phys ther.€1996; 76:609-625.lunghouse.com/public/upload/image_14255385477260.pdfphys ther. 1996;...
TRANSCRIPT
1996; 76:609-625.PHYS THER. Nancy D CieslaCare UnitChest Physical Therapy for Patients in the Intensive
http://ptjournal.apta.org/content/76/6/609found online at: The online version of this article, along with updated information and services, can be
Collections
Pulmonary Conditions: Other Airway Clearance
in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
Chest Physical Therapy for Patients in the Intensive Care Unit
Chest physical therapy is used in the intensive care unit (ICU) to minimize pulmonary secretion retention, to maximize oxygenation, and to reexpand atelectatic lung segments. This article reviews how chest physical therapy is used with patients who are critically ill. A brief historical review of the literature is presented. Chest physical therapy treatments applicable to patients in the ICU are discussed. Postural drainage, percussion, vibration, breathing exercises, cough stimulation techniques, and airway suctioning are described in detail, with current references. The importance of patient mobilization is emphasized. The advantages of chest physical therapy over therapeutic bronchoscopy also are discussed. Two patient examples are used to demonstrate the beneficial effects that may be obtained with chest physical therapy. Following the removal of retained secretions, arterial oxygenation and partial pressure of arterial oxygen/fraction of inspired oxygen concen- tration ratios improved, and atelectasis resolved without the negative hemodynamic side effects of therapeutic bronchoscopy. Physical ther- apists trained in the ICU can safely perform chest physical therapy with the majority of patients who are critically ill. [Ciesla ND. Chest physical therapy for patients in the intensive care unit. Phys Ther. 1996; 76:609- 625.1
Key Words: Airway suctioning, Breathing exercises, Bronchial hygiene, Cardiopulmonary, Chest physical
therapy, Cough, Intensive care units, Postural drainage, Thorax.
Nancy D Ciesla
Physical Therapy . Volume 76 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
he purpose of this article is to review the role of chest physical therapy in the intensive care unit (ICU). Treatments are described and critiqued for utility in the ICU. The ICU is a unique
environment, and patients are frequently mechanically ventilated and have multiple invasive lines and drainage tubes that are needed to optimize hemodynamic status. Pulmonary artery, intracranial, and central venous pres- sures are routinely monitored. Chest physical therapy is often necessary due to retained secretions following intubation and immobility. Some physicians advocate volume-controlled mechanical ventilation or mandatory synchronized intermittent ventilation, whereas others recommend pressure support and pressure control modes.' In my experience, most critically ill patients in the ICU tolerate therapy when supplemental oxygen delivery and ventilator adjustments are permitted before or during chest physical therapy to enable them to tolerate turning and mobilization.
Chest physical therapy usually consists of postural drain- age, percussion, vibration, coughing and cough stimula- tion techniques, breathing exercises, suctioning, and patient mobilization. In my experience, mobilization that includes side-to-side turning, transfer training, and ambulation while ventilating the patient with a manual resuscitator bag (MRB) usually minimizes the need for postural drainage with manual techniques. The forced- expiration technique, active cycle of breathing, positive expiratory pressure, autogenic drainage, and use of a flutter valve are newer airway clearance techniques that appear to be beneficial for cooperative patients with chronic sputum-producing diseases such as cystic fibro- is.'-^ The focus of this article is the adult patient in the ICU who is frequently intubated, receiving supplemental oxygen, and unable to follow complex instructions. Breathing exercise techniques, therefore, for patients with less acute chronic sputum-producing disease are not discussed.
Historical Review Studies of chest physical therapy did not occur until the 1950s when Palmer and Sellickhnd Thoren-tudied 352 patients following gastrectomy, hernia repair, and cholecystecomy. These authors demonstrated that pos- tural drainage, percussion and vibration, breathing exer- cises, and coughing were more effective at reducing postoperative pulmonary complications including atel- ectasis and pneumonia than either no treatment or breathing exercises alone.
The study of the effects of chest physical therapy on arterial oxygenation, oxygen consumption, total lung/ thorax compliance, cardiac output, and airway resistance was possible in the 1970s due to the routine use of mechanical ventilation and hemodynamic monitoring. Mackenzie et a17 demonstrated radiological improve- ment without hypoxemia in 47 patients with multiple trauma who received chest physical therapy and were mechanically ventilated with positive end-expiratory pressure (PEEP). The fraction of inspired oxygen con- centration ( F I O ~ ) was not altered during chest physical therapy for these patients. Chest physical therapy improved lung/thorax compliance in 42 patients with atelectasis, pneumonia, lung contusion, and adult respi- ratory distress syndrome (ARDS) who were mechanically ventilated following trauma."rway resistance was unchanged immediately following and for 2 hours after chest physical therapy.8 Mackenzie and c o l l e a g ~ e s ~ ~ ~ concluded, therefore, that chest physical therapy most likely affects the small airways rather than large airways in adult patients with traumatic injuries. Even in patients with unstable vital signs following severe multiple trauma, chest physical therapy has been shown to assist in the resolution of left lower-lobe atelectasis and to improve arterial o~ygenation.~ Investigatorsl0 also have noted that suctioning decreases the saturation of venous oxygen (SVO~) due to increased oxygen consumption when there is an inadequate increase in cardiac output. Klein et all] demonstrated an increase in cardiac output with chest physical therapy, which returned to baseline within 15 minutes of the procedure.
Only two research gro~ps~~.~"ave examined the effect of chest physical therapy on the resolution of acute primary pneumonia. Outcome variables included dura- tion of fever, radiographic clearing, hospital stay, and m~rtality.~z.'"raham and Bradley12 demonstrated no difference in the resolution of pneumonia for 27 patients treated with intermittent positive pressure breathing (IPPB) and chest physical therapy compared with a control group of 27 patients. Britton and col- leagued3 studied 177 patients. Outcomes were the same for the control group, which received advice on deep breathing and coughing, and for the study group, in which postural drainage, manual techniques, and breathing exercises were used.lVn both studies, the majority of patients received antibiotics. Patients with nosocomial pneumonia, however, were not included in either study. Patients who were intubated, patients who had undergone thoracic or upper abdominal surgery,
ND Ciesla, PT, is Clinical Instructor, Department of Physical Therapy, University of Maryland School of Medicine, Baltimore, MD 21201-1595 (USA) ([email protected]). She also was Director of Physical Therapy, R Adams Cowley Shock Trauma Center, University of Maryland Medical Center, at the time this article was written.
610 . Ciesla Physical Therapy . Volume 76 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
and patients with cystic fibrosis, lung abscess, lung Table 1. contusion, and bronchiectasis were also excluded. Indications for Chest Physical Therapya
Clinical examination and data gained from ventilation- perfusion scans, computerized tomography, magnetic resonance imaging, and portable radiographs are used to determine an indication for chest physical therapy. Monitoring in the ICU and pulse oximetry allow contin- uous assessment of patients' vital signs and oxygen saturation before, during, and after treatrnent.14 Unfor- tunately, because studies evaluating treatment tech- niques are limited, clinicians have frequently extrapo- lated the outcomes from studies of patients with chronic disease or patients who are mobile to patients in the ICU who are immobilized and mechanically ventilated.I5-l7 For example, Sutton and colleague^'^ studied eight patients with copious sputum production (five patients with br13nchiectasis, two patients with chronic bronchitis, and one patient with cystic fibrosis) who were not in the ICU and concluded that tracheobronchial clearance is unaffected by adding vibration shaking or percussion to postural drainage with the forced-expiration technique. Early ambulation following gallbladder and cardiac sur- gery has almost eliminated the need for chest physical therapy in these patients unless comorbidities are p r e ~ e n t . ' ~ - ~ ~ Whether the positioning therapy recom- mended by Dean and colleagues'2-a contributes to the resolution of acute atelectasis is unknown. The resolu- tion of acute atelectasis (37%-83%) demonstrated with postural drainage and manual techniques, however, has been shown to be equally as effective as therapeutic bronct~oscopy for the treatment of acute lobar atelectasis and has been studied in the ICU.738.'" The use of chest physical therapy without regard to the patient popula- tion or condition for which it is prescribed, and with no standard definition of treatment components, has led, in my opinion, to numerous negative reports on the efficacy.
Efficacy of Chest Physical Therapy in the Intensive Care Unit The efficacy of chest physical therapy can be determined by a reduction in the incidence of pulmonary infection or an improvement in pulmonary function. The mortal- i ty rate from nosocon~ial pneumonia remains high and ranges from 30% to 60%.26327 Other benefits of chest physical therapy may include decreased duration of mechanical ventilation and prevention of tracheosto- mies--benefits that reduce cost and shorten hospital stays.
The diagnosis of pneumonia in the critical care setting is difficult. The clinical criteria used to diagnose pneumo- nia include the presence of fever, purulent sputum expec~:oration, leukocytosis, a Gram stain showing many polymorphonuclear cells and a single morphologically
Evidence of retained secretions (blood or sputum) not removed by suctioning, coughing, and turning
Radiological evidence of acute atelectasis or infiltrate
Decrease in Pao2 or Spo2 as a result of secretion retention
Prophylactic Use
Acute neurolo ical diseases affectin the innervation of the intercostal, !iaphragmmatic, or aidominal muscles
Smoke inhalation Acute moderate to severe brain iniury
- - - " Pao,=partial pressure of oxygen, arterial: Spo,=oxygen ~aturation measured . .
by pulse oximet~y. Adapted from Ciesla ND. Chest physical therapy for the adult intensive care unit trauma patient. Pt~y\i(al ThmnIrj I%/~r.ticr. 1994;3:99.
distinct organism, and a new pulmonary infiltrate on chest radi~graph.~"-' Patients in the ICU meeting these criteria may respond to chest physical therapy without antimicrobial therapy.'"oshi and colleagues2%tudied 39 patients with trauma (32 patients were intubated) who met the criteria for diagnosis of pneumonia, at which time chest physical therapy was initiated. Within 3 days of chest physical therapy, 31 of the 39 patients showed complete or partial clearing of pulmonary infil- trates and did not require antimicrobial therapy. Over- use of antibiotics can result in toxicity, emergence of resistant strains of bacteria, superinfections, and increased hospital cost^.^^^ For some patients in the ICU, the response to chest physical therapy can differ- entiate the diagnosis of atelectasis from pneumonia and can be used to determine which patients require anti- microbial therapy.26
Although activities in the ICU, including chest physical therapy, have been reported to increase metabolic rate up to 35%, the use of short-acting narcotics usually diminishes any associated hemodynamic The importance of an increase in oxygen consumption and carbon dioxide production, which return to base- line within 15 minutes, is questionable. Therefore, most patients in the ICU who tolerate turning will tolerate the positioning necessary for chest physical therapy.
Indications for Treatment Many authors have described the inappropriate use of chest physical therapy. For example, the American Asso- ciation of Respiratory Care's clinical practice guideline for postural drainagegQonsiders recent spinal surgery, rib fractures, and bronchopleural fistulas to be contra- indications for postural drainage. This approach may be a result of prescribing therapy without a clear-cut indi- cation for treatment (Tab. 1) or of the health care provider not having the training to position the patient with neurologic and orthopedic injuries or the skills to assess the patient's breath sounds, vital signs, and ability to cough. I believe that the patient's level of mobility is
Physical Therapy . Volume 76 . Number 6 . June 1996 Ciesla . 61 1
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

often not considered in the initial patient assessment by non-physical therapists. I have found that patients who adequately clear srcretions with side-to-side turning, mobilization, and suctioning do not need postural drain- age with manual techniques. In my experience, chest physical therapy is frequently administered to both lungs without directing therapy to the anatomic area of lung involvement, is not continued until secretions reach the upper airway, or is not terminated when the patient stops producing secretions. The presence of chronic sputum-producing lung diseases, with the exception of cystic fibrosis, does rlot warrant chest physical therapy unless another indication for treatment (Tab. 1) o r recurrent pneumonia is present.
Chest Physical Therapy Components Mucociliary activity and an effective cough are needed for normal airway c l e a r a n ~ e . ~ ~ . ~ " Viscous secretions, the presence of a cuffed tracheal tube, dehydration, hypox- emia, immobility, and poor humidification of gases impede mucociliary clearance, causing secretion reten- tiotls3(i-v Neurologic conditions and phar~nacologically
induced paralysis affecting the innervation of the glottis or intercostal and abdominal muscles may diminish airflow, resulting in an ineffective cough.:'Vatients in the ICU usually have one or more of these conditions. The treatment techniques used in the ICU are similar to those advocated by ThorenQmore than 40 years ago. Postural drainage, percussion, vibration, coughing, suc- tioning, breathing exercises, patient mobilization, and sometimes manual lung inflation are the usual treat- ments used to renlove secretions. The effectiveness of positioning alol~e to remove retained secretions is unknown. Most patients in the ICU cannot tolerate strenuous exercise programs. However, turning, suction- ing, transfer training, and ambulation (with an MRB, if' necessary) are integral parts of'the chest physical therapy assessment and treatment and may minimize the need for postural drainage using manual t e c h n i q ~ e s . ~ ~ '
Positioning The benefits of positioning versus postural drainage is often difficult to discern. Changes in ventilation- perfusion relationships with positional changes have been d o c ~ r n e n t e d . ~ ~ , ~ ~ Side-to-side turning decreases postoperative fever and improves o ~ y g e n a t i o n . ~ ~ Im- provements in arterial oxygenation after patient posi- tioning, including in patients with adult respiratory distress syndrome (ARDS), have been s h o ~ n . ~ ~ - ~ ' Posi- tioning patients for chest physical therapy with the "good lung down" is associated with improved ventilation-perfusion ratios and oxygenation.U4* Patients with pathology in the superior, and frequently the atelectatic posterior, segments of the lower lobes may have better oxygenation with prone positioning than with supine po~itioning.4"~"
Postural Drainage Postural drainage refers to placing the body in a position that allows gravity to assist drainage of mucus from the lung periphery to the segmental bror~chus and upper airway."" Eleven positions are commonly used to drain 14 lung segments. A detailed description of positioning the patient in the ICU is published elsewhere." Postural drainage enhances peripheral lung clearance, increases functional residual capacity, and accelerates mucus clearanCe.~~).~?.m Postural drainage in conjunction with
mechanical ventilation and PEEP is thought to increase transpulmonary pressure, irllprove ventilation-perfusion ratios, increase lung/thorax compliance of the non- dependent hemithorax, and reduce collateral airway re~istance.5~ Atelectasis may resolve more quickly when the patient is turned with the affected lung ~ipperrnost.~:' Obese patients placed in the 19degree Trendelenburg position after abdominal surgery fbr postural drainage of the lower lobes rarely demonstrate clinically signifi- cant oxygen desaturation."" Transient decreases in oxy- gen saturation measured by pulse oximetry (Spo,) that occur with postural drainage positioning return to base- line within a few minutes. Therefore, most spontane- ously breathing and mechanically ventilated patients tolerate positional changes necessary for segmental pos- tural drainage. Infrequently, an increase in metabolic demand or worsening ventilation-perfusion ratios result in a decrease in oxygenation, insufficient gas flow, or low lung v o l u ~ n e s . ~ ~ ' . ~ ~ Increasing the patient's Fro, or addi- tional ventilator adjustments are therefore required prior to or during therapy. Positioning for postural drainage is usually continued once the patient has responded fivorably to changes in ventilator settings. The duration of postural drainage may range from 15 to 60 minutes, depending on the patient's tolerance to c:hanges in position and the amount of sputum production.
Cooperative, spontaneously breathing patients who can cough effectively may not need postural drainage. John- son et a157 found no difference in the resolution of' atelectasis when postural drainage and percussion were added to deep breathing exercises in patients with acute lobar atelectasis, although the diagnoses and mobility level of the patients studied were not addressed.
Patient Example # 7 The following example demonstrates improvement in both atelectasis and oxygenation after prone positioning and chest physical therapy. The patient was discharged 8 days after treatment was initiated. Although it was ini- tially felt that this patient would require extracorporeal lung assistance to sustain life, after positioning and chest physical therapy this was not necessary.
6 12 . Ciesla Physical Therapy . Volume 76 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
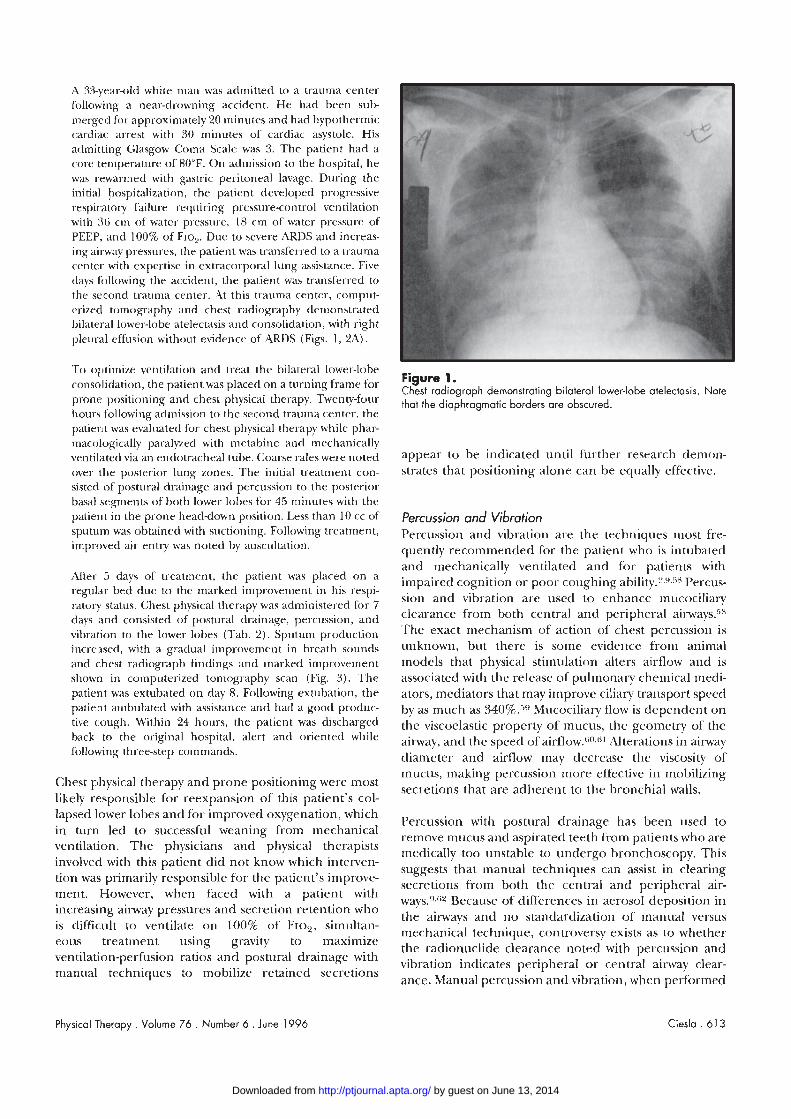
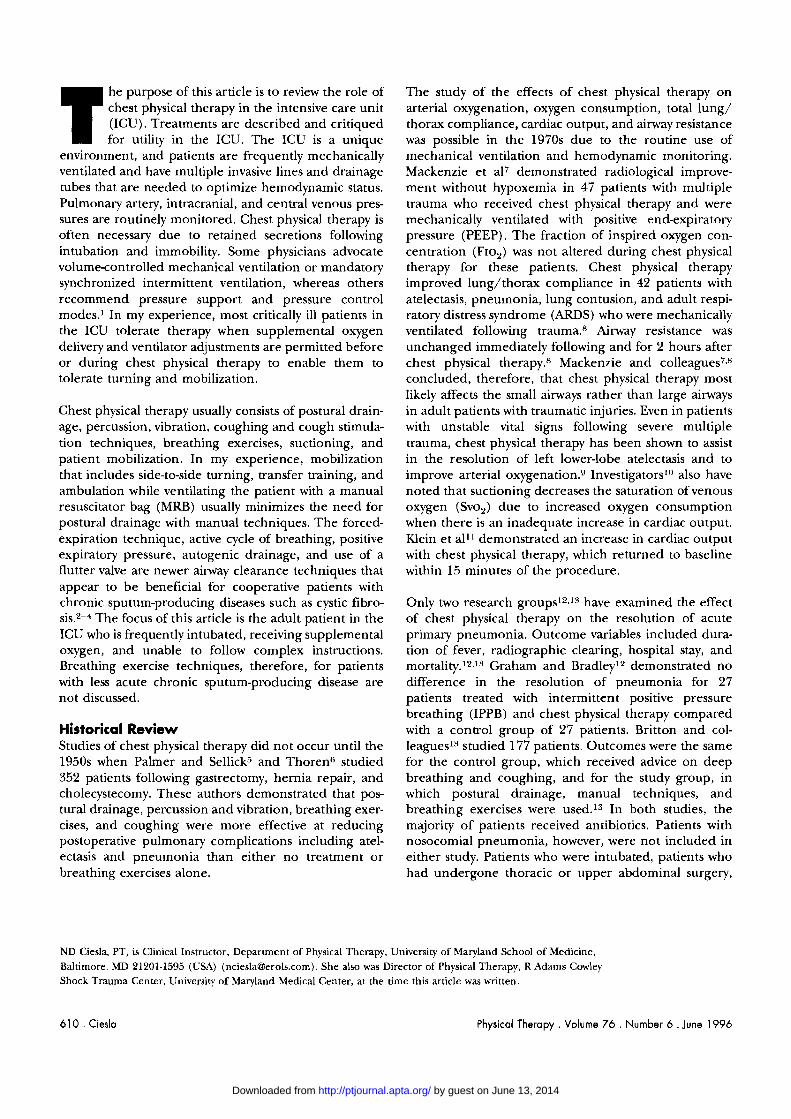
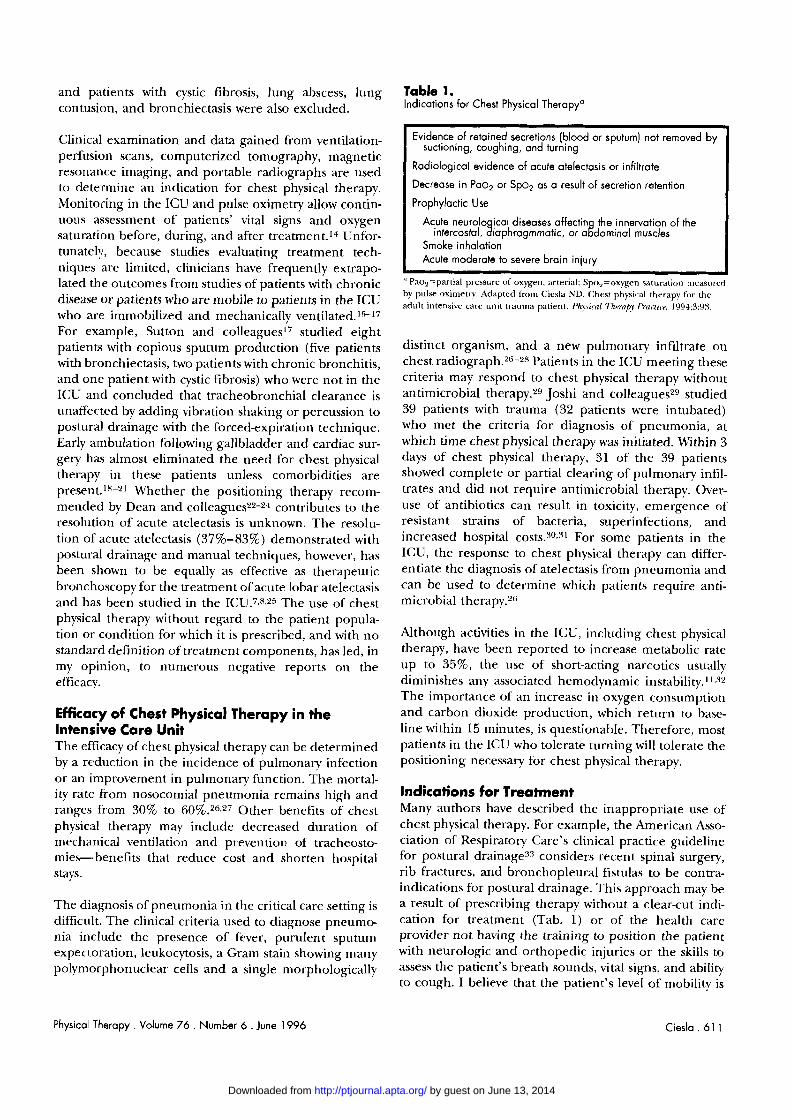
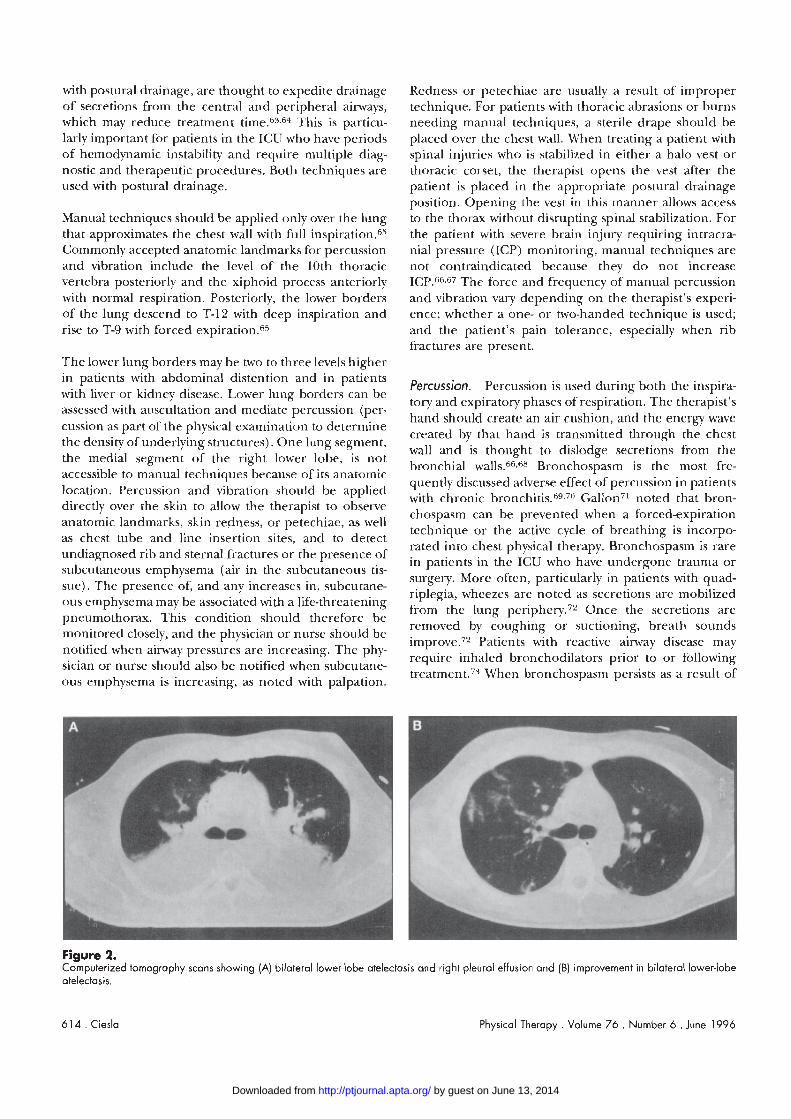
A 33-year-old white man was admitted to a trauma center following a near-drowning accident. He had been sub 1nergec-l for approximately 'LO minutes and had hypother~nic cardiac arrest with 30 rninutes of cardiac asystole. His admitting Glasgow Coma Scak was 3. The patient had a core temperature of 80°F. On admission to the hospital, he was rewal-~ned with gastric pelitoneal lavage. During the initial hospitalization, the patient developed progressive I-espiratory failure requiring pressure-control ventilation with 36 cln of water pressure, 18 cm of water pressure of PEEP, and 100% of Flo,. Due to severe ARDS and increas- ing ailway pressures, the patient was transferred to a trauma center with expertise in extracorporal lung assistance. Five <bays following the accident, the patient was t~ansferred to the second trauma center. At this trauma center, comput- erized tomography and chest radiography demonstrated bilateral lower-lobe atelectasis and consolidation, with right pleura~l effiision without evidence of ARDS (Figs. 1 , 2A).
To optimize ventilation and treat the bilateral lower-lobe consolidation, the patient was placed on a turning frame for Figure 1.
Chest radiograph demonstrating bilateral lower-lobe atelectasis. Note prone positioning and chest physical therapy. Twenty-four +hat the diaphragmatic borders are obscured, hours following admission to the second trauma center, the patient was evaluated for chest physical therapy while phar- macologically paralyzed with metabine and mechanically ventilated via an endotracheal tube. Coarse rales were noted appear to be indicated u~ltil further research demon-
over the posterior lung zones. The initial treatment con- strates that positioning alone can be equally effective. sisted of postural drainage and percussion to the posterior basal segments of both lower lobes for 45 rninutes with the patient in the prone head-down position. Less than 10 cc of Percussjon and Vibration sputum was obtained with suctioning. Following treatment, percussion and vibration are the techniques ]nost fie- improved air ent~y was noted by auscultation. quently recommended for the patient who is intubated
and mechanically ventilated and for patients with After 5 days of treatnlent, the patient was placed on a impaired cognition or poor coughing Percus- regular bed due to the marked improvement in his respi-
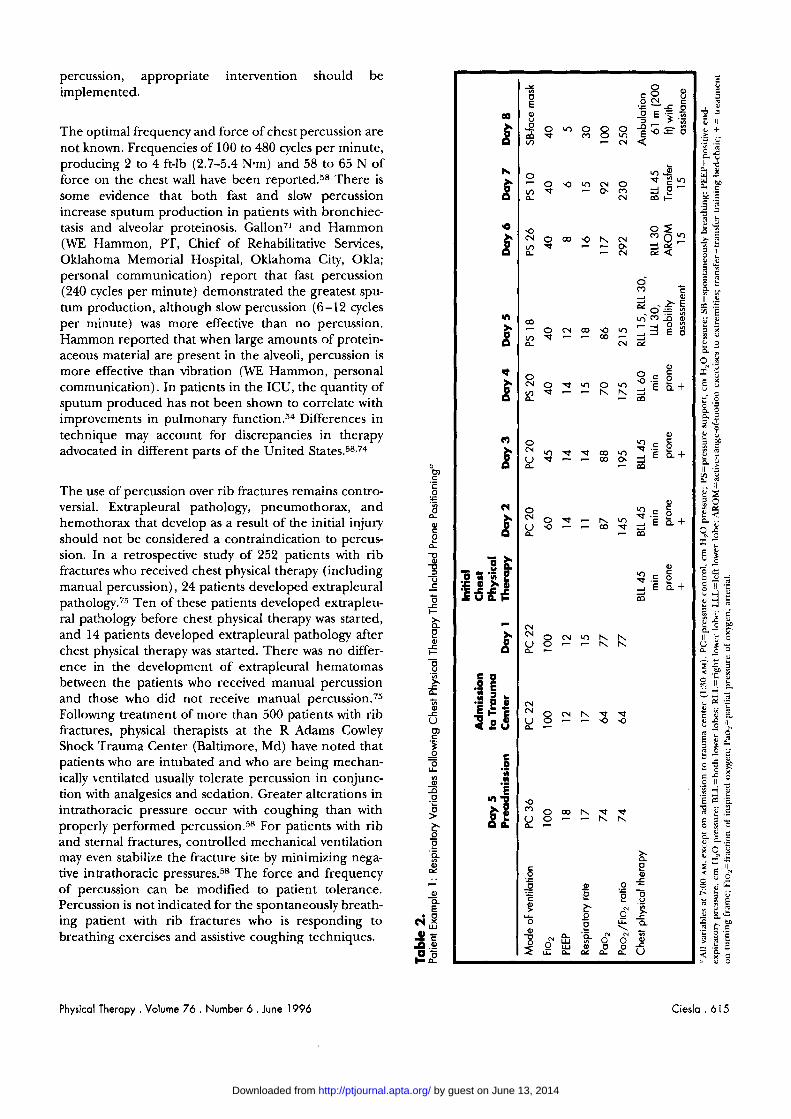
sion and vibration are used to enhance m~icociliary ratory status. Chest physical therapy was administered for 7 days and consisted of postl~ral drainage, percussion, and clearance fi-om both central and peripheral
vibration to the lower lobes (Tab, 2). Sputllm The exact niechanism of action of chest percussion is
incre:ased, with a gradual improvement in breath sounds unknown, bur there is some evidellce froln animal
and chest radiograph findings and marked in~provement models that physical stimulation alters airflow and is shown in computerized tomography scan (Fig. 3). The associated with the release of pulmonary chemical medi- patient was extubated on day 8. Following extubation, the ators, mediators that may improve ciliary trallsport speed patient ambulated with assistance and had a good prodl~c- by as much as 340%,") Mllcociliary flow is dependent on tive cough. Within 24 hours, the patient was discharged the viscoelastic property of the geometry of the back to the original hospital, alert and oriented while airnay, and the speed o fa i r f l ow .~o ,~ Luterations in aiMiay following three-step commands. diameter and airflow may decrease the viscosity of
mucus, making percussion more effective in mobilizing Chest physical therapy and prone positioning were most
secretions that are adherent to the bronchial walls. likely responsible for reexpansion of this patient's col- lapsed lower lobes and for improved oxygenation, which in turn led to successful weaning from ~nechanical ventilalion. The physicians and physical therapists involved with this patient did not know which interven- tion was primarily responsible for the patient's improve- ment. However, when faced with a patient with increasing airway pressures and secretion retention who is difficult to ventilate on 100% of Fro,, simultan- eous treatment using gravity to maximize ventilation-perfusion ratios and postural drainage with manual techniques to mobilize retained secretions
Percussion with postiiral drainage has been used to remove mucus and aspirated teeth from patients who are medically too iinstable to undergo bronchoscopy. This suggests that manual techniques can assist in clearing secretions from both the central and peripheral air- way~."~z Because of differences in aerosol deposition in the airways and no standardization of manual versus mechanical technique, controversy exists as to whether the radionuclide clearance noted with percussion and vibration indicates peripheral o r central ainvay clear- ance. Manual percussion and vibration, when performed
Physical Therapy. Volume 76 . Number 6 . June 1996 Ciesla . 61 3
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
with postural drainage, are thought to expedite drainage of secretions from the central and peripheral airways, which may reduce treatment This is particu- larly important for patients in the ICU who have periods of hernodynamic instability and require multiple diag- nostic and therapeutic procedures. Both techniques are used with postural drainage.
Manual techniques should be applied only over the lung that approximates the chest wall with full in~p i ra t ion .~~ Cornmonly accepted anatomic landmarks for percussion and vibration include the level of the 10th thoracic vertebra posteriorly and the xiphoid process anteriorly with normal respiration. Posteriorly, the lower borders of the lung descend to T-12 with deep inspiration and rise to T-9 with forced e x ~ i r a t i o n . ~ ~
The lower lung borders may be two to three levels higher in patients with abdominal distention and in patients with liver or kidney disease. Lower lung borders can be assessed with auscultation and mediate percussion (per- cussion as part of the physical examination to determine the density of underlying structures). One lung segment, the medial segment of the right lower lobe, is not accessible to manual techniques because of its anatomic location. Percussion and vibration should be applied directly over the skin to allow the therapist to observe anatomic landmarks, skin redness, or petechiae, as well as chest tube and line insertion sites, and to detect undiagnosed rib and sternal fractures or the presence of subcutaneous emphysema (air in the subcutaneous tis- sue). The presence of, and any increases in, subcutane- ous ernphysema may be associated with a life-threatening pneumothorax. This condition should therefore be monitored closely, and the physician or nurse should be notified when airway pressures are increasing. The phy- sician or nurse should also be notified when subcutane- ous emphysema is increasing, as noted with palpation.
Redness or petechiae are usually a result of improper technique. For patients with thoracic abrasions or burns needing manual techniques, a sterile drape should be placed over the chest wall. When treating a patient with spinal injuries who is stabilized in either a halo vest or thoracic corset, the therapist opens the vest after the patient is placed in the appropriate postural drainage position. Opening the vest in this manner allows access to the thorax without disrupting spinal stabilization. For the patient with severe brain injury requiring intracra- nial pressure (ICP) monitoring, manual techniques are not contraindicated because they do not increase ICP.(j"b7 The force and frequency of manual percussion and vibration vary depending on the therapist's experi- ence; whether a one- or two-handed technique is used; and the patient's pain tolerance, especially when rib fractures are present.
Percussion. Percussion is used during both the inspira- tory and expiratory phases of respiration. The therapist's hand should create an air cushion, and the energy wave created by that hand is transmitted through the chest wall and is thought to dislodge secretions from the bronchial ~ a l l s . ~ ~ ~ ~ r o n c h o s p a s m is the most fre- quently discussed adverse effect of percussion in patients with chronic bronchi ti^.^,^^^ Gallon71 noted that bron- chospasm can be prevented when a forced-expiration technique or the active cycle of breathing is incorpo- rated into chest physical therapy. Bronchospasm is rare in patients in the ICU who have undergone trauma or surgery. More often, particularly in patients with quad- riplegia, wheezes are noted as secretions are mobilized from the lung ~eriphery.~' Once the secretions are removed by coughing or suctioning, breath sounds improve.7' Patients with reactive airway disease may require inhaled bronchodilators prior to or following treat~nent.~%en bronchospasm persists as a result of
Figure 2. Computerized tomography scans showing (A) bilateral lower-lobe atelectasis and right pleural effusion and (B) improvement in bilateral lower-lobe atelectasis.
6 14 . Ciesla Physical Therapy . Volume 76 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
percussion, appropriate intervention should be implemented.
The optimal frequency and force of chest percussion are not known. Frequencies of 100 to 480 cycles per minute, producing 2 to 4 ft-lb (2.7-5.4 Nsm) and 58 to 65 N of force 011 the chest wall have been reported.58 There is some evidence that both fast and slow percussion increase sputum production in patients with bronchiec- tasis and alveolar proteinosis. Gallon7l and Hammon (WE Hammon, PT, Chief of Rehabilitative Services, Oklahoma Memorial Hospital, Oklahoma City, Okla; personal communication) report that fast percussion (240 cycles per minute) demonstrated the greatest spu- tum production, although slow percussion (6-12 cycles per minute) was more effective than no percussion. Hammon reported that when large amounts of protein- aceous material are present in the alveoli, percussion is more effective than vibration (WE Hammon, personal communication). In patients in the ICU, the quantity of sputum produced has not been shown to correlate with improvements in pulmonary function.54 Differences in technique may account for discrepancies in therapy advocated in different parts of the United state^.^^^^^
The use of percussion over rib fractures remains contro- versial. Extrapleural pathology, pneumothorax, and hemothorax that develop as a result of the initial injury should not be considered a contraindication to percus sion. I11 a retrospective study of 252 patients with rib fractures who received chest physical therapy (including manual percussion), 24 patients developed extrapleural pathology.75 Ten of these patients developed extrapleu- ral pathology before chest physical therapy was started, and 14 patients developed extrapleural pathology after chest physical therapy was started. There was no differ- ence in the development of extrapleural hematomas between the patients who received manual percussion and those who did not receive manual percu~sion.~" Followng treatment of more than 500 patients with rib fractures, physical therapists at the R Adams Cowley Shock Trauma Center (Baltimore, Md) have noted that patients who are intubated and who are being mechan- ically kentilated usually tolerate percussion in conjunc- tion with analgesics and sedation. Greater alterations in intrathoracic pressure occur with coughing than with properly performed percussion." For patients with rib and sternal fractures, controlled mechanical ventilation may even stabilize the fracture site by minimizing nega- tive intrathoracic pressure^.^^ The force and frequency of percussion can be modified to patient tolerance. Percussion is not indicated for the spontaneously breath- ing patient with rib fractures who is responding to breathing exercises and assistive coughing techniques.
-Y
a $
L
h V I S
N m +
* a
0- m *
C 2 s -& Z .oe
m m o 0 7-1 0 "
N =
* 0
m
") 0 0
- m
0 0
m
- k 2 Z'I'E&! 7 . E 0
-E x z 2 E k + - U P S A
m
r N ~ C " O " 2 I \ b .
8 2 2 I\ I\
C 0 .2 E 121 N
* L C N O " b w w 3 4 2 6 2 2 a 9
C 0 .- H H
-i
2 0
2 5 e .- * 0 - .- 0 f 6
P .= c !? ,o .g ?! f ~2 - g 0 ,
L L a > * .- : s " " s o p Z l r 2 2 2 8 u
7
Physical Therapy . Volume 76 . Number 6 . June 1996 Ciesla . 6 15
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

adult patients in the ICU, use of these devices increases cost, does not reduce staffing requirements, and intro- duces the risk of cross-infection, without documented benefit over manual techniques. Although Radford and colleagues77 advocate mechanical percussion at 25 to 35 Hz, their research using an animal model has not been extended to human subjects. Mechanical devices, used with patients who have chronic pulmonary disease, offer no benefit over forced-expiration techniques com- bined with postural drainage.7R-H0 In patients with pul- monary alveolar proteinosis, manual percussion (180- 270 cycles per minute) was almost twice as effective as mechanical percussion (36 Hz) in removing protein- aceous material from the a l~eol i .~ ' Recently, Hammon and McCaffree" studied the effects of manual percus- sion, saline alone, and a commercially available pneu-
Figure 3. matic percussor on the removal of alveolar material in Chest radiograph showing improvement in right lower-lobe atelectosis. three patients with pulmonary alveolar proteinosis. Mea-
surements of optical density were better with manual percussion than with saline alone or the pneumatic per cuss or.^ Although these results cannot be extrapo-
Vibration. Vibration is a more forceful technique than lated directly to non-saline-filled lungs, they suggest that percussion. At 12 to 20 HZ, vibration is similar to the manual percussion is capable of removing secretions normal beat frequencies of human ciliaa7"he rib cage is from the most distal airnays and alveoli and is more "shaken" during the expiratory phase of respiration. effective than mechanical percussors, vibrators, or saline Some clinicians define vigorous vibration as "rib shak- alone. ing" or "rib springing."I7 Vibration is used with both patients who are spontaneously breathing and patients High-frequency chest compression (HFCC) has recently who are mechanically ventilated. Secretions move into gained popularity as a means of enhancing mucus the upper aimaJ's when vibration is performed during clearance in patients with cystic fibrosis.60 The patient broncho~copy.~~ Forceful vibration is not recommended wears an inflatable vest that covers any lung lobes over rib fractures, which may perforate the pleura and affected with pathology. Frequencies are adjusted to cause a pneumothorax, intrapleural bleeding, or an optimize airflow and to maximize mucus extrapleural hematoma. Some clinicians use a mild clearance. Whitman and colleagues," however, found vibration of light, fast oscillations over rib fractures and no increase in mucus clearance over traditional tech- report no adverse effects. Vibration in patients with niques in six patients who had been mechanically venti- thoracic spinal fractures should be mild and performed lated for 90 to 1,203 days. Percussion was applied for 2 by clinicians trained in chest physical therapy tech- minutes to five lung regions with postural drainage. No niques. S~ontaneously breathing patients who are diffi- indications for treatment were stated other than that the cult to arollse (such as those with acute brain injury) may patients were mechanically ventilated. The practicality of benefit from vibration to erlcourage deep inspiration using HFCC with mechanical ventilation in the JCU is and stimulate a cough. questionable when patients are at high risk for cross-
contamination and access to the thorax is required for In my clirlical experience, dysrhythmias are more likely cardio\rascular monitoring. Further study is needed to to occur as a result of hemodynamic instability associated determine whether HFCC and use of a flutter valve with positiorlal change than as a result of the actual facilitate mucus clearance from central and peripheral manual technique. Percussion and vibration adjacent to for patients who are critically ill and immobile. a cardiac electrode may produce artifacts. After consul- tation with nurses and physicians, electrodes can usually Manual lung /nflation be repositioned or, in rare cases, temporarily discon- Manual lung inflation, which involves disconnecting the nected. The therapist should then closely monitor the patient from the mechanical ventilator and inflating the clinical status of the patient and any alterations in blood lungs with a large tidal volume via an MRB, is a common pressure or heart rate. practice in Great Britain, Canada, and A u ~ t r a l i a . ~ ~ After
the lungs are hyperinflated, the bag is quickly released, Mechanical devices. Mechanical percussors and vibra- producing a high expiratory flow. ~l~~ rates range from tors were introduced in the late 1960s to permit patients 123 to 340 L/rnin, depending on the type of bag used with cystic fibrosis more independence with therapy. For
6 16 . Ciesla Physical Therapy . Volume 7 6 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

and the amount of pressure generated.HVhis tech- nique, often referred to as the "bag-squeezing method," was introduced in the 1960s to prevent pulmonary segmental collapse, reexpand collapsed alveoli, mini- mize the risk of hypoxemia, and stimulate a cough in the patient who is i n t ~ b a t e d . ~ ~ ~ ~ Vibration is sometimes performed during the expiratory phase to enhance mobilization of secretions from the central airways.5H The additional tidal volume delivered, however, most likely reaches the most compliant lung zones and there- fore expands normal rather than collapsed alveoli. Because the patient is removed from the ventilator, lung volumes., PEEP, flow rates, and FIO, are not controlled. Novak and colleaguesHH studied 16 patients with hypox- emic relspiratory failure in a surgical ICU and were unable to demonstrate any improvement (<5 minutes) in gas exchange or pulmonary compliance with hyper- inflations of 40 cm H,O of pressure for 15 to 30 seconds. Flow rates were not documented. Although Jones and colleaguesw found an increase in lung compliance for up to 2 hours in patients without pulmonary disease with bagging and percussion, the same results have been demonstrated with postural drainage, percussion, and vibration in patients with pulmonary p a t h o l ~ g y . ~
Hyperinflation may be hazardous in patients with severe ARDS, because high airway pressures and overdistension of normal alveoli may damage normal lung parenchyma and increase the quantity of lung tissue contributing to the respiratory distress syndrome.'") The effect of hyper- inflation on cerebral perfusion pressure in patients with brain injury who are not medically paralyzed is unknown. Garrard and BullockY1 used ICP monitoring to study 20 patients with brain injuries. Prolonged man- ual hyperinflation with a 2-L rebreathing bag caused a 5-mm Hg increase in ICP in patients who were medically paralyzed and in patients who were not paralyzed. Because cerebral perfusion pressures were not reported, the clinical significance is unknown. Hyperinflation, with a plateau pressure of 80 cm H,O of pressure for 2 to 3 seconds, of 13 patients with severe brain injuries who were paralyzed and well-sedated did not decrease cerebral perfusion p r e s ~ u r e . ~ ~ o r patients who are mechar~ically ventilated, lung hyperinflation with vibra- tion is associated with large fluctuations in cardiotho- racic pressure, and the physiologic benefit is therefore quest i~nable.~?
Cough ing Coughing removes secretions from the trachea, main- stem bronchi, and up to the fourth generation of segmental bronchi." Many patients spontaneously breathing in the ICU are unable to cough effectively because of respiratory muscle weakness, pain, or a decreased level of consciousness. Therapists working in the ICIJ, therefore, should be familiar with cough stim-
ulating and assistance techniques. Compressing the tra- chea just above the sternal notch or huffing (after a maximal inspiration, the patient exhales several times quickly) is indicated when the patient has sufficient neuromuscular function of the respiratory and abdomi- nal muscles. While huffing, the glottis remains open and intrathoracic pressure is lower than with c ~ u g h i n g . ~ ~ When incisional pain is the limiting factor, support of thoracic and abdominal incisions and huffing are indi- cated. Upright positioning also improves cough pres- sures." Coughing is also enhanced by early tracheos- tomy removal, placing an airtight dressing over the tracheostomy stoma, and supporting the stoma site during expiration.
Loss of innervation of the intercostal and abdominal muscles decreases airflow in individuals with quadriple- gia.g"upport and compression of the upper abdomen during expiration facilitates an effective, productive cough. Abdominal support and pressure during exhala- tion are necessary with injuries or diseases that result in abdominal muscle weakness that prohibits effective coughing.
Tracheal Suctioning Tracheal suctioning is an integral component of chest physical therapy for the patient who is intubated. Deep suctioning is necessary for patients who cannot mobilize secretions to the proximal portion of the tracheal tube by coughing or huffing. Withholding suctioning may result in airway occlusion and hyp~xemia ."~ Because upper-airway secretions are most prevalent before and after a change in patient position and during or follow- ing chest physical therapy, the suctioning procedure should be timed with these interventions, particularly in patients who have difficulty tolerating the procedure.
Suctioning is a sterile procedure. Occupational Safety and Health Administration guidelinesYH for exposure to blood and body fluids, therefore, must be followed. Eye protection, a mask for protection from bloody or mucus secretions, and sterile gloves should be worn. As part of the initial assessment, the therapist should evaluate the patient's need for and response to suctioning. Airway suctioning frequently improves breath sounds and may lower airway pressures. When no segmental or lobar pathology is present, suctioning may be adequate and postural drainage with manual techniques may not be indicated. Patients who are intubated and who have a poor cough usually require tracheal suctioning. As with all physical therapy in the ICU, the patient's vital signs should be assessed before, during, and after the proce- dure. Table 3 lists the most frequently cited complica- tions associated with tracheal suctioning and the recom- mended interventions to minimize side effects.
Physical Therapy . Volume 7 6 . Number 6 . June 1996 Ciesla . 617
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

Table 3. Complications of Endotracheal Suctioning
I Complication Recommended Intervention I
I Hypoxemia, death Adequate oxygenation prior to and following the procedure
Limit suctioning to 15-20 so
I Bacterial contamination Sterile technique, changing the suction catheter every 2-4 passes I
Mechanical trauma Polyvinyl chloride catheters with multiple side holes and an end holeb; minimize the number of times the catheter is inserted into the airway; use continuous suctionC
Flow rate of 16 L/mind Negative pressure < 160 mm Hg
Atelectasis Lung inflation prior to and following the procedure
Minimize use of 100% oxygen
" Boutros AR. Arterial blood oxygenation during and after endotracheal . - suctioning in the apneic patient. Awsthesiolo~. 1970;32:114-118. "Jung RE. Gottlieb LS. Comparison of tracheobronchial suction catheters in humans: visualization by fiberoptic bronchoscopy. Chest. 1976;69:179-181. ' Czarnik RE, Stone KS, Everhart C, et al. Differential effects of continuous versus intermittent suction on tracheal tissue. Heart Lung. 1991;20:144-151. "DePew CL, Noll ML. In-line closedaystem suctioning: a research analysis. Dimmsionc (f f;ri/irrrl Care Nursing 1993;13:73-83.
Precautions and contraindications. Suctioning through an artificial airway of a patient with adequate oxygen- ation and stable vital signs has relatively few contraindi- cations. Prior to suctioning the patient with unstable vital signs or a low Spo, , the benefit of suctioning versus the risk of causing additional arrhythmias or desatura- tion should be weighed in consultation with medical and nursing staff. When coughing results from mechanical stimulation of the trachea caused by heavy ventilator tubing or a malpositioned tracheal tube, suctioning is not indicated. Appropriate treatment is to remove the stimulus triggering the coughing. For patients who have retained secretions, are unable to cough effectively, and have difficulty tolerating suctioning, suctioning should be timed with chest physical therapy to minimize the risk of hypoxemia.
Nasotracheal suctioning (suctioning through the nose into the trachea without an artificial airway in place) is contraindicated in the presence of stridor because of the increased risk of mechanical trauma to an edematous airway." Because the catheter may enter the brain, nasotracheal suctioning with basilar skull fracture, facial fractures, and known or suspected cerebrospinal fluid leaks is also contraindicated." Nasotracheal suctioning may result in apnea, laryngospasm, bronchospasm, and severe cardiac arrythmia~.~7 Nasotracheal suctioning is recommended only when vigorous chest physical ther- apy, including prolonged postural drainage, cough stim-
Table 4. Recommended Features of Suction Catheters
Size less than one half the Usually 12-14 French for adults diameter of the airway with a 7- to 9-mm endotracheal
tubeo; reduces airwa occlusion and suction-induced iypoxemia
Material PolPinylchlorideb
Tip design Straight-for routine use Coude-when it i s necessary to
intubate the leh main-stem b r o n c h ~ s ~ , ~
Side holes Two or more to minimize tracheal mucosal damage and optimize secretion removale
" DePew CL, Noll ML. In-line closed-system suctioning: a research analysis. Dimensions of Critical Care Nuwing. 1993;13:73-83. "ubota Y, Magaribuchi T, Ohara M, et al. Evaluation of selective bronchial suctioning in the adult. CKL Care Med. 1980;8:748-749. "Panacek E . Albertson TE, Rutherford WF, et al. Selective bronchial suctioning in the adult using a curved-tip catheter with a guide mark. Cnt Care Med. 1989;8:748-749. "Hart TP, Mahutte CK. Evaluation of a closed-system, directional-tip suction catheter. Respir Care. 1992;37:1260-1265. 'Jung RE, Gottlieb LS. Comparison of tracheobronchial suction catheters in humans: visualization by fiberoptic bronchoscopy. Chest. 1976;69:179-181.
ulation techniques, and suctioning of the oropharynx, is ineffective and the medical team does not plan to intubate the patient.
Systems. Suctioning can be performed using either an open or closed system. When using an open system, the patient is disconnected from the mechanical ventilator and suctioned using a conventional catheter. The patient remains on the mechanical ventilator for closed- system suctioning. Closed-system suctioning is accom- plished by using either a "port adapter" or the more recently introduced in-line s u c t i ~ n i n g . ~ ~ ~ ~ ~ ~ The recommended features of suction catheters are listed in Table 4.
Prior to suctioning a patient who is mechanically venti- lated, the therapist should be aware of the washout time (the time necessary for the gas volume in the ventilator circuit to be replaced with gases at the higher FIO,) of the ventilator in use.'Ol With current technology, the washout time may be as little as three to five breaths for ventilators such as the SERVO 900C.'02
Interventions fbr minimizing hypoxemia. The harmful effects of tracheal suctioning include hypoxia, cardiac arrhythmias, and death." Accepted methods for mini- mizing suction-induced oxygen desaturation include use of a port adapter, lung hyperinflation, preoxygenation, and in-line suctioning. Placing a valve or port adapter over the end of the endotracheal or tracheal tube allows ventilation during the procedure, maintains PEEP, and preserves functional residual capacity. The result is improved oxygenation during s u c t i ~ n i n g . ~ ~ ~ ~ ~ W s i n g the
6 1 8 . Ciesla Physical Therapy . Volume 76 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

adapter may minimize the need for preoxygenation, therefore eliminating the potential hazards of exposure to 100% oxygen."J4 A port adapter is recommended for patients who are mechanically ventilated patients and require a PEEP of > 10 cm H 2 0 and for patients who are at high risk for suction-induced arrhythmias and hypo~ernia .~~*~' )"
Proponents of in-line suctioning report less oxygen desaturation than with an open system; however, the same results have been achieved by using a port adapt- er.9!',100,104.106 Clinical impressions of in-line suctioning that need to be substantiated with further research include the following: (1) The catheter is more difficult to maneuver, (2) the additional weight of the catheter may increase tracheal damage, (3) higher inspiratory flow rates may be required, and (4) airway pressure may drop as a result with suctioning and intermittent man- datory ventilation (IMV) .100.104,106
Preoxygenation is the most commonly used method for preventing oxygen d e ~ a t u r a t i o n . ~ ~ ~ . ~ ~ Y h e mechanical ventilator or an MRB is used to inflate the lungs and increase the inspired oxygen concentration prior to suctioni~ng. For patients who are mechanically ventilated, the ventilator is preferred over the MRB. Minute venti- lation, PEEP, and FIO, are all controlled, and there are no ~ari~ations in lung volume, flow rates, and pressure based on the clinician's bagging t e ~ h n i q u e . l ~ ~ ~ ~ l ~ When using tlhe ventilator, the second clinician who may be required when using an MRB is not needed. When using an MRB, the FIO, varies from 33% to loo%, depending on flow rate, minute ventilation, and whether the bag has a r e ~ e r v o i r . l l l . ~ ~ ~
The miajority of studies evaluating tracheal suctioning have compared the effects in patients who had cardiac surgery.10i.10"111~113 Although hyperoxygenation is com- mon practice, it may not be necessary for all patients. Based on my clinical experience, I believe that suction- induced hypoxemia may not be as significant in patients such as8 young patients with traumatic injuries but with- out cardiac disease. A suctioning protocol that encour- ages clinical judgment is recommended.l14 When patients are hyperoxygenated prior to or during chest physical therapy, the effect of chest physical therapy on Sao,, Spo,, or partial pressure of arterial oxygen (Pao,) may be masked.
The most important indicators as to whether a patient will desaturate with suctioning are the resting Spo, and the resting Pao,. Depending on the patient being suc- tioned, hyperoxygenation is recommended when the Spo, is less than 90% (95% for high-risk patients). Hyperoxygenation also is recommended when the Spo, drops below 85% during suctioning and does not return
to baseline within 10 to 15 seconds and when the resting Pao, is below 85 mm Hg.
Saline installation. Saline instillation is commonly used before and during tracheal suctioning to "loosen" secre- tions.ll"aline instilled through a tracheal or endotra- cheal tube is not likely to reach the peripheral airways, where secretions are most prevalent."s To be effective, the saline must pass through several generations of segmental bronchi and reach the terminal bronchioles and alveoli. Patients should, however, receive adequate systemic hydration and airway humidification rather than saline i n ~ t i l l a t i o n . ~ ~ ~ , l l ~ Patients with copious puru- lent secretions (eg, bronchiectasis) may require saline installation to remove viscid secretions from the upper airways and tracheal tube.
Breathing Exercises Once extubated, alert, and cooperative, the patient in the ICU may benefit from breathing exercises to increase tidal volume, improve thoracic-cage mobility, increase inspiratory capacity, enhance cough efficacy, and assist in removal of ~ecretions.5~ Breathing exercises are indicated in the ICU setting for patients with neuro- muscular disease or injury affecting the respiratory mus- cles. Breathing exercises also are used when thoracic excursion is decreased as a result of retained secretions or pain or when a patient is immobile following surgery. Breathing exercises are not indicated during mechanical ventilation but may be used during weaning from mechanical ventilation.
There are several types of breathing exercises. Diaphrag- matic breathing and lateral costal and segmental costal expansion exercises are used most often postoperative- ly?l Use of a flutter valve, the forced-expiration tech- nique-more recently referred to as the active cycle of breathing (huffing at various lung volumes interspersed with diaphragmatic breathing)-and autogenic drain- age (using a sequence of breathing maneuvers at various lung volumes to optimize airflow within multiple gener- ations of bronchi) are beneficial in patients with cystic fibrosis, although the efficacy of these procedures after surgery has not been determined.5"11i Inspiratory mus- cle training and resistive diaphragmatic breathing exer- cises may be beneficial while weaning the patient with quadriplegia or chronic obstructive pulmonary disease from the ~ e n t i l a t o r . ~ ~ - ~ 2 ~ Incentive spirometry is com- monly used postoperatively, although it is no more advantageous or costeffective than instruction in deep breathing and coughing.I2l Following coronary artery bypass or gall-bladder surgely, breathing exercises offer no advantage over early patient m0bilization.~*-21
Physical Therapy. Volume 76 . Number 6 .June 1996 Ciesla . 6 19
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
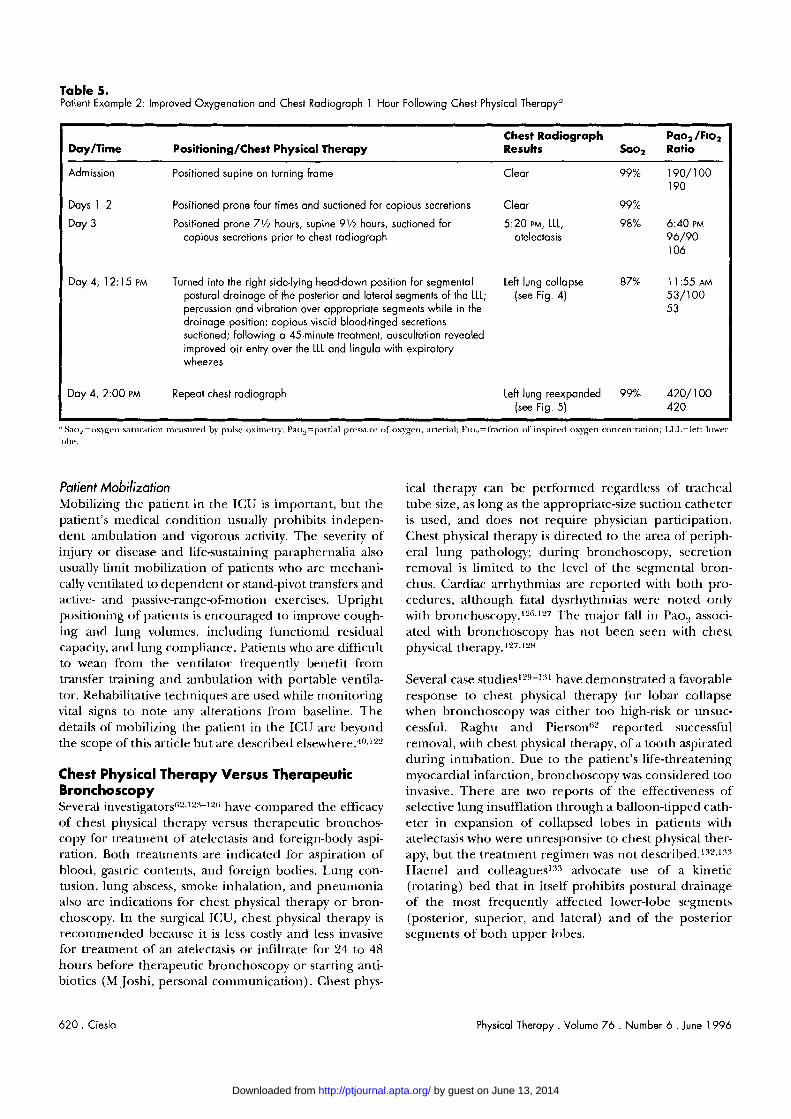
Table 5. Patient Example 2: Improved Oxygenation and Chest Radiograph 1 Hour Following Chest Physical Therapya
- - - - - -
Day/Time Positioning/Chest Physical Therapy
--- - - - --
Chest Radiograph Pao, /FIo, Results Sao, Ratio
- ---
Admission Positioned supine on turning frame Clear
Days 1-2 Positioned prone four times and suctioned for copious secretions Clear
Day 3 Positioned prone 7 % hours, supine 9'12 hours, suctioned for 5:20 PM, LLL, copious secretions prior to chest radiograph atelectasis
Day 4, 12: 15 PM Turned into the right sidelying head-down position for segmental Leh lung collapse postural drainage of the posterior and loterol segments of the LLL; (see Fig. 4) percussion and vibration over appropriate segments while in the drainage position; copious viscid blood-tinged secretions suctioned; following a 45-minute treatment, auscultation revealed improved air entry over the LLL and lingula with expiratory wheezes
I Day 4, 2:00 PM Repeat chest radiograph Leh lung reexpanded 99% 420/100 (see Fig. 5) 420 I
"Sao,=oxvgr~~ ~ a t u ~ a r i o n rnc;~cured by pulsr oxinretry; Pat,,=partial pressure of oxygcrl, arterial; F~o,=fractiotr 01' inspirrcl oxygen concentration; LL.L=left lowel- Iohc.
Patient Mobilization Mobilizirig the patient in the ICU is important, but the patient's medical condition usually prohibits indepen- dent ambulation and vigorous activity. The severity of injury or disease and life-sustaining paraphernalia also usually lirnit n~obilization of patients who are mechani- cally ventilated to dependent o r stand-pivot transfers and active- and passive-range-of-motion exercises. Upright positioning of patients is encouraged to improve cough- ing and lung volumes, including functional residual capacity, and lung compliance. Patients who are difficult to wean fi-om the ventilator frequently benefit from transfer training and ambulation with portable ventila- tor. Rehabilitative techniques are used while monitoring vital signs to note any alterations from baseline. The details of n~obilizing the patient in the ICU are beyond the scope of this article but are described el~ewhere.~~',]2'
Chest Physical Therapy Versus Therapeutic Bronchoscopy Several inve~tigators~'.""-'2(~ have compared the efficacy of chest physical therapy versus therapeutic bronchos- copy for treatment of' atelectasis and foreign-body aspi- ration. Both treatments are indicated for aspiration of blood, gastric contents, and foreign bodies. Lung con- tusion, lung abscess, smoke inhalation, and pneumonia also are indications for chest physical therapy or bron- choscopy. In the surgical ICU, chest physical therapy is recommended because it is less costly and less invasive for treatment of an atelectasis or infiltrate for 24 to 48 hours before therapeutic bronchoscopy or starting anti- biotics (M Joshi, personal communication). Chest phys-
ical therapy can be performed regardless of tracheal tube size, as long as the appropriate-size suctio~l catheter is used, and does not require physician participation. Chest physical therapy is directed to the area of periph- eral lung pathology; during bronchoscopy, secretion removal is limited to the level of the segmental bron- chus. Cardiac arrhythmias are reported with both pro- cedures, although fatal dysrhythrnias were noted only with bron~hoscopy.'"~~27 The major fall in Pao, associ- ated with bronchoscopy has riot been seen with chest physical therapy. l f l , " H
Several case studie~'"~-': 'l have demonstrated a favorable response to chest physical therapy for lobar collapse when bronchoscopy was either too high-risk or unsuc- cessful. Raghu and Piersoliw reported successful removal, with chest physical therapy, of a tooth aspirated during intubation. Due to the patient's life-threatening myocardial infarction, bronchoscopy was considered too invasive. There are two reports of the effectiveness of selective lung insufflation through a balloon-tipped cath- eter in expansion of collapsed lobes in patients with atelectasis who were unresponsive to chest physical ther- apy, but the treatment regimen was not Haenel and col leag~es ' :~~ advocate use of a kinetic (rotating) bed that in itself prohibits postural drainage of the most frequently affected lower-lobe segments (posterior, superior, and lateral) and of the posterior segments of both upper lobes.
620 . Ciesla Physical Therapy . Volume 76 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
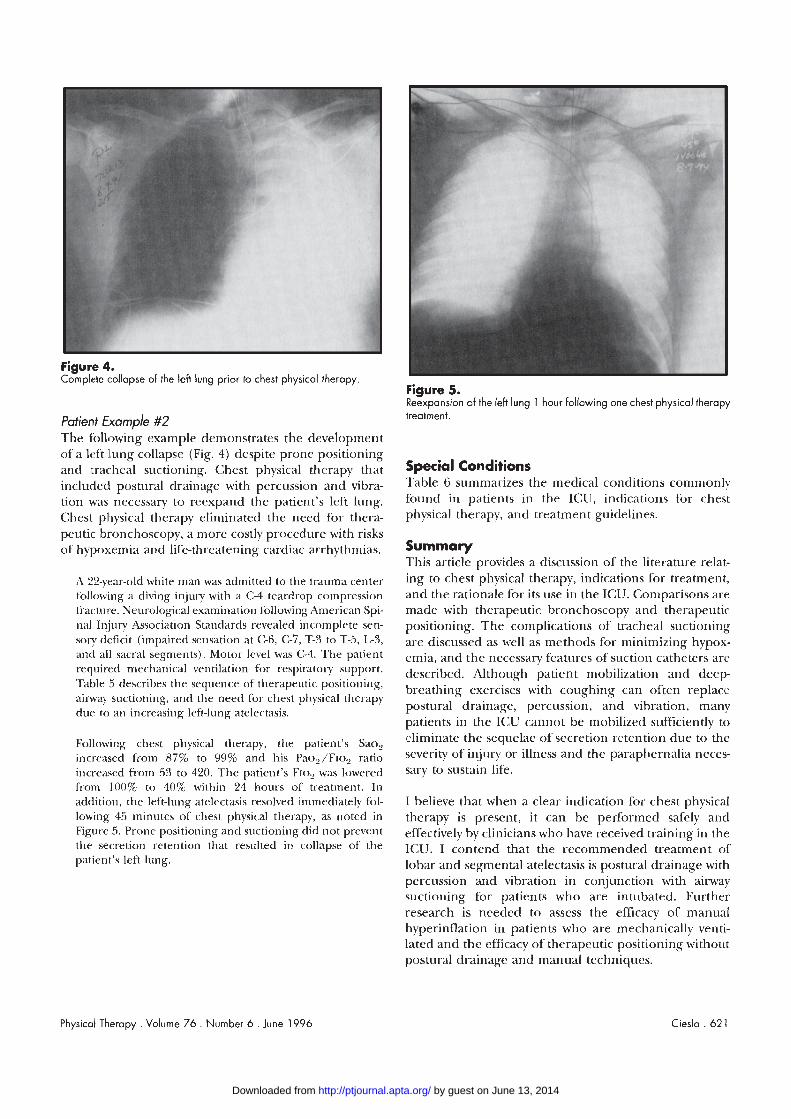
Figure 4. Complete collapse of the left lung prior to chest physical therapy
Patient Example #2 The following example demonstrates the development of a left :lung collapse (Fig. 4) despite prone positioning and tracheal suctioning. Chest physical therapy that includedl postural drainage with percussion and vibra- tion was necessary to reexpand the patient's left lung. Chest pllysical therapy eliminated the need for thera- peutic bronchoscopy, a more costly procedure with risks of hypoxemia and life-threatening cardiac arrhythmias.
A 22-year-old white man was admitted to the trauma center fbllowing a diving injury with a C-4 teardrop compression ti-acturr. Neut-ological examination following American Spi- nal Injury Association Standards revealed incomplete sen- sory deficit (impaired sensation at C-6, C-7, T-3 to T-5, L-3, and a111 sacral segments). Motor level was C-4. The patient required mechanical ventilation for respiratory support. 'Table 5 describes the sequence of therapeutic positioning, airway siictioning, and the need for chest physical therapy due to an increasing left-lung atelectasis.
Following chest physical therapy, the patient's Sao, increased from 87% to 99% and his Pao,/Flo, ratio increased from 53 to 420. The patient's FIO, was lowered from 100% to 40% within 24 hours of treatment. In addition, the left-lung atelectasis resolved immediately fol- lowing 45 minutes of chest physical therapy, as noted in Figure 5. Prone positioning and suctioni~~g did not prevent the secretion retention that resulted in collapse of the patient's left lung.
Figure 5. Reexpansion of the left lung 1 hour following one chest physical therapy treatment.
Special Conditions Table 6 summarizes the medical conditions commorilv found in patients in the ICU, indications for chest physical therapy, and treatment guidelines.
Summary This article provides a discussion of the literature relat- ing to chest physical therapy, indications for treatment, and the rationale for its use in the ICU. Comparisons are made with therapeutic bronchoscopy and therapeutic positioning. The complications of tracheal suctioning are discussed as well as methods for minimizing hypox- emia, and the necessary features of suction catheters are described. Although patient mobilization and deep- breathing exercises with coughing can often replace postural drainage, percussion, and vibration, many patients in the ICU cannot be mobilized sufficiently to eliminate the sequelae of secretion retention due to the severity of injury or illness and the paraphernalia neces- sary to sustain life.
I believe that when a clear indication for chest physical therapy is present, it can be performed safely and effectively by clinicians who have received training in the ICU. I contend that the recommended treatment of lobar and segmental atelectasis is postural drainage with percussion and vibration in conju~lction with airway suctioning for patients who are intubated. Further research is needed to assess the efficacy of manual hyperinflation i11 patients who are mechanically venti- lated and the efficacy of therapeutic positioning without postural drainage and manual techniques.
Physical Therapy . Volume 76 . Number 6 . June 1996 Ciesla . 62 1
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from
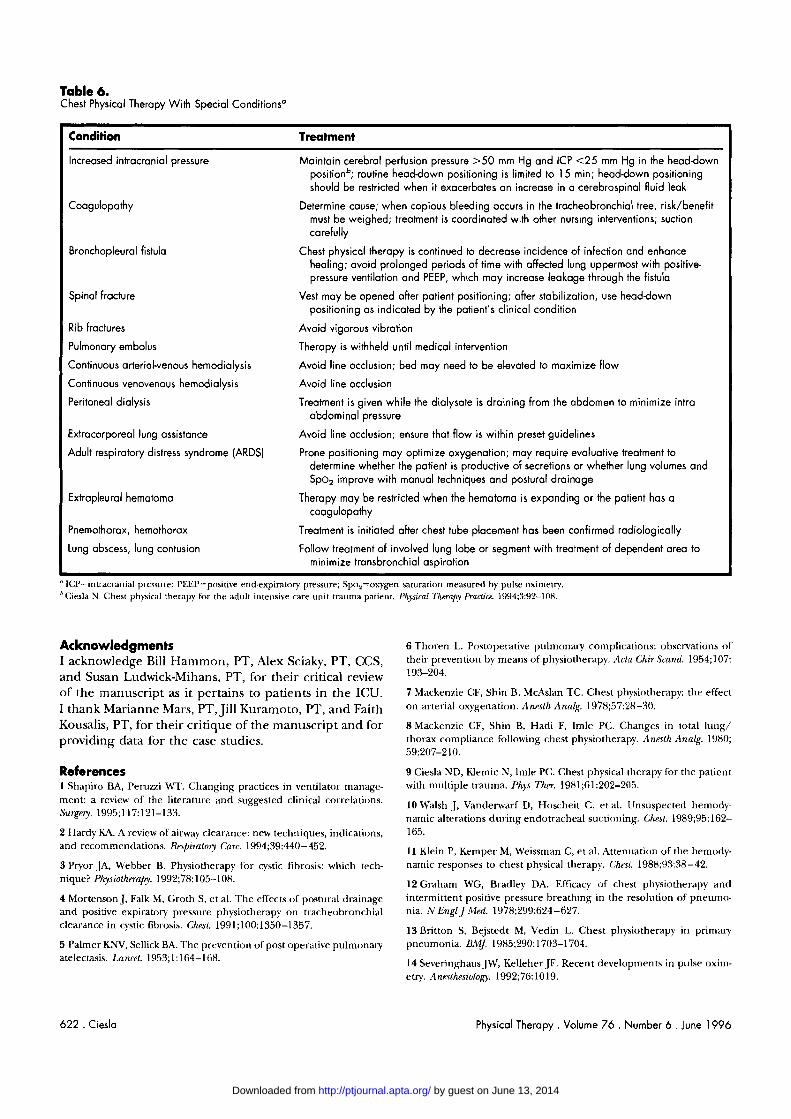
Table 6. Chest Physical Therapy With Special Conditions"
Condition Treatment
Increased intracranial pressure
Coagulopathy
Bronchopleural fistula
Spinal fracture
Rib fractures
Pulmonary embolus
Continuous arterial-venous hemodialysis
Continuous venovenous hemodialysis
Peritoneal dialysis
Extracorporeal lung assistance
Adult respiratory distress syndrome [ARDS)
Extrapleural hematoma
Pnemothorax, hemothorax
Lung abscess, lung contusion
Maintain cerebral perfusion pressure >50 mm Hg and ICP <25 mm Hg in the headdown positionb; routine headdown positioning is limited to 15 min; headdown positioning should be restricted when it exacerbates an increase in a cerebrospinal fluid leak
Determine cause; when copious bleeding occurs in the tracheobronchial tree, risk/benefit must be weighed; treatment is coordinated with other nursing interventions; suction carefully
Chest physical therapy is continued to decrease incidence of infection and enhance healing; avoid prolonged periods of time with affected lung uppermost with positive- pressure ventilation and PEEP, which may increase leakage through the fistula
Vest may be opened after patient positioning; after stabilization, use headdown positioning as indicated by the patient's clinical condition
Avoid vigorous vibration
Therapy is withheld until medical intervention
Avoid line occlusion; bed may need to be elevated to maximize flow
Avoid line occlusion
Treatment is given while the dialysate is draining from the abdomen to minimize intra- abdominal pressure
Avoid line occlusion; ensure that flow i s within preset guidelines
Prone positioning may optimize oxygenation; may require evaluative treatment to determine whether the patient is productive of secretions or whether lung volumes and Spa, improve with manual techniques and postural drainage
Therapy may be restricted when the hematoma is expanding or the patient has a coagulopathy
Treatment is initiated after chest tube placement has been confirmed radiologically
Follow treatment of involved lung lobe or segment with treatment of dependent area to minimize tronsbronchial aspiration
" ICP=intr-acraoial pressure; PEEP=positivr el~dexpiratory pressure; Spo,=oxygen saturation measured by pulse oximetry. " Ciesla N . Chest physical therapy for the adult intensive care unit trauma patient. Physiral 7'hmapy Practice. 1994;3:92-108.
Acknowledgments I acknowledge Bill Hammon, PT, Alex Sciaky, PT, CCS, and Susan Ludwick-Mihans, PT, for their critical review of the manuscript as it pertains to patients in the ICU. I thank Marianne Mars, PT, Jill Kuramoto, PT, and Faith Kousalis, PT, for their critique of the manuscript and for providing data for the case studies.
References 1 Shapiro BA, Peruzzi WT. Changing practices in ventilator manage- ment: a review of the literature and suggested clinical correlations. Su~gay. 1995;117:121-133.
2 Hardy KA. A review of airway clearance: new techniques, indications, and recommendations. Retpiratoly Care. 1994;39:440-452.
3 Pryor .]A, Webber B. Physiotherapy for cystic fibrosis: which trch- nique? Physiothmapy. 1992;78:105-I 08.
4 Mortenson J, Falk M, Groth S, et al. The effects of postural drainage and positive expiratory pressure physiotherapy on tracheohronchial clearance in cystic fibrosis. Chest. 1991;100:1350-1357.
5 Palmer KNV, Sellick BA. The prevention of post operative pulmonary atelectasis. Lancet. 1953; 1: 164-1 68.
6 Thoren L. Postoperative pulmonary complications: obselvations of their prevention by means of physiotherapy. Acta Chir Srand. 1954;107: 193-204.
7 Mackenzie CF, Shin B, McAslan TC. Chest physiotherapy: the effect on arterial oxygenation. Anesth Analg. 1978;57:28-30.
8 Mackenzie CF, Shin B, Hadi F, lmle PC. Changes in total lung/ thorax compliance following chest physiotherapy. Anesth Analg. 1980; 59:207-210.
9 Ciesla ND, Iilemic N, lmle PC. Chest physical therapy for the patient with multiple trauma. Phys Thm. 1981;61:202-205.
10 Walsh J, Vanderwarf D, Hoscheit C, et al. Unsuspected hernody- namic alterations during endotracheal suctioning. Chest. 1989;95:162- 165.
11 Klein P, Kemper M, Weissman C, et al. Attenuation of the hemody- namic responses to chest physical therapy. Chest. 1988;93:38-42.
12 Graham M'G, Bradley DA. Efficacy of chest physiotherapy and intermittent positive pressure breathing in the resolution of pneumo- nia. N Engl J Med. 1978;299:624-627.
13Britton S, Bejstedt M, Vedin L. Chest physiotherapy in primary pneumonia. BMJ. 1985;290: 1703-1704.
14 Severinghaus JW, Kelleher JF. Recent developments in p ~ ~ l s e oxim- etry. Anstthesiology. 1992;76: 1019.
622 . Ciesla Physical Therapy . Volume 76 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

15 Sutton I'P. Chest physiotherapy: time for reappraisal. BrJDis Chest. 1988;82:127-137.
16 Pavia D. The role of chest physiotherapy in mucus hypersecretion. Lung. 1990;168(suppI):614-621.
17 Sutton I'P, Lopez-Vidriero MT, Pavia D, et al. Assessment of percus- sion, vibratory shaking and breathing exercises in chest physiotherapy. EurJRespir Dis. 1985;66:147-152.
18 Jenkins S, Soutar SA, Loukota JM, et al. Physiotherapy after coro- nary artery surgery: Are breathing exercises necessary? Thorax. 1989; 44:634-639.
19 Dull JI, Dull WL. Are maximal inspiratory breathing exercises or incentive spirometry better than early mobilization after cardiac sur- gery? Phys Ther. 1983;63:655-659.
20 Hallbook T, Lindbald B, Lindroth B, et al. Prophylaxis against pulmonary complications in patients undergoing gallbladder surgery: a comparison between early mobilization, physiotherapy with and without bronchodilation. ~ n k Chir Gynaecol. i984;73:55-58.
21 Stiller R, Montarello J, Wallace M, et al. Efficacy of breathing and coughing exercises in the prevention of pulmonary complications after coronary artery surgery. Chest. 1994;105:741-747.
22 Dean E, Ross J. Oxygen transport: the basis for contemporary cardiopulmonary physical therapy and its optimization with body positioning and mobilization. Physical Therapr Practice. 1992;1:34-44.
23 Dean E, Ross J. Discordance between cardiopulmonary physiology and physical therapy. Chest. 1992;101:1694-1698.
24 Dean E. Oxygen transport: a physiologically based conceptual framework; for the practice of cardiopulmonary physiotherapy. Physie therapy. 1994;80:347-355.
25 MariniJ, Pierson DJ, Dudson L. Acute lobar atelectasis: a prospec- tive comparison of fiberoptic bronchoscopy and respiratory therapy. Am Rm Respir Dis. 1979;119:971-978.
26 Light KB. Pneumonia. In: Hall JB, Schmidt GA, Wood LD, eds. Pn'ncipb rf Critical Care. New York, NY McGraw-Hill; 1992:1249.
27 Ruiz-Santana S, Gimenez A, Esteban A, et al. ICU pneumonias: a multi-institutional study. Crit Care Med. 1987;15:930-932.
28 Stevens RM, Teres D, Skillman J, et al. Pneumonia in an ICU. Arch I n t a Met!. 1974;143:106-111.
29 Joshi PI, Ciesla N, Caplan E. Diagnosis of pneumonia in critically ill patients. Chest. 1988;94:4s. Abstract.
30 Finland M. Changing ecology of bacterial infections as related to antibacter.ia1 therapy. J Inj2ct Dis. 1970;122:419-431.
31 McDermott W. The John Barnwell Lecture: microbial drug resis- tance. Am Reu Dis. 1970;102-857-876.
32 Weissman C, Kemper M, Damast MC, etal. Effect of routine intensive care interaction on metabolic rate. Chest. 1984;86:815-818.
33 American Association of Respiratory Care Clinical Practice Guide- line: Postural Drainage Therapy. Respiratoly Care. 1991;36:1419.
34 Leith DE. The development of cough. Am Reu Respir Dis SuppL 1985;141:s39-s42.
35 Mossberg B, Cramer P. Mucociliary transport and cough as tracheo- bronchial clearance mechanisms in pathological conditions. Eur J Respir Dis Suppl. 1980;61:47-55.
36 King h4. Rheological requirements for optimal clearance of secre- tions: cili.ary transport versus cough. Eur J Respir Dis. 1980;61 (suppl): 39-42.
38 Newhouse MT. Factors affecting sputum clearance. Thurax. 1973; 28:267. Abstract.
39 Siebens AA, Kirby NA, Poulos DA. Cough following transection of the spinal cord at C-6. Arch Phys Med Rehabil. 1964;45:1-8.
40 Imle PC, Klemic N. Changes with immobility and methods of mobilization. In: Mackenzie CF, ed. Chest Physiotherapy in the Intensive Care Unit. 2nd ed. Baltimore, Md: Williams & Wilkins; 1989:188-214.
41 Clauss RH, Scalabrini BY, Ray JF, et al. Effects of changing body position upon improved ventilation-perfusion relationships. Circula- tion. 1968;37(suppl 2):214-217.
42 Douglas WW, Rehder K, Beynen EM, et al, Improved oxygenation in patients with acute respiratory failure: the prone position. Am Rm Respir Dis. 1977;115:559-566.
43 Chulay M, Brown J, Summer W. Effect of post-operative immobili- zation after coronary artery bypass. Crit Care Med. 1982;10:176-179.
44 Remolina C, Khan AU, Santiago TV, et al. Positional hypoxemia in unilateral lung disease. N Engl J Med. 1981;304:523-525.
45 Langer M, Mascheroni D, Marcolin R, et al. The prone position in ARDS patients. Chest. 1988;94:103-107.
46 Arborelius M, Granqvist U, Lija B, et al. Regional lung function and central hemodynamics in the right lateral body position during hypoxia and hyperoxia. Respiration. 1974;31:193-200.
47 Pappert D, Rossaint R, Klaus S, et al. Influence of positioning on ventilation-perfusion relationships in severe adult respiratory distress syndrome. Chest. 1994;106:1511-1516.
48 Zack MB, Pontoppidan H, Kazemi H. The effect of lateral positions on gas exchange in pulmonary disease. Am Reu Respir Dis. 1974;llO: 49-55.
49 Piehl MA, Brown MS. Use of extreme position changes in acute respiratory failure. Crit Care Med. 1976;4:13-15.
50 Wong JW, Keens TG, Wannamaker EM, et al. Effects of gravity in tracheal transport rates in normal subjects and in patients with cystic fibrosis. Pediatrics. 1977;60:146-152.
51 Ciesla N. Postural drainage, positioning, breathing exercises. In: Mackenzie CF, ed. Chest Physiotherapy in the Intensive Care Unit. Balti- more, Md: Williams & Wilkins; 1989:97-99.
52 Bateman J, Newman S, Daunt K, et al. Is cough as effective as chest physiotherapy in the removal of excessive tracheobronchial secretion? Thurax. 1981;36:683-687.
53 Sutton PP, Parker RA, Webber BA. Assessment of the forced expiration technique, postural drainage and directed coughing in chest physiotherapy. Eur J Respir Dis. 1983;64:62-68.
54 Mackenzie CF. Physiological changes following chest physiotherapy. Mackenzie CF, ed. Chest Physiotherapr in the Intensive Care Unit. 2nd ed. Baltimore, Md: Williams & Wilkins; 1989:240-242.
55 Stiller K, Geake T, Taylor J, et al. Acute lobar atelectasis: a compar- ison of two chest physiotherapy regimens. Chest. 1990;98:1336-1340.
56 Bien MY, Zadai CC, Kigin CM. The effect of selective drainage positions on oxygen saturation in obese patients after abdominal surgery. Chin Med J (Engl). 1993;51:183-192.
57 Johnson NT, Marini J, Pierson DJ, et al. Acute lobar atelectasis: effect of chest percussion and postural drainage (CPPD) on resolution. Am Reu Respir Dis. 1987;135:A433. Abstract.
58 Imle PC. Percussion and vibration. In: Mackenzie CF, ed. Chest Physiotherapy in the Intensive Care Unit. 2nd ed. Baltimore, Md: Williams & Wilkins; 1989:134, 135, 138, 141, 146.
37 Leith IDE. Cough. Phys Tho: 1968;48:439-447.
Physical Therapy . Volume 76 . Number 6 .June 1996 Ciesla . 623
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

59 King M, Phillips DM, Vartian V, et al. Enhanced tracheal mucus clearance with high frequency chest wall compression. Am Reu Respir Dis. 1983; 1 28:5 1 1-5 15.
60 Hansen LG, Wanvick WJ, Hansen KL. Mucus transport mechanisms in relation to the effect of high frequency chest compression (HFCC) on mucus clearance. Pediatr Pulmonol. 1994;17: 1 13-1 18.
61 Selby D, Jones JG. Some phvsiological and clinical aspects of chest physiotherapy. Rt. J Anaesth. 1990;64:621-631.
62 Raghu G, Pierson D. Successful removal of an aspirated tooth by chest phvsiotherapy. R@zr Care. 1986;31:1099-1101.
63 Petty TL, ed. Int~nsiue and Rthabilitative Respiratory Care. Philadel- phia, Pa: Lea & Febiger; 1974:106, 108.
64 Peruzzi WT, Shapiro BA. Respiratory support. In: Tinker J, Browne DR, Sibbald M'J, eds. Critiral Care: Standards, Audit, andEthics. London, England: Edward Arnold (Publishers) Ltd; 1996:137, 138.
65 Seidel HM, Ball JW, Dains JE, Benedict GM'. Mosby's Guide to Physical Examination. 3rd ed. St Louis, bio: Mosby; 1995:319.
66 Brimoulle S, Moraine J, Kahn RJ. Passive physical therapy and r e sp i r a to~ therapy effects on intracranial pressure. Crit Care Med. 1988;16:449. Abstract.
67 Moraineg, Brimioulle S, Kahn RJ. Effects of respiratory therapy on intracranial pressure. J Crit Care. 1991;6: 197-20 1.
68 Sutton PP, Pavia D, Bateman JRM, Clarke SW. Chest physiotherapy: a review. klur J Rtspir Dis. 1982;63:188-201.
69 Wollmer P, Ursing K, Midgren B, Eriksson L. lnefficiency of chest percussion in the physical therapy of chronic bronchitis. EurJ Respir Dis. 1985;66:233-239.
70 Campbell AH, O'Connell JM, Wilson F. The effect of chest physirr therapy on FEV, in chronic bronchitis. MedJAust. 1975;1:33-3.5.
71 Gallon A. Evaluation of chest percussion in the treatment of patients with copious sputum production. Resflir Med. 1991;85:45-51.
72 Ciesla ND. Chest physiotherapy for special patients. In: Mackenzie CF, ed. Chest Physiotherupy in t h ~ Intensiup Care Unit. 2nd ed. Baltimore, Md: Williams & Wilkins; 1989:267.
73 Imle PC:. Physical therapy for patients with cardiac, thoracic, or abdominal conditions following surgery or trauma. In: lnvin C, Tecklin .JS, eds. Cardiopulmonary Phpsiral 'I'hmpy. 3rd ed. St Louis, Mo: Mosby; 1995:382-383.
74 Kigin C:M. Advances in chest physical therapy. In: O'Donohue W, ed. C u m t Advances in Respiratoq Care. Park Ridge, 111: American C:ollege of Chest Phvsicians; 1984:145.
75 Ciesla ND, Rodriguez A, Anderson P, et al. The incidence of extrapleural hematomas in patients with rib fractures receiving chest physical therapy. Phys ?'her. 1985;76:766. Abstract.
76 Dulfano MJ, Lik C:K, Beckage M, et al. Ciliary beat frequency in human ~.espiratory explants. Am RPU RPspir Di.7. 1981 ;I 231 99-140.
77 Radford G, Barutt J, Billingsley JG, et al. A rational basis for percussion-augmented mucociliary clearance. RPspir Care. 1982;27: 556-563.
78 Hammon WE. Manual versus mechanical percussion for clearance of alveolar contents. I'hys 7'hpr. 1983;63:756. Abstract.
79 Rossman CM, Waldes R, Sampson D, Newhouse MT. Effect of chest physiotherapy on the removal of mucus in patients with cystic fibrosis. Am RPU Kpspir Dis. 1982;126:131-135.
80 Rubin EM, Scantlen GE, Chapman GA, et al. Effect of chest wall oscillation on mucus clearance: comparison of two vibrators. Pediatl- Pulmonol. 1989;6:122-126.
81 Hammon WE. McCaffree DR, Cucchiara AJ. A comparison of manual to mechanical chest percussion for clearance of alveolar material in patients with pulmonar). alveolar proteinosis. Che.51. 1993; 103:1409-1416.
82 Hammon WE, McCaffree DR. Manual percussion compared to pneumatic percussion for clearance of alveolar material in patients with pulmonary alveolar prote~nosis. In: Proceedings of the 12th Inlerna- tional Congress of the World Confederntlo,~ for Phyciral 7'h~rupy; J u n ~ 25-30, 1995; Washzngton, DC. 1995:591. Abstract.
83 Whitman J, Van Beusekom R, Olson S, et al. Preliminary evaluation of high-frequency chest compression for secretion clearance in mechanically ventilated patients. Respir Care. 1993;38:1081-1087.
84 Respiratoly and physical therapy. In: Tinker J, Browne DR, Sibbald WJ, eds. Cntical Care: Standards, Audit, and Ethirs. London, England: Edward Arnold (Publishers) Ltd; 1996:234-244.
85 Jones A m , Jones RD, Bacon-Shone J. A comparison of expiratory flow rates in two breathing circuits used for manual inflation of the lungs. Physiotherapy. 1991;77:593-595.
86 Brandstater B, Muallem M. Atelectasis following tracheal suction in infants. An~.cthesiology. 1969;31:468-473.
87 Clement AJ, Hubsch SK. Chest physiotherapy by the hag squeezing method. Physiotherapy. 1968;54:355-359.
88Novak RA, Shumaker L, Snyder JV, Pinsky MR. Do periodic hyperinflations improve gas exchange in patients with hypoxemic respiratoly failure? Crit Care Med. 1987; 15:1081-1085.
89 Jones AY, Hutchinson RC, Teik EO. Effects of bagging and percus- sion on total static compliance of the respiratory system. Physiolherapp. 1992;78:661-666.
90 Gattinoni L, Pesenti A, Bombino M, et al. Role of extracorporeal circulation in adult respiratory distress syndrome management. New Hm'z. 1993;1:603-612.
91 Garrard J Bullock M. The effect of respiratory therapy on intracra- nial pressure in ventilated neurosurgical patients. Ausl J Physiol. 1986; 32:107-111.
92 Carlsson H, Ersson U. Hedstrand U, et al. Observations on intra- cranial dynamics at endotracheal suction and bag squeezing in patients with severe brain trauma. Acta Neurochir (Wien). 1988;91:155. Abstract.
93 Laws AK, Mcintrye RW. Chest physiotherapy: a physiological assess- ment during intermittent positive pressure ventilation in respiratory failure. Can Anaesth Sor J. 1969;16:487-493.
94 Smaldone GC, Messina MS. Flow limitation, cough, and patterns of aerosol deposition in humans. J Appl Physiol. 1985;59:515.
95 Heiptas BG, Roth RD, Jensen \'M. Huff coughing and airway patency. h p i r Care. 1979;24:710-713.
96 Curry LD, Van Eeden C. The influence of posture on the effective- ness of coughing. S Aj? JPhysiothw: 1977;33:8-11.
97 Stone KS, Turner B. Endotracheal suctioning. Ann Rm Nurs Kes. 1989;7:28.
98 Goodner B. The OSHA Handbook: Int~@retatzv~ Guzdelines for the Blood-Home Pathogen Standard. El Paso, Tex: Skidrnore Roth; 1993:lO.
99 Bodai BI. A means of suctioning without cardiopulmonary depres sion. H~art I,ung. 1982;111:172-176.
100 Mayhill CG. The Trach CareTM closed tracheal suction system: a new medical device to permit tracheal suctioning without interruption of ventilatory assistance. Infect Cont~ul Hosp Epidemiol. 1988;9:125-126.
101 Benson MS, Pierson DJ. Ventilator wash-out volume: a consider- ation in endotracheal suction preoxygenation. Respir Cr1t.p. 1990;35: 1257-1 260.
6 2 4 . Ciesla Physical Therapy . Volume 7 6 . Number 6 . June 1996
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

102 Sb.'RI'O 900C Operating Manual. Solna, Sweden: Siemens-Elema. 1085;2:7.
103 Kulmar A, Falke KJ, Gefin B, et al. Continuous positive pressure ventilation in acute respiratory failure. NKngl JMed. 1970;282:1439.
104 Jung RE, Newman J. Minimizing hypoxia during endotracheal airway care. Heart 1,ung. 1982;11:208-212.
105 Brown SE, Stansbury DW, Merrill EJ. Prevention of suctioning- related arterial oxygen desaturation. Chest. 1983;4:621-627.
106 Noll IML, Hix CD, Scott G. Closed tracheal suction systems: effectiveness and nursing implications. American Association of Critical Care Aiurser. 1990;1:318-328.
107 Taggart JA, Dorinsky NL, Sheahan JS. Airway pressures during closed system suctioning. Heart Lung. 1988;17:536-542.
108 Chulay M. Arterial blood gas changes with a hyperinflation and hyperoxygenation suctioning intervention in critically ill patients. Heart I,ung. 1988;17:654-661.
109 Stone KS, Talaganis SA, Preusser B, et al. Effect of lung hyper- inflation and endotracheal suctioning on heart rate and rhythm in patients after coronary artery bypass surgey. Heart Lung. 1991;20:443- 450.
110 McCabe SM, Smeltzer SC. Comparison of tidal volumes obtained by one-harided and two-handed ventilation techniques. A m J Crit Care. 1993;2:467-473.
111 Chulzy M. Hyperinflation/hyperoxygenation to prevent endotra- cheal suctioning complications. Critical Care Nurse. 1987;7:100-102.
112 Glass C, Grap MJ, Corley MC, et al. Nurses' ability to achieve hyperinflation and hyperoxygenation with a manual resuscitation bag during endotracheal suctioning. Heart Lung. 1993;22:158-165.
113 DePevi CL, No11 ML. In-line closed-system suctioning: a research analysis. Dimensions of Critical Care Nursing. 1993;13:80.
114 Imle F'C. Methods of airway clearance: coughing and suctioning. In: Mackenzie CF, ed. Chest Physiotherapy in the Intensive Care Unit. 2nd ed. Baltimore, Md: Williams & Wilkins; 1989:70.
115 Hanley hW, Rudd T, ButlerJ. What happens to intratracheal saline instillations? Am ElPO h p i r Dis. 1979;117(suppl):124.
116 Imle PC. Adjuncts to chest physiotherapy. In: Mackenzie CF, ed. C,'hest Physzotherapy i n the Intensive Care L'nit. 2nd ed. Baltimore, Md: M'illiams &: Wilkins; 1989:281.
117 Webber B, Parker R, HofmeyrJ, et al. Evaluation of self-percussion during postural drainage using the forced expiration technique. Physical 7'herapy Practire. 1985;1:42-45.
119 Hornstein S, Ledsome J. Venti1atot-y muscle training in acute quadriplegia. Physiotherapy Canada. l986;38:145-149.
120 Derrickson J , Ciesla N, Simpson N, Imle PC. A comparison of two different breathing exercises for quadriplegic patients. Phgs ?'her. 1992;72:763-769.
121 Van de Water JM. Preoperative and operative techniques in the prevention of pulmonary complications. Surg Clin North Am. 1980;60: 1339-1348.
122 Sciaky AJ. Mobilizing the intensive care unit patient: pathophysi- ology and treatment. Physical Therapy Practice. 1994;3:69-80.
123 Jaworski A, Goldberg SK, Walkenstein MD, et al. Utility of imme- diate postlobectomy fiberoptic bronchoscopy in preventing atelectasis. Chest. 1988;94:38-43.
124 Stern RC, Boat TF, Orenstein DM, et al. Treatment and prognosis of lobar and segmental atelectasis in cystic fibrosis. A m ElPO &S& Dis. 1978;118:821-826.
125 Cotton EK, Abrams G, Van Houtte J, et al. Removal of aspirated foreign bodies by percussion and postural drainage. Clin Pediatr. 1973;12:270-276.
126 Pereira W, Kovnat D, Iacovino J, et al. A prospective study of the complications following flexible fiberoptic bronchoscopy. Chest. 1978; 73:813-816.
127 Hammon WE, Connors AF, McCaffree DR. Cardiac arrhythmias during postural drainage and chest percussion of critically ill patients. Chest. 1992;102:1836-1841.
128 Shrader DL, Lakshminarayan S. The effect of fiberoptic bronchos- copy on cardiac rhythm. Chest. 1978;73:821-824.
129 Ciesla ND. Chest physical therapy for the adult intensive care unit trauma patient. Physical Therapy Practice. 1994;3:92-108.
130 Mars M, Ciesla ND. Chest physical therapy may have prevented bronchoscopy and exploratory laparotomy: a case report. Curdtopultno- naly Physical Therapy. 1993;4:4-5.
131 Hammon WE, Martin RJ. Chest physical therapy for acute atelec- tasis: a report on its effectiveness. Phys Ther. 1981;61:217-220. Clinical report.
132 Susini G, Sisillo E, Bortone F. Postoperative atelectasis reexpansion by selective insufflation through a balloon-tipped catheter. Chesl. 1992;102:1693-1696.
133 Haenel JB, Moore FA, Moore EE, et al. Efficacy of selective intrabronchial air insumation in acute lobar collapse. A m J Surg. 1992;164:501-505.
118 Aldrich TK, Karpel JP. Inspiratory muscle training in the mechan- ically ventilated patient. Physzotherapy Canada. 1987;39:305-307.
Physical Therapy. Volume 76 . Number 6 . June 1996 Ciesla . 625
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from

1996; 76:609-625.PHYS THER. Nancy D CieslaCare UnitChest Physical Therapy for Patients in the Intensive
Cited by
http://ptjournal.apta.org/content/76/6/609#otherarticles
This article has been cited by 1 HighWire-hosted articles:
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on June 13, 2014http://ptjournal.apta.org/Downloaded from