pharmacotherapy for the treatment of nicotine dependence donna shelley, md, mph, columbia university...
Post on 19-Dec-2015
216 views
TRANSCRIPT

Pharmacotherapy for the Treatment of Nicotine Dependence
Donna Shelley, MD, MPH, Columbia University Mailman
School of Public [email protected]
Submitted by the NY/NJ AETC

Outline
System changes to increase tobacco use treatment
Pharmacotherapy Referral sources

Why should I treat tobacco use?
I in 5 deaths in the US are due to smoking
1 in 3 cancer deaths are caused by smoking
70% of smoker want to quit
64% of New Yorkers who smoke tried to quit in the past 12 months NYC Community Health Survey 2001
Less than 10% succeed without assistance

Provider
Friends
Internet
Family
TV, Radio
Faith Community
Community
Newspapers,Magazines
Co-workers
ROLE OF THE HEALTH CARE TEAM
Multiple Influences on a Tobacco User
MD assisted quit rates at one yr are 10-30%

“Not enough time”
“Minimal interventions
lasting less than 3 minutes increase overall tobacco abstinence rates.”
The PHS Guideline
(Strength of Evidence = A)

“I can’t help patients stop.”
Effective interventions
exist: Pharmacotherapy
Brief counseling
System changes
Guideline available at www.ahrq.gov

Tobacco use results in a true drug dependence
Tobacco dependence exhibits classic characteristics of drug dependence
Nicotine:Nicotine is as addictive as heroinCauses physical dependence characterized by
withdrawal symptoms upon cessationSmokers use tobacco to regulate their moods and
emotions

Tobacco dependence is achronic disease
Tobacco dependence requires ongoing rather than acute care
Relapse is a component of the chronic nature of the nicotine dependence — not an indication of personal failure by the patient or the clinician

The 5 A’sFor Patients Willing To Quit
ASK about tobacco use. ADVISE to quit. ASSESS willingness to make a
quit attempt. ASSIST in quit attempt. ARRANGE for follow-up.

Smoking as a vital signSmoking as a vital sign (SVS) (SVS) ASK ASK: :
Ask every patient at every visit
Progress note vital signs BP: __________ Weight: _______ Ht: _______ BMI :_____ Tobacco Use: Yes No Former Advise to quit Y N Ready to quit? Y N Rx given Y N Referral made Y N
“Do you currently use any tobacco products?”

Interventionrate (95% C.I.)
CessationOR Rates(95% C.I.)
38.5 % 1.0 3%
65.6% 3.1 6.4%
No Screening System
Screening system in place to ID smoking status
Impact of smoking status identification system on rates of clinician intervention:
BASED ON 9 RANDOMIZED STUDIES AHRQ GUIDELINES, 2000

ProgressNote
Vital signs
Date: ___________ Temp: __________
BP: ___________ Pulse: __________
Height: _______ Weight: ______ BMI: _______
Yes No Tobacco Use □ □ Advice Given □ □ Ready To Quit □ □ Referral Made □ □ Rx Given □ □

ADVISEADVISE
Progress note vital signs BP: __________ Weight: _______ Ht: _______ BMI :_____ Tobacco Use: Yes No Former Advise to quit Y N Ready to quit? Y N Rx given Y N Referral made Y N
Advice should be: clear, strong, personalized
ADVISE
Even brief advice to quit results in greater quit rates
“As your health care provider, I must tell you that the most important thing you
can do to improve your health is to stop smoking.”
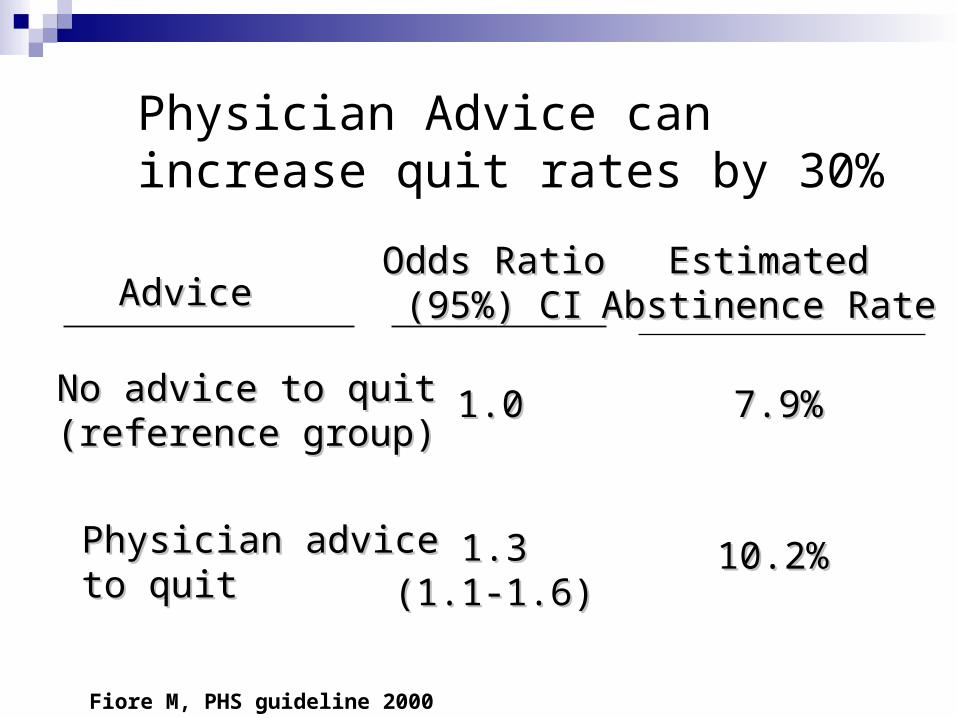
Physician Advice can increase quit rates by 30%
AdviceAdvice
Odds RatioOdds Ratio(95%) CI(95%) CI
No advice to quit No advice to quit (reference group)(reference group)
Physician advicePhysician adviceto quitto quit
7.9%7.9%1.01.0
10.2%10.2%1.31.3(1.1-1.6)(1.1-1.6)
EstimatedEstimatedAbstinence RateAbstinence Rate
Fiore M, PHS guideline 2000

Assess willingness to quitAssess willingness to quit
Progress note vital signs BP: __________ Weight: _______ Ht: _______ BMI :_____ Tobacco Use: Yes No Former Advise to quit Y N Ready to quit? Y N Rx given Y N Referral made Y N
“Are you willing to try to quit at this time? I can help you.”

ASSISTASSIST
Help set a quit date Provide practical counseling
(alcohol, other smokers in home) Past quit experiences Anticipate challenges

Counsel your patients to quit: Minimum advice increases quit rates by 30%
Level of contact Estimated odds ratio
Est. abstinence rate
No contact 1.0 10.9
Min counseling < 3 min 1.3 13.4
Low intensity
3-10 min
1.6 16
>10 minutes 2.3 22.1

Assist: Pharmacotherapy
Progress note vital signs BP: __________ Weight: _______ Ht: _______ BMI :_____ Tobacco Use: Yes No Former Advise to quit Y N Ready to quit? Y N Rx given Y N Referral made Y N

“Pharmacotherapy should be offered to all smokers trying to quit except where contraindicated.”
Fiore 2000

First-line pharmacotherapy
Nicotine Replacement Therapy
Patch
Gum Lozenge
Inhaler
Nasal spray
Bupropion (Zyban)
Non nicotine replacement

Pharmacotherapy

Estimated odds ratio for long term abstinence
1.81 1.66
2.142.35
2.05 2.1
0
0.5
1
1.5
2
2.5
Patch Gum Inhaler Spray Lozenge Bupropion
Fiore 2000

Nicotine Replacement Therapy (NRT) No evidence that nicotine causes cancer No evidence of increased cardiovascular risk with
NRT Medical contraindications:
immediate myocardial infarction (< 2 weeks) serious arrhythmia serious or worsening angina pectoris accelerated hypertension
Joseph 1996, Ford 2005, Working Group 1994 Arch Int Med

Plasma nicotine levels after a cigarette vs. different types of pharmacotherapy
0
5
10
15
20
25
30
0 20 40 60 80 100
120
Cigarette Patch Gum Nasal Spray

Withdrawal Symptoms
Anxiety/Irritability Poor concentration Restlessness Craving Headaches Drowsiness Depression Hunger

NRT: Nicotine patch
24 hr (21, 14, 7mg) Nicoderm/generic or 16 hr (15, 10, 5 mg) Nicotrol Available OTC A new patch is applied each morning Rotating placement site can reduce irritation 6 weeks for 1st dose-taper over 4-6 weeks Side effects: Insomnia, local rash

NRTs: Patches Need to be Individualized <10 CPD may consider 7mg 10-15 CPD = 14-21 mg/day patch 15-20 CPD = 21 mg/day
21mg=21 cigs/d 14mg=14 cigs/d

NRT: Nicotine gum 2 mg (<25 cigs) vs 4 mg (>24 cigs) 1-2 per hour for first 6 weeks-taper Chew (release peppery taste) and park, continue for
30 minutes Absorbed in a basic environment, avoid acidic
beverages 15 minutes pre and during dose (coffee, soda, juice)
Use enough pieces each day (max 24) Side effects: dyspepsia, mouth soreness
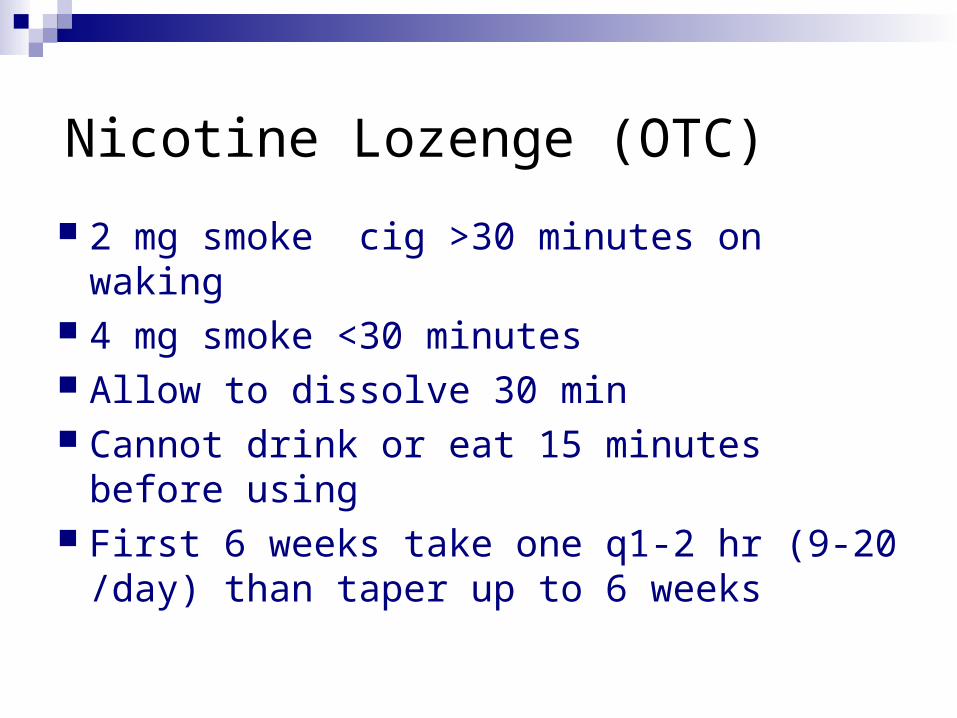
Nicotine Lozenge (OTC)
2 mg smoke cig >30 minutes on waking 4 mg smoke <30 minutes Allow to dissolve 30 min Cannot drink or eat 15 minutes before
using First 6 weeks take one q1-2 hr (9-20 /day)
than taper up to 6 weeks

NRT: Nicotine inhaler
Available by prescription
Continuous puffing over 20 minutes per dose (80 puffs per dose delivers 4 mg)
6-16 cartridges per day for 12 weeks
Eating or drinking before and during administration should be avoided


NRT: Nicotine nasal spray Available by prescription
Patient should not sniff, swallow, or inhale the medication
A dose is 2 squirts, one to each nostril
Initial dosing should be 1 to 2 doses per hour, increasing as needed up to 6-8 weeks and than taper
Dosing should not exceed 40 doses per day

Bupropion SR (Zyban®) Mechanism of action: presumably blocks
neural reuptake of dopamine and/or norepinephrine
Dosing: start 2 weeks before quit date 150 mg orally once daily x 3 day 150 mg orally twice daily x 7-12 weeks no taper necessary at end of treatment
Maintenance - efficacious as maintenance medication for 6 months post-cessation

Bupropion SR (Zyban®)
Contraindications Seizure disorder Current use of Wellbutrin Bulimia/anorexia MAO inhibitor in past 14 days Heavy alcohol use
Side effects: Dry mouth Insomnia (avoid bedtime dose)

Factors to Consider When Choosing a Pharmacotherapy
Patient preference Clinician familiarity with the medications Contraindications for selected patients Previous patient experiences with a
specific agent (positive or negative) Patient characteristics (concern about
weight gain, history of depression)

Reimbursement ICD9: 305.1 AND CPT code 99401 (15-minute physician-
provided counseling)OR
CPT code 99211 (nurse counseling) NYS Medicaid benefit: NRT, Zyban are
reimbursed (two 3 mo courses per year, may prescribe more than one medication)

Reimbursement
Medicare2 cessation attempts per year including max 4
sessions, up to 8 sessions per 12 monthsMust wait 11 months from the 1st of the 8
sessionsG0375 3-10 minutesG0376 >10 min1800 633 4227 (1 800 MEDICARE)

ASSIST: Next StepsASSIST: Next Steps
Progress note vital signs BP: __________ Weight: _______ Ht: _______ BMI :_____ Tobacco Use: Yes No Former Advise to quit Y N Ready to quit? Y N Rx given Y N Referral made Y N

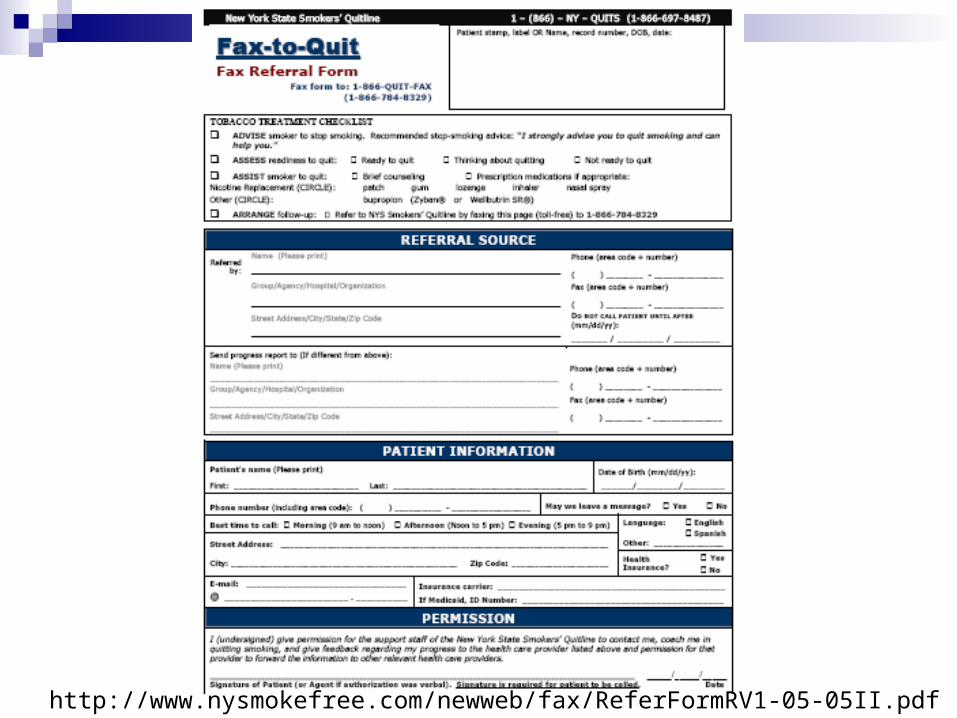
http://www.nysmokefree.com/newweb/fax/ReferFormRV1-05-05II.pdf

Resources
www.nysmokefree.org

Resources
Smoking cessation programs in NYC
http://www.nyc.gov/html/doh/html/smoke/quit.shtml


How do I treat tobacco users who are not willing to make a quit attempt?

Treating patients who are not ready to make a quit attempt
RELEVANCE: Tailor advice and discussion to each patient.
RISKS: Outline risks of continued smoking.
REWARDS: Outline the benefits of quitting.
ROADBLOCKS: Identify barriers to quitting.
REPETITION: Reinforce the motivational message at every visit.

Resources
Physician resources AHRQ www.ahrq.gov or 800-358 9295
Physician guides Patient tear sheets free
NYCDOH: City Health Informationhttp://www.nyc.gov/html/doh/html/smoke/smoke.html
http://www.nyc.gov/html/doh/pdf/chi/chi21-6.pdf
Patient websites/materials www.quitnet.com, www.smokeclinic.com http://www.nyc.gov/html/doh/html/smoke/smoke2-cess1.html

Medication – Daily Cost
Bupropion 150 SR $3.00 /day
Transdermal 7 to 21 $4.00 / patch ($40/box 14)
Lozenge 2mg or 4 mg $7.00 / 10 pieces
Gum 2 mg or 4 mg $5.00 / 10 pieces
Nasal Spray $6.00 / 12 sprays
Inhaler $11.00 / 10 cartridges