phase ii trial of trastuzumab followed by weekly paclitaxel/carboplatin as first-line treatment for...
TRANSCRIPT

Phase II Trial of Trastuzumab Followed by Phase II Trial of Trastuzumab Followed by Weekly Paclitaxel/Carboplatin as First-Line Weekly Paclitaxel/Carboplatin as First-Line
Treatment for Patients with Metastatic Breast Treatment for Patients with Metastatic Breast CancerCancer
Burris H III, Yardley D, Jones S, Houston G, Broome C, Thompson D, Greco F, White M and Hainsworth
J. J Clin Oncol 2004;22(9):1621-29.

Study ObjectivesStudy Objectives
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.
Evaluate Response rate to trastuzumab (H) in previously
untreated patients
Activity of a weekly carboplatin/paclitaxel (CT) regimen in patients not responding to H
Activity, feasibility and toxicity of weekly TCH
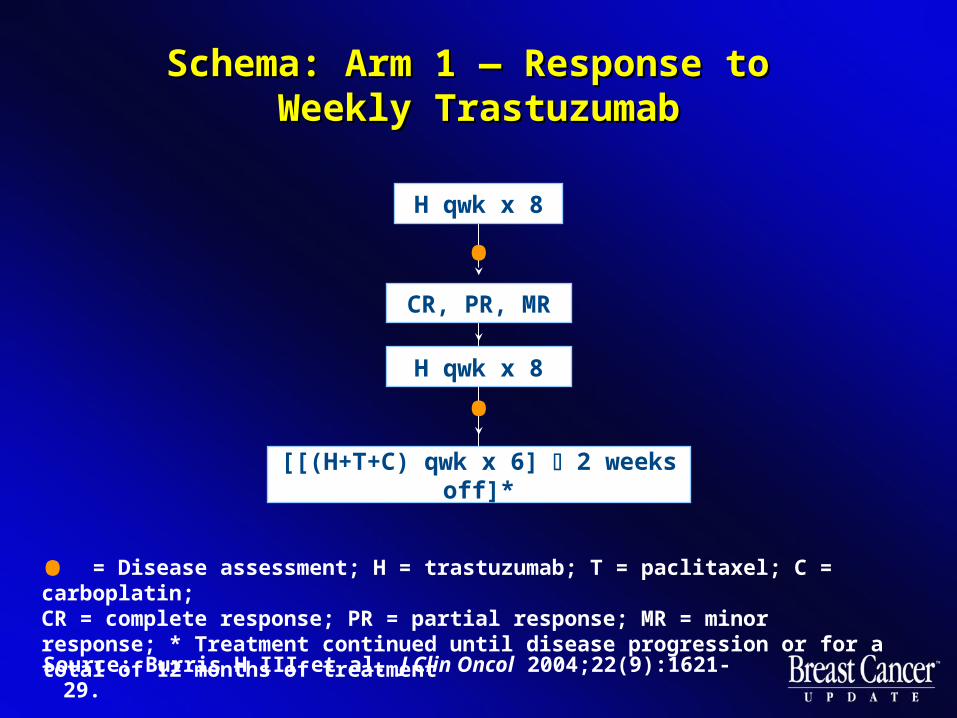
Schema: Arm 1 — Response to Schema: Arm 1 — Response to Weekly TrastuzumabWeekly Trastuzumab
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.
H qwk x 8
[[(H+T+C) qwk x 6] 2 weeks off]*
= Disease assessment; H = trastuzumab; T = paclitaxel; C = carboplatin; CR = complete response; PR = partial response; MR = minor response; * Treatment continued until disease progression or for a total of 12 months of treatment
H qwk x 8
•
•
•
CR, PR, MR

Schema: Arm 2 — Stable Disease Schema: Arm 2 — Stable Disease with Weekly Trastuzumabwith Weekly Trastuzumab
Stable disease
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.
[[(H+T+C) qwk x 6] 2 weeks off]*
= Disease assessment; H = trastuzumab; T = paclitaxel; C = carboplatin; * Treatment continued until disease progression or for a total of 12 months of treatment
H qwk x 8
•
•

Schema: Arm 3 — Disease Progression Schema: Arm 3 — Disease Progression on Weekly Trastuzumabon Weekly Trastuzumab
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.
[[(T+C) qwk x 6] 2 weeks off]*
= Disease assessment; H = trastuzumab; T = paclitaxel; C = carboplatin; * Treatment continued until disease progression or for a total of 12 months of treatment
H qwk x 8
•
•
Off treatment
CR, PR, SD
Progression
•
H+T+C*
Progression

Patient Characteristics Patient Characteristics
61 patients enrolled
Assessable for response (n=52)
Median age: 51
ER/PR-positive (n=34)
HER2-positive
IHC 3+ (n=41)
IHC 2+ (n=20)
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.

Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.
Results: Overall Response, Results: Overall Response, Progression and SurvivalProgression and Survival
Overall response rate (n=52) = 69% (9 CRs, 27 PRs) IHC 3+ (n=34): Overall response rate = 78.6% IHC 2+ (n=18): Overall response rate = 50%
Median duration of CR = 18.8 months Median duration of PR = 8.5 months Median time to progression for all patients was
10 months Median overall survival of all patients was
26.7 months

CR = complete response; PR = partial response; MR = minor response
Post 8 weeks H(n=52)
Post 16 weeks H(n=16)
CR 0% 0%
Overall response (CR + PR + MR)
32.7% 75.0%
Stable disease 28.8% 6.3%
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.
Results: Disease Response after 8 or Results: Disease Response after 8 or 16 Weeks of Single-Agent 16 Weeks of Single-Agent
Trastuzumab (H)Trastuzumab (H)

Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.
Results: Response to CT and TCHResults: Response to CT and TCH
Patients with stable disease or responding to weekly trastuzumab (H) had an 84 percent response rate to TCH. TTP was 14.2 months, and OS was 32.2 months.
Patients failing to respond to weekly trastuzumab (H) had a 69 percent response rate to the addition of carboplatin/paclitaxel (CT). TTP was 8.3 months, and OS was 22.2 months.

ToxicityToxicity
Hematologic toxicity
Grade III/IV neutropenia = 28%
Grade III thrombocytopenia = 3%
Grade III/IV anemia = 5%
No Grade IV nonhematologic toxicities
Weakness and fatigue most common
Carboplatin hypersensitivity = 7 patients
Grade III neuropathy = 3 patients
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.

CardiotoxicityCardiotoxicity
LVEF decline > 20% = 5/61 (8.2%)
LVEF in 3 patients > 20% but asymptomatic and continued trastuzumab
Two patients discontinued therapy due to declines in LVEF
• One patient exhibited symptoms of CHF
• One patient was asymptomatic but had a 40% decline in LVEF
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.

ConclusionsConclusions
Single-agent H is safe and effective initial therapy in patients with HER2-positive metastatic disease
The addition of CT to weekly H increases the response rate
Weekly CT is a highly active, well-tolerated regimen in metastatic breast cancer
Lack of response to H did not interfere with sensitivity to weekly CT
Source: Burris H III et al. J Clin Oncol 2004;22(9):1621-29.

American Society of Clinical Oncology American Society of Clinical Oncology Technology Assessment on the Technology Assessment on the
Use of Aromatase Inhibitors as Adjuvant Use of Aromatase Inhibitors as Adjuvant Therapy for Postmenopausal Women with Therapy for Postmenopausal Women with
Hormone Receptor-Positive Hormone Receptor-Positive Breast Cancer: Status Report 2004Breast Cancer: Status Report 2004
Winer EP, Hudis C, Burstein HJ, Wolff AC, Pritchard KI, Ingle JN, Chlebowski RT, Gelber R, Edge SB, Gralow J, Cobleigh MA, Mamounas
EP, Goldstein LJ, Whelan TJ, Powles TJ, Bryant J, Perkins C, Perotti J, Braun S, Langer AS, Browman GP, Somerfield MR.
J Clin Oncol 2004;22(9):1621-29.

Technology AssessmentTechnology Assessment
Describes practice procedures and therapies based on a review and synthesis of latest literature
Identifies important questions
Identifies settings for future research
Reviewed annually and updated as needed
Voluntary adherence
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Sources: Winer EP et al. J Clin Oncol 2002;20(15):3317-27. Winer EP et al. J Clin Oncol 2003;21(13):2597-9. Winer EP et al. J Clin Oncol 2005;23(3):619-29. Howell A. Presentation. SABCS 2004. Jakesz R. Presentation. SABCS 2004.
Technology Assessment TimelineTechnology Assessment Timeline
Dec 2001
May 2002
Dec 2002
May 2003
Dec 2003-Mar 2004
Dec 2004
Jan 2005
— First results of ATAC trial, 33 months
— Initial technology assessment panel report on adjuvant use of aromatase inhibitors
— ATAC results at 47 months
— First technology assessment update
— Results of ITA, MA17 and IES studies
— ATAC 68-month resultsARNO 95/ABCSG 8 results
— Second technology assessment update

Phase III Randomized Adjuvant Trials Phase III Randomized Adjuvant Trials Comparing Third-Generation Aromatase Comparing Third-Generation Aromatase
Inhibitors to Tamoxifen or PlaceboInhibitors to Tamoxifen or Placebo
Trial Design N
ATAC T vs A vs T+A in newly diagnosed patients 9,366
MA17Letrozole vs placebo in patients after 5 years of tamoxifen
5,187
ITA T vs A in patients after 2 to 3 years of tamoxifen 426
IES T vs E in patients after 2 to 3 years of tamoxifen 4,742
ARNO 95ABCSG 8
T vs A in patients after 2 years of tamoxifen 3,123
Sources: Jakesz R. Presentation. SABCS 2004; Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.
Are There New Data to Prompt a Recommendation Are There New Data to Prompt a Recommendation for an Aromatase Inhibitor as Initial Adjuvant for an Aromatase Inhibitor as Initial Adjuvant
Therapy in Unselected Postmenopausal Patients Therapy in Unselected Postmenopausal Patients with Hormone Receptor-Positive Breast Cancer? with Hormone Receptor-Positive Breast Cancer?
“...treatment with an aromatase inhibitor is a reasonable alternative to tamoxifen following primary surgery for any women with a hormone receptor-positive breast cancer.”
“An aromatase inhibitor is the treatment of choice as initial adjuvant therapy for any postmenopausal women with hormone receptor-positive invasive breast cancer with a contraindication to tamoxifen.”

Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.
Are There New Data to Prompt a Recommendation Are There New Data to Prompt a Recommendation for an Aromatase Inhibitor as Initial Adjuvant for an Aromatase Inhibitor as Initial Adjuvant
Therapy in Unselected Postmenopausal Patients Therapy in Unselected Postmenopausal Patients with Hormone Receptor-Positive Breast Cancer? with Hormone Receptor-Positive Breast Cancer?
“...For women who do not have a contraindication to tamoxifen, it remains unclear if initial treatment with an aromatase inhibitor is superior, equivalent, or inferior to a planned cross-over from tamoxifen to an aromatase inhibitor after a fixed point in time.”
Do the Results of the MA17 Trial Provide Sufficient Do the Results of the MA17 Trial Provide Sufficient Evidence to Recommend the Use of an Aromatase Evidence to Recommend the Use of an Aromatase Inhibitor in Postmenopausal Women with Hormone Inhibitor in Postmenopausal Women with Hormone
Receptor-Positive Breast Cancer who have Receptor-Positive Breast Cancer who have Completed a 5-Year Course of Tamoxifen? Completed a 5-Year Course of Tamoxifen?
“... postmenopausal women finishing 5 years of tamoxifen for ER-positive, early-stage breast cancer should consider treatment with an aromatase inhibitor. ...At present, a minimum of 2.5 years of therapy can be recommended based on the median follow-up from MA-17.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Do the Results of the MA17 Trial Provide Sufficient Do the Results of the MA17 Trial Provide Sufficient Evidence to Recommend the Use of an Aromatase Evidence to Recommend the Use of an Aromatase Inhibitor in Postmenopausal Women with Hormone Inhibitor in Postmenopausal Women with Hormone
Receptor-Positive Breast Cancer who have Receptor-Positive Breast Cancer who have Completed a 5-Year Course of Tamoxifen? Completed a 5-Year Course of Tamoxifen?
“The survival advantage in the subset of women with node-positive disease is noteworthy and strengthens the argument for use of an aromatase inhibitor after tamoxifen in this patient population.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Do the Results of the IES and ITA Trials Provide Do the Results of the IES and ITA Trials Provide Sufficient Evidence to Recommend the Use of an Sufficient Evidence to Recommend the Use of an Aromatase Inhibitor in Postmenopausal Women Aromatase Inhibitor in Postmenopausal Women with Hormone Receptor-Positive Breast Cancer with Hormone Receptor-Positive Breast Cancer Who Have Received Tamoxifen for 2 to 3 Years?Who Have Received Tamoxifen for 2 to 3 Years?
“Both studies showed that a change in treatment from tamoxifen to an aromatase inhibitor reduced the risk of breast cancer recurrence.”
“... postmenopausal women concluding 2 to 3 years of tamoxifen therapy may consider cross-over to an aromatase inhibitor. ...such patients should plan on a total of 5 years of adjuvant endocrine therapy...”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Do the Results of the IES and ITA Trials Provide Do the Results of the IES and ITA Trials Provide Sufficient Evidence to Recommend the Use of an Sufficient Evidence to Recommend the Use of an Aromatase Inhibitor in Postmenopausal Women Aromatase Inhibitor in Postmenopausal Women with Hormone Receptor-Positive Breast Cancer with Hormone Receptor-Positive Breast Cancer Who Have Received Tamoxifen for 2 to 3 Years?Who Have Received Tamoxifen for 2 to 3 Years?
“...the optimal moment of transition from tamoxifen to an aromatase inhibitor is not known.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

What is the Optimal Duration of Therapy What is the Optimal Duration of Therapy with an Aromatase Inhibitor in the with an Aromatase Inhibitor in the
Adjuvant Setting? Adjuvant Setting?
“...Treatment with more than a 5-year course of an aromatase inhibitor should only be administered as part of a clinical trial.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Should an Aromatase Inhibitor be Continued Should an Aromatase Inhibitor be Continued for Longer than 5 years Outside of a Clinical for Longer than 5 years Outside of a Clinical
Trial? Trial?
“...Treatment with more than a 5-year course of an aromatase inhibitor should only be administered as part of a clinical trial.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

In Women Who are Switched from Tamoxifen In Women Who are Switched from Tamoxifen to an Aromatase Inhibitor after 2 to 3 Years, to an Aromatase Inhibitor after 2 to 3 Years,
Should Treatment with the Aromatase Inhibitor Should Treatment with the Aromatase Inhibitor Continue Beyond the 5-Year Point?Continue Beyond the 5-Year Point?
“...Treatment with more than a 5-year course of an aromatase inhibitor should only be administered as part of a clinical trial.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Unresolved Issues: Tamoxifen after Unresolved Issues: Tamoxifen after Aromatase InhibitorsAromatase Inhibitors
Are there any studies that support the use of tamoxifen after an aromatase inhibitor?
“...there are no clinical data at this time that would support the initiation of tamoxifen after a course of therapy with an aromatase inhibitor in the adjuvant setting.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Unresolved Issues: Aromatase Inhibitor Use Unresolved Issues: Aromatase Inhibitor Use in Hormone Receptor-Negative Breast Cancerin Hormone Receptor-Negative Breast Cancer
Is there any role for the aromatase inhibitors in women with hormone receptor-negative breast cancer?
“...women whose tumors are known to be hormone receptor-negative should not receive an aromatase inhibitor as adjuvant therapy.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Unresolved Issues: Use of Aromatase Unresolved Issues: Use of Aromatase Inhibitors in Premenopausal WomenInhibitors in Premenopausal Women
Is it reasonable to use an aromatase inhibitor as initial hormonal therapy in a woman who is premenopausal at diagnosis and who appears to have gone through menopause with chemotherapy?
“...there are serious reasons for concern regarding the use of an aromatase inhibitor in women who are functionally premenopausal.”
Is it reasonable to use an aromatase inhibitor in combination with a luteinizing hormone-releasing hormone agonist or oophorectomy in a woman who is premenopausal at diagnosis?
“Until such evidence is available, aromatase inhibitors should not be used in premenopausal women outside of a clinical trial.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.
Unresolved Issues: Effect of Aromatase Unresolved Issues: Effect of Aromatase Inhibitors on Bone; Musculoskeletal ToxicityInhibitors on Bone; Musculoskeletal Toxicity
What is known about bone and musculoskeletal toxicity associated with the aromatase inhibitors?
“Overall, these three large studies support the conclusion that there is a small but statistically significant increase in arthralgias and/or myalgias with aromatase inhibitors compared with either tamoxifen or placebo.”
Sources: Winer EP et al. J Clin Oncol 2005;23(3):619-29.Hillber B et al. J Clin Oncol 2003;21(21):4042-57.

Unresolved Issues: Effect of Aromatase Unresolved Issues: Effect of Aromatase Inhibitors on Bone; Musculoskeletal ToxicityInhibitors on Bone; Musculoskeletal Toxicity
What is known about bone and musculoskeletal toxicity associated with the aromatase inhibitors?
“...The ASCO bisphosphonate guideline identifies post-menopausal breast cancer patients who receive aromatase inhibitors to be at high risk for osteoporosis and recommends that they have baseline bone mineral density evaluation.”
Sources: Winer EP et al. J Clin Oncol 2005;23(3):619-29.Hillber B et al. J Clin Oncol 2003;21(21):4042-57.

Unresolved Issues: Vascular and Unresolved Issues: Vascular and Gynecological Side Effects of AIGynecological Side Effects of AI
What is known about vascular complications and endometrial cancer in women treated on the adjuvant aromatase inhibitor trials?
“Both anastrozole and exemestane were associated with significantly fewer endometrial cancers, as well as venous and arterial vascular events, when compared with tamoxifen.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Unresolved Issues: Quality of Life Unresolved Issues: Quality of Life with Aromatase Inhibitorswith Aromatase Inhibitors
What is known about overall quality of life and sexual functioning in women on aromatase inhibitors?
“In general there have been no major differences in symptoms influencing quality of life comparing anastrozole with tamoxifen or letrozole with placebo.”
“Anastrozole, exemestane, and letrozole are all well tolerated, with small numbers of women discontinuing treatment in comparison to women on placebo or tamoxifen.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

Unresolved Issues: Tailoring Adjuvant Unresolved Issues: Tailoring Adjuvant Therapy to Individual Patient Risk/BenefitTherapy to Individual Patient Risk/Benefit
To what extent can physicians individualize decisions about adjuvant hormonal therapy? How can physicians better quantify the risks of relapse and/or second primary in women who have taken a course of tamoxifen for either two to three or five years?
“Tailoring decisions about adjuvant hormonal therapy requires an understanding of disease and patient characteristics associated with relapse and toxicity of each approach.”
“Future studies will need to address the differences in disease outcome and toxicity across patient and tumor subtypes.”
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

2004 ASCO Technology Assessment 2004 ASCO Technology Assessment Panel RecommendationsPanel Recommendations
Adjuvant therapy for postmenopausal women with hormone receptor-positive breast cancer should include an aromatase inhibitor in order to lower the risk of tumor recurrence.
Neither optimal timing nor duration of aromatase inhibitor therapy is established.
Aromatase inhibitors are appropriate as initial treatment for women with contraindications to tamoxifen.
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

2004 ASCO Technology Assessment 2004 ASCO Technology Assessment Panel RecommendationsPanel Recommendations
Treatment options include five years of an aromatase inhibitor or sequential therapy of tamoxifen for either 2 to 3 years or 5 years, followed by aromatase inhibitors for 2 to 3 years or 5 years.
Patients intolerant of aromatase inhibitors should receive tamoxifen.
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

2004 ASCO Technology Assessment Panel 2004 ASCO Technology Assessment Panel Unresolved IssuesUnresolved Issues
There are no data on the use of tamoxifen after an aromatase inhibitor in the adjuvant setting.
Women with hormone receptor-negative tumors should not receive adjuvant endocrine therapy.
The role of progesterone receptor and HER2 status in selecting optimal endocrine therapy remains controversial.
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.

2004 ASCO Technology Assessment Panel 2004 ASCO Technology Assessment Panel Unresolved IssuesUnresolved Issues
Aromatase inhibitors are contraindicated in premenopausal women.
There are limited data on the role of aromatase inhibitors in women with treatment-related amenorrhea.
The side-effect profiles of tamoxifen and aromatase inhibitors differ.
The late consequences of aromatase inhibitor therapy, including osteoporosis, are not well characterized.
Source: Winer EP et al. J Clin Oncol 2005;23(3):619-29.