pharyngeal arches and pouches
TRANSCRIPT

Majd Hasanin

2
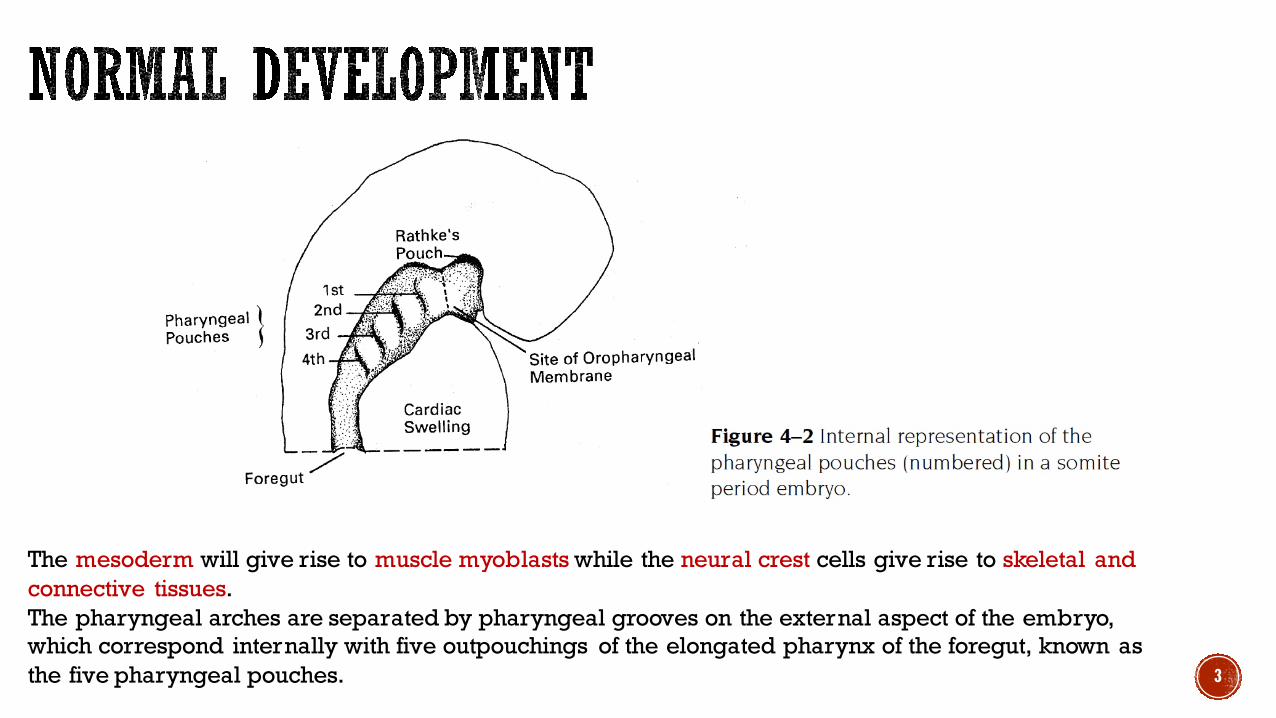
During the 4th week, the mesoderm lateral plate of the ventral foregut region becomes segmented to form a series of five distinct bilateral mesenchyme swellings called the pharyngeal (branchial) arches. Ventrally migrating neural crest cells interact with lateral extensions of the pharyngeal endoderm, surround the six aortic arch arteries, and initiate pharyngeal arch development. The initial mesodermal core of eacharch is augmented by neural crest tissue that surrounds the mesodermal core.
3
The mesoderm will give rise to muscle myoblasts while the neural crest cells give rise to skeletal and connective tissues.The pharyngeal arches are separated by pharyngeal grooves on the external aspect of the embryo, which correspond internally with five outpouchings of the elongated pharynx of the foregut, known as the five pharyngeal pouches.

4
Although derivatives of five or even six arches are described, only three (and exceptionally, four) arches appear externally.
Caudal to the third arch, there is a depression, the cervical sinus.

5

§ The first pharyngeal arch is the precursor of both the maxillary and mandibularjaws and appropriately bounds the lateral aspects of the stomodeum
§ Meckel’s cartilage§ Arises at the 41st to 45th days post conception§ Provides a template for subsequent development of the mandible (most of its
cartilage substance disappears)
§ Persisting portions of Meckel’s cartilage form the basis of major portions of two ear ossicles:§ Head and neck of the malleus§ Body and short crus of the incus§ Anterior ligament of the malleus and the sphenomandibular ligament
6
§ The cartilage of the second arch (Reichert’s cartilage) appears on the 45th to 48th days post conception
§ Basis of the greater part of the third ear ossicle (the stapes) and contributes to§ Malleus and incus§ The styloid process of the temporal bone§ Stylohyoid ligament§ Lesser horn and cranial part of the body of the hyoid bone
7

§ Produces the greater horn and the caudal part of the body of the hyoid bone
§ The remainder of the cartilage disappears
§ The mucosa of the posterior third of the tongue is derived from this arch
8

§ Forms the thyroid cartilage
9

§ A transitory structure
§ Disappears almost as soon as it forms
§ It leave no permanent structural elements
10

§ Forms the cricoid and arytenoid cartilages of the larynx
11

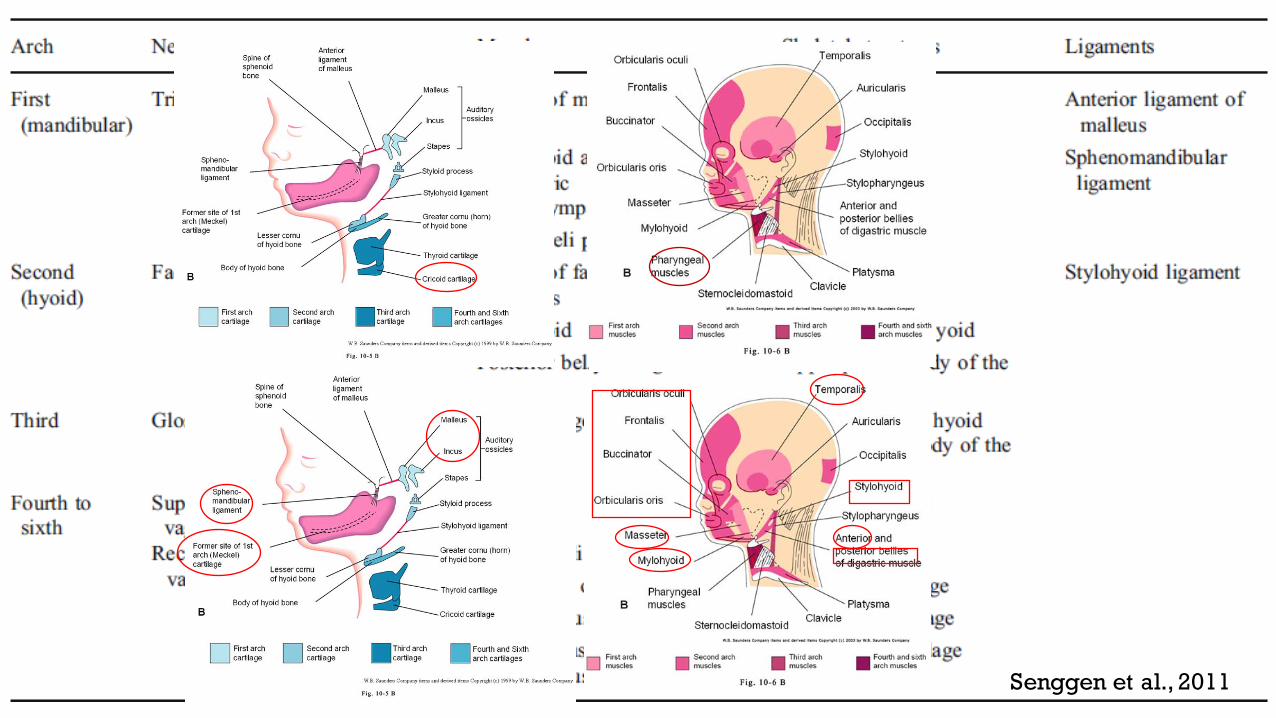
DERIVATIVES OF THE PHARYNGEAL ARCH CARTILAGES
12

§ The musculature of the first pharyngeal arch forms the muscles of mastication
§ The second pharyngeal arch forms the stapedius, stylohyoid, posterior belly of digastric, auricular and muscles of facial expression
§ The third arch forms the stylopharyngeus
§ The fourth arch forms cricothyroid, levator veli palatini and constrictors of pharynx
§ Sixth pharyngeal arch forms the intrinsic muscles of the larynx
13

14

§ Caudal two branches of trigeminal nerve (maxillary and mandibular) supply derivatives of the first pharyngeal arch
§ The facial, glossopharyngeal and vagus nerves supply the second, third and caudal (fourth to sixth) arches respectively
§ The fourth arch is supplied by superior laryngeal branch of vagus nerve
§ The sixth arch is supplied by its recurrent laryngeal branch
15

16
Controversy surrounds the embryologic origin of the tracheal cartilages and the sternomastoid and trapezius muscles. On the basis of their nerve supply (spinal accessory [11th cranial] nerve), it appears that the latter two muscles are of mixed somitic and pharyngeal-arch origin.
17

Senggen et al., 2011 18
19Senggen et al., 2011

20Senggen et al., 2011

21

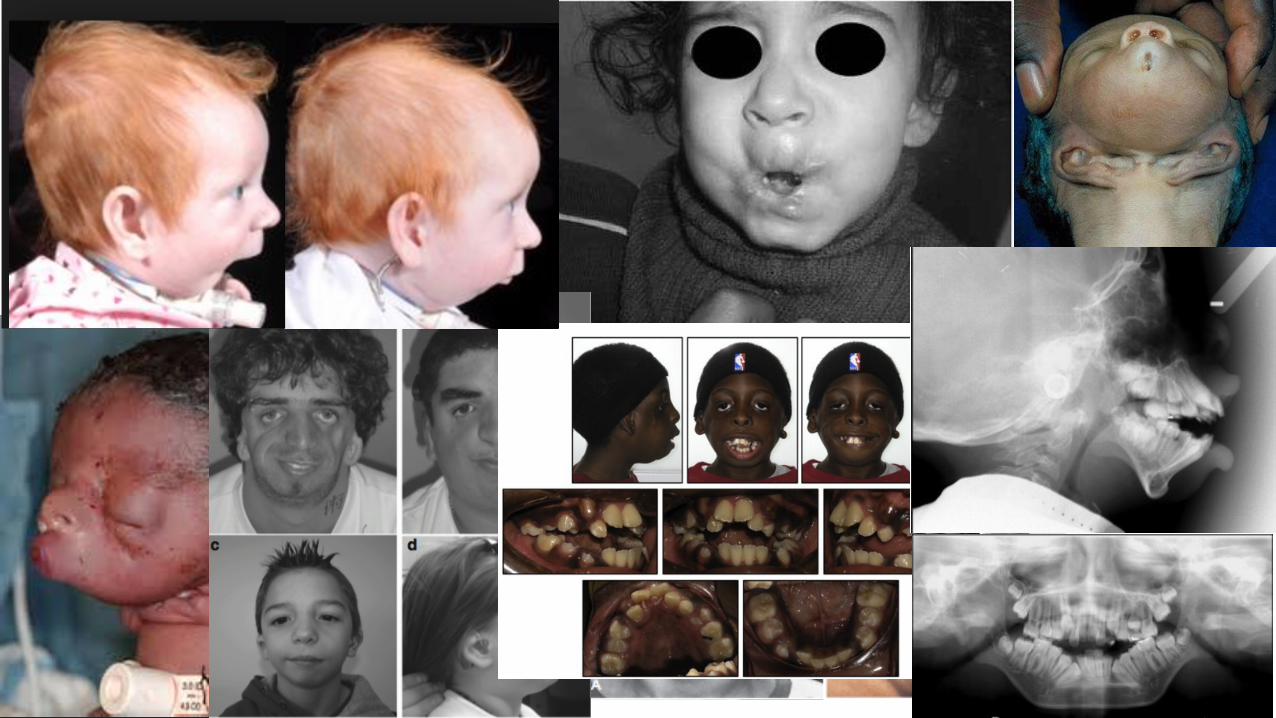
§ Deficient development of the pharyngeal arches results in syndromes that are identified according to the arch involved
§ The syndromes become rarer as the number of the arch increases.
§ Severe first-arch anomalies are:§ Agnathia§ Synotia§ Microstomia
§ Less severe:§ Treacher Collins syndrome§ Pierre Robin syndrome
§ Anomalies of the second and subsequent arches involve the hyoid
22
§ Deficient development of the pharyngeal arches results in syndromes that are identified according to the arch involved.
§ The syndromes become rarer as the number of the arch increases.
§ Severe first-arch anomalies are:§ Agnathia§ Synotia§ Microstomia
§ Less severe:§ Treacher Collins syndrome§ Pierre Robin syndrome
§ Anomalies of the second and subsequent arches involve the hyoid.
23

24

26
The primitive pharynx forms in the late embryonic period as a dilation ofthe cranial end of the foregut. Intervening between the pharyngeal arches externally are the pharyngeal grooves (ectodermal clefts).
The lining of the pharyngeal grooves is the surface ectoderm;that of the internal pharyngeal pouches is foregut endoderm.

27
Each ectodermal pharyngeal groove corresponds with each endodermal pharyngeal pouch, with a layer of mesodermal mesenchyme intervening between the outer and inner primary germ layers.
The second, third, and fourth pharyngeal grooves become obliterated by the caudal overgrowth of the second pharyngeal arch, which provides a smooth contour to the neck.

28Grevellec and Tucker, 2010

§ The first pharyngeal pouch expands into an elongate tubotympanic recess
§ The expanded distal part of this recess contacts the first pharyngeal groove, where it contributes to the formation of the tympanic membrane (eardrum)
§ The cavity of the tubotympanic recess gives rise to the tympanic cavity and mastoid antrum
29

§ The second pharyngeal pouch is largely obliterated as the palatine tonsils develop
§ Part of the cavity of this pouch remains as the tonsillar sinus or fossa
§ The endoderm of the pouch proliferates and grows into the underlying mesenchyme
§ The central parts of these buds form crypts
§ The pouch endoderm forms the surface epithelium and the lining of the tonsillar crypts
§ At about 20 weeks the mesenchyme around the crypts differentiates into lymphoid tissue
§ These tissues soon organize into the lymphatic nodules of the palatine tonsil30

§ The primordia of thymus and parathyroid glands lose their connections with the pharynx and migrate into the neck
§ Later the parathyroid glands separate from the thymus and lie on the dorsal surface of the thyroid gland
31

§ The fourth pharyngeal pouch also expands into dorsal bulbar and elongate ventral parts
§ Its connection with the pharynx is reduced to a narrow duct that soon degenerates
§ By the sixth week, each dorsal part develops into a superior parathyroid gland
§ It lies on the dorsal surface of the thyroid gland
§ The parathyroid glands derived from the third pouches descend with the thymus and are carried to a more inferior position than the parathyroid derived from the fourth pouches
§ This explains why the parathyroid glands derived from the third pair of pouches are located inferior to those from the fourth pouches
32

Fifth pouch appears as a diverticulum of the fourth pouch.
§ Forms ultimopharyngeal body
§ The calcitonin-secreting cells of this structure, are derived from neural crest tissue and eventually incorporated into the thyroid gland as parafollicularcells
§ The laryngeal ventricles could represent the remnants of the fifth pharyngeal pouch.
33

34
Defective development of the pharyngeal pouches results in defects of their derivatives
The most common anomalies are pharyngeal fistulae and cysts and persistent tracks of migrated glands derived from the pouches along with DiGeorge syndrome.
35

La Riviere and Waldhausen, 2012 36

La Riviere and Waldhausen, 2012 37

La Riviere and Waldhausen, 2012 38

The syndrome was described in 1965 by the pediatric endocrinologist Angelo DiGeorge.
22q11.2 deletion syndrome, a disorder caused by a defect in chromosome 22, results in the poor development of several body systems.
A congenital absence of the thymus and parathyroid glands (and thus, of their products) results in metabolic defects and increased susceptibility to infection.
Medical problems commonly include heart defects, poor immune system function, a cleft palate, complications related to low levels of calcium in the blood and behavioral disorders. 39

§ Many of the structures primarily affected are derivatives of the brachial arch/pharyngeal pouch system§ Face – 1st branchial arch§ Heart – branchial arch arteries – 1st-4th arches§ Thymus – 3rd pharyngeal pouch§ Parathyroid – 3rd & 4th pharyngeal pouch
12/9/15

41

42
https://youtu.be/oP1-ejJdZyc?list=PLezrE0Ume1ToegmFDeIVoVRJ_dZ-bVaD5

1. Sperber book (Chapters 4 & 5)
2. Grevellec, A., Tucker, A. S., 2010. The pharyngeal pouches and clefts: Development, evolution, structure and derivatives. Semin Cell Dev Biol. 21, 325-32
3. LaRiviere, C. A., Waldhausen, J. H., 2012. Congenital cervical cysts, sinuses, and fistulae in pediatric surgery. Surg Clin North Am. 92, 583-97, viii
4. Senggen, E., Laswed, T., Meuwly, J. Y., Maestre, L. A., Jaques, B., Meuli, R., Gudinchet, F., 2011. First and second branchial arch syndromes: multimodality approach. PediatrRadiol. 41, 549-61
5. http://medicalanomalies.blogspot.com/2012/09/digeorge-syndrome.html
6. https://youtu.be/oP1-ejJdZyc?list=PLezrE0Ume1ToegmFDeIVoVRJ_dZ-bVaD5
7. http://center-for-nonverbal-studies.org/pharynx.htm

Thank You