pharmacotherapy of child and adolescent depression
TRANSCRIPT

Child Adolesc Psychiatric Clin N Am
15 (2006) 977–998
Pharmacotherapy of Childand Adolescent Depression
Carmen Moreno, MDa,*, Ansley M. Roche, BAb,Laurence L. Greenhill, MDa
aDivision of Child Psychiatry, New York State Psychiatric Institute,
College of Physicians and Surgeons of Columbia University, 1051 Riverside Drive,
Unit 74, New York, NY 10032, USAbDivision of Child Psychiatry, New York State Psychiatry Institute,
Columbia University, New York, NY 10032, USA
At a given point in time, 3 in every 100 school aged children, 5 in every100 adolescents, and 15 in every 100 young adults experience a major de-pressive episode [1]. Prevalence of major depression in late adolescenceand early adulthood is close to adult rates [2–5]. Depressed children also ex-perience the cognitive and social impairment associated with adult depres-sion. Poor school performance, poor peer relations, troubled familyfunctioning [6], and suicidality [7] have been associated with child and ado-lescent depression. The risk of depression persisting into adulthood isincreased twofold, and the risk of a first suicide is increased fivefold in adultswho had adolescent-onset depression compared with adults who had theirfirst depressive episode in adulthood [8].
A major depressive episode can last up to 9 months in children, with 90%of them remitting within 1.5 to 2 years after onset [9]. Longitudinal studieshave shown that most major depressive episodes recur after 5 years, however[8,9]. Although the number of visits to physicians by depressed children and
This work was supported by the Alicia Koplowitz Foundation Fellowship Award in
Child and Adolescent Psychiatry, (C.M.), Conte Center for the Neuroscience of Mental
Disorder, 1005007, PI: J John Mann (L.L.G.).
Laurence L Greenhill has received grants from NIMH, McNeil (Pending), Lilly,
Cephalon, Novartis, and Otsuka (pending). He has served as a consultant to Cephalon, Lilly,
Novartis, and Otsuka. He is a member of DSMB for Janssen and Pfizer and has been
a speaker for Lilly and Janssen Cilag. None of the authors has received funding to write this
article.
* Corresponding author.
E-mail address: [email protected] (C. Moreno).
1056-4993/06/$ - see front matter � 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.chc.2006.05.006 childpsych.theclinics.com

978 MORENO et al
adolescents has increased in recent years in the United States [10], as manyas two thirds of the cases of pediatric depression are still not treated [3,11].
Untreated depression in children and adolescents remains a serious pub-lic health concern associated with significant morbidity and risk of mortal-ity. Because major depressive disorder often has its onset in early years andthe percentage of people affected seems to increase with age and persist intoadulthood, the need for identification and treatment at an early age is of ut-most importance.
Historical background
Timeline of treatment of depression in children and adolescents
Recognition that children and adolescents can experience depression isa relatively recent phenomenon [12]. This delay has contributed further tothe lag between development of child and adult treatments. Although anti-depressants have been studied and used in adults for more than 40 years, itwas not until the 1980s that the first medications used to treat depressedadults, the tricyclic antidepressants (TCAs), began being tested in pediatricpopulations in randomized controlled trials (RCTs). The first trials in de-pressed youths studied imipramine [13–16], amitryptiline [17,18], and nor-tryptiline [19,20]. Most of them were pilot studies, included only children,and were negative. In the 1990s, additional studies with TCAs were con-ducted, but almost entirely in adolescents. Besides amitriptyline [21,22], de-sipramine [23,24] and clomipramine [25] were tested, with still no clearindication of efficacy. In the late 1980s, however, a new class of antidepres-sants, the selective serotonin reuptake inhibitors (SSRIs), was introduced tothe market and began being studied in the pediatric population. The firstpositive study of an antidepressant medication in children and adolescents,fluoxetine, was published in 1997 [26], which followed a negative small trial[27]. Since then, fluoxetine [28,29], paroxetine [30], sertraline [31], and cita-lopram [32] have been tested in RCTs. Newer antidepressants also have beenstudied, but results are published only for venlafaxine [33]. There is still de-bate concerning the interpretation of the results of several of these studies, inpart because of nonpublication of negative trials. Although overall qualityhas improved with respect to the underpowered TCA studies, methodologicproblems continue, and a lack of homogeneity in the trials makes it difficultto compare them and extract meaningful generalizable results [34–36].
Increase in number of antidepressant studies in children and adolescents
In the past 10 years, the same number of pediatric antidepressant RCTsfor pediatric depression (12) than in all years prior has been published.There also has been an exponential increase in the number of youth studiedin RCTs of antidepressants over time. Sample sizes are approximately eight

979PHARMACOTHERAPY OF CHILD AND ADOLESCENT DEPRESSION
to ten times bigger in the most recent studies than in the earliest ones, andmore than 2000 children already have been studied in treatment arms.Depression still remains understudied in this age group, however.
Trends in the use of selective serotonin reuptake inhibitorsin children and adolescents
The last decade witnessed an increase in the prescription rates of SSRIsand newer antidepressants, especially by general practitioners [37]. The in-crease in the use of SSRIs was exceptionally striking among children[38,39], with notably high increases for paroxetine, fluoxetine, or sertraline[10].
Recently, regulatory agencies, first in the United Kingdom [40] and laterin the United States [41], have issued warnings against the use of SSRIs andnewer antidepressants in depressed children and adolescents because ofa possible link between their use and the appearance or worsening of sui-cidal ideation or attempts. Since then, there seems to have been a shift inpractice patterns. Analysis of general practitioners’ prescription practicesin the United Kingdom show that antidepressant prescribing to childrenand adolescents has begun to drop since the Medicines and HealthcareProducts Regulatory Agency warning. Although prescription rates of fluox-etine remained the same between 2002 and 2004, prescriptions for the otherSSRIs decreased by one third and significantly declined for TCAs in thatsame period [42]. In the United States, preliminary analysis suggests that be-ginning in 2004 there has been a decline in prescription rates of antidepres-sants by approximately 20% in the pediatric population, whereas adult rateshave remained steady [43]. If confirmed, the potential consequences of thisreduction in use of antidepressants, especially with regards to increase insuicide rates among depressed pediatric patients, must be monitored closely.
Psychopharmacologic treatment
Acute treatment
Although TCAs are still considered a viable treatment option for adultdepression [44], efficacy for pediatric depression has not been demonstrated[45]. In this section we focus on the available evidence of more promisingtreatments and comment on newer medications that are beginning to betested.
Efficacy results are presented with special mention to primary outcomemeasuresdthe ones considered by regulatory agencies when deciding the in-dication of a drug for approval (Table 1). It should be noted that in the re-viewed trials there was a wide array of proposed primary outcome measures,including change from baseline on the Children’s Depression Rating Scale-Revised (CDRS-R) [29], improvement of at least 30% [26,28] or 40% [31] on
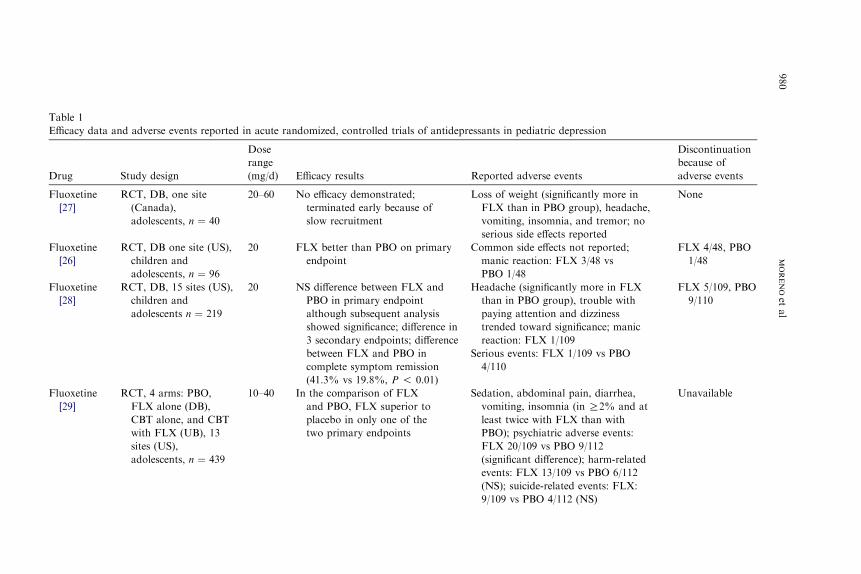
Table 1
Efficacy da n pediatric depression
Drug d adverse events
Discontinuation
because of
adverse events
Fluoxetine
[27]
weight (significantly more in
than in PBO group), headache,
ing, insomnia, and tremor; no
s side effects reported
None
Fluoxetine
[26]
n side effects not reported;
reaction: FLX 3/48 vs
1/48
FLX 4/48, PBO
1/48
Fluoxetine
[28]
e (significantly more in FLX
n PBO group), trouble with
g attention and dizziness
d toward significance; manic
on: FLX 1/109
events: FLX 1/109 vs PBO
FLX 5/109, PBO
9/110
Fluoxetine
[29]
, abdominal pain, diarrhea,
ing, insomnia (in R2% and at
wice with FLX than with
; psychiatric adverse events:
20/109 vs PBO 9/112
ficant difference); harm-related
: FLX 13/109 vs PBO 6/112
suicide-related events: FLX:
vs PBO 4/112 (NS)
Unavailable
980
MORENOet
al
ta and adverse events reported in acute randomized, controlled trials of antidepressants i
Study design
Dose
range
(mg/d) Efficacy results Reporte
RCT, DB, one site
(Canada),
adolescents, n ¼ 40
20–60 No efficacy demonstrated;
terminated early because of
slow recruitment
Loss of
FLX
vomit
seriou
RCT, DB one site (US),
children and
adolescents, n ¼ 96
20 FLX better than PBO on primary
endpoint
Commo
manic
PBO
RCT, DB, 15 sites (US),
children and
adolescents n ¼ 219
20 NS difference between FLX and
PBO in primary endpoint
although subsequent analysis
showed significance; difference in
3 secondary endpoints; difference
between FLX and PBO in
complete symptom remission
(41.3% vs 19.8%, P ! 0.01)
Headach
than i
payin
trende
reacti
Serious
4/110
RCT, 4 arms: PBO,
FLX alone (DB),
CBT alone, and CBT
with FLX (UB), 13
sites (US),
adolescents, n ¼ 439
10–40 In the comparison of FLX
and PBO, FLX superior to
placebo in only one of the
two primary endpoints
Sedation
vomit
least t
PBO)
FLX
(signi
events
(NS);
9/109
Paroxetine
[3
RCT, DB, 3 arms: 20–40 Statistical difference between PAR Somnolence (significantly more in
AR than in PBO group), headache,
usea, dizziness, dry mouth,
otional lability, hostility,
somnia, tremor
ous events: PAR 11/93
uicide-related events 5, hostility 2,
phoria/expansive mood 1) vs
BO 2/87
PAR 9/93, PBO
6/87
Par
[5
eased cough, dyspepsia, vomiting,
d dizziness (in R5% and at least
ice with PAR than with PBO)
ous events: PAR 6/104 vs
BO 1/102
ide-related events: PAR
104 vs PBO 1/102 (NS)
PAR 9/104,
PBO 2/102
Par
[4
iness, emotional lability,
somnia, somnolence (in R3%
PAR treated patients)
ous events: PAR 22/187 vs
BO 6/99
PAR 22/187,
PBO 7/99
Sert
[3
rrhea, nausea, vomiting, anorexia,
itation, insomnia (in R5% and at
ast twice with SERT than with
BO)
ous events: SERT 7/189
suicide-related, 1 hostility-events)
PBO 6/187 (2 suicide-related
ents
SERT 17/189,
PBO 4/187
(continued on next page)
981
PHARMACOTHERAPY
OFCHIL
DAND
ADOLESCENTDEPRESSIO
N
0] imipramine, PAR,
and PBO, 12 sites (10
in US, 2 in Canada),
adolescents n ¼ 180
and PBO on one primary
endpoint; difference in 3 out of
5 secondary endpoints
Statistical difference in symptom
remission between PAR and
PBO (HAM-D!8, 63.3% vs
46.0%, P ¼ 0.02)
P
na
em
in
Seri
(s
eu
P
oxetine
0,51]
RCT, DB, 41 sites (US
Canada), children and
adolescents, n ¼ 203
10–40 No efficacy demonstrated Incr
an
tw
Seri
P
Suic
3/
oxetine
8,49]
RCT, DB, 33 sites
(international),
adolescents, n ¼ 286
20–40 No efficacy demonstrated Dizz
in
of
Seri
P
aline
1]
Data pooled from 2
RCT, DB, 53 sites
(international),
children and
adolescents, n ¼ 376
50–200 No statistical difference between
SERT and PBO in any of the
studies analyzed separately;
when analyzed together, SERT
was found to be significantly
better than PBO in the primary
endpoint
Dia
ag
le
P
Seri
(5
vs
ev

Table 1 (continued )
D Reported adverse events
Discontinuation
because of
adverse events
C Nausea, rhinitis, abdominal pain
(in R10% of CIT treated patients);
fatigue, diarrhea, back pain (in
O5% of CIT treated patients); In all,
incidence in CIT exceeded incidence
in PBO
No observed serious side effects
CIT 2/93,
PBO 2/85
C Nausea, insomnia, headache, rhinitis,
abdominal pain, dizziness,
pharyngitis, diarrhea, fatigue,
influenza-like symptoms (in O5%
and more in CIT than in
PBO treated patients)
Suicide-related events: CIT
14/124 vs PBO 5/120
Serious events: CIT
16/124 vs PBO 9/120
CIT 13/124,
PBO 9/120
V Nausea, increased appetite
(significantly more in VFX
than in PBO group); no serious
events reported
VFX 1/20 vs
PBO 0/20
982
MORENOet
al
rug Study design
Dose
range
(mg/d) Efficacy results
italopram
[32]
RCT, DB, 21 sites (US),
children and
adolescents n ¼ 174
20–40 Statistical difference between CIT
and PBO in primary endpoint;
primary endpoint was also
remission (36% vs 24%,
P ! 0.05)
italopram
[52]
RCT, DB, mutli-site,
adolescents, n ¼ 244,
inpatients and
outpatients
10–40 No efficacy demonstrated
enlafaxine
[33]
RCT, DB one site (US),
children and
adolescents, n ¼ 40,
concomitant therapy
in both arms
37.5–75 No efficacy demonstrated

Venlafaxine
[
RCT, DB, multi-site, 37.5–225 No efficacy demonstrated Reported together: abdominal pain,
anorexia (in R5% and at least twice
with VFX than with PBO), nausea,
vomiting, weight loss, insomnia
erious events: VFX
14/169 vs PBO 5/165
ostility and suicide-related events,
more in VFX than in PBO
VFX 9/68,
PBO 4/73
Ve
[
VFX8/101,
PBO 1/92
Ne
[
erious events: none in NFZ,
unavailable for PBO
NFZ 3/99,
PBO 3/96
Ne
[
navailable Unavailable
Mi
[
erious events: MTZ 2 vs PBO 1 Adverse events
reported as
one sample
size for both
studies
MTZ 5.3%,
PBO 3.4%
Mi
[
navailable
Esc
[
eadache abdominal pain (in O10%
of patients in ESC and PBO groups)
uicide-related events:
ESC 1/131 vs PBO 2/133
ESC 3/131,
PBO 3/133
TZ, mirtazapine; NFZ, nefazodone; NS, nonsignificant; PAR,
par faxine.
983
PHARMACOTHERAPY
OFCHIL
DAND
ADOLESCENTDEPRESSIO
N
52,54] children and
adolescents, n ¼ 141
S
H
nlafaxine
52,54]
RCT, DB, multi-site,
children and
adolescents, n ¼ 193
37.5–225 No efficacy demonstrated
fazodone
55]
RCT, DB, 15 sites (US),
adolescents, n ¼ 195
300–600 No difference between NFZ and
PBO in primary endpoint;
difference in some secondary
endpoints
S
fazodone
55]
RCT, DB, 28 sites (US),
children and
adolescents, n ¼ 284
50–600 No efficacy demonstrated U
rtazapine
56]
RCT, DB, 17 sites (US),
children and
adolescents n ¼ 126
15–45 No efficacy demonstrated S
rtazapine
56]
RCT, DB, 17 sites (US),
children and
adolescents, n ¼ 133
15–45 No efficacy demonstrated U
italopram
53]
RCT, DB, multi-site
children and
adolescents, n ¼ 264
10–20 No efficacy demonstrated H
S
Abbreviations: CIT, citalopram; DB, double blind; ESC, escitalopram; FLX, fluoxetine; M
oxetine; RCT, randomized, controlled trial; SERT, sertraline; UB, unblinded; VFX, venla

984 MORENO et al
the CDRS-R, improvement of R50% on the Montgomery-Asperg Depres-sion Rating Scale [46], minimal symptoms of depression as measured by theHamilton Depression Scale (score %8) [30] or by CDRS- R (score %28)[32], or ‘‘much’’ or ‘‘very much’’ improved on the scale of clinical global im-provement [26,29]. This marked lack of uniformity in outcome measuresmakes comparison between trials difficult and speaks for urgent need foruniversally adopted methods to assess efficacy data. A decision should bemade as to whether to use as outcome the rate of response or remission,which is a more clinically relevant outcome measure.
Among the SSRIs there are already some data for fluoxetine, paroxetine,sertraline, citalopram, and escitalopram. Fluoxetine has been studied mostextensively: four randomized trials thus far. The first was a single-site trialin adolescents, and no difference was found between drug and placeboarms [27]. The second, a single-site trial, was the first to demonstrate efficacyof an SSRI to treat pediatric depression [26]. Results were conclusive thatmedication was significantly better than placebo in primary outcome mea-sures: reduction on weekly CDRS-R score (58% versus 32%; P ¼ 0.013)and clinical global improvement scale improvement of 1 or 2 (56% versus33%; P ¼ 0.02). A replication multi-site study published 5 years later failedto demonstrate statistical difference between fluoxetine and placebo in theprimary efficacy measure (R30% improvement in CDRS-R responserate), although changes in CDRS-R subscores, other levels of improvementon the CDRS-R (from 20%–70%), and three out of seven secondary out-comes were positive [28]. Subsequent analysis determined that the lack ofsignificance of the primary outcome was caused by an error in the waythe calculations were performed and that after controlling for the CDRS-R at study entry the difference was significant [47,48]. The most recent study,a four-pronged multi-site trial that compared placebo, fluoxetine, cognitivebehavioral therapy (CBT), and combined fluoxetine and CBT treatment,concluded that combined treatment was superior to any of the other treat-ment modalities, although comparisons involving CBT were nonblinded.The study only showed statistical differences among fluoxetine and placeboin one of the primary endpointsdthe end-of-treatment clinical global im-provement (60.6% versus 34.8%; P ¼ 0.001)dbut not in the otherdtheCDRS-R total score (36.30 versus 41.77; P ¼ 0.10) [29].
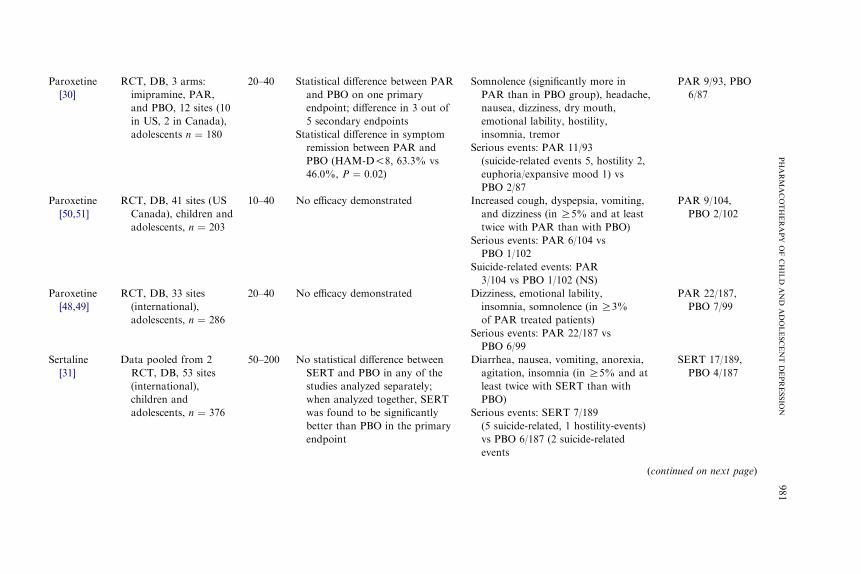
One published study compared paroxetine and placebo in depressedadolescents. In this trial, paroxetine separated from placebo in one of thetwo proposed primary outcomes (response), defined as Hamilton DepressionScale (HAM-D) score %8 at endpoint (63.3% versus 46%; P ¼ 0.02), and inthree out of five secondary outcomes [30]. Interpretation has been controver-sial. The proposed outcome was HAM-D score %8 or R50% reduction inbaseline HAM-D score at endpoint, and when both were considered, resultswere not significant (66.7% versus 55.2%; P ¼ 0.11). Two other paroxetineRCTs have been conducted and the findings presented in scientific meetings.One study did not reveal differences between paroxetine and placebo for

985PHARMACOTHERAPY OF CHILD AND ADOLESCENT DEPRESSION
depressed adolescents in the proposed outcomes, R50% reduction inMontgomery-Asperg Depression Rating Scale and change in K-SADS-Ldepression subscale at endpoint (60.45% versus 58.24%; P ¼ 0.702)[46,49]. The other unpublished paroxetine RCT, which involved childrenand adolescents, also had negative results, although in this case the endpointwas change from baseline in CDRS-R total score (P ¼ 0.684) [50,51].
Sertraline has been studied in depressed children and adolescents in twoidentically designed, international, multi-site trials, and both yielded nega-tive results [52]. Only after combining the data of the two studies did the dif-ference between sertraline and placebo arms in the primary endpoint, R40%reduction from baseline on the CDRS-R score, although small, becomesignificant (63% versus 53%; P ¼ 0.05) [31].
Citalopram was significantly better than placebo (36% versus 24%; P ¼0.05) in a study in which the primary outcome measure was defined asCDRS-R %28 at 8 weeks after baseline or termination (response) [32].A second study in depressed adolescents, whose findings were not published,did not show efficacy [52]. Escitalopram has been tested in only one trial.The results of drug versus placebo in the primary efficacy measure, meanchange in CDRS-R at endpoint, were not statistically different [53].
Newer antidepressants also have been studied, but the reported resultsare far from satisfactory. The first venlafaxine trial, the only one of thosepresented in this article that has been published, showed similar results forplacebo and medication arms, both of which were combined with psycho-therapy [33]. In two subsequent identical multi-site studies of venlafaxineconducted in children and adolescents, results were negative when analyzedindividually [52] and when the data from both were combined and ana-lyzed together [54]. Nefazodone was studied in two trials, one inadolescents and one in children and adolescents [55]. In the adolescent-only study, the secondary outcome measures were positive but not the pri-mary measuredthe change from baseline in CDRS-R score. In the study ofboth children and adolescents, results were negative. Two mirtazapinestudies also produced negative results, and most of the data could not beconsulted [56].
Recently there has been a surge in the review of efficacy data of SSRIsand newer antidepressants in treating depression in the pediatric population[34,47,48,52,56,57]. Although there is agreement regarding the efficacy offluoxetine, there is no proof yet that the other SSRIs have efficacy in pedi-atric depression.
Children versus adolescents
Children and adolescents are frequently grouped together in trials for rea-sons of power, feasibility, and availability, which increases the chances thatconsiderable differences between the two age groups are overlooked. For in-stance, although no efficacy has been reported for TCAs, a meta-analysis of

986 MORENO et al
TCA studies in depressed youth showed better response among depressedadolescents compared with children [45].
In an unpublished paroxetine study performed in children and adoles-cents [50], dividing the sample into two age groups (7–11 and 12–17 years)revealed statistically significant treatment by age group interaction (P ¼0.049) with a greater proportion of subjects who responded to placebo inthe younger group. In an unpublished adolescent paroxetine trial, therewas also significant treatment by age group interaction (P ¼ 0.002), withhigher proportion of drug responders occurring in subjects aged 17 andolder compared with subjects aged 16 and younger [49]. None of these stud-ies found a statistically significant difference between paroxetine and pla-cebo for any of the different age groups, however.
When combined data from the two trials of venlafaxine performed in chil-dren and adolescents were analyzed based on age groups (children 7–11 years,adolescents 12–17 years), there was significant difference in the primary out-come between the drug and the placebo arms for adolescents (P ¼ 0.022)but not for children (P¼ 0.53) [54].When combined, the two studies of sertra-line found similar results: a reported efficacy in adolescents aged 12 to 17 years(P ¼ 0.01) and a nonsignificant difference in children aged 6 to 11 [31].
In the recently published escitalopram study, only adolescents who com-pleted the study had a significant improvement in the outcome measure:change in CDRS-R scores (P ! 0.05) [53].
Drawing conclusions from these differences between children and adoles-cent response to medication should be done with precaution, because moststudies were not designed to address the relationship between drug efficacyand age group. Although definitive conclusions based on such data shouldbe avoided, there is reason to believe that children respond differentlythan adolescents to antidepressants. Further study that directly addressesage-related efficacy of antidepressants in the pediatric population is needed.
Maintenance treatment
Most childhood- and adolescent-onset depressive episodes recur within 5years of onset [9]. Several studies also have indicated that major depressivedisorder persists into adulthood at a rate of approximately 70% [9]. Al-though it has been suggested that rates of recurrence in children and adoles-cents equal or surpass that of adult depression, few studies have addressedmaintenance treatment of depression in children and adolescents [58].
Although caution should be used when extrapolating from adult studiesand applying findings to children and adolescents, one naturalistic follow-upstudy of efficacy of fluoxetine in children and adolescents revealed that as inadults, recurrence occurred on and off fluoxetine in a pediatric population[59]. On the other hand, the rate of recurrence within 1 year in a pediatricpopulation was higher than in adults (40% [59] versus 24% [60]). Comparedwith patients who continued with depression during the 1-year follow-up

987PHARMACOTHERAPY OF CHILD AND ADOLESCENT DEPRESSION
period, patients who recovered were younger, less severely depressed, andhad better global social and family functioning. Results, however, shouldbe taken with caution because of small sample sizes (13 nonrecovered sub-jects), which may limit the capacity to find differences between samples.
To date, only one clinical follow-up treatment study has addressedthe prevention of relapse in this population [61]. After a 32-week relapse-prevention phase, which followed a 19-week double-blind, multi-site,placebo-controlled study of fluoxetine in children and adolescents, the meantime of relapse was longer when fluoxetine treatment was uninterrupted(F/F) (180.7 days, SE ¼ 17.0) than when fluoxetine was replaced with pla-cebo (F/P) (71.2 days, SE ¼ 9.5; P ¼ 0.046). There were similar adverseevents between the two groups, and the medication was well tolerated inboth. There was no statistically significant association with fluoxetine andevents leading to discontinuation in either the F/F or F/P groups.
Adverse events of treatment
Like most medications that we typically provide to our patients, antide-pressants pose risk for adverse events. The extent to which the risk is accept-able involves the degree of expected improvement versus the potential ofharm caused by the drug and the option of no treatment. Of the antidepres-sants studied, only the SSRIs have showed some success, albeit controver-sial, in the treatment of pediatric depression; therefore, reviewing the sideeffects associated with their use may be useful in clarifying their potentialuse.
Safety of medications in industry-financed trials is most often evaluatedby assessing spontaneously reported adverse events [62]. Most of the trialsdiscussed in this review did not mention the use of a systematic way of elic-iting adverse events. Only the two fluoxetine studies by Emslie and col-leagues [26,28] used the Side Effects Checklist, a general symptomschecklist, in addition to spontaneous report. Heterogeneity in adverse eventsdefinition and elicitation led to heterogeneity in drug safety data and diffi-culty in interpretation across trials [62]. Although several instruments areavailable for obtaining adverse events (Safety Monitoring Uniform ReportForm, Pediatric Adverse Events Rating Scale), there is currently no goldstandard against which to test new methods, and standardization of safetymethodology in pediatric trials is urgently needed [63].
The adverse events reported in the SSRIs and newer antidepressantsRCTs are listed in Table 1. It should be noted that for some compounds,safety data were not available for review, just as complete efficacy datawere not available for review. This inaccessibility of unpublished safetydata impedes the process of properly assessing the use of medications andcan lead to an incorrect and perhaps dangerous interpretation of the efficacydata of a given compound.

988 MORENO et al
Conventional adverse events
The most commonly reported adverse events in RCTs of SSRIs were gas-trointestinal and neuropsychiatric effects, which were seldom severe enoughto discontinue participation in the study (Table 1). Slowed growth wasdocumented in a case report of four children [64], and a trend toward slowergrowth was found in patients aged 8 to 18 years who were treated with flu-oxetine for 52 weeks [61]. Decreased growth hormone response after stimu-lation, which was normalized after stopping drug therapy, was documentedin the case report [64]. Reversible nocturnal enuresis also has been reportedin children receiving SSRIs [65].
Behavioral adverse events
Additional adverse events include behavioral activation, switch to mania,hostility, apathy, and serotonin syndrome. Behavioral adverse events areless frequent but more serious, lead to discontinuation more frequently,and reappear after re-exposure to SSRIs in almost half of the patients[66]. In the pediatric antidepressant RCTs, the rates of behavioral adverseevents were not always reported [32]. Agitation, hostility, and irritabilitywere reported for fluoxetine [28,29], hostility for paroxetine [30], and agita-tion for sertraline [31]. The US Food and Drug Administration (FDA) anal-ysis that accessed data from published and unpublished studies found that inall major depressive disorder trials, SSRIs were associated with increase oftreatment emergent agitation or hostility (RR 1.79 [1.16, 2.76]), but theanalysis could not link hostility to suicidality [67].
Manic conversion after antidepressant exposure is more frequent in peri-pubertal children (aged 10–14 years) [68] and more frequent after treatmentwith SSRIs than with TCAs in children aged 5 to 14 years [69]. Manic/hy-pomanic reactions have been reported in RCTs of paroxetine (1%) [30], flu-oxetine (1%–6.25%) [26,28,29], and venlafaxine (1%) [52], but none of thesetrials reported statistical differences in manic/hypomanic switching while onplacebo.
Suicide controversy and complications of untreated depression
The question of antidepressant-induced suicidality has been raised fromthe time of the initial use of these compounds. When TCAs were the onlyavailable option for treating depression, careful observation of patients atthe beginning of treatment was recommended, because medication workedfirst on the neurovegetative symptoms and then acted to reduce the thoughtsof death, worthlessness, and suicidality of the depression. TCAs are lethalon overdose, however [70]. The arrival of the SSRIs in the late 1980s pre-sented a big change in prescription practices. The SSRIs were efficaciousand safer if overdosed and had a more benign profile of adverse events.Their safety with regard to suicidality was questioned early by the US

989PHARMACOTHERAPY OF CHILD AND ADOLESCENT DEPRESSION
FDA, and additional re-analysis was needed to establish that the risk-benefitratio was acceptable [71,72].
Suicidality itself (ie, ideation, attempts, and completions) is linked to de-pression. Suicidal ideation is one of the diagnostic criteria for depression rec-ognized by the DSM-IV, and suicide completion is depression’s worstoutcome. Suicide ideation (19%) and attempts (9%) are frequent in youth do-mestically [73] and internationally (ideation 29.9%, attempts 9.7%) [74].Although completion rates are lower than for adults, suicide is the third lead-ing cause of death among 10- to 19-year-old individuals and is a serious publichealth problem [75]. Depression seems to be one of the strongest predictors ofattempted and completed suicide in youth.Depressed youth aged 9 to 17 yearshave a sevenfold increase in the rate of attempts comparedwith youthwithoutpsychiatric diagnoses [76]. Prospective studies show that lifetime risk of sui-cide attempt carried over from depressed children and adolescents is as highas 45% [77]. Psychological autopsy studies show that almost all child and ad-olescent victims of completed suicides suffered from anAxis Imental disorder,and as many as two thirds suffered from depression [78].
Although depression is associated with suicide completion, the number ofsuicides in children and adolescents has been decreasing over the last de-cades [79,80]. One suggested reason is increased availability/prescriptionsof antidepressants [79,81,82]. Toxicology studies in young suicide victimsshow that the use of antidepressants among youth who commit suicide islower than in the general population, however. In New York between1993 and 1999, only 7% of the completed suicides in youth younger thanage 18 tested positive for antidepressants [83]. In Sweden between 1992and 2000 (youth !15 years) [84] and in Utah between 1996 and 1998 (youthaged 13–21) [85], none of the suicide victims tested positive for antidepres-sants. In the Utah study, 44% of the suicide victims who presented with psy-chiatric diagnoses were prescribed psychotropics, which suggested that mostyouth who commit suicide have untreated depression (or are not compliantwith treatment) and that the absence of treatment may be more harmfulthan the effect of the antidepressants.
It is difficult, however, to demonstrate the suicide preventive effect of an-tidepressants in drug trials because of some methodologic problems: usuallythe trials are designed for efficacy, underpowered for detecting signals foruncommon events such as suicide, exclude suicidal patients, and are short-term trials that do not prospectively follow the patients. In the pediatricantidepressant trials, suicidal events were neither systematically evaluatedduring the trials with objective measures nor systematically classified.
To address the issue of an increase in suicidality caused by antidepres-sants in children and adolescents, the US FDA appointed a group of suicideexperts from Columbia University to blindly reclassify the suicidal events re-ported in pediatric trials, including fluoxetine, sertraline, paroxetine,fluvoxamine, citalopram, bupropion, venlafaxine, nefazodone, and mirtaza-pine. The US FDA then conducted a meta-analysis of the suicide-related

990 MORENO et al
adverse events [67]. No suicide completions occurred during the studies. Inconcordance with the report by the Medicines and Healthcare ProductsRegulatory Agency, the findings revealed that when all trials and all indica-tions were taken together, the main focus of the analysis (which included at-tempt, preparatory actions toward imminent attempt, and ideation) wassignificantly different in antidepressant and placebo groups (RR 1.78[1.14–2.77]), although no differences were found for any individual medica-tion, except venlafaxine (RR 4.97 [1.09–22.72]). No risk was found whenonly SSRIs in major depressive disorder trials were considered (RR 1.41[0.84–2.37]). No predictive factors of suicidality were identified for eitherplacebos or antidepressants, and it was not possible to attribute the in-creased risk of suicide to the drugs or the underlying depression. Previousattempt, one of the most replicated predictors of suicide, was not docu-mented in any of the trials reviewed. Most of the suicide-related events inthe major depressive disorder trials occurred in the studies with the highestrate of patients with history of suicide attempt or ideation at baseline. Re-search using naturalistic databases supports the findings of US FDA andMedicines and Healthcare Products Regulatory Agency analyses [86,87].In a separate analysis of the antidepressant trials, the American Collegeof Neuropsychopharmacology found that the average number needed toharm (which included suicidal ideation) was 23 times greater than the num-ber needed to treat across studies [48].
Selective serotonin reuptake inhibitors in brain development
An important consideration to bear in mind when prescribing antidepres-sants to children is that these medications have potential effects on brain de-velopment, which have consequences throughout adulthood. Serotoninmodulates developmental processes, such as neurogenesis, apoptosis, andsynaptogenesis [88], and plays a critical role in the maturation of brain sys-tems involved in emotional responses to novelty and stress in adults [89].
In humans, although no teratogenic effects have been reported, there isevidence of increased risk of shorter gestational period and lower birthweight, appearance of reversible neonatal serotoninergic central nervoussystem side effects, neonatal abstinence syndrome, and impairment of motordevelopment after exposure to SSRIs during late pregnancy [90–94]. Humanstudies have not yet followed subjects enough to determine long-term con-sequences of early exposure to SSRIs, however. Studies in animals revealthat rodents exposed to an agonist of the 5HT1A receptor (8-OH-DPAT)before puberty show faster behavioral maturation, an effect not present ifthe exposure occurs later in the development [95]. Administration of fluox-etine to mice during the brain maturation period that corresponds to latepregnancy and early childhood produced altered emotional behaviors inthe adult animals, which authors suggest are related to neurodevelopmentalinsults caused by early life disruption of serotonin function [89]. This finding

991PHARMACOTHERAPY OF CHILD AND ADOLESCENT DEPRESSION
raises the possibility that prolonged treatment of young children with SSRIsmay produce alterations in their emotional behavior when they becameadults [96]. If true, the findings would suggest that therapists treat childrenwith SSRIs for a limited amount of time.
On the other hand, depression itself can be neurotoxic for the adult brainand associated with atrophic changes [97]. Studies in postnatal rodents dem-onstrate that induced serotonin depletion leads to a permanent decrease insynaptic density and learning deficits, which persist into adulthood [98]. Thereis increasing evidence that treatment with antidepressants acts to reverse sucheffects [97]. Antidepressant treatment upregulates cyclic adenosine mono-phosphate and the brain derived-neurotrophic factor, both of which are in-volved in neuronal plasticity mechanisms, and chronic antidepressanttreatment increases the rate of neurogenesis in the adult hippocampus [97].
In the absence of conclusive data in children and adolescents, we mustweigh the potential consequences of treating pediatric depression and leavingit untreated. Perhaps identifying and treating pediatric depression will affectpositively the evolution of depression and prevent its deleterious effects.
Treatment recommendations
The focus of this article is pharmacologic treatment of pediatric depres-sion. When faced with treating a depressed child or adolescent, however,other alternatives (eg, psychotherapy), should be considered. According tothe practice parameters for the assessment and treatment of children andadolescents with depressive disorders currently under review [99], the firstrecommendation for mild and uncomplicated acute depression is a combina-tion of psychoeducation and supportive psychotherapy. For nonresponsivedepressed youth or youth with moderate depression, a decision should bemade between starting them on medication or psychotherapy. Evidence-based psychotherapies, CBT and interpersonal psychotherapy, have beenproved efficacious for treatment of moderately depressed youth [100,101].To decide between psychotherapy or antidepressants, availability, patientsand family preference, clinical situation (a patient may be too psychoticor agitated to be treated with psychotherapy) and previous history of re-sponse/lack of response must be considered.
Psychopharmacologic treatment of depressed youth comprises short-term, continuation, and maintenance treatment. During the acute phaseof treatment, which is aimed at establishing remission of symptoms, medica-tions with demonstrated efficacy in short-term RCTs and favorable risk/benefit ratio should be the first consideration. Fluoxetine, the only medica-tion that is approved by the US FDA for youth depression, would be thefirst option. Just as when deciding between psychotherapy and pharmaco-logic treatment, however, previous response/lack of response/tolerabilityto a medication in a patient or in a patient’s family members, preventionof certain side effects, or patient/family/physician preference also guide

992 MORENO et al
antidepressant selection. Second-line treatments, based on the efficacy/safetyratio, would be citalopram and sertraline, albeit to a smaller extent than cit-alopram. Although paroxetine has shown promising results in one RCT,concerns about its safety, expressed by the Medicines and Healthcare Prod-ucts Regulatory Agency and the US FDA, suggest not using it [52,56]. Othercompounds, such as venlafaxine, have shown a trend toward efficacy in ad-olescents, although efficacy has yet to be proved. Again, concerns aboutsafety would limit its use [67].
During the acute phase, tolerable/adequate doses of medications shouldbe maintained for 4 to 6 weeks before considering alternative interventions.As implied in the American Academy of Child and Adolescent Psychiatrypractice parameters [99,102], there are no evidence-based recommendationsfor youth with treatment-resistant depression, although the following strat-egies are suggested. (1) When there is no response after a 4- to 6-week trialor a patient cannot tolerate treatment, change to a second-line medication.(2) When there is a partial response, the following alternatives should beconsidered: optimization of dose, augmentation with other agents such aslithium, or combination treatment (eg, addition of CBT or interpersonalpsychotherapy). Regarding the use of monotherapy or combination (psy-chopharmacology plus psychotherapy) as a first-line approach, a definitiveanswer is still unclear. Although in the Treatment for Adolescents with De-pression study the authors claimed that the combination of CBT and fluox-etine was more efficacious than medication alone, a closer look at the studyrevealed that it does not hold true for the most severe patients [29]. Limita-tions inherent to the design of the study, such as blinded medicationtreatment but not blinded psychotherapy, also suggest caution when extrap-olating conclusions. An effectiveness study aimed at testing whether the ad-dition of brief CBT and fluoxetine was advantageous over fluoxetine alonein the long-term treatment of depressed adolescents found a trend towardefficacy in one of the primary outcome measures and failed to find differ-ences in the other [103]. Sample size considerations and different dosageof antidepressants in each group were some of the explanations proposedfor the lack of efficacy [103]. Although some patients may benefit fromthe additive approach, there is still not enough evidence to suggest universaluse of combination treatment for all pediatric depressed patients. Currently,the US FDA recommends that children and adolescents who are receivingan SSRI should be seen by the treating clinician once a week for 4 weeks,once every 2 weeks for the next 4 weeks, at the end of 12 weeks of medica-tion and as frequently as deemed necessary by the clinician beyond 12 weeksof treatment.
Although not supported by evidence, the American Academy of Childand Adolescent Psychiatry practice parameters also recommend that toavoid relapses, treatment should be continued for 6 to 12 months afterachieving remission, with longer maintenance treatment needed in youthwith more severe, recurrent, and chronic disorders [99,102].

993PHARMACOTHERAPY OF CHILD AND ADOLESCENT DEPRESSION
Summary
Pediatric depression is a prevalent and recurrent condition that persistsinto adulthood and carries significant impairment, morbidity, and risk ofmortality.
Among children and adolescents, depression remains largely understudied,unrecognized, and untreated. The study of the efficacy of SSRIs and newer an-tidepressants in this age group is in a relatively early stage. Fluoxetine is theonly compound for which there is agreement in the evidence of efficacy andthe only antidepressant approved to treat depressed minors. Evidence forother antidepressants is less conclusive, although promising data exist for cit-alopram and paroxetine. The small number of studies conducted has yet toprovide conclusive results about the efficacy of SSRIs as a group and sayseven less about newer antidepressants. Marked differences in primary out-comes among studies, heterogeneity in definition and methods used to elicitadverse events, and lack of availability of unpublished data further hinderthe process of choosing the best treatment for each particular clinical situa-tion. Even less can be concluded with regard to efficacious maintenance treat-ments in depressed children and adolescents. Long-term care of pediatricdepression remains largely uncharted and in need of exploration.
Currently, the US FDA recommends more frequent visits in the earlystage of treatment. Caregivers and clinicians should look for any unusualchanges in behavior, worsening of depressive symptoms, and suicidalityupon initial treatment and at times of dosage change [41]. Although theserecommendations are not evidence based, a significant, although small, sig-nal of suicidality in pediatric antidepressant trials raises ethical concernsabout their use in children and adolescents and warrants close supervisionof youngsters treated with antidepressant medications. Depression is oneof the strongest predictors of suicide-related events and one of the commonfeatures of completed suicides, however. If, as suggested by epidemiologicdata, the increase in use of antidepressants has been a determining factorin the decrease in the rate of suicides among adolescents, change in prescrip-tion practices and decline in the number of prescribed antidepressants couldplace a significant proportion of depressed youth in danger and have seriouspublic health consequences.
Research in this area is urgently needed. Clinicians who treat depressedyouth are in need of efficacious and safe treatment alternatives to offer totheir patients.
References
[1] Costello EJ, Mustillo S, Erkanli A, et al. Prevalence and development of psychiatric
disorders in childhood and adolescence. Arch Gen Psychiatry 2003;60(8):837–44.
[2] Hasin DS, Goodwin RD, Stinson FS, et al. Epidemiology of major depressive disorder:
results from the National Epidemiologic Survey on Alcoholism and Related Conditions.
Arch Gen Psychiatry 2005;62(10):1097–106.

994 MORENO et al
[3] Substance Abuse and Mental Health Services Administration. Youth violence and illicit
drug use. Available at: http://oas.samhsa.gov/2k6/youthViolence/youthViolence.htm.
Accessed February 7, 2006.
[4] Lewinsohn PM, Rohde P, Seeley JR. Major depressive disorder in older adolescents:
prevalence, risk factors, and clinical implications. Clin Psychol Rev 1998;18(7):765–94.
[5] Kessler RC,McGonagleKA, Zhao S, et al. Lifetime and 12-month prevalence ofDSM-III-
R psychiatric disorders in theUnited States: results from theNational Comorbidity Survey.
Arch Gen Psychiatry 1994;51(1):8–19.
[6] Fleming JE, Offord DR. Epidemiology of childhood depressive disorders: a critical review.
J Am Acad Child Adolesc Psychiatry 1990;29(4):571–80.
[7] Rao U, Weissman MM, Martin JA, et al. Childhood depression and risk of suicide: a pre-
liminary report of a longitudinal study. J Am Acad Child Adolesc Psychiatry 1993;32(1):
21–7.
[8] Weissman MM, Wolk S, Goldstein RB, et al. Depressed adolescents grown up. JAMA
1999;281(18):1707–13.
[9] Birmaher B, Ryan ND, Williamson DE, et al. Childhood and adolescent depression:
a review of the past 10 years. Part I. J Am Acad Child Adolesc Psychiatry 1996;
35(11):1427–39.
[10] Ma J, Lee KV, Stafford RS. Depression treatment during outpatient visits by US children
and adolescents. J Adolesc Health 2005;37(6):434–42.
[11] Wu P, Hoven CW, Bird HR, et al. Depressive and disruptive disorders and mental health
service utilization in children and adolescents. J Am Acad Child Adolesc Psychiatry 1999;
38(9):1081–90 [discussion: 1090–2].
[12] Pearce JB. The recognition of depressive disorder in children. J R Soc Med 1978;71(7):
494–500.
[13] Hughes CW, Preskorn SH,Weller E, et al. The effect of concomitant disorders in childhood
depression on predicting treatment response. Psychopharmacol Bull 1990;26(2):235–8.
[14] Petti TA, Law W III. Imipramine treatment of depressed children: a double-blind pilot
study. J Clin Psychopharmacol 1982;2(2):107–10.
[15] Preskorn SH,Weller EB, Hughes CW, et al. Depression in prepubertal children: dexameth-
asone nonsuppression predicts differential response to imipramine vs. placebo. Psycho-
pharmacol Bull 1987;23(1):128–33.
[16] Puig-Antich J, Perel JM, Lupatkin W, et al. Imipramine in prepubertal major depressive
disorders. Arch Gen Psychiatry 1987;44(1):81–9.
[17] Kashani JH, Shekim WO, Reid JC. Amitriptyline in children with major depressive dis-
order: a double-blind crossover pilot study. J Am Acad Child Psychiatry 1984;23(3):
348–51.
[18] Kramer AD, Feiguine RJ. Clinical effects of amitriptyline in adolescent depression: a pilot
study. J Am Acad Child Psychiatry 1981;20(3):636–44.
[19] Geller B, Cooper TB,GrahamDL, et al. Double-blind placebo-controlled study of nortrip-
tyline in depressed adolescents using a ‘‘fixed plasma level’’ design. Psychopharmacol Bull
1990;26(1):85–90.
[20] Geller B, Cooper TB,McCombs HG, et al. Double-blind, placebo-controlled study of nor-
triptyline in depressed children using a ‘‘fixed plasma level’’ design. Psychopharmacol Bull
1989;25(1):101–8.
[21] Birmaher B, Waterman GS, Ryan ND, et al. Randomized, controlled trial of amitriptyline
versus placebo for adolescents with ‘‘treatment-resistant’’ major depression. J Am Acad
Child Adolesc Psychiatry 1998;37(5):527–35.
[22] Kye CH,WatermanGS, RyanND, et al. A randomized, controlled trial of amitriptyline in
the acute treatment of adolescent major depression. J Am Acad Child Adolesc Psychiatry
1996;35(9):1139–44.
[23] Klein RG, Mannuzza S, Koplewicz HS, et al. Adolescent depression: controlled desipra-
mine treatment and atypical features. Depress Anxiety 1998;7(1):15–31.
995PHARMACOTHERAPY OF CHILD AND ADOLESCENT DEPRESSION
[24] Kutcher S, Boulos C, Ward B, et al. Response to desipramine treatment in adolescent de-
pression: a fixed-dose, placebo-controlled trial. J AmAcad Child Adolesc Psychiatry 1994;
33(5):686–94.
[25] Sallee FR, VrindavanamNS, Deas-Nesmith D, et al. Parenteral clomipramine challenge in
depressed adolescents: mood and neuroendocrine response. Biol Psychiatry 1998;44(7):
562–7.
[26] Emslie GJ, RushAJ,WeinbergWA, et al. A double-blind, randomized, placebo-controlled
trial of fluoxetine in children and adolescents with depression. Arch Gen Psychiatry 1997;
54(11):1031–7.
[27] Simeon JG, Dinicola VF, Ferguson HB, et al. Adolescent depression: a placebo-controlled
fluoxetine treatment study and follow-up. Prog Neuropsychopharmacol Biol Psychiatry
1990;14(5):791–5.
[28] Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine for acute treatment of depres-
sion in children and adolescents: a placebo-controlled, randomized clinical trial. J AmAcad
Child Adolesc Psychiatry 2002;41(10):1205–15.
[29] March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their
combination for adolescents with depression: treatment for adolescents with depression
study (TADS) randomized controlled trial. JAMA 2004;292(7):807–20.
[30] KellerMB,RyanND, StroberM, et al. Efficacy of paroxetine in the treatment of adolescent
major depression: a randomized, controlled trial. J Am Acad Child Adolesc Psychiatry
2001;40(7):762–72.
[31] Wagner KD, Ambrosini P, RynnM, et al. Efficacy of sertraline in the treatment of children
and adolescents with major depressive disorder: two randomized controlled trials. JAMA
2003;290(8):1033–41.
[32] Wagner KD, Robb AS, Findling RL, et al. A randomized, placebo-controlled trial of cit-
alopram for the treatment ofmajor depression in children and adolescents. Am JPsychiatry
2004;161(6):1079–83.
[33] Mandoki MW, Tapia MR, Tapia MA, et al. Venlafaxine in the treatment of children and
adolescents with major depression. Psychopharmacol Bull 1997;33(1):149–54.
[34] Ryan ND. Treatment of depression in children and adolescents. Lancet 2005;366(9489):
933–40.
[35] Emslie GJ, Ryan ND,Wagner KD.Major depressive disorder in children and adolescents:
clinical trial design and antidepressant efficacy. J Clin Psychiatry 2005;66(Suppl 7):14–20.
[36] Courtney DB. Selective serotonin reuptake inhibitor and venlafaxine use in children and
adolescents with major depressive disorder: a systematic review of published randomized
controlled trials. Can J Psychiatry 2004;49(8):557–63.
[37] Pirraglia PA, Stafford RS, Singer DE. Trends in prescribing of selective serotonin reuptake
inhibitors and other newer antidepressant agents in adult primary care. Prim Care Com-
panion J Clin Psychiatry 2003;5(4):153–7.
[38] MurrayML, de Vries CS, Wong IC. A drug utilisation study of antidepressants in children
and adolescents using the general practice research database. Arch Dis Child 2004;89(12):
1098–102.
[39] Zito JM, SaferDJ,DosReis S, et al. Rising prevalence of antidepressants amongUS youths.
Pediatrics 2002;109(5):721–7.
[40] Medicines and Healthcare Products Regulatory Agency. Selective serotonin reuptake in-
hibitors: use in children and adolescents with major depressive disorder: Available at:
http://www.mhra.gov.uk/home/groups/pl-p/documents/drugsafetymessage/con019492.pdf.
Accessed February 7, 2006.
[41] US Food and Drug Administration. Labeling change request letter. Available at: http://
www.fda.gov/cder/drug/antidepressants/SSRIlabelChange.htm.AccessedFebruary 7, 2006.
[42] Murray ML, Thompson M, Santosh PJ, et al. Effects of the committee on safety of medi-
cines advice on antidepressant prescribing to children and adolescents in the UK. Drug Saf
2005;28(12):1151–7.
996 MORENO et al
[43] Rosack J. New data show declines in antidepressant prescribing. Psychiatr News 2005;
40(17):1.
[44] Barbui C, HotopfM. Amitriptyline v. the rest: still the leading antidepressant after 40 years
of randomised controlled trials. Br J Psychiatry 2001;178:129–44.
[45] Hazell P, O’Connell D, Heathcote D, et al. Tricyclic drugs for depression in children and
adolescents (Cochrane review). The Cochrane Library. Chichester: John Wiley and Sons;
2004.
[46] Milin R, Simeon J, Spenst W. Double-blind study of paroxetine in adolescents with
unipolar major depression (NR-67). Los Angeles (CA): American Academy of Child and
Adolescent Psychiatry; 1999.
[47] Cheung AH, Emslie GJ, Mayes TL. Review of the efficacy and safety of antidepressants in
youth depression. J Child Psychol Psychiatry 2005;46(7):735–54.
[48] Mann JJ, Emslie G, Baldessarini RJ, et al. ACNP task force report on SSRIs and suicidal
behavior in youth. Neuropsychopharmacology 2005;23:473–92.
[49] GlaxoSmithKline. Current issues: paroxetine and pediatric and adolescent patients (Study
#377). Available at: http://www.gsk.com/media/paroxetine.htm. Accessed February 7,
2006.
[50] GlaxoSmithKline. Current issues: paroxetine and pediatric and adolescent patients (Study
#701). Available at: http://www.gsk.com/media/paroxetine.htm. Accessed February 7,
2006.
[51] Emslie GJ, Wagner K, Kutcher S, et al. Paroxetine treatment in children and adolescents
with major depressive disorder. Presented at the 51st Annual Meeting of the American
Academy of Child and Adolescent Psychiatry. Washington, DC; October 19–24, 2004
[52] Medicines and Healthcare Products Regulatory Agency. Selective serotonin reuptake
inhibitors (SSRIs): overview of regulatory status and CSM advice relating to major
depressive disorder (MDD) in children and adolescents including a summary of avail-
able safety and efficacy data: Available at: http://www.mhra.gov.uk/home/idcplg?
IdcService¼SS_GET_PAGE&ssTargetNodeId¼221&useSecondary¼true&ssDocName¼CON019494&showpage¼2. Accessed February 7, 2006.
[53] Wagner KD, Jonas J, Findling RL, et al. A double-blind, randomized, placebo-controlled
trial of escitalopram in the treatment of pediatric depression. JAmAcadChildAdolesc Psy-
chiatry 2006;45(3):280–8.
[54] Emslie GJ, Findling R, Yeung P, et al. Venlafaxine XR in pediatric patients with major
depressive disorder. Presented at the 51st Annual Meeting of the American Academy of
Child and Adolescent Psychiatry. Washington, DC; October 19–24, 2004.
[55] Emslie GJ, Findling RL, RynnM, et al. Efficacy and safety of nefazodone in the treatment
of adolescents withmajor depressive disorder. Presented at the 42ndAnnualMeeting of the
NCDEU. Orlando, FL; June 10–13, 2002.
[56] US Food and Drug Administration. Antidepressant use in children, adolescents and
adults. Available at: http://www.fda.gov/cder/drugs/antidepressants. Accessed February
7, 2006.
[57] Whittington CJ, Kendall T, Fonagy P, et al. Selective serotonin reuptake inhibitors in
childhood depression: systematic review of published versus unpublished data. Lancet
2004;363(9418):1341–5.
[58] Emslie GJ, Mayes TL, Ruberu M. Continuation and maintenance therapy of early-onset
major depressive disorder. Paediatr Drugs 2005;7(4):203–17.
[59] Emslie GJ, Rush AJ, Weinberg WA, et al. Fluoxetine in child and adolescent depression:
acute and maintenance treatment. Depress Anxiety 1998;7(1):32–9.
[60] Keller MB, Shapiro RW, Lavori PW, et al. Relapse in major depressive disorder: analysis
with the life table. Arch Gen Psychiatry 1982;39(8):911–5.
[61] Emslie GJ, Heiligenstein JH,Hoog SL, et al. Fluoxetine treatment for prevention of relapse
of depression in children and adolescents: a double-blind, placebo-controlled study. J Am
Acad Child Adolesc Psychiatry 2004;43(11):1397–405.
997PHARMACOTHERAPY OF CHILD AND ADOLESCENT DEPRESSION
[62] Greenhill LL, Vitiello B, Fisher P, et al. Comparison of increasingly detailed elicitation
methods for the assessment of adverse events in pediatric psychopharmacology. J Am
Acad Child Adolesc Psychiatry 2004;43(12):1488–96.
[63] Vitiello B, Heiligenstein JH, Riddle MA, et al. The interface between publicly funded and
industry-funded research in pediatric psychopharmacology: opportunities for integration
and collaboration. Biol Psychiatry 2004;56(1):3–9.
[64] Weintrob N, Cohen D, Klipper-Aurbach Y, et al. Decreased growth during therapy with
selective serotonin reuptake inhibitors. Arch Pediatr Adolesc Med 2002;156(7):696–701.
[65] Kandil ST, Aksu HB, Ozyavuz R. Reversible nocturnal enuresis in children receiving SSRI
with or without risperidone: presentation of five cases. Isr J PsychiatryRelat Sci 2004;41(3):
218–21.
[66] Wilens TE, Biederman J, Kwon A, et al. A systematic chart review of the nature of
psychiatric adverse events in children and adolescents treated with selective serotonin
reuptake inhibitors. J Child Adolesc Psychopharmacol 2003;13(2):143–52.
[67] Hammad T. Review and evaluation of clinical data: relationship between psychotropic
drugs and pediatric suicidality. Available at: http://www.fda.gov/ohrms/dockets/ac/04/
briefing/2004-4065b1-10-TAB08-Hammads-Review.pdf. Accessed February 7, 2006.
[68] Martin A, Young C, Leckman JF, et al. Age effects on antidepressant-induced manic
conversion. Arch Pediatr Adolesc Med 2004;158(8):773–80.
[69] Baldessarini RJ, Faedda GL, Hennen J. Risk of mania with antidepressants. Arch Pediatr
Adolesc Med 2005;159(3):298 [author reply: 298–9].
[70] Licinio J, Wong ML. Depression, antidepressants and suicidality: a critical appraisal. Nat
Rev Drug Discov 2005;4(2):165–71.
[71] Kapur S, Mieczkowski T, Mann JJ. Antidepressant medications and the relative risk of
suicide attempt and suicide. JAMA 1992;268(24):3441–5.
[72] Khan A, Khan S, Kolts R, et al. Suicide rates in clinical trials of SSRIs, other
antidepressants, and placebo: analysis of FDA reports.Am JPsychiatry 2003;160(4):790–2.
[73] Grunbaum JA,KannL,Kinchen SA, et al. Youth risk behavior surveillance:United States,
2001. MMWR Surveill Summ 2002;51(4):1–62.
[74] Evans E, Hawton K, Rodham K, et al. The prevalence of suicidal phenomena in
adolescents: a systematic review of population-based studies. Suicide Life Threat Behav
2005;35(3):239–50.
[75] Anderson RN, Smith BL. Deaths: leading causes for 2001. Natl Vital Stat Rep 2003;52(9):
1–85.
[76] Gould MS, King R, Greenwald S, et al. Psychopathology associated with suicidal ideation
and attempts among children and adolescents. J Am Acad Child Adolesc Psychiatry 1998;
37(9):915–23.
[77] Fombonne E, Wostear G, Cooper V, et al. TheMaudsley long-term follow-up of child and
adolescent depression. II. Suicidality, criminality and social dysfunction in adulthood. Br J
Psychiatry 2001;179:218–23.
[78] Marttunen MJ, Aro HM, Henriksson MM, et al. Mental disorders in adolescent suicide.
DSM-III-R axes I and II diagnoses in suicides among 13- to 19-year-olds in Finland.
Arch Gen Psychiatry 1991;48(9):834–9.
[79] GouldMS,GreenbergT,VeltingDM,et al.Youth suicide risk andpreventive interventions:
a review of the past 10 years. J Am Acad Child Adolesc Psychiatry 2003;42(4):386–405.
[80] World Health Organization. Country reports and charts available. Available at: http://
www.who.int/mental_health/prevention/suicide/country_reports/en/. Accessed February
7, 2006.
[81] Olfson M, Shaffer D, Marcus SC, et al. Relationship between antidepressant medication
treatment and suicide in adolescents. Arch Gen Psychiatry 2003;60(10):978–82.
[82] ValuckRJ, LibbyAM, SillsMR, et al. Antidepressant treatment and risk of suicide attempt
by adolescents with major depressive disorder: a propensity-adjusted retrospective cohort
study. CNS Drugs 2004;18(15):1119–32.
998 MORENO et al
[83] Leon AC, Marzuk PM, Tardiff K, et al. Paroxetine, other antidepressants, and youth
suicide in New York City: 1993 through 1998. J Clin Psychiatry 2004;65(7):915–8.
[84] Isacsson G, Holmgren P, Ahlner J. Selective serotonin reuptake inhibitor antidepressants
and the risk of suicide: a controlled forensic database study of 14,857 suicides. Acta Psy-
chiatr Scand 2005;111(4):286–90.
[85] MoskosM,OlsonL,Halbern S, et al.Utah youth suicide study: psychological autopsy. Sui-
cide Life Threat Behav 2005;35(5):536–46.
[86] OlfsonM,Marcus SC, Shaffer D. A case control study of antidepressants and suicide in se-
verely depressed children and adults. Arch Gen Psychiatry, in press.
[87] Simon GE, Savarino J, Operskalski B, et al. Suicide risk during antidepressant treatment.
Am J Psychiatry 2006;163(1):41–7.
[88] Gaspar P, Cases O, Maroteaux L. The developmental role of serotonin: news from mouse
molecular genetics. Nat Rev Neurosci 2003;4(12):1002–12.
[89] AnsorgeMS, ZhouM, Lira A, et al. Early-life blockade of the 5-HT transporter alters emo-
tional behavior in adult mice. Science 2004;306(5697):879–81.
[90] Simon GE, Cunningham ML, Davis RL. Outcomes of prenatal antidepressant exposure.
Am J Psychiatry 2002;159(12):2055–61.
[91] Moses-Kolko EL, Bogen D, Perel J, et al. Neonatal signs after late in utero exposure to se-
rotonin reuptake inhibitors: literature review and implications for clinical applications.
JAMA 2005;293(19):2372–83.
[92] Zeskind PS, Stephens LE. Maternal selective serotonin reuptake inhibitor use during preg-
nancy and newborn neurobehavior. Pediatrics 2004;113(2):368–75.
[93] Casper RC, Fleisher BE, Lee-Ancajas JC, et al. Follow-up of children of depressedmothers
exposed or not exposed to antidepressant drugs during pregnancy. J Pediatr 2003;142(4):
402–8.
[94] Levinson-Castiel R,Merlob P, LinderN, et al. Neonatal abstinence syndrome after in utero
exposure to selective serotonin reuptake inhibitors in term infants. Arch Pediatr Adolesc
Med 2006;160(2):173–6.
[95] Borella A, BindraM,Whitaker-Azmitia PM. Role of the 5–HT1A receptor in development
of the neonatal rat brain: preliminary behavioral studies. Neuropharmacology 1997;
36(4–5):445–50.
[96] Gross C, Hen R. The developmental origins of anxiety. Nat Rev Neurosci 2004;5(7):
545–52.
[97] D’Sa C, Duman RS. Antidepressants and neuroplasticity. Bipolar Disord 2002;4(3):
183–94.
[98] MazerC,Muneyyirci J, TahenyK, et al. Serotonin depletion during synaptogenesis leads to
decreased synaptic density and learning deficits in the adult rat: a possible model of neuro-
developmental disorders with cognitive deficits. Brain Res 1997;760(1–2):68–73.
[99] AmericanAcademy of Child andAdolescent Psychiatry. Practice parameters for the assess-
ment and treatment of children and adolescents with depressive disorders. Journal of the
American Academy of Child and Adolescent Psychiatry, in press.
[100] Asarnow JR, Jaycox LH, Duan N, et al. Effectiveness of a quality improvement interven-
tion for adolescent depression in primary care clinics: a randomized controlled trial. JAMA
2005;293(3):311–9.
[101] Mufson L, Dorta KP, Wickramaratne P, et al. A randomized effectiveness trial of in-
terpersonal psychotherapy for depressed adolescents. Arch Gen Psychiatry 2004;61(6):
577–84.
[102] American Academy of Child and Adolescent Psychiatry. Practice parameters for the
assessment and treatment of children and adolescents with depressive disorders. J Am
Acad Child Adolesc Psychiatry 1998;37(10 Suppl):63S–83S.
[103] Clarke G, Debar L, Lynch F, et al. A randomized effectiveness trial of brief cognitive-
behavioral therapy for depressed adolescents receiving antidepressant medication. J Am
Acad Child Adolesc Psychiatry 2005;44(9):888–98.