physical therapy rehabilitation following a thoracic to
TRANSCRIPT
University of North Dakota University of North Dakota
UND Scholarly Commons UND Scholarly Commons
Physical Therapy Scholarly Projects Department of Physical Therapy
5-2020
Physical Therapy Rehabilitation Following a Thoracic to Sacroiliac Physical Therapy Rehabilitation Following a Thoracic to Sacroiliac
Spinal Fusion: A Case Report Spinal Fusion: A Case Report
Ragen Wilson University of North Dakota
Follow this and additional works at: https://commons.und.edu/pt-grad
Part of the Physical Therapy Commons
Recommended Citation Recommended Citation Wilson, Ragen, "Physical Therapy Rehabilitation Following a Thoracic to Sacroiliac Spinal Fusion: A Case Report" (2020). Physical Therapy Scholarly Projects. 700. https://commons.und.edu/pt-grad/700
This Scholarly Project is brought to you for free and open access by the Department of Physical Therapy at UND Scholarly Commons. It has been accepted for inclusion in Physical Therapy Scholarly Projects by an authorized administrator of UND Scholarly Commons. For more information, please contact [email protected].

Physical Therapy Rehabilitation Following a Thoracic to Sacroiliac Spinal Fusion: A Case Report
by
Ragen Wilson, SPT
Bachelor of Science University of Wyoming, 2017
Associate of Science Casper College, 2014
A Scholarly Project Submitted to the Graduate Faculty of the
Department of Physical Therapy
School of Medicine
University of North Dakota
in partial fulfillment of the requirements for the degree of
Doctor of Physical Therapy
Grand Forks, North Dakota May, 2020
This Scholarly Project, submitted by Ragen Wilson in partial fulfillment of the requirements for the Degree of Doctor of Physical Therapy from the University of North Dakota, has been read by the Advisor and Chairperson of Physical Therapy under whom the work has been done and is hereby approved.
ii
de½~~ Schawnn Decker, (Graduate School Advisor)
Dave Relling, (Chairperson, Physical Therapy)
Title
Department
Degree
PERMISSION
Physical Therapy Rehabilitation Following a Thoracic to Sacroiliac Spinal Fusion: A Case Report
Physical Therapy
Doctor of Physical Therapy
In presenting this Scholarly Project in partial fulfillment of the requirements for a graduate degree from the University of North Dakota, I agree that the Department of Physical Therapy shall make it freely available for inspection. I further agree that permission for extensive copying for scholarly purposes may be granted by the professor who supervised my work or, in her absence, by the Chairperson of the department. It is understood that any copying or publication or other use of this Scholarly Project or part thereof for financial gain shall not be allowed without my written permission. It is also understood that due recognition shall be given to me and the University of North Dakota in any scholarly use which may be made of any material in this Scholarly Project.
Signature ~Jifl: Date lo/zq/lC>J
'
iii
(
TABLE OF CONTENTS
LIST OF FIGURES ...................................................................... .. v
LIST OF TABLES ......................................................................... vi
ACKNOWLEDGEMENTS ........................................................... .... vii
ABSTRACT ................................................................................. viii
CHAPTER I.
II.
BACKGROUND AND PURPOSE ........................ . 1
CASE DESCRIPTION ..................................... .... 5
Examination, Evaluation and Diagnosis .................. 6
Prognosis and Plan of Care ................................. 8
Ill. INTERVENTION ............................................. . 11
IV. OUTCOMES ................................................... 13
V. DISCUSSION .................................................. 15
Reflective Practice ............................................ 18
REFERENCES ........................................................................... 20
iv
LIST OF FIGURES
1. Self-reported ABC Scale and Modified Oswestry pre-treatment versus post 9 week Interventions ............................................................................ 13
2. Self-reported level of pain (pn) using VAS pre-treatment versus 9 week interventions ..................................................................................... 14
V
LIST OF TABLES
1. Patient Reported Goals ....................................................................... 8
2. Aquatic Therapy Interventions (Weeks 1-3; 1 hour sessions; 2x/week) .......................................................................................... 10
3. Land Based Therapy Interventions (Weeks 4-9; 1 hour sessions; 2x/week) .......................................................................................... 11
(
vi
ACKNOWLEDGEMENTS
This case report could not have been completed without the consent of the
patient. I would like to send my full appreciation to this patient for displaying
motivation and compliance throughout her plan of care and granting me
permission to use her outcome for this scholarly project. I would also like to
express gratitude to my clinical instructor (PT, DPT) for her guidance and
expertise in the overall physical therapy rehabilitation process of this diagnosis
which lead to a successful outcome. I would like to thank Schawnn Decker,
DPT/Assistant Professor, for her supervision and guidance while writing this case
report. Finally, I send appreciation to Kevin Hansen, Daniel Torok, and McKenzie
Klocke who provided insight and revision advice throughout the development of
this case report.
vii
ABSTRACT
Background and Purpose. This case study described the 9 week outpatient
physical therapy rehabilitation process of a 75 year old female following a
posterior thoracic spine (T9) to sacroiliac (S 1) spinal fusion as a result of adult
degenerative scoliosis and prolonged back pain (Type 1 ). The purpose of this
case report was to describe the overall outpatient physical therapy management
of this post-operative fusion. Description. The patient presented to physical
therapy with decreased mobility, decreased function, decreased balance, lower
extremity strength deficits, pain, and loss of independence. Intervention. Initially,
treatment occurred in a therapeutic pool and then progressed to a land based
setting. Treatments involved therapeutic exercise, therapeutic activities,
neuromuscular reeducation, gait training, and education. Outcomes. Following
PT intervention, the patient achieved all stated functional goals, increased LE
strength, improved confidence in balance, and re-gained independence of ADLs.
Discussion. Rationale for treatment was based on the spine surgeon's protocol
for multiple level spinal fusion, functional tasks the patient was unable to
complete, and impairments based on the initial evaluation. The patient was able
to improve function and mobility and regain independence following 9 weeks of
outpatient physical therapy treatments.
viii
Background
CHAPTER I
BACKGROUND AND PURPOSE
Adult scoliosis is defined as a spinal deformity in a skeletally mature
patient with a Cobb angle of more than ten degrees in the coronal plain. Adult
scoliosis can be separated into four major groups: Type 1, Type 2, Type 3a, and
Type 3b. Type 1 is known as a primary degenerative scoliosis affecting the disc
and/or facet joints predominantly with back pain symptoms. Type 2 is known as
idiopathic adolescent scoliosis of the thoracic and/or lumbar spine which
progresses into adult life. Type 3a is known as secondary adult curves due to leg
length discrepancy, hip pathology, or abnormalities in the lumbosacral junction.
Type 3b is in the context of metabolic bone disease combined with asymmetric
arthritic disease. 1
Furthermore, as individual's age, and without addressing these
asymmetries, scoliosis significantly progresses due to increased asymmetric load
and deformities.1 The progression of a curve is further supported by
osteoporosis, particularly in post-menopausal females. When surgeons decide
operative treatment for adult spinal deformity (ASD), main considerations were
pain and disability.2 Surgical management consists of either decompression,
correction, stabilization, or fusion procedures or a combination of some of these. 1
Most surgeons recommend decompression along with fusion, which has been
1
widely accepted to improve spinal alignment at the expense of mobility. 3
According to the American Academy of Orthopedic Surgeons, the basic idea of a
fusion is to fuse together two or more vertebrae so that they heal into a single
solid bone in order to eliminate painful motion or to restore stability of the spine.4
Typically, people try to avoid painful situations or pain provoking
conditions. When an individual moves into a certain position and pain is the
response, that individual is going to avoid that position. When people avoid
specific movements over a long period of time due to a painful response, a
sedentary lifestyle can become the result. People are motivated to avoid
activities in which they have experienced acute episodes of pain in order to
reduce the likelihood of re-experiencing pain or causing further physical damage.
This concept is known as the fear avoidance model of chronic pain. This basic
model proposes, that if one interprets the experience of pain as significantly
threatening and begins to catastrophize about it, then pain-related fear evolves.5
Individuals with spinal injuries and disease naturally come to avoid
behaviors and postures that provoke back pain. Such activity restriction, while
minimizing increases in pain, can have significant adverse physical, emotional,
and cognitive consequences when pain becomes chronic. Perhaps, patients can
develop strong fears that their actions will worsen underlying physical problems,
further restricting activities and heightening emotional distress.6 Fear-avoidance
beliefs have been found to be significant predictors of pain and functional
outcomes for up to 2 years after lumbar spine surgery. 7 Fear avoidance
behaviors can negatively impact mental barriers associated with pushing through
2
pain which can negatively affect exercise, mobility, and functional outcomes even
after surgical intervention.
Individuals who have received thoracic to lumbar spinal fusions are at a
potential risk to have decreased range of motion of the spine due to the
mechanism of surgery and the number of joints affected. The properties of water
provide many enticing qualities to help re-educate the body and promote early
range of motion when instances may be difficult to achieve initially on land. When
compared to land-based exercises, water exercises can offer some advantages
to overweight patients, with mobility difficulties, since the body weight relief
provided by the buoyancy reduces the impact on joints and the perception of pain
intensity.8 In addition, studies in healthy adults and older subjects have shown
that water exercises are effective to increase muscle strength. Once individuals
have plateaued in aquatic environments, treatments can progress to land based
therapy.
Physical therapists strive to create interventions that focus on improving a
patient's functional ability. Function gained during or after therapy is often
measured by change, over time, in score on a functional assessment instrument.
Functional outcome measures are important for physical therapists to administer
at initial evaluation and discharge in order to determine if treatments were
clinically significant. Determining whether an improvement is significant,
researchers need to provide minimal detectable change scores.9 Minimal
detectable change is defined as the minimal amount of change that is not due to
variation in measurement.10
3
The Activities-specific Balance Confidence Scale (ABC scale) is often
used by physical therapists to determine the patient's confidence in their balance.
The scale is comprised of 16 questions, where the patient self-reports their level
of confidence (0%-100%) on performing ambulatory tasks without falling. A
higher percentage indicates a higher confidence level. The ABC scale
demonstrates excellent reliability and validity in older adults. 11 Another common
functional outcome measure used by physical therapists is the Modified
Oswestry Low Back Pain Disability Questionnaire. This test assesses how an
individual's back pain has affected their activities of daily living. The
questionnaire is comprised of 10 questions, where the patient self-reports their
perceived level of disability on a O (no impairment) to 5 (maximum impairment)
scale. A higher score reflects a higher level of disability. The Oswestry Low Back
Pain Disability Questionnaire has good reliability and validity in measuring
disability in individuals with low back pain. 12
Purpose
There is insufficient research supporting the physical therapy rehabilitation
protocol of a post-operative thoracic to sacroiliac fusion due to degenerative
scoliosis. This case report details the 9 week outpatient physical therapy
rehabilitation of a 75 year old female who underwent a posterior thoracic spine
(T9) to sacroiliac (S1) spinal fusion as a result of adult degenerative scoliosis and
prolonged back pain {Type 1 ). The purpose of this case report is to describe the
outpatient physical therapy treatment of this post-operative fusion and provide
outcomes with completion of long term goals.
4
History
CHAPTER II
CASE DESCRIPTION
The patient was a 75 year old retired and widowed female who had been
experiencing low back pain for 40+ years. Previously, she had not received any
medical attention to address her pain and symptoms. In 2013, she went to a
spine center and discovered she had Type 1 adult degenerative scoliosis. Patient
did not seek any treatment and instead dealt with the pain due to fear of surgery.
In 2017, her low back pain became so severe, she noticed her function and
independence was decreasing if not completely absent. She was unable to walk
a block, bend over to take dishes out of the oven and/or dishwasher, reach into
her cupboards, or even dress herself due to pain. The only position she was able
to find relief was in supine. She eventually stopped leaving her house and
attending community and social events due to intense pain. After weighing the
options, the patient and her orthopedic spine physician agreed upon surgery as
the best option to restore function and relieve pain.
In February 2018, the patient underwent a posterior thoracic spine (T9) to
sacroiliac spinal (S1) fusion. Before being initially evaluated at the outpatient
orthopedic clinic, the patient spent ten days in an acute care spine center
hospital, five weeks at a long term care rehabilitation center, and six weeks
5
receiving home health. Prior to surgery, the patient was independent and active
within her community. She participated in multiple book clubs, line dancing class,
deep water swimming class, and church related activities weekly. The patient
expressed the importance the social aspects her community activities brought to
her life.
Examination, Evaluation, and Diagnosis
Prior to meeting the patient, the outpatient front desk staff copied
information from the patient's referred chart into the clinics documentation
software system. Such information included; height, weight, past/current medical
history and medications. As found in the electronic medical record (EMR), the
patient was 5'5", weighing 190 lbs, which equated to a BMI of 31.6 (obese
category).13 The patient's past/current medical history included hypertension and
osteoporosis. The patient was currently taking medication that controlled
hypertension, calcium and vitamin D supplements to address osteoporosis, as
well as an anti-inflammatory for pain management associated with the fusion.
Upon observation, the patient presented to physical therapy standing in the
waiting room, alone, and ambulated with a slow, step-to gait pattern utilizing a
front wheeled walker. The patient was not wearing a thoracolumbosacral orthosis
(TLSO) brace, which she had been prescribed immediately after surgery. Patient
displayed a forward head posture with an endomorphic body stature.
The patient was referred to physical therapy to evaluate and treat. The
patient reported to lived alone in a single story home with no steps to negotiate
into or within her home. Since the patient lived alone, she reported to have
6
friends help her with activities of daily living that she was unable to complete. At
the time of initial evaluation, the patient was unable to fully sit or lie supine due to
pain and decreased range of motion and had to sit at the edge of an elevated
plinth. Similarly, the patient was prohibited to bend, twist, or lift more than 20 lbs
due to the spine surgeon's protocol. Thus, range of motion, resisted isometrics,
myotomes, and manual muscle testing for all motions of the spine and lower
extremity were deferred. Thoracic spine and lower extremity dermatomes tested
negative and equal bilateral. The incision site was healed but scar tissue
remained which measured 27.9 cm long by 1.5 cm wide. The patient was not
tender to palpation along the adhered incision site. The patient reported she had
an appointment with a massage therapist to address hypo-mobility of scar tissue.
The patient completed two functional outcome measures; The Modified
Oswestry Low Back Pain Disability Questionnaire and the Activities-specific
Balance Confidence (ABC) Scale. 14,15 The patient reported to be 74% impaired
as a result of the Modified Oswestry Low Back Pain Disability Questionnaire. 14
The patient reported to have 3.4% (<50% = low level of physical functioning) self
confidence as a result of the ABC scale. 15 Perceived level of pain was collected
using a visual analogue pain scale (VAS). The scale ranges from O to 10 with
zero being no pain and 10 being unbearable pain. The patient reported to have
6/10 pain at rest, 8/10 with motion, and 9/10 pain when attempting to bend. The
patient's complete and functional reported goals can be found in Table 1.
Physical therapy diagnosis found from the examination process included;
7
decreased mobility, decreased function, decreased range of motion, decreased
balance, lower extremity strength deficits, and pain.
Table 1. Patient Reported Goals
Goals 1. Following physical therapy intervention, the patient will be able to ambulate 4
miles/day without any assistive device in order to return to previous hobbies (9 weeks).
2. Following physical therapy intervention, the patient will be able to sit for one hour without pain in order to attend church services on Sundays (9 weeks).
3. Following physical therapy intervention, the patient will be able to stand for 2 hours without any pain in order to perform housework tasks independently (9 weeks).
4. Following physical therapy intervention, the patient will be able to get into/out of car independently in order to be able to complete grocery shopping independently (9 weeks).
Prognosis and Plan of Care
The total duration of physical therapy treatments could not surpass 9
weeks due to the patient's already purchased plane ticket to fly across the United
States to visit her family. The patient was actively involved in the plan of care
(POC) and treatments were determined to be 2x/week, 1 hour treatment
sessions, for 9 weeks with modifications if necessary or until goals were met The
patient was educated on the re-evaluation process for returning to physical
therapy once back home from her month long trip, if desired, but it was
anticipated that she would not need to return. Prognosis was good given the
patient's high level of motivation, age, health status and prior level of function.
Furthermore, this patient was appropriate for physical therapy and met the
physical therapist's scope of practice.
8
CHAPTER Ill
INTERVENTION
The patient was seen two times a week, with hour treatment sessions, for
a total of 9 weeks as per POC. In the first three weeks, interventions included
aquatic therapy treatments (Table 2). Aquatic treatments were completed in a
therapeutic pool (90 degrees) which featured a shallow (4 ft.) and deep (10 ft.)
end. Aquatic therapy allowed the patient to improve early range of motion and
strength by off-loading the spine. The Patient completed exercises while off
loading 50% of her body weight in the shallow end or with complete submersion
in the deep end while using a foam pool noodle as a floatation device.
Treatments were progressed based on patient tolerance by increasing time,
repetitions, sets, and intensity. Soft tissue mobilizations were completed once a
week for 30 minutes by a massage therapist located in the same outpatient clinic.
The massage therapist and physical therapist stayed in communication regarding
the advancement of skin integrity. By week two, the patient progressed from
presenting to physical therapy ambulating with her FWW to ambulating with
bilateral walking sticks.
9
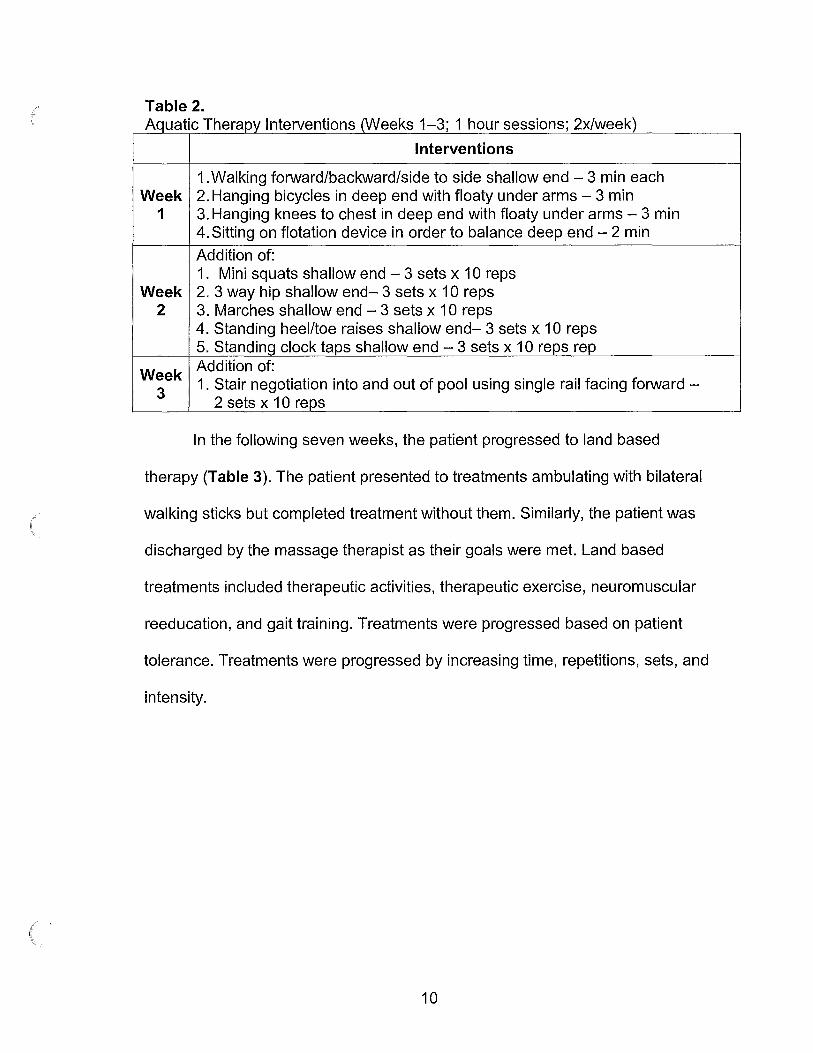
Table 2. Aquatic Therapy Interventions (Weeks 1-3; 1 hour sessions; 2x/week)
Interventions
1. Walking forward/backward/side to side shallow end - 3 min each Week 2. Hanging bicycles in deep end with floaty under arms - 3 min
1 3. Hanging knees to chest in deep end with floaty under arms - 3 min 4. Sitting on flotation device in order to balance deep end - 2 min
Addition of: 1. Mini squats shallow end - 3 sets x 10 reps
Week 2. 3 way hip shallow end- 3 sets x 10 reps 2 3. Marches shallow end - 3 sets x 10 reps
4. Standing heel/toe raises shallow end- 3 sets x 10 reps 5. Standing clock taps shallow end - 3 sets x 10 reps rep
Week Addition of:
3 1. Stair negotiation into and out of pool using single rail facing forward -
2 sets x 10 reps
In the following seven weeks, the patient progressed to land based
therapy (Table 3). The patient presented to treatments ambulating with bilateral
walking sticks but completed treatment without them. Similarly, the patient was
discharged by the massage therapist as their goals were met. Land based
treatments included therapeutic activities, therapeutic exercise, neuromuscular
reeducation, and gait training. Treatments were progressed based on patient
tolerance. Treatments were progressed by increasing time, repetitions, sets, and
intensity.
10
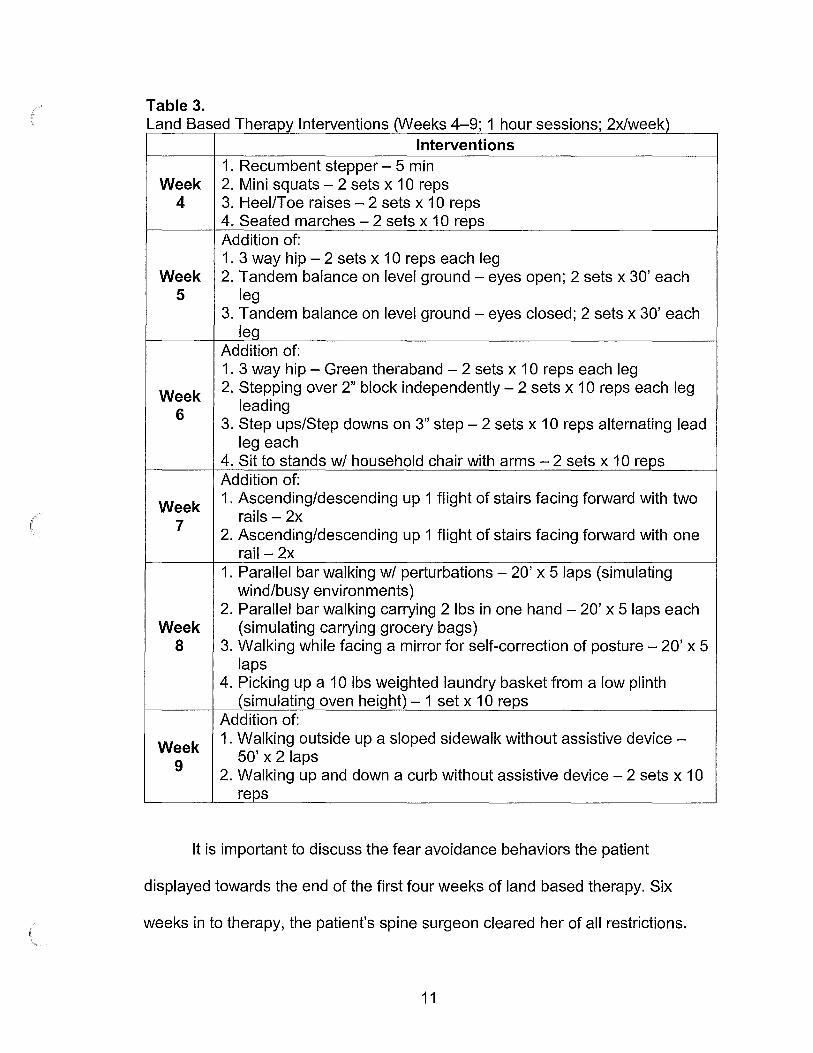
Table 3. Land Based Therapy Interventions (Weeks 4-9; 1 hour sessions; 2x/week)
Interventions 1. Recumbent stepper - 5 min
Week 2. Mini squats - 2 sets x 10 reps 4 3. Heel/Toe raises - 2 sets x 10 reps
4. Seated marches - 2 sets x 10 reps Addition of: 1. 3 way hip - 2 sets x 10 reps each leg
Week 2. Tandem balance on level ground - eyes open; 2 sets x 30' each 5 leg
3. Tandem balance on level ground - eyes closed; 2 sets x 30' each leg
Addition of: 1. 3 way hip - Green theraband - 2 sets x 10 reps each leg
Week 2. Stepping over 2" block independently - 2 sets x 10 reps each leg
6 leading
3. Step ups/Step downs on 3" step - 2 sets x 10 reps alternating lead leg each
4. Sit to stands w/ household chair with arms - 2 sets x 10 reps Addition of:
Week 1. Ascending/descending up 1 flight of stairs facing forward with two
7 rails - 2x 2. Ascending/descending up 1 flight of stairs facing forward with one
rail-2x 1. Parallel bar walking w/ perturbations - 20' x 5 laps (simulating
wind/busy environments) 2. Parallel bar walking carrying 2 lbs in one hand - 20' x 5 laps each
Week (simulating carrying grocery bags) 8 3. Walking while facing a mirror for self-correction of posture - 20' x 5
laps 4. Picking up a 10 lbs weighted laundry basket from a low plinth
(simulating oven height) - 1 set x 10 reps Addition of:
Week 1. Walking outside up a sloped sidewalk without assistive device -
9 50' x 2 laps
2. Walking up and down a curb without assistive device - 2 sets x 10 reps
It is important to discuss the fear avoidance behaviors the patient
displayed towards the end of the first four weeks of land based therapy. Six
weeks in to therapy, the patient's spine surgeon cleared her of all restrictions.
11
Unbeknownst to the physical therapist, the patient reported to still be using her
walker to ambulate to the bathroom at night, using the bench of her walker to
carry her laundry basket while ambulating, ambulating community distances with
her bilateral walking sticks, and completing other functional tasks at a level below
her true physical capabilities. The patient was educated on the importance of
challenging herself functionally and not relying on assistive devices because she
was cleared of all restrictions and was physically capable. In turn, the patient
presented to physical therapy without the use of her bilateral walking sticks the
following treatment. The last three weeks of treatments (seven, eight, and nine)
focused solely on simulating functional activities that the patient reported to be
afraid to complete. These activities included stepping up and down curbs without
using walking sticks, ambulating in busy grocery stores, ambulating in windy
environments without her walking sticks, ambulating within her house carrying
her laundry basket, loading/unloading the dishwasher, and negotiating stairs with
and without railings in buildings where her community activities were located.
12
CHAPTER IV
OUTCOMES
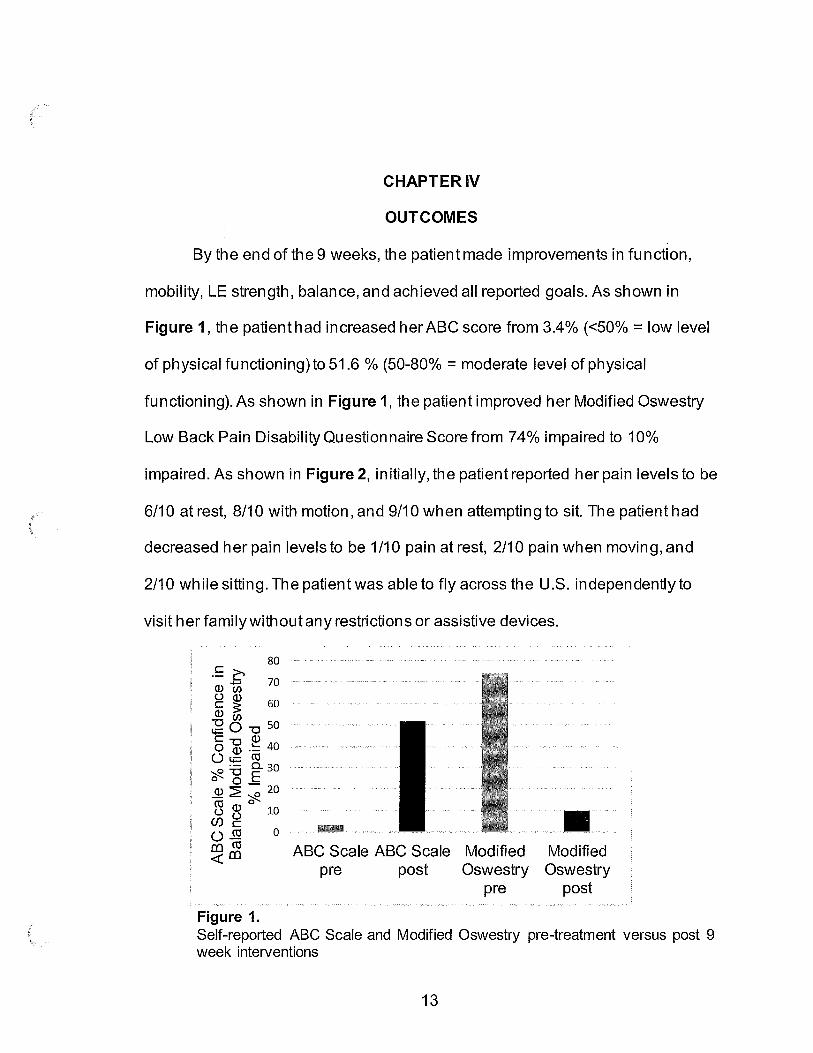
By the end of the 9 weeks, the patient made improvements in function,
mobility, LE strength, balance, and achieved all reported goals. As shown in
Figure 1, the patient had increased her ABC score from 3.4% (<50% = low level
of physical functioning)to 51.6 % (50-80% = moderate level of physical
functioning). As shown in Figure 1, the patient improved her Modified Oswestry
Low Back Pain Disability Questionnaire Score from 74% impaired to 10%
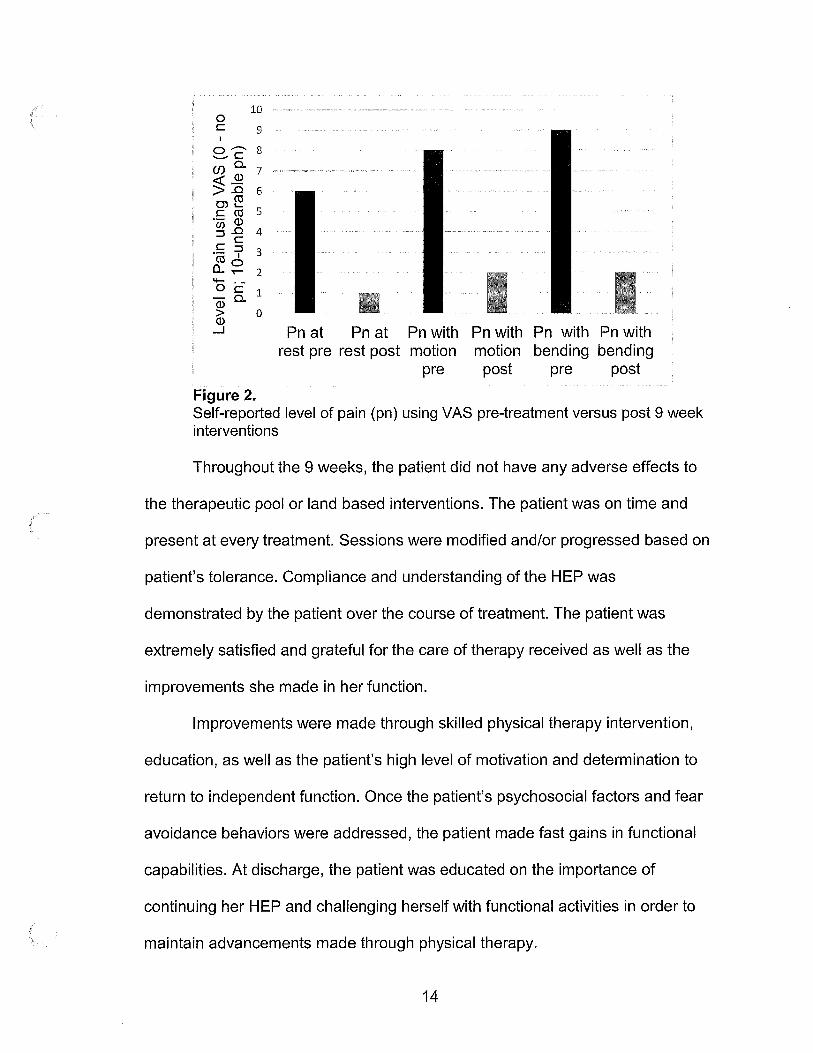
impaired. As shown in Figure 2, initially, the patient reported her pain levels to be
6/10 at rest, 8/10 with motion, and 9/10 when attempting to sit. The patient had
decreased her pain levels to be 1/10 pain at rest, 2/10 pain when moving, and
2/10 while sitting. The patient was able to fly across the U.S. independently to
visit her family without any restrictions or assistive devices.
80 £c (]) 00 70
g ~ 60 (]) (J)
;g O "O 50 C "O (]) 0 (]) .!:: 40
(_) t;::: cu ~ ~ Eo.. 30 0 0 -(]) ~ ~ 20
~ ~ 0 10 (/) C (_) CU 0 co cu <( co
Figure 1.
■ ABC Scale ABC Scale Modified Modified
pre post Oswestry Oswestry pre post
Self-reported ABC Scale and Modified Oswestry pre-treatment versus post 9 week interventions
13
(
10 0 C 9
I
8'28 CJ) Q. 7 ~~ > .0 6 O)~ C CO 5 ·- (]) CJ) .0 4 ::::IC
,!:; =? 3 co 0 a. ..- 2 4-
0 C i a3 a. > 0 (])
...J
Figure 2.
Pn at Pn at Pn with Pn with Pn with Pn with rest pre rest post motion motion bending bending
pre po~ pre po~
Self-reported level of pain (pn) using VAS pre-treatment versus post 9 week interventions
Throughout the 9 weeks, the patient did not have any adverse effects to
the therapeutic pool or land based interventions. The patient was on time and
present at every treatment. Sessions were modified and/or progressed based on
patient's tolerance. Compliance and understanding of the HEP was
demonstrated by the patient over the course of treatment. The patient was
extremely satisfied and grateful for the care of therapy received as well as the
improvements she made in her function.
Improvements were made through skilled physical therapy intervention,
education, as well as the patient's high level of motivation and determination to
return to independent function. Once the patient's psychosocial factors and fear
avoidance behaviors were addressed, the patient made fast gains in functional
capabilities. At discharge, the patient was educated on the importance of
continuing her HEP and challenging herself with functional activities in order to
maintain advancements made through physical therapy.
14
CHAPTERV
DISCUSSION
Operative treatments are on the increase because the demand for quality
of life is increased and surgical techniques are improved.2 Spine surgery
involving decompression and fusion is safe and recommended in the setting of
degenerative scoliosis treatment.3 Even for patients 75 years and older, surgery
provides significant improvements. After long level fusion, ADLs can be impaired
but gradually improved over time.2 This patient's ADLs were greatly impaired
following a T9 - S 1 fusion and did return as time passed with the aid of physical
therapy intervention and determination from the patient.
Factors such as fear of movement and low self-efficacy are identified as
barriers to physical activity.7 Fear avoidance beliefs may play a significant role in
the outcome of surgery for adult degenerative scoliosis. There is a strong
correlation that movement will increase pain and the individual avoids moving. 6
The movement may or may not create pain, but the fear of producing pain is the
main factor limiting mobility. This patient used shortcuts and assistive devices to
complete functional tasks because she wasn't aware of her therapeutic gains.
She was stuck on the fear of producing pain while completing these tasks
independently which prevented her from trying them. Once she was educated on
this concept and worked on functional activities, she became aware that she
15
could physically do these tasks without pain and that the mentality of fear was
the driving forces preventing movement.
Aquatic exercise may have advantages in acute therapy compared to
land-based exercise due to the physical properties of water. The execution of the
movements can become easier, decreasing also the sensation of pain. 8
Introducing this patient to aquatic therapy in the early phases of treatment proved
beneficial and promoted early increases in range of motion and mobility due to
the characteristics and buoyancy water possesses. Similarly, off-loading the
patient's body weight made it possible for her to complete treatment with
decreased pain levels.
Currently, there is no minimal detectable change to compare the ABC
scale to, as there is no gold standard for a subjective questionnaire such as
this. 16 Perceived physical capabilities rather than actual physical abilities is more
predictive of completing a behavior. Working on the functional tasks that the
patient was unconfident to complete, made her more confident. The patient self
reported to have an increased confidence in daily activities by 48%. According to
the Modified Oswestry Low Back Pain Disability Questionnaire score sheet, the
minimum detectable change (90% confidence) is a decrease of 10% impairment.
The patient had a decrease of 64% impairment indicating clinical change. Lastly,
pain is subjective and perceived differently for every individual. The patient had a
decrease in pain by an average of 6 points. Based on this author's clinical
judgement and feedback from the patient, the patient made clinical
16
improvements in decreased level of pain from initial evaluation to the time of
discharge.
Health care providers should strive to base treatment around functional
tasks. Individuals may be able to complete therapeutic exercise and activities,
but this does not equate to direct cross over to functional demands. As
demonstrated with this patient, once treatments focused around functional tasks,
the individual's confidence and mentality greatly improved. The patient was able
to prove to herself that she was physically capable of completing functional tasks
that she perceived she was not capable of completing.
The outcome of this patient's 9 week experience proved to be
encouraging. Promoting early off-loading in aquatic settings and transitioning to
land based therapy, understanding the psychosocial factors associated with fear
avoidance behaviors, utilizing multiple functional outcome measures to assess
clinical change, and adapting treatments to the individual are key components of
a successful outcome. Based on the outcome of this patient, this case report can
be used as a reference for an outpatient rehabilitation process of an individual
following a multilevel spinal fusion due to Type 1 scoliosis.
17
Reflective Practice
The outcome of this case report, as stated in the discussion, was
encouraging given the lack of research on this topic. However, there are some
areas in which I would have done differently. One of these areas being -
addressing the patient's psychosocial factors much sooner compared to when
they were addressed in real life. Knowing that the patient's POC was set at 9
weeks due to her pre-purchased plane ticket, there were many goals we (the
therapist and patient) were trying to accomplish in a short period of time. The
patient's fear-avoidance behaviors could have had a negative impact on her
outcome if they were never addressed. Luckily, they were addressed in an
appropriate amount of time, but potentially addressing these factors sooner
would have been more beneficial for the patient's quality of life.
The experience and process of this case report will positively impact my
future practice. This case report taught me the importance of embodying
evidence based practice as well as centering treatments around the patient.
Every individual is unique and different and there is not one formula that works
for everyone. There are many factors to consider when developing treatments
and a plan of care. This patient instilled in me the need to address health as a
whole. Enhancing health must focus on all components of the mind, body, soul,
and understanding the multidirectional relationship between physical, emotional,
and psychological factors. Similarly, this case helped me to create my PT
18
practice philosophy. Given the little research on this topic as a whole,
administering a wide range of "tools" that do have evidence based outcomes is
important. As a future clinician, I will strive to utilize a variety of techniques to
help promote a successful outcome and this patient's complexity helped me
understand the necessity of this concept.
Limitations of this case report include; lack of research on the
rehabilitation protocol per this diagnosis, potential alternative outcomes following
a patient with comorbidities, and failure to understand the maintenance of this
patient's advancements made through physical therapy long term. Following a
standardized protocol possesses many benefits as health care providers are able
to provide evidence based practice, speed recovery time, and decrease health
care associated costs. This patient did not possess any comorbidities. At this
time, it is unclear as to whether following a patient with comorbidities would
negatively impact the outcome or how said comorbidities would affect POC,
clinical judgement, and treatment activities/progressions. Finally, this case report
did not conduct any follow up treatments assessing the patient's function after
discharge. Perhaps, a six month follow up would show 100% return to function or
indicate a need for a longer POC.
19
REFERENCES
1. Aebi M. The adult scoliosis. Eur Spine J. 2005;14(10):925-948. Accessed Jun 25, 2019. doi: 10.1007/s00586-005-1053-9.
2. Kim WJ, Lee JW, Hwang SY, et al. Activity of daily living after long level fusion in adult spinal deformity: Compared with over 60-year-old degenerative spine patients without adult spinal deformity. Spine. 2018;43(23):1638-1647. Accessed Jun 25, 2019. doi: 10.1097/BRS.0000000000002676.
3. Phan K, Xu J, Maharaj MM, et al. Outcomes of short fusion versus long fusion for adult degenerative scoliosis: A systematic review and meta-analysis. Ortho Surg. 2017;9(4):342-349. https://onlinelibrary.wiley.com/doi/abs/10.1111/os.12357. doi: 10.1111/os.12357.
4. Orthoinfo.aaos.org. (2019). Spinal Fusion - Ortholnfo -AAOS. [online] Available at: https://orthoinfo.aaos.org/en/treatment/spinal-fusion/ [Accessed 25 Jun. 2019].
5. Gatchel RJ, Neblett R, Kishino N, Ray CT. Fear-avoidance beliefs and chronic pain. The J Orthop Sports Phys. 2016;46(2):38-43. https :/ /www.ncbi.nlm.nih.gov/pubmed/2682823 6. doi: 10 .2519 /j ospt.2016.0601.
6. Haddas R, Lieberman IH, Block A. The relationship between fear-avoidance and objective biomechanical measures of function in patients with adult degenerative scoliosis. Spine. 2018;43(9):647-653. Accessed Jun 25, 2019. doi: IO .1097 /BRS. 00000000000023 81.
7. Lotzke H, Jakobsson M, Gutke A, et al. Patients with severe low back pain exhibit a low level of physical activity before lumbar fusion surgery: A cross-sectional study. BMC Musculoskelet Disord. 2018;19(1):365. Accessed Jun 25, 2019. doi: 10. l 186/s12891-018-2274-5.
8. Mattos Fd, Leite N, Pitta A, Bento PCB. Effects of aquatic exercise on muscle strength and functional performance of individuals with osteoarthritis: A systematic review. Rev Bras Reumatol Engl Ed. 2016;56(6):530-542. Accessed Jun 25, 2019. doi: 10.1016/j.rbre.2016.09.003.
9. Steffen T, Seney M. Test-retest reliability and minimal detectable change on balance and ambulation tests, the 36-item short-form health survey, and the unified parkinson disease rating scale in people with parkinsonism. Phys Ther. 2008;88( 6):733-746. https:/ /academic.oup.com/ptj/article/88/6/733/27423 l 7. Accessed Jun 25, 2019. doi: 10.2522/ptj.20070214.
10. Haley SM, Fragala-Pinkham MA. Interpreting change scores of tests and measures used in physical therapy. Phys Ther. 2006;86(5):735-743. https://academic.oup.com/ptj/article/86/5/735/2857473. Accessed Jun 25, 2019. doi: 10.1093/ptj/86.5.735
11. Raad, Jason, MSIMoore, Jennifer, PT, DHS, NCSIHamby, Julie, SPTJRivadelo, Ryan Lainez, SPTIStraube, Don, PT, PhD, NCS. A briefreview of the activitiesspecific balance confidence scale in older adults. Arch Phys Med Rehab. 2013;94(7): 1426-1427. https://www.clinicalkey.es/playcontent/1-s2.0-S00039993 l3003663. doi: 10.1016/j.apmr.2013.05.002.
12. Lee C, Fu T, Liu C, Hung C. Psychometric evaluation of the oswestry disability index in patients with chronic low back pain: Factor and mokken analyses. Health
20
I \
Qua! Life Out. 2017;15(1):192-7. https://www.ncbi.nlm.nih.gov/pubmed/28974227. doi: 10.l 186/s12955-017-0768-8.
13. Nhlbi.nih.gov. (2019). Calculate Your BMI - Standard BMI Calculator. [online] Available at: https :/ /www.nhlbi.nih.gov/health/ educational/lose_ wt/BMI/bmicalc.htm [Accessed 25 Jun. 2019].
14. St-marys.org. (2019). [ online] Available at: https:/ /www.stmarys.org/assets/pdfs/2017 /back-pain-questionnaire.pdf [ Accessed 25 Jun. 2019].
15. Drayerpt.com. (2019). [online] Available at: https :// drayerpt.com/ content/uploads/2015/10/Balance-Gait-Falls-ABC-Scale. pdf [Accessed 25 Jun. 2019].
16. Steffen T. Activities-Specific Balance Confidence (ABC) Scale. https:/ /pdfs.semanticscholar.org/172a/3dbe594a09108933701 aa3de9c20b4a98206 .pdf. 2012. [Accessed 25 Jun. 2019].
21