phase ii trial of continuous course re- irradiation concurrent with weekly cisplatinum and cetuximab...
TRANSCRIPT

Phase II Trial of Continuous Course Re-irradiation Concurrent with Weekly
Cisplatinum and Cetuximab for Recurrent Squamous Cell Carcinoma of The Head And
Neck: A Preliminary Report
Min Yao, MD, PhDUniversity Hospitals Case Medical Center
Cleveland, Ohio

Disclosure
The study was funded by a research grant from
Bristol-Myers Squibb.

UT Southwestern Medical Center
Randall Hughes, MDLarry Myers, MDLucien Nedzi, MDIrma Smith, CSABaran Sumer, MDJohn Truelson, MDJohn Yordy, MD,
PhD
University Hospitals Case Medical Center
Min Yao, MD, PhDPierre Lavertu, MD
Medical College of Wisconsin
Dian Wang, MDStuart Wong, MD
Participating Institutions

Eligibility
1) Pathologically confirmed recurrent or second primary SCC of the upper aerodigestive tract (excluding nasopharynx and salivary gland tumors). No metastatic disease
2) Unresectable disease or positive margins after surgical resection.
3) Majority of recurrent tumor in areas previously irradiated to > 45 Gy, but not exceeding 75 Gy.
4) Prior radiotherapy completed more than 6 months prior to study entry
5) No prior chemotherapy for recurrent disease
6) KPS > 70 %. Adequate bone marrow, hepatic and renal function

Treatment Schema
Week 1:cetuximab 400mg/m2 as a loading dose
Weeks 2-7cetuximab 250mg/m2 weekly
cisplatinum 30mg/m2 weekly
continuous course IMRT 60-66 Gy/30/6 weeks

Intensity-Modulated Radiotherapy
GTVClinically and radiographically defined gross tumor or in patients after surgery, tumor bed that include pre-operative gross disease
Integrated boostsCTV = GTV + 0.5 cmPTV = CTV + 0.5 cm (0.2 – 0.3 cm with IGRT)• GTV 60 to 66 Gy/30 fractions• PTV 60 Gy/30 fractions

Critical Structures
Spinal cord PRV = cord + 0.5 cm (0.2 cm with IGRT)
Cumulative dose not to exceed 54 Gy (including prior
radiotherapy)
Brainstem PRV = brainstem + 0.5 cm (0.2 cm with IGRT)
Cumulative dose not to exceed 60 Gy (including prior
radiotherapy)
Intensity-Modulated Radiotherapy

Intensity-Modulated Radiotherapy
A patient with unresectable nodal recurrence 6 years after postop XRT for an oral tongue cancer

Intensity-Modulated Radiotherapy

Patient Population
48 patients rerolled between March 2009 – May 2013Male 36, Female 12, median age 62Two withdrew and 46/48 received protocol treatment40% re-PORT after attempted surgical resection with positive marginMedian follow-up 9 months

Kaplan-Meier curve for overall survival
The 1 year survival probability is 0.60 (95% CI: 0.41 – 0.75)
Treatment Outcome
Treatment Outcome
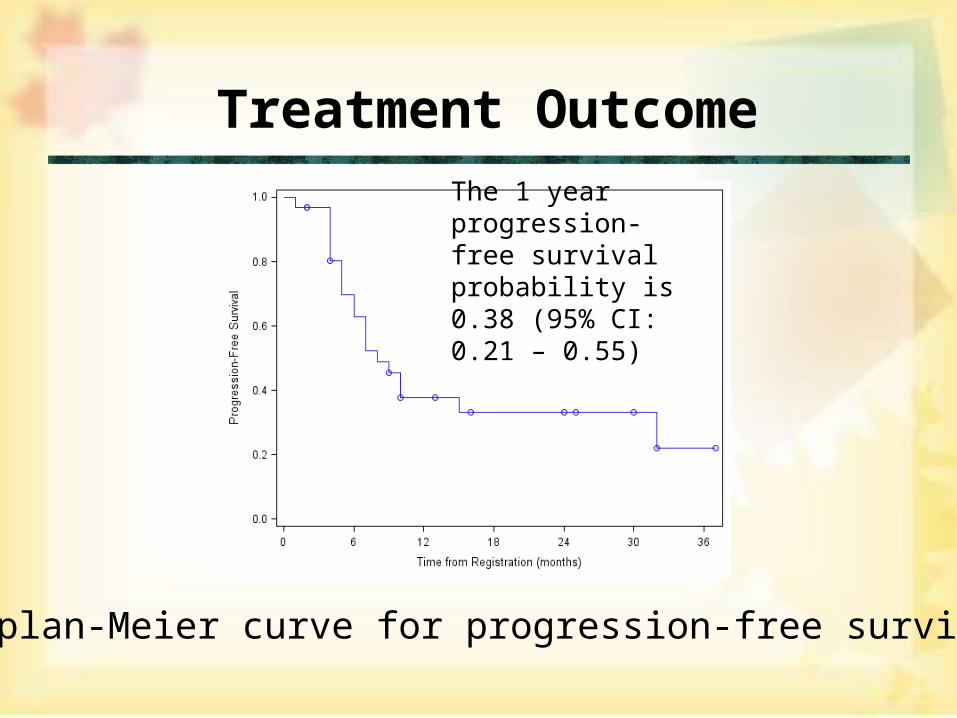
Kaplan-Meier curve for progression-free survival
The 1 year progression-free survival probability is 0.38 (95% CI: 0.21 – 0.55)

Treatment Delivery
Only one patient did not complete the treatment
course, received only 3 cycles of chemo
All other patients completed the treatment course

Acute Toxicity: Highest GradeGrade
Acute Toxicity 3 4 5 Total %lymphopenia 17 4 21 46dysphagia 6 6 13
rash: dermatitis assoc. w/ XRT 5 1 6 13anorexia 5 5 11mucositis 5 5 11neutropenia 3 1 4 9fatigue 3 3 7hemoglobin 2 1 3 7hyponatremia 3 3 7hypophosphatemia 3 3 7leukocytes 2 1 3 7dehydration 2 2 4hyperglycemia 2 2 4hypoalbuminemia 2 2 4

Late Toxicity 90 days after treatmentGrade
Late Toxicity 1 2 3 Total %dysphagia 4 4 2 10 22%hemoglobin 8 2 10 22%lymphopenia 2 6 2 10 22%fatigue 3 6 9 20%xerostomia 5 2 7 15%edema: head & neck 6 6 13%mucositis 3 3 6 13%fibrosis 2 3 5 11%hypoalbuminemia 3 2 5 11%trismus 4 1 5 11%weight loss 5 5 11%platelets 4 4 9%hypomagnesemia 3 3 7%hypothyroidism 1 2 3 7%nausea 3 3 7%pain: gastrointestinal: oral cavity 3 3 7%pain: musculoskeletal: Neck 1 2 3 7%

Conclusions
• Compared to RTOG 9610 and RTOG 9911,
the treatment is better tolerated with superior
one year overall survival.
• Longer follow up is needed, with future
analysis of failure pattern and prognostic
indicators