL-C, accelerating the formation of atherosclerotic plaques and possiblyleading to coronary heart disease (Brown and Goldstein 1986).
Figure 7. The first and rate-limiting step in cholesterol synthesis is the synthesis of mevalonatefrom acetate. Mevalonate is further metabolized to squalene, which is cyclized to lanosterol.The formation of cholesterol from lanosterol involves several metabolic reactions in the latecholesterol biosynthesis pathway.

REVIEW OF THE LITERATURE
38
OHCholesterol
Figure 8. Chemical structure of cholesterol.
4.1 Cholesterol synthesis
The liver is the major organ for cholesterol synthesis, but most human organs such as theintestine, skin and muscle are also capable of synthesizing cholesterol (Dietschy 1984). Undernormal cholesterol intake and metabolism conditions, endogenous synthesis of cholesterolcontributes two-thirds of the total cholesterol input into the whole-body cholesterol pool(Dietschy 1984, Miettinen et al. 1992). Cholesterol is synthesized from acetyl coenzyme A(acetyl-CoA) through mevalonate (HMG-CoA reductase) pathway in the cytoplasm,endoplasmic reticulum and peroxisomes in a multistep manner (Figure 7 and 8) (Biardi andKrisans 1996). In the liver, acetyl-CoA is mainly derived from fatty acids. The cholesterolsynthesis rate is regulated by variable factors including cholesterol and fatty acid intake,cholesterol absorption and enterohepatic circulation of bile salts (Table 4) (Martini and Pallottini2007). Sterol regulatory-element binding proteins (SREBPs) are transcription factors, whichsense the intracellular and membrane levels of fatty acids and cholesterol and coordinate theuptake, de novo synthesis and oxidative catabolism of lipids (Raghow et al. 2008).
Table 4. Factors affecting cholesterol synthesis rate.Determinant Effect ReferencesInterrupted enterohepaticcirculation of bile acids
Färkkila et al. 1988
Cholesterol malabsorption Gylling and Miettinen 1995Dietary intake of
Cholesterol Gylling and Miettinen 1992, Duane 1993Polyunsaturated fatty acids , Connor et al. 1969, Glatz and Katan 1993Saturated fatty acids , Connor et al. 1969, Glatz and Katan 1993Squalene Strandberg et al. 1990Fibres Kesäniemi et al. 1990, Theuwissen and Mensink 2008
Diabetes Gylling and Miettinen 1997Thyroid hormones Abrams and Grundy 1981Obesity Miettinen 1971Weight reduction Leijd 1981
Indicates reduced cholesterol synthesis rate; Indicates increased cholesterol synthesis rate

REVIEW OF THE LITERATURE
39
4.2 Cholesterol absorption
Intestinal cholesterol consists of a mixture of cholesterol derived from dietary lipids, bile andthe desquamation of mucosal cells. Free cholesterol in mixed micelles is translocated from theintestinal lumen into the enterocytes by the Niemann-Pick C1-like 1 (NPC1L1) protein (Dawsonand Rudel 1999, Huff 2003, 2006, Martini and Pallottini 2007). In the enterocytes,approximately 75% of the absorbed cholesterol is esterified by acyl-coenzyme A:cholesterolacyltransferase (ACAT). Cholesterol esterification facilitates chylomicron assembly, whichprevents the resecretion of cholesterol back into the intestinal lumen via the ABCG5/G8transporter (Martini and Pallottini 2007). Cholesterol, cholesterol esters, triglycerides andphospholipids are packaged within the endoplasmic reticulum together with apoB48 intochylomicrons that enter the circulation via the thoracic duct (Huff 2003). Nascent chylomicronsacquire other apolipoproteins from endogenous lipoproteins and the chylomicron triglyceridesare hydrolysed by endothelial cell-bound lipoprotein lipase into cholesterol-rich chylomicronremnants. These remnants are taken into the liver with the interaction of apoE and lipidreceptors such as the LDL receptor. Within the hepatocyte, remnant derived cholesterol canregulate cholesterol metabolism through down-regulation of HMG-CoA reductase andexpression of LDL receptors. Remnant cholesterol can be packaged into endogenouslipoproteins that enter the circulation, catabolised to bile acids or secreted into the bile (Dawsonand Rudel 1999).
4.3 Cholesterol elimination and bile acid metabolism
The enzymatic catabolism of cholesterol in the liver produces amphipathic steroidal compoundscalled bile acids, predominantly cholic acid (CA) and chenodeoxycholic acid (CDCA).Cholesterol 7 -hydroxylase (CYP7A1) is encoded by the CYP7A gene and is the first and rate-limiting step in bile-acid synthesis in the main (classical) pathway. The catabolism ofcholesterol to bile acids is an important route for the elimination of cholesterol from the body,accounting for approximately 50% of the cholesterol eliminated daily. The nonhepatic pathwaysof cholesterol elimination are via production of steroid hormones and desquamation of epithelialcells (Russell 1999, St-Pierre et al. 2001).
After their synthesis in hepatocytes, bile acids are conjugated with the amino acids glycine ortaurine to improve their solubility and excreted as bile salts. The detergent properties of bilesalts allow solubilization of biliary phospholipids and free cholesterol into mixed micelles,which are translocated across the hepatocyte canalicular membrane (Table 5). A small part ofthe bile is directly returned to the liver by intrahepatic cycling through the periductular capillaryplexus (cholehepatic shunt pathway), but most of the bile is secreted via the bile duct and gallbladder into the lumen of the small intestine (St-Pierre et al. 2001, Meier and Stieger 2002,Kullak-Ublick et al. 2004, Stieger et al. 2007). In the intestinal lumen, bile salts act as detergentsto emulsify dietary lipids and lipid-soluble vitamins as well as regulate pancreatic secretions andthe release of gastrointestinal peptides, and thus play an essential role in lipid absorption (Koopet al. 1996).

REVIEW OF THE LITERATURE
40
Reabsorption of bile salts occurs primarily in the ileum via active uptake of bile salts into theenterocytes (Table 5) and by passive diffusion in the small and large intestines (Lin et al. 1990,Dawson et al. 2005, Alrefai and Gill 2007). The absorbed bile salts are then returned to the livervia the portal circulation and resecreted into the bile. Approximately 80% of the hepatic uptakeof bile salts back into the hepatocytes is mediated by NTCP and the rest is transported bysodium-independent mechanisms, mainly OATPs (Table 5) (St-Pierre et al. 2001, Kullak-Ublicket al. 2001, Lee et al. 2005b, Niemi 2007). Cholesterol and bile salts that escape intestinalreabsorption are excreted into the faeces (Dietschy 1984).
Bile salts can regulate their own uptake and efflux systems and also the expression of key bileacid-synthesizing enzymes and thus cholesterol homeostasis through activation of nuclearhormone receptors such as PXR and FXR (Russell 1999, Meier and Stieger 2002). Overall,hepatic cholesterol availability is regulated by complex feedback loops that involve cholesterolsynthesis, intestinal absorption, and elimination, and the enterohepatic circulation of bile acids(Miettinen et al. 1992, Huff 2003).
4.4 Plasma noncholesterol sterols
In addition to cholesterol, small amounts of noncholesterol sterols, including plant sterols fromdietary plant materials and cholesterol precursor sterols, circulate in the human blood stream.Plasma concentrations of several noncholesterol sterols, including demethylated and methylatedcholesterol precursor sterols, cholesterol derivatives and plant sterols reflect the rate ofcholesterol metabolism in humans (Miettinen 1970, Miettinen et al. 1986).
Lathosterol and desmosterol are late intermediates in the cholesterol synthesis pathway and themajor demethylated precursor sterols present in fasting plasma. Their plasma levels areassociated with the activity of hepatic HMG-CoA reductase and, accordingly, reflect thecholesterol synthesis rate in a normal population (Björkhem et al. 1987, Miettinen et al. 1990).
Squalene is synthesized from acetate and further metabolized to cholesterol. The dietary intakeof squalene also contributes significantly to the total squalene pool in humans. Squalene plasmalevels reflect cholesterol synthesis less consistently, but are also used to assess lipid homeostasis(Miettinen 1970, Miettinen and Vanhanen 1994).
Cholestanol is a 5 -saturated derivative of cholesterol that is derived mainly from endogenoussynthesis; less than 5% of the intestinal cholestanol from dietary intake is absorbed (Miettinen etal. 1989). On the other hand, plant sterols such as sitosterol, avenasterol and campesterol are notsynthesized in humans but are acquired from dietary sources, including vegetable oils and nuts.Around 5–10% of plant sterols are absorbed from the intestine. In normal populations, fastingplasma levels of plant sterols and cholestanol reflect cholesterol absorption efficiency(Miettinen et al. 1989, 1990).

REVIEW OF THE LITERATURE
41
Table 5. Bile acid transporters in humans.Cell type Localization Transporter Function ReferencesHepatocyte Basolateral NTCP Na+-dependent uptake of
bile acids into hepatocytesHagenbuch and Meier1994
Cholangiocyte OATP1A2 Na+-independent uptakeof bile acids, multispecific
Kullak-Ublick et al.2001, Hagenbuch andMeier 2004
Hepatocyte Basolateral OATP1B1 Na+-independent uptakeof bile acids intohepatocytes, multispecific
Kullak-Ublick et al.2001, Hagenbuch andMeier 2004
Hepatocyte Basolateral OATP1B3 Na+-independent uptakeof bile acids intohepatocytes, multispecific
Kullak-Ublick et al.2001, Hagenbuch andMeier 2004
EnterocyteCholangiocyteRenal tubular cell
Apical ASBT Na+-dependent uptake ofbile acids into enterocytes,cholangiocytes and re-uptake into renal tubules
Wong et al. 1995,Craddock et al. 1998
Hepatocyte Apical/Canalicular
BSEP ATP-dependent excretionof bile acids intocanaliculus
Noe et al. 2002
Hepatocyte Apical/Canalicular
MRP2 ATP-dependent excretionof bile acids intocanaliculus, multispecific
Keppler et al. 1997
HepatocyteCholangiocyteEnterocyte
Basolateral MRP3a ATP-dependent bile acidefflux?, multispecific
Scheffer et al. 2002,Borst et al. 2007
Hepatocyte Basolateral MRP4a ATP-dependent bile acidefflux?, multispecific
Zelcer et al. 2003, Borstet al. 2007
Enterocyte Cytosolic IBABP Intracellular bile acidtransport in enterocytes
Lin et al. 1990
Enterocyte Basolateral OST /ß Na+-independent bile acidefflux from enterocytesinto portal blood
Dawson et al. 2005
ASBT, Apical sodium dependent bile acid transporter; BSEP, Bile salt export pump; IBABP, Ileal bile acidbinding protein; MRP, Multidrug resistance-associated protein; NTCP, Sodium-dependent taurocholate co-transporting protein; OATP, Organic anion-transporting polypeptide; OST, Organic solute transportera The role of MRP3 and MRP4 in bile salt homeostasis is uncertain (Borst et al. 2007).

REVIEW OF THE LITERATURE
42
5. HMG-CoA reductase inhibitors (statins)
Several classes of lipid-modifying drugs are available, including HMG-CoA reductase inhibitors(statins), bile acid-binding resins (e.g. cholestyramine), nicotinic acid (niacin), fibrates (e.g.gemfibrozil) and cholesterol-absorption inhibitors (e.g. ezetimibe). Of the lipid-modifyingtherapies, statins are the most commonly prescribed (Downton and Clark 2003). Large-scalestudies have demonstrated the beneficial effects of statins in both primary and secondaryprevention of cardiovascular disease, regardless of gender, age or baseline lipid values(Scandinavian Simvastatin Survival Study Group 1994, Shepherd et al. 1995, Sacks et al. 1996,Strandberg et al. 2001, 2008, Heart Protection Study Collaborative Group 2002, Law et al.2003).
The technique for cholesterol-lowering with statins emerged from the discovery in 1976 of aclass of fungal metabolites that inhibit HMG-CoA reductase. The original compound,compactine, is a Penicillium citrium derivative. It is a potent competitive inhibitor of HMG-CoA reductase, with an inhibitory constant of approximately 10-9 M (Endo et al. 1976, Albertset al. 1980, Endo 1985). Lovastatin is a product of Aspergillus terreus fermentation, and it wasthe first statin to become available for prescription in 1987. Simvastatin and pravastatin arechemically modified derivatives of lovastatin and were approved for marketing in 1988 and1991, respectively. Fluvastatin, atorvastatin, cerivastatin, rosuvastatin and pitavastatin are alltotally synthetic statins and were approved for marketing in 1994, 1997, 1998, 2003 and 2003(only in the Asian market), respectively (Tobert 2003, Mahley and Bersot 2006). Six differentstatins (simvastatin, lovastatin, pravastatin, fluvastatin, atorvastatin and rosuvastatin) arecurrently on the Finnish market together with other lipid-modifying agents, and over 600 000Finnish patients receive statin therapy (Ruokoniemi et al. 2008; http://www.nam.fi).
5.1 Pharmacodynamics and clinical use
Statins are reversible competitive inhibitors of the HMG-CoA reductase enzyme, whichcatalyses the first and rate-limiting step from HMG-CoA to mevalonate in de novo cholesterolsynthesis (Figure 9). Inhibition of this enzyme reduces cholesterol synthesis in the hepatocytes,leading to a reduction in intracellular cholesterol concentration and a responsive increase inLDL receptor expression on the hepatocyte cell surface. This results in increased extraction ofLDL-C from the blood and decreased circulating total cholesterol and LDL-C concentrations. Ameta-analysis showed that statins can lower LDL-C by an average of 1.8 mmol/l, which reducesthe risk of CHD events by about 60% and stroke by 17% (Law et al. 2003).
In addition to lowering plasma LDL-C and total cholesterol levels, statins also moderatelyreduce triglyceride levels and increase HDL-cholesterol levels (Kreisberg and Oberman 2002).Secondary mechanisms by which statins may reduce lipoprotein levels include inhibition ofhepatic synthesis of apoB100 and reduction in synthesis and secretion of triglyceride-richlipoproteins (VLDL and IDL). In addition, the inhibition of synthesis of nonsteroidal isoprenoidcompounds (also produced from mevalonate) (Figure 9) may explain the pleiotropic properties

REVIEW OF THE LITERATURE
43
of statins leading to beneficial cardiovascular effects independent of their lipid-modifyingproperties. These include restoration of endothelial cell function, modification of inflammatoryresponses, antithrombotic and antioxidant effects, as well as reduction of smooth muscle cellproliferation and cholesterol accumulation. These biological effects beyond LDL reduction maydiffer among statins (Rosenson and Tangney 1998, Chong et al. 2001, Bonetti et al. 2003).Statins have been shown to slow the progression or even promote regression of coronaryatherosclerosis, possibly due to shrinkage of the lipid core of the atherosclerotic plaque,avoiding plaque rupture that would otherwise trigger intramural haemorrhage and intraluminalthrombosis (Kreisberg and Oberman 2002, Liao 2002).
The roughly equipotent doses of statins needed to reduce LDL-C by 25–35% from baseline arefluvastatin 80 mg, pravastatin 40 mg, simvastatin 20 mg, rosuvastatin 5 mg and atorvastatin 10mg (Jones et al. 1998, Chong et al. 2001, Law et al. 2003). Generally, doubling a statin doseresults in an additional 6% decrease in LDL-C. However, considerable interindividualdifferences exist in the efficacy of statins (Jones et al. 1998).
Statins are principally administered with the evening meal or at bedtime, due to diurnal variationin the cholesterol synthesis rate (Miettinen 1980). However, statins such as atorvastatin (and itsmetabolites) and rosuvastatin have long half-lives and therefore administration any time of theday is equally effective (Table 6).
Figure 9. Simplified scheme of the biosynthetic pathway of cholesterol and other cometabolites.

REVIEW OF THE LITERATURE
44
5.2 Pharmacokinetic properties
The chemical structures of fluvastatin, pravastatin, simvastatin, rosuvastatin and atorvastatin areshown in Figure 10. These structures can be divided broadly into three parts: an analogue of thenatural substrate (HMG-CoA), a complex hydrophobic ring structure that is covalently linked tothe substrate analogue and involved in the binding of statin to the reductase, and side groups onthe rings that define the solubility and other pharmacokinetic properties (Schachter 2005).Crystal structures have shown that statins act by binding to the active site of the HMG-CoAreductase enzyme, thus sterically preventing the substrate from binding. The substrate-bindingpocket of the enzyme undergoes a conformational change that enables the hydrophobic ringstructures of statins to be accommodated to the enzyme (Istvan and Deisenhofer 2001). Thesignificance of the differences in the binding sites of different statins is not fully understood, butthe additional binding interactions of rosuvastatin with the HMG-CoA reductase may explain inpart its increased potency compared with other statins (Schachter 2005).
Simvastatin is administered as a lipophilic lactone prodrug, whereas fluvastatin, pravastatin,rosuvastatin and atorvastatin are given as active acid forms. Generally, the lipophilic statins aremore readily distributed into the peripheral tissues by passive diffusion than hydrophilic statinssuch as pravastatin and rosuvastatin (Lennernäs and Fager 1997, Hamelin and Turgeon 1998).However, many statins are converted in the body to their lactone forms or metabolites that canbe more lipophilic than the parent acid form. Both acid and lactone forms as well as metabolitescan be important in statin interactions (Neuvonen et al. 2006). Generally, lipophilic drugs appearto be more susceptible to oxidative metabolism by CYP enzymes than hydrophilic drugs(Schachter 2005).
Substantial interindividual differences are seen in the pharmacokinetics of different statins. Forexample, AUC of pravastatin ranges by more than 10-fold in young healthy adults (Shitara andSugiyama 2006). Since many statins are subject to considerable first-pass metabolism in theintestinal wall and liver and substrates of various transporters, the variable activity ofmetabolizing CYP enzymes and transporters mediating statin uptake and efflux can lead toconsiderable differences in statin bioavailability (Lennernäs and Fager 1997, Schachter 2005).The contents and pH of the gastrointestinal tract during statin absorption can also causevariability in statin bioavailability (Neuvonen et al. 2006). The pharmacokinetic properties ofstatins are summarized in Table 6.
5.2.1 Fluvastatin
Fluvastatin is administered in the active hydroxyl acid form; its octanol/water partitioncoefficient (logP) is 3.2. Over 90% of the fluvastatin is absorbed from the intestinal tract and asubstantial proportion undergoes first-pass hepatic extraction, leading to a systemicbioavailability of around 30%. Fluvastatin is highly bound to plasma proteins in the circulation.It is almost completely biotransformed to inactive metabolites, mainly by CYP2C9. The 6-hydroxy and N-desisopropyl metabolites are formed by CYP2C9, and the 5-hydroxy metabolite

REVIEW OF THE LITERATURE
45
is formed by CYP2C9, CYP3A4, CYP2C8 and CYP2D6. Fluvastatin has a short eliminationhalf-life (t½) of 0.5 to 1 hour and is excreted mainly as metabolites, primarily into the bile(Fischer et al. 1999, Scripture and Pieper 2001, Schachter 2005). Fluvastatin is also available inextended-release formulations, the pharmacokinetic properties of which differ from thoseintroduced here (Sabia et al. 2001). Fluvastatin is a substrate of at least the OATP1B1,OATP1B3 and BCRP transporters (Hirano et al. 2005b, Kopplow et al. 2005).
Itraconazole or other CYP3A inhibitors do not have a significant effect on fluvastatinpharmacokinetics (Kivistö et al. 1998, Neuvonen et al. 2006). Fluconazole, a potent CYP2C9inhibitor, has increased the AUC of fluvastatin by 80% (Kantola et al. 2000, Scripture andPieper 2001). Gemfibrozil, an inhibitor of CYP2C8 and OATP1B1, has not affected the plasmaconcentrations of fluvastatin (Spence et al. 1995) and cyclosporine, an inhibitor of at leastOATP1B1, OATP2B1, OATP1B3, MRP2, MDR1 and CYP3A4, has only moderately increasedthe plasma concentrations of fluvastatin (Åsberg 2003, Neuvonen et al. 2006). Rifampicin, aninducer of CYP3A4, OATP1B1 and MDR1, has decreased the fluvastatin AUC by 50%(Scripture and Pieper 2001, Niemi et al. 2003a, Jigorel et al. 2006).
Figure 10. Chemical structures of HMG-CoA and the investigated statins.
S-CoA
O
O
OH
CH3
OH O
OH
O
N CH3
CH3F
OH
CH3
OH
O
O
CH3
H
O
OH
O
HMG-CoA Fluvastatin Pravastatin
O
OOH
H
CH3
CH3
O
O
CH3 CH3H
OH OO
OH
N N
F
CH3
CH3
NS CH3
O
CH3
O
OH O
OH
O
N CH3
CH3F
NH
O
Simvastatin Rosuvastatin Atorvastatin

REVIEW OF THE LITERATURE
46
5.2.2 Pravastatin
Pravastatin is a relatively hydrophilic statin (logP –0.2) (Igel et al. 2002). It is administered asthe sodium salt of active pravastatin acid, preferably without food intake, which seems todecrease pravastatin bioavailability by approximately 35–40% (Pan et al. 1993). The hepaticextraction ratio of pravastatin is 45–66%, and the resulting bioavailability around 20%(Lennernäs and Fager 1997). The circulating levels of unbound pravastatin are high (50%)compared with other statins, which are in general largely bound to plasma proteins. Sulphationis more important than CYP-mediated metabolism in pravastatin elimination, but principallypravastatin is excreted unchanged into both the bile and urine (Igel et al. 2002). Carrier-mediated processes are important for the hepatic uptake of especially hydrophilic statins, such aspravastatin, to enable hepatic accumulation and biliary excretion. Pravastatin is a substrate of atleast the uptake transporters OATP1B1, OATP2B1, OAT3, as well as the efflux transportersMRP2, MDR1 and BCRP (Nakai et al. 2001, Nozawa et al. 2004a, Takeda et al. 2004, Chen etal. 2005, Matsushima et al. 2005). In addition, BSEP transported pravastatin in one study(Hirano et al. 2005a).
Itraconazole, or other strong inhibitors of CYP3A, do not significantly increase the plasmaconcentrations of pravastatin (Neuvonen et al. 1998, 2006). Cyclosporine has increased theAUC of pravastatin by 5–10-fold (Åsberg 2003, Hedman et al. 2004). Gemfibrozil increases andrifampicin decreases the pravastatin AUC by 30% and 100%, respectively (Kyrklund et al.2003, 2004).
5.2.3 Simvastatin
Simvastatin is a semisynthetic derivative of lovastatin and is administered as a rather lipophiliclactone prodrug (logP 4.7), of which approximately 60–85% is absorbed from thegastrointestinal tract. The plasma protein binding of simvastatin is high (> 95%) compared withthat of the more hydrophilic statins. The inactive parent simvastatin lactone is either oxidized byCYP3A4 (and by CYP3A5) in the intestinal mucosa and liver to more than 10 metabolites, orhydrolysed to simvastatin acid, the main active metabolite of simvastatin (Vickers et al. 1990,Igel et al. 2002). The bioavailability of simvastatin is only around 5%, largely due to itsextensive first-pass metabolism in the intestinal wall and liver (Todd and Goa 1990). The majoractive metabolites are the ß-hydroxy acid and its 6’-hydroxy, 6’-hydroxymethyl and 6’-exomethylene derivatives (Vickers et al. 1990, Lennernäs and Fager 1997). Active simvastatinacid is also further metabolized, mainly by CYP3A4 and CYP2C8 (Prueksaritanont et al. 2002,2003). The active metabolites also account for the HMG-CoA reductase inhibition (Schachter2005). Simvastatin is eliminated principally as metabolites into the bile. Simvastatin lactone isnot transported by OATP1B1, but simvastatin acid strongly inhibits OATP1B1-mediatedhepatic uptake of pravastatin, suggesting it to be an OATP1B1 substrate (Hsiang et al. 1999,Chen et al. 2005). In addition, simvastatin acid is an MDR1 substrate (Chen et al. 2005).

REVIEW OF THE LITERATURE
47
CYP3A4 inhibitors markedly elevate the plasma concentrations of both simvastatin andsimvastatin acid (Neuvonen et al. 2006). For example, concomitant administration ofitraconazole increased the AUC of simvastatin by approximately 20-fold (Neuvonen et al.1998). On the other hand, gemfibrozil, which is an inhibitor of CYP2C8 and OATP1B1, but notCYP3A4, increases the simvastatin acid AUC by approximately 200%, but does notsignificantly affect the parent lactone form (Backman et al. 2000). Rifampicin decreasessimvastatin and simvastatin acid AUC by approximately 90% (Kyrklund et al. 2000).Cyclosporine increased the AUC and plasma concentrations of simvastatin by approximately 6-to 8-fold (Arnadottir et al. 1993, Ichimaru et al. 2001, Åsberg 2003).
5.2.4 Rosuvastatin
Rosuvastatin is a relatively hydrophilic (logP -0.3) statin, with a long t½ (19 hours) (McTaggartet al. 2001, Schachter 2005). Approximately 50% of the rosuvastatin is absorbed from theintestinal tract and the hepatic extraction ratio is 63%. The oral bioavailability of rosuvastatin isabout 20% and its level of protein binding is rather high (90%), despite marked hydrophilicity.Faecal excretion accounts for approximately 90% of the elimination of oral rosuvastatin and itsmetabolites, probably due to high levels of hepatic extraction, and only 10% is recovered in theurine (McTaggart et al. 2001, Lee et al. 2005a). Metabolism is not a major mechanism forrosuvastatin elimination, but it is partly biotransformed via CYP2C9-mediated N-demethylationand UGT1A1- and UGT1A3-mediated acyl-glucuronidation and spontaneous lactonization(Prueksaritanont et al. 2002). Rosuvastatin is a substrate of the uptake transporters OATP1B1,OATP2B1, OATP1B3, OATP1A2 and NTCP. Rosuvastatin efflux is mediated by at least theefflux transporters BCRP and MRP2 (Cooper et al. 2003, Hirano et al. 2005b, Ho et al. 2006,Huang et al. 2006, Kitamura et al. 2008b).
Itraconazole has had only a modest effect on rosuvastatin plasma concentrations (Cooper et al.2003), while fluconazole has increased the rosuvastatin AUC only marginally (Cooper et al.2002). Cyclosporine and gemfibrozil increase the AUC of rosuvastatin approximately 7-fold and2-fold, respectively (Schneck et al. 2004, Simonson et al. 2004). Rifampicin does notsignificantly affect the pharmacokinetics of rosuvastatin (Zhang et al. 2008).
5.2.5 Atorvastatin
Atorvastatin is administered as the calcium salt of the active hydroxy acid form (logP 4.1). It iswell absorbed but undergoes marked first-pass metabolism, resulting in an oral bioavailabity ofabout 15% (Lennernäs 2003). The administration time of the day affects the rate and extent ofatorvastatin absorption but does not appear to affect the lipid-lowering response (Schachter2005). Atorvastatin has a relatively long half-life of 14 hours. Atorvastatin acid isbiotransformed to the more lipophilic atorvastatin lactone, either by a coA-dependent or an acylglucuronide intermediate pathway (Kearney et al. 1993, Prueksaritanont et al. 2002). Bothatorvastatin and its lactone form are metabolized primarily by CYP3A4, and also by CYP2C8 at

REVIEW OF THE LITERATURE
48
a low rate (Jacobsen et al. 2000, Neuvonen et al. 2006). The lactone forms of atorvastatin and itsmetabolites can be hydrolysed to the respective acid forms nonenzymatically or by esterases andparaoxonases. The major hydroxy acid metabolites, 2-hydroxyatorvastatin and 4-hydroxyatorvastatin, are pharmacologically active, contributing to HMG-CoA reductaseinhibition during atorvastatin treatment (Lennernäs 2003). Atorvastatin acid is a substrate ofOATP1B1, OATP2B1 and the efflux transporters MDR1 and BCRP (Wu et al. 2000, Chen et al.2005, Hirano et al. 2005b, Grube et al. 2006).
The atorvastatin plasma concentrations have been significantly elevated when administeredconcomitantly with CYP3A4 inhibitors, gemfibrozil and cyclosporine (Hermann et al. 2004,Neuvonen et al. 2006). Gemfibrozil only moderately increases the AUC values of atorvastatinand its active acid metabolites, whereas cyclosporine has increased the AUC of atorvastatin 6-to 15-fold (Åsberg et al. 2001, Hermann et al. 2004). Itraconazole has increased the AUC ofatorvastatin 3-fold (Kantola et al. 1998). Multiple-dose rifampicin decreases the atorvastatinAUC by about 80% (Backman et al. 2005), but a single dose of rifampicin has increased theatorvastatin AUC by over 600% (Lau et al. 2006, 2007). This is probably due to the inhibition ofOATP-mediated hepatic uptake of atorvastatin by rifampicin (Vavricka et al. 2002).
Table 6. Pharmacokinetic properties of statins.Fluvastatin Pravastatin Simvastatin Rosuvastatin Atorvastatin
Optimal time of dosing Evening Evening Evening Any time ofday
Any time ofday
Absorption (%) > 90 35 60–85 ~50 30Hepatic extraction(% of absorbed dose)
68 45–66 78–87 63–90 70
Bioavailability (%) 24-30 18 <5 20 12Effect of food onbioavailabilitytmax (h) 0.5–1.5 0.9–1.6 1.3–2.4 3 2–4t½ (h) 1–3 1–3 2–5 20 7–20Solubility Lipophilic Hydrophilic Lipophilic Hydrophilic LipophilicProtein binding (%) 98 ~50 95–98 90 98Elimination half-life (h) 1.2 1.8 2 19 14Substrate of OATP1B1a Yes Yes Yesb Yes YesMetabolizing CYPenzymes (of metabolite)
CYP2C9 (CYP3A4) CYP3A4CYP2C8
CYP2C9(CYP2C19)
CYP3A4(CYP2C8)
Active metabolites No No Yes Minor YesRenal excretion (%) 6 20 13 10 <5Max FDA approveddose (mg)
80 80 80 40 80
Adapted from Igel et al. (2002), Schachter (2005) and Neuvonen et al. (2006) Indicates that food reduces bioavailability; Indicates that food does not affect bioavailability
FDA, Food and Drug Administration (US)a Obtained from Niemi (2007) b Simvastatin acid is a substrate of OATP1B1

REVIEW OF THE LITERATURE
49
5.3 Adverse effects
In general, statins are regarded as a safe and well-tolerated class of drugs; serious adverse eventsare rare (Pasternak et al. 2002). A small percentage of patients experience asymptomatic,reversible increase in liver enzymes (notably alanine and aspartate transaminases), but thisincrease is not generally associated with liver damage (Armitage 2007). Statins can also causemuscle pain or weakness (myalgia), sometimes in association with elevated creatine kinase(CK) levels (myopathy), which may progress to muscle breakdown (rhabdomyolysis),myoglobin release, renal failure and even death (Vaklavas et al. 2008). Asymptomatic elevationof CK can sometimes also occur with statin therapy, but the clinical relevance of this is unclear.In addition, some patients receiving statin therapy develop significant muscle symptoms withdemonstrable weakness and histopathologic findings of myopathy despite normal CK levels(Phillips et al. 2002).
The mechanisms by which statins cause these muscle-related adverse effects remain largelyunknown, but myopathy appears to be a class-effect of statins, dose-dependent and associatedwith statin concentrations in the blood (Bradford et al. 1991, Dujovne et al. 1991, Laaksonen2006). Nonspecific muscle aches or joint pains that are not associated with significant increasesin CK are reported generally by 1–5% of participants in placebo-controlled trials, with nosignificant differences in reporting between the statin and the placebo groups (Thompson et al.2003, Armitage 2007). The incidence of statin-induced myopathy is approximately 11 in 100000 person-years of follow-up, whereas rhabdomyolysis is even more rare (approximately 3.4per 100 000 person-years), but the incidences of both increase with higher doses of statins andother predisposing factors (Graham et al. 2004, Law and Rudnicka 2006, Armitage 2007).However, accurate estimation of the occurrence of muscle-related symptoms less severe thanrhabdomyolysis is difficult, due to poor reporting and general exclusion of patient groups proneto statin-induced myopathy from large clinical trials (Law and Rudnicka 2006, Vaklavas et al.2008). It has been suggested that the frequencies of mild and moderate muscle symptoms withhigh-dose statin therapy may be more common than as estimated from the large clinical trials.For example, in the PRIMO (Prediction du Risque Musculaire en Observationnel) study, 10.5%of patients receiving high-dose statin therapy complained of muscle pain, and the highest rate(18.2%) was associated with high-dose simvastatin treatment (Bruckert et al. 2005).
Most of the predisposing factors for statin-induced muscle-related adverse effects promotemyopathy by altering the metabolism and increasing the bioavailability of statins (Table 7).Comedication with drugs that share common metabolic pathways can significantly increase thelikelihood of muscle toxicity (Thompson et al. 2003, Law and Rudnicka 2006, Neuvonen et al.2006, Armitage 2007). This was emphasized by the worldwide withdrawal of cerivastatin fromthe market in August 2001 after the drug was associated with approximately 100rhabdomyolysis-related deaths. Many of these cases occurred in patients using concomitantfibrates, especially gemfibrozil, and cerivastatin, which is mainly metabolized via CYP2C8(Staffa et al. 2002). The pharmacokinetic interaction between statins and gemfibrozil leading tosubstantially elevated plasma concentrations of statins is probably due mainly to the inhibitionof the CYP2C8-mediated metabolism and OATP1B1-mediated hepatic uptake of statins by

REVIEW OF THE LITERATURE
50
gemfibrozil (Backman et al. 2002). The combination of statins with a fibrate is an attractiveoption for effective treatment of complex hyperlipidaemias since statins primarily lower plasmaLDL-C, and fibrates primarily lower plasma triglycerides and increase HDL. Gemfibrozil has agreater probability of causing myotoxicity in both monotherapy and in combination therapy withstatins compared with other fibrates, such as fenofibrate, bezafibrate and ciprofibrate, whichemploy different pathways for their elimination than statins (Graham et al. 2004, Owczarek etal. 2005, Law and Rudnicka 2006, Vaklavas et al. 2008).
Table 7. Potential factors predisposing to statin-induced myopathy.Alcohol consumptionCoadministration of interacting drugs (CYP3A4 inhibitors, fibrates, cyclosporine, amiodarone)a
DiabetesGenetic differences in drug disposition genesb
Increasing ageIncreasing statin doseFemale genderRenal insufficiencyHepatic dysfunctionHypothyroidismPerioperative periodMetabolic muscle diseasesPolymyalgia rheumaticaSteroid useStrenuous exerciseFreely adapted from Vaklavas et al. (2008) and Armitage (2007), with some additionsa CYP3A4 inhibitors: itraconazole, ketoconazole, erythromycin, clarithromycin, HIV protease inhibitors,grapefruit juice (Neuvonen et al. 2006)b e.g. SLCO1B1 c.521T>C SNP
Genetic differences in drug metabolizing enzymes or drug transporters can also predispose tostatin myotoxicity. An article published during the final preparation of this thesis associatedSLCO1B1 polymorphism with a considerably elevated risk for myopathy (SEARCHCollaborative Group 2008). In this study, two sets of patient and control groups from large trialsinvolving approximately 12 000 and 20 000 participants were treated with 80 mg and 40 mg ofsimvastatin per day, respectively. A strong association was found between myopathy and twotightly linked variants in SLCO1B1, the other one being the c.521T>C variant. The odds ratiofor myopathy was 4.5 per copy of the c.521C allele, and 16.9 in c.521CC, compared with thec.521TT homozygotes. In this large-scale study, approximately 60% of the simvastatin-inducedmyopathy cases were attributable to the c.521 variant allele. In a previous Japanese study, theSLCO1B1*15 haplotype also containing the c.521T>C SNP (c.388G-c.521G) was associatedwith pravastatin-induced myopathy (Morimoto et al. 2004, 2005).

REVIEW OF THE LITERATURE
51
Despite concerted efforts, little is known about the precise mechanisms through which statinsare transported into skeletal muscle cells and how they produce muscle injury. The inhibition ofHMG-CoA reductase by statins also reduces the production of downstream intermediatemetabolites in the cholesterol synthesis pathway, including isoprenoid cometabolites (Figure 9).This in turn may interfere with protein modification at multiple levels and affect proteinprenylation and glycosylation, leading to depletion of muscle fibres from growth signals andsusceptibility to mechanical stress (Thompson et al. 2003, Dirks and Jones 2006, Shitara andSugiyama 2006). Statin-induced myopathy may also be associated with mitochondrialdysfunction, since ubiquinone biosynthesis is interrupted (Laaksonen 2006, Littarru andLangsjoen 2007). High-dose statin therapy has been shown to lead to changes in skeletal musclesterol metabolism and to decreased mitochondrial volume and mitochondrial DNA in skeletalmuscle (Päivä et al. 2005, Schick et al. 2007).
5.4 Pharmacogenetics
Interindividual variation in the response to statins limits the beneficial effects of statin therapy.The factors influencing the statin response of a patient include diseases, concomitantmedications and adherence to treatment, physiologic condition, and genetic background (Hutzand Fiegenbaum 2008).
Several studies with controversial results have associated different polymorphisms in the genesencoding statin-metabolizing enzymes and statin transporters with altered pharmacokinetics andpharmacodynamics of statins. The CYP2C9*3 allele has been associated with increased AUC offluvastatin (Kirchheiner et al. 2003). Expression of CYP3A5 was associated with impairedcholesterol-lowering efficacy of lovastatin, simvastatin and atorvastatin, but not fluvastatin andpravastatin, in one study with 69 Caucasian patients (Kivistö et al. 2004b). The CYP3A4*1Ballele has been associated with lower posttreatment LDL levels of atorvastatin, but these resultshave not been confirmed in later studies (Kajinami et al. 2004a, Thompson et al. 2005). In alarge study with 16 candidate genes and 43 SNPs, the only significant associations withenhanced LDL reduction in atorvastatin therapy were found with the apoE2 phenotype and withthe c.2677G>T SNP in ABCB1 (Thompson et al. 2005). However, these findings were notconsidered clinically relevant. The ABCB1 c.3435C>T variant allele has also been associatedwith enhanced LDL-C reduction of atorvastatin and simvastatin (Kajinami et al. 2004b,Fiegenbaum et al. 2005). The ABCC2 c.1446C>G variant has been associated with increasedhepatic expression of MRP2 and a markedly reduced AUC of the MRP2 substrate pravastatin(Niemi et al. 2006), and the ABCG2 c.421C>A polymorphism has been associated with elevatedplasma concentrations of rosuvastatin in Chinese subjects (Zhang et al. 2006).
In previous studies, the SLCO1B1 c.521C allele has been associated with increased plasmaconcentrations of pravastatin, rosuvastatin and pitavastatin (Nishizato et al. 2003, Mwinyi et al.2004, Niemi et al. 2004, Chung et al. 2005, Lee et al. 2005a). In addition, the acute effect ofpravastatin on hepatic cholesterol synthesis was significantly reduced in carriers of the *17haplotype (g.-11187A-g.-10499A-c.388G-c.521C) (Niemi et al. 2005c), although this effect was

REVIEW OF THE LITERATURE
52
not seen in a 3-week multiple-dose pravastatin study (Igel et al. 2006). On the other hand, thec.521TC genotype has been associated with a reduced cholesterol-lowering efficacy in Japanesepatients using simvastatin, atorvastatin or pravastatin (Tachibana-Iimori et al. 2004). Moreover,the c.521T>C variant and the c.388A>G variant were associated with a slightly attenuatedresponse (1.28% ± 0.25% smaller reduction in LDL-C per c.521C allele) and a slightlyenhanced response (0.62% ± 0.18% larger reduction in LDL-C per c.388G allele) in 4–6 weeksof simvastatin therapy, respectively (Heart Protection Study Collaborative Group 2002,SEARCH Collaborative Group 2008). This is in line with studies that have associated theSLCO1B1 c.521T>C variant with decreased activity of OATP1B1 and the SLCO1B1*1Bhaplotype with increased activity of OATP1B1 (Mwinyi et al. 2004, Maeda et al. 2006a).

AIMS OF THE STUDY
53
AIMS OF THE STUDY
Several sequence variations have been discovered recently in the OATP1B1-encodingSLCO1B1 gene, some associated with altered transporter activity in vitro and in vivo. However,the frequencies of different SLCO1B1 sequence variations in individual populations have notbeen systematically investigated. Furthermore, the effects of SLCO1B1 polymorphism on thedisposition of different statins have not been compared. In addition, SLCO1B1 polymorphismmay affect cholesterol synthesis. Thus, we investigated SLCO1B1 polymorphism in Caucasians(Finnish population) and in different ethnic populations globally, and compared the effects ofSLCO1B1 polymorphism on statin pharmacokinetics and pharmacodynamics as well as oncholesterol homeostasis.
The specific aims of the study were:
1. To investigate the frequency of SLCO1B1 sequence variations in different ethnicpopulations.
2. To compare the effects of SLCO1B1 polymorphism on the pharmacokinetics offluvastatin, pravastatin, simvastatin, atorvastatin and rosuvastatin.
3. To investigate the effect of SLCO1B1 polymorphism on the short-term effects ofstatins and cholesterol homeostasis.

MATERIALS AND METHODS
54
MATERIALS AND METHODS
1. Population genetic studies (I, II)
1.1 Subjects and study design
In all, 468 healthy Finnish volunteers (223 women and 245 men) participated in Study I. Oneblood sample was obtained from each participant for DNA extraction during a time period ofapproximately 6 months. The study was fully carried out in the Department of ClinicalPharmacology, University of Helsinki.
In Study II, blood specimens from 1064 individuals belonging to 52 ethnically diversepopulations were collected by investigators of the Human Genome Diversity Project (HGDP)(Cann et al. 2002). The DNA of these samples was obtained from cultured lymphoblastoid celllines (LCLs) deposited at the Fondation Jean Dausset – Centre d’Étude du PolymorphismeHumain (CEPH), Paris, France (http://www.cephb.fr/HGDP-CEPH-Panel). From the 1064 DNAsamples obtained, duplicate pairs, close relative pairs and atypical samples were excluded(Ramachandran et al. 2005), as well as samples that were not available in our sample set. Thesamples from individuals in different populations were grouped into eight large geographicregions (Table 8): Sub-Saharan Africa, North Africa, Middle East, Central/South Asia, EastAsia, Oceania, Europe and America. This grouping followed the original CEPH documents,with the exception of dividing Asia into two regions (Rosenberg et al. 2002). Apart from thecollection of blood samples and the DNA extraction, Study II was carried out in the Departmentof Clinical Pharmacology, University of Helsinki.
1.2 Blood sampling and genomic DNA extraction
A 10-ml blood sample from each participant was collected in a tube containingethylenediaminetetraacetic acid (EDTA) and stored at -20 ºC prior to DNA extraction (Study I).Genomic DNA was extracted with standard methods (QIAamp DNA Blood Mini Kit; Qiagen,Hilden, Germany).
1.3 Genotyping
In all, 11 and 12 sequence variations were investigated in Study I and Study II, respectively(Table 9 and 10). The SNPs studied cover the entire SLCO1B1 gene, from the promoter area tothe 3’ UTR. The reference sequences were obtained from the National Center for BiotechnologyInformation (NCBI; Bethesda, MD, USA) database (http://www.ncbi.nlm.nih.gov/). Genotypingwas performed, using allelic discrimination with Taqman 5’ nuclease assays. The reactionvolume in polymerase chain reactions (PCR) was 12 µl containing assay-specific primers,allele-specific TaqMan minor groove binder (MGB) probes, TaqMan 2x Universal PCR MasterMix No AmpErase uracil-N-glycosylase (UNG) and genomic DNA. The PCR was carried out inan Applied Biosystems 7300 Real-Time PCR system or a 2720 Thermal Cycler (AppliedBiosystems, Foster City, CA, USA). Pre- and post-PCR fluorescence measurements and

MATERIALS AND METHODS
55
genotype calls were performed with the 7300 Real-Time PCR System. Genotyping forc.571T>C, c.597C>T and c.*439T>G were performed with Validated TaqMan GenotypingAssays, and genotyping for c.1086C>T and c.1463G>C were performed with the TaqMan DMEassays. All of these assays were purchased from Applied Biosystems. The genotyping assays,except for c.*439T>G, c.1086C>T and c.1463G>C which had been validated by AppliedBiosystems, were validated by genotyping 41 previously sequenced samples (Niemi et al. 2004).The genotyping accuracy was 100% for all SNPs.
Table 8. Subjects in the global population genetic study.Population (country) n Population (country) nSub-Saharan Africa Central/South Asia
Biaka Pygmies (Central African Republic) 23 Brahui (Pakistan) 25Mbuti Pygmies (Congo) 13 Balochi (Pakistan) 24Mandenka (Senegal) 22 Hazara (Pakistan) 22Yoruba (Nigeria) 22 Makrani (Pakistan) 25Bantu (Kenya) 11 Sindhi (Pakistan) 24San (Namibia) 6 Pathan (Pakistan) 24Bantu (South Africa) 8 Kalash (Pakistan) 23Total 105 Burusho (Pakistan) 25
North Africa Total 192Mozabite (Algeria) 29 Oceania
Middle East Papuan (New Guinea) 17Bedouin (Israel) 46 NAN Melanesian (New Guinea) 11Druze (Israel) 42 Total 28Palestinian (Israel) 45 EuropeTotal 133 French (France) 23
East Asia French Basque (France) 22Han (China) 44 Sardinian (Italy) 28Tujia (China) 10 North Italian (Italy) 13Yizu (China) 10 Tuscan (Italy) 8Miaozu (China) 10 Orcadian (Orkney Islands) 15Oroqen (China) 9 Adygei (Russia Caucasus) 17Daur (China) 10 Russian (Russia) 25Mongola (China) 10 Total 151Hezhen (China) 9 AmericaXibo (China) 9 Pima (Mexico) 14Uygura (China) 10 Maya (Mexico) 21Dai (China) 10 Colombian (Colombia) 7Lahu (China) 8 Karitiana (Brazil) 14She (China) 10 Surui (Brazil) 8Naxi (China) 9 Total 64Tu (China) 10Yakut (Siberia) 25 Total 941Japanese (Japan) 27Cambodian (Cambodia) 9Total 239
NAN, Non-Austronesian; a In some analyses, the Uygur population from China (East Asia) was analysed togetherwith the populations from Central/South Asia.

MATERIALS AND METHODS
56
Table 9. PCR conditions.Study I Initial Steps PCR (each of 40 cycles)
AmpliTaq Gold DNA Polymerase activation Melting Annealing/Extending95 ºC for 10 min 92 ºC for 15 s 60 ºC for 1 min
Study II Initial Steps PCR (each of 50 cycles)AmpliTaq Gold DNA Polymerase activation Melting Annealing/Extending95 ºC for 10 min 92 ºC for 15 s 60 ºC for 90 s
1.4 Population genetics and statistical analyses
The SNP and haplotype frequencies are given with 95% confidence intervals (CI). Arlequinsoftware version 2.000 (University of Geneva, Switzerland; http://lgb.unige.ch/arlequin) wasused to evaluate the SNP and genotype frequencies for consistency with the Hardy-Weinbergequilibrium. The significance of departure from the Hardy-Weinberg equilibrium was testedusing the procedure described by Guo and Thompson (1992), with a test analogous to the Fisherexact test on a 2 x 2 contingency table, but extended to a triangular contingency table ofarbitrary size. The test was done using a modified version of the Markov-chain random walkalgorithm. The LD for each pair of SNPs within each geographical region and in the Finnishpopulation was quantified by the correlation r2 and D’ values calculated with the programLinkage Disequilibrium Analyzer 1.0 (Beijing, China; http://www.chgb.org.cn/lda/lda.htm).Small populations (North Africa and Oceania) were excluded from the LD analysis. Thehaplotypes were statistically inferred with the software PHASE version 2.1.1, using analgorithm based on Bayesian inference (Stephens et al. 2001, Stephens and Donnelly 2003). Tofacilitate the comparison of frequencies of functionally significant haplotypes, a haplotypeanalysis with only the c.521T>C and c.388A>G SNPs was also carried out in Study II.
In Study II, genetic diversity was quantified at three levels: between members of the samepopulation, between populations within the same region and between geographical regions, byanalysis of molecular variance (AMOVA), using Arlequin software version 3.11 (Excoffier etal. 1992). Correlation of the SNP and haplotype frequencies with the latitude in the NorthernHemisphere was investigated with Pearson correlation coefficients using SPSS software 13.0(SPSS Inc., Chicago, IL, USA). Prior to analysis, the allele and haplotype frequencies werechanged into the form arcsin( p), where p is the frequency (angular transformation). Matrices ofgeographic (great circle) distances and genetic distances were calculated between all pairs ofpopulations. The likely routes of human migration out of Africa via five waypoints were used inestimating the geographic distances to make the distance estimates more reflective of humanmigration patterns. These waypoints were: Anadyr, Russia (64ºN, 177ºE); Cairo, Egypt (30ºN,31ºE); Istanbul, Turkey (41ºN, 28ºE); Phnom Penh, Cambodia (11ºN, 104ºE); and PrinceRupert, Canada (54ºN, 130ºW) (Ramachandran et al. 2005). The genetic distances wereestimated as pairwise fixation index (FST) values. Correlation of Slatkin’s linearized FST valueswith the great circle distances, using waypoints, was investigated with a Mantel test of matrixcorrelation. P values below 0.05 were considered statistically significant.

Table 10. SLCO1B1 SNPs investigated in population genetic studies.Location SNP dbSNP ID Amino acid Study
IStudy
IIPrimersa TaqMan MGB probes
Promoter g.-11187G>A rs4149015 X X 5’-CATATATGCATCCTCACATTACCACAT-3’
5’-AATAAAGTACAGACCCTTCTCTCACATAAA-3’
VIC-TGTATACAGGTAAAAGTG
FAM-TGTGTATACAAGTAAAAG
Promoter g.-11110T>G X 5’-CTCATATATGCATCCTCACATTACCACAT-3’
5’-GAAATAAAGTACAGACCCTTCTCTCACA-3’
VIC-ACACTTTTCTGAAATATATATAT
FAM-ACTTTTCTGAAATAGATATAT
Promoter g.-10499A>C rs59710386 X X 5’-TGTTAAGATTAACAAAAAATAATGTGAGAATTCTGAGAAAT-3’
5’-ATGTCATTGCTCTAGTCAAACATATAAAACCT-3’
VIC-TCACTCCAGTTGCCAAT
FAM-ACTCCAGGTGCCAAT
Exon 4 c.388A>G rs2306283 Asn130Asp X X 5’-TTTAATTCAGTGATGTTCTTACAGTTACAGGT-3’
5’-GAGTGATAAAATTTGATTAATTAAACAAGTGGATAAGGT-3’
VIC-CTAAAGAAACTAATATCAATTCAT
FAM-AAAGAAACTAATATCGATTCAT
Exon 4 c.411G>A rs11045818 Ser137Ser X X 5’-CAGTGATGTTCTTACAGTTACAGGTATTCT-3’
5’-GTCAATATTAATTCTTACCTTTTCCCACTATCTCA-3’
VIC-AATTCAACATCGACCTTAT
FAM-AAATTCAACATCAACCTTAT
Exon 4 c.463C>A rs11045819 Pro155Thr X X 5’-CAGTGATGTTCTTACAGTTACAGGTATTCTAA-3’
5’-GAAGACTTTTTACTGTCAATATTAATTCTTACCTTTTCC-3’
VIC-ACTATCTCAGGTGATGCT
FAM-CACTATCTCAGTTGATGCT
Exon 5 c.521T>C rs4149056 Val174Ala X X 5’-GAAACACTCTCTTATCTACATAGGTTGTTTA-3’
5’-CCCCTATTCCACGAAGCAT-3’
VIC-TACCCATGAACACATATA
FAM-TACCCATGAACGCATATA
Exon 5 c.571T>C rs4149057 Leu191Leu X X C_1901691_10b
Exon 5 c.597C>T rs2291075 Phe199Phe X X C_1901690_1b
Exon 8 c.1086C>T rs57040246 Tyr362Tyr X C_25605972_20b
Exon 10 c.1463G>C rs59502379 Gly488Ala X C_30633910_10b
Exon 14 c.1929A>C rs34671512 Leu643Phe X X 5’-GGGCTTGTCTTCAATGTTAAGAGTCT-3’
5’-GACACTTCCATTTTCTGATGCATTGATAT-3’
VIC-TTCATGGCATAAATTAATATA
FAM-ATGGCATAAATGAATATA
3’UTR c.*439T>G rs4149087 X X C_1901734_10b
The positions of the SNPs are given in relation to the NCBI reference sequences NM_006446.2 (coding DNA; c.) and NC_000012.9 (genomic; g.) with the firstnucleotide of the ATG first codon set to 1 and the nucleotide 5’ of ATG set to -1. The position of c.*439T>G is given with the first nucleotide 3’ of the stop codon(TAA) set to *1.dbSNP ID, NCBI single nucleotide polymorphism database identity; MGB, minor groove bindera Upper line, forward primer; lower line, reverse primerb Assay ID for validated TaqMan genotyping assays

MATERIALS AND METHODS
58
2. Pharmacokinetic and pharmacodynamic studies (III–VI)
2.1 Subjects
A total of 32 (14 female and 18 male) healthy volunteers participated in Studies III-VI (Table11). The subjects were recruited from a pool of over 300 healthy genotyped subjects and wereselected based on the SLCO1B1 c.521T>C SNP as well as the g.-11187G>A, g.-10499A>C andc.388A>G SNPs. The subjects were allocated into one of three groups according to thegenotype: the c.521CC group comprised four subjects, the c.521TC group comprised 12subjects and the c.521TT (control group) comprised 16 subjects. The participants wereascertained to be healthy by medical history, physical examination and routine laboratory testsbefore entering the study. One subject (in the control group) was a tobacco smoker, and noneused any continuous medication, including oral contraceptives. The use of other drugs wasprohibited for 1 week and the use of grapefruit products was prohibited for 3 days before eachstudy day. Participation in any other trial and blood donation within 4 weeks before and after thestudy were also prohibited.
2.1.1 Genotyping
The subjects were genotyped for SLCO1B1 SNPs as described previously (see Materials andMethods, section 1.3). In addition, the participants were genotyped for the CYP3A5*3(g.6986A>G) and the ABCC2 c.1446C>G alleles (Kivistö et al. 2004b, Niemi et al. 2006), asdescribed previously. Genotyping for the CYP2C9*3 (c.1075A>C) allele was carried out withTaqMan Pre-Developed Assay Reagents for Allelic Discrimination (Applied Biosystems) usingthe 7300 Real-Time PCR system according to the manufacturer’s instructions. Only subjectswith the CYP3A5 nonexpressor genotype (CYP3A5*3/*3), CYP2C9 c.1075AA referencegenotype and ABCC2 c.1446CC reference genotype were recruited.
2.2 Study design
Studies III–VI were prospective genotype panel investigations with a crossover design and fivephases (1–5) and were carried out in the Department of Clinical Pharmacology, University ofHelsinki. Following an 8-hour overnight fast, the subjects ingested a single oral dose offluvastatin, pravastatin, simvastatin, rosuvastatin or atorvastatin with 150 ml water at 08:00hours (Table 12). A standardized warm meal was served 4 hours after statin ingestion and astandardized light meal after 7 and 10 hours. During the study days, the subjects were underdirect medical supervision. There was a washout period of at least 1 week between each phase.Food intake was identical in the different study phases.

MATERIALS AND METHODS
59
Table 11. Characteristics of the subjects in pharmacokinetic and pharmacodynamic studies.
SLCO1B1 genotypea SubjectNo. Sex Age
(years)Height(cm)
Weight(kg)
BMI(kg/m2)
c.521CC (*16/*17) 1 m 22 185 92 26.9c.521CC (*16/*17) 2 f 21 170 74 25.6c.521CC (*16/*16) 3 m 25 187 90 25.7c.521CC (*16/*16) 4 m 24 178 80 25.3Mean SD 23 2 180 8 84 8 25.9 0.7c.521TC (*1A/*17) 5 m 29 181 77 23.5c.521TC (*1A/*17) 6 f 21 160 53 20.7c.521TC (*1B/*17) 7 m 21 187 71 20.3c.521TC (*1A/*17) 8 f 21 172 66 22.3c.521TC (*1B/*16) 9 f 20 160 65 25.4c.521TC (*1A/*16) 10 m 27 173 82 27.4c.521TC (*1B/*16) 11 f 34 167 61 21.9c.521TC (*1A/*16) 12 m 21 178 70 22.1c.521TC (*1B/*15) 13 f 21 175 65 21.2c.521TC (*1A/*15) 14 m 24 188 73 20.7c.521TC (*1B/*15) 15 m 23 175 75 24.5c.521TC (*1A/*15) 16 m 20 175 75 24.5Mean SD 24 4 174 9 69 8 22.9 2.2c.521TT (*1A/*1A) 17 f 22 172 68 23.0c.521TT (*1A/*1A) 18 f 21 175 67 21.9c.521TT (*1A/*1A) 19 f 21 165 54 19.8c.521TT (*1A/*1A) 20 m 22 181 83 25.3c.521TT (*1A/*1A) 21 f 20 165 70 25.7c.521TT (*1A/*1A) 22 m 24 184 78 23.0c.521TT (*1A/*1A) 23 m 22 182 65 19.6c.521TT (*1A/*1A) 24 f 22 165 63 23.1c.521TT (*1A/*1A) 25 m 24 172 58 19.6c.521TT (*1A/*1A) 26 f 21 172 57 19.3c.521TT (*1A/*1A) 27 f 27 170 60 20.8c.521TT (*1A/*1A) 28b m 25 177 85 27.1c.521TT (*1A/*1A) 29 m 22 180 83 25.6c.521TT (*1A/*1A) 30 f 28 154 56 23.6c.521TT (*1A/*1A) 31 m 19 182 68 20.5c.521TT (*1A/*1A) 32 m 21 186 80 23.1Mean SD 23 2 174 9 68 10 22.6 2.5BMI, body mass index; f, female; m, male; SD, standard deviationa The predicted diplotype based on the g.-11187G>A, g.-10049A>C, c.388A>G, and c.521T>C SNPs isgiven in parenthesis.b This subject was a tobacco smoker.

MATERIALS AND METHODS
60
Table 12. Details of the drugs used in the studies.Phase Statin Dose Medicinal
productManufacturer
1 Fluvastatin 40 mg Canef tablet AstraZeneca AB, Södertälje, Sweden2 Pravastatin 40 mg Pravachol tablet Bristol-Myers Squibb, Epernon, France3 Simvastatin 40 mg Zocor tablet Merck Sharp & Dohme, Haarlem, The Netherlands4 Rosuvastatin 10 mg Crestor tablet AstraZeneca AB, Södertälje, Sweden5 Atorvastatin 20 mg Lipitor tablet Pfizer, Freiburg, Germany
2.3 Blood sampling
A forearm vein of each subject was cannulated for blood sampling on the study days and thetimed blood samples (5–10 ml each) were collected prior to and at 0.5, 1, 1.5, 2, 3, 4, 5, 7, 9 and12 hours (phases 1–3) after administration of statin. In phases 4 and 5, similar blood sampleswere drawn before and 0.5, 1, 2, 3, 4, 5, 7, 9, 12, 24, 34 and 48 hours after statin administration.In all phases, the venous samples were taken into tubes containing EDTA and placedimmediately on ice after sampling. The plasma was separated by centrifugation within 30minutes after blood sampling and stored at -70 °C until analysis.
2.4 Quantification of plasma statins
Plasma fluvastatin, pravastatin, simvastatin, atorvastatin and rosuvastatin concentrations werequantified by the use of liquid chromatography-tandem mass spectrometry (LC-MS-MS) (Table13). The systems used were the SCIEX Q-Trap mass spectrometer (Sciex Division of MDS Inc,Foster City, CA, USA) for fluvastatin, rosuvastatin, atorvastatin and atorvastatin metabolites,and PE SCIEX API 3000 mass spectrometer (Sciex Division of MDS Inc, Toronto, Ontario,Canada) for pravastatin, simvastatin and simvastatin acid. No authentic reference compoundswere available for atorvastatin lactone, 2-hydroxy atorvastatin acid and 2-hydroxy atorvastatinlactone, and their concentrations are given in arbitrary units (u/ml) relative to the ratio of thepeak height of each metabolite to that of the internal standard in the chromatogram.
Table 13. Summary of the quantification methods.Phase Analytes quantified LC-MS-MS system used Limit of quantification Interday CV a
1 Fluvastatin SCIEX Q-Trap 0.5 ng/ml < 13%2 Pravastatin PE SCIEX API 3000 0.1 ng/ml < 9%3 Simvastatin PE SCIEX API 3000 0.05 ng/ml < 6%
Simvastatin acid PE SCIEX API 3000 0.1 ng/ml < 10%4 Rosuvastatin SCIEX Q-Trap 0.25 ng/ml < 15%5 Atorvastatin SCIEX Q-Trap 0.1 ng/ml < 11%
a Interday coefficient of variation (CV) was determined for different concentrations in the relevant concentrationrange; the highest of these values is presented.

MATERIALS AND METHODS
61
2.5 Quantification of plasma sterols
The plasma cholesterol and noncholesterol sterol concentrations were measured by gas-liquidchromatography (GLC). For this purpose, 0.2 ml of plasma was saponified using 5 -cholestaneas an internal standard. The extracted sterols were analysed as trimethyl silyl derivatives withGLC on a 50-m capillary column (Ultra 2, 5890, Hewlett Packard, Wilmington, DE, USA). Thenoncholesterol sterol concentrations were adjusted for plasma total cholesterol analysed in thesame GLC run and are expressed as absolute concentrations (µg/100 ml) and as ratios tocholesterol (µg/100 mg cholesterol). The lower limit of quantification for sterols was 5 µg/100ml. The coefficients of variation (CVs) for the various sterols at relevant concentrations were:cholesterol 3.2%, cholestanol 2.7%, desmosterol 6.0%, lathosterol 3.7%, campesterol 1.8% andsitosterol 2.4% (n = 24).
2.6 Pharmacokinetic calculations
The pharmacokinetics of the statins studied and their metabolites, if applicable, werecharacterized by peak concentration (Cmax), time to peak concentration (tmax), t½, AUC from 0 toinfinity (AUC0- ) and to the last point of measurement (AUC0-t). The Cmax and tmax values weretaken directly from the original data. The terminal log-linear part of each concentration-timecurve was identified visually, and the elimination rate constant (ke) was determined from ln-transformed data with linear regression analysis. The t½ was calculated by the equation t½ =ln2/ke. The AUC values were calculated by a combination of the linear and log-lineartrapezoidal rules, with extrapolation to infinity, when appropriate, by division of the lastmeasured concentration by ke.
2.7 Pharmacodynamic variables
Desmosterol, lathosterol and squalene were used to assess the cholesterol synthesis rate andcholestanol, campesterol, sitosterol and avenasterol were used to assess the cholesterolabsorption rate. Baseline (fasting) values of plasma cholesterol and the above-mentionednoncholesterol sterols and their ratios to cholesterol were used to characterize differencesbetween the genotype groups in cholesterol homeostasis.
The statin response was determined by changes in the noncholesterol sterol to cholesterol ratiosafter statin intake. Incremental net areas under the plasma sterol to cholesterol ratio versus thetime curve were calculated from 0 hours to 12 hours (AUC0-12) with the linear trapezoidal rule.The mean percentage changes from baseline were obtained by dividing the incremental net areaby 12 hours and expressing this value as a percentage of the respective baseline value. Inaddition, the percentages of maximum decreases from the respective baseline values in theplasma sterol to cholesterol ratio were determined.

MATERIALS AND METHODS
62
2.8 Statistical analysis
The data were analysed with the statistical program SPSS 11.0 for Windows (SPSS Inc.). Thedifferences were considered statistically significant at a P value of less than 0.05. Statisticalcomparisons of the pharmacokinetic variables of statins, and their metabolites if applicable,between subjects with the SLCO1B1 c.521TT, c.521TC, and c.521CC genotypes and betweenthe sexes were done using analysis of variance (ANOVA) and pairwise testing with the Tukeytest. Homogeneity of variance was tested using Levene’s Test of Equality. Compatibility of theresiduals with the normal distribution was assessed with the Shapiro-Wilk test. In case ofunequal variances or unsatisfactory distribution of the residuals, pairwise testing was performedwith the Games-Howell test, or the data were logarithmically transformed before analysis oranalysed, as were the tmax data, using the Kruskal-Wallis test with a posteriori pairwise testingby the Mann-Whitney U test with Bonferroni correction, as appropriate. Differences in theeffect of SLCO1B1 polymorphism on the AUC0-48 of atorvastatin and rosuvastatin were testedwith the paired t-test. The possible contributions of subject characteristics (sex, weight andBMI) to variability in the AUC0- of pravastatin and fluvastatin were investigated using aforward stepwise multiple linear regression analysis. A P value threshold of 0.05 was used forentering and removing independent variables from the model.
The results of Study VI are expressed as mean values and estimated marginal mean values with95% CIs. Comparisons of the cholesterol and non-cholesterol sterol variables were done usingANOVA for repeated measurements, with study phase as a intrasubject factor and the SLCO1B1genotype as a intersubject factor. When the ANOVA P value was below 0.05, pairwisecomparisons between genotypes were performed using a Dunnet’s t-test, adjusting for multipletesting, with the c.521TT group used as a control.
3. Ethical considerations
All participants (I, III–VI) received both oral and written information and gave written informedconsent before entering the studies. In Study II, the LCLs were freely donated under conditionsof informed consent and confidentiality was ensured by CEPH by reviewing consent forms,institutional review board approvals or detailed reports from the investigators who organized thecollection of the samples. Only samples for which sufficient evidence was found of informedconsent were included in the panel. Information on each LCL was limited to sex, population andgeographic origin of the individual (Cann et al. 2002). The studies were approved by theCoordinating Ethics Committee of the Helsinki and Uusimaa Hospital District (I, II) or by theCoordinating Ethics Committee of the Helsinki and Uusimaa Hospital District and the NationalAgency for Medicines (III–VI).

RESULTS
63
RESULTS
1. SLCO1B1 allele frequencies
1.1 Finnish population (I)
All SNPs, except the g.-11110T>G and c.1929A>C, occurred at allele frequencies higher than5%. The frequency of c.521T>C SNP was 20.2% (95% CI, 18–23%) and the frequency of thec.388A>G SNP was 46.2% (95% CI, 43–49%) (Table 14). In the Finnish population, thec.521CC genotype occurred with a frequency of 4.3% (95% CI, 2.8–6.5%). The three promoterSNPs g.-11187G>A, g.-11110T>G and g.-10499A>C were relatively rare in the Finnishpopulation; they occurred at frequencies of less than 10% each. The observed genotypefrequencies were in the Hardy-Weinberg equilibrium.
The variants c.411G>A and c.463C>A were in perfect LD, with an r2 value of 1.00. Thec.521T>C SNP showed the strongest correlation with the g.-10499A>C SNP (r2 = 0.33, D’ =0.98). The most common haplotype contained the variant allele C at position c.571 and had thereference nucleotide at all other positions. The c.521T>C SNP was found in four majorhaplotypes: *5, *15, *16 and *17, which occurred at frequencies of 2.7% (95% CI, 1.8–3.9%),2.4% (95% CI, 1.6–3.5%), 7.9% (95% CI, 6.3–9.8%) and 6.9% (95% CI, 5.5–8.8%),respectively.
1.2 Global analysis (II)
Large differences in allele frequencies existed between different populations (Table 14). Thehighest frequencies of the c.521T>C SNP were found in America (24%; 95% CI, 18–32%),Middle East (20%; 95% CI, 15–25%) and Europe (18%; 95% CI, 14–23%); the smallestfrequency of c.521T>C was found in Sub-Saharan Africa (1.9%; 95% CI, 0.7–4.8%). Thefrequency of c.521T>C was 12% (95% CI, 9.5–15%) in East Asia and 9.4% (95% CI, 6.9–13%)in Central/South Asia. No carriers of the c.521T>C SNP were found in Oceania. The frequencyof the homozygous variant c.521CC genotype was around 1.3% (95% CI, 0.4–4.7%) inEuropeans (Caucasians). Three population-specific SNPs were found, namely g.-10499A>C(Europe), c.1086C>T (Sub-Saharan Africa) and c.1463G>C (Sub-Saharan Africa). Thefrequency of c.388A>G was over 40% in all populations, with the highest frequency found inSub-Saharan Africa (79%; 95% CI, 74–84%). The African continent showed the highestdiversity, since all investigated SNPs were found there.
The LD was generally strong in all populations, suggesting that intralocus recombination hasplayed only a minor role in shaping SLCO1B1 variation. The largest number of haplotypes wasfound in South/Central Asia (28 different haplotypes). In the present study, the most commonhaplotype was that containing the c.571C allele and the reference nucleotide at other positions.The second most common haplotype contained the G allele at position c.388 and at positionc.*439, and the reference nucleotide at other positions. These two most common haplotypes

RESULTS
64
were found in all regions and accounted for 42% of all chromosomes. The frequencies of theSLCO1B1 haplotypes *1A, *1B, *5 and *15 varied considerably among geographical regions(Figure 11). The *5 was found only in North Africa, Europe and the Middle East. The *1B wasmore frequent than the reference haplotype *1A in North Africa, East Asia, Sub-Saharan Africa,Oceania and America.
The differences between regions accounted for 8.5% of the total molecular variance (AMOVA).This is consistent with estimates based on neutral markers. Sub-Saharan Africa and Oceaniashowed the highest variance among populations (6.3% and 7.7%, respectively). In general, thevariance within populations considerably exceeded the variance between populations.
The frequency of the SLCO1B1 c.521C allele and the *15 haplotype correlated positively withlatitude in the Northern Hemisphere (r = 0.525, P < 0.001 and r = 0.510, P < 0.001,respectively). In contrast, the frequency of the high-activity haplotype *1B showed a negativecorrelation with northern latitude (r = -0.405, P = 0.006). There was also a tendency towards anegative correlation in the c.388A>G variant allele frequency (r = -0.249, P = 0.099). Thenormalized SLCO1B1 genetic distances correlated significantly with geographic great circledistances between populations (r = 0.235, P = 0.001).

Table 14. Allelic frequencies (%) of SLCO1B1 variants in different populations.
Ethnic group n g.-1
1187
G>
A
g.-1
1110
T>G
g.-1
0499
A>C
c.38
8A>
G
c.41
1G>
A
c.46
3C>
A
c.52
1T>
C
c.57
1T>
C
c.59
7C>
T
c.10
86C
>T
c.14
63G
>C
c.19
29A>
C
c.*4
39T>
G
ReferenceFinnish Caucasian 468 9.7 0.4 8.0 46 13 13 20 53 46 0.0a 0.0a 4.0 49 ICaucasian (European) 151 6.6 - 4.3 41 16 17 18 61 42 0.0 0.0 5.0 30 IICaucasian 423 - - - 37 - - 15 - - - - - - Mwinyi et al. 2004German Caucasian 300 - - - 37 16 16 15 35 38 - 0.0 3.1b - Mwinyi et al. 2008Caucasian living in Singapore 36 - - - 51 - - 22 - - - - - - Lee et al. 2005aNative American 64 0.8 - 0.0 63 1.6 1.6 24 33 28 1.0 0.5 0.0 41 IIEuropean American 49 - - - 30 18 16 14 54 - - 0.0 - - Tirona et al. 2001African American 22 - - - 75 41 2.3 2.3 4.5 - - 9 - - Tirona et al. 2001Sub-Saharan African 105 0.5 - 0.0 79 1.0 4.8 1.9 13 50 7.1 3.3 10 76 IINorth African (Algerian) 29 10 - 3.5 64 3.5 3.5 17 21 59 1.7 0.0 16 72 IIAfrican (Ugandan) 115 - - - 78 0.0 2.2 3.9 6.1 0.0 - 1.7 7.3b - Mwinyi et al. 2008Japanese 27 17 - 0.0 74 0.0 0.0 19 26 39 0.0 0.0 0.0 19 IIJapanese 267 - - - 64 - - 11 - - - - - - Nozawa et al. 2002Japanese 120 - - - 63 - - 16 36 43 - - - - Nishizato et al. 2003Korean 22 - - - 75 - - 25 - - - - - - Chung et al. 2005Chinese 178 13 - 0.0 73 0.3 0.6 11 27 42 0.0 0.0 0.6 27 IIChinese 35 - - - 67 - - 8.6 - - - - - - Lee et al. 2005aChinese 100 13 0.0 - 80 0.0 0.0 13 26 50 0.0 - - - Jada et al. 2007Malay 35 - - - 83 - - 13 - - - - - - Lee et al. 2005aMalay 100 7 0.0 - 87 2.5 2.5 11 24 50 0.0 - - - Jada et al. 2007Asian-Indian 35 - - - 60 - - 7.1 - - - - - - Lee et al. 2005aIndian 100 5 0.0 - 57 1.5 1.5 6.5 44 22 0.0 - - - Jada et al. 2007Turkish 94 - - - 46 14 14 12 38 36 - 0.0 5.1b - Mwinyi et al. 2008Pakistani 192 6.3 - 0.3 47 7.0 7.3 9.4 56 26 0.0 0.5 5.5 59 IIIsraeli 133 7.5 - 0.4 46 15 15 20 56 45 0.0 0.0 3.4 55 IIOceanian 28 8.9 - 0.0 66 0.0 0.0 0.0 48 52 3.6 0.0 0.0 30 IIa Frequencies determined for a reduced number of Finnish subjects: n = 193 (previously unpublished data)b Frequencies determined for a reduced number of subjects. German: n = 276, African: n = 109, Turkish: n = 78

Figure 11. Distribution of the SLCO1B1 haplotypes.

RESULTS
67
2. Effect of SLCO1B1 polymorphism on statin pharmacokinetics
2.1 Fluvastatin (III)
The SLCO1B1 genotype was not significantly associated with the pharmacokinetics offluvastatin. In subjects with the c.521CC genotype, the AUC0- of fluvastatin was approximately19% larger than that in subjects with the c.521TT genotype, but the difference was notstatistically significant (Figure 12). No subject characteristic, including sex, was associated withfluvastatin pharmacokinetics.
2.2 Pravastatin (III)
The SLCO1B1 genotype was significantly associated with the pharmacokinetics of pravastatin.In subjects with the homozygous variant c.521CC genotype, the mean Cmax and AUC0- ofpravastatin were 107% (P = 0.009) and 91% (P = 0.018) larger than those in subjects with thereference c.521TT genotype and 92% (P = 0.021) and 74% (P = 0.044) larger than those insubjects with the heterozygous variant c.521TC genotype (Figure 12). The Cmax and AUC0- ofpravastatin varied 19-fold and 11-fold between individual subjects. The SLCO1B1 genotype wasnot associated with differences in the tmax or t½ of pravastatin.
The effect of the genotype was greater in men than in women. In men with the c.521CCgenotype, the mean Cmax and AUC0- of pravastatin were 275% (P = 0.001) and 232% (P =0.002) larger than those in men with the c.521TT genotype and 120% (P = 0.026) and 102% (P= 0.040) larger than those in men with the c.521TC genotype. The Cmax and AUC0- ofpravastatin were generally similar among women with different SLCO1B1 genotypes. Womenwith the c.521TT genotype had a 147% larger mean Cmax (P = 0.028) and a 124% larger meanAUC0- (P = 0.034) than those in men with the c.521TT genotype. No subject characteristicother than sex was significantly associated with the pharmacokinetics of pravastatin andadjusting the variables by subject weight or lean body weight only slightly changed the resultsbut did not affect the statistical significance. No statistically significant differences were seen inthe pharmacokinetic variables of pravastatin between the c.521TC heterozygous subjects withdifferent SLCO1B1 haplotypes (*15, *16 and *17).
2.3 Simvastatin (IV)
The SLCO1B1 genotype was significantly associated with the pharmacokinetics of simvastatinacid, but not with the pharmacokinetics of the parent simvastatin lactone. In subjects with thevariant c.521CC genotype, the mean Cmax and AUC0- of simvastatin acid were 200% (P <0.001) and 221% (P < 0.001) larger than those in subjects with the reference c.521TT genotypeand 162% (P < 0.001) and 120% (P < 0.001) larger than those in subjects with the heterozygousvariant c.521TC genotype (Figure 12). In addition, the tmax of simvastatin acid was significantlyshorter in participants with the c.521CC genotype than in those with the c.521TC or c.521TT

RESULTS
68
genotypes (P < 0.05); no significant effect of the SLCO1B1 genotype was seen on t½. The Cmax
and AUC0- of simvastatin acid varied 25-fold and 16-fold between individual subjects. Oneparticipant with the c.521TC genotype was excluded from statistical analysis as an outlier,because the simvastatin acid Cmax and AUC0- values were more than 3 standard deviations(SDs) above the respective mean values. No statistically significant differences were seen in thepharmacokinetic variables of simvastatin or simvastatin acid between the c.521TC heterozygoussubjects with different SLCO1B1 haplotypes (*15, *16 and *17).
2.4 Rosuvastatin (V)
The SLCO1B1 genotype was significantly associated with the pharmacokinetics of rosuvastatin.In subjects with the variant c.521CC genotype, the mean Cmax and AUC0-48 of rosuvastatin were79% (P = 0.003) and 65% (P = 0.002) larger than those in subjects with the reference c.521TTgenotype (Figure 12). The mean Cmax and AUC0-48 were 52% and 58% larger in c.521CCsubjects than those in subjects with the heterozygous c.521TC genotype, but the differenceswere not statistically significant (P = 0.062 and P = 0.053, respectively). The Cmax and AUC0-48
of rosuvastatin varied 20-fold and 12-fold between individual subjects. The SLCO1B1 genotypewas not associated with differences in the tmax or t½ of rosuvastatin. No statistically significantdifferences were seen in the pharmacokinetic variables of rosuvastatin between the c.521TCheterozygous subjects with different SLCO1B1 haplotypes (*15, *16 and *17).
2.5 Atorvastatin (V)
The SLCO1B1 genotype was significantly associated with the pharmacokinetics of atorvastatin.In subjects with the variant c.521CC genotype, the mean AUC0-48 of the parent atorvastatin(acid) was 144% (P < 0.001) larger than that in subjects with the reference c.521TT genotypeand 61% larger (P = 0.049) than that in subjects with the heterozygous c.521TC genotype(Figure 12). The Cmax and AUC0-48 of atorvastatin varied 17-fold and 7-fold between individualsubjects. No statistically significant differences were seen in the pharmacokinetic variables ofatorvastatin between the c.521TC heterozygous subjects with different SLCO1B1 haplotypes(*15, *16 and *17). The SLCO1B1 genotype was not associated with differences in the Cmax,tmax or t½ of atorvastatin.
The mean AUC0-48 of 2-hydroxyatorvastatin (acid) was 100% larger in subjects with thec.521CC genotype than that in subjectes with the c.521TT genotype (P = 0.018). The SLCO1B1genotype was not associated with differences in the Cmax, tmax or t½ of 2-hydroxyatorvastatin.
The mean plasma concentrations of atorvastatin lactone and 2-hydroxyatorvastatin lactone werelower in subjects with the c.521TT genotype than those in subjects with the c.521CC genotype,but the effect of the SLCO1B1 genotype was not statistically significant on any of thepharmacokinetic variables.

RESULTS
69
Figure 12. Effect of SLCO1B1 genotype on the AUC0- , Cmax and t½ of fluvastatin, pravastatin,simvastatin, rosuvastatin and atorvastatin. Bars represent geometric mean ratios and thewhiskers represent 95% confidence intervals.

RESULTS
70
3. Effect of SLCO1B1 polymorphism on statin pharmacodynamics (VI)
No significant differences were seen between the SLCO1B1 genotype groups in the response toa single dose of any investigated statin. Among cholesterol synthesis markers, the greatestresponse after statin intake was seen in the lathosterol to cholesterol ratio, which was decreasedby all statins compared with the baseline value. The desmosterol to cholesterol ratio decreasedonly to a limited extent after statin ingestion. The maximum percentage decrease (0–12 hours)in the desmosterol to cholesterol ratio throughout the study population ranged from a mean of7.5% ± 3.5% (fluvastatin) to 11.6% ± 4.3% (atorvastatin) and there were no significantdifferences between the genotype groups.
Among cholesterol absorption markers, the greatest response after statin intake was seen in theavenasterol to cholesterol ratio. All statins decreased the avenasterol to cholesterol ratiocompared with the baseline value. Even though there was a trend towards a larger decrease inthe avenasterol ratio in the variant c.521CC subjects, the difference between the genotypes wasnot significant.
4. Effect of SLCO1B1 polymorphism on cholesterol homeostasis (VI)
The SLCO1B1 genotype had no significant effect on the fasting plasma total cholesterolconcentrations. The mean total cholesterol concentration was 148.4 mg/100 ml (95% CI, 136.8–159.9 mg/100 ml), 161.0 mg/100 ml (95% CI, 147.7–174.4 mg/100 ml) and 164.0 mg/100 ml(95% CI, 140.9–187.1 mg/100 ml) in subjects with the c.521TT, c.521TC and c.521CCgenotype, respectively (P = 0.256).
The mean fasting desmosterol to cholesterol ratio was 40% higher (P = 0.022) or 45% higher (P= 0.018) in subjects with the homozygous c.521CC variant genotype than in those with thec.521TT or c.521TC genotypes, respectively. The difference in desmosterol to cholesterol ratiobetween genotype groups was consistently seen during all five study phases. In addition, theplasma concentrations of desmosterol were higher in the c.521CC group than in the controlgroup (P = 0.051): the mean desmosterol concentration was 141.5 µg/100 ml (95% CI, 108.3–174.6 µg/100 ml), 148.4 µg/100 ml (95% CI, 110.1–186.7 µg/100 ml) and 233.0 µg/100 ml(95% CI, 166.7–299.3 µg/100 ml) in subjects with the c.521TT, c.521TC and c.521CCgenotypes, respectively.
The mean lathosterol to cholesterol ratio was 30% higher in subjects with the c.521CC genotypethan in those with the c.521TT genotype, but the difference was not statistically significant (P =0.298). The mean plasma lathosterol concentration was 187.5 µg/100 ml (95% CI, 143.1–231.8µg/100 ml), 210.3 µg/100 ml (95% CI, 159.1–261.5 µg/100 ml) and 266.7 µg/100 ml (95% CI,178.0–355.3 µg/100 ml) in subjects with the c.521TT, c.521TC and c.521CC genotypes,respectively (P = 0.273). The SLCO1B1 genotype had no significant effect on fasting plasmaplant sterol concentrations or their ratios to cholesterol, although they tended to be lower inindividuals with the c.521CC genotype than in those with the c.521TT or c.521TC genotype.

DISCUSSION
71
DISCUSSION
1. Methodological considerations
1.1 Population genetic studies
The population genetic studies were large-scale investigations in which 468 (I) and 941 (II)DNA samples were genotyped from volunteers in different populations. From the CEPH panelof 1064 samples, individuals that were close relatives were excluded. Information on the degreeof relationship of the subjects was not specifically gathered in Study I. The information on thegenotypes and the participants was kept in a secured file with limited access and the genotypedata were analysed in coded form. Random sampling variation affecting the results of SNP andhaplotype frequencies was reduced with the large number of subjects enrolled in the studies.The allelic frequencies were in the Hardy-Weinberg equilibrium.
The SNPs investigated in Study I were selected, based on a previous study in which theSLCO1B1 gene was completely sequenced in 41 healthy Finnish subjects (Niemi et al. 2004).All identified coding region SNPs were included. In addition, one common SNP in the 3’UTRof SLCO1B1 gene was selected from the NCBI single nucleotide polymorphism database(dbSNP) to cover the entire gene. In Study II, the g.-11110T>G SNP was excluded due to rarityand lack of effect on transporter function, based on published studies. In addition, two otherSNPs (c.1086C>T and c.1463G>C) with potential impact on transporter function were includedin Study II. Rapid and robust genotyping assays were established for the SNPs investigated andwere validated by genotyping previously sequenced samples.
The SNPs studied were originally discovered in North American individuals of European orAfrican ancestry or in Caucasians. Typing of SNPs known to be polymorphic in certainpopulations may lead to an underestimation of the genetic variation in other populations, and thestatistics estimated may therefore suffer from ascertainment bias. It is possible that otherSLCO1B1 SNPs, not yet identified, may also explain some of the variation in OATP1B1 activityamong populations.
1.2 Pharmacokinetic and pharmacodynamic studies
The pharmacokinetic and pharmacodynamic studies were carried out using a prospectivegenotype panel study design with 32 healthy volunteers with different SLCO1B1 genotypes(homozygous variant group, 4 subjects; heterozygous variant group, 12 subjects; control group,16 subjects). The subjects served as their own controls in the five phases, which enabledcomparison of the effects of the SLCO1B1 polymorphism on the pharmacokinetics of differentstatins. The number of subjects in each genotype group was estimated to be sufficient to detectpossible clinically meaningful effects of the SLCO1B1 polymorphism on the pharmacokineticsof each statin (approximately 50% greater AUC in subjects with the c.521CC genotype than in

DISCUSSION
72
those with the c.521TT genotype), with a power of at least 80% ( -level 0.05), while avoidingunnecessary exposure of healthy volunteers to drugs.
The number of subjects in the homozygous variant (c.521CC) genotype group was smallcompared with the other genotype groups. The frequency of the homozygousSLCO1B1 c.521CC genotype is 1–5% in Caucasians and the four homozygotes for the variantallele were recruited from a pool of over 300 subjects. In addition, only subjects with theCYP3A5*3/*3, ABCC2 c.1446CC, and CYP2C9 c.1075AA genotypes were included in thestudy to exclude other polymorphisms affecting statin pharmacokinetics, which also decreasedthe number of possible subjects to be considered for participation in the study.
The subjects were not screened for rare mutations in SLCO1B1 and it is thus not possible toexclude the possibility that a rare mutation in SLCO1B1 or in some other gene could haveaffected the disposition of statins in the study subjects. However, the other known functionalSNPs in SLCO1B1 are rare in Caucasians and it is unlikely that any of the subjects would havebeen a carrier of such a variant. So far, there is no certain evidence for in vivo significance ofSLCO1B1 variants other than the c.388A>G and the c.521T>C SNPs.
The statin doses used were selected to be sufficient for reliable quantification, yet to allow theleast possible drug exposure to the healthy subjects. The washout period of at least 1 week wassufficient to minimize possible carry-over effects, since the t½ of the investigated statins andtheir metabolites have been reported to be no more than 19 hours. Timed blood samples weredrawn up to 48 hours after rosuvastatin and atorvastatin ingestion, and up to 12 hours afterfluvastatin, pravastatin and simvastatin ingestion, due to the varying elimination kinetics ofthese different statins. Food intake may have minor effects on the pharmacokinetics offluvastatin, pravastatin and atorvastatin. The investigated statins were administered after anovernight fast and food intake during the five study days was standardized and controlled.
In clinical practice, statins are administered on a regular basis. However, the results from thissingle-dose study can be extrapolated to multiple-dose statin therapy when a steady state hasbeen achieved. According to the pharmacokinetic theory (Rowland and Tozer 1995), the relativedifferences in the dose-interval AUC at steady state between individuals with differentSLCO1B1 genotypes should not be significantly different from those in the AUC after a singledose.
The pharmacodynamic study (VI) investigating the effect of the SLCO1B1 polymorphism on theresponse to a single dose of different statins had sufficient power to detect only a relatively largedifference in statin response between genotypes (40%). Moreover, the study was not designed tocompare the effects of different statins, since their doses were not equally effective and thesampling time (12 hours) covered only a part of their total effect. Thus, the effect of theSLCO1B1 polymorphism on the effects of statins on cholesterol synthesis and absorption duringlong-term use of a statin may differ from the effects observed in this single-dose study.

DISCUSSION
73
In Study VI, the baseline cholesterol and noncholesterol sterol samples were drawn after anovernight fast of at least 8 hours (beginning at 00:00 hours). The last meal in the evening was anonstandardized normal diet meal and the overnight fast was not controlled under in-houseconditions. The use of alcohol was prohibited the evening before statin ingestion and on thestudy days. The use of any medication was prohibited for 1 week before administration ofstatins and the use of grapefruit juice and grapefruit was prohibited for 3 days before theadministration of statin and on the study days. No vegetarians participated in the study and allsubjects were young and healthy with a normal activity level. The use of caffeine and level ofcholesterol in normal everyday diets were not controlled. Thus, not all factors affecting thebaseline cholesterol homeostasis could be strictly standardized in this study.
2. Population genetics of SLCO1B1
Our data on the genetic variation of the SLCO1B1 gene confirm that SLCO1B1 is highlypolymorphic and functional variants occur at varying frequencies in different populations. Theallelic frequencies in the Finnish population and in the 52 ethnic populations in eightgeographical regions throughout the world found in this study are generally in line with previousand later studies on SLCO1B1 diversity.
The high-activity *1B haplotype (and the c.388A>G SNP) is encountered rather frequently in allpopulations, since it is the most common of the haplotypes formed by the c.388A>G andc.521T>C SNPs (*1A, *1B, *5, *15) in North African (48%), Sub-Saharan (77%), East Asian(63%), Oceanian (66%) and American populations (39%). The low-activity *5 and *15haplotypes (and the c.521T>C SNP) are encountered considerably less frequently (0–5% and 0–24% in all populations, respectively). Moreover, a cline in the Northern Hemisphere was seen inthe frequencies of *1B and *15 haplotypes, in which the frequency of *1B (and c.388A<G SNP)was higher in populations near the equator, whereas the frequency of *15 (and c.521T>C SNP)was higher in populations in the north. The contrasting geographical patterns of distribution ofthese two haplotypes with contrasting functional consequences suggest that selective pressuremay have acted on the global distribution of SLCO1B1 variants. However, SLCO1B1 diversity,within and among populations, was generally similar to that found with neutral autosomalmarkers, suggesting that SLCO1B1 variation is mainly determined by the same factors affectingrandom genome markers.
SLCO1B1 diversity was greatest in Africa which is consistent with the out-of-Africareplacement model of modern human origin, stating that African populations are the oldesthuman populations and have therefore accumulated the most genetic variants. Furthermore, theSLCO1B1 genetic distances correlated with the geographic great circle distances betweenpopulations, consistent with human migration patterns. Geographic distance is a good predictorof genetic distance on a global scale (Ramachandran et al. 2005).

DISCUSSION
74
Due to the geographical differences in the distribution of SLCO1B1 variants and to thesubstantial functional effect of certain variants on statin pharmacokinetics (III–V), the efficacyand risk of adverse effects of statins that are affected by OATP1B1 activity could also showgeographical distribution. For example, the benefit-to-risk ratio of simvastatin therapy could bemore attenuated in populations in the Middle East, Europe and America, with high frequenciesof low-activity variants. On the other hand, interindividual differences in statin therapy could belargest in areas, such as North Africa and America, with high frequencies of both low- and high-activity variants. Substantial interethnic differences have been described in thepharmacokinetics of SLCO1B1 substrate drugs. For example, European-Americans havesignificantly higher plasma pravastatin AUCs than African-Americans (Ho et al. 2007). Inaddition, the AUC of rosuvastatin is significantly higher in Chinese, Malay and Indian subjectsthan in Caucasian subjects, all residing in the same environment (Lee et al. 2005a). However,the differences in these studies could not be explained by the SLCO1B1 c.521T>C or c.388A>GSNPs. To what extent other genetic characteristics concerning the SLCO1B1 gene or other genescan explain these differences, remains to be clarified.
3. Role of SLCO1B1 polymorphism in statin pharmacokinetics andpharmacodynamics
It is becoming increasingly evident that SLCO1B1 polymorphism, notably the c.521T>C SNP,has a major effect on OATP1B1 activity and on the disposition of many OATP1B1 substrates.In our studies, substantial differences existed in the effects of the SLCO1B1 c.521T>C varianton the pharmacokinetics of different statins. The variant c.521CC genotype had the greatesteffect on the plasma concentrations of active simvastatin acid (mean increase 221%). It alsoconsiderably increased the plasma concentrations of atorvastatin, pravastatin and rosuvastatin,but had no significant effect on the plasma concentrations of fluvastatin. The smaller effect ofthe SLCO1B1 polymorphism on the pharmacokinetics of fluvastatin may be explained by itsrelatively high lipophilicity facilitating passive diffusion through the hepatocyte plasmamembrane. Alternatively, some other transporters apart from OATP1B1 in the sinusoidalmembrane of hepatocytes could mediate the uptake of fluvastatin or compensate for the reduceduptake by OATP1B1.

DISCUSSION
75
In a similar manner to that of cyclosporine, the SLCO1B1 c.521T>C SNP increased mainly theCmax and AUC of the investigated statins, with no effect on their elimination half-lives. This isalso generally seen with other OATP1B1 substrates, e.g. repaglinide (Niemi et al. 2005a). Indrugs with very high hepatic extraction ratios, this lack of effect on the t½ values could be due toincrease in only the oral bioavailability as:
HI EEF 11
and
HH EQCL
where F, EI, EH, CL and QH represent oral bioavailability, intestinal extraction ratio, hepaticextraction ratio, clearance and hepatic blood flow, respectively. However, statins do notgenerally have such high hepatic extraction ratios (EH) which suggests that the lack of effect ofreduced OATP1B1 activity on the elimination half-life (t½) of statins (and on that of otherOATP1B1 substrates) could be mainly explained by corresponding decreases in drug clearance(CL) and the volume of distribution (Vd) when access to the hepatocyte is limited, as:
CLVlnt d
½2
Genetically impaired activity of OATP1B1 may decrease the entry of statins into theirintracellular site of action, thus limiting their inhibition of HMG-CoA reductase whileincreasing statin plasma concentrations. The SLCO1B1 c.521T>C SNP was very recently foundto be a considerable risk factor for simvastatin-induced myopathy in high-dose simvastatintherapy (Figure 13) (SEARCH Collaborative Group 2008). In this genomewide study conductedby the Study of the Effectiveness of Additional Reductions in Cholesterol and Homocysteine(SEARCH) Collaborative Group, 300 000 SNPs were screened in each patient with myopathywhile taking 80 mg simvastatin per day and the prevalences of these SNPs were compared withthat in matched control patients using the same dose of simvastatin without myopathy(SEARCH Collaborative Group 2008). The only genetic marker strongly associated withmyopathy was the SLCO1B1 c.521T>C SNP, the same variant that was associated withconsiderably higher plasma concentrations of simvastatin acid in Study IV (Figure 13). The riskfor muscle toxicity increases greatly along with increased statin doses and increased statinconcentrations in peripheral blood and muscle cells (Baigent et al. 2005). Although myopathy isa class effect of statins, our studies suggest that the increased risk for myopathy imposed by thec.521T>C variant may be smaller with statins other than simvastatin and possibly negligiblewith fluvastatin.

DISCUSSION
76
Figure 13. Effect of SLCO1B1 polymorphism on the pharmacokinetics of simvastatin and onmyopathy risk during high-dose simvastatin therapy. (A) Mean plasma concentrations of activesimvastatin acid after a single 40-mg oral dose of simvastatin in healthy volunteers according tothe SLCO1B1 c.521T>C genotype (II). (B) Estimated cumulative risk of myopathy associatedwith 80-mg daily simvastatin therapy according to the SLCO1B1 c.521T>C genotype(SEARCH Collaborative Group 2008; Copyright © 2008 Massachusetts Medical Society. Allrights reserved).
There may also be other genetic factors that substantially affect the pharmacokinetics andpharmacodynamics of statins or cellular mechanisms of muscle damage, which could determinean individual’s susceptibility to myopathy during statin therapy. For example, lipidomics-basedsafety biomarkers are a novel approach for predicting statin safety. Plasma lipidomic profilesmay be used as sensitive biomarkers to assess statin-induced metabolic changes in musclebefore muscle toxicity occurs and to identify patients susceptible to myopathy (Laaksonen et al.2006, 2008).
Despite the significant effect on statin pharmacokinetics, the SLCO1B1 genotype did not affectthe response to a single dose of statin in our studies. This lack of effect may be partly explainedby the log-linear relationship between drug concentration and effect. Moreover, the impact ofSLCO1B1 polymorphism on statin response could be different during long-term treatment. Inthe Heart Protection Study, the c.521T>C variant was associated with a slightly smallerreduction in plasma LDL-C produced by 40 mg simvastatin, whereas the c.388A>G wasassociated with a slightly larger reduction in plasma LDL-C (Heart Protection StudyCollaborative Group 2002).
Interestingly, a single dose of all the statins investigated decreased the plasma avenasterol tocholesterol ratio compared with the baseline. There was a trend towards a larger decrease in theavenasterol to cholesterol ratio in the c.521CC subjects, but the differences between thegenotype groups were not significant. In a previous study, the ratios of plant sterols tocholesterol were increased in long-term simvastatin treatment (Miettinen et al. 2000). Theclinical relevance of the effect of statins and the SLCO1B1 genotype on plant sterols warrantsfurther studies.

DISCUSSION
77
4. Role of SLCO1B1 polymorphism in cholesterol homeostasis
The SLCO1B1 c.521CC variant genotype was associated with an increased baseline cholesterolsynthesis rate. Individuals with the c.521CC genotype had higher plasma desmosterol tocholesterol ratios and higher plasma desmosterol concentrations than those with the c.521TT(control) genotype. In line with this finding, the plasma lathosterol to cholesterol ratio andplasma lathosterol concentration tended to be higher in the c.521CC subjects than in thec.521TT subjects. Desmosterol and lathosterol as well as their respective ratios to cholesterolreflect the cholesterol synthesis rate. In contrast, a trend towards lower plasma concentrations ofthe plant sterols reflecting the cholesterol absorption rate was seen in the c.521CC subjectscompared with the c.521TT subjects.
A functional link between cholesterol homeostasis and OATP1B1 could be through bile acidhomeostasis, as the regulation of bile acid synthesis and cholesterol homeostasis is tightly linked(Figure 14) (Fuchs 2003). The hepatic uptake of approximately 20% of bile acids is thought tobe mediated by basolateral OATP transporters (OATP1B1, OATP1B3, OATP2B1), althoughthe exact contribution of different OATPs to the uptake of individual bile acids is unknown.OATP1B1 may play a major role in the uptake of certain bile acids. The intracellular bile acidconcentration is determined by the balance of basolateral uptake, intracellular synthesis, andsinusoidal and basolateral efflux. Excess cholesterol in the liver is catabolised into bile acids,whereas excess bile acids in the liver down-regulate cholesterol catabolism. Impaired activity ofOATP1B1 could decrease the bile acid concentration in the liver by limiting the access of bileacids from the portal blood into the liver. This could lead to increased cholesterol catabolism viaCYP7A1, which reduces the negative feedback loop on HMG-CoA reductase and acceleratescholesterol synthesis. Another possible association between OATP1B1 and the cholesterolsynthesis rate may be through thyroid hormones, because thyroid hormones increase thecholesterol synthesis rate and are OATP1B1 substrates (Abrams and Grundy 1981, Abe et al.1999, Hsiang et al. 1999, van der Deure et al. 2008).
The exact mechanism and clinical importance of the higher basal cholesterol synthesis rate inindividuals with the c.521CC genotype requires further investigations to be clarified. However,the driving force for the cline seen in the functional SLCO1B1 haplotypes *15 and *1B could bepartly related to the differences in cholesterol homeostasis seen in this study.

DISCUSSION
78
Figure 14. Schematic representation of the interrelationship between bile acid and cholesterolhomeostasis. Solid arrows indicate metabolic pathways involving cholesterol and bile acids.Dashed arrows indicate activation (+) or suppression (-) of transcription factors. Solid linesindicate increase (+) or decrease (-) in gene expression. Acetyl-CoA, acetyl-coenzyme A; HMG-CoAR, 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase; CYP7A1, cholesterol 7 -hydroxylase; CYP8B1, sterol 12 -hydroxylase; SREBP2, sterol regulatory element bindingprotein 2; LXR, liver X receptor; SHP, small heterodimer partner; FGF-19, fibroblast growthfactor-19; FXR, farnesoid X receptor; CA, cholic acid; CDCA, chenodeoxycholic acid;OATP1B1, organic-anion transporting polypeptide 1B1.
5. Clinical implications
It already became apparent in the 1950s and 1960s that elevated concentrations of plasmacholesterol are a major risk factor for the development of coronary heart disease. During recentdecades, health research has contributed significantly to the reduction in deaths caused bycardiovascular diseases (Tunstall-Pedoe et al. 2000). The observed decrease in death ratesevolved partially from better understanding of the main modifiable risk factors forcardiovascular disease, including high cholesterol level, but also smoking, high blood pressureand diabetes, as well as from use of pharmacologic interventions to reduce these factors. Expertpanels throughout the world have recommended lifestyle changes and, according to each
DISCUSSION
79
patient’s individual risk for developing cardiovascular disease, also lipid-modifying therapy todecrease elevated cholesterol concentrations (De Backer et al. 2003). Statins have the potentialto lighten the global burden of cardiovascular disease, because they reduce the incidence ofmajor coronary events, coronary revascularization and stroke by about 20% for each reductionof 1 mmol/l in the plasma LDL-C level (Baigent et al. 2005). In addition, statins are generallysafe and well-tolerated (Law and Rudnicka 2006, Armitage 2007). Since the extent of CHD riskreduction is directly proportional to the degree to which LDL-C is lowered (Chen et al. 1991),there has been an increasing trend towards aggressive treatment with high statin doses, whichincreases the risk of adverse effects of statins, e.g. myopathy (Thompson et al. 2003).
Generally, the potential causes and mechanisms of adverse drug effects are diverse, with onepossibility being genetic variations predisposing the patient to altered drug disposition. Theidentification and characterization of these genetic variations may aid in developing morepersonalized drug therapies, taking into account the susceptibility of an individual patient toadverse effects. In this thesis, the SLCO1B1 c.521T>C variant allele was associated withsubstantially increased exposure to certain statins, suggesting that it could increase the risk ofstatin-induced myopathy in patients with the SLCO1B1 variant genotype. In addition, since theeffects of the genotype varied between different statins, this increased risk could be differentdepending on the statin used. The large-scale study published during the final preparation of thisthesis showed an unequivocal association between the c.521T>C allele and simvastatin-inducedmyopathy (SEARCH Collaborative Group 2008). It has been suggested that avoiding high-dosesimvastatin administration to patients carrying the c.521C allele (approximately 32% of theFinnish population in our studies) could reduce the incidence of simvastatin-induced myopathyby nearly 60% (Nakamura 2008). Alternatively, simvastatin could be avoided in patients withthe c.521CC genotype (approximately 4% of the Finnish population) and prescribed only atlower doses to patients who are carriers of one c.521C allele. The risk for myopathy imposed bythe c.521C allele could be predicted to be smaller in users of some other statins. Interestingly,there have been very few, if any, published cases of rhabdomyolysis and relatively lowincidences of myopathy in patients using fluvastatin (Law and Rudnicka 2006), thepharmacokinetics of which was least sensitive to the effect of the c.521C variant allele.Moreover, since the frequencies of SLCO1B1 variants differ markedly between populations, theclinical importance of the increased risk for statin-induced myopathy imposed by the c.521Cvariant may vary according to the ethnic background.
In conclusion, SLCO1B1 genotype-based prescription may help to achieve the benefits of statintherapy more safely and effectively. In addition, SLCO1B1 polymorphism could also be ofclinical importance in therapies with other OATP1B1 substrate drugs.

CONCLUSIONS
80
CONCLUSIONS
Functionally significant sequence variations in SLCO1B1 are widely distributed globally andtheir frequencies vary considerably between different populations. The frequencies of SLCO1B1SNPs in the Finnish population are consistent with those in other Caucasian populations. Thefunctionally detrimental homozygous variant c.521CC genotype is relatively common inCaucasians. SLCO1B1 diversity is far greater within than between populations.
The SLCO1B1 polymorphism was significantly associated with the pharmacokinetics ofpravastatin, simvastatin acid, rosuvastatin and atorvastatin. Subjects with the homozygousvariant c.521CC genotype had considerably higher plasma concentrations of these statins thanthose with the c.521TT (reference) genotype. Differences existed in the effect of the SLCO1B1genotype on statin pharmacokinetics and the most profound effect was seen in the plasmaconcentrations of simvastatin acid, the main active form of simvastatin. Since the risk of statinmyotoxicity is clearly associated with increased plasma concentrations of statins, SLCO1B1polymorphism could considerably decrease the benefit-to-risk ratio of certain statin therapiesand render patients more susceptible to statin-induced myopathy. Fluvastatin pharmacokineticswas not significantly associated with SLCO1B1 polymorphism.
The SLCO1B1 polymorphism was not associated with the short-term effects of any of the statinsinvestigated on the markers for cholesterol synthesis and absorption. However, the effect of thispolymorphism on statin response during long-term treatment may differ from the effectsobserved in a single-dose study. In addition, the SLCO1B1 polymorphism was associated withincreased basal cholesterol synthesis rate, as characterized by significantly higher plasmacholesterol synthesis marker concentrations.
These studies underline the importance of large-scale genotyping studies in investigating geneticvariation in clinically important transporter genes to better understand interindividual andinterethnic variation in drug response. In addition, the results of these studies highlight theclinical importance of the SLCO1B1 polymorphism in statin therapy and may help to clarifywhy individual patients respond differently to various statins.

ACKNOWLEDGEMENTS
81
ACKNOWLEDGEMENTS
This work was carried out in the Department of Clinical Pharmacology, University of Helsinki,during the years 2003–2008. I wish to express my sincere gratitude to all those who have helpedme during these years.
I am deeply grateful to my other supervisor and the head of the department Professor PerttiNeuvonen, whose expertise and devotion to the field of clinical pharmacology are trulyimpressive. It has been a privilege to work under his encouraging supervision and be a part ofthe warm and inspiring KLIFA team.
I am most grateful to my supervisor, Docent Mikko Niemi, who has introduced me to thescientific research in the field of pharmacogenetics. His extensive knowledge, contagiousenthusiasm, friendly encouragement and patient guidance have been invaluable for this thesiswork to be carried out.
I would like to thank Docent Reijo Laaksonen and Docent Miia Turpeinen for their promptreview and constructive comments concerning this thesis work. I thank James Thompson forediting the language of this thesis.
I am grateful to Docent Janne Backman for all the kind advice and guidance in clinicalpharmacology throughout these years, and collaboration in study I.
I thank the collaborators Professor Tatu Miettinen and Professor Helena Gylling for theircontribution in study VI.
I am very grateful to Jouko Laitila, Mikko Neuvonen and Hanna Fredrikson for their skillfuldrug concentration measurements. I wish to thank the “ladies” Lisbet Partanen, Eija Mäkinen-Pulli and Kerttu Mårtensson for their skillful technical assistance and cheerful company in thelab and on study days.
I wish to thank Aleksi Tornio for friendship as well as all the help and support, especially incomputer-related issues and in reminding me not to be late for everything. Lauri Kajosaari,Marika Schröder (Granfors), Marjo Pitkänen (Karjalainen) and Annikka Kalliokoski are thankedfor their experienced advices, friendly company and enjoyable discussions.
I want to thank also all the other fantastic colleagues at the Department of ClinicalPharmacology for pleasant company and help: Jenni Keskitalo, Samuel Fanta, Carl Kyrklund,Tuure Saarinen, Kati Ahonen, Mika Isohanni, Jari Lilja, Tiina Jaakkola, Heli Malm, KariRaaska, Kalle Hoppu (and the staff of the Poison Information Center), Lasse Lehtonen, KaisaKurkinen, Johanna Honkalammi, Han Yi and Xiang Xiaoqiang. Thanks are also due to TuijaItkonen for excellent assistance in many practical manners.

ACKNOWLEDGEMENTS
82
I am grateful to all the volunteers who participated in these studies. The Biomedicum vaksit arethanked for letting me in every time I forgot my keys.
This work was financially supported by the Clinical Drug Research Graduate School, theBiomedicum Helsinki Foundation, the Paulo Foundation, the Orion-Farmos ResearchFoundation and the Finnish Medical Society Duodecim, all of which are gratefullyacknowledged.
I wish to thank all my friends for (still) being there. Your support and friendship are trulyappreciated. My loving thanks go especially to the VP: you are amazing.
Finally, I would like to thank my parents and other family members for unconditional love,support and encouragement during these years despite all my ventures; especially Anski for allthe help and loving care as well as technical assistance in study II; and Janne, for catering andfor being who you are.
Helsinki, November 2008
Marja Pasanen
“Tea was just a temporary solution to the cares of the world, althoughit certainly helped…. Most problems could be diminished by thedrinking of tea and the thinking through of things that could be donewhile tea was being drunk. And even if that did not solve problems, atleast it could put them off for a little while, which we sometimesneeded to do, we really did.”
Alexander McCall Smith (Blue Shoes and Happiness)

REFERENCES
83
REFERENCES
Abe T, Kakyo M, Tokui T, Nakagomi R, Nishio T, Nakai D, Nomura H, Unno M, Suzuki M,Naitoh T, Matsuno S, Yawo H. Identification of a novel gene family encoding human liver-specificorganic anion transporter LST-1. J Biol Chem 1999;274:17159-63.
Abe T, Unno M, Onogawa T, Tokui T. [Molecular identification of organic anion transporter oatp/LSTfamily]. Tanpakushitsu Kakusan Koso 2001;46:612-20.
Abrams JJ, Grundy SM. Cholesterol metabolism in hypothyroidism and hyperthyroidism in man. JLipid Res 1981;22:323-38.
Alberts AW, Chen J, Kuron G, Hunt V, Huff J, Hoffman C, Rothrock J, Lopez M, Joshua H,Harris E, Patchett A, Monaghan R, Currie S, Stapley E, Albers-Schönberg G, Hensens O,Hirshfield J, Hoogsteen K, Liesch J, Springer J. Mevinolin: a highly potent competitive inhibitor ofhydroxymethylglutaryl-coenzyme A reductase and a cholesterol-lowering agent. Proc Natl Acad Sci U SA 1980;77:3957-61.
Allen JD, Schinkel AH. Multidrug resistance and pharmacological protection mediated by the breastcancer resistance protein (BCRP/ABCG2). Mol Cancer Ther 2002;1:427-34.
Alrefai WA, Gill RK. Bile acid transporters: structure, function, regulation and pathophysiologicalimplications. Pharm Res 2007;24:1803-23.
Anderle P, Nielsen CU, Pinsonneault J, Krog PL, Brodin B, Sadee W. Genetic variants of the humandipeptide transporter PEPT1. J Pharmacol Exp Ther 2006;316:636-46.
Armitage J. The safety of statins in clinical practice. Lancet 2007;370:1781-90.
Arnadottir M, Eriksson LO, Thysell H, Karkas JD. Plasma concentration profiles of simvastatin 3-hydroxy-3-methyl-glutaryl-coenzyme A reductase inhibitory activity in kidney transplant recipients withand without ciclosporin. Nephron 1993;65:410-3.
Backman JT, Kyrklund C, Kivistö KT, Wang JS, Neuvonen PJ. Plasma concentrations of activesimvastatin acid are increased by gemfibrozil. Clin Pharmacol Ther 2000;68:122-9.
Backman JT, Kyrklund C, Neuvonen M, Neuvonen PJ. Gemfibrozil greatly increases plasmaconcentrations of cerivastatin. Clin Pharmacol Ther 2002;72:685-91.
Backman JT, Luurila H, Neuvonen M, Neuvonen PJ. Rifampin markedly decreases and gemfibrozilincreases the plasma concentrations of atorvastatin and its metabolites. Clin Pharmacol Ther2005;78:154-67.
Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, Kirby A, Sourjina T, Peto R,Collins R, Simes R. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis ofdata from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267-78.
Biardi L, Krisans SK. Compartmentalization of cholesterol biosynthesis. Conversion of mevalonate tofarnesyl diphosphate occurs in the peroxisomes. J Biol Chem 1996;271:1784-8.
REFERENCES
84
Björkhem I, Miettinen T, Reihner E, Ewerth S, Angelin B, Einarsson K. Correlation between serumlevels of some cholesterol precursors and activity of HMG-CoA reductase in human liver. J Lipid Res1987;28:1137-43.
Bohan A, Boyer JL. Mechanisms of hepatic transport of drugs: implications for cholestatic drugreactions. Semin Liver Dis 2002;22:123-36.
Bonetti PO, Lerman LO, Napoli C, Lerman A. Statin effects beyond lipid lowering--are theyclinically relevant? Eur Heart J 2003;24:225-48.
Borst P, de Wolf C, van de Wetering K. Multidrug resistance-associated proteins 3, 4, and 5. PflugersArch 2007;453:661-73.
Bradford RH, Shear CL, Chremos AN, Dujovne C, Downton M, Franklin FA, Gould AL, HesneyM, Higgins J, Hurley DP, et al. Expanded Clinical Evaluation of Lovastatin (EXCEL) study results. I.Efficacy in modifying plasma lipoproteins and adverse event profile in 8245 patients with moderatehypercholesterolemia. Arch Intern Med 1991;151:43-9.
Brandsch M, Knutter I, Bosse-Doenecke E. Pharmaceutical and pharmacological importance ofpeptide transporters. J Pharm Pharmacol 2008;60:543-85.
Briz O, Serrano MA, Rebollo N, Hagenbuch B, Meier PJ, Koepsell H, Marin JJ. Carriers involvedin targeting the cytostatic bile acid-cisplatin derivatives cis-diammine-chloro-cholylglycinate-platinum(II) and cis-diammine-bisursodeoxycholate-platinum(II) toward liver cells. Mol Pharmacol2002;61:853-60.
Briz O, Serrano MA, MacIas RI, Gonzalez-Gallego J, Marin JJ. Role of organic anion-transportingpolypeptides, OATP-A, OATP-C and OATP-8, in the human placenta-maternal liver tandem excretorypathway for foetal bilirubin. Biochem J 2003;371:897-905.
Brown CDA, Windass AS, Bleasby K, Lauffart B. Rosuvastatin is a high affinity substrate of hepaticorganic anion transporter OATP-C. Atheroscler Suppl 2001;2:90.
Brown MS, Goldstein JL. Lipoprotein receptors in the liver. Control signals for plasma cholesteroltraffic. J Clin Invest 1983;72:743-7.
Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterol homeostasis. Science1986;232:34-47.
Bruckert E, Hayem G, Dejager S, Yau C, Begaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients--the PRIMO study. Cardiovasc Drugs Ther2005;19:403-14.
Campbell SD, de Morais SM, Xu JJ. Inhibition of human organic anion transporting polypeptideOATP 1B1 as a mechanism of drug-induced hyperbilirubinemia. Chem Biol Interact 2004;150:179-87.
Cann HM, de Toma C, Cazes L, Legrand MF, Morel V, Piouffre L, Bodmer J, Bodmer WF,Bonne-Tamir B, Cambon-Thomsen A, Chen Z, Chu J, Carcassi C, Contu L, Du R, Excoffier L,Ferrara GB, Friedlaender JS, Groot H, Gurwitz D, Jenkins T, Herrera RJ, Huang X, Kidd J, KiddKK, Langaney A, Lin AA, Mehdi SQ, Parham P, Piazza A, Pistillo MP, Qian Y, Shu Q, Xu J, ZhuS, Weber JL, Greely HT, Feldman MW, Thomas G, Dausset J, Cavalli-Sforza LL. A humangenome diversity cell line panel. Science 2002;296:261-2.

REFERENCES
85
Chang C, Pang KS, Swaan PW, Ekins S. Comparative pharmacophore modeling of organic aniontransporting polypeptides: a meta-analysis of rat Oatp1a1 and human OATP1B1. J Pharmacol Exp Ther2005;314:533-41.
Chen C, Mireles RJ, Campbell SD, Lin J, Mills JB, Xu JJ, Smolarek TA. Differential interaction of3-hydroxy-3-methylglutaryl-coa reductase inhibitors with ABCB1, ABCC2, and OATP1B1. Drug MetabDispos 2005;33:537-46.
Chen Z, Peto R, Collins R, MacMahon S, Lu J, Li W. Serum cholesterol concentration and coronaryheart disease in population with low cholesterol concentrations. Bmj 1991;303:276-82.
Chong PH, Seeger JD, Franklin C. Clinically relevant differences between the statins: implications fortherapeutic selection. Am J Med 2001;111:390-400.
Chorley BN, Wang X, Campbell MR, Pittman GS, Noureddine MA, Bell DA. Discovery andverification of functional single nucleotide polymorphisms in regulatory genomic regions: current anddeveloping technologies. Mutat Res 2008;659:147-57.
Chung JY, Cho JY, Yu KS, Kim JR, Oh DS, Jung HR, Lim KS, Moon KH, Shin SG, Jang IJ.Effect of OATP1B1 (SLCO1B1) variant alleles on the pharmacokinetics of pitavastatin in healthyvolunteers. Clin Pharmacol Ther 2005;78:342-50.
Collins FS, Brooks LD, Chakravarti A. A DNA polymorphism discovery resource for research onhuman genetic variation. Genome Res 1998;8:1229-31.
Connor WE, Witiak DT, Stone DB, Armstrong ML. Cholesterol balance and fecal neutral steroid andbile acid excretion in normal men fed dietary fats of different fatty acid composition. J Clin Invest1969;48:1363-75.
Cooper KJ, Martin PD, Dane AL, Warwick MJ, Schneck DW, Cantarini MV. The effect offluconazole on the pharmacokinetics of rosuvastatin. Eur J Clin Pharmacol 2002;58:527-31.
Cooper KJ, Martin PD, Dane AL, Warwick MJ, Schneck DW, Cantarini MV. Effect of itraconazoleon the pharmacokinetics of rosuvastatin. Clin Pharmacol Ther 2003;73:322-9.
Craddock AL, Love MW, Daniel RW, Kirby LC, Walters HC, Wong MH, Dawson PA. Expressionand transport properties of the human ileal and renal sodium-dependent bile acid transporter. Am JPhysiol 1998;274:G157-69.
Cribb AE, Peyrou M, Muruganandan S, Schneider L. The endoplasmic reticulum in xenobiotictoxicity. Drug Metab Rev 2005;37:405-42.
Cucchiara S, Latiano A, Palmieri O, Staiano AM, D'Inca R, Guariso G, Vieni G, Rutigliano V,Borrelli O, Valvano MR, Annese V. Role of CARD15, DLG5 and OCTN genes polymorphisms inchildren with inflammatory bowel diseases. World J Gastroenterol 2007;13:1221-9.
Cui Y, König J, Leier I, Buchholz U, Keppler D. Hepatic uptake of bilirubin and its conjugates by thehuman organic anion transporter SLC21A6. J Biol Chem 2001;276:9626-30.
Daly AK. Pharmacogenetics of the major polymorphic metabolizing enzymes. Fundam Clin Pharmacol2003;17:27-41.
Dawson PA, Rudel LL. Intestinal cholesterol absorption. Curr Opin Lipidol 1999;10:315-20.

REFERENCES
86
Dawson PA, Hubbert M, Haywood J, Craddock AL, Zerangue N, Christian WV, Ballatori N. Theheteromeric organic solute transporter alpha-beta, Ostalpha-Ostbeta, is an ileal basolateral bile acidtransporter. J Biol Chem 2005;280:6960-8.
De Backer G, Ambrosioni E, Borch-Johnsen K, Brotons C, Cifkova R, Dallongeville J, Ebrahim S,Faergeman O, Graham I, Mancia G, Manger Cats V, Orth-Gomer K, Perk J, Pyörälä K, RodicioJL, Sans S, Sansoy V, Sechtem U, Silber S, Thomsen T, Wood D. European guidelines oncardiovascular disease prevention in clinical practice. Third Joint Task Force of European and OtherSocieties on Cardiovascular Disease Prevention in Clinical Practice. Eur Heart J 2003;24:1601-10.
Deng JW, Song IS, Shin HJ, Yeo CW, Cho DY, Shon JH, Shin JG. The effect of SLCO1B1*15 onthe disposition of pravastatin and pitavastatin is substrate dependent: the contribution of transportingactivity changes by SLCO1B1*15. Pharmacogenet Genomics 2008;18:424-33.
Dietschy JM. Regulation of cholesterol metabolism in man and in other species. Klin Wochenschr1984;62:338-45.
Dirks AJ, Jones KM. Statin-induced apoptosis and skeletal myopathy. Am J Physiol Cell Physiol2006;291:C1208-12.
Downton C, Clark I. Statins--the heart of the matter. Nat Rev Drug Discov 2003;2:343-4.
Doyle LA, Yang W, Abruzzo LV, Krogmann T, Gao Y, Rishi AK, Ross DD. A multidrug resistancetransporter from human MCF-7 breast cancer cells. Proc Natl Acad Sci U S A 1998;95:15665-70.
Dresser MJ, Leabman MK, Giacomini KM. Transporters involved in the elimination of drugs in thekidney: organic anion transporters and organic cation transporters. J Pharm Sci 2001;90:397-421.
Duane WC. Effects of lovastatin and dietary cholesterol on sterol homeostasis in healthy humansubjects. J Clin Invest 1993;92:911-8.
Dujovne CA, Chremos AN, Pool JL, Schnaper H, Bradford RH, Shear CL, Higgins J, Downton M,Franklin FA, Nash DT, et al. Expanded clinical evaluation of lovastatin (EXCEL) study results: IV.Additional perspectives on the tolerability of lovastatin. Am J Med 1991;91:25S-30S.
Endo A, Kuroda M, Tanzawa K. Competitive inhibition of 3-hydroxy-3-methylglutaryl coenzyme Areductase by ML-236A and ML-236B fungal metabolites, having hypocholesterolemic activity. FEBSLett 1976;72:323-6.
Endo A. Compactin (ML-236B) and related compounds as potential cholesterol-lowering agents thatinhibit HMG-CoA reductase. J Med Chem 1985;28:401-5.
Excoffier L, Smouse PE, Quattro JM. Analysis of molecular variance inferred from metric distancesamong DNA haplotypes: application to human mitochondrial DNA restriction data. Genetics1992;131:479-91.
Faber KN, Muller M, Jansen PL. Drug transport proteins in the liver. Adv Drug Deliv Rev2003;55:107-24.
Fehrenbach T, Cui Y, Faulstich H, Keppler D. Characterization of the transport of the bicyclic peptidephalloidin by human hepatic transport proteins. Naunyn Schmiedebergs Arch Pharmacol 2003;368:415-20.

REFERENCES
87
Fiegenbaum M, da Silveira FR, Van der Sand CR, Van der Sand LC, Ferreira ME, Pires RC, HutzMH. The role of common variants of ABCB1, CYP3A4, and CYP3A5 genes in lipid-lowering efficacyand safety of simvastatin treatment. Clin Pharmacol Ther 2005;78:551-8.
Fischer V, Johanson L, Heitz F, Tullman R, Graham E, Baldeck JP, Robinson WT. The 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor fluvastatin: effect on human cytochrome P-450 andimplications for metabolic drug interactions. Drug Metab Dispos 1999;27:410-6.
Fischer WJ, Altheimer S, Cattori V, Meier PJ, Dietrich DR, Hagenbuch B. Organic aniontransporting polypeptides expressed in liver and brain mediate uptake of microcystin. Toxicol ApplPharmacol 2005;203:257-63.
Fromm MF. Importance of P-glycoprotein at blood-tissue barriers. Trends Pharmacol Sci 2004;25:423-9.
Fuchs M. Bile acid regulation of hepatic physiology: III. Regulation of bile acid synthesis: past progressand future challenges. Am J Physiol Gastrointest Liver Physiol 2003;284:G551-7.
Färkkila MA, Tilvis RS, Miettinen TA. Raised plasma cholesterol precursors in patients with gutresections. Gut 1988;29:188-95.
Giacomini KM, Sugiyama Y. Membrane transporters and Drug Response. In: Brunton LL, Lazo JS,Parker KL. Goodman and Gillman's the pharmacological basis of therapeutics. New York: McGraw-Hill; 2006. 41-70
Giacomini KM, Krauss RM, Roden DM, Eichelbaum M, Hayden MR, Nakamura Y. When gooddrugs go bad. Nature 2007;446:975-7.
Glaeser H, Bailey DG, Dresser GK, Gregor JC, Schwarz UI, McGrath JS, Jolicoeur E, Lee W,Leake BF, Tirona RG, Kim RB. Intestinal drug transporter expression and the impact of grapefruitjuice in humans. Clin Pharmacol Ther 2007;81:362-70.
Glatz JF, Katan MB. Dietary saturated fatty acids increase cholesterol synthesis and fecal steroidexcretion in healthy men and women. Eur J Clin Invest 1993;23:648-55.
Glavy JS, Wu SM, Wang PJ, Orr GA, Wolkoff AW. Down-regulation by extracellular ATP of rathepatocyte organic anion transport is mediated by serine phosphorylation of oatp1. J Biol Chem2000;275:1479-84.
Gottesman MM, Pastan I, Ambudkar SV. P-glycoprotein and multidrug resistance. Curr Opin GenetDev 1996;6:610-7.
Gradhand U, Kim RB. Pharmacogenomics of MRP transporters (ABCC1-5) and BCRP (ABCG2).Drug Metab Rev 2008;40:317-54.
Graff CL, Pollack GM. Drug transport at the blood-brain barrier and the choroid plexus. Curr DrugMetab 2004;5:95-108.
Graham DJ, Staffa JA, Shatin D, Andrade SE, Schech SD, La Grenade L, Gurwitz JH, Chan KA,Goodman MJ, Platt R. Incidence of hospitalized rhabdomyolysis in patients treated with lipid-loweringdrugs. Jama 2004;292:2585-90.

REFERENCES
88
Grube M, Köck K, Oswald S, Draber K, Meissner K, Eckel L, Böhm M, Felix SB, Vogelgesang S,Jedlitschky G, Siegmund W, Warzok R, Kroemer HK. Organic anion transporting polypeptide 2B1 isa high-affinity transporter for atorvastatin and is expressed in the human heart. Clin Pharmacol Ther2006;80:607-20.
Guo SW, Thompson EA. Performing the exact test of Hardy-Weinberg proportion for multiple alleles.Biometrics 1992;48:361-72.
Gylling H, Miettinen TA. Cholesterol absorption and synthesis related to low density lipoproteinmetabolism during varying cholesterol intake in men with different apoE phenotypes. J Lipid Res1992;33:1361-71.
Gylling H, Miettinen TA. The effect of cholesterol absorption inhibition on low density lipoproteincholesterol level. Atherosclerosis 1995;117:305-8.
Gylling H, Miettinen TA. Cholesterol absorption, synthesis, and LDL metabolism in NIDDM. DiabetesCare 1997;20:90-5.
Hagenbuch B, Meier PJ. Molecular cloning, chromosomal localization, and functional characterizationof a human liver Na+/bile acid cotransporter. J Clin Invest 1994;93:1326-31.
Hagenbuch B, Meier PJ. The superfamily of organic anion transporting polypeptides. Biochim BiophysActa 2003;1609:1-18.
Hagenbuch B, Meier PJ. Organic anion transporting polypeptides of the OATP/ SLC21 family:phylogenetic classification as OATP/ SLCO superfamily, new nomenclature and molecular/functionalproperties. Pflugers Arch 2004;447:653-65.
Haimeur A, Conseil G, Deeley RG, Cole SP. The MRP-related and BCRP/ABCG2 multidrugresistance proteins: biology, substrate specificity and regulation. Curr Drug Metab 2004;5:21-53.
Hamelin BA, Turgeon J. Hydrophilicity/lipophilicity: relevance for the pharmacology and clinicaleffects of HMG-CoA reductase inhibitors. Trends Pharmacol Sci 1998;19:26-37.
Handschin C, Meyer UA. Induction of drug metabolism: the role of nuclear receptors. Pharmacol Rev2003;55:649-73.
Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterollowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet2002;360:7-22.
Hediger MA, Romero MF, Peng JB, Rolfs A, Takanaga H, Bruford EA. The ABCs of solutecarriers: physiological, pathological and therapeutic implications of human membrane transportproteinsIntroduction. Pflugers Arch 2004;447:465-8.
Hedman M, Neuvonen PJ, Neuvonen M, Holmberg C, Antikainen M. Pharmacokinetics andpharmacodynamics of pravastatin in pediatric and adolescent cardiac transplant recipients on a regimenof triple immunosuppression. Clin Pharmacol Ther 2004;75:101-9.
Henriksen U, Gether U, Litman T. Effect of Walker A mutation (K86M) on oligomerization andsurface targeting of the multidrug resistance transporter ABCG2. J Cell Sci 2005;118:1417-26.

REFERENCES
89
Hermann M, Asberg A, Christensen H, Holdaas H, Hartmann A, Reubsaet JL. Substantiallyelevated levels of atorvastatin and metabolites in cyclosporine-treated renal transplant recipients. ClinPharmacol Ther 2004;76:388-91.
Hirano M, Maeda K, Shitara Y, Sugiyama Y. Contribution of OATP2 (OATP1B1) and OATP8(OATP1B3) to the hepatic uptake of pitavastatin in humans. J Pharmacol Exp Ther 2004;311:139-46.
Hirano M, Maeda K, Hayashi H, Kusuhara H, Sugiyama Y. Bile salt export pump (BSEP/ABCB11)can transport a nonbile acid substrate, pravastatin. J Pharmacol Exp Ther 2005a;314:876-82.
Hirano M, Maeda K, Matsushima S, Nozaki Y, Kusuhara H, Sugiyama Y. Involvement of BCRP(ABCG2) in the biliary excretion of pitavastatin. Mol Pharmacol 2005b;68:800-7.
Hirano M, Maeda K, Shitara Y, Sugiyama Y. Drug-drug interaction between pitavastatin and variousdrugs via OATP1B1. Drug Metab Dispos 2006;34:1229-36.
Ho RH, Kim RB. Transporters and drug therapy: implications for drug disposition and disease. ClinPharmacol Ther 2005;78:260-77.
Ho RH, Tirona RG, Leake BF, Glaeser H, Lee W, Lemke CJ, Wang Y, Kim RB. Drug and bile acidtransporters in rosuvastatin hepatic uptake: function, expression, and pharmacogenetics.Gastroenterology 2006;130:1793-806.
Ho RH, Choi L, Lee W, Mayo G, Schwarz UI, Tirona RG, Bailey DG, Michael Stein C, Kim RB.Effect of drug transporter genotypes on pravastatin disposition in European- and African-Americanparticipants. Pharmacogenet Genomics 2007;17:647-56.
Hsiang B, Zhu Y, Wang Z, Wu Y, Sasseville V, Yang WP, Kirchgessner TG. A novel human hepaticorganic anion transporting polypeptide (OATP2). Identification of a liver-specific human organic aniontransporting polypeptide and identification of rat and human hydroxymethylglutaryl-CoA reductaseinhibitor transporters. J Biol Chem 1999;274:37161-8.
Huang CS, Huang MJ, Lin MS, Yang SS, Teng HC, Tang KS. Genetic factors related tounconjugated hyperbilirubinemia amongst adults. Pharmacogenet Genomics 2005;15:43-50.
Huang L, Wang Y, Grimm S. ATP-dependent transport of rosuvastatin in membrane vesiclesexpressing breast cancer resistance protein. Drug Metab Dispos 2006;34:738-42.
Huang MJ, Kua KE, Teng HC, Tang KS, Weng HW, Huang CS. Risk factors for severehyperbilirubinemia in neonates. Pediatr Res 2004;56:682-9.
Huff MW. Dietary cholesterol, cholesterol absorption, postprandial lipemia and atherosclerosis. Can JClin Pharmacol 2003;10 Suppl A:26A-32A.
Huff MW, Pollex RL, Hegele RA. NPC1L1: evolution from pharmacological target to physiologicalsterol transporter. Arterioscler Thromb Vasc Biol 2006;26:2433-8
Hutz MH, Fiegenbaum M. Impact of Genetic Polymorphisms on the Efficacy of HMG-CoA ReductaseInhibitors. Am J Cardiovasc Drugs 2008;8:161-70.
Ichimaru N, Takahara S, Kokado Y, Wang JD, Hatori M, Kameoka H, Inoue T, Okuyama A.Changes in lipid metabolism and effect of simvastatin in renal transplant recipients induced bycyclosporine or tacrolimus. Atherosclerosis 2001;158:417-23.

REFERENCES
90
Ieiri I, Suzuki H, Kimura M, Takane H, Nishizato Y, Irie S, Urae A, Kawabata K, Higuchi S,Otsubo K, Sugiyama Y. Influence of common variants in the pharmacokinetic genes (OATP-C,UGT1A1, and MRP2) on serum bilirubin levels in healthy subjects. Hepatol Res 2004;30:91-95.
Igel M, Sudhop T, von Bergmann K. Pharmacology of 3-hydroxy-3-methylglutaryl-coenzyme Areductase inhibitors (statins), including rosuvastatin and pitavastatin. J Clin Pharmacol 2002;42:835-45.
Igel M, Arnold KA, Niemi M, Hofmann U, Schwab M, Lütjohann D, von Bergmann K,Eichelbaum M, Kivistö KT. Impact of the SLCO1B1 polymorphism on the pharmacokinetics and lipid-lowering efficacy of multiple-dose pravastatin. Clin Pharmacol Ther 2006;79:419-26.
Iida A, Saito S, Sekine A, Mishima C, Kondo K, Kitamura Y, Harigae S, Osawa S, Nakamura Y.Catalog of 258 single-nucleotide polymorphisms (SNPs) in genes encoding three organic aniontransporters, three organic anion-transporting polypeptides, and three NADH:ubiquinone oxidoreductaseflavoproteins. J Hum Genet 2001;46:668-83.
Inui KI, Masuda S, Saito H. Cellular and molecular aspects of drug transport in the kidney. Kidney Int2000;58:944-58.
Istvan ES, Deisenhofer J. Structural mechanism for statin inhibition of HMG-CoA reductase. Science2001;292:1160-4.
Iwai M, Suzuki H, Ieiri I, Otsubo K, Sugiyama Y. Functional analysis of single nucleotidepolymorphisms of hepatic organic anion transporter OATP1B1 (OATP-C). Pharmacogenetics2004;14:749-57.
Jacobsen W, Kuhn B, Soldner A, Kirchner G, Sewing KF, Kollman PA, Benet LZ, Christians U.Lactonization is the critical first step in the disposition of the 3-hydroxy-3-methylglutaryl-CoA reductaseinhibitor atorvastatin. Drug Metab Dispos 2000;28:1369-78.
Jada SR, Xiaochen S, Yan LY, Xiaoqiang X, Lal S, Zhou SF, Ooi LL, Chowbay B.Pharmacogenetics of SLCO1B1: haplotypes, htSNPs and hepatic expression in three distinct Asianpopulations. Eur J Clin Pharmacol 2007;63:555-63.
Jigorel E, Le Vee M, Boursier-Neyret C, Parmentier Y, Fardel O. Differential regulation ofsinusoidal and canalicular hepatic drug transporter expression by xenobiotics activating drug-sensingreceptors in primary human hepatocytes. Drug Metab Dispos 2006;34:1756-63.
Jones P, Kafonek S, Laurora I, Hunninghake D. Comparative dose efficacy study of atorvastatinversus simvastatin, pravastatin, lovastatin, and fluvastatin in patients with hypercholesterolemia (theCURVES study). Am J Cardiol 1998;81:582-7.
Josephy DP, Guengerich PF, Miners JO. "Phase I and Phase II" drug metabolism: terminology that weshould phase out? Drug Metab Rev 2005;37:575-80.
Kajinami K, Brousseau ME, Ordovas JM, Schaefer EJ. CYP3A4 genotypes and plasma lipoproteinlevels before and after treatment with atorvastatin in primary hypercholesterolemia. Am J Cardiol2004a;93:104-7.
Kajinami K, Brousseau ME, Ordovas JM, Schaefer EJ. Polymorphisms in the multidrug resistance-1(MDR1) gene influence the response to atorvastatin treatment in a gender-specific manner. Am J Cardiol2004b;93:1046-50.

REFERENCES
91
Kajosaari LI, Niemi M, Neuvonen M, Laitila J, Neuvonen PJ, Backman JT. Cyclosporine markedlyraises the plasma concentrations of repaglinide. Clin Pharmacol Ther 2005;78:388-99.
Kalliokoski A, Backman JT, Neuvonen PJ, Niemi M. Effects of the SLCO1B1*1B haplotype on thepharmacokinetics and pharmacodynamics of repaglinide and nateglinide. Pharmacogenet Genomics2008a;in press:
Kalliokoski A, Neuvonen M, Neuvonen PJ, Niemi M. Different effects of SLCO1B1 polymorphism onthe pharmacokinetics and pharmacodynamics of repaglinide and nateglinide. J Clin Pharmacol2008b;48:311-21.
Kameyama Y, Yamashita K, Kobayashi K, Hosokawa M, Chiba K. Functional characterization ofSLCO1B1 (OATP-C) variants, SLCO1B1*5, SLCO1B1*15 and SLCO1B1*15+C1007G, by usingtransient expression systems of HeLa and HEK293 cells. Pharmacogenet Genomics 2005;15:513-22.
Kantola T, Kivistö KT, Neuvonen PJ. Effect of itraconazole on the pharmacokinetics of atorvastatin.Clin Pharmacol Ther 1998;64:58-65.
Kantola T, Backman JT, Niemi M, Kivistö KT, Neuvonen PJ. Effect of fluconazole on plasmafluvastatin and pravastatin concentrations. Eur J Clin Pharmacol 2000;56:225-9.
Katz DA, Carr R, Grimm DR, Xiong H, Holley-Shanks R, Mueller T, Leake B, Wang Q, Han L,Wang PG, Edeki T, Sahelijo L, Doan T, Allen A, Spear BB, Kim RB. Organic anion transportingpolypeptide 1B1 activity classified by SLCO1B1 genotype influences atrasentan pharmacokinetics. ClinPharmacol Ther 2006;79:186-96.
Kearney AS, Crawford LF, Mehta SC, Radebaugh GW. The interconversion kinetics, equilibrium,and solubilities of the lactone and hydroxyacid forms of the HMG-CoA reductase inhibitor, CI-981.Pharm Res 1993;10:1461-5.
Keppler D, Leier I, Jedlitschky G. Transport of glutathione conjugates and glucuronides by themultidrug resistance proteins MRP1 and MRP2. Biol Chem 1997;378:787-91.
Kerb R. Implications of genetic polymorphisms in drug transporters for pharmacotherapy. Cancer Lett2006;234:4-33.
Kesäniemi YA, Tarpila S, Miettinen TA. Low vs high dietary fiber and serum, biliary, and fecal lipidsin middle-aged men. Am J Clin Nutr 1990;51:1007-12.
Kim RB, Wandel C, Leake B, Cvetkovic M, Fromm MF, Dempsey PJ, Roden MM, Belas F,Chaudhary AK, Roden DM, Wood AJ, Wilkinson GR. Interrelationship between substrates andinhibitors of human CYP3A and P-glycoprotein. Pharm Res 1999;16:408-14.
Kirchheiner J, Kudlicz D, Meisel C, Bauer S, Meineke I, Roots I, Brockmöller J. Influence ofCYP2C9 polymorphisms on the pharmacokinetics and cholesterol-lowering activity of (-)-3S,5R-fluvastatin and (+)-3R,5S-fluvastatin in healthy volunteers. Clin Pharmacol Ther 2003;74:186-94.
Kitamura S, Maeda K, Sugiyama Y. Recent progresses in the experimental methods and evaluationstrategies of transporter functions for the prediction of the pharmacokinetics in humans. NaunynSchmiedebergs Arch Pharmacol 2008a;377:617-28.
Kitamura S, Maeda K, Wang Y, Sugiyama Y. Involvement of multiple transporters in thehepatobiliary transport of rosuvastatin. Drug Metab Dispos 2008b;

REFERENCES
92
Kivistö KT, Bookjans G, Fromm MF, Griese EU, Münzel P, Kroemer HK. Expression of CYP3A4,CYP3A5 and CYP3A7 in human duodenal tissue. Br J Clin Pharmacol 1996a;42:387-9.
Kivistö KT, Griese EU, Fritz P, Linder A, Hakkola J, Raunio H, Beaune P, Kroemer HK.Expression of cytochrome P 450 3A enzymes in human lung: a combined RT-PCR andimmunohistochemical analysis of normal tissue and lung tumours. Naunyn Schmiedebergs ArchPharmacol 1996b;353:207-12.
Kivistö KT, Kantola T, Neuvonen PJ. Different effects of itraconazole on the pharmacokinetics offluvastatin and lovastatin. Br J Clin Pharmacol 1998;46:49-53.
Kivistö KT, Niemi M, Fromm MF. Functional interaction of intestinal CYP3A4 and P-glycoprotein.Fundam Clin Pharmacol 2004a;18:621-6.
Kivistö KT, Niemi M, Schaeffeler E, Pitkälä K, Tilvis R, Fromm MF, Schwab M, Eichelbaum M,Strandberg T. Lipid-lowering response to statins is affected by CYP3A5 polymorphism.Pharmacogenetics 2004b;14:523-5.
Koepsell H, Endou H. The SLC22 drug transporter family. Pflugers Arch 2004;447:666-76.
Koepsell H, Lips K, Volk C. Polyspecific organic cation transporters: structure, function, physiologicalroles, and biopharmaceutical implications. Pharm Res 2007;24:1227-51.
Koop I, Schindler M, Bosshammer A, Scheibner J, Stange E, Koop H. Physiological control ofcholecystokinin release and pancreatic enzyme secretion by intraduodenal bile acids. Gut 1996;39:661-7.
Kopplow K, Letschert K, König J, Walter B, Keppler D. Human hepatobiliary transport of organicanions analyzed by quadruple-transfected cells. Mol Pharmacol 2005;68:1031-8.
Kreisberg RA, Oberman A. Clinical review 141: lipids and atherosclerosis: lessons learned fromrandomized controlled trials of lipid lowering and other relevant studies. J Clin Endocrinol Metab2002;87:423-37.
Krishna DR, Klotz U. Extrahepatic metabolism of drugs in humans. Clin Pharmacokinet 1994;26:144-60.
Kroetz DL, Pauli-Magnus C, Hodges LM, Huang CC, Kawamoto M, Johns SJ, Stryke D, FerrinTE, DeYoung J, Taylor T, Carlson EJ, Herskowitz I, Giacomini KM, Clark AG. Sequence diversityand haplotype structure in the human ABCB1 (MDR1, multidrug resistance transporter) gene.Pharmacogenetics 2003;13:481-94.
Kullak-Ublick GA, Hagenbuch B, Stieger B, Schteingart CD, Hofmann AF, Wolkoff AW, MeierPJ. Molecular and functional characterization of an organic anion transporting polypeptide cloned fromhuman liver. Gastroenterology 1995;109:1274-82.
Kullak-Ublick GA, Ismair MG, Stieger B, Landmann L, Huber R, Pizzagalli F, Fattinger K, MeierPJ, Hagenbuch B. Organic anion-transporting polypeptide B (OATP-B) and its functional comparisonwith three other OATPs of human liver. Gastroenterology 2001;120:525-33.
Kullak-Ublick GA, Stieger B, Meier PJ. Enterohepatic bile salt transporters in normal physiology andliver disease. Gastroenterology 2004;126:322-42.
Kyrklund C, Backman JT, Kivistö KT, Neuvonen M, Laitila J, Neuvonen PJ. Rifampin greatlyreduces plasma simvastatin and simvastatin acid concentrations. Clin Pharmacol Ther 2000;68:592-7.

REFERENCES
93
Kyrklund C, Backman JT, Kivistö KT, Neuvonen M, Laitila J, Neuvonen PJ. Plasma concentrationsof active lovastatin acid are markedly increased by gemfibrozil but not by bezafibrate. Clin PharmacolTher 2001;69:340-5.
Kyrklund C, Backman JT, Neuvonen M, Neuvonen PJ. Gemfibrozil increases plasma pravastatinconcentrations and reduces pravastatin renal clearance. Clin Pharmacol Ther 2003;73:538-44.
Kyrklund C, Backman JT, Neuvonen M, Neuvonen PJ. Effect of rifampicin on pravastatinpharmacokinetics in healthy subjects. Br J Clin Pharmacol 2004;57:181-7.
König J, Cui Y, Nies AT, Keppler D. A novel human organic anion transporting polypeptide localizedto the basolateral hepatocyte membrane. Am J Physiol Gastrointest Liver Physiol 2000;278:G156-64.
König J, Seithel A, Gradhand U, Fromm MF. Pharmacogenomics of human OATP transporters.Naunyn Schmiedebergs Arch Pharmacol 2006;372:432-43.
Laaksonen R. On the mechanisms of statin-induced myopathy. Clin Pharmacol Ther 2006;79:529-31.
Laaksonen R, Katajamaa M, Päivä H, Sysi-Aho M, Saarinen L, Junni P, Lütjohann D, Smet J,Van Coster R, Seppänen-Laakso T, Lehtimäki T, Soini J, Oresic M. A systems biology strategyreveals biological pathways and plasma biomarker candidates for potentially toxic statin-inducedchanges in muscle. PLoS ONE 2006;1:e97.
Laaksonen R, Janis MT, Oresic M. Lipidomics-based safety biomarkers for lipid-lowering treatments.Angiology 2008;59:65S-8S.
Lamba JK, Lin YS, Schuetz EG, Thummel KE. Genetic contribution to variable human CYP3A-mediated metabolism. Adv Drug Deliv Rev 2002;54:1271-94.
LaRosa JC, He J, Vupputuri S. Effect of statins on risk of coronary disease: a meta-analysis ofrandomized controlled trials. Jama 1999;282:2340-6.
Lau YY, Huang Y, Frassetto L, Benet LZ. Effect of OATP1B Transporter Inhibition on thePharmacokinetics of Atorvastatin in Healthy Volunteers. Clin Pharmacol Ther 2006;[Epub ahead ofprint].
Lau YY, Huang Y, Frassetto L, Benet LZ. Effect of OATP1B transporter inhibition on thepharmacokinetics of atorvastatin in healthy volunteers. Clin Pharmacol Ther 2007;81:194-204.
Law M, Rudnicka AR. Statin safety: a systematic review. Am J Cardiol 2006;97:52C-60C.
Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on low density lipoprotein cholesterol,ischaemic heart disease, and stroke: systematic review and meta-analysis. Bmj 2003;326:1423.
Leabman MK, Huang CC, Kawamoto M, Johns SJ, Stryke D, Ferrin TE, DeYoung J, Taylor T,Clark AG, Herskowitz I, Giacomini KM. Polymorphisms in a human kidney xenobiotic transporter,OCT2, exhibit altered function. Pharmacogenetics 2002;12:395-405.
Lee E, Ryan S, Birmingham B, Zalikowski J, March R, Ambrose H, Moore R, Lee C, Chen Y,Schneck D. Rosuvastatin pharmacokinetics and pharmacogenetics in white and Asian subjects residingin the same environment. Clin Pharmacol Ther 2005a;78:330-41.

REFERENCES
94
Lee W, Glaeser H, Smith LH, Roberts RL, Moeckel GW, Gervasini G, Leake BF, Kim RB.Polymorphisms in human organic anion-transporting polypeptide 1A2 (OATP1A2): implications foraltered drug disposition and central nervous system drug entry. J Biol Chem 2005b;280:9610-7.
Leijd B. The effect of weight reduction on biliary lipid metabolism in patients with hyperlipoproteinemiatype IV. Metabolism 1981;30:1185-9.
Lennernäs H, Fager G. Pharmacodynamics and pharmacokinetics of the HMG-CoA reductaseinhibitors. Similarities and differences. Clin Pharmacokinet 1997;32:403-25.
Lennernäs H. Clinical pharmacokinetics of atorvastatin. Clin Pharmacokinet 2003;42:1141-60.
Leschziner GD, Andrew T, Pirmohamed M, Johnson MR. ABCB1 genotype and PGP expression,function and therapeutic drug response: a critical review and recommendations for future research.Pharmacogenomics J 2007;7:154-79.
Lewis DF. 57 varieties: the human cytochromes P450. Pharmacogenomics 2004;5:305-18.
Li L, Lee TK, Meier PJ, Ballatori N. Identification of glutathione as a driving force and leukotriene C4as a substrate for oatp1, the hepatic sinusoidal organic solute transporter. J Biol Chem 1998;273:16184-91.
Li L, Meier PJ, Ballatori N. Oatp2 mediates bidirectional organic solute transport: a role forintracellular glutathione. Mol Pharmacol 2000;58:335-40.
Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol 2002;86:5-18.
Lin JH, Yamazaki M. Role of P-glycoprotein in pharmacokinetics: clinical implications. ClinPharmacokinet 2003;42:59-98.
Lin MC, Kramer W, Wilson FA. Identification of cytosolic and microsomal bile acid-binding proteinsin rat ileal enterocytes. J Biol Chem 1990;265:14986-95.
Littarru GP, Langsjoen P. Coenzyme Q10 and statins: biochemical and clinical implications.Mitochondrion 2007;7 Suppl:S168-74.
Liu L, Cui Y, Chung AY, Shitara Y, Sugiyama Y, Keppler D, Pang KS. Vectorial transport ofenalapril by Oatp1a1/Mrp2 and OATP1B1 and OATP1B3/MRP2 in rat and human livers. J PharmacolExp Ther 2006;318:395-402.
Lockhart AC, Tirona RG, Kim RB. Pharmacogenetics of ATP-binding cassette transporters in cancerand chemotherapy. Mol Cancer Ther 2003;2:685-98.
Läpple F, von Richter O, Fromm MF, Richter T, Thon KP, Wisser H, Griese EU, Eichelbaum M,Kivistö KT. Differential expression and function of CYP2C isoforms in human intestine and liver.Pharmacogenetics 2003;13:565-75.
Maeda K, Ieiri I, Yasuda K, Fujino A, Fujiwara H, Otsubo K, Hirano M, Watanabe T, KitamuraY, Kusuhara H, Sugiyama Y. Effects of organic anion transporting polypeptide 1B1 haplotype onpharmacokinetics of pravastatin, valsartan, and temocapril. Clin Pharmacol Ther 2006a;79:427-39.

REFERENCES
95
Maeda K, Kambara M, Tian Y, Hofmann AF, Sugiyama Y. Uptake of ursodeoxycholate and itsconjugates by human hepatocytes: role of Na(+)-taurocholate cotransporting polypeptide (NTCP),organic anion transporting polypeptide (OATP) 1B1 (OATP-C), and oatp1B3 (OATP8). Mol Pharm2006b;3:70-7.
Maeda K, Sugiyama Y. Impact of genetic polymorphisms of transporters on the pharmacokinetic,pharmacodynamic and toxicological properties of anionic drugs. Drug Metab Pharmacokinet2008;23:223-35.
Mahley RW, Bersot TP. Drug therapy of dyslipidemia. In: Brunton LL, Lazo JS, Parker KL. Goodmanand Gillman's the pharmacological basis of therapeutics. New York: McGraw-Hill; 2006.
Martini C, Pallottini V. Cholesterol: from feeding to gene regulation. Genes Nutr 2007;2:181-93.
Matsushima S, Maeda K, Kondo C, Hirano M, Sasaki M, Suzuki H, Sugiyama Y. Identification ofthe hepatic efflux transporters of organic anions using double-transfected Madin-Darby canine kidney IIcells expressing human organic anion-transporting polypeptide 1B1 (OATP1B1)/multidrug resistance-associated protein 2, OATP1B1/multidrug resistance 1, and OATP1B1/breast cancer resistance protein. JPharmacol Exp Ther 2005;314:1059-67.
Matsushima S, Maeda K, Ishiguro N, Igarashi T, Sugiyama Y. Investigation of the inhibitory effectsof various drugs on the hepatic uptake of fexofenadine in humans. Drug Metab Dispos 2008;36:663-9.
McTaggart F, Buckett L, Davidson R, Holdgate G, McCormick A, Schneck D, Smith G, WarwickM. Preclinical and clinical pharmacology of Rosuvastatin, a new 3-hydroxy-3-methylglutaryl coenzymeA reductase inhibitor. Am J Cardiol 2001;87:28B-32B.
Meier PJ, Eckhardt U, Schroeder A, Hagenbuch B, Stieger B. Substrate specificity of sinusoidal bileacid and organic anion uptake systems in rat and human liver. Hepatology 1997;26:1667-77.
Meier PJ, Stieger B. Bile salt transporters. Annu Rev Physiol 2002;64:635-61.
Meier Y, Eloranta JJ, Darimont J, Ismair MG, Hiller C, Fried M, Kullak-Ublick GA, VavrickaSR. Regional distribution of solute carrier mRNA expression along the human intestinal tract. DrugMetab Dispos 2007;35:590-4.
Meier-Abt F, Faulstich H, Hagenbuch B. Identification of phalloidin uptake systems of rat and humanliver. Biochim Biophys Acta 2004;1664:64-9.
Meier-Abt F, Mokrab Y, Mizuguchi K. Organic anion transporting polypeptides of the OATP/SLCOsuperfamily: identification of new members in nonmammalian species, comparative modeling and apotential transport mode. J Membr Biol 2005;208:213-27.
Merino G, van Herwaarden AE, Wagenaar E, Jonker JW, Schinkel AH. Sex-dependent expressionand activity of the ATP-binding cassette transporter breast cancer resistance protein (BCRP/ABCG2) inliver. Mol Pharmacol 2005;67:1765-71.
Meyer UA. Overview of enzymes of drug metabolism. J Pharmacokinet Biopharm 1996;24:449-59.
Michalski C, Cui Y, Nies AT, Nuessler AK, Neuhaus P, Zanger UM, Klein K, Eichelbaum M,Keppler D, König J. A naturally occurring mutation in the SLC21A6 gene causing impaired membranelocalization of the hepatocyte uptake transporter. J Biol Chem 2002;277:43058-63.
Miettinen TA. Detection of changes in human cholesterol metabolism. Ann Clin Res 1970;2:300-20.
REFERENCES
96
Miettinen TA. Cholesterol production in obesity. Circulation 1971;44:842-50.
Miettinen TA. Diurnal variation of LDL and HDL cholesterol. Ann Clin Res 1980;12:295-8.
Miettinen TA, Kesäniemi YA, Järvinen H, Hastbacka J. Cholesterol precursor sterols, plant sterols,and cholestanol in human bile and gallstones. Gastroenterology 1986;90:858-64.
Miettinen TA, Tilvis RS, Kesäniemi YA. Serum cholestanol and plant sterol levels in relation tocholesterol metabolism in middle-aged men. Metabolism 1989;38:136-40.
Miettinen TA, Tilvis RS, Kesäniemi YA. Serum plant sterols and cholesterol precursors reflectcholesterol absorption and synthesis in volunteers of a randomly selected male population. Am JEpidemiol 1990;131:20-31.
Miettinen TA, Gylling H, Vanhanen H, Ollus A. Cholesterol absorption, elimination, and synthesisrelated to LDL kinetics during varying fat intake in men with different apoprotein E phenotypes.Arterioscler Thromb 1992;12:1044-52.
Miettinen TA, Vanhanen H. Serum concentration and metabolism of cholesterol during rapeseed oiland squalene feeding. Am J Clin Nutr 1994;59:356-63.
Miettinen TA, Strandberg TE, Gylling H. Noncholesterol sterols and cholesterol lowering by long-term simvastatin treatment in coronary patients: relation to basal serum cholestanol. Arterioscler ThrombVasc Biol 2000;20:1340-6.
Mikkaichi T, Suzuki T, Tanemoto M, Ito S, Abe T. The organic anion transporter (OATP) family.Drug Metab Pharmacokinet 2004;19:171-9.
Miners JO, Birkett DJ. Cytochrome P4502C9: an enzyme of major importance in human drugmetabolism. Br J Clin Pharmacol 1998;45:525-38.
Morimoto K, Oishi T, Ueda S, Ueda M, Hosokawa M, Chiba K. A novel variant allele of OATP-C(SLCO1B1) found in a Japanese patient with pravastatin-induced myopathy. Drug Metab Pharmacokinet2004;19:453-5.
Morimoto K, Ueda S, Seki N, Igawa Y, Kameyama Y, Shimizu A, Oishi T, Hosokawa M, Iesato K,Mori S, Saito Y, Chiba K. OATP-C(OATP01B1)*15 is associated with statin-induced myopathy inhypercholesterolemic patients. Clin Pharmacol Ther 2005;77:21.
Muck W, Mai I, Fritsche L, Ochmann K, Rohde G, Unger S, Johne A, Bauer S, Budde K, Roots I,Neumayer HH, Kuhlmann J. Increase in cerivastatin systemic exposure after single and multipledosing in cyclosporine-treated kidney transplant recipients. Clin Pharmacol Ther 1999;65:251-61.
Mwinyi J, Johne A, Bauer S, Roots I, Gerloff T. Evidence for inverse effects of OATP-C (SLC21A6)5 and 1b haplotypes on pravastatin kinetics. Clin Pharmacol Ther 2004;75:415-21.
Mwinyi J, Kopke K, Schaefer M, Roots I, Gerloff T. Comparison of SLCO1B1 sequence variabilityamong German, Turkish, and African populations. Eur J Clin Pharmacol 2008;64:257-66.
Mölsä M, Heikkinen T, Hakkola J, Hakala K, Wallerman O, Wadelius M, Wadelius C, Laine K.Functional role of P-glycoprotein in the human blood-placental barrier. Clin Pharmacol Ther2005;78:123-31.

REFERENCES
97
Nakagomi-Hagihara R, Nakai D, Kawai K, Yoshigae Y, Tokui T, Abe T, Ikeda T. OATP1B1,OATP1B3, and mrp2 are involved in hepatobiliary transport of olmesartan, a novel angiotensin IIblocker. Drug Metab Dispos 2006;34:862-9.
Nakai D, Nakagomi R, Furuta Y, Tokui T, Abe T, Ikeda T, Nishimura K. Human liver-specificorganic anion transporter, LST-1, mediates uptake of pravastatin by human hepatocytes. J PharmacolExp Ther 2001;297:861-7.
Nakamura Y. Pharmacogenomics and Drug Toxicity. N Engl J Med 2008;
Nebert DW, Russell DW. Clinical importance of the cytochromes P450. Lancet 2002;360:1155-62.
Neuvonen PJ, Kantola T, Kivistö KT. Simvastatin but not pravastatin is very susceptible to interactionwith the CYP3A4 inhibitor itraconazole. Clin Pharmacol Ther 1998;63:332-41.
Neuvonen PJ, Niemi M, Backman JT. Drug interactions with lipid-lowering drugs: mechanisms andclinical relevance. Clin Pharmacol Ther 2006;80:565-81.
Niemi M, Backman JT, Fromm MF, Neuvonen PJ, Kivistö KT. Pharmacokinetic interactions withrifampicin : clinical relevance. Clin Pharmacokinet 2003a;42:819-50.
Niemi M, Backman JT, Neuvonen M, Neuvonen PJ. Effects of gemfibrozil, itraconazole, and theircombination on the pharmacokinetics and pharmacodynamics of repaglinide: potentially hazardousinteraction between gemfibrozil and repaglinide. Diabetologia 2003b;46:347-51.
Niemi M, Schaeffeler E, Lang T, Fromm MF, Neuvonen M, Kyrklund C, Backman JT, Kerb R,Schwab M, Neuvonen PJ, Eichelbaum M, Kivistö KT. High plasma pravastatin concentrations areassociated with single nucleotide polymorphisms and haplotypes of organic anion transportingpolypeptide-C (OATP-C, SLCO1B1). Pharmacogenetics 2004;14:429-40.
Niemi M, Backman JT, Kajosaari LI, Leathart JB, Neuvonen M, Daly AK, Eichelbaum M, KivistöKT, Neuvonen PJ. Polymorphic organic anion transporting polypeptide 1B1 is a major determinant ofrepaglinide pharmacokinetics. Clin Pharmacol Ther 2005a;77:468-78.
Niemi M, Kivistö KT, Hofmann U, Schwab M, Eichelbaum M, Fromm MF. Fexofenadinepharmacokinetics are associated with a polymorphism of the SLCO1B1 gene (encoding OATP1B1). Br JClin Pharmacol 2005b;59:602-4.
Niemi M, Neuvonen PJ, Hofmann U, Backman JT, Schwab M, Lütjohann D, von Bergmann K,Eichelbaum M, Kivistö KT. Acute effects of pravastatin on cholesterol synthesis are associated withSLCO1B1 (encoding OATP1B1) haplotype *17. Pharmacogenet Genomics 2005c;15:303-9.
Niemi M, Arnold KA, Backman JT, Pasanen MK, Godtel-Armbrust U, Wojnowski L, Zanger UM,Neuvonen PJ, Eichelbaum M, Kivistö KT, Lang T. Association of genetic polymorphism in ABCC2with hepatic multidrug resistance-associated protein 2 expression and pravastatin pharmacokinetics.Pharmacogenet Genomics 2006;16:801-8.
Niemi M. Role of OATP transporters in the disposition of drugs. Pharmacogenomics 2007;8:787-802.
Nies AT, Keppler D. The apical conjugate efflux pump ABCC2 (MRP2). Pflugers Arch 2007;453:643-59.
Nishizato Y, Ieiri I, Suzuki H, Kimura M, Kawabata K, Hirota T, Takane H, Irie S, Kusuhara H,Urasaki Y, Urae A, Higuchi S, Otsubo K, Sugiyama Y. Polymorphisms of OATP-C (SLC21A6) and

REFERENCES
98
OAT3 (SLC22A8) genes: consequences for pravastatin pharmacokinetics. Clin Pharmacol Ther2003;73:554-65.
Noe J, Stieger B, Meier PJ. Functional expression of the canalicular bile salt export pump of humanliver. Gastroenterology 2002;123:1659-66.
Nozawa T, Nakajima M, Tamai I, Noda K, Nezu J, Sai Y, Tsuji A, Yokoi T. Genetic polymorphismsof human organic anion transporters OATP-C (SLC21A6) and OATP-B (SLC21A9): allele frequenciesin the Japanese population and functional analysis. J Pharmacol Exp Ther 2002;302:804-13.
Nozawa T, Tamai I, Sai Y, Nezu J, Tsuji A. Contribution of organic anion transporting polypeptideOATP-C to hepatic elimination of the opioid pentapeptide analogue [D-Ala2, D-Leu5]-enkephalin. JPharm Pharmacol 2003;55:1013-20.
Nozawa T, Imai K, Nezu J, Tsuji A, Tamai I. Functional characterization of pH-sensitive organicanion transporting polypeptide OATP-B in human. J Pharmacol Exp Ther 2004a;308:438-45.
Nozawa T, Sugiura S, Nakajima M, Goto A, Yokoi T, Nezu J, Tsuji A, Tamai I. Involvement oforganic anion transporting polypeptides in the transport of troglitazone sulfate: implications forunderstanding troglitazone hepatotoxicity. Drug Metab Dispos 2004b;32:291-4.
Nozawa T, Minami H, Sugiura S, Tsuji A, Tamai I. Role of organic anion transporter OATP1B1(OATP-C) in hepatic uptake of irinotecan and its active metabolite, 7-ethyl-10-hydroxycamptothecin: invitro evidence and effect of single nucleotide polymorphisms. Drug Metab Dispos 2005;33:434-9.
Olbricht C, Wanner C, Eisenhauer T, Kliem V, Doll R, Boddaert M, O'Grady P, Krekler M,Mangold B, Christians U. Accumulation of lovastatin, but not pravastatin, in the blood of cyclosporine-treated kidney graft patients after multiple doses. Clin Pharmacol Ther 1997;62:311-21.
Omura T, Sato R. A new cytochrome in liver microsomes. J Biol Chem 1962;237:1375-6.
Oswald S, König J, Lütjohann D, Giessmann T, Kroemer HK, Rimmbach C, Rosskopf D, FrommMF, Siegmund W. Disposition of ezetimibe is influenced by polymorphisms of the hepatic uptakecarrier OATP1B1. Pharmacogenet Genomics 2008;18:559-68.
Owczarek J, Jasinska M, Orszulak-Michalak D. Drug-induced myopathies. An overview of thepossible mechanisms. Pharmacol Rep 2005;57:23-34.
Pan HY, DeVault AR, Brescia D, Willard DA, McGovern ME, Whigan DB, Ivashkiv E. Effect offood on pravastatin pharmacokinetics and pharmacodynamics. Int J Clin Pharmacol Ther Toxicol1993;31:291-4.
Pang KS, Rowland M. Hepatic clearance of drugs. I. Theoretical considerations of a "well-stirred"model and a "parallel tube" model. Influence of hepatic blood flow, plasma and blood cell binding, andthe hepatocellular enzymatic activity on hepatic drug clearance. J Pharmacokinet Biopharm 1977;5:625-53.
Park JW, Siekmeier R, Lattke P, Merz M, Mix C, Schuler S, Jaross W. Pharmacokinetics andpharmacodynamics of fluvastatin in heart transplant recipients taking cyclosporine A. J CardiovascPharmacol Ther 2001;6:351-61.
Pasternak RC, Smith SC, Jr., Bairey-Merz CN, Grundy SM, Cleeman JI, Lenfant C.ACC/AHA/NHLBI Clinical Advisory on the Use and Safety of Statins. Circulation 2002;106:1024-8.

REFERENCES
99
Pazzucconi F, Dorigotti F, Gianfranceschi G, Campagnoli G, Sirtori M, Franceschini G, SirtoriCR. Therapy with HMG CoA reductase inhibitors: characteristics of the long-term permanence ofhypocholesterolemic activity. Atherosclerosis 1995;117:189-98.
Petzinger E, Geyer J. Drug transporters in pharmacokinetics. Naunyn Schmiedebergs Arch Pharmacol2006;372:465-75.
Phillips PS, Haas RH, Bannykh S, Hathaway S, Gray NL, Kimura BJ, Vladutiu GD, England JD.Statin-associated myopathy with normal creatine kinase levels. Ann Intern Med 2002;137:581-5.
Prueksaritanont T, Subramanian R, Fang X, Ma B, Qiu Y, Lin JH, Pearson PG, Baillie TA.Glucuronidation of statins in animals and humans: a novel mechanism of statin lactonization. DrugMetab Dispos 2002;30:505-12.
Prueksaritanont T, Ma B, Yu N. The human hepatic metabolism of simvastatin hydroxy acid ismediated primarily by CYP3A, and not CYP2D6. Br J Clin Pharmacol 2003;56:120-4.
Päivä H, Thelen KM, Van Coster R, Smet J, De Paepe B, Mattila KM, Laakso J, Lehtimäki T, vonBergmann K, Lütjohann D, Laaksonen R. High-dose statins and skeletal muscle metabolism inhumans: a randomized, controlled trial. Clin Pharmacol Ther 2005;78:60-8.
Raghow R, Yellaturu1 C, Deng X, Park EA, Elam MB. SREBPs: the crossroads of physiological andpathological lipid homeostasis. Trends Endocrinol Metab. 2008;19:65-73.
Ramachandran S, Deshpande O, Roseman CC, Rosenberg NA, Feldman MW, Cavalli-Sforza LL.Support from the relationship of genetic and geographic distance in human populations for a serialfounder effect originating in Africa. Proc Natl Acad Sci U S A 2005;102:15942-7.
Raviv Y, Puri A, Blumenthal R. P-glycoprotein-overexpressing multidrug-resistant cells are resistant toinfection by enveloped viruses that enter via the plasma membrane. Faseb J 2000;14:511-5.
Regazzi MB, Iacona I, Campana C, Raddato V, Lesi C, Perani G, Gavazzi A, Vigano M. Altereddisposition of pravastatin following concomitant drug therapy with cyclosporin A in transplantrecipients. Transplant Proc 1993;25:2732-4.
Riley RJ. The potential pharmacological and toxicological impact of P450 screening. Curr Opin DrugDiscov Devel 2001;4:45-54.
Rizwan AN, Burckhardt G. Organic anion transporters of the SLC22 family: biopharmaceutical,physiological, and pathological roles. Pharm Res 2007;24:450-70.
Rose G, Shipley M. Plasma cholesterol concentration and death from coronary heart disease: 10 yearresults of the Whitehall study. Br Med J (Clin Res Ed) 1986;293:306-7.
Rosenberg NA, Pritchard JK, Weber JL, Cann HM, Kidd KK, Zhivotovsky LA, Feldman MW.Genetic structure of human populations. Science 2002;298:2381-5.
Rosenson RS, Tangney CC. Antiatherothrombotic properties of statins: implications for cardiovascularevent reduction. Jama 1998;279:1643-50.
Rowland M, Tozer TN. Clinical Pharmacokinetics: concepts and applications. Baltimore: Williams &Wilkins; 1995.

REFERENCES
100
Ruokoniemi P, Helin-Salmivaara A, Klaukka T, Neuvonen PJ, Huupponen R. Shift of statin usetowards the elderly in 1995-2005: a nation-wide register study in Finland. Br J Clin Pharmacol2008;66:405-10.
Russell DW. Nuclear orphan receptors control cholesterol catabolism. Cell 1999;97:539-42.
Sabia H, Prasad P, Smith HT, Stoltz RR, Rothenberg P. Safety, tolerability, and pharmacokinetics ofan extended-release formulation of fluvastatin administered once daily to patients with primaryhypercholesterolemia. J Cardiovasc Pharmacol 2001;37:502-11.
Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, Brown L, Warnica JW,Arnold JM, Wun CC, Davis BR, Braunwald E. The effect of pravastatin on coronary events aftermyocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events Trialinvestigators. N Engl J Med 1996;335:1001-9.
Sakaeda T, Nakamura T, Okumura K. Pharmacogenetics of drug transporters and its impact on thepharmacotherapy. Curr Top Med Chem 2004;4:1385-98.
Sandhu P, Lee W, Xu X, Leake BF, Yamazaki M, Stone JA, Lin JH, Pearson PG, Kim RB. Hepaticuptake of the novel antifungal agent caspofungin. Drug Metab Dispos 2005;33:676-82.
Sasaki M, Suzuki H, Ito K, Abe T, Sugiyama Y. Transcellular transport of organic anions across adouble-transfected Madin-Darby canine kidney II cell monolayer expressing both human organic anion-transporting polypeptide (OATP2/SLC21A6) and Multidrug resistance-associated protein 2(MRP2/ABCC2). J Biol Chem 2002;277:6497-503.
Satlin LM, Amin V, Wolkoff AW. Organic anion transporting polypeptide mediates organicanion/HCO3- exchange. J Biol Chem 1997;272:26340-5.
Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet1994;344:1383-9.
Schachter M. Chemical, pharmacokinetic and pharmacodynamic properties of statins: an update.Fundam Clin Pharmacol 2005;19:117-25.
Scheffer GL, Kool M, de Haas M, de Vree JM, Pijnenborg AC, Bosman DK, Elferink RP, van derValk P, Borst P, Scheper RJ. Tissue distribution and induction of human multidrug resistant protein 3.Lab Invest 2002;82:193-201.
Schick BA, Laaksonen R, Frohlich JJ, Päivä H, Lehtimäki T, Humphries KH, Cote HC. Decreasedskeletal muscle mitochondrial DNA in patients treated with high-dose simvastatin. Clin Pharmacol Ther2007;81:650-3.
Schneck DW, Birmingham BK, Zalikowski JA, Mitchell PD, Wang Y, Martin PD, Lasseter KC,Brown CD, Windass AS, Raza A. The effect of gemfibrozil on the pharmacokinetics of rosuvastatin.Clin Pharmacol Ther 2004;75:455-63.
Scripture CD, Pieper JA. Clinical pharmacokinetics of fluvastatin. Clin Pharmacokinet 2001;40:263-81.
SEARCH Collaborative Group. SLCO1B1 Variants and Statin-Induced Myopathy -- A GenomewideStudy. N Engl J Med 2008;359:

REFERENCES
101
Seithel A, Eberl S, Singer K, Auge D, Heinkele G, Wolf NB, Dorje F, Fromm MF, König J. Theinfluence of macrolide antibiotics on the uptake of organic anions and drugs mediated by OATP1B1 andOATP1B3. Drug Metab Dispos 2007;35:779-86.
Seithel A, Glaeser H, Fromm MF, König J. The functional consequences of genetic variations intransporter genes encoding human organic anion-transporting polypeptide family members. Expert OpinDrug Metab Toxicol 2008a;4:51-64.
Seithel A, Klein K, Zanger UM, Fromm MF, König J. Non-synonymous polymorphisms in the humanSLCO1B1 gene: an in vitro analysis of SNP c.1929A>C. Mol Genet Genomics 2008b;279:149-57.
Shen DD, Kunze KL, Thummel KE. Enzyme-catalyzed processes of first-pass hepatic and intestinaldrug extraction. Adv Drug Deliv Rev 1997;27:99-127.
Shepherd J, Cobbe SM, Ford I, Isles CG, Lorimer AR, MacFarlane PW, McKillop JH, PackardCJ. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West ofScotland Coronary Prevention Study Group. N Engl J Med 1995;333:1301-7.
Shitara Y, Itoh T, Sato H, Li AP, Sugiyama Y. Inhibition of transporter-mediated hepatic uptake as amechanism for drug-drug interaction between cerivastatin and cyclosporin A. J Pharmacol Exp Ther2003;304:610-6.
Shitara Y, Sato H, Sugiyama Y. Evaluation of drug-drug interaction in the hepatobiliary and renaltransport of drugs. Annu Rev Pharmacol Toxicol 2005;45:689-723.
Shitara Y, Horie T, Sugiyama Y. Transporters as a determinant of drug clearance and tissuedistribution. Eur J Pharm Sci 2006;27:425-46.
Shitara Y, Sugiyama Y. Pharmacokinetic and pharmacodynamic alterations of 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors: drug-drug interactions and interindividualdifferences in transporter and metabolic enzyme functions. Pharmacol Ther 2006;112:71-105.
Shu Y, Brown C, Castro RA, Shi RJ, Lin ET, Owen RP, Sheardown SA, Yue L, Burchard EG,Brett CM, Giacomini KM. Effect of genetic variation in the organic cation transporter 1, OCT1, onmetformin pharmacokinetics. Clin Pharmacol Ther 2008;83:273-80.
Simonson SG, Raza A, Martin PD, Mitchell PD, Jarcho JA, Brown CD, Windass AS, Schneck DW.Rosuvastatin pharmacokinetics in heart transplant recipients administered an antirejection regimenincluding cyclosporine. Clin Pharmacol Ther 2004;76:167-77.
Spence JD, Munoz CE, Hendricks L, Latchinian L, Khouri HE. Pharmacokinetics of thecombination of fluvastatin and gemfibrozil. Am J Cardiol 1995;76:80A-83A.
Staffa JA, Chang J, Green L. Cerivastatin and reports of fatal rhabdomyolysis. N Engl J Med2002;346:539-40.
Stamler J, Dyer AR, Shekelle RB, Neaton J, Stamler R. Relationship of baseline major risk factors tocoronary and all-cause mortality, and to longevity: findings from long-term follow-up of Chicagocohorts. Cardiology 1993;82:191-222.
Stephens M, Smith NJ, Donnelly P. A new statistical method for haplotype reconstruction frompopulation data. Am J Hum Genet 2001;68:978-89.

REFERENCES
102
Stephens M, Donnelly P. A comparison of bayesian methods for haplotype reconstruction frompopulation genotype data. Am J Hum Genet 2003;73:1162-9.
Stieger B, Meier Y, Meier PJ. The bile salt export pump. Pflugers Arch 2007;453:611-20.
St-Pierre MV, Kullak-Ublick GA, Hagenbuch B, Meier PJ. Transport of bile acids in hepatic andnon-hepatic tissues. J Exp Biol 2001;204:1673-86.
Strandberg TE, Tilvis RS, Miettinen TA. Metabolic variables of cholesterol during squalene feeding inhumans: comparison with cholestyramine treatment. J Lipid Res 1990;31:1637-43.
Strandberg TE, Pitkälä K, Berglind S, Nieminen MS, Tilvis RS. Multifactorial cardiovascular diseaseprevention in patients aged 75 years and older: A randomized controlled trial: Drugs and Evidence BasedMedicine in the Elderly (DEBATE) Study. Am Heart J 2001;142:945-51.
Strandberg TE, Pitkälä KH, Tilvis RS. Statin treatment is associated with clearly reduced mortalityrisk of cardiovascular patients aged 75 years and older. J Gerontol A Biol Sci Med Sci 2008;63:213-4;author reply 214.
Suzuki M, Suzuki H, Sugimoto Y, Sugiyama Y. ABCG2 transports sulfated conjugates of steroids andxenobiotics. J Biol Chem 2003;278:22644-9.
Syme MR, Paxton JW, Keelan JA. Drug transfer and metabolism by the human placenta. ClinPharmacokinet 2004;43:487-514.
Tachibana-Iimori R, Tabara Y, Kusuhara H, Kohara K, Kawamoto R, Nakura J, Tokunaga K,Kondo I, Sugiyama Y, Miki T. Effect of genetic polymorphism of OATP-C (SLCO1B1) on lipid-lowering response to HMG-CoA reductase inhibitors. Drug Metab Pharmacokinet 2004;19:375-80.
Takada T, Weiss HM, Kretz O, Gross G, Sugiyama Y. Hepatic transport of PKI166, an epidermalgrowth factor receptor kinase inhibitor of the pyrrolo-pyrimidine class, and its main metabolite,ACU154. Drug Metab Dispos 2004;32:1272-8.
Takeda M, Noshiro R, Onozato ML, Tojo A, Hasannejad H, Huang XL, Narikawa S, Endou H.Evidence for a role of human organic anion transporters in the muscular side effects of HMG-CoAreductase inhibitors. Eur J Pharmacol 2004;483:133-8.
Tamai I, Nezu J, Uchino H, Sai Y, Oku A, Shimane M, Tsuji A. Molecular identification andcharacterization of novel members of the human organic anion transporter (OATP) family. BiochemBiophys Res Commun 2000;273:251-60.
Tamai I, Nozawa T, Koshida M, Nezu J, Sai Y, Tsuji A. Functional characterization of human organicanion transporting polypeptide B (OATP-B) in comparison with liver-specific OATP-C. Pharm Res2001;18:1262-9.
Tanihara Y, Masuda S, Sato T, Katsura T, Ogawa O, Inui K. Substrate specificity of MATE1 andMATE2-K, human multidrug and toxin extrusions/H(+)-organic cation antiporters. Biochem Pharmacol2007;74:359-71.
Terada T, Inui K. Peptide transporters: structure, function, regulation and application for drug delivery.Curr Drug Metab 2004;5:85-94.
Theuwissen E, Mensink R. Water-soluble dietary fibers and cardiovascular disease. Physiol Behav2008;94:285-92.

REFERENCES
103
Thompson JF, Man M, Johnson KJ, Wood LS, Lira ME, Lloyd DB, Banerjee P, Milos PM,Myrand SP, Paulauskis J, Milad MA, Sasiela WJ. An association study of 43 SNPs in 16 candidategenes with atorvastatin response. Pharmacogenomics J 2005;5:352-8.
Thompson PD, Clarkson P, Karas RH. Statin-associated myopathy. Jama 2003;289:1681-90.
Tirona RG, Leake BF, Merino G, Kim RB. Polymorphisms in OATP-C: identification of multipleallelic variants associated with altered transport activity among European- and African-Americans. J BiolChem 2001;276:35669-75.
Tirona RG, Leake BF, Wolkoff AW, Kim RB. Human organic anion transporting polypeptide-C(SLC21A6) is a major determinant of rifampin-mediated pregnane X receptor activation. J PharmacolExp Ther 2003;304:223-8.
Tirona RG, Kim RB. Nuclear receptors and drug disposition gene regulation. J Pharm Sci2005;94:1169-86.
Tobert JA. Lovastatin and beyond: the history of the HMG-CoA reductase inhibitors. Nat Rev DrugDiscov 2003;2:517-26.
Todd PA, Goa KL. Simvastatin. A review of its pharmacological properties and therapeutic potential inhypercholesterolaemia. Drugs 1990;40:583-607.
Treiber A, Schneiter R, Hausler S, Stieger B. Bosentan is a substrate of human OATP1B1 andOATP1B3: inhibition of hepatic uptake as the common mechanism of its interactions with cyclosporinA, rifampicin, and sildenafil. Drug Metab Dispos 2007;35:1400-7.
Tunstall-Pedoe H, Vanuzzo D, Hobbs M, Mähönen M, Cepaitis Z, Kuulasmaa K, Keil U.Estimation of contribution of changes in coronary care to improving survival, event rates, and coronaryheart disease mortality across the WHO MONICA Project populations. Lancet 2000;355:688-700.
Urban TJ, Brown C, Castro RA, Shah N, Mercer R, Huang Y, Brett CM, Burchard EG, GiacominiKM. Effects of genetic variation in the novel organic cation transporter, OCTN1, on the renal clearanceof gabapentin. Clin Pharmacol Ther 2008;83:416-21.
Vaklavas C, Chatzizisis YS, Ziakas A, Zamboulis C, Giannoglou GD. Molecular basis of statin-associated myopathy. Atherosclerosis 2008;
van der Deure WM, Friesema EC, de Jong FJ, de Rijke YB, de Jong FH, Uitterlinden AG, BretelerMM, Peeters RP, Visser TJ. OATP1B1: an important factor in hepatic thyroid hormone and estrogentransport and metabolism. Endocrinology 2008;
Wang P, Kim RB, Chowdhury JR, Wolkoff AW. The human organic anion transport proteinSLC21A6 is not sufficient for bilirubin transport. J Biol Chem 2003;278:20695-9.
Vavricka SR, Van Montfoort J, Ha HR, Meier PJ, Fattinger K. Interactions of rifamycin SV andrifampicin with organic anion uptake systems of human liver. Hepatology 2002;36:164-72.
Vickers S, Duncan CA, Chen IW, Rosegay A, Duggan DE. Metabolic disposition studies onsimvastatin, a cholesterol-lowering prodrug. Drug Metab Dispos 1990;18:138-45.
Wong MH, Oelkers P, Dawson PA. Identification of a mutation in the ileal sodium-dependent bile acidtransporter gene that abolishes transport activity. J Biol Chem 1995;270:27228-34.

REFERENCES
104
Wrighton SA, Stevens JC. The human hepatic cytochromes P450 involved in drug metabolism. CritRev Toxicol 1992;22:1-21.
Wrighton SA, Schuetz EG, Thummel KE, Shen DD, Korzekwa KR, Watkins PB. The humanCYP3A subfamily: practical considerations. Drug Metab Rev 2000;32:339-61.
Wu X, Whitfield LR, Stewart BH. Atorvastatin transport in the Caco-2 cell model: contributions of P-glycoprotein and the proton-monocarboxylic acid co-transporter. Pharm Res 2000;17:209-15.
Yabuuchi H, Tamai I, Nezu J, Sakamoto K, Oku A, Shimane M, Sai Y, Tsuji A. Novel membranetransporter OCTN1 mediates multispecific, bidirectional, and pH-dependent transport of organic cations.J Pharmacol Exp Ther 1999;289:768-73.
Yamada A, Maeda K, Kamiyama E, Sugiyama D, Kondo T, Shiroyanagi Y, Nakazawa H, OkanoT, Adachi M, Schuetz JD, Adachi Y, Hu Z, Kusuhara H, Sugiyama Y. Multiple human isoforms ofdrug transporters contribute to the hepatic and renal transport of olmesartan, a selective antagonist of theangiotensin II AT1-receptor. Drug Metab Dispos 2007;35:2166-76.
Yamashiro W, Maeda K, Hirouchi M, Adachi Y, Hu Z, Sugiyama Y. Involvement of transporters inthe hepatic uptake and biliary excretion of valsartan, a selective antagonist of the angiotensin II AT1-receptor, in humans. Drug Metab Dispos 2006;34:1247-54.
Yamazaki M, Suzuki H, Sugiyama Y. Recent advances in carrier-mediated hepatic uptake and biliaryexcretion of xenobiotics. Pharm Res 1996;13:497-513.
Zair ZM, Eloranta JJ, Stieger B, Kullak-Ublick GA. Pharmacogenetics of OATP (SLC21/SLCO),OAT and OCT (SLC22) and PEPT (SLC15) transporters in the intestine, liver and kidney.Pharmacogenomics 2008;9:597-624.
Zanger UM, Turpeinen M, Klein K, Schwab M. Functional pharmacogenetics/genomics of humancytochromes P450 involved in drug biotransformation. Anal Bioanal Chem 2008;
Zelcer N, Reid G, Wielinga P, Kuil A, van der Heijden I, Schuetz JD, Borst P. Steroid and bile acidconjugates are substrates of human multidrug-resistance protein (MRP) 4 (ATP-binding cassette C4).Biochem J 2003;371:361-7.
Zhang W, Yu BN, He YJ, Fan L, Li Q, Liu ZQ, Wang A, Liu YL, Tan ZR, Fen J, Huang YF, ZhouHH. Role of BCRP 421C>A polymorphism on rosuvastatin pharmacokinetics in healthy Chinese males.Clin Chim Acta 2006;373:99-103.
Zhang W, Deng S, Chen XP, Zhou G, Xie HT, He FY, Cao D, Li YJ, Zhou HH. Pharmacokinetics ofrosuvastatin when coadministered with rifampicin in healthy males: a randomized, single-blind, placebo-controlled, crossover study. Clin Ther 2008;30:1283-9.
Zhou F, You G. Molecular insights into the structure-function relationship of organic anion transportersOATs. Pharm Res 2007;24:28-36.
Åsberg A, Hartmann A, Fjeldsa E, Bergan S, Holdaas H. Bilateral pharmacokinetic interactionbetween cyclosporine A and atorvastatin in renal transplant recipients. Am J Transplant 2001;1:382-6.
Åsberg A. Interactions between cyclosporin and lipid-lowering drugs: implications for organ transplantrecipients. Drugs 2003;63:367-78.

ORIGINAL PUBLICATIONS
105
ORIGINAL PUBLICATIONS