pharmacology for nursing (introduction) by mohie aldien ...€¦ · absorption, distribution,...
TRANSCRIPT
1
PHARMACOLOGY FOR NURSING (Introduction)
By
Mohie Aldien Elsayed (MD)
Learning Objectives
At the end of this chapter the student will be able to: 1. Define various terminologies used in Pharmacology.
2. Know about nature and sources of drugs.
3. Understand pharmacodynamics like mechanism of drug action, dose relation ship and pharmacokinetics like
absorption, distribution, metabolism and excretion (ADME) of drugs. 4. Understand theoritical pharmacokinetics like half-life, order of kinetics, steady state plasma concentration.
5. Understand drug safety and effectiveness like factors affecting drug action and adverse drug reactions.
6. Understand new drug development and evaluation.
2
A. Definitions:
1. Pharmacology: Pharmacology is the study of interaction of drugs with living organisms.It also
includes history, source, physicochemical properties, dosage forms, methods of administration,
absorption, distribution mechanism of action, biotransformation, excretion, clinical uses and adverse
effects of drugs.
2. Clinical Pharmacology: It evaluate the pharmacological action of drug preferred route
of administration and safe dosage range in human by clinical trails.
3. Drugs: Drugs are chemicals that alter functions of living organisms. Drugs are generally given for the
diagnosis, prevention, control or cure of disease.
4. Pharmacy: It is the science of identification, selection, preservation, standardisation, compounding and
dispensing of medical substances.
5. Pharmacodynamics: The study of the biological and therapeutic effects of drugs (i.e, “what the drug
does to the body”).
6. Pharmacokinetics: Study of the absorption, distribution metabolism and excretion (ADME) of drugs
(“i.e what the body does to the drug”).
7. Pharmacotherapeutics: It deals with the proper selection and use of drugs for the prevention and
treatment of disease.
8. Toxicology: It’s the science of poisons. Many drugs in larger doses may act as poisons. Poisons are
substances that cause harmful, dangerous or fatal symptoms in living substances.
9. Chemotherapy: It’s the effect of drugs upon microorganisms, parasites and neoplastic cells living and
multiplying in living organisms.
10. Pharmacopoeia: An official code containing a selected list of the established drugs and medical B.
Drugs are obtained from:
1. Minerals: Liquid paraffin, magnesium sulfate, magnesium trisilicate, kaolin, etc.
2. Animals: Insulin, thyroid extract, heparin and antitoxin sera, etc.
3. Plants: Morphine, digoxin, atropine, castor oil, etc.
4. Synthetic source: Aspirin, sulphonamides, paracetamol, zidovudine, etc.
5. Micro organisms: Penicillin, streptomycin and many other antibiotics.
6. Genetic engineering: Human insulin, human growth hormone etc.
Out of all the above sources, majority of the drugs currently used in therapeutics are from synthetic
source.
II. Pharmacodynamics:
Mechanism of Drug Action
1- Physical: a- Adsorption: Kaolin & Activated charcoal in diarrhea.
b- Osmotic: Mannitol as a diuretic & MgSO4 as a purgative.
c- Demulcent: Liquorice as an anti-tussive.
d- Astringent: Tannic acid mouth wash in gingivitis
2- Chemical:a- Neutralization:- NaHCO3 (Antacid) + HCl (Gastric acid) in treatment of hyperacidity.
b- Chelation: Organic compound + Heavy metal Non-toxic easy excreted complex.
i- Dimercaprol (British Anti-Lewisite or BAL) for Mercury (Hg), Arsenic (As) & Antimony (Sb)
ii- Sodium Edetate for Calcium (Ca+2). iii- d.Penicillamine for Copper (Cu+2).
iv- Desferrioxamine for ferric iron (Fe+3).
3- Interference with Cell Division: Anti-cancer drugs e.g. Nitrogen mustard.
4- Interference with Metabolic Pathway: Sulfonamides compete with PABA in bacteria Synthesis
of folic acid.

3
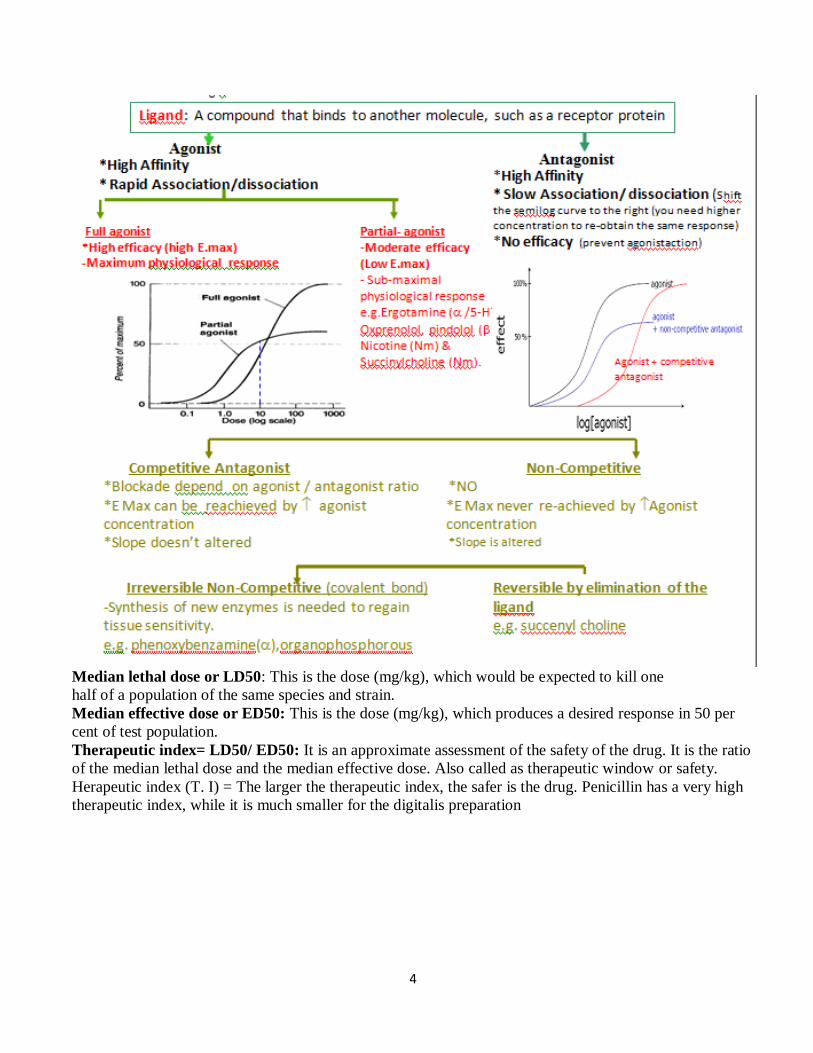
5- Inhibition of Enzymes: Physostigmine ( Cholinesterase)
6- Action on Voltage Dependent Ion Channel:
a-Local anesthetics block Sodium (Na+) channels. b-Calcium channel blockers (CCB) e.g. Verapamil
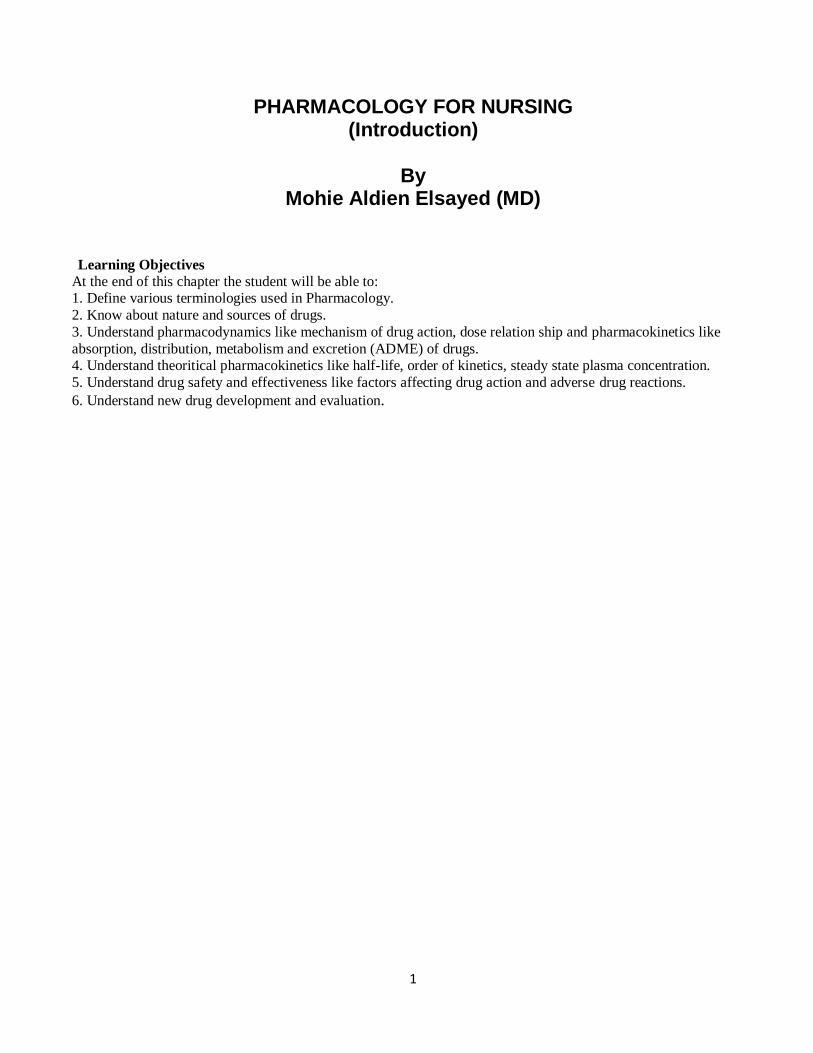
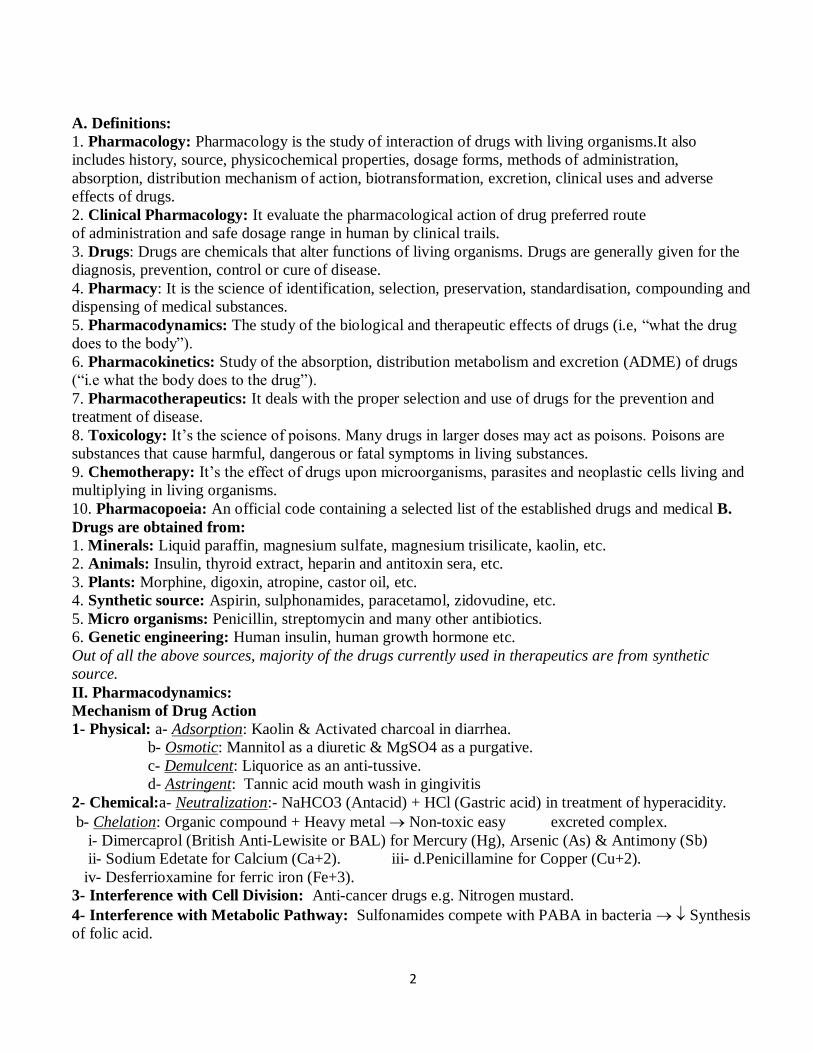
7. Receptor. :
Affinity: Ability of the ligand to fit in receptor.It is assessed by Equilibrium constant Which is the conc. Of ligand occupy 50% of R. Efficacy: (Ability of L-R complex to initiate response.It is assessed by the Maximum effect (Emax.) of the ligand. Potency: (the ligand concentration .which produce 50% of the response (ED50%).It is used to compare different
doses of different drugs..
4
Median lethal dose or LD50: This is the dose (mg/kg), which would be expected to kill one
half of a population of the same species and strain.
Median effective dose or ED50: This is the dose (mg/kg), which produces a desired response in 50 per
cent of test population.
Therapeutic index= LD50/ ED50: It is an approximate assessment of the safety of the drug. It is the ratio
of the median lethal dose and the median effective dose. Also called as therapeutic window or safety.
Herapeutic index (T. I) = The larger the therapeutic index, the safer is the drug. Penicillin has a very high
therapeutic index, while it is much smaller for the digitalis preparation
5
.III. Pharmacokinetics : Pharmacokinetics deals with the absorption, distribution, metabolism and
excretion drugs in the body.
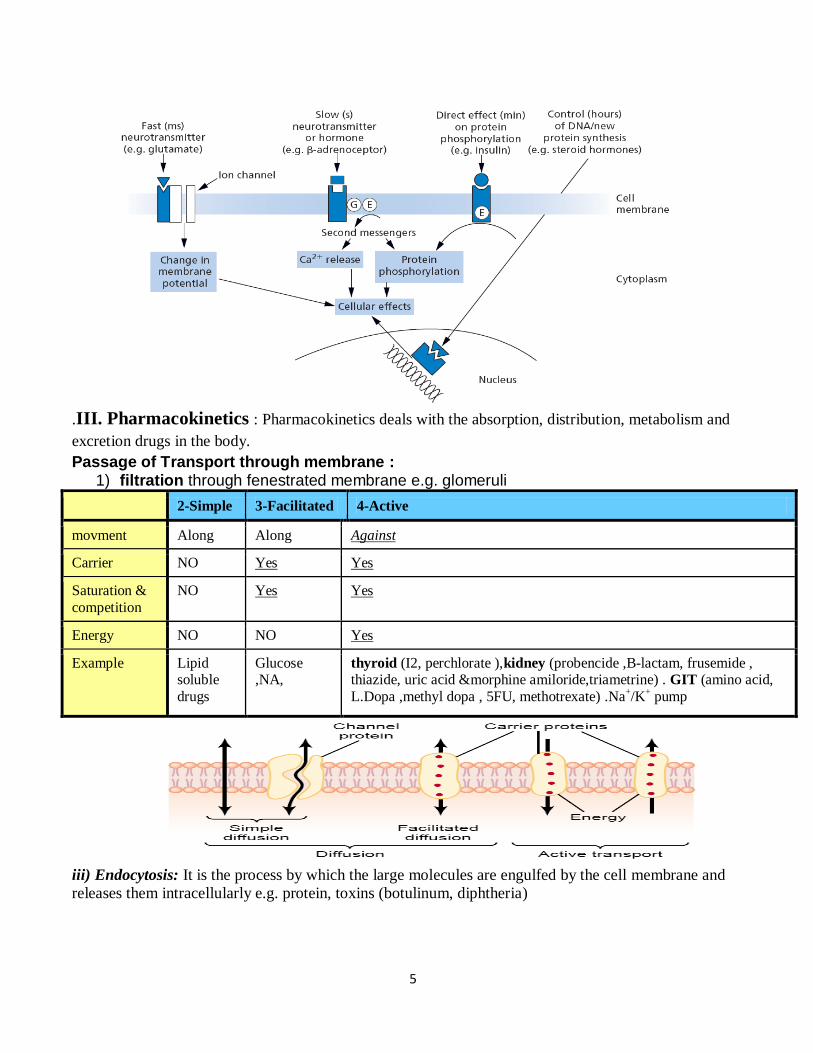
Passage of Transport through membrane : 1) filtration through fenestrated membrane e.g. glomeruli
2-Simple 3-Facilitated 4-Active
movment Along Along Against
Carrier NO Yes Yes
Saturation &
competition
NO Yes Yes
Energy NO NO Yes
Example Lipid soluble
drugs
Glucose ,NA,
thyroid (I2, perchlorate ),kidney (probencide ,B-lactam, frusemide , thiazide, uric acid &morphine amiloride,triametrine) . GIT (amino acid,
L.Dopa ,methyl dopa , 5FU, methotrexate) .Na+/K
+ pump
iii) Endocytosis: It is the process by which the large molecules are engulfed by the cell membrane and
releases them intracellularly e.g. protein, toxins (botulinum, diphtheria)
6
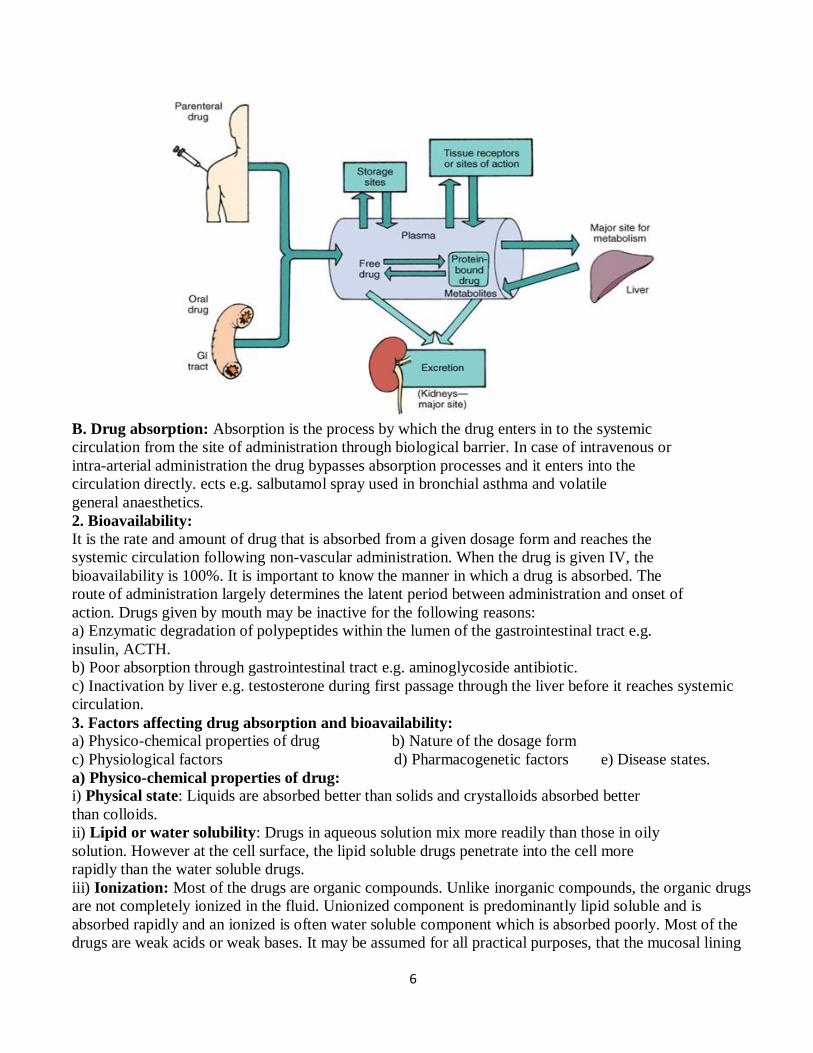
B. Drug absorption: Absorption is the process by which the drug enters in to the systemic
circulation from the site of administration through biological barrier. In case of intravenous or
intra-arterial administration the drug bypasses absorption processes and it enters into the
circulation directly. ects e.g. salbutamol spray used in bronchial asthma and volatile
general anaesthetics.
2. Bioavailability:
It is the rate and amount of drug that is absorbed from a given dosage form and reaches the
systemic circulation following non-vascular administration. When the drug is given IV, the
bioavailability is 100%. It is important to know the manner in which a drug is absorbed. The
route of administration largely determines the latent period between administration and onset of
action. Drugs given by mouth may be inactive for the following reasons:
a) Enzymatic degradation of polypeptides within the lumen of the gastrointestinal tract e.g.
insulin, ACTH.
b) Poor absorption through gastrointestinal tract e.g. aminoglycoside antibiotic.
c) Inactivation by liver e.g. testosterone during first passage through the liver before it reaches systemic
circulation.
3. Factors affecting drug absorption and bioavailability:
a) Physico-chemical properties of drug b) Nature of the dosage form
c) Physiological factors d) Pharmacogenetic factors e) Disease states.
a) Physico-chemical properties of drug:
i) Physical state: Liquids are absorbed better than solids and crystalloids absorbed better
than colloids.
ii) Lipid or water solubility: Drugs in aqueous solution mix more readily than those in oily
solution. However at the cell surface, the lipid soluble drugs penetrate into the cell more
rapidly than the water soluble drugs.
iii) Ionization: Most of the drugs are organic compounds. Unlike inorganic compounds, the organic drugs
are not completely ionized in the fluid. Unionized component is predominantly lipid soluble and is
absorbed rapidly and an ionized is often water soluble component which is absorbed poorly. Most of the
drugs are weak acids or weak bases. It may be assumed for all practical purposes, that the mucosal lining
7
of the G.I.T is impermeable to the ionized form of a weak organic acid or a weak organic base. These
drugs exist in two forms.
• Weak base in acid media, ( pKa > pH ) ionized non-diffusible form predominate
• Weak base In alkali media, ( pKa < pH ) non-ionized, diffusible. form predominate
Acidic drugs: rapidly absorbed from the stomach e.g. salicylates and barbiturates.
Basic drugs: Not absorbed until they reach to the alkaline environment i.e. small intestine when
administered orally e.g. pethidine and ephedrine
b) Dosage forms:
i) Particle size: Small particle size is important for drug absorption. Drugs given in a dispersed or
emulsified state are absorbed better e.g. vitamin D and vitamin A.
ii) Disintegration time and dissolution rate.
Disintegration time: The rate of break up of the tablet or capsule into the drug granules.
Dissolution rate: The rate at which the drug goes into solution.
iii) Formulation: Usually substances like lactose, sucrose, starch and calcium phosphate are used as inert
diluents in formulating powders or tablets. Fillers may not be totally inert but may affect the absorption as
well as stability of the medicament. Thus a faulty formulation can render a useful drug totally useless
therapeutically.
c) Physiological factors:
i) Gastrointestinal transit time: Rapid absorption occurs when the drug is given on empty stomach.
However certain irritant drugs like salicylates and iron preparations are deliberately administred after food
to minimize the gastrointestinal irritation. But some times the presence of food in the G.I tract aids the
absorption of certain drugs e.g. griseofulvin, propranolol and riboflavin.
ii) Presence of other agents: Vitamin C enhances the absorption of iron from the G.I.T.
Calcium present in milk and in antacids forms insoluble complexes with the tetracycline
antibiotics and reduces their absorption.
iii) Area of the absorbing surface and local circulation: Drugs can be absorbed better from the small
intestine than from the stomach because of the larger surface area of the former. Increased vascular supply
can increase the absorption.
iv) Enterohepatic cycling: Some drugs move in between intestines and liver before they
reach the site of action. This increases the bioavailability e.g. phenolphthalein.
v) Metabolism of drug/first pass effect: Rapid degradation of a drug by the liver during the first pass
(propranolol) or by the gut wall (isoprenaline) also affects the bioavailability. Thus a drug though
absorbed well when given orally may not be effective because of its extensive first pass metabolism.
d) Pharmacogenetic factors: Individual variations occur due to the genetically mediated reason in drug
absorption and response.
e) Disease states: Absorption and first pass metabolism may be affected in conditions like malabsorption,
thyrotoxicosis, achlorhydria and liver cirrhosis.
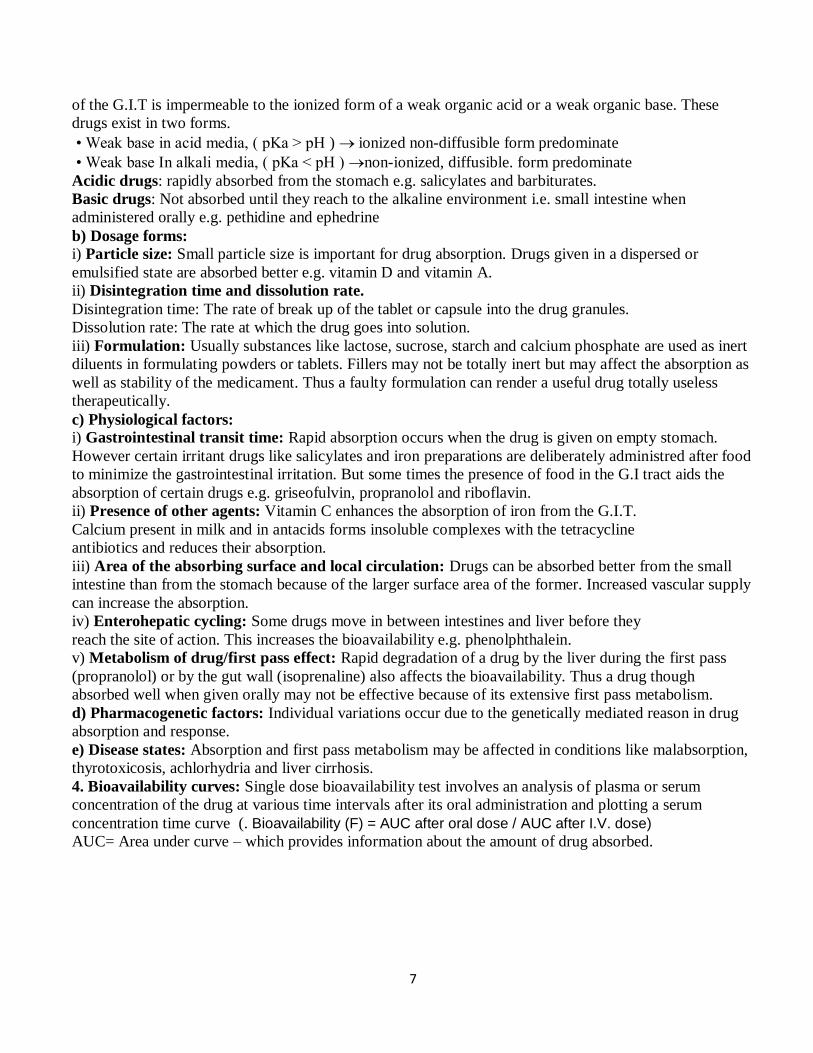
4. Bioavailability curves: Single dose bioavailability test involves an analysis of plasma or serum
concentration of the drug at various time intervals after its oral administration and plotting a serum
concentration time curve (. Bioavailability (F) = AUC after oral dose / AUC after I.V. dose)
AUC= Area under curve – which provides information about the amount of drug absorbed.
8
MTC: Minimum toxic concentration MEC: Minimum effective concentration
Fig 1.2 : The plasma drug level curves following administration of three formulations (A, B and C) of the
same basic drug. Formulation A = would produce quick onset and short duration of action, produce toxic
effects. Formation B = Effect would last much longer and nontoxic Formulation C = gives inadequate
plasma level so therapeutically ineffective
C) Distribution of drugs
1. Definition: Penetration of a drug to the sites of action through the walls of blood vessels from
the administered site after absorption is called drug distribution. Drugs distribute through
various body fluid compartments such as (a) plasma (b) interstitial fluid compartment (c)
trans-cellular compartment.
Apparent Volume of distribution (VD): The volume into which the total amount of a drug in
the body would have to be uniformly distributed to provide the concentration of the drug actually
measured in the plasma. It is an apparent rather than real volume.
Vd = dose (mg) / Plasma concentration (mg/L) what is the significance of Vd?
1) A low Vd (>5L) indicates that the drug is restricted to plasma.
- Large size, High MW > 500 e.g (heparin, insulin, dextran)
- Plasma Protein Bound = NoT (active,/excreted/filtered/Metabolized) • Drugs extensively bound to plasma proteins e.g. Thiopentone (I.V. Anesthesia) have to be injected slowly
rather Rapidly I.V.
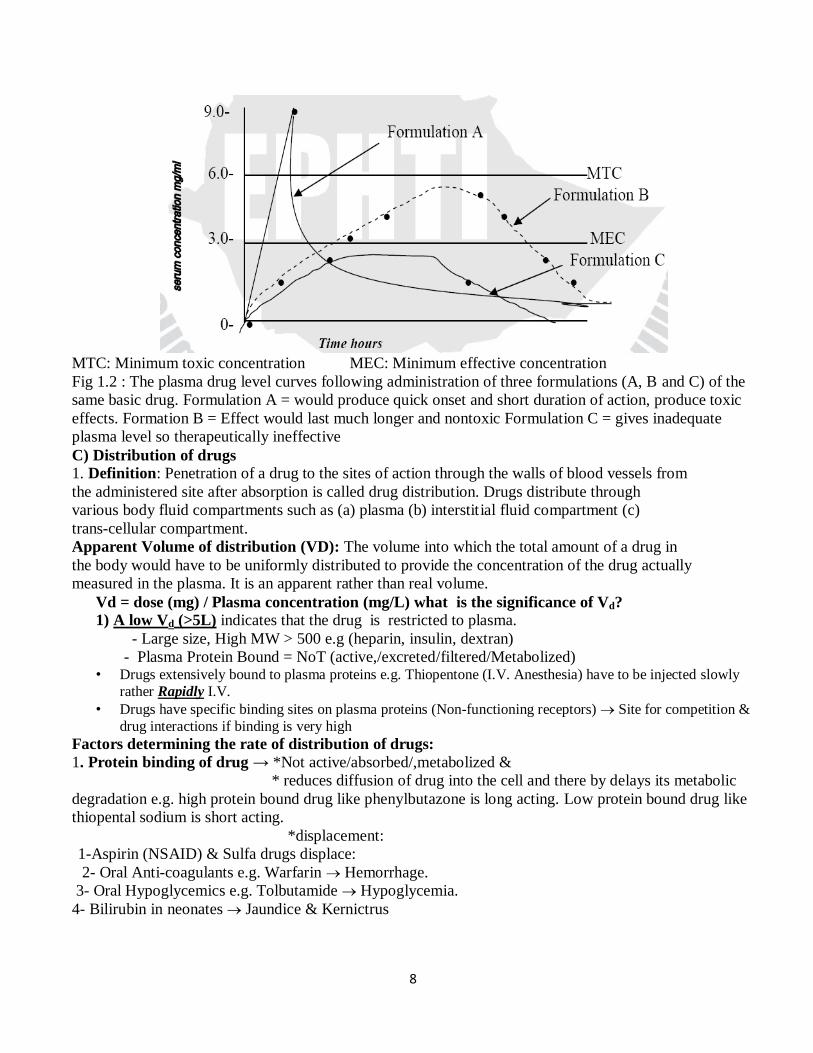
• Drugs have specific binding sites on plasma proteins (Non-functioning receptors) Site for competition &
drug interactions if binding is very high Factors determining the rate of distribution of drugs:
1. Protein binding of drug → *Not active/absorbed/,metabolized &
* reduces diffusion of drug into the cell and there by delays its metabolic
degradation e.g. high protein bound drug like phenylbutazone is long acting. Low protein bound drug like
thiopental sodium is short acting.
*displacement:
1-Aspirin (NSAID) & Sulfa drugs displace:
2- Oral Anti-coagulants e.g. Warfarin Hemorrhage.
3- Oral Hypoglycemics e.g. Tolbutamide Hypoglycemia.
4- Bilirubin in neonates Jaundice & Kernictrus
9
.3. Clearance: Volume of plasma cleared off the drug by metabolism and excretion per unit time.
Protein binding reduces the amount of drug available for filtration at the glomeruli and hence
delays the excretion, thus the protein binding reduces the clearance.
4. Physiological barriers to distribution: There are some specialized barriers in the body due
to which the drug will not be distributed uniformly in all the tissues. These barriers are:
a) Blood brain barrier (BBB) through which thiopental sodium is easily crossed but not dopamine.
b) Placental barrier: which allows non-ionized drugs with high lipid/water partition coefficient by a
process of simple diffusion to the foetus e.g. alcohol, morphine.
5. Affinity of drugs to certain organs: The concentration of a drug in certain tissues after a
single dose may persist even when its plasma concentration is reduced to low. Thus the
hepatic concentration of mepacrine is more than 200 times that of plasma level. Their
concentration may reach a very high level on chronic administration. Iodine is similarly
concentrated in the thyroid tissue.
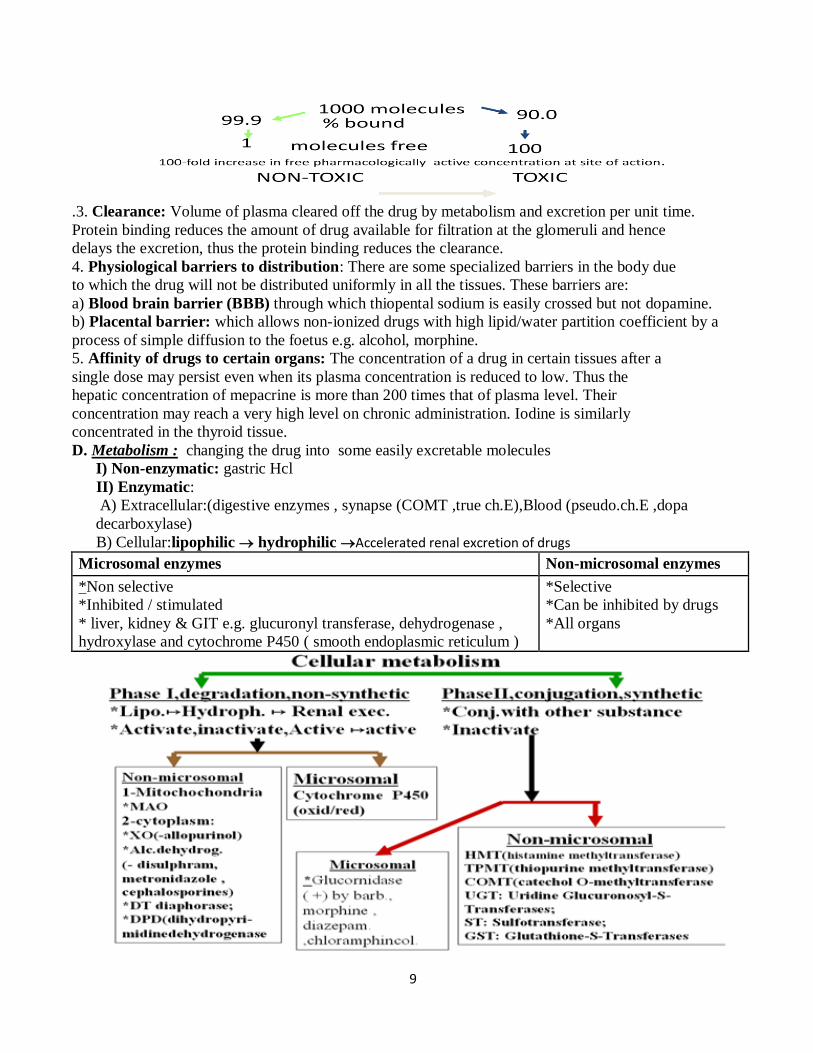
D. Metabolism : changing the drug into some easily excretable molecules
I) Non-enzymatic: gastric Hcl
II) Enzymatic:
A) Extracellular:(digestive enzymes , synapse (COMT ,true ch.E),Blood (pseudo.ch.E ,dopa
decarboxylase)
B) Cellular:lipophilic hydrophilic Accelerated renal excretion of drugs
Microsomal enzymes Non-microsomal enzymes
*Non selective
*Inhibited / stimulated
* liver, kidney & GIT e.g. glucuronyl transferase, dehydrogenase ,
hydroxylase and cytochrome P450 ( smooth endoplasmic reticulum )
*Selective
*Can be inhibited by drugs
*All organs
10
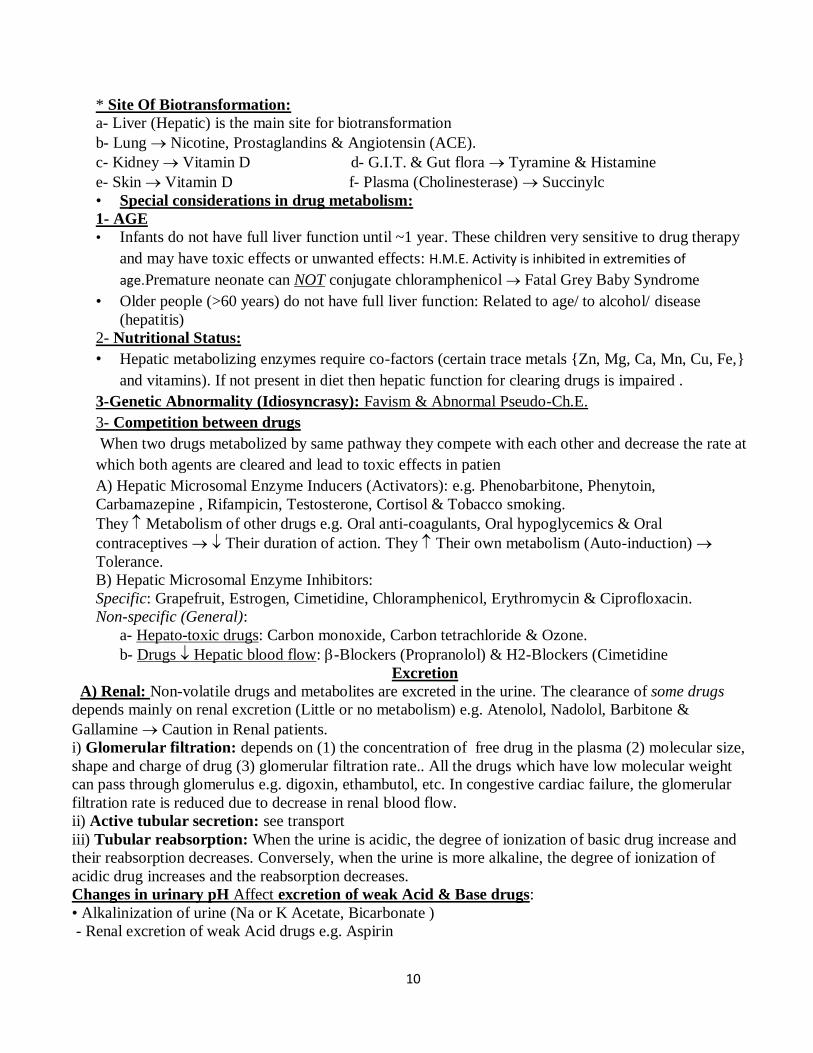
* Site Of Biotransformation:
a- Liver (Hepatic) is the main site for biotransformation
b- Lung Nicotine, Prostaglandins & Angiotensin (ACE).
c- Kidney Vitamin D d- G.I.T. & Gut flora Tyramine & Histamine
e- Skin Vitamin D f- Plasma (Cholinesterase) Succinylc
• Special considerations in drug metabolism:
1- AGE
• Infants do not have full liver function until ~1 year. These children very sensitive to drug therapy
and may have toxic effects or unwanted effects: H.M.E. Activity is inhibited in extremities of
age.Premature neonate can NOT conjugate chloramphenicol Fatal Grey Baby Syndrome
• Older people (>60 years) do not have full liver function: Related to age/ to alcohol/ disease
(hepatitis)
2- Nutritional Status:
• Hepatic metabolizing enzymes require co-factors (certain trace metals {Zn, Mg, Ca, Mn, Cu, Fe,}
and vitamins). If not present in diet then hepatic function for clearing drugs is impaired .
3-Genetic Abnormality (Idiosyncrasy): Favism & Abnormal Pseudo-Ch.E.
3- Competition between drugs
When two drugs metabolized by same pathway they compete with each other and decrease the rate at
which both agents are cleared and lead to toxic effects in patien
A) Hepatic Microsomal Enzyme Inducers (Activators): e.g. Phenobarbitone, Phenytoin,
Carbamazepine , Rifampicin, Testosterone, Cortisol & Tobacco smoking.
They Metabolism of other drugs e.g. Oral anti-coagulants, Oral hypoglycemics & Oral
contraceptives Their duration of action. They Their own metabolism (Auto-induction)
Tolerance.
B) Hepatic Microsomal Enzyme Inhibitors:
Specific: Grapefruit, Estrogen, Cimetidine, Chloramphenicol, Erythromycin & Ciprofloxacin.
Non-specific (General):
a- Hepato-toxic drugs: Carbon monoxide, Carbon tetrachloride & Ozone.
b- Drugs Hepatic blood flow: -Blockers (Propranolol) & H2-Blockers (Cimetidine
Excretion
A) Renal: Non-volatile drugs and metabolites are excreted in the urine. The clearance of some drugs
depends mainly on renal excretion (Little or no metabolism) e.g. Atenolol, Nadolol, Barbitone &
Gallamine Caution in Renal patients.
i) Glomerular filtration: depends on (1) the concentration of free drug in the plasma (2) molecular size,
shape and charge of drug (3) glomerular filtration rate.. All the drugs which have low molecular weight
can pass through glomerulus e.g. digoxin, ethambutol, etc. In congestive cardiac failure, the glomerular
filtration rate is reduced due to decrease in renal blood flow.
ii) Active tubular secretion: see transport
iii) Tubular reabsorption: When the urine is acidic, the degree of ionization of basic drug increase and
their reabsorption decreases. Conversely, when the urine is more alkaline, the degree of ionization of
acidic drug increases and the reabsorption decreases.
Changes in urinary pH Affect excretion of weak Acid & Base drugs:
• Alkalinization of urine (Na or K Acetate, Bicarbonate )
Renal excretion of weak Acid drugs e.g. Aspirin
11
• Acidification of Urine (NH4Cl or “Vit C”) ®
Renal excretion of weak Base drugs e.g. Ephedrine & Amphetamine.
B) Lung: Gases (CO2) & Volatile Liquids (Halothane)
C) Alimentary Tract:
1- Saliva (pH = 8): Morphine & Aspirin 2- Stomach : Morphine.
3- Bile:
b- Reabsorbed Entero-Hepatic Circulation e.g. Morphine& Indomethacin, l, oral estrogen
c- Some antimicrobials are excreted in bile in an active form e.g. Ampicillin & Rifampicin
chloramphenicoTetracylines Useful in treatment of Cholecystitis & Typhoid carrier.
4- Large Intestine: Either via the bile or unabsorbed oral drugs.
D) Skin Glands: 1- Sweat: Vit B-1, Hg, As & Rifampicin Red discoloration of sweat.
2- Milk May affect suckling baby e.g. Morphine, nicotine, Purgatives, Tetracyclines & Chloramphenicol.
ampicillin, aspirin, chlordiazepoxide, coffee, diazepam, furosemide, streptomycin etc.
Clearance of a drug: It is the volume of plasma cleared of the drug by metabolism (hepatic) and
excretion (renal) and other organs.
Total clearance will be calculated by Ct = Ch( hepatic clearance) + Cr (Renal clearance) + C others
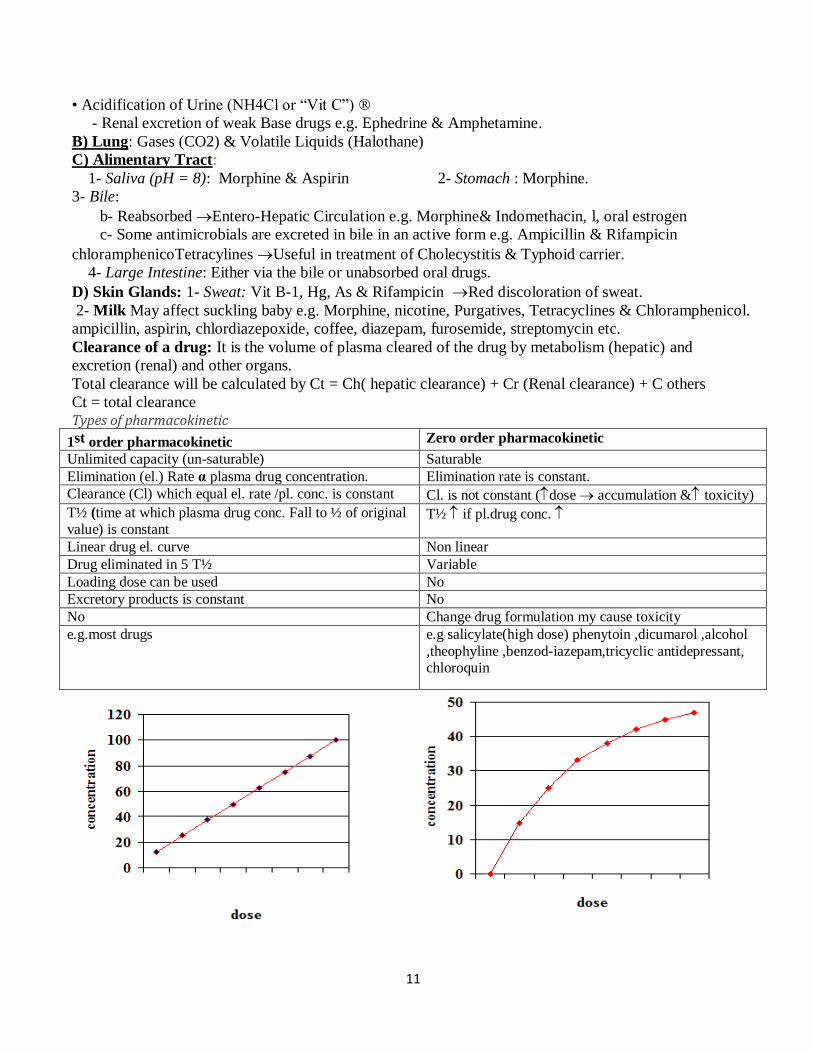
Ct = total clearance Types of pharmacokinetic
1st order pharmacokinetic Zero order pharmacokinetic
Unlimited capacity (un-saturable) Saturable
Elimination (el.) Rate α plasma drug concentration. Elimination rate is constant.
Clearance (Cl) which equal el. rate /pl. conc. is constant Cl. is not constant (dose accumulation & toxicity)
T½ (time at which plasma drug conc. Fall to ½ of original value) is constant
T½ if pl.drug conc.
Linear drug el. curve Non linear
Drug eliminated in 5 T½ Variable
Loading dose can be used No
Excretory products is constant No
No Change drug formulation my cause toxicity
e.g.most drugs
e.g salicylate(high dose) phenytoin ,dicumarol ,alcohol
,theophyline ,benzod-iazepam,tricyclic antidepressant, chloroquin
12
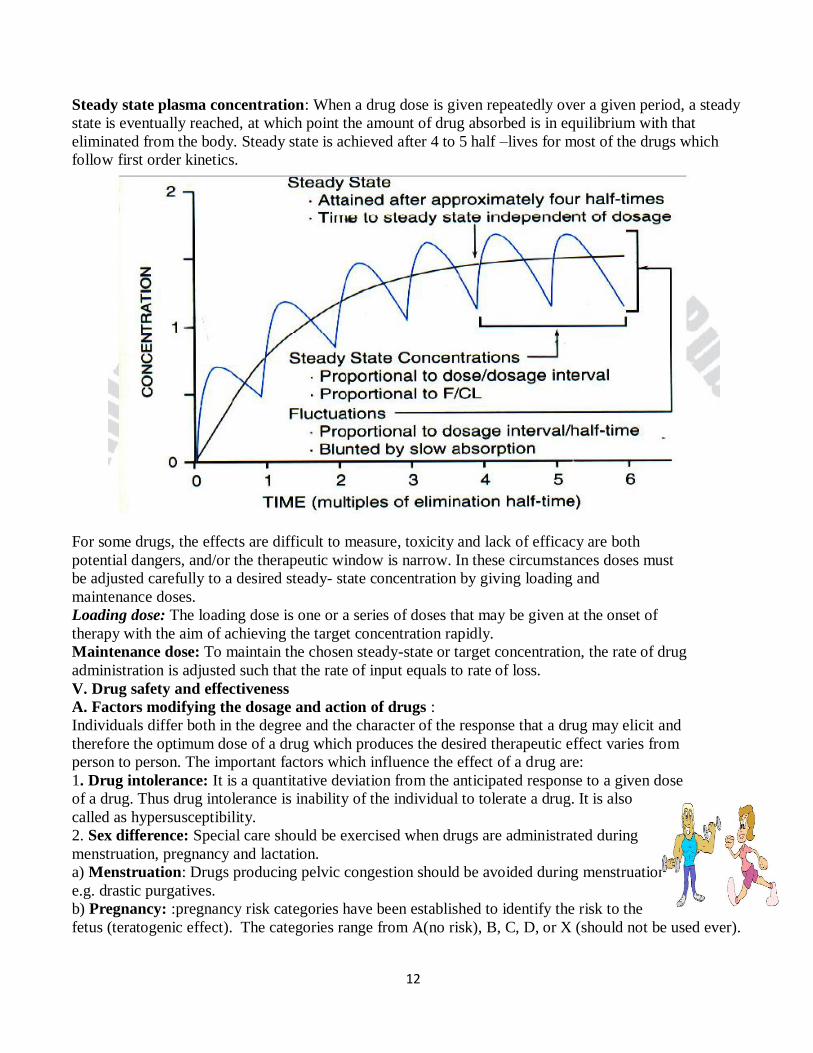
Steady state plasma concentration: When a drug dose is given repeatedly over a given period, a steady
state is eventually reached, at which point the amount of drug absorbed is in equilibrium with that
eliminated from the body. Steady state is achieved after 4 to 5 half –lives for most of the drugs which
follow first order kinetics.
For some drugs, the effects are difficult to measure, toxicity and lack of efficacy are both
potential dangers, and/or the therapeutic window is narrow. In these circumstances doses must
be adjusted carefully to a desired steady- state concentration by giving loading and
maintenance doses.
Loading dose: The loading dose is one or a series of doses that may be given at the onset of
therapy with the aim of achieving the target concentration rapidly.
Maintenance dose: To maintain the chosen steady-state or target concentration, the rate of drug
administration is adjusted such that the rate of input equals to rate of loss.
V. Drug safety and effectiveness
A. Factors modifying the dosage and action of drugs :
Individuals differ both in the degree and the character of the response that a drug may elicit and
therefore the optimum dose of a drug which produces the desired therapeutic effect varies from
person to person. The important factors which influence the effect of a drug are:
1. Drug intolerance: It is a quantitative deviation from the anticipated response to a given dose
of a drug. Thus drug intolerance is inability of the individual to tolerate a drug. It is also
called as hypersusceptibility.
2. Sex difference: Special care should be exercised when drugs are administrated during
menstruation, pregnancy and lactation.
a) Menstruation: Drugs producing pelvic congestion should be avoided during menstruation
e.g. drastic purgatives.
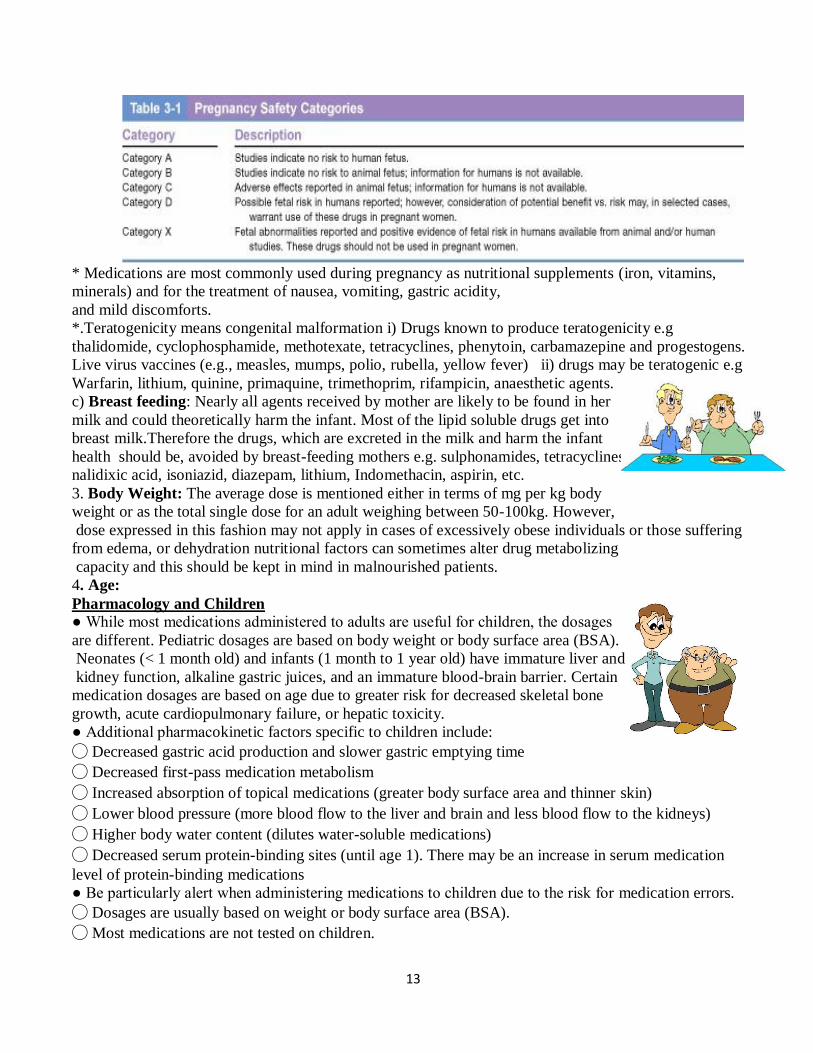
b) Pregnancy: :pregnancy risk categories have been established to identify the risk to the
fetus (teratogenic effect). The categories range from A(no risk), B, C, D, or X (should not be used ever).
13
* Medications are most commonly used during pregnancy as nutritional supplements (iron, vitamins,
minerals) and for the treatment of nausea, vomiting, gastric acidity,
and mild discomforts.
*.Teratogenicity means congenital malformation i) Drugs known to produce teratogenicity e.g
thalidomide, cyclophosphamide, methotexate, tetracyclines, phenytoin, carbamazepine and progestogens.
Live virus vaccines (e.g., measles, mumps, polio, rubella, yellow fever) ii) drugs may be teratogenic e.g
Warfarin, lithium, quinine, primaquine, trimethoprim, rifampicin, anaesthetic agents.
c) Breast feeding: Nearly all agents received by mother are likely to be found in her
milk and could theoretically harm the infant. Most of the lipid soluble drugs get into
breast milk.Therefore the drugs, which are excreted in the milk and harm the infant
health should be, avoided by breast-feeding mothers e.g. sulphonamides, tetracyclines,
nalidixic acid, isoniazid, diazepam, lithium, Indomethacin, aspirin, etc.
3. Body Weight: The average dose is mentioned either in terms of mg per kg body
weight or as the total single dose for an adult weighing between 50-100kg. However,
dose expressed in this fashion may not apply in cases of excessively obese individuals or those suffering
from edema, or dehydration nutritional factors can sometimes alter drug metabolizing
capacity and this should be kept in mind in malnourished patients.
4. Age:
Pharmacology and Children
● While most medications administered to adults are useful for children, the dosages
are different. Pediatric dosages are based on body weight or body surface area (BSA).
Neonates (< 1 month old) and infants (1 month to 1 year old) have immature liver and
kidney function, alkaline gastric juices, and an immature blood-brain barrier. Certain
medication dosages are based on age due to greater risk for decreased skeletal bone
growth, acute cardiopulmonary failure, or hepatic toxicity.
● Additional pharmacokinetic factors specific to children include:
◯ Decreased gastric acid production and slower gastric emptying time
◯ Decreased first-pass medication metabolism
◯ Increased absorption of topical medications (greater body surface area and thinner skin)
◯ Lower blood pressure (more blood flow to the liver and brain and less blood flow to the kidneys)
◯ Higher body water content (dilutes water-soluble medications)
◯ Decreased serum protein-binding sites (until age 1). There may be an increase in serum medication
level of protein-binding medications
● Be particularly alert when administering medications to children due to the risk for medication errors.
◯ Dosages are usually based on weight or body surface area (BSA).
◯ Most medications are not tested on children.
14
◯ Adult medication forms and concentrations may require dilution, calculation, preparation, and
administration of very small doses.
◯ Limited sites exist for IV medication administration
The pharmacokinetics of many drugs changes with age. Thus gastric emptying is prolonged and the
gastric pH fluctuates in neonates and infant, further the liver capacity to
metabolize drugs is low, renal function is less developed and the proportion of body water is
higher in the newborn and the neonates. Hence children may not react to all drugs in the
same fashion as young adults. With a few exceptions, drugs are more active and more toxic
in the new born than the adults.
They have immature drug-elimination mechanisms (metabolism & excretion).
Calculate the dose by:
1- Infant (< 1 year) dose (Clark’s Formula) = Adult dose X (Weight of infant in Pounds/150)
2- Child (1 – 12 year) dose (Young’s Formula) = Adult dose X [Age in years / (Age + 12)]
-or (Dilling’s Formula) = Adult Dose X (Age in Years / 20)
-or = Adult Dose X (wt of child in Kg / 70)
Pharmacology and Older Adults (65+ Years)
● Physiologic changes associated with aging that impact pharmacokinetics include:
◯ Increased gastric pH (alkaline)
◯ Decreased GI motility and gastric emptying time
◯ Decreased blood flow through cardiovascular system, liver, and kidneys individual considerations of
medication administration 80 rn pharmacology for nursing
◯ Decreased hepatic enzyme function
◯ Decreased kidney function and glomerular filtration rate
◯ Decreased protein-binding sites
◯ Decreased body water, increased body fat, and decreased lean body mass
● Other factors affecting medication therapy for older adults may include:
◯ Impaired memory or altered mental state ◯ Changes in vision and hearing
◯ Decreased mobility and dexterity ◯ Poor adherence
◯ Reduced financial resources ◯ Polypharmacy
■ They have exhausted drug-elimination mechanisms (metabolism & excretion). Use 2/3 or 3/4 of the adult dose
■ The practice of taking several medications simultaneously (prescribed and/or over-the-counter [OTC])
together with diminished bodily functions and certain medical conditions can contribute to the potential
for medication toxicity.
● Nursing interventions for older adults:
◯ Decreasing the risk of adverse medication effects
■ Obtain a complete medication history and include all OTC medications.
■ Make sure medication therapy starts at the lowest possible dose.
■ Assess/monitor for therapeutic and adverse effects.
■ Assess/monitor for drug-drug and drug-food interactions.
■ Document findings.
■ Notify the provider of adverse effects.
◯ Promoting adherence
■ Give clear and concise instructions, verbally and in writing.
■ Ensure that the dosage form is appropriate. Administer liquid forms to clients who have difficulty
swallowing.
15
■ Provide clearly marked containers that are easy to open.
■ Assist the client to set up a daily calendar with the use of pill containers The paediatric doses are
expressed in terms of body weight (mg/kg per dose or day) or in terms of body surface area (mg/m2per
day). The body surface area can be calculated from the height and weight of the child. Like children, old
people also present problems in dosage adjustment and this may vary widely with different people. The
metabolism of drugs may diminish in the elderly and the renal function declines with age. Elderly are
sensitive to the drugs like hypnotics, tranquilizers, phenylbutazone, diazepam, pethidine, etc.
5. Disease state: Some antimicrobial agents penetrate the cerebrospinal fluid well across the
normal meninges while other antimicrobials penetrate well only when the meninges are
inflammed (meningitis) e.g. sulphonamides, metronidazole, chloramphenicol, isoniazid
and rifampicin penetrate well through the normal meninges and other antimicrobial agent s
like benzyl penicillin, ampicillin, tetracycline, streptomycin, gentamicin and cephalosporin
penetrate only when the meninges are inflammed.
Acute or chronic liver diseases markedly modify the rate and extent of biotransformation
of drugs. The t1/2 of chlordiazepoxide and diazepam in patients with liver cirrhosis is greatly
increased with corresponding prolongation of their effects.
Cardiac disease by limiting blood flow to the liver may impair disposition of those drugs whose
biotransformation is flow limited e.g. imipramine, isoniazid, lignocaine, morphine and
propranolol. Similarly renal and pulmonary diseases may modify the biotransformation of drugs like
insulin or isoprenaline. Excretion of drug is impaired in chronic renal disease.
6. Pharmacogenetics: The science pharmacogenetics is concerned with the geneticallymediated
variations in drug responses. Some examples of genetically mediated variations are:
Acetylation and hydroxylation of drugs: The rate of acetylation of INH, dapsone, hydralazine
procainamide and some sulfonamides is controlled by an autosomal recessive gene and the
dosage of these drugs depends up on the acetylator status of individuals.
Drug-Drug Interactions
Definition: Drug interaction -- when one drug affects the pharmacological response of a second drug
given at the same time.
A) Outside the body (mixing 2 drugs prior injection)
1-precipitation: *Protamin zinc insulin +soluble insulin *heparin + aminoglycoside/hydrocortisone
2-Inactivation: *heparin+dextrose *ampicillin + hydrocortisone
B) Inside the body:
1-Transport to site of action:
*Absorption from GIT ,
a- Motility: Metoclopramide Gastric emptying Paracetamol Absorption& digoxin absorption.
b- pH: - Acid stomach Absorption of weak acid drugs e.g. Aspirin and barbiturates
- Alkaline intestine ® Abs. of weak alkaline drugs e.g. Ephedrine & amphetamine
c- Content: - Tetracyclines chelate Ca (Milk), Mg, Al, & ferrous iron
2. Distribution:
*Plasma protein binding (clinically important if displaced drug is highly bind ) e.g salicylae,
phenylbutazone, sulphonamide Displace oral anticoagulants & Oral hypoglycemics ,phenytoin, , bilirubin
from their plasma binding sites Their activity.
3. Metabolism: Enzyme inhibitors/inducers
4. Excretion: a- Probenecid Active renal tubular excretion of Penicillin & Frusemide.
b- Alkalinization of urine (NaHCO3) Excretion of weak acid drugs e.g. Aspirin
16
c) acidification by Vit. C Excretion of weak base drugs e.g. quinidine, amphetamine
II- At site of action:
A-Synergism (1+1 > 2):
* amino glycoside + b.lactams * amino glycoside +Neuromuscular blocker.
B-Addition (1+1=2):*Ach + H on intestinal motility
C-Potentiation: Inactive drug (inert) increases the activity of Active Drug (0 +1 = > 1). Dose of
active drug.
-Physostigmine (Anticholines-terase) potentates ACh.
-Barbiturates (NOT analgesic) potentiate the analgesic effect of aspirin.
-Change pH:
*alkalinize urine by NaCo3 efficacy of aminoglycoside, sulphonamid
*Acidify urine by vit, C efficacy of B lactam, nitrofurantoin.
--hypokalemia digitalis toxicity.
C-Antagonism: *Chemical e.g.Heparin(Ac.) +Pr.So4(base) *Physiological e.g. Ad& H on bronchi
*Pharmacological One Agonist + One Blocker + One Receptor.
Importance of drug antagonism
(i) Correcting adverse effects of drugs
(ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate compounds with atropine.
(iii) Predicting drug combinations which would reduce drug efficacy.
Iatrogenic Disease:
Drug-induced disease.
- Large dose of Reserpine & Chlorpromazine (Iatrogenic Parkinsonism)
-Large dose of Cortisol (Iatrogenic Cushing’s disease.
8) Repeated administration and drug cumulation:
If a drug is excreted slowly, its administration may build up a sufficiently high concentration in
the body to produce toxicity. e.g. digitalis, emetine.
To avoid cumulation. a) One must know if a drug is eliminated slowly or rapidly, b) Stop the drug administration at the appearance of the first warning symptoms c) Carefully select the form in which the
drug is to be administered.
d) Check liver and kidney function before and during drug administration, as even an otherwise
non-cumulative drug would produce cumulation in the presence of hepatic and renal damage.
Tachyphylaxis: Rapid development of tolerance on repeated administration is called Tachyphylaxis e.g.
Ephedrine, amphetamine and nitroglycerine which produce tachyphylaxis on repeated administration.
10) Emotional factors. eg. Placebo response.
Placebo: It is a Latin word meaning” I shall please” and it is a tablet looking exactly like the
active treatment but containing no active component. It refers originally to substances merely to
please the patient when no specific treatment was available.
Adverse Drug Effects
I) Predictable pharmacodynamic response. More common ,less dangerous ,Dose dependent 1) 1ry: A) overdosing e.g Morphine) B) lacking selectivity (e.g Atropine)
C) Rapid withdrawal e.g.* steroid adrenal failure, * clonidine rebound hypertension
D) Tolerance (response due to absorption /efficacy or elimination).can be reachieved by dose):
*Congenital (ephidrine is not medyratic in negroes.
*Acquired: - Acute (tachyphylaxis)e.g Ephidrine on BP - Chronic (drug abuse,antibiotic resistance)
2) 2nd (broad spectrum antibiotic kill gut flora 2nd candidiasis & vit k,B deficiency)
II) Un-predictable (idiosyncrasy): Less common, more dangerous. Dose independent
17
A-genetic abnormality.
1) Rapid & slow acetylators e.g.isoniazide ,procainamide ,hydralazine, sulphonamide, dapson.
2) G.6.p dehydrogenase deficiency (haemolytic anaemia) e.g.primaquine ,aspirine, sulphonamide.
3) Aplastic anaemia e.g chloramphinicol
4) Acute intermittent porphyria e.g barbiturate,alcohol
Protoporphyrine Porphyrine Haeme (Poryphyrin accumulation cause
haemolysis& nerve degeneration. It is treated by Haemin (ALA synthase Is)
5) Ch.E. Abnormalities (apnea) e.g succinyl choline
6) Malignant hyperthrmia e.g. halothane,succinyl choline.
7) Increase IOP e.g. steroid
B-hypersenstivity (Exaggerated immune response damage the tissue .Most of the drugs and
sera used in therapeutics are capable of causing allergic or hypersensitive reactions. These reactions may
be mild or very severe like anaphylaxis. When an individual has been sensitized to an antigen (allergen)
further contact with that antigen can some times lead to tissue damaging reactions. These allergic
reactions are 4 types.
• Type-I reactions or anaphylactic reactions (Immediate hypersensitive reaction).
• Type-II reactions or cytotoxic reactions.
• Type-III reactions or immune complex mediated reactions.
• Type-IV reactions or cell mediated reactions (Delayed hypersensitive reactions).
4) Idiosyncratic reactions: The term idiosyncrasy means one’s peculiar response to drugs. With the
increasing knowledge of pharmacogenetics, many idiosyncratic reactions have been found to be
genetically determined. e.g: Drugs like primaquine, sulfonamides and dapsone may cause haemolysis in
patients with glucose -6 phosphate dehydrogenase defeciency.
Routes of drug administration:
A- Oral:
B- Sublingual: Instruct clients to keep the medication in place until it is absorbed.
Advantage Disadvantage Nursing implications
The oral
route is
safe,
inexpensive, easy and
convenient.
• Oral medications
have a highly
variable
absorption. • Inactivation can
occur by GI tract or
first-pass effect. • The client must
be cooperative and
conscious.
• Contraindications include nausea and
vomiting.
•Contraindications for oral medication administration include vomiting, absence
of gag reflex, difficulty swallowing, and decreased level of consciousness.
• Have the client sitting upright, in Fowler’s or semi- Fowler’s position to
facilitate swallowing. • Administer irritating medications with small amounts of food.
• Do not mix with large amounts of food or beverages in case the client is unable
to consume the entire quantity. • Avoid administration with contraindicated foods or beverages such as
grapefruit juice.
• In general, administer oral medications on an empty stomach (1 hr before
meals, 2 hr after meals). • Follow the manufacturer’s directions for crushing, cutting, and diluting
medications. A complete list can be found at the Institute for Safe Medication
Practice’s Web site (http://www.ismp.org/Tools/DoNotCrush.pdf). • Enteric-coated or time-release medications must be swallowed whole.
• Time-release medications must be swallowed whole to prevent faster
absorption. • Use a liquid form of the medication to facilitateswallowing whenever possible.
ALA synthase
18
C- Liquids, suspensions, elixirs:*Follow directions for dilution and shaking.
• When administering the medication, the base of the meniscus (lowest fluid line) is at the level of the desired dose
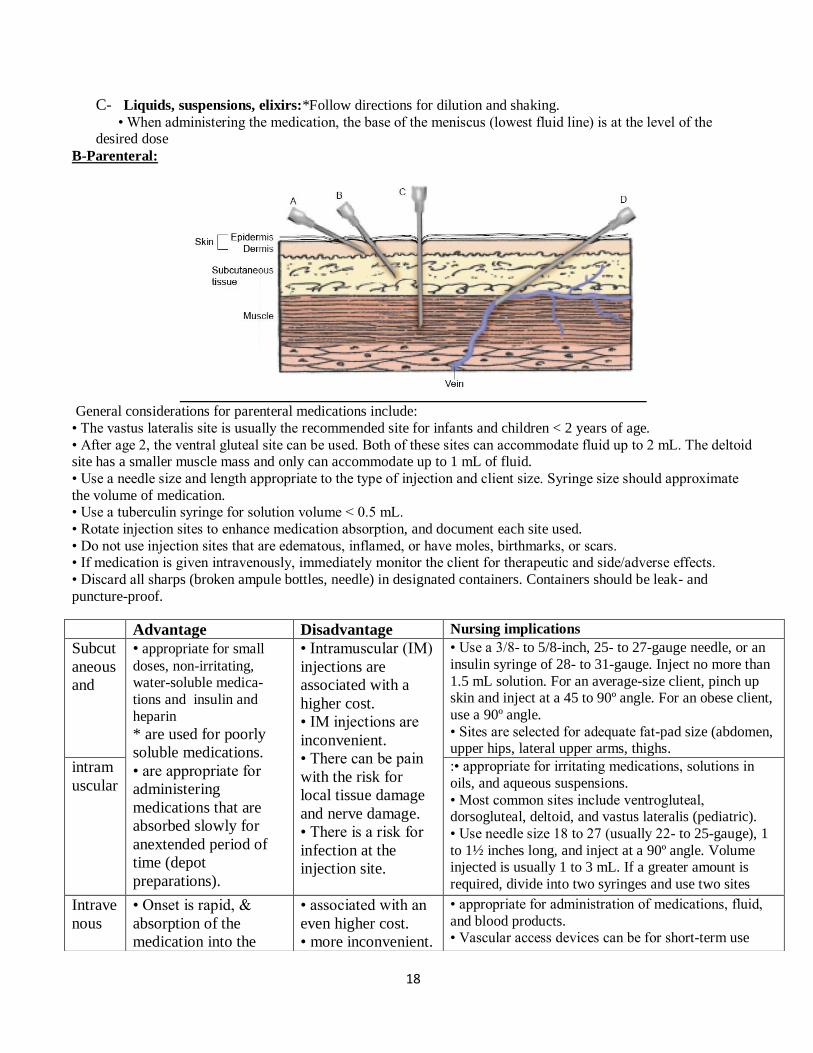
B-Parenteral:
General considerations for parenteral medications include:
• The vastus lateralis site is usually the recommended site for infants and children < 2 years of age.
• After age 2, the ventral gluteal site can be used. Both of these sites can accommodate fluid up to 2 mL. The deltoid site has a smaller muscle mass and only can accommodate up to 1 mL of fluid.
• Use a needle size and length appropriate to the type of injection and client size. Syringe size should approximate
the volume of medication. • Use a tuberculin syringe for solution volume < 0.5 mL.
• Rotate injection sites to enhance medication absorption, and document each site used.
• Do not use injection sites that are edematous, inflamed, or have moles, birthmarks, or scars. • If medication is given intravenously, immediately monitor the client for therapeutic and side/adverse effects.
• Discard all sharps (broken ampule bottles, needle) in designated containers. Containers should be leak- and
puncture-proof.
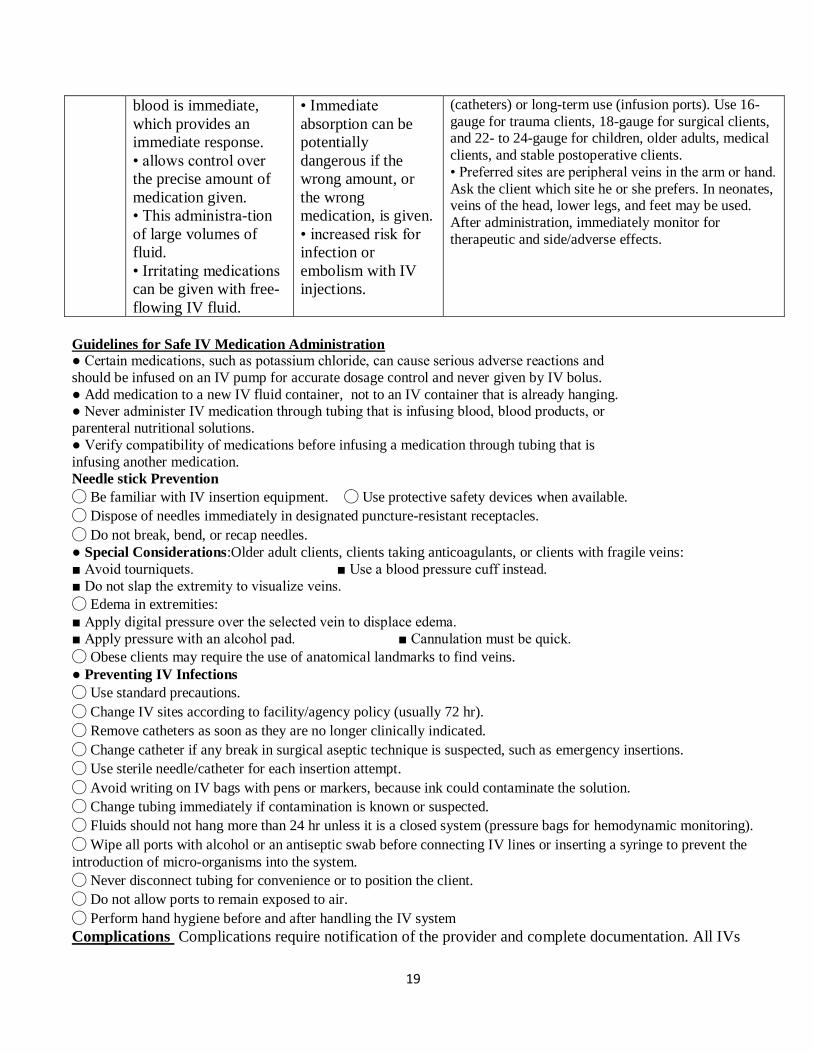
Advantage Disadvantage Nursing implications
Subcut
aneous
and
• appropriate for small
doses, non-irritating, water-soluble medica-
tions and insulin and
heparin
* are used for poorly
soluble medications.
• are appropriate for
administering
medications that are
absorbed slowly for
anextended period of
time (depot
preparations).
• Intramuscular (IM)
injections are
associated with a
higher cost.
• IM injections are
inconvenient.
• There can be pain
with the risk for
local tissue damage
and nerve damage.
• There is a risk for
infection at the
injection site.
• Use a 3/8- to 5/8-inch, 25- to 27-gauge needle, or an
insulin syringe of 28- to 31-gauge. Inject no more than
1.5 mL solution. For an average-size client, pinch up skin and inject at a 45 to 90º angle. For an obese client,
use a 90º angle.
• Sites are selected for adequate fat-pad size (abdomen, upper hips, lateral upper arms, thighs.
intram
uscular
:• appropriate for irritating medications, solutions in
oils, and aqueous suspensions.
• Most common sites include ventrogluteal, dorsogluteal, deltoid, and vastus lateralis (pediatric).
• Use needle size 18 to 27 (usually 22- to 25-gauge), 1
to 1½ inches long, and inject at a 90º angle. Volume injected is usually 1 to 3 mL. If a greater amount is
required, divide into two syringes and use two sites
Intrave
nous
• Onset is rapid, &
absorption of the
medication into the
• associated with an
even higher cost.
• more inconvenient.
• appropriate for administration of medications, fluid,
and blood products. • Vascular access devices can be for short-term use
19
Guidelines for Safe IV Medication Administration ● Certain medications, such as potassium chloride, can cause serious adverse reactions and
should be infused on an IV pump for accurate dosage control and never given by IV bolus.
● Add medication to a new IV fluid container, not to an IV container that is already hanging. ● Never administer IV medication through tubing that is infusing blood, blood products, or
parenteral nutritional solutions.
● Verify compatibility of medications before infusing a medication through tubing that is
infusing another medication.
Needle stick Prevention
◯ Be familiar with IV insertion equipment. ◯ Use protective safety devices when available.
◯ Dispose of needles immediately in designated puncture-resistant receptacles.
◯ Do not break, bend, or recap needles.
● Special Considerations:Older adult clients, clients taking anticoagulants, or clients with fragile veins:
■ Avoid tourniquets. ■ Use a blood pressure cuff instead.
■ Do not slap the extremity to visualize veins.
◯ Edema in extremities:
■ Apply digital pressure over the selected vein to displace edema.
■ Apply pressure with an alcohol pad. ■ Cannulation must be quick.
◯ Obese clients may require the use of anatomical landmarks to find veins.
● Preventing IV Infections
◯ Use standard precautions.
◯ Change IV sites according to facility/agency policy (usually 72 hr).
◯ Remove catheters as soon as they are no longer clinically indicated.
◯ Change catheter if any break in surgical aseptic technique is suspected, such as emergency insertions.
◯ Use sterile needle/catheter for each insertion attempt.
◯ Avoid writing on IV bags with pens or markers, because ink could contaminate the solution.
◯ Change tubing immediately if contamination is known or suspected.
◯ Fluids should not hang more than 24 hr unless it is a closed system (pressure bags for hemodynamic monitoring).
◯ Wipe all ports with alcohol or an antiseptic swab before connecting IV lines or inserting a syringe to prevent the
introduction of micro-organisms into the system.
◯ Never disconnect tubing for convenience or to position the client.
◯ Do not allow ports to remain exposed to air.
◯ Perform hand hygiene before and after handling the IV system
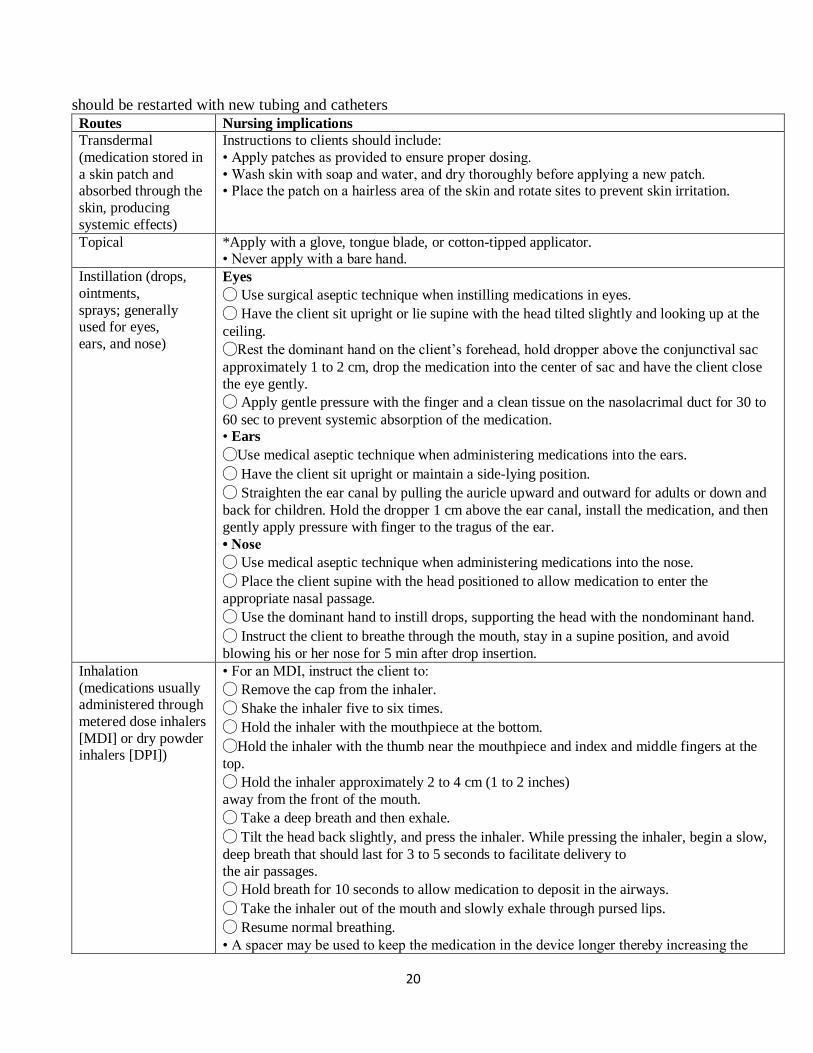
Complications Complications require notification of the provider and complete documentation. All IVs
blood is immediate,
which provides an
immediate response.
• allows control over
the precise amount of
medication given.
• This administra-tion
of large volumes of
fluid.
• Irritating medications
can be given with free-
flowing IV fluid.
• Immediate
absorption can be
potentially
dangerous if the
wrong amount, or
the wrong
medication, is given.
• increased risk for
infection or
embolism with IV
injections.
(catheters) or long-term use (infusion ports). Use 16-
gauge for trauma clients, 18-gauge for surgical clients, and 22- to 24-gauge for children, older adults, medical
clients, and stable postoperative clients.
• Preferred sites are peripheral veins in the arm or hand.
Ask the client which site he or she prefers. In neonates, veins of the head, lower legs, and feet may be used.
After administration, immediately monitor for
therapeutic and side/adverse effects.
20
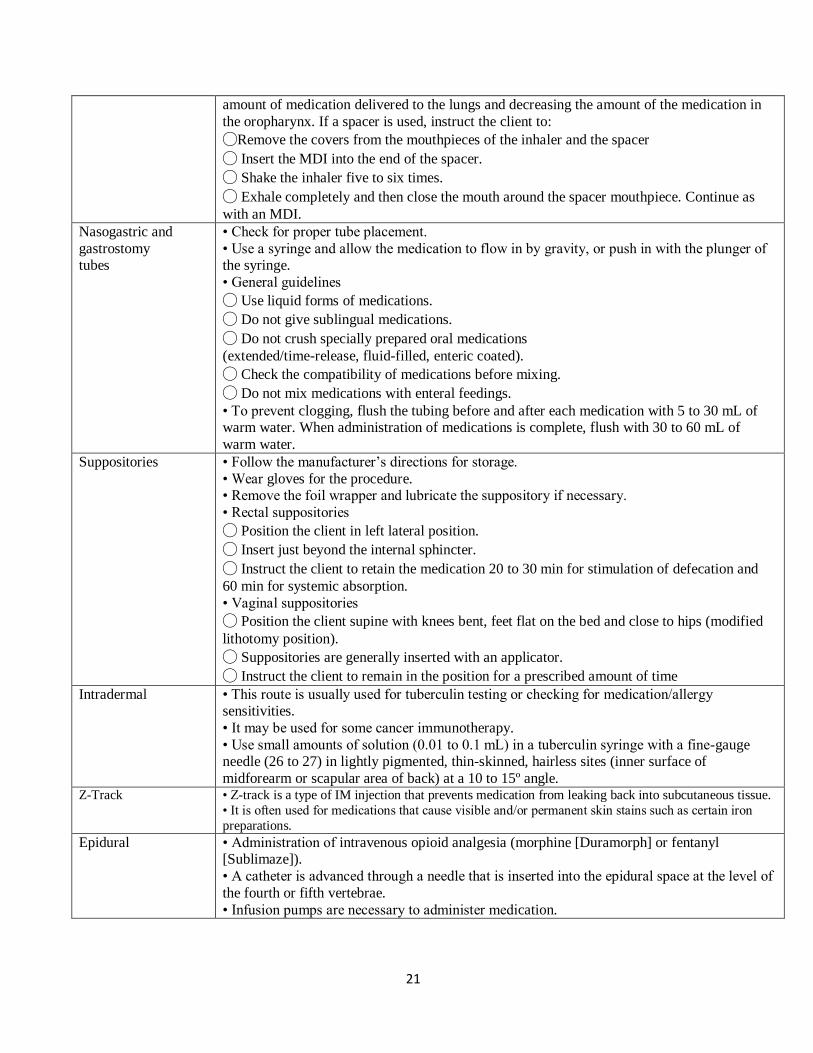
should be restarted with new tubing and catheters
Routes Nursing implications
Transdermal
(medication stored in
a skin patch and absorbed through the
skin, producing
systemic effects)
Instructions to clients should include:
• Apply patches as provided to ensure proper dosing.
• Wash skin with soap and water, and dry thoroughly before applying a new patch. • Place the patch on a hairless area of the skin and rotate sites to prevent skin irritation.
Topical *Apply with a glove, tongue blade, or cotton-tipped applicator. • Never apply with a bare hand.
Instillation (drops,
ointments,
sprays; generally used for eyes,
ears, and nose)
Eyes
◯ Use surgical aseptic technique when instilling medications in eyes.
◯ Have the client sit upright or lie supine with the head tilted slightly and looking up at the
ceiling.
◯Rest the dominant hand on the client’s forehead, hold dropper above the conjunctival sac
approximately 1 to 2 cm, drop the medication into the center of sac and have the client close
the eye gently.
◯ Apply gentle pressure with the finger and a clean tissue on the nasolacrimal duct for 30 to
60 sec to prevent systemic absorption of the medication. • Ears
◯Use medical aseptic technique when administering medications into the ears.
◯ Have the client sit upright or maintain a side-lying position.
◯ Straighten the ear canal by pulling the auricle upward and outward for adults or down and
back for children. Hold the dropper 1 cm above the ear canal, install the medication, and then
gently apply pressure with finger to the tragus of the ear.
• Nose
◯ Use medical aseptic technique when administering medications into the nose.
◯ Place the client supine with the head positioned to allow medication to enter the
appropriate nasal passage.
◯ Use the dominant hand to instill drops, supporting the head with the nondominant hand.
◯ Instruct the client to breathe through the mouth, stay in a supine position, and avoid
blowing his or her nose for 5 min after drop insertion.
Inhalation
(medications usually administered through
metered dose inhalers
[MDI] or dry powder inhalers [DPI])
• For an MDI, instruct the client to:
◯ Remove the cap from the inhaler.
◯ Shake the inhaler five to six times.
◯ Hold the inhaler with the mouthpiece at the bottom.
◯Hold the inhaler with the thumb near the mouthpiece and index and middle fingers at the
top.
◯ Hold the inhaler approximately 2 to 4 cm (1 to 2 inches)
away from the front of the mouth.
◯ Take a deep breath and then exhale.
◯ Tilt the head back slightly, and press the inhaler. While pressing the inhaler, begin a slow,
deep breath that should last for 3 to 5 seconds to facilitate delivery to
the air passages.
◯ Hold breath for 10 seconds to allow medication to deposit in the airways.
◯ Take the inhaler out of the mouth and slowly exhale through pursed lips.
◯ Resume normal breathing.
• A spacer may be used to keep the medication in the device longer thereby increasing the
21
amount of medication delivered to the lungs and decreasing the amount of the medication in
the oropharynx. If a spacer is used, instruct the client to:
◯Remove the covers from the mouthpieces of the inhaler and the spacer
◯ Insert the MDI into the end of the spacer.
◯ Shake the inhaler five to six times.
◯ Exhale completely and then close the mouth around the spacer mouthpiece. Continue as
with an MDI.
Nasogastric and
gastrostomy tubes
• Check for proper tube placement.
• Use a syringe and allow the medication to flow in by gravity, or push in with the plunger of the syringe.
• General guidelines
◯ Use liquid forms of medications.
◯ Do not give sublingual medications.
◯ Do not crush specially prepared oral medications
(extended/time-release, fluid-filled, enteric coated).
◯ Check the compatibility of medications before mixing.
◯ Do not mix medications with enteral feedings.
• To prevent clogging, flush the tubing before and after each medication with 5 to 30 mL of warm water. When administration of medications is complete, flush with 30 to 60 mL of
warm water.
Suppositories • Follow the manufacturer’s directions for storage.
• Wear gloves for the procedure. • Remove the foil wrapper and lubricate the suppository if necessary.
• Rectal suppositories
◯ Position the client in left lateral position.
◯ Insert just beyond the internal sphincter.
◯ Instruct the client to retain the medication 20 to 30 min for stimulation of defecation and
60 min for systemic absorption.
• Vaginal suppositories
◯ Position the client supine with knees bent, feet flat on the bed and close to hips (modified
lithotomy position).
◯ Suppositories are generally inserted with an applicator.
◯ Instruct the client to remain in the position for a prescribed amount of time
Intradermal • This route is usually used for tuberculin testing or checking for medication/allergy sensitivities.
• It may be used for some cancer immunotherapy.
• Use small amounts of solution (0.01 to 0.1 mL) in a tuberculin syringe with a fine-gauge needle (26 to 27) in lightly pigmented, thin-skinned, hairless sites (inner surface of
midforearm or scapular area of back) at a 10 to 15º angle. Z-Track • Z-track is a type of IM injection that prevents medication from leaking back into subcutaneous tissue.
• It is often used for medications that cause visible and/or permanent skin stains such as certain iron
preparations.
Epidural • Administration of intravenous opioid analgesia (morphine [Duramorph] or fentanyl [Sublimaze]).
• A catheter is advanced through a needle that is inserted into the epidural space at the level of
the fourth or fifth vertebrae.
• Infusion pumps are necessary to administer medication.
22