phase 1: formulating for success goals for phase i (first-in-human) studies koppenol, aaps, 2015,...
TRANSCRIPT

Phase 1: Formulating for Success
Sandy Koppenol, PhD Gilead Sciences, Inc. (Foster City, CA) AAPS Sunrise Session Wednesday, October 28, 2015

The Goals for Phase I (First-in-Human) Studies
Koppenol, AAPS, 2015, Sunrise Session
Phase 1
– Test a new drug or treatment in a small group of humans to evaluate safety, determine a safe dose range, and identify side effects.
– Typically this is done in two parts, 1.) single-ascending dose followed by 2.) multiple-ascending dose study.
– Performed in a well-controlled clinic where subjects are closely monitored.
2

The Role of the Formulation Scientist in Phase I Studies
Provide a dosage form that allows evaluation of the safety of subjects in the proposed study.
– Provide dose flexibility (OK to dose multiple tablets/capsules)
– Use excipients with known safety profile
– Be manufactured using a well-controlled process under GCP /GMP
– Must be chemically/physically stable
– Develop acceptable limits and analytical methods to assure the identity, strength, quality and purity of the drug product
FDA Guidance, “Content and Format of Investigational New Drug Applications for Phase 1 Studies of Drugs, Including Well-Characterized, Therapeutic, Biotechnology-Derived Products.” November 1995
Koppenol, AAPS, 2015, Sunrise Session 3

Challenges for the Formulation Scientist in Phase I Studies
Challenges for the development of the Phase 1 formulation scientist
– Uncertain/changing wide dose range
– Limited amount of representative drug substance (API)
– Limited knowledge of API physical/chemical characteristics
– Limited stability data available on API ± excipients
– Short timelines
– Balancing resource commitment vs. likelihood of success
Koppenol, AAPS, 2015, Sunrise Session 4

The Drug Must be in Solution to be Absorbed
Koppenol, AAPS, 2015, Sunrise Session 5

The Most Common Oral Formulation Options for Phase 1
Powder in Bottle API in Capsule
(Blend/solution)
Tablet
Advantages • Fast
• Small amount of API
• Manufacture at the
API site or weighed
at the clinic
• Fast
• Small amount of API
• Have PK data on a
solid dosage form
• Have PK data on
intended dosage
form
• Faster transition
to Phase 2
Disadvantages • May need
taste/color-masking
for placebo
• Not acceptable for
Phase 2
• Likely need to do an
rBA study to
transition to Phase 2
dosage form
• Formulation
development has
been delayed
• Not ideal for Phase
2
• Likely need to do an
rBA study to
transition to Phase 2
dosage form
• Formulation
development has
been delayed
• Requires more
development time
• API needs are
larger
• Must be
manufactured in
advance of the
clinical trial
Koppenol, AAPS, 2015, Sunrise Session 6
Powder in Bottle (PIB)
Typically put 8 to 10 doses in one bottle
Can be reconstituted to a solution or suspension
Diluents/suspending agents
– Water or juice
– Ora-sweet: may provide taste-masking
– Ora-plus: suspending agent
Suspension challenges
– Particle size can impact bioavailability
– Need to demonstrate uniformity of dosage units
– Suspension may require homogenization
– Recovery of the dose may require rinsing of oral syringe/dose cup
– Placebo must be blinded with insoluble powder
Manufacture
– API manufacturer can usually weigh bulk powder into a bottle
– Phase 1 clinical site pharmacy will perform reconstitution
Koppenol, AAPS, 2015, Sunrise Session 7

API (Powder or Solution) in Capsule
Manual Filling
– Can be performed in Phase 1 pharmacies as a compounding operation*
– Analytical balance limitations for dose.
*USP <795>
Automated Filling with Capsugel’s Xcelodose
– Must be manufactured under cGMPs
– Can fill as low as 100 mcg
– Capable of filling up to 600+ capsules/hour
Koppenol, AAPS, 2015, Sunrise Session 8

Prototype Solid Dosage Form
Likely need 2 to 3 unit doses to span Phase 1 dosing range (10-100x)
Excipient compatibility
– Diluents: Lactose, Mannitol, Microcrystalline cellulose, Dicalcium phosphate
– Binders: HPMC, HPC, PVP
– Disintegrant: croscarmaellose Na, Crospovidone
– Lubricant: Mg stearate, stearic acid
Development of tablet need 0.5kg+ of a granulation/batch
– Direct compression
– Dry or wet granulation
Clinical batches must be manufactured under cGMPs
Koppenol, AAPS, 2015, Sunrise Session 9

Analytical Methods, Stability and Specifications for Tablets
Analytical method development
– Blend and content uniformity
– Dissolution
Stability
– In-use stability of reconsitituted solutions and suspensions must be examined
– ICH stability protocols are recommended for the dosage form provided to the clinic (ICH Q1A).
Specifications for excipients and drug product
Koppenol, AAPS, 2015, Sunrise Session 10
Test Acceptance Criteria
Appearance Round, plain-faced, film-coated, white tablets
Identification by HPLC Consistent with reference standard
Water Content Report
Strength by HPLC 90.0-110.0% of Label Claim
Impurity Content
Uniformity of Dosage Units Meets current USP<905>
Dissolution Report amount dissolved at 15, 30 and 45 min
Microbiological Examination Meets current USP
Regulatory Requirements for Tablets
Regulatory requirements*
– Pharmaceutical development and manufacturing
Section 3.2.P.2 Pharmaceutical Development
Section 3.2.P.3 Manufacture of Drug Product
– Acceptable limits and analytical test methods must be described.
– Certificate of Analysis must be provided
– Information to support the stability of the drug product packaged in the proposed container/closure and storage conditions for at least one month
Koppenol, AAPS, 2015, Sunrise Session 11
*FDA Guidance, “Content and Format of Investigational New Drug Applications for Phase 1 Studies of Drug, Including Well-Characterized, Therapeutic, Biotechnology-derived Products.: November 1995.

Case Study 1: API Solution-Filled Capsule
Dose range for Phase 1: 5 to 250 mg
BCS Class I/II compound
API is amorphous
– Tg (dry) = 56°C
– Spray drying yields are low
– Solid is hygroscopic
– Compound has a bitter taste
Koppenol, AAPS, 2015, Sunrise Session 12
Aqueous
Solubility
(mg/ml)
P/ (x10-6
cm/s)
A to B
P/ (x10-6
cm/s)
B to A
Ratio
0.66 2.10 6.72 3.2
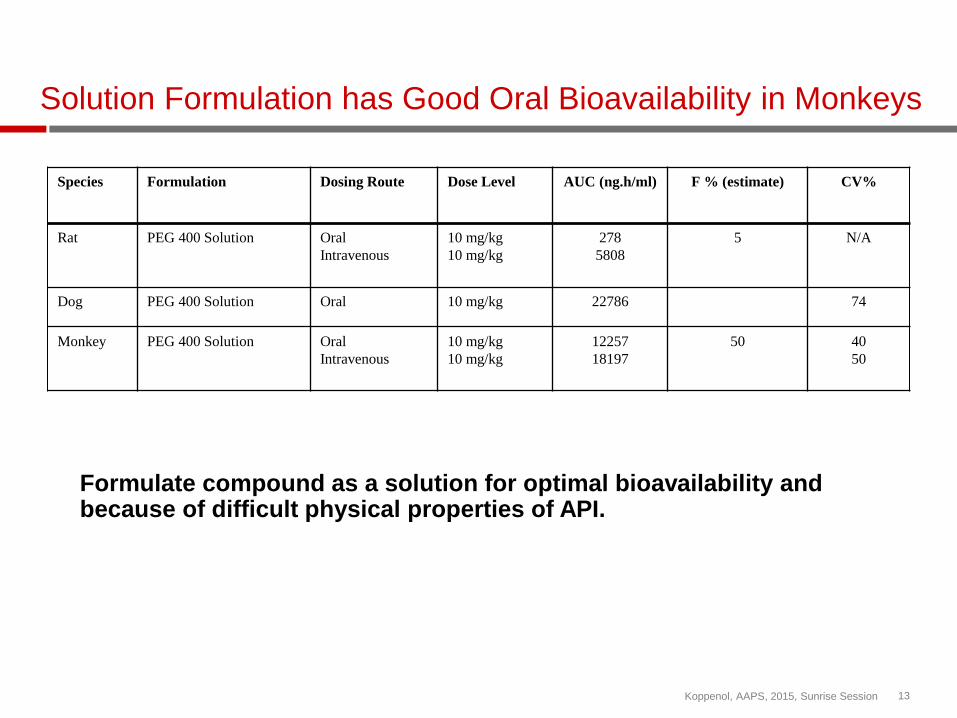
Solution Formulation has Good Oral Bioavailability in Monkeys
Species Formulation Dosing Route Dose Level AUC (ng.h/ml) F % (estimate) CV%
Rat PEG 400 Solution Oral
Intravenous
10 mg/kg
10 mg/kg
278
5808
5 N/A
Dog PEG 400 Solution Oral 10 mg/kg 22786 74
Monkey PEG 400 Solution Oral
Intravenous
10 mg/kg
10 mg/kg
12257
18197
50 40
50
Formulate compound as a solution for optimal bioavailability and because of difficult physical properties of API.
Koppenol, AAPS, 2015, Sunrise Session 13
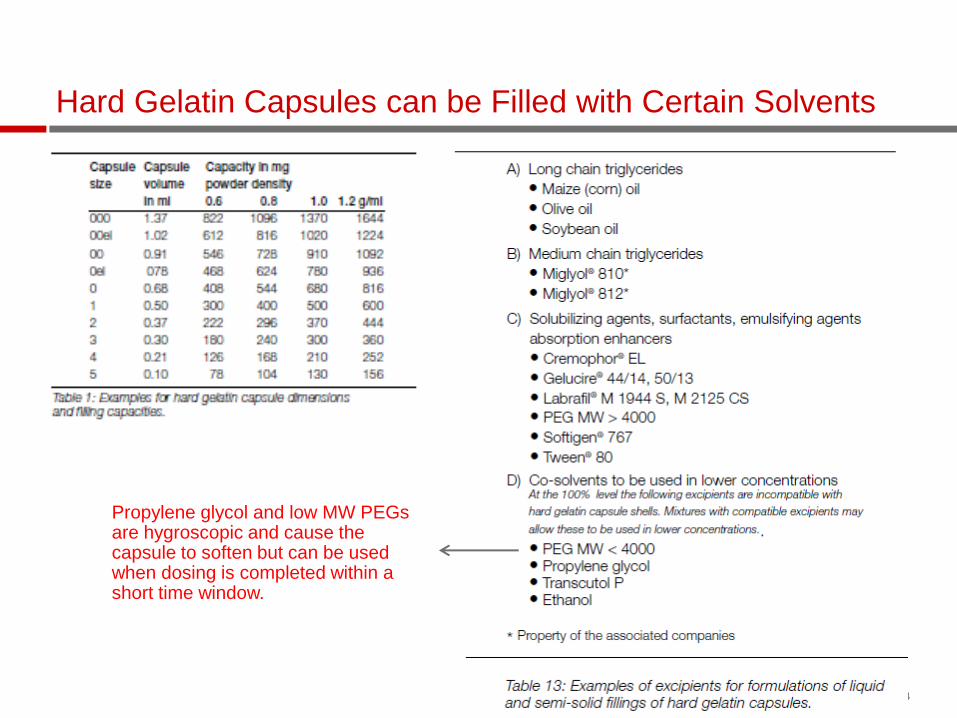
Hard Gelatin Capsules can be Filled with Certain Solvents
Koppenol, AAPS, 2015, Sunrise Session 14
Propylene glycol and low MW PEGs are hygroscopic and cause the capsule to soften but can be used when dosing is completed within a short time window.

Capsules Were Filled Manually at the Phase 1 Pharmacy
Koppenol, AAPS, 2015, Sunrise Session 15
Powder in bottle was supplied to the Phase 1 pharmacy • Each bottle contained a pre-weighed
quantity of API to make 10 unit doses (1 bottle per clinical cohort)
• API was weighed into bottles by the API manufacturer using a batch record
• Weight was checked by 200% inspection • Bottles were released by QA based on batch
record and ID and appearance testing.
Solution was prepared by adding specified amount of PEG400 and shaking at RT overnight.
Capsules are filled and dispensed by the Phase 1 pharmacy • Compounding instructions and preparation
worksheets were created. • Capsules were filled based on weight and
density of the drug solution. • Weight was checked by 200% inspection • All steps are documented in worksheets • Capsules were stored upright and
administered to the patient within 12 hours • QA reviews the worksheets.

API Solution-Filled Capsule has Good Oral Bioavailability
Species Formulation Dosing Route Dose Level AUC (ng.h/ml) F % (estimate) CV%
Rat PEG 400 Solution Oral
Intravenous
10 mg/kg
10 mg/kg
278
5808
5 N/A
Dog PEG 400 Solution Oral 10 mg/kg 22786 74
Monkey PEG 400 Solution Oral
Intravenous
10 mg/kg
10 mg/kg
12257
18197
50 40
50
Human Gel capsule with PEG
400 Solution
Oral 100 mg
250 mg
24881
42207
55
13
Koppenol, AAPS, 2015, Sunrise Session 16

Case Study 2: Prototype Tablet
Dose range for Phase 1: 0.1 to 9 mg
BCS Class I compound
Weak base
API has good physical properties
– Crystalline, Tm = 165°C
– Non-hygroscopic:1.4% water at 25°C/90% RH
– Small particle size of the API: d50 = 4.39µm
0.5 kg of API available
Good oral bioavailability from a powder in capsule in dog model
Koppenol, AAPS, 2015, Sunrise Session 17
Formulation (Dog PK) Average AUClast (nM*hr) Average Cmax (nM)
0.25mg/Kg PIC 1120 ±415 583 ±209
0.25mg/Kg solution 1563 ±663 334 ±88
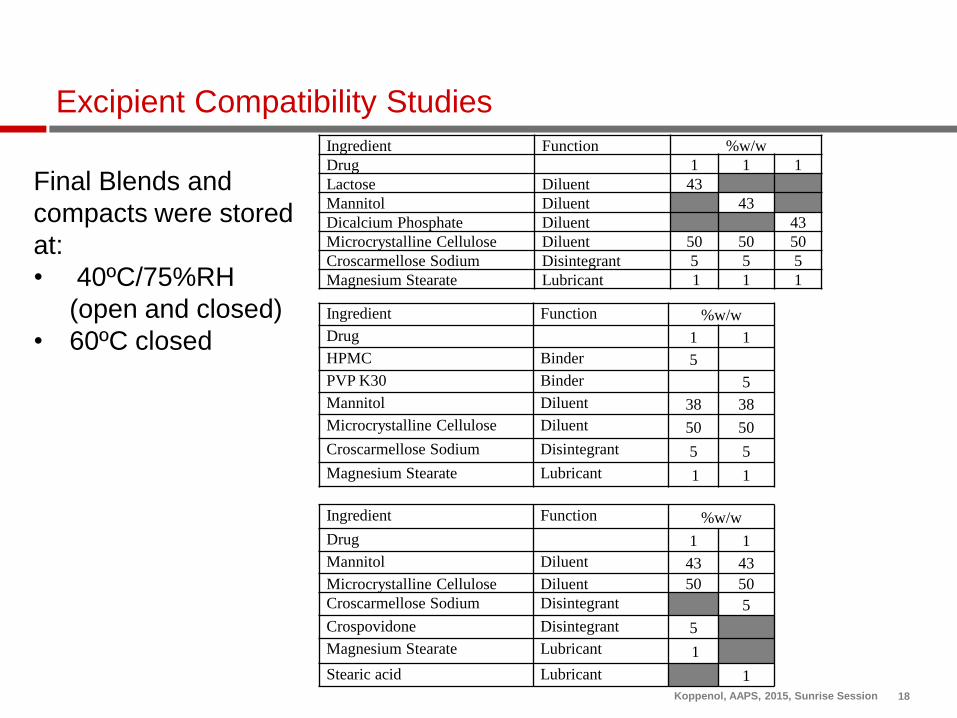
Excipient Compatibility Studies
Ingredient Function %w/w
Drug 1 1 1
Lactose Diluent 43
Mannitol Diluent 43
Dicalcium Phosphate Diluent 43
Microcrystalline Cellulose Diluent 50 50 50
Croscarmellose Sodium Disintegrant 5 5 5
Magnesium Stearate Lubricant 1 1 1
Final Blends and
compacts were stored
at:
• 40ºC/75%RH
(open and closed)
• 60ºC closed
18
Ingredient Function %w/w
Drug 1 1
HPMC Binder 5
PVP K30 Binder 5
Mannitol Diluent 38 38
Microcrystalline Cellulose Diluent 50 50
Croscarmellose Sodium Disintegrant 5 5
Magnesium Stearate Lubricant 1 1
Ingredient Function %w/w
Drug 1 1
Mannitol Diluent 43 43
Microcrystalline Cellulose Diluent 50 50
Croscarmellose Sodium Disintegrant 5
Crospovidone Disintegrant 5
Magnesium Stearate Lubricant 1
Stearic acid Lubricant 1
Koppenol, AAPS, 2015, Sunrise Session

Phase 1 Film-Coated Tablet Formulation
19
Components
Composition
0.1 mg 1 mg 5 mg
% w/w mg/tablet % w/w mg/tablet % w/w mg/tablet
Intragranular
Drug 0.1 0.1 1 1 1 5
Diluent 1 50 50 50 50 50 250
Diluent 2 45.9 45.9 45 45 45 225
Disintegrant 3.0 3.0 3.0 3.0 3.0 15
Lubricant 0.5 0.5 0.5 0.5 0.5 1.5
Extragranular
Lubricant 0.5 0.5 0.5 0.5 0.5 1.5
Total 100 100 100 100 100 500
Tablet Coating
Opadry blue 3 3 3 3 3 15
Total 103 103 103 103 103 515
Koppenol, AAPS, 2015, Sunrise Session

Development Lot Stability Protocol
Materials
– 0.1 mg tablets
– 1 mg tablets
– 5 mg tablets
Container/closure: 30 count tablets in a 60 cc white, high density polyethylene (HDPE) bottles with polyester fiber coil, capped with a white, continuous thread, child-resistant, polypropylene screw cap fitted with an induction-sealed, aluminum-faced liner.
Tests: Content uniformity (T0), Strength, Impurities/Deg products, Dissolution, Disintegration, and water content
20
Time (months)
T0 0.5 1 2 3 6 9 12
Condition
25 ºC/60%RH X
X X X X X
40 ºC/75%RH X X X
40 ºC/75%RH, open X X X
Koppenol, AAPS, 2015, Sunrise Session

Even Though The Tablets Reach >80% Dissolved at 15 Minutes, the Oral Bioavailability in Dogs is Lower Than a Solution
21
Formulation (Dog PK) Average AUClast (nM*hr) Average Cmax (nM)
0.25mg/Kg* PIC 1120 ±415 583 ±209
0.25mg/Kg solution 1563 ±663 334 ±88
0.25mg/Kg
1 mg tablets, 3 tablets/animal 732 ±158 265 ±93
Dissolution conditions: Type II apparatus with 50 mM sodium citrate buffer, pH 5.5 with 0.5% SDS
with 75rpm paddle speed
* ¼ of the clinical dose Koppenol, AAPS, 2015, Sunrise Session

Prototype Tablet Shows Good Bioavailability in Humans with Dose Proportional AUC and Cmax
S/MAD : Doses are 0.1, 0.3, 1, 3 and 9 mg (SAD only), MAD dosing is 10 days
– Single doses exhibit dose-proportional PK over the studied dose range
– Multiple dose plasma concentrations suggest moderate accumulation
– The terminal half-life is approximately 16 hours
– No significant safety observations
22 Koppenol, AAPS, 2015, Sunrise Session

Summary
Phase 1 studies are challenging
– require flexibility in dosing and may require large dose range
– Limited time and material
– Difficulty to predict dose linearity from animal models and in-vitro dissolution
– Not a lot of information available on the physical/chemical properties of the API
– Analytical methods not optimized
There are 3 common approaches to Phase 1 oral formulations
– Powder in bottle
– API in capsule
– Prototype tablet
Opportunities
– Phase 1 formulation scientists work closely with clinicians to optimize the drug product for safety and bioavailability
– Good early understanding of the physical/chemical properties of the API and the link to product performance can accelerate products to the market. Koppenol, AAPS, 2015, Sunrise Session 23