phenylketonuria ( pku )
TRANSCRIPT
PhenylketonuriaPKU
Abbas A. A. Shawka
Medical student
2nd grade
Introduction • Phenylketonuria (PKU), less commonly known as
phenylalanine hydroxylase deficiency.
• the most common inborn error of amino acid metabolism.
• The results of a deficiency of the enzyme phenylalanine hydroxylase (PAH) impairs the body’s ability to metabolize the essential amino acid phenylalanine.
• This leads to accumulation of phenylalanine in body fluids.
• Elevated phenylalanine levels negatively impact cognitive function, and individuals with classic PKU almost always have intellectual disability unless levels are controlled through dietary or pharmacologic treatment.
Signs and symptoms • Fair skin and hair: Resulting from impairment of melanin
synthesis, this is the most characteristic cutaneous manifestation of PKU
• Eczema (including atopic dermatitis)• Light sensitivity• Increased incidence of pyogenic infections• Increased incidence of keratosis pilaris• Decreased number of pigmented nevi• Sclerodermalike plaques• Hair loss• Intellectual disability (the most common finding overall)• Musty or mousy odor• Epilepsy (50%) [2]• Extrapyramidal manifestations (eg, parkinsonism)• Eye abnormalities (eg, hypopigmentation)
Signs and symptoms • About one-third of these children are never able to walk,
and two-thirds cannot talk.
• Seizures, other neurologic abnormalities, decreased pigmentation of hair and skin, and eczema often accompany the mental retardation in untreated children.
•
• Hyperphenylalaninemia and the resultant mental retardation can be avoided by restricting phenylalanine intake early in life.
• Hence, several screening procedures are routinely performed to detect PKU in the immediate postnatal period.
Diagnosis • Screening for PKU involves the following:
• Determination of phenylalanine levels :- The standard amino acid analysis done by means of ion exchange chromatography or tandem mass spectrometry
• The Guthrie test as a bacterial inhibition assay :- Formerly used, but now being replaced by tandem mass spectrometry
• Molecular testing :- is generally unnecessary for a diagnosis of PKU. However, limited genotype-phenotype correlation has been described. In addition, molecular testing is required for prenatal diagnosis.
Management • Dietary treatment• The mainstay of dietary management for patients with PKU
consists of phenylalanine restriction, as well as the use of medical foods to supplement the patient’s intake of other essential amino acids and of vitamins and minerals. Energy and variety are provided by low-protein foods, including fruits, nonstarchy vegetables, and specially ordered low-protein items.
• Pharmacologic management• Patients who have suboptimal dietary treatment may benefit
to some degree from consuming large neutral amino acids, which may block phenylalanine entry into the brain and may also result in a modest lowering of plasma phenylalanine levels.
• Some patients with PKU experience significant lowering of plasma phenylalanine levels after administration of sapropterin, a form of the tetrahydrobiopterin (BH4) cofactor. Patients with some residual enzyme activity are more likely to respond than are patients with no residual enzyme.
Background • Several different classifications have been used in the past
to describe PKU severity.
• Commonly, classic PKU is considered to be present when untreated plasma phenylalanine levels exceed 20 mg/dL(1200 µmol/L) without treatment.
• Lesser degrees of plasma phenylalanine elevation are often referred to as hyperphenylalaninemia.
Pathophysiology • In normal children, less than 50% of the dietary intake of
phenylalanine is necessary for protein synthesis.
• The remainder is converted to tyrosine by the phenylalanine hydroxylase system
• When phenylalanine metabolism is blocked because of a lack of PAH enzyme, shunt pathways come into play, yielding several intermediates that are excreted in large amounts in the urine and in the sweat. These impart a strong musty or mousy odor to affected infants.
• It is believed that excess phenylalanine or its metabolites contribute to the brain damage in PKU.
• Concomitant lack of tyrosine, a precursor of melanin, is responsible for the light color of hair and skin.
Pathophysiology • Although 98% of cases of hyperphenylalaninemia are
attributable to mutate ons in PAH, approximately 2% arise from abnormalities in synthesis or recycling of the cofactor tetrahydrobiopterin.
• Clinical recognition of these variant forms is important because these patients cannot be treated by dietary restriction of phenylalanine alone, but also require supplementation with tetrahydrobiopterin, certain neurotransmitter precursors, and folic acid.
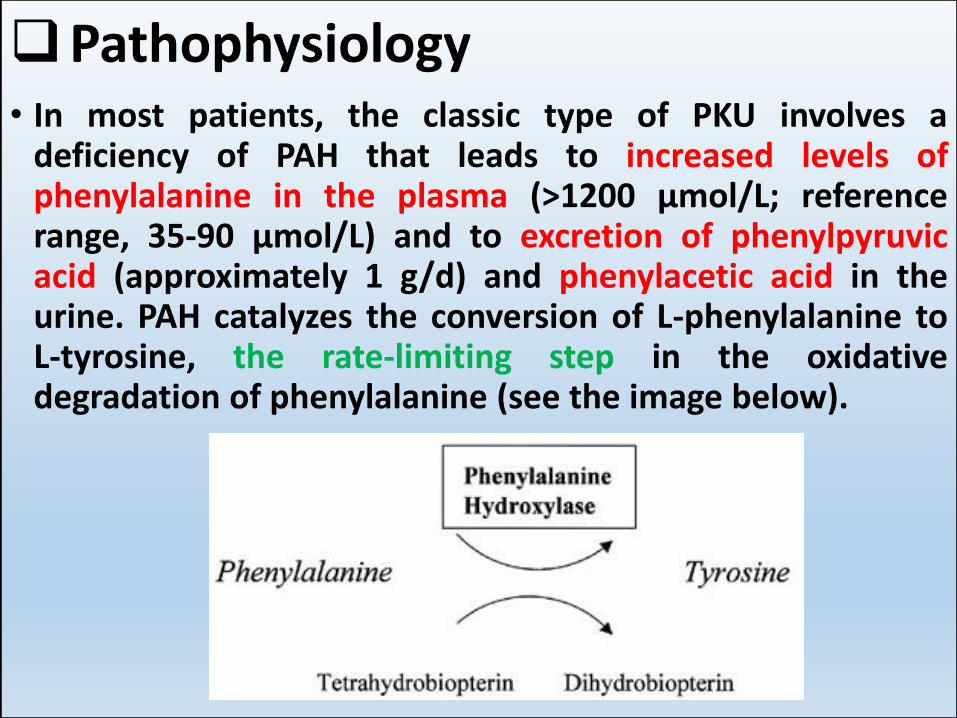
Pathophysiology • In most patients, the classic type of PKU involves a
deficiency of PAH that leads to increased levels of phenylalanine in the plasma (>1200 µmol/L; reference range, 35-90 µmol/L) and to excretion of phenylpyruvicacid (approximately 1 g/d) and phenylacetic acid in the urine. PAH catalyzes the conversion of L-phenylalanine to L-tyrosine, the rate-limiting step in the oxidative degradation of phenylalanine (see the image below).
Pathophysiology • The enzyme PAH crystallizes as a tetramer, with each monomer
consisting of a catalytic domain and a tetramerization domain. Examination of the mutations causing PKU reveals that some of the most frequent mutations are located at the interface of the catalytic and tetramerization domains.
• The mechanism by which elevated phenylalanine levels cause intellectual disability is not known !! , although restriction of dietary phenylalanine ameliorates this effect if initiated within a few weeks of birth. A strong relation between control of blood phenylalanine levels in childhood and intelligence quotient (IQ) is recognized.
• Subtle neuropsychological deficits in children with treated PKU are under investigation. Some investigators have attributed these deficits to small residual neurotransmitter abnormalities (eg, reduced production of neurotransmitters as a result of deficient tyrosine transport across the neuronal cell membranes).
Pathophysiology• PAH requires a nonprotein cofactor termed
tetrahydrobiopterin (BH4).
• A small percentage of children with elevated phenylalanine levels exhibit normal PAH levels but have a deficiency in synthesis or recycling of BH4
• The BH4 cofactor is also required for hydroxylation of tyrosine (a precursor of dopamine) and tryptophan (a precursor of serotonin).
• Thus, individuals with BH4 cofactor deficiency can have additional neurologic problems that are not fully corrected by dietary phenylalanine reduction alone, but often require additional treatments that may not be fully effective.
Pathophysiology • PKU is an autosomal recessive disorder caused by mutations in the
PAH gene, which expresses PAH. This gene is located on 12q23.2, spans about 171 kb, and contains 13 exons.
• More than 500 different mutations in the PAH gene have been identified.
• The PAH gene shows great allelic variation, and pathogenic mutations have been described in all 13 exons of the PAH gene and its flanking region. The mutations can be of various types, including missense mutations (62% of PAH alleles), small or large deletions (13%), splicing defects (11%), silent polymorphisms (6%), nonsense mutations (5%), and insertions (2%). [8]
• The three genes related to biopterin synthesis defects are located at 11q22.3-23.3, 10q22, and 2p13, and the gene for biopterin recyclingdefects is located at 4p15.1-16.1.
• PKU displays a marked genotypic heterogeneity, both within populations and between different populations.
• There is some broad genotype-phenotype correlation (alleles that tend to be severe and alleles that tend to be mild), but unrelated individuals with identical mutations have some degree of variability in phenylalanine tolerance.
Epidemiology • 4 cases per 100,000 individuals in US
• A low incidence is reported in African Americans (1/50,000).
• A high incidence is reported in Turkey (approximately 1 case in 2600 births ).
• PKU is most commonly diagnosed in neonates because of newborn screening programs.
• Women with PKU must restrict their phenylalanine levels during pregnancy to avoid birth defects and intellectual disability in their infants.
• Untreated PKU during pregnancy can result in maternal PKU syndrome, which can variably cause congenital heart defects, brain malformations, microcephaly, and intellectual impairment.
Prognosis • The prognosis for normal intelligence is excellent when
patients have been put on a diet low in phenylalanine in the first month of life, with careful monitoring.
• A quantitative, proportional relation exists between blood phenylalanine levels and IQ for early-treated patients with PKU assessed either during the critical early childhood years (age 0-12 y) or by a lifetime Index of Dietary Control.
• Most untreated individuals with PKU have profound intellectual disability.
• After the discovery of PKU, routine testing of institutionalized patients with intellectual disability identified a 1% incidence of PKU in this group.
• Psychiatric disorders have been frequently described among individuals with PKU, including anxiety, depression, personality disorders, and psychosis.
History • Most individuals with phenylketonuria (PKU) appear
normal at birth. If an affected patient does not undergo newborn screening or has false-negative results (rare), progressive developmental delay is the most common presentation.
• Those same individuals evidence of white matter changes visible on MRI, who ceased dietary treatment in childhood may also have and those patients may experience an intelligence quotient (IQ) decline of 10 points or more.
Complications • The incidence of neuropsychiatric disease in PKU appears
to be higher than in the general population and includes increased risk of depression, anxiety, and inattention, among others.
• It has been shown that these symptoms are exacerbated by high phenylalanine levels and improved by lower phenylalanine levels.
• These findings underscore the need for lifelong diet maintenance
Differential diagnosis • In addition to the conditions listed in the differential
diagnosis, other problems to be considered include the following:
• Liver disease
• Other diseases with mental retardation
• Tyrosinemia type II (Richner-Hanhart syndrome)
Differential Diagnoses
1. Hyperphenylalaninemia
2. Tetrahydrobiopterin Deficiency
3. Tyrosinemia
Approach consideration • A qualified laboratory should measure plasma
phenylalanine and tyrosine.
• A qualified laboratory should perform blood and urine analysis of biopterin and neopterins in order to rule out defects of biopterin synthesis or recycling.
• DNA mutation analysis is adjunctive and may be helpful in some cases, although is not required for diagnosis.
• Prenatal diagnosis is available but rarely used since the disorder is so treatable.
• Prenatal diagnosis can be accomplished by DNA mutation analysis following chorionic villous sampling or amniocentesis
Screening tests • Screening for PKU involves the following:
1. Determination of phenylalanine levels, the standard amino acid analysis done by means of ion exchange chromatography or tandem mass spectrometry
2. The Guthrie test as a bacterial inhibition assay; formerly used, now being replaced by tandem mass spectrometry
• Guthrie test is a screening for phenylketonuria (PKU) used to detect the abnormal presence of phenylalanine metabolites in the blood.
• A small amount of blood is obtained and placed in a medium with a strain of Bacillus subtilis, a bacterium that cannot grow without phenylalanine.
Treatment • Treatment consists of dietary restriction of phenylalanine
often with tyrosine supplementation.
• Stringent phenylalanine-restricted diets have been reported to cause deficiencies of iron, zinc, selenium, and other nutrients and essential amino acids in patients.
• The diet should not be terminated after adolescence, because strong evidence indicates that hyperphenylalaninemia can have detrimental effects in adult patients.
• Surveys have revealed that maternal phenylalanine blood concentrations higher than 1200 µmol/L are associated with maternal PKU syndrome dysmorphic facies, fetal microcephaly, learning difficulties, congenital heart defects, and intrauterine growth retardation.
Treatment • Treatment at any time during pregnancy may reduce the
severity of developmental delay. • Women with PKU should start a phenylalanine-restricted diet
before conception, and those contemplating pregnancy or who are pregnant should be treated in metabolic or PKU clinics.
• Sapropterin is a synthetic form of BH4, the cofactor for the enzyme phenylalanine hydroxylase (PAH).
• PAH hydroxylates phenylalanine through an oxidative reaction to form tyrosine.
• PAH activity is absent or deficient in patients with PKU. • Treatment with BH4 can activate residual PAH, improve normal
oxidative metabolism of phenylalanine, and decrease phenylalanine levels in some patients.
• Sapropterin is indicated to reduce blood phenylalanine levels in patients with hyperphenylalaninemia caused by BH4-responsive PKU.
• It is used in conjunction with a phenylalanine-restricted diet.
Why maternal PKU more severe than classical PKU ?
• Between 75% and 90% of children born to such women ( Have classical PKU ) are mentally retarded and microcephalic, and 15% have congenital heart disease, even though the infants themselves are heterozygotes.
• This syndrome, termed maternal PKU, results from the teratogenic effects of phenylalanine or its metabolites that cross the placenta and affect specific fetal organs during development.
• The presence and severity of the fetal anomalies directly correlate with the maternal phenylalanine level, so it is imperative that maternal dietary restriction of phenylalanine be initiated before conception and continued throughout pregnancy.
Summary
• PKU is an autosomal recessive disorder caused by a lack of the enzyme phenylalanine hydroxylase and a consequent inability to metabolize phenylalanine.
• Clinical features of untreated PKU may include severe mental retardation, seizures, and decreased pigmentation of skin, which can be avoided by restricting the intake of phenylalanine in the diet.
• Female patients with PKU who discontinue dietary treatment can give birth to children with malformations and neurologic impairment resulting from transplacentalpassage of phenylalanine metabolites.