photodynamic therapy: a novel approach in the … · photodynamic therapy: a novel approach in the...
TRANSCRIPT

PHOTODYNAMIC THERAPY: A NOVEL APPROACH IN THE TREATMENT OF AGE RE-LATED MACULAR DEGENERATION
Dr.med. Irene A BarbazettoFlanzer Eye Institute, Columbia University Presbyterian Hospital
635W 165th StreetNew York, New York 10032USA
e-mail: [email protected]
AbstractChoroidal neovascularization secondary to age-related macular degeneration or pathologic myopiacan cause severe loss of central vision and lead tolegal blindness. For many years thermal photoco-agulation has been the preferred treatment for thisdisease, but it is only suitable for a small number ofpatients and may cause additional immediate visualloss after treatment. Photodynamic therapy (PDT)using verteporfin is a new therapeutic approach,which has shown to be beneficial in the treatment ofsuch lesions in recently completed clinical trials. Thetreatment uses an intravenously administeredphotosensitive compound (verteporfin), which isactivated by a non-thermal laser light. The inducedphotochemical reaction within the neovascularvessels leads to secondary occlusion. This mecha-nism allows selective occlusion of the neovascularcomplex while causing only minimal damage tosurrounding retinal tissue. Therefore PDT can safelyreduce the risk of vision loss in patients with CNVsecondary to AMD and may even improve vision inpatients with pathologic myopia as clinical studiesdemonstrated. The basic principle of photodynamictherapy, the results of the two major clinical trials aswell as current treatment guidelines are describe inthis review.IntroductionAge related macular degeneration (AMD) is adegenerative eye disease that can cause severe andirreversible loss of central vision. While most pa-tients with AMD experience only a slow, moderateloss of visual acuity due to atrophic changes of theretina, 10% of patients suffer from a severe andrapidly developing visual loss. According to literatureand clinical experience up to 90% of this significantlyeffected group present with the neovascular form ofAMD 1. This form is characterized by the develop-ment of abnormal blood vessels under the retina,which leak fluid, lipids and blood. Over time theleakage leads to fibrosis of the central retina withloss of photoreceptors and concomitant visiondecline. In North America and Europe this is theleading cause of legal blindness in people over 65years of age 2.
While age related macular degeneration presentswith numerous phenotypes, the etiology has beenonly poorly understood. Therefore any potential
treatment will be limited to the prevention of visualloss, as long as the mechanisms leading to thedevelopment of choroidal neovascularization and theunderlying role of changes in the RPE, Bruch’smembrane and photoreceptors remain unclear.However, the pathological correlate for a poorprognosis can be clearly identified: it is the choroidalneovascularization3. Targeting this structure andthereby treating the severest form of AMD shouldhave highest priority in our therapeutic consider-ations.For many years conventional laser photocoagulationwas the only approved treatment based on thecriteria established by the Macular PhotocoagulationStudy (MPS) 4. The thermal laser photocoagulationleads to a non-selective necrosis of the CNV and alladjacent outer retinal and inner choroidal structures.Many patients with subfoveal lesions experienceimmediate additional visual loss due to the destruc-tive treatment 5. Recurrence after therapy is notuncommon and seen in up to 50% of patients withintwo years. In addition the majority of patients withneovascular AMD do not meet the criteria for lasertreatment because the lesion is too large or not welldefined in angiography 6.Other treatments like radiation and interferontherapy have been investigated and not shown to bebeneficial. Transpupillary Thermal Therapy (TTT)still needs to prove it’s role in the AMD treatmentwith supporting study data from clinical controlledtrials 7,8.Surgical approaches such as submacular surgery,macular rotation and translocation are highly inva-sive and therefore may not be suitable for largepatient collectives of this age group. Also thesetechniques have to be investigated in larger clinicaltrials, to evaluate their true potential 9, 10, 11.Photodynamic therapy (PDT) is a novel therapeuticapproach, which has been recently approved byhealth authorities in various countries for the treat-ment of predominantly classic CNV secondary toAMD. The therapy combines the potential of non-thermal laser light to induce localized chemo-toxicreactions by activating a photosensitizer (light-activable compound) in neovascular tissue 12. Itallows a more selective treatment of the CNV due toa preferential concentration of the photosensitizer inthe target tissue and the possibility in ophthalmology

Journal of the Bombay Ophthalmologists’ Association Vol. 11 No. 116
to direct the light irradiation to the specific targetarea by using a laser light sources 13. The inducedphotochemical reaction differs substantially fromother treatments, as it does not involve any thermalor mechanical damage. Two major cl inical trialsdemonstrated that PDT could safely reduce the riskfor vision loss in patients with subfoveal CNV 14,15,16 .The therapy is currently recommended for patientswith predominantly classic CNV in AMD or CNVsecondary to pathologic myopia.
The principle of photodynamic vascular occlu-sion
Over the last decades photodynamic therapy hasbeen used to treat various types of solid tumors forclinical or investigational purpose. Only recently thedevelopment of specific photosensitive agents suchas verteporfin (benzoporphyrin derivate monoacid A,BPD-MA) 17,18 and the availability of more sophisti-cated light delivery systems have expended thepossible therapeutic use to nononcologic applications13,19,20,21,22,23,24.One of the new applications is age related maculardegeneration, where the subretinal neovascularcomplex is the target structure of photodynamictherapy (PDT). The aim of the treatment is theinactivation of the choroidal neovascular membranewith reduction of size and exudation of fluid underthe surrounding neurosensory retina. This isachieved by the initiation of a photochemical reac-tion. In a two-step procedure first a photosensitizer(light-activable compound) is administered intrave-nously and accumulates in the CNV. In a second stepthe sensitizer is activated by light irradiation of aspecific wavelength that is appropriate for theabsorption by the dye 25 .When the molecules of the photosensitizer areactivated by light, active forms of oxygen and freeradicals are generated, which results in photochemi-cal damage of endothelial cells. The destruction ofthe vascular endothelial cells leads partially to aninstant thrombosis of neovascular structures 26.Secondary vascular repair mechanisms will causeadditional stabilization of the initiated barrier struc-ture and also cause cessation of exudation from theCNV.Here lays the principle difference between PDT andconventional photocoagulation. The applied laserenergy alone is not intensive enough to causeheating or thermal destruction of tissue. The lightenergy is used only to activate chemical processeswithin the dye molecules and the immediate sur-rounding tissue, e.g. surfaces of vascular endothelialcells 27 . The primarily induced pharmacological effectis not visible, even with ophthalmoscopy. In oppositeto the conventional, thermal laser coagulation nonecrosis or even loss of transparency appears on
the retina in the treated area 12. Clinical examinationdoes not allow evaluation of the achieved therapeu-tic effect at this point. The successful occlusion ofthe CNV is clinically invisible during the first 1-2weeks after treatment because outer retinal struc-tures are not damaged. Functional examinationsshowed that recovery of photoreceptor function ispossible and scotoma may disappear a few weeksafter photodynamic therapy 28.Without a doubt, photodynamic intervention does noteliminate the cause of AMD in general but rathertreats the symptoms, especially those pathologicalmechanisms like invasive growth of new vessels andpersistent exudation, which cause severe functionalloss of the central retina.
Current status of photodynamic therapy
The vision stabilizing effects of photodynamictherapy have been investigated in large, randomizedclinical trials (TAP/VIP) 14 ,15,16. International, placebocontrolled studies showed that in the majority ofpatients treated with photodynamic therapy and asensitizer of the porphyrin group the progression ofthe disease could be stopped. The results of thesestudies lead to official approval of the method andthe associated medication. Starting in December1999 PDT was approved in the USA, EuropeanCommunity and Canada as well as in a number ofAsian and Middle Eastern Countries. Meanwhileseveral thousands of patients have been treatedworldwide.
Many ophthalmologists now have the opportunity togain experience with this treatment method them-selves. In the evaluation of photodynamic therapyone must consider not only the different parametersand the specific technical procedures. A number ofother factors such as diagnostic features, carefulselection, care and control of patients are critical tosuccessful application of this form of therapy.
Indications for different forms of lasertherapy
Photodynamic therapy is a laser procedure butophthalmoscopic and angiographic features differsignificantly from the typical features of conventionallaser therapy. Especially the cri teria for indicatingPDT treatment vary from those established forphotocoagulation.Thermal laser therapy is mainly used for subfovealCNV no larger than 2 disc diameters and a visualacuity of 0.1 (20/200). Photodynamic therapy allowsthe treatment of patients with better visual acuityand larger lesion size 29 . In principle the maximumtreatment size for CNV lesions is only limited by the

January - March 2001 17
laser equipment. Though, to achieve best treatmentresults patient should be at an early stage of thedisease with a maximum of photoreceptor function.Clinical and angiographic characteristics
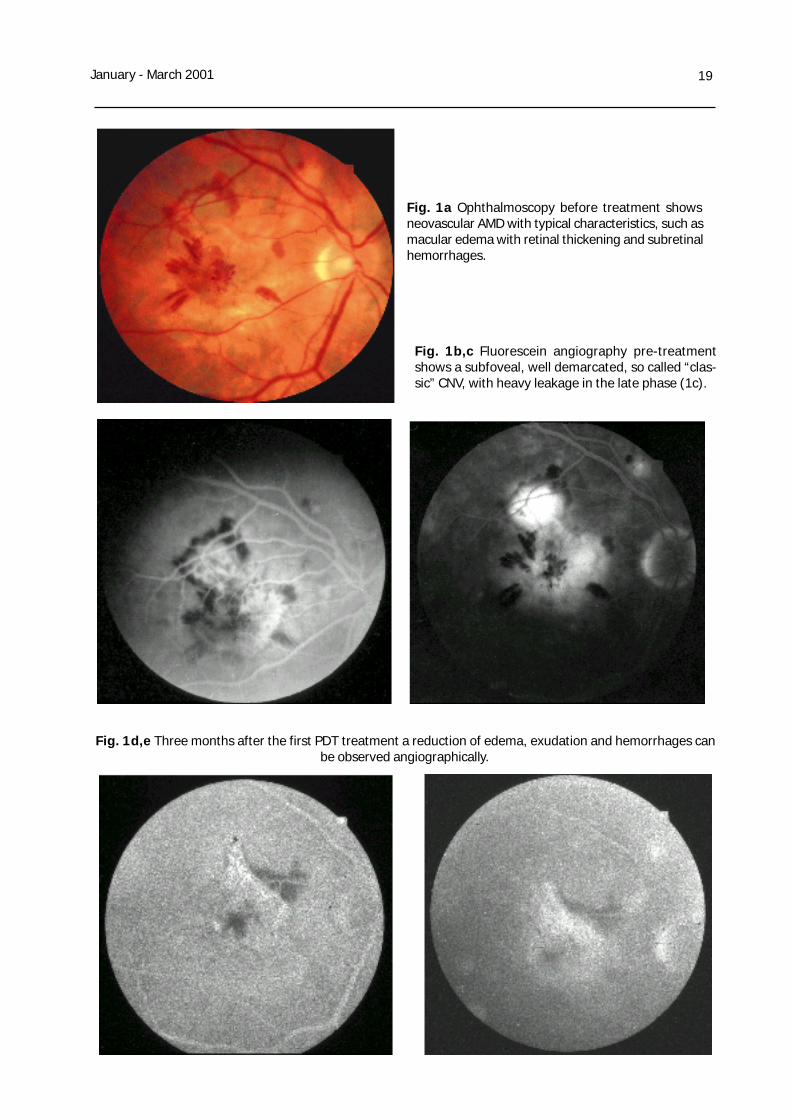
The first example represents a typical patientsuitable for photodynamic therapy. The picture of a57 years old woman shows the central edema of themacular with intraretinal hemorrhages. The imagereveals already atrophic changes underlying andsurrounding the neovascular pathology (Fig. 1a).Fluorescein angiography clearly shows a welldemarcated so called “classic” choroidalneovascularization in the early phase (Fig. 1b) withexcessive leakage overlaying the boundaries in thelate phase (Fig. 1c). The patient reported loss ofreading ability about 4 months ago and complainedof severe metamorphopsia. Visual acuity was 0.3(20/60).Usually no destructive funduscopic changes arevisible in the first couple of weeks after photody-namic therapy. Some patients report a transientdecrease in vision shortly after treatment. Thesevisual disturbances usually can’t be documented orobjectified by visual acuity tests. They develop dueto a transient increase in exudation during the firstdays after treatment and resolve within a few days.A follow up visit during this time is not necessary. Acontrol visit is currently recommended after 3months, based on study results. In case of a benefi-cial therapeutic effect and reduction of edema,exudation and hemorrhages can be observedclinically and angiographically (Fig. 1d,e).
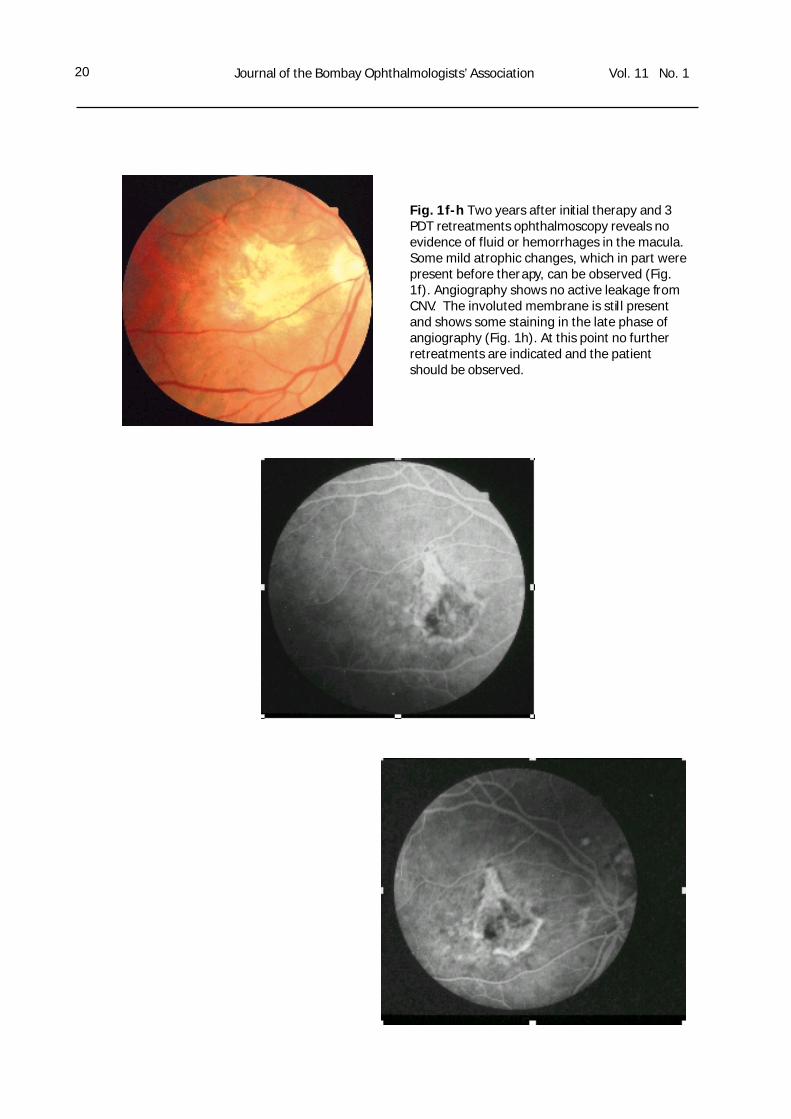
Only a few cases show a lasting therapeutic effectafter one treatment only 30. A slight increase of CNVactivity at the beginning does not prevent or excludea later treatment success. Even 3 months aftertherapy a final decision about the long-term treat-ment effect cannot be made. A better evaluation canbe made based on the 6 and 9 months results. Themajority of patients don’t present with active exuda-tion, lipid deposits or hemorrhages at this point anymore. These patients report a significant reductionor resolution of their metamorphopsia. Central visualacuity usually remains stable within + 2 lines. Thepatient of figure 1 had a visual acuity of 20/50 after4 treatments (Fig. 1f-g).
The interpretation of the angiogram after treatmentrequires some experience, because it deviates fromthe results after conventional photocoagulation. Themain difference is the persistent staining of theinvoluted membrane after therapy, which remainseven years after successful treatment (Fig.1f,g).Signs of involution are stagnation of growth andresolution of active leakage. Angiography threemonths after treatment should show an unchanged,
decreased or only minimal increased size of themembrane (Fig.1c,d). Important is the evaluation ofthe late phase of the angiogram, where a reductionof size and intensity of leakage should be present.Short-term follow-ups with fluorescein and ICGangiography demonstrated that this post-therapyCNV is not a recurrence as seen after photocoagula-tion. Instead this structure represents the residualcentral membrane, many times including the originalfeeder vessel.
The reduction of leakage from the neovascularcomplex in fluorescein angiography is a reliableparameter for the evaluation of treatment success.Cases, which show a good response after therapy,usually present with only minimal persistent leakageafter 2 to 3 treatments. Another positive criteria isthe appearance of a dark pigmented rim due to areactive RPE hyperplasia. This can be observed bothclinically and in the early phase angiogram. Unre-sponsive cases show continuation of leakage and nocessation of membrane growth.
As the therapy continuous the interpretation ofpersistent leakage in late angiography becomesincreasingly difficult. Highly active exudation is easilyobserved with angiography. Minimal residual leakageis more difficult to observe. It is important to takeinto account that minimal, subretinal fibrosis throughinvolution of the fibrovascular membrane causes alate pooling of fluorescein called “staining” and doesnot need additional treatment. Of absolute impor-tance is the comparison of angiographic findings tothe clinical presentation. This allows recognition andlocation of subretinal fibrosis and makes interpretingthe angiogram easier.
Clinical experience shows that minimal residualleakage does not lead to reduction of visual acuity.And also that retreatment has little or no effect onthe persistence of leakage.Therefore at this point one would consider discon-tinuing retreatment while continuing to monitorfunctional and clinical progress closely.
Study Results
TAP-Study
Several clinical studies evaluated the effected ofphotodynamic therapy in the treatment ofneovascularization secondary to age related maculardegeneration. The majority of these clinical studiesused verteporfin as a photosensitizer. Based on aphase III clinical trial called “TAP-Study” (Treatmentof age-related macular degeneration with photody-namic therapy) 14,15 verteporfin became the firstapproved photosensitizer in ophthalmology within

Journal of the Bombay Ophthalmologists’ Association Vol. 11 No. 118
the US, Canada and Europe.In the TAP-Study 609 patients with subfovealchoroidal neovascularization secondary to AMDwere randomly treated with verteporfin or placebo.
Primary inclusion criteria were a visual acuity of 20/200 to 20/40 on the ETDRS chart (early treatmentdiabetic retinopathy study chart) and clinical evi-dence of AMD. Angiographic criteria were subfovealleakage from CNV, which included an obligate partof “classic’ CNV and a facultative part of “occult”CNV. The CNV had to be more than 50% of theentire lesion. The maximum diameter of the lesionto be included was 5400µm (equivalent to 9 discdiameter). Starting December 1996 twenty-twostudy centers in North America and Europe partici-pated in the TAP-Study.Because of the lack of experience with the use ofPDT in ophthalmology, this first clinical trial focusedon patients with advanced stages of the disease,who had no therapeutic alternatives. Therefore it isnot surprising that the mean visual acuity of re-cruited patients was 20/160 and the mean maxi-mum diameter was as large as 4.5 disc diametersat baseline.
TAP-Study: Study procedure
The protocol for the TAP-Study included a standardprotocol, refraction, best corrected visual acuity,
contrast sensitivity (Pelli-Robson), fundus photogra-phy and fluorescein angiography. Follow up visitswere performed every three months. Retreatmentwas performed, if the angiogram showed persis-
tent leakage from CNV. Angiographic inclusioncriteria were verified by an independent photo-graph reading center (The Wilmer Eye Institute,John Hopkins University, Baltimore). Patients weretreated according to a 2/3 randomization: 3 pa-tients were treated with visudyne; two patientsreceived sham treatment (dextrose solution).Verteporfin therapy was applied using 6mgVerteporfin / m2 body surface area. The infusion ofthe sensitizer was administered over a time of 10minutes. Light irradiation (600mW/ m2 at a lightdose of 50J/ m2) was applied 15 minutes afterstart of infusion using a diode laser with an emis-sion wavelength of 692nm. All study personal,investigators, reading center and patients weremasked for the duration of the study.
TAP-Study: Results
The two-year results of the TAP-Study wereannounced in March 2000. The results showed asignificant difference regarding the risk of moder-ate to severe visual loss between the verteporfintreated groups compared to the placebo group.Verteporfin treated patients were also more than
Table 1: Glossary of Terms relevant to PDT (modified from: Schmidt-Erfurth U, Hasan T (2000)Mechanism of Action of Photodynamic Therapy with Verteporfin for the Treatment of Age-Related Macular Degeneration. Surv Ophthalmol 45: 195-214)
Term s r eleva nt to PD T
P h ot oc o agu l ati on
T h erm al m o da li ty to i n du c e str u c tu ra l d am ag e b yab so rp ti on o f h i gh l evel s o f l ig h t en erg y w it hi nb io l og i cal c hro m o ph o res su ch as m el ani n o rh em o gl o b in
P h ot od yn am i c T he ra py (P D T )
A n o n- t herm al m o d ali ty u si n g li g ht , an act ivab l ech ro m o ph o re an d o xyg en to in d uc e a l o cal iz edcy to to x ic r eact io n in vo l v in g ch em i ca l r ad ic al s an do x id at ive p ro ces se s
P h ot os en si ti v ityP h ot oto x i c re acti v i ty o f ti ss u e fo ll o w i n g li gh t exp os u red u e to p ro l o ng ed r eten ti o n of sen si ti zer, e. g. w i th insk in o r in n er o rgan s
P h ot os en si ti zerA l ig h t-act iva bl e c om p o u nd w h ic h pro d u ces hi g h lyto x i c s in g le t o xyg en ra di ca ls up o n ir r ad i atio n w it h l i gh tat i ts sp ec ifi c abs o rpt io n pe ak
P h ot os en si ti zi ng p o ten cyD ete rm in es t he li gh t do s e r eq ui r ed fo r op tim u msp ec if ic ity
T yp e I r eact io nP h ot od yn am i c p ro ces s w i th fo rm a tio n o f cy to to x ic fr eerad ic als
T yp e I I r eacti o nIn teract io n o f exc ite d s en si ti zer m o le cu le s w it h o xyg enl ead in g to th e g en erati on o f s in g le t o xyg en ra di ca ls ,m ajo r m ec ha ni sm o f p h o to ch em i cal ti ss ue da m age
January - March 2001 19
Fig. 1a Ophthalmoscopy before treatment showsneovascular AMD with typical characteristics, such asmacular edema with retinal thickening and subretinalhemorrhages.
Fig. 1b,c Fluorescein angiography pre-treatmentshows a subfoveal, well demarcated, so called “clas-sic” CNV, with heavy leakage in the late phase (1c).
Fig. 1d,e Three months after the first PDT treatment a reduction of edema, exudation and hemorrhages canbe observed angiographically.
Journal of the Bombay Ophthalmologists’ Association Vol. 11 No. 120
Fig. 1f-h Two years after initial therapy and 3PDT retreatments ophthalmoscopy reveals noevidence of fluid or hemorrhages in the macula.Some mild atrophic changes, which in part werepresent before therapy, can be observed (Fig.1f). Angiography shows no active leakage fromCNV. The involuted membrane is still presentand shows some staining in the late phase ofangiography (Fig. 1h). At this point no furtherretreatments are indicated and the patientshould be observed.
January - March 2001 21
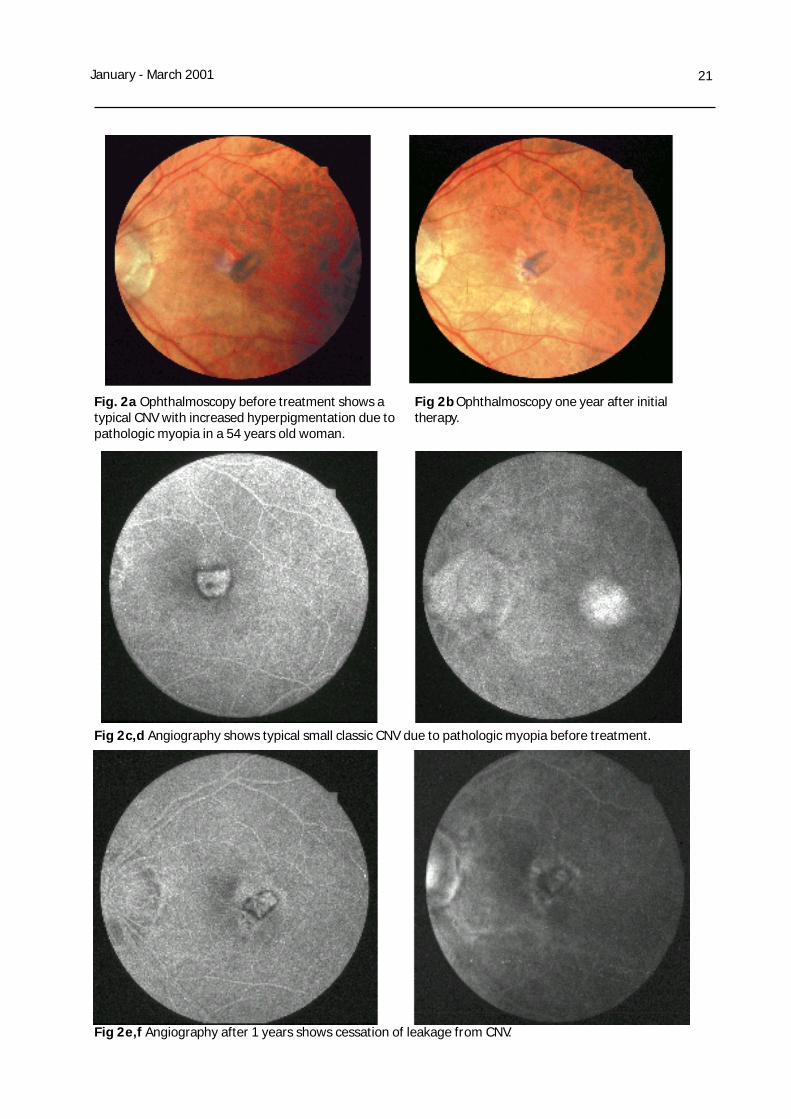
Fig. 2a Ophthalmoscopy before treatment shows atypical CNV with increased hyperpigmentation due topathologic myopia in a 54 years old woman.
Fig 2b Ophthalmoscopy one year after initialtherapy.
Fig 2c,d Angiography shows typical small classic CNV due to pathologic myopia before treatment.
Fig 2e,f Angiography after 1 years shows cessation of leakage from CNV.

January - March 2001 23
twice as likely to stabilize their baseline visual acuity.In addition 13% of verteporfin patients compared to7% of placebo patients had an increase in visualacuity > 1 line. Results of contrast sensitivity testingand angiographic outcomes such as lesion growthand evidence of leakage were in favor of theverteporfin treated group.
TAP-Study: Subgroup analysis
Critical for the understanding of the mechanism ofPDT were the angiographic subgroup analysis of theTAP trial. The results showed that the treatmentbenefit was dependent on the area of classic CNVwith regard to the entire lesion. Lesions with pre-dominately classic CNV responded best to thetherapy and had the greatest chance for long-termvision stabilization. Fifty-nine percent of verteporfintreated patients with predominately classic CNV lostfewer than 15 letters at the month 24 examinationscompared to 31% in the control group 15. Howeverone third of the placebo patients presented with astabilization of visual acuity as well, which should becarefully considered before advising invasive treat-ments for these patients.
The VIP-Study
A second trial using Verteporfin as a photosensitizerwas designed to investigate the efficacy of PDTtreatment for occult membranes as well as smallclassic membranes in AMD, which were not includedin the TAP-Study 16. Overall the entire populationincluded mainly patients with occult CNV withoutclassic components, plus some patients with acomponent of classic CNV and with vision betterthan 20/40. A second part of the VIP trial investi-gated the effect on CNV in pathologic myopia.The one-year results for occult membranes onlywere somehow disappointing: no significant differ-ence was found between the e verteporfin treatedgroup compared to the placebo group. Based onthese results and in combination with the findings ofthe TAP-Study, PDT was recommended and ap-proved for patients with predominately classic CNVonly. However the recently (March 2001) announcedtwo-year results may change those recommenda-tions31:At the 24-month examination, 46% of those patientstreated with Verteporfin therapy lost less than 3lines of vision, or 15 letters, on a standard eye chart(moderate vision loss) compared to 33% of patientson placebo (p=0.023). The difference of 13%between the treated and placebo group was statisti-cally significant and higher than the 4% difference(p=0.51) seen at 12 months. With respect to severevision loss, 70% of Verteporfin treated patients lost
less than 6 lines of vision, or 30 letters, on a stan-dard eye chart versus 53% of patients on placebo, adifference of 17% (p=0.001). Again, this result washigher than the 8% difference (p=0.14) seen at 12months. At the 24-month time point, Verteporfin alsoshowed statistically significant outcomes for othervisual acuity endpoints (e.g. improvement of visualacuity and contrast sensitivity.).
VIP-Study: Subgroup analysis (occult CNV)
In those patients with occult CNV without classiccomponents, who comprised approximately 75% ofpatients enrolled in the VIP-Study, results werefound to be similar to those achieved in the overallpopulation. At 24 months, a difference of 14% wasfound between the treatment and placebo groupswith respect to the avoidance of moderate visionloss (Visudyne 45% vs. placebo 31%; p=0.03).Additionally, an 18% difference between treatmentgroups was found with respect to the avoidance ofsevere vision loss (Visudyne 71% vs. placebo 53%;p=0.004). This compares to differences betweentreatment groups of 4% (p=0.51) and 10% (p=0.07)seen at 12 months for moderate and severe visionlosses, respectively 31.
These subgroup results and currently ongoingstudies, which were designed to optimize treatmentparameters for occult and classic CNV, may changethe recommendations of Verteporfin therapy in AMDin the near future.
While additional subgroup analyses are ongoing,preliminary results suggest that the benefit ofVisudyne therapy is greatest in patients presentingwith relatively small lesions or lower levels of visualacuity (an approximate Snellen equivalent of lessthan 20/50). This subgroup comprised about 70% ofstudy patients with occult CNV without classiccomponents. Visudyne therapy may not be beneficialfor individual patients presenting with both largelesions (>4 disc areas) and good visual acuity(approximately 20/50 or better) according to thepress release by QLT Phototherapeutics Inc. inFebruary 2001. During the two-year period,Visudyne treated patients received an average offive treatments. No new safety concerns werefound.
Photodynamic therapy for pathologic myopia
Also reported were two-year results from a separatePhase IIIb multi-center randomized placebo-controlledstudy involving 120 patients with a similar but distinctcondition referred to as CNV due to pathologic myo-pia. Inclusion criteria were fundus manifestations con-sistent with diagnosis (e.g. lacquer crackers) and ei-

Journal of the Bombay Ophthalmologists’ Association Vol. 11 No. 124
ther a spherical equivalent greater than 6 diopters oran axial length at least equal to 26.5 mm. Study pro-cedure and follow ups were performed according tothe TAP Study protocol.In the primary analysis performed at 12 months, itwas found that patients showed a definite benefit fromVisudyne therapy with respect to the primary endpoint.Specifically, 86% of Visudyne treated patients lost lessthan three lines of vision, or 15 letters, on a standardeye chart, compared to 67% of patients administereda placebo (p=0.01). The percentage difference droppedover the second year from 19% to 7% in favor ofVisudyne (p=0.38). However, the percent of patientswho showed an improvement in vision after treatmentwith Visudyne was much higher than placebo. Fortypercent of Visudyne treated patients gained one ormore lines of vision versus 13% of those treated withplacebo (p=0.003). Furthermore, 12% ofPatients treated with Visudyne experienced an increaseof three or more lines of vision compared to 0% ofthose on placebo (p=0.03) 16,31.
Figure 2a illustrates the typical features of CNV inpathologic myopia including a central edema withoutintraretinal hemorrhages and the absence of degen-erative changes, which are typical for AMD. PDTshows excellent results in these patients. Visualacuity improvements of up to 6 lines have beendescribed especially in younger patients. Severalcases present with regression of the subretinalmembrane after a few treatments. Only (Fig. 2b,e,f). Good prognostic criteria are a hyperplastic,pigmented rim and a small surrounding area ofretinal atrophy, which is presenting as a windowdefect in angiography (Fig. 2c,d). Ophthalmoscopyreveals local scarring with partial fibrosis, whichdepends on the preexisting area of fibrosis 32.Myopic patients need less retreatment in general. Inour experience PDT retreatment should be discontin-ued, when RPE hyperplasia occurs, because this canbe interpreted as a factor for continuing goodremission 33. Nevertheless patients should be moni-tored for any changes as discussed for AMD pa-tients.
Safety issues
PDT is minimally invasive and well tolerated andtherefore can be safely used in large patient collec-tives. This is especially important for elderly pa-tients, who are many times suffering from additionalage related diseases like hypertension or diabetes.The clinical trials confirmed the favorable safetyprofile of PDT with verteporfin as no serious safetyconcerns were identified during the time of treat-ment. The most frequently reported adverse eventsattributed to the treatment were injection site events(15.9 % / TAP Study) and visual disturbances
(22,1% / TAP Study). Extravasation of the drug isthe most serious complication in this group, becauseit can lead to severe skin necrosis if not treatedproperly. Photosensitive reactions were infrequent,occurring in only 3.5 % of study patients. In the TAPStudy 2.5% of patients complained of infusion-related backpain. Allergic reactions were uncommonand less frequent in the verteporfin treated groupcompared to the placebo group (2.0% versus 3.9%).In addition, during the VIP trial for AMD patients, 4%of patients experienced a severe vision decreasewithin 7 days of treatment, which was transient insome of these cases 15.In general patients should be advised to avoid directsunlight for at least 48h (5 days according to FDAregulations). They should were special protectivesunglasses, which shield their eyes from direct sunor halogen light. Because of the characteristic ofverteporfin, patients with decreased liver functionshould be aware of possible prolonged photosensi-tivity. Patients with porphyrinuria or allergies tobenzoporphyrine derivates (e.g. verteporfin) shouldbe excluded from any treatments.
Guidelines for photodynamic therapy
New therapies require the development of cleartreatment guidelines. Especially for a successfultreatment it is necessary to identify the group ofpatients, who will benefit of this therapeutic ap-proach. In the case of photodynamic therapy thecriteria for treatment indication are based on objec-tive diagnostic features. Most important are thenature of the disease itself (choroidalneovascularization secondary to AMD or pathologicmyopia) and angiographic and functional aspects.Other factors such as size and location of the CNVas well as potential risk factors may also play a role.
Angiographic Criteria
Angiographic characteristics are the base for anytreatment decision. Based on the study data itseems that the area covered by so-called “classic”CNV relates to the treatment effect. 100% classiclesions seem to respond best to the treatment.Based on the TAP Study results 14,15, treatment forlesions with at least 50% classic CNV is recom-mended currently. However, the latest results of theVIP Study may change those recommendations andfurther studies will show, in which way the therapycan be further improved.
The Lesion size is determined on mid and latephase angiographic images. The laser device limitsthe maximum treatment spot size. If the lesion

January - March 2001 25
exceeds that diameter, one should only treat theactive part of the lesion. In lesions larger then5400µm, visual recovery seems unlikely and thereason to pursue with the treatment can only bepreservation of the visual filed. Here a comparisonwith the also effected partner eye maybe of use toevaluate potential progression of the membrane andscaring process.
Photodynamic therapy is approved for the treatmentof subfoveal lesion only. Extrafoveal membranesshould be treated with thermal laser according tothe guidelines developed by the MPS Study Group.More controversy is the treatment of juxtafovealCNV, when the leakage already touches upon thefoveal avascular zone. In these cases thermal laseris more likely to compromise central visual acuity.The TAP Study results showed that PDT for recur-rent CNV after laser therapy is less efficient 15. Thisis of special importance considering that up to 70%of juxtafoveal CNVs show recurrence after therapyaccording to the MPS-Study results 6. Also patientswith small, classic, juxtafoveal membranes had amost favourable outcome in the TAP Study. However,as long as a conventional treatment is possiblewithout affecting the foveal avascular zone, no PDTshould be indicated.
Visual acuity is a more subjective treatmentcriteria. Inclusion criteria for the TAP Study were avisual acuity of 20/40 to 20/200 Snellen equivalent.Again patients with visual acuity below 20/200 mightbe treated for preservation of visual field in selectedcases.In our experience, small membranes with poorvisual acuity should be treated once and observedcarefully with functional and angiographic follow upafter 4 to 6 weeks. In case of no functional oranatomical improvement the treatment should bediscontinued and thermal laser intervention shouldbe discussed 4.PDT: Whom not to treat
Currently PDT treatment should not be consideredunder the following circumstances:
1. Chorioretinal anastomosis (or retinal angioma-tous proliferations), which can be seen in 5 -10% of patients with predominantly classic CNV,don’t respond to the treatment. A reason couldbe the increased blood flow through the retinalanastomosis, which may cause a “wash-out”effect of the dye secondary to increased perfu-sion of the neovascular complex.
2. Fibrovascular detachment of the pigmentepithelium. All adverse events with significantvisual loss after treatment (see: results of the
phase III clinical trials) were seen in patientspresenting with this subtype of occultneovascularization. Treating these lesions cancause a rupture of the retinal pigment epithe-lium (RIP-Syndrome) with severe vision loss.
PDT: Future Indications
PDT allows a selective occlusion of vascular tissuethrough secondary alterations of the vascularstructure itself. As long as angiography reveals aclassic choroidal neovascular complex a therapeuticeffect can be achieved. Therefore limiting theapplication of PDT to the treatment of CNV in AMDor pathologic myopia seems not to be sensible.Other patients with choroidal neovascularizationsecondary to RPE scaring, trauma, multifocal chor-oiditis and angioid streaks could potentially benefitfrom the treatment as well. However, regardless ofthe indication angiography remains to be the basisfor any treatment decision.
PDT: Current Benefit and Perspectives
Photodynamic therapy has been approved onlyrecently. To date clinical experience is mainly basedon only two major clinical trials (TAP, VIP) 14,15,16.These studies were the first major trials evaluatingefficacy and safety of PDT in ophthalmology. Withthe rapidly increasing number of treatments newindications and treatment strategies will develop.For example combined therapeutic approaches usingPDT and feeder vessel coagulation or the additionalapplication of antiangiogenetic substances seem tobe promising and are currently evaluated in clinicaltrials.Another important approach is to optimize thetreatment parameters by shortening treatmentintervals as it is investigated in an ongoing Germanmulticenter trail 34. The results of these studies mayhelp us in future to treat patients more efficientlyand with even better visual results.Finally new photosensitizers continue to be devel-oped, which may have improved characteristics forPDT of ocular structures.At this point PDT is recommended for patients withpredominantly classic CNV secondary to AMD orpathologic myopia. However, we are just beginningto explore the broad potential of this exciting newtreatment modal ity.References
1. Bressler SB, Bressler NM, Fine SL et al. (1982)

Journal of the Bombay Ophthalmologists’ Association Vol. 11 No. 126
Natural course of choroidalneovascular membranes within the foveal avascularzone in senile maculardegeneration. Am J Ophthalmol 93:157-163
2. Leibowitz H et al. (1980) The Framingham EyeStudy Monograph; an ophthalmological andepidemiological study of cataract, glaucoma,diabetic retinopathy, macular degeneration,and visual acuity in a general population of2631 adults, 1973-1977. Surv Ophthalmol24:355
3. Guyer DR et al. (1986) Subfoveal choroidalneovascular membranes in age-relatedmacular degeneration. Visual prognosis ineyes with relatively good initial visual acuity.Arch Ophthalmol 104:702-705
4. Macular Photocoagulation Study Group (1991)Argon laser photocoagulation for neovascularmaculopathy: Five-year results from tworandomized clinical trials. Arch Ophthalmol109:1109-1114
5. Macular Photocoagulation Study Group (1994)Visual outcomes after laser photocoagulationfor subfoveal choroidal neovascularizationsecondary to age related macular degenera-tion: the influence of initial lesion size andinitial visual acuity. Arch Ophthalmol 112:480-484
6. Macular Photocoagulation Study Group (1986)Recurrent choroidal neovascularization afterargon laser treatment for neovascularmaculopathy, Arch Ophthalmol 104:503-512
7. Reichel E, Berrocal AM, Ip M, et al (1999)Transpupillary thermotherapy of occultsubfoveal neovascularization in patients withage related macular degeneration. Ophthal-mology 106:1908-1914
8. Mainster MA, Reichel E (2000) TranspupillaryThermotherapy for Age-Related MacularDegeneration: Long-Puklse Photocoagulation,Apoptosis and Heat shock Proteins. OphthalmicSurg Lasers 31:359-373
9. Machemer R, Steinhorst UH (1993) Retinalseparation, retinotomy, and macular reloca-tion: II. A surgical approach for age-relatedmacular degeneration? Graefes Arch Clin ExpOphthalmol Nov;231(11):635-41
10. Bressler NM (1986) Submacular surgery: are
randomized trials necessary? Arch ophthalmol113:1557-1560
11. Eckardt C, Eckardt U, Conrad HG (1999)Macular rotation with and without counter-rotation of the globe in patients with age-related macular degeneration. Graefes ArchClin Exp Ophthalmol Apr;237(4):313-25
12. Schmidt-Erfurth U, Miller JW, Sickenberg M,Bunse A, Laqua H et al. (1998) Photodynamictherapy of subfoveal choroidalneovascularization: clinical and angiographicexamples. Graefe‘s Arch Clin Exp Ophthalmol236:365-374
13. Schmidt-Erfurth U, Hasan T (2000) Mechanismof Action of Photodynamic Therapy withVerteporfin for the Treatment of Age-RelatedMacular Degeneration. Surv Ophthalmol 45:195-214
14. Treatment of age-related macular degenera-tion with photodynamic therapy (TAP) studygroup (1999) Photodynamic therapy ofsubfoveal choroidal neovascularization in age-related macular degeneration with verteporfin.One-year results of 2 randomized clinical trials- TAP report 1. Arch Ophthalmol 117:1329-1345
15. Treatment of age-related macular degenera-tion with photodynamic therapy (TAP) studygroup (2001) Photodynamic Therapy ofSubfoveal Choroidal Neovascularization in Age-Related Macular Degeneration withVerteporfin. Two year results of 2 randomizedclinical trials – TAP Report 2. Arch Ophthalmol119:198-207
16. VIP-Report in print
17. Boyle RW, Dolphin D (1996) Structure andbiodistribution relationships of photodynamicsensitizers. Photochem Photobiol 64:469-85
18. He J, Larkin HE, Li YS, et al (1997) The synthe-sis, photophysical and photobiological proper-ties and in vitro structure-activity relationshipsof a set of silicone phthalocyanine PDT photo-sensitizers. Photochem Photobiol 65:581-6
19. Brown SG (1998) Science, medicine and thefuture. New techniques in laser therapy. BMJ316:754-7
20. Jori G (1990) Factors controlling the selectivity

January - March 2001 27
and efficiency of tumor damage in photody-namic therapy. Lasers Med Sci 5:115-20
21. Levy JG (1995) Photodynamic Therapy.Trends Biotechnol 13:14-8
22. Rowe PM (1998) Photodynamic Therapybegins to shine (news). Lancet 351:1496
23. Schmidt-Erfurth U, Diddens H, Birngruber R,Hasan T (1997) Photodynamic targeting ofhuman retinoblastoma cells using covalentlow-density lipoprotein conjugates. Br JCancer 75(1):54-61
24. Tao J, Sanghera JS, Pelech SI, et al. (1996)Stimulation of stress-activated protein kinaseand p38 HOG1 kinase in murine keratinocytesfollowing photodynamic therapy withbenzoporphyrine derivates. J Biol Chem271:27107-15
25. Schmidt-Erfurth U, Hasan T, Gragoudas E etal. (1994) Vascular targeting in photodynamicocclusion of subretinal vessels.Ophthalmology 101:1953-1961
26. Miller JW, Walsh AW, Kramer M et al. (1995)Photodynamic therapy of experimentalchoroidal neovascularization using lipopro-tein-delivered benzoporphyrin. ArchOphthalmol 113: 810-8
27. Fingar VH, Wilman TJ, Wiehle SA (1992) Therole of microvascular damage in photody-namic therapy: The effect of treatment onvessel constriction, permeability and leuko-cyte adhesion. Cancer Res 52:4914-4921
28. Schmidt-Erfurth U (1999) Indocyanine greenangiography and retinal sensitivity after
photodynamic therapy of subfoveal choroidalneovascularization. Sem Ophthalmol 14:35-44
29. Miller JW, Schmidt-Erfurth U, Sickenberg M etal. (1999) Photodynamic therapy withverteporfin for choroidal neovascularizationcaused by age-related macular degeneration:results of a single treatment in a phase 1 and2 study. Arch Ophthalmol 117: 1161-1173
30. Schmidt-Erfurth U, Miller JW, Sickenberg M etal. (1999) Photodynamic therapy withverteporfin for choroidal neovascularizationcaused by age-related macular degeneration:results of retreatments in a phase 1 and 2study. Arch Ophthalmol 117:1177-1187
31. QLT/ Novartis Press release (February 7th,2001): Favorable visudyne clinical resultsannounced for occult and pathologic myopiapatients. www.visudyne.com
32. Sickenberg M et al. (2000) A preliminarystudy of photodynamic therapy usingverteporfin for choroidal neovascularization inpathologic myopia, ocular histoplasmosissyndrome, angioid streaks and idiopathiccauses. Arch Ophthalmol 118:327-336
33. Miller H, Miller B, Ryan SJ (1986) The role ofretinal pigment epithelium in the involution ofsubretinal neovascularization. InvestOphthalmol Vis Sci 27:1644-1652
34. Schmidt-Erfurth U, Laqua H (2001)OphthalmolPhotodynamische Therapie:Empfehlungen fuer Indikation undBehandlung. Ophthalmologe Feb;98(2):216-9
A proverb is a short sentence based on long experience. Miguel de Cervantes